Orthopedic Surgery Board Exam: 100 High-Yield MCQs (Set 924)
14 Apr 2026
107 min read
111 Views
Key Takeaway
This page offers 100 high-yield orthopedic board review MCQs, ideal for ABOS, OITE, and FRCS exam preparation. Covering critical topics like minimally invasive approaches, Mock Exam Set 924 helps surgeons master concepts and confidently approach board certification.
Minimally Invasive Approach for Femur Intrame...
00:00
Start Quiz
Question 1High Yield
A soccer player who sustained a twisting injury to the right ankle while making a cut is unable to bear weight and has diffuse tenderness over the anterior and lateral aspects of the ankle. Examination also shows a positive squeeze test. Plain radiographs and a stress radiograph are shown in Figures 26a through 26c. Radiographs of the leg and knee are normal. What is the most appropriate management?
Explanation
Explanation
26b 26c The mechanism of injury, physical examination, and radiographs indicate a "high" ankle sprain with disruption of the distal tibiofibular ligaments and interosseous membrane. These injuries typically involve pronation and external rotation forces. In addition, recovery is significantly delayed, often requiring 6 to 8 weeks to heal. Radiographs obtained months after recovery often show calcification within the distal syndesmosis, which is not typically symptomatic. This patient has gross instability, resulting in a high incidence of chronic diastasis and subluxation leading to impaired function. Treatment should consist of reduction and stabilization with a transsyndesmotic screw because this injury demonstrates a widened syndesmosis. Boytim MJ, Fisher DA, Neumann L: Syndesmotic ankle sprains. Am J Sports Med 1991;19:294-298.
References:
- Miller CD, Shelton WR, Barrett GR, et al: Deltoid and syndesmosis ligament injury of the ankle without fracture. Am J Sports Med 1995;23:746-750.
Question 2High Yield
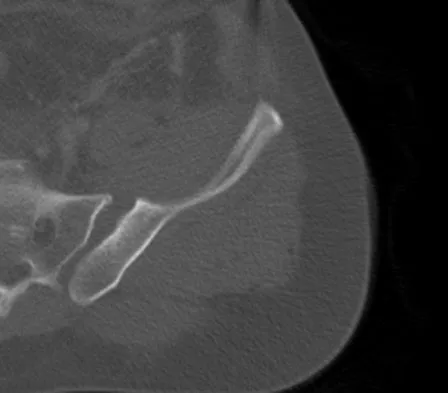
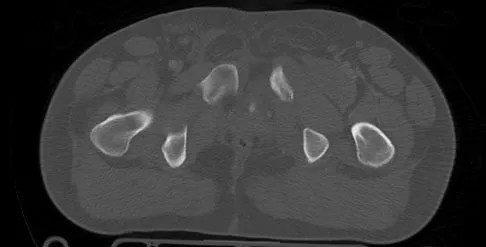
A 22-year-old cheerleader who fell from the top of a pyramid now reports anterior and posterior pelvic pain. A radiograph and CT scans are shown in Figures 43a through 43c. What is the best treatment for this injury?
Explanation
Symphyseal widening of greater than 2.5 cm and less than 5 cm denotes an AP II injury and a rotationally unstable pelvis. An AP II pelvic ring injury is best treated with anterior open reduction and internal fixation. Nonsurgical management is reserved for AP I injuries. Pelvic binders are used only acutely and should not be used for definitive management. Iliosacral screws usually are not necessary in the acute management of AP II injuries. Matta JM: Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res 1996;329:88-96. Templeman DC, Schmidt AH, Sems AS, et al: Diastasis of the symphysis pubis: Open reduction internal fixation, in Wiss D (ed): Masters Techniques in Orthopaedic Surgery-Fractures, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 639-648.
Question 3High Yield
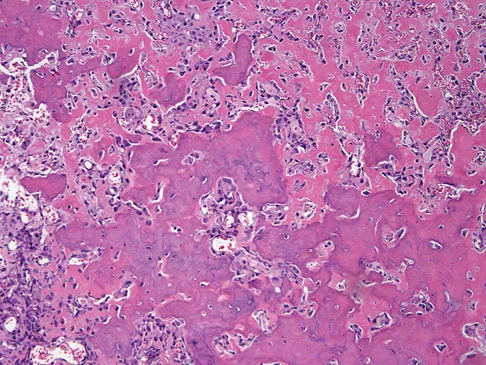
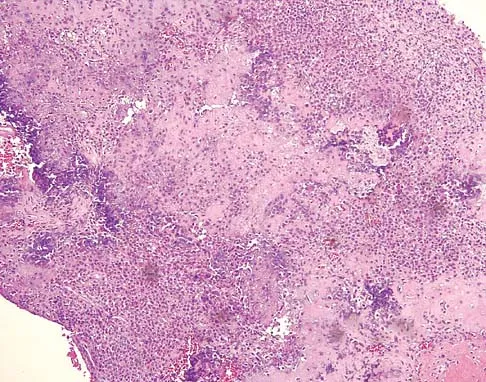
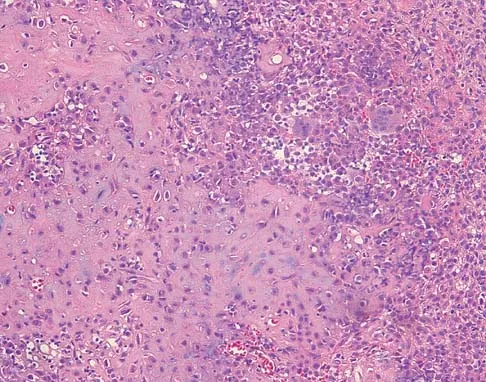
A healthy 16-year-old boy has had increasing pain in the right knee for the past 3 months. Examination reveals warmth and swelling around the distal femur. Radiographs and an MRI scan are shown in Figures 51a through 51c, and a biopsy specimen is shown in Figure 51d. What is the most likely diagnosis?


Explanation
The radiographs show a bone-producing lesion in the distal femoral metaphysis in this case of classic osteosarcoma presenting in the most common location, the distal femur. The coronal MRI scan reveals a marrow-occupying lesion with extension into the soft tissues. The histology shows osteoid production by pleomorphic cells consistent with an osteosarcoma. Ewing's sarcoma is a bone tumor characterized by uniform small blue cells on histology. Rhabdomyosarcoma is the most common childhood soft-tissue sarcoma. Osteomyelitis has an inflammatory appearance on histology. Malignant fibrous histiocytoma of bone has a lytic radiographic appearance and a pleomorphic storiform pattern without osteoid on histology. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
Question 4High Yield
A 26-year-old right hand-dominant man has had right shoulder pain for the past 6 months. History reveals that he was the starting pitcher for his high school team. Activity modification, physical therapy, cortisone injection, and anti-inflammatory drugs have failed to improve his symptoms. He has a positive O'Brien's active compression test. What is the next most appropriate step in the diagnosis of this patient?
Explanation
Explanation
MRI-arthrography has been shown to be an accurate technique for assessing the glenoid labrum in patients with suspected labral tears. Often standard MRI technique will not identify labral lesions. The use of MRI-arthrography with an intra-articular injection of gadolinium provides improved visualization of labral lesions. Bencardino and associates demonstrated a sensitivity of 89%, a specificity of 91%, and an accuracy of 90% in detecting labral lesions. SLAP lesions can be visualized on coronal oblique sequences as a deep cleft between the superior labrum and the glenoid that extends well around and below the biceps anchor. Often, contrast will diffuse into the labral fragment, causing it to appear ragged or indistinct. Applegate GR, Hewitt M, Snyder SJ, et al: Chronic labral tears: Value of magnetic resonance arthrography in evaluating the glenoid labrum and labral-bicipital complex. Arthroscopy 2004;20:959-963. Bencardino JT, Beltran J, Rosenberg ZS, et al: Superior labrum anterior-posterior lesions: Diagnosis with MR arthrography of the shoulder. Radiology 2000;214:267-271.
References:
- Nam EK, Snyder SJ: The diagnosis and treatment of superior labrum, anterior and posterior (SLAP) lesions. Am J Sports Med 2003;31:798-810.
Question 5High Yield
A 40-year-old laborer sustains the injury shown in the radiograph and CT scan in Figures 56a and 56b. What is the most common complication associated with surgical intervention?

Explanation
The patient has a severe Sanders type 4 calcaneus fracture. By far the most common complication associated with surgical treatment of calcaneus fractures is wound dehiscence. Sanders R: Displaced intra-articular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250.
Question 6High Yield
Immediately after undergoing lumbar instrumentation, a patient reports severe right leg pain and has 4+/5 weakness. Figure 24 shows an axial CT scan of L5. Exploratory surgery will most likely reveal
Explanation
Explanation
The most common finding at exploration of an inappropriately placed pedicle screw is displacement of the nerve. Pedicle breach is common, ranging from 2% to 20%, but most are asymptomatic. All of the choices are possible, but in a large series conducted by Lonstein and associates, the authors reported that displacement of the root, most often medial, was the most common finding. Laceration, contusion, or transfixion usually was not seen. Spinal fluid leakage occurs less frequently and is not expected in the minimal broach illustrated. Esses SI, Sachs BL, Dreyzin V: Complications associated with the technique of pedicle screw fixation: A selected survey of ABS members. Spine 1993;18:2231-2238. Laine T, Lund T, Ylikoski M, et al: Accuracy of pedicle screw insertion with and without computer assistance: A randomised controlled clinical study in 100 consecutive patients. Eur Spine J 2000;9:235-240.
References:
- Lonstein JE, Denis F, Perra JH, et al: Complications associated with pedicle screws. J Bone Joint Surg Am 1999;81:1519-1528.
Question 7High Yield
A 28-year-old anesthesia resident has aching pain in his dominant right forearm after injuring it while playing basketball 1 week ago. He reports that he is unable to perform regional anesthesia that requires manipulation of a needle. Examination reveals that he is unable to flex the interphalangeal joint of the thumb, and flexion of the distal interphalangeal joint of the index finger is weak. Management should consist of
Explanation
Explanation
The patient has anterior interosseous nerve palsy. Initial management should consist of splinting followed by observation; surgical decompression may be required if there is no improvement in the functional deficit in 6 months. Anterior interosseous nerve palsy is classically described as an inability to flex the interphalangeal joint of the thumb because of flexor pollicis longus paralysis and a weakness or inability to flex the distal interphalangeal joint of the index finger because of weakness and/or paralysis of the flexor digitorum profundus to the index finger. There has been some controversy in the literature as to whether this represents a true peripheral compression neuropathy or neuritis. Recent recommendations have been to extend the period of observation from 3 to 6 months before surgical decompression, as most cases will resolve within 6 months. Miller-Breslow A, Terrono A, Millender LH: Nonoperative treatment of anterior interosseous nerve paralysis. J Hand Surg Am 1990;15:493-496.
References:
- Stern PJ, Fassler PR: Anterior interosseous nerve compression syndrome, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, 1991, vol 2, pp 983-1002.
Question 8High Yield
Figures 39a and 39b show the radiographs of an otherwise healthy 10-year-old boy who has had thigh pain and a limp for the past 9 months. Examination reveals that the left lower extremity is 1 cm shorter, with reduced flexion, abduction, and internal rotation on the left side. The patient is at the 50th percentile for height and the 90th percentile for weight. Serum studies will most likely show

Explanation
The patient has a slipped capital femoral epiphysis (SCFE) at a younger than average age (average age 13.5 years for boys and 12.0 years for girls); therefore, an etiology that is not idiopathic must be considered. Hypothyroidism can result in a SCFE, but these children typically fall into the category of less than the 10th percentile for height. SCFE may develop in children with a growth hormone deficiency who have undergone hormonal replacement. Osteodystrophy caused by chronic renal failure may result in a SCFE, but the bone quality is markedly osteopenic on radiographs and the children are chronically ill with both low height and weight percentiles. An elevated estrogen level results in physeal closure and is protective to physeal slippage. Therefore, this child will most likely have normal laboratory values. Loder RT, Hensinger RN: Slipped capital femoral epiphysis associated with renal failure osteodystrophy. J Pediatr Orthop 1997;17:205-211.
Question 9High Yield
An AP radiograph of the pelvis is shown in Figure 4. What muscle attaches to the avulsed fragment of bone identified by the arrow?
Explanation
Explanation
The radiograph reveals an avulsion of the ischial apophysis, most likely the result of violent contraction of the attached hamstring tendons (semimembranosus, semitendinosus, and long head of the biceps femoris). The short head of the biceps femoris arises from the linea aspera on the posterior femur. The pectineus and adductor longus attach to the pubic portion of the pelvis. The piriformis runs from the sacrum to the femur. Woodburne RT (ed): Essentials of Human Anatomy. New York, NY, Oxford University Press, 1978, pp 542-545.
References:
- Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Question 10High Yield
Figure 50 shows the radiograph of a 26-year-old man who sustained an isolated open injury to his foot. Examination reveals no gross contamination in the wound. There is a palpable dorsalis pedis pulse and sensation is present on the dorsal and plantar aspects of the foot. Initial treatment should consist of wound debridement, antibiotics, and
Explanation
The radiograph shows a complete extrusion of the talus. Reimplantation of the talus after wound debridement has been reported to be safe and successful, and provides for flexibility with any future reconstructive procedures. Smith CS, Nork SE, Sangeorzan BJ: The extruded talus: Results of reimplantation. J Bone Joint Surg Am 2006;88:2418-2424.
Question 11High Yield
A 2-day-old infant has the hyperextended knee deformity shown in Figure 7. No other deformities are found on examination. A radiograph shows that the ossified portion of the proximal tibia is slightly anterior to that of the distal femur. Management should consist of
Explanation
Explanation
Congenital dislocation of the knee is an uncommon deformity that varies in presentation from simple hyperextension to complete anterior dislocation of the tibia on the femur. Treatment varies with the age at presentation and the severity of the deformity. Most authors recommend early nonsurgical management. A recent study of 24 congenital knee dislocations in 17 patients found that satisfactory results were obtained in most instances using closed treatment. Based on their findings, the authors concluded that immediate reduction or serial casting should be performed when the patient is seen early after birth. If the patient is seen late and correction cannot be achieved by serial casting, traction followed by closed or open reduction may be necessary. Early percutaneous quadriceps recession has been described for complex congenital knee dislocations associated with underlying disorders, such as arthrogryposis and Ehlers-Danlos syndrome. Ko JY, Shih CH, Wenger DR: Congenital dislocation of the knee. J Pediatr Orthop 1999;19:252-259. Johnson E, Audell R, Oppenheim WL: Congenital dislocation of the knee. J Pediatr Orthop 1987;7:194-200.
References:
- Roy DR, Crawford AH: Percutaneous quadriceps recession: A technique for management of congenital hyperextension deformities of the knee in the neonate. J Pediatr Orthop 1989;9:717-719.
Question 12High Yield
Examination of a 30-year-old professional singer who has persistent neck and shoulder pain reveals a positive Hoffman's sign and clonus because of anterior C2-3 cord compression. The MRI scan shown in Figure 11a and the cervical CT scan shown in Figure 11b reveal focal anterior cord compression at the C2-3 level. Which of the following surgical approaches would least affect her professional career?
Explanation
Explanation
11b Protection of the superior laryngeal nerve is critical in a professional singer. The nerve is easily injured with retraction when using vertical extension of common anterior surgical approaches to gain exposure to the C2-3 level. McAfee and associates reported on 17 patients with C1-2 and C2-3 pathology. They used a modified submandibular approach as an anterior retropharyngeal exposure with modification of the superior extension of the Smith-Robinson technique that allows visualization of the superior laryngeal nerve and surrounding structures. No incidences of superior laryngeal nerve injury were recorded. The transoral approach should be avoided because of the high rate of infection and limited exposure. McAfee PC, Bohlman HH, Reilly LH Jr, Robinson RA, Southwick WO, Nachlas NE: The anterior retropharyngeal approach to the upper part of the cervical spine. J Bone Joint Surgery Am 1987;69:1371-1383.
References:
- Lu J, Ebraheim NA, Nadim Y, Huntoon M: Anterior approach to the cervical spine: Surgical anatomy. Orthopedics 2000;23:841-845.
Question 13High Yield
Figure 44 shows the AP radiograph of the hip of a patient who underwent screw fixation of the acetabulum. Which of the following structures is at least risk for injury during screw placement in the acetabular component?
Explanation
Acetabular screws are inserted to supplement fixation. The acetabular component can be divided into four quadrants. Anatomic studies have shown that screws placed in the anterior superior and anterior inferior quadrants of the cup may injure the external iliac vein and obturator artery, respectively. Posterior superior and posterior inferior placement (in screws greater than 25 mm) may injure the sciatic nerve or the superior gluteal artery. The common iliac artery is proximal to the acetabulum and is at least risk for injury from acetabular screw placement.
Question 14High Yield
The mother of a 2-year-old boy reports that he had pain in the right hip all night and refuses to walk on the leg this morning. He is afebrile. Examination reveals pain on hip extension and adduction, but he is able to internally and externally rotate the hip approximately 20 degrees in each direction without pain. Laboratory studies reveal a WBC count of 7,400/mm3, with 62% polymorphonuclear neutrophil leukocytes. The AP radiograph shown in Figure 15 reveals a left teardrop distance of 8 mm, while the right side measures 10 mm. Which of the following diagnostic studies will best help confirm the diagnosis?
Explanation
Explanation
The differential diagnosis includes septic hip and transient synovitis. Both disorders may present with a joint effusion. The increased teardrop distance and loss of range of motion implies that there is excess fluid in the joint. While the other tests can confirm this, only aspiration can characterize the fluid further, thereby indicating the etiology of the effusion. Provided there is enough fluid obtained at aspiration, the joint fluid should be sent for Gram stain, culture, cell count, glucose, and protein studies.
References:
- Tachdjian MO: Pediatric Orthopedics, ed 2. Philadelphia, PA, WB Saunders, 1990, pp 1415-1435.
Question 15High Yield
A 56-year-old woman has a painful mass on the bottom of her left foot, and orthotic management has failed to provide relief. Examination reveals that the mass is contiguous with the plantar fascia. An MRI scan shows a homogenous nodule within the plantar fascia. Resection of the tumor is shown in the clinical photograph in Figure 39. What type of cell is most likely responsible for the formation of this tumor?
Explanation
Explanation
The history, examination, and surgical findings are most consistent with plantar fibromatosis. Plantar fibromatosis is a benign tumor of the plantar fascia that consists chiefly of fibromyoblasts. These cells produce excessive collagen and are similar to the cells found in the palmar fascia of patients with Dupuytren's contracture of the hand. The myocyte, synovial cell, and osteocyte all produce their respective individual tissue types but do not contribute to the formation of a plantar fibromatosis. The T-cell is an important immunologic cell that is most affected in patients with HIV.
References:
- Sammarco GJ, Mangone PG: Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21:563-569.
Question 16High Yield
Which of the following benign bone lesions can develop lung metastases?
Explanation
Although considered benign bone lesions, lung metastases can develop in giant cell tumors and chondroblastomas. These often can be treated with multiple thoracotomies, resulting in long-term survival. Roberts PF, Taylor JG: Multifocal benign chondroblastomas: Report of a case. Hum Pathol 1980;11:296-298.
Question 17High Yield
Which of the following lesions most closely resembles Ewing's sarcoma histologically?
Explanation
Explanation
Ewing's sarcoma is characterized by small round blue cells. Lesions with a similar appearance include lymphoma, primitive neuroectodermal tumor, rhabdomyosarcoma, small cell lung tumor, and metastatic neuroblastoma. Karyotyping, immunohistochemistry, and electron microscopy can help differentiate these lesions.
References:
- Wold LE, McLeod RA, Sim FH, Unni KK: Atlas of Orthop Pathology. Philadelphia, PA, WB Saunders, 1990.
Question 18High Yield
A 12-year-old girl sustains an acute injury to the right elbow in a fall. An AP radiograph is shown in Figure 5. Nonsurgical management will most likely result in
Explanation
The patient has a significantly displaced medial epicondyle fracture. The only absolute indication for surgical treatment is irreducible incarceration in the joint. Nonsurgical management usually results in a painless nonunion with good elbow function and little elbow instability. Prolonged immobilization should be avoided to prevent stiffness. Tardy ulnar nerve palsy and cubitus varus are not complications of medial epicondyle fractures. Chamber HG, Wilkins KE: Part IV: Apophyseal injuries of the distal humerus, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 801-812.
Question 19High Yield
An 18-year-old man sustains an injury to his lateral ankle after being kicked while playing soccer. He reports persistent pain on the lateral ankle as well as a popping sensation with attempted ankle dorsiflexion and eversion. Which of the following structures anatomically restrains the retracted structure shown in Figure 12?
Explanation
The peroneus brevis and peroneus longus muscles are the main evertors of the hindfoot. As they descend along the posterior fibula, they pass through the retromalleolar sulcus, formed by the concavity of the retromalleolar fibula. This sulcus is deepened by a fibrocartilaginous rim. The superior peroneal retinaculum covers the fibular groove and stabilizes the peroneal tendons within the retromalleolar sulcus. It originates from the posterolateral ridge of the fibula and inserts onto the lateral calcaneus. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 81-89.
Question 20High Yield
The arthroscopic views shown in Figures 31a and 31b reveal extensive synovitis in the anterolateral corner of the ankle overlying a band of tissue sometimes implicated in soft-tissue impingement of the ankle following a chronic sprain injury. This band is a portion of the
Explanation
Explanation
31b The arthroscopic views show the lateral side of the ankle as demonstrated by the presence of the tibiofibular articulation. As is typical in chronic anterolateral impingement, synovitis overlies the anteroinferior band of the tibiofibular ligament, the most distal portion of the anterior syndesmosis. Hypertrophic scar formed on or in this ligament can impinge on the lateral margin of the talar dome and has been associated with chronic anterolateral ankle pain. Bassett FH III, Gates HS III, Billys JB, et al: Talar impingement by the anteroinferior tibiofibular ligament: A cause of chronic pain in the ankle after inversion sprain. J Bone Joint Surg Am 1990;72:55-59.
References:
- DiGiovanni BF, Fraga CJ, Cohen BE, et al: Associated injuries found in chronic lateral ankle instability. Foot Ankle Int 2000;21:809-815.
Question 21High Yield
What ligament is the primary restraint to applied valgus loading of the knee?
Explanation
Explanation
The superficial portion of the MCL contributes 57% and 78% of medial stability at 5 degrees and 25 degrees of knee flexion, respectively. The deep MCL and posteromedial capsule act as secondary restraints at full knee extension. The anterior cruciate ligament and PCL also provide secondary resistance to valgus loads.
References:
- Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 767.
Question 22High Yield
A 22-year-old patient sustained a jamming injury to the right little finger. The lateral radiograph shown in Figure 18 reveals comminution of the base of the middle phalanx, with palmar and dorsal metaphyseal cortical involvement. The articular surface also is disrupted. Management should consist of
Explanation
This fracture, known as a pilon fracture, represents comminution of the base of the middle phalanx with both palmar and dorsal cortical disruption. The treatment method that allows the best function and fewest complications is indirect reduction achieved through specific dynamic splinting or the use of specifically designed proximal interphalangeal joint external fixators. Early mobilization can be achieved by either of these techniques. Volar plate arthroplasty is indicated for a simple fracture-dislocation of the proximal interphalangeal joint with comminution of the volar fracture fragment and dorsal dislocation of the remaining articular surface. Open reduction and internal fixation or percutaneous pinning adds surgical risks and scarring and typically will not provide added stability. Cast immobilization will not achieve the goal of early range of motion. Stern PJ, Roman RJ, Kiefhaber TR, McDonough JJ: Pilon fractures of the proximal interphalangeal joint. J Hand Surg Am 1991;16:844-850.
Question 23High Yield
A 13-year-old boy hyperextends his knee while playing basketball and reports a pop that is followed by a rapid effusion. A lateral radiograph is shown in Figure 4. Initial management consists of attempted reduction with extension, with no change in position of the fragment. What is the next most appropriate step in management?
Explanation
Explanation
Avulsion fractures of the tibial spine are rare injuries that result from rapid deceleration or hyperextension of the knee in skeletally immature individuals. This injury is the equivalent of ruptures of the anterior cruciate ligament in adults. These fractures are classified as types 1 through 3. Type 1 is a minimally displaced fracture, type 2 fractures have an intact posterior hinge, and type 3 fractures have complete separation. The radiograph demonstrates a completely displaced, or type III, tibial spine avulsion. Surgical reduction is indicated in type 2 fractures that fail to reduce with knee extension and in all type 3 fractures. Reduction may be arthroscopic or open, with fixation of the bony fragment using a method that maintains physeal integrity and prevents later growth arrest. Preferred techniques would be with suture or an intra-epiphyseal screw Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60. Mulhall KJ, Dowdall J, Grannell M, et al: Tibial spine fractures: An analysis of outcome in surgically treated type III injuries. Injury 1999;30:289-292. Owens BD, Crane GK, Plante T, et al: Treatment of type III tibial intercondylar eminence fractures in skeletally immature athletes. Am J Orthop 2003;32:103-105.
References:
- Vocke AK, Vocke AR: Cartilaginous avulsion fracture of the tibial spine. Orthopedics 2002;25:1293-1294.
Question 24High Yield
A young man sustains a lumbar strain in an on-the-job motor vehicle accident. Both he and his treating physician feel that he is capable of limited duty with appropriate restrictions shortly after the injury. What term best describes his work status?
Explanation
Because the man is only recently removed from his injury and is judged capable of returning to work with some restrictions, the term that best describes his work status is temporary partial disability.
Question 25High Yield
A 53-year-old man reports acute, severe left shoulder pain after undergoing abdominal surgery 10 days ago. Initial management, consisting of anti-inflammatory drugs, physical therapy, and a subacromial injection of corticosteroid, fails to provide relief. Reexamination of the shoulder 2 months after the onset of symptoms reveals atrophy of the infraspinous and supraspinous fossa and profound weakness of active abduction and external rotation. His neck is supple with a full range of motion. Plain radiographs and an MRI scan of the shoulder are normal. What diagnostic study should be performed next in the evaluation of this patient?
Explanation
Explanation
Suprascapular nerve palsy is a fairly uncommon yet well-known cause of shoulder pain and weakness. A variety of causes have been described, including compression by a ganglion cyst, an anomalous or thickened superior transverse scapular ligament, a humeral and scapular fracture, and traction or kinking of the nerve in the suprascapular notch. In this patient, the injury is most likely caused by traction or compression of the nerve in the suprascapular notch as the result of positioning during abdominal surgery; therefore, the studies of choice are electromyography and nerve conduction velocity studies. While MRI of the cervical spine may be of some value in ruling out a radiculopathy, the clinical history does not support such a cause for this condition. Rengachary SS, Neff JP, Singer PA, Brackett CE: Suprascapular entrapment neuropathy: A clinical, anatomical, and comparative study. Part 1: Clinical study. Neurosurgery 1979;5:441-446. Rengachary SS, Burr D, Lucas S, Hassanein KM, Mohn MP, Matzke H: Suprascapular entrapment neuropathy: A clinical, anatomical and comparative study. Part 2: Anatomical study. Neurosurgery 1979;5:447-451.
References:
- Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthoscopy 1990;6:301-305.
Question 26High Yield
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms?
Explanation
Explanation
Traumatic posterior instability is a common finding in football players, especially in the blocking positions as well as in the defensive linemen and linebackers. A traumatic blow to the outstretched arm results in posterior glenohumeral forces. Labral detachment at the glenoid rim is common. Patients report slipping or pain with posteriorly directed pressure. Rarely do these patients have true dislocations that require reduction; however, recurrent episodes of subluxation or pain are not uncommon. Posterior repair has been shown to be successful in the treatment of traumatic instability. Bottoni CR, Franks BR, Moore JH, et al: Operative stabilization of posterior shoulder instability. Am J Sports Med 2005;33:996-1002. Williams RJ III, Strickland S, Cohen M, et al: Arthroscopic repair for traumatic posterior shoulder instability. Am J Sports Med 2003;31:203-209.
References:
- Kim SH, Ha KI, Park JH, et al: Arthroscopic posterior labral repair and capsular shift for traumatic unidirectional recurrent posterior subluxation of the shoulder. J Bone Joint Surg Am 2003;85:1479-1487.
Question 27High Yield
A 64-year-old man has had increasing pain in the left hip for the past 6 months. A radiograph and MRI scan are shown in Figures 25a and 25b. Biopsy specimens are shown in Figures 25c and 25d. What is the recommended treatment?
Explanation
Explanation
25b 25c 25d The radiograph shows a lytic lesion in the left periacetabular area consistent with chondrosarcoma. A large soft-tissue mass is present along with extension through the supra-acetabular region and pubic ramus. The histology shows a hypercellular lesion infiltrating through the bony trabeculae with a basophilic cytoplasm. This is classified as a grade 2 chondrosarcoma. The treatment of a pelvic chondrosarcoma is wide resection via either an internal hemipelvectomy or amputation. Chondrosarcoma requires surgical resection for control and does not traditionally respond to chemotherapy or external beam irradiation therapy. Pring M, Weber, KL, Unni KK, et al: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg 2001;83:1630-1642.
References:
- Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 255.
Question 28High Yield
Examination of the shoulder seen in Figure 52 shows atrophy and tenderness of the infraspinous fossa and profound weakness in external rotation. The supraspinous fossa shows normal muscle bulk. What is the most likely cause of this condition?
Explanation
Compression of the suprascapular nerve by a ganglion cyst is a well-documented cause of pain and weakness in the shoulder. Isolated involvement of the infraspinatus indicates that the area of entrapment is at the spinoglenoid notch and not the suprascapular notch. The majority of ganglion cysts found in the shoulder are related to tears of the labrum. When such a compressive lesion is found, decompression can be accomplished through either an open or arthroscopic approach. Several authors have shown the value of arthroscopy in the treatment of this condition. It has been shown that it is technically possible to decompress a paralabral ganglion cyst using arthroscopy; this method is usually followed by repair of the torn labrum. Alternatively, arthroscopic repair of the labrum can be performed and the cyst may be aspirated at the time of surgery. Open cyst excision through a posterior approach is also an acceptable method of treatment. Schickendantz MS, Ho CP: Suprascapular nerve compression by a ganglion cyst: Diagnosis by magnetic resonance imaging. J Shoulder Elbow Surg 1993;2:110-114. Thompson RC, Schneider W, Kennedy T: Entrapment neuropathy of the inferior branch of the suprascapular nerve by ganglia. Clin Orthop 1982;166:185-187.
Question 29High Yield
Figures 31a and 31b show the radiograph and MRI scan of an otherwise normal 3-month-old infant who has a spinal deformity. MRI reveals no intraspinal anomalies. What is the next step in management?

Explanation
Congenital scoliosis in an infant warrants evaluation of the renal, cardiac, and neurologic systems because frequently there is concurrent pathology. Progression in this instance is possible but not certain; therefore, progression must be documented prior to any surgical intervention. Close observation with serial radiographs every 4 to 6 months is appropriate. All of the surgical options listed may be reasonable choices in the future, but cardiac evaluation is the most important issue at this time. Basu PS, Elsebaie H, Noordeen MH: Congenital spinal deformity: A comprehensive assessment at presentation. Spine 2002;27:2255-2259.
Question 30High Yield
A 23-year-old woman with a history of bilateral recurrent ankle sprains, progressive cavovarus feet, and a family history of high arches and foot deformities is seen for evaluation. Management consisting of bracing and physical therapy has been poorly tolerated. Heel varus is partially corrected with a Coleman block. There are thick calluses under the first metatarsal heads. Sensation to touch and Weinstein monofilament is normal. Tibialis anterior and peroneus brevis are weak but present. What is the most appropriate management?
Explanation
The history and presentation are consistent with type I Charcot-Marie-Tooth (CMT), the most common form of hereditary peripheral motor sensory neuropathy. Type I CMT is the most common, occurring in 50% of patients with CMT, and is characterized by marked slowing of motor neuron velocities, and inconsistent slowing of sensory neuron velocities. Peroneus longus to brevis transfer is indicated to release the overpull of the peroneus longus, and restore the eversion and dorsiflexion function of the peroneus brevis. A lateralizing calcaneal osteotomy with proximal translation is indicated to correct heel varus given that the Coleman block only allows for partial correction of heel varus. Proximal translation of the posterior tuber corrects for the increased calcaneal dorsiflexion, improving the lever arm for the triceps surae. A medial column closing wedge osteotomy is often required to correct a rigid, or semirigid plantar flexed first ray to allow for a balanced, plantigrade foot. Triple arthrodesis is indicated for rigid, arthritic hindfoot deformities. Transfer of the posterior tibial tendon to the tibialis anterior is not indicated since it is an out-of-phase transfer. Transfer of the posterior tibial tendon, when performed, should be to the lateral aspect of the foot. A medializing calcaneal osteotomy would accentuate the heel varus. There is no indication for Botox in CMT; Botox injection of the calf would further weaken push-off during gait. Bracing of a progressive semirigid or rigid deformity is not recommended. Younger AS, Hansen ST Jr: Adult cavovarus foot. J Am Acad Orthop Surg 2005;13:302-315. Sammarco GJ, Taylor R: Cavovarus foot treated with combined calcaneus and metatarsal ostetotomies. Foot Ankle Int 2001;22:19-30.
Question 31High Yield
You are asked to evaluate the patient whose current clinical photographs are shown in Figures 46a and 46b following aortic valve replacement 9 days ago. He is currently taking anticoagulation medication. He has no systemic signs of sepsis. What is the best management?
Explanation
Explanation
46b These lesions are emboli related to the cardiac surgery, and the patient is already on anticoagulation medication. The foot reveals no signs consistent with gangrene or infection. Unless the patient shows local or systemic signs of sepsis, the best management is observation. It is unlikely that formal debridement will be necessary. Bowker JH, Pfeiffer MA (eds): The Diabetic Foot. St Louis, MO, Mosby, 2001, pp 219-260.
Question 32High Yield
A 25-year-old woman with a healed proximal tibiofibular fracture treated with an intramedullary nail 2 years ago is currently wearing an ankle-foot orthosis (AFO) and reports a persistent foot drop. She is unhappy with the AFO and has not seen any functional improvement despite months of physical therapy. Serial electromyograms (EMG) show no recent change over the past year. Examination and EMG findings are consistent with a tibialis anterior 1/5, extensor hallucis longus 2/5, extensor digitorum longus 2/5, posterior tibial tendon (PTT) 5/5, peroneals 3/5, flexor hallucis longus 5/5, and gastrocsoleus 5/5. No discrete nerve lesion was identified. The patient has a flexible equinovarus contracture. What is the most appropriate management?
Explanation
This pattern of injury is consistent with an unrecognized compartment syndrome of the anterior and lateral compartments. Transfer of the PTT through a long incision in the interosseous membrane corrects the foot drop deformity, and allows adequate dorsiflexion provided that the tendon to be transferred has a strength of 5/5. Muscles/tendons typically lose one grade of strength after transfer. Transfer into the tendons at the level of the ankle prevents overtensioning or pullout of a PTT tendon that is not long enough. Debridement of the scarred muscle in the anterior compartment decreases the risk of scarring down to the tendon transfer. Transfer of the peroneus longus is not preferred given its relative lack of strength and line of pull. Continued therapy and bracing are unlikely to lead to further improvement at 2 years after injury. An ankle fusion would correct the foot drop but would not address the tendon imbalances between the tibialis anterior and the peroneus longus, and the PTT and the peroneus brevis. Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 192. Atesalp AS, Yildiz C, Komurcu M, et al: Posterior tibial tendon transfer and tendo-Achilles lengthening for equinovarus foot deformity due to severe crush injury. Foot Ankle Int 2002;23:1103-1106. Scott AC, Scarborough N: The use of dynamic EMG in predicting the outcome of split posterior tibial tendon transfers in spastic hemiplegia. J Pediatr Orthop 2006;26:777-780.
Question 33High Yield
A 21-year-old professional baseball player has had painful catching and stiffness in his dominant right elbow for the past year. Examination reveals a flexion contracture of 2 degrees and mild pain with full elbow flexion. Radiographs are shown in Figures 33a and 33b. The most effective management should consist of

Explanation
The radiographs show osteochondritis dissecans of the capitellum and a loose body in the anterior compartment. Arthroscopic removal is indicated because symptoms referable to the loose body are present. Baumgarten TE: Osteochondritis dissecans of the capitellum. Sports Med Arthroscopy Rev 1995;3:219-223.
Question 34High Yield
Which of the following is considered the appropriate initial management protocol for an unconscious football player without spontaneous respirations?
Explanation
The on-field evaluation and management of the seriously injured athlete requires advance preparation and planning. It is imperative that the health care team have a game plan in place and the proper equipment readily available. The initial step consists of stabilizing the head and neck by manually holding the head and neck in a neutral position. Then, in the following order, check for breathing, pulses, and level of consciousness. If the athlete is breathing, simply remove the mouth guard and maintain the airway. If the athlete is not breathing, the face mask must be removed and the chin strap left in place. An open airway must be established, followed by assisted breathing. CPR is only instituted when breathing and circulation are compromised. If the athlete is unconcious or has a suspected cervical spine injury, the helmet must not be removed until the athlete has been transported to an appropriate facility and the cervical spine has been completely evaluated. McSwain NE, Garnelli RL: Helmet removal from injured patients. Bull Am Coll Surg 1997;82:42-44. Vegso JJ, Lehman RC: Field evaluation and management of head and neck injuries. Clin Sports Med 1987;6:1-15.
Question 35High Yield
Figure 50 shows the cross table lateral radiograph of a 31-year-old paratrooper who has recalcitrant groin pain. The pain is worse after activities such as standing or sitting (driving). Examination reveals that pain can be reproduced by internal rotation of the leg with the hip and knee in 90 degrees of flexion. Extensive nonsurgical managment has failed to provide relief. What is the treatment of choice?
Explanation
The radiograph reveals the classic "bump" that is seen in patients with femoroacetabular impingement (FAI). Ganz and associates described two types of FAI. This patient has cam impingement, which describes a nonspherical femoral head being forced into the acetabulum during hip motion and resulting in labral and chondral injury. Hip arthroscopy and labral debridement is unlikely to control the symptoms because the underlying anatomic abnormality is often difficult to address with arthroscopy. The treatment involves surgical dislocation of the hip with preservation of the blood supply to the femoral head, removal of the asphericity on the femoral side (femoral osteoplasty), and removal of the acetabular rim (acetabular osteoplasty) if the latter is found to contribute to impingement. Ganz R, Gill TJ, Gautier E, et al: Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-1124. Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for early osteoarthritis of the hip. Clin Orthop 2003;417:112-120.
Question 36High Yield
A 54-year-old woman sustained an elbow injury 3 months ago that was treated with open reduction and internal fixation. She now reports pain and limited elbow motion. Radiographs are shown in Figures 10a and 10b. Treatment should now consist of

Explanation
Radiographs reveal malunion of a Monteggia fracture-dislocation. Dislocation of the posterior radial head is caused by the malunited ulnar fracture. The deformity includes shortening with an apex posterior angulation. In the acute setting, open reduction of the radial head rarely is necessary; however, in chronic dislocations, open reduction is required. Without ulnar osteotomy, recurrent radial head dislocation is likely.
Question 37High Yield
A 50-year-old electrician who is right-hand dominant has had right shoulder pain and stiffness after sustaining an electric shock 2 months ago. An AP radiograph obtained at the time of injury was considered negative, and the patient was diagnosed with a shoulder sprain. The patient now reports continued shoulder pain and restricted motion. AP and axillary radiographs and a CT scan are shown in Figures 41a through 41c. Management should consist of


Explanation
Open reduction and transfer of the subscapularis and lesser tuberosity into the humeral head defect is the treatment of choice for chronic posterior dislocations in which the articular defect consists of 20% to 40% of the articular surfaces. Closed reduction can be used if the dislocation is recognized early and the articular defect is less than 20% of the articular surface. Humeral arthroplasty is reserved for patients with an articular defect that is greater than 45% to 50% of the head. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 38High Yield
A 23-year-old man reports pain on the superior aspect of his right shoulder with repetitive overhead activities and when lying on his right side. Figure 29 shows an axial MRI scan. What is the most likely diagnosis based on the MRI findings?
Explanation
Explanation
Os acromiale represents a failure of fusion of the anterior acromial apophysis and has been reported in approximately 8% of the population. Patients with a symptomatic os acromiale often report impingement-type symptoms with pain over the superior acromion, especially with overhead activities or sleeping. When nonsurgical management is unsuccessful, surgical options include excision, open reduction and internal fixation, and arthroscopic decompression. Kurtz CA, Humble BJ, Rodosky MW, et al: Symptomatic os acromiale. J Am Acad Orthop Surg 2006;14:12-19.
References:
- Ortiguera CJ, Buss DD: Surgical management of the symptomatic os acromiale. J Shoulder Elbow Surg 2002;11:521-528.
Question 39High Yield
A 62-year-old man with a long history of ankylosing spondylitis has neck pain after lightly bumping his head on the wall. Examination reveals neck pain with any attempted motion; the neurologic examination is normal. Plain radiographs show extensive ankylosis of the cervical spine and kyphosis but no fracture. What is the next most appropriate step in management?
Explanation
A high level of suspicion must be given for a fracture in any patient with ankylosing spondylitis who reports neck pain, even with minimal or no trauma. The neck should be immobilized in its normal position, which is often kyphotic, and plain radiographs should be obtained. If no obvious fracture is seen, CT with reconstruction should be obtained. The placement of in-line traction can have catastrophic effects because it may malalign the spine. Brigham CD: Ankylosing spondylitis and seronegative spondyloarthropathies, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 724-727.
Question 40High Yield
Which of the following factors has the greatest effect on the pull-out strength of a lumbar pedicle screw?
Explanation
All of the factors listed contribute to some extent to the pull-out strength of lumbar pedicle screws, but bone mineral density correlates most precisely. Wittenberg RH, Shea M, Swartz DE, et al: Importance of bone mineral density in instrumented spine fusions. Spine 1991;16:647-652.
Question 41High Yield
A 6-year-old Little League pitcher has had pain in the right elbow for the past 2 weeks. Examination reveals mild lateral elbow joint tenderness with full range of motion and no effusion or collateral laxity. A radiograph is shown in Figure 38. Initial management should consist of
Explanation
Explanation
The radiograph shows osteochondritis dissecans (OCD) of the capitellum, one manifestation of "pitcher's elbow." The lesion is nondisplaced, and healing is possible if the inciting throwing activities are curtailed. Long arm cast treatment may be reasonable for the noncompliant patient but should not exceed 6 weeks duration. Surgical treatment is indicated for loose bodies or cartilage flaps. Elbow OCD lesions are now being seen in younger children as more participate in organized sports, especially baseball and gymnastics. Bauer M, Jonsson K, Josefsson PO, et al: Osteochondritis dissecans of the elbow: A long-term follow-up study. Clin Orthop 1992;284:156-160. Takahara M, Ogino T, Sasaki I, et al: Long term outcome of osteochondritis dissecans of the humeral capitellum. Clin Orthop 1999;363:108-115.
References:
- Byrd JW, Jones KS: Arthroscopic surgery for isolated capitellar osteochondritis dissecans in adolescent baseball players: Minimum three-year follow-up. Am J Sports Med 2002;30:474-478.
Question 42High Yield
A 20-year-old professional female jockey who is wearing a helmet is thrown from her horse. What is the most likely location of her injury?
Explanation
The incidence of injury associated with horseback rising is estimated to be one per 350 riding hours to one per 1,000 riding hours. Of these injuries, approximately 15% to 27% are severe enough to warrant hospital admission. Significant and serious injuries in equestrian activities are associated with recreational riders and those not wearing a helmet. Head and spine injuries are more common in recreational and nonhelmeted riders. Extremity injuries are more common in professional and helmeted riders. Professional riders are less likely to be admitted to the hospital than recreational riders, and are about half as likely to be disabled at 6 months after injury as recreational riders. Lim J, Puttaswamy V, Gizzi M, et al: Pattern of equestrian injuries presenting to a Sydney teaching hospital. ANZ J Surg 2003;73:567-571.
Question 43High Yield
A 42-year-old man who is right-hand dominant injured his right shoulder when he fell from a ladder onto his outstretched arm 1 hour ago. Radiographs reveal a two-part greater tuberosity anterior fracture-dislocation. Initial management should consist of
Explanation
Greater tuberosity anterior fractures associated with anterior glenohumeral dislocations respond very well to closed methods in the majority of patients. Closed reduction of the glenohumeral joint often anatomically reduces the greater tuberosity into its cancellous bed, without the need for open fixation or cuff repair. Once closed reduction of the joint is performed, tuberosity displacement and joint articulation should be evaluated radiographically with AP and scapular lateral views as well as an axillary view. The axillary view will not only definitively show the joint articulation but also demonstrate posterior displacement of the greater tuberosity missed on the AP and lateral views. If no or minimal (5 mm) displacement is found, then nonsurgical management consisting of a sling and gentle passive range-of-motion exercises can be instituted. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Question 44High Yield
A 60-year-old woman has activity-related hip pain after undergoing arthroplasty 5 years ago. She has severe Parkinsonism and denies fevers or chills. Radiographs are shown in Figures 45a and 45b. What is the most likely cause of her pain?

Explanation
The radiographs reveal both cement debonding at the lateral shoulder of the prosthesis and a cement mantle fracture. Both of these indicate a loose femoral component. The radiographs show a stress fracture with reactive bone on the lateral femoral cortex in conjunction with the cement mantle fracture. The acetabular component shows no evidence of loosening. Heterotopic bone usually is not a source of pain when it is Brooker grade I, as in this case. Parkinsonism generally is not associated with hip pain. Harris WH, McCarthy JC, O'Neill DA: Femoral component loosening using contemporary techniques of femoral cement fixation. J Bone Joint Surg Am 1982;64:1063-1067. Callaghan JJ, Rosenberg AG, Rubash H (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 960, 1228-1229.
Question 45High Yield
A 35-year-old woman who is training for a triathlon has had a 2-month history of heel pain with weight bearing and is unable to run. History reveals that she is amenorrheic. Examination reveals that she is thin and has pain over the heel that is exacerbated with medial and lateral compression. Range of motion and motor and sensory function are normal. Radiographs are normal. What is the most likely diagnosis?
Explanation
Explanation
The most likely diagnosis is a stress fracture of the calcaneus and is supported by the history of running, female gender, and amenorrhea. Reproducing pain with medial and lateral compression of the heel also supports the diagnosis. A bone scan or MRI would most likely confirm the diagnosis. Plantar fasciitis would result in pain on the bottom of the heel with point tenderness. The lack of other areas of involvement or other symptoms does not support a seronegative inflammatory arthritis. Tarsal tunnel syndrome and peripheral neuropathy are unlikely because of the normal neurologic examination. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
References:
- Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 179-191.
Question 46High Yield
An 18-year-old gymnast has had a 1-year history of foot pain. Examination reveals medial midfoot tenderness without swelling. Non-weight-bearing in a cast for 6 weeks has failed to provide relief. An axial CT scan of the midfoot is shown in Figure 20. What is the optimal treatment for this condition?
Explanation
Stress fractures of the navicular are often seen in running and jumping sports. Whereas most individuals heal with nonsurgical management consisting of 6 weeks of casting, this gymnast has had pain for 1 year and nonsurgical management has failed. Open reduction with bone grafting is the preferred treatment. Quirk RM: Stress fractures of the navicular. Foot Ankle Int 1998;19:494-496.
Question 47High Yield
A 24-year-old man sustains an injury to his right elbow after falling 10 feet. Radiographs are shown in Figures 41a and 41b. Treatment should consist of
Explanation
Explanation
41b Transolecranon fracture-dislocations are most effectively managed with open reduction and internal fixation, followed by early aggressive range of motion. Concomitant injury to the collateral ligament is rare, and stability is achieved by anatomic reconstruction of the olecranon fracture with rigid fixation. The need for collateral ligament repair or a hinged external fixator is uncommon in this fracture pattern.
References:
- Ring D, Jupiter JB, Sanders RW, et al: Transolecranon fracture-dislocation of the elbow. J Orthop Trauma 1997;11:545-550.
Question 48High Yield
In Figure 14, the primary fracture line in a calcaneal fracture is best depicted by which of the following schematics?
Explanation
The schematic labeled A best depicts the primary fracture line in a calcaneal fracture. The primary fracture line in an axial-loading fracture of the calcaneus occurs from superior-lateral to inferior-medial. This fracture line separates the calcaneus into sustentacular and tuberosity fragments and typically enters the subtalar joint through the posterior facet. Although additional fracture lines typically occur, the primary fracture line is almost always present. If surgical reduction is planned, reducing the primary fracture is always a key step. Macey LR, Benirschke SK, Sangeorzan BJ, Hansen ST: Acute calcaneal fractures: Treatment option and results. J Am Acad Orthop Surg 1994;2:36-43.
Question 49High Yield
Figure 12a shows the clinical photograph of a 36-year-old man who has left shoulder pain and dysfunction after undergoing a lymph node biopsy 2 years ago. The appearance of the shoulder during abduction and a wall push-up maneuver is shown in Figures 12b and 12c, respectively. Which of the following procedures provides the best pain relief and function?
Explanation
Explanation
12b 12c Injury to the spinal accessory nerve can occur after penetrating trauma to the shoulder. Blunt trauma may also cause loss of trapezius function. Most commonly, surgical dissection in the posterior triangle of the neck, such as lymph node biopsy, may expose the nerve to possible damage. Surgical repair of the nerve may be considered up to 1 year after injury; after this time muscle transfer is usually associated with a better functional outcome. Steinman SP, Spinner RJ: Nerve problems in the shoulder, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1013-1015.
References:
- Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop Relat Res 1999;368:5-16.
Question 50High Yield
Bioabsorbable polymers are used in a wide range of orthopaedic devices, including anchors, staples, pins, plates, and screws. What is the primary drawback for bioabsorbable implants?
Explanation
A number of bioabsorbable polymers are used in orthopaedic applications, and all have in common reports of foreign body reactions, which occur in more than 50% of patients in some series. In general, the high cost of these polymers is offset by the elimination of a second surgery to remove the implant. Bioabsorbable polymers are low strength in comparison to metallic alloys but of sufficient strength for many orthopaedic applications. The elastic modulus is not as high as many other orthopaedic biomaterials, making them suitable for applications where lower stiffness is an asset. Ambrose CG, Clanton TO: Bioabsorbable implants: Review of clinical experience in orthopedic surgery. Ann Biomed Eng 2004;32:171-177.
Question 51High Yield
Figure 20 shows the resting and stress radiographs of a patient who has had pain and feelings of instability after undergoing a total knee arthroplasty 1 year ago. Which of the following ligaments is not functional and is therefore responsible for the patient's symptoms?
Explanation
Explanation
The radiographs show posterior instability caused by an absent posterior cruciate ligament. The tibia is significantly displaced posteriorly with respect to the femur. This can be demonstrated with a lateral radiograph obtained with the knee in flexion. The anterior cruciate ligament has been resected but is not responsible for the instability shown.
References:
- Incavo SJ, Churchill DL: The role of the posterior cruciate ligament in total knee arthroplasty. Techniques Orthop 1999;14:267-273.
Question 52High Yield
A 29-year-old woman reports shoulder pain after sustaining a minor fall 6 weeks ago. She has a history of celiac sprue. Radiographs of the forearm and shoulder are shown in Figures 53a and 53b. Which of the following serum abnormalities would be expected?
Explanation
Explanation
53b Celiac sprue results in rapid gastrointestinal transit and fatty stools that impair the absorption of calcium and vitamin D and result in nutritional-deficiency osteomalacia with secondary hyperparathyroidism. The radiographs show marked osteopenia with brown tumors. A pathologic fracture is seen in the proximal humerus through a large brown tumor. Serum findings include low or normal calcium, low phosphate, elevated alkaline phosphatase, low 1,25(OH)2D, and increased PTH levels. Secondary hyperparathyroidism is associated with a variety of conditions including malabsorption syndromes. Potts JT: Parathyroid hormone: Past and present. J Endocrinol 2005;187:311-325. Corazza GR, Di Stefano M, Maurino E, et al: Bones in coeliac disease: Diagnosis and treatment. Best Pract Res Clin Gastroenterol 2005;19:453-465.
References:
- Mankin HJ, Mankin CJ: Metabolic bone disease: An update. Instr Course Lect 2003;52:769-784.
Question 53High Yield
Dislocation following primary total hip arthroplasty is more likely to occur in which of the following situations?
Explanation
Explanation
Dislocation following total hip arthroplasty is twice as common in women than in men. It is more likely to occur in older patients. There is no clear association between dislocation and the method of fixation or the type of bearing, so long as the bearing diameter is the same.
References:
- Berry DJ: Dislocation, in Steinberg ME (ed): Revision Total Hip Arthroplasty. Philadelphia, PA, 1999, pp 463-482.
Question 54High Yield
Kinematic analysis of the medial and lateral menisci has demonstrated that the lateral meniscus has which of the following characteristics compared with the medial meniscus?
Explanation
Explanation
Kinematic analysis of both menisci demonstrates anterior movement with extension and posterior movement with flexion. The lateral meniscus has more mobility than the medial meniscus because of less soft-tissue attachments. Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. New York, NY, Churchill Livingstone, 2001, vol 1, p 474. Thompson WO, Thaete FL, Fu FH, et al: Tibial meniscal dynamics using 3D reconstructions of MR images, in Proceedings of the Orthopaedic Research Society 1990;389.
References:
- Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 15-28.
Question 55High Yield
Which of the following is NOT considered a risk factor for nonunion of a type II odontoid fracture?
Explanation
Although obesity can make brace or halo wear difficult, it has not been associated with an increased risk for nonunion. Carson GD, Heller JG, Abitbol JJ, et al: Odontoid fractures, in Levine AM, Eismont FJ, Garfin SR, et al (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 235-238.
Question 56High Yield
A 16-year-old girl has had pain in the left groin for the past 4 months. She notes that the pain is worse at night; however, she denies any history of trauma and has no constitutional symptoms. There is no history of steroid or alcohol use. Examination reveals pain in the left groin with rotation of the hip. There is no associated soft-tissue mass. A radiograph and MRI scan are shown in Figures 32a and 32b, and biopsy specimens are shown in Figures 32c and 32d. What is the most likely diagnosis?

Explanation
Based on the epiphyseal location and sharp, well-defined borders, the radiograph suggests chondroblastoma. Histologically, multinucleated giant cells are scattered among mononuclear cells. The nuclei are homogenous and contain a characteristic longitudinal groove. Although not seen here, "chicken-wire calcification" with a bland giant cell-rich matrix is also typical for chondroblastoma. Clear cell chondrosarcoma occurs in epiphyseal locations but has a more aggressive histologic pattern and occurs in an older age group. Giant cell tumors occur in the epiphysis but have a more uniform giant cell population histologically. Aneurysmal bone cyst often results in bone remodeling and has a different pathologic appearance. Osteonecrosis has a typical histologic pattern of empty lacunae and necrotic bone. Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755. Simon M, Springfield D, et al: Chrondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Question 57High Yield
Figure 3a shows the preoperative radiograph of a 5-year-old girl who achieved complete correction with valgus osteotomies. Figure 3b shows a radiograph obtained 2 years later. What is the cause of the recurrent deformity on the right side?
Explanation
Explanation
3b Although inadequate correction, obesity, patient age of older than 5 years and an increased metaphyseal-diaphyseal angle are all associated with a poorer outcome, the radiographs show a growth arrest of the medial tibial physis. If not recognized and treated with early surgery, progressive genu varum will occur with continued growth of the lateral physis. In addition to repeat osteotomy, options for treating the arrest include physeal bar resection or, as necessary, completion of the growth arrest by epiphyseodesis of the lateral physes, followed by a limb equalization procedure at a later date. Brooks WC, Gross RH: Genu varum in children: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:326-335. Herring JA: Tachdjian's Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, pp 840-950.
References:
- Schoenecker PL, Rich MM: The lower extremity, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 1068-1073.
Question 58High Yield
A 35-year-old man is seen in the emergency department with a bullet wound to the foot that occurred 2 hours ago. Examination reveals a 0.5-cm entrance wound on the dorsum of the foot and a 1.5-cm exit wound on the plantar aspect. Exploration of the plantar wound in the emergency department reveals bone and metal fragments. Radiographs reveal a comminuted, unstable fracture of the base of the first metatarsal and cuneiform. Management should consist of tetanus toxoid, and
Explanation
Explanation
The patient sustained a type I unstable fracture that requires debridement of superficial fragments from the sole and surgical stabilization. Low-velocity wounds less than 8 hours old are considered type I open fractures. In contrast, gunshot wounds with associated fractures more than 8 hours old are considered type II open fractures using the Gustilo and Anderson classification. Gustilo type I stable fractures due to gunshot wounds and seen within 8 hours can be treated with tetanus toxoid (if no history of immunization or booster within 5 years), surface irrigation, and casting or a hard sole shoe. Antibiotics are not required unless gross contamination is present. However, if the extent of contamination is unclear, or if a joint is penetrated, then routine antibiotic prophylaxis is recommended. Indications for surgery include: articular involvement, unstable fractures, presentation 8 or more hours after injury, tendon involvement, and superficial fragments in the palm or sole. Type I unstable fractures may be stabilized with internal or external fixation. Type II unstable fractures should be treated with external fixation and repeat debridements until clean. Holmes GB Jr: Gunshot wounds of the foot. Clin Orthop Relat Res 2003;408:86-91.
References:
- Bartlett CS, Helfet DL, Hausman MR, et al: Ballistics and gunshot wounds: Effects on musculoskeletal tissues. J Am Acad Orthop Surg 2000;8:21-36.
Question 59High Yield
Which of the following palpable bony landmarks is correctly matched with its corresponding vertebral level?
Explanation
The carotid tubercle is usually located at the level of C6. The angle of the mandible is at C1-C2; the hyoid is at C4; the superior portion of the thyroid cartilage is C4-C5; and the cricoid cartilage is at C6. Smith GW, Robinson RA: The treatment of certain cervical-spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am 1958;40:607.
Question 60High Yield
Figures 17a and 17b show the radiographs of a 32-year-old professional athlete who sustained an injury to the first metatarsal. A view of the opposite noninjured side is shown in Figure 17c. Management of the fracture should consist of
Explanation
Explanation
17b 17c Parameters for first metatarsal fracture management are different than for shaft fractures of the central second, third, and fourth metatarsals. The first metatarsal carries a greater load and if malunited, can create transfer lesions by virtue of uneven weight distribution; therefore, nonsurgical management is not indicated for this patient. Percutaneous pinning is not as likely to result in an anatomic reduction as open reduction and internal fixation. As his livelihood depends on an expeditious return to function, the choice of open reduction and internal fixation allows for earlier motion and rehabilitation. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 64-65.
References:
- Shereff MJ: Compartment syndromes of the foot. Instr Course Lect 1990;39:127-132.
Question 61High Yield
A 60-year-old woman with a history of breast cancer has progressive paraparesis. The MRI scan is shown in Figure 28. What form of management is most likely to restore or maintain ambulation?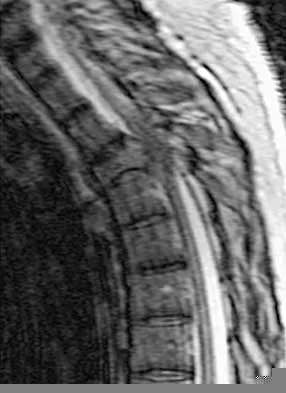
Explanation
Surgical decompression and stabilization have been shown to be the most effective means of improving neurologic function. Decompression is most reliably done from the side of the compression, which is anterior in this patient. Harrington KD: Metastatic tumors of the spine: Diagnosis and treatment. J Am Acad Orthop Surg 1993;1:76-86.
Question 62High Yield
A 53-year-old man with a history of severe left hip pain has a significant limp that is the result of a 5-cm limb-length discrepancy. An AP radiograph is shown in Figure 48. The underlying etiology is most likely related to a history of
Explanation
Radiographic abnormalities such as coxa magna, coxa breva secondary to growth arrest, and coxa plana and acetabular deformities are associated with healed Legg-Calve-Perthes disease. Femoral heads that were flat yet congruent with the acetabulum are at risk for disabling arthritis in the sixth decade of life in 50% of these untreated patients. As the normal ball-and-socket joint deforms to a flattened cylinder, the hip loses abduction and rotation capability, while retaining flexion and extension potential. If the femoral head is flat and is not concentric with the acetabulum, early severe arthritis occurs. Hinge abduction and anterior impingement are known sequelae of a flat, incongruent femoral head.
Question 63High Yield
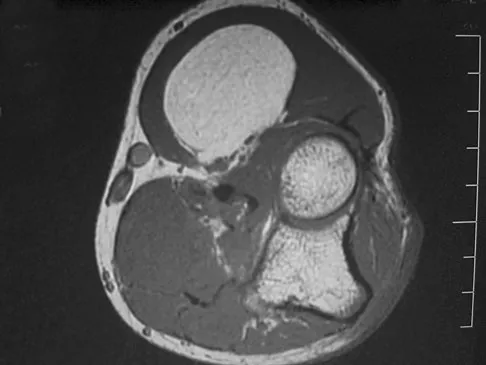
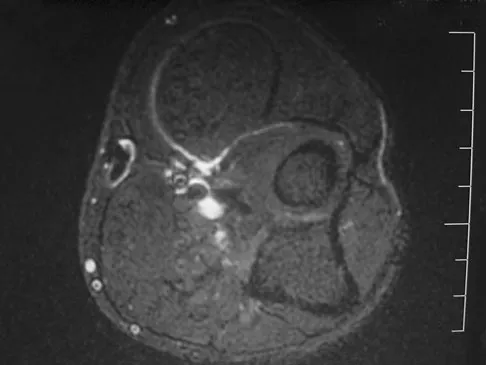
A 33-year-old man reports an enlarging painful soft-tissue mass in his right forearm. A radiograph and MRI scans are shown in Figures 45a through 45c. Treatment should consist of
Explanation
An intramuscular lipoma is a benign soft-tissue lesion that can grow and has a small risk of progressing to a liposarcoma. Radiographs usually show a globular radiolucent mass adjacent to higher-density muscle tissue shadows. When the patient has symptoms and reports an increase in size of the mass, the treatment of choice after appropriate radiographic analysis is complete excision of the mass with marginal resection. Sampling error is a problem with fatty lesions and core or incisional biopsies are frequently unnecessary, especially if an MRI scan of the lesion shows signal intensity that matches subcutaneous fat on all sequences. Damron TA: What to do with deep lipomatous tumors. Instr Course Lect 2004;53:651-655. Gaskin CM, Helms CA: Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): Results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol 2004;182:733-739.
Question 64High Yield
Which of the following anatomic changes is observed as part of the normal aging process of the adult spine?
Explanation
The primary change that takes place in the aging spine is degeneration of the lumbar disks and loss of the overall lumbar lordosis. This also may be associated with osteopenic-related compression fractures. With these changes, the sagittal vertical line moves anteriorly relative to the sacrum; cervical scoliosis is uncommon and not part of the normal aging process. Overall kyphosis in the thoracic spine gradually increases, but the coronal balance remains essentially the same unless scoliosis develops. Gelb DE, Lenke LG, Bridwell KH, et al: An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine 1995;20:1351-1358.
Question 65High Yield
In a retroperitoneal approach to the lumbar spine, what nerve is commonly found on the psoas muscle?
Explanation
The genitofemoral nerve and the sympathetic plexus consistently lie on the ventral surface of the psoas muscle. The ilioinguinal and iliohypogastric nerves are the most superior branches of the lumbar plexus and emerge along the upper lateral border of the psoas muscle traveling toward the quadratus lumborum. Both the obturator and femoral nerves are deep and lateral to the psoas muscle. Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer-Verlag, 1983, p 107. Johnson R, Murphy M, Southwick W: Surgical approaches to the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1559.
Question 66High Yield
Which of the following complications is uniquely associated with an anterior approach to the lumbosacral junction?
Explanation
Explanation
Retrograde ejaculation is a sequela of injury to the superior hypogastric plexus. The structure needs protection, especially during anterior exposure of the lumbosacral junction. The use of monopolar electrocautery should be avoided in this region. The ideal exposure starts with blunt dissection just to the medial aspect of the left common iliac vein, sweeping the prevertebral tissues toward the patient's right side. Although erectile dysfunction can be seen after spinal surgery, it is not typically related to the surgical exposure because erectile function is regulated by parasympathetic fibers derived from the second, third, and fourth sacral segments that are deep in the pelvis and are not at risk with the anterior approach. The other choices are complications of spinal surgery but are not uniquely associated with an anterior L5-S1 exposure. Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492. Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer-Verlag, 1983, p 107.
References:
- An HS, Riley LH III: An Atlas of Surgery of the Spine. New York, NY, Lippincott Raven, 1998, p 263.
Question 67High Yield
Figure 17 shows the radiograph of a 25-year-old professional football player who has superior shoulder pain that prevents him from sports participation. History reveals that he sustained a shoulder injury that was treated with closed reduction and temporary pinning 3 years ago. The best course of action should be
Explanation
The radiograph shows a complete acromioclavicular separation. Because the patient is a professional athlete who is unable to participate, surgery is indicated. Chronic separations, especially those with previous trauma from joint pinning, should be treated with resection of the distal clavicle and stabilization to the coracoid. Some type of biologic reconstruction of the coracoclavicular ligaments is generally recommended. Open repair of the ligaments is generally not possible in such a delayed fashion. Screw fixation alone will not provide a lasting solution as the screws usually need to be removed, leaving no fixation in place. Reconstruction using the coracoacromial ligament is generally recommended with coracoclavicular fixation to protect the repair while it heals. Nuber GW, Bowen MK: Disorders of the acromioclavicular joint: Pathophysiology, diagnosis and management, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999.
Question 68High Yield
A 26-year-old woman who noted right-sided lumbosacral pain 10 days ago while vacuuming now reports that the pain has intensified. She denies any history of back problems. No radicular component is present, and her neurologic examination is normal. The next most appropriate step in management should consist of
Explanation
Explanation
The initial management of a lumbar strain should consist of 2 to 3 days of bed rest when symptoms are severe, activity restrictions, and nonsteroidal anti-inflammatory drugs. It has been estimated that 60% to 80% of the adult population experiences back pain, with 2% to 5% affected yearly. Spontaneous improvement generally will occur within 4 weeks. Further study is indicated by the presence of radiculopathy, weakness, trauma, or suspicion of malignancy. Bigos S, Boyer O, Braen GR, et al: Acute low back pain in adults: Clinical practice guideline No. 14. AHCPR Publication No. 95-0642. Rockville, MD, Agency for Health Care Policy and Research, Public Health Service, US Department of Health and Human Services, December, 1994.
References:
- Deyo RA: Conservative therapy for low back pain: Distinguishing useful from useless therapy. JAMA 1983;250:1057-1062.
Question 69High Yield
In the spine, osteoblastomas usually originate in the
Explanation
Osteoblastomas are benign lesions that represent less than 5% of benign bone tumors. Most lesions are located in the spine, followed by the femur, tibia, and skull. Patients with spinal lesions usually have pain that may be associated with scoliosis. The most common location in the spine is within the posterior elements.
Question 70High Yield
Figures 25a and 25b show the radiographs of a 66-year-old man who has had a long history of bilateral painful flatfoot deformities. Examination reveals that his foot is partially correctable passively, albeit with discomfort, and he has an Achilles tendon contracture. An ankle-foot orthosis has failed to provide relief. Treatment should now consist of

Explanation
The patient has a pronounced deformity with pain and degenerative arthritis; therefore, triple arthrodesis is the treatment of choice. Gastrocnemius or Achilles tendon lengthening may be a necessary adjunct to the triple arthrodesis, but alone is inadequate to allow for correction. Because the ankle-foot orthosis has failed to provide relief, a UCBL is not likely to help. Osteotomy procedures are designed for lesser deformities and well-preserved joints. Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 115-120.
Question 71High Yield
An 8-year-old boy reports progressive difficulty with walking. Examination reveals muscle weakness, with proximal groups more affected than distal muscles. Deep tendon reflexes are within normal limits. Laboratory studies show a creatine kinase level of 7,200 IU. Based on these findings, what is the most likely diagnosis?
Explanation
Explanation
Patients with Becker muscular dystrophy have an abnormality in dystrophin, but unlike patients with Duchenne muscular dystrophy, some dystrophin is present. As a result, the progression of muscle weakness is slower, with the diagnosis typically made after age 8 years. Similar to patients with Duchenne muscular dystrophy, patients with Becker muscular dystrophy have pseudohypertrophy of the calves, markedly increased creatine kinase levels, and X-linked transmission of the condition. In addition, these patients are more prone to cardiomyopathy; a condition that should be carefully evaluated if any surgery is required. Patients with spinal muscular atrophy also have proximal muscle weakness, but the onset of weakness occurs earlier in childhood. These patients also have absent deep tendon reflexes and fasciculations, but pseudohypertrophy is absent and creatine kinase levels are normal. Patients with Emery-Dreifuss dystrophy may have a similar clinical picture to Becker's muscular dystrophy, but pseudohypertrophy is absent and creatine kinase levels are only mildly elevated. In addition, neck extension, elbow flexion, and ankle equinus contractures develop at an early age. Limb girdle dystrophy is a group of progressive muscular dystrophies that is not associated with pseudohypertrophy or a significant elevation of creatine kinase levels. Guillain-Barre syndrome is a condition associated with results from postinfectious demyelination of the peripheral nerve. These patients have the acute onset of weakness, hypotonia, and areflexia; creatine kinase levels are normal. Sussman MD: Muscular dystrophy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1573-1583.
References:
- Thompson GH, Berenson FR: Other neuromuscular disorders, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, vol 1, pp 633-676.
Question 72High Yield
Which of the following are considered characteristic features of degeneration of a disk?
Explanation
Explanation
Gradual dessication of the disk begins in the third decade as glycosaminoglycan levels within the nucleus begin to decline. The original water content of 88% decreases to 70% in the sixth decade and beyond. As glycosaminoglycan content decreases, there is a corresponding increase in noncollagen glycoprotein. Happey F, Weissman A, Naylor A: Polysaccharide content of the prolapsed nucleus pulposus of the human intervertebral disc. Nature 1961;192:868. Naylor A, Shentall R: Biomechanical aspects of intervertebral discs in aging and disease, in Jayson M (ed): The Lumbar Spine and Back Pain. New York, NY, Grune and Stratton Inc, 1976, pp 317-326.
References:
- Watkins RG, Collis JS: Lumbar Discectomy and Laminectomy. Rockville, MD, Aspen, 1987, pp 2-3.
Question 73High Yield
An 18-year-old woman sustains a twisting injury of the knee while skiing. Figures 7a and 7b show the radiograph and coronal MRI scan of the knee. In addition to the injury shown, what is the most likely associated injury?
Explanation
Explanation
7b The MRI scan shows a Segond fracture, which is a small avulsion of the lateral joint capsule from the anterolateral aspect of the proximal tibia. It is almost always associated with anterior cruciate ligament rupture and often with a tear of either the medial or lateral meniscus. Goldman AB, Pavlov H, Rubenstein D: The Segond fracture of the proximal tibia: A small avulsion that reflects major ligamentous damage. Am J Roentgenol 1988;151:1163-1167. Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
References:
- Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 74High Yield
A 32-year-old construction worker reports a persistent burning, tingling sensation on the dorsum of his right foot and significant sensitivity on the plantar surface after a 500-lb steel beam dropped on it 8 weeks ago. Initial radiographs revealed no fractures, and the skin remained intact at the time of injury. Physical therapy, anti-inflammatory drugs, and a serotonin reuptake inhibitor have failed to provide relief. What is the next most appropriate step in management?
Explanation
Explanation
Following failure of physical therapy and pharmacologic management in a patient with complex regional pain syndrome, the management of choice is sympathetic blocks. While continued physical therapy would be assistive, sympathetic blocks allow a more rapid relief of symptoms. Neurostimulation is not appropriate at this stage because of its invasive nature. Cepeda MS, Lau J, Carr DB: Defining the therapeutic role of local anesthetic sympathetic blockade in complex regional pain syndrome: A narrative and systematic review. Clin J Pain 2002;18:216-233. Perez RS, Kwakkel G, Zuurmond WW, et al: Treatment of reflex sympathetic dystrophy (CRPS type 1): A research synthesis of 21 randomized clinical trials. J Pain Symptom Manage 2001;21:511-526. Tran KM, Frank SM, Raja SN, et al: Lumbar sympathetic block for sympathetically maintained pain changes in cutaneous temperatures and pain perception. Anesth Analg 2000;90:1396-1401.
References:
- Stanton-Hicks M, Baron R, Boas R, et al: Complex regional pain syndromes: Guidelines for therapy. Clin J Pain 1998;14:155-166.
Question 75High Yield
A 22-year-old college basketball player who was hit from behind while going up for a rebound is rendered immediately quadraparetic for approximately 10 minutes, followed by complete resolution of motor loss and return of full sensation. The radiograph and MRI scan of the cervical spine shown in Figures 2a and 2b reveal a canal diameter of 13 mm, loss of cerebrospinal fluid space about the spinal cord, and no signal change within the cord. What is the best course of action?

Explanation
The correct decision on return to sports participation after episodes of transient quadraparesis is controversial. Cantu and Mueller feel strongly that the loss of cerebrospinal fluid space about the spinal cord signifies an unacceptable risk for future spinal cord injury if the athlete returns to sports. However, Watkins and Torg and Lasgow have reported no evidence of increased spinal cord injury in athletes with narrow spinal canals, even in football. These authors suggest judgment be used in advising return to contact or high-energy sports and that the physician's responsibility is to give accurate and relevant information, allowing the athlete to make his or her own choice regarding return to sports participation. Cantu R, Mueller FO: Catastrophic spine injuries in football (1977-1989). J Spinal Disord 1990;3:227-231. Watkins RG: Neck injuries in football players. Clin Sports Med 1986;5:215-246. Torg JS, Lasgow SG: Criteria for return to contact activities following cervical spine injury. Clin Sports Med 1991;1:12-26.
Question 76High Yield
What clinical parameter will most likely decrease the need for blood transfusion after total joint arthroplasty?
Explanation
Bilateral joint replacement, chronic disease, and preoperative autologous donation all increase the risk of needing blood. Young patients and a high hemoglobin level (greater than 15 g/dL) are considered clinical parameters that decrease the risk for requiring allogenic blood. Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 77High Yield
A 40-year-old woman with no history of back problems has a symptomatic L4-5 disk herniation with an L5 radiculopathy that has failed to respond to 12 weeks of nonsurgical management. In the preoperative discussion, the surgeon advises the patient that the chance of recurrence of the herniation after successful diskectomy is what percent?
Explanation
The incidence of recurrent disk herniation after a successful diskectomy is approximately 5% to 10%. Indications for surgical diskectomy for a recurrence are the same as for a primary diskectomy. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 685-698.
Question 78High Yield
A 19-year-old soccer player feels a pop in his knee while making a cut and notes the development of an effusion over several hours. Examination reveals medial joint line tenderness, but the knee is stable to manual stress testing of all ligaments. Examination under anesthesia confirms a stable knee. What is the most critical factor in determining healing after repair of the lesion shown in Figure 14?
Explanation
Explanation
Numerous clinical and basic science investigations have evaluated meniscal tear characteristics to identify factors that either promote or mitigate against meniscal healing. Complex tears have been noted to heal poorly, while longitudinal tears heal more predictably. Tear length, time from injury to repair, medial versus lateral meniscal tears, and the use of a fibrin clot have not been shown to consistently affect meniscal healing. However, rim width, the distance of the tear site from the peripheral meniscocapsular junction (vascular supply), has been shown to have a significant role in the ability of a meniscus repair to heal. DeHaven KE, Arnoczky SP: Meniscus repair: Basic science, indications for repair, and open repair. Instr Course Lect 1994;43:65-76.
References:
- Henning CE, Lynch MA, Clark JR: Vascularity for healing of meniscus repairs. Arthroscopy 1987;3:13-18.
Question 79High Yield
Which of the following best describes the relative content of the components of articular cartilage in decreasing order?
Explanation
Explanation
Water is the most abundant component of articular cartilage with a wet weight of 65% to 80%. Of the water, 80% is at the surface and 65% at the deep zone. Collagen accounts for 10% to 20% of the wet weight, with type II collagen accounting for 90% to 95% of the total collagen content. Small amounts of types V, VI, IX, X, and XI collagen are also present. Proteoglycans comprise 10% to 15% of the wet weight of collagen. The remainder of the wet weight is made up of other collagens, noncollagenous proteins, and chondrocytes.
References:
- Schiller AL: Pathology of osteoarthritis, in Kuettner KE, Goldberg VM: Osteoarthritic Disorders. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 95-101.
Question 80High Yield
A patient has had a locked posterior dislocation of the shoulder for the past 6 months. After undergoing total shoulder arthroplasty that includes adequate anterior releases and posterior capsulorrhaphy, the patient still exhibits posterior instability intraoperatively. The postoperative rehabilitation regimen should include
Explanation
Achieving stability in chronic locked posterior dislocations of the shoulder remains a difficult challenge. Intraoperative measures include decreased humeral retroversion, anterior releases, and posterior capsular tightening. Postoperative rehabilitation is of equal importance. Immobilization in an external rotation brace (10 degrees to 15 degrees) with the arm at the side for 4 to 6 weeks is recommended to decrease tension in the posterior capsule. When passive range-of-motion exercises are instituted, they should be performed in the plane of the scapula to avoid stress posteriorly. Internal rotation and supine elevation should be avoided for similar reasons. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 81High Yield
A 10-year-old girl has a midshaft both bone forearm fracture. After attempted closed reduction, alignment consists of bayonet apposition, 10 degrees of malrotation, and 8 degrees of volar angulation. Management should now consist of
Explanation
Acceptable alignment in both bone forearm fractures is related to age and location. In children younger than age 9 years, angulations of 15 degrees and malrotation of 45 degrees are acceptable. In children older than age 9 years, acceptable alignment is 10 degrees of angulation and 30 degrees of malrotation. Bayonet apposition is acceptable provided that the angular and rotational reductions are held within these guidelines. A long arm cast provides better control of deforming forces than a short arm cast. Do TT, Strub WM, Foad SL, et al: Reduction versus remodeling in pediatric distal forearm fractures: A preliminary cost analysis. J Pediatr Orthop B 2003;12:109-115. Flynn JM: Pediatric forearm fractures: Decision making, surgical techniques, and complications. Instr Course Lect 2002;51:355-360. Ring D, Waters PM, Hotchkiss RN, et al: Pediatric floating elbow. J Pediatr Orthop 2001;21:456-459.
Question 82High Yield
A 42-year-old woman has a history of nontraumatic ankle swelling with tenderness over the Achilles tendon and plantar fascia. She reports that while vacationing in Connecticut 2 months ago she noted the presence of a "red bull's eye" rash. Management should consist of
Explanation
The most likely diagnosis is Lyme disease because of the patient's recent vacation in an area with a high risk of exposure. The most effective treatment is doxycycline. Neu HC: A perspective on therapy of Lyme infection. Ann NY Acad Sci 1988;539:314-316.
Question 83High Yield
Figure 24 shows an axial MRI scan of the ankle. The arrowhead is pointing to what structure?
Explanation
Explanation
The peroneus brevis is easily identified by its location behind the fibula and its distal muscle belly. Axial MRI images provide a reliable guide even when one of the peroneals is completely ruptured, subluxated out of the peroneal groove, or absent. Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. New York, NY, Lippincott, 1993, pp 234-235.
References:
- Sammarco GJ: Peroneus longus tendon tears: Acute and chronic. Foot Ankle Int 1995;16:245-253.
Question 84High Yield
In obstetrical brachial plexus palsy, which of the following signs is associated with the poorest prognosis for recovery in a 2-month-old infant?
Explanation
Explanation
Persistent Horner's sign (ptosis, myosis, and anhydrosis) is a sign of proximal injury, usually avulsion of the roots from the cord which disrupts the sympathetic chain. Root rupture or avulsion proximal to the myelin sheath has less chance of healing. Two-month-old infants with persistent weakness in the other areas described may still have a good prognosis for recovery. Concurrent clavicle fracture has been shown to have no prognostic value. Clarke HM, Curtis CG: An approach to obstetrical brachial plexus injuries. Hand Clin 1995;11:563-581.
References:
- Narakas AO: Injuries to the brachial plexus, in Bora FW (ed): The Pediatric Upper Extremity: Diagnosis and Management. Philadelphia, PA, WB Saunders, 1986, p 247.
Question 85High Yield
An adult patient has a closed humeral fracture that was treated nonsurgically and a concomitant radial nerve injury. Six weeks after injury, electromyography shows no evidence of recovery. Management should now consist of
Explanation
Explanation
In patients with radial nerve injuries with closed humeral fractures, it has been reported that 85% to 95% spontaneously recover. Based on this premise, most surgeons favor expectant management of these injuries. Even if there is no evidence of recovery at 6 weeks, repeat electromyography at 12 weeks is advocated. If there is no clinical or electromyographic signs of recovery at 6 months, exploration is recommended. If the nerve is in continuity at the time of exploration, nerve action potentials are useful in helping determine the need for neurolysis, excision, and grafting, or if excision and repair is the best option. Pollock FH, Drake D, Bovill EG, et al: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
References:
- Mohler LR, Hanel DP: Closed fractures complicated by peripheral nerve injury. J Am Acad Orthop Surg 2006;14:32-37.
Question 86High Yield
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in
Explanation
The patient has a distal biceps rupture. While the distal biceps contributes to elbow flexion, its main function is forearm supination. Baker BE, Bierwagen D: Rupture of the distal tendon of the biceps brachii: Operative versus non-operative treatment. J Bone Joint Surg Am 1985;67:414-417. D'Arco P, Sitler M, Kelly J, et al: Clinical, functional, and radiographic assessments of the conventional and modified Boyd-Anderson surgical procedures for repair of distal biceps tendon ruptures. Am J Sports Med 1998;26:254-261.
Question 87High Yield
Figure 17 shows the radiograph of an 11-year-old boy with Duchenne muscular dystrophy who has been nonambulatory for the past 2 years. Management of the spinal deformity should consist of
Explanation
Explanation
The presence of any curve greater than 20 degrees in a nonambulatory patient with Duchenne muscular dystrophy is an indication for posterior fusion with instrumentation. Because of progressive cardiomyopathy and pulmonary deficiency, waiting until the curve is larger can increase the risk of pulmonary or cardiac complications during or following surgery. There is some disagreement as to whether all such fusions must extend to the pelvis. Bracing or other nonsurgical management is ineffective and is not indicated in this situation. Sussman M: Duchenne muscular dystrophy. J Am Acad Orthop Surg 2002;10:138-151.
References:
- Mubarek SJ, Morin WD, Leach J: Spinal fusion in Duchenne muscular dystrophy: Fixation and fusion to the sacropelvis? J Pediatr Orthop 1993;13:752-757.
Question 88High Yield
A 9-year-old girl reports progressive right knee pain. Radiographs are shown in Figures 59a and 59b. Work-up reveals no other sites of disease. Low- and high-power photomicrographs are shown in Figures 59c and 59d. What is the most appropriate treatment?
Explanation
Explanation
59b 59c 59d This classic case of osteosarcoma illustrates the typical radiographic and histologic characteristics of this disease. The radiographs show an aggressive-appearing lesion of the distal femur. The lesion has both lytic and blastic areas. Periosteal reaction is present in the form of a Codman's triangle. The radiographs are highly suggestive of osteosarcoma. The photomicrographs show malignant spindle cells that produce osteoid, thus confirming the diagnosis of osteosarcoma. Treatment of osteosarcoma is multimodal including multi-agent chemotherapy and surgery (wide resection or amputation). Bacci G, Ferrari S, Bertoni F, et al: Long-term outcome for patients with nonmetastatic osteosarcoma of the extremity treated at the Instituto Ortopedico Rizzoli according to the Instituto Ortopedico Rizzoli/osteosarcoma-2 protocol: An updated report. J Clin Oncol 2000;18:4016-4037. Bielack SS, Kempf-Bielack B, Delling G, et al: Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol 2002;20:776-790.
References:
- Mankin HJ, Hornicek FJ, Rosenberg AE, et al: Survival data for 648 patients with osteosarcoma treated at one institution. Clin Orthop Relat Res 2004;429:286-291.
Question 89High Yield
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?

Explanation
The sagittal image reveals increased signal and decreased size of the supraspinatus and infraspinatus muscles, indicating muscle atrophy. The rotator cuff tendon signal is normal. The subscapularis and teres minor muscles are unaffected. Muscular dystrophy and thoracic outlet syndrome would be expected to have a more global effect. Although muscular atrophy can occur in the setting of a rotator cuff tear, the coronal image shows an intact supraspinatus. The suprascapular nerve supplies the supraspinatus and infraspinatus muscles. Therefore, suprascapular nerve entrapment would result in atrophy of these muscles with sparing of the surrounding musculature. Any lesion within the suprascapular notch, including neoplastic disease, a venous varix, or neuroma, can place pressure on the suprascapular nerve. Suprascapular nerve entrapment most commonly results from extension of a paralabral cyst or ganglion, often with associated labral pathology. Spinal accessory nerve disruption would show trapezius muscle atrophy. Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
Question 90High Yield
A 71-year-old woman who reports long-term use of oral steroids for asthma is referred for treatment of a distal humerus fracture. Radiographs reveal diffuse osteopenia and a severely comminuted intra-articular fracture. What is the most appropriate treatment?
Explanation
Explanation
Several studies have documented the satisfactory outcomes of total elbow arthroplasty when osteosynthesis is not feasible for fixation of a distal humerus fracture, particularly in the physiologically older patient with low functional demands. Total elbow arthroplasty should be considered when a comminuted intra-articular distal humerus fracture occurs in a woman older than age 65 years, particularly with such associated comorbidities as systemic steroid use, osteoporosis, or rheumatoid arthritis. Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement. J Bone Joint Surg Am 2004;86:940-947. Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intraarticular distal humerus fractures in women older than 65. J Orthop Trauma 2003;17:473-480.
Question 91High Yield
Examination of a 5-year-old boy with amyoplasia shows a flexion contracture of 70 degrees of the right knee. The active arc of motion is from 70 degrees to 90 degrees, and the opposite knee has a flexion contracture of 10 degrees. Both hips are dislocated with flexion contractures of 10 degrees, passive hip motion is from 10 degrees to 90 degrees of flexion, and the feet are plantigrade and easily braceable. Despite a daily stretching program, the parents and physical therapists note that it is increasingly difficult for him to walk because of the flexion contracture of the right knee. Management of the knee flexion contracture should now include
Explanation
Most children with amyoplasia are ambulatory and when a decrease in function occurs because of a severe contracture, it must be addressed. A radical posterior soft-tissue release, including the posterior knee capsule and often the collateral ligaments and the posterior cruciate ligament, is needed to obtain extension. After the age of 1 year, aggressive physical therapy will do little to correct a contracture. Botulinum toxin A is indicated for spasticity and is contraindicated with severe contractures. Supracondylar femoral extension osteotomy works well, but will remodel at an average rate of 1 degree per month, which is not considered ideal in a young patient. Gradual correction with a circular ring external fixator is an option, but a soft-tissue release will also most likely be needed for a contracture of this severity. Sarwark JF, MacEwen GD, Scott CI Jr: Amyoplasia (a common form of arthrogryposis). J Bone Joint Surg Am 1990;72:465-469. DelBello DA, Watts HG: Distal femoral extension osteotomy for knee flexion contracture in patients with arthrogryposis. J Pediatr Orthop 1996;16:122-126.
Question 92High Yield
A 20-year-old collegiate football player who sustained blunt head trauma during the first half of a game is emotional and confused. During the halftime intermission, his affect, memory, and disorientation are totally resolved and have returned to preinjury baseline. The only residual finding is a very mild headache. He wants to play the second half. What is the most appropriate course of action?
Explanation
Explanation
There is almost universal acceptance that an athlete may return to play after blunt head trauma only if he or she is totally asymptomatic. Mild residual symptoms are considered an absolute contraindication for return to play. Returning to play after a cardiovascular challenge or sport-specific activities is permitted on the pretext that the athlete is totally asymptomatic prior to these maneuvers. Neuropsychiatric testing is being used more frequently to monitor residual cognitive effects after head trauma. It has not been used as a return to play criterion. Garrick J (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 29-48.
References:
- Guskiewicz KM, McCrea, Marshall SW, et al: Cumulative effects associated with recurrent concussion in collegiate football players: The NCAA Concussion Study. JAMA 2003;290:2549-2555.
Question 93High Yield
A 65-year-old man with ankylosing spondylitis has neck pain after falling back over his lawnmower, striking his thoracic spine, and forcing his neck into extension. Examination reveals subtle weakness of the intrinsics and finger flexors at approximately 4+/5. Initial management consists of immobilization in a rigid collar, and placing his head in the anatomic position. Radiographs reveal a subtle extension fracture of the lower cervical spine. Approximately 6 hours after the injury, he reports increasing paresthesias in his upper and lower extremities, and examination now shows his intrinsics are 2/5, finger flexors are 3/5, and his triceps are now weak at 4/5 on manual motor testing. In addition, his lower extremities now show weakness in both dorsal and plantar flexion of the ankle in the range of 4/5. Repeat radiographs appear unchanged. An MRI scan is shown in Figure 2. Management should now consist of
Explanation
Explanation
It is not uncommon for patients with ankylosing spondylitis to sustain extension-type fractures, most typically of the cervicothoracic junction. These fractures can appear nondisplaced or minimally displaced initially, making them difficult to diagnose. Because there is no mobility between vertebrae, fractures tend to occur more like those of a transverse fracture of a long bone. In addition, the vertebral bodies are vascular and their canals are relatively enclosed, making them vulnerable to epidural bleeding. The MRI scan reveals an epidural hematoma located posteriorly on the cord; therefore, the treatment of choice is surgical evacuation and a posterior laminectomy. Because of the intrinsic instability of such fractures at the time of the laminectomy, internal fixation and stabilization with a posterior fusion is warranted. A simple laminectomy will only increase instability, and control is unlikely with halo vest immobilization. An anterior procedure will not effectively treat the problem given the location of the hematoma. Consideration can be given to methylprednisolone and observation; however, this will not eradicate the problem. Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142.
References:
- Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spine fracture and spinal stenosis in ankylosing spondylitis. J Neurosurg 1982;57:609-616.
Question 94High Yield
Figure 30 shows an axial T1-weighted MRI scan of a patient's right shoulder. The arrows are pointing to what normal structure?
Explanation
Explanation
Tears of the pectoralis major tendon are frequently missed during examination. MRI provides excellent visualization of the tendon if the study extends low enough down the arm. The pectoralis major tendon inserts on the crest of the greater tubercle of the humerus, just lateral to the long head of the biceps tendon. The latissimus dorsi tendon inserts medial to the long head of the biceps tendon on the lesser tubercle. The subscapularis tendon inserts on the lesser tuberosity more proximally. The deltoid insertion is more distal. Connell DA, Potter HG, Sherman MF, et al: Injuries of the pectoralis major muscle: Evaluation with MR imaging. Radiology 1999;210:785-791. Carrino JA, Chandnanni VP, Mitchell DB, et al: Pectoralis major muscle and tendon tears: Diagnosis and grading using magnetic resonance imaging. Skeletal Radiol 2000;29:305-313.
References:
- Ohashi K, El-Khoury GY, Albright JP, et al: MRI of complete rupture of the pectoralis major muscle. Skeletal Radiol 1996;25:625-628.
Question 95High Yield
What is the known manner in which the growth hormone-insulin-like growth factor-I (GH-IGF-I) system functions to stimulate bone growth?
Explanation
Explanation
IGF-I, formerly known as somatomedin-C, possibly acts by both paracrine and endocrine hormone pathways. The products of the GH-IGF-I system induce proliferation without maturation of the growth plate and thus induce linear skeletal growth. The action of the thyroid hormone axis is via an active metabolite that enters target cells and signals a nuclear receptor to stimulate both proliferation and maturation of the growth plate. Increased amounts of the active steroid hormone metabolite promote proliferation and maturation of the growth plate. Calcitonin inhibits bone resorption. Binder G, Grauer ML, Wehner AV, et al: Outcome in tall stature: Final height and psychological aspects in 220 patients with and without treatment. Eur J Pediatr 1997;156:905-910. Wang J, Zhou J, Cheng CM, et al: Evidence supporting dual, IGF-I-independent and IGF-I-dependent, roles for GH in promoting longitudinal bone growth. Endocrinol 2004;180:247-255.
References:
- Gertner JM: Childhood and adolescence, in Favus MJ (ed): Primer on Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 45-47.
Question 96High Yield
What is the primary role of superficial zone protein (SZP) in articular cartilage?
Explanation
Lubricin and SZP share a similar primary structure but may differ in posttranslational modifications with O-linked oligosaccharides. The primary physiologic function of SZP appears to be boundary lubrication. SZP does not influence interleukin-1, collagenase, or TIMP directly because these proteins are associated with articular cartilage turnover. Hlavacek M: The influence of the acetabular labrum seal, intact articular superficial zone and synovial fluid thixotropy on squeeze-film lubrication of a spherical synovial joint. J Biomech 2002;35:1325-1335.
Question 97High Yield
Steroids are thought to prevent neurologic deterioration after traumatic spinal cord injury by which of the following mechanisms?
Explanation
Explanation
The proposed mechanisms by which steroids such as methylprednisolone are thought to prevent neurologic deterioration by limiting secondary insult, include: decreasing the area of ischemia in the cord, reducing TNF-alpha expression and NF-kB binding activity, decreasing free radical oxidation and thus stabilizing cell and lysosomal membranes, and checking the influx of calcium into the injured cells, thus reducing cord edema. Slucky AV: Pathomechanics of spinal cord injury. Spine: State Art Rev 1999;13:409-417.
Question 98High Yield
A 16-year-old girl has had anterior leg pain and a mass for the past 8 months. Figures 2a and 2b show a radiograph and an H & E histologic specimen. Which of the following disorders is believed to be a precursor of this lesion?

Explanation
The radiograph and pathology are consistent with adamantinoma. While the mechanism underlying adamantinoma has not been identified, it is believed to be closely related to osteofibrous dysplasia, which may represent a precursor. The other diagnoses are not known to give rise to adamantinoma.
Question 99High Yield
A 75-year-old woman notes a slowly enlarging mass in the right anterior thigh. Her medical history is significant only for hypertension. An MRI scan of her thigh is shown in Figures 60a through 60d. Which of the following surgical margins is the most appropriate for removal of this lesion?
Explanation
Explanation
60b 60c 60d The patient has a large deep anterior thigh mass that has imaging characteristics of mature fat. Intramuscular lipomas are effectively treated with marginal resections with very low recurrence rates. Large lipomas often have small amounts of intralesional signal changes frequently representing trapped muscle fibers and do not necessitate more extensive margins. Gaskin CM, Helms CA: Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): Results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol 2004;182:733-739.
References:
- Rozental TD, Khoury LD, Donthineni-Rao R, et al: Atypical lipomatous masses of the extremities: Outcome of surgical treatment. Clin Orthop Relat Res 2002;398:203-211.
Question 100High Yield
In the arthroscopic photograph shown in Figure 5, the structure labeled "A" functions primarily as a restraint to translation of the humeral head in what direction?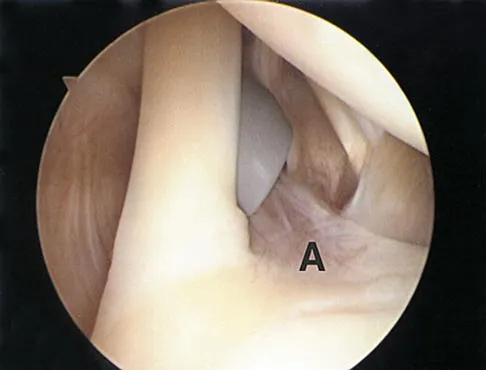
Explanation
The superior glenohumeral ligament identified as "A" in the figure functions primarily as a restraint to inferior glenohumeral translation of the adducted arm. The middle glenohumeral ligament is highly variable and pooly defined in up to 40% of the population and functions to restrain anterior translation of the externally rotated arm in the midrange of abduction. The anterior band of the inferior glenohumeral ligament is the primary restraint to anterior/inferior translation of the head with the shoulder abducted to 90 degrees and in maximum external rotation. Ticker JB, Bigliani LU, Soslowskiy LJ, et al: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon