Orthopedic Board Review: Mock Exam Set #958 - 100 High-Yield MCQs
14 Apr 2026
107 min read
82 Views
Key Takeaway
This page offers 100 high-yield orthopedic board review questions (Mock Exam Set #958) specifically designed to help orthopedic surgeons prepare for ABOS, OITE, and FRCS board exams. Master key concepts, test your knowledge, and boost your confidence.
Posterolateral Approach to the Thoracic Spine...
00:00
Start Quiz
Question 1High Yield
A 45-year-old woman has idiopathic scoliosis. Surgery is to include an anterior thoracic release through an open left thoracotomy. The thoracotomy will have what effect on the patient's pulmonary function postoperatively?
Explanation
Explanation
A thoracotomy in an adult with idiopathic scoliosis causes a reduction in pulmonary function that often does not return to preoperative levels. What pulmonary function that does recover, recovers over many months. Long-term improvement in pulmonary function, compared to preoperative function, is rarely seen. This should be considered in planning surgical intervention in adults with scoliosis. Graham EJ, Lenke LG, Lowe TG, et al: Prospective pulmonary function evaluation following open thoracotomy for anterior spinal fusion in adolescent idiopathic scoliosis. Spine 2000;25:2319-2325.
Question 2High Yield
A 63-year-old woman reports giving way of the knee and pain after undergoing primary total knee arthroplasty (TKA) 1 year ago. Examination reveals that the knee is stable in full extension but has gross anteroposterior instability at 90 degrees of flexion. The patient can fully extend her knee with normal quadriceps strength. Studies for infection are negative. AP and lateral radiographs are shown in Figures 12a and 12b, respectively. What is the appropriate management?
Explanation
Explanation
12b The radiographs show posterior flexion instability that is the result of a flexion-extension gap imbalance and posterior cruciate ligament incompetence after a posterior cruciate ligament-retaining TKA. The femur is anteriorly displaced on the tibia, with lift-off of the femoral component from the tibial polyethylene. Revision to a larger femoral component will address the larger flexion gap relative to the extension gap, and a posterior stabilized implant will address the posterior cruciate ligament insufficiency. Pagnano and associates, reporting on a series of painful TKAs previously diagnosed as pain of unknown etiology, showed that the pain was secondary to flexion instability. Pain relief was achieved by revision to a posterior stabilized implant. Pagnano MW, Hanssen AD, Lewallen DG, et al: Flexion instability after primary posterior cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46. Fehring TK, Valadie AL: Knee instability after total knee arthroplasty. Clin Orthop 1994;299:157-162.
References:
- Fehring TK, Odum S, Griffin WL, et al: Early failures in total knee arthroplasty. Clin Orthop 2001;392:315-318.
Question 3High Yield
When comparing the failure load of an evenly tensioned four-stranded hamstring tendon anterior cruciate ligament autograft to a 10-mm bone-patellar tendon-bone autograft, the hamstring graft will fail at a tension
Explanation
The failure load of an evenly tensioned four-stranded hamstring tendon autograft has been reported to be 4,500 Newtons. The failure load of a 10-mm patellar tendon autograft has been estimated at 2,600 Newtons. The intact anterior cruciate ligament failure load has been calculated at 1,725 Newtons. Corry IS, Webb JM, Clingeleffer AJ, Pinczewski LA: Arthroscopic reconstruction of the anterior cruciate ligament: A comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am J Sports Med 1999;27:448-454. Hamner DL, Brown CH Jr, Steiner ME, et al: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557.
Question 4High Yield
A 52-year-old woman reports mild pain localized to the left sternoclavicular joint. History is notable for chronic renal failure requiring dialysis for the last 5 years. A clinical photograph, chest radiograph, and bone scan are shown in Figures 58a through 58c. What is the most likely diagnosis?


Explanation
Spontaneous swelling with the appearance of joint subluxation may be associated with an acute, subacute, or chronic bacterial infection of the sternoclavicular joint. Common causes of infection include bacteremia, rheumatoid arthritis, alcoholism, intravenous drug use, and chronic debilitating diseases. Subclavian vein catheterization and renal dialysis can predispose patients to sepsis and osteomyelitis of the sternoclavicular joint. Renoult B, Lataste A, Jonon B, et al: Sternoclavicular joint infection in hemodialysis patients. Nephron 1990;56:212-213.
Question 5High Yield
A 19-year-old woman reports persistent neck pain for 2 years. Pain is relieved with aspirin. A bone scan shows intense uptake in the superior, posterior portion of the C3 vertebral body. A sagittal CT reconstruction is shown in Figure 5. Treatment should consist of
Explanation
The CT scan shows an osteoblastic nidus pathognomic for an osteoid osteoma. Surgical treatment should include an en bloc excision of the lesion. Surgical treatment is not mandatory because the lesion often becomes asymptomatic over time. This lesion is not amenable to radiofrequency ablation due to its proximity to the spinal cord. A complete corpectomy is not necessary to adequately resect the lesion, as only the nidus needs to be removed. Radiation therapy and antibiotics are not appropriate treatments for an osteoid osteoma. Posterior C2-C3 fusion will not address the pathology. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 351-366.
Question 6High Yield
When the great toe deviates into a valgus position, the action of the abductor hallucis muscle becomes one of
Explanation
Explanation
The abductor hallucis muscle inserts together with the medial tendon of the flexor hallucis brevis into the medial base of the proximal phalanx of the great toe. When the hallux assumes a valgus position, the action of the abductor becomes one of flexion and pronation of the first metatarsal. Resch S: Functional anatomy and topography of the foot and ankle, in Myerson M (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 1, pp 25-49.
Question 7High Yield
Which of the following is most associated with local recurrence of the lesion seen in the radiograph and MRI scan shown in Figures 27a and 27b?
Explanation
Explanation
27b The lesion is an aneurysmal bone cyst. These lesions are known to have a local recurrence rate of 5% to 50%. Young age, open physes, stage, and type of surgical removal and resulting margin have all been shown to affect the recurrence rate. Chemotherapy is not used in the treatment of aneurysmal bone cysts. Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
References:
- Vergel De Dios AM, Bond JR, Shives TC, et al: Aneurysmal bone cyst: A clinicopathologic study of 238 cases. Cancer 1992;69:2921-2931.
Question 8High Yield
Venous thrombolembolism is a common complication following total hip and total knee arthroplasty; therefore, prophylaxis is deemed efficacious. Several studies on low-molecular-weight heparin (LMWH) have shown which of the following findings?
Explanation
Prophylactic LMWH is associated with a risk of bleeding complications, especially if administered too soon after surgery. The risk of major bleeding is 0.3% for control, 0.4% for aspirin, 1.3% for warfarin, 1.8% for LMWH, and 2.6% for unfractionated heparin. Colwell and associates conducted a prospective, randomized trial on over 1,500 total hip arthroplasty patients. Overall, the risk of clinically apparent venous thrombolembolism was 3.6% for LMWH and 3.7% for warfarin. LMWH acts in several sites of the coagulation cascade, with its principal action being inhibition of factor 10a. Thrombocytopenia is less common with LMWH than with unfractionated heparin. The use of LMWH is a relative contraindication with indwelling epidural anesthesia. Colwell CW Jr, Collis DK, Paulson R, et al: Comparison of enoxaparin and warfarin for the prevention of venous thromboembolic disease after total hip arthroplasty:. Evaluation during hospitalization and three months after discharge. J Bone Joint Surg Am 1999;81:932-940.
Question 9High Yield
Figure 41a shows the AP radiograph of a 15-year-old boy who reports lateral knee pain. Figures 41b and 41c show a radiograph of the distal femur that was obtained 5 years ago and a current CT scan. The indication for surgery in this patient would be
Explanation
Explanation
41b 41c In a young person with solitary osteochondroma, the best surgical indication is symptoms that limit activity. A growth deformity is unlikely to occur at this age. Malignant degeneration is exceptionally rare and noted most commonly in adults. Growth is expected until skeletal maturity. Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 1626-1659.
References:
- Simon MA, Springfield DS, et al: Common Benign Bone Tumors and Usual Treatment: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 181-205.
Question 10High Yield
Compared to similar patients who do not donate autologous blood, patients with normal baseline hemoglobin who donate autologous blood prior to undergoing primary total hip arthroplasty are likely to
Explanation
Explanation
Billote and associates compared patients with normal baseline hemoglobin levels who did and did not donate autologous blood prior to total hip arthroplasty. No patients received allogeneic blood perioperatively, and the autologous donors had significantly lower hemoglobin levels at the time of surgery and in the recovery room. Of the autologous donors, 69% received an autologous transfusion. The authors concluded that autologous donation was unnecessary in patients undergoing primary total hip arthroplasty who had a normal hemoglobin. Billote D, Glisson SN, Green D, Wixson RL: A prospective, randomized study of preoperative autologous donation for hip replacement surgery. J Bone Joint Surg Am 2002;84:1299-1304.
References:
- Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 47-53.
Question 11High Yield
A 26-year-old woman is seen in the emergency department with an intra-articular distal tibia fracture and a fibular fracture (pilon). The patient, her husband, and three small children have recently immigrated to the United States from Mexico. The husband and wife have both been in a migrant labor camp but have no immediate relatives in the States. What factor is most important when considering her recommended care and treatment?
Explanation
With documented use of a competent interpreter, informed consent should not be an issue. In Hispanic families, the husband often makes the ultimate decision regarding proceeding with surgery; however, he would not be expected to withhold recommended treatment. Hispanics may have a higher risk of comorbidities, but you do not expect this to be a significant concern with this patient. Claustrophobia and some fear of the unfamiliar may make additional imaging studies more difficult to arrange, but not impossible. The real concern is that with no extended family and three small children, the postoperative demand on the patient could significantly jeopardize her ability to comply with weight-bearing restrictions and overall ambulatory demands. Discharge planning and appropriate help may be paramount for a good outcome.
Question 12High Yield
Examination of an 18-year-old professional soccer player who was forcefully kicked across the shin while attempting a slide tackle reveals a marked effusion and limited motion of the knee. The tibia translates 12 mm posterior to the femoral condyles when the knee is held in 90 degrees of flexion. There is no posteromedial or posterolateral instability. Management should consist of
Explanation
The patient has an acute grade III posterior cruciate ligament injury. The majority of grade I and II injuries can be treated with protected weight bearing and quadriceps rehabilitation, and most patients can return to sports within 2 to 4 weeks. In contrast, grade III injuries require immobilization in full extension for 2 to 4 weeks to protect the posterior cruciate ligament and the other posterolateral structures presumed to be damaged. The mainstay of postinjury rehabilitation for all posterior cruciate ligament injuries is quadriceps strengthening exercises, which have been shown to counteract posterior tibial subluxation. Miller MD, Bergfeld JA, Fowler PJ, Harner CD, Noyes FR: The posterior cruciate ligament injured knee: Principles of evaluation and treatment. Instr Course Lect 1999;48:199-207.
Question 13High Yield
Figures 27a and 27b show the radiographs of a 32-year-old woman who was involved in a high-speed motor vehicle accident. She is neurologically intact. After stabilization and assessment, treatment should consist of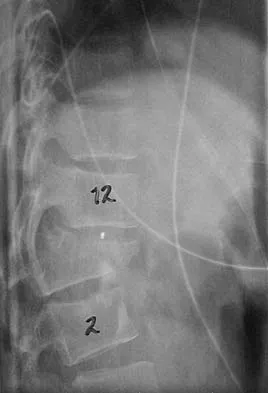

Explanation
The radiographs show a fracture-dislocation with translation in both the coronal and sagittal planes, evidence of significant instability requiring surgical stabilization. Anterior instrumentation is not as effective as posterior instrumentation in restoring stability, and because there is little bony destruction, the anterior column can be successfully reconstructed with simple realignment. The treatment of choice is multisegment posterior fusion with instrumentation. Lewandrowski KU, McLain RF: Thoracolumbar fractures: Evaluation, classification, and treatment, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 817-843.
Question 14High Yield
An axillary nerve lesion may cause weakness in the deltoid and the
Explanation
While the most prominent functional deficit from axillary nerve lesions occurs from denervation of the deltoid, denervation of the teres minor also occurs.
Question 15High Yield
What is the recommended treatment of a skeletally immature 12-year-old boy who has an anterior cruciate ligament-deficient knee?
Explanation
Traditional surgeries for anterior cruciate ligament-deficient knees carry the potential risk of premature physeal closure in young athletes. Therefore, most surgeons are reluctant to recommend intra-articular reconstruction using bone tunnels with bone-patellar tendon-bone autografts or hamstring tendons. The current recommendation for young athletes is activity modification, rehabilitation, and functional bracing until the patient is near skeletal maturity. At that time, for the very symptomatic patient, the treatment of choice is intra-articular repair of the anterior cruciate ligament. If a skeletally immature patient continues to have instability despite rehabilitation and bracing, a modification of the femoral tunnel to the over-the-top position will not place the lateral femoral physis at risk for premature closure and deformity. A centrally placed tibial tunnel will minimize the risk of angular deformity and minimize limb-length discrepancy if physeal arrest occurs. Barry P: Anterior cruciate ligament injuries, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy. Philadelphia, Pa, WB Saunders, 1997, p 358. McCarroll JR, Shelbourne KD, Porter DA, Rettig AC, Murray S: Patellar tendon graft reconstruction for midsubstance anterior cruciate ligament rupture in junior high school athletes: An algorithm for management. Am J Sports Med 1994;22:478-484. Nottage WM, Matsuura PA: Management of complete traumatic anterior cruciate ligament tears in the skeletally immature patient: Current concepts and review of the literature. Arthroscopy 1994;10:569-573.
Question 16High Yield
Figure 6 shows a sagittal oblique MRI scan. The arrow is pointing to what structure?
Explanation
The meniscofemoral ligaments connect the posterior horn of the lateral meniscus to the intercondylar wall of the medial femoral condyle. The ligament of Humphrey (arrow) passes anterior to the posterior cruciate ligament, whereas the ligament of Wrisberg passes posterior to the posterior cruciate ligament. One or the other has been identified in 71% to 100% of cadaver knees, with the ligament of Wrisberg being more common. Clarke HD, Scott WN, Insall JN, et al: Anatomy, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 3-66.
Question 17High Yield
A 58-year-old woman has had a painless periscapular mass for the past year. An MRI scan and biopsy specimen are shown in Figures 4a and 4b. What is the most likely diagnosis?

Explanation
Elastofibroma is a rare tumor that most commonly occurs in adults who are older than age 55 years. The lesions usually grow between the chest wall and the scapula, and 10% are bilateral. Histologic analysis shows that they are composed of equal amounts of elastin and collagen with occasional fibroblasts. Briccoli A, Casadei R, Di Renzo M, Favale L, Bacchini P, Bertoni F: Elastofibroma dorsi. Surg Today 2000;30:147-152.
Question 18High Yield
A 45-year-old man has had left thigh pain for the past 4 months. An AP radiograph, bone scan, MRI scans, and biopsy specimens are shown in Figures 6a through 6f. What is the most appropriate treatment?





Explanation
The radiograph demonstrates thickened trabeculae and thickened cortices in the left proximal femur compared to the right, and the bone scan shows increased uptake in this area. The MRI scans show thickened trabeculae with normal marrow signal. These findings are diagnostic of Paget's disease. Medical treatment, including bisphosphonates and calcitonin, is indicated for painful bone lesions. Hadjipavlou AG, Gaitanis IN, Kontakis GM: Paget's disease of the bone and its management. J Bone Joint Surg Br 2002;84:160-169.
Question 19High Yield
A 14-year-old boy sustains a twisting injury to his right shoulder and recalls feeling a snap during a wrestling match. Examination shows hesitancy to raise the arm away from the side, diffuse tenderness and swelling of the upper arm, and no evidence of neurovascular compromise. Figures 6a and 6b show an AP radiograph and MRI scan. What is the most likely diagnosis?

Explanation
While difficult to appreciate on the AP radiograph of the shoulder, the increased physeal signal demonstrated on the axial MRI scan is consistent with a nondisplaced growth plate fracture. A comparison radiograph of the left shoulder also could be considered and the injured shoulder evaluated for physeal widening. Proximal humeral fractures in children are somewhat unusual, representing less than 1% of all fractures seen in children and only 3% to 6% of all epiphyseal fractures. Physeal injuries are classified according to the Salter-Harris classification scheme. Salter-Harris type I fractures represent approximately 25% of physeal injuries to the proximal humerus in adolescents. The proximal humeral physis is responsible for 80% of the longitudinal growth of the humerus; therefore, there is tremendous potential for remodeling of fractures in this region. Management for nondisplaced Salter-Harris type I fractures is limited to a short period of immobilization followed by a gradual return to activities as clinical symptoms resolve. Curtis RJ, Rockwood CA Jr: Fractures and dislocations of the shoulder in children, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 991-1007.
Question 20High Yield
A 42-year-old woman has cervical stenosis and radicular deficits at the C5-6 and C6-7 levels. History reveals that she has smoked one pack of cigarettes a day for 25 years. Because nonsurgical management has failed to provide relief, she is now seeking surgical treatment. After preoperative counseling, it becomes clear that she is not likely to stop smoking. Which of the following surgical procedures should be used?
Explanation
Explanation
In a review of 190 anterior cervical fusions, Hilibrand and associates reported that only 20 of 40 patients who smoked had solid fusion at all levels, whereas 64 of 91 nonsmokers had solid fusions at all levels when treated with multilevel interbody technique (Smith-Robinson). When fused with strut grafts, 14 of 15 smokers and 41 of 44 nonsmokers had solid fusions with a fusion rate of 93% in the same series. Multilevel allografts have a lower fusion rate than autografts, and diskectomy without fusion has an increased rate of residual neck pain. Hilibrand AS, Fye MA, Emery SE, et al: Impact of smoking on the outcome of anterior cervical arthrodesis with interbody or strut-grafting. J Bone Joint Surg Am 2001;83:668-673.
References:
- Zdeblick TA, Ducker TB: The use of freeze-dried allograft bone for anterior cervical fusions. Spine 1991;16:726-729.
Question 21High Yield
What is the current 5-year survival rate for patients with classic nonmetastatic, high-grade osteosarcoma of the extremity?
Explanation
Multidisciplinary treatment combining systemic chemotherapy and adequate surgical resection has resulted in a 5-year survival rate of 70% in patients with nonmetastatic osteosarcoma of the extremity . The advent of effective chemotherapy has increased the overall survival rate from 20% to 70% in current studies. Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Question 22High Yield
Sterilization of ultra-high molecular weight polyethylene by gamma irradiation in air will degrade its wear performance because of
Explanation
Explanation
Gamma irradiation has long been used as a sterilization method for polyethylene. Exposure to gamma irradiation causes breakage of the chemical bonds in the polyethylene, and oxidation will occur if the material is subsequently exposed to air. The amount of oxidation and decrease in wear performance is also related to the length of time that the gamma-irradiated polyethylene is exposed to oxygen. Collier JP, Sutula LC, Currier BH, et al: Overview of polyethylene as a bearing material: Comparison of sterilization methods. Clin Orthop 1996;333:76-86. McKellop H, Shen FW, Lu B, et al: Effect of sterilization method and other modifications on the wear resistance of acetabular cups made of ultra-high molecular weight polyethylene: A hip-simulator study. J Bone Joint Surg Am 2000;82:1708-1725.
References:
- Sychterz CJ, Young AM, Orishimo K, et al: The relationship between shelf life and in vivo wear for polyethylene acetabular liners. J Arthroplasty 2005;20:168-173.
Question 23High Yield
The insurance carrier of a patient who underwent total knee arthroplasty 4 days ago is now demanding that the patient be discharged from the hospital. However, examination reveals that the patient has a range of motion of only 10 degrees to 55 degrees, and the patient is concerned whether she will ever move her knee normally. The insurance company representative should be advised that
Explanation
Explanation
Examination findings that show flexion of only 55 degrees at discharge should alert the surgeon that the patient will require close scrutiny and follow-up. Mauerhan and associates examined the records of 745 patients who had a primary total knee arthroplasty from 1993 to 1996. At their institution, development and implementation of clinical pathways resulted in a significant decrease in the average length of stay, beginning in 1993 with 6.4 days +/- 1.8 days and progressively decreasing to 4.4 days +/- 1.0 days in 1996. The rate of manipulation (patients manipulated at 6 weeks/total number of patients receiving total knee arthroplasty) was 6.0% in 1993, 11.3% in 1994, 13.5% in 1995, and 12.0% in 1996. In the period of 1993 to 1996, patients requiring manipulation consistently had a lower range of motion of 69.0 degrees +/- 10 degrees at the time of discharge compared with patients not requiring manipulation who had a range of motion of 80.7 degrees +/- 10.6 degrees. In this era of outpatient services, however, another solution would be to arrange for outpatient physical therapy on a more frequent basis and to see the patient more frequently in the office until an acceptable range of motion is established.
References:
- Mauerhan DR, Mokris JG, Ly A, Kiebzak GM: Relationship between length of stay and manipulation rate after total knee arthroplasty. J Arthroplasty 1998;13:896-900.
Question 24High Yield
Accurate evaluation of the upper portion of the subscapularis muscle is best accomplished with active internal rotation
Explanation
Internal rotators of the shoulder include the subscapularis, pectoralis major, teres major, and latissimus dorsi muscles. The subscapularis has two portions, with the upper portion receiving its innervation from the upper subscapular nerve (C5) and the lower portion from the lower subscapular nerve (C5-6). The two tests commonly performed to isolate the internal rotation to the subscapularis muscle are the lift-off test and the belly press test. Electromyographic findings have shown the lift-off test to be more accurate for the lower portion of the subscapularis and the belly press test to be more sensitive for the upper portion. Hintermeister RA, Lange GW, Schultheis JM, Bey MJ, Hawkins RJ: Electromyographic activity and applied load during shoulder rehabilitation exercises using elastic resistance. Am J Sports Med 1998;26:210-220.
Question 25High Yield
A 13-year-old girl sustained an isolated midshaft left femoral fracture in a motor vehicle accident. The fracture was treated with a rigid, antegrade intramedullary nail placed through the piriformis fossa. The fracture healed uneventfully, as shown in Figure 46a; however, at 12 months postoperatively she now reports left hip pain. A current AP radiograph and MRI scan are shown in Figures 46b and 46c. What complication occurred in this patient?
Explanation
Explanation
46b 46c The development of femoral head ischemic necrosis is the iatrogenically created complication in this skeletally immature patient. Placement of a rigid, antegrade intramedullary nail through the piriformis fossa is likely to damage the vascular supply to the femoral head as the vessels ascend the femoral neck on the way to the femoral head. The MRI scan reveals ischemic necrosis with early collapse of the femoral head. The joint space is preserved on the MRI scan, ruling out chondrolysis. Letts M, Jarvis J, Lawton L, et al: Complications of rigid intramedullary rodding of femoral shaft fractures in children. J Trauma 2002;52:504-516. Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop Relat Res 1997;338:60-73.
Question 26High Yield
The scoring system for impending pathologic fractures devised by Mirels involves assessment of which of the following factors?
Explanation
Explanation
The scoring system published by Mirels in 1989 is based on the following characteristics: the location of the lesion, the amount of pain the patient is experiencing, the type of lesion (either lucent, mixed, or blastic), and the lesion size. The tumor is scored from 1 to 3 in each category and a total score is obtained that correlates to fracture risk. Prophylactic fixation is advised for lesions with scores of higher than 8, and consideration for stabilization should be strongly considered for scores of 8. The Mirels scoring system can be useful as an adjunct to clinical decision making. Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. 1989. Clin Orthop Relat Res 2003;415:S4-S13.
References:
- Damron TA, Morgan H, Prakash D, et al: Critical evaluation of Mirels' rating system for impending pathologic fractures. Clin Orthop Relat Res 2003;415:S201-S207.
Question 27High Yield
Late surgical treatment of posttraumatic cubitus varus (gunstock deformity) is usually necessitated by the patient reporting problems related to
Explanation
Cubitus varus, elbow hyperextension, and internal rotation are all typical components of the gunstock deformity. This deformity results from malunion of a supracondylar fracture of the humerus. All of the problems listed above have been reported as sequelae of a gunstock deformity, although the malunion usually causes no functional limitations. Unacceptable appearance is the most common reason why patients or parents request corrective osteotomy. O'Driscoll SW, Spinner RJ, McKee MD, et al: Tardy posterolateral rotatory instability of the elbow due to cubitus varus. J Bone Joint Surg Am 2001;83:1358-1369. Gurkan I, Bayrakci K, Tasbas B, et al: Posterior instability of the shoulder after supracondylar fractures recovered with cubitus varus deformity. J Pediatr Orthop 2002;22:198-202.
Question 28High Yield
A 25-year-old woman has significant pain and swelling in her left ankle after falling off her bicycle. Examination reveals that she is neurovascularly intact. Radiographs are shown in Figures 33a through 33c. What is the next most appropriate step in management?


Explanation
The radiographs show a displaced ankle fracture with widening of the syndesmosis. Open reduction and internal fixation is indicated with fixation of the mortise with syndesmotic screws. Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Question 29High Yield
A 14-year-old football player has had right knee pain for the past 2 months; however, he denies any history of trauma. Examination shows an abductor lurch and increased external rotation of the right lower extremity. The best course of action should be to
Explanation
Explanation
Slipped capital femoral epiphysis is the most common pathology involving the hip in adolescents. While patients with acute slips may report severe pain and are unable to ambulate, those with chronic slips often have pain during ambulation, a limp, and increased external rotation of the hip. While 60% of the patients specifically report hip pain, the remainder have pain in the thigh or knee. The initial diagnostic study of choice is AP and frog-lateral radiographs of the pelvis; bilateral involvement is frequently seen. Boyer DW, Mickelson MR, Ponseti IV: Slipped capital femoral epiphysis: Long-term follow-up study of one hundred and twenty-one patients. J Bone Joint Surg Am 1981;63:85-95.
References:
- Stasikelis PJ, Sullivan CM, Philips WA, Polard JA: Slipped capital femoral epiphysis: Prediction of contralateral involvement. J Bone Joint Surg Am 1996;78:1149-1155.
Question 30High Yield
A 35-year-old carpenter sustained an injury to his dominant shoulder in a fall. He reports that he felt a sharp tearing sensation as he held on to a scaffold to keep from falling. Examination reveals swelling and ecchymosis down the upper arm, weakness to internal rotation, and deformity of the anterior axilla. He has good strength in external rotation and no apprehension with instability testing. Radiographs are normal. Management should consist of
Explanation
The findings are classic for a pectoralis major tendon avulsion. Deformity of the anterior axillary fold is a classic finding, and ecchymosis down the arm suggests that the injury is at the humeral attachment rather than at the musculotendinous junction. Good external rotation strength indicates that function in the supraspinatus and infraspinatus has been preserved. The treatment of choice for a tendon avulsion in a young individual is early surgical repair. Conversely, if the injury is within the muscle or at the musculotendinous junction, initial nonsurgical management is recommended. If the location of the injury cannot be determined by physical examination, then MRI of the pectoralis major can be helpful. Hanna CM, Glenny AB, Stanley SN, et al: Pectoralis major tears: Comparison of surgical and conservative treatment. Br J Sports Med 2001;35:202-206.
Question 31High Yield
A 57-year-old woman with diabetes mellitus has purulent drainage from a lateral incision after undergoing open reduction and internal fixation of a displaced ankle fracture 10 days ago. Examination reveals moderate erythema and a foul odor coming from the wound. Cultures are obtained. What is the next most appropriate step in management?
Explanation
Early postoperative wound infections after open reduction and internal fixation should be treated with aggressive debridement and maintenance of stability of the fracture. If infection persists following healing of the fracture, the hardware should be removed. Carragee EJ, Csongradi JJ, Bleck EE: Early complications in the operative treatment of ankle fractures: Influence of delay before operation. J Bone Joint Surg Br 1991;73:79-82.
Question 32High Yield
A 22-year-old woman reports a 4-year history of worsening low back and left lower extremity pain following a motor vehicle accident. Management consisting of physical therapy, chiropractic manipulation, and interventional pain management, including sacroiliac joint injections and epidural steroid injections, has failed to provide relief. A sagittal T2-weighted MRI scan is shown in Figure 8. No nerve root compression is seen on axial images. She is currently working and lives with her fiancé. She smokes half a pack of cigarettes per day and reports depression on her health history. She is being maintained on narcotic analgesics and is having increasing difficulty performing her activities of daily living secondary to pain. What is the most appropriate management at this time?
Explanation
Explanation
The MRI scan reveals a rudimentary disk at the L5-S1 level, suggesting transitional anatomy. There is a posterior disk bulge at L3-4. At L4-5, there is disk desiccation and loss of disk height, with a posterior disk bulge and a high intensity zone in the posterior annulus, suggesting an annular tear. While these and similar radiographic findings have been associated with the severity of a patient's pain, they are also commonly found in cross-sectional studies of asymptomatic subjects. Carragee and associates found 59% of symptomatic patients undergoing diskography have high intensity zones as compared to 25% of asymptomatic subjects of a similar patient profile. Diskographic injections provoked pain in disks with high intensity zones approximately 70% of the time whether the individual was previously symptomatic or not. This patient's non-specific pain pattern does not require further work-up as she is not a surgical candidate. Carragee EJ, Paragioudakis SJ, Khurana S: 2000 Volvo Award winner in clinical studies: Lumbar high-intensity zone and discography in subjects without low back problems. Spine 2000;25:2987-2992. Pneumaticos SG, Reitman CA, Lindsey RW: Diskography in the evaluation of low back pain. J Am Acad Orthop Surg 2006;14:46-55. Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Question 33High Yield
Figure 40 shows the plain radiograph of a 30-year-old woman who has had a long history of standing bilateral anterior knee pain and a sense of patellar instability without frank dislocation. Nonsurgical management consisting of anti-inflammatory drugs and physical therapy has failed to provide relief. Examination reveals full range of motion of both knees, with moderate patellofemoral crepitance. Patellar apprehension and patellar grind tests are positive. The Q-angle measures 20 degrees. Management should now consist of
Explanation
Explanation
The history, physical examination, and radiographs indicate that the patellofemoral pain is most likely caused by excessive lateral patellar pressure and patellar maltracking. Because the radiographs reveal the lateral tilt of the patella and lateral subluxation, the treatment of choice is bilateral lateral releases with anteromedialization of the tibial tubercles. This procedure corrects not only the excessive lateral patellar pressure, but also the lateral subluxation. The use of patella-stabilizing braces or taping may provide temporary relief, but these implements are not well-tolerated and they will not change the underlying biomechanics of the knee. Simple lateral release is indicated for isolated lateral tilt, but it does not correct the lateral subluxation. The use of thermal capsular shrinkage for the medial retinaculum has not been proven to provide long-term correction of the deformity. Boden BP, Pearsall AW, Garrett We Jr, et al: Patellofemoral instability: Evaluation and management. J Am Acad Orthop Surg 1997;5:47-57.
References:
- Fulkerson JP: Patellofemoral pain disorders: Evaluation and management. J Am Acad Orthop Surg 1994;2:124-132.
Question 34High Yield
The use of nasotracheal intubation for airway management is contraindicated in the acute multiply injured patient when the patient has
Explanation
Explanation
The use of nasotracheal intubation is less desirable in patients with respiratory arrest because placement of the tube is most reliable when the patient is breathing. Nasotracheal intubation is advantageous in patients with suspected cervical spine trauma because it does not require hyperextension of the neck. A nasotracheal tube may be more comfortable than an orally placed tube because it is fixed at several points and moves less freely within the larynx, subglottic area, and trachea. The presence of a hemothorax or pneumothorax does not affect the choice of airway control but does require placement of a chest tube. Colice GL: Prolonged intubation versus tracheostomy in the adult. J Intern Care Med 1987;2:85.
References:
- Shackford S: Spine injury in the polytrauma patient: General surgical and orthopaedic considerations, in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 9-15.
Question 35High Yield
Which of the following is most commonly associated with an open clavicular fracture?
Explanation
Explanation
Open clavicular fractures are rare and result from high-energy trauma. In a series of 20 patients with open clavicular fractures, 13 (65%) sustained a closed head injury. Fifteen (75%) had associated pulmonary injuries and 35% had a cervical or thoracic spine fracture. Only one demonstrated scapulothoracic dissociation. Screening for pulmonary and closed head injuries should be considered in the setting of traumatic open clavicular fractures.
Question 36High Yield
A farmer is seen in the emergency department after falling out of a hay loft onto the barn floor below. He is unable to bear weight. Exploration of a 0.5 cm laceration over the anterior tibia reveals bone. Radiographs reveal oblique displaced midshaft tibial and fibular fractures. Based on these findings, what is the most appropriate antibiotic prophylaxis?
Explanation
Explanation
A farm injury is automatically considered a grade III (Gustillo classification) injury regardless of size, energy, or additional soft-tissue injury due to the likelihood of substantial contamination. Antibiotic recommendations for grade III injuries include a first- or second-generation cephalosporin with an aminoglycoside or fluoroquinolone within 3 hours of injury, with penicillin added for farm injuries. Okike K, Bhattacharyya T: Trends in the management of open fractures: A critical analysis. J Bone Joint Surg Am 2006;88:2739-2748.
Question 37High Yield
A 77-year-old man has had increasing right knee pain for the past 3 months. A radiograph and coronal T1-weighted MRI scan are shown in Figures 19a and 19b. A biopsy specimen is shown in Figure 19c. What is the most likely diagnosis?
Explanation
Explanation
19b 19c The radiograph shows a calcified lesion in the medullary canal of the distal femoral diaphysis. The MRI scan shows extensive marrow change distal to the lesion, which is not consistent with an enchondroma. The histology shows a biphasic pattern with low-grade cartilage just apposed to high-grade spindle cell sarcoma. The overall appearance is consistent with dedifferentiated chondrosarcoma. The radiographic appearance is not consistent with enchondroma, and the histologic appearance is not consistent with the other choices. Mitchell AD, Ayoub K, Mangham DC, et al: Experience in the treatment of dedifferentiated chondrosarcoma. J Bone Joint Surg Br 2000;82:55-61.
References:
- Frassica FJ, Unni KK, Beabout JW, Sim FH: Dedifferentiated chondrosarcoma: A report of the clinicopathological features and treatment of seventy-eight cases. J Bone Joint Surg Am 1986;68:1197-1205.
Question 38High Yield
Which of the following is NOT considered a risk factor for nonunion of a type II odontoid fracture?
Explanation
Although obesity can make brace or halo wear difficult, it has not been associated with an increased risk for nonunion. Carson GD, Heller JG, Abitbol JJ, et al: Odontoid fractures, in Levine AM, Eismont FJ, Garfin SR, et al (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 235-238.
Question 39High Yield
A 38-year-old woman fell from a ladder onto her right hip. The radiographs and CT scan are shown in Figures 52a through 52d. What is the best surgical approach for this fracture?
Explanation
Explanation
52b 52c 52d The fracture is an associated both column fracture. The best approach for this fracture is the ilioinguinal. The Kocher-Langenbeck is best for posterior injuries to the acetabulum and some transverse fractures. The iliofemoral alone is limited to high anterior column injuries. The extended iliofemoral and triradiate approaches although useful for this fracture, have a higher rate of complications. Letournel E: The treatment of acetabular fractures through the ilioinguinal approach. Clin Orthop Relat Res 1993;292:62-76.
Question 40High Yield
What three structures are considered the primary constraints necessary for elbow stability?
Explanation
Explanation
The three primary constraints necessary for elbow stability in all directions are the ulnar part of the lateral collateral ligament (also called the lateral ulnar collateral ligament), the anterior band of the medial collateral ligament, and the coronoid. The radial head and capsule are secondary constraints to elbow instability. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
References:
- Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354.
Question 41High Yield
A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow 9 years ago. Over the past year the patient has had increasing pain and elbow instability. There is no clinical evidence of infection, and radiographs show no new bony process. What is the best option for this patient?
Explanation
Explanation
In a series reported by Blaine and associates, 12 patients were converted from interposition to total elbow arthroplasty. This procedure was successful in 10 out of 12 patients. Blaine TA, Adams R, Morrey BF: Total elbow arthroplasty after interposition arthroplasty for elbow arthritis. J Bone Joint Surg Am 2005;87;286-292.
References:
- Cheng SL, Morrey FB: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Question 42High Yield
Figure 38 shows the radiograph of a 5-year-old child who sustained a type III supracondylar fracture. Examination reveals the absence of a radial pulse, but an otherwise well-perfused hand. Following closed reduction and percutaneous pinning, the radial pulse remains absent; however, the hand is pink and well perfused. Management should now include
Explanation
In a study of over 400 patients with displaced supracondylar fractures, 3.2% of the fractures were associated with the absence of the radial pulse with an otherwise well-perfused hand. Based on this study, a period of close observation with frequent neurovascular checks should be completed before attempting invasive correction of the problem. Because of the satisfactory results with expectant management, angiography, exploration, removal of fixation and exploration, and thrombectomy are contraindicated.
Question 43High Yield
A 12-year-old girl who is Risser stage 3 has had intermittent mild midback pain for the past 4 weeks. The pain is worse after prolonged sitting and after carrying a heavy backpack at school. She occasionally takes acetaminophen, but the pain does not limit sport activities. Examination reveals a mild right rib prominence during forward bending. Neurologic examination is normal. Radiographs show a 20-degree right thoracic scoliosis with no congenital anomalies or lytic lesions. Management should consist of
Explanation
Mild scoliosis is not a painful condition, but it usually presents during adolescence. Intermittent back pain is reported by 25% to 30% of adolescents whether or not scoliosis is present. Such pain is often attributed to muscle strain from tight muscles, poor posture, or heavy school backpacks. The clinician must distinguish typical pain (mild, intermittent, nonlimiting) from atypical pain. The latter requires more careful examination and imaging studies (bone scan or MRI) to determine the source of pain. The patient's age and right thoracic curve pattern are typical for idiopathic scoliosis; therefore, imaging of the neuroaxis is not necessary to look for cord syrinx, tethering, or tumor. Brace treatment is not required for this small curve unless future progression is demonstrated. Ramirez N, Johnston CE, Browne RH: The prevalence of back pain in children who have idiopathic scoliosis. J Bone Joint Surg Am 1997;79:364-368. Hollingworth P: Back pain in children. Br J Rheum 1996;35:1022-1028.
Question 44High Yield
A 12-year-old girl has had pain in her right knee for 1 month that started as activity-related and progressed to night pain. Radiographs are shown in Figures 16a and 16b, and a biopsy specimen is shown in Figure 16c. What is the recommended treatment?
Explanation
Explanation
16b 16c This is a classic appearance for an osteosarcoma. The radiographs reveal a mixed osteolytic and osteoblastic lesion in a skeletally immature patient in the distal right femoral metaphysis. The pain pattern with progressive symptoms leading to the presence of night pain is also typical for this condition. The biopsy specimen reveals pleomorphic cells and the presence of osteoid. The current standard of care in the treatment of osteosarcoma is neoadjuvant chemotherapy followed by surgical resection or amputation followed by additional postoperative chemotherapy. Osteosarcoma is not radiosensitive. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
References:
- McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 205.
Question 45High Yield
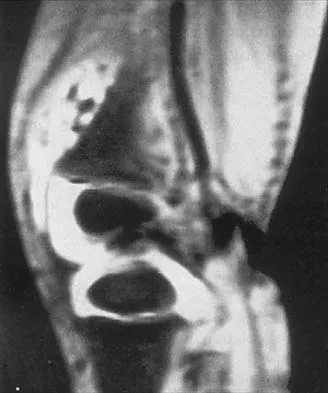
A 44-year-old woman has had lower extremity dysesthesias, urinary incontinence, and has been unable to walk for the past 2 days. She reports no pain or history of trauma. She notes that 3 weeks ago she missed work for 2 days because of back pain, but it resolved with rest. Examination shows decreased or absent sensation below the knees, no motor function below the knees, and decreased rectal tone. Catheterization results in a postvoid residual of 2,000 mL. Plain radiographs and MRI scans without contrast are shown in Figures 1a through 1d. What is the next most appropriate step in management?
Explanation
Explanation
1b 1c 1d The patient has had a clear and sudden onset of a profound neurologic deficit. The radiographic studies suggest a lesion in the conus medullaris that appears to be intradural and intramedullary. MRI, with and without contrast, will best evaluate this mass further. The addition of gadolinium allows further evaluation of vascularity and the extent of the lesion. Eichler ME, Dacey RG: Intramedullary spinal cord tumors, in Bridwell KH, Dewald RL (eds): The Textbook of Spine Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, vol 2, pp 2089-2116.
References:
- Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 81-87.
Question 46High Yield
Cementation technique has a definite influence on the long-term survival of cemented femoral components. Both clinical and autopsy studies support the use of a cement mantle with a thickness of how many millimeters?
Explanation
Explanation
Long-term radiographic analysis of cemented total hips supports the creation of a 2- to 5-mm cement mantle in the proximal medial region. Autopsy studies have shown that the incidence of crack formation was greatest when the cement mantle was less than 2 mm. Ebramzadeh E, Sarmiento A, McKellop HA, Llinas A, Gogan W: The cement mantle in total hip arthroplasty: Analysis of long-term radiographic results. J Bone Joint Surg Am 1994;76:77-87. Jasty M, Maloney WJ, Bragdon CR, O'Connor DO, Haire T, Harris WH: The initiation of failure in cemented femoral components of hip arthroplasty. J Bone Joint Surg Br 1991;73:551-558.
References:
- Maloney WJ III: The cemented femoral component, in Callaghan JJ, Rubash HE, Rosenberg AG (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 965-966.
Question 47High Yield
Which of the following findings is an indication for adjunctive use of high-dose steroids?
Explanation
Explanation
According to NASCIS III, the high-dose steroid protocol involves infusion of 30 mg/kg methylprednisolone followed by 5.4 mg/kg/h for 24 hours if the patient has sustained a spinal cord injury within the last 3 hours. The drip is continued for 48 hours if administration is started between 3 and 8 hours of the onset of neurologic deficit. No benefit has been conclusively demonstrated with steroids administered beginning 8 hours or longer after injury. Steroid use is not indicated for nerve root deficits, brachial plexus deficits, or gunshot wounds. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 319-328.
References:
- Bracken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the Third National Acute Spinal Cord Injury randomized controlled trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
Question 48High Yield
A 38-year-old man who is an avid tennis player has had persistent pain over the medial aspect of his knee for the past 6 years. He notes that the pain occurs on a daily basis with any significant activity. Nonsteroidal anti-inflammatory drugs have failed to provide relief. Radiographs are shown in Figures 22a and 22b. What is the best course of action?

Explanation
In a relatively young patient who is an avid tennis player, the treatment of choice is a joint preserving procedure. The radiographs reveal varus alignment with loading of the medial compartment. After all nonsurgical management options have been used, the best treatment option is a medial opening wedge osteotomy. A lateral closing wedge osteotomy of the proximal tibia is also a reasonable option, but it is not one of the choices. A unicompartmental arthroplasty or a total knee arthroplasty would place significant restrictions in this patient. A unispacer may be a temporizing procedure but is controversial and without substantial data in the literature. The knee arthroscopy will not address the medial compartment osteoarthritis. Nagel A, Insall JN, Scuderi GR: Proximal tibial osteotomy: A subjective outcome study. J Bone Joint Surg Am 1996;78:1353-1358. Rinonapoli E, Mancini GB, Corvaglia A, et al: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
Question 49High Yield
Compared to postoperative radiation therapy, preoperative radiation therapy has a higher rate of what complication?
Explanation
Explanation
Radiation therapy is commonly used as an adjuvant in the treatment of soft-tissue sarcomas, but a controversy exists whether it should be preoperative or postoperative. Radiation therapy can be given prior to or following resection of the tumor. Postoperative radiation is usually given in a higher dose to a larger treatment field. This commonly results in a higher incidence of fibrosis and lymphedema. There is no statistical difference in local recurrence rate between the two radiation treatment plans. Neuropathy is more commonly a complication of chemotherapy. Preoperative radiation therapy has been shown to have a higher wound complication rate than postoperative radiation. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
References:
- Davis AM, O'Sullivan B, Turcotte R, et al: Late radiation morbidity following randomization to preoperative versus postoperative radiotherapy in extremity soft tissue sarcoma. Radiother Oncol 2005;75:48-53.
Question 50High Yield
Figure 14 shows the clinical photographs and radiograph of an 8-year-old girl who has a progressive equinus deformity of the right ankle. There is no history of trauma or infection. What is the most likely diagnosis?
Explanation
Explanation
14 14 Focal scleroderma is characterized by the formation of patches of sclerotic skin, also known as morphea, or streaks of sclerosis (linear scleroderma). Systemic involvement in focal scleroderma is unusual; however, progression during childhood is common. Contracture of underlying tissues is common, often resulting in serious joint contractures. Bony changes similar to those seen in melorheostosis can be seen. This patient has characteristic skin changes, atrophy of the soft tissues, Achilles tendon contractures, and calcaneal deformities. There are no signs of arthrogryposis, which usually presents with bilateral congenital deformities, including equinovarus. Klippel-Trenaunay-Weber syndrome is characterized by venous malformation in association with focal overgrowth.
References:
- Bottoni CR, Reinker KA, Gardner RD, Person DA: Scleroderma in childhood: A 35-year history of cases and review of the literature. J Pediatr Orthop 2000;20:442-449.
Question 51High Yield
What common cytologic abnormality is associated with Ewing's sarcoma?
Explanation
Cytogenetic abnormalities have been well characterized in a number of tumors. Translocation t (2, 13), (x, 18), (12, 16), and (12, 22) have been characterized in rhabdomyosarcoma, synovial cell sarcoma, myxoid liposarcoma, and clear cell sarcoma, respectively. Translocation t(11:22) can be identified in 95% of patients with Ewing's sarcoma. This was first described by Turc-Carel and associates in 1984. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby Year Book, 1995, pp 105-118. Turc-Carel C, Philip I, Berger MP, Philip T, Lenoir GM: Chromosome study of Ewing's sarcoma (ES) cell lines: Consistency of a reciprocal translocation t(11;22) (q24;q12). Cancer Genet Cytogenet 1984;12:1-19.
Question 52High Yield
A 55-year-old man sustained an isolated closed fracture of the humerus. Initial neurologic examination reveals no active wrist or finger extension. Radiographs are shown in Figures 28a and 28b. Management should consist of
Explanation
Explanation
28b The patient has an isolated closed injury involving the humeral diaphysis. The lack of wrist and finger extension indicates injury to the radial nerve. Based on these findings, ongoing observation of the nerve is warranted with delayed exploration after 3 to 4 months if there are no signs of progressive return of nerve function. Treatment of the fracture should include external immobilization and fracture bracing. An indication for nerve exploration and surgical stabilization would be an open fracture. Zuckerman JD, Kovil KJ: Fractures of the shaft of the humerus, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1025-1053.
References:
- Pollock FH, Drake D, Bovill EG, Day L, Trafton PG: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Question 53High Yield
Figures 23a and 23b show the AP and lateral radiographs of the elbow of a 30-year-old professional pitcher. The pathology shown in these studies is most consistent with which of the following conditions?
Explanation
Explanation
23b The radiographs show the osteophytic build-up of the posteromedial corner of the elbow that occurs with valgus extension overload in the pitching elbow. This is the result of excessive valgus forces during the acceleration and deceleration phases of throwing. These forces, coupled with medial elbow stresses, cause a wedging of the olecranon into the medial wall of the olecranon fossa. Valgus instability of the elbow may further stimulate osteophyte formation. Repetitive impact of a spur within the olecranon fossa may cause fragmentation and eventual formation of loose bodies. Azar FM, Wilk KE: Nonoperative treatment of the elbow in throwers. Oper Tech Sports Med 1996;4:91-99. Field LD, Savoie FJ: Common elbow injuries in sport. Sports Med 1988;26:193-205.
References:
- Wilson FD, Andrews JR, Blackburn TA, et al: Valgus extension overload in the pitching elbow. Am J Sports Med 1983;11:83-88.
Question 54High Yield
A 12-year-old boy reports limping and chronic knee pain that is now inhibiting his ability to participate in sports. Clinical examination and radiographs of the knee are normal. Additional evaluation should include
Explanation
Explanation
While all of the answers may be appropriate, radiating pain from hip pathology must be excluded. At this age, a slipped capital femoral epiphysis is likely. Therefore, the hip must be examined. Kocher MS, Bishop JA, Weed B, et al: Delay in diagnosis of slipped capital femoral epiphysis. Pediatrics 2004;113:322-325.
References:
- Matava MJ, Patton CM, Luhmann S, et al: Knee pain as the initial symptom of slipped capital femoral epiphysis: An analysis of initial presentation and treatment. J Pediatr Orthop 1999;19:455-460.
Question 55High Yield
During C1-C2 transarticular screw fixation, screw misplacement is most likely to result in injury to the
Explanation
Explanation
With C1-C2 transarticular screw fixation, the following structures are potentially at risk: vertebral artery, spinal cord, occiput-C1 joint, and hypoglossal nerve. The vertebral artery is most vulnerable to injury with drill misdirection or anatomic variations in the vertebral foramen. The hypoglossal nerve may be injured if the drill, tap, or screw passes too far anterior to the lateral mass of C1. This complication is extremely rare. The occiput-C1 joint may be injured if the screw trajectory is too cephalad or cranially directed; however,this scenario is very unlikely because the exposure tends to direct the screw into a caudally inclined direction. This caudal orientation has the potential to cause vertebral artery injury, especially in patients who have a large vertebral foramen in the lateral mass of C2 because of erosions (rheumatoid arthritis) or anatomic variation. CT of the vertebral foramen is recommended when C1-C2 transarticular fixation is being considered. Spinal cord injury is extremely unlikely because of the very large size of the spinal canal in the upper cervical spine; the spinal cord lies far away from the lateral masses of C1 and C2. Mueller ME, Allgower M, et al: Manual of Internal Fixation, ed 3. New York, NY, Springer-Verlag, 1991, pp 634-636.
References:
- Gebhard JS, Schimmer RC, Jeanneret B: Safety and accuracy of transarticular screw fixation C1-C2 using an aiming device: An anatomic study. Spine 1998;23:2185-2189.
Question 56High Yield
The presence of S100B tumor marker typically corresponds with which of the following as being the most likely source of the metastasis?
Explanation
Advances in development of new tumor markers and techniques of antigen retrieval have enhanced the sensitivity and reliability of identifying the primary source of metastasis. New markers such as CK7, CK20, CA125, and thyroid transcription factor-1 (TTF-1) can help to determine the origin of an adenocarcinoma or aid in the recognition of other tumors. In patients who do not have an obvious primary site of disease or screening radiographs, these new markers can help focus the search for and guide the treatment of the underlying lesion. CA125 is positive in patients with ovarian cancer, CK7 is positive in patients with breast and lung carcinoma, and CK20 is indicative of colon carcinoma if the CK7 marker is negative. Gastrointestinal stromal tumor (GIST) is positive for CD117 (c-kit) and CD34, whereas 75% of bronchogenic carcinomas are positive for TTF-1. Histochemical staining of the S100 protein family has been used for many years in the diagnosis of malignant melanoma. Recent markers HMB-45, MART-1, and Melan-A have proved to be useful in diagnosis of melanoma. S100B protein has been implicated in downregulation of p53 (oncosuppressor gene). Harpio R, Einarsson R: S100 proteins as cancer biomarkers with focus on S100B in malignant melanoma. Clin Biochem 2004;37:512-518.
Question 57High Yield
A 6-year-old girl has the bilateral foot deformity shown in Figure 1. There is no family history of disease. Examination reveals fixed hindfoot equinus, and muscle function testing shows strong posterior tibial function, fair plus anterior tibial function, poor peroneal function, and strong gastrocnemius function. A Coleman block test shows a correctable hindfoot. Nerve conduction velocity studies show diminished function in the peroneal and ulnar nerves on both sides. Pathologic changes found in a sural nerve biopsy include "onion bulb" formation, and DNA testing confirms the presence of a mutation in the MPZ gene, consistent with hereditary motor sensory neuropathy type III (HMSN-III). What is the best course of action?
Explanation
The patient has HMSN-III or Dejerine-Sottas syndrome. This form of HMSN progresses very rapidly and frequently results in severe foot deformity in early childhood. The changes are progressive and are the result of muscle imbalance during growth. Balancing of the foot musculature is essential, particularly during the phases of rapid growth of the foot. However, this cannot be accomplished using the anterior tibial muscle because it is already weak and the transfer will further weaken it. Bony procedures also may be required, and tendon transfers cannot be depended on to correct bony deformity. However, these procedures can be deferred until the foot is closer to adult size. Surgeries that lead to joint arthrodesis, such as triple arthrodesis and some midfoot osteotomies, are contraindicated because the feet may lose protective sensation as the disease progresses. Fusions in insensate feet are less successful than realignment procedures that maintain mobility. Wetmore RS, Drennan JC: Long-term results of triple arthrodesis in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 1989;71:417-422. Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth. J Bone Joint Surg Br 1989;71:17-20.
Question 58High Yield
A 20-year-old professional female jockey who is wearing a helmet is thrown from her horse. What is the most likely location of her injury?
Explanation
The incidence of injury associated with horseback rising is estimated to be one per 350 riding hours to one per 1,000 riding hours. Of these injuries, approximately 15% to 27% are severe enough to warrant hospital admission. Significant and serious injuries in equestrian activities are associated with recreational riders and those not wearing a helmet. Head and spine injuries are more common in recreational and nonhelmeted riders. Extremity injuries are more common in professional and helmeted riders. Professional riders are less likely to be admitted to the hospital than recreational riders, and are about half as likely to be disabled at 6 months after injury as recreational riders. Lim J, Puttaswamy V, Gizzi M, et al: Pattern of equestrian injuries presenting to a Sydney teaching hospital. ANZ J Surg 2003;73:567-571.
Question 59High Yield
A 10-year-old soccer player has bilateral heel pain and reports that the pain is worse during and immediately after sports. Examination reveals that the calcaneal tuberosities are painful to palpation bilaterally. What is the most likely diagnosis?
Explanation
Explanation
Calcaneal apophysitis (Sever's disease) is a common cause of heel pain in children who are active in sports. The symptoms are most commonly bilateral and will often respond to a gastrocnemius-soleus complex stretching program. In addition, rest, anti-inflammatory drugs, and heel pads for the shoe may be prescribed. There is no effect on the long-term growth of the calcaneus. Micheli LJ, Ireland ML: Prevention and management of calcaneal apophysitis in children: An overuse syndrome. J Pediatr Orthop 1987;7:34-38.
References:
- Bernhardt DT, Landry GL: Sports injuries in young athletes. Adv Pediatr 1995;42:465-500.
Question 60High Yield
The space available for the cord is an important determinant in neurologic recovery. Recent analysis suggests that the most reliable radiographic predictor for neurologic recovery after surgery in patients with rheumatoid arthritis and paralysis is a preoperative
Explanation
Boden and associates' recent article presents significant evidence that patients with rheumatoid arthritis, neurologic deterioration, and C1-2 instability are more likely to improve after surgery if the posterior alanto-odontoid interval is greater than 10 mm preoperatively. The accepted safe range for the posterior atlanto-odontoid interval is 14 mm. This measurement is believed to better represent the space available for the cord than the anterior alanto-odontoid interval. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 273-279. Boden SD, Dodge LD, Bohlman HH, Rechtine GR: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Question 61High Yield
A 53-year-old man has a 4- x 5-cm high-grade soft-tissue sarcoma in the midthigh. As part of the staging evaluation, regional nodes should be assessed by
Explanation
In general, soft-tissue metastases to regional nodes are a relatively rare occurrence (less than 5% overall). The incidence of lymphatic metastasis is highest for synovial sarcoma, rhabdomyosarcoma, clear cell sarcoma, and epithelioid sarcoma. Regional nodes should be assessed clinically. CT is not used to routinely assess regional nodes. Evaluation of a sentinal node is not indicated because of the low incidence of regional nodal involvement. Fine needle aspiration may be indicated to assess clinically suspicious nodes. Prophylactic inguinal node dissection is contraindicated because it may lead to unnecessary complications such as lymphedema.
Question 62High Yield
Figure 3 shows the AP radiograph of a patient with diabetes mellitus who has knee pain. A semiconstrained knee prosthesis was used in this patient to prevent which of the following complications?
Explanation
The radiographic appearance of the joint is highly suspicious for neuropathic joint (Charcot's joint). Evidence of bone loss on both the tibial and the femoral sides may necessitate the use of metal and/or bone augments. Patients with a neuropathic joint often have excellent range of motion, and postoperative stiffness is not a problem. The main problem with these patients is instability that occurs secondary to ligamentous laxity. Use of a semiconstrained prosthesis prevents the latter complication. Parvizi J, Marrs J, Morrey BF: Total knee arthroplasty for neuropathic (Charcot) joints. Clin Orthop 2003;416:145-150.
Question 63High Yield
Figures 36a and 36b show the MRI scans of a 15-year-old girl who has had pain and recurrent hemarthrosis in the knee for the past year. Plain radiographs are normal. What is the most likely diagnosis?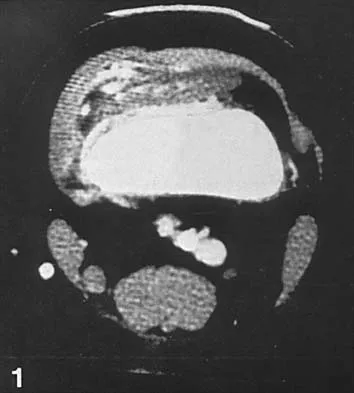
Explanation
In pediatric patients who have pain and recurrent hemarthrosis in the knee, hemangioma is often seen as an internal derangement of the knee, and long delays in diagnosis are common. An MRI scan is noninvasive and will best aid in diagnosis. In this patient, the MRI scan shows a hemangioma with no evidence of meniscal injury or discoid meniscus. Hemophilia is unlikely because the patient is female. The presence of hemarthrosis makes JRA an unlikely diagnosis.
Question 64High Yield
If a laminectomy for spinal stenosis is performed, which of the following is an indication for concomitant arthrodesis at that level?
Explanation
Explanation
A prospective randomized study of patients with degenerative spondylolisthesis and spinal stenosis by Herkowitz and Kurz showed significantly improved clinical outcomes in patients who also received a lumbar arthrodesis. Patients with a laminectomy at an adjacent level do not have improved outcomes with an arthrodesis. Minimal lumbar scoliosis does not require arthrodesis. Arthrodesis is indicated in cases where there is removal of more than 50% of the facets bilaterally but not with an associated foraminal stenosis. Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-807.
References:
- Garfin SR, Rauschning W: Spinal stenosis. Instr Course Lect 2001;50:145-152.
Question 65High Yield
Varus deformity after talar fractures is often seen due to collapse of the medial cortex. What artery supplies this portion of the talus?
Explanation
Explanation
The artery of the tarsal canal is a branch of the posterior tibial artery. Among the branches of the artery of the tarsal canal is the deltoid artery. This arterial complex supplies the medial one third of the talar body. Disruption of this artery may lead to osteonecrosis of the medial body and subsequent collapse into varus. This is most commonly seen with talar body fractures but may be seen in Hawkins type 3 talar neck fractures. The artery of the tarsal sinus arises from the dorsalis pedis, lateral malleolar, and perforating peroneal arteries. The peroneal artery anastomoses with the calcaneal branches of the posterior tibial artery to form a plexus of vessels that supplies the posterior tubercle of the talus. Disruption of this artery would not result in collapse of the medial body, and thus would not lead to a varus deformity. Halibruton RA, Sullivan CR, Kelly PJ, et al: The extra-osseous and intra-osseous blood supply of the talus. J Bone Joint Surg Am 1958;40:1115.
References:
- Mulfinger GL, Trueta J: The blood supply of the talus. J Bone Joint Surg Br 1970;52:160-167.
Question 66High Yield
What structure is located immediately posterior to the capsule at the posterior cruciate ligament tibial insertion?
Explanation
The popliteal artery lies just posterior to the posterior cruciate ligament tibial insertion, separated only by the posterior capsule of the knee. When performing a posterior cruciate ligament reconstruction, this artery is at risk for injury during creation of the tibial tunnel. Jackson DW, Proctor CS, Simon TM: Arthroscopic assisted PCL reconstruction: A technical note on potential neurovascular injury related to drill bit configuration. J Arthroscopy 1993;9:224-227.
Question 67High Yield
A child born with myelomeningocele is expected to be an ambulator with bracing. Examination by the consulting orthopaedic surgeon reveals rigid clubfeet in addition to the neurologic issues. Management should consist of
Explanation
Explanation
In a child with myelomeningocele, the guiding principle of treatment is to achieve a plantigrade foot by the time the child is ready to stand. The standard clubfoot protocol should be followed, but these children will require an aggressive surgical release to obtain a sufficient correction. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 65-78.
References:
- Kasser JE (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 503-514.
Question 68High Yield
Figure 21 shows the radiograph of a 32-year-old patient with right hip pain that has failed to respond to nonsurgical management. What is the most appropriate surgical treatment at this time?
Explanation
The radiograph reveals developmental dysplasia of both hips. The patient has classic anterolateral undercoverage of the femoral head on the right side as demonstrated by a high acetabular index (measured at 27 degrees). Anterior undercoverage can be determined by drawing the marking for the anterior wall that fails to overlap the femoral head in this patient. Currently in North America, the most accepted surgical management for symptomatic dysplasia of the hip with good joint space is a Bernese (Ganz) periacetabular osteotomy. Surgical dislocation of the hip and femoroacetabular osteoplasty may be considered for patients with symptomatic femoroacetabular impingement of the hip. Ganz R, Klaue K, Vinh TS, et al: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 69High Yield
A 12-year-old girl has had lower back pain for the past 6 months that interferes with her ability to participate in sports. She denies any history of radicular symptoms, sensory changes, or bowel or bladder dysfunction. Examination reveals a shuffling gait, restriction of forward bending, and tight hamstrings. Radiographs show a grade III spondylolisthesis of L5 on S1, with a slip angle of 20 degrees. Management should consist of
Explanation
Indications for surgical treatment of spondylolisthesis include pain and/or progression of deformity. Specifically, surgery is necessary when there is persistent pain or a neurologic deficit that fails to respond to nonsurgical therapy, there is significant slip progression, or the slip is greater than 50%. For patients with mild spondylolisthesis, in situ posterolateral L5-S1 fusion is adequate. In patients with more severe slips (greater than 50%), extension of the fusion to L4 offers better mechanical advantage. Postoperative immobilization may be achieved with instrumentation, casting, or both. In patients with a slip angle of greater than 45 degrees, reduction of the lumbosacral kyphosis with instrumentation or casting is desirable to prevent slip progression. Laminectomy alone is contraindicated in a child. Nerve root decompression is indicated if radiculopathy is present clinically. Seitsalo S, Osterman K, Hyvarinen H, Tallroth K, Schlenzka D, Poussa M: Progression of spondylolisthesis in children and adolescents: A long-term follow-up of 272 patients. Spine 1991;16:417-421.
Question 70High Yield
Figure 48 shows an MRI scan of the knee. The arrow is pointing to what structure?
Explanation
The arrow points to the biceps femoris, which is inserted onto the fibula. The biceps femoris lies at the posterolateral aspect of the thigh. The semimembranosus and the semitendinous lie at the posterior medial aspect of the thigh. Gray H: Anatomy of the Human Body. Philadelphia, PA, Lea and Febiger, 1918, 2000.
Question 71High Yield
A 75-year-old patient returns for follow-up after undergoing bilateral total hip arthroplasty (THA). The right hip is a hybrid THA performed 12 years ago, whereas the left hip is a cementless THA performed 10 years ago. Both acetabular components are the same type, same size, and from the same manufacturer. Both femoral heads are 28-mm cobalt-chromium components. What is the most likely explanation for the advanced polyethylene wear in one hip?
Explanation
Explanation
Over the past three decades, gamma irradiation and air has been the most common method of sterilizing polyethylene used in total joint arthroplasty. This method of sterilization results in breakage of the chemical bonds within the polymer. While this promotes cross-linking, it also leaves the polyethylene vulnerable to oxidation, especially if packaged in an air environment. Oxidation has been shown to decrease polyethylene's molecular weight, ultimate tensile strength, elongation, and toughness which results in a stiffer, more brittle material that is less resistant to wear. Severity of oxidation and a decrease in mechanical properties have been shown to be related to the length of time that the component is exposed to air (the shelf life). Currier and associates studied the clinical performance of gamma irradiated in air polyethylene components that had been shelf aged. They demonstrated that for the first 5 years of shelf life, polyethylene oxidized rather slowly. However, polyethylene components with a shelf life of more than 5 years would be expected to have minimal mechanical toughness and would likely fail rapidly if implanted. Bohl and associates evaluated 135 patients who had undergone total knee arthroplasty. Survivorship at 5 years was 100% for components with a shelf life of less than 4 years, 89% for components with a shelf life of 4 to 8 years, and 79% for components with a shelf life of more than 8 years. Sychterz and associates reported no correlation between shelf life and true wear rates for components with a shelf life of less than 3 years. In summary, both in vivo and in vitro data suggest that shelf life in excess of 3 to 5 years has a direct effect on wear of polyethylene. Currier BH, Currier JH, Collier JP, et al: Shelf life and in vivo duration: Impacts on performance of tibial bearings. Clin Orthop 1997;342:111-122. Bohl JR, Bohl WR, Postak PD, et al: The Coventry Award: The effects of shelf life on clinical outcome for gamma sterilized polyethylene tibial components. Clin Orthop 1999;367:28-38.
References:
- Sychterz CJ, Young AM, Orishimo K, et al: The relationship between shelf life and in vivo wear for polyethylene acetabular liners. J Arthroplasty 2005;20:168-173.
Question 72High Yield
Within the menisci, the majority of the large collagen fiber bundles are oriented in what configuration?
Explanation
The majority of large collagen fibers within the menisci are oriented circumferentially. It is these fibers that develop the hoop stress with compressive loading of the menisci. Most meniscal tears are longitudinal and occur between these circumferential fibers. Mow VC, et al: Structure and function relationships of the menisci of the knee, in Mow VC, Arnoczky SP, Jackson DW (eds): Knee Meniscus: Basic and Clinical Foundations. New York, NY, Raven Press, 1992, pp 37-57.
Question 73High Yield
Figures 28a and 28b show the radiographs of a 79-year-old man who has constant knee pain. Prior to performing elective knee replacement surgery, management should include
Explanation
Explanation
28b The radiographs show established Paget's disease. Bony expansion is evident, with thickened trabeculae consistent with the disordered bone remodeling process. A reduction of the serum alkaline phosphatase level to 50% of the pretreatment level may reduce pain from Paget's disease, and it is recommended prior to consideration of joint replacement. In elective cases, treatment of Paget's disease should begin at least 6 weeks prior to surgery. The other modalities are not related to the treatment of Paget's disease. Kaplan FS, Singer FS: Paget's disease of bone: Pathophysiology, diagnosis, and management. J Am Acad Orthop Surg 1995;3:336-344. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 129-184.
References:
- Siris ES: Paget's disease of bone, in Favus MJ (ed): Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism. New York, NY, Raven Press, 1993, pp 375-384.
Question 74High Yield
A 14-year-old patient has anterior knee pain. Radiographs, an MRI scan, and biopsy specimens are shown in Figures 6a through 6e. What is the most likely diagnosis?
Explanation
Explanation
6b 6c 6d 6e Although the imaging studies are consistent with a unicameral bone cyst, aneurysmal bone cyst, or giant cell tumor, the histology shows small round blue cells that are typical of Ewing's sarcoma. Although Ewing's sarcoma frequently occurs in the diaphysis, it can occur in the metaphysis.
References:
- Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989, vol 2, ch 18.
Question 75High Yield
A 12-year-old girl has had progressive left knee pain for the past 4 months. She reports that the pain is unrelated to activity, and she has no history of fever or recent infections. Examination reveals full range of motion of the knee but tenderness along the medial joint line. Plain radiographs and MRI scans are shown in Figures 39a through 39d. A biopsy specimen of the lesion is shown in Figure 39e. Treatment should include
Explanation
Explanation
39b 39c 39d 39e The lesion is a chondroblastoma. The plain radiographs show a well-defined radiolucent lesion in the distal femoral epiphysis of a skeletally immature patient. The margins are well defined, suggesting a benign growth. The epiphysis is an unusual location for bone tumors, except for chondroblastomas. Of all chondroblastomas, 95% are located within the epiphysis. The MRI scans show a punctate appearance that is commonly seen in cartilage lesions. The biopsy specimen shows a chondroid lesion with polygonal chondrocytes. These findings are consistent with a chondroblastoma. The natural history of chondroblastomas is for continued growth and bone destruction if left untreated. Treatment should consist of curettage, with or without the use of physical or chemical adjuvants, and bone grafting.
References:
- Springfield DS, Capanna R, Gherlinzoni F, Picci P, Campanacci M: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Question 76High Yield
A 22-year-old man reports anterior knee pain, swelling, and is unable to perform a straight leg raise after undergoing endoscopic anterior cruciate ligament (ACL) reconstruction with a bone-patellar tendon-bone autograft 1 week ago. He is afebrile. Examination reveals a clean incision, moderate effusion, a weak isometric quadriceps contraction, active knee range of motion of 5 degrees to 45 degrees, and the patella is ballottable. Knee radiographs show postoperative changes with good femoral and tibial tunnel placements, and normal patellar height. What is the next most appropriate step in management?
Explanation
Knee pain and swelling in the first week after ACL reconstruction is usually related to a postoperative hemarthrosis. A large hemarthrosis creates capsular distension, which inhibits active quadriceps contraction by a neurologic reflex, the H. reflex. Kennedy and associates reported that an experimentally induced knee effusion at 60 mL was found to result in profound inhibition of reflexly evoked quadriceps contraction. Removal of the hemarthrosis by aspiration will improve strength and often instantaneously restore the ability to contract the quadriceps muscle. A large effusion will also limit knee flexion. EMG and NCVS are not necessary unless there is a high index of suspicion of a femoral neuropathy. Diagnostic ultrasonography is not necessary in this patient but can be useful in the assessment of patellar tendon integrity. MRI is not indicated and would most likely be limited by artifact and postoperative changes. Continuous passive motion is not indicated and would most likely worsen the patient's symptoms. Kennedy JC, Alexander IJ, Hayes KC: Nerve supply of the human knee and its functional importance. Am J Sports Med 1982;10:329-335.
Question 77High Yield
Analysis of primary total hip arthroplasty using press-fit acetabular components without supplementary screw fixation reveals that screw fixation
Explanation
Using mechanical failure of fixation as the end point, Udomkiat and associates demonstrated a 12-year survivorship of 99.1% for titanium press-fit acetabular components without supplementary screw fixation. This study suggests that it is unlikely that the use of supplementary screws would lead to improved results. In addition, polyethylene wear debris tends to migrate through screw holes and along the course of screws. Screw holes also decrease the available surface for bone ingrowth. Screws that back up may be a source of backside polyethylene wear. This suggests that screw holes and the use of screws should be avoided when they are unnecessary for cup fixation.
Question 78High Yield
Osteophyte formation at the posteromedial olecranon and olecranon articulation in high-caliber throwing athletes is most often the result of underlying
Explanation
Explanation
During the late acceleration phase of throwing, the triceps forcibly contracts, extending the elbow as the ball is released. Normally, this force is absorbed by the anterior capsule and the brachialis and biceps muscles. However, if the ulnar collateral ligament is insufficient, the elbow will be in a subluxated position during extension and cause impaction of the olecranon and the olecranon fossa posteromedially. Over time, osteophyte formation is likely to occur. Conway JE, Jobe FW, Glousman RE, Pink M: Medial instability of the elbow in throwing athletes: Treatment by repair or reconstruction of the ulnar collateral ligament. J Bone Joint Surg Am 1992;74:67-83.
References:
- Wilson FD, Andrews, JR, Blackburn TA, McCluskey G: Valgus extension overload in the pitching elbow. Am J Sports Med 1983;11:83-88.
Question 79High Yield
A 30-year-old woman has had pain in her right leg for the past 6 months. A lytic lesion is noted in the anterior cortex of the midtibia, extending 5 cm in length without a soft-tissue mass. A radiograph and a biopsy specimen are shown in Figures 35a and 35b. What is the preferred treatment?
Explanation
Explanation
35b In an adult with an anterior cortical tibial lesion, this is the classic histologic appearance and anatomic location for an adamantinoma. The histology reveals areas of epithelial cells (in a glandular pattern) within a fibrous stroma. The epithelial cells are shown in nests. They would stain positively for keratin. Adamantinoma is a rare malignant bone tumor with a propensity for late metastasis. It has a high incidence of local recurrence unless resected with a wide margin. Chemotherapy and radiation therapy are not helpful in the treatment of this disease. Amputation generally is not necessary because a diaphyseal resection is usually possible. McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 263.
References:
- Moon NF, Mori H: Adamantinoma of the appendicular skeleton: Updated. Clin Orthop Relat Res 1986;204:215-237.
Question 80High Yield
A 29-year-old woman who underwent an anterior cruciate ligament (ACL) reconstruction 6 months ago now reports difficulty achieving full knee extension, and physical therapy fails to provide relief. The knee is stable on ligament testing. Figure 3 shows the findings at a repeat arthroscopy. Treatment should now include
Explanation
The patient has a cyclops lesion. This is a nodule of fibroproliferative tissue that originates from either drilling debris from the tibial tunnel or remnants of the ACL stump; more rarely it is the result of broken graft fibers. The treatment of choice is excision of the nodule and, if needed, additional notchplasty. Marked improvements in function and symptoms have been noted after removal of the extension block and resumption of a rehabilitation program. Delince P, Krallis P, Descamps PY, et al: Different aspects of the cyclops lesion following anterior cruciate ligament reconstruction: A multifactorial etiopathogenesis. Arthroscopy 1998;14:869-876.
Question 81High Yield
A 14-year-old boy has medial ankle pain, progressive unilateral flatfoot deformity, and pain with most activities of daily living. He denies any recent injury. His parents recall that at age 7 years he sustained an injury that was treated as a sprain. Examination reveals valgus deformity with painless, unrestricted passive motion of the ankle. He has grossly equal limb lengths. A radiograph of the affected ankle is shown in Figure 48a, and the contralateral ankle is shown in Figure 48b. Management should consist of
Explanation
Explanation
48b Angular deformities of the ankle can occur following physeal injury. While an orthosis may be beneficial, the deformity is at the level of the ankle rather than the hindfoot. An epiphysiodesis or physeal bar resection would not be indicated as the growth plates are closed. Correction of the angular deformity should level the ankle joint and normalize the weight-bearing stresses on the ankle. This is most easily achieved with a closing wedge distal tibial osteotomy with or without concomitant osteotomy of the fibula. Thompson DM, Calhoun JH: Advanced techniques in foot and ankle reconstruction. Foot Ankle Clin 2000;5:417-442. Ting AJ, Tarr RR, Sarmiento A, Wagner K, Resnick C: The role of subtalar motion and ankle contact pressure changes from angular deformities of the tibia. Foot Ankle 1987;7:290-299.
References:
- Tarr RR, Resnick CT, Wagner KS, Sarmiento A: Changes in tibiotalar joint contact areas following experimentally induced tibial angular deformities. Clin Orthop 1985;199:72-80.
Question 82High Yield
Kyphosis from a vertebral osteoporotic compression fracture often results in progressive kyphosis due to
Explanation
Explanation
Kayanja and associates, in a number of biomechanical studies, showed that in a kyphotic spine the strain is located at the apex of the deformity, the force is transmitted to the superior adjacent vertebrae, and that realignment and cement augmentation effectively normalize the load transfer. Kayanja MM, Ferrara LA, Lieberman IH: Distribution of anterior cortical shear strain after a thoracic wedge compression fracture. Spine J 2004;4:76-87. Kayanja MM, Togawa D, Lieberman IH: Biomechanical changes after the augmentation of experimental osteoporotic vertebral compression fractures in the cadaveric thoracic spine. Spine J 2005;5:55-63. Kayanja MM, Schlenk R, Togawa D, et al: The biomechanics of 1, 2, and 3 levels of vertebral augmentation with polymethylmethacrylate in multilevel spinal segments. Spine 2006;31:769-774.
Question 83High Yield
Figures 19a through 19c show radiographs of the cervical spine of an asymptomatic patient with Down syndrome who wants to participate in a Special Olympics running event. The neurologic examination is normal. Management should consist of
Explanation
Explanation
19b 19c An atlanto-dens interval (ADI) of up to 4 mm in children is considered normal. Children with Down syndrome have increased ligamentous laxity, with atlantoaxial instability occurring in as many as 15% to 20% of patients. These patients are at risk for catastrophic injury following minor trauma and should be routinely screened for instability, generally beginning when the patient starts to walk. Patients with an ADI of greater than 5 mm should avoid contact sports and high-risk activities such as gymnastics, diving, the high jump, and the butterfly stroke. The American Academy of Pediatrics Committee of Sports Medicine and Fitness guidelines recommend that lateral views of the cervical spine in neutral, flexion, and extension should be obtained in all children with Down syndrome who wish to participate in sports. Patients with normal radiographs and examinations do not need repeat radiographs, although some authors suggest that instability increases with age, and therefore recommend repeat radiographs every 5 years. Cervical spine fusion in patients with Down syndrome has a high rate of complications and should be performed only on patients with symptoms and evidence of myelopathy. American Academy of Pediatrics Committee of Sports Medicine and Fitness: Atlantoaxial instability in Down syndrome. Pediatrics 1995;96:151-154. Copley LA, Dormans JP: Cervical spine disorders in infants and children. J Am Acad Orthop Surg 1998;6:204-214.
References:
- Tredwell SJ, Newman DE, Lockitch G: Instability of the upper cervical spine in Down syndrome. J Pediatr Orthop 1990;10:602-606.
Question 84High Yield
A 42 year-old-woman who underwent surgery for lumbar scoliosis 2 years ago now has fixed sagittal plane imbalance and severe back pain. Which of the following is considered a contraindication to isolated pedicle subtraction osteotomy for the treatment of iatrogenic flatback syndrome in this patient?
Explanation
Pedicle subtraction osteotomy is the preferred osteotomy technique for the treatment of many patients with iatrogenic flatback syndrome. In the presence of an anterior pseudarthrosis, however, it must be done in conjunction with an anterior procedure. Prior laminectomy is not a contraindication. Significant correction, usually averaging about 30 degrees, can be obtained through each osteotomy. Osteotomies should be performed at L2 or below in the presence of kyphosis at the thoracolumbar junction. The pedicle subtraction technique is preferred with vascular calcifications because it does not lengthen the anterior column, which could risk vascular injury. Potter BK, Lenke LG, Kuklo TR: Prevention and management of iatrogenic flatback deformity. J Bone Joint Surg Am 2004;86:1793-1808.
Question 85High Yield
The vascular supply to the medial meniscus comes primarily from what artery?
Explanation
Explanation
The vascular supply to the medial and lateral menisci originates predominantly from the medial and lateral genicular arteries. The popliteal artery splits into the superior genicular, which splits into medial and lateral branches supplying the patellar cartilage and the posterior cruciate ligament. The middle genicular artery also supplies the anterior curciate ligament, posterior cruciate ligament, and collateral ligaments. The inferior genicular splits into medial and lateral branches and supplies the menisci and other knee ligaments. Despite propagation of incorrect terminology, there is no superior or lateral genicular artery.
References:
- Mow VC, Arnoczky SP, Jackson DW (eds): Knee Meniscus: Basic and Clinical Foundations. New York, NY, Raven Press, 1992, p 4.
Question 86High Yield
Figures 8a through 8c show the lateral radiograph and T1- and T2-weighted MRI scans of a 14-year-old soccer player who reports aching thigh pain. The next most appropriate step in management should consist of


Explanation
Although the MRI findings could be misinterpreted as an aggressive soft-tissue process, the periosteal-based ossification on the radiograph in an athlete most likely suggests myositis ossificans. The radiograph should be repeated to see further maturation of the ossification with a typical "zoning" pattern. The zoning pattern is one of peripheral ossification. This is often best seen on a CT scan. King JB: Post-traumatic ectopic calcification in the muscles of athletes: A review. Br J Sports Med 1998;32:287-290.
Question 87High Yield
The so-called high ankle sprain from an external rotation mechanism of injury typically involves injury to which of the following structures?
Explanation
Explanation
Ankle sprains most commonly involve injury to the lateral collateral ligaments of the ankle (anterior talofibular, posterior talofibular, and calcaneofibular) from an inversion mechanism of injury. A different entity has been more recently described that involves an external rotation mechanism of injury that widens the ankle mortise and disrupts the anterior inferior tibiofibular ligament. Deltoid ligament and extensor retinaculum injuries do occur, although infrequently, and involve eversion and extreme plantar flexion mechanisms, respectively. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 182. Kaye RA: Stabilization of ankle syndesmosis injuries with a syndesmosis screw. Foot Ankle 1989;9:290-293. Baxter DE: The Foot and Ankle in Sports. St Louis, MO, Mosby-Year Book, 1995, p 30.
References:
- Pfeffer GB (ed): Chronic Ankle Pain in the Athlete. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 11.
Question 88High Yield
Figure 5 shows the radiograph of a 10-year-old girl who reports chronic shoulder pain after her gymnastics classes. Examination reveals pain on internal and external rotation but no instability. What is the most likely diagnosis?
Explanation
The patient has a very wide humeral growth plate, indicating the presence of a proximal humeral stress fracture, an uncommon diagnosis in gymnasts. Gymnasts are prone to stress fractures of the scaphoid, distal radius, elbow, and clavicle. Proximal humeral stress fractures are more commonly seen in those participating in racket or throwing sports. Stress fractures can lead to growth arrest or inhibition, particularly in the distal radius. The radiograph shows normal findings for the acromion, acromioclavicular joint, scapula, and triceps origin. Fallon KE, Fricker PA: Stress fracture of the clavicle in a young female gymnast. Br J Sports Med 2001;35:448-449. Sinha AK, Kaeding CC, Wadley GM: Upper extremity stress fractures in athletes: Clinical features of 44 cases. Clin J Sports Med 1999;9:199-202. Caine D, Howe W, Ross W, Bergman G: Does repetitive physical loading inhibit radial growth in female gymnasts? Clin J Sports Med 1997;7:302-308.
Question 89High Yield
Figures 14a and 14b show the plain radiographs of an 85-year-old woman who has had severe pain in the right knee for the past 4 months. Management should consist of
Explanation
Explanation
14b The patient has osteonecrosis of the lateral femoral condyle with collapse of the articular surface. Because there is already collapse of the articular surface, a total knee arthroplasty is the treatment of choice. The results of total knee arthroplasty in these patients are usually excellent. However, knee replacement is only a resurfacing procedure, and some patients with global osteonecrosis of the distal femur may have residual pain after knee replacement. High tibial osteotomy may be indicated in younger patients who have a varus deformity and localized osteonecrosis. Arthroscopic surgery would provide minimal relief for this patient because there is already collapse of the articular surface. A hinged knee brace will not adequately unload the joint. An osteochondral allograft should be considered only for younger patients with localized osteonecrosis. Bergman NR, Rand JA: Total knee arthroplasty in osteonecrosis. Clin Orthop 1991;273:77-82.
References:
- Lotke PA, Abend JA, Ecker ML: The treatment of osteonecrosis of the medial femoral condyle. Clin Orthop 1982;171:109-116.
Question 90High Yield
What is the most common benign bone tumor in childhood?
Explanation
Explanation
The most common benign bone tumor in childhood is a nonossifying fibroma. It is estimated that 30% of children have a nonossifying fibroma. In most patients, the lesion is not identified until a radiograph is obtained for unrelated reasons. Similarly, most identified cases of fibrous cortical defect are not biopsied because the radiographic and clinical presentations are diagnostic. Aboulafia AJ, Kennon RE, Jelinek JS: Benign bone tumors of childhood. J Am Acad Orthop Surg 1999;7:377-388.
References:
- Biermann JS: Common benign lesions of bone in children and adolescents. J Pediatr Orthop 2002;22:268-273.
Question 91High Yield
A 4-year-old girl sustains an isolated spiral femoral fracture after falling from her tricycle. Management should consist of
Explanation
Immediate spica casting is ideal for younger children with uncomplicated femoral fractures that are the result of relatively low-energy injury. Surgical stabilization of pediatric femoral fractures is most commonly performed in children who are older than age 6 years or in children with other factors associated with their femoral fracture, such as concomitant head injury, open fracture, floating knee, severe comminution, or vascular injury. Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659. Sponseller PD: Surgical management of pediatric femoral fractures. Instr Course Lect 2002;51:361-365. Wright JG: The treatment of femoral shaft fractures in children: A systematic overview and critical appraisal of the literature. Can J Surg 2000;43:180-189.
Question 92High Yield
What are the most likely symptoms and examination findings related to the mass in zone 2 of Guyon's canal seen in Figure 17?
Explanation
Explanation
The lesion lies in zone II of the ulnar tunnel. In that zone the deep motor branch of the ulnar nerve is susceptible to compression. Distal to the hook of the hamate, the motor branch of the ulnar nerve dives deep to innervate the interossei as it begins to move from an ulnar to radial direction. Because of its course, it has little or no give in response to a mass effect from the floor of Guyon's canal. Ganglions are the most common cause of ulnar nerve entrapment in the wrist. Lesions in zone I can affect both sensory and motor aspects of the ulnar nerve as well as the motor innervation of the hypothenar muscles. Lesions at the elbow or mid-to-proximal forearm are associated with dorsal hand numbness and tingling. Kuschner SH, Gelberman RH, Jennings C: Ulnar nerve compression at the wrist. J Hand Surg Am 1988;13:577-580.
References:
- Posner MA: Compressive neuropathies of the ulnar nerve at the elbow and wrist. Instr Course Lect 2000;49:305-317.
Question 93High Yield
A 12-year-old boy who has had a 1-month history of right thigh pain and a limp reports worsening of the pain after a fall, and he can no longer walk or bear weight on the involved extremity. Radiographs of the pelvis reveal a slipped capital femoral epiphysis with moderate to severe displacement. While positioning the patient on the fracture table for screw fixation, partial reduction of the slip is achieved. No further reduction maneuvers are attempted, and the epiphysis is stabilized with a single cannulated screw. What complication is most likely to develop following this procedure?
Explanation
Explanation
Traditional classification of slipped capital femoral epiphyses is based on the following temporal criteria: acute (symptoms that persist for less than 3 weeks); chronic (symptoms that persist for more than 3 weeks); or acute on chronic (acute exacerbation of long-standing symptoms). A newer classification differentiates between a stable slip where weight bearing is possible, and an unstable slip if it is not. Reduction of an unstable slip often occurs unintentionally with induction of anesthesia and positioning of the patient for surgery. The rate of satisfactory results is lower primarily because of a much higher incidence of osteonecrosis following internal fixation of an unstable slip. Loder RT, Richards BS, Shapiro PS, Reznick LR, Aronson DD: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
References:
- Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 151-159.
Question 94High Yield
A 17-year-old high school track athlete has had progressive midfoot pain for the past 3 weeks that prevents him from running. Examination reveals pain over the tarsal navicular. Radiographs are normal, but a CT scan reveals a nondisplaced sagittally oriented fracture line. Management should consist of
Explanation
The patient has a nondisplaced stress fracture of the tarsal navicular. Weight bearing is associated with a high rate of nonunion; therefore, management should consist of immobilization and no weight bearing for 8 weeks. Delayed union or nonunion is treated by excision of sclerotic fracture margins and bone grafting, with or without internal fixation. Generally, CT should be repeated to document healing before permitting a return to sports. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
Question 95High Yield
A 39-year-old man has had a foot mass for the past several months. MRI scans are shown in Figures 78a through 78c. A core biopsy specimen reveals synovial sarcoma, and a staging chest CT scan is normal. Which of the following treatments offers the best local tumor control and expedites the patient's return to normal function?
Explanation
Explanation
78b 78c Certain histologic subtypes of soft-tissue sarcoma have been noted to arise preferentially in the hand and the foot, such as epithelioid sarcoma, clear cell sarcoma, and synovial sarcoma. Synovial sarcoma is the most common foot sarcoma. Frequently there is a delay in diagnosis because the lesions are rare. The lesions tend to occur in younger adults, typically between the ages of 15 and 40 years. Patients with hand and foot sarcomas have been described as having improved overall survival, but this is likely a result of the smaller size of tumors arising in these locations. In this patient, the tumor has grown to a substantial size and involves many of the bones of the midfoot. Limb salvage may be a possibility when incorporated into a multidisciplinary treatment program, but this will entail months of adjuvant treatment and significant morbidity. Amputation and early prosthetic fitting still have a role in management of some soft-tissue sarcomas, most frequently in the foot. Ferguson PC: Surgical considerations for management of distal extremity soft tissue sarcomas. Curr Opin Oncol 2005;17:366-369.
References:
- Scully SP, Temple HT, Harrelson JM: Synovial sarcoma of the foot and ankle. Clin Orthop Relat Res 1999;364:220-226.
Question 96High Yield
The mother of a 24-month-old girl reports that the child cannot rotate her right forearm. She also notes delayed development, with the child first walking at 18 months. The child has a five-word vocabulary and has not begun using simple phrases. Examination reveals that the right forearm is fixed in 80 degrees of pronation. The remainder of the examination of both upper extremities is otherwise normal. A radiograph is shown in Figure 41. Which of the following studies will best aid in diagnosis?
Explanation
Explanation
The patient has classic radioulnar synostosis. Patients with this disorder frequently have duplication of sex chromosomes. Synostosis is often seen in females with 48-XXXX or 49-XXXXX in association with delayed development and mental retardation. In males, it can be associated with 48-XXXY or 49-XXXXY. Radioulnar synostosis is not usually associated with muscle disorders, congenital heart disease, or renal anomalies. MRI of the forearm can reveal other soft-tissue anomalies, but this information is not particularly helpful in planning therapy. Osteotomy is sometimes indicated to improve rotational position of the wrist, but this patient's rotation is quite functional for everyday tasks, and rotational osteotomy is not indicated.
References:
- Rimoin DL, Connor JM, Pyeritz RE, Korf BR: Emery & Rimoin's Principles and Practice of Medical Genetics, ed 4. New York, NY, Churchill Livingstone, 2002, pp 1196-1197.
Question 97High Yield
Which of the following definitions best describes Batson's vertebral vein system?
Explanation
The venous plexus was described by Batson and helps to explain the common distribution of metastatic cells to the vertebrae, skull, ribs, and proximal long bones. Batson studied the vertebral vein system extensively by using contrast agents in human cadavers and live monkeys. Batson's plexus is a valveless system that allows retrograde embolism from the major organs such as the breast, prostate, lung, kidney, and thyroid. It is located within the thoracoabdominal cavity and has connections to the proximal long bones and an intercommunicating network of thin-walled veins with a low intraluminal pressure. Batson OV: Function of vertebral veins and their role in spread of metastases. Ann Surg 1940;112:138-149.
Question 98High Yield
What is the most common cause of the new onset of amenorrhea in a female endurance athlete who is not sexually active?
Explanation
Insufficient caloric intake caused by either a poor diet or an eating disorder is the most common cause for the loss of menses in a female athlete. In the face of adequate caloric intake, stress is unlikely to cause amenorrhea. Oral contraceptives control menses but do not eliminate it. Diabetes mellitus does not cause the new onset of amenorrhea. Pregnancy can be a cause in a sexually active athlete. Chromosomal abnormalities can result in delayed or absent menarche but not the onset of amenorrhea in a postmenarchal female. Constantini NW: Clinical consequences of amenorrhea. Sports Med 1994;17:213-223.
Question 99High Yield
A 2-year-old child is being evaluated for limb-length and girth discrepancy. As a newborn, the patient was large for gestational age and had hypoglycemia. Current examination shows enlargement of the entire right side of the body, including the right lower extremity and foot. The skin shows no abnormal markings, and the neurologic examination is normal. The spine appears normal. Radiographs confirm a 2-cm discrepancy in the lengths of the lower extremities. Additional imaging studies should include
Explanation
Explanation
The patient may have Beckwith-Wiedemann syndrome (BWS), which consists of exophthalmos, macroglossia, gigantism, visceromegaly, abdominal wall defects, and neonatal hypoglycemia. Hemihypertrophy develops in approximately 15% of patients with BWS. Patients with hemihypertrophy that is the result of BWS have a 40% chance of developing malignancies such as Wilms' tumor or hepatoblastoma; therefore, frequent ultrasound screening is recommended until about age 7 years. The absence of nevi and vascular markings helps to rule out other causes of hemihypertrophy, such as neurofibromatosis, Proteus syndrome, and Klippel-Trenaunay syndrome. Bone age estimations are not accurate at this young age but may become more useful later to help predict the timing of epiphysiodesis procedures. DeBaun MR, Tucker MA: Risk of cancer during the first four years of life in children from The Beckwith-Wiedemann Syndrome Registry. J Pediatr 1998;132:398-400. Ballock RT, Wiesner GL, Myers MT, et al: Hemihypertrophy concepts and controversies. J Bone Joint Surg Am 1997;79:1731-1738.
References:
- Carpenter CT, Lester EL: Skeletal age determination in young children: Analysis of three regions of the hand/wrist film. J Pediatr Orthop 1993;13:76-79.
Question 100High Yield
A 25-year-old semiprofessional football player sustains a hyperextension injury to the left foot. He is unable to bear weight. Examination reveals tenderness along the midfoot with swelling and plantar ecchymosis. Radiographs are negative. What is the next step in evaluation of this patient?
Explanation
Explanation
The patient has a suspected Lisfranc sprain based on the plantar ecchymosis. The first step in diagnosis is a dynamic radiographic study. This should include a physician-assisted midfoot stress examination or standing weight-bearing radiographs to evaluate for displacement. There is no evidence of compartment syndrome, and a bone scan, CT, and MRI are expensive tests that are not warranted. Early JS: Fractures and dislocations of the midfoot and forefoot, in Bucholz R, Heckman JD, Court-Brown CM (eds): Rockwood and Green's Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 2337-2400.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon