Orthopedic Board Review: 100 ABOS, OITE, FRCS MCQs (Mock Exam Set 1026)
14 Apr 2026
101 min read
97 Views
Key Takeaway
This page offers 100 high-yield orthopedic board review multiple-choice questions (MCQs) to help orthopedic surgeons prepare for ABOS, OITE, and FRCS examinations. Mock Exam Set #1026 covers essential topics, making it an invaluable resource to test your knowledge and master concepts for board success.
Achieve Faster Recovery: Hip Minimally Invasi...
00:00
Start Quiz
Question 1High Yield
Osteophyte formation at the posteromedial olecranon and olecranon articulation in high-caliber throwing athletes is most often the result of underlying
Explanation
Explanation
During the late acceleration phase of throwing, the triceps forcibly contracts, extending the elbow as the ball is released. Normally, this force is absorbed by the anterior capsule and the brachialis and biceps muscles. However, if the ulnar collateral ligament is insufficient, the elbow will be in a subluxated position during extension and cause impaction of the olecranon and the olecranon fossa posteromedially. Over time, osteophyte formation is likely to occur. Conway JE, Jobe FW, Glousman RE, Pink M: Medial instability of the elbow in throwing athletes: Treatment by repair or reconstruction of the ulnar collateral ligament. J Bone Joint Surg Am 1992;74:67-83.
References:
- Wilson FD, Andrews, JR, Blackburn TA, McCluskey G: Valgus extension overload in the pitching elbow. Am J Sports Med 1983;11:83-88.
Question 2High Yield
It is important to avoid which of the following exercises in the immediate postoperative period after humeral head replacement for an acute four-part fracture?
Explanation
Explanation
It is critical to withhold active range of motion of the shoulder within the first 6 weeks after arthroplasty for acute fracture to prevent tuberosity avulsion. When radiographic and clinical findings show that the tuberosities are healed, active motion may be instituted, usually at 6 to 8 weeks. Immediate passive range-of-motion exercises, including external rotation with a stick, pendulum, and passive elevation, should begin within the limits of the repair on the day of surgery to prevent stiffness. Hartstock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humerus fractures. Orthop Clin North Am 1998;29:467-475.
References:
- Hughes M, Neer CS: Glenohumeral joint replacment and postoperative rehabilitation. Phys Ther 1975;55:850-858.
Question 3High Yield
Which of the following findings can cause a dorsal bunion in a patient with neuromuscular disease?
Explanation
Unopposed action of the tibialis anterior with weakness of the peroneus longus will lead to a dorsal bunion and supination deformity. Overpull of the gastrocnemius-soleus complex and posterior tibialis with weakness of the peroneus brevis will cause equinovarus deformity. A strong posterior tibialis with weakness of the peroneals will cause varus of the hindfoot. Unopposed peroneus brevis and incompetence of the posterior tibialis will lead to a flatfoot deformity. The etiology of a cavus foot is complex, but findings usually include a contracted plantar fascia and weakness of the tibialis anterior. Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 289-302.
Question 4High Yield
An obese 4-year-old boy has infantile Blount's disease. Radiographs reveal a metaphyseal-diaphyseal angle of 18 degrees and a depression of the medial proximal tibial physis. Management should consist of
Explanation
Explanation
The deformity is too severe for observation, and at age 4 years, the child is too old for orthotic treatment. To prevent recurrence, surgery should be performed before irreversible changes occur in the medial physis. A proximal tibial osteotomy should overcorrect the mechanical axis to 10 degrees of valgus. Bar resection has not been shown to be as effective in this severe deformity, especially without a concomitant osteotomy. Raney EM, Topoleski TA, Yaghoubian R, Guidera KJ, Marshall JG: Orthotic treatment of infantile tibia vara. J Pediatr Orthop 1998;18:670-674.
References:
- Loder RT, Johnston CE: Infantile tibia vara. J Pediatr Orthop 1987;7:639-646.
Question 5High Yield
During placement of an external fixator for a distal radius fracture, the most commonly injured nerve is a branch of which of the following nerves?
Explanation
Explanation
Pin track infections and sensory injuries are among the most common complications of external fixation for distal radius fractures. The proximal pins of most distal radius external fixators are placed in the "bare area" of the distal radius, about four finger-breadths above the radial styloid. This corresponds to the area where the dorsal sensory branch of the radial nerve penetrates the fascia dorsal to the brachioradialis tendon to become a subcutaneous structure. Injury to the superficial radial nerve may produce painful dysesthesias and neuromas.
References:
- Beldner S, Zlotolow DA, Melone CP, et al: Anatomy of the lateral antebrachial cutaneous and superficial radial nerves in the forearm: A cadaveric and clinical study. J Hand Surg Am 2005;30:1226-1230.
Question 6High Yield
Figures 37a and 37b show the clinical photographs of a 43-year-old patient with type I diabetes mellitus who has a stump ulcer after undergoing successful transtibial amputation 1 year ago. Which of the following is considered the most predictable method of healing the ulcer and preventing recurrent ulceration?
Explanation
Explanation
37b The ulcer occurred as the result of a mismatch between the shape of the residual limb and the prosthetic socket. With the mismatch, the residual limb pistoned and the tissue failed because of the applied shear forces. The most predictable short- and long-term solution is reconstruction of the residual limb. Refraining from use of the prosthesis will prevent the patient from walking for months. It is unlikely that prosthetic socket modification will allow resolution of this large ulcer.
References:
- Hadden W, Marks R, Murdoch G, et al: Wedge resection of amputation stumps: A valuable salvage procedure. J Bone Joint Surg Br 1987;69:306-308.
Question 7High Yield
Figure 36 shows an AP radiograph of a 65-year-old man who reports activity-related groin pain. History reveals that he underwent total hip arthroplasty 12 years ago. What is the most likely diagnosis?
Explanation
Explanation
The AP radiograph demonstrates extensive periacetabular osteolysis. The central hole eliminator has dissociated from the shell and migrated into a lytic defect in the ischium. In a retrieval study, most periacetabular osteolytic lesions had a clear communication pathway with the joint space. Lesions with communication to the joint via several pathways or through a central dome hole (as in this patient) were larger and more likely to be associated with cortical erosion. Although periprosthetic tumors have been described, they are rare and particle-induced inflammation around a prosthesis does not seem to increase the risk for carcinogenesis. Visuri T, Pulkkinen P, Paavolainen P: Malignant tumors at the site of total hip prosthesis: Analytic review of 46 cases. J Arthroplasty 2006;21:311-323. Bezwada HP, Shah AR, Zambito K, et al: Distal femoral allograft reconstruction for massive osteolytic bone loss in revision total knee arthroplasty. J Arthroplasty 2006;21:242-248.
References:
- Kitamura N, Naudie DD, Leung SB, et al: Diagnostic features of pelvic osteolysis on computed tomography: The importance of communication pathways. J Bone Joint Surg Am 2005;87:1542-1550.
Question 8High Yield
When performing knee arthroplasty, which of the following procedures provides the most consistent fixation for the tibial component?
Explanation
Explanation
All of the options, except cementing the metaphyseal portion and press fitting the keel of the tibial component, have been shown to create strong and long-lasting constructs; however, cementing of both the platform and the keel offers the most predictable solution. Cementing the platform and not the keel has been shown to have a higher loosening rate than the more traditional methods of fully cementing or using screws to augment fixation.
References:
- Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 457-468.
Question 9High Yield
Which of the following nerves innervates the muscle that originates from the middle third of the dorsal surface of the lateral border of the scapula, as shown in Figure 7?
Explanation
Explanation
Teres minor originates from the middle third of the dorsal surface of the lateral border of the scapula. It is supplied by the axillary nerve (C5). Williams PL, Warwick R, Dyson M, Bannister LH: Myology, in Gray's Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 611-615.
References:
- Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 68-72.
Question 10High Yield
What is the most important feature in choosing an outcome instrument to assess shoulder disorders?
Explanation
There has been a recent increase in the use of outcome instruments to document and measure effects of treatment of medical conditions, including shoulder disorders. The most important feature of an instrument is whether it actually measures what it purports to measure; this is defined as its validity. Leggin BG, Iannotti JP: Shoulder outcome measurement, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, p 1027.
Question 11High Yield
An 82-year-old man is seen in consultation after being admitted for a fall from ground level. There was no loss of consciousness and the patient recalls striking his head and sustaining a hyperextension-type injury to the cervical spine. Examination reveals an 8-cm head laceration with only mild axial neck tenderness. He has generalized weakness throughout the upper extremities and maintained motor function of the lower extremities. There are no obvious sensory deficits, and the bulbocavernous reflex and deep tendon reflexes are maintained. What is the most appropriate diagnosis at this time?
Explanation
Explanation
Incomplete cord syndromes have variable neurologic findings with partial loss of sensory and/or motor function below the level of injury. Incomplete cord syndromes include the anterior cord syndrome, the Brown-Séquard syndrome, central cord syndrome, and posterior cord syndrome. Central cord syndrome is characterized with greater motor weakness in the upper extremities than in the lower extremities. The pattern of motor weakness shows greater distal involvement in the affected extremity than proximal muscle weakness. Anterior cord syndrome involves a variable loss of motor function and pain and/or temperature sensation, with preservation of proprioception. The Brown-Séquard syndrome involves a relatively greater ipsilateral loss of proprioception and motor function, with contralateral loss of pain and temperature sensation. Posterior cord syndrome is a rare injury and is characterized by preservation of motor function, sense of pain, and light touch, with loss of proprioception and temperature sensation below the level of the lesion. Spinal shock is the period of time, usually 24 hours, after a spinal injury that is characterized by absent reflexes, flaccidity, and loss of sensation below the level of the injury. Penrod LE, Hegde SK, Ditunno JF: Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Arch Phys Med Rehab 1990;71:963-968.
Question 12High Yield
Figure 35 shows the radiograph of a 44-year-old woman with rheumatoid arthritis who reports neck pain. Below what threshold number is surgical stabilization warranted for the interval shown by the arrow?
Explanation
The posterior atlanto-dens interval represents the space available for the spinal cord and a distance of less than 14 mm is predictive of neurologic progression, thus warranting consideration for fusion, even in the absence of symptoms.
Question 13High Yield
A sagittal T1-weighted MRI scan of the knee joint is shown in Figure 23. What structure is identified by the arrow?
Explanation
On T1-weighted images, the posterior cruciate ligament is a low-signal (black) structure that courses from the posterior aspect of the tibia to the medial femoral condyle. The posterior cruciate ligament can appear as arcuate, U-shaped, or kinked. The other structures have similar signal but different anatomic locations. Gross ML, Grover JS, Bassett LW, Seeger LL, Finerman GA: Magnetic resonance imaging of the posterior cruciate ligament: Clinical use to improve diagnostic accuracy. Am J Sports Med 1992;20:732-737.
Question 14High Yield
The injury seen in the CT scan shown in Figure 56 is related to or associated with injury to which of the following structures?
Explanation
Explanation
The right syndesmosis appears disrupted on the CT scan when compared to the normal left side. CT can be helpful in determining injury to the syndesmosis, especially with occult clinical findings. Ebraheim NA, Lu J, Yang H, et al: The fibular incisure of the tibia on CT scan: A cadaver study. Foot Ankle Int 1998;19:318-321. Ebraheim NA, Lu J, Yang H, et al: Radiographic and CT evaluation of tibiofibular syndesmotic diastasis: A cadaver study. Foot Ankle Int 1997;18:693-698.
References:
- Harper MC: Delayed reduction and stabilization of the tibiofibular syndesmosis. Foot Ankle Int 2001;22:15-18.
Question 15High Yield
The cervical disk herniation shown in the MRI scans in Figures 30a and 30b will most likely create which of the following constellations of symptoms?
Explanation
Explanation
30b The MRI scans reveal a right-sided C5-6 herniated nucleus pulposus. A disk herniation in this region encroaches on the C6 root and is accompanied by a sensory change along the thumb and index finger, alterations in the brachioradialis reflex, and possible wrist extension weakness. Although the nerve root associated with the vertebral body passes above the pedicles such that the C6 root passes above the C6 pedicle, it is still the C6 root that is encroached on because the herniation affects the exiting root rather than the traversing root as seen in the lumbar spine. Klein JD, Garfin SR: Clinical evaluation of patients with suspected spine problems, in Frymoyer JW (ed): Adult Spine: Principles and Practice, ed 2. Philadephia, PA, Lippincott-Raven, 1997, pp 319-330.
References:
- Hoppenfeld S: Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-49.
Question 16High Yield
A 50-year-old woman who underwent a joint replacement of the hallux metatarsophalangeal joint 6 months ago now has pain and swelling about the great toe. Radiographs are shown in Figures 39a and 39b. What is the next most appropriate step in management?

Explanation
The radiographs show displacement of the prosthesis, and there has been large amounts of bone resected to insert the implant. Arthrodesis is indicated with interposition bone graft to stabilize the joint and restore length to the first ray.
Scientific References
- :
Question 17High Yield
Following application of a short leg cast, a patient reports a complete foot drop. A compression injury of the peroneal nerve at the fibular neck is confirmed by electrical studies. Which of the following muscles is expected to be the last to recover function during the ensuing months?
Explanation
The recovery process from peroneal nerve palsy may take many months as axonal regrowth occurs. Of the muscles listed, the extensor hallucis is innervated most distally by the peroneal nerve. The flexor digitorum longus is innervated by the tibial nerve.
Question 18High Yield
An otherwise healthy 37-year-old man fell off the flatbed of a delivery truck and landed directly on his dominant left hand. Surgical stabilization of a distal radius fracture is performed. An intraoperative radiograph is shown in Figure 22. What is the next most appropriate step in management?
Explanation
The intraoperative radiograph reveals a scapholunate ligament disruption. Repair of the stout dorsal scapholunate interosseous ligaments is required. Interestingly, the results of scapholunate ligament injuries associated with distal radius fractures appear to be superior to those of isolated ligament injuries. Smith DW, Henry MK: Comprehensive management of soft-tissue injuries associated with distal radius fractures. J ASSH 2002;3:153-164.
Question 19High Yield
An otherwise healthy 45-year-old man has a 3-cm subcutaneous mass on his anterior thigh that is presumed to be a lipoma. Removal of the mass is performed in the office of his primary care physician. Pathologic evaluation shows a high-grade malignant fibrous histiocytoma. Staging reveals no evidence of metastatic disease. Management at this time should consist of
Explanation
Explanation
Resection of a previously excised soft-tissue sarcoma is recommended. Reoperation is recommended after removal of malignant tumors previously believed to be benign, as approximately one half of the patients will have residual tumor in the re-excised specimen. Observation is not indicated in most patients because local recurrence is likely. Radiation therapy alone may result in long-term local control but is felt to be less effective than reoperation. Chemotherapy and radiation therapy alone are not recommended. Wide excision is the most important factor for local disease control. Radiation therapy after surgical re-excision may also decrease the risk of local recurrence. Peabody TD, Monson D, Montag A, Schell MJ, Finn H, Simon MA: A comparison of the prognoses for deep and subcutaneous sarcomas of the extremities. J Bone Joint Surg Am 1994;76:1167-1173. Giuliano AE, Eilber FR: The rationale for planned reoperation after unplanned total excision of soft-tissue sarcomas. J Clin Oncol 1985;3:1344-1348. Lewis JJ, Leung D, Espat J, Woodruff JM, Brennan MF: Effect of resection in extremity soft tissue sarcoma. Ann Surg 2000;231:655-663.
References:
- Noria S, Davis A, Kardel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 20High Yield
Figure 39 shows the AP radiograph of a 62-year-old man with degenerative osteoarthritis secondary to trauma. History reveals that he underwent total elbow arthroplasty 3 years ago. He continues to report instability and constant pain. A complete work-up, including aspiration and cultures, is negative. Treatment should consist of removal of the components and
Explanation
An unconstrained prosthesis dislocation is a disconcerting problem that is not easily resolved; however, revision to a semiconstrained prosthesis would best achieve both pain relief and stability. Removal of the components and distraction arthroplasty or conversion to a resection arthroplasty are options, but the results would be unpredictable with regards to pain relief, postoperative motion, or elbow stability. Arthrodesis is poorly tolerated. With revision to another unconstrained prosthesis, there is the risk of continued redislocation because of chronic ligamentous insufficiency. Linscheid RL: Resurfacing elbow replacement arthroplasty: Rationale, technique and results, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 602-610.
Question 21High Yield
A 52-year-old woman slips in her bathroom and strikes her right hand on a cabinet. She notes swelling, ecchymosis, and pain with attempted motion. There are no open wounds. Radiographs are shown in Figures 5a through 5c. What is the most appropriate treatment?


Explanation
Nondisplaced transverse fractures of the phalanges are stable. Immobilization in the intrinsic plus position will prevent MCP joint stiffness. Displaced oblique fractures are more at risk for instability. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green's Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Question 22High Yield
In a longitudinal study of children with spastic diplegia, analysis of long-term function will most likely reveal
Explanation
In a longitudinal study of 18 patients with spastic diplegia over a period of 32 months, three-dimensional gait analysis revealed a deterioration of gait stability with increases in double support time and decreases in single support time. Kinematic data also identified a loss of excursion about the knee, ankle, and pelvis. Interestingly, the static examination of the children showed a decrease in the popliteal angle over time. The authors concluded that ambulatory ability tends to worsen over time in children with spastic diplegia.
Question 23High Yield
Which of the following is most associated with local recurrence of the lesion seen in the radiograph and MRI scan shown in Figures 27a and 27b?
Explanation
Explanation
27b The lesion is an aneurysmal bone cyst. These lesions are known to have a local recurrence rate of 5% to 50%. Young age, open physes, stage, and type of surgical removal and resulting margin have all been shown to affect the recurrence rate. Chemotherapy is not used in the treatment of aneurysmal bone cysts. Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
References:
- Vergel De Dios AM, Bond JR, Shives TC, et al: Aneurysmal bone cyst: A clinicopathologic study of 238 cases. Cancer 1992;69:2921-2931.
Question 24High Yield
A 19-year-old collegiate baseball player injures the ring finger on his dominant hand while sliding headfirst into second base. He reports that he is unable to actively flex or extend the distal interphalangeal joint of the finger. Radiographs are shown in Figures 19a and 19b. What is the anatomic lesion leading to this injury?
Explanation
Explanation
19b The radiographs reveal a bony avulsion of the flexor profundus insertion (Jersey finger). The large bony fragment classifies this as a Leddy type III injury. The bony fragment has retracted to the level of the annular pulley (A4). Leddy JP, Packer JW: Avulsion of the insertion of the profundus tendon insertion in athletes. J Hand Surg 1977;2:66-69.
Question 25High Yield
The mother of an otherwise healthy 1-month-old infant reports that he is not moving his left leg after falling from his high chair 2 days ago. He has a temperature of 99.5 degrees F (37.5 degrees C). Examination reveals that the left thigh is moderately tender to palpation. Because the infant is apprehensive, range of motion is difficult to quantify, but appears to be normal at the hips and ankles. Range of motion of the left knee is approximately 25 degrees to 90 degrees. A radiograph of the leg is shown in Figure 27. Management should consist of
Explanation
Explanation
The patient has a bucket-handle fracture of the distal femur with bilateral corner fractures of the distal femur and a transverse fracture of the proximal tibia. These fractures are virtually pathognomonic of child abuse. The infant should be admitted to the hospital, and child protection services should be notified for investigation of possible abuse. A skeletal survey should be obtained, along with laboratory studies that include a CBC, a platelet count, a prothrombin time, a partial thromboplastin time, and a bleeding time. Akbarnia BA: The role of the orthopaedic surgeon in child abuse, in Morrissy RT, Weinstein SL (eds): Lovell & Winter's Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1315-1334.
References:
- Black GB: Child abuse fractures, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 931-944.
Question 26High Yield
An otherwise healthy 54-year-old man who underwent a successful multilevel lumbar decompression and fusion 4 years ago now reports increasingly severe bilateral thigh claudication with paresthesia and severe back pain for the past 12 months. Physical therapy, bracing, and epidural steroids have failed to provide relief. A radiograph and MRI scans are shown in Figures 15a through 15c. He is afebrile, and laboratory studies show an erythrocyte sedimentation rate of 5 mm/h and a normal WBC count. What is the best course of action?


Explanation
The patient has degeneration of an adjacent segment with resultant kyphosis and stenosis. Because he is healthy, has responded well to previous surgery, and has a potentially correctable lesion, he is not a good candidate for an end-stage failed back procedure such as a morphine pump. The stenosis is exacerbated by the deformity; therefore, a simple decompression will contribute to instability. Because of the kyphosis and the patient's relatively young age, the treatment of choice is restoration of sagittal alignment and posterior decompression.
Question 27High Yield
Figures 28a through 28d show the radiographs and MRI scans of a 20-year-old basketball player who sustained an inversion injury to his right ankle. Management should consist of
Explanation
Explanation
28b 28c 28d Osteochondral fractures involving the talar dome have been classified based on radiographic and MRI findings. A nondisplaced and incomplete fracture may be treated effectively with a short leg cast and no weight bearing for 6 weeks. This patient has a complete, separated, and displaced osteochondral fragment involving the midlateral talar dome that will most likely cause pain, mechanical symptoms, and effusion if treated nonsurgically. In addition, there is very little bone remaining on the fragment, making the likelihood of healing with open reduction and internal fixation problematic. The treatment of choice includes arthroscopy, removal of the loose fragment, curettage or drilling of the base, and a rehabilitation program that emphasizes peroneal strengthening, range of motion, and proprioceptive training. Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
References:
- Baker CL, Morales RW: Arthroscopic treatment of tranchondral talar dome fractures: A long-term follow-up study. Arthroscopy 1999;15:197-202.
Question 28High Yield
Which of the following medications may have a negative effect on bone healing following fracture?
Explanation
Nonsteroidal anti-inflammatory drugs that are COX-1 primary inhibitors have been shown in animal studies to delay or inhibit fracture healing. COX-2 inhibitors also delay healing but to a lesser extent than COX-1 inhibitors. The other medications listed do not alter fracture callus formation. Gerstenfeld LC, Thiede M, Seibert K, et al: Differential inhibition of fracture healing by non-selective and cyclooxygenase-2 selective non-steroidal anti-inflammatory drugs. J Orthop Res 2003;21:670-675.
Question 29High Yield
What assay most directly assesses gene expression at the posttranslational level?
Explanation
Explanation
Gene expression at the posttranslational level refers to proteins, as opposed to DNA or RNA. The only assay above that targets protein expression directly is the Western blot. Standard PCR is amplification of targeted DNA segments, regardless of whether or not they are actively expressed. Real-time PCR, Northern blot, and microarray expression profile analysis all quantify RNA as a means to determine posttranscriptional gene expression. Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94.
References:
- Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 19-76.
Question 30High Yield
What bilateral surgical intervention is considered inappropriate based on the findings shown in the radiograph in Figure 52?
Explanation
The radiograph reveals osteonecrosis of both femoral heads with reasonably maintained joint surfaces. There may be some slight flattening of the femoral heads. Hip arthrodesis is difficult to perform because of the necrotic bone. Its use in patients with osteonecrotic hips is limited because of the 80% bilaterality; therefore, it is not an acceptable alternative. All the other options are acceptable interventions. Mont MA, Jones LC, Sotereanos DG, et al: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect 2000;49:169-185.
Question 31High Yield
A 25-year-old woman who fell on her outstretched hand reports chronic pain over the hypothenar eminence region and some dorsal ulnar wrist pain. She also notes difficulty playing golf and tennis. Plain radiographs of the hand and wrist are unremarkable. A CT scan is shown in Figure 36. What is the next most appropriate step in management?
Explanation
The CT scan reveals a hook of the hamate nonunion with irregular resorption at the fracture site, which is at the base of the hamate. Symptomatic relief of the pain and discomfort has been well documented after excision of the hook of the hamate. Ultrasound therapy will not provide long-term symptomatic relief or induce nonunion healing. MRI for further soft-tissue evaluation is inappropriate because this is a bony problem; the bony architecture of the wrist is best visualized by CT. Open reduction and internal fixation of the hook of the hamate does not provide the symptomatic relief that is found with excision of the hook of the hamate. In addition, the technical difficulties and relative risk of persistent nonunion after open reduction and internal fixation are not merited when hamate excision can be effected easily and causes no long-term untoward effects. Electrodiagnostic evaluation is inappropriate because there is no history of the persistent numbness and tingling that is found in peripheral compression neuropathies. Stark HH, Chao EK, Zemel NP, Rickard TA, Ashworth CR: Fracture of the hook of the hamate. J Bone Joint Surg Am 1989;71:1206-1207. Failla JM: Hook of hamate vascularity: Vulnerability to osteonecrosis and nonunion. J Hand Surg Am 1993;18:1075-1079. Carter PR, Easton RG, Littler JW: Ununited fracture of the hook of the hamate. J Bone Joint Surg Am 1977;59:583-588.
Question 32High Yield
An otherwise healthy 75-year-old man has a painful mass in the popliteal fossa of his right knee. A lateral radiograph of the knee, a CT scan of the distal femur, and a histopathologic specimen are shown in Figures 13a through 13c. Management should consist of


Explanation
The patient has a parosteal osteosarcoma of the distal femur. The findings of mild knee pain, radiographic evidence of a radiodense mass involving the parosseous space or surface of the distal femur, and histologic findings of a spindle cell lesion forming immature osteoid with little to no necrosis most likely suggest a parosteal osteosarcoma. The treatment of choice is surgical resection. Okada K, Frassica FJ, Sim FH, Beabout JW, Bond JR, Unni KK: Parosteal osteosarcoma: A clinicopathological study. J Bone Joint Surg Am 1994;76:366-378.
Question 33High Yield
A 66-year-old patient with type 1 diabetes mellitus has a deep, nonhealing ulcer under the first metatarsal head and a necrotic tip of the great toe. He has been under the direction of a wound care clinic for 4 months, and has had orthotics and shoe wear changes. What objective findings are indicative of the patient's ability to heal the wound postoperatively?
Explanation
Absolute toe pressures greater than 40 to 50 mm Hg are a good sign of healing potential. An ABI of greater than 0.45 favors healing, but indices greater than 1 are falsely positive due to calcifications in the vessels. Normal albumin is an overall indication of nutritional status. A transcutaneous oxygen level should be greater than 40 mm Hg for healing. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-122.
Question 34High Yield
A 22-year-old professional ballet dancer reports a 3-month history of posterior ankle pain that occurs when she changes from a flat foot to pointe (hyperplantar flexed position). Examination does not elicit the pain with forced passive plantar flexion. A radiograph is shown in Figure 8. What is the most likely cause of the pain?
Explanation
Explanation
The most common causes of posterior ankle pain in ballet dancers are flexor hallucis longus tenosynovitis and os trigonum syndrome. Flexor hallucis longus tenosynovitis differs from a symptomatic os trigonum by the absence of pain with forced plantar flexion and the presence of pain with resisted plantar flexion of the great toe. The pain is often felt in the posterior ankle and can be associated with a snapping or triggering sensation. Os trigonum syndrome commonly occurs in ballet dancers who perform in a position of extreme plantar flexion. The pain occurs from entrapment of the os trigonum between the posterior portion of the talus and calcaneus. Hamilton WG, Geppert MJ, Thompson FM: Pain in the posterior aspect of the ankle in dancers: Differential diagnosis and operative treatment. J Bone Joint Surg Am 1996;78:1491-1500.
References:
- Khan K, Brown J, Way S, et al: Overuse injuries in classical ballet. Sports Med 1995;19:341-357.
Question 35High Yield
A 22-year-old woman reports a 4-year history of worsening low back and left lower extremity pain following a motor vehicle accident. Management consisting of physical therapy, chiropractic manipulation, and interventional pain management, including sacroiliac joint injections and epidural steroid injections, has failed to provide relief. A sagittal T2-weighted MRI scan is shown in Figure 8. No nerve root compression is seen on axial images. She is currently working and lives with her fiancé. She smokes half a pack of cigarettes per day and reports depression on her health history. She is being maintained on narcotic analgesics and is having increasing difficulty performing her activities of daily living secondary to pain. What is the most appropriate management at this time?
Explanation
Explanation
The MRI scan reveals a rudimentary disk at the L5-S1 level, suggesting transitional anatomy. There is a posterior disk bulge at L3-4. At L4-5, there is disk desiccation and loss of disk height, with a posterior disk bulge and a high intensity zone in the posterior annulus, suggesting an annular tear. While these and similar radiographic findings have been associated with the severity of a patient's pain, they are also commonly found in cross-sectional studies of asymptomatic subjects. Carragee and associates found 59% of symptomatic patients undergoing diskography have high intensity zones as compared to 25% of asymptomatic subjects of a similar patient profile. Diskographic injections provoked pain in disks with high intensity zones approximately 70% of the time whether the individual was previously symptomatic or not. This patient's non-specific pain pattern does not require further work-up as she is not a surgical candidate. Carragee EJ, Paragioudakis SJ, Khurana S: 2000 Volvo Award winner in clinical studies: Lumbar high-intensity zone and discography in subjects without low back problems. Spine 2000;25:2987-2992. Pneumaticos SG, Reitman CA, Lindsey RW: Diskography in the evaluation of low back pain. J Am Acad Orthop Surg 2006;14:46-55. Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Question 36High Yield
Figures 21a and 21b show the radiographs of a 12-year-old patient with an L4-level myelomeningocele who has scoliosis that has been slowly progressing for the past several years. There has been no loss of motor function. An MRI scan shows no syringomyelia or increased hydrocephalus. Management should consist of

Explanation
Scoliosis is a common occurrence in children with myelomeningocele, with the incidence increasing as the neurologic level moves cephalad. The rate of pseudarthrosis for isolated anterior or posterior fusions has been reported as high as 75%. The combination of anterior and posterior fusions with some type of instrumentation has been shown to decrease the rate of pseudarthrosis to 20%. Brace treatment in smaller curves can be used as a temporizing measure to delay surgery, but as with idiopathic scoliosis, the brace is ineffective for larger curves. Observation is not indicated with a curve of this magnitude. Ward WT, Wenger DR, Roach JW: Surgical correction of myelomeningocele scoliosis: A critical appraisal of various spinal instrumentation systems. J Pediatr Orthop 1989;9:262-268.
Question 37High Yield
A 20-year-old collegiate football player who sustained blunt head trauma during the first half of a game is emotional and confused. During the halftime intermission, his affect, memory, and disorientation are totally resolved and have returned to preinjury baseline. The only residual finding is a very mild headache. He wants to play the second half. What is the most appropriate course of action?
Explanation
Explanation
There is almost universal acceptance that an athlete may return to play after blunt head trauma only if he or she is totally asymptomatic. Mild residual symptoms are considered an absolute contraindication for return to play. Returning to play after a cardiovascular challenge or sport-specific activities is permitted on the pretext that the athlete is totally asymptomatic prior to these maneuvers. Neuropsychiatric testing is being used more frequently to monitor residual cognitive effects after head trauma. It has not been used as a return to play criterion. Garrick J (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 29-48.
References:
- Guskiewicz KM, McCrea, Marshall SW, et al: Cumulative effects associated with recurrent concussion in collegiate football players: The NCAA Concussion Study. JAMA 2003;290:2549-2555.
Question 38High Yield
A 60-year-old woman reports a painful hip arthroplasty after undergoing surgery 18 months ago. Radiographs show stable cementless implants without signs of ingrowth. Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h. Management should now consist of
Explanation
Explanation
Significant elevation of the erythrocyte sedimentation rate in a patient with a painful hip arthroplasty mandates a complete work-up for infection prior to considering revision surgery. Reproducibility and reliability of ultrasonography as a diagnostic test still needs clarification. Aspiration is the easiest and most cost-effective test and should be performed prior to nuclear imaging. The latter is most valuable if the results are negative, strongly predicting the absence of infection. Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
References:
- McAuley JP, Moreau G: Sepsis: Etiology, prophylaxis, and diagnosis, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 1295-1306.
Question 39High Yield
In addition to pain, which of the following factors are considered most predictive of the risk of pathologic fracture?
Explanation
While guidelines for predicting fracture risk are at best imprecise, the scoring system by Mirels (pain, anatomic location, and pattern of bony destruction) has been shown to be most predictive of fracture risk. Functional pain, peritrochanteric location, and lytic bone destruction are the greatest risk factors for pathologic fracture. The factors of patient weight, age, soft-tissue mass, and location within bone are all of lesser importance. Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Question 40High Yield
A 3-year-old boy sustains a complete paralysis following a high thoracic spinal cord injury consistent with a SCIWORA-type injury (spinal cord injury without radiographic abnormality). Subsequent progressive spinal deformity will develop in what percent of patients with this injury?
Explanation
Explanation
Spinal cord injury in skeletally immature patients almost always leads to the development of paralytic spinal deformity. The age at injury is the most important factor affecting the development of scoliosis. Spinal cord injury that occurs more than 1 year prior to skeletal maturity is almost always followed by the development of scoliosis. In one study, scoliosis developed in 100% of children who were younger than age 10 years at the time of spinal cord injury. Scoliosis can occur after injury at any level. Spasticity is often a contributing factor. Up to two thirds of patients who have paralytic scoliosis prior to skeletal maturity will eventually require surgery for curve control. Mayfield JK, Erkkila JC, Winter RB: Spine deformity subsequent to acquired childhood spinal cord injury. J Bone Joint Surg Am 1981;63:1401-1411. Lancourt JE, Dickson JH, Carter RE: Paralytic spinal deformity following traumatic spinal cord injury in children and adolescents. J Bone Joint Surg Am 1981;63:47-53.
References:
- Dearolf WW III, Betz RR, Vogel LC, Levin J, Clancy M, Steel HH: Scoliosis in pediatric spinal cord injured patients. J Pediatr Orthop 1990;10:214-218.
Question 41High Yield
A 45-year-old woman who recently underwent biopsy of a lymph node in the right posterior cervical triangle now finds it difficult to hold objects overhead and has diffuse aching in the right shoulder region. What is the most likely diagnosis?
Explanation
Explanation
The trapezius is innervated by the spinal accessory nerve. The nerve is superficial in the area of the posterior cervical triangle and is prone to injury during dissection. Paralysis of the trapezius causes loss of scapular stability when forward flexion or abduction of the shoulder is attempted. Vastamaki M, Solonen KA: Accessory nerve injury. Acta Orthop Scand 1984;55:296-299.
References:
- Leffert RD: Neurological Problems, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 2, pp 759-760.
Question 42High Yield
A 35-year-old man who is an avid weight lifter competing in local tournaments reports new onset pain and loss of motion in his dominant right shoulder. Examination reveals joint line tenderness, active elevation to 100 degrees, and external rotation to 10 degrees. His contralateral shoulder reveals 170 degrees forward elevation and 50 degrees external rotation. Radiographs are shown in Figures 46a and 46b. What is the next most appropriate step in management?
Explanation
Explanation
46b New onset pain and stiffness in the young arthritic shoulder is a difficult problem to treat. Initial management should be aimed at reducing pain and improving motion in all planes. This patient's activities and age preclude a shoulder arthroplasty at this time. If nonsurgical management fails to provide relief, then arthroscopic debridement and capsular release may be beneficial. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 257-266.
References:
- Skedros JG, O'Rourke PJ, Zimmerman JM, et al: Alternatives to replacement arthroplasty for glenohumeral arthritis, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 485-499.
Question 43High Yield
A 20-year-old college baseball pitcher reports the insidious onset of medial elbow pain. Examination reveals medial elbow tenderness, a normal neurologic examination, and no obvious valgus laxity. Plain radiographs are normal. MRI scans are shown in Figures 39a and 39b. Management should consist of
Explanation
Explanation
39b Throwers and in particular, pitchers, are prone to high valgus loads to the elbow. A constellation of medial elbow pathology can develop, including medial epicondylitis, ulnar nerve neuritis, medial ulnar collateral ligament injuries, and posteromedial osteophytes of the olecranon. The MRI scans show significant increases in signal intensing as well as fiber disruption of the medial collateral ligament, indicating a complete tear. The common flexor origin shows a homogeneous signal and normal morphology. Therefore, excision of posterior osteophytes and debridement of the common flexor origin are not indicated. Likewise, this patient's symptoms do not indicate ulnar nerve pathology; therefore ulnar nerve transposition is not indicated. Primary repair of medial collateral ligament tears of the elbow lead to unpredictable results with an unacceptable rate of reoperation. The most predictable result in treating this high-demand athlete is reconstruction of the medial collateral ligament with autogenous tissue. Norris TR (ed): Athletic Injuries of the Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 311-323.
References:
- Hyman J, Breazeale NM, Altchek DW: Valgus instability of the elbow in athletes. Clin Sports Med 2001;20:11-24.
Question 44High Yield
A 22-year-old wrestler who underwent an open anterior shoulder reconstruction to repair a dislocated shoulder 6 months ago now reports shoulder pain after attempting a takedown. Examination reveals external rotation that is 15 degrees greater than the contralateral side. He has pain associated with abduction and external rotation but no apprehension. Which of the following tests would most likely reveal positive findings?
Explanation
Postoperative subscapularis detachment can be identified with a positive lift-off test that reveals weakness in internal rotation. This complication does not necessarily compromise the anterior capsule repair. The load-and-sift maneuver and articular contrast studies may be normal. Supraspinatus tests for impingement and weakness should be negative. Gerber C, Krushell RJ: Isolated ruptures of the tendon of the subscapularis muscle: Clinical fractures in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Question 45High Yield
What normal tissue has a low signal intensity (appears black) on both T1- and T2-weighted images?
Explanation
Tendons, cortical bone, ligaments, menisci, and fibrous tissue will show low signal intensity (SI) on both T1- and T2-weighted images. Fat-containing tissues, such as subcutaneous fat and bone marrow, will show high SI on T1-weighted images and low SI on T2-weighted images. Tissues with high water content, such as joint fluid, intervertebral disk, and edema, will show low SI on T1-weighted images and high SI on T2-weighted images. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 65-70.
Question 46High Yield
What is the most common location of osteosarcoma?
Explanation
Explanation
The most common location of osteosarcoma is the knee area (50% to 55%), followed by the proximal humerus and iliac wing. The most commonly involved long bone is the femur (40% to 45%), followed by the tibia (15% to 25%). Within these bones, tumors are typically adjacent to the epiphyses in most patients. The flat bones of the pelvis and spine are less frequently involved. Malawer MM, Sugarbaker PH, Malawer M: Musculoskeletal Cancer Surgery: Treatment of Sarcomas and Allied Diseases. Kluwer Academic Publishers, 2001.
References:
- Wold LA, et al: Osteogenic Sarcoma: Atlas of Orthopedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 47High Yield
A 27-year-old woman reports the acute atraumatic onset of burning pain in her right shoulder followed a week later by significant weakness and the inability to abduct her shoulder. One week prior to this incident she had recovered from a flu-like syndrome. Examination reveals full passive motion of the shoulder and the inability to actively raise the arm. Sensation in the right upper extremity is normal. Cervical spine examination is normal. Radiographs of the shoulder and cervical spine are normal. What is the most likely diagnosis?
Explanation
Explanation
The patient has symptoms and examination findings of acute brachial neuritis which is often a diagnosis of exclusion. The recent viral flu-like symptoms have shown a correlation with the development of this disorder. The acute, severe shoulder weakness excludes calcific tendinitis, impingement, and poliomyelitis. A normal cervical spine examination makes cervical disk disease unlikely. Turner JW, Parsonage MJ: Neuralgic amyotrophy (paralytic brachial neuritis). Lancet 1957;2:209-212.
References:
- Omer GE, Spinner M, Van Beek AL (eds): Management of Peripheral Nerve Problems, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 101-104.
Question 48High Yield
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
Explanation
Explanation
Subscapularis tears can be associated with disruption of the transverse ligament supporting the biceps. The remaining aspects of the rotator cuff, superior labrum, and capsule can be intact with this injury. Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
References:
- Gerber C, Sebesta A: Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: A preliminary report. J Shoulder Elbow Surg 2000;9:483-490.
Question 49High Yield
What is the most common malignant bone tumor seen in patients with multiple hereditary exostosis?
Explanation
Explanation
Secondary chondrosarcomas are most common in patients with multiple hereditary exostosis. Dedifferentiated chondrosarcoma is less common and refers to bone lesions in which a high-grade spindle cell sarcoma component is located immediately adjacent to a low-grade cartilage neoplasm. Mesenchymal chondrosarcoma, clear cell chondrosarcoma, and periosteal osteosarcoma are no more common in patients with multiple hereditary exostosis than in the general population. Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 1660-1669.
References:
- Simon MA, Springfield DS, et al: Common Malignant Bone Tumors: Chondrosarcoma. Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 275-286.
Question 50High Yield
A 53-year-old man reports acute, severe left shoulder pain after undergoing abdominal surgery 10 days ago. Initial management, consisting of anti-inflammatory drugs, physical therapy, and a subacromial injection of corticosteroid, fails to provide relief. Reexamination of the shoulder 2 months after the onset of symptoms reveals atrophy of the infraspinous and supraspinous fossa and profound weakness of active abduction and external rotation. His neck is supple with a full range of motion. Plain radiographs and an MRI scan of the shoulder are normal. What diagnostic study should be performed next in the evaluation of this patient?
Explanation
Explanation
Suprascapular nerve palsy is a fairly uncommon yet well-known cause of shoulder pain and weakness. A variety of causes have been described, including compression by a ganglion cyst, an anomalous or thickened superior transverse scapular ligament, a humeral and scapular fracture, and traction or kinking of the nerve in the suprascapular notch. In this patient, the injury is most likely caused by traction or compression of the nerve in the suprascapular notch as the result of positioning during abdominal surgery; therefore, the studies of choice are electromyography and nerve conduction velocity studies. While MRI of the cervical spine may be of some value in ruling out a radiculopathy, the clinical history does not support such a cause for this condition. Rengachary SS, Neff JP, Singer PA, Brackett CE: Suprascapular entrapment neuropathy: A clinical, anatomical, and comparative study. Part 1: Clinical study. Neurosurgery 1979;5:441-446. Rengachary SS, Burr D, Lucas S, Hassanein KM, Mohn MP, Matzke H: Suprascapular entrapment neuropathy: A clinical, anatomical and comparative study. Part 2: Anatomical study. Neurosurgery 1979;5:447-451.
References:
- Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthoscopy 1990;6:301-305.
Question 51High Yield
The spread of malignant cells to the vertebrae is often through
Explanation
In 1940, Batson described a valveless plexus of veins that extend from the dural venous sinuses of the skull to the sacrum. This system permits retrograde blood flow and enables tumor cells to enter vertebral bodies at multiple levels. Increased intra-abdominal pressure will enhance this retrograde blood flow.
Question 52High Yield
Figure 30 shows the MRI scan of a 68-year-old woman who has left hip pain. What is the most appropriate treatment?
Explanation
The patient has a large zone of osteonecrosis of the left femoral head. The wedge-shaped zone of decreased signal intensity on the T1 image in the subchondral region of the femoral head is typical. Based on these findings, total hip arthroplasty is the most appropriate treatment. Open reduction and internal fixation will not help this condition. Incisional biopsy is indicated only if the MRI scan shows a probable neoplasm. Resection of the proximal femur is indicated only for aggressive malignancy. Arthrodesis may be considered in a younger patient but not in a 68-year-old individual. Other treatments, not listed, such as core decompression, vascularized fibular transplant, and osteotomy may be options in selected patients. Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 213-223.
Question 53High Yield
In overhead athletic activities, the kinetic chain generates what percentage of force from the leg and trunk segments of the chain?
Explanation
Explanation
The leg and trunk provide a stable base for arm motion, supply rotational momentum for force generation, and generate 50% to 55% of the total force and kinetic energy in the tennis serve. Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, p 47. McClure PW, Michener LA, Sennett BJ, et al: Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. J Shoulder Elbow Surg 2001;10:269-277.
References:
- Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part III: The SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation. Arthroscopy 2003;19:641-661.
Question 54High Yield
A patient is treated with volar plating for a distal radius fracture. The CT scan shown in Figure 15 is obtained after union of the fracture because the patient reports ongoing symptoms. The prominent hardware is most likely injuring what tendon?
Explanation
Explanation
Extensor tendon injuries have been reported after volar plating of distal radius fractures. The CT scan shows prominent dorsal hardware a few millimeters ulnar to Lister's tubercle. The second compartment, the ECRL and ECRB, is radial to Lister's tubercle. The ECU runs along the distal ulna. The contents of the fourth dorsal compartment run just ulnar to Lister's tubercle. The EDC tendon is likely irritated in this patient. The EPB runs along the radial border of the radius and is well away from prominent hardware. Benson EC, Decarvalho A, Mikola EA, et al: Two potential causes of EPL rupture after distal radius volar plate fixation. Clin Orthop Relat Res 2006;451:218-222.
References:
- Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist: Diagnosis and Operative Treatment. Philadelphia, PA, Mosby-Year Book, 1998.
Question 55High Yield
A 100-lb 9-year-old boy has a closed midshaft transverse femoral fracture. The oblique fracture is shortened by 3 cm with a 10-degree varus angulation. Surgical management consists of intramedullary, retrograde flexible titanium nailing. To optimize fracture stability, the surgeon should
Explanation
The technique of intramedullary nailing with titanium elastic nails is based on the concept of balanced forces across the fracture site with two equally sized nails. Implantation of the largest sized nails possible, with two equally sized nails, maximizes the stiffness at the fracture site, thereby optimizing fracture alignment and stability. Impacting the nails into the medullary canal can impact the fixation by minimizing distal purchase of the nail at the cortical insertion site. Closed reduction commonly permits bony reduction and passage of the nails; open reduction is reserved for inability to align the fracture. Luhmann SJ, Schootman M, Schoenecker PL, et al: Complications of titanium elastic nails for pediatric femur fractures. J Pediatr Orthop 2003;23:443-447. Lascombes P, Haumont T, Journeau P: Use and abuse of flexible intramedullary nailing in children and adolescents. J Pediatr Orthop 2006;26:827-834.
Question 56High Yield
Figure 23 shows the radiograph of a 55-year-old man who underwent a total hip arthroplasty 5 years ago. Management should now consist of
Explanation
Because the radiograph shows that the femoral stem is loose within the femoral canal and there is a fracture in the distal cement mantle, the stem should be revised. The Ogden-type plate and the allograft bone plates will reconstruct the femur but will not restore stability to the stem. Similarly, traction may allow the femur to heal but will not restore stability to the femoral stem within the femur. Resection arthroplasty is considered a salvage option following failure of the other procedures. Lewallen DG, Berry DJ: Periprosthetic fracture of the femur after total hip arthroplasty: Treatment and results to date, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-249.
Question 57High Yield
A 20-year-old woman has had wrist pain for the past 5 months. A radiograph, MRI scans, and biopsy specimen are shown in Figures 46a through 46d. The patient is then treated with intralesional surgery. The patient should be counseled that her risk of developing lung metastasis is approximately what percent?
Explanation
Explanation
46b 46c 46d Giant cell tumor of bone has about a 2% risk of benign pulmonary metastasis in all cases and 6% risk in recurrent cases. The radiograph and MRI scans show a lytic destructive lesion in the distal radius with no matrix mineralization. The lesion extends up to the subchondral bone. In a young woman, the most likely diagnosis is giant cell tumor of bone, which is supported by the pathology results that show monotonous fibrovascular stroma with numerous multinucleated giant cells where the nuclei that make up the giant cells are identical to the nuclei that make up the background stromal cells. Athanasian EA, Wold LE, Amadio PC: Giant cell tumors of the bones in the hand. J Hand Surg Am 1997;22:91-98.
References:
- Siebenrock KA, Unni KK, Rock MC: Giant-cell tumor of bone metastasizing to the lungs: A long-term follow-up. J Bone Joint Surg Br 1998;80:43-47.
Question 58High Yield
Figure 9 shows the radiograph of a 75-year-old woman who reports the sudden onset of disabling medial knee pain. What is the most likely diagnosis?
Explanation
Explanation
Idiopathic osteonecrosis of the medial femoral condyle occurs predominantly in women older than age 60 years. It is characterized by pain centered in the medial anterior aspect of the knee, and onset is sudden. Flattening, sclerosis, and the radiolucent crescent sign are radiographic indicators of osteonecrosis. The radiographs show no narrowing of the joint space or osteophyte formation to indicate osteoarthritis, and there are no loose bodies to indicate synovial osteochondromatosis. A meniscal tear is not consistent with the radiographic findings shown here. Meniscal tears can coexist with osteonecrosis, but the pain is not eliminated merely by partial meniscectomy. Metastatic lesions to the distal femoral epiphysis are exceedingly rare. Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 413-418.
References:
- Insall JN, Windsor RE, Scott WN, Kelly MA, Aglietti P (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 609-634.
Question 59High Yield
Which of the following types of iliac osteotomy provides the greatest potential for increased coverage?
Explanation
Explanation
The degree of acetabular dysplasia and the age of the child are important considerations when choosing what type of osteotomy to perform. The ability to obtain concentric reduction is a prerequisite of all osteotomies that redirect the acetabulum. Procedures that cut all three pelvic bones allow more displacement and, therefore, correction of acetabular dysplasia. The closer the osteotomy is to the acetabulum, the greater the coverage of the femoral head. Compared with the other acetabular osteotomies, the Ganz periacetabular osteotomy provides the greatest potential for correcting acetabular deficiency because there are no bone or ligamentous restraints to limit correction, but it has the disadvantage of being a technically demanding procedure. The amount of coverage provided by the Salter osteotomy is limited. Millis MB, Poss R, Murphy SB: Osteotomies of the hip in the prevention and treatment of osteoarthritis, in Eilert RE (ed): Instructional Course Lectures XLI. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1992, pp 145-154.
References:
- Weinstein SL: Developmental hip dysplasia and dislocation, in Morrissy RT, Weinstein SL (eds): Lovell & Winter's Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 903-950.
Question 60High Yield
The condition shown in Figures 9a and 9b is most likely the result of

Explanation
The clinical photograph and radiograph show gout, which is the result of urate deposition in the joint and soft tissues. Radiographs frequently reveal periarticular erosions. The crystals are intracellular and negatively birefringent under the polarized microscope. Treatment for acute flares include colchicines, indomethacin, and corticosteroids (including injections). Medications such as allopurinol help prevent recurrent flares. Tophi such as that seen in this patient are often confused with and associated with infection. Wortmann RL, Kelley WM: Crystal-induced inflammation: Gout and hyperuricemia, in Harris ED, Budd RC, Firestein GS, et al (eds): Kelley's Textbook of Rheumatology, ed 7. New York, NY, Elsevier Science, 2005, pp 1402-1429. Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 61High Yield
A 9-year-old boy has a painless enlarged mass on the dorsum of his hand. Figures 14a through 14d show the clinical photograph, radiographs, and biopsy specimen. What is the most likely diagnosis?



Explanation
Multiple hereditary exostosis and enchondroma commonly present as multiple lesions in the hand. Multiple hereditary exostosis consists of cartilage capped bony exostoses arising from the metaphyseal end of rapidly growing bones. Osteosarcoma and chondrosarcoma rarely appear as multiple lesions. Fracture callus can exhibit enchondral ossification that is usually circumferential, but the radiographic findings are not consistent with fracture. Porter DE, Emerton ME, Villanueva-Lopez F, Simpson AH: Clinical and radiographic analysis of osteochondromas and growth disturbance in hereditary multiple exostoses. J Pediatr Orthop 2000;20:246-250.
Question 62High Yield
A 60-year-old patient had the procedure shown in Figure 7 performed 5 years ago. When converting this patient to a total knee arthroplasty (TKA), what patellar problem is commonly encountered intraoperatively?
Explanation
Patella baja is commonly encountered when converting a high tibial osteotomy (HTO) to a TKA. Patella baja most likely occurs because of scarring. Meding and associates' study did not show an increased rate of lateral release when converting a knee that had undergone a previous HTO. Yoshino N, Shinro T: Total knee arthroplasty after failed high tibial osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1265-1271.
Question 63High Yield
Which of the following mechanisms of inhibition has been linked to cigarette smoking and lumbar spinal fusion?
Explanation
Cigarette smoking has been directly linked to pseudarthrosis in spinal fusions. The direct mechanism of action is diminished revascularization of cancellous bone graft. Additionally, a smaller area of revascularization is seen in these grafts, as well as an increased area of necrosis. Increased activity of osteoblasts would result in more bone production. Increased activity of osteocytes would not affect the fusion because osteocytes are mature bone cells.
Question 64High Yield
With the increasing availability of total hip arthroplasty (THA) to younger patients with hip osteoarthritis, there has been increased use of alternative bearing surfaces. Compared to a ceramic-on-ceramic articulation, which of the following is a specific advantage of a metal-on-metal bearing surface?
Explanation
Alternative bearing surfaces in THA have received much attention in recent years as more and more hip arthroplasties are being performed on younger patients with hip arthritis. The two most popular nonmetal-on-polyethylene bearing surfaces are metal-on-metal and ceramic-on-ceramic. There are arguments supporting the use of either, but ceramic bearings have been shown to have a theoretic increased risk of fracture compared with cobalt-chromium. This has been shown to be clinically relevant with zirconium ceramics. Newer alumina ceramics are being produced with lower porosity and grain size and with higher density and purity, resulting in lower fracture risk but still greater than that of cobalt-chromium. Heisel C, Silva M, Schmalzried TP: Bearing surface options for total hip replacement in young patients. Instr Course Lect 2004;53:49-65.
Question 65High Yield
A 58-year-old woman with a history of severe asthma and long-term prednisone use reports a progression of chronic shoulder pain for the past 6 months. Radiographs and MRI scans are shown in Figures 30a through 30d. What is the most likely diagnosis?
Explanation
Explanation
30b 30c 30d The patient has osteonecrosis of the humeral head. The radiographs show increased density in the superior subchondral region of the humeral head. The MRI scans reveal a central collapse of the humeral head. The patient's history of severe asthma and long-term prednisone use predisposes her to this condition. The MRI scans show no evidence of a full- or partial-thickness rotator cuff tear. Without a history of fevers, chills, or other systemic signs or symptoms, there is no indication of septic arthritis. The radiographs do not reveal periarticular erosions, commonly seen in rheumatoid arthritis. Matsen FA III, Rockwood CA Jr, Wirth MA, et al: Glenohumeral arthritis and its management, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 871-874.
References:
- Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Results of replacement. J Shoulder Elbow Surg 2000;9:177-182.
Question 66High Yield
When polyethylene is exposed to radiation and subsequently heated, certain chemical changes occur in the material. Which of the following statements best describes these changes?
Explanation
Explanation
Exposure of polyethylene to radiation and then heating it to quench the free radicals leads to a cross-linked material. It converts a high molecular weight polyethylene macromolecule to an interpenetrating network structure of polymer chains. The ductility of the material is decreased, hence the greater risk of fracture. While the wear rate (measured as fewer and smaller particles) against a smooth counterface is markedly reduced, cross-linked polyethylene has shown a larger increase in wear rate when a rougher counterface is used compared to noncross-linked material. Due to reduced mechanical strength, highly cross-linked polyethylene is less resistant to abrasive wear.
References:
- Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 32-33.
Question 67High Yield
In Figure 49, line AB connects the anterior arch of C1 to the posterior margin of the foramen magnum. Line CD connects the anterior margin of the foramen magnum to the posterior arch of C1. What is the normal ratio of displacement from CD to AB (Power's ratio)?
Explanation
Explanation
The ratio of displacement from CD to AB normally equals 1.0. If the ratio is greater than 1.0, an anterior atlanto-occipital dislocation may exist. Ratios slightly less than 1.0 are normal except in posterior dislocations, fractures of the odontoid process or ring of the atlas, or congenital abnormalities of the foramen magnum. In these conditions, the ratio may approach 0.7. Powers B, Miller MD, Kramer RS, et al: Traumatic anterior atlanto-occipital dislocation. Neurosurgery 1979;4:12-17.
References:
- Clark CR: The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 50-51.
Question 68High Yield
A 15-year-old diver has had persistent, activity-related low back pain for the past 2 months. He denies any history of trauma. Examination reveals that the pain is localized to the lumbosacral junction, and there are no radicular symptoms. The pain is worse with back extension. Neurologic examination is normal, as are AP, lateral, and oblique radiographs of the lumbosacral spine. Further evaluation should include
Explanation
Explanation
Spondylolysis may develop as a stress fracture resulting from repetitive hyperextension during athletic activities. In young people, the pars interarticularis is thin, the neural arch has not yet reached maximum strength, and the intravertebral disk is less resistant to shear. While clinical symptoms may lead to the suspicion of spondylolysis, radiographic confirmation may be difficult in early cases. Plain radiographs may be negative initially, and the plain MRI scan may not offer good visualization of the pars. A bone scan with SPECT is very sensitive initially. CT scans with regular axial and reverse-gantry angled cuts may help determine the type of fracture and the course of treatment. Congeni J, McCulloch J, Swanson K: Lumbar spondylolysis: A study of natural progression in athletes. Am J Sports Med 1997;25:248-253.
References:
- Harvey CJ, Richenberg JL, Saifuddin A, Wolman RL: The radiological investigation of lumbar spondylolysis. Clin Radiol 1998;53:723-728.
Question 69High Yield
A 16-year-old girl was involved in a motorcycle accident that resulted in a significant right tibial fracture with soft-tissue loss over the distal 4 cm of the anterior medial tibia. The patient has had two irrigations and debridements and recently had an intramedullary nail placed for the skeletal injury. Vacuum-assisted closure (VAC) has been used to cover the defect since the injury. The risk of infection developing in the tibia is
Explanation
The risk of infection in a 3B open tibia fracture is most directly related to the timing of the soft-tissue coverage and less related to the size or location of the wound. The wound VAC does not lower or raise the risk of infection in open fractures. It does appear to increase the window of time to obtain coverage without increasing the risk of infection. Additionally, the wound VAC may decrease the probability of needing free tissue coverage. Intramedullary nailing has not been shown to lower the risk of infection in 3B fractures. Godina M: Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78:285-292. Dedmond BT, Kortesis B, Punger K, et al: The use of negative-pressure wound therapy (NPWT) in the temporary treatment of soft-tissue injuries associated with high-energy open tibia shaft fractures. J Orthop Trauma 2007;21:11-17.
Question 70High Yield
A 67-year-old woman has had pain in the area of the metatarsal heads and toes bilaterally for the past 18 months. She describes a diffuse discomfort and a constant burning sensation. She notes that the area feels swollen. Examination reveals that her pulses are normal, and there is no frank swelling or focal tenderness. What is the most likely diagnosis?
Explanation
Explanation
Patients with peripheral neuropathy will often initially see an orthopaedic surgeon and report symptoms of burning, numb, dead, or wooden feet. A simple diagnostic evaluation with a tuning fork (to test vibratory sensibility) or use of the Semmes-Weinstein monofilaments will help make the diagnosis. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-121.
References:
- Gorson KC, Ropper AH: Idiopathic distal small fiber neuropathy. Acta Neurol Scand 1995;92:376-382.
Question 71High Yield
To avoid damage to the ascending branch of the anterior humeral circumflex artery during open reduction and internal fixation of a proximal humeral fracture, the blade plate should be placed in what position?
Explanation
Explanation
The pectoralis major tendon inserts lateral to the biceps tendon, which runs in the bicipital groove. The primary vascular supply of the articular surface of the humeral head is derived from the anterior circumflex humeral artery, which continues into the arcuate artery once it enters the bone. The entry point is on the anterolateral aspect of the humerus just medial to the greater tuberosity within the bicipital groove. To avoid compromising circulation, the blade plate should be placed lateral to the bicipital groove and pectoralis major tendon insertion. Loebenberg M, Plate AM, Zuckerman J: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
References:
- Gerber C, Schneeberger AG: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
Question 72High Yield
A 14-year-old boy has an anteromedial distal thigh mass. A radiograph and MRI scan are shown in Figures 39a and 39b. An open biopsy of the mass should include
Explanation
Biopsy of the soft-tissue component is often diagnostic. Alternatively, in centers with pathologists familiar with bone tumors, needle biopsy is usually successful. The principles of biopsy of bone tumors include avoiding contamination of uninvolved structures and compartments, taking the most direct path to the tumors, making an excisable biopsy tract, and obtaining diagnostic tissue. Transverse biopsy incisions should be avoided because they hinder the definitive surgical procedure. Peabody TD, Simon MA: Making the diagnosis: Keys to a successful biopsy in children with bone and soft-tissue tumors. Orthop Clin North Am 1996;27:453-459. Mankin HJ, Mankin CJ, Simon MA: The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am 1996;78:656-663.
Question 73High Yield
An 18-month-old infant with myelomeningocele and rigid clubfeet has grade 5 quadriceps and hamstring strength, but no muscles are functioning below the knee. What is the best treatment option for the rigid clubfeet?
Explanation
This child has the potential to walk and therefore should have all the contracted structures in the feet released as necessary to place the feet in a plantigrade position for fitting of ankle-foot orthoses. Physical therapy, manipulation, and casting may provide some benefit in a newborn with flexible feet but are not effective in an older infant with rigid clubfeet. Botulinum injections and tendon transfers are of no use because there are no muscles functioning below the knee. Tendon releases are more effective than tendon transfers in children with myelomeningocele. Mazur JM: Management of foot and ankle deformities in the ambulatory child with myelomeningocele, in Sarwark JR, Lubicky JP (eds): Caring for the Child with Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 155-160.
Question 74High Yield
Which of the following antibiotics is contraindicated in children?
Explanation
The tetracycline family of medications can stain teeth and bone in skeletally immature patients and as a result should be avoided in those patients. The remaining antibiotics have no known specific contraindication to use in children.
Question 75High Yield
Examination of a 5-year-old boy with amyoplasia shows a flexion contracture of 70 degrees of the right knee. The active arc of motion is from 70 degrees to 90 degrees, and the opposite knee has a flexion contracture of 10 degrees. Both hips are dislocated with flexion contractures of 10 degrees, passive hip motion is from 10 degrees to 90 degrees of flexion, and the feet are plantigrade and easily braceable. Despite a daily stretching program, the parents and physical therapists note that it is increasingly difficult for him to walk because of the flexion contracture of the right knee. Management of the knee flexion contracture should now include
Explanation
Most children with amyoplasia are ambulatory and when a decrease in function occurs because of a severe contracture, it must be addressed. A radical posterior soft-tissue release, including the posterior knee capsule and often the collateral ligaments and the posterior cruciate ligament, is needed to obtain extension. After the age of 1 year, aggressive physical therapy will do little to correct a contracture. Botulinum toxin A is indicated for spasticity and is contraindicated with severe contractures. Supracondylar femoral extension osteotomy works well, but will remodel at an average rate of 1 degree per month, which is not considered ideal in a young patient. Gradual correction with a circular ring external fixator is an option, but a soft-tissue release will also most likely be needed for a contracture of this severity. Sarwark JF, MacEwen GD, Scott CI Jr: Amyoplasia (a common form of arthrogryposis). J Bone Joint Surg Am 1990;72:465-469. DelBello DA, Watts HG: Distal femoral extension osteotomy for knee flexion contracture in patients with arthrogryposis. J Pediatr Orthop 1996;16:122-126.
Question 76High Yield
The use of elevated rim acetabular liners and long femoral necks may result in
Explanation
Explanation
Elevated rim acetabular liners may improve the anteversion of the acetabular component that, in turn, might improve the stability of the hip replacement through a range of motion. Long femoral necks with skirts will increase the abductor tension and may be necessary to equalize limb lengths. However, either of these measures may increase the likelihood of impingement of the femoral component on the acetabular rim and may lead to dislocation. The restricted range of motion secondary to impingement has been shown to lead to further polyethylene wear that may result in osteolysis. Cobb TK, Morrey BF, Ilstrup DM: The elevated rim acetabular liner in total hip arthroplasty: Relationship to postoperative dislocation. J Bone Joint Surg Am 1996;78:80-86.
References:
- Urquhart AG, D'Lima DD, Venn-Watson E, Colwell CW Jr, Walker RH: Polyethylene wear after total hip arthroplasty: The effect of a modular femoral head with an extended flange-reinforced neck. J Bone Joint Surg Am 1998;80:1641-1647.
Question 77High Yield
Which of the following conditions is transmitted by an autosomal dominant trait?
Explanation
Explanation
Multiple hereditary exostosis is transmitted by an autosomal dominant trait. Li-Fraumeni syndrome and retinoblastoma are autosomal recessive or associated with autosomal recessive mutations. No genetic predisposition to Ollier's disease or Maffucci's syndrome has been identified. Mirra J (ed): Bone Tumors: Clinical, Radiologic and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, p 1627.
References:
- Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 107.
Question 78High Yield
In the preoperative planning of revision acetabular reconstruction, the surgeon should identify significant posterior column deficiency by noting which of the following radiographic features?
Explanation
Proximal and medial migration of the femoral head usually indicates deficiencies of the dome or anterior column. Wear of the polyethylene may result in osteolysis and impingement, which are not indicative of any major bone deficiency. A significant osteolytic lesion in the ischium may represent a major posterior column deficiency that can create a technical challenge during the reconstruction. Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: Acetabular technique. Clin Orthop 1994;298:147-155.
Question 79High Yield
A 24-year-old man sustains an injury to his right elbow after falling 10 feet. Radiographs are shown in Figures 41a and 41b. Treatment should consist of
Explanation
Explanation
41b Transolecranon fracture-dislocations are most effectively managed with open reduction and internal fixation, followed by early aggressive range of motion. Concomitant injury to the collateral ligament is rare, and stability is achieved by anatomic reconstruction of the olecranon fracture with rigid fixation. The need for collateral ligament repair or a hinged external fixator is uncommon in this fracture pattern.
References:
- Ring D, Jupiter JB, Sanders RW, et al: Transolecranon fracture-dislocation of the elbow. J Orthop Trauma 1997;11:545-550.
Question 80High Yield
Figure 11 shows a consecutive sequence of MRI scans obtained in a 12-year-old boy who has had increasing lateral knee pain and catching for the past 6 months. Examination reveals pain localized to the lateral joint line. Range-of-motion testing reveals a 5-degree lack of full extension on the involved side. Plain radiographs and laboratory values are within normal limits. What is the most appropriate management?
Explanation
Discoid menisci are rare causes of lateral knee pain in children. Various etiologies have been proposed, including failure of central absorption of the developing meniscus and hereditary transmission. Patients with discoid menisci have pain, clicking, and locking with a loss of active extension on range-of-motion testing. Classification of discoid menisci according to the Watanabe classification include complete, incomplete, and Wrisberg ligament type. The Wrisberg variant contains an abnormal posterior meniscal attachment. MRI is the diagnostic tool of choice, revealing a thick, flat meniscus generally seen in three consecutive MRI images. Symptomatic knees are often associated with a meniscal tear or degeneration and are managed with arthroscopic partial excision to a more normal shape (saucerization). Vandermeer RD, Cunningham FK: Arthroscopic treatment of the discoid lateral meniscus: Results of long-term follow-up. Arthroscopy 1989;5:101-109.
Question 81High Yield
A 55-year-old man who works as a carpenter reports chronic right anterior shoulder pain and weakness. Examination reveals 90 degrees of external rotation (with the arm at the side) compared to 45 degrees on the left side. His lift-off examination is positive, along with a positive belly press finding. An MRI scan reveals a chronic, retracted atrophied subscapularis tendon. What is the most appropriate management of his shoulder pain and weakness?
Explanation
Chronic subscapularis tendon ruptures preclude primary repair. In such instances, subcoracoid pectoralis major tendon transfers may improve function and diminish pain. The subcoracoid position of the transfer allows redirection of the pectoralis major in a direction recreating the vector of the subscapularis tendon. Shoulder fusion is a salvage procedure, and corticosteroid injection may reduce pain but will not improve function. Jost B, Puskas GJ, Lustenberger A, et al: Outcome of pectoralis major transfer for the treatment of irreparable subscapularis tears. J Bone Joint Surg Am 2003;85:1944-1951.
Question 82High Yield
A healthy 16-year-old boy has had increasing pain in the right knee for the past 3 months. Examination reveals warmth and swelling around the distal femur. Radiographs and an MRI scan are shown in Figures 51a through 51c, and a biopsy specimen is shown in Figure 51d. What is the most likely diagnosis?


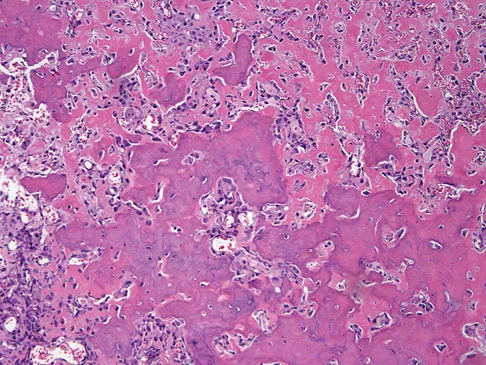
Explanation
The radiographs show a bone-producing lesion in the distal femoral metaphysis in this case of classic osteosarcoma presenting in the most common location, the distal femur. The coronal MRI scan reveals a marrow-occupying lesion with extension into the soft tissues. The histology shows osteoid production by pleomorphic cells consistent with an osteosarcoma. Ewing's sarcoma is a bone tumor characterized by uniform small blue cells on histology. Rhabdomyosarcoma is the most common childhood soft-tissue sarcoma. Osteomyelitis has an inflammatory appearance on histology. Malignant fibrous histiocytoma of bone has a lytic radiographic appearance and a pleomorphic storiform pattern without osteoid on histology. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
Question 83High Yield
A 14-year-old girl with polyarticular juvenile rheumatoid arthritis (JRA) has severe neck pain and reports the onset of urinary incontinence. A lateral radiograph and lateral tomogram of the cervical spine are shown in Figures 15a and 15b. An MRI scan of the upper cervical spine is shown in Figure 15c. Management should consist of
Explanation
Explanation
15b 15c The plain radiograph and tomogram show an abnormality of the upper cervical spine, with erosion of the dens. The MRI scan shows evidence of cord impingement. The cervical spine is frequently involved in polyarticular JRA. Stiffness and autofusion are commonly seen, but C1-2 instability can also occur secondary to synovitis and bony erosion. Basilar invagination is rare in JRA. There is no consensus regarding fusion in the asymptomatic patient. In patients with symptoms and neurologic signs, C1-2 posterior fusion is indicated. Fried JA, Athreya B, Gregg JR, Das M, Doughty R: The cervical spine in juvenile rheumatoid arthritis. Clin Orthop 1983;179:102-106.
References:
- Hensinger RN, DeVito PD, Ragsdale CG: Changes in the cervical spine in juvenile rheumatoid arthritis. J Bone Joint Surg Am 1986;68:189-198.
Question 84High Yield
A 28-year-old man has a painful nodule on the plantar aspect of his foot in the midarch. Use of a soft orthosis has failed to provide relief. Examination reveals that the mass is approximately 2 1/2 cm in diameter, firm, and tender to palpation. An MRI scan confirms the presence of a plantar fibroma. Management should now consist of
Explanation
Plantar fibromas have an extremely high recurrence rate (approximately 60%) with local excision only. Resection of the entire plantar fascia is effective at irradicating the lesion. There is no role for chemotherapy or amputation with plantar fibromatosis. Radiation therapy may be helpful in combination with resection of the plantar fascia. Kirby EJ, Shereff MJ, Lewis MM: Soft-tissue tumors and tumor-like lesions of the foot: An analysis of 83 cases. J Bone Joint Surg Am 1989;71:621-626.
Question 85High Yield
A 7-year-old boy has had chronic left leg pain that is worse at night but is not activity related. Use of nonsteroidal anti-inflammatory drugs for the past 6 months has failed to provide relief. A CBC count with differential, erythrocyte sedimentation rate, and C-reactive protein are within normal limits. Radiographs and a CT scan are shown in Figures 31a through 31c. Management should consist of
Explanation
Explanation
31b 31c Osteoid osteomas are painful bone lesions, with radiographs revealing a dense sclerotic cortex surrounding a small radiolucency or nidus. Symptoms often are worse at night but usually are not activity related. While treatment in the past has consisted of open en bloc excision, current means of removal include percutaneous drilling under CT guidance and percutaneous radiofrequency coagulation. Success rates of percutaneous treatment are comparable to those seen following open procedures. The characteristic radiographic appearance of this lesion usually obviates the need for biopsy. Because the lesion is not caused by pyogenic organisms, antibiotics are not indicated. Donahue F, Ahmad A, Mnaymneh W, Pevsner NH: Osteoid osteoma: Computed tomography guided percutaneous excision. Clin Orthop 1999;366:191-196.
References:
- Rosenthal DI, Hornicek FJ, Wolfe MW, et al: Percutaneous radiofrequency coagulation of osteoid osteoma compared with operative treatment. J Bone Joint Surg Am 1998;80:815-821.
Question 86High Yield
A 2-year-old child has refused to bear weight on his leg for the past 2 days. His parents report that he will crawl, has no fever, and has painless full range of motion of his hip and knee. Examination reveals no deformity or bruising, but there is mild swelling and tenderness over the anterior tibia. C-reactive protein, WBC count, and erythrocyte sedimentation rate studies are normal. Radiographs are negative. What is the best course of action?
Explanation
Explanation
Despite the negative radiographic findings, the child's age and presentation are most consistent with a toddler's fracture. There is often not a witnessed injury. The differential diagnosis of infection is unlikely given that the child is afebrile and shows no signs of illness. Immobilization will make the child more comfortable and will often allow weight bearing. Repeat radiographs at the end of treatment will show a healing fracture and confirm the diagnosis. Aspiration of the tibial metaphysis would be indicated to obtain material for culture. The bone scan and MRI would show abnormalities, but these studies are nonspecific, costly, and time-consuming. Occasionally, oblique radiographs will show the fracture. Halsey MF, Finzel KC, Carrion WV, Haralabatos SS, et al: Toddler's fracture: Presumptive diagnosis and treatment. J Pediatr Orthop 2001;21:152-156.
References:
- Oudjihane K, Newman B, Oh KS, et al: Occult fractures in preschool children. Trauma 1988;28:858-860.
Question 87High Yield
A 28-year-old hockey player has a shoulder deformity after being checked into the boards. Examination reveals that swelling has improved, but there is tenderness along the distal clavicle. Radiographs reveal a grade II acromioclavicular joint separation. Initial management should consist of
Explanation
The most common shoulder injury in hockey players is to the acromioclavicular joint. Early rest and control of pain and inflammation is the preferred management. Surgery is reserved for patients with significant coracoclavicular disruption that has failed to respond to nonsurgical management. Cross-chest stretches and overhead exercises may increase symptoms. A cortisone injection within the glenohumeral joint will have little effect. Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Question 88High Yield
An 18-year-old man sustains an injury to his lateral ankle after being kicked while playing soccer. He reports persistent pain on the lateral ankle as well as a popping sensation with attempted ankle dorsiflexion and eversion. Which of the following structures anatomically restrains the retracted structure shown in Figure 12?
Explanation
The peroneus brevis and peroneus longus muscles are the main evertors of the hindfoot. As they descend along the posterior fibula, they pass through the retromalleolar sulcus, formed by the concavity of the retromalleolar fibula. This sulcus is deepened by a fibrocartilaginous rim. The superior peroneal retinaculum covers the fibular groove and stabilizes the peroneal tendons within the retromalleolar sulcus. It originates from the posterolateral ridge of the fibula and inserts onto the lateral calcaneus. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 81-89.
Question 89High Yield
In addition to the radiographic features seen in Figures 49a and 49b, this patient will most likely have which of the following findings?
Explanation
Explanation
49b The radiographs show the characteristic features of osteopetrosis. The condition results from defective resorption of immature bone by osteoclasts. There are three distinct clinical forms: (1) infantile-malignant, which is autosomal recessive and fatal in the first few years of life if untreated; (2) intermediate autosomal recessive; and (3) autosomal dominant. These conditions do not follow a malignant course, and patients have normal life expectancy with orthopaedic problems and anemia. In the malignant form, the clinical features include frequent fractures, macrocephaly, progressive deafness and blindness, hepatosplenomegaly, and severe anemia beginning in early infancy or in utero. Deafness and blindness are generally thought to represent effects of pressure on nerves and usually occur later in life. The anemia is caused by encroachment of bone on marrow, resulting in obliteration, and the hepatosplenomegaly is caused by compensatory extramedullary hematopoiesis. Dental caries and abscesses, as well as osteomyelitis of the mandible, are also seen. Most patients have normal intelligence. Treatment of the malignant form includes high dose 1,25 dihydroxy vitamin D with a low-calcium diet to stimulate bone resorption, not because there are vitamin deficiencies. Bone marrow transplant has also been successful. Herring JA: Tachdjian's Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, p 1550. Zaleske DJ: Metabolic and endocrine abnormalities, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 212-214.
References:
- Kaplan FS, August CS, Fallon MD, et al: Successful treatment of infantile malignant osteopetrosis by bone-marrow transplantation: A case report. J Bone Joint Surg Am 1988;70:617-623.
Question 90High Yield
Removal of both hallucal sesamoids should be reserved as a salvage procedure because of the high incidence of which of the following postoperative complications?
Explanation
Removal of both sesamoids is associated with a high incidence of postoperative hallux valgus and cock-up deformity of the great toe because of weakening of the flexor hallucis brevis tendon. The sesamoids lie within these tendons and require meticulous repair following excision. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 17-25.
Question 91High Yield
Which of the following is considered the most important factor in eliminating infection in chronic osteomyelitis?
Explanation
Explanation
The most important factor in eliminating infection in chronic osteomyelitis is a complete debridement of the compromised bone and soft tissue. Antibiotics should be used in conjunction with surgical debridement. However, the foundation of treating infected bone is removal of the diseased tissue. Cierny G III, Cook WG, Mader JT: Ankle arthrodesis in the presence of ongoing sepsis: Indications, methods, and results. Orthop Clin North Am 1989;20:709-721. Cierny G, Zorn EZ: Arthrodesis of the tibiotalar joint for sepsis. Foot Ankle Clin 1996;1:177-197.
References:
- Richter D, Hahn MP, Laun RA, Ekkernkamp A, Muhr G, Osterman PA: Arthrodesis of the infected ankle and subtalar joint: Technique, indications and results of 45 consecutive cases. J Trauma 1999;47:1072-1078.
Question 92High Yield
A 22-year-old volleyball player has atrophy of the infraspinatus muscle. This deficit is the result of entrapment of what nerve?
Explanation
Suprascapular deficits, as the result of repetitive forceful internal rotation with overhead ball striking, occur in the spinoglenoid notch. Compression interferes with distal suprascapular nerve innervation to the infraspinatus, while allowing the supraspinatus to function normally. A scapular notch entrapment of this nerve would involve both the supraspinatus and the infraspinatus. The axillary, dorsal scapular, and subscapular nerves do not affect the infraspinatus. Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Question 93High Yield
A 13-year-old boy is comatose and has irregular breathing after being struck by a car while riding his bicycle. Auscultation suggests a pneumothorax on the right side and swelling about the right arm and leg. Initial management should consist of
Explanation
Explanation
The first priority is to gain control of the airway with intubation. Following intubation, management should consist of ventilation and placement of a chest tube if needed, vascular access and circulatory stabilization, radiographs of the cervical spine and chest, and CT of the brain. American College of Surgeons Committee on Trauma. Advanced Trauma Life Support Course. Instructor's Manual. Chicago, IL, American College of Surgeons, 1984.
References:
- Eichelberger MR, Randolph JG: Pediatric trauma: An algorithm for diagnosis and therapy. J Trauma 1983;23:91-97.
Question 94High Yield
A 28-year-old man has had a 2-year history of progressive lateral ankle pain. History reveals that he underwent a triple arthrodesis at age 13 for a tarsal coalition. The pain has been refractory to braces, custom inserts, and nonsteroidal anti-inflammatory drugs. Weight-bearing radiographs of the ankle and foot are shown in Figures 3a through 3d. Surgical management should include which of the following?



Explanation
The patient has a valgus-supination triple arthrodesis malunion. Weight-bearing radiographs show excessive residual valgus through the subtalar joint, producing lateral subfibular impingement, and residual forefoot abduction and midfoot supination through the talonavicular joint, lateralizing the weight-bearing forces through the foot. The deformity is best managed with a medial displacement calcaneal osteotomy and transverse tarsal derotational osteotomy. Ankle arthroscopy and lateral ligament reconstruction are indicated in the event of ligament instability. Tendon transfer, lateral column lengthening, and heel cord lengthening are used for treatment of adult flatfoot from posterior tibial tendon insufficiency. Ankle arthrodesis and ankle arthroplasty are not indicated in this patient because the lateral ankle symptoms are the result of the underlying deformity in the hindfoot, the patient is young, and the ankle joint is relatively normal. Haddad SL, Myerson MS, Pell RF IV: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
Question 95High Yield
Which of the following is considered the best method for the prevention of wrong-site surgery?
Explanation
Explanation
The best method of preventing wrong-site surgery is for the surgeon to initial the surgical site in the preoperative holding area after discussion and confirmation of the site with the patient. This should be done before sedating medications are administered. A recent study found that patient noncompliance with specific preoperative instructions to mark the site with a "yes" at home was surprisingly high; only 59% of the patients marked the extremity correctly and 37% made no mark. Noncompliance was higher in those with workers' compensation claims (70%) and those with previous related surgery (51%). DeGiovanni CW, Kang L, Manuel J: Patient compliance in avoiding wrong site surgery. J Bone Joint Surg Am 2003;85:815-819.
References:
- American Academy of Orthopaedic Surgeons. Advisory Statement: Wrong-site Surgery. Document 1015, 2002 Sept. www.aaos.org/wordhtml/papers/advismt/wrong.htm.
Question 96High Yield
Figure 25 shows an arthroscopic thermal capsular shrinkage device being used in the anterior inferior quadrant of a patient with a subluxating shoulder. Which of the following neurologic complications is most frequently reported with this technique?
Explanation
The axillary nerve lies within millimeters of the anterior inferior capsule. The inferior capsule is of varying thickness, and thermal energy used in shortening the ligament can cause damage to the sensory fibers of the axillary nerve. Clinically, this is manifested as a burnt skin sensation in the axillary nerve distribution area. The motor branch of the axillary nerve is usually spared. The suprascapular nerve and the radial nerve are far from the shrinkage zone. The musculocutaneous nerve, frequently at risk with open procedures, lies well anterior. Fanton GS: Arthroscopic electrothermal surgery of the shoulder. Op Tech Sports Med 1998;6:157-160.
Question 97High Yield
A 41-year-old man who plays golf regularly has had ulnar-sided wrist pain for the past several days after striking a tree root with a golf club. Examination reveals significant pain with resisted flexion of the ring and small fingers and tenderness over the hook of the hamate. Which of the following radiographic views would be most helpful in identifying the pathology of this injury?
Explanation
The history and examination findings suggest an acute fracture of the hook of the hamate. The radiographic study considered most helpful in identifying this type of fracture is the carpal tunnel view. PA and lateral views of the wrist will not adequately visualize the hook of the hamate. Bruerton's view is intended for the assessment of the metacarpophalangeal joints. Pathology would not be suspected in the scaphoid, metacarpals, or the phalanges, so the scaphoid view and the PA, lateral, and oblique views of the hand would not be helpful. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, p 855.
Question 98High Yield
A patient who has recalcitrant medial plantar heel pain and pain directly over the medial side of the heel undergoes open release of the plantar fascia. After releasing a portion of the plantar fascia, the deep fascia of the abductor hallucis muscle is released to relieve pressure on which of the following structures?
Explanation
Explanation
The deep fascia of the abductor hallucis muscle is released to relieve pressure on the first branch of the lateral plantar nerve. The tibial nerve lies more proximal to this area. The medial plantar nerve has already passed dorsally and medially, while the sural nerve lies on the lateral side of the foot. The flexor hallucis brevis muscle lies deep to the plantar fascia, not the abductor fascia. Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop 1992;279:229-236.
References:
- Davies MS, Weiss GA, Saxby TS: Plantar fasciitis: How successful is surgical intervention? Foot Ankle Int 1999;20:803-807.
Question 99High Yield
A 61-year-old woman has increasing pain in her left great toe. She states that she has had discomfort for years but now has pain with all shoe wear. A radiograph is shown in Figure 35. To provide the most predictable pain-free result, treatment should consist of
Explanation
Because the patient has a hallux valgus with increased intermetatarsal and hallux valgus angles and advanced degenerative arthritis of the joint, arthrodesis of the first metatarsophalangeal joint will provide the most predictable pain-free result. An attempt to correct the bunion with a bunionectomy or osteotomy would most likely fail. The hallux valgus and advanced degenerative changes put the foot beyond the indications for a cheilectomy. Long-term results with silicone arthroplasty have been disappointing. Mann RA: Disorders of the first metatarsophalangeal joint. J Am Acad Orthop Surg 1995;3:34-43.
Question 100High Yield
A 70-year-old former baseball catcher reports long-standing pain in the ring and little fingers. A gradient-echo MRI scan is shown in Figure 26. What is the most likely diagnosis?
Explanation
Explanation
The gradient-echo MRI scan highlights the ulnar and radial arteries, as indicated by the arrow. This technique suppresses the signal of the surrounding fat and causes the stationary surrounding tissues to become intermediate in signal intensity. The flowing blood is then easily identified with a bright signal because it does not absorb the radiofrequency pulse. Based on the findings, the diagnosis is an ulnar artery aneurysm, most likely caused by years of repetitive trauma as the result of catching baseballs. Neurolemmoma and giant cell tumor of the tendon sheath would be intermediately enhanced on this image sequence, and the continuity with the ulnar artery, demonstrated here, would not be expected. Lipomas are not enhanced using the gradient-echo technique. The chronic nature of the patient's symptoms is not indicative of a hematoma, and the hematoma would be dark on this imaging sequence since it is stationary tissue. Koman LA, Ruch DS, Patterson Smith B, et al: Vascular disorders, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 2, pp 2254-2302.
References:
- Holder LE, Merine DS, Yang A: Nuclear medicine, contrast angiography, and magnetic resonance imaging for evaluating vascular problems in the Hand: Vasospastic disorders. Hand Clin 1993;9:95-113.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon