Orthopedic Board Review MCQs: Mock Exam 435 (100 Questions)
14 Apr 2026
104 min read
122 Views
Key Takeaway
This page offers 100 high-yield orthopedic board review questions designed to help surgeons master their ABOS, OITE, and FRCS exams. As Mock Exam Set #435, it provides comprehensive, randomized multiple-choice questions covering critical orthopedic concepts. Practice now to enhance your knowledge and exam readiness for certification.
Master the Hip Anterolateral Approach: Techni...
00:00
Start Quiz
Question 1High Yield
In the normal adult, the distance between the basion and the tip of the dens with the head in neutral position is how many millimeters?
Explanation
In the normal adult, the distance between the basion and the tip of the dens is 4 mm to 5 mm. Any distance greater than 5 mm is considered abnormal. This is one way to detect occipitocervical dissociation other than using the Power's ratio, which relies on an anterior dislocation. Wiesel SW, Rothman RH: Occipitoatlantal hypermobility. Spine 1979;4:187-191.
Question 2High Yield
A 21-year-old basketball player inverts his foot during practice. Examination reveals obvious deformity of the hindfoot with a prominence of the talar head dorsolaterally and medial displacement of the forefoot. A radiograph is shown in Figure 17. What is the most likely obstacle to closed reduction?
Explanation
The patient has a medial subtalar dislocation. These injuries should be reduced as soon as possible to minimize risk to the skin. Most often, this can be done easily, and further radiographic evaluation then can be performed as necessary. On rare occasions, closed reduction is not possible because of fractures of the articular surface of the talus, navicular, interposed extensor digitorum brevis, or transverse fibers of the cruciate crural ligament. The posterior tibial tendon is the most common obstruction to closed reduction in lateral subtalar dislocations, which are less common than medial dislocations. The majority of both injuries can be managed by closed reduction and immobilization. Mulroy RD: The tibialis posterior tendon as an obstacle to reduction of a lateral anterior subtalar dislocation. J Bone Joint Surg Am 1953;37:859-863. Heckman JD: Fractures and dislocations of the foot, in Rockwood CA, Green DP, Bucholz RW (eds): Fractures in Adults. Philadelphia, PA, JB Lippincott, 1991, pp 2093-2100.
Question 3High Yield
What is the most common associated pathology in patients who have suprascapular nerve entrapment secondary to ganglion cysts?
Explanation
Explanation
It is well known that suprascapular nerve entrapment can be secondary to many entities, and its association with ganglion cysts and SLAP lesions has been well documented. Because of a superior labral tear, synovial fluid will leak out of the joint underneath the labrum, causing the cyst and secondary compression of the nerve. Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734. Iannotti JP, Ramesey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
References:
- Moore TP, Fritts HM, Quick DC, Buss DD: Suprascapular nerve entrapment caused by supraglenoid cyst compression. J Shoulder Elbow Surg 1997;6:455-462.
Question 4High Yield
A 15-year-old girl has left knee pain and an enlarging mass in the distal thigh. AP and lateral radiographs are shown in Figures 52a and 52b, and a biopsy specimen is shown in Figure 52c. What is the most likely diagnosis?
Explanation
Explanation
52b 52c A bone-producing lesion in the metaphysis of an adolescent is most likely an osteosarcoma. The radiographs show a distal femoral bone-producing lesion extending into the surrounding soft tissues. The histologic appearance consists of pleomorphic cells producing osteoid. Ewing's sarcoma and metastatic neuroblastoma do not produce a matrix. Chondrosarcoma is a radiographically destructive lesion with calcification and cartilage cells on histologic section. An osteochondroma is a benign cartilage lesion that is continuous with the medullary cavity of the underlying bone and extends into a bony lesion and covered by a cartilage cap. Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
References:
- Gibbs CP, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 5High Yield
Figures 38a and 38b show the AP and lateral radiographs of a 12-year-old baseball pitcher who has pain in his right dominant elbow. Management should consist of
Explanation
Explanation
38b The patient has a stress fracture of the olecranon; therefore, the most appropriate management is modification of activities below the threshold of symptoms to allow for healing. Ultrasound provides no benefit, and immobilization is not necessary. MRI is not necessary because there is no associated ligamentous injury. Arthroscopy is not indicated. Cabanela ME, Morrey BF: Fractures of the olecranon, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 2000, pp 365-379.
References:
- Nuber GW, Diment MT: Olecranon stress fractures in throwers: A report of two cases and a review of the literature. Clin Orthop 1992;278:58-61.
Question 6High Yield
When the elbow is extended and an axial load is applied, what percent of stress distribution occurs across the ulnohumeral and radiohumeral articular surface, respectively?
Explanation
When load is applied to the wrist, most of the stress is absorbed by the radius. As the load is transferred through the forearm, the interosseous membrane transfers some of the load from the radius to the ulna. The load at the elbow is distributed with 40% at the ulnohumeral articulation and 60% at the radiohumeral articulation. Halls AA, Travill R: Transmission of pressure across the elbow joint. Anat Rec 1964;150:243.
Question 7High Yield
Figure 11 shows the lateral radiograph of a 16-year-old boy who has been unable to participate in sports activities because of pain in the anterior aspect of the knee. He states that the pain is aching in nature and is located in the region of the tibial tuberosity. He denies having joint effusion or symptoms of instability. Management should consist of
Explanation
Explanation
The prognosis for most patients with Osgood-Schlatter disease is good. When the secondary ossification center unites with the main body of the tibial tubercle, the patellar tendon has a more rigid anchor, and heterotopic ossification and its associated reaction often become quiescent. However, even after closure of the growth plates, some patients have persistent symptoms. Excision of the ossicle and prominence of the tibial tuberosity decompresses the patellar tendon and allows most patients to resume sports activities. Nonsurgical modalities are ineffective. Better results have been reported after excision than after drilling of the tubercle. Excision of the ossicle is not indicated prior to skeletal maturity because symptoms will resolve in most patients when the secondary ossification center unites. Flowers MJ, Bhadreshwar DR: Tibial tuberosity excision for symptomatic Osgood-Schlatter disease. J Pediatr Orthop 1995;15:292-297.
References:
- Greene WB: Osteochondrosis and tibia vara, in Canale ST, Beaty JH (eds): Operative Pediatric Orthopaedics, ed 2. Philadelphia, Pa, Mosby, 1995, pp 804-854.
Question 8High Yield
A 20-year-old man sustains the injury shown in Figures 1a and 1b in a motorcycle accident. In addition to a prompt closed reduction, his outcome might be optimized by

Explanation
Lateral subtalar dislocations, which are less common than medial subtalar dislocations, are high-energy injuries that are frequently associated with small osteochondral fractures. It is generally recommended that large fragments be internally fixed, and small fragments entrapped within the joint be excised. Although arthrosis frequently occurs after this injury and is the most common long-term complication, primary subtalar arthrodesis is not indicated. A talar neck fracture is not evident on the radiographs, and lateral subtalar dislocation usually does not lead to instability.
Question 9High Yield
Where is the underlying defect in a rhizomelic dwarf with the findings shown in Figure 5?
Explanation
The radiograph shows the typical findings of achondroplasia. The defect is in fibroblast growth factor receptor 3. The pedicles narrow distally in the lumbar spine. The pelvis is low and broad with narrow sciatic notches and ping-pong paddle-shaped iliac wings. This is often called a champagne glass pelvis. Type I collagen abnormalities are typically found in osteogenesis imperfecta, and type II collagen defects are found in spondyloepiphyseal dysplasia and Kneist syndrome. COMP is defective in multiple epiphyseal dysplasia. Sulfate transport defects are seen in diastrophic dysplasia. Johnson TR, Steinbach LS: Essentials of Musculoskeletal Imaging. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 809-812.
Question 10High Yield
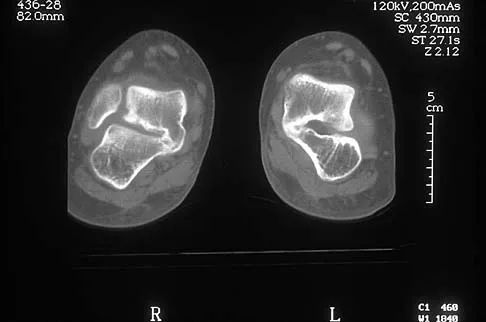
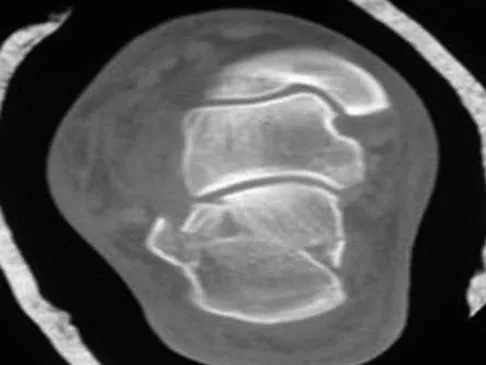
A 12-year-old boy has had progressive pain and flatfeet for the past year. Pain is increased with weight-bearing activities. Examination reveals that subtalar motion is absent. On standing, the patient has obvious hindfoot valgus and loss of the normal arch bilaterally. Plain radiographs are shown in Figures 43a through 43c, and a CT scan is shown in Figure 43d. What is the most likely diagnosis?


Explanation
The axial views show fusion of the talus and calcaneus at the medial facet (talocalcaneal coalition). Peroneal spastic flatfoot is a descriptive term applying to the symptoms of painful flatfoot associated with apparent peroneal spasm and is sometimes caused by tarsal coalition; however, this is not the most appropriate diagnosis for this patient. Flexible flatfoot with a short Achilles tendon often causes symptoms similar to the ones listed above, but subtalar motion should be normal. A diagnosis of calcaneonavicular coalition can be made based on plain oblique views of the foot but is not seen in these views. Posterior tibial tendon dysfunction in the absence of other pathology is uncommon in children. Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 11High Yield
A 7-year-old girl has pain and a mass in the left scapula. A MRI scan and biopsy specimen are shown in Figures 30a and 30b. After staging studies, initial management should consist of

Explanation
The histology shows small round blue cells that are uniform in appearance; these findings are consistent with Ewing's sarcoma. The MRI scan shows infiltration of the marrow and a large surrounding soft-tissue mass. Based on these findings, the management of choice is systemic chemotherapy. Local control of the primary lesion is addressed by either surgical resection or radiation therapy or a combination of the two after the patient receives systemic chemotherapy. The clinical, radiographic, and histologic presentation of Ewing's sarcoma often can be confused with osteomyelitis. The histology shows an absence of inflammatory cells. Grier HE: The Ewing family of tumors: Ewing's sarcoma and primitive neuroectodermal tumors. Pediatr Clin North Am 1997;44:991-1004.
Question 12High Yield
A 52-year-old woman has bicompartmental osteoarthritis following patellectomy. Treatment should consist of
Explanation
The patient has extensive degenerative changes in both the medial and lateral compartments within the knee; therefore, arthroscopic debridement or an osteotomy will not be helpful. A patellar arthroplasty will not address the medial and lateral compartments. Because the extensor mechanism provides a significant amount of anteroposterior stability, a posterior cruciate-substituting total knee arthroplasty is the treatment of choice for this patient. Martin SD, Haas SB, Insall JN: Primary total knee arthroplasty after patellectomy. J Bone Joint Surg Am 1995;77:1323-1330.
Question 13High Yield
A 43-year-old bus driver sustains a hyperextension injury to her arm and shoulder 4 months after undergoing an open Bankart repair. Examination reveals increased external rotation, anterior shoulder pain, and internal rotation weakness. Her examination also reveals the findings shown in Figure 44. What is the most likely diagnosis?
Explanation
An isolated tear of the subscapularis tendon has been noted as early as 1835 by Smith. In Gerber and associates' 1991 report of 16 men with an average age of 51 years, isolated subscapularis tendon rupture was often caused by a violent hyperextension injury. All patients reported pain anteriorly along with night pain. They also noted pain and weakness of the arm. The lift-off test is performed by having the patient lift the palm of the hand away from the small of the back. The patient must have sufficient internal rotation to allow this test to be performed. A subscapularis rupture is likely if the patient cannot perform the lift-off test. Hertel R, Ballmer FT, Lombert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-313. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394. Greis PE, Kuhn JE, Schultheis J, Hintermeister R, Hawkins R: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Question 14High Yield
A 24-year-old man who was involved in a high speed motor vehicle accident is transferred for definitive care after having been diagnosed with an acute spinal cord injury from a fracture-dislocation at C6-7. He has a complete C6 neurologic level and it is now approximately 10 hours from his injury. What is the most appropriate pharmacologic treatment at this time?
Explanation
Explanation
The standard practice in the pharmacologic treatment of a spinal cord injury in the United States has been the administration of methylprednisolone with an initial bolus of 30 mg/kg followed by 5.4 mg/kg for 24 hours, in accordance with the findings of the second and third National Acute Spinal Cord Injury Studies (NASCIS). Although the studies have subsequently drawn criticism for their methodology and outcomes, it has been generally accepted that beneficial neurologic outcomes were anticipated in patients who were able to start the protocol within 8 hours of their initial injury. Further improvement was noted in patients receiving the methylprednisolone within 3 hours of their injury and continuing an infusion for 48 hours. In this patient, who is outside the 8-hour treatment window, no studies have supported starting the methylprednisolone protocol at this time. Braken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
Question 15High Yield
A 68-year-old woman underwent a successful total right hip arthroplasty with a metal-on-metal articulation and cementless porous-coated components. Three months later, she underwent identical surgery on the left hip. Three months after surgery on the left hip, she reports groin pain on ambulation. Examination reveals significant groin discomfort with passive hip motion, particularly at the extremes of motion. Radiographs are shown in Figures 21a and 21b. Laboratory studies show an erythrocyte sedimentation rate of 35 mm/h and a C-reactive protein of 0.9. Aspiration yields scant growth of Staphylococcus epidermidis in the broth only, with no evidence of loosening on arthrography. A second aspiration yields scant growth of Staphylococcus epidermidis in the broth only. What is the most likely cause of the patient's pain?
Explanation
Explanation
21b The difference in the clinical results combined with the laboratory findings points to infection. While there is a significant risk of false-positive findings with aspiration, the fact that two successive aspirations grew the same organism strongly suggests infection. The radiograph shows that there is more radiolucency around the left acetabular component than the right component. White RE: Evaluation of the painful total hip arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, vol 2, pp 1377-1385.
References:
- Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
Question 16High Yield
A 19-year-old woman has a painful right knee. A radiograph, MRI scan, CT scan, and histopathologic specimen are shown in Figures 24a through 24d. What is the most likely oncologic stage of the lesion?



Explanation
The patient has a high-grade osteosarcoma of the distal femur with a skip lesion, and pulmonary metastasis is seen on the CT scan. This corresponds to a stage III lesion according to the Musculoskeletal Tumor Society System as adopted from Enneking.
Question 17High Yield
What type of brace is shown in Figures 22a and 22b?
Explanation
Explanation
22b The figures show a Charcot restraining orthotic walker (CROW). This brace has been used as a customized total contact fit removable brace to maintain foot alignment as the patient evolves from Eichenholz stage 1 to Eichenholz stage 3 Charcot arthropathy. Mehta JA, Brown C, Sargeant N: Charcot restraint orthotic walker. Foot Ankle Int 1998;19:619-623.
References:
- Morgan JM, Biehl WC III, Wagner FW Jr: Management of neuropathic arthropathy with the Charcot restraint orthotic walker. Clin Orthop 1993;296:58-63.
Question 18High Yield
Figures 35a and 35b show the radiographs of a patient who underwent debridement of a chronically infected, fully constrained knee prosthesis and now reports pain and instability despite bracing. History reveals that the patient has had no drainage since undergoing the last debridement 6 months ago. A C-reactive protein level and aspiration are negative for infection. Treatment should now consist of

Explanation
The radiographs show a significant loss of the proximal anterior tibial cortex, consistent with an extensively damaged or deficient extensor mechanism. Such a deficit precludes insertion of another knee arthroplasty. Arthrodesis is the treatment of choice for this patient and is indicated for loss of the extensor mechanism and knee instability. A recent report on arthrodesis following removal of an infected prosthesis showed a union rate of 91% using a short intramedullary nail. Insertion of an antibiotic-impregnated PMMA spacer is not indicated because the rationale for using a spacer is to maintain a space for reinsertion of another prosthesis. Reconstruction of the extensor mechanism would not address the loss of the joint. Amputation is the final treatment option if the arthrodesis fails. Rand JA: Alternatives to reimplantation for salvage of the total knee arthroplasty complicated by infection. J Bone Joint Surg Am 1993;75:282-289. Lai KA, Shen WJ, Yang CY: Arthrodesis with a short Huckstep nail as a salvage procedure for failed total knee arthroplasty. J Bone Joint Surg Am 1998;80:380-388.
Question 19High Yield
What is the most common surgical cause of the foot deformity shown in Figure 9?
Explanation
The radiograph shows a hallux varus deformity. Iatrogenically acquired hallux varus is most often the result of excessive lateral soft-tissue release, sesamoidectomy, or both. It also can be caused by a medial tibial sesamoid subluxation in conjunction with excessive postoperative dressing application, overcorrection of the intermetatarsal angle, or excessive medial eminence resection. Donley BG: Acquired hallux varus. Foot Ankle Int 1997;18:586-592.
Question 20High Yield
When a structure like a long bone is under a bending load, its maximum stress is most dependent on what factor?
Explanation
The maximum stress in a bone occurs at the periosteal surface (the greatest distance from the center of the bone). The magnitude of the stress is equal to the magnitude of the applied moment (M) multiplied by the distance to the surface (roughly the radius of the bone, r) divided by the area moment of inertia (I), so that stress = Mr/I. Of the possible answers, only area moment of inertia of the cross section contains any of these three items. The stress can also depend on the length of the bone, but it cannot be determined without knowing the location at which the bending load is applied, information that was not given in the problem. The type of structural support may influence local stresses where the support contacts the bone, but it has little effect on the maximum stress in the bone. The cross-sectional area is not as important as the area moment of inertia because the stress is not evenly distributed over the cross-section. Plastic modulus is a material property, not a geometric or structural property, and it does not affect stress. Hayes WC, Bouxsein ML: Biomechanics of cortical and trabecular bone: Implications for assessment of fracture risk, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 76-82.
Question 21High Yield
Which of the following is accurate regarding low-molecular-weight heparin used for deep venous thrombosis (DVT) prophylaxis in total joint arthroplasty?
Explanation
Low-molecular-weight heparin is highly bioavailable with a half-life of 3 to 18 hours. This is greater than the 1 hour half-life of unfractionated heparin. Low-molecular-weight heparin offers an advantage over unfractionated heparin by selectively targeting Factor Xa while having a lesser effect on circulating thrombin (Factor IIa). Circulating thrombin Factor IIa is needed for local hemostasis at the site of the surgical wound. Clinical studies have shown a reduction by one third in the incidence of thrombocytopenia with the use of low-molecular-weight heparin. Low-molecular-weight heparin has been shown to demonstrate similar clinical results compared to warfarin with respect to preventing thromboembolic disease after total hip arthroplasty and complications such as bleeding. Zimlich RH, Fulbright BM, Friedman RJ: Current status of anticoagulation therapy after total hip and total knee arthroplasty. J Am Acad Orthop Surg 1996;4:54-62. Colwell CW Jr, Spiro TE, Trowbridge AA, et al: Use of enoxaparin, a low-molecular-weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14.
Question 22High Yield
A 20-year-old man has a symptomatic lesion of fibrous dysplasia in the femoral neck. Management should consist of
Explanation
Explanation
Fibrous dysplasia in the femoral neck frequently warrants treatment because of the risk of pathologic fracture. Cortical strut grafts reduce the risk of local recurrence compared with cancellous bone grafting. Because of the consequences associated with fracture in this location, prophylactic fixation is recommended. Radiation therapy and chemotherapy are not used for this benign condition. Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 197.
References:
- Enneking WF, Gearen PF: Fibrous dysplasia of the femoral neck: Treatment by cortical bone grafting. J Bone Joint Surg Am 1986;68:1415.
Question 23High Yield
A 65-year-old man with ankylosing spondylitis sustains an extension injury to his cervical spine. Two days later, a progressive neurologic deficit develops at the C6 level. An MRI scan is shown in Figure 1. What is the most likely diagnosis?
Explanation
It is common for patients with ankylosing spondylitis to sustain extension-type fractures, typically near the cervicothoracic junction. These fractures can be minimally displaced, making them difficult to diagnose. In addition, the vertebral bodies are vascular and their canals are relatively enclosed, making them vulnerable to epidural bleeding. The MRI scan shows an epidural hematoma posteriorly compressing the cord. Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142. Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spine fracture and spinal stenosis in ankylosing spondylitis. J Neurosurg 1982;57:609-616.
Question 24High Yield
What is the effect on knee kinematics following placement of an anterior cruciate ligament (ACL) graft at the 12 o'clock position?
Explanation
Explanation
Endoscopic ACL reconstructive techniques may result in a vertical graft placement. The reconstructed ligament will resist anterior translation of the tibia but the graft will not restore rotatory stability. Decreased flexion and extension are caused by placement of the femoral tunnel too anterior and posterior, respectively. Impingement of the graft on the femoral notch is caused by anterior placement of the tibial tunnel or inadequate notchplasty. Scopp JM, Jasper LE, Belkoff SM, et al: The effect of oblique femoral tunnel placement on rotational constraint of the knee reconstructed using patellar tendon autografts. Arthroscopy 2004;20:294-299.
References:
- Carson EW, Simonian PT, Wickiewicz TL, et al: Revision anterior cruciate ligament reconstruction. Instr Course Lect 1998;47:361-368.
Question 25High Yield
The condition shown in Figures 9a and 9b is most likely the result of

Explanation
The clinical photograph and radiograph show gout, which is the result of urate deposition in the joint and soft tissues. Radiographs frequently reveal periarticular erosions. The crystals are intracellular and negatively birefringent under the polarized microscope. Treatment for acute flares include colchicines, indomethacin, and corticosteroids (including injections). Medications such as allopurinol help prevent recurrent flares. Tophi such as that seen in this patient are often confused with and associated with infection. Wortmann RL, Kelley WM: Crystal-induced inflammation: Gout and hyperuricemia, in Harris ED, Budd RC, Firestein GS, et al (eds): Kelley's Textbook of Rheumatology, ed 7. New York, NY, Elsevier Science, 2005, pp 1402-1429. Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 26High Yield
An extended head hemiarthroplasty (rotator cuff tear arthropathy head) has what theoretic advantage when compared to a standard hemiarthroplasty?
Explanation
Explanation
The theoretic advantage of a metal-to-bone articulation with the acromion is that there is a greater arc in which a smooth metal surface contacts the glenoid and acromion. This may improve pain and function, but no studies have evaluated this to date. One study showed results comparable to that of a standard hemiarthroplasty. There are no other biomechanic advantages. Visotsky JL, Basamania C, Seebauer L, et al: Cuff tear arthropathy: Pathogenesis, classification, and algorithm for treatment. J Bone Joint Surg Am 2004;86:35-40.
References:
- Zuckerman JD, Scott AJ, Gallagher MA: Hemiarthroplasty for cuff tear arthropathy. J Shoulder Elbow Surg 2000;9:169-172.
Question 27High Yield
A patient undergoes hip arthroscopy, and the pathology is seen in Figure 18. What is the most likely diagnosis?
Explanation
The motorized shaver is adjacent to the acetabular labrum, which is torn. The femoral head and acetabulum are normal in appearance. Neither the fat pad nor a loose body is identified.
Question 28High Yield
The Keller proximal phalanx resection procedure is most useful for which of the following conditions?
Explanation
Explanation
A Keller proximal phalanx resection procedure usually results in reduced weight bearing under the first ray because of shortening of the toe and disruption of intrinsic flexor function. This can be an effective method of offloading a neuropathic ulcer under the great toe at the interphalangeal or metatarsophalangeal joint area. However, these features are generally undesirable in young active patients. The procedure has a high rate of recurrent deformity in patients with rheumatoid arthritis. It would exacerbate transfer metatarsalgia in a patient with a hypermobile first ray. Lin SS, Bono CM, Lee TH: Total contact casting and Keller arthroplasty for diabetic great toe ulceration under the interphalangeal joint. Foot Ankle Int 2000;21:588-593.
References:
- Downs DM, Jacobs RL: Treatment of resistant ulcers on the plantar surface of the great toe in diabetics. J Bone Joint Surg Am 1982;64:930-933.
Question 29High Yield
The peroneus tertius is a commonly used landmark for arthroscopic portal placement. What is the function of this tendon?
Explanation
The peroneus tertius, although absent in 10% of the population, originates on the distal third of the extensor surface of the fibula and inserts onto the base of the fifth metatarsal, possibly extending to the fascia over the fourth interosseous space. The muscle is located in the anterior compartment of the leg and is innervated by the deep peroneal nerve. The tendon produces dorsiflexion and eversion when walking and can be used as an insertion point during tendon transfers to assist dorsiflexion. This tendon is peculiar to humans and is a proximally migrated deep extensor of the fifth toe. Joshi SD, Joshi SS, Athavale SA: Morphology of the peroneus tertius muscle. Clin Anat 2006;19:611-614. Williams PL, Bannister LH, Berry MM, et al (eds): Gray's Anatomy, ed 38. London, Churchill Livingston, 1995, p 883.
Question 30High Yield
A 19-year-old man was struck by a car and is seen in the emergency department with a grade IIIC open distal tibia and fibula fracture. Examination reveals that the toes are cool and dusky with a sluggish capillary refill. Angiography reveals a lesion in the posterior tibial artery amenable to repair. There is no sensation on the plantar aspect of the foot, and he is unable to flex his toes. A clinical photograph and radiograph are shown in Figures 2a and 2b. What is the next most appropriate step in management?
Explanation
Explanation
2b In the past, loss of plantar sensation in this grade IIIC tibial fracture would have been an indication for below-knee amputation regardless of the potential for vascular repair. However the 2002 LEAP study divided 55 patients with loss of plantar sensation into two groups, the insensate amputation group and the insensate limb salvage group, with 55% of patients in the insensate salvage group regaining normal sensation 2 years after injury. Furthermore, those in the salvage group who remained insensate after 2 years had equivalent outcomes to those in the amputation group. Because of these findings, limb salvage with vascular repair and external stabilization with delayed closure is deemed appropriate treatment. Immediate intramedullary fixation is not indicated. Because ischemia, contusion, and stretch can adversely affect the tibial nerve, the additional insult of exploration of the nerve is also not advisable given the soft-tissue compromise. Bosse MJ, McCarthy ML, Jones AL, et al: The insensate foot following severe lower extremity trauma: An indication for amputation? J Bone Joint Surg Am 2005;87:2601-2608. Lange RH, Bach AW, Hansen ST Jr, et al: Open tibial fractures with associated vascular injuries: Prognosis for limb salvage. J Trauma 1985;25:203-208. Mackenzie EJ, Bosse MJ, Kellam JF, et al: Factors influencing the decision to amputate or reconstruct after high-energy lower extremity trauma. J Trauma 2002;52:641-649.
References:
- Baumgaertner MR, Tornetta P III (eds): Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 65-74.
Question 31High Yield
A 30-year-old man falls off a 7-foot ladder and sustains the injury seen in the radiograph and the CT scan shown in Figures 39a and 39b. Medical history is negative. Management of this injury should include which of the following?
Explanation
A Sanders type 2 intra-articular calcaneus fracture in a young healthy nonsmoker is best treated with open reduction and internal fixation. Whereas nonsurgical management is an option, Buckley and associates have shown that these fractures have a better outcome with surgical care. Percutaneous fixation is reserved for tongue-type fractures and subtalar arthrodesis is used in some type 4 fractures. External fixation has not been shown to be advantageous in closed fractures. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744. Sanders R: Displaced intraarticular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250.
Question 32High Yield
A 60-year-old woman has activity-related hip pain after undergoing arthroplasty 5 years ago. She has severe Parkinsonism and denies fevers or chills. Radiographs are shown in Figures 45a and 45b. What is the most likely cause of her pain?

Explanation
The radiographs reveal both cement debonding at the lateral shoulder of the prosthesis and a cement mantle fracture. Both of these indicate a loose femoral component. The radiographs show a stress fracture with reactive bone on the lateral femoral cortex in conjunction with the cement mantle fracture. The acetabular component shows no evidence of loosening. Heterotopic bone usually is not a source of pain when it is Brooker grade I, as in this case. Parkinsonism generally is not associated with hip pain. Harris WH, McCarthy JC, O'Neill DA: Femoral component loosening using contemporary techniques of femoral cement fixation. J Bone Joint Surg Am 1982;64:1063-1067. Callaghan JJ, Rosenberg AG, Rubash H (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 960, 1228-1229.
Question 33High Yield
Which of the following statements about injury of the anterior vascular structures during lumbar disk surgery is true?
Explanation
Explanation
Vascular injury most commonly occurs at L4-L5, followed by L5-S1 and are associated with use of the pituitary rongeur. Hohf reported that 17 of 58 patients died as a result. Early recognition and treatment of this complication is vital; unfortunately, intraoperative bleeding from the disk space may occur in up to 50% of these patients. Some may be first recognized in the recovery room. Common clinical findings include hypotension, tachycardia, and a rigid abdomen. Formation of an arteriovenous fistula is the most common vascular injury resulting from lumbar disk surgery but is usually not recognized until months after surgery. Cardiomegaly and high output cardiac failure are common presenting symptoms. Hohf RP: Arterial injuries occurring during orthopaedic operations. Clin Orthop 1963;28:21-37. Montorsi W, Ghiringhelli C: Genesis, diagnosis and treatment of vascular complications after intervertebral disk surgery. Int Surg 1973;58:233-235.
References:
- Stambough JL, Simeone FA: Vascular complications in spine surgery, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 323-341.
Question 34High Yield
A 36-year-old woman is brought to the emergency department intubated and sedated following a motor vehicle accident. She is moving her upper and lower extremities spontaneously. She cannot follow commands. CT scans are shown in Figures 7a through 7c. The initial survey does not reveal any other injuries. Initial management of the cervical injury should consist of immediate
Explanation
Explanation
7b 7c The patient has a bilateral facet dislocation of C6-C7 with preservation of at least some neurologic function. Urgent reduction is necessary. However, because she is sedated and unable to follow commands, an MRI scan is necessary before any closed or open posterior reduction to look for an associated disk herniation. If a disk herniation is present, it must be removed prior to any reduction maneuver to prevent iatrogenic neurologic injury. It is very unlikely that this injury can be reduced with an open anterior procedure alone. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 189-199.
Question 35High Yield
Figures 41a and 41b show the radiographs of a 22-year-old woman who has a bunion on her left foot. She denies pain in the foot, but she reports increasing difficulty with shoe wear. Management should consist of

Explanation
Surgery is not indicated in a patient who has a mild deformity and no pain. Shoe wear modifications should be recommended.
Question 36High Yield
Figure 6 shows a sagittal oblique MRI scan. The arrow is pointing to what structure?
Explanation
The meniscofemoral ligaments connect the posterior horn of the lateral meniscus to the intercondylar wall of the medial femoral condyle. The ligament of Humphrey (arrow) passes anterior to the posterior cruciate ligament, whereas the ligament of Wrisberg passes posterior to the posterior cruciate ligament. One or the other has been identified in 71% to 100% of cadaver knees, with the ligament of Wrisberg being more common. Clarke HD, Scott WN, Insall JN, et al: Anatomy, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 3-66.
Question 37High Yield
Figure 40 shows the MRI scan of a 23-year-old man with a history of recurrent anterior shoulder instability. What is the most likely diagnosis?
Explanation
The MRI scan shows an ALPSA lesion. This is also known as a medialized Bankart with medial displacement of the torn anterior labrum. During surgical stabilization, the labrum and periosteal sleeve must be mobilized and repaired laterally to reduce recurrent instability. A Perthes lesion is a nondisplaced labral tear. A GLAD lesion represents a nondisplaced anterior labral tear with an associated articular cartilage injury. Neviaser TJ: The anterior labroligamentous periosteal sleeve avulsion lesion: A cause of anterior instability of the shoulder. Arthroscopy 1993;9:17-21.
Question 38High Yield
A 30-year-old woman injures her knee while skiing. Based on the MRI scan shown in Figure 5, treatment should consist of
Explanation
The MRI scan demonstrates a grade III MCL tear. Basic science and clinical studies have shown that nonsurgical management is preferred for MCL tears. Functional rehabilitation and early motion have led to consistently better results than has surgical repair.
Question 39High Yield
A patient has had a locked posterior dislocation of the shoulder for the past 6 months. After undergoing total shoulder arthroplasty that includes adequate anterior releases and posterior capsulorrhaphy, the patient still exhibits posterior instability intraoperatively. The postoperative rehabilitation regimen should include
Explanation
Achieving stability in chronic locked posterior dislocations of the shoulder remains a difficult challenge. Intraoperative measures include decreased humeral retroversion, anterior releases, and posterior capsular tightening. Postoperative rehabilitation is of equal importance. Immobilization in an external rotation brace (10 degrees to 15 degrees) with the arm at the side for 4 to 6 weeks is recommended to decrease tension in the posterior capsule. When passive range-of-motion exercises are instituted, they should be performed in the plane of the scapula to avoid stress posteriorly. Internal rotation and supine elevation should be avoided for similar reasons. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 40High Yield
A 2-year-old girl has had a swollen right knee for the past 7 weeks. There is no history of significant trauma, and she has not had a fever or been ill. Her parents report that she is stiff in the morning but otherwise does not report pain. A CBC count and erythrocyte sedimentation rate are normal. Treatment with naproxen at appropriate doses for the past 2 weeks has resulted in some improvement. Radiographs show only soft-tissue swelling. Examination reveals a healthy-appearing child with a warm and swollen right knee that is only slightly tender but lacks full extension by 20 degrees. What is the next most appropriate step in management?
Explanation
Explanation
Up to 30% of children with juvenile rheumatoid arthritis (increasingly known now as juvenile idiopathic arthritis or JIA) already have potentially damaging uveitis at the time of diagnosis. This patient has typical oligoarticular JRA (JIA) and therefore is at significant risk for uveitis. MRI, radioisotope scanning, or an ACE level most likely would not provide additional useful diagnostic information because intra-articular derangement, osteomyelitis, or sarcoidosis are all unlikely. Arthrocentesis and triamcinolone hexacetonide joint injection might be indicated if continued use of nonsteroidal medication does not result in improvement, but should be held off for at least an additional 4 to 6 weeks to see if continued use of naproxen results in control of the arthritis. Wolf MD, Lichter PR, Ragsdale CG: Prognostic factors in the uveitis of juvenile rheumatoid arthritis. Ophthalmology 1987;94:1242. Cassidy JT, Petty RE: Textbook of Pediatric Rheumatology. Philadelphia, PA, WB Saunders, 2001, p 220.
References:
- Chalom ED, Goldsmith DP, Koehler MA, et al: Prevalence and outcome of uveitis in a regional cohort of patients with juvenile rheumatoid arthritis. J Rheumatol 1997;24:2031-2034.
Question 41High Yield
Figures 28a and 28b show AP and lateral radiographs of the knee. Based on these findings, which of the following structures has most likely been injured?

Explanation
The radiographs show a posterior knee dislocation. Knee dislocations almost always involve rupture of both the anterior and posterior cruciate ligaments. Collateral ligament injuries also are common. Arterial, nerve, and tendon injuries each occur in less than half of knee dislocations. Schenck RC Jr, Hunter RE, Ostrum RF, et al: Knee dislocations. Instr Course Lect 1999;48:515-522.
Question 42High Yield
Contraindications to cervical laminectomy as a treatment for cervical spondylotic myelopathy include which of the following findings?
Explanation
Explanation
Cervical laminectomy is an accepted treatment for multilevel cervical spondylotic myelopathy. When the compression is posterior, laminectomy addresses it directly; when the compression is anterior, it is addressed indirectly (the spinal cord floats posteriorly away from the anterior compression). Preexisting kyphosis is a contraindication to laminectomy because the cord is unable to float posteriorly away from the anterior compression, and the risk for increasing kyphosis is significant. Kyphosis after laminectomy is more likely to develop in younger patients who have fewer degenerative changes to stabilize the spine. Malone DG, Benzyl EC: Laminotomy and laminectomy for spinal stenosis causing radiculopathy or myelopathy, in Clark CR (ed.): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 817-825.
References:
- Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 673-680.
Question 43High Yield
A 35-year-old man has atraumatic painless limited elbow motion. Radiographs are shown in Figures 33a and 33b. What is the most likely diagnosis?

Explanation
Based on the radiographic findings, the patient has melorheostosis, a rare, benign connective tissue disorder that is characterized by a cortical thickening of bone. It produces a "dripping candle wax" appearance with dense hyperostosis that flows along the cortex. Ectopic bone formation is a consideration but is associated with injuries or burns. Bone infarcts produce intraosseous sclerosis typically affecting the distal femur with the "smoke up chimney" appearance. Infection is always a consideration but typically does not have the linear osteitis seen in melorheostosis. Juxacortical chondroma is a benign cartilage growth that arises from the capsule and may involve the underlying cortical bone but rarely the medullary canal. Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
Question 44High Yield
What is the most commonly reported complication following elbow arthroscopy?
Explanation
Explanation
The complication rate following elbow arthroscopy is reported at 5%. The most commonly reported complication is transient neurapraxia, with nerve transection remaining an unfortunate and rare event. While infection remains the most common serious complication, it is uncommon (0.8%). Synovial cutaneous fistula and compartment syndrome, while reported, are the least frequent complications of elbow arthroscopy. Kelly EW, Morrey BF, O'Driscoll SW: Complications of elbow arthroscopy. J Bone Joint Surg Am 2001;83:25-34.
References:
- Morrey BF: Elbow complication, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 519-522.
Question 45High Yield
A 19-year-old college student reports a 1-week history of wrist pain following an intramural rugby match. A PA radiograph is shown in Figure 6. He denies any prior wrist injury. What is the best course of action?
Explanation
The patient has a scaphoid fracture involving the proximal pole. Surgical treatment is recommended for such fractures because of the prolonged period of cast immobilization necessary and the increased risk of delayed union, nonunion, and/or osteonecrosis with nonsurgical management. A cannulated compression screw, inserted in the central scaphoid via a dorsal approach, is biomechanically advantageous and provides greater stability for fracture healing than Kirschner wires. Recently, good outcomes have been reported with arthroscopic-assisted percutaneous fixation of nondisplaced or minimally displaced scaphoid fractures. Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210. Chan KW, McAdams TR: Central screw placement in percutaneous screw scaphoid fixation: A cadaveric comparison of proximal and distal techniques. J Hand Surg Am 2004;29:74-79. Bedi A, Jebson PJ, Hayden RJ, et al: Internal fixation of acute non-displaced scaphoid waist fractures via a limited dorsal approach: An assessment or radiographic and functional outcomes. J Hand Surg Am 2007;32:326-333.
Question 46High Yield
A 52-year-old woman with diabetes mellitus has had a plantar foot ulcer under the second metatarsal head for the past week. The patient had a similar ulcer 2 months ago, and total contact casting resulted in healing. Examination reveals no signs of infection. What procedure will best prevent recurrence of the ulcer?
Explanation
The contracted Achilles tendon leads to increased forefoot pressure, thus increasing the risk for ulceration in neuropathic patients. Several studies have shown the benefit of Achilles tendon lengthening to heal and prevent forefoot ulceration in these patients. The flexor hallucis longus transfer is used for chronically torn/deficient Achilles tendons, not a contracted Achilles tendon. The Jones procedure works well for the first ray but does not help to alleviate pressure under the second ray. Peripheral bypass surgery is unnecessary because the ulcer healed during the initial treatment, indicating that the patient has adequate circulation. The posterior tibial tendon transfer is used for foot drop or other neuromuscular conditions to correct deformity and increase function. It is not used for forefoot ulcers in patients with diabetes mellitus. Armstrong DG, Stacpoole-Shea S, Nguyen H, et al: Lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot. J Bone Joint Surg Am 1999;81:535-538.
Question 47High Yield
A 45-year-old man has severe pain in both feet after his boots become wet while hunting. Examination 3 hours after the onset of symptoms reveals that his feet are cold to touch and the skin appears blanched. Management should consist of
Explanation
Explanation
The patient has frostbite involving both feet. Rapid rewarming in a protected environment is the initial treatment. A footbath with water at 104.0 degrees F to 107.6 degrees F (40 degrees C to 42 degrees C) is ideal. This facilitates a uniform rewarming of the involved tissue. The other choices are less than ideal. Appliances such as heating pads provide uneven heating and may actually burn the skin. Pinzur MS: Frostbite: Prevention and treatment. Biomechanics 1997;4:14-21.
References:
- Fritz RL, Perrin DH: Cold exposure injuries: Prevention and treatment. Clin Sports Med 1989;8:111-128.
Question 48High Yield
A 14-year-old boy has medial ankle pain, progressive unilateral flatfoot deformity, and pain with most activities of daily living. He denies any recent injury. His parents recall that at age 7 years he sustained an injury that was treated as a sprain. Examination reveals valgus deformity with painless, unrestricted passive motion of the ankle. He has grossly equal limb lengths. A radiograph of the affected ankle is shown in Figure 48a, and the contralateral ankle is shown in Figure 48b. Management should consist of
Explanation
Explanation
48b Angular deformities of the ankle can occur following physeal injury. While an orthosis may be beneficial, the deformity is at the level of the ankle rather than the hindfoot. An epiphysiodesis or physeal bar resection would not be indicated as the growth plates are closed. Correction of the angular deformity should level the ankle joint and normalize the weight-bearing stresses on the ankle. This is most easily achieved with a closing wedge distal tibial osteotomy with or without concomitant osteotomy of the fibula. Thompson DM, Calhoun JH: Advanced techniques in foot and ankle reconstruction. Foot Ankle Clin 2000;5:417-442. Ting AJ, Tarr RR, Sarmiento A, Wagner K, Resnick C: The role of subtalar motion and ankle contact pressure changes from angular deformities of the tibia. Foot Ankle 1987;7:290-299.
References:
- Tarr RR, Resnick CT, Wagner KS, Sarmiento A: Changes in tibiotalar joint contact areas following experimentally induced tibial angular deformities. Clin Orthop 1985;199:72-80.
Question 49High Yield
Which of the following best describes the mechanism of action of gentamycin?
Explanation
Explanation
Gentamycin and the aminoglycosides (ie, streptomycin, tobramycin, amikacin, and neomycin) work by binding to the 30s ribosome subunit, leading to the misreading of mRNA. This misreading results in the synthesis of abnormal peptides that accumulate intracellularly and eventually lead to cell death. These antibiotics are bactericidal. Cephalosporins, vancomycin, and penicillins interfere with cell wall synthesis by inhibiting the transpeptidase enzyme. Polymyxin, nystatin, and amphotericin increase cell membrane permeability by disrupting the functional integrity of the cell membrane. The quinolones inhibit the enzyme, DNA gyrase. Lastly, metronidazole forms oxygen radicals that are toxic to anaerobic organisms because they lack the protective enzymes, superoxide dismutase and catalase.
References:
- Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 217-236.
Question 50High Yield
Which of the following is considered an inherent problem in using the distal oblique shortening (Weil) metatarsal osteotomy for dorsal metatarsophalangeal subluxation?
Explanation
The distal oblique shortening (Weil) metatarsal osteotomy has not been associated with transfer lesions to the extent of other shortening osteotomies, and malunions and nonunions are unusual complications. Recurrent dorsal contracture of the toe has been reported. Recommendations to reduce this problem include release of the dorsal capsule and tendons, as well as a flexor tendon transfer. A potential cause suspected for this phenomenon is the relatively dorsal positioning of the intrinsic tendons after plantar displacement of the metatarsal head. Trnka HJ, Nyska M, Parks BG, Myerson MS: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int 2001;22:47-50. Trnka HJ, Muhlbauer M, Zettl R, Myerson MS, Ritschl P: Comparison of the results of the Weil and Helal osteotomies for the treatment of metatarsalgia secondary to dislocation of the lesser metatarsophalangeal joints. Foot Ankle Int 1999;20:72-79.
Question 51High Yield
Figure 22 shows the MRI scan of a 20-year-old female basketball player who has pain over the anterior knee that interferes with her performance. Examination reveals phase III Blazina patellar tendinosis. Management should consist of
Explanation
Excision of the affected mucoid degenerative area is considered appropriate management in the Blazina classification system. A finding of phase III indicates persistent pain with or without activities, as well as deterioration of performance. With the appearance of the mucoid degeneration and the vigorous activity level of the intercollegiate basketball player, it is unlikely that nonsurgical management will provide adequate relief. When excising the affected degenerative area, care must be taken to retain normal tendon fibers. The defect in the patellar tendon is closed with absorbable sutures, as is the paratenon. Postoperative rehabilitation involves initial mobilization extension, with progressive range-of-motion and mobilization exercises as tolerated and weight bearing as tolerated. Open chain and isokinetic exercises are delayed until full range of motion and mobility is obtained, generally within 4 weeks. A return to activities is achieved by 80% to 90% of athletes, although there may be occasional activity-related aching for 4 to 6 months after surgery. Blazina ME, et al: Jumper's knee. Orthop Clin North Am 1973;4:665. Kelly DW, Carter VS, Jobe FW, Kerlan RK: Patellar and quadriceps tendon ruptures: Jumper's knee. Am J Sports Med 1984;12:375-380. Krums PE, Ryder B: Operative treatment of patella tendon disorders. Operative Techniques Sports Med 1994;2:303.
Question 52High Yield
What spinal nerves in the cauda equina are primarily responsible for innervation of the bladder?
Explanation
Explanation
The spinal nerves primarily responsible for bladder function are the S2, S3, and S4 nerve roots. With significant compression of the cauda equina by either disk herniation, tumor, or degenerative stenosis, bladder dysfunction may result. Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton-Century-Crofts, 1976, p 254.
References:
- Pick TP, Howden R (edS): Gray's Anatomy. New York, NY, Bounty Books, 1977, p 1004.
Question 53High Yield
Outcome measures should have established psychometric properties of reliability, validity, and responsiveness. Reliability refers to which of the following?
Explanation
Explanation
The recent JBJS article by Kocher and associates defines the different psychometric properties that are used in outcome measures. Reliability is a measure of how reproducible a test is. This can be interobserver reliability (ie, reliability between people), or intraobserver reliability (ie, reliability for the same person doing the outcome measure at different occasions).
References:
- Kocher MS, Horan MP, Briggs KK, et al: Reliability, validity, and responsiveness of the American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability, rotator cuff disease, and glenohumeral arthritis. J Bone Joint Surg Am 2005;87:2006-2011.
Question 54High Yield
A 30-year-old patient has had severe left hip pain and difficulty ambulating, necessitating the use of a cane, for the past 6 months. A photomicrograph of the femoral head sectioned at the time of surgery is shown in Figure 31. What is the most likely diagnosis?
Explanation
The photomicrograph demonstrates a wedge-shaped infarct with femoral head collapse; therefore, the diagnosis is osteonecrosis of the femoral head. Perthes disease and osteoarthritis do not involve a wedge-shaped defect. Tuberculosis of the hip joint results in greater destruction of the articular cartilage. Basset LW, Mirra JM, Cracchiolo A III: Ischemic necrosis of the femoral head: Correlation between magnetic resonance imaging and histologic sections. Clin Orthop 1987;223:181-187.
Question 55High Yield
Nutritional rickets is associated with which of the following changes in chemical blood level?
Explanation
Nutritional rickets is associated with decreased dietary intake of Vitamin D, resulting in low levels of Vitamin D that result in decreased intestinal absorption of calcium and low to normal serologic levels of calcium. To boost serum calcium levels, there is a compensatory increase in PTH and bone resorption, leading to increased alkaline phosphatase levels. Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94. Pettifor J: Nutritional and drug-induced rickets and osteomalacia, in Farrus MJ (ed): Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 399-466.
Question 56High Yield
A 16-year-old boy has had thigh pain for the past several months. He denies any history of trauma. Examination reveals a large, deeply fixed, soft-tissue mass in the thigh. Laboratory results show an elevated erythrocyte sedimentation rate (ESR) and leukocytosis. A plain radiograph and MRI scan are shown in Figures 1a and 1b. Biopsy specimens are shown in Figures 1c and 1d. What is the most likely diagnosis?



Explanation
Ewing's sarcoma typically can occur in the diaphysis of the long bones (50% to 55%). It is often accompanied by a large soft-tissue mass. Abnormal findings are common, including a low-grade fever, an elevated ESR, and leukocytosis. The histology is consistent with a small round blue cell tumor. The unique pathology and other findings exclude osteosarcoma. Giant cell tumor and chondrosarcoma have a different histologic appearance and typically are more metaphyseal in location. Chondrosarcoma typically is found in older age groups, has a different histologic pattern, and rarely occurs in the midshaft of the femur.
Question 57High Yield
During C1-C2 transarticular screw fixation, screw misplacement is most likely to result in injury to the
Explanation
Explanation
With C1-C2 transarticular screw fixation, the following structures are potentially at risk: vertebral artery, spinal cord, occiput-C1 joint, and hypoglossal nerve. The vertebral artery is most vulnerable to injury with drill misdirection or anatomic variations in the vertebral foramen. The hypoglossal nerve may be injured if the drill, tap, or screw passes too far anterior to the lateral mass of C1. This complication is extremely rare. The occiput-C1 joint may be injured if the screw trajectory is too cephalad or cranially directed; however,this scenario is very unlikely because the exposure tends to direct the screw into a caudally inclined direction. This caudal orientation has the potential to cause vertebral artery injury, especially in patients who have a large vertebral foramen in the lateral mass of C2 because of erosions (rheumatoid arthritis) or anatomic variation. CT of the vertebral foramen is recommended when C1-C2 transarticular fixation is being considered. Spinal cord injury is extremely unlikely because of the very large size of the spinal canal in the upper cervical spine; the spinal cord lies far away from the lateral masses of C1 and C2. Mueller ME, Allgower M, et al: Manual of Internal Fixation, ed 3. New York, NY, Springer-Verlag, 1991, pp 634-636.
References:
- Gebhard JS, Schimmer RC, Jeanneret B: Safety and accuracy of transarticular screw fixation C1-C2 using an aiming device: An anatomic study. Spine 1998;23:2185-2189.
Question 58High Yield
Figure 44 shows the radiograph of a 65-year-old man who underwent a revision arthroplasty to remove a loose, cemented femoral stem. When planning the postoperative restrictions, the surgeon should be aware that
Explanation
Explanation
The transfemoral approach, also known as the extended trochanteric osteotomy, is an important technique to master for revision hip surgery. When performed correctly, it allows excellent exposure of the femoral canal and aids in exposure of the acetabulum. As demonstrated in the study cited, however, it markedly reduces the torque that the composite can withstand without failure. This type of basic science study is important to guide postoperative rehabilitation.
References:
- Noble AR, Branham D, Willis M, et al: Mechanical effects of the extended trochanteric osteotomy. J Bone Joint Surg Am 2005;87:521-529.
Question 59High Yield
Figure 24 shows the radiograph of a 4-year-old girl with spina bifida. Examination reveals an L3 motor level, excellent sitting and standing balance, and satisfactory range of motion at the hips. Management should consist of
Explanation
Explanation
Children with spina bifida and bilateral symmetrical dislocation of the hips usually do not require treatment. A level pelvis and good range of motion of the hips are more important for ambulation than reduction of bilateral hip dislocations. Because the patient has good sitting and standing balance and good range of motion, maintenance of that range of motion and symmetry is more important than reduction. Surgery is not recommended.
References:
- Heeg M, Broughton NS, Menelaus MB: Bilateral dislocation of the hip in spina bifida: A long-term follow-up study. J Pediatr Orthop 1998;18:434-436.
Question 60High Yield
When examining a patient with marked hyperreflexia, which of the following findings best suggests that the condition is not caused by a cerivcal spine pathology?
Explanation
A positive jaw jerk reflex suggests that the problem is above the level of the pons. All of the other physical signs are exhibited in patients with cervical myelopathy. Although these signs also may be present in conditions affecting the brain, they do not help differentiate between a brain etiology and a cervical spine etiology. A jaw jerk reflex, however, is not present in patients with cervical myelopathy alone. Montgomery DM, Brower RS: Cervical spondylotic myelopathy: Clinical syndrome and natural history. Orthop Clin North Am 1992;23:487-493. Ono K, Ebara S, Fuji T, Yonenobu K, Fujiwara K, Yamashita K: Myelopathy hand: New clinical signs of cervical cord damage. J Bone Joint Surg Br 1987;69:215-219.
Question 61High Yield
A 27-year-old man has had pain in the right index finger for the past 9 months. The pain is completely relieved with ibuprofen. An AP radiograph and CT scan are shown in Figures 80a and 80b. What is the most likely diagnosis?

Explanation
Osteoid osteoma is a round or oval, well-circumscribed lesion with a radiolucent nidus. A small area of calcification may be present within the center of the nidus. The radiolucent nidus is surrounded by a thick rim of sclerotic bone. These diagnostic features are frequently better seen on CT. An increase in cyclooxygenase activity has been demonstrated within osteoid osteomas, which may explain why aspirin and other nonsteroidal anti-inflammatory drugs classically relieve the pain associated with these lesions. Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid-osteoma. J Bone Joint Surg Am 1992;74:179-185.
Question 62High Yield
Figures 8a through 8c show the lateral radiograph and T1- and T2-weighted MRI scans of a 14-year-old soccer player who reports aching thigh pain. The next most appropriate step in management should consist of


Explanation
Although the MRI findings could be misinterpreted as an aggressive soft-tissue process, the periosteal-based ossification on the radiograph in an athlete most likely suggests myositis ossificans. The radiograph should be repeated to see further maturation of the ossification with a typical "zoning" pattern. The zoning pattern is one of peripheral ossification. This is often best seen on a CT scan. King JB: Post-traumatic ectopic calcification in the muscles of athletes: A review. Br J Sports Med 1998;32:287-290.
Question 63High Yield
At the time of the revision surgery shown in Figure 14, the acetabular component was found to be stable. Polyethylene exchange with a standard ultra-high molecular weight polyethylene liner and grafting was performed. The patient is at significantly increased risk for
Explanation
Explanation
Maloney and associates reported a 35% increased risk of pelvic osteolysis after total hip arthroplasty with a porous-coated acetabular component without cement. All components were stable at the time of revision. Only liners were exchanged and debridement of the granuloma with or without bone graft was performed. No defects progressed and one third of the lesions were no longer visible on radiographs, regardless of bone grafting. Unfortunately, despite the technical ease of many of these types of revisions, the dislocation rate for these cases is significant. Precautions should be taken postoperatively, and patients should be educated about this risk preoperatively. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 411-424. Boucher HR, Lynch C, Young AM, et al: Dislocation after polyethylene liner exchange in total hip arthroplasty. J Arthroplasty 2003;18:654-657.
References:
- Maloney WJ, Herzwurm P, Paprosky W, et al: Treatment of pelvic osteolysis associated with a stable acetabular component inserted without cement as part of a total hip replacement. J Bone Joint Surg Am 1997;79:1628-1634.
Question 64High Yield
As reflected by the SF-36 scores, patients with which of the following conditions demonstrate the most disability in physical function?
Explanation
Explanation
Pollak and associates found that the average SF-36 score for patients who sustained a pilon fracture was significantly lower than patients with diabetes mellitus, AIDS, hypertension, asthma, migraines, pelvic fracture, polytrauma, and AMI. Moreover, patients having undergone pilon fixation scored lower on all but three of the SF-36 scales (vitality, mental health, and emotional health).
Question 65High Yield
A 13-year-old girl was riding on an all-terrain vehicle when the driver struck a tree. She sustained the injury shown in Figures 45a through 45d. This injury is best described as what type of acetabular fracture pattern?
Explanation
Explanation
45b 45c 45d The fracture is a both-column fracture in the Judet/Letournel classification and a C3 in the AO classification. There is extension into the sacroiliac joint along the pelvic brim and comminution along the posterior column above the sciatic notch. Both the anterior and posterior columns are separately broken and displaced. However, the defining feature of a both-column pattern, as seen in this patient, is that all articular fragments are on fracture fragments and no joint surface is left intact to the axial skeleton above. The use of three-dimensional images makes it easier to view the location of the fracture fragments and the amount and direction of displacement. Helfet DL, Beck M, Gautier E, et al: Surgical techniques for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 533-603. Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
References:
- Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 66High Yield
A 15-year-old boy reports a 2-day history of progressive left buttock pain and severe limping. He denies any history of trauma or radiation of the pain. He has an oral temperature of 100.4 degrees F (38 degrees C). Examination reveals that the lumbar spine and left hip have unguarded motion. The abdomen is nontender. There is moderate tenderness of the left sacroiliac region with no palpable swelling. Pain is elicited when the left lower extremity is placed in the figure-4 position (FABER test). Laboratory studies show a peripheral WBC count of 11,500/mm3 (normal to 10,500/mm3) and an erythrocyte sedimentation rate of 38 mm/h (normal up to 20 mm/h). Radiographs of the pelvis, hips, and lumbar spine are normal. A nucleotide bone scan (posterior view) is shown in Figure 44. Initial management should consist of
Explanation
Explanation
The symptoms, physical findings, and laboratory studies are most consistent with a diagnosis of infectious sacroiliitis, usually caused by Staphylococcus aureus. Initial radiographs will be normal, and the diagnosis of sacroiliitis is often delayed. A technetium Tc 99m bone scan will localize the problem in 90% of patients but may occasionally give a false-negative result in early cases. If suspicion is high, a gallium scan or MRI scan may help confirm the diagnosis of sacroiliitis. Needle aspiration of the sacroiliac joint is difficult; therefore, antibiotic selection is usually empiric or based on blood cultures. Sacroiliitis that is the result of connective tissue inflammatory disease is usually bilateral and without fever or leukocytosis. The lack of hip irritability, spinal rigidity, and abdominal tenderness helps to rule out other causes of limping with fever, such as psoas abscess, diskitis, and septic hip. Aprin H, Turen C: Pyogenic sacroiliitis in children. Clin Orthop 1993;287:98-106.
References:
- Osman AA, Govender S: Septic sacroiliitis. Clin Orthop 1995;313:214-219.
Question 67High Yield
A newborn has an anterolateral bow of the tibia and a duplication of the great toe. Which of the following conditions will develop as the infant grows?
Explanation
Anterolateral bowing of the tibia is normally associated with congenital pseudarthrosis of the tibia. This, in turn, is associated with neurofibromatosis. Posterior bowing is more benign and usually corrects spontaneously. However, anterolateral bowing also corrects spontaneously, and the limb-length discrepancy may be the only remaining sequela when associated with duplication of the great toe. Lisch nodules and axillary freckling are pathognomonic findings in neurofibromatosis but would not be expected in this patient because this type of tibial deformity is not associated with neurofibromatosis.
Question 68High Yield
A 42-year-old woman who observes traditional Muslim practices is seen in your office accompanied by her physician husband to discuss possible elective bunion correction. In considering the treatment of this patient, what is one of the most important considerations?
Explanation
Explanation
In considering faith-based issues regarding treatment of this patient, the presence of her husband for the office visit would imply an agreement with her decision to have surgery. It also may facilitate her examination. Her role as caregiver, dietary concerns, and cleansing rituals are less important considerations with an outpatient-based procedure. Privacy concerns remain paramount to Muslim women, which include limited exposure during examination, during surgery, and in subsequent follow-up visits.
Question 69High Yield
A 37-year-old electrician is diagnosed with a frozen shoulder after sustaining an electrical injury at work 2 weeks ago. Examination reveals that he cannot actively or passively externally rotate or abduct the arm. The glenohumeral joint and scapula move in a 1:1 ratio. Radiographs are shown in Figures 15a and 15b. The best course of action should be

Explanation
The patient's history, examination, and radiographs are classic for locked posterior dislocation of the glenohumeral joint. Posterior dislocation of the shoulder remains the most commonly missed dislocation of a major joint. Up to 80% are missed on initial presentation. The primary cause for failure to accurately diagnose this injury is inadequate radiographic evaluation. The typical presentation is a shoulder locked in internal rotation with loss of abduction. An axillary view not only will make the definitive diagnosis but will help assess the size of the articular surface defect and help plan treatment. This view can be done expediently as part of every trauma series. The AP view is suspicious for a posteriorly dislocated humerus with loss of the humeral neck profile, a vacant glenoid sign, and an anterior humeral head compression fracture (reverse Hill-Sachs lesion). Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosement, IL, American Academy of Orthopaedic Surgeons, 1997, pp 181-189.
Question 70High Yield
Which of the following nerves is most commonly injured during ankle arthroscopy?
Explanation
The superficial peroneal nerve, which is adjacent to the location of the lateral arthroscopic portal is most commonly injured. Ferkel RD, Heath DD, Guhl JF: Neurological complications of ankle arthroscopy. Arthroscopy 1996;12:200-208.
Question 71High Yield
An 8-year-old boy sustains injuries to his head, abdomen, and left lower extremity after being struck by a truck. In the emergency department, his mental status deteriorates and he is intubated after assessment reveals a Glasgow Coma Scale score of 3; the score subsequently improves to 10. A CT scan reveals a right parietal intracranial hemorrhage, and an abdominal ultrasound reveals free fluid. Prior to an emergency laparotomy, the swollen left thigh is evaluated. Radiographs reveal a transverse fracture of the mid-diaphysis. Management of the fracture should consist of
Explanation
The prognosis for a young patient with a head injury is more favorable compared to that for adults. Full neurologic recovery generally occurs. Spasticity may occur within a few days after injury, which can lead to fracture displacement if immediate spica casting or traction is used. Early surgical stabilization will reduce problems with shortening and malunion and will facilitate transportation of the child for diagnostic tests. Surgery may be performed when it is best for the patient, either on the day of injury or later if time is needed for stabilization. In this patient, the fracture is ideally suited to stabilization using flexible intramedullary nails. Heinrich and associates' report of 78 diaphyseal femur fractures stabilized with flexible intramedullary nails included 14 patients with an associated closed head injury. All fractures healed, and there were no major complications. Tolo VT: Management of the multiply injured child, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 83-95.
Question 72High Yield
A 65-year-old woman has significant neck pain after falling and striking her head. A radiograph and sagittal CT scan are shown in Figures 23a and 23b. What is the most likely diagnosis?
Explanation
Explanation
23b The radiograph shows a displacement of C5 on C6 of approximately 25%. The CT scan shows a perched facet at C5-6. There is no evidence of a facet fracture. A bilateral facet dislocation would show a displacement of more than 50%. Rothman RH, Simeone FA (eds): The Spine, ed 4. Philadelphia PA, WB Saunders, 1999, pp 927-937.
References:
- Vaccaro AR, Betz RR, Zeidman SM (eds): Principles and Practice of Spine Surgery. St Louis, MO, Mosby, 2003, pp 455-458.
Question 73High Yield
Figures 10a and 10b show the radiographs of a 47-year-old man who reports pain in both shoulders. He has a history of leukemia that was treated with chemotherapy and high-dose cortisone. What is the most reliable treatment option for pain relief in this patient?

Explanation
The radiographs reveal osteonecrosis with collapse. The most reliable and durable treatment for osteonecrosis of the humeral head remains prosthetic shoulder arthroplasty. Osteonecrosis of the humeral head may be seen after the use of steroids, and there is an increasing demand for shoulder arthroplasty in young people because of the use of high-dose steroids in chemotherapy regimes for the treatment of malignant tumors. The indications for most shoulder arthrodeses today include posttraumatic brachial plexus injury, paralytic disorders in infancy, insufficiency of the deltoid muscle and rotator cuff, chronic infection, failed revision arthroplasty, severe refractory instability, and bone deficiency following resection of a tumor in the proximal aspect of the humerus. Clearly, the role of arthroscopy and related minimally invasive techniques in the treatment of humeral head osteonecrosis remains unknown. Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg 2002;11:281-298. Hattrup SJ: Indications, technique, and results of shoulder arthroplasty in osteonecrosis. Orthop Clin North Am 1998;29:445-451.
Question 74High Yield
Which of the following mechanisms is considered the most common cause of failure of osteoarticular allografts used for articular reconstruction?
Explanation
Mechanical loosening and infection can occur as complications after surgery, but the most common cause of osteoarticular allograft failure is graft collapse during revascularization. Clinical rejection because of an immune response is an unusual means of failure. Meyers MH, Akeson W, Convery FR: Resurfacing of the knee with fresh osteochondral allograft. J Bone Joint Surg Am 1989;71:704-713.
Question 75High Yield
A 60-year-old woman reports a painful hip arthroplasty after undergoing surgery 18 months ago. Radiographs show stable cementless implants without signs of ingrowth. Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h. Management should now consist of
Explanation
Explanation
Significant elevation of the erythrocyte sedimentation rate in a patient with a painful hip arthroplasty mandates a complete work-up for infection prior to considering revision surgery. Reproducibility and reliability of ultrasonography as a diagnostic test still needs clarification. Aspiration is the easiest and most cost-effective test and should be performed prior to nuclear imaging. The latter is most valuable if the results are negative, strongly predicting the absence of infection. Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
References:
- McAuley JP, Moreau G: Sepsis: Etiology, prophylaxis, and diagnosis, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 1295-1306.
Question 76High Yield
A 25-year-old tennis player has shoulder pain and weakness to external rotation. MRI scans are shown in Figures 16a and 16b. What is the most likely cause of his weakness?

Explanation
The MRI scans show a paralabral cyst, which is most commonly associated with labral tears. Compression of the suprascapular nerve results in weakness of the supraspinatus and/or infraspinatus depending on the level of compression. Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Question 77High Yield
A 78-year-old woman has had activity-limiting cervical pain and occipital headaches for the past 4 years. Management consisting of injections, analgesics, and part-time collar wear has provided temporary relief. Examination reveals that her neck pain seems to be primarily located immediately below the skull and is aggravated by long periods of sitting and rotation of her head. Plain radiographs are shown in Figures 36a through 36c. What is the best course of action?
Explanation
Explanation
36b 36c Posterior atlantoaxial arthrodesis predictably relieves pain associated with arthrosis of the atlantoaxial joints. Typically, these patients have pain at the base of the occiput and in the most cephalad portion of the posterior aspect of the neck. Associated headache is common and often severe. Pain is aggravated by rotation but usually not by flexion and extension. Diagnostic blocks of the C1-C2 joint and the greater occipital nerve may be helpful to confirm the diagnosis preoperatively. Ghanayem AJ, Leventhal M, Bohlman HH: Osteoarthrosis of the atlanto-axial joints: Long-term follow-up after treatment with arthrodesis. J Bone Joint Surg Am 1996;78:1300-1307.
References:
- Star MJ, Curd JG, Thorne RP: Atlantoaxial lateral mass osteoarthritis: A frequently overlooked cause of severe occipitocervical pain. Spine 1992;17:S71-S76.
Question 78High Yield
A 3-year-old boy had been treated with serial casting for a right congenital idiopathic clubfoot deformity. The parents are concerned because the child now walks on the lateral border of the right foot. Examination shows that the foot passively achieves a plantigrade position with neutral heel valgus and ankle dorsiflexion to 15 degrees. The forefoot inverts during active ankle dorsiflexion. Mild residual metatarsus adductus is present. Management should now consist of
Explanation
Explanation
Dynamic midfoot supination that is the result of peroneal weakness is a common residual problem after cast correction or surgical reconstruction of a congenital idiopathic clubfoot. Dynamic supination is unlikely to resolve spontaneously. Most parents do not want to use brace support forever. Transfer of the posterior tibialis to the dorsum of the foot has shown poor results in clubfeet. Preferred treatments include: 1) transfer of the entire anterior tibialis tendon to the lateral cuneiform, or 2) split transfer of the anterior tibialis tendon to the cuboid or to the peroneus brevis tendon. Kuo KN, Hennigan SP, Hastings ME: Anterior tibial tendon transfer in residual dynamic clubfoot deformity. J Pediatr Orthop 2001;21:35-41. Garceau GJ: Anterior tibial tendon transfer for recurrent clubfoot. Clin Orthop 1972;84:61-65.
References:
- Miller GM, Hsu JD, Hoffer MM, et al: Posterior tibial tendon transfer: A review of the literature and analysis of 74 procedures. J Pediatr Orthop 1982;2:363-370.
Question 79High Yield
The spring ligament of the foot connects what two bones?
Explanation
Explanation
The spring ligament is also known as the calcaneonavicular ligament and connects the calcaneus to the navicular. This ligament supports the talar head and is an important anatomic supporting structure of the medial longitudinal arch of the foot. Choi K, Lee S, Otis JC, et al: Anatomical reconstruction of the spring ligament using peroneus longus tendon graft. Foot Ankle Int 2003;24:430-436.
Question 80High Yield
A 58-year-old woman with a history of severe asthma and long-term prednisone use reports a progression of chronic shoulder pain for the past 6 months. Radiographs and MRI scans are shown in Figures 30a through 30d. What is the most likely diagnosis?
Explanation
Explanation
30b 30c 30d The patient has osteonecrosis of the humeral head. The radiographs show increased density in the superior subchondral region of the humeral head. The MRI scans reveal a central collapse of the humeral head. The patient's history of severe asthma and long-term prednisone use predisposes her to this condition. The MRI scans show no evidence of a full- or partial-thickness rotator cuff tear. Without a history of fevers, chills, or other systemic signs or symptoms, there is no indication of septic arthritis. The radiographs do not reveal periarticular erosions, commonly seen in rheumatoid arthritis. Matsen FA III, Rockwood CA Jr, Wirth MA, et al: Glenohumeral arthritis and its management, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 871-874.
References:
- Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Results of replacement. J Shoulder Elbow Surg 2000;9:177-182.
Question 81High Yield
A 12-year-old boy has severe left shoulder pain after being struck by an automobile. A chest radiograph, AP and lateral radiographs, and a CT scan with three-dimensional reconstruction of the scapula are shown in Figures 38a through 38d. Management should consist of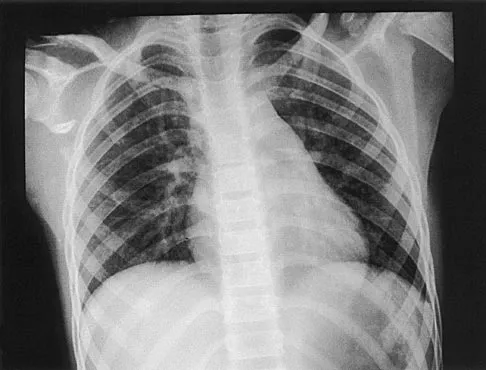


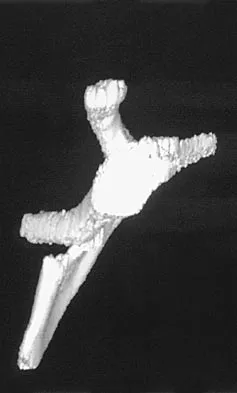
Explanation
Scapular body fractures in children are rare and are often associated with other injuries of the chest and thorax. Management is generally nonsurgical, unless the injury is open, and usually consists of support with a sling and gentle range-of-motion exercises to minimize shoulder stiffness. Green N, Swiontkowski M: Skeletal Trauma in Children, ed 2. Philadelphia, PA, WB Saunders, 1998, vol 3, pp 319-341.
Question 82High Yield
The majority of severe cervical spine injuries occurring in contact sports evolve during axial loading and flexion of the cervical spine. At what minimum degree of flexion does axial loading place the cervical spine at risk during contact sports?
Explanation
Explanation
The paravertebral musculature, the intervertebral disks, and the normal lordotic curvature of the cervical spine can absorb much of the imparted energy of collision. However, when the neck is flexed approximately 30 degrees, the normal lordotic curvature is flattened and the forces applied to the vertex of the head are directed at a straight segmented column. In this situation, the cervical spine is less able to absorb the applied force. With mounting axial load, compressive deformation occurs within the intervertebral disks, causing angular deformation and buckling. The spine will fail in flexion, with resultant fracture, subluxation, or dislocation. A rotatory component added to axial compression can cause concomitant extension, rotation, and shear injury patterns. The National Football Head and Neck Injury Registry has made two recommendations to the NCAA Football Rules Committee to minimize the risk of such injuries: (1) No player should intentionally strike an opponent with the crown or top of the helmet; and (2) No player should deliberately use his helmet to butt or ram an opponent. Thomas BE, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
References:
- Torg JS, Truex R Jr, Quedenfeld TC, Burstein A, Spealman A, Nichols C III: The National Football Head and Neck Injury Registry: Report and conclusions 1978.
- JAMA 1979;241:1477-1479.
Question 83High Yield
Figures 29a and 29b show the AP and lateral radiographs of a 30-year-old man who has increasingly worse back pain and stiffness. Examination shows painful, limited spinal range of motion. There is no neurologic deficit. What laboratory study would be most helpful in confirming the diagnosis?

Explanation
The radiographs show ankylosing spondylitis with sclerosis of the sacroiliac joints and a "bamboo spine" in the lumbar region. HLA-B27 is positive in 80% to 90% of patients with ankylosing spondylitis and in about 8% of the general population. The findings do not represent diffuse idiopathic skeletal hyperostosis (DISH), which is a radiographic diagnosis in which there are three consecutive levels of nonmarginated osteophytes without disk degeneration. Calin A: Ankylosing spondylitis. Clin Rheum Dis 1985;11:41-60. Booth R, Simpson J, Herkowitz H: Arthritis of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 431.
Question 84High Yield
A 66-year-old man has a high-grade angiosarcoma of the right tibia. A radiograph is shown in Figure 43. Treatment should consist of
Explanation
Angiosarcoma is a locally aggressive sarcoma. The radiograph shows extensive multiple discontinuous lesions throughout the entire tibia. The extent of bone involvement precludes resection; therefore, the treatment of choice is amputation, either above the knee or through the knee. Radiation therapy is not needed after amputation, and chemotherapy remains investigational for soft-tissue sarcoma.
Question 85High Yield
A 64-year-old woman has left wrist pain and deformity after falling on her hand. Examination shows intact skin and no neurologic or vascular injuries. Radiographs are shown in Figures 43a and 43b. What is the most appropriate management for the injury?

Explanation
The patient has a volar displaced two-part intra-articular distal radial fracture-dislocation of the wrist. Although a closed reduction is usually easily obtained, it is very difficult to maintain the reduction without internal fixation. The approach is determined by the direction of the dislocation, in this case volar. Stabilization with a buttress plate neutralizes the axial loading forces on the fractured fragment. A dorsal placed angular stable plate will not provide this buttress effect and will make the reduction difficult.
Question 86High Yield
A 35-year-old laborer who sustained a forefoot injury 10 years ago has returned to work but reports a progressively painful deformity of the hallux and continued midfoot pain that is aggravated by weight-bearing activities. Shoe wear modifications have failed to provide relief. Direct palpation reveals no pain at the first metatarsocuneiform joint. A radiograph is shown in Figure 11. What is the next most appropriate step in management?
Explanation
The patient has nonunions of the metatarsal fractures and a hallux valgus deformity with arthritic changes. To address all of the findings, management should consist of open treatment of the metatarsal nonunions and hallux metatarsophalangeal arthrodesis. Cast immobilization and a bone stimulator are unlikely to be beneficial at this time. Isolated correction of the hallux valgus deformity will not address the metatarsal nonunions or the arthritis at the hallux metatarsophalangeal joint. Kitaoka HB, Patzer GL: Arthrodesis versus resection arthroplasty for failed hallux valgus operations. Clin Orthop 1998;347:208-214. McGarvey WC, Braly WG: Bone graft in hindfoot arthrodesis: Allograft vs autograft. Orthopedics 1996;19:389-394.
Question 87High Yield
What nerve is most at risk during placement of the anterolateral portal in elbow arthroscopy?
Explanation
The radial nerve is only 4 mm from the anterolateral portal, while the median nerve is 11 mm away from the anteromedial portal. The ulnar nerve is only at risk on the medial side of the elbow. Anterior and posterior interosseous nerves are more distal within the forearm and are not in danger during portal placement. O'Driscoll SW, Morrey BF: Elbow arthroscopy, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 21-34.
Question 88High Yield
A 64-year-old man has had increasing pain in the left hip for the past 6 months. A radiograph and MRI scan are shown in Figures 25a and 25b. Biopsy specimens are shown in Figures 25c and 25d. What is the recommended treatment?
Explanation
Explanation
25b 25c 25d The radiograph shows a lytic lesion in the left periacetabular area consistent with chondrosarcoma. A large soft-tissue mass is present along with extension through the supra-acetabular region and pubic ramus. The histology shows a hypercellular lesion infiltrating through the bony trabeculae with a basophilic cytoplasm. This is classified as a grade 2 chondrosarcoma. The treatment of a pelvic chondrosarcoma is wide resection via either an internal hemipelvectomy or amputation. Chondrosarcoma requires surgical resection for control and does not traditionally respond to chemotherapy or external beam irradiation therapy. Pring M, Weber, KL, Unni KK, et al: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg 2001;83:1630-1642.
References:
- Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 255.
Question 89High Yield
Eosinophilic granuloma frequently occurs as a solitary lesion in the tubular long bones. After biopsy, what is the best course of action?
Explanation
Most lesions of eosinophilic granuloma are simply observed, but larger aggressive lesions may require curettage and bone grafting. Frequently, biopsy is required to rule out a malignant diagnosis. The differential diagnosis of eosinophilic granuloma is osteomyelitis, Ewing's sarcoma of bone, or osteogenic sarcoma. The biopsy alone can be followed by spontaneous resolution. In some patients, low-dose radiation therapy is used. Chemotherapy or amputation is not indicated for these benign lesions.
Question 90High Yield
A 30-year-old man requires surgical stabilization of a hypermobile spondylolisthesis of L5 on S1. History reveals that he has smoked one pack of cigarettes a day for 15 years. During preoperative counseling, the patient should be advised to
Explanation
Explanation
Many studies have shown the negative effects of cigarette smoking on the success of lumbar arthrodesis. Some have suggested preoperative cessation is a significant factor for good results. However, Deguchi and associates, in a review of spondylolisthesis fusions, and Glassman and associates, in a review of scoliosis fusions, showed no significant benefit from preoperative cessation of smoking. In every report, however, postoperative smoking correlated with a significantly increased rate of pseudarthrosis. Cessation of smoking with the use of nicotine substitutes would not be beneficial because animal studies and human clinical trials have shown that nicotine is a major factor in failure of fusion in patients who continue to smoke. Silcox DH III, Daftari T, Boden SD, Schimandle JH, Hutton WC, Whitesides TE Jr: The effect of nicotine on spinal fusion. Spine 1995;20:1549-1553. Deguchi M, Rapoff AJ, Zdeblick TA: Posterolateral fusion for isthmic spondylolisthesis in adults: Analysis of fusion rate and clinical results. J Spinal Disord 1998;11:459-464.
References:
- Glassman SD, Anagnost SC, Parker A, Burke D, Johnson JR, Dimar JR: The effect of cigarette smoking and smoking cessation on spinal fusion. Spine 2000;25:2608-2615.
Question 91High Yield
A 42-year-old woman who has had an 18-month history of severe low back pain is referred to your office for surgical evaluation. She reports that the pain initially began with right lower extremity pain and management consisted of oral analgesics, nonsteroidal anti-inflammatory drugs, and muscle relaxants. She has seen a chiropractor as well as a pain management specialist and she is status-post epidural steroid injections. She has also completed exhaustive physical therapy, as she is a certified athletic trainer and runs a health fitness program at a community hospital. Currently, she denies lower extremity pain and her pain is isolated to her low back and is subjectively graded as 8/10, with 10 being the worst pain she has ever experienced. The pain is interfering with her activities of daily living and she is seeking definitive treatment. Figures 32a through 32c show current MRI scans. Based on the current available medical literature, what is the most appropriate treatment?
Explanation
Explanation
32b 32c The MRI scans reveal advanced degenerative disk disease at L5-S1. Nonsurgical management has failed to provide relief and the patient is quite debilitated as a result of her back pain. Fritzell and associates demonstrated that in a well-informed and selected group of patients with severe low back pain, lumbar fusion can diminish pain and decrease disability more efficiently than commonly used nonsurgical treatments. In a recent updated Cochrane Review of surgery for degenerative lumbar spondylosis, it was noted that while Fritzell and associates appeared to provide strong evidence in favor of fusion, a more recent trial by Brox and associates demonstrated no difference between those patients undergoing lumbar fusion compared to those receiving cognitive intervention and exercise. The Cochrane Review suggests that this may reflect a difference between the control groups. Fritzell and associates compared lumbar fusion to standard 1990s "usual care," whereas Brox and associates compared lumbar fusion to a "modern rehabilitation program." Bear in mind that this patient is a certified athletic trainer and runs a hospital health fitness department; therefore, at least for purposes of this question, it can be assumed that she has participated in a "modern rehabilitation program." The Cochrane Review goes on to state that preliminary results of three small trials of intradiskal electrotherapy suggest that it is ineffective and that preliminary data from three trials of disk arthroplasty do not permit firm conclusions. Gibson JN, Waddell G: Surgery for degenerative lumbar spondylosis: Updated Cochrane Review. Spine 2005;30:2312-2320. Fritzell P, Hagg O, Wessberg P, et al: 2001 Volvo Award Winner in Clinical Studies: Lumbar fusion versus nonsurgical treatment for chronic low back pain: A multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group. Spine 2001;26:2521-2532.
Question 92High Yield
The radiographs and CT scan seen in Figures 28a through 28d reveal what type of acetabular fracture pattern?


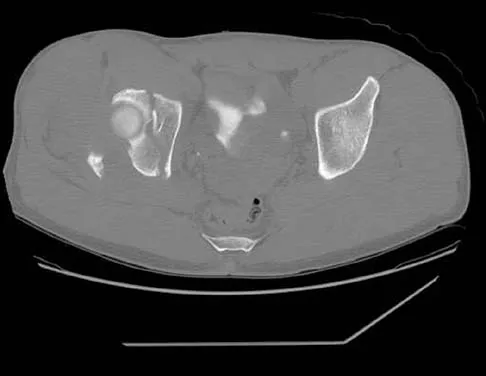
Explanation
The AP, obturator oblique, and iliac oblique views of the pelvis reveal a fracture that disrupts the iliopectineal and ilioischial lines, indicating a fracture that involves both anterior and posterior columns. However, it does not have the other features of anterior or posterior column fracture patterns. A displaced posterior wall fracture is also present, best seen on the obturator oblique view. The anterior to posterior directed fracture line on the CT scan indicates a transverse fracture; therefore, the patient has a transverse with posterior wall fracture pattern. A T-type fracture would be similar but would have a break into the obturator ring. Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Question 93High Yield
Figure 6 shows the radiograph of a 14-year-old baseball player who felt a pop and had an immediate onset of pain in his elbow after a hard throw from the outfield. The best course of action should be to
Explanation
The valgus stress at the elbow caused by throwing strains the medial collateral ligament. The medial epicondyle, on which the ligament inserts, is the last ossification center to fuse to the distal humerus, and acute avulsion of the medial epicondyle can occur in adolescents. If the elbow is allowed to heal in a displaced position, valgus instability and loss of elbow extension may result. Valgus instability is especially problematic for the throwing athlete. Surgical treatment with rigid internal fixation is the treatment of choice for displaced medial epicondyle avulsion fractures. Valgus instability is prevented, and the rigid fixation allows for early range of motion. Case SL, Hennrikus WL: Surgical treatment of displaced medial epicondyle fractures in adolescent athletes. Am J Sports Med 1997;25:682-686.
Question 94High Yield
A 26-year-old right hand-dominant man has had right shoulder pain for the past 6 months. History reveals that he was the starting pitcher for his high school team. Activity modification, physical therapy, cortisone injection, and anti-inflammatory drugs have failed to improve his symptoms. He has a positive O'Brien's active compression test. What is the next most appropriate step in the diagnosis of this patient?
Explanation
Explanation
MRI-arthrography has been shown to be an accurate technique for assessing the glenoid labrum in patients with suspected labral tears. Often standard MRI technique will not identify labral lesions. The use of MRI-arthrography with an intra-articular injection of gadolinium provides improved visualization of labral lesions. Bencardino and associates demonstrated a sensitivity of 89%, a specificity of 91%, and an accuracy of 90% in detecting labral lesions. SLAP lesions can be visualized on coronal oblique sequences as a deep cleft between the superior labrum and the glenoid that extends well around and below the biceps anchor. Often, contrast will diffuse into the labral fragment, causing it to appear ragged or indistinct. Applegate GR, Hewitt M, Snyder SJ, et al: Chronic labral tears: Value of magnetic resonance arthrography in evaluating the glenoid labrum and labral-bicipital complex. Arthroscopy 2004;20:959-963. Bencardino JT, Beltran J, Rosenberg ZS, et al: Superior labrum anterior-posterior lesions: Diagnosis with MR arthrography of the shoulder. Radiology 2000;214:267-271.
References:
- Nam EK, Snyder SJ: The diagnosis and treatment of superior labrum, anterior and posterior (SLAP) lesions. Am J Sports Med 2003;31:798-810.
Question 95High Yield
The recurrent motor branch of the median nerve innervates which of the following muscles?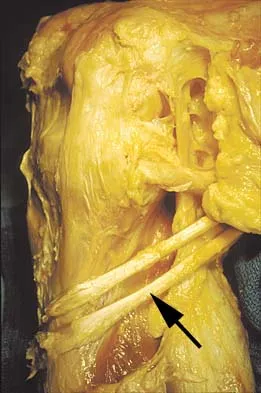
Explanation
The recurrent motor branch of the median nerve supplies the thenar muscles (abductor pollicis brevis, flexor pollicis brevis, and opponens pollicis) that are primarily responsible for thumb opposition. The nerve can be injured in carpal tunnel release. A branch of the nerve also supplies the first lumbrical. The adductor pollicis and the interossei are supplied by the ulnar nerve. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 109.
Question 96High Yield
An 8-year-old boy sustained an isolated distal radial fracture that was reduced and immobilized with 10 degrees of residual dorsal tilt. What is the next step in management?
Explanation
Distal radial fractures in children are common, and a large amount of displacement is acceptable. In general, 20 degrees of dorsal displacement and complete bayonet apposition in girls to age 12 years and in boys to age 14 years can be expected to remodel with an excellent outcome. The potential for increased fracture displacement and subsequent malunion may exist in up to one third of patients with displaced fractures with less than anatomic reduction. Therefore, early follow-up is recommended and remanipulation is indicated should loss in reduction occur. Consideration for percutaneous pinning of isolated distal radial fracture is reasonable in patients with little growth remaining. In these patients, higher rates of redisplacement exist with little chance for remodeling. Gibbons CL, Woods DA, Pailthorpe C, et al: The management of isolated distal radius fractures in children. J Pediatr Orthop 1994;14:207-210. McLauchlan GJ, Cowan B, Annan IH, et al: Management of completely displaced metaphyseal fractures of the distal radius in children. J Bone Joint Surg Br 2002;84:413-417. Proctor MT, Moore DJ, Patterson JH: Redisplacement after manipulation of distal radial fractures in children. J Bone Joint Surg Br 1993;75:453-454.
Question 97High Yield
Which of the following lumbar disk components has the highest tensile modulus to resist torsional, axial, and tensile loads?
Explanation
The annulus fibrosis has a multilayer lamellar architecture mode of type I collagen fibers. Each successive layer is oriented at 30 degrees to the horizontal in the opposite direction, leading to a "criss-cross" type pattern. This composition allows the annulus, which has the highest tensile modulus, to resist torsional, axial, and tensile loads.
Question 98High Yield
A patient with a 5-cm synovial sarcoma located in the distal portion of the rectus femoris muscle undergoes excision of the mass. The procedure is performed through a 10-cm longitudinal incision. Only a portion of the rectus femoris is removed; the vast majority of the muscle is preserved. The plane of dissection is beyond the reactive zone, and the pathology reveals that the margins are negative. This procedure is classified as
Explanation
Explanation
The patient underwent a wide resection, which involves excision of the tumor along with a cuff of normal tissue that completely surrounds the tumor. The plane of resection is beyond the reactive zone. A radical resection involves removal of the entire affected muscle from origin to insertion. In a marginal excision, the plane of dissection is through the reactive zone of the tumor. A marginal excision is generally considered inadequate surgery for high-grade sarcomas. In an intralesional resection, the plane of dissection is through the tumor. Excision within the reactive zone but beyond the tumor is the same as a marginal excision. Enneking WF: Staging of musculoskeletal neoplasms, in Current Concepts of Diagnosis and Treatment of Bone and Soft Tissue Tumors. Heidelberg, Germany, Springer-Verlag, 1984.
References:
- Simon MA, Springfield D: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998.
Question 99High Yield
Staphylococcus aureus develops methicillin resistance through production of which of the following agents?
Explanation
Explanation
Organisms may develop resistance to antibiotics by production of specific enzymes. S aureus develops methicillin resistance by production of penicillin-binding protein 2a (PBP2a). The strains of S aureus that have acquired the mecA gene for PBP2a are designated as methicillin-resistant S aureus (MRSA). The enzyme manifests resistance to covalent modification by beta-lactam antibiotics at the active-site serine residue in two ways. First, the microscopic rate constant for acylation (k2) is attenuated by three to four orders of magnitude over the corresponding determinations for penicillin-sensitive PBPs. Second, the enzyme shows elevated dissociation constants (Kd) for the noncovalent preacylation complexes with the antibiotics, the formation of which ultimately would lead to enzyme acylation. The two factors working in concert effectively prevent enzyme acylation by the antibiotics in vivo, giving rise to drug resistance. Catalase and oxidase are enzymes produced by some bacteria that confer virulence to the organism but do not make the organisms methicillin resistant. Glycocalix is the pericellular layer produced by bacteria that serves many functions including attachment to surfaces. Beta-lactam describes a class of antibiotics. Fuda C, Suvorov M, Vakulenko SB, et al: The basis for resistance to beta-lactam antibiotics by penicillin-binding protein 2a (PBP2a) of methicillin-resistant staphylococcus aureus. J Biol Chem 2004;279:40802-40806. Lim D, Strynadka NC: Structural basis for the beta lactam resistance of PBP2a from methicillin-resistant Staphylococcus aureus. Nat Struct Biol 2002;9:870-876.
References:
- Schwarz EM: Infections in orthopaedics, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 100High Yield
What is the primary indication for performing an arthroscopic synovectomy on a patient with hemophilia that is the result of factor VIII deficiency?
Explanation
Explanation
Improved medical management has changed musculoskeletal outcomes for individuals with hemophilia. Patients with severe hemophilia receiving prophylactic administration of factor VIII may never develop a target joint that requires further orthopaedic intervention. Patients with moderate hemophilia and those patients with severe hemophilia not receiving prophylactic treatment will still develop joints that have recurrent hemarthroses. When recurrent hemarthrosis continues despite optimal medical management, synovectomy is indicated. While synovectomy is predictable in its ability to decrease joint bleeding, it does not necessarily improve joint range of motion or prevent the development of hemophilic arthropathy over time. It will not reverse articular damage to the joint once it has developed. Dunn AL, Busch MT, Wyly JB; et al: Arthroscopic synovectomy for hemophilic joint disease in a pediatric population. J Pediatr Orthop 2004;24:414-426.
References:
- Journeycake JM, Miller KL, Anderson AM, et al: Arthroscopic synovectomy in children and adolescents with hemophilia. J Pediatr Hematol Oncol 2003;25:726-731.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon