High-Yield Orthopedic MCQs: Mock Exam 549 for ABOS, OITE, FRCS Prep
14 Apr 2026
104 min read
85 Views
Key Takeaway
Prepare for ABOS, OITE, and FRCS with 100 high-yield orthopedic surgery MCQs. This comprehensive practice set (Mock Exam #549) helps surgeons master crucial concepts, ensuring robust preparation for their board certification and in-training exams. Start your review now!
Demystifying the Posterolateral Approach to t...
00:00
Start Quiz
Question 1High Yield
A 38-year-old man underwent a transtibial amputation for chronic posttraumatic foot and ankle pain and chronic calcaneal osteomyelitis. Postoperative radiographs are seen in Figures 41a and 41b. What is the proposed purpose of the surgical modification seen in the radiographs?

Explanation
The Ertl modification of a below-knee amputation has been proposed to create a more stable "platform" to aid in transferring the load of weight bearing between the residual limb and the prosthetic socket. It is felt that a stable platform allows total contact loading over an enlarged stable surface area. Early studies have suggested that this modification may enhance the patient's perceived functional outcome. Pinzur MS, Pinto MA, Saltzman M, et al: Health-related quality of life in patients with transtibial amputation and reconstruction with bone bridging of the distal tibia and fibula. Foot Ankle Int 2006;27:907-912.
Question 2High Yield
A 35-year-old man is seen for evaluation of his left ankle following multiple previous ankle sprains and frequent episodes of the ankle giving way. Examination reveals marked laxity about the lateral ankle with associated tenderness along the peroneal tendons. Physical therapy, anti-inflammatory drugs, and supportive bracing have failed to provide relief. An MRI scan shows peroneal tenosynovitis and a possible tear. He elects to undergo a peroneal tendon repair and lateral ligament reconstruction. Which of the following best describes the structure labeled "A" in Figure 45?
Explanation
The structure labeled "A" is a peroneus quartus, a supernumary muscle arising most commonly from the peroneus brevis. The presence of peroneus quartus is not uncommon, with an incidence of up to 21%, and is associated with lateral ankle pain and peroneal tendon symptoms, theoretically as a result of mass effect within the peroneal tendon sheath. Zammit J, Singh D: The peroneus quartus muscle: Anatomy and clinical relevance. J Bone Joint Surg Br 2003;85:1134-1137.
Question 3High Yield
A 16-year-old boy with spastic quadriplegic cerebral palsy has been referred for evaluation and management of scoliosis. His parents report increasing problems with sitting balance, positioning, and hygiene because of the deformity. The radiograph shown in Figure 46 reveals a lordoscoliosis of 105 degrees with marked pelvic obliquity. Attempts at correcting the pelvic obliquity on supine bending radiographs show significant rigidity. Management should consist of
Explanation
Explanation
Spinal stabilization is the treatment of choice in patients with severe scoliosis who have progressive positioning, sitting balance, and/or hygiene problems despite maximal nonsurgical management. Pelvic rigidity and marked frontal plane deformity necessitate anterior and posterior procedures so as to maximize correction and fusion. Weinstein SL (ed): The Pediatric Spine: Principles and Practice. New York, NY, Raven Press, 1994, pp 977-997.
References:
- Frymoyer JW (ed): Orthopaedic Knowledge Update 4. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1993, pp 447-459.
Question 4High Yield
Figure 22 shows the radiograph of a 7-year-old boy who underwent retrograde elastic nailing of a femoral shaft fracture. What is the most common problem following this procedure?
Explanation
Explanation
Several large clinical studies have shown that the most common problem after elastic nailing of a femoral shaft fracture is persistent pain and irritation at the nail insertion site. Unacceptable shortening and malunion are very rare in a 7-year-old patient. Rotational malalignment also is unusual. Osteonecrosis has been reported in solid antegrade nailing but not with elastic nailing of femoral shaft fractures in skeletally immature patients. Flynn JM, Luedtke LM, Ganley TJ, et al: Comparison of titanium elastic nails with traction and a spica cast to treat femoral fractures in children. J Bone Joint Surg Am 2004;86:770-777. Flynn JM, Hresko T, Reynolds RA, et al: Titanium elastic nails for pediatric femur fractures: A multicenter study of early results with analysis of complications. J Pediatr Orthop 2001;21:4-8.
References:
- Ligier JN, Metaizeau JP, Prevot J, et al: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77.
Question 5High Yield
A patient who underwent an L5-S1 diskectomy 18 months ago has persistent pain in the left leg. Figures 9a and 9b show postoperative axial T1-weighted MRI scans at the L5-S1 level without and with gadolinium. What is the most likely diagnosis?
Explanation
Explanation
9b Persistent or recurrent symptoms after lumbar diskectomy are troublesome and can be difficult to assess. Gadolinium-enhanced MRI scans may be helpful. The images show enhancement about the left S1 root, a finding that is most consistent with perineural (epidural) fibrosis. The root itself does not enhance. Root enhancement has been associated with compressive radicular symptoms. A disk herniation does not enhance with gadolinium. A neurilemmoma enhances with gadolinium, but the involved root would be enlarged. There is no evidence of a fluid collection which would be consistent with an epidural abscess. Babar S, Saifuddin A: MRI of the post-discectomy lumbar spine. Clin Radiol 2002;57:969-981. Kikkawa I, Sugimoto H, Saita K, et al: The role of Gd-enhanced three-dimensional MRI fast low-angle shot (FLASH) in the evaluation of symptomatic lumbosacral nerve roots. J Orthop Sci 2001;6:101-109.
References:
- Vroomen PC, Van Hapert SJ, Van Acker RE, et al: The clinical significance of gadolinium enhancement of lumbar disc herniations and nerve roots on preoperative MRI. Neuroradiology 1998;40:800-806.
Question 6High Yield
A 13-year-old girl was riding on an all-terrain vehicle when the driver struck a tree. She sustained the injury shown in Figures 45a through 45d. This injury is best described as what type of acetabular fracture pattern?
Explanation
Explanation
45b 45c 45d The fracture is a both-column fracture in the Judet/Letournel classification and a C3 in the AO classification. There is extension into the sacroiliac joint along the pelvic brim and comminution along the posterior column above the sciatic notch. Both the anterior and posterior columns are separately broken and displaced. However, the defining feature of a both-column pattern, as seen in this patient, is that all articular fragments are on fracture fragments and no joint surface is left intact to the axial skeleton above. The use of three-dimensional images makes it easier to view the location of the fracture fragments and the amount and direction of displacement. Helfet DL, Beck M, Gautier E, et al: Surgical techniques for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 533-603. Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
References:
- Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 7High Yield
The cervical disk herniation shown in the MRI scans in Figures 30a and 30b will most likely create which of the following constellations of symptoms?
Explanation
Explanation
30b The MRI scans reveal a right-sided C5-6 herniated nucleus pulposus. A disk herniation in this region encroaches on the C6 root and is accompanied by a sensory change along the thumb and index finger, alterations in the brachioradialis reflex, and possible wrist extension weakness. Although the nerve root associated with the vertebral body passes above the pedicles such that the C6 root passes above the C6 pedicle, it is still the C6 root that is encroached on because the herniation affects the exiting root rather than the traversing root as seen in the lumbar spine. Klein JD, Garfin SR: Clinical evaluation of patients with suspected spine problems, in Frymoyer JW (ed): Adult Spine: Principles and Practice, ed 2. Philadephia, PA, Lippincott-Raven, 1997, pp 319-330.
References:
- Hoppenfeld S: Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-49.
Question 8High Yield
On MRI, a nonsanguinous effusion has what appearance?
Explanation
Nonbloody effusions that are greater than 1 mL are readily detected by MRI. They appear black on T1-weighted images and white on T2-weighted images. A sanguinous effusion is seen as white on T1-weighted images and black on T2-weighted images. Resnick D, Kang HS: Synovial joints, in Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 49-53.
Question 9High Yield
Figures 51a through 51c show the radiographs of a 7-year-old soccer player who reports a gradual onset of midfoot pain that began shortly after the start of soccer season. He states that the pain is worse with activity and is partially alleviated by rest. Examination reveals soft-tissue swelling, and tenderness and warmth in the region of the talonavicular and navicular cunieform joints. Management should consist of
Explanation
Explanation
51b 51c Osteochondrosis of the tarsal navicular (Kohler disease) is an infrequent cause of midfoot pain in children, and the etiology is unknown. The typical radiographic findings include flattening and irregular ossification of the tarsal navicular. The medial cunieform and talus maintain their normal articular contours. The acute process is best treated with rest and immobilization. A short leg walking cast results in relief of pain and a quicker return to activity compared with orthotics, although long-term success is similar with either method of treatment. Children may return to activities when the symptoms subside. The radiographic appearance of the talus begins to normalize by about 8 to 10 months following the onset of symptoms.
References:
- Lutter LD: Sports-related injuries, in Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992.
Question 10High Yield
The posterior circumflex artery provides blood supply to what portion of the proximal humerus?
Explanation
Explanation
The posterior circumflex artery provides blood supply only to the posterior portion of the greater tuberosity and a small posteroinferior portion of the humeral head. The humeral head is supplied primarily by the anterolateral ascending branch of the anterior circumflex artery; the terminal branch of this artery is termed the arcuate artery. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 267-274.
References:
- Gerber C, Schneeberger AG, Vinh TS: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
Question 11High Yield
A 23-year-old woman sustains an injury to her right hand after falling off her snowboard. Examination reveals that she has difficulty moving her fingers. A radiograph and a clinical photograph are shown in Figures 8a and Figure 8b. Management should consist of

Explanation
The radiograph reveals oblique fractures of the third and fourth metacarpals. The rotational component of the fracture displacement is well visualized on the clinical photograph, which shows scissoring of the middle finger over the ring finger. The fracture obliquity results in rotational deformity that cannot be adequately maintained and held by closed treatment. The treatment of choice is open reduction and internal fixation. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771. Freeland AE, Benoist LA, Melancon KP: Parallel miniature screw fixation of spiral and long oblique hand phalangeal fractures. Orthopedics 1994;17:199-200.
Question 12High Yield
A 25-year-old man injures his shoulder while skiing. Examination reveals increased passive external rotation, pain in the cocked position, and a positive lift-off test. What is the most likely diagnosis?
Explanation
Explanation
A positive lift-off test and increased passive external rotation are diagnostic of a subscapularis tear or detachment. Although a similar injury could produce anterior instability, this will test the integrity of the subscapularis. A locked dislocation has limited passive movement. A ruptured biceps tendon will most likely produce ecchymosis and findings similar to supraspinatus trauma. Internal impingement is not associated with subscapularis weakness. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
References:
- Hawkins RJ, Bokor DJ: Clinical evaluation of the shoulder, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 149-177.
Question 13High Yield
A 21-year-old male construction worker fell from a roof and sustained an injury to his left foot. Radiographs and CT scans are shown in Figures 24a through 24e. Compared to nonsurgical management, surgical treatment offers which of the following advantages?
Explanation
Explanation
24b 24c 24d 24e The radiographs and CT scans show a displaced intra-articular calcaneal fracture, with loss of calcaneal height and length. Recent multicenter, randomized, prospective studies suggest that surgical treatment of displaced intra-articular calcaneal fractures is associated with an almost six-fold decrease in the risk of posttraumatic subtalar arthritis (necessitating subtalar arthrodesis) compared to nonsurgical treatment. Despite ongoing controversy, surgical treatment has not been shown to be advantageous with respect to activity, time to return to work, or subtalar joint range of motion. A nonunion of a calcaneal fracture is exceedingly rare regardless of the treatment method. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
References:
- Csizy M, Buckley R, Tough S, et al: Displaced intra-articular calcaneal fractures: Variables predicting late subtalar fusion. J Orthop Trauma 2003;17:106-112.
Question 14High Yield
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?
Explanation
A concern in the multiply injured patient who has a pulmonary contusion is the potential for further pulmonary compromise because of embolization of marrow, blood clot, or fat during manipulation of the medullary canal. Recent evidence has shown that the presence of a lung injury is the most important determining factor in future deterioration. However, despite the lung injury and its potential consequences, this patient's femur fracture needs stabilization. Because damage control in the multiply injured patient requires a technique that can be performed rapidly and consistently, the treatment of choice is application of an external fixator. By placing two pins above and below the fracture and with longitudinal traction, the fracture is quickly realigned and stabilized. This allows the patient to be resuscitated and treated at a later date when definitive management of the fracture can be carried out. There is little difference between plate fixation and intramedullary nailing. Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809. Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Question 15High Yield
After excising a mass from the thigh that was thought to be a lipoma, the pathology reveals that the mass is a high-grade sarcoma. Subsequent treatment should include
Explanation
Following excision of a suspected benign soft-tissue tumor that proves to be malignant, repeat excision of the tumor bed is recommended. The initial surgical margins are inadequate after an intralesional or marginal excision, necessitating additional surgery for more definitive local control. While radiation therapy and/or chemotherapy may help to reduce the risk of local recurrence in patients with microscopic residual disease, local control is improved following repeat excision. Radiation therapy alone is inadequate to address poor surgical margins, and would likely be given postoperatively. Bisphosphonates have no current role in the treatment of soft-tissue sarcoma. Noria S, Davis A, Kandel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 16High Yield
A 40-year-old woman with no history of back problems has a symptomatic L4-5 disk herniation with an L5 radiculopathy that has failed to respond to 12 weeks of nonsurgical management. In the preoperative discussion, the surgeon advises the patient that the chance of recurrence of the herniation after successful diskectomy is what percent?
Explanation
The incidence of recurrent disk herniation after a successful diskectomy is approximately 5% to 10%. Indications for surgical diskectomy for a recurrence are the same as for a primary diskectomy. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 685-698.
Question 17High Yield
Which of the following types of displaced posterior pelvic disruptions must undergo anatomic reduction and internal fixation to ensure the best clinical outcome?
Explanation
Although all of the above displaced injuries require reduction, the sacroiliac joint dislocation is a ligamentous injury. Without fixation, healing is unlikely and the result will be a painful dislocation. Both Holdsworth and Tile showed that the sacroiliac joint must be reduced anatomically and stabilized. The injuries through bone will unite fairly rapidly and, if reduced and stabilized with traction or external fixation, will generally result in an acceptable outcome unless modified by other associated problems such as neurologic injury. Tile M: Fractures of the Pelvis and the Acetabulum. Baltimore, MD, Williams and Wilkins, 1995. Holdsworth F W: Dislocation and fracture dislocation of the pelvis. J Bone Joint Surg Br 1948;30:461-465.
Question 18High Yield
Which of the following patients is considered the most appropriate candidate for selective dorsal rhizotomy?
Explanation
Explanation
While other surgical and nonsurgical options exist for management of spasticity, the criteria originally laid out by Peacock and associates describe the most appropriate candidate for rhizotomy as a patient with spastic diplegia who is between the ages of 4 to 8 years and has a stable gait pattern that is limited by lower extremity spasticity. Rhizotomy is not recommended in patients with athetosis because of unpredictable results. In addition, rhizotomy should be avoided in nonambulatory patients with spastic quadriplegia because it is associated with significant spinal deformities. Peacock WJ, Arens LJ, Berman B: Cerebral palsy spasticity: Selective posterior rhizotomy. Pediatr Neurosci 1987;13:61-66. Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29.
References:
- Mooney JF III, Millis MB: Spinal deformity after selective dorsal rhizotomy in patients with cerebral palsy. Clin Orthop 1999;364:48-52.
Question 19High Yield
What does Dual Energy X-ray Absorptiometry (DEXA) testing, as a technique, measure?
Explanation
Explanation
DEXA can provide data on bone mineral content and soft-tissue composition, and requires cross-sectional dimension for accuracy. DEXA provides a quantitative, not qualitative, measurement of bone mineral content and is incapable of differentiating between trabecular and cortical bone. Osteoarthritis falsely elevates the values, especially in the AP spinal analysis. Genant HK, Faulkner KG, Gluer CC: Measurement of bone mineral density: Current status. Am J Med 1991;91:49S-53S. Genant HK, Engelke K, Fuerst T, et al: Review: Noninvasive assessment of bone mineral density and stature: State of the art. J Bone Miner Res 1996;11:707-730.
References:
- Engelke K, Gluer CC, Genant HK: Factors influencing short-term precision of dual X-ray bone absorptiometry (DXA) of spine and femur. Calcif Tissue Int 1995;56:19-25.
Question 20High Yield
A patient undergoes excision of a 3- x 3-cm soft-tissue sarcoma. The final histology results show tumor at the surgical margin. The surgical procedure performed is classified as
Explanation
Explanation
Surgical margins are classified according to the plane of dissection in relation to the tumor. An intralesional procedure is where the plane of dissection passes through the tumor. A marginal resection involves a resection where the plane of dissection is through the reactive zone of the tumor. A wide resection is through completely normal tissue outside of the reactive zone. A radical resection removes all of the muscles and/or bone of the compartment that are involved by the tumor.
References:
- Enneking WF, Spanier SS, Goodman MA: A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop 1980;153:106-120.
Question 21High Yield
What is the most common organism found following a nail puncture wound through tennis shoes in a host without immunocompromise?
Explanation
The association of a nail puncture wound with a gram-negative infection (Pseudomonas aeruginosa) has been attributed to the local environmental factors in shoes. Osteomyelitis is rare, occurring only in about 1% of patients. Tetanus prophylaxis should be given if it is not up to date. While the remaining organisms listed are periodically involved, they are more common in patients who are immunocompromised or who have diabetes mellitus. Therefore, obtaining a culture of the infected wound is appropriate in such individuals because of the multifactorial nature of the infection. Green NE, Bruno J III: Pseudomonas infections of the foot after puncture wounds. South Med J 1980;73:146-149.
Question 22High Yield
Which of the following extensor tendons commonly have multiple slips?
Explanation
Explanation
The extensor digiti mini quinti is most typically a tendon with two slips. The abductor pollicis longus has multiple slips that insert in order of frequency on the base of the first metacarpal, trapezium, and thenar muscles. The extensor pollicis longus, extensor carpi radialis brevis, and extensor indicis proprius consistantly have only one slip. von Schroeder HP, Botte MJ: Anatomy of the extensor tendons of the fingers: Variations and multiplicity. J Hand Surg Am 1995;20:27-34.
References:
- Bouchlis G, Bhatia A, Asfazadourian H, et al: Distal insertions of abductor pollicis longus muscle and arthritis of the first carpometacarpal joint in 104 dissections. Ann Chir Main Memb Super 1997;16:326-338.
Question 23High Yield
A 60-year-old woman with a history of breast cancer has progressive paraparesis. The MRI scan is shown in Figure 28. What form of management is most likely to restore or maintain ambulation?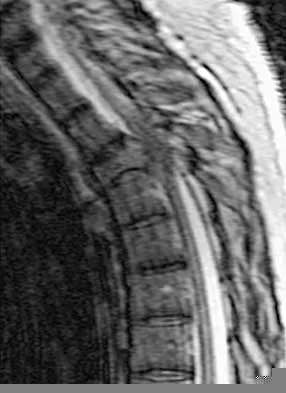
Explanation
Surgical decompression and stabilization have been shown to be the most effective means of improving neurologic function. Decompression is most reliably done from the side of the compression, which is anterior in this patient. Harrington KD: Metastatic tumors of the spine: Diagnosis and treatment. J Am Acad Orthop Surg 1993;1:76-86.
Question 24High Yield
Which of the following is considered an advantage of metal femoral heads compared with ceramic heads?
Explanation
Ceramic-on-ceramic bearing surfaces have superior tribological properties and show lower linear wear than metal-on-metal implants. However, because of their lower strength and vulnerability to fracture, design considerations constrain the neck-length options available to ensure optimal taper fit.
Question 25High Yield
Figure 4 shows the AP radiograph of a 28-year-old woman who has had moderate pain in the left hip for the past year. Nonsurgical management has failed to provide relief. She denies any history of hip pain, pathology, or trauma. Management should consist of
Explanation
The radiograph shows developmental dysplasia of the hip with the hip reduced and congruent. The treatment of choice is a periacetabular osteotomy because it can improve hip biomechanics and prolong the function of the hip joint. This procedure should be performed prior to the development of severe degenerative changes. Observation will not alter the patient's natural history or the biomechanics of the hip. A total hip arthroplasty should be delayed until severe degenerative changes are present. A Chiari osteotomy is a salvage osteotomy used for a noncongruent subluxated hip. A Pemberton osteotomy requires an open triradiate cartilage; therefore, it is not an option in an adult. Trousdale RT, Ekkernkamp A, Ganz R, Wallrichs SL: Periacetabular and intertrochanteric osteotomy for the treatment of osteoarthrosis in dysplastic hips. J Bone Joint Surg Am 1995;77:73-85.
Question 26High Yield
A 45-year-old man has persistent hindfoot pain that is aggravated by weight-bearing activities. History reveals that he sustained a calcaneus fracture 2 years ago, and he underwent a subtalar fusion 1 year ago. Examination reveals tenderness in the sinus tarsi and across the transverse tarsal joint. A plain radiograph and a CT scan are shown in Figures 24a and 24b. A technetium Tc 99m bone scan reveals uptake at the subtalar joint and at the transverse tarsal joints. Management should now consist of
Explanation
Explanation
24b The patient has a nonunion at the subtalar joint because of poor preparation of the arthrodesis site with incomplete removal of the articular cartilage. Clinically, he has arthritis at the transverse tarsal joint. Casting with a bone stimulator is not expected to result in a union of the subtalar arthrodesis. To address both the subtalar nonunion and the transverse tarsal joint arthritis, revision of the subtalar arthrodesis and conversion to a triple arthrodesis is the preferred option. Graves SC, Mann RA, Graves KO: Triple arthrodesis in older adults: Results after long-term follow-up. J Bone Joint Surg Am 1993;75:355-362. Haddad SL, Myerson MS, Pell RF IV, Schon LC: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499. Sangeorzan BJ, Smith D, Veith R, Hansen ST Jr: Triple arthrodesis using internal fixation in treatment of adult foot disorders. Clin Orthop 1993;294:299-307. Sangeorzan BJ: Salvage procedures for calcaneus fractures. Instr Course Lect 1997;46:339-346.
References:
- Wapner KL: Triple arthrodesis in adults. J Am Acad Orthop Surg 1998;6:188-196.
Question 27High Yield
When conducted at near physiologic strain rates, tensile studies of the inferior glenohumeral ligament (IGHL) have shown that the
Explanation
Explanation
Tensile testing of the inferior glenohumeral ligament at near physiologic strain rates has shown that the anterior band of the IGHL has the greatest stiffness of the three ligament regions and the glenoid insertion site shows greater strain than the ligament midsubstance. Bigliani LU, Pollock RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
References:
- Ticker JB, Bigliani LU, Soslowsky LJ, Pawluk RJ, Flatow EL, Mow VC: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
Question 28High Yield
A 6-year-old boy presents with a mass and a lucent lesion involving the tibial shaft as seen in Figure 17a. The mass is mildly tender to palpation. The bone scan is focally hot in the tibia. Biopsy specimens are shown in Figures 17b and 17c. What is the most likely diagnosis?
Explanation
Explanation
17b 17c Osteofibrous dysplasia frequently presents at a very young age, usually less than 10 years. In most patients, it involves the anterior cortex of the tibial shaft and minor anterior bowing of the tibia is frequently seen. The lesion is unpredictable in nature, but local recurrence is very high in patients who undergo surgery before 15 years of age. Campanacci M, Laus M: Osteofibrous dysplasia of the tibia and fibula. J Bone Joint Surg Am 1981;63:367-375.
References:
- McCaffery M, Letts M, Carpenter B, et al: Osteofibrous dysplasia: A review of the literature and presentation of an additional 3 cases. Am J Orthop 2003;32:479-486.
Question 29High Yield
A 1-year-old infant has the hand deformities shown in Figure 40. What pathologic process is the most likely cause of these deformities?
Explanation
Streeter's dysplasia is clearly related to rupture of the amnion in utero and is now most commonly referred to as premature amnion rupture sequence. The deformities arise from amniotic bands that wrap about protruding parts and from uterine packing because of the accompanying oligohydramnios. Clubfoot can develop as a result of the latter mechanism. Three limb involvement is most commonly seen, along with syndactyly. Treatment involves resection of bands and Z-plasty of skin. The disease is not genetic and has not been related to teratogen exposure or to iatrogenic influences such as amniocentesis. Developmental field disruption is not seen in this disease, and the growth potential of the involved parts is normal unless neurovascular disruption has arisen from band formation.
Question 30High Yield
A 30-year-old woman has had pain in her right leg for the past 6 months. A lytic lesion is noted in the anterior cortex of the midtibia, extending 5 cm in length without a soft-tissue mass. A radiograph and a biopsy specimen are shown in Figures 35a and 35b. What is the preferred treatment?
Explanation
Explanation
35b In an adult with an anterior cortical tibial lesion, this is the classic histologic appearance and anatomic location for an adamantinoma. The histology reveals areas of epithelial cells (in a glandular pattern) within a fibrous stroma. The epithelial cells are shown in nests. They would stain positively for keratin. Adamantinoma is a rare malignant bone tumor with a propensity for late metastasis. It has a high incidence of local recurrence unless resected with a wide margin. Chemotherapy and radiation therapy are not helpful in the treatment of this disease. Amputation generally is not necessary because a diaphyseal resection is usually possible. McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 263.
References:
- Moon NF, Mori H: Adamantinoma of the appendicular skeleton: Updated. Clin Orthop Relat Res 1986;204:215-237.
Question 31High Yield
A 13-year-old boy hyperextends his knee while playing basketball and reports a pop that is followed by a rapid effusion. A lateral radiograph is shown in Figure 4. Initial management consists of attempted reduction with extension, with no change in position of the fragment. What is the next most appropriate step in management?
Explanation
Explanation
Avulsion fractures of the tibial spine are rare injuries that result from rapid deceleration or hyperextension of the knee in skeletally immature individuals. This injury is the equivalent of ruptures of the anterior cruciate ligament in adults. These fractures are classified as types 1 through 3. Type 1 is a minimally displaced fracture, type 2 fractures have an intact posterior hinge, and type 3 fractures have complete separation. The radiograph demonstrates a completely displaced, or type III, tibial spine avulsion. Surgical reduction is indicated in type 2 fractures that fail to reduce with knee extension and in all type 3 fractures. Reduction may be arthroscopic or open, with fixation of the bony fragment using a method that maintains physeal integrity and prevents later growth arrest. Preferred techniques would be with suture or an intra-epiphyseal screw Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60. Mulhall KJ, Dowdall J, Grannell M, et al: Tibial spine fractures: An analysis of outcome in surgically treated type III injuries. Injury 1999;30:289-292. Owens BD, Crane GK, Plante T, et al: Treatment of type III tibial intercondylar eminence fractures in skeletally immature athletes. Am J Orthop 2003;32:103-105.
References:
- Vocke AK, Vocke AR: Cartilaginous avulsion fracture of the tibial spine. Orthopedics 2002;25:1293-1294.
Question 32High Yield
Bisphosphonates are indicated in the treatment of osteoporosis in patients who have a DEXA T-score of
Explanation
Explanation
Bisphosphonates are indicated in the treatment of osteoporosis. They have been shown to reduce the incidence of vertebral and extremity fractures in patients with a T-score of less than -1.
Question 33High Yield
A 32-year-old woman sustained an injury to her left upper extremity in a motor vehicle accident. Examination reveals a 2-cm wound in the mid portion of the dorsal surface of the upper arm and deformities at the elbow and forearm; there are no other injuries. Her vital signs are stable, and she has a base deficit of minus 1 and a lactate level of less than 2. Radiographs are shown in Figures 9a and 9b. In addition to urgent debridement of the humeral shaft fracture, management should include

Explanation
With a severe injury to the upper extremity, the best opportunity for achieving a good functional result for a floating elbow is immediate debridement of the open fracture, followed by internal fixation of the fractures. The ability to do this depends on the patient's physiologic status. In this patient, the procedure is acceptable because she has normal vital signs and no chest or abdominal injuries, and normal physiologic parameters (base excess and lactate) show adequate peripheral perfusion. The surgical approaches will be determined by the associated injury patterns and open wounds. In this patient, the humerus was debrided and stabilized through a posterior approach as was the medial condyle fracture. The ulna was fixed through an extension of the posterior incision and the radius through a separate dorsal approach. Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Question 34High Yield
In children between the ages of 4 and 8 years, the major blood supply to the femoral head comes from the
Explanation
Explanation
From birth until the age of 4 years, the primary blood supply to the femoral head is from the medial and lateral circumflex arteries that traverse the femoral neck. After the age of 4 years, the contribution of the lateral femoral circumflex artery, which traverses the anterior portion of the femoral neck, becomes negligible. The posterosuperior and posteroinferior retinacular vessels, branches of the medial femoral circumflex artery, become the primary blood supply to the epiphysis. The contribution of the artery of the ligamentum teres is minimal after the age of 4 years. Hughes LO, Beaty JH: Fractures of the head and neck of the femur in children. J Bone Joint Surg Am 1994;76:283-292.
References:
- Ogden JA: Changing patterns of proximal femoral vascularity. J Bone Joint Surg Am 1974;56:941-950.
Question 35High Yield
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured?
Explanation
The athlete has symptoms referable to the axillary, musculocutaneous, and suprascapular nerves resulting from an injury to the upper trunk of the brachial plexus. This portion of the plexus is formed by contributions of the fourth through sixth cervical nerve roots. This area is often contused or stretched following a tackling maneuver that results in either depression of the shoulder from contact at Erb's point or traction of the upper plexus from forced stretching of the neck to the contralateral side. Schenck CD: Anatomy of the innervation of the upper extremity, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face, ed 2. St Louis, MO, Mosby-Year Book, 1991.
Question 36High Yield
Following an episode of transient quadriplegia in contact sports, an athlete's return to play is absolutely contraindicated when
Explanation
Return to play decisions after traumatic spinal or spinal cord injury are not always clear-cut and often must be made on a patient-by-patient basis. The Torg ratio has been found to have low sensitivity in patients with large vertebral bodies. Abnormal electromyographic studies can persist in the face of normal function and do not define spinal injury. Duration of quadriplegia is not related to anatomic pathology. Findings on MRI scans or contrast-enhanced CT scans consistent with stenosis include lack of a significant cerebrospinal fluid signal around the cord, bony or ligament hypertrophy, or disk encroachment. Based on these findings, return to play should be avoided. Cantu RC, Bailes JE, Wilberger JE Jr: Guidelines for return to contact or collision sport after a cervical spine injury. Clin Sports Med 1998;17:137-146. Herzog RJ, Wiens JJ, Dillingham MF, Sontag MJ: Normal cervical spine morphometry and cervical stenosis in asymptomatic professional football players: Plain film radiography, multiplanar computer tomography, and magnetic resonance imaging. Spine 1991;16:178-186.
Question 37High Yield
A 16-year-old boy has had a painful ingrown nail on his great toe for the past 3 months. When initial management consisting of soaking the foot in Epsom salts and trimming the nail failed to provide relief, his family physician recommended 2 weeks of oral antibiotics. His symptoms persist, and he is now seeking a second opinion. A clinical photograph is shown in Figure 18. Management should now consist of
Explanation
Explanation
The patient has a chronic ingrown nail on his great toe, which is not an uncommon occurrence in teenagers because of improper nail care. There is local infection and a foreign body reaction because of the nail. Continued conservative management with soaks and antibiotics will not improve the clinical situation. In the presence of local chronic infection, nail matrix ablation is contraindicated. Additionally, in the absence of a history of an ingrown nail, a nail matrix ablation is not medically indicated. The appropriate treatment is partial removal of the nail plate. With nail plate removal, the inflammation and local infection will resolve rapidly. Pettine KA, Cofield RH, Johnson KA, Bussey RM: Ingrown toenail: Results of surgical treatment. Foot Ankle 1988;9:130-134.
References:
- Coughlin MJ, Mann RA: Toenail abnormalities, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 2, pp 1033-1070.
Question 38High Yield
A 55-year-old woman with a 15-year history of systemic lupus erythematosus has had left shoulder pain for the past 3 months. She reports that the pain has grown progressively worse over the past few months, and her shoulder function is severely limited. She is presently being treated with azathioprine and has used corticosteroids in the past. AP and axillary radiographs are shown in Figures 19a and 19b, and MRI scans are shown in Figures 19c and 19d. Which of the following forms of management will yield the most predictable pain relief and return of shoulder function?
Explanation
Explanation
19b 19c 19d Prosthetic shoulder arthroplasty has been shown to provide predictable results for treating stage III and stage IV osteonecrosis of the humeral head. The decision to resurface the glenoid (total shoulder arthroplasty versus humeral hemiarthroplasty) usually is made based on the radiographic and intraoperative appearance of the glenoid. Core decompression of the humeral head has been reported to be effective for earlier stages (pre collapse) but would not be appropriate for a patient with stage IV disease. Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Results of replacement. J Shoulder Elbow Surg 2000;9:177-182. L'Insalata JC, Pagnani MJ, Warren RF, et al: Humeral head osteonecrosis: Clinical course and radiographic predictors of outcome. J Shoulder Elbow Surg 1996;5:355-361.
References:
- Cruess RL: Steroid-induced avascular necrosis of the head of the humerus: Natural history and management. J Bone Joint Surg Br 1976;58:313-317.
Question 39High Yield
A 52-year-old man has a stage IIB malignant fibrous histiocytoma of the distal femur. Local treatment should consist of
Explanation
Explanation
Local control of malignant fibrous histiocytoma of bone typically consists of wide excision. Curettage and bone grafting is a procedure with an intralesional surgical margin, with an unacceptable rate of local recurrence. Prophylactic fixation is considered for patients with metastatic disease. Radiation therapy alone is not adequate for local control of this tumor. Neoadjuvant chemotherapy is often used primarily for systemic tumor control.
References:
- Bacci G, Picci P, Mercuri M, Bertoni F, Ferrari S: Neoadjuvant chemotherapy for high grade malignant fibrous histiocytoma of bone. Clin Orthop 1998;346:178-189.
Question 40High Yield
When harvesting an iliac crest bone graft from the posterior approach, what anatomic structure is at greatest risk for injury if a Cobb elevator is directed too caudal?
Explanation
If a Cobb elevator is directed caudally while stripping the periosteum over the iliac wing, it will encounter the sciatic notch. Although this puts the sciatic nerve at risk, the first structure encountered is the superior gluteal artery. Because it is tethered at the superior edge of the notch, it is very vulnerable to injury and can then retract inside the pelvis, making it difficult to obtain hemostasis. The inferior gluteal artery exits the sciatic notch below the piriformis and is more protected. The cluneal nerves are at risk only if the incision extends too anteriorly, and the sacroiliac joint can be entered while harvesting the graft. Banwart JC, Asher MA, Hassanein RS: Iliac crest bone graft harvest donor site morbidity: A statistical evaluation. Spine 1995;20:1055-1060.
Question 41High Yield
Which of the following factors has the most effect on the pullout strength of lumbar transpedicular screw fixation?
Explanation
Explanation
Although all of the factors listed contribute to the pullout strength of transpedicular screw fixation, low bone density generally is felt to be the most influential. Wittenberg RH, Shea M, Swartz DE, Lee KS, White AA III, Hayes WC: Importance of bone mineral density in instrumented spine fusions. Spine 1991;16:647-652.
References:
- Zindrick MR, Wiltse LL, Widell EH, et al: A biomechanical study of intrapeduncular screw fixation in the lumbosacral spine. Clin Orthop 1986;203:99-112.
Question 42High Yield
A 55-year-old patient is seeking a surgical consultation for a painful flatfoot deformity that has failed to respond to nonsteroidal anti-inflammatory drugs, shoe and activity modifications, and orthoses. The patient is of medium build, a nonsmoker, and has no history of diabetes mellitus. Radiographs are shown in Figures 43a through 43c. Based on these findings, treatment should consist of
Explanation
Explanation
43b 43c The patient has a degenerative collapse of the midfoot through the tarsometatarsal joints with significant forefoot abduction; therefore, a midfoot arthrodesis is required to address the arthritic joints and deformity at the tarsometatarsal articulation. All of the other procedures correct hindfoot deformities and therefore would not be appropriate treatment. Brage M: Degenerative joint disease of the midfoot. Foot Ankle Clin 1999;4:355-367.
References:
- Mann RA, Prieskorn D, Sobel M: Mid-tarsal and tarsometatarsal arthrodesis for primary degenerative osteoarthrosis or osteoarthrosis after trauma. J Bone Joint Surg Am 1996;78:1376-1385.
Question 43High Yield
A 56-year-old woman sustained the fracture shown in Figures 30a and 30b in a motor vehicle accident. What mechanism is most likely responsible for the injury?

Explanation
The CT scans show a burst fracture that results from an axial load injury. The radiographic hallmark of a burst fracture is compression of the posterior cortex of the vertebral body with retropulsion of bone into the spinal canal. AP radiographs often show widening of the interpedicular distance with a fracture of the lamina. Theiss SM: Thoracolumbar and lumbar spine trauma, in Stannard JP, Schmidt AH, Kregor PJ (eds): Surgical Treatment of Orthopaedic Trauma. New York, NY, Thieme, 2007, pp 179-207.
Question 44High Yield
A 65-year-old man with ankylosing spondylitis sustains an extension injury to his cervical spine. Two days later, a progressive neurologic deficit develops at the C6 level. An MRI scan is shown in Figure 1. What is the most likely diagnosis?
Explanation
It is common for patients with ankylosing spondylitis to sustain extension-type fractures, typically near the cervicothoracic junction. These fractures can be minimally displaced, making them difficult to diagnose. In addition, the vertebral bodies are vascular and their canals are relatively enclosed, making them vulnerable to epidural bleeding. The MRI scan shows an epidural hematoma posteriorly compressing the cord. Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142. Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spine fracture and spinal stenosis in ankylosing spondylitis. J Neurosurg 1982;57:609-616.
Question 45High Yield
A 68-year-old woman has been progressing slowly after undergoing humeral head replacement for a four-part fracture 3 months ago. She has not regained active elevation, she feels an audible clunk on attempting elevation, and she reports pain and weakness. She used a sling for 2 weeks in the immediate postoperative period. Radiographs are shown in Figure 37a through 37c. Management should consist of
Explanation
Explanation
37b 37c Immediate repair of the tuberosity and rotator cuff is recommended on identifying the avulsion or nonunion. Revising the humeral component to increase tension and length will overtighten the cuff and increase the chance of tuberosity pull-off. The glenoid is uninvolved and should not be replaced. Attempts to strengthen the rotator cuff will be unsuccessful because the insertions are no longer attached to the humerus when the tuberosities avulse. Brown TD, Bigliani LU: Complications with humeral head replacement. Orthop Clin North Am 2000;31:77-90.
References:
- Muldoon MP, Cofield RH: Complications of humeral head replacement for proximal humeral fractures. Instr Course Lect 1997;46:15-24.
Question 46High Yield
A 22-year-old professional ballet dancer reports a 3-month history of posterior ankle pain that occurs when she changes from a flat foot to pointe (hyperplantar flexed position). Examination does not elicit the pain with forced passive plantar flexion. A radiograph is shown in Figure 8. What is the most likely cause of the pain?
Explanation
Explanation
The most common causes of posterior ankle pain in ballet dancers are flexor hallucis longus tenosynovitis and os trigonum syndrome. Flexor hallucis longus tenosynovitis differs from a symptomatic os trigonum by the absence of pain with forced plantar flexion and the presence of pain with resisted plantar flexion of the great toe. The pain is often felt in the posterior ankle and can be associated with a snapping or triggering sensation. Os trigonum syndrome commonly occurs in ballet dancers who perform in a position of extreme plantar flexion. The pain occurs from entrapment of the os trigonum between the posterior portion of the talus and calcaneus. Hamilton WG, Geppert MJ, Thompson FM: Pain in the posterior aspect of the ankle in dancers: Differential diagnosis and operative treatment. J Bone Joint Surg Am 1996;78:1491-1500.
References:
- Khan K, Brown J, Way S, et al: Overuse injuries in classical ballet. Sports Med 1995;19:341-357.
Question 47High Yield
An 18-year-old high school football player sustains a left posterior hip dislocation that is reduced in the emergency department under IV sedation. Postreduction radiographs reveal a concentric reduction with no evidence of fracture or loose bodies within the joint. What is the most common complication of hip dislocations?
Explanation
Explanation
Traumatic dislocation of the hip in sports injuries is uncommon, and 85% to 92% occur in a posterior direction. In dislocations without fractures, osteonecrosis is the most common complication occurring in 10% to 20% of patients. MRI should be performed at 3 months postreduction to rule out osteonecrosis. Nerve injuries are rare in this setting, and recurrent dislocations are unusual without acetabular fractures. Chondrolysis has been reported as a rare occurrence. Anderson K, Strickland S, Warren R: Hip and groin injures in athletes. Am J Sports Med 2001;29:521-533.
References:
- Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 407-416.
Question 48High Yield
Which of the following changes of calcium metabolism accompany the loss of bone during menopause?
Explanation
There is a negative change of calcium balance with a decrease in intestinal absorption and an increase in urinary calcium loss. The reduction of intestinal absorption is accompanied by reduced circulating concentrations of total, but not free 1,25-dihydroxyvitamin D. However, estrogen may also directly regulate intestinal calcium resorption independent of vitamin D. Tubular resorption of calcium is higher in the presence of estrogen. Studies of the levels of PTH in the presence of estrogen are controversial. Oh KW, Rhee EJ, Lee WY, et al: The relationship between circulating osteoprotegerin levels and bone mineral metabolism in healthy women. Clin Endocrinol (Oxf) 2004;61:244-249.
Question 49High Yield
Which of the following nerves is susceptible to entrapment near the calcaneal attachment site of the plantar fascia and can mimic or co-exist with plantar fasciitis?
Explanation
Explanation
The first branch of the lateral plantar nerve is susceptible to entrapment beneath the deep fascia of the adductor hallucis muscle adjacent to the calcaneal attachment of the plantar fascia. This can be a cause of chronic heel pain. Additionally, the nerve is vulnerable to injury by a blind dissection in releasing the plantar fascia. The dorsal cutaneous branch of the superficial peroneal nerve supplies sensation to the dorsum of the foot. The medial calcaneal branch of the posterior tibial nerve lies in the subcutaneous tissues and innervates the skin of the heel. It is vulnerable to injury from skin incisions on the medial side of the heel. The lateral branch of the medial plantar nerve forms the second and third common digital nerves. Entrapment of the proper medial plantar nerve can occur at the master knot of Henry. This is well distal to the calcaneal attachment of the plantar fascia, and the pain usually radiates more distally in the arch, separate from heel pain. The communicating branch of the fourth common digital nerve crosses to the third common digital nerve. Therefore, the third common digital nerve receives supply from both the lateral and medial plantar nerves. This dual supply has been implicated in the increased incidence of digital neuroma of the third common digital nerve. Bordelon RL: Heel pain, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 837-857. Mann RA, Baxter DE: Diseases of the nerves, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 543-574.
References:
- Baxter DE: The heel in sport. Clin Sports Med 1994;13:683-693.
Question 50High Yield
A 10-year-old boy with an L1 myelomeningocele has a low-grade fever and a swollen thigh that is warm to touch and erythematous. AP and lateral radiographs are shown in Figures 24a and 24b. Management should consist of

Explanation
Fractures of the long bones are common in patients with myelodysplasia, and the frequency of fracture increases with higher level defects. Fractures also occur following surgery and immobilization secondary to disuse osteoporosis. The response to the fracture (swelling, fever, warmth, erythema) is often confused with infection, osteomyelitis, or cellulitis. Management should consist of a short period of immobilization in a well-padded splint. Long-term casting results in further osteopenia and repeated fractures. Lock TR, Aronson DD: Fractures in patients who have myelomeningocele. J Bone Joint Surg Am 1989;71:1153-1157.
Question 51High Yield
A 15-year-old athlete collapses suddenly during practice and dies. What is the most likely cause of death?
Explanation
The number one cause of sudden death in the young athlete is myocardial pathology, with hypertrophic cardiomyopathy being most common. Because of cardiac muscle hypertrophy, the ventricular capacity is diminished and can result in decreased cardiac output. During exertional activities, the increased demand may not be able to be met and leads to sudden death. While the other choices can be the cause of sudden death in an otherwise healthy young athlete, their incidence is even more rare. Van Camp SP, Bloor CM, Mueller FO, et al: Nontraumatic sports death in high school and college athletes. Med Sci Sports Exerc 1995;27:641-647. Maron BJ, Shirani J, Pollac LC, et al: Sudden death in young competitive athletes: Clinical, demographic, and pathological profiles. JAMA 1996;276:199-204.
Question 52High Yield
A 37-year-old man who works in a factory has isolated, lateral unicompartmental pain about his knee with activities. Nonsurgical management has failed to provide relief. The radiograph shown in Figure 45 reveals a tibiofemoral angle of approximately 15 degrees which is clinically correctable to neutral. What is the best surgical option in this patient?
Explanation
Explanation
Patients with a valgus alignment about the knee can have lateral compartment arthritis. Similar to a high tibial osteotomy, a supracondylar femoral osteotomy is indicated in younger patients who have a more active lifestyle and isolated unicompartmental disease. In this young patient who works in a factory and has a valgus knee, a medial closing wedge supracondylar femoral osteotomy is the treatment of choice. The role of arthroplasty is limited in younger patients. Mathews J, Cobb AG, Richardson S, et al: Distal femoral osteotomy for lateral compartment osteoarthritis of the knee. Orthopedics 1998;21:437-440.
References:
- Cameron HU, Botsford DJ, Park YS: Prognostic factors in the outcome of supracondylar femoral osteotomy for lateral compartment osteoarthritis of the knee. Can J Surg 1997;40:114-118.
Question 53High Yield
Figure 48 shows the initial AP chest radiograph of a 21-year-old motorcycle rider who sustained multiple injuries after striking a telephone pole at high speed. What is the most significant radiographic finding leading to a diagnosis?
Explanation
Scapulothoracic dissociation is a rare, violent traumatic injury in which the scapula is torn away from the chest wall but the skin remains intact. Massive swelling and ecchymosis are common. Neurovascular injury is the rule with possible subclavian or axillary artery disruption and severe partial or complete brachial plexus paralysis. The diagnosis is made on a nonrotated chest radiograph that shows significant lateral displacement of the medial scapular border from the sternal notch. A right midshaft clavicular fracture is present but is not considered the most significant finding. Ebraheim NA, An HS, Jackson WT, et al: Scapulothoracic dissociation. J Bone Joint Surg Am 1988;70:428-432. Ebraheim NA, Pearlstein SR, Savolaine ER, et al: Scapulothoracic dissociation. J Orthop Trauma 1987;1:18-23. Sampson LN, Britton JC, Eldrup-Jorgensen J, et al: The neurovascular outcome of scapulothoracic dissociation. J Vasc Surg 1993;17:1083-1088.
Question 54High Yield
A 68-year-old woman undergoes a complicated four-level anterior cervical diskectomy and fusion at C3-7 with iliac crest bone graft and instrumentation for multilevel cervical stenosis. Surgical time was approximately 6 hours and estimated blood loss was 800 mL. Neuromonitoring was stable throughout the procedure. The patient's history is significant for smoking. The most immediate appropriate postoperative management for this patient should include
Explanation
Explanation
Airway complications after anterior cervical surgery can be a catastrophic event necessitating emergent intubation for airway protection. Multilevel surgeries requiring long intubation and prolonged soft-tissue retraction as well as preexisting comorbidities may predispose a patient to postoperative airway complications. Sagi and associates reported that surgical times greater than 5 hours, blood loss greater than 300 mL, and multilevel surgery at or above C3-4 are risk factors for airway complications. In surgical procedures with the aforementioned factors, serious consideration should be given to elective intubation for 1 to 3 days to avoid urgent reintubation. Sagi HC, Beutler W, Carroll E, et al: Airway complications associated with surgery on the anterior cervical spine. Spine 2002;27:949-953. Epstein NE, Hollingsworth R, Nardi D, et al: Can airway complications following multilevel anterior cervical surgery be avoided? J Neurosurg 2001;94:185-188.
Question 55High Yield
An obese 56-year-old woman with hypertension has had posterior heel pain for the past 6 months. She also notes some enlargement over the posterior aspect of the heel. Examination reproduces pain with palpation at the insertion of the Achilles tendon. A lateral radiograph is shown in Figure 45. What is the most likely diagnosis?
Explanation
Explanation
The lateral radiograph shows a traction spur consistent with tendinopathy of the Achilles tendon. There is no displacement of the spur to suggest a rupture of the Achilles tendon, and os trigonum is not seen on the radiograph. The examination findings are not consistent with nerve entrapment. Schepsis AA, Wagner C, Leach RE: Surgical management of Achilles tendon overuse injuries: A long-term follow-up study. Am J Sports Med 1994;22:611-619.
References:
- Saltzman CL, Tearse DS: Achilles tendon injuries. J Am Acad Orthop Surg 1998;6:316-325.
Question 56High Yield
What is the most accurate description of the relationship between gender and knee loading during landing while playing basketball?
Explanation
Explanation
Ford and associates studied 81 high school basketball players and found that females landed with greater total valgus knee loading and a greater maximum valgus knee angle than male athletes. Hewett and associates reported in a study of 205 female athletes that those with increased dynamic valgus and high abduction loads were at increased risk of anterior cruciate ligament injury. Hewett TE, Myer GD, Ford KR, et al: Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am J Sports Med 2005;33:492-501.
References:
- Ford KR, Meyer GD, Hewett TE: Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exer 2003;35:1745-1750.
Question 57High Yield
A 63-year-old woman has a femoral neck fracture. A biopsy specimen obtained from the fracture site at the time of her hemiarthroplasty reveals metastatic carcinoma. Seven days after surgery, she becomes confused and lethargic. Which of the following laboratory values is most likely implicated in the patient's symptoms at this time?
Explanation
Explanation
Although many hematologic and electrolyte abnormalities may be present in a patient with advanced metastatic cancer, an elevated serum calcium level is most commonly associated with confusion. Treatment with hydration, diuretics, and bisphosphonates is recommended. Clohishy D: Management of skeletal metastasis in clinical orthopaedics, in Craig E (ed): Operative Orthopaedics. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 994-997.
References:
- Mundy GR: Hypercalcemia of malignancy revisited. J Clin Invest 1988;82:1-6.
Question 58High Yield
A construction worker sustained a comminuted calcaneus fracture 2 years ago. He now reports progressive hindfoot pain with the recent onset of anterior ankle pain. A lateral hindfoot radiograph is shown in Figure 31. Treatment should consist of
Explanation
The patient has subtalar arthrosis, a loss of heel height with anterior ankle impingement. The mechanics of the ankle are impaired, and dorsiflexion is painful and limited. The talar declination angle is measured by drawing a line through the longitudinal axis of the talus and the plane of support of the foot on a weight-bearing lateral radiograph. Anterior impingement is suggested with any value below 20°. By performing a distraction arthrodesis through the subtalar joint, the normal declination of the talus is reestablished, eliminating the anterior ankle impingement. Tibiotalocalaneal fusion would be inappropriate because the patient does not have arthritic symptoms in the ankle. Ankle arthroscopy or in situ arthrodesis would not reestablish appropriate ankle mechanics, and the osteophytes would be prone to redevelop. Lateral wall ostectomy may help with impingement at the level of the fibula or the lateral ankle but would provide no benefit to anterior ankle impingement. Carr JB, Hansen ST, Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
Question 59High Yield
A 40-year-old woman has local back pain and intense burning pain in her perianal region after being shot twice in the back. Motor and sensory examination of her lower extremities reveals no apparent deficit. She has present but decreased sensation in her perianal region, an intact anal wink, good rectal tone, and an intact bulbocavernosus reflex. Radiographs and CT scans are shown in Figures 3a through 3d. What is the next most appropriate step in management?
Explanation
Explanation
3b 3c 3d Because the patient has an apparent compressive neuropathy secondary to the metallic fragments, removal of the fragments in this incomplete lesion at the cauda equina level can be expected to improve her sensory dysesthesias and pain. Steroids are not indicated in a root lesion secondary to a penetrating injury. MRI will have significant artifact effect and will not provide much additional information. The posterior bony elements are not significantly injured; therefore, stabilization is not indicated. Bracken MB, Shepard MJ, Holford TR: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury. JAMA 1997;277:1597-1604. Waters RL, Adkins RH: The effects of removal of bullet fragments retained in the spinal canal: A collaborative study by the National Spinal Cord Injury Model Systems. Spine 1991;16:934-939.
References:
- Stauffer ES, Wood RW, Kelly EG: Gunshot wounds of the spine: The effects of laminectomy. J Bone Joint Surg Am 1979;61:389-392.
Question 60High Yield
Figure 29 shows the AP radiograph of a 14-year-old boy. The radiographic findings are most consistent with what pathologic process?
Explanation
Explanation
The severe depression of the proximal medial tibial epiphysis is most consistent with the diagnosis of neglected infantile Blount's disease. Blount's disease in adolescents produces a deformity in the metaphyseal region. Septic arthritis and JRA affect both sides of the joint. Hemophilia produces a characteristic widening of the intercondylar notch. Thompson GH, Carter JR: Late-onset tibia vara (Blount's Disease). Clin Orthop 1990;255:24-35.
References:
- Raney EM, Topoleski TA, Yaghoubian R, et al: Orthotic treatment of infantile tibia vara. J Pediatr Orthop 1998;18:670-674.
Question 61High Yield
A 35-year-old man has had progressive right knee pain for the past 2 months. An AP radiograph, bone scan, MRI scan, and photomicrograph are shown in Figures 34a through 34d. What is the most appropriate treatment of this lesion?
Explanation
Explanation
34b 34c 34d This is a classic case of giant cell tumor of bone. The radiograph and the MRI scan reveal a purely lytic lesion in the medial femoral condyle. The lesion is well-demarcated without a rim of sclerotic bone. It is eccentrically located and abuts the subchondral bone. The lesion demonstrates increased uptake on a technetium TC 99m bone scan. These imaging studies are highly suggestive of giant cell tumor arising in its most common location. The photomicrograph confirms the diagnosis of giant cell tumor. Based on these findings, the most widely accepted treatment is extended curettage plus a local adjuvant such as polymethylmethacrylate bone cement, argon beam coagulation, liquid nitrogen, and/or phenol. Lackman RD, Hosalkar HS, Ogilvie CM, et al: Intralesional curettage for grades II and III giant cell tumors of bone. Clin Orthop Relat Res 2005;438:123-127.
References:
- Ward WG Sr, Li G III: Customized treatment algorithm for giant cell tumor of bone: Report of a series. Clin Orthop Relat Res 2002;397:259-270.
Question 62High Yield
A 13-year-old boy has a painless "knot" over his left hip. History reveals that he injured his left hip playing soccer 4 months ago. A radiograph and MRI scan obtained at the time of injury are shown in Figures 7a and 7b. He is very active and is currently asymptomatic. A current radiograph is shown in Figure 7c. What is the next most appropriate step in management?


Explanation
The diagnosis is myositis ossificans resulting from an injury. The initial radiograph reveals a small amount of mineralization in the soft tissues overlying the left hip. The MRI scan shows signal abnormality of the entire gluteus minimus muscle with a mineralized mass in the center. The current radiograph shows a lesion within the abductor musculature with mature ossification peripherally. The imaging studies are diagnostic and the patient is asymptomatic; therefore, the management of choice is observation with no further evaluation or treatment indicated. Miller AE, Davis BA, Beckley OA: Bilateral and recurrent myositis ossificans in an athlete: A case report and review of treatment options. Arch Phys Med Rehabil 2006;87:286-290.
Question 63High Yield
The inheritance of the deformity shown in Figure 1 is most commonly
Explanation
Explanation
Cleft hand and cleft foot malformations are commonly inherited as autosomal-dominant traits and are associated with a number of syndromes. An autosomal-recessive and an x-linked inheritance pattern have also been described, but these are much less common and are usually atypical. In the common autosomal-dominant condition, nearly one third of the known carriers of the gene show no hand or foot abnormalities. This is known as reduced penetrance. The disorder may be variably expressed; affected family members often exhibit a range from mild abnormalities in one limb only to severe anomalies in four limbs. Variable expressivity and reduced penetrance can cause difficulty in counseling families regarding future offspring in an affected family. Many patients have a cleft hand that may be caused by the split-hand, split-foot gene (SHFM1) localized on chromosome 7q21.
References:
- Kay SPJ: Cleft hand, in Green DP (ed): Green's Operative Hand Surgery. Philadelphia, Pa, Churchill Livingston, 1999, pp 402-414.
Question 64High Yield
Based on the type of articulation shown in Figure 32, wear is not affected by which of the following factors?
Explanation
Explanation
Wear in total hip arthroplasty is a very complex phenomenon. The radial mismatch of the femoral head to the acetabular component has been shown in multiple studies to be a significant factor in wear. The mismatch can neither be too small nor too large. When the mismatch is too small, seizing of the implants can occur. When the mismatch is too large, contact stresses increase and produce exceptionally high wear. The ideal radial mismatch should be approximately 50 microns. Surface roughness and ball sphericity are two items that are extremely important with respect to wear. High carbon content has been shown to decrease wear. This device has a very large head-to-neck ratio, so impingement-related wear is unlikely. Amstutz HC, Grigoris P: Metal on metal bearings in hip arthroplasty. Clin Orthop 1996;329:S11-S34. Amstutz HC, Campbell P, McKellop H, et al: Metal on metal total hip replacement workshop consensus document. Clin Orthop 1996;329:S297-S303.
References:
- McKellop H, Park SH, Chiesa R, et al: In vivo wear of three types of metal on metal hip prostheses during two decades of use. Clin Orthop 1996;329:S128-S140.
Question 65High Yield
Initial management of a pathologic fracture of the humerus secondary to a unicameral bone cyst should include
Explanation
Explanation
Most pathologic humeral fractures secondary to a unicameral bone cyst are minimally displaced and should be immobilized and allowed to heal. Persistent and/or progressive lesions may require treatment. Various treatments of unicameral bone cysts have been described. Acceptable treatment options include curettage and bone grafting, intralesional steroid injection, and percutaneous grafting with bone graft substitutes. MRI is not indicated when the diagnosis of unicameral bone cyst is known. Wilkins RM: Unicameral bone cysts. J Am Acad Orthop Surg 2000;8:217-224.
References:
- Bensahel H, Jehanno P, Desgrippes Y, Pennecot GF: Solitary bone cyst: Controversies and treatment. J Pediatr Orthop B 1998;7:257-261.
Question 66High Yield
A patient is scheduled to undergo total knee arthroplasty (TKA) following failure of nonsurgical management. History reveals that she underwent a patellectomy as a teenager as the result of a motor vehicle accident. Examination reveals normal ligamentous stability. For the most predictable outcome, which of the following implants should be used?
Explanation
Explanation
Paletta and Laskins performed a retrospective study of the results of TKA with cement in 22 patients who had a previous patellectomy. Nine of the patients had insertion of a posterior cruciate ligament-substituting implant. Thirteen patients had insertion of a posterior cruciate ligament-sparing implant. The 5-year postoperative knee scores were 89 for the posterior cruciate ligament-substituting knee versus 67 for the posterior cruciate ligament-sparing knee (P < 0.01). The patella functions to increase the lever arm of the extensor mechanism and to position the quadriceps tendon and the patellar ligament roughly parallel to the anterior cruciate ligament and posterior cruciate ligament, respectively. The patellar ligament thereby provides a strong reinforcing structure that functions to prevent excessive anterior translation of the femur during flexion of the knee. The absence of the patella results in the patellar ligament and the quadriceps tendon being relatively in line with one another. After a patellectomy, the resultant quadriceps force is no longer parallel to the posterior cruciate ligament. This results in loss of the reinforcing function of the patellar ligament. The authors believe this loss of reinforcing function may place increased stresses on the posterior cruciate ligament and posterior aspect of the capsule, which may result in stretching of these structures over time. They found a high rate of anteroposterior instability, a high prevalence of recurvatum, and a high rate of loss of full active extension compared with passive extension in the posterior cruciate ligament-sparing group, which supports their theory. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
References:
- Paletta GA Jr, Laskins RS: Total knee arthroplasty after a previous patellectomy. J Bone Joint Surg Am 1995;77:1708-1712.
Question 67High Yield
A patient with a below-the-knee amputation is being evaluated for a new prosthesis. He wants to improve his ability to walk on uneven surfaces. What modification to the prosthesis can be made to accommodate this request?
Explanation
Changing from a solid keel to a keel with a sagittal split allows an amputee to navigate uneven terrain more easily. Changing the length of the keel affects the responsiveness of the prosthesis but does not address the surface conditions for ambulation. The SACH is not used as frequently anymore, because overload problems to the nonamputated foot have been observed. Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 31-45.
Question 68High Yield
During particle-induced osteolysis around implants, what cell secretes most of the interleukin-6 (IL-6)?
Explanation
Explanation
During osteolysis, IL-6 is secreted by fibroblasts in the membrane surrounding the prosthesis. IL-6 also can be secreted by osteoblasts in other settings, but they are not the predominant source of IL-6 in particle-induced osteolysis. The remaining cells are not major sources of IL-6.
References:
- Bukata SV, Gelinas J, Wei X, et al: PGE2 and IL-6 production by fibroblasts in response to titanium wear debris particles is mediated through a Cox-2 dependent pathway. J Orthop Res 2004;22:6-12.
Question 69High Yield
A 63-year-old woman with a history of poliomyelitis has a fixed 30-degree equinus contracture of the ankle, rigid hindfoot valgus, and normal knee strength and stability. She reports persistent pain and has had several medial forefoot ulcerations despite a program of stretching, bracing, and custom footwear. What is the next most appropriate step in management?
Explanation
Explanation
The patient has a fixed deformity of the hindfoot and an Achilles tendon contracture; therefore, the treatment of choice is triple arthrodesis with Achilles tendon lengthening. Further bracing will not be helpful. Amputation is not indicated, and ankle arthrodesis will not address the hindfoot deformity. Palliative management would be more appropriate if the knee was unstable or the quadriceps were weak, because the equinus balances the ground reaction force across the knee. Perry J, Fontaine JD, Mulroy S: Findings in post-poliomyelitis syndrome: Weakness of muscles of the calf as a source of late pain and fatigue of muscles of the thigh after poliomyelitis. J Bone Joint Surg Am 1995;77:1148-1153.
References:
- Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
Question 70High Yield
A 22-year-old competitive volleyball player has shoulder pain, and rest and a cortisone injection have failed to provide relief. Examination reveals atrophy along the posterior scapula, but an MRI scan does not reveal a rotator cuff tear or labral cyst. What is the most likely cause for the shoulder weakness?
Explanation
Explanation
Repetitive overhead slams and serves may produce a traction injury to the distal branch of the suprascapular nerve. Bankart, biceps, and superior labrum anterior and posterior injuries can occur but usually do not produce visible atrophy. Muscle avulsion is uncommon. Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
References:
- Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthroscopy 1990;6:301-305.
Question 71High Yield
A 56-year-old mechanic has had pain in the hypothenar region of his dominant right hand for the past 6 months. He reports weakness in his grip and pain is worse with activity. Which of the following examination findings is most suggestive of a cervical etiology?
Explanation
Hypothenar atrophy is a nonspecific sign that can be seen in ulnar neuropathy, C8 radiculopathy, or even cervical myelopathy; however, the atrophy usually is not unilateral and includes other muscle groups. The Spurling test is an excellent method of eliciting cervical radicular pain but involves hyperextension and ipsilateral rotation of the cervical spine, resulting in nerve root compression by reducing the cross-sectional area of the ipsilateral neuroforamen. Tinel's sign at the levator scapulae, if present, is indicative of an upper cervical (C3 or C4) radiculopathy. A subluxable ulnar nerve at the cubital tunnel, while often asymptomatic, points toward cubital tunnel syndrome as an etiology for this patient's pain. The shoulder abduction relief (SAR) sign (relief of upper extremity pain with shoulder abduction) is virtually pathognomic of cervical radiculopathy because this maneuver results in relaxation of a compressed and/or inflamed cervical nerve root. The SAR sign is the converse analog of the straight leg raising sign in the lumbar examination for lumbar radiculopathy, as it relieves tension in the nerve root, thereby relieving symptoms. Ducker TB, Zeidman SM: Neurologic and functional evaluation, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 143-161. An HS: Clinical presentation of discogenic neck pain, radiculopathy, and myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 755-764.
Question 72High Yield
To preserve blood supply to the fractured bone seen in Figures 12a and 12b, care should be taken when exposing which of the following areas?
Explanation
Explanation
12b The blood supply to the adult capitellum and lateral trochlea comes from posterior vessels arising from the radial recurrent, radial collateral, and interosseous recurrent arteries. These arteries penetrate the distal humerus posterior and superior to the capitellum.
References:
- Yamaguchi K, Sweet FA, Bindra R, et al: The extraosseous and intraosseous arterial anatomy of the adult elbow. J Bone Joint Surg Am 1997;79:1653-1662.
Question 73High Yield
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on
Explanation
The patient has heterotopic ossification, a more common finding in patients who have sustained head injuries. Treatment will require removal of the heterotopic bone and anterior and posterior capsulectomies. The main concern about timing is the possible recurrence of heterotopic bone. While an extended wait was once thought necessary, this is no longer true. The timing is based on the time since injury and evidence of bone maturation on plain radiographs. A sharp marginal demarcation of the new bone and a trabecular pattern within it are usually present 3 to 6 months after onset, indicating that it is safe to proceed with surgical excision. It is not necessary to wait more than 6 months. Bone scan results are not good indicators because they may remain "hot" for long periods of time. The levels of alkaline phosphatase and serum calcium-phosphorus product do not need to be measured.
Question 74High Yield
When an adult hip is surgically dislocated for relief of femoro-acetabular impingment, what is the risk of postoperative iatrogenic osteonecrosis?
Explanation
Explanation
In a report of more than 70 hips treated by surgical dislocation, iatrogenic osteonecrosis failed to develop in any of the hips.
References:
- Ganz R, Gill TJ, Gautier E, Ganz K, Krugel N, Berlemann U: Surgical dislocation of the adult hip: A technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-1124.
Question 75High Yield
In children with moderate to severe osteogenesis imperfecta (OI), intravenous pamidronate therapy has been shown to increase the thickness of cortical bone. This occurs primarily as a consequence of
Explanation
Histologic studies have shown that increased bone turnover is the rule in OI. Pamidronate (and all bisphosphonates) reduce osteoclast-mediated bone resorption. Osteoblastic new bone formation on the periosteal surface of long bones is minimally impaired. With inhibition of osteoclastic bone resorption on the endosteal surface, the cortex of the bone can begin to thicken as it does with normal growth in individuals unaffected by OI. Mineralization and collagen matrix organization are not directly affected by pamidronate. Zeitlin L, Fassier F, Glorieux FH: Modern approach to children with osteogenesis imperfecta. J Pediatr Orthop B 2003;12:77-87. Falk MJ, Heeger S, Lynch KA, et al: Intravenous bisphosphonate therapy in children with osteogenesis imperfecta. Pediatrics 2003;111:573-578.
Question 76High Yield
A 2-year-old girl has had a swollen right knee for the past 7 weeks. There is no history of significant trauma, and she has not had a fever or been ill. Her parents report that she is stiff in the morning but otherwise does not report pain. A CBC count and erythrocyte sedimentation rate are normal. Treatment with naproxen at appropriate doses for the past 2 weeks has resulted in some improvement. Radiographs show only soft-tissue swelling. Examination reveals a healthy-appearing child with a warm and swollen right knee that is only slightly tender but lacks full extension by 20 degrees. What is the next most appropriate step in management?
Explanation
Explanation
Up to 30% of children with juvenile rheumatoid arthritis (increasingly known now as juvenile idiopathic arthritis or JIA) already have potentially damaging uveitis at the time of diagnosis. This patient has typical oligoarticular JRA (JIA) and therefore is at significant risk for uveitis. MRI, radioisotope scanning, or an ACE level most likely would not provide additional useful diagnostic information because intra-articular derangement, osteomyelitis, or sarcoidosis are all unlikely. Arthrocentesis and triamcinolone hexacetonide joint injection might be indicated if continued use of nonsteroidal medication does not result in improvement, but should be held off for at least an additional 4 to 6 weeks to see if continued use of naproxen results in control of the arthritis. Wolf MD, Lichter PR, Ragsdale CG: Prognostic factors in the uveitis of juvenile rheumatoid arthritis. Ophthalmology 1987;94:1242. Cassidy JT, Petty RE: Textbook of Pediatric Rheumatology. Philadelphia, PA, WB Saunders, 2001, p 220.
References:
- Chalom ED, Goldsmith DP, Koehler MA, et al: Prevalence and outcome of uveitis in a regional cohort of patients with juvenile rheumatoid arthritis. J Rheumatol 1997;24:2031-2034.
Question 77High Yield
A previously asymptomatic 14-year-old girl sustained a twisting injury to her ankle. Radiographs are shown in Figures 2a and 2b. Management should consist of

Explanation
The radiographs show a well-defined, irregular, eccentric lesion in the distal tibia metaphysis with a thin sclerotic margin. The radiographs are diagnostic of nonossifying fibroma, a common entity in this age group and in this location. No further work-up is indicated. The patient was asymptomatic prior to the injury and the lesion is small and thus not worrisome for an impending pathologic fracture; therefore, no treatment is indicated beyond observation. The natural history of these lesions is to gradually ossify as the patient reaches skeletal maturity. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 69-75.
Question 78High Yield
A 22-month-old child has scrapes and bruises on his head and a severe deformity of the forearm after being thrown from a car as an unrestrained passenger in a motor vehicle accident. Examination reveals a Glasgow Coma Scale score of 12. Prior to treatment of the forearm, management should include
Explanation
Explanation
As CT scanning has become available, the use of radiographs of the skull has decreased in importance for evaluation of head trauma. The indications for CT scanning for suspected head trauma include any degree of obtundation, focal neurologic deficit, history of a high-velocity injury, amnesia for the injury, progressive headache, persistent vomiting, children younger than age 2 years, serious facial injury, posttraumatic seizure, skull penetration, or a Glasgow Coma Scale score of 13 or less. Evidence of improved outcome with use of steroids in head trauma is lacking. Steroids are useful for increased intracranial pressure caused by brain tumors or abscesses. High-dose IV methylprednisolone is indicated for spinal cord trauma and improves the ultimate degree of recovery of function. When herniation is suspected in a patient with asymmetric neurologic findings or the patient's condition is deteriorating rapidly, a mannitol infusion may be used. Hall DE: Head injuries, in Hoekelman RA (ed): Primary Pediatric Care. St Louis, Mo, Mosby, 1997, pp 1709-1712. Nelson WE, Behrman RE, Kliegman RM (eds): Nelson Essentials of Pediatrics. Philadelphia, Pa, WB Saunders, 1998, p 712.
References:
- Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 123-130.
Question 79High Yield
Iliosacral screws placed for stabilization of posterior pelvic ring injuries (eg, sacroiliac dislocation) that exit the sacrum anteriorly are most likely to injure which of the following structures?
Explanation
Iliosacral screws have gained popularity for posterior stabilization of pelvic ring disruptions, but complications attributed to incorrect placement are a clinical problem. The L5 nerve root is at greatest risk and is in closest proximity to a malpositioned screw (exiting the sacrum). The L4 root is more anterior at this level. The S1 root is still intraosseous at this level and is at risk but not from the screw exiting anteriorly at this level. The arteries are at risk but are more anterior and are at less risk than the L5 nerve root.
Question 80High Yield
What effect does deep freezing have on allograft tissue?
Explanation
Explanation
Deep freezing is the simplest and most widely used method of ligament allograft storage. All cells in the tissue are destroyed with the freezing. However, for this reason, it is not a preferred storage method for menisci or cartilage allografts. Although this method may enhance success because it removes potential antigens located on the cells, it cannot guarantee elimination of HIV transmission. The advantage of cryopreservation storage is that a significant number of cells will survive the process, a factor important in meniscal allograft survival after implantation. No deleterious effects are noted clinically because of the acellularity of the tissue. Shelton WR, Treacy SH, Dukes AD, Bomboy AL: Use of allografts in knee reconstruction: I. Basic science aspects and current status. J Am Acad Orthop Surg 1998;6:165-168.
References:
- Caspari RB, Botherfield S, Horwitz RL, et al: HIV transmission via allograft organs and tissues. Sports Med Arthroscopy Rev 1993;1:42-46.
Question 81High Yield
A 70-year-old woman had poliomyelitis as a young child, and the residual weakness she has as an adult principally involves the lower extremities. She now notes progressive weakness in both legs and she tires easily. What is the best course of action?
Explanation
The most likely diagnosis is postpolio syndrome, which is characterized by increasing weakness in both the paretic and previously normal muscles. Fatigability, joint pain, muscle atrophy, respiratory insufficiency, dysphagia, and sleep apnea are also seen. Gentle exercise and modification in lifestyle demands are generally recommended. Vigorous rehabilitation is likely to be detrimental in this condition. Further diagnostic work-up is not indicated at this time. Dalakas MC, Elder G, Hallett M, et al: A long-term follow-up study of patients with post-poliomyelitis neuromuscular symptoms. N Eng J Med 1986;314:959-963.
Question 82High Yield
Following reconstruction of the anterior cruciate ligament (ACL), which of the following rehabilitation exercises has the greatest potential to harm the graft?
Explanation
Isometric quadriceps contraction between 15 and 30 degrees of flexion creates significant strain in the ACL and potential damage to the reconstructed graft. Isolated quadriceps contraction with knee flexion of greater than 60 degrees, hamstring contraction at any angle of knee flexion, and active knee motion between 35 and 90 degrees of flexion create substantially less strain in the properly implanted ACL graft. Beynnon BD, Gleming BC, Johnson RL, Nichols CE, Renstrom PA, Pope MH: Anterior cruciate ligament strain behavior during rehabilitation exercises in vivo. Am J Sports Med 1995;23:24-34.
Question 83High Yield
Nonsurgical management of pectoralis major tears is likely to result in weakness of glenohumeral
Explanation
Nonsurgical management is considered for proximal tears as well as partial tears in some individuals. Surgical management is often not appropriate in older or sedentary patients. However, patients treated nonsurgically will have a significant cosmetic defect, as well as weakness in adduction and internal rotation. Schepsis AA, Grafe MW, Jones HP, et al: Rupture of the pectoralis major muscle: Outcome or repair of acute and chronic injuries: Am J Sports Med 2000;28:9-15.
Question 84High Yield
What is the most common neurologic complication following an anterior cervical diskectomy and fusion?
Explanation
The recurrent laryngeal nerve provides innervation to the vocal cords and was the most common neurologic injury reported in a series of 36,000 patients. The nerve is felt to be more vulnerable during a right-sided approach because of its anatomic course. A recent study has also suggested a role for increased endotracheal cuff pressures in this nerve injury. Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Question 85High Yield
Figures 26a through 26c show the MRI scans of a 47-year-old man who underwent arthroscopic shoulder surgery 6 months ago and continues to have pain despite a prolonged course of rehabilitation. Management should now consist of


Explanation
The MRI scans show an os acromiale of the mesoacromion type. This represents an unfused acromial apophysis. Pain is thought to be caused by either motion at the site or downward displacement of the anterior aspect of the acromion onto the rotator cuff, causing impingement. Most patients can be treated nonsurgically as they are usually asymptomatic. In those patients with persistent symptoms of pain and tenderness over the acromion, surgery consisting of rigid internal fixation and bone grafting has yielded satisfactory results. Excision may be a viable treatment option for the preacromion type. Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20. Warner JP, Beim GM, Higgins L: The treatment of symptomatic os acromiale. J Bone Joint Surg Am 1998;80:1320-1326.
Question 86High Yield
A 21-year-old football player who sustained a direct blow to the posterior hindfoot while making a cut is unable to bear weight on the injured foot. Examination reveals tenderness and swelling of the great toe metatarsophalangeal (MTP) joint. Radiographs are shown in Figures 9a and 9b. What is the most likely diagnosis?
Explanation
Explanation
9b Turf toe occurs in collision and contact sports in which the athlete pushes off to accelerate or change direction and there is hyperextension of the great toe MTP joint. Typically, there is also axial loading of the posterior hindfoot, which increases the hyperextension of the MTP joint. The most common presentation is pain and swelling of the MTP joint and inability to hyperextend the joint without significant symptoms. With significant force, fractures of the sesmoids and plantar soft tissues can occur. The radiographs do not show a dislocation of the great toe MTP joint because it is concentrically located on both radiographs. However, the radiographs show a fracture of the lateral sesamoid or a diastasis of a bipartite lateral sesamoid. The medial sesamoid is also proximal indicating a rupture of the plantar (volar) plate. Therefore, the most likely diagnosis is a fracture of the lateral sesamoid with rupture of the plantar plate leading to proximal migration of the proximal fragment of the lateral sesamoid and the medial sesamoid. Rodeo SA, et al: Diastasis of bipartite sesamoids of the first metatarsophalangeal joint. Foot Ankle 1993;l4:425-434.
References:
- Rodeo SA, O'Brien S, Warren RF, et al: Turf toe: An analysis of metatarsal joint sprains in professional football players. Am J Sports Med 1990;18:280-285.
Question 87High Yield
A 47-year-old man ruptured his left patellar tendon and twisted his right ankle in a fall. Initial radiographs of the ankle are unremarkable. One week following repair of the left patellar tendon, he reports increased pain with weight bearing in his right ankle. A follow-up radiograph is shown in Figure 38. Management of the ankle injury should consist of
Explanation
Explanation
The radiograph reveals disruption of the syndesmosis with lateral displacement of the talus and widening of the medial ankle clear space. No fibular fracture is noted, although radiographs of the entire tibia and fibula are necessary to rule out a more proximal fibula fracture. There is clear instability of the syndesmosis, and surgical stabilization is needed, either by direct repair of the ligaments or more commonly with surgical stabilization of the fibula to the tibia with screws. Functional rehabilitation and early range of motion are indicated with anterior-lateral ankle sprains but not with true instability of the syndesmosis. In anterior syndesmotic injuries in which there are no signs of instability on plain radiographs or with stressing, cast immobilization and protected weight bearing until tenderness subsides is warranted. Long leg cast immobilization is unlikely to be adequate in maintaining reduction of the syndesmosis. Repair of the talofibular ligaments or fibular osteotomy does not address the pathology at the syndesmosis. Chronic syndesmotic disruption is likely to lead to chronic ankle pain and early arthrosis. Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
References:
- Edwards GS Jr, DeLee JC: Ankle diastasis without fracture. Foot Ankle 1984;4:305-312.
Question 88High Yield
What is the most appropriate indication for replantation in an otherwise healthy 35-year-old man?
Explanation
Vascular anastamoses are exceedingly difficult with amputations distal to the nail fold as the digital vessels bifurcate or trifurcate at this level, and little functional benefit is gained compared to other means of soft-tissue coverage. Single digit amputations, other than the thumb, are a relative contraindication for replantation. Replantations at the level of the proximal phalanx lead to poor motion of the proximal interphalangeal joint. In a healthy active adult, an amputation through the wrist is an appropriate situation to proceed with a replantation. A transverse forearm amputation is a good indication with a warm ischemia time of less than 6 hours. Urbaniak JR: Replantation, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1085.
Question 89High Yield
What vessel is marked with an asterisk in Figure 44?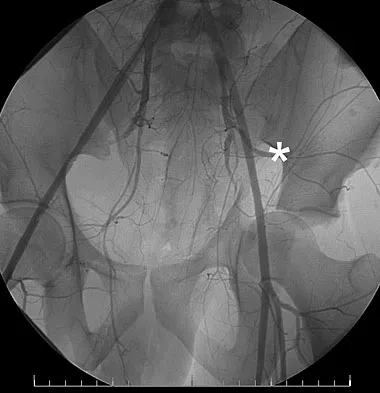
Explanation
The superior gluteal artery is a branch of the posterior division of the internal iliac artery and exits the pelvis through the greater sciatic notch. It can be injured as a result of a pelvic ring fracture or acetabular fracture that has a fracture of the posterior column. Agur AM, Dalley AF (eds): Grant's Atlas of Anatomy, ed 12. Philadelphia, PA, Lippincott Williams and Wilkins, 2008.
Question 90High Yield
Figure 15 shows the radiograph of an active 60-year-old woman. Which of the following variables is considered the strongest contraindication to a unicompartmental knee arthroplasty in this patient?
Explanation
Explanation
Unicompartmental arthroplasty of the knee for single compartment arthrosis has recently become more popular. Contraindications to unicompartmental knee arthroplasty include fixed varus or valgus deformity of more than 5 degrees, restricted range of motion, fixed flexion contracture, joint subluxation of 5 mm or greater, and arthrosis of the opposite and/or patellofemoral compartment. Cossey AJ, Spriggins AJ: The use of computer-assisted surgical navigation to prevent malalignment in unicompartmental knee arthroplasty. J Arthroplasty 2005;20:29-34. Iorio R, Healy WL: Unicompartmental arthritis of the knee. J Bone Joint Surg Am 2003;85:1351-1364.
References:
- Argenson JN, Chevrol-Benkeddache Y, Aubaniac JM: Modern unicompartmental knee arthroplasty with cement: A three to ten-year follow-up study. J Bone Joint Surg Am 2002;84:2235-2239.
Question 91High Yield
Which of the following accurately describes the biosynthetic materials tricalcium phosphate (TCP) and hydroxyapatite?
Explanation
Explanation
TCP is resorbed more rapidly, at a rate of 10 to 20 times faster than hydroxyapatite, partially because its larger pore size makes it a weaker substance. It provides significantly less compressive strength than hydroxyapatite. It does partially convert to hydroxyapatite, thus slowing its resorption rate. The absorbing cell of hydroxyapatite is the foreign body giant cell, not the osteoclast. Optimum pore size appears to be between 150 and 500 um. Lane JM, Bostrom MP: Bone grafting and new composite biosynthetic graft materials. Instr Course Lect 1998;47:525-534.
References:
- Walsh WR, Chapman-Sheath PJ, Cain S, et al: A resorbable porous ceramic composite bone graft substitute in a rabbit metaphyseal defect model. J Orthop Res 2003;21:655-661.
Question 92High Yield
Figures 61a and 61b show the CT and MRI scans of a 40-year-old man who has hip pain. He undergoes total hip arthroplasty and curettage and cementation of the lesion as shown in Figure 61c. Histopathologic photomicrographs of the curettage specimen are shown in Figures 61d and 61e. What is the best course of treatment?
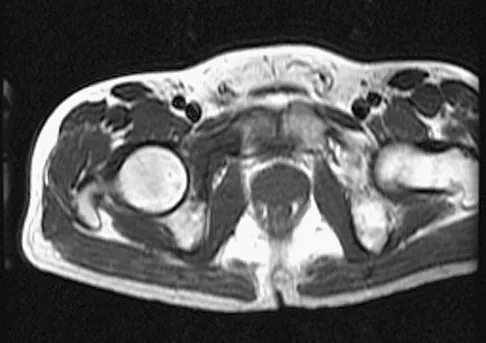

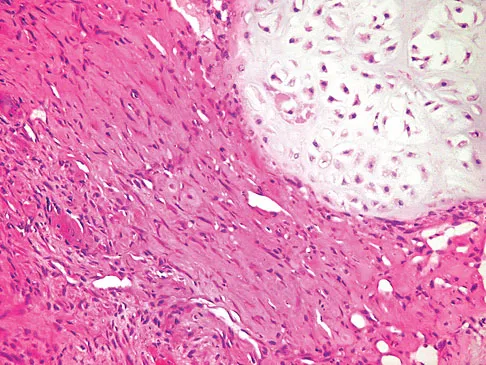
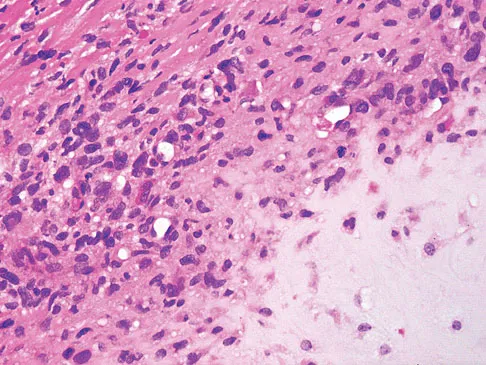
Explanation
The definitive surgery would be removal of the entire resection bed, and in this case of dedifferentiated chondrosarcoma, a hemipelvectomy was performed. The MRI and CT scans show an aggressive cartilage lesion. The histology, representative of a dedifferentiated chondrosarcoma, shows a bimorphic low-grade cartilage lesion with high-grade spindle cell sarcoma. The cartilage lesion is usually an enchondroma or low-grade chondrosarcoma. The dedifferentiated portion is typically a malignant fibrous histocytoma, osteosarcoma, or fibrosarcoma. Weber KL, Pring ME, Sim FH: Treatment and outcome of recurrent pelvic chondrosarcoma. Clin Orthop Relat Res 2002;397:19-28.
Question 93High Yield
An 18-month-old child sustains a crush amputation of the tip of the index finger. Bone is exposed, but the nail is intact. Management should consist of
Explanation
Children have a much greater capacity to heal soft-tissue injuries than adults. Most crush or avulsion fingertip amputations in children, particularly those younger than age 2 years, can be treated with serial dressing changes, even with bone exposed. Das SK, Brown HG: Management of lost finger tips in children. Hand 1978;10:16-27.
Question 94High Yield
A 55-year-old woman with type I diabetes mellitus has a chronic ulcer over the dorsum of her right foot and reports forefoot pain. Examination reveals 1- x 2-cm nondraining ulcer over the dorsum of the foot. The patient has 1-2+ pain with compression of the foot and ankle. She has a weakly palpable posterior tibial pulse and an absent dorsalis pedis pulse. There is no erythema, cellulitis, or drainage. Radiographs are normal. Which of the following diagnostic studies should be obtained?
Explanation
The presence of a dorsal ulcer in the presence of weak or absent pulses strongly suggests the possibility of arterial insufficiency. The best initial noninvasive study to assess for ischemia is the Doppler arterial study. A determination of the vascular status is of a greater priority than an assessment for infection or neuropathy because of the location and presentation of the ulcer. If ankle pressures are less than 45 mm Hg, there is a high risk that these lesions will not heal without revascularization. Wagner FW Jr: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981;2:64-122.
Question 95High Yield
In Figure 2, which of the following structures is the primary stabilizer in preventing valgus instability of the elbow?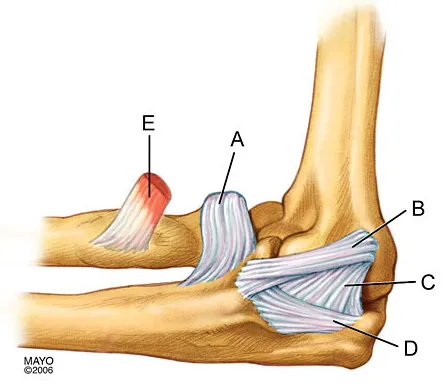
Explanation
The anterior bundle of the medial collateral ligament is the prime stabilizer of the medial aspect of the elbow and is indicated by "B" in the figure. When intact, this anterior bundle of the medial collateral ligament is a restraint to valgus instability of the elbow. The posterior bundle is regarded as a secondary stabilizer of the medial elbow (C). The transverse bundle (D), annular ligament (A), and biceps tendon (E) do not play a role in valgus stability of the elbow. Jobe F, Elattrache N: Diagnosis and treatment of ulnar collateral ligament injuries in athletes, in Morrey B (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1993, p 566.
Question 96High Yield
A 32-year-old motorcycle rider is involved in a motor vehicle accident and radiographs show a burst fracture at L2 with 20 degrees of kyphosis. The neurologic examination is consistent with unilateral motor and sensory involvement of the L5, S1, S2, S3, and S4 nerve roots. He has no other injuries. CT demonstrates 20% anterior canal compromise with displaced laminar fractures at the level of injury. What is the best option for management of this patient?
Explanation
The patient has a burst fracture with probable unilateral entrapment of the cauda equina within the elements of the fractured lamina. A dural tear is likely in this scenario as well. It is recommended that this type of burst fracture be treated surgically with laminectomy, freeing of the entrapped nerve roots, and dural repair followed by stabilization of the fracture by either a posterior or combined approach. The degree of kyphosis and the extent of anterior canal compromise does not warrant corpectomy in this patient. Therefore, after completing the laminectomy and dural repair, posterior fusion and instrumentation should be sufficient to stabilize the fracture. Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Question 97High Yield
Resuscitation of a trauma patient who has been in hypovolemic shock is complete when which of the following has occurred?
Explanation
Shock can be defined as inadequate tissue perfusion. Resuscitation or the resolution of shock is defined as when oxygen debt has been repaid, tissue acidosis is eliminated, and aerobic metabolism has been restored in all tissue beds. The end points for resuscitation are not clearly defined, but occult shock can still be present in the setting of normal vital signs and normal urine output due to selective perfusion of organ systems. Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: End point of resuscitation. J Trauma 2004;57:898-912. Moore FA, McKinley BA, Moore EE, et al: Inflammation and the Host Response to Injury, a large-scale collaborative project: Patient-oriented research core--standard operating procedures for clinical care. III. Guidelines for shock resuscitation. J Trauma 2006;61:82-89.
Question 98High Yield
What inflammatory mediator has been most closely associated with the magnitude of the systemic inflammatory response to trauma and with the development of multiple organ dysfunction syndrome (MODS)?
Explanation
Explanation
Multiple cytokines (inflammatory mediators) are released following trauma, and their levels can be measured in serum. Persistent elevated levels of IL-6 (> 800 pg/mL) indicate an exaggerated systemic inflammatory response to trauma and have been associated with the development of MODS. Recent work has shown that extensive surgical procedures should be avoided when IL-6 levels remain elevated to prevent the precipitation of MODS. In the future, it is likely that this mediator and possibly others will be used to determine timing and techniques of future treatment. Patrick DA, Moore FA, Moore EE, et al: Jack A. Barney Resident Research Award winner: The inflammatory profile of interleukin-6, interleukin-8, and soluble intercellular adhesion molecule-1 in postinjury multiple organ failure. Am J Surg 1996;172:425-429. Pape HC, van Griesven M, Rice J, et al: Major secondary surgery in blunt trauma patients and perioperative cytokine liberation: Determination of the clinical relevance of biochemical markers. J Trauma 2001;50:989-1000.
References:
- Giannoudis PV: When is the safest time to undertake secondary definitive fracture stabilization procedures in multiply injured patients who were initially managed using a strategy of primary temporary skeletal fixation. J Trauma 2002;52:811-812.
Question 99High Yield
What region of the spine is most susceptible to changes in the vascular supply to the spinal cord during an anterior approach?
Explanation
The thoracic spinal cord is characterized by a variable and, at times, complicated blood supply. The artery of Adamkiewicz, also known as the great anterior medullary artery, most typically arises off the left side of the aorta between T8 and T12. It represents the sole medullary blood supply to the thoracic spine. When this artery is divided or injured, the blood supply to the thoracic cord may be interrupted. It is important to avoid electocautery of blood vessels within or near the thoracic foramen because this is a site of important, albeit limited, collateral circulation. Sharma M, Anderson FC: Spinal vascular lesions, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 301-306.
Question 100High Yield
An infant is born with a mass that involves both the volar and dorsal compartments of the left arm. A clinical photograph and biopsy specimen are shown in Figures 41a and 41b. What is the best initial course of action?
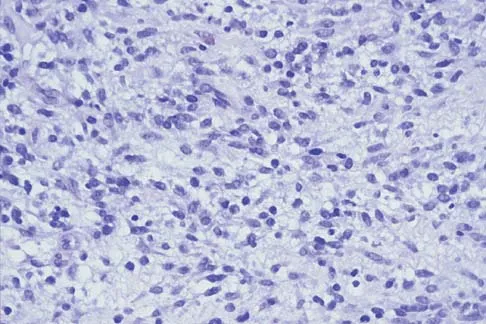
Explanation
The patient has infantile fibrosarcoma. For unresectable lesions, the treatment of choice is chemotherapy with vincristine, actinomycin-D, and cyclophosphamide, followed by excision if there is an adequate decrease in the size of the lesion.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon