Ultimate Orthopedic Board Review: 100 High-Yield MCQs for ABOS, OITE, & FRCS
14 Apr 2026
103 min read
87 Views
Key Takeaway
This page offers 100 randomized high-yield multiple-choice questions specifically designed for ABOS, OITE, and FRCS orthopedic board exams. Sharpen your knowledge, identify key areas for improvement, and master critical concepts to confidently pass your certification tests. Start your comprehensive orthopedic surgery review today.
Optimizing the Femur Lateral Approach: Compre...
00:00
Start Quiz
Question 1High Yield
Within the menisci, the majority of the large collagen fiber bundles are oriented in what configuration?
Explanation
The majority of large collagen fibers within the menisci are oriented circumferentially. It is these fibers that develop the hoop stress with compressive loading of the menisci. Most meniscal tears are longitudinal and occur between these circumferential fibers. Mow VC, et al: Structure and function relationships of the menisci of the knee, in Mow VC, Arnoczky SP, Jackson DW (eds): Knee Meniscus: Basic and Clinical Foundations. New York, NY, Raven Press, 1992, pp 37-57.
Question 2High Yield
Figure 6 shows an object being held in an outstretched hand. To offset the moment created by the object (ignoring the weight of the forearm), the biceps must generate a force of
Explanation
Explanation
Answering this question requires understanding of two important biomechanics concepts. First, because neither the object being held in the hand nor the body is moving and, hence, their accelerations are zero, the problem is one of static equilibrium in which the sum of the moments acting on the body is zero. Second, a moment is the action of a force that causes an object to rotate about any point away from its line of action. The magnitude of the moment is the magnitude of the force multiplied by the perpendicular distance between the line of action and the point (often called the moment arm or lever arm). In this problem, two forces are causing moments about the elbow. The magnitude of the moment caused by the object in the hand is 5 N times 30 cm or 150 N-cm. To maintain equilibrium, the moment caused by the biceps force must also have a magnitude of 150 N-cm. Its moment arm is 2 cm, so the magnitude of the biceps force is 150 N-cm divided by 2 cm, which equals 75 N. In general, functional loads such as the object are always at a mechanical advantage (ie, have a longer moment arm) over the muscle. Therefore, muscles must generate large forces to overcome the moments caused by even small functional loads. An KN, Chao ES, Kaufman KR: Analysis of muscle and joint loads, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 1-14.
References:
- Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-143.
Question 3High Yield
A 7-year-old girl has pain and swelling of the right elbow after falling off her bicycle. Radiographs are shown in Figure 31. What is the most appropriate initial step in management?
Explanation
Explanation
Lateral condylar fractures are challenging to treat because of late displacement and development of a nonunion that may lead to valgus instability, pain, or tardy ulnar nerve palsy. Fractures such as this one with more than 2 mm of displacement on any radiographic view are prone to nonunion and should be stabilized. Fractures with less than 2 mm of displacement usually are stable and may be treated nonsurgically. In these patients, careful follow-up is recommended within several days of casting to check for fracture displacement. Arthrography or MRI may be helpful in these minimally displaced fractures. Fractures with an intact articular cartilage surface, such as noted on these studies, are unlikely to displace further. Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425. Attarian DE: Lateral condyle fractures: Missed diagnoses in pediatric elbow injuries. Mil Med 1990;155:433-434. Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
References:
- Badelon O, Bensahel H, Mazda K, et al: Lateral humeral condylar fractures in children: A report of 47 cases. J Pediatr Orthop 1988;8:31-34.
Question 4High Yield
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?
Explanation
The combination of an elbow dislocation and a fracture of the radial head and coronoid is known as a terrible triad injury. To restore elbow stability, each injury must be addressed. The nonreconstructable radial head fracture requires implant arthroplasty. Open reduction and internal fixation of the coronoid is also necessary as is repair of the lateral collateral ligament complex which is usually avulsed from the lateral epicondyle region. Ring D, Quintero J, Jupiter JB: Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002;84:1811-1815. Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Question 5High Yield
A 22-year-old college basketball player who was hit from behind while going up for a rebound is rendered immediately quadraparetic for approximately 10 minutes, followed by complete resolution of motor loss and return of full sensation. The radiograph and MRI scan of the cervical spine shown in Figures 2a and 2b reveal a canal diameter of 13 mm, loss of cerebrospinal fluid space about the spinal cord, and no signal change within the cord. What is the best course of action?

Explanation
The correct decision on return to sports participation after episodes of transient quadraparesis is controversial. Cantu and Mueller feel strongly that the loss of cerebrospinal fluid space about the spinal cord signifies an unacceptable risk for future spinal cord injury if the athlete returns to sports. However, Watkins and Torg and Lasgow have reported no evidence of increased spinal cord injury in athletes with narrow spinal canals, even in football. These authors suggest judgment be used in advising return to contact or high-energy sports and that the physician's responsibility is to give accurate and relevant information, allowing the athlete to make his or her own choice regarding return to sports participation. Cantu R, Mueller FO: Catastrophic spine injuries in football (1977-1989). J Spinal Disord 1990;3:227-231. Watkins RG: Neck injuries in football players. Clin Sports Med 1986;5:215-246. Torg JS, Lasgow SG: Criteria for return to contact activities following cervical spine injury. Clin Sports Med 1991;1:12-26.
Question 6High Yield
Figure 20 shows the radiograph of a 21-year-old college basketball player who jammed his left index finger on the rim. He reports pain and tenderness over the dorsum of the distal interphalangeal (DIP) joint. Examination reveals that he is unable to actively extend the DIP joint; however, the skin is intact. Management should consist of
Explanation
Explanation
Mallet fingers without DIP joint subluxation can be treated with extension splinting. Surgical fixation may be necessary in bony mallet injuries when the joint is subluxated. Size of the bony fragment, while often correlating with stability, is not always an indication for fixation. Buddy taping allows motion; therefore, the fragment will not heal in the appropriate position. Intermittent splinting with range-of-motion exercises also will not allow the fragment to heal in the appropriate position. Crawford GP: The molded polyethylene splint for mallet finger deformities. J Hand Surg Am 1984;9:231-237.
References:
- Wehbe MA, Schneider LH: Mallet fractures. J Bone Joint Surg Am 1984;66:658-669.
Question 7High Yield
Figures 5a and 5b show the radiographs of an 11-year-old boy who felt a pop and immediate pain in his right knee as he was driving off his right leg to jam a basketball. Examination reveals that the knee is flexed, and the patient is unable to actively extend it or bear weight on that side. There is also a large effusion. Management should include

Explanation
Fractures through the cartilage on the inferior pole of the patella, the so-called sleeve fracture, are often difficult to diagnose because of the paucity of ossified bone visible on the radiographs. If the fracture is missed and the fragments are widely displaced, the patella may heal in an elongated configuration that may result in compromise of the extensor mechanism function. The treatment of choice is open reduction and internal fixation using a tension band wire technique to achieve close approximation of the fragments and restore full active knee extension. Heckman JD, Alkire CC: Distal patellar pole fractures: A proposed common mechanism of injury. Am J Sports Med 1984;12:424-428.
Question 8High Yield
A 22-year-old professional ballet dancer reports a 3-month history of posterior ankle pain that occurs when she changes from a flat foot to pointe (hyperplantar flexed position). Examination does not elicit the pain with forced passive plantar flexion. A radiograph is shown in Figure 8. What is the most likely cause of the pain?
Explanation
Explanation
The most common causes of posterior ankle pain in ballet dancers are flexor hallucis longus tenosynovitis and os trigonum syndrome. Flexor hallucis longus tenosynovitis differs from a symptomatic os trigonum by the absence of pain with forced plantar flexion and the presence of pain with resisted plantar flexion of the great toe. The pain is often felt in the posterior ankle and can be associated with a snapping or triggering sensation. Os trigonum syndrome commonly occurs in ballet dancers who perform in a position of extreme plantar flexion. The pain occurs from entrapment of the os trigonum between the posterior portion of the talus and calcaneus. Hamilton WG, Geppert MJ, Thompson FM: Pain in the posterior aspect of the ankle in dancers: Differential diagnosis and operative treatment. J Bone Joint Surg Am 1996;78:1491-1500.
References:
- Khan K, Brown J, Way S, et al: Overuse injuries in classical ballet. Sports Med 1995;19:341-357.
Question 9High Yield
Which of the following is considered an important factor in improved cemented femoral stem survivorship?
Explanation
Cement technique, relative stem to canal size and position, stem design, surgical technique, and femoral anatomy are important factors in cemented stem survivorship. Varus stem position, a wide diaphyseal to metaphyseal ratio (stovepipe femur), thin cement mantles (1 mm or less), and nonrounded femoral stem designs are negative prognostic factors for stem survivorship. Precoating with methylmethacrylate has not been shown to provide any increased survivorship over nonprecoated stems. Noble PC, Collier MB, Maltry JA, Kamaric E, Tullos HS: Pressurization and centalization enhance the quality and reproducibility of cement mantles. Clin Orthop 1998;355:77-89. Crowninshield RD, Brand RA, Johnston RC, Milroy JC: The effect of femoral stem cross-sectional geometry on cement stresses in total hip reconstruction. Clin Orthop 1980;146:71-77.
Question 10High Yield
In what decade does the peak incidence of conventional osteosarcoma occur?
Explanation
Explanation
Conventional osteosarcoma most frequently occurs in the second decade, followed by the third decade. Approximately 70% to 75% of patients with osteosarcoma are between the ages of 10 and 25 years. Secondary osteosarcoma (arising in Paget's disease or radiation-induced) is seen in older adults. Simon MA, Springfield DS, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 266. Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989.
References:
- Wold L, et al: Osteogenic sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, p 14.
Question 11High Yield
What percent of patients initially diagnosed with classic, high-grade osteosarcoma of the extremity have visible evidence of pulmonary metastasis on CT of the chest?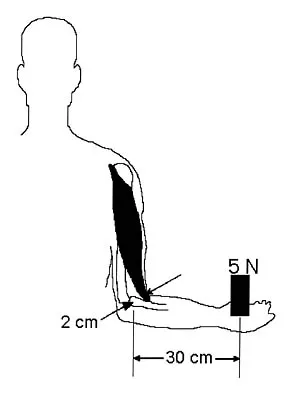
Explanation
CT studies show that approximately 10% to 20% of patients with high-grade osteosarcoma have pulmonary metastases at diagnosis. Although not visible on current staging studies, it is believed that up to 80% of patients have micrometastatic disease that requires systemic chemotherapy. Because it is not possible to identify those patients who do not have disseminated micrometastatic disease, most patients are treated presumptively with chemotherapy. Kaste SC, Pratt CB, Cain AM, et al: Metastases detected at the time of diagnosis of primary pediatric extremity osteosarcoma at diagnosis: Imaging features. Cancer 1999;86:1602-1608.
Question 12High Yield
A 27-year-old professional baseball pitcher who underwent arthroscopic olecranon debridement continues to have medial-sided elbow pain during late cocking. Physical examination reveals laxity and pain with valgus stress testing. What is the most likely cause of his pain?
Explanation
Both the medial collateral ligament and the olecranon contribute to valgus stability of the elbow. Excessive olecranon resection increases the demand placed on the medial collateral ligament in resisting valgus forces during throwing. Bone removal from the olecranon should be limited to osteophytes. Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 101-111.
Question 13High Yield
A 12-year-old girl sustains an acute injury to the right elbow in a fall. An AP radiograph is shown in Figure 5. Nonsurgical management will most likely result in
Explanation
The patient has a significantly displaced medial epicondyle fracture. The only absolute indication for surgical treatment is irreducible incarceration in the joint. Nonsurgical management usually results in a painless nonunion with good elbow function and little elbow instability. Prolonged immobilization should be avoided to prevent stiffness. Tardy ulnar nerve palsy and cubitus varus are not complications of medial epicondyle fractures. Chamber HG, Wilkins KE: Part IV: Apophyseal injuries of the distal humerus, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 801-812.
Question 14High Yield
A 45-year-old woman sustains an injury to her lower leg. Examination reveals that there is a deformity with no neurologic or vascular problems. The skin is intact. Radiographs are shown in Figures 46a and 46b. Which of the following factors would make closed management the least appropriate choice for this injury?
Explanation
Explanation
46b All the factors listed, with the exception of an ipsilateral femoral fracture, are representative of a low-energy stable tibial shaft fracture that will do well with closed reduction and immobilization in a long leg cast, followed by weight bearing as tolerated and then a functional brace or patellar tendon bearing cast until union is achieved. Shortening will not increase from that seen on these initial radiographs. The spiral fracture provides a broad surface for healing, and the fibular fracture at another level indicates a stable soft-tissue envelope which, with the immobilization device, will stabilize the fracture reduction. An ipsilateral femoral fracture is a strong indication to surgically stabilize both fractures. Trafton PG: Tibial shaft fractures, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 2153-2169.
References:
- Martinez A, Sarmiento A, Latta LL: Closed fractures of the proximal tibia treated with a functional brace. Clin Orthop 2003;417:293-302.
Question 15High Yield
The medial collateral ligament complex of the elbow originates on what portion of the medial epicondyle?
Explanation
The medial collateral ligament complex of the elbow consists of three portions: the anterior bundle, the posterior bundle, and a transverse component that has little biomechanic significance. The origin of the ligament is from the central two thirds of the anteroinferior undersurface of the medial epicondyle.
Question 16High Yield
A 16-year-old girl injured her hip in a fall. Radiographs are shown in Figures 14a and 14b. She denies any history of pain prior to the fall and is currently asymptomatic. A bone scan, MRI scan, and biopsy specimens are shown in Figures 14c through 14f. What is the most likely diagnosis?





Explanation
Although the classic radiographic appearance of fibrous dysplasia is one of a central metaphyseal lesion with ground glass matrix, it is not unusual to see either a more radiodense-appearing lesion or a more peripheral location. The histologic finding of spicules of woven bone without osteoblastic rimming in a bland fibrous background is diagnostic of fibrous dysplasia. The imaging studies could be consistent with low-grade osteosarcoma, osteoblastoma, or osteomyelitis, but all have a very different histologic picture. Observation is indicated in the absence of symptoms, impending fracture, or deformity. Fibrous dysplasia most commonly occurs in the proximal femur. Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 30-43.
Question 17High Yield
A 45-year-old man with a painful varus knee is being considered for an upper tibial osteotomy. Which of the following factors is considered the most compelling argument against this procedure?
Explanation
Proximal tibial osteotomy is appropriate for the younger and/or athletic patient who has mild to moderate medial compartment osteoarthritis. Relative contraindications include limited range of motion (eg, flexion contracture of 15 degrees), anatomic varus of greater than 10 degrees, advanced patellofemoral arthritis, and tibial subluxation. Inflammatory arthritides involve all the compartments and are a contraindication to osteotomies around the knee.
Question 18High Yield
Figure 50 shows the cross table lateral radiograph of a 31-year-old paratrooper who has recalcitrant groin pain. The pain is worse after activities such as standing or sitting (driving). Examination reveals that pain can be reproduced by internal rotation of the leg with the hip and knee in 90 degrees of flexion. Extensive nonsurgical managment has failed to provide relief. What is the treatment of choice?
Explanation
The radiograph reveals the classic "bump" that is seen in patients with femoroacetabular impingement (FAI). Ganz and associates described two types of FAI. This patient has cam impingement, which describes a nonspherical femoral head being forced into the acetabulum during hip motion and resulting in labral and chondral injury. Hip arthroscopy and labral debridement is unlikely to control the symptoms because the underlying anatomic abnormality is often difficult to address with arthroscopy. The treatment involves surgical dislocation of the hip with preservation of the blood supply to the femoral head, removal of the asphericity on the femoral side (femoral osteoplasty), and removal of the acetabular rim (acetabular osteoplasty) if the latter is found to contribute to impingement. Ganz R, Gill TJ, Gautier E, et al: Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-1124. Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for early osteoarthritis of the hip. Clin Orthop 2003;417:112-120.
Question 19High Yield
What is the most commonly reported complication following elbow arthroscopy?
Explanation
Explanation
The complication rate following elbow arthroscopy is reported at 5%. The most commonly reported complication is transient neurapraxia, with nerve transection remaining an unfortunate and rare event. While infection remains the most common serious complication, it is uncommon (0.8%). Synovial cutaneous fistula and compartment syndrome, while reported, are the least frequent complications of elbow arthroscopy. Kelly EW, Morrey BF, O'Driscoll SW: Complications of elbow arthroscopy. J Bone Joint Surg Am 2001;83:25-34.
References:
- Morrey BF: Elbow complication, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 519-522.
Question 20High Yield
A 42-year-old patient undergoes resection of the medial clavicle for painful sternoclavicular degenerative joint disease. The postoperative course is complicated by an increase in symptoms, a medial bump, and subjective tingling in the digits. A clinical photograph and radiograph are shown in Figures 20a and 20b. What is the most appropriate procedure at this time?

Explanation
Improved peak-to-load failure data have been demonstrated by reconstruction of the sternoclavicular joint using a semitendinosis graft in a figure-of-eight pattern through the clavicle and manubrium. Resection of the medial clavicle, which compromises the integrity of the costoclavicular ligament, results in medial clavicular instability. Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 608-609.
Question 21High Yield
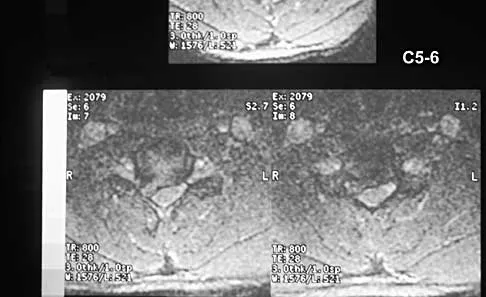
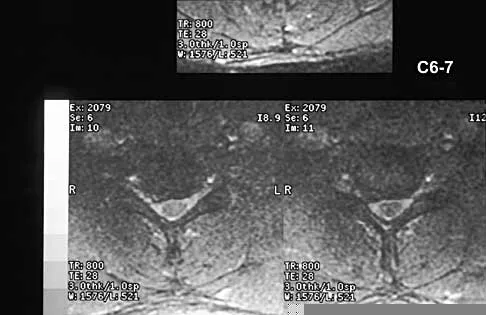
A 51-year-old woman with no preoperative neurologic deficit is undergoing elective anterior cervical diskectomy and fusion (ACDF) with plating and fusion for a C5-6 disk herniation with right-sided neck pain. Thirty minutes into the surgery the neurophysiologic monitoring shows a rapid drop and then loss of amplitude in the right cortical somatosensory-evoked potential waveform. All other waveforms remained normal and unchanged, including right-sided cervical (subcortical) and peripheral (Erb's point), and those from the left-sided upper extremity and both lower extremities. What is the most likely cause of the change?
Explanation
Explanation
The change noted is focal and confined to the cortex, sparing the opposite side, both lower extremities, and the subcortical waveforms, making all the choices unlikely with the exception of carotid compression with focal cortical ischemia. This may be associated with poor collateral flow from the opposite hemisphere due to an incomplete circle of Willis. Drummond JC, Englander RN, Gallo CJ: Cerebral ischemia as an apparent complication of anterior cervical discectomy in a patient with an incomplete circle of Willis. Anesth Analg 2006;102:896-899.
Question 22High Yield
Figure 13 shows the MRI scan of a 29-year-old rock climber who reports increasing shoulder pain and weakness. Based on these findings, atrophy will most likely occur in which of the following muscles?
Explanation
Explanation
The MRI scan shows a cyst at the spinoglenoid notch. These cysts are often associated with a labral injury, such as a superior labrum anterior and posterior (SLAP) lesion. The suprascapular nerve passes through the suprascapular notch and sends motor branches to the supraspinatus and sensory branches to the capsule. At the spinoglenoid notch, the infraspinatus branch of the suprascapular nerve is compressed by the cyst, leading to isolated infraspinatus atrophy. The teres minor and the deltoid are innervated by the axillary nerve. Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734. Ianotti JP, Ramsey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
References:
- Tirman PF, Feller JF, Janzen DL, Peterfy CG, Bergman AG: Association of glenoid labral cysts and labral tears in glenohumeral instability: Radiologic findings and clinical significance. Radiology 1994;190:653-658.
Question 23High Yield
Figures 26a and 26b show the radiograph and MRI scan of a 22-year-old man with knee pain. What is the most likely diagnosis?
Explanation
Explanation
26b The lesion is an osteochondroma. This is demonstrated by a pedunculated bone-forming lesion where the medullary space of the lesion communicates with the medullary space of the host bone. The cortex of the exostosis is in continuity with the cortex of the underlying bone. The MRI scan reveals that there is no significant cartilage cap, alleviating concern for malignant conversion to a chondrosarcoma. Osteoblastoma and osteosarcoma typically have mixed areas of bone formation and bone destruction. Malignant fibrous histiocytoma of bone is usually purely lytic. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
References:
- Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Question 24High Yield
A 28-year-old female firefighter fell from the top of a three-story building in the line of duty. She sustained a displaced pelvic fracture with more than 5 mm displacement. Compared to normal healthy controls, these patients have a higher incidence of
Explanation
Explanation
Pelvic trauma in women has been shown to increase the risk of sexual dysfunction and dyspareunia. Additionally, caesarean section childbirth is almost universal following pelvic trauma regardless of whether anterior pelvic hardware is present or not. Copeland CE, Bosse MJ, McCarthy ML et al: Effect of trauma and pelvic fracture on female genitourinary, sexual, and reproductive function. J Orthop Trauma 1997;11:73-81.
Question 25High Yield
A 59-year-old woman who underwent a total hip arthroplasty 5 years ago now has recurrent dislocation following bariatric surgery and a weight loss of 200 lb. An attempt at converting to a larger head size and trochanteric advancement has failed. Her components are well aligned. What is the best course of action?
Explanation
Explanation
When a patient has well-aligned components and soft-tissue tensioning with a larger femoral head and trochanteric advancement has failed, options are limited. The use of a constrained acetabular liner is the best option in this situation. Goetz and associates and Shrader and associates have demonstrated good results with these implants. Shrader used this device on 109 patients with recurrent instability with a successful outcome in all but 2 patients. Resection arthroplasty is a salvage situation and is not the best option at the present time. A hip abduction brace does not address the soft-tissue laxity. Conversion to a bipolar arthroplasty, although possibly minimizing the incidence of dislocation, will lead to groin pain and migration of the component with diminished functional results. Goetz DD, Capello WN, Callaghan JJ, et al: Salvage of recurrently dislocating hip prosthesis with use of a constrained acetabular component: A retrospective analysis of fifty-six cases. J Bone Joint Surg Am 1998;80:502-509. Shrader MW, Parvizi J, Lewallen DG: The use of constrained acetabular component to treat instability after total hip arthroplasty. J Bone Joint Surg Am 2003;85:2179-2183.
References:
- Hamilton WG, McAuley JP: Evaluation of the unstable total hip arthroplasty. Inst Course Lect 2004;53:87-92.
Question 26High Yield
A 14-year-old boy reports pain in the distal thigh. He denies any history of trauma. Examination reveals tenderness and swelling of the distal thigh without effusion. A radiograph and CT scan are shown in Figures 10a and 10b. A biopsy specimen is shown in Figure 10c. Management should consist of
Explanation
Explanation
10b 10c Based on these findings, the patient has an aneurysmal bone cyst. Frequently, fluid-fluid levels can be detected on MRI or CT images. The histologic results show a lesion that consists of cavernous spaces filled with blood. The lining of the cavity contains spindle cells, multinucleated giant cells, and reactive bone. Curettage and bone grafting is the preferred treatment method. Without treatment, these lesions can become quite large and destructive. Radiation therapy is not recommended for resectable lesions. Chemotherapy is not required for these benign lesions. Simon MA, Springfield DS, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-200.
References:
- Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, p 232.
Question 27High Yield
A 52-year-old man has shoulder pain and stiffness after undergoing a "mini-lateral" rotator cuff repair 6 months ago. Examination reveals that he is afebrile with normal vital signs. There is slight erythema but no drainage from the incision. Range of motion is limited in all planes, and there is weakness with resisted external rotation and abduction. Radiographs show a well-positioned metal implant within the greater tuberosity. Laboratory studies reveal a WBC count of 8,400/mm3 (normal 3,500 to 10,500/mm3) and an erythrocyte sedimentation rate of 63 mm/h (normal up to 20 mm/h). What is the next most appropriate step in management?
Explanation
Explanation
Deep sepsis of the shoulder following rotator cuff repair is an uncommon problem. Patients with infections of this type typically report persistent pain and are not systemically ill. They may have signs of local wound problems such as erythema, drainage, and dehiscence. Laboratory studies can be helpful in making an accurate diagnosis. Most patients will not show a significant elevation of the WBC count; however, an elevated erythrocyte sedimentation rate is nearly always present and should alert the clinician to the presence of infection. Aspiration of both subacromial and glenohumeral joint spaces is necessary to confirm the diagnosis. The most effective treatment for deep shoulder sepsis following rotator cuff repair involves extensive surgical debridement, removing all suspicious soft tissue as well as implants. Administration of appropriate antibiotic therapy is needed for complete control of the infection. Mirzayan R, Itamura JM, Vangsness CT, et al: Management of chronic deep infection following rotator cuff repair. J Bone Joint Surg Am 2000;82:1115-1121. Settecerri JJ, Pitnu MA, Rock MG, et al: Infection after rotator cuff repair. J Shoulder Elbow Surg 1994;8:105.
References:
- Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Question 28High Yield
Which of the following procedures is included in third-generation cement technique?
Explanation
Explanation
The so-called third-generation cement technique adds porosity reduction techniques, centralization devices, and surface modifications to the femoral component. The surgeon must be aware of the meaning of the various generations of cement technique when interpreting the results presented at meetings and in the literature. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 181-193.
References:
- Maloney WJ, Hartford JM: The cemented femoral component, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, vol 2, pp 959-979.
Question 29High Yield
When a structure like a long bone is under a bending load, its maximum stress is most dependent on what factor?
Explanation
The maximum stress in a bone occurs at the periosteal surface (the greatest distance from the center of the bone). The magnitude of the stress is equal to the magnitude of the applied moment (M) multiplied by the distance to the surface (roughly the radius of the bone, r) divided by the area moment of inertia (I), so that stress = Mr/I. Of the possible answers, only area moment of inertia of the cross section contains any of these three items. The stress can also depend on the length of the bone, but it cannot be determined without knowing the location at which the bending load is applied, information that was not given in the problem. The type of structural support may influence local stresses where the support contacts the bone, but it has little effect on the maximum stress in the bone. The cross-sectional area is not as important as the area moment of inertia because the stress is not evenly distributed over the cross-section. Plastic modulus is a material property, not a geometric or structural property, and it does not affect stress. Hayes WC, Bouxsein ML: Biomechanics of cortical and trabecular bone: Implications for assessment of fracture risk, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 76-82.
Question 30High Yield
Figure 11a shows the AP pelvis radiograph of a 25-year-old man who sustained a spinal cord injury 10 years ago. A bone scan and a CT scan are shown in Figures 11b and 11c. To prevent recurrence after resection, management should consist of


Explanation
The studies reveal significant heterotopic ossification that appears to be mature. Following resection, the most reliable way to prevent recurrence is with low-dose external-beam radiation therapy. Bisphosphonate therapy can be considered; however, when terminated, heterotopic bone may reform. Heterotopic ossification is unrelated to the patient's endocrine status and is not associated with any metabolic abnormalities. Moore K, Goss K, Anglen J: Indomethacin versus radiation therapy for prophylaxis against heterotopic ossification in acetabular fracture. J Bone Joint Surg Br 1998;80:259.
Question 31High Yield
The wear resistance of ultra-high molecular weight polyethylene can be improved by exposing the polymer to high-energy radiation (eg, gamma or electron beam), followed by a thermal treatment. What is one detrimental side effect of this process?
Explanation
Explanation
Highly cross-linked polyethylene has gained widespread acceptance for joint arthroplasty components because of reported experimental and early clinical accounts of significant reductions in wear. Cross-linking is increased by imparting additional energy into the polymer (above that conventionally used for sterilization). The thermal treatments after cross-linking stabilize the material against oxidative degradation by quenching free radicals and also reduce the elastic modulus. One disadvantage of the increased cross-linking is a reduction in toughness that makes the polyethylene more susceptible to crack initiation and propagation. The reduced toughness raises concerns for gross component fracture and fracture at stress concentrations that can arise with the locking mechanisms used to secure polyethylene inserts into metallic backings. Nonconsolidated polyethylene particles have been associated with increased subsurface density secondary to oxidative degradation in conventional polyethylene implants. The quenching of free radicals by thermal treatment in highly cross-linked polyethylene should prevent this problem. Collier JP, Currier BH, Kennedy FE, et al: Comparison of cross-linked polyethylene materials for orthopaedic applications. Clin Orthop 2003;414:289-304. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 203-208.
References:
- Wright TM, Maher SA: Biomaterials, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 32High Yield
What are the most common portals for arthroscopic surgery of the ankle?
Explanation
Explanation
The most commonly used portals are the anterolateral, anteromedial, and posterolateral portals. They have been shown to be the safest areas for portal placement, allowing no penetration of neurovascular structures. All the other portals involve placing another structure at risk. The anterocentral portal is close to the deep peroneal nerve and anterior tibular artery. The trans-Achilles portal is not recommended because of its limited utility and potential to injure the Achilles tendon. The posteromedial portal is too close to the posterotibial artery and nerve, the flexor hallucis longus and flexor digitorum longus tendons, and the branches of the calcaneal nerve. Stetson WB, Ferkel RD: Ankle arthroscopy: I. Technique and complications. J Am Acad Orthop Surg 1996;4:17-23.
References:
- Ferkel RD: Diagnostic arthroscopic examination, in Ferkel RD, Whipple TL (eds): Arthroscopic Surgery: The Foot and Ankle. Philadelphia, PA, Lippincott-Raven, 1996, pp 103-118.
Question 33High Yield
A 15-year-old boy has hindfoot pain and very limited subtalar motion. A CT scan reveals a talocalcaneal coalition involving 40% of the middle facet. He has no degeneration of the posterior subtalar facet. Following failure of nonsurgical management, treatment should consist of
Explanation
Explanation
The CT scan is an important test to help determine the extent of involvement of the talocalcaneal facet in a talocalcaneal coalition. In a young patient with no arthritis and joint involvement of less than 50%, resection of the coalition and fat pad interposition has been shown to be successful. A calcaneal osteotomy does not address the coalition. Subtalar arthroereisis has been used for treatment of a flexible flatfoot; tarsal coalition patients have a rigid-type flatfoot deformity. Sullivan JA: The child's foot, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 2, pp 1077-1135.
References:
- Scranton PE Jr: Treatment of symptomatic talocalcaneal coalition. J Bone Joint Surg Am 1987;69:533-539.
Question 34High Yield
When 6 weeks of noninvasive nonsurgical management fails to provide relief for a lumbar disk herniation, a trial of epidural steroid injections is likely to yield which of the following results?
Explanation
Explanation
Lumbar epidural steroid injections appear to play a role in management of a lumbar disk herniation that has failed to respond to at least 6 weeks of nonsurgical treatment. Approximately 42% to 56% of patients report significant pain relief compared with 92% to 98% of those patients treated with diskectomy. Patients with extruded or sequestered herniations report the greatest and most rapid relief. Similarly, those with well-hydrated disk fragments report rapid relief of symptoms. A smaller percentage of patients report symptom relief compared with those having surgery, but the degree of improvement is similar for both groups and the improvement lasts up to 3 years. Butterman GR: Treatment of lumbar disc herniation: Epidural steroid injection compares with discectomy: A prospective, randomized study. J Bone Joint Surg Am 2004;86:670-679.
References:
- Butterman GR: Lumbar disc herniation regression after successful epidural steroid injection. J Spinal Disord Tech 2002;15:469-476.
Question 35High Yield
In providing culturally competent care to a Muslim woman with a cervical spine injury, which of the following most accurately describes the steps a male orthopaedist should take to respect her religious beliefs during his examination?
Explanation
Explanation
In examining a traditional Muslim woman, a male physician should have another woman present, and the patient's husband, if possible. Only the affected limb or area needing examination should be exposed.
Question 36High Yield
What complication is more likely following excessive medial retraction of the anterior covering structures during the anterolateral (Watson-Jones) approach to the hip?
Explanation
The femoral nerve is the most lateral structure in the anterior neurovascular bundle. The femoral artery and vein lie medial to the nerve. Retractors placed in the anterior acetabular lip should be safe, although neurapraxia of the femoral nerve may occur if retraction is prolonged or forceful leading to quadriceps weakness. The femoral artery and nerve are well protected by the interposed psoas muscle. Damage to the lateral femoral cutaneous nerve, causing numbness over the anterolateral thigh, can occur while developing the interval between the tensor fascia latae and sartorious in the anterior (Smith-Petersen) approach but less likely in the Watson-Jones approach. Superior gluteal injury and accompanying abductor insufficiency may occur during excessive splitting of the glutei during the direct lateral (Hardinge) approach. Foot drop secondary to sciatic injury is more common with a posterior exposure or posterior retractor placement. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 325.
Question 37High Yield
A 5-year-old girl has had a low-grade fever, right hip and buttock pain, and a right-sided limp for the past 5 days. Examination shows diffuse tenderness and extreme pain on range of motion of the hip. Laboratory studies show a peripheral WBC count of 13,500/mm3 and an erythrocyte sedimentation rate of 55 mm/h. A radiograph is shown in Figure 46a, and an axial postgadolinium T1-weighted MRI scan with fat suppression and an axial T2-weighted fast spin echo MRI scan are shown in Figures 46b and 46c. What is the most likely diagnosis?


Explanation
MRI findings of acute osteomyelitis include a decrease in the normally high signal intensity of bone marrow on T1-weighted imaging; however, a postgadolinium T1-weighted image with fat suppression will show osteomyelitis as a bright marrow signal compared to the surrounding fat. Osteomyelitis is also brighter than normal fat on T2-weighted imaging. There is no rim-enhancing lesion suggesting an abscess, although myositis is seen in the obturator internus and short external rotators. The clinical scenario and imaging studies do not support the diagnosis of septic hip, eosinophilic granuloma, or pelvic fracture. Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Question 38High Yield
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?
Explanation
The MRI scan shows a far lateral disk herniation. With the L4-5 disk, a far lateral herniation abuts the left L4 nerve root. The findings would be consistent with those of a left L4 radiculopathy and would include pain or a sensory deficit on the anteromedial aspect of the knee, diminished patellar tendon reflex, and quadriceps weakness, perhaps making it difficult to walk up and down stairs. Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
Question 39High Yield
Which of the following malignant tumors most commonly contains soft-tissue calcifications seen on radiographs or CT?
Explanation
Focal calcifications causing small radiopacities are found in 15% to 20% of synovial sarcomas. Their irregular contours differentiate them from the phleboliths found in a benign hemangioma. Ewing's sarcoma, clear cell sarcoma, and malignant fibrous histiocytoma do not commonly have calcifications within the lesions. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 761.
Question 40High Yield
When converting the knee shown in Figure 20 to a total knee arthroplasty, satisfactory outcome can be expected in what percent of patients?
Explanation
Naranja and associates reviewed 37 knees (35 patients, with 28 women and 7 men) without any motion that were converted to total knee arthroplasties. After an average follow-up of 90 months, the patients lacked an average of 7 degrees of extension and had 62 degrees of flexion. Results showed a short-term complication rate of 24% (stiffness requiring manipulation, delayed wound healing, and recurrent hemarthrosis), a major complication rate of 35% (patellar tendon or tibial tubercle avulsion, persistent pain requiring arthrodesis, loosening, and joint stiffness requiring arthrotomy for excision of scar tissue), and an infection rate of 14%. The total complication rate was 57%. A satisfactory outcome (no pain and an unlimited ambulation distance) was obtained in only 10 patients (29%). There was no relationship between results and the angle at which the knee was ankylosed preoperatively. This study revealed that although success in reconstructing a previously ankylosed or arthrodesed knee is possible, the lack of consistent adequate motion and the complication rate may suggest that the surgeon reconsider the risks and benefits of this difficult procedure.
Question 41High Yield
Figure 43 shows the lateral radiograph of a 12-year-old boy with mild osteogenesis imperfecta who injured his left elbow after pushing his brother. Treatment should consist of
Explanation
The patient has a displaced fracture of the apophysis of the olecranon for which most authorities recommend surgical treatment. In older children, stability of the reduction may be achieved by the use of two parallel medullary Kirschner wires and a figure-of-8 tension band loop of either stainless steel wire or absorbable suture. The use of an absorbable suture does not require removal of the implant. Absorbable suture alone is best used in very young patients who have this type of injury. An intramedullary screw would pose an unnecessary risk of future growth disturbance. A displaced, isolated fracture of the apophysis of the olecranon is an unusual injury in a child. It has been suggested by several authors that children who have osteogenesis imperfecta may be especially prone to this injury. One study reported seven of these fractures occurring in five children who had the mild form of osteogenesis imperfecta (Sillence type IA). The authors of this study suggest that the diagnosis of osteogenesis imperfecta be considered in any child who has a displaced fracture of the apophysis of the olecranon, especially when the injury is associated with relatively minor trauma. Stott NS, Zionts LE: Displaced fractures of the apophysis of the olecranon in children who have osteogenesis imperfecta. J Bone Joint Surg Am 1993;75:1026-1033. Gaddy BC, Strecker WB, Schoenecker PL: Surgical treatment of displaced olecranon fractures in children. J Pediatr Orthop 1997;17:321-324.
Question 42High Yield
A 14-year-old competitive gymnast has had activity-related low back pain for the past month. Examination reveals no pain with forward flexion, but she has some discomfort when resuming an upright position. She also has pain with extension and lateral bending of the spine. The neurologic examination is normal. Popliteal angles measure 20 degrees. AP, lateral, and oblique views of the lumbar spine are negative. What is the next most appropriate step in management?
Explanation
Symptoms of activity-related low back pain, physical findings of pain with extension, lateral bending, and resuming an upright position, and relative hamstring tightness are consistent with spondylolysis. While the initial diagnostic work-up should include plain radiographs of the lumbosacral spine, the findings may be negative because it can take weeks or months for the characteristic changes to become apparent. SPECT has been a useful adjunct in the diagnosis of spondylolysis when plain radiographs are negative. Since the patient's pain is activity related and she is otherwise healthy, evaluation for infection is not indicated. Because the neurologic examination is normal, electromyography, nerve conduction velocity studies, and MRI are not indicated. CT can be used in those instances in which SPECT and bone scans are negative. Ciullo JV, Jackson DW: Pars interarticularis stress reaction, spondylolysis, and spondylolisthesis in gymnasts. Clin Sports Med 1985;4:95-110. Collier BD, Johnson RP, Carrera GF, et al: Painful spondylolysis or spondylolisthesis studied by radiography and single photon emission computed tomography. Radiology 1985;154:207-211. Jackson DW, Wiltse LL, Cirincione RT: Spondylolysis in the female gymnast. Clin Orthop 1976;117:68-73.
Question 43High Yield
A 19-year-old college football player reports persistent weakness, tingling, and numbness of both upper extremities at half time. He states that these symptoms initially occurred after tackling an opposing player with his head early in the game. History reveals that he has had "burners" in the past that typically resolved within 15 to 30 minutes. Examination reveals pain-free cervical motion, weakness to shoulder abduction testing bilaterally, normal upper extremity reflexes, and decreased sensation over both shoulders and the upper arms. Appropriate initial management should consist of
Explanation
The player's symptoms represent more than the mere "burner syndrome," which leads to unilateral symptoms that typically last less than 1 minute. Return to play following a burner is allowed following nonsurgical management and once the symptoms have subsided and the player exhibits normal strength and motion of the neck and upper extremities. This player has the history, symptoms, and examination findings that are consistent with cervical neurapraxia. Return to play in contact sports is contraindicated with bilateral symptoms prior to MRI evaluation of the cervical spine. CT of the brain is indicated with a history of loss of consciousness or other symptoms suggestive of a concussion. Torg JS, Sennett B, Pavlov H, et al: Spear tackler's spine: An entity precluding participation in tackle football and collision activities that expose the cervical spine to axial energy inputs. Am J Sports Med 1993;21:640-649. Torg JS: Cervical spinal stenosis with cord neurapraxia and transient quadriplegia. Sports Med 1995;20:429-434.
Question 44High Yield
Figure 22 shows the radiograph of a 7-year-old boy who underwent retrograde elastic nailing of a femoral shaft fracture. What is the most common problem following this procedure?
Explanation
Explanation
Several large clinical studies have shown that the most common problem after elastic nailing of a femoral shaft fracture is persistent pain and irritation at the nail insertion site. Unacceptable shortening and malunion are very rare in a 7-year-old patient. Rotational malalignment also is unusual. Osteonecrosis has been reported in solid antegrade nailing but not with elastic nailing of femoral shaft fractures in skeletally immature patients. Flynn JM, Luedtke LM, Ganley TJ, et al: Comparison of titanium elastic nails with traction and a spica cast to treat femoral fractures in children. J Bone Joint Surg Am 2004;86:770-777. Flynn JM, Hresko T, Reynolds RA, et al: Titanium elastic nails for pediatric femur fractures: A multicenter study of early results with analysis of complications. J Pediatr Orthop 2001;21:4-8.
References:
- Ligier JN, Metaizeau JP, Prevot J, et al: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77.
Question 45High Yield
A 56-year-old mechanic has had pain in the hypothenar region of his dominant right hand for the past 6 months. He reports weakness in his grip and pain is worse with activity. Which of the following examination findings is most suggestive of a cervical etiology?
Explanation
Hypothenar atrophy is a nonspecific sign that can be seen in ulnar neuropathy, C8 radiculopathy, or even cervical myelopathy; however, the atrophy usually is not unilateral and includes other muscle groups. The Spurling test is an excellent method of eliciting cervical radicular pain but involves hyperextension and ipsilateral rotation of the cervical spine, resulting in nerve root compression by reducing the cross-sectional area of the ipsilateral neuroforamen. Tinel's sign at the levator scapulae, if present, is indicative of an upper cervical (C3 or C4) radiculopathy. A subluxable ulnar nerve at the cubital tunnel, while often asymptomatic, points toward cubital tunnel syndrome as an etiology for this patient's pain. The shoulder abduction relief (SAR) sign (relief of upper extremity pain with shoulder abduction) is virtually pathognomic of cervical radiculopathy because this maneuver results in relaxation of a compressed and/or inflamed cervical nerve root. The SAR sign is the converse analog of the straight leg raising sign in the lumbar examination for lumbar radiculopathy, as it relieves tension in the nerve root, thereby relieving symptoms. Ducker TB, Zeidman SM: Neurologic and functional evaluation, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 143-161. An HS: Clinical presentation of discogenic neck pain, radiculopathy, and myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 755-764.
Question 46High Yield
A patient with degenerative osteoarthritis of the sternoclavicular (SC) joint reports constant pain, discomfort, and marked prominence and instability of the SC joint following medial clavicle resection. Which of the following procedures is most likely to produce these signs and symptoms?
Explanation
Medial clavicle excision alone can be associated with postoperative instability of the clavicle. The clavicle should be stabilized to the first rib by reconstructing the costoclavicular ligament if it is torn or if the resection is lateral to its clavicular insertion. Therefore, care must be taken to resect only that part of the clavicle that is medial to the costoclavicular ligament. Adequate protection for vital structures that lie posterior to the medial end of the clavicle must be provided. Bremner RA: Nonarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Question 47High Yield
A 40-year-old carpenter has a 3-month history of right arm pain and neck pain that now leaves him unable to work. Examination reveals a positive Spurling test, weakness of the biceps, and a mildly positive Hoffman's sign on the right side. Electromyography and nerve conduction velocity studies show a right C6 deficit. Figures 27a through 27c show MRI scans that reveal two-level spondylotic disease at C5-6 and C6-7, a large herniated nucleus pulposus at C5-6, and a prominent ridge and hard disk at C6-7. Nonsurgical management fails to provide relief, so the patient elects surgical intervention. Which of the following surgical options would give the best long-term results?
Explanation
The patient has a single-level deficit by clinical examination but an adjacent level that may be pathologic. Hilibrand and associates, in a review of 374 patients with myeloradiculopathy treated with single-level or multilevel anterior cervical diskectomy and fusion, showed that 25% of patients had an occurrence of new radiculopathy or myelopathy at an adjacent level within 10 years after surgery. Reoperation rates were highest in those patients where the adjacent nonfused segment was C5-6 or C6-7. Those patients who had multilevel fusions had a lower incidence of adjacent segment disease. The authors recommended incorporating an adjacent level in the initial procedure in patients with myelopathy or radiculopathy when significant disease was noted. Posterior keyhole foraminotomy is an excellent procedure for single-level radiculopathy but is not effective in relieving myelopathy. Anterior cervical diskectomy without fusion has an increased incidence of hypermobility and neck pain on long-term follow-up. In a later review, these authors reported improved fusion rates and better clinical outcomes with the use of strut fusions instead of multilevel interbody grafts. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH: Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am 1999;81:519-528. Henderson CM, Hennessy RG, Shuey HM Jr, Shackelford EG: Posterior-lateral foraminotomy as an exclusive operative technique for cervical radiculopathy: A review of 846 consecutively operated cases. Neurosurgery 1983;13:504-512.
Question 48High Yield
What is the primary limiting membrane and mechanical support for the periphery of the physis?
Explanation
The perichondrial fibrous ring of La Croix acts as a limiting membrane that provides mechanical support for the bone-cartilage junction of the growth plate. It is continuous with the ossification groove of Ranvier, which contributes chondrocytes for the increase in width of the growth plate. The zone of provisional calcification lies at the bottom of the hypertrophic zone and is the site of initial calcification of the matrix. It is quite weak and usually is the cleavage plane for fractures; therefore, it does not qualify as mechanical support. The last intact transverse septum separates the zone of provisional calcification from the primary spongiosa and provides no real support to the physis. The primary spongiosa is the part of the metaphysis nearest the physis. Netter FH: Growth plate, in Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 166-167.
Question 49High Yield
The therapeutic effect of etanercept in the treatment of rheumatoid arthritis is primarily mediated through
Explanation
Explanation
Etanercept is a fusion protein that combines the ligand-binding domain of the TNF-a receptor to the Fc portion of human immunoglobulin G (IgG). Protein serves as a competitive inhibitor of TNF-a signaling. COX2 is the target of NSAIDs, including newer formulations that are more COX2-specific. The remaining responses are not direct targets of etanercept. Weinblatt ME, Kremer JM, Bankhurst AD, et al: A trial of etanercept, a recombinant tumor necrosis factor receptor: Fc fusion protein, in patients with rheumatoid arthritis receiving methotrexate. N Engl J Med 1999;340:253-259.
References:
- Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 489-530.
Question 50High Yield
Figures 25a and 25b show the clinical photographs of a 19-year-old baseball outfielder who has shoulder pain after sliding headfirst into second base. He reports pain while batting, sliding, and catching. Examination reveals a posterior prominence during midranges of forward elevation, which then disappears with a palpable clunk during terminal elevation and abduction. What is the most likely diagnosis?
Explanation
Explanation
25b A headfirst slide with the arm extended can injure the posterior shoulder. Winging of the scapula is dynamic and is considered a compensatory effort to prevent subluxation; it is not related to nerve injury. Posterior glenohumeral subluxation can be present during the initiation of a bat swing. Rotator cuff function, interval tears, and superior labrum tears can be painful but do not produce winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
References:
- Fiddian NJ, Kling RJ: The winged scapula. Clin Orthop 1984;185:228-236.
Question 51High Yield
Which of the following treatments of polyethylene results in the highest amount of oxidative degradation?
Explanation
Explanation
Oxidative degradation of polyethylene occurs as a function of time in an air environment. In an environment such as argon, nitrogen, or a vacuum, the process is reduced. Ethylene oxide is an alternative for sterilization in which the cross-link degradation is minimized because of the absence of oxidative interactions. Gamma sterilization or use of ethylene oxide gas is the industry standard; however, oxygen concentrations are now reduced to a minimal level to retard the oxidation phenomenon. Sanford WM, Saum KA: Accelerated oxidative aging testing of UHMWPE. Trans Orthop Res Soc 1995;20:119. Sun DC, Schmidig G. Stark C, et al: On the origins of a subsurface oxidation maximum and its relationship to the performance of UHMWPE implants. Trans Soc Biomater 1995;18:362. Callaghan JJ, Dennis DA, Paprosky WA, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 35-41.
References:
- McKellup HA: Bearing surfaces in total hip replacement: State of the art and future developments. Instr Course Lect 2001;50:165-179.
Question 52High Yield
When compared to traditional open repair through a posterior incision, percutaneous Achilles tendon repair clearly results in a reduction of what complication?
Explanation
Prospective studies, including randomized and randomized multicenter reports, have shown that percutaneous or mini-open acute Achilles tendon repair has comparable functional results when compared to traditional open techniques. Calder and Saxby reported one superficial infection out of 46 patients with a mini-open repair; Assal and associates and Cretnik and associates had no wound complications or infections. The other complications have not proved to be less likely with the mini-open or percutaneous technique. Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures: A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am 2002;84:161-170. Calder JD, Saxby TS: Early, active rehabilitation following mini-open repair of Achilles tendon rupture: A prospective study. Br J Sports Med 2005;39:857-859.
Question 53High Yield
A 33-year-old man had his foot run over by a forklift 1 hour ago. Examination reveals that the head of the fifth metatarsal is extruded through the plantar aspect of the foot. The foot is severely swollen and pale, there is no sensation in the toes, and the pulses are not palpable. Radiographs are shown in Figures 42a and 42b. Emergent management should consist of

Explanation
Following a severe crush injury, the patient has an acute compartment syndrome. Even though there is an open fracture, this is not sufficient to decompress the compartment syndrome. Therefore, splinting and observation are not appropriate. The surgical treatment of choice is fasciotomy with fixation of the multiple fractures. A primary amputation is not indicated because there is potential for salvage of this devastating injury. Fakhouri AJ, Manoli A II: Acute foot compartment syndromes. J Orthop Trauma 1992;6:223-228. Myerson MS: Management of compartment syndromes of the foot. Clin Orthop 1991;271:239-248.
Question 54High Yield
Figure 40 shows the AP radiograph of a 55-year-old man who reports left knee pain. Which of the following conditions is least likely to produce this radiographic presentation?
Explanation
The radiograph reveals densities within the articular cartilage of the knee commonly referred to as chondrocalcinosis. The term chondrocalcinosis refers to the presence of calcium-containing crystals detected as radiodensities in cartilage. Calcium-containing crystals other than calcium pyrophosphate dihydrate may also deposit in articular cartilage and menisci, producing both radiographically detectable densities in cartilage and joint inflammation or degeneration. Hemochromatosis, alkaptonuria (ochronosis), and Wilson's disease are characterized by cellular deposition of iron, calcium, and copper ions, respectively, into various tissues including articular cartilage and can give this appearance. Septic arthritis does not usually cause chondrocalcinosis. Klippel JH (ed): Primer on the Rheumatic Diseases, ed 11. Atlanta, GA, Arthritis Foundation, 1997, pp 226-229 and 328-331.
Question 55High Yield
A 30-year-old woman injures her knee while skiing. Based on the MRI scan shown in Figure 5, treatment should consist of
Explanation
The MRI scan demonstrates a grade III MCL tear. Basic science and clinical studies have shown that nonsurgical management is preferred for MCL tears. Functional rehabilitation and early motion have led to consistently better results than has surgical repair.
Question 56High Yield
The dorsal digital cutaneous nerve of the great toe shown in Figure 8 is a branch of what nerve?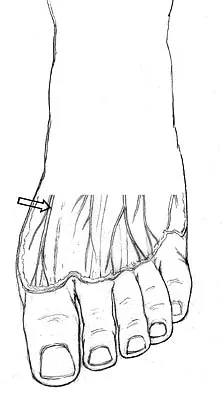
Explanation
The dorsal digital cutaneous nerve of the great toe is a branch of the medial branch of the superficial peroneal nerve. The deep peroneal nerve supplies the first web space. McMinn RMH, Hutchings RT, Logan BM: Color Atlas of Foot and Ankle Anatomy. Weert, Netherlands, Wolfe Medical Publications, 1982, p 50.
Question 57High Yield
A 60-year-old woman reports a painful hip arthroplasty after undergoing surgery 18 months ago. Radiographs show stable cementless implants without signs of ingrowth. Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h. Management should now consist of
Explanation
Explanation
Significant elevation of the erythrocyte sedimentation rate in a patient with a painful hip arthroplasty mandates a complete work-up for infection prior to considering revision surgery. Reproducibility and reliability of ultrasonography as a diagnostic test still needs clarification. Aspiration is the easiest and most cost-effective test and should be performed prior to nuclear imaging. The latter is most valuable if the results are negative, strongly predicting the absence of infection. Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
References:
- McAuley JP, Moreau G: Sepsis: Etiology, prophylaxis, and diagnosis, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 1295-1306.
Question 58High Yield
Figures 43a and 43b show the T1- and T2-weighted MRI scans of a 78-year-old woman who reports the sudden atraumatic onset of well-localized medial knee pain. Pain is worse at night and also occurs with weight-bearing activity. What is the most likely diagnosis?
Explanation
Explanation
43b Osteonecrosis of the tibial plateau occurs infrequently. The symptoms are similar to those of idiopathic osteonecrosis of the medial femoral condyle and include pain and tenderness of the medial aspect of the knee and a slight synovitis. The range of motion of the knee remains within normal limits, and no gross deformity is present. Osteonecrosis of the tibial plateau is easily misdiagnosed as degenerative meniscus or osteoarthritis of the compartment of the knee. Review of lateral radiographs may reveal an osteopenic area in the subchondral bone of the medial tibial plateau. The diagnosis is more easily established with a bone scan where increased uptake of radionucleides is shown over the medial tibial plateau. In osteoarthritic involvement of the medial compartment, uptake is over both the medial femoral condyle and the medial tibial plateau, whereas if osteoarthritis involves the entire knee, uptake is diffuse over the entire joint. Radiographic findings in complex regional pain syndrome are normal as opposed to the findings for osteonecrosis or osteoarthritis. Osteosarcoma has a characteristic radiographic appearance of a bone-forming tumor. Loose bodies can derive from osteochondral fractures; a history of trauma is usually elicited. Osteoarthritis usually presents with joint space narrowing accompanying the weight-bearing pain. Soucacos PN, Berris AE, Xenakis TH, et al: Knee osteonecrosis: Distinguishing features in differential diagnosis, in Urbanik JR, Jones JD (eds): Osteonecrosis. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 413-424.
References:
- Ecker ML, Lotke PA: Osteonecrosis of the medial part of the tibial plateau. J Bone Joint Surg Am 1995;77:596-601.
Question 59High Yield
A 68-year-old man with no significant medical history underwent a total knee arthroplasty 4 years ago. A radiograph is shown in Figure 55. He reports that he had no problems with the knee until 6 weeks ago when he noted the gradual onset of pain following a colonoscopy. Examination reveals a painful, swollen knee. Knee aspiration reveals a WBC count of 40,000/mm3. Management should consist of
Explanation
Explanation
The treatment of choice for a late hematogenous infection is two-stage resection arthroplasty and reimplantation, with parenteral antibiotics prior to reimplantation. This is particularly true when septic loosening has occurred as in this patient. Open irrigation and debridement with polyethylene exchange has been used successfully when the duration of symptoms is 3 weeks or less. Long-term suppressive antibiotics are most commonly used when the patient's medical condition precludes further surgery. Delayed reimplantation has been shown to be superior to immediate reimplantation in multiple studies. Little data support the use of arthroscopic irrigation and debridement. Swanson KC, Windsor RE: Diagnosis of infection after total knee arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1485-1491.
References:
- Hanssen AD, Rand JA, Osmon DR: Management of the infected total knee arthroplasty, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 1070-1089.
Question 60High Yield
A patient with refractory long head biceps pain in the shoulder undergoes biceps tenotomy. The patient is concerned about possible postoperative deformity and loss of supination strength. Which of the following techniques provides the strongest initial fixation to prevent distal migration?
Explanation
Recent articles have looked at the cyclic load failure and ultimate load failure of biceps tenodesis techniques. The interference screw has proved superior to bone tunnel, suture anchor, and soft-tissue tenodesis techniques in laboratory cadaveric testing. Whether this is clinically relevant or not is still unknown. Ozalay M, Akpinar S, Karaeminogullari O, et al: Mechanical strength of four different biceps tenodesis techniques. Arthroscopy 2005;21:992-998.
Question 61High Yield
A 64-year-old man undergoes a primary total knee arthroplasty. Three months after surgery he reports persistent pain, weakness, and difficulty ambulating. Postoperative radiographs are shown in Figures 6a through 6c. What is the best course of action at this time?


Explanation
The Merchant view reveals subluxation of the patellar component. The etiology of maltracking of the patella includes internal rotation of the femoral component, internal rotation of the tibial component, excessive patellar height, and lateralization of the patella component. The treatment of choice in this patient is revision total knee arthroplasty with external rotation of the femoral component. Preoperatively the patient also may require a lateral release, revision of the tibial component if it is internally rotated, and possibly a soft-tissue realignment. Component malalignment needs to be addressed first. Kelly MA: Extensor mechanism complications in total knee arthroplasty. Instr Course Lect 2004;53:193-199. Malkani AL, Karandikar N: Complications following total knee arthroplasty. Sem Arthroplasty 2003;14:203-214.
Question 62High Yield
Figure 29a shows the clinical photograph of a 26-year-old woman who has had the leg deformity since birth. She reports difficulty with walking and weight bearing and notes increased discomfort and swelling when the leg is dependent. She denies any history of trauma or family history of a similar disorder. Examination reveals a fixed equinovarus deformity of the foot but no evidence of a limb-length discrepancy. No other cutaneous findings or soft-tissue masses are noted. Sagittal and axial T1- and T2-weighted MRI scans are shown in Figures 29b and 29c. What is the most likely diagnosis?


Explanation
Because the MRI scans show marked dilation and proliferation of lymphatic channels that completely involve all the leg muscles and the clinical photograph shows the severe swelling associated with this disease, the most likely diagnosis is lymphangiomatosis. Poliomyelitis affects the anterior horn cells and manifests as muscle atrophy. Neurofibromatosis can have a similar clinical appearance but usually is associated with other systemic and cutaneous findings. Congenital band syndrome results in amputated or shortened extremities. Chronic venous stasis disease usually is not associated with joint contractures, and typically it affects older individuals. Surgical excision is the only known treatment; this patient underwent an above-knee amputation. Berquist TH (ed): MRI of the Musculoskeletal System, ed 3. Philadelphia, PA, Lippincott Raven, 1997, p 771.
Question 63High Yield
Which of the following is NOT considered a risk factor for nonunion of a type II odontoid fracture?
Explanation
Although obesity can make brace or halo wear difficult, it has not been associated with an increased risk for nonunion. Carson GD, Heller JG, Abitbol JJ, et al: Odontoid fractures, in Levine AM, Eismont FJ, Garfin SR, et al (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 235-238.
Question 64High Yield
A 25-year-old man has chronic back pain that has been slowly worsening. He has no constitutional symptoms, and he denies any previous medical problems. Examination shows a tall lean build with no objective neurologic findings or skin lesions. Figure 32 shows a T2-weighted sagittal MRI scan. What is the most likely diagnosis?
Explanation
The MRI scan shows significant dural ectasia, which is seen in more than 60% of patients with Marfan syndrome. It is also relatively common in patients with neurofibromatosis, but this patient has no skin lesions. It has also been described in Ehlers-Danlos syndrome but is less common. Ahn NU, Sponseller PD, Ahn UM, Nallamshetty L, Kuszyk BS, Zinreich SJ: Dural ectasia is associated with back pain in Marfan' syndrome. Spine 2000;25:1562-1568.
Question 65High Yield
Figure 26 shows the MRI scan of a 60-year-old man who has had groin pain for the past 2 months. The patient reports pain with ambulation, and examination reveals an antalgic gait. He denies any history of steroid or alcohol abuse. Plain radiographs are normal. Management should include
Explanation
Explanation
The patient has transient osteoporosis of the hip. Transient osteoporosis is usually a self-limited condition that is most frequently seen in women in the third trimester of pregnancy and in men in the sixth decade of life. Transient osteoporosis is best treated with protected weight bearing.
References:
- Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Question 66High Yield
A patient undergoes an arthroscopic debridement for lateral epicondylitis. Postoperatively she reports pain and a sense of clicking of the elbow. Examination reveals apprehension to supination, load, and extension. What structure has been injured resulting in the clinical presentation?
Explanation
Explanation
The patient has an iatrogenic injury to the lateral ulnar collateral ligament following the arthroscopic procedure. Failure to adhere to known anatomic landmarks can lead to this devastating complication. The examination findings are classic for posterolateral elbow instability. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 318.
References:
- O' Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
Question 67High Yield
What is the reported failure rate for surgical treatment of a Morton's neuroma?
Explanation
Explanation
The reported failure rate is in the range of 15%, which may be the result of incorrect diagnosis, improper web space selection, or formation of a stump neuroma. Therefore, the procedure should be approached with caution, measures should be taken to ensure that the diagnosis is accurate, and nonsurgical options should be exhausted. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111. Beskin JL: Nerve entrapment syndromes of the foot and ankle. J Am Acad Orthop Surg 1997;5:261-269.
References:
- Mann RA, Reynolds JC: Interdigital neuroma: A critical clinical analysis. Foot Ankle 1983;3:238-243.
Question 68High Yield
A 52-year-old woman slipped on ice in her driveway. Radiographs are shown in Figures 19a and 19b. The patient was treated in a short leg cast with weight bearing as tolerated for 6 weeks. Due to persistent tenderness at the fracture site, a CAM walker was used for an additional 8 weeks. Nine months after the injury, the patient still walks with a limp and reports pain with deep palpation at the fracture site. What is the next most appropriate step in management?

Explanation
Persistent pain at the fracture site in the absence of infection is most likely due to a nonunion, best detected by CT. Walsh and DiGiovanni reported on a series of closed rotational fibular fractures in which nonunions were detected by CT in the absence of standard ankle radiographic findings. Repeat immobilization would not be appropriate at this late date. Pain management/sympathetic blocks would be considered if the patient displayed pain with light touch and disproportionate pain consistent with a complex mediated pain syndrome. Acupuncture would be expected to be of limited benefit. Walsh EF, DiGiovanni C: Fibular nonunion after closed rotational ankle fracture. Foot Ankle Int 2004;25:488-495.
Question 69High Yield
An 18-year-old high school football player sustains a thigh injury that results in the findings shown in Figure 1. Initial management should consist of
Explanation
Explanation
The radiograph shows myositis ossificans within the quadriceps muscle. This condition occurs as a complication of muscle injury. Initial treatment should include rest, ice, compression, and elevation. While gentle active range of motion is encouraged in the functional recovery from this injury, passive stretching is contraindicated as it can enhance hemorrhage and accentuate the development of myositis ossificans. Ultrasound is similarly contraindicated because it can enhance the development of myositis ossificans and has no proven efficacy in this patient; electrical stimulation also has no proven benefits. Massage is contraindicated in the initial management of this injury because of its influence on increasing local blood flow. Anderson JE (ed): Grant's Atlas of Anatomy. Baltimore, MD, Williams & Wilkins, 1978, pp 4.39-4.49. Brumet ME, Hontas RB: The thigh, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112. Antao NA: Myositis of the hip in a professional soccer player: A case report. Am J Sports Med 1988;16:82-83.
References:
- Jackson DW, Feagin JA: Quadriceps contusions in young athletes: Relation of severity of injury to treatment and prognosis. J Bone Joint Surg Am 1973;55:95-105.
Question 70High Yield
A 58-year-old woman has had a painless periscapular mass for the past year. An MRI scan and biopsy specimen are shown in Figures 4a and 4b. What is the most likely diagnosis?

Explanation
Elastofibroma is a rare tumor that most commonly occurs in adults who are older than age 55 years. The lesions usually grow between the chest wall and the scapula, and 10% are bilateral. Histologic analysis shows that they are composed of equal amounts of elastin and collagen with occasional fibroblasts. Briccoli A, Casadei R, Di Renzo M, Favale L, Bacchini P, Bertoni F: Elastofibroma dorsi. Surg Today 2000;30:147-152.
Question 71High Yield
The parents of a 3-year-old girl who has had pain and swelling in the right ankle for the past 3 months now report that she has a limp and that the right knee and both ankles are painful and swollen. The limp and difficulty walking are most severe in the morning when the child first gets out of bed and are also more severe after extended walking. The parents deny fever, chills, weight loss, or night pain. Examination shows mild swelling and slightly restricted motion of the right knee and both ankles but is otherwise normal. In addition to initiation of treatment, the child should be referred to which of the following specialists?
Explanation
Pauciarticular juvenile rheumatoid arthritis (JRA) is the most common subgroup of JRA. It typically presents between the ages of 2 to 4 years with a mild swelling of one to four joints. Girls are affected four times more often than boys. The ankle and knee are commonly involved, and limping is typically worse in the morning and after extended activity. The diagnosis of pauciarticular JRA is typically one of exclusion because laboratory studies, including erythrocyte sedimentation rate and rheumatoid factor, are usually within normal limits. Pauciarticular JRA has the highest incidence of chronic uveitis, and in the subgroup with elevated antinuclear antibody (ANA) titers, the incidence is 75%. In JRA, uveitis usually occurs after the onset of synovitis but may precede the joint symptoms. At the early stage of uveitis, the patient is asymptomatic. If the eye condition is not detected and treated, progressive loss of vision may occur. Orthopaedic surgeons may be instrumental in making the diagnosis of pauciarticular JRA. Pauciarticular JRA is not associated with conditions that require input from the other specialists. Carey TP: Inflammatory arthritides: Juvenile rheumatoid arthritis, seronegative spondyloarthropathies, transient synovitis, hemophilic arthropathy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1315-1321.
Question 72High Yield
Intrinsic muscles of the foot act on the toes by
Explanation
Explanation
Intrinsic muscles of the foot function to flex the metatarsophalangeal joints and extend the interphalangeal joints. Myerson MS, Shereff MJ: The pathologic anatomy of claw and hammertoes. J Bone Joint Surg Am 1989;71:45-49.
Question 73High Yield
A 13-year-old girl who is 2 years postmenarche has been referred for management of scoliosis. She denies any history of back pain. Radiographs show a right thoracic curve of 35 degrees. She has a Risser sign of 4 and a bone age of 15.5 years. Management should consist of
Explanation
Because the patient is skeletally mature with a curve of less than 40 degrees, there is no benefit to bracing and surgery is not indicated. Management should consist of observation and follow-up radiographs in 6 months. Lonstein JE, Carlson JM: The prediction of curve progression in untreated idiopathic scoliosis during growth. J Bone Joint Surg Am 1984;66:1061-1071.
Question 74High Yield
The palmar cutaneous branch of the median nerve (PCBMN) originates from the
Explanation
Explanation
The PCBMN originates from the median nerve proper between 3 and 21 cm proximal to the wrist with moderate variation. It virtually always originates from the radial side of the nerve and travels distally with the median nerve, radial to the palmaris longus, and ulnar to the flexor carpi radialis. Hobbs RA, Magnussen PA, Tonkin MA: Palmar cutaneous branch of the median nerve. J Hand Surg Am 1990;15:38-43.
References:
- Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System: Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, p 52.
Question 75High Yield
Figure 17 shows the AP radiograph of a 75-year-old man with right hip pain. The femoral component is loose. The mechanism of loosening is most likely secondary to
Explanation
Explanation
The femoral construct shown in the radiograph has failed to produce ingrowth of the stem. The stem has subsided and rotated. Impingement of the trochanter did not occur until after the stem subsided. There is no evidence of osteolysis or third-body wear debris from the cerclage wire. A larger femoral stem needs to be implanted to achieve rigid fixation. Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 217-238.
References:
- Peter CL, Rivero DP, Kull LR, et al: Revision total hip arthroplasty without cement: Subsidence of proximally porous-coated femoral components. J Bone Joint Surg Am 1995;77:1217-1226.
Question 76High Yield
A 23-year-old woman reports right knee pain and fullness. The pain is worse with activity but also present at rest. Radiographs are shown in Figures 20a and 20b. What is the most likely diagnosis?

Explanation
The radiographs reveal a predominantly lytic, destructive lesion of the distal femur, although there is a hint of some blastic change as well. The lesion has violated the cortex, and there is mineralization outside the cortex laterally. The lateral radiograph suggests a soft-tissue density. These aggressive changes on radiographs in this age group are strongly suggestive of osteosarcoma. Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Question 77High Yield
What is a common clinical finding in patients with severe hypercalcemia secondary to bony metastasis?
Explanation
Explanation
Increased levels of calcium are known to cause anorexia, nausea, vomiting, dehydration, muscle weakness, polyuria, and polydipsia. Treatment may include hydration, saline diuresis, and bisphosphonates.
References:
- Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 78High Yield
A 12-year-old boy has severe left shoulder pain after being struck by an automobile. A chest radiograph, AP and lateral radiographs, and a CT scan with three-dimensional reconstruction of the scapula are shown in Figures 38a through 38d. Management should consist of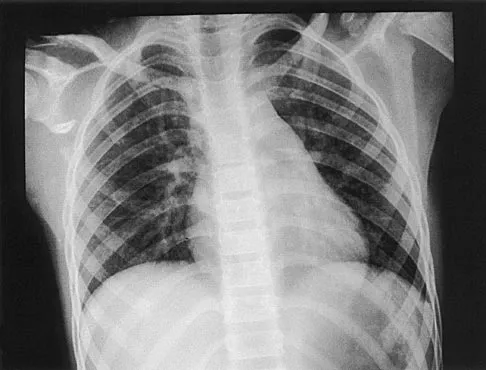


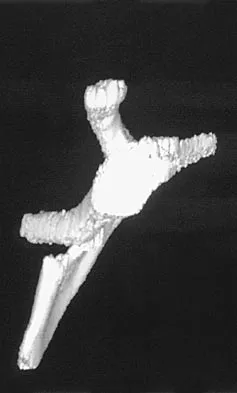
Explanation
Scapular body fractures in children are rare and are often associated with other injuries of the chest and thorax. Management is generally nonsurgical, unless the injury is open, and usually consists of support with a sling and gentle range-of-motion exercises to minimize shoulder stiffness. Green N, Swiontkowski M: Skeletal Trauma in Children, ed 2. Philadelphia, PA, WB Saunders, 1998, vol 3, pp 319-341.
Question 79High Yield
Figure 11 shows the radiograph of a 26-year-old man with type I diabetes mellitus who was struck by a motor vehicle. What is the most common complication associated with this pelvic fracture?
Explanation
The most common complication following acetabular or pelvic ring injury is deep venous thrombosis (DVT). Without prophylaxis, rates of DVT are as high as 70% to 80%. With prophylaxis, the rates are around 10%. Infection rates in surgical repair of acetabular fractures are relatively low but a history of diabetes mellitus and a significant Morel-Lavalle lesion certainly increase the risk. However, even with these two complicating factors, the rates of infection are still lower than 10%. Sciatic nerve palsy rates from the injury alone approach 20% and iatrogenic injury is usually less than 2%. Degenerative changes to the hip following this injury approach 20% to 25%, even with an anatomic reduction. Geerts WH, Code KI, Jay RM, et al: A prospective study of venous thromboembolism after major trauma. N Engl J Med 1994;331:1601-1606.
Question 80High Yield
The Keller proximal phalanx resection procedure is most useful for which of the following conditions?
Explanation
Explanation
A Keller proximal phalanx resection procedure usually results in reduced weight bearing under the first ray because of shortening of the toe and disruption of intrinsic flexor function. This can be an effective method of offloading a neuropathic ulcer under the great toe at the interphalangeal or metatarsophalangeal joint area. However, these features are generally undesirable in young active patients. The procedure has a high rate of recurrent deformity in patients with rheumatoid arthritis. It would exacerbate transfer metatarsalgia in a patient with a hypermobile first ray. Lin SS, Bono CM, Lee TH: Total contact casting and Keller arthroplasty for diabetic great toe ulceration under the interphalangeal joint. Foot Ankle Int 2000;21:588-593.
References:
- Downs DM, Jacobs RL: Treatment of resistant ulcers on the plantar surface of the great toe in diabetics. J Bone Joint Surg Am 1982;64:930-933.
Question 81High Yield
A 10-year-old soccer player has bilateral heel pain and reports that the pain is worse during and immediately after sports. Examination reveals that the calcaneal tuberosities are painful to palpation bilaterally. What is the most likely diagnosis?
Explanation
Explanation
Calcaneal apophysitis (Sever's disease) is a common cause of heel pain in children who are active in sports. The symptoms are most commonly bilateral and will often respond to a gastrocnemius-soleus complex stretching program. In addition, rest, anti-inflammatory drugs, and heel pads for the shoe may be prescribed. There is no effect on the long-term growth of the calcaneus. Micheli LJ, Ireland ML: Prevention and management of calcaneal apophysitis in children: An overuse syndrome. J Pediatr Orthop 1987;7:34-38.
References:
- Bernhardt DT, Landry GL: Sports injuries in young athletes. Adv Pediatr 1995;42:465-500.
Question 82High Yield
In the nonsurgical management of posterior tibial tendon dysfunction with flexible deformity, a common strategy is to prescribe an ankle-foot orthosis or a University of California Biomechanics Laboratory (UCBL) orthosis with medial posting. A high patient satisfaction rating and favorable outcome with this nonsurgical management is most likely in which of the following situations?
Explanation
Most authors recommend an initial trial of nonsurgical management in the treatment of adult-acquired flatfoot deformity such as posterior tibial tendon dysfunction. Chao and associates found that there is high patient satisfaction with ankle-foot orthoses and UCBL-type inserts in elderly patients with a relatively sedentary lifestyle. Alternatively, there was a higher dissatisfaction rate in young active patients, those with balance and ambulation difficulties (Parkinson's, severe arthritis of the hip or knee), and patients with inflammatory systemic disorders. Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Question 83High Yield
Figures 23a and 23b show the AP and lateral radiographs of the elbow of a 30-year-old professional pitcher. The pathology shown in these studies is most consistent with which of the following conditions?
Explanation
Explanation
23b The radiographs show the osteophytic build-up of the posteromedial corner of the elbow that occurs with valgus extension overload in the pitching elbow. This is the result of excessive valgus forces during the acceleration and deceleration phases of throwing. These forces, coupled with medial elbow stresses, cause a wedging of the olecranon into the medial wall of the olecranon fossa. Valgus instability of the elbow may further stimulate osteophyte formation. Repetitive impact of a spur within the olecranon fossa may cause fragmentation and eventual formation of loose bodies. Azar FM, Wilk KE: Nonoperative treatment of the elbow in throwers. Oper Tech Sports Med 1996;4:91-99. Field LD, Savoie FJ: Common elbow injuries in sport. Sports Med 1988;26:193-205.
References:
- Wilson FD, Andrews JR, Blackburn TA, et al: Valgus extension overload in the pitching elbow. Am J Sports Med 1983;11:83-88.
Question 84High Yield
A 62-year-old man with diabetes mellitus has had a persistent 2-cm ulcer under the third metatarsal head for the past 4 months. He reports that he has had similar ulcers twice before, and both healed with nonsurgical management. He has used multiple types of commercial walking braces, shoes, and commercial dressings without resolution. He is insensate to the Semmes-Weinstein 5.07 monofilament. When the wound is probed with culture swab, there is no communication with the metatarsal head. Radiographs, bone scans, and laboratory studies reveal no evidence of osteomyelitis. What is the most predictable method of accomplishing wound healing without recurrence?
Explanation
The patient has a persistent diabetic foot ulcer without evidence of osteomyelitis. He has evidence of a sensory peripheral neuropathy and a concomitant motor neuropathy, leading to a dynamic motor imbalance. Use of a total contact cast would offer a high probability of healing the resistant ulcer but with a high potential for recurrence. Combining the total contact cast with Achilles tendon lengthening allows wound healing without a high risk for recurrence. Excision of the noninfected metatarsal head would make the patient vulnerable to the development of a transfer lesion under one of the remaining metatarsal heads. Robertson DD, Mueller MJ, Smith KE, et al: Structural changes in the forefoot of individuals with diabetes and a prior plantar ulcer. J Bone Joint Surg Am 2002;84:1395-1404.
Question 85High Yield
The primary purpose of obtaining the radiograph shown in Figure 9 is to assess
Explanation
Explanation
The radiograph shows a faux profil view of the hip. The primary purpose of this view is to evaluate anterior coverage of the femoral head. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492. Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
References:
- Lequesne M, deSez S: Le faux profil du bassin: Nouvelle incidence radiographique pour l'etude de la hance. Son utilite dans les dysplasies et les differentes coxopathies. Rev Rhum Mal Osteoartic 1961;28:643.
Question 86High Yield
A 60-year-old patient had the procedure shown in Figure 7 performed 5 years ago. When converting this patient to a total knee arthroplasty (TKA), what patellar problem is commonly encountered intraoperatively?
Explanation
Patella baja is commonly encountered when converting a high tibial osteotomy (HTO) to a TKA. Patella baja most likely occurs because of scarring. Meding and associates' study did not show an increased rate of lateral release when converting a knee that had undergone a previous HTO. Yoshino N, Shinro T: Total knee arthroplasty after failed high tibial osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1265-1271.
Question 87High Yield
Which of the following is most predictive of a medial side ankle injury in the presence of a fibula fracture above the level of the joint?
Explanation
Explanation
Isolated Lauge-Hansen supination-external rotation-type ankle fractures comprise 20% to 40% of ankle fractures and nonsurgical management is effective for managing SER-2 ankle fractures. Tornetta and associates recently showed that medial ankle tenderness, ecchymosis, and swelling are not reliable findings when trying to determine deltoid competence. Stress radiographs showing a medial clear space of greater than 4 mm or one that is also 1 mm greater than the superior joint space, or any lateral talar subluxation are indicative of deltoid incompetence and indicative of a SER-4 ankle fracture. McConnell T, Creevy W, Tornetta P III: Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am 2004:86;2171-2178. Kristensen KD, Hansen T: Closed treatment of ankle fractures: Stage II supination-eversion fractures followed for 20 years. Acta Orthop Scand 1985;56:107-109.
Question 88High Yield
The management of a complex multifragmentary diaphyseal fracture of either the tibia or femur has changed during the last decade. Which of the following principles of treatment is now considered less important?
Explanation
Although the original concept of internal fixation was one of anatomic reduction and stable fixation, over the past 10 to 15 years there has been a change based on the advent of intramedullary nailing and bridge plating. It is now appreciated that in a multifragmentary diaphyseal fracture, particularly of the lower extremity, the achievement of axis alignment (mechanical and anatomic axis) is all that is required. Healing will occur by callus. Relatively stable fixation is achieved through intramedullary nailing or bridge plating, providing adequate pain relief for functional aftercare. Perren SM, Claes L: Biology and mechanics of fracture management, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 7-32. deBoer P: Diaphyseal fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 93-104.
Question 89High Yield
In a patient with a C5-6 herniation, the most likely sensory deficit will be in the
Explanation
Explanation
A C5-6 herniation compresses the C6 root, which innervates the radial forearm, thumb, and index finger. The lateral shoulder is innervated by C5. The dorsal forearm and the middle finger typically are innervated by C7. The ulnar forearm, ring finger, and little finger are innervated by C8. There is no specific nerve associated with the volar forearm and palm.
References:
- Hoppenfeld S: Evaluation of nerve root lesions involving the upper extremity, in Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-23.
Question 90High Yield
A 10-year-old girl with a monoarticular pattern of juvenile rheumatoid arthritis (JRA) has had a 3-cm limb-length discrepancy since age 8 years when inflammation in the right knee came under good medical control. Because her right leg is longer, the patient states that she would like her legs to be close to equal in length in the future. A growth-remaining chart is shown in Figure 14. Management should consist of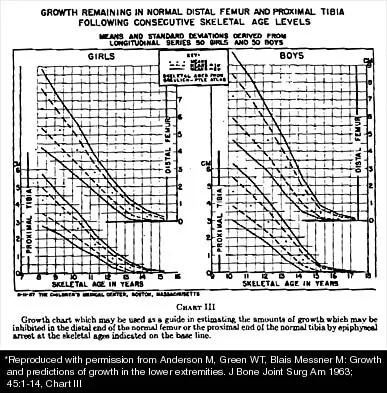
Explanation
In a subgroup of patients with monoarticular JRA and a limb-length discrepancy that developed before the age of 9 years, Simon and associates showed that a subsequent growth deceleration on the affected side may correct a large part of the difference in length. This possibility would make surgery unnecessary and should prompt further observation. Simon S, Whiffen J, Shapiro F: Leg-length discrepancies in monoarticular and pauciarticular juvenile rheumatoid arthritis. J Bone Joint Surg Am 1981;63:209-215.
Question 91High Yield
A 19-year-old man has had back pain with activity, especially running in soccer and baseball, for the past 4 months. He denies any history of trauma. Examination reveals no motor weakness or sensory changes in the lower extremities. Range of motion shows increased pain with extension and mild limitation with flexion. A sitting straight leg raising test is limited at approximately 60 degrees bilaterally by back and buttocks pain. Plain radiographs are normal. MRI scans are shown in Figures 13a through 13e. What is the most likely diagnosis?
Explanation
Explanation
13b 13c 13d 13e The patient has an isthmic spondylolysis. The plain radiographs are normal, but the MRI scans show increased marrow edema and signal at the L5 pars interarticularis. Findings of bilateral hamstring tightness and increased pain with extension over flexion suggests spondylolysis. The MRI scans do not show any signs of the other conditions. Wiltse LL, Rothman SL: Spondylolisthesis: Classification, diagnosis and natural history. Sem Spine Surg 1993;5:264-280.
References:
- Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 129-137.
Question 92High Yield
What is the most appropriate orthotic management for the lesion shown in Figure 6?
Explanation
The figure shows an intractable plantar keratosis (IPK). The keratoma usually forms beneath a bony prominence. This can occur under the sesamoids, most commonly the tibial sesamoid, or under the fibular condyle of a prominent metatarsal head. The initial treatment of an IPK consists of paring down the callused lesion and placing a metatarsal pad proximal to the lesion to provide posting to unload the bony prominence.
Question 93High Yield
A 49-year-old woman with serologically proven rheumatoid arthritis has Larsen grade II radiographic changes in the elbow. Examination reveals a preoperative arc of flexion of less than 90 degrees and there is no instability. Nonsurgical management has failed to provide relief. What is the best treatment option?
Explanation
Explanation
Larsen grade I and II rheumatoid arthritis is best treated with synovectomy with arthroplasty reserved for later stages, especially in younger patients. Open synovectomy with or without a radial head excision has yielded good results for pain and function, with arthroscopic synovectomies yielding similar results. Arthroscopic synovectomy has been shown to be more effective in restoring function in patients with a flexion arc of less than 90 degrees. Tanaka N, Sakahashi H, Hirose K, et al: Arthroscopic and open synovectomy of the elbow in rheumatoid arthritis. J Bone Joint Surg Am 2006;88:521-525. Horiuchi K, Momohara S, Tomatsu T, et al: Arthroscopic synovectomy of the elbow in rheumatoid arthritis. J Bone Joint Surg Am 2002;84:342-347.
References:
- Maenpaa HM, Kuusela PP, Kaarela KK, et al: Reoperation rate after elbow synovectomy in rheumatoid arthritis. J Shoulder Elbow Surg 2003;12:480-483.
Question 94High Yield
Figure 53 shows the pedigree of a family with an unusual type of muscular dystrophy. This pedigree is most consistent with what type of inheritance pattern?
Explanation
The pedigree documents involvement of male offspring only, and it also shows transmission through an uninvolved female carrier. This inheritance pattern is most consistent with a x-linked recessive inheritance. It would be inconsistent with a dominant inheritance pattern unless there was incomplete penetrance. Autosomal-recessive inheritance would be possible only if the family member labeled II.F was also a carrier of the same gene; however, this is unlikely. Mitochondrial inheritance is possible, but as with autosomal patterns, mitochondrial inheritance normally affects both male and female offspring. It is transmitted only through the maternal line.
Question 95High Yield
A previously healthy 13-year-old girl has had thigh pain for the past 3 weeks. The radiograph shown in Figure 47a reveals a lesion in the right femur. A bone scan and CT scan of the chest show no evidence of other lesions. A biopsy specimen is shown in Figure 47b. What is the most likely diagnosis?

Explanation
The patient has Langerhans cell histiocytosis that may be solitary (eosinophilic granuloma) or associated with systemic illness (Hand-Schuller-Christian disease and Letterer-Siwe disease). The solitary form of the disease, eosinophilic granuloma, typically affects patients in the first three decades of life. Radiographically, it is characterized as a well-defined, lytic, "punched out" intramedullary lesion. Histologically, two cell types, eosinophils and Langerhans cells, are seen. The Langerhans cells are seen as mononuclear histiocyte-like cells with oval nuclei with well-defined round or oval cytoplasm. A prominent nuclear groove can be seen in most of the nuclei (coffee bean nuclei). A mixture of inflammatory cells and lipid-laden foam cells with nuclear debris may be present as well. The lack of nuclear atypia and atypical mitoses excludes malignant conditions such as Ewing's sarcoma, lymphoma of bone, and metastatic neuroblastoma. The lack of acute inflammatory cells excludes the diagnosis of osteomyelitis. The eosinophils have bi-lobed nuclei and granular eosinophilic cytoplasm. Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby, 1988.
Question 96High Yield
Which of the following structures may help maintain radial length after a radial head fracture?
Explanation
Explanation
Essex-Lopresti injuries affect axial stability of the forearm. Injury to the interosseous membrane or the triangular fibrocartilage complex can result in proximal migration of the radius. Morrey BF, Chao EY, Hui FC: Biomechanical study of the elbow following excision of the radial head. J Bone Joint Surg Am 1979;61:63-68.
References:
- Coleman DA, Blair WF, Shurr D: Resection of the radial head for fracture of the radial head: Long-term follow-up of seventeen cases. J Bone Joint Surg Am 1987;69:385-392.
Question 97High Yield
A 72-year-old man who underwent total shoulder arthroplasty 2 years ago slipped on ice and fell on his shoulder 3 weeks ago. Immediately after falling he was unable to elevate his arm. Motor examination reveals deltoid 5-/5, subscapularis 5-/5, external rotation 4-/5, and supraspinatus 2/5. Radiographs are shown in Figures 8a and 8b. What is the most likely diagnosis?

Explanation
The patient has a traumatic rotator cuff tear. The history of the fall, the weakness on examination, and normal radiographic findings make a traumatic rotator cuff tear the most likely diagnosis. An MRI scan can be obtained to further evaluate the integrity of the rotator cuff. The axillary radiograph shows a reduced, nondislocated total shoulder arthroplasty. His radiographs show a well-seated humeral stem and no signs of loosening. The glenoid is a cemented all-polyethylene component with no evidence of radiolucent lines surrounding the cemented pegs. The polyethylene glenoid component is radiolucent; however, the space between the metallic humeral head and the glenoid bone is the thickness of the polyethylene glenoid component. If the humeral head were directly against the glenoid bone, then catastrophic fracture of the glenoid would be the working diagnosis. Hattrup SJ, Cofield RH, Cha SS: Rotator cuff repair after shoulder replacement. J Shoulder Elbow Surg 2006;15:78-83.
Question 98High Yield
A 60-year-old man with diabetes mellitus is referred for evaluation of nonhealing ulcers of his left foot. Nonsurgical management has failed to provide relief, and a below-the-knee amputation is being considered. Which of the following studies best predicts successful amputation wound healing?
Explanation
Explanation
The TcPO2 measures the O2 delivering capacity of the local vasculature. Values above 40 mm Hg have been shown to correlate with positive healing potential. The hemoglobin A1c is a good indicator of long-term glucose levels; however, it has no direct correlation with wound healing potential. Serum albumin is an indirect measure of nutritional status, and deficiencies in nutrition must be addressed before any surgery. Adequate hemoglobin levels are also necessary to promote adequate oxygenation to the amputation site. The ankle-brachial index may be falsely elevated as a result of calcified vessels in patients with diabetes mellitus. Wyss CR, Harrington RM, Burgess EM, et al: Transcutaneous oxygen tension as a predictor of success after amputation. J Bone Joint Surg Am 1988;70:203-207.
References:
- Dwars BJ,van den Broek TA, Rauwerda JA, et al: Criteria for reliable selection of the lowest level of amputation in peripheral vascular disease. J Vasc Surg 1992;15:536-542.
Question 99High Yield
What is the most appropriate treatment for a chordoma involving the sacrum?
Explanation
Explanation
Chordomas are very radio- and chemotherapy resistant; therefore, en bloc resection with a negative margin is the preferred treatment. Lesions at or below S3 can be resected without compromising pelvis stability, and continence usually is maintained. The mean survival rate for patients with sacral chordomas is approximately 7 years. Patients with chordoma of the mobile (cervical, thoracic, or lumbar) spine have a mean survival rate of approximately 5 years. This difference is most likely the result of an earlier diagnosis. Fardin DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 123-133. Stener B, Gunterberg B: High amputation of the sacrum for extirpation of tumors: Principles and technique. Spine 1978;3:351-366.
References:
- Stener B: Resection of the sacrum for tumors. Chir Organi Mov 1990;75:S108-S110.
Question 100High Yield
A 28-year-old man sustained a fracture-dislocation of T8 in a motor vehicle accident 1 week ago. The injury resulted in complete paraplegia. Management should consist of
Explanation
With a complete injury in the thoracic spinal cord, the likelihood of neurologic recovery is small. If possible, treatment should be planned to allow rapid mobilization and rehabilitation without the use of braces and their associated skin problems. The use of long segment fixation provides for rapid mobilization without having to use braces postoperatively. The use of steroid protocol is controversial and should be considered only if it can be started within 8 hours of the injury. Laminectomy is contraindicated because it will increase instability.
You Might Also Like
Previous ChapterOrthopedic Board Review: 100 High-Yield MCQs | Mock Exam Se…
Next Chapter Orthopedic Surgery Board Exam Prep: 100 High-Yield MCQs (Se…

Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon