Orthopedic Board Review Mock Exam Set 1082: 100 High-Yield MCQs for ABOS, OITE & FRCS
14 Apr 2026
100 min read
144 Views
Key Takeaway
This page provides 100 high-yield orthopedic board review questions (Mock Exam Set 1082) designed for ABOS, OITE, and FRCS exam preparation. Surgeons can test their knowledge across diverse topics, solidify understanding, and master key concepts essential for board certification and continuing education success.
Posterior Hip Approach: Optimize the Aspect o...
00:00
Start Quiz
Question 1High Yield
A 47-year-old woman falls and sustains a direct blow to her middle finger. She notes pain and swelling and is unable to move the proximal interphalangeal (PIP) or distal interphalangeal (DIP) joints. Radiographs are shown in Figures 8a through 8c. Proper management should consist of
Explanation
Explanation
8b 8c The oblique nature of the fracture and extension of the fracture to the condyles implies an unstable fracture. Lag screw fixation provides an excellent chance of union, and the ability to start early range of motion. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green's Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Question 2High Yield
A healthy 25-year-old man sustains a grade IIIB open tibial fracture. Following appropriate debridement, irrigation, and stabilization with an external fixator, the soft-tissue injury is shown in Figure 30. What is the most appropriate definitive soft-tissue coverage procedure?
Explanation
Explanation
This is a very large near circumferential defect with posterior as well as anterior skin and muscle injury. Bone is exposed. The posterior muscles cannot be rotated since they are part of the zone of injury. The bone and other poorly vascularized areas of this wound would not accept a skin graft. The best chance for limb salvage will be to obtain soft-tissue coverage with a free tissue transfer using the latissimus dorsi. Mathes SJ, Nahai F: Vascular anatomy of muscle: Classification and applications, in Mathes SJ, Nahai F (eds): Clinical Application for Muscle and Musculocutaneous Flaps. St Louis, MO, CV Mosby, 1982, p 20.
References:
- Bos GD, Buehler MJ: Lower-extremity local flaps. J Am Acad Orthop Surg 1994;2:342-351.
Question 3High Yield
What inflammatory mediator has been most closely associated with the magnitude of the systemic inflammatory response to trauma and with the development of multiple organ dysfunction syndrome (MODS)?
Explanation
Explanation
Multiple cytokines (inflammatory mediators) are released following trauma, and their levels can be measured in serum. Persistent elevated levels of IL-6 (> 800 pg/mL) indicate an exaggerated systemic inflammatory response to trauma and have been associated with the development of MODS. Recent work has shown that extensive surgical procedures should be avoided when IL-6 levels remain elevated to prevent the precipitation of MODS. In the future, it is likely that this mediator and possibly others will be used to determine timing and techniques of future treatment. Patrick DA, Moore FA, Moore EE, et al: Jack A. Barney Resident Research Award winner: The inflammatory profile of interleukin-6, interleukin-8, and soluble intercellular adhesion molecule-1 in postinjury multiple organ failure. Am J Surg 1996;172:425-429. Pape HC, van Griesven M, Rice J, et al: Major secondary surgery in blunt trauma patients and perioperative cytokine liberation: Determination of the clinical relevance of biochemical markers. J Trauma 2001;50:989-1000.
References:
- Giannoudis PV: When is the safest time to undertake secondary definitive fracture stabilization procedures in multiply injured patients who were initially managed using a strategy of primary temporary skeletal fixation. J Trauma 2002;52:811-812.
Question 4High Yield
A 42 year-old-woman who underwent surgery for lumbar scoliosis 2 years ago now has fixed sagittal plane imbalance and severe back pain. Which of the following is considered a contraindication to isolated pedicle subtraction osteotomy for the treatment of iatrogenic flatback syndrome in this patient?
Explanation
Pedicle subtraction osteotomy is the preferred osteotomy technique for the treatment of many patients with iatrogenic flatback syndrome. In the presence of an anterior pseudarthrosis, however, it must be done in conjunction with an anterior procedure. Prior laminectomy is not a contraindication. Significant correction, usually averaging about 30 degrees, can be obtained through each osteotomy. Osteotomies should be performed at L2 or below in the presence of kyphosis at the thoracolumbar junction. The pedicle subtraction technique is preferred with vascular calcifications because it does not lengthen the anterior column, which could risk vascular injury. Potter BK, Lenke LG, Kuklo TR: Prevention and management of iatrogenic flatback deformity. J Bone Joint Surg Am 2004;86:1793-1808.
Question 5High Yield
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?
Explanation
The MRI scan shows a far lateral disk herniation. With the L4-5 disk, a far lateral herniation abuts the left L4 nerve root. The findings would be consistent with those of a left L4 radiculopathy and would include pain or a sensory deficit on the anteromedial aspect of the knee, diminished patellar tendon reflex, and quadriceps weakness, perhaps making it difficult to walk up and down stairs. Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
Question 6High Yield
A 17-year-old high school football player reports wrist pain 5 months after the conclusion of the football season. A radiograph and MRI scan are shown in Figures 29a and 29b. What is the recommended intervention?
Explanation
Explanation
29b The patient has a nonunion of the proximal pole of the scaphoid. Acutely, this can be repaired with a screw alone, but as a nonunion the proximal pole has very poor healing potential. Vacularized bone grafts have been successful for these challenging nonunions, particularly in adolescents. A cast can be used for nondisplaced acute waist fractures, and corticocancellous grafts can be used for nonunions of the waist. Waters PM, Stewart SL: Surgical treatment of nonunion and avascular necrosis of the proximal part of the scaphoid in adolescents. J Bone Joint Surg Am 2002;84:915-920.
References:
- Steinmann SP, Bishop AT, Berger RA: Use of the 1,2 intercompartmental supraretinacular artery as a vascularized pedicle bone graft for difficult scaphoid nonunion. J Hand Surg Am 2002;27:391-401.
Question 7High Yield
Figure 63 shows the radiographs of a 23-year-old man who sustained a twisting injury at work. Swelling, tenderness, and ecchymosis are noted about the entire midfoot. What associated injury is most likely to be problematic?
Explanation
This cuboid compression fracture ("nutcracker" injury) is associated with subtle injury to the Lisfranc complex. This diagnosis must be made to ensure proper treatment.
Question 8High Yield
Figure 23 shows failure of the femoral stem in a patient. What is the most likely reason for the failure?
Explanation
Explanation
A two-dimensional stress analysis has been used to study the effects of some of the factors leading to early fatigue failure of the femoral stem in total hip arthroplasty. It has been demonstrated that loss of proximal stem support at the level of the calcar femorale and subsequent stem stress can lead to fatigue failure. In addition, the role of body weight and range of cyclic stress fluctuation play an important role in fatigue life under conditions where the stem has lost proximal support. These results indicate that stem design could be improved by incorporating some means of adequate support at the calcar femorale where maximum tensile stresses are found to occur. Femoral component fracture is a rare but well-documented complication after total hip arthroplasty. Historically, most stem fractures occur at the middle third of the implant where proximal stem loosening and solid distal stem fixation result in cantilever bending and eventual fatigue failure. The component shown is a modular fluted cementless stem that occasionally fractures at the modular junction in patients with poor proximal bone support. Andriacchi TP, Galante JO, Belytschko TB, et al: A stress analysis of the femoral stem in total hip prostheses. J Bone Joint Surg Am 1976;58:618-624.
References:
- Gruen TA, McNeice GM, Amstutz HC: "Modes of failure" of cemented stem-type femoral components: A radiographic analysis of loosening. Clin Orthop 1979;141:17-27.
Question 9High Yield
A previously healthy 13-year-old girl has had thigh pain for the past 3 weeks. The radiograph shown in Figure 47a reveals a lesion in the right femur. A bone scan and CT scan of the chest show no evidence of other lesions. A biopsy specimen is shown in Figure 47b. What is the most likely diagnosis?

Explanation
The patient has Langerhans cell histiocytosis that may be solitary (eosinophilic granuloma) or associated with systemic illness (Hand-Schuller-Christian disease and Letterer-Siwe disease). The solitary form of the disease, eosinophilic granuloma, typically affects patients in the first three decades of life. Radiographically, it is characterized as a well-defined, lytic, "punched out" intramedullary lesion. Histologically, two cell types, eosinophils and Langerhans cells, are seen. The Langerhans cells are seen as mononuclear histiocyte-like cells with oval nuclei with well-defined round or oval cytoplasm. A prominent nuclear groove can be seen in most of the nuclei (coffee bean nuclei). A mixture of inflammatory cells and lipid-laden foam cells with nuclear debris may be present as well. The lack of nuclear atypia and atypical mitoses excludes malignant conditions such as Ewing's sarcoma, lymphoma of bone, and metastatic neuroblastoma. The lack of acute inflammatory cells excludes the diagnosis of osteomyelitis. The eosinophils have bi-lobed nuclei and granular eosinophilic cytoplasm. Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby, 1988.
Question 10High Yield
A 15-year-old high school soccer player collides with an opponent and is unconscious when the trainer arrives on the field. He is conscious within 15 seconds, breathing appropriately, and denies any headache, neck pain, or nausea. It is his first head injury. Provided that the athlete is free of symptoms, when should he be allowed to return to athletic activity?
Explanation
The loss of consciousness indicates a grade 2 concussion, which necessitates a 4-week period out of sport. The last week prior to return must be symptom-free and the athlete should not have symptoms in practice. Cantu RC: Return to play guidelines after a head injury. Clin Sports Med 1998;17:45-60.
Question 11High Yield
What is the most appropriate treatment for a 50-year-old woman who sustains the injury shown in Figures 14a and 14b?
Explanation
Explanation
14b This intra-articular distal humerus fracture with displacement at the joint surface is best treated with surgical fixation. The most biomechanically sound construct is two plates applied to either column 180 degrees from one another. Elbow arthroplasty is most appropriate for low demand elderly patients. Schemitsch EH, Tencer AF, Henley MB: Biomechanical evaluation of methods of internal fixation of the distal humerus. J Orthop Trauma 1994;8:468-475. McCarty LP, Ring D, Jupiter JB: Management of distal humerus fractures. Am J Orthop 2005;34:430-438.
Question 12High Yield
A 48-year-old ski instructor dislocates his nondominant shoulder in a fall. Management consisting of application of a sling for 1 week results in improvement in his pain. Follow-up examination 6 weeks after the injury reveals that the patient continues to have difficulty with shoulder elevation. Management should now include
Explanation
Explanation
Patients who are older than age 45 years and have initial dislocations are at greater risk for tearing the rotator cuff. Patients who are unable to lift the upper extremity or who have continued pain should undergo further evaluation for potential rotator cuff tears; early diagnosis is preferred. Physical therapy or continued use of a sling will be of little benefit. A corticosteroid injection might delay the diagnosis and compromise subsequent rotator cuff repair. Repairing the labrum generally is not necessary in a patient of this age who has an initial dislocation. Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
References:
- Matsen FA III, Thomas SC, Rockwood CA: Anterior glenohumeral instability, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 526-622.
Question 13High Yield
A college football player performs bicep curls as part of his weight lifting routine. During the flexion phase of the curl, what term defines the type of muscle contraction?
Explanation
Explanation
Muscle contractions can be classified by tension, length, and velocity. Isometric contractions involve changing tension in the muscle while the muscle stays at a constant length. An example would be pushing against a wall. Isokinetic contractions occur when the muscle maximally contracts at a constant velocity. Isotonic contractions involve constant tension throughout the range of motion. Eccentric contraction is when the muscle lengthens during contraction. Eccentric contractions have the highest risk of injury. Plyometrics are eccentric contractions at a rapid rate. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 89-125.
References:
- Evans WJ: Effects of exercise on senescent muscle. Clin Orthop 2002;403:S211-S220.
Question 14High Yield
Figure 7 shows a sagittal T1-weighted MRI scan. What muscle/tendon is identified by the arrow?
Explanation
Explanation
The sagittal T1-weighted MRI scan is useful for interpreting the quality of muscle. The arrow is pointing to the teres minor. Goutallier D, Postel JM, Gleyze P, et al: Influence of cuff muscle fatty degeneration on anatomic and functional outcomes after simple suture of full-thickness tears. J Shoulder Elbow Surg 2003;12:550-554.
References:
- Agur AM (ed): Grant's Atlas of Anatomy, ed 9. Baltimore, MD, Lippincott Williams & Wilkins, 1991, p 394.
Question 15High Yield
A 30-year-old man has chronic pain, joint stiffness, and symmetrical polyarthropathy but no significant synovitis. Examination reveals enlargement of the second and third metatarsal heads. Radiographs show chondrocalcinosis of the ankles and bony enlargement of the midfoot; no marginal erosions are evident at the metatarsophalangeal level. What is the most likely diagnosis?
Explanation
Explanation
The patient's clinical picture is considered the classic presentation for hemochromatosis. Osteoarthritis and pseudogout more commonly affect an older age group. Rheumatoid arthritis is more common in women and is not commonly associated with chondrocalcinosis. The radiographic appearance of the forefoot in Reiter's syndrome is one of a pencil in cup deformity of the metatarsophalangeal joint, not enlargement. Stevens FM, Edwards C: Recognizing and managing hemochromatosis and hemochromatosis arthropathy. J Musculoskeletal Med 2004;4:212-225.
References:
- Baker ND, Jahss MH, Levanthal GH: Unusual involvement of the feet in hemochromatosis. Foot Ankle 1984;4:212-215.
Question 16High Yield
The vascularity of the digital flexor tendons is significantly richer in what cross-sectional region?
Explanation
The vascularity of the dorsal portion of the digital flexor tendons is considerably richer than the volar portion. The other regions are not preferentially more vascular. Hunter JM, Scheider LH, Makin EJ (eds): Tendon Surgery in the Hand. St Louis, MO, Mosby, 1987, pp 91-99.
Question 17High Yield
Figure 16 shows the radiograph of a 23-year-old man who has severe right shoulder pain after his motorcyle hit a bridge guardrail. He is neurologically intact. Nonsurgical management will most likely result in
Explanation
Internal fixation of the clavicle, glenoid, or both has been recommended for fractures of the clavicle and glenoid neck (floating shoulders). Recently, the inherent instability of these dual fractures has been questioned in a biomechanical model without further disruption of the coracoclavicular or acromioclavicular ligamentous structures. Nonsurgical management of the majority of combined scapular/glenoid fractures in patients with less than 10 mm of displacement has resulted in excellent shoulder function and will most likely achieve an excellent result in this patient. Egol KA, Connor PM, Karunakar MA, Sims SH, Bosse MJ, Kellam JF: The floating shoulder: Clinical and functional results. J Bone Joint Surg Am 2001;83:1188-1194. Williams GR Jr, Naranja J, Klimkiewicz J, et al: The floating shoulder: A biomechanical basis for classification and management. J Bone Joint Surg Am 2001;83:1182-1187.
Question 18High Yield
An active 60-year-old man is evaluated 4 years following surgical correction of a hallux valgus deformity. The patient reports that a hallux varus deformity developed rapidly following his initial surgery. Conservative management consisting of wider shoes, toe strapping, and anti-inflammatory drugs has failed to provide relief. Examination reveals a hallux varus deformity with restricted painful motion of the metatarsophalangeal joint and callus formation under the second metatarsal head. What is the next most appropriate step in management?
Explanation
Explanation
Hallux varus may occur as a complication following hallux valgus surgery, most commonly a modified McBride-type procedure. Conservative management is the initial treatment of choice; however, if unsuccessful, surgical options for reconstruction include soft-tissue reconstruction or metatarsophalangeal joint arthrodesis. The patient has evidence of joint arthrosis, making an arthrodesis the preferred method of reconstruction. Fascial arthroplasty, Silastic arthroplasty, and Keller resection arthroplasty will not correct the underlying deformity. Kitaoka HB, Patzer GL: Arthrodesis versus resection arthroplasty for failed hallux valgus operations. Clin Orthop 1998;347:208-214.
References:
- Ouzounian TJ: Metatarsophalangeal arthrodesis for salvage of failed hallux valgus surgery. Foot Ankle Clin 1997;2:741-752.
Question 19High Yield
A quarterback sustains a rough tackle after which he appears confused, has a dazed look on his face and an unsteady gait on standing. He denies loss of consciousness. Reexamination within 10 minutes is normal, the patient is lucid, and he wants to return to play. The coach and the player should be advised that he may
Explanation
The patient has a grade I (mild) concussion that can result in confusion and disorientation, without loss of consciousness. This concussion syndrome is completely reversible, with no long-term sequelae. Athletes who sustain a grade I concussion may return to play after 15 minutes if there are no lingering symptoms, such as headache or vertigo. A grade II concussion is characterized by loss of consciousness of less than 5 minutes. With this type of injury, the athlete can return to play in 1 week, if asymptomatic. If a grade III (severe) concussion is sustained, the athlete should avoid contact for a minimum of 1 month before considering a return to competition. A grade III concussion is characterized by a loss of consciousness of greater than 5 minutes or posttraumatic amnesia of greater than 24 hours. A CT scan is not indicated in a grade I injury. An athlete who sustains three grade I or grade II concussions, or two grade III concussions may not return to play for the season. Torg JS, Gennarelli TA: Head and cervical spine injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine Principles & Practice. Philadelphia, PA, WB Saunders, 1994, vol 1, pp 417-462.
Question 20High Yield
Examination of a 9-year-old boy reveals a right thoracic prominence on forward flexion. Neurologic examination is normal, and no other abnormalities are noted. AP radiographs reveal a 30-degree right thoracic curve. Initial management should consist of
Explanation
The patient has juvenile scoliosis. MRI has shown an association between juvenile scoliosis and intraspinal abnormalities, most often syringomyelia and Arnold-Chiari malformations. All juvenile curves greater than 20 degrees should be evaluated with MRI despite the absence of neurologic findings. Weinstein SL (ed): The Pediatric Spine: Principles and Practice, ed 1. New York, NY, Raven Press, 1994, pp 685-705 Nohria V, Oakes WJ: Chiari I malformation: A review of 43 patients. Pediatr Neurosurg 1990-91;16:222-227.
Question 21High Yield
Pacinian corpuscles are lamellated nerve endings that are responsible for providing the perception of
Explanation
Pacinian corpuscles are nerve endings that provide the perception of pressure.
Question 22High Yield
A 20-year-old professional baseball pitcher has had a 3-year history of increased aching in his shoulder that is associated with pitching, and he is now seeking a second opinion. Nonsurgical management consisting of rest, anti-inflammatory drugs, ice, heat, and cortisone injections has failed to provide relief. A previous work-up that included radiographs and gadolinium-enhanced MRI arthrography was negative. Results of an arteriogram suggest quadrilateral space syndrome. Assuming that this is the correct diagnosis, what nerve needs to be decompressed?
Explanation
Quadrilateral space syndrome is a rare condition and is the result of compression of the contents of the quadrilateral space. The contents of the quadrilateral space include the posterior circumflex vessels and the axillary nerve. Cahill BR, Palmer RE: Quadrilateral space syndrome. J Hand Surg 1983;8:65-69.
Question 23High Yield
Posterior sternoclavicular dislocations are most commonly associated with which of the following complications?
Explanation
Posterior sternoclavicular dislocations are commonly associated with tracheal compression, which can be a life-threatening condition requiring immediate reduction. The other listed complications are less common. Brooks AL, Henning GD: Injury to the proximal clavicular epiphysis, abstracted. J Bone Joint Surg Am 1972;54:1347-1348.
Question 24High Yield
A 43-year-old soccer player who had knee pain following a twisting injury underwent an arthroscopic meniscectomy 6 months ago. He continues to report posterior knee pain. Examination reveals soft-tissue fullness and tenderness just above the popliteal fossa, trace knee effusion, full range of knee motion, no instability, and negative meniscal signs. Radiographs show some mild medial joint space narrowing but no other bony changes. What is the next most appropriate step in management?
Explanation
Explanation
The phenomenon of tumors misdiagnosed as athletic injuries has been termed "sports tumors." Lewis and Reilly presented a series of 36 patients who initially were thought to have a sports-related injury but ultimately were diagnosed with a primary bone tumor, soft-tissue tumor, or tumor-like condition. Muscolo and associates presented a series of 25 tumors that had been previously treated with an intra-articular procedure as a result of a misdiagnosis of an athletic injury. Initial diagnoses included 21 meniscal lesions, one traumatic synovial cyst, one patellofemoral subluxation, one anterior cruciate ligament tear, and one case of nonspecific synovitis. The final diagnoses were a malignant tumor in 14 patients and a benign tumor in 11 patients. The authors noted that oncologic surgical treatment was affected in 15 of the 25 patients. The most frequent causes of erroneous diagnosis were initial poor quality radiographs and an unquestioned original diagnosis despite persistent symptoms. Persistent symptoms warrant further diagnostic studies, not additional treatment such as physical therapy, corticosteroid injection, or an unloader brace. Although a bone scan may be helpful in this case and confirm arthrosis of the medial compartment, the suspicion of a soft-tissue mass makes MRI the imaging modality of choice. Muscolo DL, Ayerza MA, Makino A, et al: Tumors about the knee misdiagnosed as athletic injuries. J Bone Joint Surg Am 2003;85:1209-1214.
References:
- Lewis MM, Reilly JF: Sports tumors. Am J Sports Med 1987;15:362-365.
Question 25High Yield
Injury to which of the following structures has been reported following iliac crest bone graft harvest?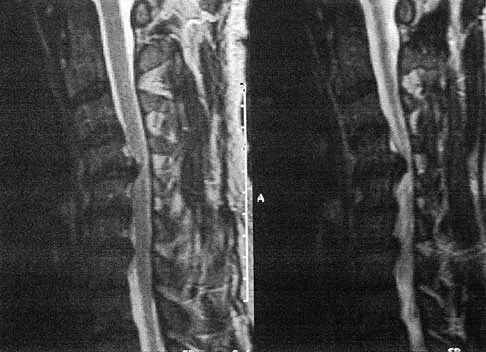
Explanation
Injury to the lateral femoral cutaneous nerve and the ilioinguinal nerve have both been described with an anterior iliac crest bone graft harvest. The lateral femoral cutaneous nerve may be injured from retraction after elevating the iliacus muscle or from direct injury when the nerve actually courses over the crest. A posterior crest harvest can injure the superior gluteal artery if a surgical instrument violates the sciatic notch. Injury to the inferior gluteal artery has not been described; it leaves the pelvis below the piriformis muscle belly and should not be at risk even with a violation of the sciatic notch. Injury to the ilioinguinal nerve has been reported from vigorous retraction of the iliacus muscle after exposing the inner table of the anterior ilium. Cluneal nerve injury may occur with posterior crest harvest, particularly if the skin incision is horizontal or extends more than 8 cm superolateral from the posterior superior iliac spine. Kurz LT, Garfin SR, Booth RE Jr: Iliac bone grafting: Techniques and complications of harvesting, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 323-341.
Question 26High Yield
A 71-year-old woman undergoes a posterior lumbar decompression and fusion from L4-S1. Thirty-six hours after the procedure, she reports severe right-sided chest pain and shortness of breath. Doppler ultrasound reveals a clot proximal to the knee within the femoral vein. A large pulmonary embolus is confirmed by CT angiography. The next most appropriate step in management should consist of
Explanation
Explanation
In a review of 13,000 spinal procedures, nine patients were treated with heparin following development of pulmonary emboli. Of these patients, six had serious complications ranging from wound drainage to paralysis. Heparin therapy instituted within 10 days of the surgical procedure resulted in a 100% complication rate. Vena cava filter placement has a complication rate of 0.12% to 10.1%. Removable filters are currently in clinical trials. Cain JE Jr, Major MR, Lauerman WC, et al: The morbidity of heparin therapy after development of pulmonary embolus in patients undergoing thoracolumbar or lumbar spinal fusion. Spine 1995;20:1600-1603. Roberts AC: Venous imaging and inferior vena cava filters. Curr Opin Radiol 1992;4:88-96.
References:
- Becker DM, Philbrick JT, Selby JB: Inferior vena cava filters. Arch Intern Med 1992;152:1985-1994.
Question 27High Yield
Which of the following bearing materials is most resistant to scratching from third-body debris?
Explanation
Alumina is the hardest of all the materials listed. Clinical retrieval demonstrates resistance to scratching from third-body debris.
Question 28High Yield
A 23-year-old man has had right posterolateral knee pain and occasional lateral calf dysesthesias for the past 8 months. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 62a through 62e. What is the most likely diagnosis?
Explanation
Explanation
62b 62c 62d 62e The radiograph shows an eccentric, cortically based lytic lesion in the proximal fibula. The CT and MRI scans confirm that it is well circumscribed and cortically based with significant surrounding edema. The radiographic differential diagnosis would be a Brodie's abscess or osteoid osteoma. An osteoblastoma would have to be greater than 2 cm in size. A chondroblastoma may also have significant edema around it, but it is an epiphyseal-based lesion, not cortically based. The well-circumscribed nature of the lesion is not consistent with osteosarcoma. The pathology shows a very cellular and vascular stroma with plump, but not atypical osteoblast cells making a matrix of immature woven bone. There are no abundant inflammatory cells or dead bone suggestive of osteomyelitis or a Brodie's abscess. Therefore, the clinical and histologic picture is most consistent with an osteoid osteoma. Percutaneous radiofrequency ablation, usually with CT guidance, has become the preferred method for treating most cases of osteoid osteoma. Rosenthal DI: Radiofrequency treatment. Orthop Clin North Am 2006;37:475-484.
References:
- Ghanem I: The management of osteoid osteoma: Updates and controversies. Curr Opin Pediatr 2006;18:36-41.
Question 29High Yield
A 12-year-old girl who has a history of frequent tripping and falling also has bilateral symmetric hand weakness, high arched feet, absent patellar and Achilles tendon reflexes, and excessive wear on the lateral border of her shoes. She reports that she has multiple paternal family members with similar deformities. She most likely has a defect of what protein?
Explanation
Explanation
The girl shows clinical features of hereditary motor sensory neuropathy type 1, Charcot-Marie-Tooth disease. The most common type of this autosomal-dominant disease is due to an underlying defect in the gene coding for peripheral myelin protein-22 on chromosome 17. Many other less common mutations have been identified in this family of neuropathies. Dystrophin is a protein that is abnormal in Duchenne's muscular dystrophy, which affects males and is diagnosed earlier. Type I collagen is defective in osteogenesis imperfecta. Alpha-L-iduronidase is defective in mucopolysaccharidosis type I, Hurler's syndrome. Defective cartilage oligomeric matrix protein is associated with some forms of multiple epiphyseal dysplasia. Patel PI, Roa BB, Welcher AA, et al: The gene for the peripheral myelin protein PMP-22 is a candidate for Charcot-Marie-Tooth disease type 1A. Nat Genet 1992;1:159-165.
References:
- Harding AE: From the syndrome of Charcot, Marie and Tooth to disorders of peripheral myelin proteins. Brain 1995;118:809-818.
Question 30High Yield
A 43-year-old bus driver sustains a hyperextension injury to her arm and shoulder 4 months after undergoing an open Bankart repair. Examination reveals increased external rotation, anterior shoulder pain, and internal rotation weakness. Her examination also reveals the findings shown in Figure 44. What is the most likely diagnosis?
Explanation
An isolated tear of the subscapularis tendon has been noted as early as 1835 by Smith. In Gerber and associates' 1991 report of 16 men with an average age of 51 years, isolated subscapularis tendon rupture was often caused by a violent hyperextension injury. All patients reported pain anteriorly along with night pain. They also noted pain and weakness of the arm. The lift-off test is performed by having the patient lift the palm of the hand away from the small of the back. The patient must have sufficient internal rotation to allow this test to be performed. A subscapularis rupture is likely if the patient cannot perform the lift-off test. Hertel R, Ballmer FT, Lombert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-313. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394. Greis PE, Kuhn JE, Schultheis J, Hintermeister R, Hawkins R: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Question 31High Yield
A 14-year-old boy sustained a femoral neck fracture in a fall from a tree and underwent open reduction and internal fixation 6 months ago. Follow-up examination now reveals an antalgic Trendelenburg gait and painful range of motion. A radiograph is shown in Figure 23, and a CT scan shows a nonunion. Treatment should consist of
Explanation
The coxa vara deformity and fracture nonunion should be treated simultaneously; therefore, the treatment of choice is curettage of the nonunion, intertrochanteric valgus osteotomy, and revision internal fixation. In addition, valgus osteotomy will convert the shear forces across the nonunion to compression, aiding in healing of the nonunion. None of the other procedures addresses both issues, and hip fusion is inappropriate under these conditions. Lam SF: Fractures of the neck of the femur in children. J Bone Joint Surg Am 1971;53:1165-1179.
Question 32High Yield
Chronic anterior donor site pain following the harvest of autologous iliac crest bone graft for use during anterior cervical diskectomy and fusion is reported by approximately what percent of patients?
Explanation
Explanation
Four years after surgery, more than 90% of patients are satisfied with the cosmetic appearance of the iliac donor site scar. Approximately 25% still have pain and/or functional difficulty, including 12.7% who still report difficulty with ambulation, 11.9% difficulty with recreational activities, 7.5% with sexual intercourse, and 11.2% require pain medication for iliac donor site symptoms. Silber JS, Anderson DG, Daffner SD, et al: Donor site morbidity after anterior iliac crest bone harvest for single-level anterior cervical discectomy and fusion. Spine 2003;28:134-139.
References:
- Cockin J: Autologous bone-grafting complications at the donor site. J Bone Joint Surg Br 1971;49:153.
Question 33High Yield
Which of the following factors has the most effect on the pullout strength of lumbar transpedicular screw fixation?
Explanation
Explanation
Although all of the factors listed contribute to the pullout strength of transpedicular screw fixation, low bone density generally is felt to be the most influential. Wittenberg RH, Shea M, Swartz DE, Lee KS, White AA III, Hayes WC: Importance of bone mineral density in instrumented spine fusions. Spine 1991;16:647-652.
References:
- Zindrick MR, Wiltse LL, Widell EH, et al: A biomechanical study of intrapeduncular screw fixation in the lumbosacral spine. Clin Orthop 1986;203:99-112.
Question 34High Yield
A 35-year-old man has numbness and tingling in the index, middle, and ring fingers. History reveals that he also has had vague wrist pain and stiffness since being injured in a motorcycle accident 1 year ago. Radiographs are shown in Figures 47a through 47c. Management should consist of


Explanation
The patient has a chronic unrecognized volar lunate dislocation. Median nerve compression is the result of the lunate displaced into the carpal tunnel. The diagnosis can be made by radiographs; MRI is not necessary. A volar approach allows median nerve decompression with excision of the lunate, whereas a dorsal approach facilitates excision of the scaphoid and triquetrum. Rettig ME, Raskin KB: Long-term assessment of proximal row carpectomy for chronic perilunate dislocations. J Hand Surg Am 1999;24:1231-1236.
Question 35High Yield
What is the most likely type of pathology seen in Figure 16?
Explanation
The figure shows the missing pedicle or "winking owl" sign that is characteristic of tumor involvement of the cortical bone of the pedicle. None of the other pathologic processes commonly gives this radiographic picture. Thinned, but not missing pedicles, have been described as a normal variant. McLain R, Weinstein J: Tumors of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1173.
Question 36High Yield
A 64-year-old man who underwent total shoulder arthroplasty 4 weeks ago is making satisfactory progress in physical therapy, but his therapist notes limitations in external rotation to neutral. A stretching program is started, and the patient suddenly gains 90 degrees of external rotation but now reports increased pain and weakness. What is the best course of action?
Explanation
Explanation
Nearly all approaches to shoulder arthroplasty require detachment of the subscapularis tendon from the humerus and subsequent repair. Healing of this tenotomy is one of the limiting factors in postoperative recovery. Failure of the tenotomy repair must be recognized and treated early with repeat repair or pectoralis muscle transfer for optimal results. Failure of the subscapularis is diagnosed clinically as excessive external rotation and weakness, especially in the lift-off or belly press position. Muscle testing can be difficult in the postoperative period and may not be possible to assess in those positions. Although MRI might be useful to confirm the diagnosis, studies may be limited by artifact. CT or electromyography would not be diagnostic. Wirth MA, Rockwood CA Jr: Complications of total shoulder-replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
References:
- Miuer SL, Hazrati Y, Klepps S, et al: Loss of subscapularis function after shoulder replacement: A seldom recognized problem. J Shoulder Elbow Surg 2003;12:29-34.
Question 37High Yield
What is the most common reason an individual with a malignant soft-tissue tumor in the extremities seeks medical attention?
Explanation
Explanation
Unlike malignant bone tumors, malignant soft-tissue tumors usually are asymptomatic and present with the presence of a mass. Malignant soft-tissue tumors enlarge by centrifugal growth, creating a mass while compressing surrounding tissue. Symptoms may develop as the result of direct compression on neurovascular structures as the tumor enlarges. This is especially true in the pelvis where the tumor can enlarge appreciably without being noticed. However, in the extremities, the tumor is most often apparent before neurologic symptoms develop. An asymptomatic mass is not necessarily benign; therefore, biopsy should not be delayed. It is uncommon for a malignant soft-tissue mass to be discovered incidentally. Soft-tissue tumors are not typically apparent on radiographs; they are best identified with MRI. Brouns F, Stas M, De Wever I: Delay in diagnosis of soft tissue sarcomas. Eur J Surg Oncol 2003;29:440-445. Rougraff B: The diagnosis and management of soft tissue sarcomas of the extremities in the adult. Curr Probl Cancer 1999;23:1-50.
References:
- Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 38High Yield
Which of the following drawbacks is associated with the Ganz periacetabular osteotomy?
Explanation
Although technically challenging, the Ganz periacetabular osteotomy offers advantages over other rotational pelvic osteotomies. Posterior column integrity is maintained, as is the acetabular vascular supply. Free mobility of the fragment makes large corrections in the center edge angle possible. Because of the asymmetric cuts and the need to restore anterior coverage, there is a tendency to anterior displacement of the joint while flexing the acetabulum. The procedure is commonly performed through a Smith-Petersen incision. Trousdale RT, Ganz R: Periacetabular osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, Pa, Lippincott-Raven, 1998, pp 789-802. Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 39High Yield
What type of metastatic tumor most often has a lytic radiographic appearance?
Explanation
Lung carcinoma most often has a lytic radiographic appearance. Bladder and prostate carcinoma are usually blastic. Breast carcinoma can be both blastic and lytic. Thyroid carcinoma may be difficult to visualize radiographically and may be seen only on MRI scans. Metastatic osteosarcomas typically produce bone. Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Question 40High Yield
A 14-year-old football player has had right knee pain for the past 2 months; however, he denies any history of trauma. Examination shows an abductor lurch and increased external rotation of the right lower extremity. The best course of action should be to
Explanation
Explanation
Slipped capital femoral epiphysis is the most common pathology involving the hip in adolescents. While patients with acute slips may report severe pain and are unable to ambulate, those with chronic slips often have pain during ambulation, a limp, and increased external rotation of the hip. While 60% of the patients specifically report hip pain, the remainder have pain in the thigh or knee. The initial diagnostic study of choice is AP and frog-lateral radiographs of the pelvis; bilateral involvement is frequently seen. Boyer DW, Mickelson MR, Ponseti IV: Slipped capital femoral epiphysis: Long-term follow-up study of one hundred and twenty-one patients. J Bone Joint Surg Am 1981;63:85-95.
References:
- Stasikelis PJ, Sullivan CM, Philips WA, Polard JA: Slipped capital femoral epiphysis: Prediction of contralateral involvement. J Bone Joint Surg Am 1996;78:1149-1155.
Question 41High Yield
The incidence of osteosarcoma is highest in what age group?
Explanation
The peak incidence of osteosarcoma occurs in the second decade, followed by the third decade. Up to 75% of all cases of osteosarcoma occur in patients between 10 and 25 years. It rarely occurs after age 30. Affected women tend to be younger than affect men. Osteosarcoma associated with Paget's disease or in radiation-induced osteosarcoma occurs in an older population. Simon M, Springfield D, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 266. Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989.
Question 42High Yield
A 34-year-old woman has had painful snapping and popping in the elbow since falling while in-line skating 6 months ago. The popping also occurs when she pushes off with her hands to rise from a seated position. Initial radiographs were normal, and she was told that she had sprained her elbow. Examination reveals few findings except that she is very apprehensive when the forearm is forcefully supinated with the elbow extended or partially flexed. A radiograph taken in that position is shown in Figure 24. Treatment should consist of
Explanation
Explanation
The radiograph reveals posterolateral rotatory subluxation of the radiohumeral and ulnohumeral joints. The space between the ulna and trochlea is enlarged, particularly posteriorly at the olecranon. These findings are diagnostic of posterolateral rotatory instability, which causes recurrent subluxation and reduction as the elbow is flexed from an extended and supinated position with valgus load. The posterolateral rotatory instability apprehension test was performed on this patient and the result was positive. The lateral pivot-shift test causes a clunk as the elbow reduces but is more difficult to perform, even under general anesthesia. The patient does not have isolated subluxation of the radial head, although these findings can be mistakenly diagnosed as such. The radial head is normally shaped and does not represent a congenital dislocation. There are no findings here to suggest osteochondritis dissecans or loose bodies. O'Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446. Burgess RC, Sprague HH: Post-traumatic posterior radial head subluxation: Two case reports. Clin Orthop 1984;186:192-194.
References:
- Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354.
Question 43High Yield
Figure 23 shows the radiograph of a 7 year-old girl with a low thoracic-level myelomeningocele. She has a history of skin ulcers over the apex of the deformity, but her current skin condition is good. Management of the spinal deformity should consist of
Explanation
This form of severe kyphosis results in intractable difficulties with sitting position, compression of internal organs, and chronic skin breakdown. Kyphectomy and posterior fusion with instrumentation, while associated with a high rate of complications, provides one of the best solutions to this clinical dilemma. The other choices are either completely ineffective or inadequate in managing this degree of deformity. Lindseth RE: Spine deformity in myelomeningocele. Instr Course Lect 1991;40:273-279.
Question 44High Yield
Figures 4a and 4b show the radiographs of a 32-year-old man who has right groin pain with activity or prolonged standing. Which of the following factors would not prohibit consideration of acetabular liner exchange and grafting of the defects?
Explanation
Explanation
4b Polyethylene particles generated as mechanical wear debris can be phagocytized by macrophages and enter a metabolically active state that releases cytokines, causing periprosthetic bone resorption. Significant osteolysis can occur in the pelvis with a porous-coated cementless socket without loosening of the component. If the acetabular component is modular, well positioned, well-designed with a good survivorship record, and remains undamaged after liner removal, the polyethylene liner can be exchanged and the lytic defects can be debrided and bone grafted. This implant is well positioned, has a good survivorship record, a good locking mechanism, and is modular. The hip arthroplasty needs to be aseptic for consideration of liner exchange. Maloney WJ, Herzwurm P, Paprosky W, Rubash HE, Engh CA: Treatment of pelvic osteolysis associated with a stable acetabular component inserted without cement as part of a total hip replacement. J Bone Joint Surg Am 1997;79:1628-1634.
References:
- Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 45High Yield
The majority of severe cervical spine injuries occurring in contact sports evolve during axial loading and flexion of the cervical spine. At what minimum degree of flexion does axial loading place the cervical spine at risk during contact sports?
Explanation
Explanation
The paravertebral musculature, the intervertebral disks, and the normal lordotic curvature of the cervical spine can absorb much of the imparted energy of collision. However, when the neck is flexed approximately 30 degrees, the normal lordotic curvature is flattened and the forces applied to the vertex of the head are directed at a straight segmented column. In this situation, the cervical spine is less able to absorb the applied force. With mounting axial load, compressive deformation occurs within the intervertebral disks, causing angular deformation and buckling. The spine will fail in flexion, with resultant fracture, subluxation, or dislocation. A rotatory component added to axial compression can cause concomitant extension, rotation, and shear injury patterns. The National Football Head and Neck Injury Registry has made two recommendations to the NCAA Football Rules Committee to minimize the risk of such injuries: (1) No player should intentionally strike an opponent with the crown or top of the helmet; and (2) No player should deliberately use his helmet to butt or ram an opponent. Thomas BE, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
References:
- Torg JS, Truex R Jr, Quedenfeld TC, Burstein A, Spealman A, Nichols C III: The National Football Head and Neck Injury Registry: Report and conclusions 1978.
- JAMA 1979;241:1477-1479.
Question 46High Yield
A 58-year-old woman has a fracture through a metacarpal lesion after a motor vehicle accident. She denies any preinjury symptoms and the fracture heals uneventfully. Based on the radiograph and MRI scans shown in Figures 22a through 22c obtained following fracture healing, follow-up management should consist of
Explanation
Explanation
22b 22c Enchondromas are the most common benign skeletal lesions identified in the bones of the hand. Most are incidentally found or initially become clinically evident after a pathologic fracture. If the patient has a fracture, the hand is immobilized until union. If the lesion is large and further pathologic fractures are expected, then an intralesional curettage and grafting procedure may be warranted. In this patient, the lesion has not significantly altered the size, shape, or morphology of the involved metacarpal head and recurrent fracture is unlikely. Observation with follow-up radiographs is considered appropriate management. Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 213-228.
References:
- Marco RA, Gitelis S, Brebach GT, et al: Cartilage tumors: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:292-304.
Question 47High Yield
A 54-year-old man with metastatic renal cell carcinoma has had increasing pain in the left hip for the past 6 weeks. A radiograph is shown in Figure 36. Prophylactic stabilization will most likely result in
Explanation
Explanation
Prophylactic stabilization of impending fractures does not directly affect the overall survival rate, but it does improve factors related to intraoperative and postoperative complications and decreased recovery time. Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
References:
- Harrington KD: Impending pathologic fractures from metastatic malignancy: Evaluation and management. Instr Course Lect 1986;35:357-381.
Question 48High Yield
A 35-year-old man is seen in the emergency department with a bullet wound to the foot that occurred 2 hours ago. Examination reveals a 0.5-cm entrance wound on the dorsum of the foot and a 1.5-cm exit wound on the plantar aspect. Exploration of the plantar wound in the emergency department reveals bone and metal fragments. Radiographs reveal a comminuted, unstable fracture of the base of the first metatarsal and cuneiform. Management should consist of tetanus toxoid, and
Explanation
Explanation
The patient sustained a type I unstable fracture that requires debridement of superficial fragments from the sole and surgical stabilization. Low-velocity wounds less than 8 hours old are considered type I open fractures. In contrast, gunshot wounds with associated fractures more than 8 hours old are considered type II open fractures using the Gustilo and Anderson classification. Gustilo type I stable fractures due to gunshot wounds and seen within 8 hours can be treated with tetanus toxoid (if no history of immunization or booster within 5 years), surface irrigation, and casting or a hard sole shoe. Antibiotics are not required unless gross contamination is present. However, if the extent of contamination is unclear, or if a joint is penetrated, then routine antibiotic prophylaxis is recommended. Indications for surgery include: articular involvement, unstable fractures, presentation 8 or more hours after injury, tendon involvement, and superficial fragments in the palm or sole. Type I unstable fractures may be stabilized with internal or external fixation. Type II unstable fractures should be treated with external fixation and repeat debridements until clean. Holmes GB Jr: Gunshot wounds of the foot. Clin Orthop Relat Res 2003;408:86-91.
References:
- Bartlett CS, Helfet DL, Hausman MR, et al: Ballistics and gunshot wounds: Effects on musculoskeletal tissues. J Am Acad Orthop Surg 2000;8:21-36.
Question 49High Yield
Figure 49 shows a histologic section of the lung in a patient who died during total hip arthroplasty. What unexpected finding is seen in the pulmonary capillaries?
Explanation
Sudden death during total hip arthroplasty has been reported. In a report from the Mayo Clinic, intraoperative death occurred during cemented total hip arthroplasty in 23 patients. Fat and marrow embolization during preparation of the femur or cementing of the femoral component was believed to be responsible for the cardiopulmonary collapse that occurred during arthroplasty. Although fat and marrow emboli were found in the pulmonary capillaries of most of the patients on autopsy, this histologic section shows two particles of cement in the pulmonary capillaries. Parvizi J, Holiday AD, Ereth MH, et al: The Frank Stinchfield Award. Sudden death during primary hip arthroplasty. Clin Orthop 1999;369:39-48.
Question 50High Yield
When an acute infection of a total elbow arthroplasty is managed with irrigation and debridement, which of the following organisms is associated with the highest risk of persistent infection?
Explanation
Explanation
Salvage of a total elbow arthroplasty is possible with early aggressive management of acute infection (symptoms for less than 30 days) with serial irrigation and debridement and antibiotic bead placement. This form of treatment is indicated when there are no radiographic or intraoperative signs of loosening. However, successful treatment is largely dependent on the organism. Staphylococcus epidermidis is associated with persistent infection because it is an encapsulating organism, and it is best treated with implant removal and IV antibiotics. Yamaguchi K, Adams RA, Morrey BF: Infection after total elbow arthroplasty. J Bone Joint Surg Am 1998;80:481-491.
References:
- Schoifet SD, Morrey BF: Treatment of infection after total knee arthroplasty by debridement with retention of the components. J Bone Joint Surg Am 1990;72:1383-1390.
Question 51High Yield
A patient underwent anterior stabilization of the shoulder 6 months ago, and examination now reveals lack of external rotation beyond 0 degrees. The patient has a normal apprehension sign and normal strength, and the radiographs are normal. Based on these findings, the patient is at greater risk for the development of
Explanation
Because the patient's shoulders are overtensioned anteriorly, premature osteoarthritis may develop. This may create obligate translation posteriorly and increase the interarticular pressure of the humeral head against the glenoid. Patients should achieve 20 degrees to 30 degrees of external rotation with the elbow at the side. Late degenerative arthritis following a Putti-Platt procedure is associated with significant restriction of external rotation. This patient's shoulder has a reduced risk of anterior instability, rotator cuff tear, and internal impingement because of the limitation of motion. Hawkins RJ, Angelo RL: Glenohumeral osteoarthritis: A late complication of the Putti-Platt repair. J Bone Joint Surg Am 1990;72:1193-1197.
Question 52High Yield
Figure 53 shows the arteriogram of a 45-year-old man who has severe vasculitis. What do the findings show?
Explanation
Explanation
The arterial supply to the hand is abundant and normally duplicated. The deep palmar arch as shown in this arteriogram typically receives its primary contribution from the radial artery which travels deep to the first dorsal compartment tendons and then returns to the volar aspect of the palm through the first web space. The superficial palmar arch receives its supply from the ulnar artery and is not visualized in this patient.
References:
- Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist: Diagnosis and Operative Treatment. Philadephia, PA, Mosby-Year Book, 1998, p 110.
Question 53High Yield
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
Explanation
Explanation
Subscapularis tears can be associated with disruption of the transverse ligament supporting the biceps. The remaining aspects of the rotator cuff, superior labrum, and capsule can be intact with this injury. Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
References:
- Gerber C, Sebesta A: Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: A preliminary report. J Shoulder Elbow Surg 2000;9:483-490.
Question 54High Yield
A 37-year-old woman has had intermittent paresthesias and numbness in the plantar foot for the past 6 months. She reports that the symptoms are worse with activity, and the paresthesias are beginning to awaken her at night. MRI scans are shown in Figures 6a and 6b. What is the most likely diagnosis?

Explanation
The symptoms are consistent with tarsal tunnel syndrome. Ganglion cysts are a well-known cause of tarsal tunnel syndrome. The MRI scans show a high intensity, well-circumscribed mass in the tarsal tunnel that is consistent with a fluid-filled cyst. Patients usually respond well to excision of the ganglion and resolution of the tarsal tunnel symptoms. The surrounding fat is a different signal intensity on the MRI scans, which rules out a lipoma. Synovial cell sarcoma has a heterogeneous appearance on an MRI scan. Metastatic tumors are most commonly found in the osseous structures of the foot, not the soft tissues. Rozbruch SR, Chang V, Bohne WH, et al: Ganglion cysts of the lower extremity: An analysis of 54 cases and review of the literature. Orthopedics 1998;21:141-148. Llauger J, Palmer J, Monill JM, et al: MR imaging of benign soft-tissue masses of the foot and ankle. Radiographics 1998;18:1481-1498.
Question 55High Yield
In the posterior approach to the proximal radius (proximal Thompson approach), the supinator is exposed through the interval between what two muscles?
Explanation
Explanation
The proximal exposure of the radius is most often used for internal fixation of fractures, resection of tumors, or decompression of the posterior interosseous nerve beneath the supinator muscle. The supinator muscle is exposed through the interval between the extensor carpi radialis brevis and the extensor digitorum comminus muscles. This interval can be more easily palpated further distal in the forearm. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 136-146.
References:
- Tubiana R, McCullough C, Masquelet A: An Atlas of Surgical Exposures of the Upper Extremity. London, UK, JB Lippincott, 1990, pp 137-141.
Question 56High Yield
A 40-year-old man has had hip pain with increased activity over the past year. Examination reveals restriction of motion and tenderness with combined hip flexion, adduction, and internal rotation. An AP radiograph is shown in Figure 34. What is the most likely diagnosis?
Explanation
Explanation
Femoral acetabular impingement (FAI) is a pathologic entity leading to pain, reduced range of motion in flexion and internal rotation, and development of secondary arthritis of the hip. There are two types of FAI: cam impingement and pincher impingement. Cam impingement is seen when a nonspherical femoral head produces a cam effect when the prominent portion to the femoral head rotates into the joint. This mechanism produces shear forces that damage articular cartilage. Radiographs reveal early joint degeneration and flattening of the head neck junction (the so-called "pistol grip deformity") as seen in this image. The pincher type of impingement involves abnormal contact between the femoral head neck junction and the acetabulum, in the presence of a spherical femoral head. Beall DP, Sweet CF, Martin HD, et al: Imaging findings of femoraoacetabular impingement syndrome. Skeletal Radiol 2005;34:691-701.
References:
- Mardones RM, Gonzalez C, Chen Q, et al: Surgical treatment of femoroacetabular impingement: Evaluation of the effect of the size of the resection. J Bone Joint Surg Am 2006;88:84-91.
Question 57High Yield
A 23-year-old woman sustains an injury to her right hand after falling off her snowboard. Examination reveals that she has difficulty moving her fingers. A radiograph and a clinical photograph are shown in Figures 8a and Figure 8b. Management should consist of

Explanation
The radiograph reveals oblique fractures of the third and fourth metacarpals. The rotational component of the fracture displacement is well visualized on the clinical photograph, which shows scissoring of the middle finger over the ring finger. The fracture obliquity results in rotational deformity that cannot be adequately maintained and held by closed treatment. The treatment of choice is open reduction and internal fixation. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771. Freeland AE, Benoist LA, Melancon KP: Parallel miniature screw fixation of spiral and long oblique hand phalangeal fractures. Orthopedics 1994;17:199-200.
Question 58High Yield
A 15-year-old boy who participates in track reports acute pain along the left iliac crest during a sprint. Examination reveals that the anterior superior iliac spine is nontender. The most likely diagnosis is an injury to the
Explanation
Explanation
The patient has iliac apophysitis. The radiographic findings are easily overlooked but usually reveal slight asymmetric widening of the iliac crest apophysis. The apophysis is the most vulnerable structure, as it is three to five times weaker than the tendon. This is not an epiphyseal site, and injury to the muscle or the tendinous insertion to bone (enthesis) is unlikely. Clancy WG Jr, Foltz AS: Iliac apophysitis and stress fractures in adolescent runners. Am J Sports Med 1976;4:214-218. Waters PM, Millis MB: Hip and pelvic injuries in the young athlete, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 279-293. Lombardo SJ, Retting AC, Kerlan RK: Radiographic abnormalities of the iliac apophysis in adolescent athletes. J Bone Joint Surg Am 1983;65:444-446.
References:
- Paletta GA Jr, Andrish JT: Injuries about the hip and pelvis in the young athlete. Clin Sports Med 1995;14:591-628.
Question 59High Yield
Figure 3 shows the AP radiograph of a patient with diabetes mellitus who has knee pain. A semiconstrained knee prosthesis was used in this patient to prevent which of the following complications?
Explanation
The radiographic appearance of the joint is highly suspicious for neuropathic joint (Charcot's joint). Evidence of bone loss on both the tibial and the femoral sides may necessitate the use of metal and/or bone augments. Patients with a neuropathic joint often have excellent range of motion, and postoperative stiffness is not a problem. The main problem with these patients is instability that occurs secondary to ligamentous laxity. Use of a semiconstrained prosthesis prevents the latter complication. Parvizi J, Marrs J, Morrey BF: Total knee arthroplasty for neuropathic (Charcot) joints. Clin Orthop 2003;416:145-150.
Question 60High Yield
Immediately after undergoing lumbar instrumentation, a patient reports severe right leg pain and has 4+/5 weakness. Figure 24 shows an axial CT scan of L5. Exploratory surgery will most likely reveal
Explanation
Explanation
The most common finding at exploration of an inappropriately placed pedicle screw is displacement of the nerve. Pedicle breach is common, ranging from 2% to 20%, but most are asymptomatic. All of the choices are possible, but in a large series conducted by Lonstein and associates, the authors reported that displacement of the root, most often medial, was the most common finding. Laceration, contusion, or transfixion usually was not seen. Spinal fluid leakage occurs less frequently and is not expected in the minimal broach illustrated. Esses SI, Sachs BL, Dreyzin V: Complications associated with the technique of pedicle screw fixation: A selected survey of ABS members. Spine 1993;18:2231-2238. Laine T, Lund T, Ylikoski M, et al: Accuracy of pedicle screw insertion with and without computer assistance: A randomised controlled clinical study in 100 consecutive patients. Eur Spine J 2000;9:235-240.
References:
- Lonstein JE, Denis F, Perra JH, et al: Complications associated with pedicle screws. J Bone Joint Surg Am 1999;81:1519-1528.
Question 61High Yield
In Figure 14, the primary fracture line in a calcaneal fracture is best depicted by which of the following schematics?
Explanation
The schematic labeled A best depicts the primary fracture line in a calcaneal fracture. The primary fracture line in an axial-loading fracture of the calcaneus occurs from superior-lateral to inferior-medial. This fracture line separates the calcaneus into sustentacular and tuberosity fragments and typically enters the subtalar joint through the posterior facet. Although additional fracture lines typically occur, the primary fracture line is almost always present. If surgical reduction is planned, reducing the primary fracture is always a key step. Macey LR, Benirschke SK, Sangeorzan BJ, Hansen ST: Acute calcaneal fractures: Treatment option and results. J Am Acad Orthop Surg 1994;2:36-43.
Question 62High Yield
What is the main function of collagen found within articular cartilage?
Explanation
The main function of collagen in articular cartilage is to provide the tissue's tensile strength. It also immobilizes proteoglycans within the extracellular matrix. Compressive properties are maintained by proteoglycans. Cartilage metabolism is maintained by the indwelling chondrocytes. The flow of water through the tissue promotes transport of nutrients and provides a source of lubricant for the joint. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 3-44.
Question 63High Yield
A patient sustained the injuries shown in the radiographs and clinical photograph seen in Figures 10a through 10c. The neurovascular examination is normal. The first step in emergent management of the extremity injuries should consist of
Explanation
Explanation
10b 10c The figures show an open tibial fracture, a femoral shaft fracture, and femoral head dislocation. The most urgent treatment is reduction of the femoral head, as timing to reduction has been correlated with preventing osteonecrosis. After reduction of the femoral head, the next priority is wound management, followed by stabilization of the femoral and tibial fractures with either splinting, traction, or external fixation. Sahin V, Karakas ES, Aksu S, et al: Traumatic dislocation and fracture-dislocation of the hip: A long-term follow-up study. J Trauma 2003;54:520-529.
References:
- Moed BR, WillsonCarr SE, Watson JT: Results of operative treatment of fractures of the posterior wall of the acetabulum. J Bone Joint Surg Am 2002;84:752-758.
Question 64High Yield
A 42-year-old woman sustained a closed, displaced talar neck fracture in a motor vehicle accident. Which of the following is an avoidable complication of surgical treatment?
Explanation
Malunion of the talus is a devastating complication that leads to malpositioning of the foot and subsequent arthrosis of the subtalar joint complex. This is considered an avoidable complication in that accurate surgical reduction will minimize its development. Posttraumatic arthritis of the subtalar joint, osteonecrosis of the talus, posttraumatic arthritis of the ankle joint, and complex regional pain syndrome all may develop as a result of the initial traumatic event and may not be avoidable despite anatomic reduction. Rockwood and Green's Fractures in Adults, ed 5. Philadelphia, PA, Lippincott, Williams and Wilkins, 2001, pp 2091-2132.
Question 65High Yield
The pathophysiology of a claw toe deformity includes muscular imbalance caused by which of the following relatively strong structures?
Explanation
The dynamic forces acting to maintain the position of the proximal phalanx at the head of the metatarsal are a balance between the extensor digitorum longus and the weaker intrinsic muscles. With hyperextension at the metatarsophalangeal joint, the intrinsic muscles become less efficient as plantar flexors. Consequently, the hyperextension deformity progresses in the metatarsophalangeal joint as the opposition of the intrinsic muscles to the extensor tendon lessens. This is in contrast to the situation in the interphalangeal joints, where the stronger flexors overpower the weaker intrinsic muscles, which act as the extensors. This combination of events leads to hyperextension at the metatarsophalangeal joint and flexion deformities at the interphalangeal joints, resulting in claw toe. Mizel MS, Yodlowski ML: Disorders of the lesser metatarsophalangeal Joints. J Am Acad Orthop Surg 1995;3:166-173.
Question 66High Yield
Figure 17 shows the radiograph of an 11-year-old boy with Duchenne muscular dystrophy who has been nonambulatory for the past 2 years. Management of the spinal deformity should consist of
Explanation
Explanation
The presence of any curve greater than 20 degrees in a nonambulatory patient with Duchenne muscular dystrophy is an indication for posterior fusion with instrumentation. Because of progressive cardiomyopathy and pulmonary deficiency, waiting until the curve is larger can increase the risk of pulmonary or cardiac complications during or following surgery. There is some disagreement as to whether all such fusions must extend to the pelvis. Bracing or other nonsurgical management is ineffective and is not indicated in this situation. Sussman M: Duchenne muscular dystrophy. J Am Acad Orthop Surg 2002;10:138-151.
References:
- Mubarek SJ, Morin WD, Leach J: Spinal fusion in Duchenne muscular dystrophy: Fixation and fusion to the sacropelvis? J Pediatr Orthop 1993;13:752-757.
Question 67High Yield
A 45-year-old woman with a long-standing history of diabetes mellitus has a large draining plantar ulcer of the right foot. Examination reveals some local cellulitis and erythema surrounding the ulcer. A clinical photograph is shown in Figure 7. Based on these findings, what is the most appropriate antibiotic?
Explanation
Combination drugs with activity against both aerobic and anaerobic organisms have been determined to be the best approach. The first-generation cephalosporins do not provide adequate coverage for gram-negative and anaerobic organisms. Gentamicin alone would not provide adequate activity against anaerobes, and there is the risk of renal and auditory toxicity. Pinzur MS, Slovenkai MD, Trepman E: Guidelines for diabetic foot care. Foot Ankle Int 1999;20:695-702.
Question 68High Yield
The bone avulsion shown in Figure 32 has a high correlation with tearing of the
Explanation
Explanation
As described by Segond in 1987, an avulsion fracture of the lateral tibial plateau is commonly referred to as a Segond fracture. Subsequent to 1987, several authors have also found that the lateral capsular sign represents, but is not limited to, a disruption of the middle third of the lateral capsule and a tear of the anterior cruciate ligament. Bach BR, Warren RF: Radiographic indicators of anterior cruciate ligament injury, in Feagin JA (ed): The Crucial Ligaments. New York, NY, Churchill Livingston, 1988, pp 301-327. Segond P: Recherches cliniques et experimentales sur les epanchements sanguins du genou par entorse. Prog Med (Paris) 1987;7:297.
References:
- Johnson LL: Lateral capsular ligament complex: Anatomical and surgical considerations. Am J Sports Med 1979;7:156-160.
Question 69High Yield
Figure 2 shows the radiograph of a 72-year-old woman who reports pain after a fall. History includes several years of increasing thigh pain and limb shortening. Management consisting of an extensive work-up for infection reveals normal laboratory studies, a positive bone scan, and a negative hip aspiration. What is the most likely etiology of this complication?
Explanation
The patient has a midstem periprosthetic fracture, which commonly results in loosening of the prosthesis. Patients who have a large amount of bone loss may require an allograft with the surgical reconstruction. Although the patient reported a fall, her history is also consistent with preexisting loosening of the prosthesis. Chronic infection has been shown in up to 16% of these fractures; however, the patient's work-up revealed no infection. Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242. Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Question 70High Yield
Figures 39a and 39b show the current radiographs of an 8-year-old girl who has had pain in the left thigh for the past 3 months. She was recently diagnosed with hypothyroidism and started treatment 1 week ago. Examination reveals a mild abductor deficiency limp on the left side. She lacks 30 degrees internal rotation on the left hip compared with the right hip. Management should consist of
Explanation
Explanation
39b The radiographs confirm a slipped capital femoral epiphysis of the left hip, as well as a widened growth plate on the contralateral hip. This is considered a stable slip because the patient is able to walk. Treatment options for stable slips include in situ pinning, bone graft epiphysiodesis, and in some centers severe slips are treated with primary osteotomy and epiphyseal fixation. Percutaneous in situ fixation is the most popular and widely used method of treatment. This juvenile patient has an endocrine condition and a widened growth plate on the right side; therefore, strong consideration should be given to pinning the contralateral hip "pre-slip." Muscle strengthening, hip spica casting, and closed reduction have no place in the primary treatment of a stable slipped capital femoral epiphysis. Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140. Loder R, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
References:
- Aronson DD, Carlson WE: Slipped capital femoral epiphysis: A prospective study of fixation with a single screw. J Bone Joint Surg Am 1992;74:810-819.
Question 71High Yield
A 20-year-old woman has lateral foot and ankle pain after sustaining an inversion injury of the ankle while playing soccer 3 months ago. Activity modifications and physical therapy have failed to provide relief. She describes burning pain that extends from the anterior aspect of the ankle to the foot and lateral two toes. The pain is often worse at night. Plain radiographs, a bone scan, and an MRI scan are normal. Stress examination reveals no instability. What is the most likely diagnosis?
Explanation
Explanation
Persistent pain following an ankle sprain can present a diagnostic dilemma. All of the injuries listed should be considered in the differential diagnosis. The superficial peroneal nerve courses in the lateral compartment and exits the crural fascia 12 to 15 cm above the level of the ankle. Muscle herniation through the fascial defect has been reported to be associated with entrapment of this nerve. The fascial hiatus also may serve as a potential tether in cases of inversion injuries causing injury to the superficial peroneal nerve. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
References:
- Baumhauer JF: Superficial peroneal nerve entrapment. Foot Ankle Clin 1998;3:439-446.
Question 72High Yield
Spontaneous recovery of upper extremtiy motor function after a cerebrovascular accident occurs in which of the following predictable patterns?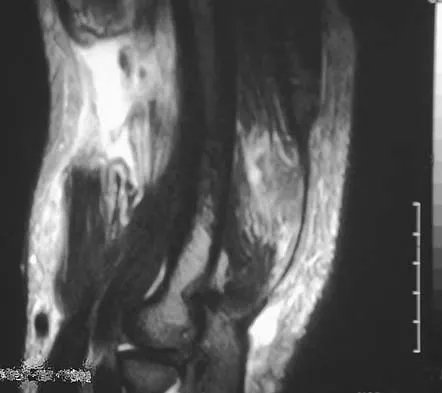
Explanation
Recovery of upper extremity motor function after a cerebrovascular accident follows a predictable pattern. The greatest amount of recovery is seen within the first 6 weeks. Return of function proceeds from proximal to distal. Shoulder flexion occurs first, followed by return of flexion to the elbow, wrist, and fingers. Return of forearm supination follows the return of finger flexion.
Question 73High Yield
Embolic material generated during total knee arthroplasty (TKA) shown in Figure 29 is composed of which of the following substances?
Explanation
Explanation
Emboli are created during TKA. Usually there is an increased incidence with the use of intramedullary rods that disrupt the marrow contents. These are not fat emboli per se. They are material composed of fat cells and marrow that act like pulmonary emboli to obstruct small arterioles in the lung. They are different from free fat emboli that are seen in fractures and that lead to chemical injury to the lung rather than obstructive injury. Markel DC, Femino JE, Farkas P, et al: Analysis of lower extremity embolic material after total knee arthroplasty in a canine model. J Arthroplasty 1999;14:227-232. Pell AC, Christie J, Keating JF, et al: The detection of fat embolism by transoesophageal echocardiography during reamed intramedullary nailing: A study of 24 patients with femoral and tibial fractures. J Bone Joint Surg Br 1993;75:921-925.
References:
- McGrath BJ, Hsia J, Boyd A, et al: Venous embolization after deflation of lower extremity tourniquets. Anesth Analg 1994;78:349-353.
Question 74High Yield
Figure 7 shows the radiograph of an 18-year-old hockey player who sustained a shoulder injury during a fall into the side boards. Examination reveals a significant prominence at the acromioclavicular joint. Management should consist of
Explanation
The radiograph shows a type V acromioclavicular separation with greater than 100% superior elevation of the clavicle. This finding implies detachment of the deltoid and trapezius from the distal clavicle. Because of severe compromise of function and potential compromise to the overlying skin, surgery is the treatment of choice for type V acromioclavicular separations. During reduction and repair, meticulous repair of the deltotrapezial fascia will also aid in securing the repair. Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Question 75High Yield
The dorsal digital cutaneous nerve of the great toe shown in Figure 8 is a branch of what nerve?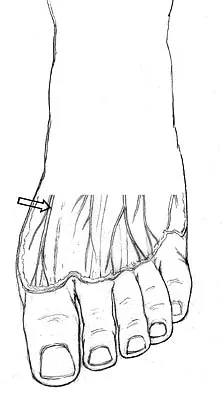
Explanation
The dorsal digital cutaneous nerve of the great toe is a branch of the medial branch of the superficial peroneal nerve. The deep peroneal nerve supplies the first web space. McMinn RMH, Hutchings RT, Logan BM: Color Atlas of Foot and Ankle Anatomy. Weert, Netherlands, Wolfe Medical Publications, 1982, p 50.
Question 76High Yield
Patients with tarsal tunnel syndrome are most likely to obtain a favorable outcome from decompression of the posterior tibial nerve if which of the following conditions is present?
Explanation
Explanation
In one series, only 44% of patients demonstrated good results from tarsal tunnel decompression if they did not have a mass in the tarsal tunnel. Conditions that produce a traction neuropathy of the posterior tibial nerve are unlikely to respond to neurolysis. The most favorable condition associated with a good response to decompression is when a compressing anatomic structure can be removed from the tarsal tunnel. Frey C, Kerr R: Magnetic resonance imaging and the evaluation of tarsal tunnel syndrome. Foot Ankle 1993;14:159-164. Garrett AL: Poliomyelitis, in Nickel VL (ed): Orthopaedic Rehabilitation. New York, NY, Churchill Livingston, 1982, pp 449-458.
References:
- Pfeiffer WH, Cracchiolo A III: Clinical results after tarsal tunnel decompression. J Bone Joint Surg Am 1994;76:1222-1230.
Question 77High Yield
An 11-year-old boy sustained an ankle injury while playing football. Figure 20 shows an AP radiograph obtained the day of injury. Treatment should consist of
Explanation
Explanation
The child has an injury involving both the growth plate and the articular surface of the ankle. Because of the significant displacement, open reduction and internal fixation is indicated to realign the physis and joint surface. The best method of fixation to avoid growth arrest is one that does not cross the physis. This is usually achieved by a transverse epiphyseal screw parallel to the physis. If the metaphyseal fragment was large enough, a transverse metaphyseal screw could be used instead. The incidence of growth arrest following physeal ankle injuries is as high as 50%, and long-term follow-up is indicated. Cass JR, Peterson HA: Salter-Harris Type-IV injuries of the distal tibial epiphyseal growth plate, with emphasis on those involving the medial malleolus. J Bone Joint Surg Am 1983;65:1059-1070.
References:
- Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibia physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-739.
Question 78High Yield
A 19-year-old man who plays college volleyball undergoes a routine preparticipation physical examination. Figure 35 shows a posterior view of his dominant shoulder. An electromyogram shows that this is a chronic injury, and an MRI scan shows no abnormalities. The best course of action should be
Explanation
Explanation
Isolated palsy of the infraspinatus portion of the suprascapular nerve is common in volleyball players and is seen frequently in the throwing arm of baseball players. The exact cause is not known, but it may be the result of either tethering or traction on the nerve at the spinoglenoid notch. Synovial cysts in the spinoglenoid notch also can be a cause, but the patient's negative MRI findings rule out that entity. Because many isolated nerve palsies of the infraspinatus branch are asymptomatic, initial management should always be nonsurgical. Surprisingly, many athletes with this injury can participate fully in sports. Surgical treatment with decompression at the notch is unpredictable and generally is indicated only if nonsurgical management fails. Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
References:
- Martin SD, Warren RF, Martin TL, Kennedy K, O'Brien SJ, Wickiewicz TL: Suprascapular neuropathy: Results of non-operative treatment. J Bone Joint Surg Am 1997;79:1159-1165.
Question 79High Yield
A 52-year-old woman reports the sudden onset of intense pain in the right shoulder. She denies any history of injury or previous shoulder problems. At a 2-week follow-up examination, she notes that the pain has decreased, but she now has severe weakness of the external rotators and abductors. Her cervical spine and remaining shoulder examination are otherwise unremarkable. Radiographs of the shoulder and neck are normal. What is the most likely diagnosis?
Explanation
Explanation
Patients with brachial neuritis or Parsonage-Turner syndrome usually report the sudden onset of intense pain that subsides in 1 to 2 weeks, followed by weakness for a period of up to 1 year in the muscle that is supplied by the involved nerve. Calcific tendinitis usually can be diagnosed radiographically, with calcium deposits seen in the rotator cuff. Bursitis and rotator cuff tendinosis usually are seen after an increase in activity, and both decrease with rest and medication. Glenohumeral arthritis is a slow, progressive problem that results in a loss of range of motion. Misamore GW, Lehman DE: Parsonage-Turner syndrome (acute brachial neuritis). J Bone Joint Surg Am 1996;78:1405-1408.
References:
- Dillin L, Hoaglund FT, Scheck M: Brachial neuritis. J Bone Joint Surg Am 1985;67:878-880.
Question 80High Yield
Which of the following types of exercise used to increase flexibility is considered most beneficial in increasing joint range of motion?
Explanation
Explanation
Evidence has shown that PNF is the treatment of choice to increase joint range of motion and flexibility. PNF has the advantage of pushing the patient to stretch a little further when the muscle tendon unit is relaxed by a partner. While isokinetic and eccentric exercises can improve flexibility, and therefore increase range of motion, their main purpose is to increase strength and endurance. Ballistic stretching involves a large load applied rapidly; however, evidence has shown that static stretching, where a low load is applied for a long duration, offers a more significant benefit. Sady SP, Wortman M, Blanke D: Flexibility training: Ballistic, static or proprioceptive neuromuscular facilitation? Arch Phys Med Rehabil 1982;63:261-263. Tanigawa MC: Comparison of the hold-relax procedure and passive mobilization on increasing muscle length. Phys Ther 1972;52:725-735.
References:
- Wallin D, Ekblom B, Grahn R, Nordenberg T: Improvement of muscle flexibility: A comparison between two techniques. Am J Sports Med 1985;13:263-268.
Question 81High Yield
A 16-year-old boy has had thigh pain for the past several months. He denies any history of trauma. Examination reveals a large, deeply fixed, soft-tissue mass in the thigh. Laboratory results show an elevated erythrocyte sedimentation rate (ESR) and leukocytosis. A plain radiograph and MRI scan are shown in Figures 1a and 1b. Biopsy specimens are shown in Figures 1c and 1d. What is the most likely diagnosis?



Explanation
Ewing's sarcoma typically can occur in the diaphysis of the long bones (50% to 55%). It is often accompanied by a large soft-tissue mass. Abnormal findings are common, including a low-grade fever, an elevated ESR, and leukocytosis. The histology is consistent with a small round blue cell tumor. The unique pathology and other findings exclude osteosarcoma. Giant cell tumor and chondrosarcoma have a different histologic appearance and typically are more metaphyseal in location. Chondrosarcoma typically is found in older age groups, has a different histologic pattern, and rarely occurs in the midshaft of the femur.
Question 82High Yield
A 19-year-old female long-distance runner has an incomplete tension-side femoral neck stress fracture. Management should consist of
Explanation
Explanation
Unlike compression-side stress fractures, tension-side stress fractures on the superior side of the femoral neck are at a very high risk of displacement, even if the patient is not bearing weight. It is highly recommended to treat these fractures like acute fractures and to proceed with internal fixation emergently. Once the fracture has displaced, the prognosis is poor in terms of returning to sports, even when reduced and internally fixed. Nonsurgical management, such as limited weight bearing and low-impact activities, works very well for other lower extremity stress fractures. A training program evaluation (shoes, tracks, schedule) is always indicated for all patients with stress fractures.
References:
- Boden BP, Osbahr DC: High-risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Question 83High Yield
A 42-year-old man reports the recent onset of right hip pain. A radiograph and MRI scan are shown in Figures 38a and 38b. A WBC count, erythrocyte sedimentation rate, and hip aspiration are within normal limits. Management should now consist of
Explanation
Explanation
38b Transient osteoporosis of the hip is an uncommon problem, usually affecting women in the last trimester of pregnancy and middle-aged men. Symptoms include pain in the involved hip with temporary osteopenia; however, there is no joint space involvement. In this patient, the imaging findings are consistent with transient osteoporosis. Short TR/TE (repetition time/echo time) images reveal diffusely decreased signal intensity in the femoral head and intracapsular region of the femoral neck. Increased signal intensity is seen with increased T2-weighting. Within a few months, the pain, as well as the imaging findings, will completely resolve without intervention. Distinguishing the diffuse features of transient osteoporosis of the hip from the segmental findings of osteonecrosis is essential. Unlike transient osteoporosis of the hip, osteonecrosis will have a double-density signal on MRI and may progress radiographically. Surgical intervention and oral corticosteriods are not indicated for treatment. Protected weight bearing until the pain resolves may decrease symptoms while the transient osteoporosis resolves. Potter H, Moran M, Scheider R, et al: Magnetic resonance imaging in diagnosis of transient osteoporosis of the hip. Clin Orthop 1992;280:223-229. Bijl M, van Leeuwen MA, van Rijswijk MH: Transient osteoporosis of the hip: Presentation of typical cases for review of the literature. Clin Exp Rheumatol 1999;17:601-604.
References:
- Montella BJ; Nunley JA, Urbaniak JR: Osteonecrosis of the femoral head associated with pregnancy: A preliminary report. J Bone Joint Surg Am 1999;81:790-798.
Question 84High Yield
Figure 37 shows the clinical photograph of a 1-day-old infant who weighed 10.25 lb at birth. Examination reveals an absent right Moro reflex and limited active motion of the right shoulder, elbow, and wrist, but flexion of the fingers. Passive range of motion of the shoulder and elbow is normal. What is the most likely diagnosis?
Explanation
The patient's right upper extremity is held in the "head waiter's" posture with the shoulder internally rotated, the elbow extended, and the wrist in flexion. The Erb type of obstetrical brachial plexus palsy involves the C5 and C6 nerve root, and occasionally, as in this child, the C7 nerve root. Obstetrical palsy is a traction injury, and is associated with a high birth weight, shoulder dystocia, cephalopelvic disproportion, or the use of forceps. Erb palsy is four times more common than injury to the entire plexus or injury to the C8 and T1 nerve roots. It results from the shoulder being depressed while the head and neck are laterally rotated, extended, and tilted in the opposite direction. Most patients recover wrist extension and elbow flexion. Patients with residual weakness of shoulder external rotation and abduction will benefit from release of the pectoralis major, latissimus dorsi, and teres major, with transfer of the latissimus dorsi and the teres major to the posterosuperior aspect of the rotator cuff. Recent studies using arthrograms and CT scans have shown a higher incidence of posterior glenoid deficiency and posterior subluxation than that observed with plain radiographs. The posterior subluxation or dislocation can be effectively reduced by tendon release and transfer procedures. Hoffer MM, Phipps GJ: Closed reduction and tendon transfer for treatment of dislocation of the glenohumeral joint secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:997-1001. Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:659-667.
Question 85High Yield
The artery located within the substance of the coracoacromial ligament is a branch of what artery?
Explanation
The acromial branch of the thoracoacromial artery courses along the medial aspect of the coracoacromial ligament and may be encountered when performing an open or arthroscopic subacromial decompression. Bleeding can be controlled by ligation of its branch from the thoracoacromial artery. The other arteries may be injured in other surgical exposures of the shoulder. Esch JC, Baker CL: The shoulder and elbow, in Whipple TL (ed): Arthroscopic Surgery. Philadelphia, PA, JB Lippincott, 1993, pp 65-66.
Question 86High Yield
Figure 16 shows the radiograph of a 56-year-old man who has neck pain after a rollover accident on his lawnmower. The injury appears to be isolated, and he is neurologically intact. Management of the fracture should consist of
Explanation
The radiograph shows a type IIa Hangman's fracture, and the classic treatment is halo vest immobilization. Traction should be avoided in type IIa injuries because of the risk of overdistraction. A lesser form of immobilization such as a hard collar or a Minerva jacket can be used for nondisplaced (type I) fractures. Surgery generally is reserved for type III fractures (includes C2-3 facet dislocation), or extenuating circumstances such as multiple trauma or other fractures of the cervical spine that require surgical stabilization. Levine AM, Edwards CC: The management of traumatic spondylolisthesis of the axis. J Bone Joint Surg Am 1985;67:217-226.
Question 87High Yield
A patient undergoes cartilage implantation requiring amplification of donor cells. Which of the following statements best describes the transplants?
Explanation
Chondrocytes are obtained from cartilage harvested from non-weight-bearing areas of the knee. The extracellular matrix is digested, and the chondrocytes are expanded for later transplantation. Cells implanted into a defect are secured with a flap of periosteum. Cells are expanded to obtain 20 to 50 times the original number of cells to transplant at a cell density of 3x10-7 cells/mL. There is a direct relationship between cell number and biosynthetic activity. Osteochondral lesions of up to 8 mm may be treated with autologous transplant alone; larger depth lesions should be bone grafted at the time of harvest. Mesenchymal stem cells differentiate easily into fibrous tissue, bone, and fat; conversion of mesenchymal stem cells into cartilage in vitro currently is difficult to accomplish. Goldberg and Caplan, however, were able to obtain cartilage repair using mesenchymal stem cells transplanted into defects in rabbits in vivo. In animal studies, fluorescent-labeled cells persist for at least 14 weeks, integrate with the surrounding normal margins, and become part of the repaired tissue replete with sulfated proteoglycans and type II collagen. Brittberg M, Peterson L, Sjogren-Jansson E, et al: Articular cartilage engineering with autologous chondrocyte transplantation. J Bone Joint Surg Am 2003;85:109-115.
Question 88High Yield
What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?
Explanation
Of the incomplete spinal cord injuries, Brown-Sequard syndrome has the best prognosis for ambulation. Central cord syndrome has a variable recovery. Anterior cord syndrome has the worst prognosis, with motor recovery rare below the level of the injury. Apple DF: Spinal cord injury rehabilitation, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 1130-1131.
Question 89High Yield
A patient with a below-the-knee amputation is being evaluated for a new prosthesis. He wants to improve his ability to walk on uneven surfaces. What modification to the prosthesis can be made to accommodate this request?
Explanation
Changing from a solid keel to a keel with a sagittal split allows an amputee to navigate uneven terrain more easily. Changing the length of the keel affects the responsiveness of the prosthesis but does not address the surface conditions for ambulation. The SACH is not used as frequently anymore, because overload problems to the nonamputated foot have been observed. Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 31-45.
Question 90High Yield
Titanium and its alloys are unsuitable candidates for which of the following implant applications?
Explanation
Titanium alloy is highly biocompatible, has higher strength than stainless steel, and is highly resistant to corrosion. It is particularly suited for use in fracture plates, bone screws, and intramedullary nails because of its low modulus of elasticity (low stiffness), which can reduce stress shielding. It is also widely used for porous-ingrowth coatings. However, clinical experience has shown that titanium alloy bearing surfaces such as a femoral ball are highly susceptible to severe metallic wear, particularly in the presence of third-body abrasive particles (PMMA fragments, bone chips, metal debris, etc). McKellop HA, Sarmiento A, Schwinn CP, et al: In vivo wear of titanium-alloy hip prostheses. J Bone Joint Surg Am 1990;72:512-517. Salvati EA, Betts F, Doty SB: Particulate metallic debris in cemented total hip arthroplasty. Clin Orthop 1993;293:160-173.
Question 91High Yield
Figures 36a and 36b show the MRI scans of a 15-year-old girl who has had pain and recurrent hemarthrosis in the knee for the past year. Plain radiographs are normal. What is the most likely diagnosis?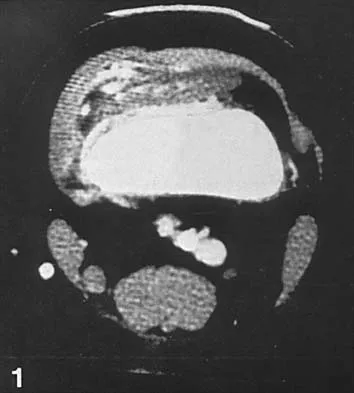
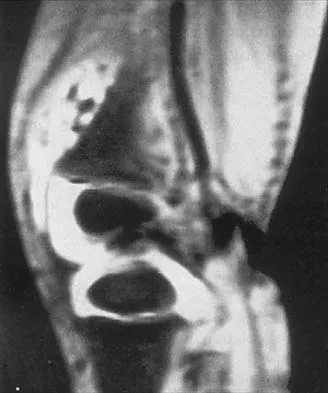
Explanation
In pediatric patients who have pain and recurrent hemarthrosis in the knee, hemangioma is often seen as an internal derangement of the knee, and long delays in diagnosis are common. An MRI scan is noninvasive and will best aid in diagnosis. In this patient, the MRI scan shows a hemangioma with no evidence of meniscal injury or discoid meniscus. Hemophilia is unlikely because the patient is female. The presence of hemarthrosis makes JRA an unlikely diagnosis.
Question 92High Yield
What are the proposed biomechanical advantages of the Grammont reverse total shoulder arthroplasty when compared to a standard shoulder arthroplasty?
Explanation
The Grammont reverse total shoulder arthroplasty is designed to medialize the center of rotation, thereby increasing the deltoid moment arm and lengthening the deltoid. Werner CM, Steinmann PA, Gilbert M: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Question 93High Yield
A 42-year-old woman has cervical stenosis and radicular deficits at the C5-6 and C6-7 levels. History reveals that she has smoked one pack of cigarettes a day for 25 years. Because nonsurgical management has failed to provide relief, she is now seeking surgical treatment. After preoperative counseling, it becomes clear that she is not likely to stop smoking. Which of the following surgical procedures should be used?
Explanation
Explanation
In a review of 190 anterior cervical fusions, Hilibrand and associates reported that only 20 of 40 patients who smoked had solid fusion at all levels, whereas 64 of 91 nonsmokers had solid fusions at all levels when treated with multilevel interbody technique (Smith-Robinson). When fused with strut grafts, 14 of 15 smokers and 41 of 44 nonsmokers had solid fusions with a fusion rate of 93% in the same series. Multilevel allografts have a lower fusion rate than autografts, and diskectomy without fusion has an increased rate of residual neck pain. Hilibrand AS, Fye MA, Emery SE, et al: Impact of smoking on the outcome of anterior cervical arthrodesis with interbody or strut-grafting. J Bone Joint Surg Am 2001;83:668-673.
References:
- Zdeblick TA, Ducker TB: The use of freeze-dried allograft bone for anterior cervical fusions. Spine 1991;16:726-729.
Question 94High Yield
Which of the following best describes athletic pubalgia?
Explanation
Explanation
Athletic pubalgia refers to a distinct syndrome of lower abdominal and adductor pain that is mostly commonly seen in high performance male athletes. This condition must be distinguished from others such as painful inflammation of the symphysis pubis, referred to as osteitis pubis. Symptoms attributable to the iliopsoas tendon are most commonly associated with snapping of the tendon. Stress fracture of the pubic ramus may cause symptoms in this area, but it is usually confirmed by imaging studies. Neurapraxia of the pudendal nerve is associated with pressure from the seat in cycling sports and also as a complication associated with traction during surgical procedures. Meyers WC, Foley DP, Garrett WE, Lohnes JH, Mandlebaum BR: Management of severe lower abdominal or inguinal pain in high-performance athletes: PAIN (Performing Athletes with Abdominal or Inguinal Neuromuscular Pain Study Group). Am J Sports Med 2000;28:2-8.
References:
- Albers SL, Spritzer CE, Garrett WE Jr, Meyers WC: MR findings in athletes with pubalgia. Skeletal Radiol 2001;30:270-277.
Question 95High Yield
What anatomic site is considered at highest risk for pathologic fracture?
Explanation
Explanation
The subtrochanteric femur has been identified as an anatomic site that is particularly prone to pathologic fracture. An avulsion fracture of the lesser trochanter is a sign of impending femoral fracture. While the other anatomic locations are also frequently involved in metastatic bone disease, pathologic fractures occur less commonly. Simon MA, Springfield DS, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 683.
References:
- Harrington KD, Sim FH, Enis JE, Johnston JO, Diok HM, Gristina AG: Methylmethacrylate as an adjunct in internal fixation of pathological fractures: Experience with three hundred and seventy-five cases. J Bone Joint Surg Am 1976;58:1047-1055.
Question 96High Yield
The correct starting point for an external fixation half pin placed into the anterior inferior iliac spine (AIIS) is labeled by what letter in Figure 3?
Explanation
Half pins placed in the AIIS are an alternative to pins placed in the iliac crest. A strong pillar of bone runs from the AIIS to the posterior iliac crest and less soft tissue is typically present in this area. The starting point is best seen on an obturator outlet view. The obturator outlet view is a combination of the pelvic outlet view and the obturator view of Judet and Letournel. The beam is rotated "over the top" of the patient since the iliac wing is externally rotated as well as cephalad to best visualize this column of bone running from the AIIS to the posterior iliac spine. This corridor of bone will appear as a teardrop. Once the correct view is obtained, the pin should be started at least 2 cm proximal to the hip joint to avoid placing a pin within the hip capsule. Blunt dissection and a guide sleeve should be used to prevent damage to the lateral femoral cutaneous nerve. An iliac oblique view is used after the pin has been partially inserted to make sure the pin is passing superior to the superior gluteal notch, and an obturator inlet view can be used at the completion of the procedure to make sure the pin is contained within the bone for its entire length. Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273. Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
Question 97High Yield
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured?
Explanation
The athlete has symptoms referable to the axillary, musculocutaneous, and suprascapular nerves resulting from an injury to the upper trunk of the brachial plexus. This portion of the plexus is formed by contributions of the fourth through sixth cervical nerve roots. This area is often contused or stretched following a tackling maneuver that results in either depression of the shoulder from contact at Erb's point or traction of the upper plexus from forced stretching of the neck to the contralateral side. Schenck CD: Anatomy of the innervation of the upper extremity, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face, ed 2. St Louis, MO, Mosby-Year Book, 1991.
Question 98High Yield
At the level of the midcalf, the plantaris tendon is found at which of the following locations?
Explanation
The plantaris tendon is often harvested to augment a tendon reconstruction. The origin of the plantaris muscle is on the posterolateral aspect of the distal femur, and the muscle lies lateral to the tibial nerve and the posterior tibial artery. The tendon then courses posteriorly between the soleus and the medial head of the gastrocnemius. Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3. Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 475.
Question 99High Yield
What is the most commonly reported complication following elbow arthroscopy?
Explanation
Explanation
The complication rate following elbow arthroscopy is reported at 5%. The most commonly reported complication is transient neurapraxia, with nerve transection remaining an unfortunate and rare event. While infection remains the most common serious complication, it is uncommon (0.8%). Synovial cutaneous fistula and compartment syndrome, while reported, are the least frequent complications of elbow arthroscopy. Kelly EW, Morrey BF, O'Driscoll SW: Complications of elbow arthroscopy. J Bone Joint Surg Am 2001;83:25-34.
References:
- Morrey BF: Elbow complication, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 519-522.
Question 100High Yield
An active 48-year-old woman has had progressive retrocalcaneal pain for the past 2 years. She reports that an injection into the retrocalcaneal bursa 3 weeks ago provided relief, but she now has swelling and weakness after tripping on the stairs 3 days ago. The Thompson test is positive. A radiograph is shown in Figure 36. What is the next most appropriate step in management?
Explanation
Explanation
The patient's long-standing symptoms and radiograph indicate a chronic insertional Achilles tendinopathy that has progressed to complete rupture. This situation is best treated with tendon debridement and repair, often requiring supplementation graft from the flexor hallucis longus. MRI could provide additional information on the quality of the Achilles tendon, but neither MRI nor ultrasound is necessary to make a diagnosis or determine the surgical indication. Conservative management will be unpredictable with a chronic degenerative tendon injury. Myerson MS, McGarvey W: Disorders of the Achilles tendon: Insertion and Achilles tendinitis. Instr Course Lect 1999;48:211-218. Wilcox DK, Bohay DR, Anderson JG: Treatment of chronic Achilles tendon disorders with flexor hallucis longus tendon transfer/augmentation. Foot Ankle Int 2000;21:1004-1010.
References:
- Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 253-277.
You Might Also Like
Previous ChapterOrthopedic Board Review: 100 High-Yield MCQs | Mock Exam Se…
Next Chapter Orthopedic Board Review MCQs: Mock Exam Set #1027 (100 Ques…

Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon