Orthopedic Surgery Board Review: 100 High-Yield MCQs (Set 348)
14 Apr 2026
99 min read
121 Views
Key Takeaway
Prepare for ABOS, OITE, and FRCS exams with 100 high-yield Orthopedic Surgery MCQs. This mock exam, Set #348, helps surgeons test their knowledge, identify weaknesses, and master critical concepts for board success. Enhance your orthopedic board review.
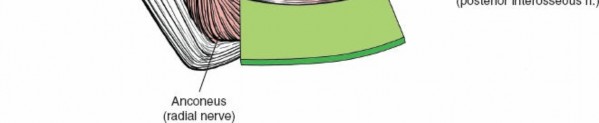
Mastering the Posterolateral Approach to the ...
00:00
Start Quiz
Question 1High Yield
A 30-year-old man caught his dominant little finger on the straps of his windsurfing board 10 days ago. He reports swelling about the distal phalanx and has difficulty completely extending the distal interphalangeal joint. A radiograph is shown in Figure 47. What is the most appropriate treatment for this injury?
Explanation
The radiograph reveals a "bony mallet injury." As the distal phalanx is not volarly subluxated, extension splinting, similar to a classic mallet injury without bony involvement, is appropriate. If there is volar subluxation associated with a large bony fragment, surgical intervention is appropriate. Baratz ME, Schmidt CC, Hughes TB: Extensor tendon injuries, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green's Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 192.
Question 2High Yield
A newborn with myelomeningocele has no movement below the waist and has bilateral hips that dislocate with provocative flexion and adduction. What is the best treatment option for the hip instability?
Explanation
Explanation
The status of the hips (located or dislocated) in children with thoracic-level myelomeningocele has no effect on the functional outcome of these patients. Management of unstable hips in this population should be limited to treatment of the contractures that may lead to poor limb positioning in either braces or a wheelchair. The use of the Pavlik harness and/or spica cast is contraindicated because they would promote flexion and abduction contractures. In the past, open reduction either through an anterior or medial approach had been performed with a high incidence of redislocation and other complications, with little functional gain for the child. Gabriel KG: Natural history of hip deformity in spina bifida, in Sarwark JR, Lubicky JP (eds): Caring for the Child With Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 89-103.
References:
- Schoenecker PL: Surgical management of hip problems in children with myelomeningocele, in Sarwark KR, Lubicky JP (eds): Caring for the Child With Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 117-131.
Question 3High Yield
Which of the following findings is a contraindication to isolated percutaneous pinning of a distal radius fracture?
Explanation
Intrafocal pinning allows the Kirschner wires to be placed through a site of comminution and then drilled through intact cortex. Generally Kapandji intrafocal pinning is done for dorsal comminuted extra-articular dorsal bending fractures, but it also may be used to elevate and buttress radial comminution. Simple intra-articular fractures can also be treated with pinning alone. Intrafocal pinning works best as a dorsal or radial buttress to prevent shortening. When there is volar comminution, the fracture is prone to shortening and supplemental external fixation or plating is recommended. Trumble TE, Wagner W, Hanel DP, et al: Intrafocal (Kapandji) pinning of distal radius fractures with and without external fixation. J Hand Surg Am 1998;23:381-394. Choi KY, Chan WS, Lam TP, et al: Percutaneous Kirschner-wire pinning for severely displaced distal radial fractures in children: A report of 157 cases. J Bone Joint Surg Br 1995;77:797-801.
Question 4High Yield
A 24-year-old dancer sustains the injury shown in Figure 28. Management should consist of
Explanation
The patient has a moderately displaced distal diaphyseal fracture of the fifth metatarsal, and the most appropriate treatment is brief immobilization and symptomatic management. Attempts at closed reduction are unlikely to appreciably alter the position of the fracture. Surgical techniques for either reduction of the fracture or fixation have not been shown to result in improved functional outcomes. O'Malley MJ, Hamilton WG, Munyak J: Fractures of the distal shaft of the fifth metatarsal: "Dancer's Fracture." Am J Sports Med 1996;24:240-243. DeLee JC: Fractures and dislocations of the foot, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 1465-1703.
Question 5High Yield
An 18-month-old boy has 45 degrees of kyphosis in the thoracolumbar spine secondary to type I congenital kyphosis. Examination reveals that he is neurologically intact, and an MRI scan shows no evidence of intraspinal pathology. Management should consist of
Explanation
Explanation
Surgery is indicated for congenital kyphosis once the deformity reaches a certain size or if significant progression is documented. In a young patient with a relatively small deformity, the treatment of choice is isolated in situ posterior fusion and postoperative immobilization. If an adequate posterior fusion can be obtained, an epiphyseodesis effect can be generated, allowing the remaining anterior growth to cause some correction. Because there is no evidence of neurologic compression and the deformity is less than 50 degrees, anterior surgery is not indicated. There is no role for bracing in the management of congenital kyphosis. Winter RB: Congenital Deformities of the Spine. New York, NY, Thieme-Stratton, 1983, pp 229-261.
References:
- Winter RB, Moe JH: The results of spinal arthrodesis for congenital spinal deformity in patients younger than five years old. J Bone Joint Surg Am 1982;64:419-432.
Question 6High Yield
What is the most common complication following total disk arthroplasty in the lumbar spine?
Explanation
Explanation
In a midterm (7 to 11 years) follow-up study of lumbar total disk arthroplasty, 5 of 55 patients had transient radicular leg pain without evidence of nerve root compression. Implant migration is rare. Deep venous thrombosis, incisional hernia, and retrograde ejaculation are less common complications of disk arthroplasty.
References:
- Tropiano P, Huang RC, Girardi FP, et al: Lumbar total disc replacement: Seven to eleven-year follow-up. J Bone Joint Surg Am 2005;87:490-496.
Question 7High Yield
A 45-year-old man sustains a low-velocity gunshot wound to the base of the right thumb. The open wound is allowed to heal by secondary intention, resulting in a contracture of the first web space. Clinical photographs are shown in Figures 49a through 49c. Treatment should now consist of


Explanation
The contracture is too large for a Z-plasty, which allows a 75% increase in length. Excision of the scar with placement of a skin graft is prone to contracture. A posterior interosseous fasciocutaneous flap will provide enough well-vascularized tissue and is well suited to reach the first dorsal web space. Buchler U, Frey HP: Retrograde posterior interosseous flap. J Hand Surg Am 1991;16:283-292.
Question 8High Yield
Which of the following methods of meniscal repair has the highest load to failure strength?
Explanation
Explanation
Numerous experimental studies have shown that vertical suture techniques are superior to all of the other noted methods. In fact, vertical sutures have been shown to be twice as strong as several of these techniques. DeHaven KE: Meniscus repair. Am J Sports Med 1999;27:242-250. Dervin GF, Downing KJ, Keene GC, McBride DG: Failure strengths of suture versus biodegradable arrow for meniscal repair: An in vitro study. Arthroscopy 1997;13:296-300.
References:
- Barber FA: Endoscopic meniscal repair: The T-fix technique. Sports Med Arthroscopy Rev 1999;7:28-33.
Question 9High Yield
A 7-year-old boy sustained an acute puncture wound of the foot after stepping barefoot on a piece of glass 1 day ago. His mother states that she is not sure if she got the piece of glass out; however, she reports that his immunizations are up-to-date. Examination reveals that the wound is slightly erythematous, less than 1 mm in length on the heel, and is not currently draining. What is the next most appropriate step im management?
Explanation
The child has an up-to-date tetanus; therefore, a booster is not recommended. Pseudomonas coverage is most likely not needed because the child was barefoot. It is too early to evaluate for abscess or osteomyelitis with MRI, and a formal debridement is rarely indicated without signs of an abscess or a retained foreign body. Radiographs with soft-tissue penetration should be obtained to check for a retained foreign body. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 199-205.
Question 10High Yield
A 68-year-old man reports a 4-week history of progressive left-sided lower back and hip pain. The pain is in the posterior buttock region with radiation to the groin and to the left anterior knee region. The pain is aggravated with walking and improves with rest. There is no history of previous trauma. Radiographs are seen in Figures 14a and 14b, and MRI scans are seen in Figures 14c through 14e. What is the most appropriate treatment option at this time?
Explanation
Explanation
14b 14c 14d 14e Although the imaging reveals generalized lumbar spondylosis and stenosis, in particular at L4-5, the MRI scan of the left hip clearly reveals a stress fracture of the femoral neck. Therefore, the treatment of choice is non-weight-bearing of the left lower extremity. During the evaluation of acute back pain, clinicians must include other possibilities within the differential diagnosis that may mimic mechanical axial back pain; thus, potential complications from a missed diagnosis can be avoided. Wong DA, Transfeldt E: Macnab's Backache, ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2007, pp 339-361.
Question 11High Yield
A 22-year-old college quarterback is tackled and sustains a reducible first carpometacarpal dislocation. What is the recommended treatment?
Explanation
When comparing closed reduction and pinning to ligament reconstruction, the reconstruction group had slightly better abduction and pinch strength. The volar oblique ligament usually tears off the first metacarpal in a subperiosteal fashion. In this young patient, motion-sparing procedures are preferred. Simonian PT, Trumble TE: Traumatic dislocation of the thumb carpometacarpal joint: Early ligamentous reconstruction versus closed reduction and pinning. J Hand Surg Am 1996;21;802-806.
Question 12High Yield
Which of the following structures may help maintain radial length after a radial head fracture?
Explanation
Explanation
Essex-Lopresti injuries affect axial stability of the forearm. Injury to the interosseous membrane or the triangular fibrocartilage complex can result in proximal migration of the radius. Morrey BF, Chao EY, Hui FC: Biomechanical study of the elbow following excision of the radial head. J Bone Joint Surg Am 1979;61:63-68.
References:
- Coleman DA, Blair WF, Shurr D: Resection of the radial head for fracture of the radial head: Long-term follow-up of seventeen cases. J Bone Joint Surg Am 1987;69:385-392.
Question 13High Yield
What neurovascular structure is most at risk when performing an inside-out repair of the posterior horn of the medial meniscus?
Explanation
The saphenous nerve is located on the posterior medial aspect of the knee and must be protected when performing an inside-out repair of the medial meniscus. The peroneal nerve is most at risk with lateral meniscal repairs. The other structures usually are not at risk with meniscal repair. Cannon WD Jr, Morgan CD: Meniscal repair: Arthroscopic repair techniques. Instr Course Lect 1994;43:77-96.
Question 14High Yield
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5 degrees of angulation. When the MCP joint is flexed 30 degrees, a radially directed stress produces 45 degrees of angulation. Radiographs are otherwise normal. Management should consist of
Explanation
Injuries to the ulnar collateral ligament of the MCP joint of the thumb commonly occur in recreational skiers. Historically, this injury has been referred to as "gamekeeper's thumb." The ligament consists of the proper collateral ligament and the more volar accessory collateral ligament. In extension, the accessory ligament is taut, and in flexion, the proper ligament is taut. For a complete tear of the ligament complex to occur, there must be laxity in full extension. Incomplete tears respond well to thumb spica splinting or casting for 2 to 3 weeks and gradual resumption of range of motion. Prolonged immobilization of incomplete injuries leads to higher rates of MCP joint stiffness. Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Question 15High Yield
A 65-year-old man has a painful mass of the middle finger. A clinical photograph, lateral radiograph, coronal MRI scan, and biopsy specimen are seen in Figures 20a through 20d. What is the most likely diagnosis?



Explanation
Although the degeneration of an isolated benign cartilaginous lesion into a chondrosarcoma is rare, it occurs in roughly 10% of patients with Ollier's disease. Pain is the most common symptom of chondrosarcoma. The treatment of low-grade chondrosarcoma ranges from intralesional excision to wide amputation. The intent of the surgery is to remove all the disease to decrease the chance of local recurrence. Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome. J Bone Joint Surg Am 1999;81:326-338.
Question 16High Yield
An obese patient undergoing total knee arthroplasty is at increased risk for which of the following complications?
Explanation
Explanation
The rate of wound complications is significantly increased after total knee arthroplasty in obese patients. Knee scores and the rate of aseptic loosening or patellar subluxation do not appear to be significantly altered. Winiarsky R, Barth P, Lotke P: Total knee arthroplasty in morbidly obese patients. J Bone Joint Surg Am 1998;80:1770-1774. Stern SH, Insall JN: Total knee arthroplasty in obese patients. J Bone Joint Surg Am 1990;72:1400-1404.
References:
- Griffin FM, Scuderi GR, Insall JN, Colizza W: Total knee arthroplasty in patients who were obese with 10 years follow-up. Clin Orthop 1998;356:28-33.
Question 17High Yield
A 37-year-old electrician is diagnosed with a frozen shoulder after sustaining an electrical injury at work 2 weeks ago. Examination reveals that he cannot actively or passively externally rotate or abduct the arm. The glenohumeral joint and scapula move in a 1:1 ratio. Radiographs are shown in Figures 15a and 15b. The best course of action should be

Explanation
The patient's history, examination, and radiographs are classic for locked posterior dislocation of the glenohumeral joint. Posterior dislocation of the shoulder remains the most commonly missed dislocation of a major joint. Up to 80% are missed on initial presentation. The primary cause for failure to accurately diagnose this injury is inadequate radiographic evaluation. The typical presentation is a shoulder locked in internal rotation with loss of abduction. An axillary view not only will make the definitive diagnosis but will help assess the size of the articular surface defect and help plan treatment. This view can be done expediently as part of every trauma series. The AP view is suspicious for a posteriorly dislocated humerus with loss of the humeral neck profile, a vacant glenoid sign, and an anterior humeral head compression fracture (reverse Hill-Sachs lesion). Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosement, IL, American Academy of Orthopaedic Surgeons, 1997, pp 181-189.
Question 18High Yield
Figure 16 shows the MRI scan of a 43-year-old man who has had worsening low back pain for the past 4 months. What is the most likely diagnosis?
Explanation
Explanation
Tuberculosis of the spine is seen in 50% to 60% of skeletal disease and is most commonly found in the lower thoracic or upper lumbar spine. Typically two or more adjacent bodies are involved as seen in this MRI scan. The disk space is narrowed but still relatively preserved as opposed to pyogenic infections (black arrow). Epidural extensions often spread from vertebrae to vertebrae (white arrow); however, the posterior elements are not frequently involved (arrowhead). Tumors rarely spread to adjacent vertebrae. The anterior and posterior spread of the infectious process rules out trauma. Boachie-Adjei O, Squillante RG: Tuberculosis of the spine. Orthop Clin North Am 1996;27:95-103.
Question 19High Yield
What is the most common malignant bone tumor seen in patients with multiple hereditary exostosis?
Explanation
Explanation
Secondary chondrosarcomas are most common in patients with multiple hereditary exostosis. Dedifferentiated chondrosarcoma is less common and refers to bone lesions in which a high-grade spindle cell sarcoma component is located immediately adjacent to a low-grade cartilage neoplasm. Mesenchymal chondrosarcoma, clear cell chondrosarcoma, and periosteal osteosarcoma are no more common in patients with multiple hereditary exostosis than in the general population. Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 1660-1669.
References:
- Simon MA, Springfield DS, et al: Common Malignant Bone Tumors: Chondrosarcoma. Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 275-286.
Question 20High Yield
Which of the following is considered an inherent problem in using the distal oblique shortening (Weil) metatarsal osteotomy for dorsal metatarsophalangeal subluxation?
Explanation
The distal oblique shortening (Weil) metatarsal osteotomy has not been associated with transfer lesions to the extent of other shortening osteotomies, and malunions and nonunions are unusual complications. Recurrent dorsal contracture of the toe has been reported. Recommendations to reduce this problem include release of the dorsal capsule and tendons, as well as a flexor tendon transfer. A potential cause suspected for this phenomenon is the relatively dorsal positioning of the intrinsic tendons after plantar displacement of the metatarsal head. Trnka HJ, Nyska M, Parks BG, Myerson MS: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int 2001;22:47-50. Trnka HJ, Muhlbauer M, Zettl R, Myerson MS, Ritschl P: Comparison of the results of the Weil and Helal osteotomies for the treatment of metatarsalgia secondary to dislocation of the lesser metatarsophalangeal joints. Foot Ankle Int 1999;20:72-79.
Question 21High Yield
During the evaluation of a patient suspected of having a lumbar disk herniation, T1- and T2-weighted MRI scans reveal a hyperintence lobular, well-defined lesion in the L2 vertebral body. What is the most likely diagnosis?
Explanation
The findings are characteristic of hemangioma. When the hemangioma is large enough, vertical striations may be visible on plain radiographs. Axial CT scans commonly reveal a speckled appearance. Metastatic lesions are typically hypointense on T1-weighted images because they replace the fatty marrow. Bony islands, like cortical bone, are dark on T1- and T2-weighted images. Intravertebral disk herniation would have characteristics similar to the disk and be in continuity with the disk. Osteoporosis is more diffuse. Ross JS, Masaryk TJ, Modic MT, Carter JR, Mapstone T, Dengel FH: Vertebral hemangiomas: MR imaging. Radiology 1987;165:165-169.
Question 22High Yield
A football player sustains a traumatic anterior inferior dislocation of the shoulder in the last game of the season. It is reduced 20 minutes later in the locker room. The patient is neurologically intact and has regained motion. If the patient undergoes arthroscopic evaluation, what finding is seen most consistently?
Explanation
Explanation
In an acute first-time dislocation, arthroscopy has been shown to reveal a Bankart lesion in most shoulders. The classic finding of labral detachment from the anterior inferior glenoid along with occasional hemorrhage within the inferior glenohumeral ligament is the most common sequelae of a traumatic anterior inferior dislocation. Acute treatment, if chosen, is repair of the labral tissue back to the glenoid plus or minus any capsular plication to address potential plastic deformation of the glenohumeral ligament. Acute treatment of a patient sustaining a first-time dislocation remains controversial. The potential indications may be patients whose dislocation occurs at the end of a season and when the desire to minimize risk of future instability outweighs the risks of surgical intervention. Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311. DeBerardino TM, Arciero RA, Taylor DC, et al: Prospective evaluation of arthroscopic stabilization of acute, initial anterior shoulder dislocations in young athletes: Two- to five-year follow-up. Am J Sports Med 2001;29:586-592.
References:
- Bottoni CR, Wilckens JH, DeBerardino TM, et al: A prospective, randomized evaluation of arthroscopic stabilization versus nonoperative treatment in patients with acute, traumatic, first-time shoulder dislocations. Am J Sports Med 2002;30:576-580.
Question 23High Yield
Figure 22 shows the radiographs of a 16-year-old boy who injured his elbow in a fall 1 year ago. Although he has no pain, he reports restricted forearm rotation and elbow flexion. What is the most likely diagnosis?
Explanation
Congenital dislocation of the radial head is often confused with posttraumatic dislocation. The distinguishing feature here is the dome-shaped radial head. Some patients with congenital anomalies fail to recognize their limitations until an injury occurs. Soft-tissue contractures do not cause radial head dislocation nor do they usually cause this pattern of motion restriction (mainly flexion and rotation without significant loss of extension). There is no deformity of the ulna to suggest an old Monteggia lesion. Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 196.
Question 24High Yield
A 20-year-old professional baseball pitcher has had a 3-year history of increased aching in his shoulder that is associated with pitching, and he is now seeking a second opinion. Nonsurgical management consisting of rest, anti-inflammatory drugs, ice, heat, and cortisone injections has failed to provide relief. A previous work-up that included radiographs and gadolinium-enhanced MRI arthrography was negative. Results of an arteriogram suggest quadrilateral space syndrome. Assuming that this is the correct diagnosis, what nerve needs to be decompressed?
Explanation
Quadrilateral space syndrome is a rare condition and is the result of compression of the contents of the quadrilateral space. The contents of the quadrilateral space include the posterior circumflex vessels and the axillary nerve. Cahill BR, Palmer RE: Quadrilateral space syndrome. J Hand Surg 1983;8:65-69.
Question 25High Yield
The anatomy of the sciatic nerve as it exits the pelvis is best described as exiting through the
Explanation
The sciatic nerve is formed by the roots of the lumbosacral plexus. It exits the pelvis through the greater sciatic notch and appears in the buttock anterior to the piriformus. From that point, the sciatic nerve passes posteriorly over the superior gemellus, obturator internus, inferior gemellus, and quadratus femoris before it passes deep to the biceps femoris. The tendon of the obturator internus passes through the lesser sciatic notch. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 347. Anderson JE: Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-34, 4-36.
Question 26High Yield
An 11-year-old girl has had pain in the medial arch of her foot for the past 3 months. She reports that pain is present even with daily activities such as walking to class at school, and ibuprofen provides some relief. She denies any history of trauma. Examination reveals a flexible pes planus with focal tenderness over a prominent tarsal navicular tuberosity. Radiographs show a prominent accessory navicular. Management should consist of
Explanation
Explanation
The patient has the classic symptoms, examination findings, and radiographs for a painful accessory navicular. Initial treatment should always be nonsurgical, specifically cast immobilization. Surgery should be reserved for those patients who fail nonsurgical management. Corticosteroids should not be injected into a posterior tibial tendon or insertion point because they can weaken the tendon and possibly cause tendon rupture. Triple arthrodesis and biopsy have no role in the management of a painful accessory navicular.
References:
- Bordelon RL: Flatfoot in children and young adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 717-756.
Question 27High Yield
A 15-year-old girl reports a 6-month history of activity-related knee pain and swelling. A radiograph, MRI scan, and biopsy specimen are shown in Figures 21a through 21c. What is the most likely diagnosis?

Explanation
The epiphyseal location on the radiograph and MRI scan and the histologic findings of polyhedral cells separated by a chondroid matrix with pericellular, lattice-like "chicken wire" calcification all suggest chondroblastoma. Although giant cell tumors of bone typically occupy an epiphyseal location, they are rare in children and when present are often metaphyseal in skeletally immature patients. Enchondromas and osteoblastomas are generally metaphyseal and, along with giant cell tumors, have very different histology than seen here. Chondromyxoid fibromas are typically metaphyseal in location. Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 295-313.
Question 28High Yield
A collegiate football player who sustained a blow to the head during the first quarter of a game is confused for several minutes after the hit but does not lose consciousness. He had two similar episodes in games earlier in the season. When should he be allowed to return to play?
Explanation
Using the traditional concussion grading scale, the patient sustained a grade I concussion because he did not lose consciousness and his abnormal cognitive level lasted less than 1 hour. If this was the player's first concussion, theoretically he could return to play later in the game provided that he had no confusion, headache, or associated symptoms. However, because it was the third concussion for the year, participation in contact sports should be terminated for the season. Guskiewwicz KM, Barth JT: Head injuries, in Schenk RC Jr (ed): Athletic Training and Sports Medicine. Rosemont, IL, American Academy of Orthopedic Surgeons, 1999, pp 143-167.
Question 29High Yield
A 58-year-old woman sustained a ruptured Achilles tendon 1 year ago, and management consisted of an ankle-foot orthosis. She now reports increasing difficulty with ambulation and increasing pain. An MRI scan shows a 6-cm defect in the right Achilles tendon. Management should now consist of
Explanation
With a gap of less than 4 cm, a V-Y repair would be appropriate without a tendon transfer. For gaps greater than 5 cm, a lengthening with augmentation is the most appropriate treatment. Therefore, the treatment of choice is an Achilles tendon turndown with flexor hallucis longus tendon transfer. The plantaris tendon is not a strong enough repair, and direct repair is not possible given the large defect in the Achilles tendon. Continued use of the ankle-foot orthosis will not provide adequate relief for this patient.
Question 30High Yield
During cemented total hip arthroplasty, peak pulmonary embolization of marrow contents occurs when the
Explanation
Peak embolization is observed during femoral stem insertion. Embolization is also observed during acetabular preparation and hip reduction. Lewallen DG, Parvizi J, Ereth MH: Perioperative mortality associated with hip and knee arthroplasty, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 119-127.
Question 31High Yield
A 40-year-old woman has local back pain and intense burning pain in her perianal region after being shot twice in the back. Motor and sensory examination of her lower extremities reveals no apparent deficit. She has present but decreased sensation in her perianal region, an intact anal wink, good rectal tone, and an intact bulbocavernosus reflex. Radiographs and CT scans are shown in Figures 3a through 3d. What is the next most appropriate step in management?
Explanation
Explanation
3b 3c 3d Because the patient has an apparent compressive neuropathy secondary to the metallic fragments, removal of the fragments in this incomplete lesion at the cauda equina level can be expected to improve her sensory dysesthesias and pain. Steroids are not indicated in a root lesion secondary to a penetrating injury. MRI will have significant artifact effect and will not provide much additional information. The posterior bony elements are not significantly injured; therefore, stabilization is not indicated. Bracken MB, Shepard MJ, Holford TR: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury. JAMA 1997;277:1597-1604. Waters RL, Adkins RH: The effects of removal of bullet fragments retained in the spinal canal: A collaborative study by the National Spinal Cord Injury Model Systems. Spine 1991;16:934-939.
References:
- Stauffer ES, Wood RW, Kelly EG: Gunshot wounds of the spine: The effects of laminectomy. J Bone Joint Surg Am 1979;61:389-392.
Question 32High Yield
What is the most appropriate orthotic management for the lesion shown in Figure 6?
Explanation
The figure shows an intractable plantar keratosis (IPK). The keratoma usually forms beneath a bony prominence. This can occur under the sesamoids, most commonly the tibial sesamoid, or under the fibular condyle of a prominent metatarsal head. The initial treatment of an IPK consists of paring down the callused lesion and placing a metatarsal pad proximal to the lesion to provide posting to unload the bony prominence.
Question 33High Yield
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by
Explanation
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by the use of a direct lateral approach to the ankle. The superficial peroneal nerve and its branches exit the fascial hiatus approximately 9 cm to 10 cm proximal to the tip of the distal fibula with a range of 4 cm to 13 cm, and their course is typically anterior to the midlateral plane of the fibula. However, small branches may course across the surgical plane directly laterally. A posterior-lateral approach diminishes the risk of injury to the superficial peroneal nerve and its branches; however, by moving farther posterior, the sural nerve and its branches may be at increased risk. Cast immobilization may injure the cutaneous nerves about the ankle; however, the risks are greater with surgical intervention. A medial or anterior-medial approach to the ankle will not injure the superficial peroneal nerve at the ankle level. Redfern DJ, Sauve PS, Sakellariou A: Investigation of incidence of superficial peroneal nerve injury following ankle fracture. Foot Ankle Int 2003;24:771-774.
Question 34High Yield
Ganglion cysts about the wrist most commonly arise from what structure?
Explanation
Ganglion cysts are the most common mass or mass-like lesions seen in the hand and wrist. They arise in a variety of locations, including synovial joints or tendon sheaths. The most common location is the dorsal/radial wrist arising from the dorsal scapholunate interosseous ligament.
Question 35High Yield
What is the most common malignancy involving the hand?
Explanation
Skin cancers far outnumber primary musculoskeletal malignancies of the hand and the most common of these is squamous cell carcinoma. Metatastic lung carcinoma, while classic for the carcinoma that metastasizes to the hand, does so at an extremely low rate. Fink JA, Akelman E: Nonmelanotic malignant skin tumors of the hand. Hand Clin 1995;11:255-264.
Question 36High Yield
When an acute infection of a total elbow arthroplasty is managed with irrigation and debridement, which of the following organisms is associated with the highest risk of persistent infection?
Explanation
Explanation
Salvage of a total elbow arthroplasty is possible with early aggressive management of acute infection (symptoms for less than 30 days) with serial irrigation and debridement and antibiotic bead placement. This form of treatment is indicated when there are no radiographic or intraoperative signs of loosening. However, successful treatment is largely dependent on the organism. Staphylococcus epidermidis is associated with persistent infection because it is an encapsulating organism, and it is best treated with implant removal and IV antibiotics. Yamaguchi K, Adams RA, Morrey BF: Infection after total elbow arthroplasty. J Bone Joint Surg Am 1998;80:481-491.
References:
- Schoifet SD, Morrey BF: Treatment of infection after total knee arthroplasty by debridement with retention of the components. J Bone Joint Surg Am 1990;72:1383-1390.
Question 37High Yield
Figure 43 shows the lateral radiograph of a 12-year-old boy with mild osteogenesis imperfecta who injured his left elbow after pushing his brother. Treatment should consist of
Explanation
The patient has a displaced fracture of the apophysis of the olecranon for which most authorities recommend surgical treatment. In older children, stability of the reduction may be achieved by the use of two parallel medullary Kirschner wires and a figure-of-8 tension band loop of either stainless steel wire or absorbable suture. The use of an absorbable suture does not require removal of the implant. Absorbable suture alone is best used in very young patients who have this type of injury. An intramedullary screw would pose an unnecessary risk of future growth disturbance. A displaced, isolated fracture of the apophysis of the olecranon is an unusual injury in a child. It has been suggested by several authors that children who have osteogenesis imperfecta may be especially prone to this injury. One study reported seven of these fractures occurring in five children who had the mild form of osteogenesis imperfecta (Sillence type IA). The authors of this study suggest that the diagnosis of osteogenesis imperfecta be considered in any child who has a displaced fracture of the apophysis of the olecranon, especially when the injury is associated with relatively minor trauma. Stott NS, Zionts LE: Displaced fractures of the apophysis of the olecranon in children who have osteogenesis imperfecta. J Bone Joint Surg Am 1993;75:1026-1033. Gaddy BC, Strecker WB, Schoenecker PL: Surgical treatment of displaced olecranon fractures in children. J Pediatr Orthop 1997;17:321-324.
Question 38High Yield
What is the most common location for localized pigmented villonodular synovitis (PVNS) to occur?
Explanation
Localized PVNS is a form of the disease in which synovial proliferation is restricted to one area of a joint and causes the formation of a small mass-like lesion. The true incidence of this is unknown but is probably less common than the diffuse form of the disease. PVNS presents as a usually painful discrete mass. The anterior compartment of the knee is the most common location. Tyler WK, Vidal AF, Williams RJ, et al: Pigmented villonodular synovitis. J Am Acad Orthop Surg 2006;14:376-385.
Question 39High Yield
Figures 14a and 14b show the clinical photographs of a patient who was stranded in a subzero region for several days. The photographs were taken the morning after arrival in the hospital. The patient is otherwise healthy and fit, and takes no medication. He has no clinical signs of sepsis. He reports burning pain and tingling in both feet. What is the best treatment?

Explanation
The patient has no clinical or observed signs of sepsis. The skin just proximal to the gangrenous tissue appears somewhat hyperemic and is clearly viable. These wounds should be managed much like burn wounds. Moist dressings should be used until the tissue clearly demarcates. Much of the insult may simply be superficial and only require late debridement. McAdams TR, Swenson DR, Miller RA: Frostbite: An orthopedic perspective. Am J Orthop 1999;28:21-26.
Question 40High Yield
A 32-year-old man has intense right hand and wrist pain, a deformed wrist, and numbness in his fingers after falling off his motorcycle. This is an isolated injury. Examination reveals a swollen wrist, normal capillary refill to all fingers, and limited flexion of all fingers. Radiographs are shown in Figures 21a and 21b. Neurologic examination of the hand will most likely reveal

Explanation
The patient has a perilunate dislocation. A volar dislocation of the lunate is often associated with median nerve dysfunction. This injury to the wrist is often overlooked because of its benign clinical appearance and the presence of other injuries, as it is caused by high-energy mechanisms. Ruby LK, Cassidy C: Fractures and dislocations of the carpus, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1297-1300.
Question 41High Yield
Which of the following forms of nonsurgical management is considered best for acute low back pain without radiculopathy?
Explanation
Explanation
Temporary bed rest (less than 4 days) with gradual resumption of activities can be efficacious. Epidural steroid injections may be indicated for acute low back pain with radiculopathy. Acupuncture, facet joint injections, or ligamentous (sclerosant) injections are not indicated. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, Appendix A15.
References:
- Helfgott SM: Sensible approach to low back pain. Bull Rheum Dis 2001;3:50.
Question 42High Yield
A 24-year-old runner who underwent an allograft reconstruction of the anterior cruciate ligament (ACL) 3 years ago now reports anterior knee pain. Examination reveals no swelling or effusion, and the patient has full motion. A Lachman test and a pivot-shift test are negative. Palpation reveals tenderness on the patellar tendon and at the inferior pole of the patella. AP and lateral radiographs are shown in Figures 41a and 41b. Management should consist of
Explanation
Explanation
41b The radiographs show tunnel enlargement, which is seen after ACL reconstruction, particularly with allografts. Occasionally, there will be formation of an associated subcutaneous pretibial cyst. It has been proposed that the tunnel enlargement and cyst are the result of incomplete incorporation of allograft tissues within the bone tunnels. There may be residual graft necrosis, allowing synovial fluid to be transmitted through the tunnel to collect in the pretibial area, manifesting as a synovial cyst. In the absence of cyst formation, the presence of tunnel enlargement does not appear to adversely affect the clinical outcome. Based on studies by Fahey and associates, continued tunnel expansion does not occur. Victoroff and associates report good results with curettage and bone grafting of the tibial tunnel if a pretibial cyst is present. Because this patient does not have a pretibial cyst, observation with activity modification is the preferred treatment. Fahey M, Indelicato PA: Bone tunnel enlargement after anterior cruciate ligament replacement. Am J Sports Med 1994;22:410-414.
References:
- Victoroff BN, Paulos L, Beck C, Goodfellow DB: Subcutaneous pretibial cyst formation associated with anterior cruciate ligament allografts: A report of four cases and literature review. Arthroscopy 1995;11:486-494.
Question 43High Yield
An excessively large radial styloidectomy poses a risk for wrist instability. What ligament is at greatest risk for injury?
Explanation
Explanation
The radioscaphocapitate ligament is the most radial of the extrinsic volar ligaments of the wrist. It has a mean attachment to the radius 4 mm from the tip of the radial styloid. Nakamura T, Cooney WP III, Lui WH, et al: Radial styloidectomy: A biomechanical study on the stability of the wrist joint. J Hand Surg Am 2001;26:85-93.
References:
- Siegel DB, Gelberman RH: Radial styloidectomy: An anatomical study with special reference to radiocarpal intracapsular ligamentous morphology. J Hand Surg Am 1991;16:40-44.
Question 44High Yield
A 65-year-old woman has nausea, vomiting, and abdominal distention after undergoing total knee arthroplasty 48 hours ago. An abdominal radiograph is shown in Figure 14. Associated risk factors for this disorder include
Explanation
Explanation
The prevalence of postoperative ileus associated with total joint arthroplasty has been reported to be as high as 3%. Metabolic abnormalities such as hypokalemia are believed to contribute to the onset of ileus and Ogilvie's syndrome (acute pseudo-obstruction of the colon). Prolonged bed rest also has been associated with the development of ileus and Ogilvie's syndrome. Untreated Ogilvie's syndrome can result in cecal perforation. Ileus usually is not accompanied by mechanical obstruction. Antibiotic administration and the type of anesthesia used have not been correlated with development of ileus. Administration of warfarin has been associated with elevated prothrombin time/partial thromboplastin time and international normalized ratio levels when ileus is managed with a nasogastric tube and suction. Metabolic imbalances must be corrected to reverse the ileus process. Iorio R, Healy WL, Appleby D: The association of excessive warfarin anticoagulation and postoperative ileus after total joint replacement surgery. J Arthroplasty 2000;15:220-223.
References:
- Clarke HD, Berry DJ, Larson DR: Acute pseudo-obstruction of the colon as a postoperative complication of hip arthroplasty. J Bone Joint Surg Am 1997;79:1642-1647.
Question 45High Yield
A 40-year-old man reports an enlarging soft-tissue mass in his right shoulder. Based on the MRI scan and biopsy specimens shown in Figures 40a through 40c, what is the most likely diagnosis?


Explanation
Nodular fasciitis is a pseudosarcomatous, self-limiting reactive process composed of fibroblasts and myofibroblasts. Most patients give a history of a rapidly growing mass that has been present for only a few weeks. Many have pain associated with the mass and can recall a specific traumatic event predating the presence of the lesion. It can occur at any age but is most commonly seen in adults who are 20 to 40 years of age. Histologically, the lesion is composed of predominantly plump, immature-appearing fibroblasts that bear a close resemblance to the fibroblasts found in granulation tissue. Characteristically, the fibroblasts are arranged in short, irregular bundles and fascicles and are adjacent to collagen and reticulin. The lesions can appear to be more myxoid or more fibrotic in nature and this correlates to the duration of symptoms. The lesions with a short duration of symptoms have a more myxoid appearance in contrast to those of longer duration characterized by hyaline fibrosis. Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss's Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 250-266.
Question 46High Yield
A 21-year-old man who underwent repair of a distal biceps tendon rupture using a two-incision approach 4 months ago now reports difficulty gaining rotation of his forearm. Figures 49a and 49b show the AP and lateral radiographs. What is the most likely cause of his problem?

Explanation
The radiographs show early ectopic bone formation originating between the ulna and the radius. The development of ectopic bone in this area following a two-incision approach for anatomic repair of the distal biceps tendon is thought to be related to exposure of the periosteum of the lateral ulna during surgery. This can be avoided by the use of a muscle-splitting incision between the extensor carpi ulnaris and common extensor muscles. Full pronation of the forearm allows for the necessary exposure of the radial tuberosity during the procedure and for fixation of the tendon at its maximal length. Morrey BF: Tendon injuries about the elbow, in Morrey BF (ed): The Elbow and Its Disorders, ed. 2. Philadelphia, PA, WB Saunders, 1993, pp 492-503.
Question 47High Yield
A 14-year-old football player has had right knee pain for the past 2 months; however, he denies any history of trauma. Examination shows an abductor lurch and increased external rotation of the right lower extremity. The best course of action should be to
Explanation
Explanation
Slipped capital femoral epiphysis is the most common pathology involving the hip in adolescents. While patients with acute slips may report severe pain and are unable to ambulate, those with chronic slips often have pain during ambulation, a limp, and increased external rotation of the hip. While 60% of the patients specifically report hip pain, the remainder have pain in the thigh or knee. The initial diagnostic study of choice is AP and frog-lateral radiographs of the pelvis; bilateral involvement is frequently seen. Boyer DW, Mickelson MR, Ponseti IV: Slipped capital femoral epiphysis: Long-term follow-up study of one hundred and twenty-one patients. J Bone Joint Surg Am 1981;63:85-95.
References:
- Stasikelis PJ, Sullivan CM, Philips WA, Polard JA: Slipped capital femoral epiphysis: Prediction of contralateral involvement. J Bone Joint Surg Am 1996;78:1149-1155.
Question 48High Yield
A 30-year-old woman sustained a nondisplaced unilateral facet fracture of C5 in a motor vehicle accident. She is neurologically intact and has no other injuries. Management should consist of
Explanation
The patient has a stable bony fracture that will heal with immobilization in a rigid collar. Flexion-extension radiographs may be obtained at 6 weeks to verify that there is no instability; mobilization may then be begun.
Question 49High Yield
What is the primary concern for arthrodesis of a failed infected total knee arthroplasty using internal fixation?
Explanation
Explanation
Arthrodesis of the failed infected total knee arthroplasty may be accomplished by external fixation, intramedullary rod fixation, and dual plates and screws. External fixation runs the risk of pin tract infection, although after its removal, there are no metal surfaces left in place. Intramedullary rods have been used successfully in the treatment of infected total knees, although they also leave metal within the region of the infection. The dual plate technique of knee fusion is useful in patients with rheumatoid arthritis who require fusion in the absence of infection because it provides good initial stability and avoids the use of external pins. However, in the face of infection, the large surface area of the screws and plates may serve as a site for bacteria to hide within a glycocalyx and make eradication of the infection almost impossible.
References:
- Windsor RE: Knee arthrodesis, in Insall JN, Windsor R, Kelly M, et al (eds): Surgery of the Knee. New York, NY, Churchill Livingstone, 1993, pp 1103-1116.
Question 50High Yield
What joint always remains uninvolved in all stages of scapholunate advanced collapse (SLAC) deformity of the wrist?
Explanation
The development of arthritis in SLAC wrist follows a consistent pattern. Beginning at the radial styloid to the scaphoid articulation, it progresses through the entire radioscaphoid joint and the midcarpal joint. In all stages, the radiolunate joint is spared, which is the basis for a scaphoid excision and four-corner fusion performed as a motion-sparing procedure for treatment of this condition. Wyrick JD: Proximal row carpectomy and intercarpal arthrodesis for the management of arthritis. J Am Acad Orthop Surg 2003;11:277-281. Watson HK, Ballett FL: The SLAC wrist: Scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg Am 1984;9:358-365.
Question 51High Yield
What is the heaviest weight that can be safely applied to the adult cervical spine via Gardner-Wells tong traction?
Explanation
Explanation
Cotler and associates reported on the use of awake skeletal traction to reduce facet fracture-dislocations in 24 patients. Seventeen patients required more than 50 pounds of traction (the "traditional" limit) to achieve reduction. More than 100 pounds of traction was safely used in one-third of the patients in this study. A cadaver study has supported the safe use of traction with weights in excess of 100 pounds. Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.
Question 52High Yield
The superior glenohumeral ligament primarily restrains
Explanation
Explanation
Several cutting studies have evaluated the primary static restraints and the role of the glenohumeral ligaments in providing static stability. With the arm at the side in adduction, the superior glenohumeral ligament and coracohumeral ligament are the primary restraints to inferior translation. The middle glenohumeral ligament functions with the arm in 45 degrees of abduction and resists anterior translation. The inferior glenohumeral ligament is the primary restraint to anterior translation at 90 degrees of abduction. Warner JJ, Deng XH, Warren RF, et al: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
References:
- Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy Orthopaedic Surgeons, 1994, pp 165-177.
Question 53High Yield
A 14-year-old boy reports pain in the distal thigh. He denies any history of trauma. Examination reveals tenderness and swelling of the distal thigh without effusion. A radiograph and CT scan are shown in Figures 10a and 10b. A biopsy specimen is shown in Figure 10c. Management should consist of
Explanation
Explanation
10b 10c Based on these findings, the patient has an aneurysmal bone cyst. Frequently, fluid-fluid levels can be detected on MRI or CT images. The histologic results show a lesion that consists of cavernous spaces filled with blood. The lining of the cavity contains spindle cells, multinucleated giant cells, and reactive bone. Curettage and bone grafting is the preferred treatment method. Without treatment, these lesions can become quite large and destructive. Radiation therapy is not recommended for resectable lesions. Chemotherapy is not required for these benign lesions. Simon MA, Springfield DS, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-200.
References:
- Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, p 232.
Question 54High Yield
An elite skier training for the Olympics sustains an isolated traumatic dislocation of the peroneal tendons that have spontaneously reduced. The games are 9 months away and the athlete does not want to miss them. Treatment should consist of
Explanation
Explanation
Most of these injuries occur in young, active patients. Success rates for nonsurgical management are only marginally better than 50%. The treatment of choice is early surgery for patients who desire a quick return to a sport or active lifestyle. Subluxation of the peroneal tendons leads to longitudinal tears over time. McLennan JG: Treatment of acute and chronic luxations of the peroneal tendons. Am J Sports Med 1980;8:432-436.
References:
- Krause JO, Brodsky JW: Peroneus brevis tendon tears: Pathophysiology, surgical reconstruction, and clinical results. Foot Ankle Int 1998;19:271-279.
Question 55High Yield
In an effort to reduce costs, a limited MRI sequence is planned to detect a possible occult hip fracture. What is the anticipated fracture signal?
Explanation
Explanation
At present, radiologists perform multiple MRI images to rule out all possible diagnoses. The ability to specify the anticipated changes on MRI should become more important as a means of reducing costs. MRI is sensitive to changes in free water (or hemorrhage) and thus this will appear dark on T1 and bright on T2. Miller MD: Review of Orthopaedics, ed 3. Philadelphia PA, WB Saunders, 2000, p 116.
References:
- Guanche CA, Kozin SH, Levy AS, et al: The use of MRI in the diagnosis of occult hip fractures in the elderly: A preliminary review. Orthopedics 1994;17:327-330.
Question 56High Yield
The modified Brostrom lateral ankle ligamentous reconstruction uses which of the following structures to provide supplementary stabilization?
Explanation
Explanation
The modified Brostrom lateral ankle ligament stabilization procedure uses the remnants of the anterior talofibular and the calcaneofibular ligaments, supplemented by the inferior retinaculum and the transferred talocalcaneal ligament to stabilize the lateral ankle. Chrisman and associates described the use of one half of the peroneus brevis. Watson-Jones and Evans used the entire peroneus brevis. The peroneus longus has been taken by mistake. The plantaris has been used in triligamentous reconstruction. Gould N, Seligson D, Gassman J: Early and late repair of lateral ligament of the ankle. Foot Ankle 1980;1:84-89. Hamilton WG, Thompson FM, Snow SW: The modified Brostrom procedure for lateral ankle instability. Foot Ankle 1993;14:1-7. Chrisman OD, Snook GA: Reconstruction of lateral ligament tears of the ankle: An experimental study and clinical evaluation of seven patients treated by a new modification of the Elmslie procedure. J Bone Joint Surg Am 1969;51:904-912. Evans DL: Recurrent instability of the ankle: My method of surgical treatment. Proc R Soc Med 1953;46:343. Watson-Jones R: Fractures and Joint Injuries, ed 3. Baltimore, MD, Williams and Wilkins, 1946, p 234.
References:
- Liu SH, Baker CL: Comparison of lateral ankle ligamentous reconstruction procedures. Am J Sports Med 1994;22:313-317.
Question 57High Yield
A 10-year-old child reports acute leg pain after wrestling with his brother. AP and lateral radiographs are shown in Figures 21a and 21b. What is the best course of action?

Explanation
The radiographs show an eccentric metaphyseal lesion with a well-defined reactive rim of bone that is consistent with a nonossifying fibroma. Pathologic fractures through benign lesions should be treated as appropriate for the fracture, allowing the fracture to heal. Biopsy is not needed when the radiographic diagnosis is benign. MRI, in the presence of a fracture, is not particularly helpful because of the hematoma. If radiographic findings reveal that the lesion appears aggressive, a biopsy should be performed, obtaining tissue away from the fracture site. Marks KE, Bauer TW: Fibrous tumors of bone. Orthop Clin North Am 1989;20:377.
Question 58High Yield
A 63-year-woman has an elbow flexion contracture. History reveals that she underwent three previous surgeries to remove a malignant fibrous histiocytoma of the forearm. An MRI scan reveals a locally recurrent tumor at the site of the previous surgery. Which of the following is considered the most predictive factor for local recurrence?
Explanation
Explanation
The greatest risk factor for local recurrence is an inadequate surgical margin. The tumor grade, histologic subtype, and size are predictive of systemic relapse. Sarcomas that arise in some anatomic sites, such as the forearm or retroperitoneum, may be more difficult to completely resect compared with other sites. The optimum margin is generally considered to be a cuff of normal tissue beyond the tumor. Bell RS, O'Sullivan B, Liu FF, et al: The surgical margin in soft-tissue sarcoma. J Bone Joint Surg Am 1989;71:370-375. Sadoski C, Suit HD, Rosenberg A, Mankin H, Efird J: Preoperative radiation, surgical margins, and local control of extremity sarcomas of soft tissues. J Surg Oncol 1993;52:223-230.
References:
- Wilson AN, Davis A, Bell RS, et al: Local control of soft tissue sarcoma of the extremity: The experience of a multidisciplinary sarcoma group with definitive surgery and radiotherapy. Eur J Cancer 1994;30:746-751.
Question 59High Yield
A 27-year-old man sustained a gunshot wound to the lumbar spine and undergoes an exploratory laparotomy. An injury to the cecum is identified and treated. Management should now include
Explanation
Explanation
Gunshot wounds to the spine present relatively little risk of infection in most cases. When there has been an injury to the colon, the risk of infection can be minimized with a 7-day course of broad-spectrum antibiotics. Fragment removal is not indicated. Roffi RP, Waters RL, Adkins RH: Gunshot wounds to the spine associated with a perforated viscus. Spine 1989;14:808-811.
References:
- Velmahoos GC, Demetriades D: Gunshot wounds of the spine: Should retained bullets be removed to prevent infection? Ann R Coll Surg Engl 1976;94:85-87.
Question 60High Yield
Figure 49 shows the radiograph of a 3-year-old child with progressive bowlegs. Laboratory studies show a calcium level of 9.5 mg/dL (normal 9.0 to 11.0 mg/dL), a phosphorus level of 4.2 mg/dL (normal 3 to 5.7 mg/dL), and an alkaline phosphatase level of 305 IU/L (normal 104 to 345 IU/L). What is the most likely diagnosis?
Explanation
Explanation
The patient has bowlegs associated with very wide physes, particularly noted at the hips. The widening of the growth plates is a classic sign of rickets; however, the normal levels of calcium, phosphorus, and alkaline phosphatase rule out both nutritional and hypophosphatemic rickets. Patients with nutritional rickets or hypophosphatemic rickets have hypophosphatemia and increased alkaline phosphatase levels. Jansen metaphyseal dysostosis has very severe radiographic findings that are not found in this patient; however, these radiographic findings are classic for Schmid metaphyseal dysostosis. This disorder is caused by a mutation in the gene for type X collagen, which is found only in the growth plates of growing children. Lachman RS, Rimoin DL, Spranger J: Metaphyseal chondrodysplasia - Schmid type: Clinical and radiographic delineation with a review of the literature. Pediatr Radiol 1988;18:93-102.
References:
- Warman ML, Abbot M, Apte SS, et al: A type X collagen mutation causes Schmid metaphyseal chondrodysplasia. Nat Genet 1993;5:79-82.
Question 61High Yield
A patient reports progessive bilateral hand clumsiness and ataxia. Examination reveals a positive Hoffmann's sign and intrinsic atrophy. MRI reveals multilevel cervical spondylosis, and lateral flexion and extension radiographs show cervical kyphosis in the neutral position, with restoration of lordosis on extension. Which of the following procedures is most likely to result in poor long-term results?
Explanation
Adequate decompression of the cervical cord can be achieved in a variety of ways depending on the pathoanatomy of the compression, but kyphosis is a relative contraindication to laminectomy alone. For laminectomy to be effective, the lordosis must be maintained so the cord can displace posteriorly away from the anterior structures. In addition, removing the posterior tension band increases the probability that the kyphosis will progress, therefore increasing the force against the front of the cord as it tents across the kyphosis. Albert TJ, Vaccaro A: Postlaminectomy kyphosis. Spine 1998;23:2738-2745. Truumees E, Herkowitz HN: Cervical spondylotic myelopathy and radiculopthy. Instr Course Lect 2000;49:339-360.
Question 62High Yield
Figure 35 shows the lateral radiograph of a 15-year-old basketball player who felt a dramatic pop in his knee when landing after a lay-up. The patient reports that he cannot bear weight on the injured extremity. Management should consist of
Explanation
Explanation
Tibial tubercle avulsion is an injury of the adolescent knee that most often occurs just before the end of growth. The fracture usually occurs with jumping, either at push-off or landing. This patient has a type III injury. In type III injuries, the articular surface is disrupted, and meniscal injury and compartment syndrome can occur. Open reduction is the treatment of choice, and anterior fasciotomy should be considered prophylactically at the time of surgery. Although the fracture heals with an anterior epiphysiodesis of the proximal tibia, little growth remains in this patient and no special handling of the physis is warranted. Ogden JA, Tross RB, Murphy MJ: Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-215.
References:
- Pape JM, Goulet JA, Hensinger RN: Compartment syndrome complicating tibial tubercle avulsion. Clin Orthop 1993;295:201-204.
Question 63High Yield
Figures 5a and 5b show the clinical photograph and radiograph of a patient who has difficulty wearing shoes and has persistent symptoms medially and laterally at the first and fifth metatarsophalangeal joints. Because shoe modifications have failed to provide relief, management should now consist of
Explanation
Explanation
5b A significant bunionette deformity that fails to respond to conservative management is best addressed surgically, in this case with the bunion deformity. The radiograph reveals a prominent lateral condyle at the fifth metatarsal head without a significant increase in the intermetatarsal angle. Simple exostectomy is preferred with less risk of complications. Complete excision would risk transfer lesions to the medial metatarsals. Mann RA, Coughlin MJ: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 415-435.
References:
- Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 163-173.
Question 64High Yield
What clinical parameter will most likely decrease the need for blood transfusion after total joint arthroplasty?
Explanation
Bilateral joint replacement, chronic disease, and preoperative autologous donation all increase the risk of needing blood. Young patients and a high hemoglobin level (greater than 15 g/dL) are considered clinical parameters that decrease the risk for requiring allogenic blood. Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 65High Yield
An 18-year-old man sustains an injury to his lateral ankle after being kicked while playing soccer. He reports persistent pain on the lateral ankle as well as a popping sensation with attempted ankle dorsiflexion and eversion. Which of the following structures anatomically restrains the retracted structure shown in Figure 12?
Explanation
The peroneus brevis and peroneus longus muscles are the main evertors of the hindfoot. As they descend along the posterior fibula, they pass through the retromalleolar sulcus, formed by the concavity of the retromalleolar fibula. This sulcus is deepened by a fibrocartilaginous rim. The superior peroneal retinaculum covers the fibular groove and stabilizes the peroneal tendons within the retromalleolar sulcus. It originates from the posterolateral ridge of the fibula and inserts onto the lateral calcaneus. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 81-89.
Question 66High Yield
Which of the following nerves innervates the muscle that originates from the middle third of the dorsal surface of the lateral border of the scapula, as shown in Figure 7?
Explanation
Explanation
Teres minor originates from the middle third of the dorsal surface of the lateral border of the scapula. It is supplied by the axillary nerve (C5). Williams PL, Warwick R, Dyson M, Bannister LH: Myology, in Gray's Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 611-615.
References:
- Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 68-72.
Question 67High Yield
The axis of forearm rotation occurs between what two anatomic points?
Explanation
Explanation
Forearm rotation results from a complex interaction of osseous articulations and soft tissues including the radiocapitellar articulation, proximal and distal radioulnar joints, the interosseous membrane, and the adjacent forearm muscles. The rotation occurs around a longitudinal forearm axis extending from the center of the radial head proximally through the foveal region of the ulnar head distally. Werner FW, An KN: Biomechanics of the elbow and forearm. Hand Clin 1994;10:357-373.
Question 68High Yield
A 33-year-old man had his foot run over by a forklift 1 hour ago. Examination reveals that the head of the fifth metatarsal is extruded through the plantar aspect of the foot. The foot is severely swollen and pale, there is no sensation in the toes, and the pulses are not palpable. Radiographs are shown in Figures 42a and 42b. Emergent management should consist of

Explanation
Following a severe crush injury, the patient has an acute compartment syndrome. Even though there is an open fracture, this is not sufficient to decompress the compartment syndrome. Therefore, splinting and observation are not appropriate. The surgical treatment of choice is fasciotomy with fixation of the multiple fractures. A primary amputation is not indicated because there is potential for salvage of this devastating injury. Fakhouri AJ, Manoli A II: Acute foot compartment syndromes. J Orthop Trauma 1992;6:223-228. Myerson MS: Management of compartment syndromes of the foot. Clin Orthop 1991;271:239-248.
Question 69High Yield
A 72-year-old woman who was doing well after undergoing total shoulder arthroplasty for arthritis 4 months ago is suddenly unable to elevate her arm. Examination reveals 70 degrees of external rotation compared with 45 degrees on the uninvolved side, and she is unable to lift her hand off her lower back. Radiographs are shown in Figures 43a through 43c. Treatment should consist of


Explanation
Results of treatment of subscapularis rupture are best when immediate repair is performed. When the cause of the anterior instability is the result of rupture of the subscapularis tendon and the component position is acceptable, revising the position of the component is unnecessary. Restoring the coracoacromial arch and subacromial decompression are related to superior instability and rotator cuff pathology, respectively, and would not correct the instability caused by subscapularis rupture. Moeckel BH, Altchek DW, Warren RF, Wickiewicz TL, Dines DM: Instability of the shoulder after arthroplasty. J Bone Joint Surg Am 1993;75:492-497.
Question 70High Yield
A 68-year-old woman with serologically proven rheumatoid arthritis underwent an open synovectomy and radial head resection 10 years ago. She now has severe pain that has failed to respond to nonsurgical management. Examination reveals a flexion arc of greater than 90 degrees. Radiographs are shown in Figures 15a and 15b. What is the most appropriate management?
Explanation
Explanation
15b The radiographs reveal severe arthritic changes with no joint space, and the AP view shows a progressive malalignment secondary to the radial head resection. A prosthetic arthroplasty is indicated given the severe arthritis (Larsen grade III). Unconstrained arthroplasties have not performed as well as semiconstrained arthroplasties after previous radial head resections. However, both types of arthroplasties performed better in native elbows. Synovectomies should be reserved for less advanced disease states. Whaley A, Morrey BF, Adams R: Total elbow arthroplasty after previous resection of the radial head and synovectomy. J Bone Joint Surg Br 2005;87:47-53. Maenpaa HM, Kuusela PP, Kaarela KK, et al: Reoperation rate after elbow synovectomy in rheumatoid arthritis. J Shoulder Elbow Surg 2003;12:480-483.
References:
- Schemitsch EH, Ewald FC, Thornhill TS: Results of total elbow arthroplasty after excision of the radial head and synovectomy in patients who had rheumatoid arthritis. J Bone Joint Surg Am 1996;78:1541-1547.
Question 71High Yield
The use of posting (a wedge added to the medial or lateral side of an insole) is useful to balance forefoot or hindfoot malalignment. Assuming normal subtalar joint pronation, what is the maximum amount of recommended hindfoot posting?
Explanation
Explanation
Generally, patients cannot tolerate more than 5 degrees of hindfoot posting. Donatelli RA, Hurlbert C, Conaway D, et al: Biomechanics foot orthotics: A retrospective study. J Orthop Sports Phys Ther 1988;10:205-212. Michaud TM: Foot Orthoses and Other Forms of Conservative Foot Care. Baltimore, MD, Williams & Wilkins, 1993, pp 61-65, 186.
References:
- Root MC, Orien WP, Weed JH: Normal and Abnormal Function of the Foot. Los Angeles, CA, Clinical Biomechanics Corporation, 1977, vol 2, pp 29-33.
Question 72High Yield
Figure 1 shows the radiograph of an 18-year-old patient who has severe knee pain. Treatment consisting of osteotomy should be perfomed
Explanation
Very large corrections of tibial deformity can be achieved at or just below the tibial tubercle. This level of osteotomy maintains the relationship between the tubercle and the rest of the joint, does not alter patellofemoral mechanics, and avoids complicating possible future conversion to total knee arthroplasty. High tibial osteotomy is contraindicated for large corrections because of excessive elevation of the tibial tubercle and overhang of the lateral plateau. Correction in the tibial diaphysis creates a zig zag pattern in the tibia by correcting below the deformity and risks nonunion in cortical bone. There is no evidence that the femur is deformed; therefore, femoral osteotomy is not indicated.
Question 73High Yield
A 21-year-old man has had right groin pain for the past year. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 50a through 50e. What is the most likely diagnosis?
Explanation
Explanation
50b 50c 50d 50e The pathology demonstrates a very cellular chondroid matrix with multinucleated forms, atypia, and myxomatous regions. This is most consistent with a myxoid chondrosarcoma. The radiograph shows a well-circumscribed lesion in the superior and medial aspect of the right acetabulum. The CT and MRI scans confirm these same findings with no evidence of matrix mineralization or significant surrounding edema. Unfortunately, in this location with this appearance, the radiographic differential diagnosis includes all the diagnoses listed. Terek RM: Recent advances in the basic science of chondrosarcoma. Orthop Clin North Am 2006;37:9-14. Donati D, El Ghoneimy A, Bertoni F, et al: Surgical treatment and outcome of conventional pelvic chondrosarcoma. J Bone Joint Surg Br 2005;87:1527-1530.
References:
- Pring ME, Weber KL, Unni KK, et al: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Question 74High Yield
A 25-year-old woman returns for her first postoperative visit after arthroscopic thermal capsulorrhaphy for recurrent multidirectional instability. Examination reveals that the portals are healed, there is no swelling; and passive range of motion is within the normal range. However, she is unable to actively raise her arm. Shoulder radiographs are normal. What is the most likely cause of these findings?
Explanation
Treatment of shoulder instability with thermal devices has lead to numerous complications including recurrent instability, chondrolysis, stiffness, and capsular necrosis. This patient's findings are consistent with a heat-induced axillary nerve injury. Normal radiographs exclude extensive chondrolysis. Levine WN, Bigliani LU, Ahmad CS: Thermal capsulorrhaphy. Orthopedics 2004;27:823-826.
Question 75High Yield
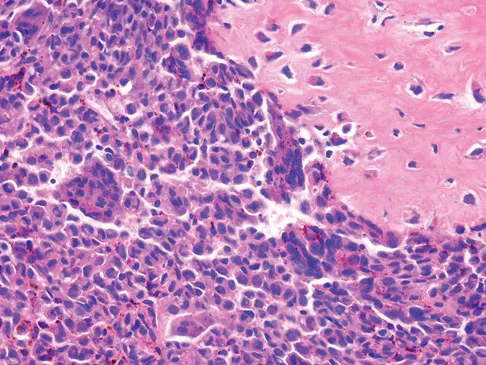
A previously healthy 13-year-old girl has had thigh pain for the past 3 weeks. The radiograph shown in Figure 47a reveals a lesion in the right femur. A bone scan and CT scan of the chest show no evidence of other lesions. A biopsy specimen is shown in Figure 47b. What is the most likely diagnosis?

Explanation
The patient has Langerhans cell histiocytosis that may be solitary (eosinophilic granuloma) or associated with systemic illness (Hand-Schuller-Christian disease and Letterer-Siwe disease). The solitary form of the disease, eosinophilic granuloma, typically affects patients in the first three decades of life. Radiographically, it is characterized as a well-defined, lytic, "punched out" intramedullary lesion. Histologically, two cell types, eosinophils and Langerhans cells, are seen. The Langerhans cells are seen as mononuclear histiocyte-like cells with oval nuclei with well-defined round or oval cytoplasm. A prominent nuclear groove can be seen in most of the nuclei (coffee bean nuclei). A mixture of inflammatory cells and lipid-laden foam cells with nuclear debris may be present as well. The lack of nuclear atypia and atypical mitoses excludes malignant conditions such as Ewing's sarcoma, lymphoma of bone, and metastatic neuroblastoma. The lack of acute inflammatory cells excludes the diagnosis of osteomyelitis. The eosinophils have bi-lobed nuclei and granular eosinophilic cytoplasm. Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby, 1988.
Question 76High Yield
What tendon is closest to an appropriately placed anterolateral portal for ankle arthroscopy?
Explanation
Explanation
The appropriate placement of the anterolateral portal provides access to the lateral gutter of the joint while avoiding the superficial peroneal nerve. The safest location for the portal is approximately 4 mm lateral to the peroneus tertius tendon, the closest of the tendons listed to the anterolateral portal. Because the superficial peroneal nerve location is variable, attempts to visualize, palpate, or transilluminate the nerve are mandatory.
References:
- Ogut T, Akgun I, Kesmezacar H, et al: Navigation for ankle arthroscopy: Anatomical study of the anterolateral portal with reference to the superficial peroneal nerve. Surg Radiol Anat 2004;26:268-274.
Question 77High Yield
A 35-year-old man has profound deltoid weakness after sustaining a traumatic anterior shoulder dislocation 6 weeks ago. Electromyographic (EMG) studies confirm an axillary nerve injury. Follow-up examination at 3 months reveals no recovery of function. What is the best course of action?
Explanation
Explanation
Documenting the status of recovery at this time is appropriate; therefore, repeat EMG studies should be conducted to check for early signs of reinnervation. Timing of nerve exploration in this setting is debated, with authors suggesting exploration if there is no sign of recovery at 6 to 9 months. Perlmutter GS: Axillary nerve injury. Clin Orthop 1999;368:28-36. Artico M, Salvati M, D'Andrea V, et al: Isolated lesions of the axillary nerves: Surgical treatment and outcome in twelve cases. Neurosurgery 1991;29:697-700. Vissar CP, Coene LN, Brand R, et al: The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery: A prospective clinical and EMG study. J Bone Joint Surg Br 1999;81:679-685.
References:
- Pasila M, Jarma H, Kiviluoto O, et al: Early complications of primary shoulder dislocations. Acta Orthop Scand 1978;49:260-263.
Question 78High Yield
What structure is most at risk with anterior penetration of C1 lateral mass screws?
Explanation
Posterior screw fixation of the upper cervical spine has gained a great deal of popularity due to its stable fixation, obviating the use of halo vest immobilization, and its high fusion rates. The use of screws in this location, however, has introduced a whole new set of potential complications. Vertebral artery injury is one of the most feared complications associated with screws in the C1/C2 region. This structure, however, is lateral and posterior at the C2 level and then penetrates the foramen transversarium of C1 to lie cephalad to the arch of C1 before entering the foramen magnum. It is the internal carotid artery that lies immediately anterior to the arch of C1 that is particularly at risk by anterior penetration of C1 lateral mass or C1-C2 transarticular screws as demonstrated by Currier and associates. The internal carotid artery lies posterior to the pharynx. The external carotid artery and the glossopharyngeal nerve are not at risk with this method of fixation. Currier BL, Todd LT, Maus TP, et al: Anatomic relationship of the internal carotid artery to the C1 vertebra: A case report of cervical reconstruction for chordoma and pilot study to assess the risk of screw fixation of the atlas. Spine 2003;28:E461-E467. Grant JC: Grant's Atlas of Anatomy, ed 6. Baltimore, MD, Williams & Wilkins, 1972.
Question 79High Yield
A 60-year-old man is evaluated in the ICU after a rollover motor vehicle accident 3 days ago. He has multiple upper and lower extremity trauma and was found unresponsive at the accident scene. Surgery is planned for the extremity trauma once the patient is medically stable. He remains intubated and the cervical spine is immobilized in a semi-rigid collar. Examination reveals mild erythema in the posterior occipital cervical region. Initial AP and lateral radiographs of the cervical spine have not revealed any obvious fracture. What is the most appropriate treatment option at this time?
Explanation
Ackland and associates demonstrated that the failure to achieve early spinal clearance in an unconscious blunt trauma patient predisposed the patient to increased morbidity secondary to the prolonged used of cervical immobilization. They demonstrated that the four significant predictors of collar-related ulcers were ICU admission, mechanical ventilation, the necessity for cervical MRI, and the time to cervical spine clearance and collar removal. The risk of pressure-related ulceration increased by 66% for every 1-day increase in Philadelphia collar time and this highlights the need for definitive C-spine clearance. Ackland HM, Cooper DJ, Malham GM, et al: Factors predicting cervical collar-related decubitus ulceration in major trauma patients. Spine 2007;32:423-428.
Question 80High Yield
A 20-year-old man sustained a closed tibial fracture and is treated with a reamed intramedullary nail. What is the most common complication associated with this treatment?
Explanation
The most common complication is anterior knee pain (57%). The knee pain is activity related (92%) and exacerbated by kneeling (83%). Although knee pain is the most common complication, most patients rate it as mild to moderate and only 10% are unable to return to previous employment. Some authors report less knee pain with a peritendinous approach when compared to a tendon-splitting approach. In one study, nail removal resolved pain in 27%, improved it in 70%, and made it worse in 3%. The incidence of the other complications was: infection 0% to 3%, nonunion 0% to 6%, and malunion 2% to 13%. Compartment syndrome is rare after nailing. Court-Brown CM: Reamed intramedullary tibial nailing: An overview and analysis of 1106 cases. J Orthop Trauma 2004;18:96-101. McQueen MM, Gaston P, Court-Brown CM: Acute compartment syndrome: Who is at risk? J Bone Joint Surg Br 2000;82:200-203.
Question 81High Yield
Which of the following radiographic views best assesses anterior coverage of the dysplastic hip?
Explanation
Explanation
Anterior coverage of the hip may be best estimated by the anterior center edge angle of Lequesne and de Seze (analogous to Wiberg's angle), which is measured on the well-defined faux profil view. Evaluation with CT scans also has been described. Klaue K, Wallin A, Ganz R: CT evaluation of coverage and congruency of the hip prior to osteotomy. Clin Orthop 1988;232:15-25.
References:
- Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 82High Yield
Which of the following complications is uniquely associated with an anterior approach to the lumbosacral junction?
Explanation
Explanation
Retrograde ejaculation is a sequela of injury to the superior hypogastric plexus. The structure needs protection, especially during anterior exposure of the lumbosacral junction. The use of monopolar electrocautery should be avoided in this region. The ideal exposure starts with blunt dissection just to the medial aspect of the left common iliac vein, sweeping the prevertebral tissues toward the patient's right side. Although erectile dysfunction can be seen after spinal surgery, it is not typically related to the surgical exposure because erectile function is regulated by parasympathetic fibers derived from the second, third, and fourth sacral segments that are deep in the pelvis and are not at risk with the anterior approach. The other choices are complications of spinal surgery but are not uniquely associated with an anterior L5-S1 exposure. Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492. Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer-Verlag, 1983, p 107.
References:
- An HS, Riley LH III: An Atlas of Surgery of the Spine. New York, NY, Lippincott Raven, 1998, p 263.
Question 83High Yield
Figures 45a and 45b show the AP and lateral radiographs of a 15-year old patient who is undergoing surgery to add 3 cm of length to the femur. Based on the radiographic findings, what is the next most appropriate step in management?
Explanation
Explanation
45b Because the radiographs reveal poor regenerate bone, especially anteriorly and laterally, the first step in management is to slow the distraction rate. If this does not solve the problem, temporary reversal of the distraction, or "accordionization," can be used to induce a greater healing response. Maintaining the same distraction rate will further impair regenerate formation and delay healing. Bone grafting should be reserved as an option if decreasing the distraction rate or alternating a week of compression with a week of distraction fails to improve the callus formation. Repeat corticotomy is performed in patients with premature consolidation. Raney EM: Limb-length discrepancy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1519-1526.
References:
- Ilizarov GA: Pseudarthroses and defects of long tubular bones, in Transosseous Osteosynthesis: Theoretical and Clinical Aspects of the Regeneration and Growth of Tissue. Berlin, Springer-Verlag, 1992, p 453.
Question 84High Yield
An 8-year-old girl sustained a displaced fracture at the base of the femoral neck in a motor vehicle accident. Management should consist of
Explanation
Explanation
Pediatric intracapsular hip fractures are challenging because of the high rates of complications, including osteonecrosis and varus malunion. These patients should be treated as emergencies. Principles of treatment include anatomic reduction with internal fixation. Screw fixation short of the physis is preferred and may need to be supplemented with spica cast immobilization. Fixation may be achieved with smooth pins across the physis when little metaphyseal bone is available. Fixation across the physis with threaded screws is acceptable only when the patient is close to skeletal maturity. Pediatric hip screws are appropriate if immediately available. Emergent open reduction, capsulotomy, or joint aspiration may decrease the rate of osteonecrosis. Cheng JC, Tang N: Decompression and stable internal fixation of femoral neck fractures in children can affect the outcome. J Pediatr Orthop 1999;19:338-343. Azouz EM, Karamitsos C, Reed MH, et al: Types and complications of femoral neck fractures in children. Pediatr Radiol 1993;23:415-420. Song KS, Kim YS, Sohn SW, et al: Arthrotomy and open reduction of the displaced fracture of the femoral neck in children. J Pediatr Orthop B 2001;10:205-210.
References:
- Morsy HA: Complications of fracture of the neck of the femur in children: A long-term follow-up study. Injury 2001;32:45-51.
Question 85High Yield
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in
Explanation
The patient has a distal biceps rupture. While the distal biceps contributes to elbow flexion, its main function is forearm supination. Baker BE, Bierwagen D: Rupture of the distal tendon of the biceps brachii: Operative versus non-operative treatment. J Bone Joint Surg Am 1985;67:414-417. D'Arco P, Sitler M, Kelly J, et al: Clinical, functional, and radiographic assessments of the conventional and modified Boyd-Anderson surgical procedures for repair of distal biceps tendon ruptures. Am J Sports Med 1998;26:254-261.
Question 86High Yield
Figures 5a and 5b show the radiographs of a 45-year-old patient. What is the most likely diagnosis?

Explanation
Glenoid dysplasia is an uncommon anomaly that usually has a benign course but may result in shoulder pain, arthritis, or multidirectional instability. Shoulder pain and instability often improve with shoulder strengthening exercises. Wirth MA, Lyons FR, Rockwood CA Jr: Hypoplasia of the glenoid: A review of sixteen patients. J Bone Joint Surg Am 1993;75:1175-1184.
Question 87High Yield
A 37-year-old racquet player had dominant shoulder pain for 1 year, and cortisone injections provided only temporary relief. Because MRI findings did not reveal a rotator cuff tear, he underwent arthroscopic treatment including subacromial decompression and spur removal below the distal clavicle. Three years following surgery, he now reports that the pain has returned. What is the most likely cause of his pain?
Explanation
Co-planing the distal clavicle may lead to painful acromioclavicular joints in up to 35% of patients; this is felt to be related to destabilizing the distal clavicle. Intra-articular diagnosis of synovitis, degenerative joint disease, and superior labrum anterior and posterior lesions would have been identified at initial arthroscopy (not necessarily seen in open surgery). Ganglions are seen on MRI. Fischer BW, Gross RM, McCarthy JA: Incidence of acromioclavicular joint complications after arthroscopic subacromial decompression. Arthroscopy 1999;15:241-248. Hazel RM, Tasto JP, Klassen J: Arthroscopic subacromial decompression: A 9-year follow-up. Arthroscopy 1998;14:419.
Question 88High Yield
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?
Explanation
A concern in the multiply injured patient who has a pulmonary contusion is the potential for further pulmonary compromise because of embolization of marrow, blood clot, or fat during manipulation of the medullary canal. Recent evidence has shown that the presence of a lung injury is the most important determining factor in future deterioration. However, despite the lung injury and its potential consequences, this patient's femur fracture needs stabilization. Because damage control in the multiply injured patient requires a technique that can be performed rapidly and consistently, the treatment of choice is application of an external fixator. By placing two pins above and below the fracture and with longitudinal traction, the fracture is quickly realigned and stabilized. This allows the patient to be resuscitated and treated at a later date when definitive management of the fracture can be carried out. There is little difference between plate fixation and intramedullary nailing. Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809. Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Question 89High Yield
When a structure like a long bone is under a bending load, its maximum stress is most dependent on what factor?
Explanation
The maximum stress in a bone occurs at the periosteal surface (the greatest distance from the center of the bone). The magnitude of the stress is equal to the magnitude of the applied moment (M) multiplied by the distance to the surface (roughly the radius of the bone, r) divided by the area moment of inertia (I), so that stress = Mr/I. Of the possible answers, only area moment of inertia of the cross section contains any of these three items. The stress can also depend on the length of the bone, but it cannot be determined without knowing the location at which the bending load is applied, information that was not given in the problem. The type of structural support may influence local stresses where the support contacts the bone, but it has little effect on the maximum stress in the bone. The cross-sectional area is not as important as the area moment of inertia because the stress is not evenly distributed over the cross-section. Plastic modulus is a material property, not a geometric or structural property, and it does not affect stress. Hayes WC, Bouxsein ML: Biomechanics of cortical and trabecular bone: Implications for assessment of fracture risk, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 76-82.
Question 90High Yield
The use of a screw between the clavicle and the coracoid process to maintain the clavicle and acromioclavicular (AC) joint in a reduced position is a treatment option for AC joint separations. Screw removal is generally recommended after soft-tissue healing. What effect does this rigid coracoclavicular fixation have on shoulder kinematics?
Explanation
This issue has been debated since Inman published his classic study on clavicular rotation in 1944. Subsequently, it has been shown by several authors that the clinical evaluation of patients with either coracoclavicular screws in place or with arthrodesis of the coracoclavicular reveals little to no loss of shoulder motion. This is most likely the result of synchronous motion of the scapula and clavicle in shoulder movements. Flatow EL: The biomechanics of the acromioclavicular, sternoclavicular, and scapulothoracic joints. Instr Course Lect 1993;42:237-245. Kenedy JC, Cameron H: Complete dislocation of the acromioclavicular joint. J Bone Joint Surg Br 1954;36:202-208. Rockwood CA Jr, Williams GR, Young CD: Disorders of the acromioclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 483-553.
Question 91High Yield
What is the most common adverse postoperative complication of laminoplasty for multilevel cervical spondylotic myelopathy?
Explanation
A 30% to 50% loss of cervical range of motion is reported postoperatively in most patients following cervical laminoplasty. Inadvertent closure of the laminoplasty does occur but is rare. Laminoplasty is advocated in lieu of laminectomy to prevent progressive kyphosis and can effectively decompress the spinal cord. C5 nerve root palsies are a poorly understood but rare complication of surgical decompression for cervical spondylotic myelopathy. Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Question 92High Yield
Figures 35a and 35b show the radiographs of a 20-year-old man who is unable to rotate his dominant forearm. Examination reveals that the arm is fixed in supination. To regain motion, management should consist of

Explanation
The patient has a proximal synostosis; therefore, resection of the synostosis is considered the best option to regain motion. While forearm osteotomy can place the hand in a more functional position, rotation will not be restored. Proximal radial excision can provide forearm rotation; however, this procedure is reserved for patients who have a proximal radioulnar synostosis that is too extensive to allow a safe resection, involves the articular surface, and is associated with an anatomic deformity. Motion will not be restored with dynamic splinting. Kamineni S, Maritz NG, Morrey BF: Proximal radial resection for posttraumatic radioulnar synostosis: A new technique to improve forearm rotation. J Bone Joint Surg Am 2002;84:745-751.
Question 93High Yield
Figure 45 shows the radiograph of a 2-year-old patient who has progressive lumbar scoliosis as the result of hemivertebra. Examination reveals no associated cutaneous lesions, and an MRI scan shows no associated intraspinal anomalies. Treatment should consist of
Explanation
Explanation
In a retrospective review of 10 patients treated with hemivertebra excision for hemivertebra in the levels of T12 to L3, the procedure was found to be safe and effective. The procedure provided an average curve correction of 67 degrees and was greatest in patients who were younger than age 4 years at the time of surgery. Long anterior and posterior fusion with instrumentation is not the treatment of choice at this age. Either anterior hemiepiphyseodesis or posterior hemiarthrodesis in this isolated hemivertebra setting would be inadequate. Brace treatment is ineffective in management of the primary curvature.
References:
- Callahan BC, Georgopoulos G, Eilert RE: Hemivertebral excision for congenital scoliosis. J Pediatr Orthop 1997;17:96-99.
Question 94High Yield
A 48-year-old woman has knee pain that is worse with weight bearing. She reports no night pain or pain at rest. History reveals that she underwent total knee arthroplasty with cementless components 2 years ago. Examination reveals tenderness along the medial joint line. Figures 12a through 12c show radiographs and a bone scan. What is the most likely cause of the patient's pain?
Explanation
Explanation
12b 12c The radiographs show a halo-like sclerotic margin around the tibial stem and lucency under the baseplate. The bone scan shows markedly increased uptake under the tibial component, particularly on the medial side (not diffusely through the knee as seen with infection). These studies indicate lack of bone ingrowth fixation of the cementless porous-coated tibial component. The recent report of Fehring and associates has identified failure of ingrowth of a porous-coated implant as a dominant mode of early failure of total knee arthroplasties. Fehring TK, Odum S, Griffin WL, Mason B, Nadaud M: Early failures of total knee arthroplasty. Clin Orthop 2001;392:315-318.
References:
- Fehring TK: Revision TJA corrects flexion extension gap imbalance. Orthop Today 2002;22:44.
Question 95High Yield
Which of the following lumbar disk components has the highest tensile modulus to resist torsional, axial, and tensile loads?
Explanation
The annulus fibrosis has a multilayer lamellar architecture mode of type I collagen fibers. Each successive layer is oriented at 30 degrees to the horizontal in the opposite direction, leading to a "criss-cross" type pattern. This composition allows the annulus, which has the highest tensile modulus, to resist torsional, axial, and tensile loads.
Question 96High Yield
The parents of a 10-year-old boy with Down syndrome are seeking sports clearance for participation in the high jump at the Special Olympics. He is asymptomatic, and the neurologic examination is normal. The hips and patellae are clinically stable. Radiographs of the cervical spine in flexion and extension show a maximum atlanto-dens interval (ADI) of 6 mm. Based on these findings, what recommendation should be made?
Explanation
Explanation
In approximately 15% of children with Down syndrome, atlantoaxial instability develops because of ligament laxity, making them susceptible to spinal cord injury with relatively minor trauma. The American Academy of Pediatrics recommends lateral flexion-extension views of the cervical spine in any patient with Down syndrome who wishes to participate in sports. A normal ADI is up to 4 mm. Patients with Down syndrome with an ADI of more than 5 mm should not participate in contact sports or sports with a high risk for neck injury, such as diving, gymnastics, high jump, or butterfly stroke. Cervical fusion has a very high rate of complications in patients with Down syndrome and is recommended only for patients who have myelopathic signs or symptoms. Atlantoaxial instability in Down syndrome: Subject review. American Academy of Pediatrics Committee on Sports Medicine and Fitness. Pediatrics 1995;96:151-154. Tredwell SJ, Newman DE, Lockitch G: Instability of the upper cervical spine in Down syndrome. J Pediatr Orthop 1990;10:602-606.
References:
- Segal LS, Drummond DS, Zanotti RM, et al: Complications of posterior arthrodesis of the cervical spine in patients who have Down syndrome. J Bone Joint Surg Am 1991;73:1547-1554.
Question 97High Yield
Figures 39a and 39b show the MRI scans of a 25-year-old man with right shoulder pain. Figure 39c shows the arthroscopic view from a posterior portal in the beach chair position. What is the most likely diagnosis?
Explanation
Explanation
39b 39c The MRI scans show coronal oblique and sagittal oblique views of a partial articular surface supraspinatus tear or tendon avulsion (PASTA lesion). The arthroscopic view is a posterior portal of the glenohumeral joint viewing the articular surface of the supraspinatus. These tears are a common source of shoulder pain and are often amenable to transtendon arthroscopic repair without detachment of the intact bursal surface. Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the shoulder. Am J Sports Med 2005;33:1088-1105. McConville OR, Iannotti JP: Partial-thickness tears of the rotator cuff: Evaluation and management. J Am Acad Orthop Surg 1999;7:32-43.
References:
- Burkhart SS: Arthroscopic management of rotator cuff tears, in McGinty JB (ed): Operative Arthroscopy, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 508-546.
Question 98High Yield
A 2-year-old child has marked hypotonia and depressed reflexes. History reveals that the child was normal at birth and developed normally for the first year. The child also began to ambulate, but lost this ability during the next 6 months. Laboratory studies show a creatine phosphokinase level that is within the normal range. DNA testing confirms a deletion in the survival motor neuron (SMN) gene. What is the most likely diagnosis?
Explanation
The patient has spinal muscular atrophy, type 2. This type is intermediate in severity between the Werdnig-Hoffmann type (type 1) and the Kugelberg-Welander type (type 3). It normally manifests itself between the ages of 3 and 15 months. Survival until adolescence is common. All three types of spinal muscular atrophy have been linked to the SMN gene at the 5q12.2-13.3 locus. DNA testing is available and is preferred to muscle biopsy because it is less invasive and more definitive. Biros I, Forrest S: Spinal muscular atrophy: Untangling the knot? J Med Genet 1999;36:1-8.
Question 99High Yield
During the application of halo skeletal fixation, the most appropriate position for the placement of the anterior halo pins is approximately 1 cm above the superior orbital rim and
Explanation
Explanation
Halo fixation is the most rigid form of cervical orthosis, but complications can arise from improper placement of the initial halo ring. A relatively safe zone for anterior pin placement is located 1 cm above the orbital rim and superior to the lateral two thirds of the orbit. This position avoids the supraorbital and supratrochlear nerves and arteries over the medial one third of the orbit. The more lateral positions in the temporal fossa have very thin bone and can interfere with the muscles of mastication. Posterior pin site locations are less critical; positioning on the posterolateral aspect of the skull, diagonal to the contralateral anterior pins, is generally desirable. Botte MJ, Byrne TP, Abrams RA, et al: Halo skeletal fixation: Techniques of application and prevention of complications. J Am Acad Orthop Surg 1996;4:44-53.
Question 100High Yield
A 29-year-old woman was injured in a high-speed motor vehicle accident 3 hours ago. Radiographs are shown in Figures 7a through 7e. Her right foot injury is open and contaminated. Her associated injuries include a closed head injury and a ruptured spleen requiring resection. She has had 6 units of packed red blood cells and the trauma surgeon has turned her care over to you. Her current base deficit is 10 and her urinary output has averaged 0.4 mL/kg for the last 2 hours. What is the best treatment at this time?
Explanation
Explanation
7b 7c 7d 7e The patient appears to be a borderline or unstable surgical patient following her initial trauma and spleenectomy (high base excess and low urine output). She needs continued resuscitation and minimal additional blood loss. This is best accomplished with irrigation and debridement of the ankle, external fixation of the ankle, foot, and femur, and splinting of the forearm. A traction pin for the femoral fracture will not control bleeding as well as an external fixator. Intramedullary nailing of the femur and open reduction and internal fixation of the forearm would be appropriate in patients that are euvolemic and stable. Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461. Taeger G, Ruchholtz S, Waydhas C, et al: Damage control orthopedics in patients with multiple injuries is effective, time saving, and safe. J Trauma 2005;59:409-416. Harwood PJ, Giannoudis PV, van Griensven M, et al: Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J Trauma 2005;58:446-452.
You Might Also Like
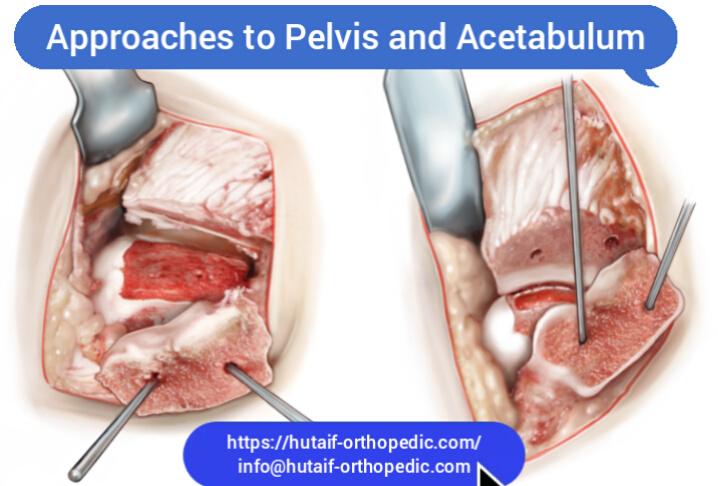
Previous ChapterOrthopedic Board Review: 100 High-Yield MCQs | Mock Exam Se…
Next Chapter Orthopedic Board Exam Prep: 100 High-Yield MCQs | Set 426

Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon