Orthopedic Board Exam Set 703: 100 High-Yield Ortho MCQs
14 Apr 2026
100 min read
107 Views
Key Takeaway
This page offers Mock Exam Set #703, with 100 high-yield Orthopedic Surgery Multiple Choice Questions. Tailored for ABOS, OITE, and FRCS board exams, these MCQs help surgeons master critical concepts, ensuring effective preparation and success for their certification exams.
Posterior Approach: Safe Access to Thoracic a...
00:00
Start Quiz
Question 1High Yield
Linazolid exerts its antimicrobial action by inhibiting bacterial
Explanation
Linazolid is the first agent of the oxazolidinone group of antibiotics and is very active against methicillin-sensitive Staphylococus aureus, S epidermidis, and vancomycin-resistant enterococci. The drug has no gram-negative activity. Linazolid inhibits protein synthesis by blocking formation of the 70S ribosomal translation complex. This mechanism of action is unique to the oxazolidinones. Rybak MJ, Cappelletty DM, Moldovan T, et al: Comparative in vitro activities and postantibiotic effects of the oxazolidinone compounds eperezolid (PNU-100592) and linezolid (PNU-100766) versus vancomycin against Staphylococcus aureus, coagulase-negative staphylococci, Enterococcus faecalis, and Enterococcus faecium. Antimicrob Agents Chemother 1998;42:721-724.
Question 2High Yield
What property of titanium alloys accounts for their high corrosion resistance in vivo?
Explanation
Explanation
In both room temperature air and physiologic fluids, titanium alloys self-passivate or spontaneously form a layer of titanium oxide very rapidly. This layer makes titanium alloys resistant to surface breakdown. Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, Lippincott, 2003, vol 1, pp 269-278.
References:
- Lemons JE: Metallic alloys, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 19-27.
Question 3High Yield
Which of the following have been found to affect the rate of perioperative infections or wound complication rates in foot and ankle surgery?
Explanation
Explanation
Clinical studies have shown that smoking cessation for 4 weeks reduces the risk of infection to the level of nonsmokers. Adverse effects on wound healing caused by chemotherapy used to treat rheumatoid arthritis has not been borne out in the literature. Bibbo C, Anderson RB, Davis WH, et al: The influence of rheumatoid chemotherapy, age, and presence of rheumatoid nodules on postoperative complications in rheumatoid foot and ankle surgery: Analysis of 725 procedures in 104 patients. Foot Ankle Int 2003;24:40-44. Bibbo C, Goldberg JW: Infections and healing complications after elective orthopaedic foot and ankle surgery during tumor necrosis factor-alpha inhibition therapy. Foot Ankle Int 2004;25:331-335.
Question 4High Yield
Which of the following illustrations shown in Figures 21a through 21e correctly shows the projection of the sacroiliac joint on the outer table of the ilium?
Explanation
Explanation
21b 21c 21d 21e The projection of the sacroiliac joint on the outer surface of the ilium should be well understood to avoid violation of the joint during bone graft harvesting and to help in insertion of the screw across the joint. The sacroiliac joint has superior and inferior limbs. The average lengths of the superior and inferior limbs are 4.4 cm and 5.6 cm, respectively. The average width of each limb is 2.0 cm. The average distance from the longitudinal axis of the superior limb to the posterior superior iliac spine is 5.5 cm. The average longitudinal axis of the inferior limb is 1.2 cm superior to the inferior margin of the posterior inferior iliac spine. The average angle between the two axes is 93 degrees. Figure 21c most closely shows the projection of the sacroiliac joint on the outer table of the ilium. Waldrop JT, Ebraheim NA, Yeasting RA, Jackson WT: The location of the sacroiliac joint on the outer table of the posterior ilium. J Orthop Trauma 1993;7:510-513.
References:
- Xu R, Ebraheim NA, Yeasting RA, Jackson WT: Anatomic considerations for posterior iliac bone harvesting. Spine 1996;21:1017-1020.
Question 5High Yield
Figure 35 shows the AP radiograph of a patient who underwent a previous upper tibial osteotomy (UTO). The patient may be at risk for which of the following during total knee arthroplasty (TKA)?
Explanation
Explanation
The results of TKA for patients with a prior UTO are reported to be slightly suboptimal. The major problems are patella baja, difficulty in exposure, and instability. Most of the patients exhibit some degree of instability prior to TKA, and ligamentous balancing may be difficult. Ligamentous structures are at risk of rupture during the difficult exposure. The problem of ligamentous balancing is exacerbated by the change in the joint slope that can occur after UTO. Parvizi J, Hanssen AD, Spangehl MJ: Total knee arthroplasty following proximal tibial osteotomy: Risk factors for failure. J Bone Joint Surg Am 2004;86:474-479.
References:
- Meding JB, Keating EM, Ritter MA, et al: Total knee arthroplasty after high tibial osteotomy: A comparison study in patients who had bilateral total knee replacement. J Bone Joint Surg Am 2000;82:1252-1259.
Question 6High Yield
Figures 23a and 23b show the radiographs of a 75-year-old woman who sustained an injury to her nondominant hand. Initial treatment should consist of
Explanation
Explanation
23b Definitive treatment decisions for displaced distal radius fractures in the elderly are based on a number of factors related to the fracture pattern and patient demographics. The first step in any treatment algorithm is a closed reduction and splinting with reassessment of alignment parameters. This is an extra-articular fracture with dorsal angulation. Low-demand elderly patients can be treated well with accepted minor malreduction. Handoll HH, Madhok R: Conservative interventions for treating distal radial fractures in adults. Cochrane Database Syst Rev 2003;2:CD000314.
Question 7High Yield
A 32-year-old man has posttraumatic arthritis after undergoing open reduction and internal fixation of a left acetabular fracture. A total hip arthroplasty is performed, and the radiograph is shown in Figure 18. What is the most common mode of failure leading to revision in this group of patients?
Explanation
Explanation
Acetabular component loosening has been reported as the most common mode of failure following total hip arthroplasty in patients with a previous acetabular fracture. Following acetabular fracture and subsequent open reduction and internal fixation, the bone quality and vascularity are compromised, thus reducing the success rate of acetabular component cementless fixation. Jimenez ML, Tile M, Schenk RS: Total hip replacement after acetabular fracture. Orthop Clin 1997;28:435-446.
References:
- Romness DW, Lewallen DG: Total hip arthroplasty after fracture of the acetabulum: Long-term results. J Bone Joint Surg Br 1990;72:761-764.
Question 8High Yield
A female cross-country runner has an insidious onset of right groin pain. Radiographs of the right hip reveal a tension-side stress fracture. History reveals that she was treated for a "foot" fracture 1 year ago. In addition to performing internal fixation of the femoral neck, which of the following should be obtained?
Explanation
Explanation
Stress fractures in female long distance runners are frequently associated with the Female Athletic Triad. The triad consists of osteoporosis, amenorrhea, and altered eating habits. A thorough menstrual history, including age of menarche, history of amenorrhea, and use of oral contraceptives, is imperative. Amenorrhea leads to osteoporosis and predisposes the athlete to fractures. An MRI of the hip is not necessary because a fracture is evident on the radiograph. Serum calcium levels are normal in osteoporosis, a family history would be noncontributory, and it is highly unlikely that a contralateral hip radiograph will yield useful information. Bennell KL, Malcolm SA, Thomas SA, et al: Risk factors for stress fractures in track and field athletes: A twelve-month prospective study. Am J Sports Med 1996;24:810-818.
References:
- Barrow GW, Saha H: Menstrual irregularity and stress fractures in collegiate female distance runners. Am J Sports Med 1988;16:209-216.
Question 9High Yield
What is the primary limiting membrane and mechanical support for the periphery of the physis?
Explanation
The perichondrial fibrous ring of La Croix acts as a limiting membrane that provides mechanical support for the bone-cartilage junction of the growth plate. It is continuous with the ossification groove of Ranvier, which contributes chondrocytes for the increase in width of the growth plate. The zone of provisional calcification lies at the bottom of the hypertrophic zone and is the site of initial calcification of the matrix. It is quite weak and usually is the cleavage plane for fractures; therefore, it does not qualify as mechanical support. The last intact transverse septum separates the zone of provisional calcification from the primary spongiosa and provides no real support to the physis. The primary spongiosa is the part of the metaphysis nearest the physis. Netter FH: Growth plate, in Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 166-167.
Question 10High Yield
Which of the following structures are found in the anterior tarsal tunnel?
Explanation
The contents of the anterior tarsal tunnel are the extensor hallucis longus, tibialis anterior, extensor digitorum longus, dorsalis pedis artery, and the deep peroneal nerve. The term "anterior tarsal tunnel syndrome" is used to specifically describe the compression of the deep peroneal nerve under the inferior extensor retinaculum. With nerve compression, patients report a burning sensation across the dorsum of the foot with paresthesias in the first web space. There also may be wasting and weakness of the extensor digitorum brevis. Kuritz HM: Anterior entrapment syndromes. J Foot Surg 1976;15:143-148.
Question 11High Yield
Radiographs of an 80-year-old woman with back pain reveal a compression fracture. Which of the following imaging studies best evaluates the acuity of the fracture?
Explanation
The best method of evaluating the acuity of osteoporotic compression fractures is to look for edema in the vertebral body. This is best accomplished with a STIR-weighted MRI scan. Bone scans can show increased uptake at the site of fracture for many months after the fracture. T1-weighted MRI scans show loss of normal marrow fat that may not necessarily correspond with acuity of the fracture. CT scans and radiographs show fracture deformity but cannot be used to judge acuity. Phillips FM: Minimally invasive treatments of osteoporotic vertebral compression fractures. Spine 2003;28:S45-S53.
Question 12High Yield
A 45-year-old man who smokes reports the rapid onset of color changes and coolness in the fingers. Examination shows an abnormal Allen test. Plain radiographs of the hand and wrist are normal. Which of the following studies will best aid in diagnosis?
Explanation
The patient has symptoms typical of Raynaud's phenomenon secondary to underlying vascular disease. The next most appropriate step in the management of this patient should be to perform contrast angiography on the involved upper extremity to look for proximal or distal arterial lesions or insufficiencies. MRI and contrast CT are not as specific as angiography for the identification of vascular lesions of the upper extremity. Although patients with primary Raynaud's vasospastic disease can have normal angiographic findings, they typically are younger than age 40 years, are female, and have normal results on an Allen test. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2288-2290.
Question 13High Yield
Which of the following types of displaced posterior pelvic disruptions must undergo anatomic reduction and internal fixation to ensure the best clinical outcome?
Explanation
Although all of the above displaced injuries require reduction, the sacroiliac joint dislocation is a ligamentous injury. Without fixation, healing is unlikely and the result will be a painful dislocation. Both Holdsworth and Tile showed that the sacroiliac joint must be reduced anatomically and stabilized. The injuries through bone will unite fairly rapidly and, if reduced and stabilized with traction or external fixation, will generally result in an acceptable outcome unless modified by other associated problems such as neurologic injury. Tile M: Fractures of the Pelvis and the Acetabulum. Baltimore, MD, Williams and Wilkins, 1995. Holdsworth F W: Dislocation and fracture dislocation of the pelvis. J Bone Joint Surg Br 1948;30:461-465.
Question 14High Yield
After making a tackle, a football player is found prone and unconscious without spontaneous respirations. Initial management should consist of
Explanation
The on-field evaluation and management of a seriously injured athlete requires that health care teams have a game plan in place and proper equipment that is readily available. The initial step, which consists of stabilizing the head and neck by manually holding them in a neutral position, is then followed by assessment of breathing, pulses, and level of consciousness. If the athlete is breathing, management should consist of mouth guard removal and airway maintenance. If the athlete is not breathing, the face mask should be removed, with the chin strap left in place. The airway must be established, followed by initiation of assisted breathing. CPR is instituted only when breathing and circulation are compromised. In the unconscious athlete or if a cervical spine injury is suspected, the helmet must not be removed until the athlete has been transported to an appropriate facility and the cervical spine has been completely evaluated. McSwain NE, Garnelli, RL: Helmet removal from injured patients. Bull of Am Coll Surg 1997;82:42-44.
Question 15High Yield
A 62-year-old man with a long history of ankylosing spondylitis has neck pain after lightly bumping his head on the wall. Examination reveals neck pain with any attempted motion; the neurologic examination is normal. Plain radiographs show extensive ankylosis of the cervical spine and kyphosis but no fracture. What is the next most appropriate step in management?
Explanation
A high level of suspicion must be given for a fracture in any patient with ankylosing spondylitis who reports neck pain, even with minimal or no trauma. The neck should be immobilized in its normal position, which is often kyphotic, and plain radiographs should be obtained. If no obvious fracture is seen, CT with reconstruction should be obtained. The placement of in-line traction can have catastrophic effects because it may malalign the spine. Brigham CD: Ankylosing spondylitis and seronegative spondyloarthropathies, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 724-727.
Question 16High Yield
An 8-year-old boy is diagnosed with acute onset cauda equina syndrome. A radiograph, MRI scans, and a biopsy specimen are shown in Figures 57a through 57d. What is the most appropriate treatment?
Explanation
Explanation
57b 57c 57d The findings are consistent with an aneurysmal bone cyst. The MRI scan demonstrates a lesion involving the posterior elements of the vertebrae with fluid-fluid levels and neural compression. Fibrovascular tissue with multinucleated giant cells surrounding a vascular lake is seen on the histology. The most appropriate treatment is a marginal resection of the involved posterior elements. Although the recurrence rate can be as high as 25% to 30%, wide surgical resection could result in permanent neurologic injury and is not necessary. Aspiration and steroid injection have been advocated but would not relieve the nerve compression in this patient. Radiation therapy and chemotherapy are not indicated. Mankin HJ, Hornicek FJ, Ortiz-Cruz E, et al: Aneurysmal bone cyst: A review of 150 patients. J Clin Oncol 2005;23:6756-6762.
References:
- Garg S, Mehta S, Dormans JP: Modern surgical treatment of primary aneurysmal bone cyst of the spine in children and adolescents. J Ped Orthop 2005;25:387-392.
Question 17High Yield
An 18-year-old high school football player sustains a left posterior hip dislocation that is reduced in the emergency department under IV sedation. Postreduction radiographs reveal a concentric reduction with no evidence of fracture or loose bodies within the joint. What is the most common complication of hip dislocations?
Explanation
Explanation
Traumatic dislocation of the hip in sports injuries is uncommon, and 85% to 92% occur in a posterior direction. In dislocations without fractures, osteonecrosis is the most common complication occurring in 10% to 20% of patients. MRI should be performed at 3 months postreduction to rule out osteonecrosis. Nerve injuries are rare in this setting, and recurrent dislocations are unusual without acetabular fractures. Chondrolysis has been reported as a rare occurrence. Anderson K, Strickland S, Warren R: Hip and groin injures in athletes. Am J Sports Med 2001;29:521-533.
References:
- Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 407-416.
Question 18High Yield
Which of the following findings is the best radiographic indicator of segmental instability at L4-L5?
Explanation
Explanation
Motion segments that demonstrate more than 4 mm of translation or 10 degrees of angulation compared with adjacent motion segments on flexion-extension radiographs have excessive motion and instability. Anterior marginal osteophytes form at the insertion of the annulus from increased forces but do not indicate increased motion. A spondylolisthesis or lateral listhesis is often static without increased motion. More than 3.5 mm of translation or 11 degrees of angulation is considered instability criteria for the cervical spine. Internal disk disruption does not denote instability. Boden SD, Wiesel SW: Lumbosacral segmental motion in normal individuals. Have we been measuring instability properly? Spine 1990;15:571-576.
References:
- Garfin SR, Rauschning W: Spinal stenosis. Instr Course Lect 2001;50:145-152.
Question 19High Yield
An 8-year-old girl injures her elbow playing soccer. After attempted reduction in the emergency department, radiographs of the elbow are shown in Figures 35a through 35c. What is the next most appropriate step in treatment?
Explanation
Explanation
35b 35c Ninety percent of injuries to the proximal radius in children are radial neck fractures, and 50% of these fractures are through the metaphyseal bone. The remaining 50% are Salter-Harris type I or II fractures. These radiographs show a fracture of the radial head and subluxation of the radius anteriorly. Most congenital radial head dislocations are posterior lateral. Nonsurgical treatment modalities are unlikely to be successful due to the wide displacement of the fracture fragments, as well as dislocation of the radial head. Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop 2000;20:7-14. Hashemi-Nejad A, Goddard NJ: Radial head fractures. Br J Hosp Med 1994;51:223-226.
Question 20High Yield
Figures 17a and 17b show the AP and lateral radiographs of a 75-year-old woman who reports giving way and shifting of the knee, particularly when she is descending stairs or ambulating on level surfaces. History reveals a total knee replacement 5 years ago. Treatment should consist of

Explanation
The radiographs show well-fixed components of a posterior cruciate-retaining total knee replacement. The relative position of the femoral component is anteriorly subluxated relative to the tibial component. The AP radiograph shows that the articular space is markedly asymmetric, indicating either failure or fracture of the polyethylene or subluxation of the femur relative to the tibia. The patient's symptoms suggest a failure of the posterior cruciate ligament that is consistent with the radiographic findings; therefore, the treatment of choice is revision to a posterior cruciate-substituting implant.
Question 21High Yield
When planning scoliosis surgery for a patient with a 50-degree thoracolumbar curve and spinal muscular atrophy, it is most important to include
Explanation
Typically, posterior spinal fusion to the pelvis is recommended for patients with spinal muscular atrophy and advanced scoliosis. Examination for lower extremity muscle contractures is important because the contractures may interfere with good sitting balance. Anterior release and fusion usually are not advised. Diaphragmatic pacing is not indicated because diaphragm function usually is not affected. Patients with spinal muscular atrophy usually are not ambulatory or only marginally ambulatory at the time of scoliosis surgery; therefore, gait analysis usually is not relevant. While a muscle biopsy may have a role in the diagnosis of this disorder, it plays no subsequent role in determining life expectancy or the value of spinal surgery. Daher YH, Lonstein JE, Winter RB, Bradford DS: Spinal surgery in spinal muscular atrophy. J Pediatr Orthop 1985;5:391-395.
Question 22High Yield
A 40 year-old-man was involved in a motor vehicle accident and sustained the pelvic injury seen in Figures 24a and 24b. Definitive management of the injury should consist of reduction by
Explanation
Explanation
24b The radiograph reveals disruption of the symphysis pubis and a displaced left sacral fracture. A posterior injury with displacement of greater than 1 cm is unstable, and a sacral fracture is particularly unstable. Surgical stabilization is required for these unstable anterior and posterior injuries. External fixation provides little stability to an unstable posterior pelvic injury. Reduction and internal fixation of the symphysis pubis and sacral fracture will provide the most stable pelvis with the least resultant deformity and allow patient mobilization. Tile M: Management of pelvic ring injuries, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 168-202.
References:
- Kabak S, Halici M, Tuncel M, et al: Functional outcome of open reduction and internal fixation for completely unstable pelvic ring fractures (type C): A report of 40 cases. J Orthop Trauma 2003;17:555-562.
Question 23High Yield
A left-handed 23-year-old man who fell 5 feet from a ladder onto his left elbow sustained the closed injury shown in Figure 26. Management should consist of
Explanation
Explanation
The radiographs reveal a displaced olecranon fracture. To maximize joint congruity of this intra-articular injury, open reduction and internal fixation is the treatment of choice. A tension band plate will assist with maintenance of the reduction and may aid in early range of motion because injuries to the elbow are prone to stiffness. The oblique fracture line is particularly well suited to plate fixation. Percutaneous pin fixation is unlikely to achieve anatomic joint reduction that can be obtained with open means. External immobilization will not accomplish joint reduction and will most likely lead to a nonunion. Hotchkiss RN: Fractures and dislocations of the elbow, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 929-1024. Murphy DF, Greene WB, Gilbert JA, Dameron TB Jr: Displaced olecranon fractures in adults: Biomechanical analysis of fixation methods. Clin Orthop 1987;224:210-214.
References:
- Hume MC, Wiss DA: Olecranon fractures: A clinical and radiographic comparison of tension band wiring and plate fixation. Clin Orthop 1992;285:229-235.
Question 24High Yield
What is the most common location of osteosarcoma?
Explanation
Explanation
The most common location of osteosarcoma is the knee area (50% to 55%), followed by the proximal humerus and iliac wing. The most commonly involved long bone is the femur (40% to 45%), followed by the tibia (15% to 25%). Within these bones, tumors are typically adjacent to the epiphyses in most patients. The flat bones of the pelvis and spine are less frequently involved. Malawer MM, Sugarbaker PH, Malawer M: Musculoskeletal Cancer Surgery: Treatment of Sarcomas and Allied Diseases. Kluwer Academic Publishers, 2001.
References:
- Wold LA, et al: Osteogenic Sarcoma: Atlas of Orthopedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 25High Yield
A 21-year-old woman who was wearing a seat belt sustained an injury of the thoracolumbar junction in a motor vehicle accident. The AP radiograph shows widening between the L1 and L2 spinous processes, and the CT scan shows the empty facet sign at this level. The initial evaluation should include
Explanation
The patient has a flexion-distraction injury of the thoracolumbar spine that is often associated with wearing a seat belt. The fracture has a high risk of associated intra-abdominal injury; therefore, the initial evaluation should include a CT of the abdomen. The most common visceral injury is to the bowel. Smith WS, Kaufer H: Patterns and mechanisms of lumbar injuries associated with lap seat belts. J Bone Joint Surg Am 1969;51:239-254.
Question 26High Yield
Figure 20 shows the MRI scan of a 20-year-old athlete who has a painful shoulder. This pathology is most commonly seen in
Explanation
Explanation
The MRI scan reveals a posterior labral detachment. This injury is the result of a posteriorly directed force and is common to football players in blocking positions. Although this injury can occur with trauma in all types of athletes, it is seen with relative frequency in football. Treatment is aimed at labral repair with posterior capsulorrhaphy. Both open and arthroscopic techniques can be used. Misamore GW, Facibene WA: Posterior capsulorrhaphy for the treatment of traumatic recurrent posterior subluxations of the shoulder in athletes. J Shoulder Elbow Surg 2000;9:403-408.
References:
- Mair SD, Zarzour RH, Speer KP: Posterior labral injury in contact athletes. Am J Sports Med 1998;26:753-758.
Question 27High Yield
Figures 34a and 34b show the radiographs of a 28-year-old man who fell on his outstretched arm with significant force while mountain biking. The nerve deficit most likely to occur would result in weakness of

Explanation
The patient has a Monteggia fracture-dislocation (proximal ulnar fracture and radial head dislocation). The posterior interosseous nerve branch of the radial nerve is the most likely to be injured and could result in weakness of thumb extension and finger metacarpal extension. Considerably less likely are injuries to the more proximal radial nerve branches supplying the extensor carpi radialis longus and brevis, resulting in weak wrist extension; the ulnar nerve supplying the digital intrinsics, resulting in weak finger abduction; the anterior interosseous branch of the median nerve, resulting in weakness of the flexor pollicis longus; and the distal median nerve, resulting in weakness of thumb opposition. Bado JL: The Monteggia lesion. Clin Orthop 1967;50:71-86.
Question 28High Yield
Which of the following is considered the preferred approach to resect a lesion in the posterior one third of the proximal humerus?
Explanation
Explanation
At least 8 cm of the posterior aspect of the proximal region of the humeral diaphyseal cortex can be exposed through the interval between the lateral head of the triceps and the deltoid muscle. No nerves or blood vessels need to be exposed in the dissection. The deltoid muscle is innervated by the axillary nerve and the triceps muscle by the radial nerve. This is a true internervous plane.
References:
- Berger RA, Buckwalter JA: A posterior surgical approach to the proximal part of the humerus. J Bone Joint Surg Am 1989;71:407-410.
Question 29High Yield
A 22-year-old volleyball player has atrophy of the infraspinatus muscle. This deficit is the result of entrapment of what nerve?
Explanation
Suprascapular deficits, as the result of repetitive forceful internal rotation with overhead ball striking, occur in the spinoglenoid notch. Compression interferes with distal suprascapular nerve innervation to the infraspinatus, while allowing the supraspinatus to function normally. A scapular notch entrapment of this nerve would involve both the supraspinatus and the infraspinatus. The axillary, dorsal scapular, and subscapular nerves do not affect the infraspinatus. Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Question 30High Yield
A 19-year-old soccer player feels a pop in his knee while making a cut and notes the development of an effusion over several hours. Examination reveals medial joint line tenderness, but the knee is stable to manual stress testing of all ligaments. Examination under anesthesia confirms a stable knee. What is the most critical factor in determining healing after repair of the lesion shown in Figure 14?
Explanation
Explanation
Numerous clinical and basic science investigations have evaluated meniscal tear characteristics to identify factors that either promote or mitigate against meniscal healing. Complex tears have been noted to heal poorly, while longitudinal tears heal more predictably. Tear length, time from injury to repair, medial versus lateral meniscal tears, and the use of a fibrin clot have not been shown to consistently affect meniscal healing. However, rim width, the distance of the tear site from the peripheral meniscocapsular junction (vascular supply), has been shown to have a significant role in the ability of a meniscus repair to heal. DeHaven KE, Arnoczky SP: Meniscus repair: Basic science, indications for repair, and open repair. Instr Course Lect 1994;43:65-76.
References:
- Henning CE, Lynch MA, Clark JR: Vascularity for healing of meniscus repairs. Arthroscopy 1987;3:13-18.
Question 31High Yield
Figure 53 shows a thoracolumbar specimen as viewed from posterior to anterior following removal of all posterior elements. Which of the following structures does the red string pass under?
Explanation
Explanation
The string passes under the ligamentum flavum as it runs from the posterior aspect of the vertebra above to the inferior aspect of the vertebra below in the sagittal midline. This is an important structure in diskectomy and in posterior approaches to the thoracolumbar spine and neural elements. It is rarely visualized in its entirety because typical exposures provide only a limited view.
References:
- Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, vol 2, p 1465.
Question 32High Yield
A 51-year-old plumber has a failed peroneus brevis tendon repair. He reports continued pain and swelling in the distal retrofibular area. MRI shows longitudinal tears of the peroneus longus and peroneus brevis. What is the surgical treatment of choice at this time?
Explanation
Explanation
A flexor digitorum longus transfer, while not as strong as the peroneals, improves the tendon balance and maintains hindfoot mobility. Subtalar fusion is a salvage procedure. Posterior tibial tendon transfer compromises inversion strength and arch height. Functional absence of the peroneals results in an imbalance that could lead to forefoot varus. Redfern D, Myerson M: The management of concomitant tears of the peroneus longus and brevis tendons. Foot Ankle Int 2004;25:695-707.
References:
- Borton DC, Lucas P, Jomha NM, et al: Operative reconstruction after transverse rupture of the tendons of both peroneus longus and brevis: Surgical reconstruction by transfer of the flexor digitorum longus tendon. J Bone Joint Surg Br 1998;80:781-784.
Question 33High Yield
A 12-year-old girl sustains an acute injury to the right elbow in a fall. An AP radiograph is shown in Figure 5. Nonsurgical management will most likely result in
Explanation
The patient has a significantly displaced medial epicondyle fracture. The only absolute indication for surgical treatment is irreducible incarceration in the joint. Nonsurgical management usually results in a painless nonunion with good elbow function and little elbow instability. Prolonged immobilization should be avoided to prevent stiffness. Tardy ulnar nerve palsy and cubitus varus are not complications of medial epicondyle fractures. Chamber HG, Wilkins KE: Part IV: Apophyseal injuries of the distal humerus, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 801-812.
Question 34High Yield
A 2-year-old child is being evaluated for limb-length and girth discrepancy. As a newborn, the patient was large for gestational age and had hypoglycemia. Current examination shows enlargement of the entire right side of the body, including the right lower extremity and foot. The skin shows no abnormal markings, and the neurologic examination is normal. The spine appears normal. Radiographs confirm a 2-cm discrepancy in the lengths of the lower extremities. Additional imaging studies should include
Explanation
Explanation
The patient may have Beckwith-Wiedemann syndrome (BWS), which consists of exophthalmos, macroglossia, gigantism, visceromegaly, abdominal wall defects, and neonatal hypoglycemia. Hemihypertrophy develops in approximately 15% of patients with BWS. Patients with hemihypertrophy that is the result of BWS have a 40% chance of developing malignancies such as Wilms' tumor or hepatoblastoma; therefore, frequent ultrasound screening is recommended until about age 7 years. The absence of nevi and vascular markings helps to rule out other causes of hemihypertrophy, such as neurofibromatosis, Proteus syndrome, and Klippel-Trenaunay syndrome. Bone age estimations are not accurate at this young age but may become more useful later to help predict the timing of epiphysiodesis procedures. DeBaun MR, Tucker MA: Risk of cancer during the first four years of life in children from The Beckwith-Wiedemann Syndrome Registry. J Pediatr 1998;132:398-400. Ballock RT, Wiesner GL, Myers MT, et al: Hemihypertrophy concepts and controversies. J Bone Joint Surg Am 1997;79:1731-1738.
References:
- Carpenter CT, Lester EL: Skeletal age determination in young children: Analysis of three regions of the hand/wrist film. J Pediatr Orthop 1993;13:76-79.
Question 35High Yield
A 54-year-old man with metastatic renal cell carcinoma has had increasing pain in the left hip for the past 6 weeks. A radiograph is shown in Figure 36. Prophylactic stabilization will most likely result in
Explanation
Explanation
Prophylactic stabilization of impending fractures does not directly affect the overall survival rate, but it does improve factors related to intraoperative and postoperative complications and decreased recovery time. Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
References:
- Harrington KD: Impending pathologic fractures from metastatic malignancy: Evaluation and management. Instr Course Lect 1986;35:357-381.
Question 36High Yield
Which of the following knee ligament injury patterns is most associated with an increase in external tibial rotation with the knee at 90 degrees of flexion?
Explanation
Cadaveric studies have shown that external rotation of the tibia is most pronounced following transection of the posterior cruciate and lateral collateral ligaments with the knee at 90 degrees of flexion. Isolated release of the lateral collateral ligament results in increased external tibial rotation at 30 degrees. Gollehon DL, Torzilli PA, Warren RF: The role of the posterolateral and cruciate ligaments in the stability of the human knee: A biomechanical study. J Bone Joint Surg Am 1987;69:233-242. Cooper DE: Tests for posterolateral instability of the knee in normal subjects: Results of examination under anesthesia. J Bone Joint Surg Am 1991;73:30-36.
Question 37High Yield
A 25-year-old man injures his shoulder while skiing. Examination reveals increased passive external rotation, pain in the cocked position, and a positive lift-off test. What is the most likely diagnosis?
Explanation
Explanation
A positive lift-off test and increased passive external rotation are diagnostic of a subscapularis tear or detachment. Although a similar injury could produce anterior instability, this will test the integrity of the subscapularis. A locked dislocation has limited passive movement. A ruptured biceps tendon will most likely produce ecchymosis and findings similar to supraspinatus trauma. Internal impingement is not associated with subscapularis weakness. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
References:
- Hawkins RJ, Bokor DJ: Clinical evaluation of the shoulder, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 149-177.
Question 38High Yield
Figure 40 shows the AP radiograph of a 55-year-old man who reports left knee pain. Which of the following conditions is least likely to produce this radiographic presentation?
Explanation
The radiograph reveals densities within the articular cartilage of the knee commonly referred to as chondrocalcinosis. The term chondrocalcinosis refers to the presence of calcium-containing crystals detected as radiodensities in cartilage. Calcium-containing crystals other than calcium pyrophosphate dihydrate may also deposit in articular cartilage and menisci, producing both radiographically detectable densities in cartilage and joint inflammation or degeneration. Hemochromatosis, alkaptonuria (ochronosis), and Wilson's disease are characterized by cellular deposition of iron, calcium, and copper ions, respectively, into various tissues including articular cartilage and can give this appearance. Septic arthritis does not usually cause chondrocalcinosis. Klippel JH (ed): Primer on the Rheumatic Diseases, ed 11. Atlanta, GA, Arthritis Foundation, 1997, pp 226-229 and 328-331.
Question 39High Yield
Figure 12 shows the radiograph of a 15-year-old boy with cerebral palsy who has pain at the first metatarsophalangeal joints. He is a community ambulator. Management consisting of accommodative shoes has failed to provide relief. What is the treatment of choice?
Explanation
While other surgeries have provided some success, first metatarsophalangeal joint arthrodesis has the highest overall success rate compared to other surgeries in ambulatory and nonambulatory children with cerebral palsy. The recurrence rate is unacceptably high with the other procedures listed above. In contrast, neurologically normal children are amenable to osteotomies and soft-tissue procedures. Davids JR, Mason TA, Danko A, et al: Surgical management of hallux valgus deformity in children with cerebral palsy. J Pediatr Orthop 2001;21:89-94.
Question 40High Yield
Cementation technique has a definite influence on the long-term survival of cemented femoral components. Both clinical and autopsy studies support the use of a cement mantle with a thickness of how many millimeters?
Explanation
Explanation
Long-term radiographic analysis of cemented total hips supports the creation of a 2- to 5-mm cement mantle in the proximal medial region. Autopsy studies have shown that the incidence of crack formation was greatest when the cement mantle was less than 2 mm. Ebramzadeh E, Sarmiento A, McKellop HA, Llinas A, Gogan W: The cement mantle in total hip arthroplasty: Analysis of long-term radiographic results. J Bone Joint Surg Am 1994;76:77-87. Jasty M, Maloney WJ, Bragdon CR, O'Connor DO, Haire T, Harris WH: The initiation of failure in cemented femoral components of hip arthroplasty. J Bone Joint Surg Br 1991;73:551-558.
References:
- Maloney WJ III: The cemented femoral component, in Callaghan JJ, Rubash HE, Rosenberg AG (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 965-966.
Question 41High Yield
Stiffness relates the amount of load applied to a structure like a long bone or an intramedullary nail to the amount of resulting deformation that occurs in the structure. What is the most important material property affecting the axial and bending stiffness of a structure?
Explanation
The amount of deformation resulting in response to an applied load depends on the stress distribution that the load creates in the structure and the stress versus strain behavior of the material that makes up the structure. Axial and bending loads create stress distributions that involve normal stresses and normal strains. Although all five responses are indeed material properties, only one, elastic modulus, relates normal stresses to normal strains. In fact, axial and bending stiffness are directly proportional to modulus, so that a nail made from stainless steel will have nearly twice the stiffness of a nail made from titanium alloy (because their respective elastic moduli differ by about a factor of two). Hayes WC, Bouxsein ML: Analysis of muscle and joint loads, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 74-82. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 159-165.
Question 42High Yield
Which of the following procedures is included in third-generation cement technique?
Explanation
Explanation
The so-called third-generation cement technique adds porosity reduction techniques, centralization devices, and surface modifications to the femoral component. The surgeon must be aware of the meaning of the various generations of cement technique when interpreting the results presented at meetings and in the literature. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 181-193.
References:
- Maloney WJ, Hartford JM: The cemented femoral component, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, vol 2, pp 959-979.
Question 43High Yield
During primary total knee arthroplasty, what is the maximum distance the joint line can be raised or lowered before poor motion, joint instability, and increased chance of revision occur?
Explanation
Explanation
Positioning of the femoral and tibial components is a common cause of early failure of total knee arthroplasty. Two modes of possible position are raising or lowering the joint line from its anatomic level. Raising or lowering the joint line beyond an established threshold can cause limited range of motion, poor patellar function, and possible instability. It has been determined that a threshold of approximately 8 mm provides consistently good results after knee arthroplasty.
References:
- Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 339-365.
Question 44High Yield
A 66-year-old man has a high-grade angiosarcoma of the right tibia. A radiograph is shown in Figure 43. Treatment should consist of
Explanation
Angiosarcoma is a locally aggressive sarcoma. The radiograph shows extensive multiple discontinuous lesions throughout the entire tibia. The extent of bone involvement precludes resection; therefore, the treatment of choice is amputation, either above the knee or through the knee. Radiation therapy is not needed after amputation, and chemotherapy remains investigational for soft-tissue sarcoma.
Question 45High Yield
When performing surgery on a patient with insertional Achilles tendinitis and a Haglund's deformity, how much of the Achilles tendon insertion can be safely detached without having to consider reattachment with bone anchors?
Explanation
The Achilles tendon insertion encompasses a broad area on the posterior area of the calcaneus. A biomechanical study has shown that up to 50% of the Achilles tendon insertion point can be detached before the strength of the attachment point starts to weaken. It is recommended that if more than this amount is detached to remove the posterior superior calcaneal prominence, consideration should be given to either securing the tendon to the bone with suture anchors or performing a tendon transfer. Kolodziej P, Glisson RR, Nunley JA: Risk of avulsion of the Achilles tendon after partial excision for treatment of insertional tendinitis and Haglund's deformity: A biomechanical study. Foot Ankle Int 1999;20:433-437.
Question 46High Yield
A 19-year-old female long-distance runner has an incomplete tension-side femoral neck stress fracture. Management should consist of
Explanation
Explanation
Unlike compression-side stress fractures, tension-side stress fractures on the superior side of the femoral neck are at a very high risk of displacement, even if the patient is not bearing weight. It is highly recommended to treat these fractures like acute fractures and to proceed with internal fixation emergently. Once the fracture has displaced, the prognosis is poor in terms of returning to sports, even when reduced and internally fixed. Nonsurgical management, such as limited weight bearing and low-impact activities, works very well for other lower extremity stress fractures. A training program evaluation (shoes, tracks, schedule) is always indicated for all patients with stress fractures.
References:
- Boden BP, Osbahr DC: High-risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Question 47High Yield
A 6-year-old boy with severe spastic quadriplegic cerebral palsy is nonambulatory. Examination reveals 10 degrees of hip abduction on the left and 30 degrees on the right with the hips and knees extended. The Thomas test shows 20 degrees of flexion bilaterally, and Ely test results are 3+/4 bilaterally. Radiographs show a center edge angle of 0 degrees on the left and -10 degrees on the right. The neck shaft angles are 170 degrees bilaterally. Which of the following procedures would offer the best results?
Explanation
The patient has bilateral subluxated hips, with nearly vertical neck shaft angles; therefore, the treatment of choice is varus derotation osteotomy. Shortening of the bone on one or both sides may be necessary to allow adequate range of motion postoperatively. In patients this age and with this degree of bony deformity, soft-tissue releases are not likely to lead to hip stability. Botulinum toxin has been shown to be effective in the treatment of ankle equinus, but its efficacy in other areas has not been demonstrated as yet. The indications for obturator neurectomy are unclear at present. Proximal femoral resection is a salvage procedure for long-standing hip dislocations that are symptomatic and not reconstructable. Tylkowski CM, Rosenthal RK, Simon SR: Proximal femoral osteotomy in cerebral palsy. Clin Orthop 1980;151:183-192.
Question 48High Yield
Which of the following is an indication for surgical management of a Weber type B distal fibular fracture?
Explanation
Explanation
A widened medial clear space indicates instability caused by an associated tear of the deltoid ligament; therefore, nonsurgical management is not warranted. Weber type B distal fibular fractures without a deltoid tear have a medial clear space of < 4 mm, even under stress, and may be successfully treated nonsurgically. The presence of medial hindfoot ecchymosis and medial ankle tenderness is not fully indicative of medial soft-tissue instability; however, these findings may indicate a deltoid injury and should raise suspicion of an unstable fracture injury pattern. Stress testing is necessary to demonstrate the presence or absence of instability. A small amount of comminution is also cause for increased suspicion of an unstable pattern; however, it is not a direct contraindication when considering nonsurgical management. Two millimeters of fibular displacement without lateral shift of the talus is an acceptable position when considering nonsurgical management of Weber type B distal fibular fractures. Michelson JD, Magid D, Ney DR, et al, Examination of the pathologic anatomy of ankle fractures. J Trauma 1992;32:65-70.
References:
- Marsh JL, Saltzman CL: Ankle fractures, in Rockwood & Green's Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 2001-2090.
Question 49High Yield
Which of the following is considered an important component in treating the lesion shown in Figure 56?
Explanation
Explanation
Mucoid cysts are commonly associated with DIP joint arthritis. Two treatment options are commonly used: (1) aspiration/drainage and injection of corticosteroid and (2) surgical excision. When performing the surgery, excision of the bony osteophytes about the DIP joint is helpful in achieving a cure. There are no reports of significant benefit with nail removal or partial ligament or extensor tendon resection. Some authors have advocated skin excision and rotational flaps for wound coverage, but this is somewhat controversial. Rizzo M, Beckenbaugh RD: Treatment of mucous cysts of the fingers: Review of 134 cases with minimum 2-year follow-up evaluation. J Hand Surg Am 2003;28:519-524.
References:
- Eaton RG, Dobranski AI, Littler JW: Marginal osteophyte excision in treatment of mucous cysts. J Bone Joint Surg Am 1973;55:570-574.
Question 50High Yield
A previously asymptomatic 12-year-old girl sustained a direct blow to the right lateral knee from a baseball bat. Examination reveals an area of ecchymosis and tenderness over the lateral thigh. The patient can walk without pain, but range of motion of the knee causes discomfort. Plain radiographs of the knee are shown in Figures 11a and 11b. To address the bone lesion, management should consist of

Explanation
The plain radiographs reveal a pedunculated osteochondroma with a fracture. There is a bony growth in the metaphysis of a long bone, on a stalk that is directed away from the nearby epiphysis. On the AP view, the host cortical and medullary bone are shown as "blending" with lesional bone. There is also a fracture through the lesion. Based on these radiographic findings, the diagnosis is an osteochondroma; therefore, initial management of an acute fracture of an osteochondroma is symptomatic treatment alone. Additional imaging studies are not indicated in this patient. At times it may be difficult to distinguish a sessile osteochondroma from a parosteal osteosarcoma. In the latter case, the host medullary bone and lesion bone are not confluent. A CT scan may be helpful to distinguish if the host medullary and cortical bone are confluent with the lesion.
Question 51High Yield
Acral metastases are most commonly seen in what type of carcinoma?
Explanation
Explanation
Metastatic lesions to bone are usually located in the axial and proximal appendicular skeleton. Metastases below the elbow and knee are rare, but when they do occur they are most commonly from lung carcinoma. Hayden RJ, Sullivan LG, Jebson PJ: The hand in metastatic disease and acral manifestations of paraneoplastic syndromes. Hand Clin 2004;20:335-343.
References:
- Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 313.
Question 52High Yield
Figure 53 shows the arteriogram of a 45-year-old man who has severe vasculitis. What do the findings show?
Explanation
Explanation
The arterial supply to the hand is abundant and normally duplicated. The deep palmar arch as shown in this arteriogram typically receives its primary contribution from the radial artery which travels deep to the first dorsal compartment tendons and then returns to the volar aspect of the palm through the first web space. The superficial palmar arch receives its supply from the ulnar artery and is not visualized in this patient.
References:
- Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist: Diagnosis and Operative Treatment. Philadephia, PA, Mosby-Year Book, 1998, p 110.
Question 53High Yield
A previously healthy 13-year-old girl has had thigh pain for the past 3 weeks. The radiograph shown in Figure 47a reveals a lesion in the right femur. A bone scan and CT scan of the chest show no evidence of other lesions. A biopsy specimen is shown in Figure 47b. What is the most likely diagnosis?

Explanation
The patient has Langerhans cell histiocytosis that may be solitary (eosinophilic granuloma) or associated with systemic illness (Hand-Schuller-Christian disease and Letterer-Siwe disease). The solitary form of the disease, eosinophilic granuloma, typically affects patients in the first three decades of life. Radiographically, it is characterized as a well-defined, lytic, "punched out" intramedullary lesion. Histologically, two cell types, eosinophils and Langerhans cells, are seen. The Langerhans cells are seen as mononuclear histiocyte-like cells with oval nuclei with well-defined round or oval cytoplasm. A prominent nuclear groove can be seen in most of the nuclei (coffee bean nuclei). A mixture of inflammatory cells and lipid-laden foam cells with nuclear debris may be present as well. The lack of nuclear atypia and atypical mitoses excludes malignant conditions such as Ewing's sarcoma, lymphoma of bone, and metastatic neuroblastoma. The lack of acute inflammatory cells excludes the diagnosis of osteomyelitis. The eosinophils have bi-lobed nuclei and granular eosinophilic cytoplasm. Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby, 1988.
Question 54High Yield
A 9-year-old boy sustained a traumatic brain injury and right lower extremity trauma in an accident involving a motor vehicle and a pedestrian. Initial evaluation in the emergency department reveals an obtunded patient who is breathing spontaneously and withdraws appropriately to painful stimuli. After initial resuscitation and stabilization, a CT scan reveals a right parietal intracranial hemorrhage. Radiographs of the swollen right thigh are shown in Figures 32a and 32b. Management of the fractured femur should ultimately consist of
Explanation
Explanation
32b A child with a traumatic brain injury generally achieves significant neurologic recovery and has a more favorable prognosis than an adult. Early stabilization of fractures facilitates transportation of the child for diagnostic tests and decreases the incidence of shortening and malunion. Surgical treatment of the fracture is indicated when cerebral perfusion pressure has stabilized. Casting or traction is not the most appropriate treatment of a femoral fracture in a child of this age with a brain injury. Fracture reduction is difficult to maintain if the brain injury leads to spasticity, and transportation within the hospital for tests is more difficult. Insertion of a reamed antegrade intramedullary nail inserted at the piriformis fossa is associated with a small risk of osteonecrosis of the femoral head. The transverse femoral fracture in this patient is ideally suited for stabilization with flexible intramedullary nails. Ligier and associates treated 123 femoral shaft fractures in children with flexible intramedullary nails, including 35 patients with head injury. In one patient with hemiplegia and a urinary tract infection, a deep wound infection developed, necessitating nail removal. The remaining patients all healed without major complications. Heinrich and associates treated 78 diaphyseal femoral fractures with flexible intramedullary nails, including 14 with head injury. No major complications were reported and all fractures healed. Tolo VT: Management of the multiply injured child, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 83-95. Ligier JN, Metaizeau JP, Prevot J, et al: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77. Heinrich MS, Drvaric DM, Darr K, et al: The operative stabilization of pediatric diaphyseal femur fractures with flexible intramedullary nails: A prospective analysis. J Pediatric Orthop 1994;14:501-507.
References:
- Canale ST, Tolo VT: Fractures of the femur in children. Instr Course Lect 1995;44:255-273.
Question 55High Yield
Figure 16a shows the radiograph of a 34-year-old woman who sustained a basicervical fracture of the femoral neck. The fracture was treated with a compression screw and side plate. Seven months postoperatively, she continues to have significant hip pain and cannot bear full weight on her hip. A recent radiograph is shown in Figure 16b. Management should now consist of

Explanation
The patient sustained a high-angle femoral neck fracture. The follow-up clinical findings and radiograph show that she now has a nonunion with failed internal fixation. The joint appears preserved. In a healthy, young patient, arthroplasty of the femoral head, although possible, is not ideal. Excellent healing and function can be obtained in 70% to 80% of patients with femoral neck nonunion with a valgus intertrochanteric osteotomy. Marti RK, Schuller HM, Raaymakers EL: Intertrochanteric osteotomy for non-union of the femoral neck. J Bone Joint Surg Br 1989;71:782-787.
Question 56High Yield
Which of the following ligaments is the primary static restraint against inferior translation of the arm when the shoulder is in 0 degrees of abduction?
Explanation
The superior glenohumeral ligament (SGHL) and coracohumeral ligament serve as primary static restraints against inferior translation of the arm when the shoulder is in 0 degrees of abduction. Of these, the coracohumeral ligament has been shown to have a greater cross-sectional area, greater stiffness, and greater ultimate load than the SGHL. The inferior glenohumeral ligament plays a greater stabilizing role with increasing abduction of the arm. The coracoacromial ligament may help provide superior stability, especially when the rotator cuff is deficient. The coracoclavicular ligaments stabilize the acromioclavicular joint. Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Question 57High Yield
A 7-year-old girl who sustained a type III posteromedial extension supracondylar fracture underwent a closed reduction at the time of injury. Figure 27a shows the position of the fracture fragments prior to percutaneous medial and lateral pin fixation. Following surgery, healing was uneventful and the patient regained a full painless range of motion. Fifteen months after the injury, she now reports loss of elbow motion and moderate pain with activity. A current AP radiograph is shown in Figure 27b. What is the most likely cause of her symptoms?
Explanation
Explanation
27b The patient sustained a very distal supracondylar fracture of the humerus. Fractures in this area can disrupt the blood vessels supplying the lateral ossification center of the trochlea. With disturbance of the blood supply in this area, local osteonecrosis occurs and disrupts the support for the overlying articular surface, producing joint incongruity and localized degenerative arthritis. Haraldsson S: The interosseous vasculature of the distal end of the humerus with special reference to the capitellum. Acta Orthop Scand 1957;27:81-93.
References:
- Morrissy RT, Wilkins KE: Deformities following distal humeral fracture in childhood. J Bone Joint Surg Am 1984;66:557-562.
Question 58High Yield
A 19-year-old man sustains a low-velocity gunshot wound to the forearm. What factor most strongly correlates with the development of compartment syndrome after this injury?
Explanation
Explanation
In a multivariate analysis, the strongest factor for the development of compartment syndrome is fracture of the proximal third of the forearm. However, compartment syndrome can still occur without a fracture. Therefore, these patients should be followed with a high level of suspicion for the development of compartment syndrome. Moed BR, Fakhouri AJ: Compartment syndrome after low-velocity gunshot wounds to the forearm. J Orthop Trauma 1991;5:134-137.
References:
- Hahn M, Strauss E, Yang EC: Gunshot wounds to the forearm. Orthop Clin North Am 1995;26:85-93.
Question 59High Yield
A patient with refractory long head biceps pain in the shoulder undergoes biceps tenotomy. The patient is concerned about possible postoperative deformity and loss of supination strength. Which of the following techniques provides the strongest initial fixation to prevent distal migration?
Explanation
Recent articles have looked at the cyclic load failure and ultimate load failure of biceps tenodesis techniques. The interference screw has proved superior to bone tunnel, suture anchor, and soft-tissue tenodesis techniques in laboratory cadaveric testing. Whether this is clinically relevant or not is still unknown. Ozalay M, Akpinar S, Karaeminogullari O, et al: Mechanical strength of four different biceps tenodesis techniques. Arthroscopy 2005;21:992-998.
Question 60High Yield
What is the mechanism of action of bisphosphonates?
Explanation
Bisphosphonates are stable analogues of pyrophosphate that have a strong affinity for bone hydroxyapatite; these agents inhibit bone resorption by reducing the recruitment and activity of osteoclasts and increasing apoptosis. Bone formed while patients are receiving bisphosphonate treatment is histologically normal. Bisphosphonates have been shown to be effective in decreasing pathologic fractures, bone pain, and the need for radiation therapy in patients with multiple myeloma and metastatic carcinoma to bone. The most effective method of administration is via monthly intravenous infusion. Osteonecrosis of the mandible is sometimes a complication of this treatment. Gass M, Dawson-Hughes B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.
Question 61High Yield
A 67-year-old woman has persistent anterior thigh and knee pain after undergoing total knee arthroplasty 1 year ago. Examination and radiographs reveal no problems in the knee, mild hip flexor weakness (grade 4+), and decreased sensation over the anterior thigh including and proximal to the incision. MRI of the lumbar spine will most likely reveal which of the following findings?
Explanation
Explanation
Degenerative spondylolisthesis at L3-4 is the most likely diagnosis. This spondylolisthesis would result in foraminal stenosis affecting the third lumbar root and leading to anterior thigh and knee pain and hip flexor weakness. L4-5 spondylolisthesis would impinge on the L4 root in the foramen. Degenerative disk disease without hypertrophy is unlikely to have root impingement. Posterolateral herniations typically affect the inferior root and are less common in this age group. Hoppenfeld S: Physical Examination of the Spine and Extremities. Upper Saddle River, NJ, Prentice Hall, 1976, p 250.
References:
- Lauerman WC, Goldsmith ME: Spine, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 353-378.
Question 62High Yield
Figure 31 shows the radiograph of an 8-year-old boy who has a swollen forearm after falling out of a tree. Examination reveals that all three nerves are functionally intact, and there is no evidence of circulatory embarrassment. Management should consist of
Explanation
Explanation
The patient has a Bado type IV Monteggia lesion. It involves dislocation of the radial head and fractures of both the radial and ulnar shafts. These fractures are very difficult to manage by closed reduction alone. The radial and ulnar shafts first have to be stabilized surgically to give a lever arm to reduce the radial head. In this age group, intramedullary pins are easy to insert percutaneously and cause less tissue trauma than plates and screws. In these types of injuries, the focus is often on the forearm fracture; the radial head dislocation may not be appreciated as was the case with this patient. Gibson WK, Timperlake RW: Operative treatment of a type IV Monteggia fracture-dislocation in a child. J Bone Joint Surg Br 1992;74:780-781.
References:
- Stanley EA, DeLaGarza JF: Part IV: Monteggia fracture. Dislocations in children, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 576-577.
Question 63High Yield
A 35-year-old man reports forefoot pain with weight-bearing activities. He reports that he has had high arches since adolescence but has never been treated. Examination reveals stiff cavus feet. He has no plantar callus or hammer toe formation. The ankle can be passively dorsiflexed 10 degrees. Initial management should consist of
Explanation
Explanation
The patient has cavus feet with minimal clinical symptoms. At this stage, conservative management is preferred. The use of a molded orthosis will allow better support of the midfoot and provide cushioning of the forefoot. This will most likely result in long-term relief. In more advanced cases with forefoot callus formation, Achilles tendon lengthening or calcaneal osteotomy and Steindler stripping are effective in correcting the cavus deformity. In the presence of arthritic changes in the hindfoot, a triple arthrodesis with corrective bone resection may be necessary. Janisse DJ: Indications and prescriptions for orthoses in sports. Orthop Clin North Am 1994;25:95-107.
References:
- Franco AH: Pes cavus and pes planus: Analyses and treatment. Phys Ther 1987;67:688-694.
Question 64High Yield
A 10-year-old child has leg discomfort with activity. A radiograph, bone scan, and biopsy specimen are shown in Figures 1a through 1c. What is the most likely diagnosis?
Explanation
Explanation
1b 1c The ground glass appearance on the radiograph, the hot bone scan, and histologic findings of bony spicules without osteoblastic rimming in a background of bland fibrous tissue all suggest fibrous dysplasia. Stress-related pain is common with activity because of the dysplastic bone. Parosteal osteosarcomas are surface lesions. Simple cysts, aneurysmal bone cysts, and eosinophilic granuloma are all possible radiographically; however, the histology is most consistent with fibrous dysplasia. Harris WH, Dudley HR Jr, Barry RS: The natural history of fibrous dysplasia: An orthopaedic, pathological and roentgenographic study. J Bone Joint Surg Am 1962;44:207.
References:
- Campanacci M: Bone and Soft Tissue Tumors. Vienna, Austria, Springer-Verlag, 1990.
Question 65High Yield
A 58-year-old reports pain and stiffness in his left shoulder following a seizure episode. Diagnosis at the time of the seizure is a frozen shoulder, and management consists of an aggressive physical therapy program of stretching exercises. Four months later he continues to have shoulder pain and has not gained any additional range of motion. A CT scan is shown in Figure 50. Management should now consist of
Explanation
Humeral arthroplasty is indicated for chronic posterior dislocations when the impression defect in the humeral head is greater than 45% to 50%. If the condition remains undiagnosed for more than 9 to 12 months, secondary degenerative changes on the glenoid may occur, necessitating total shoulder arthroplasty. Open reduction and transfer of the subscapularis and lesser tuberosity are used for impression defects that consist of 20% to 40% of the humeral articular surface. Closed reduction and immobilization with the arm in slight extension and external rotation is useful when the posterior dislocation is diagnosed within the first 6 weeks and the articular defect is less than 20%. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 66High Yield
A 58-year-old man has persistent pain and weakness of his right shoulder after undergoing primary rotator cuff repair 1 year ago. A clinical photograph is shown in Figure 11. Which of the following factors might make functional improvement problematic with revision rotator cuff surgery?
Explanation
Explanation
Functional improvement after revision rotator cuff surgery is most likely to occur in patients with an intact deltoid, good-quality rotator cuff tissue, preoperative active elevation alone to 90 degrees, and only one prior rotator cuff repair. In this patient, the compromised deltoid origin might make functional improvement less likely. Djurasovic M, Marra G, Arroyo JS, et al: Revision rotator cuff repair: Factors influencing results. J Bone Joint Surg Am 2001;83:1849-1855. Bigliani LU, Cordasco FA, McIlveen SJ, et al: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515.
References:
- Neviaser RJ, Neviaser TJ: Operation for failed rotator cuff repair: Analysis of fifty cases. J Shoulder Elbow Surg 1992;1:283-286.
Question 67High Yield
A 15-year-old boy reports feeling a pop and notes sudden giving way of the left knee while playing basketball. He has immediate pain and swelling in the knee. An AP radiograph is shown in Figure 32. A small avulsion fragment from the lateral tibial margin is the only finding. What is the most likely diagnosis?
Explanation
Explanation
An avulsion fracture from the lateral tibial margin carries the eponym Segond fracture and is pathognomonic for an anterior cruciate ligament (ACL) tear. The fragment is located posterior to Gerdy's tubercle and is superior and anterior to the fibular head. It represents an avulsion of the lateral capsular ligament of the knee and is caused by the same mechanism that causes the ACL tear. The pes anserinus is the insertion point of the medial hamstrings and would not be affected in a lateral avulsion injury. The posterior cruciate ligament may be seen on a lateral view if associated with an avulsion fragment, but a tear of the PCL generally cannot be diagnosed on an AP view. The insertion of the iliotibial band is broad and is unlikely to produce an avulsion injury such as that seen in the radiograph. This view is not consistent with the appearance of a lateral collateral ligament injury. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 533-557.
References:
- Larson RL, Tailon M: Anterior cruciate ligament insufficiency: Principles of treatment. J Am Acad Orthop Surg 1994;2:26-35.
Question 68High Yield
What pathology is most likely to result in failure of an arthroscopic Bankart repair?
Explanation
Explanation
Recent studies have documented that an arthroscopic Bankart repair performed with good technique can produce success rates similar to an open repair. However, the results of an arthroscopic repair deteriorate significantly if there is a 25% or greater anterior-inferior glenoid rim defect (inverted pear configuration) or an engaging Hill-Sachs lesion in which the humeral head defect keys onto the glenoid rim in abduction and external rotation. If either of these entities exist or there is multidirectional instability with pathologic hyperextensible tissue laxity, an open repair is recommended. An associated SLAP lesion would not significantly affect the result of the Bankart procedure. Not infrequently, the anterior glenoid labrum is partially or completely disrupted and, in itself, is not a contraindication to arthroscopic Bankart repair. In almost all patients with predominantly unidirectional instability, some degree of capsular/anterior-inferior glenohumeral ligament attenuation is present and can be addressed during the arthroscopic repair. Burkhart SS, De Beer JF: Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy 2000;16:677-694.
References:
- Cole BJ, Romeo AA: Arthroscopic shoulder stabilization with suture anchors: Technique, technology, and pitfalls. Clin Orthop 2001;390:17-30.
Question 69High Yield
What is the most common diagnosis in a patient older than age 40 years with a destructive bony lesion?
Explanation
The most common destructive lesions in a patient older than age 40 years are, in decreasing incidence, metastatic carcinoma, multiple myeloma, lymphoma, and chondrosarcoma. Osteosarcoma is found primarily in younger patients.
Question 70High Yield
Figure 45 shows the radiograph of a 2-year-old patient who has progressive lumbar scoliosis as the result of hemivertebra. Examination reveals no associated cutaneous lesions, and an MRI scan shows no associated intraspinal anomalies. Treatment should consist of
Explanation
Explanation
In a retrospective review of 10 patients treated with hemivertebra excision for hemivertebra in the levels of T12 to L3, the procedure was found to be safe and effective. The procedure provided an average curve correction of 67 degrees and was greatest in patients who were younger than age 4 years at the time of surgery. Long anterior and posterior fusion with instrumentation is not the treatment of choice at this age. Either anterior hemiepiphyseodesis or posterior hemiarthrodesis in this isolated hemivertebra setting would be inadequate. Brace treatment is ineffective in management of the primary curvature.
References:
- Callahan BC, Georgopoulos G, Eilert RE: Hemivertebral excision for congenital scoliosis. J Pediatr Orthop 1997;17:96-99.
Question 71High Yield
The use of posting (a wedge added to the medial or lateral side of an insole) is useful to balance forefoot or hindfoot malalignment. Assuming normal subtalar joint pronation, what is the maximum amount of recommended hindfoot posting?
Explanation
Explanation
Generally, patients cannot tolerate more than 5 degrees of hindfoot posting. Donatelli RA, Hurlbert C, Conaway D, et al: Biomechanics foot orthotics: A retrospective study. J Orthop Sports Phys Ther 1988;10:205-212. Michaud TM: Foot Orthoses and Other Forms of Conservative Foot Care. Baltimore, MD, Williams & Wilkins, 1993, pp 61-65, 186.
References:
- Root MC, Orien WP, Weed JH: Normal and Abnormal Function of the Foot. Los Angeles, CA, Clinical Biomechanics Corporation, 1977, vol 2, pp 29-33.
Question 72High Yield
Figure 33a shows a line drawing of a normal hemipelvis. The anterior acetabular rim is bold. Figure 33b illustrates a hemipelvis with a crossover sign, which is indicative of what acetabular pathology?
Explanation
Explanation
33b In a normal AP pelvis radiograph, the anterior rim of the acetabulum runs medially and distally, diverging from the posterior rim which runs much more vertically. In excessive acetabular retroversion, the anterior rim (bold line in Figure 33b) and posterior rim start laterally, and as these lines progress medially and distally, the anterior line crosses the posterior line. This predisposes to femoral acetabular impingement. Reynolds D, Lucas J, Klaue K: Retroversion of the acetabulum: A cause of hip pain. J Bone Joint Surg Br 1999;81:281-288.
References:
- Espinosa N, Rothenfluh DA, Beck M, et al: Treatment of femoro-acetabular impingement: Preliminary results of labral refixation. J Bone Joint Surg Am 2006;88:925-935.
Question 73High Yield
A 15-year-old girl reports popping and clicking at the sternoclavicular joint and an intermittent asymmetrical prominence of the medial head of the clavicle. She denies any history of trauma or other symptoms. Management should consist of
Explanation
Explanation
Atraumatic subluxation or dislocation of the sternoclavicular joint typically occurs in individuals with generalized ligamentous laxity. It is generally not painful, has no long-term sequelae, and needs no treatment. In fact, it is more likely to be painful following surgery than if managed nonsurgically. Rockwood CA Jr, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
References:
- Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, p 583.
Question 74High Yield
Figure 38a shows the radiograph of a 12-year-old boy who underwent a reamed intramedullary nailing for a closed femoral shaft fracture. One year after rod removal, he reports groin pain. A current radiograph is shown in Figure 38b. The findings are most likely the result of
Explanation
Explanation
38b Osteonecrosis of the femoral head is a known complication from the use of rigid intramedullary nails for femoral fractures in adolescents. When the nails are placed through the piriformis fossa, the lateral ascending vessels of the femoral neck may be injured, resulting in osteonecrosis of the femoral head in 1% to 2% of patients. Rigid reamed nails placed into the piriformis fossa are contraindicated in children with open growth plates because the physis is a barrier to blood supply and the ligamentum teres does not provide sufficient vascularity. Alternative fixation methods for femoral fractures in adolescents include external fixation and open reduction and internal fixation. Nailing through the tip of the trochanter may decrease the incidence of this serious complication. Letts M, Jarvis J, Lawton L, et al: Complications of rigid intramedullary rodding of femoral shaft fractures in children. J Trauma 2002;52:504-516. Stans AA, Morrissy RT, Renwick SE: Femoral shaft fracture treatment in patients age 6 to 16 years. J Pediatr Orthop 1999;19:222-228. Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop 1997;338:60-73.
References:
- Beaty JH, Austin SM, Warner WC, et al: Interlocking intramedullary nailing of femoral-shaft fractures in adolescents: Preliminary results and complications. J Pediatr Orthop 1994;14:178-183.
Question 75High Yield
Figure 18a shows the clinical photograph of a 31-year-old man who has a slowly growing nodule on his right middle finger. It is minimally tender, and there is no erythema on examination. A biopsy specimen is shown in Figure 18b. What is the most likely diagnosis?
Explanation
Explanation
18b Epithelioid sarcoma is the most common soft-tissue sarcoma in the hand and most commonly occurs in young adults. The tumors can be superficial and may become ulcerated. Deeper lesions are often attached to tendons, tendon sheaths, or fascial structures. These are usually minimally symptomatic. The biopsy specimen reveals the typical appearance of a nodular pattern with central necrosis. They can mimic a necrotizing granulomatous process. Usually there are chronic inflammatory cells along the margin of the tumor nodules. This biopsy specimen does not have the clear cells necessary for a clear cell carcinoma or sarcoma. Nora's tumor is a bizarre parosteal osteochondromatous proliferation (BPOP) first described in 1983 by the pathologist, Nora. The lesion is defined as a reactive heterotopic ossification and is mostly found in the hands or feet of adults in the third decade of life. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 1074.
References:
- Halling AC, Wollan PC, Pritchard DJ, et al: Epithelioid sarcoma: A clinicopathologic review of 55 cases. Mayo Clin Proc 1996;71:636-642.
Question 76High Yield
Patients in compensated shock (normal vital signs) are thought to be at risk for which of the following?
Explanation
Patients who are in compensated shock have normal vital signs but still have hypoperfusion of organ beds such as the splanchnic circulation due to preferential perfusion of the heart and brain. The response to this continued hypoperfusion may be the development of a systemic inflammatory response that may lead to multiple organ failure. The patients are thought to be at risk for a "primed" immune system due to the ongoing stimulation of the immune system and may have an exaggerated response to a second stimulus such as surgery or infection. Other markers of resuscitation should be used besides vital signs to determine when resuscitation has been completed. The use of temporizing fixation has been shown to lower systemic complication rates, and the infection and union rate after staged fixation is not altered. Schulman AM, Claridge JA, Carr G, et al: Predictors of patients who will develop prolonged occult hypoperfusion following blunt trauma. J Trauma 2004;57:795-800.
Question 77High Yield
A 56-year-old woman sustained the fracture shown in Figures 30a and 30b in a motor vehicle accident. What mechanism is most likely responsible for the injury?

Explanation
The CT scans show a burst fracture that results from an axial load injury. The radiographic hallmark of a burst fracture is compression of the posterior cortex of the vertebral body with retropulsion of bone into the spinal canal. AP radiographs often show widening of the interpedicular distance with a fracture of the lamina. Theiss SM: Thoracolumbar and lumbar spine trauma, in Stannard JP, Schmidt AH, Kregor PJ (eds): Surgical Treatment of Orthopaedic Trauma. New York, NY, Thieme, 2007, pp 179-207.
Question 78High Yield
What preoperative factor correlates best with the outcome of rotator cuff repair?
Explanation
Explanation
The size of the rotator cuff tear in both anteroposterior and mediolateral dimensions has been found to correlate best with outcome. Older patient age and rupture of the long head of the biceps tend to be associated with larger tears and, therefore, may be associated indirectly with a poorer outcome. Iannotti JP: Full-thickness rotator cuff tears: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
References:
- Iannotti JP, Bernot MP, Kuhlman JR, Kelley MJ, Williams GR: Postoperative assessment of shoulder function: A prospective study of full-thickness rotator cuff tears. J Shoulder Elbow Surg 1996;5:449-457.
Question 79High Yield
A 32-year-old man sustained a closed injury after falling 25 feet from a roof. His ankle and foot are severely swollen. Radiographs and CT scans are shown in Figures 29a through 29d. Initial management should consist of

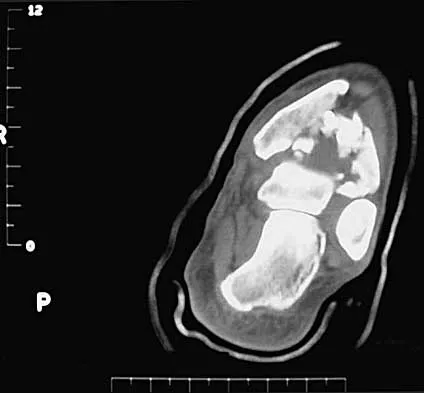
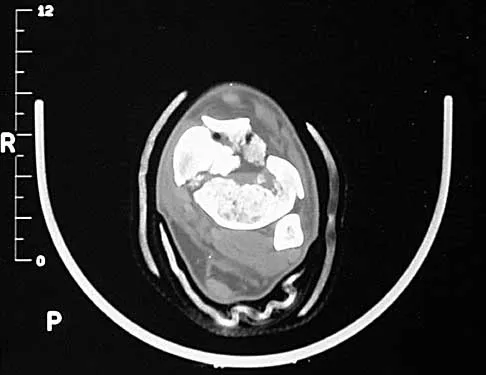
Explanation
The patient has a severe high-energy injury from axial loading to the left ankle and distal tibia. This is a closed injury, but the soft tissues are injured and severely swollen. Initial treatment should focus on skeletal stabilization, and incisions directly over the fracture area should be avoided until soft-tissue stabilization has occurred. Immediate spanning external fixation with plans for a delayed reconstruction as needed for the joint surface is the treatment of choice. Closed reduction and application of a constrictive long leg cast may lead to increased risk of tissue necrosis. Immediate open procedures to internally fix the fracture add the risks of soft-tissue necrosis and are to be avoided. Percutaneous plating may be one of the delayed fixation options but should not be used immediately. Primary ankle arthrodesis is not indicated. Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265. Marsh JL, Bonar S, Nepola JV, DeCoster TA, Hurwitz SR: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Question 80High Yield
A 74-year-old woman with rheumatoid arthritis reports shoulder pain that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 23a and 23b. Examination reveals active forward elevation to 120 degrees and external rotation to 30 degrees. What treatment option results in the most predictable pain relief and function?
Explanation
Explanation
23b Most studies have shown that total shoulder arthroplasties yield better pain relief and improved forward elevation when compared to hemiarthroplasty in patients with rheumatoid arthritis. Although rotator cuff tears are more common in this patient population, this patient has good forward elevation and no significant superior migration of the humeral head; therefore, a reverse arthroplasty is not indicated. The arthritis is too advanced in this patient to consider arthroscopy, but in less advanced cases it can improve range of motion and decrease pain. Metal-backed glenoid components have shown higher rates of loosening. Collin DN, Harryman DT II, Wirth MA: Shoulder arthroplasty for the treatment of inflammatory arthritis. J Bone Joint Surg Am 2004;86:2489-2496. Baumgarten KM, Lashgari CM, Yamaguchi K: Glenoid resurfacing in shoulder arthroplasty: Indications and contraindications. Instr Course Lect 2004;53:3-11.
References:
- Martin SD, Zurakowski D, Thornhill TS: Uncemented glenoid component in total shoulder arthroplasty: Survivorship and outcomes. J Bone Joint Surg Am 2005;87:1284-1292.
Question 81High Yield
The mother of a 3-month-old infant states that she has difficulty positioning the infant's legs during diaper changes. Examination reveals limited abduction of both hips and a negative Ortolani sign. A radiograph reveals bilaterally dislocated hips. Initial management consists of guided reduction in a Pavlik harness, with weekly follow-up. Figures 57a and 57b show the radiograph and CT scan obtained after 6 weeks in the harness. Management should now consist of
Explanation
Explanation
57b In an infant younger than age 6 months with a complete dislocation of the hip that is not initially reducible, the Pavlik harness may be used for a trial of guided reduction. When the harness is used in these patients, the infant should be followed at weekly intervals to see if reduction has been achieved. If the hip does not reduce after 3 to 4 weeks of harness wear, the harness should be discontinued, and closed or open reduction should be considered to avoid secondary deformation of the posterolateral acetabulum, also known as Pavlik harness pathology. Changing to other abduction braces is not indicated. Jones GT, Schoenecker PL, Dias LS: Developmental hip dysplasia potentiated by inappropriate use of the Pavlik harness. J Pediatr Orthop 1992;12:722-726. Atar D, Lehman WB, Grant AD: Pavlik harness pathology. Isr J Med Sci 1991;27:325-330.
References:
- Weinstein SL: Developmental hip dysplasia and dislocation, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 903-950.
Question 82High Yield
What is the current 5-year survival rate for patients with classic nonmetastatic, high-grade osteosarcoma of the extremity?
Explanation
Multidisciplinary treatment combining systemic chemotherapy and adequate surgical resection has resulted in a 5-year survival rate of 70% in patients with nonmetastatic osteosarcoma of the extremity . The advent of effective chemotherapy has increased the overall survival rate from 20% to 70% in current studies. Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Question 83High Yield
What nerve is at the highest risk for injury with a percutaneous repair of an Achilles tendon injury?
Explanation
Cadaver and clinical studies have shown that the sural nerve is at the highest risk for injury with a percutaneous repair of the Achilles tendon.
Question 84High Yield
During anterior surgery on the cervical spine, at what level would the lateral dissection of the longus coli muscle most likely cause Horner's syndrome?
Explanation
The sympathetic chain approaches the lateral border of the longus coli muscle at C6 and is more vulnerable to injury at this level. Injury to the chain will cause Horner's syndrome, usually seen as unilateral ptosis.
Question 85High Yield
Figure 48 shows an MRI scan of the knee. The arrow is pointing to what structure?
Explanation
The arrow points to the biceps femoris, which is inserted onto the fibula. The biceps femoris lies at the posterolateral aspect of the thigh. The semimembranosus and the semitendinous lie at the posterior medial aspect of the thigh. Gray H: Anatomy of the Human Body. Philadelphia, PA, Lea and Febiger, 1918, 2000.
Question 86High Yield
What artery provides the only direct vascularizaton to both the intraneural and extraneural blood supply of the ulnar nerve just proximal to the cubital tunnel?
Explanation
The superior ulnar collateral, inferior ulnar collateral, and posterior ulnar recurrent arteries provide consistent vascular supply to the ulnar nerve. This supply is segmental in nature. No identifiable direct anastomosis is seen between the superior ulnar collateral and the posterior ulnar recurrent arteries. The inferior ulnar collateral artery provides the only direct vascularization to the nerve and is located in the region just proximal to the cubital tunnel. The segmental nature of the blood supply to the ulnar nerve underscores the importance of its preservation during transposition.
Question 87High Yield
A 40-year-old man has a painless mass around his left ankle. He notes minimal growth over the past year. An MRI scan is shown in Figure 73a, and biopsy specimens are shown in Figures 73b and 73c. What is the most likely diagnosis?


Explanation
The biopsy specimen is a low-power view of a soft-tissue sarcoma with a biphasic pattern of epithelial cells and fibrous spindle cells that are typical of a synovial sarcoma. A deep, painless soft-tissue mass greater than 5 cm in size is suspicious for a sarcoma. The imaging in this patient is indeterminate and the patient requires a biopsy for an accurate diagnosis. The biopsy reveals a tumor with a biphasic appearance consistent with a synovial sarcoma. These tumors are slow growing, occur primarily in the lower extremities, and are found in a younger demographic population compared to malignant fibrous histiocytoma and liposarcoma. They can occur in a biphasic pattern with clumps of epithelial cells and fibrous spindle cells or in a monophasic pattern. Synovial sarcomas stain positively for keratin. Keratin is positive in nearly all biphasic types and in many tumors of the monophasic fibrous type. Sixty percent of these tumors are found in the lower extremity. The area around the knee is the most common location, followed by the ankle and foot. Epithelioid and clear cell sarcomas are found associated with tendon sheaths of the hand and feet and are generally smaller in size. Epithelioid sarcoma may resemble granulomatous inflammation histologically; clear cell sarcoma is composed of nests of clear cells with occasional multinucleated giant cells. Pigmented villonodular synovitis is found within the synovium and is characterized by a villous histologic appearance with hemosiderin-laden macrophages. Malignant fibrous histiocytoma has a storiform histologic pattern with an abundance of pleomorphic cells. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 757.
Question 88High Yield
Figure 54 shows the preoperative radiograph of a 45-year-old woman who is considering total hip arthroplasty with her orthopaedic surgeon. What femoral characteristic is a typical concern in this patient?
Explanation
Explanation
Developmental dysplasia of the hip (DDH) leads to early arthritis of the hip as seen in this patient. Although DDH is believed to mostly affect the acetabulum, most patients with DDH also have anatomic aberrations of the femur. Using three-dimensional computer models generated by reconstruction of CT scans, dysplastic femurs were shown to have shorter necks and smaller, straighter canals than the controls. The shape of the canal became more abnormal with increasing subluxation. The studies also have shown that the primary deformity of the dysplastic femur is rotational, with an increase in anteversion of 5 degrees to 16 degrees, depending on the degree of subluxation of the hip. The rotational deformity of the dysplastic femur arises within the diaphysis between the lesser trochanter and the isthmus and is not attributable to a torsional deformity of the metaphysis. Osteopenia is not a concern in a patient with an excellent cortical index (thick cortices and narrow canal). Femoral varus or bowing of the femur is not a typical finding in patients with DDH. Noble PC, Kamaric E, Sugano N, et al: Three-dimensional shape of the dysplastic femur: Implications for THR. Clin Orthop 2003;417:27-40.
References:
- Sugano N, Noble PC, Kamaric E, et al: The morphology of the femur in developmental dysplasia of the hip. J Bone Joint Surg Br 1998;80:711-719.
Question 89High Yield
Figures 57a through 57c show the radiographs of a patient who has pain, discomfort, and a popping sensation localized to the posterior aspect of the knee after undergoing primary left total knee arthroplasty 6 months ago. Examination reveals that the patient is able to ambulate without a limp. There is no significant swelling, erythema, or effusion. Range of motion is 0 degrees to 115 degrees, and a palpable crepitation or snapping is detected at the posterior lateral joint line. What is the most likely diagnosis?


Explanation
Popliteal snapping syndrome represents the most likely diagnosis. Barnes and Scott noted that the popliteus tendon can be a potential source of internal derangement after total knee arthroplasty. They noted that it can be subluxated anteriorly and posteriorly over a retained lateral femoral condyle osteophyte. Allardyce and associates described the condition as a popliteus condition, snapping as it rolls over a retained lateral femoral condylar osteophyte. Patellar clunk syndrome is a distinct syndrome associated with the patella and has been reported in posterior stabilized knees. In addition to crepitation with range of motion, the patella literally snaps or jumps as the knee is taken from flexion to extension. Beight JL, Yao B, Hozack WJ, et al: The patellar "clunk" syndrome after posterior stabilized total knee arthroplasty. Clin Orthop 1994;299:139-142. Barnes CL, Scott RD: Popliteus tendon dysfunction following total knee arthroplasty. J Arthroplasty 1995;10:543-545.
Question 90High Yield
Figure 2 shows the radiograph of a 26-year-old auto mechanic who injured his right dominant elbow in a fall during a motocross race. Examination reveals pain and catching that limits his range of motion to 45 degrees of supination and 20 degrees of pronation. The interosseous space and distal radioulnar joint are stable. Management should consist of
Explanation
Explanation
The radial head is an important secondary stabilizer of the elbow, helping to resist valgus forces. There has been a movement toward open reduction and internal fixation of the radial head when technically feasible, especially in a relatively high-demand athlete or laborer. The examination and radiograph suggest that displacement of the fragment is great enough to create a mechanical block. Extended splinting would only serve to encourage arthrofibrosis. Early range of motion is appropriate if there is minimal displacement of the radial head fragement, it is stable, and there is no mechanical block to motion. Fragments larger than one third of the joint surface should be excised only if it is not possible to reduce and repair the fragment. Primary excision of the radial head should be avoided if possible. Complications after excision of the radial head include muscle weakness, wrist pain, valgus elbow instability, heterotopic ossification, and arthritis. Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
References:
- Esser RD, Davis S, Taavao T: Fractures of the radial head treated by internal fixation: Late results in 26 cases. J Orthop Trauma 1995;9:318-323.
Question 91High Yield
Figures 42a and 42b show the radiographs of a 52-year-old man who sustained a fall from a motorcycle 6 months ago and now reports pain and stiffness in his left shoulder. What is the most reliable treatment to improve function and comfort of the shoulder?
Explanation
Explanation
42b Appropriate treatment is based on multiple considerations, which include the chronicity of the dislocation, the amount of humeral head involvement, the medical condition, and functional limitations of the patient. It has been shown that shoulder arthroplasty for locked posterior dislocation provides pain relief and improved motion. Transfer of the lesser tuberosity with its attached subscapularis tendon into the defect is recommended for anteromedial humeral defects that are smaller than approximately 40% of the joint surface. Subscapularis transfer as described by McLaughlin and the modification thereof later described by Hawkins and associates in which the lesser tuberosity is transferred into the defect, have yielded good results if the defect is less than 40% of the humeral head. Prosthetic replacement is preferred for larger defects. If the dislocation is less than 3 weeks old and has less than 25% of humeral head involvement, closed reduction with the patient under general anesthesia should be attempted and the stability assessed by internally rotating the arm. If the arm can be safely internally rotated to the abdomen, then 6 weeks of immobilization in an orthosis that maintains the shoulder in slight extension and external rotation can yield a good result. If the dislocation has been present for more than 3 weeks, closed reduction becomes exceedingly difficult. Gerber C, Lambert SM: Allograft reconstruction of segmental defects of the humeral head for the treatment of chronic locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1996;78:376-382. Spencer EE Jr, Brems JJ: A simple technique for management of locked posterior shoulder dislocations: Report of two cases. J Shoulder Elbow Surg 2005;14:650-652. Sperling JW, Pring M, Antuna SA, et al: Shoulder arthroplasty for locked posterior dislocation of the shoulder. J Shoulder Elbow Surg 2004;13:522-527. Hawkins RJ, Neer CS II, Pianta RM, et al: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
References:
- McLaughlin HL: Posterior dislocation of the shoulder. J Bone Joint Surg Am 1952;34:584-590.
Question 92High Yield
Figure 33 shows the CT scan of a 40-year-old man who injured his left shoulder while skiing. What structure is attached to the bony fragment?
Explanation
Explanation
The scan reveals a bony Bankart lesion. The anterior band of the inferior glenohumeral ligament is the major restraint to anterior translation of the humeral head and is usually injured with anterior shoulder dislocations. It inserts onto the glenoid labrum at the anteroinferior aspect of the glenoid rim. The labrum most frequently avulses from the glenoid (Bankart lesion), but occasionally the bony attachment is avulsed. O'Brien SJ, Neves MC, Arnoczky SP, et al: The anatomy and histology of the inferior glenohumeral ligament complex of the shoulder. Am J Sports Med 1990;18:449-456.
References:
- Warner JP: The gross anatomy of the joint surfaces, ligaments, labrum and capsule, in Matsen FA, Fu FF, Hawkins RJ (eds): The Shoulder: A Balance of Mobility and Stability. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1992, pp 7-28.
Question 93High Yield
Which of the following statements best describes synovial fluid?
Explanation
Synovial tissue is composed of vascularized connective tissue that lacks a basement membrane. Two cell types (type A and type B) are present: type B cells produce synovial fluid. Synovial fluid is made of hyaluronic acid and lubricin, proteinases,and collagenases. It is an ultrafiltrate of blood plasma added to fluid produced by the synovial membrane. It does not contain erythrocytes, clotting factors, or hemoglobin. It lubricates articular cartilage and provides nourishment via diffusion. Synovial fluid exhibits non-Newtonian flow characteristics. The viscosity coefficient is not a constant, the fluid is not linearly viscous, and its viscosity increases as the shear rate decreases.
Question 94High Yield
Figure 36a shows the current radiograph of a 65-year-old woman who slipped and fell. History reveals that prior to the fall she was actively functioning without pain. Figure 36b shows a radiograph obtained 1 year ago. Based on the fracture pattern, the failure is most likely related to

Explanation
The radiograph shows a fracture distal to the prosthesis in a stable, apparently well-fixed prosthetic stem. The well-fixed prosthesis-bone composite is stiff, creating a modulus mismatch between the proximal and distal femur. Therefore, the risk of fracture, particularly in osteoporotic bone, is increased at this level. Revision of the stem to a longer construct is unnecessary, and standard plate and screw fixation has been shown to yield union rates of greater than 90%. Nonsurgical treatment of fractures distal to the tip of the prosthesis results in high nonunion rates, reported to be from 25% to 42%. Johansson JE, McBroom R, Barrington TW, Hunter GA: Fracture of the ipsilateral femur in patients with total hip replacement. J Bone Joint Surg Am 1981;63:1435-1442. Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Question 95High Yield
Figure 23 shows the radiograph of a 55-year-old man who underwent a total hip arthroplasty 5 years ago. Management should now consist of
Explanation
Because the radiograph shows that the femoral stem is loose within the femoral canal and there is a fracture in the distal cement mantle, the stem should be revised. The Ogden-type plate and the allograft bone plates will reconstruct the femur but will not restore stability to the stem. Similarly, traction may allow the femur to heal but will not restore stability to the femoral stem within the femur. Resection arthroplasty is considered a salvage option following failure of the other procedures. Lewallen DG, Berry DJ: Periprosthetic fracture of the femur after total hip arthroplasty: Treatment and results to date, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-249.
Question 96High Yield
Which of the following benign bone lesions can develop lung metastases?
Explanation
Although considered benign bone lesions, lung metastases can develop in giant cell tumors and chondroblastomas. These often can be treated with multiple thoracotomies, resulting in long-term survival. Roberts PF, Taylor JG: Multifocal benign chondroblastomas: Report of a case. Hum Pathol 1980;11:296-298.
Question 97High Yield
Figure 8 shows the radiograph of a 72-year-old man who has had severe pain in the left hip for the past 3 weeks. History reveals alcohol abuse. The next most appropriate step should consist of
Explanation
Explanation
The radiograph reveals destruction of the femoral head with loss of the articular cartilage. These findings are consistent with an infected hip, and aspiration will confirm the diagnosis. Although the patient could have advanced osteonecrosis, typically the cartilage interval is maintained and such destruction is rarely associated with osteonecrosis.
References:
- Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 157-161.
Question 98High Yield
Figure 52 shows the MRI scan of a 28-year-old baseball pitcher. Examination will most likely reveal which of the following findings?
Explanation
A ganglion cyst compressing the suprascapular nerve results in poorly localized pain in the shoulder girdle. Sensation is intact, with weakness of external rotation and abduction. Supraspinatus and infraspinatus atrophy is often noted when viewed from behind. These cysts are typically associated with labral tears. Deltoid weakness is associated with an axillary nerve injury, and scapular winging results from injury to the long thoracic nerve. Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Question 99High Yield
Closed-chain exercise differs from open-chain exercise in which of the following ways?
Explanation
Explanation
Closed-chain exercise requires the distal portion of the extremity to be fixed. It is more commonly used in lower extremity exercise, and movement is produced by co-contraction of muscles. Joint compression is increased, and multiple joints are involved with closed-chain exercise. In open-chain exercise, the distal portion of the extremity is free. Braddom RL (ed): Physical Medicine and Rehabilitation, ed 2. Philadelphia, PA, Saunders, 2000, pp 975-976.
References:
- Childs DC, Irrang JJ: The language of exercise and rehabilitation, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 329.
Question 100High Yield
Which of the following tendons is the primary antagonist of the posterior tibialis tendon?
Explanation
The primary action of the posterior tibialis tendon is inversion of the foot; secondarily, it plantar flexes the ankle. The anterior tibialis tendon also inverts the foot and only partially antagonizes the posterior tibialis tendon. The primary action of the peroneus longus is plantar flexion of the first ray. It secondarily everts the posterior tibialis tendon. The action of the flexor digitorum longus tendon is synergistic with the posterior tibialis tendon. The primary action of the peroneus brevis tendon is eversion; therefore, it is the primary antagonist of the posterior tibialis tendon. Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 550-551.
You Might Also Like
Previous Chapter100 Orthopedic Board Review MCQs: Mock Exam Set #280
Next Chapter Orthopedic Board Review: 100 High-Yield MCQs | Mock Exam Se…

Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon