Orthopedic Board Review: Mock Exam Set #1088 - 100 High-Yield MCQs
14 Apr 2026
105 min read
130 Views
Key Takeaway
This page presents Mock Exam Set #1088, offering 100 high-yield orthopedic surgery multiple-choice questions. It's designed to help surgeons preparing for ABOS, OITE, and FRCS board exams to practice critical concepts, assess knowledge, and master their exam material effectively.
Surgical Hip Approaches: Master the Tensor Fa...
00:00
Start Quiz
Question 1High Yield
Figure 18a shows the clinical photograph of a 31-year-old man who has a slowly growing nodule on his right middle finger. It is minimally tender, and there is no erythema on examination. A biopsy specimen is shown in Figure 18b. What is the most likely diagnosis?
Explanation
Explanation
18b Epithelioid sarcoma is the most common soft-tissue sarcoma in the hand and most commonly occurs in young adults. The tumors can be superficial and may become ulcerated. Deeper lesions are often attached to tendons, tendon sheaths, or fascial structures. These are usually minimally symptomatic. The biopsy specimen reveals the typical appearance of a nodular pattern with central necrosis. They can mimic a necrotizing granulomatous process. Usually there are chronic inflammatory cells along the margin of the tumor nodules. This biopsy specimen does not have the clear cells necessary for a clear cell carcinoma or sarcoma. Nora's tumor is a bizarre parosteal osteochondromatous proliferation (BPOP) first described in 1983 by the pathologist, Nora. The lesion is defined as a reactive heterotopic ossification and is mostly found in the hands or feet of adults in the third decade of life. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 1074.
References:
- Halling AC, Wollan PC, Pritchard DJ, et al: Epithelioid sarcoma: A clinicopathologic review of 55 cases. Mayo Clin Proc 1996;71:636-642.
Question 2High Yield
A patient with Charcot-Marie-Tooth disease has a progressively rigid cavovarus foot deformity. The patient states that the pain is restricted to the forefoot, where rigid claw toe deformities have developed. Which of the following structures is primarily involved in creation of a claw toe deformity?
Explanation
Explanation
Diseases such as Charcot-Marie-Tooth result in spasticity to the extrinsic flexor tendons. This results in hyperflexion of the proximal and distal interphalangeal joints of the involved toe, as well as hyperextension at the metatarsophalangeal joint. The tendon often becomes contracted with progressive equinus of the ankle. Correction of ankle equinus exaggerates the claw toe deformity. The interosseous tendon plays no role in the etiology of a claw toe but may become contracted in later stages of the disease. Laxity of the volar plate may precipitate a claw toe deformity in a nonspastic situation. In patients with a head injury, claw toe deformities are generally the result of overactivity of the extensor tendons. Keenan MA, Gorai AP, Smith CW, Garland DE: Intrinsic toe flexion deformity following correction of spastic equinovarus deformity in adults. Foot Ankle 1987;7:333-337. Pichney GA, Derner R, Lauf E: Digital "V" arthrodesis. J Foot Ankle Surg 1993;32:473-479.
References:
- Mizel MS, Michelson JD: Nonsurgical treatment of monarticular nontraumatic synovitis of the second metatarsophalangeal joint. Foot Ankle Int 1997;18:424-426.
Question 3High Yield
Figure 1 shows the radiograph of a 71-year-old man who has had increasing pain and weakness in his shoulder for the past 3 years. Nonsurgical management has failed to provide relief. Examination shows 130 degrees of active forward flexion and intact external rotation strength. During surgery, a 1- x 1-cm rotator cuff tear involving the supraspinatus is encountered. Treatment should include
Explanation
Explanation
Given the size of the rotator cuff tear, it is likely to be repaired; therefore, the treatment of choice is a total shoulder replacement with rotator cuff repair. Severe rotator cuff insufficiency can lead to early glenoid failure because of superior instability, and glenoid resurfacing should be avoided in those instances. Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
References:
- Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for treatment of defects in the rotator cuff and surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491.
Question 4High Yield
The primary function of structure "A" in Figure 29 is to limit
Explanation
Explanation
The primary function of the popliteofibular ligament is to resist posterolateral rotation of the tibia on the femur, although it also secondarily resists varus angulation and posterior displacement of the tibia on the femur. The posterior cruciate ligament resists posterior tibial displacement, especially at 90 degrees of flexion. The lateral collateral ligament primarily resists varus displacement at 30 degrees of flexion but also resists posterolateral rotatory displacement with flexion that is less than approximately 50 degrees. The anterior and posterior cruciate ligaments resist varus displacement (along with the lateral collateral ligament) at 0 degrees of flexion. The anterior cruciate ligament primarily resists anterolateral displacement of the tibia on the femur. Sugita T, Amis AA: Anatomic and biomechanical study of the lateral collateral and popliteofibular ligaments. Am J Sports Med 2001;29:466-472.
References:
- Veltri DM, Deng XH, Torzilla PA, et al: The role of the cruciate and posterolateral ligaments in stability of the knee: A biomechanical study. Am J Sports Med 1995;23:436-443.
Question 5High Yield
A 57-year-old woman with diabetes mellitus has purulent drainage from a lateral incision after undergoing open reduction and internal fixation of a displaced ankle fracture 10 days ago. Examination reveals moderate erythema and a foul odor coming from the wound. Cultures are obtained. What is the next most appropriate step in management?
Explanation
Early postoperative wound infections after open reduction and internal fixation should be treated with aggressive debridement and maintenance of stability of the fracture. If infection persists following healing of the fracture, the hardware should be removed. Carragee EJ, Csongradi JJ, Bleck EE: Early complications in the operative treatment of ankle fractures: Influence of delay before operation. J Bone Joint Surg Br 1991;73:79-82.
Question 6High Yield
With increasing abduction in the scapular plane, maintaining neutral rotation, contact area, and contact pressure per unit area between the humeral head and glenoid follows what pattern if the total load across the joint is held constant?
Explanation
Explanation
The glenohumeral joint becomes more congruent at higher levels of abduction. As a consequence, contact area increases. As the load is spread more evenly across the joint, contact pressure per unit area decreases as long as the total load across the joint is held constant. Warner JJP, Bowen MK, Deng XH, et al: Articular contact patterns of the normal glenohumeral joint. J Shoulder Elbow Surg 1998;7:381-388.
References:
- Greis PE, Scuderi MG, Mohr A, et al: Glenohumeral articular contact areas and pressures following labral and osseous injury to the anteroinferior quadrant of the glenoid. J Shoulder Elbow Surg 2002;11:442-451.
Question 7High Yield
A 73-year-old man has stiffness after undergoing primary posterior cruciate ligament-retaining total knee arthroplasty 18 months ago. Extensive physiotherapy, dynamic splinting, and manipulations under anesthesia have failed to result in improvement. Examination reveals range of motion from 30 degrees to 60 degrees of flexion. The components are well fixed, and the evaluation for infection is negative. In discussing the possibility of revision arthroplasty, the patient should be advised that
Explanation
Explanation
Stiffness following primary total knee arthroplasty remains a vexing problem. Treatment options have included extensive physical therapy, dynamic splinting, manipulation under anesthesia, arthroscopic arthrolysis, open arthrolysis with polyethylene exchange, and ultimately revision arthroplasty. Results are not as gratifying as would be expected. Babis and associates performed an open arthrolysis and polyethylene exchange on seven patients who were followed for a mean of 4.2 months. The results were poor. The mean improvement in arc of motion was only 20 degrees. Nicholls and Dorr treated 13 patients for stiffness. Only 40% of those patients obtained good to excellent results. Four patients (30%) required manipulation because of recurrent stiffness postoperatively. They noted they could not predictably improve the arc of motion with a revision operation. Haidukewych and associates reported on 15 patients who underwent revision of well-fixed components after total knee arthroplasty for stiffness. Of the 15 patients, 10 (66%) were satisfied with the outcome revision. Interestingly, they noted that in patients for whom the total arc of motion did not improve but who regained near full extension, there was a greater amount of satisfaction with the procedure than for those who did not regain full extension. Babis GC, Trousdale RT, Pagnano MW, et al: Poor outcomes of isolated tibial insert exchange and arthrolysis for the management of stiffness following total knee arthroplasty. J Bone Joint Surg Am 2001;83:1534-1536. Nicholls DW, Dorr LD: Revision surgery for stiff total knee arthroplasty. J Arthroplasty 1990;5:S73-S77.
References:
- Haidukewych GJ, Jacofsky DJ, Pagnano MW, et al: Functional results after revision of well-fixed components for stiffness after primary total knee arthroplasty. J Arthroplasty 2005;20:133-138.
Question 8High Yield
A 24-year-old man sustains the injury shown in Figures 19a through 19e in a paragliding accident. He is neurologically intact. He also sustained fractures of his left femur and right distal radius. Which of the following represents the best option for management of the spinal injury?
Explanation
Explanation
19b 19c 19d 19e The injury pattern is that of a burst fracture at L1 contiguous with a compression fracture at T12. There is associated kyphosis and slight spondylolisthesis of T12 on L1. Treatment of this type of burst fracture in neurologically intact patients is somewhat controversial, with at least one study demonstrating equal long-term results comparing nonsurgical treatment to surgical treatment. In this study, however, body casts were used initially in the nonsurgical group. Moreover, because this patient has multiple fractures, spinal fracture stabilization should be considered to facilitate early mobilization. Surgical stabilization and fusion via a posterior approach is the best treatment option in this patient. Anterior decompression is not necessary since the patient is neurologically intact. McLain RF, Benson DR: Urgent surgical stabilization of spinal fractures in polytrauma patients. Spine 1999;24:1646-1654. Wood K, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit: A prospective, randomized study. J Bone Joint Surg Am 2003;85:773-781.
Question 9High Yield
What is the most common complication following total disk arthroplasty in the lumbar spine?
Explanation
Explanation
In a midterm (7 to 11 years) follow-up study of lumbar total disk arthroplasty, 5 of 55 patients had transient radicular leg pain without evidence of nerve root compression. Implant migration is rare. Deep venous thrombosis, incisional hernia, and retrograde ejaculation are less common complications of disk arthroplasty.
References:
- Tropiano P, Huang RC, Girardi FP, et al: Lumbar total disc replacement: Seven to eleven-year follow-up. J Bone Joint Surg Am 2005;87:490-496.
Question 10High Yield
A 20-year-old basketball player reports a 6-month history of right groin pain that radiates into his testicles with activities of daily living. He denies any history of trauma. Examination reveals tenderness about the groin, and he has full hip range of motion. The abdomen is soft. Radiographs are normal. Nonsurgical management has consisted of rest and physical therapy, but he continues to have pain. What is the next step in management?
Explanation
Sports hernias may be one of the most common causes of groin pain in athletes. Resisted hip adduction is painful in the case of groin disruption. Radiation of pain into the testicles and/or adductor region is often present. Sports hernias are associated with weakening of the posterior inguinal wall. In contrast with sports hernias, traditional or classic hernias can be readily detected on physical examination. Diagnostic imaging studies are not helpful and only serve to help exclude other diagnoses. Systemic high-dose steroids or sacroiliac joint injections have no role in treatment. High success rates have been reported for laparoscopic hernia repair in athletes. Kluin J, den Hoed PT, van Linschoten R, et al: Endoscopic evaluation and treatment of groin pain in the athlete. Am J Sports Med 2004;32:944-949. Genitsaris M, Goulimaris I, Sikas N: Laparoscopic repair of groin pain in athletes. Am J Sports Med 2004;32:1238-1242.
Question 11High Yield
Patients with rheumatoid arthritis may exhibit an increase in viral load for which of the following viruses?
Explanation
Explanation
Rheumatoid arthritis (RA) is a complex multisystem disorder. It has been suggested that patients with RA have an impaired capacity to control infection with Epstein-Barr virus. Epstein-Barr virus has oncogenic potential and is implicated in the development of some lymphomas. Recent publications provide evidence for an altered Epstein-Barr virus-host balance in patients with RA who have a relatively high Epstein-Barr virus load. Large epidemiologic studies confirm that lymphoma is more likely to develop in patients with RA than in the general population. The overall risk of development of lymphoma has not risen with the increased use of methotrexate or biologic agents. Histologic analysis reveals that most lymphomas in patients with RA are diffuse large B cell lymphomas, a form of non-Hodgkin lymphoma. Epstein-Barr virus is detected in a proportion of these. Patients with RA do not have prevalence for infection with any of the other mentioned viruses. Callan MF: Epstein-Barr virus, arthritis, and the development of lymphoma in arthritis patients. Curr Opin Rheumatol 2004;16:399-405.
References:
- Baecklund E, Sundstrom C, Ekbom A, et al: Lymphoma subtypes in patients with rheumatoid arthritis: Increased proportion of diffuse large B cell lymphoma. Arthritis Rheum 2003;48:1543-1550.
Question 12High Yield
A 32-year-old man sustained an L1 burst fracture with 90% canal compromise, intact posterior elements, and kyphosis of 25% at the L1 level. He has an incomplete neurologic injury. Definitive management should consist of
Explanation
Explanation
With an incomplete injury, the best chance for recovery occurs when the canal is cleared and the neural structures are decompressed. Anterior decompression, vertebral body reconstruction, and anterior stabilization have been shown to be highly effective in the treatment of burst-type injuries. Laminectomy alone is contraindicated because it increases the instability. Short segment posterior fixation has a high rate of failure in this type of injury at this level. Kaneda K, Abumi K: Burst fractures with neurologic deficits of the thoracolumbar spine. J Bone Joint Surg Am 1997;79:69-83.
References:
- McGuire R Jr: The role of anterior surgery in the treatment of thoracolumbar fractures. Orthopedics 1997;20:959-962.
Question 13High Yield
The rate of complications after in situ pinning of a chronic slipped capital femoral epiphysis is highest with placement of the screw in what quadrant of the femoral head?
Explanation
The rate of complications increases as the pin moves farther from the ideal position, which is the center of the head. This is the strongest argument for the use of a single pin. The highest rate of complications, primarily osteonecrosis and pin penetration, is associated with pin placement in the anterior superior quadrant. Raney EM, Ogden JA: Slipped capital femoral epiphysis. Current Ortho 1995;9:111-116.
Question 14High Yield
What radiographic measurement is best used to assess the adequacy of deformity correction for the patient shown in Figure 22?
Explanation
Explanation
Developmental coxa vara develops in early childhood and results in a progressive decrease in the proximal femoral neck-shaft angle with growth. The characteristic radiographic features are seen in this patient and include a decreased neck-shaft angle, a more vertical position of the physeal plate, and a triangular metaphyseal fragment in the inferior femoral neck, surrounded by an inverted radiolucent Y pattern. The main goal of surgery is to correct the varus angulation into a more normal range. Valgus overcorrection is preferred. A recent study emphasized the importance of adequately correcting the Hilgenreiner physeal angle to less than 38 degrees to minimize the risk of recurrent angulation. No study has documented the use of any of the other listed radiographic measurements to the outcome of treating developmental coxa vara. Carroll K, Coleman S, Stevens PM: Coxa vara: Surgical outcomes of valgus osteotomies. J Pediatr Orthop 1997;17:220-224.
References:
- Cordes S, Dickens DR, Cole WG: Correction of coxa vara in childhood: The use of Pauwels' Y-shaped osteotomy. J Bone Joint Surg Br 1991;73:3-6.
Question 15High Yield
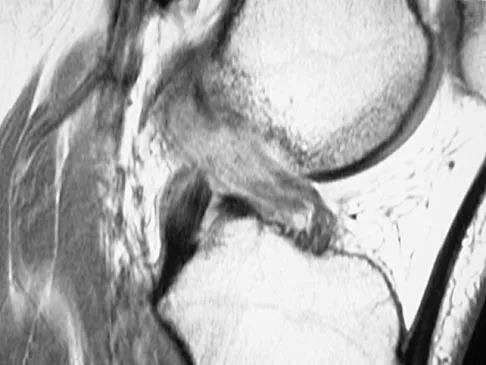
Figures 21a through 21c show the MRI scans of a 21-year-old football player who sustained a valgus knee injury while changing direction. Examination reveals swelling and tenderness along the medial aspect of the knee. There is a positive Lachman test, 3+ valgus laxity at 30 degrees, and 1+ valgus laxity at 0 degrees extension. The anterior drawer test is increased with the tibia in external rotation. The increase in the anterior drawer test with the tibia in external rotation is most likely the result of

Explanation
The injury mechanism involves a valgus load applied to the knee with the foot in external rotation. The primary stabilizer to valgus laxity is the medial collateral ligament. The secondary restraints to valgus rotation are the cruciate ligaments. Examination indicates disruption of the medial collateral and anterior cruciate ligaments. Valgus opening in extension should also arouse suspicion for an injury to the posterior cruciate ligament; however, in this patient, the valgus opening in extension is mild. The slight opening in extension and the increased anterior drawer, especially with external rotation, indicates disruption of the posteromedial capsule and posterior oblique ligament. Figure 21a shows complete disruption of the superficial and deep medial collateral ligaments involving the meniscofemoral ligament. Figure 21b shows a more posterior coronal section with a torn posterior oblique ligament. Figure 21c shows disruption of the anterior cruciate ligament, while the posterior cruciate ligament at the tibial insertion appears with a homogenous normal signal. Warren LA, Marshall JL, Girgis F: The prime static stabilizer of the medial side of the knee. J Bone Joint Surg Am 1974;56:665-674.
Question 16High Yield
A right-handed 20-year-old college baseball pitcher has had a 6-month history of vague right elbow pain while pitching. Examination reveals full flexion of the elbow and a loss of only a few degrees of full extension. The elbow is stable, but palpation reveals tenderness over the olecranon. Plain radiographs are inconclusive. MRI and CT scans are shown in Figures 20a and 20b. Management should consist of

Explanation
The patient has a stress fracture of the olecranon that occurs with repetitive throwing motions. If the fracture is not displaced, the initial treatment of choice is rest and rehabilitation to maintain elbow motion, followed by aggressive strengthening at 6 to 8 weeks. A light throwing program generally can begin at 8 to 12 weeks. Complete recovery may require 3 to 6 months. If the fracture is displaced or if nonsurgical management fails, surgery is indicated for internal fixation of the stress fracture. Azar FM, Wilk KE: Nonoperative treatment of the elbow in throwers. Oper Tech Sports Med 1996;4:91-99.
Question 17High Yield
Plots of stress versus strain for four orthopaedic biomaterials are shown in Figure 3. Referring to the figure, what is the correct identification of the curves?
Explanation
Stress-strain plots allow easy comparison of a number of important mechanical properties, including elastic modulus (the slope of the initial straight line portion of the curve) and yield stress (the stress at the break in the curves for bone, steel, and titanium alloy). Important considerations here are much lower modulus and ultimate stress of bone and cement compared to the two metallic alloys, the fact that titanium is lower modulus but higher strength than stainless steel, and the identification of cement as the only brittle material among the four. Burstein AH, Wright TM: Fundamentals of Orthopaedic Biomechanics. Baltimore, MD, Williams and Wilkins, 1994, pp 97-129.
Question 18High Yield
A patient is treated with volar plating for a distal radius fracture. The CT scan shown in Figure 15 is obtained after union of the fracture because the patient reports ongoing symptoms. The prominent hardware is most likely injuring what tendon?
Explanation
Explanation
Extensor tendon injuries have been reported after volar plating of distal radius fractures. The CT scan shows prominent dorsal hardware a few millimeters ulnar to Lister's tubercle. The second compartment, the ECRL and ECRB, is radial to Lister's tubercle. The ECU runs along the distal ulna. The contents of the fourth dorsal compartment run just ulnar to Lister's tubercle. The EDC tendon is likely irritated in this patient. The EPB runs along the radial border of the radius and is well away from prominent hardware. Benson EC, Decarvalho A, Mikola EA, et al: Two potential causes of EPL rupture after distal radius volar plate fixation. Clin Orthop Relat Res 2006;451:218-222.
References:
- Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist: Diagnosis and Operative Treatment. Philadelphia, PA, Mosby-Year Book, 1998.
Question 19High Yield
What is the most common adverse postoperative complication of laminoplasty for multilevel cervical spondylotic myelopathy?
Explanation
A 30% to 50% loss of cervical range of motion is reported postoperatively in most patients following cervical laminoplasty. Inadvertent closure of the laminoplasty does occur but is rare. Laminoplasty is advocated in lieu of laminectomy to prevent progressive kyphosis and can effectively decompress the spinal cord. C5 nerve root palsies are a poorly understood but rare complication of surgical decompression for cervical spondylotic myelopathy. Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Question 20High Yield
Sterilization of ultra-high molecular weight polyethylene by gamma irradiation in air will degrade its wear performance because of
Explanation
Explanation
Gamma irradiation has long been used as a sterilization method for polyethylene. Exposure to gamma irradiation causes breakage of the chemical bonds in the polyethylene, and oxidation will occur if the material is subsequently exposed to air. The amount of oxidation and decrease in wear performance is also related to the length of time that the gamma-irradiated polyethylene is exposed to oxygen. Collier JP, Sutula LC, Currier BH, et al: Overview of polyethylene as a bearing material: Comparison of sterilization methods. Clin Orthop 1996;333:76-86. McKellop H, Shen FW, Lu B, et al: Effect of sterilization method and other modifications on the wear resistance of acetabular cups made of ultra-high molecular weight polyethylene: A hip-simulator study. J Bone Joint Surg Am 2000;82:1708-1725.
References:
- Sychterz CJ, Young AM, Orishimo K, et al: The relationship between shelf life and in vivo wear for polyethylene acetabular liners. J Arthroplasty 2005;20:168-173.
Question 21High Yield
Where does the median nerve pass in the proximal forearm?
Explanation
Explanation
The median nerve passes through the pronator teres and deep to the flexor digitorum superficialis. The ulnar artery passes deep to both. Anderson JE (ed): Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Williams and Wilkins, 1978, pp 6-55.
References:
- Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 120.
Question 22High Yield
A 12-year-old girl who plays softball has chronic lateral hindfoot aching pain that is aggravated by weight-bearing activity. She reports that the pain has recurred after initial improvement with cast immobilization, and it continues to limit her overall level of activity. Radiographs are seen in Figures 40a through 40c. What is the most appropriate surgical treatment?
Explanation
Explanation
40b 40c The patient has a calcaneonavicular tarsal coalition. Symptoms of calcaneonavicular coalitions typically are seen between the ages of 10 and 14 years. The cause of pain has not been clearly established. It has been postulated that the coalition stiffens with maturity and microfractures can result, producing pain. Resection of a calcaneonavicular coalition generally has been associated with a satisfactory result. Soft-tissue interposition, most commonly using the extensor digitorum brevis muscle, appears to be helpful. A hindfoot arthrodesis (usually triple) would be reserved if coalition resection proves to be unsuccessful. Achilles tendon lengthening and orthotic support, as well as debridement of the sinus tarsi, are not expected to result in a satisfactory outcome. The patient does not have a flatfoot deformity. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 757-765.
Question 23High Yield
A 12-year-old boy reports the acute onset of pain and a pop over the right side of his pelvis while swinging a baseball bat during a Little League game. Radiographs reveal an avulsion of the anterior superior iliac spine with 2 cm of displacement. Management should consist of
Explanation
Anterior superior iliac spine avulsion fractures are caused by sudden, forceful contractions of the sartorius and tensor fascia lata. These injuries occur in young athletes through the growth plate with the hip extended and the knee flexed, such as while sprinting or swinging a baseball bat. The athlete will often report a pop or snap at the time of injury. Displaced fractures usually can be seen on radiographs. CT or MRI can be obtained to confirm the diagnosis. In most patients, nonsurgical management consisting of rest and protected weight bearing yields satisfactory outcomes. Surgery is usually reserved for fractures with displacement of more than 3 cm and painful nonunions. Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 139-153.
Question 24High Yield
A 53-year-old patient is seen in the emergency department after sustaining a fall onto her left hip. A current radiograph is shown in Figure 40. What is the best treatment option?
Explanation
The patient has sustained a Vancouver B2 periprosthetic femoral fracture (a femoral fracture that occurs around or just distal to a loose stem, with adequate proximal bone stock). The stem is no longer fixed to proximal bone; therefore, retention of the femoral component is not recommended. Nonsurgical management is contraindicated because of the high risk of nonunion and malunion with significant component settling in the distal fragment and leg shortening. Revision femoral arthoplasty must attain distal fixation in adequate host bone, which is usually successful with a porous-coated cylindrical stem. Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol for proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.
Question 25High Yield
A 35-year-old man has had a mass on the bottom of his foot for the past 6 months. He reports that initially the mass was exquisitely painful but now is minimally tender. Examination reveals a 2.5- x 2.0-cm firm, noncompressible, nonmobile mass contiguous with the plantar fascia in the distal arch. The mass is particularly prominent with passive dorsiflexion of the ankle and toes. What is the best course of action?
Explanation
The history is most consistent with a plantar fibroma. The nodules typically are located within the substance of the plantar aponeurosis. The clinical appearance is usually diagnostic without the need for advanced imaging studies. While the lesion may be prominent and painful to direct palpation, the anatomic location is usually off of the weight-bearing surface. Observation with or without an accommodative orthotic is the treatment of choice. Recurrence is common following attempted excision. Sammarco GJ, Mangone PG: Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21:563-569.
Question 26High Yield
Figure 36 shows the hip arthrogram of a newborn. Which of the following structures is enclosed by the circle?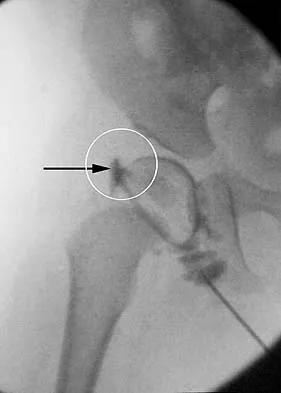
Explanation
The structure enclosed by the circle is the acetabular labrum. It is visible as the white point of tissue outlined by the darkly radiopaque contrast. The appearance of the contrast surrounding the sharp white point of a normal labrum is called the "rose thorn sign." The limbus is the term reserved for a rounded, infolded labrum seen with arthrography. The pulvinar is the fatty tissue seen in the empty acetabulum when the hip is dislocated. The ligamentum teres is seen as a white stripe outlined by contrast coursing from the central acetabulum to the dislocated femoral head. The transverse acetabular ligament courses across the inferior portion of the acetabulum and is not clearly seen with arthrography. Herring JA: Tachdjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 532-533.
Question 27High Yield
A 19-year-old man was struck by a car and is seen in the emergency department with a grade IIIC open distal tibia and fibula fracture. Examination reveals that the toes are cool and dusky with a sluggish capillary refill. Angiography reveals a lesion in the posterior tibial artery amenable to repair. There is no sensation on the plantar aspect of the foot, and he is unable to flex his toes. A clinical photograph and radiograph are shown in Figures 2a and 2b. What is the next most appropriate step in management?
Explanation
Explanation
2b In the past, loss of plantar sensation in this grade IIIC tibial fracture would have been an indication for below-knee amputation regardless of the potential for vascular repair. However the 2002 LEAP study divided 55 patients with loss of plantar sensation into two groups, the insensate amputation group and the insensate limb salvage group, with 55% of patients in the insensate salvage group regaining normal sensation 2 years after injury. Furthermore, those in the salvage group who remained insensate after 2 years had equivalent outcomes to those in the amputation group. Because of these findings, limb salvage with vascular repair and external stabilization with delayed closure is deemed appropriate treatment. Immediate intramedullary fixation is not indicated. Because ischemia, contusion, and stretch can adversely affect the tibial nerve, the additional insult of exploration of the nerve is also not advisable given the soft-tissue compromise. Bosse MJ, McCarthy ML, Jones AL, et al: The insensate foot following severe lower extremity trauma: An indication for amputation? J Bone Joint Surg Am 2005;87:2601-2608. Lange RH, Bach AW, Hansen ST Jr, et al: Open tibial fractures with associated vascular injuries: Prognosis for limb salvage. J Trauma 1985;25:203-208. Mackenzie EJ, Bosse MJ, Kellam JF, et al: Factors influencing the decision to amputate or reconstruct after high-energy lower extremity trauma. J Trauma 2002;52:641-649.
References:
- Baumgaertner MR, Tornetta P III (eds): Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 65-74.
Question 28High Yield
When performing a posterior cruciate ligament reconstruction with a tibial inlay-type approach, what is the approximate anatomic distance of the popliteal artery from the screws used for fixation of the bone block?
Explanation
Explanation
Miller and associates reported the results of a cadaveric study of the vascular risk of a posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. The average distance from the screw to the popliteal artery was 21.1 mm (range, 18.1 mm to 31.7 mm). Other approaches, such as the transtibial tunnel technique which involves drilling an anterior-posterior tunnel, have also been studied in cadavers. Matava and associates noted that increasing flexion reduces but does not completely eliminate the risk of arterial injury during arthroscopic posterior cruciate ligament reconstruction. However, this study did not use the small, medial utility incision recommended by Fanelli and associates, which creates an interval for the surgeon's finger between the medial gastrocnemius and the posteromedial capsule so that any migration of the guidepin can be palpated and changed prior to any injury to the posterior neurovascular bundle. Matava MJ, Sethi NS, Totty WG: Proximity of the posterior cruciate ligament insertion to the popliteal artery as a function of the knee flexion angle: Implications for posterior cruciate ligament reconstruction. Arthroscopy 2000;16:796-804. Miller MD, Kline AJ, Gonzales J, et al: Vascular risk associated with posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. J Knee Surg 2002;15:137-140.
References:
- Johnson DH, Fanelli GC, Miller MD: PCL 2002: Indications, double-bundle versus inlay technique and revision surgery. Arthroscopy 2002;18:40-52.
Question 29High Yield
A 25-year-old professional baseball pitcher reports a 4-month history of gradually increasing medial elbow pain that occurs during the late cocking and acceleration phases of throwing. The pain occasionally refers distally along the ulnar aspect of the forearm. He denies any weakness; however, he notes occasional paresthesias. A nerve conduction velocity study demonstrates increased latency across the cubital tunnel. Management consisting of 6 weeks of rest and rehabilitation fails to provide relief as the symptoms returned when he resumed throwing. What is the best course of action?
Explanation
In the thrower's elbow, ulnar neuritis is felt to result from both chronic compression and traction on the nerve that occurs during the throwing motion. Occasionally, subluxation of the nerve also can lead to symptoms. If nonsurgical management fails to provide relief, transposition of the nerve to an anterior subcutaneous location is the surgical procedure of choice. The nerve is held in its new position by one or two fascial slings created from the fascia of the common flexor origin. Schickendantz MS: Diagnosis and treatment of elbow disorders in the overhead athlete. Hand Clin 2002;18:65-75.
Question 30High Yield
A 65-year-old woman has significant neck pain after falling and striking her head. A radiograph and sagittal CT scan are shown in Figures 23a and 23b. What is the most likely diagnosis?
Explanation
Explanation
23b The radiograph shows a displacement of C5 on C6 of approximately 25%. The CT scan shows a perched facet at C5-6. There is no evidence of a facet fracture. A bilateral facet dislocation would show a displacement of more than 50%. Rothman RH, Simeone FA (eds): The Spine, ed 4. Philadelphia PA, WB Saunders, 1999, pp 927-937.
References:
- Vaccaro AR, Betz RR, Zeidman SM (eds): Principles and Practice of Spine Surgery. St Louis, MO, Mosby, 2003, pp 455-458.
Question 31High Yield
The natural history of cervical spondylolytic myelopathy is best described as
Explanation
Explanation
The natural history of cervical myelopathy has been described by Lees and Turner as exacerbations of symptoms followed by often long periods of static or deteriorating function (or very rarely improvement). This stepwise pattern of decreasing function has been corroborated by Clarke and Robinson. These authors described long periods of stable neurologic function, sometimes lasting for years, in about 75% of their patients. In the majority of the patients, however, the condition deteriorated between quiescent streaks. About 20% of their patients showed a slow, steady progression of symptoms and signs without a stable period, and 5% had rapid deterioration of neurologic function. Emery SF: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388. Lees F, Turner JA: The natural history and prognosis of cervical spondylosis. Brit Med J 1963;2:1607-1610.
References:
- Clarke E, Robinson PK: Cervical myelopathy: A complication of cervical spondylosis. Brain 1956;79:486-510.
Question 32High Yield
Which of the following bearing materials is most resistant to scratching from third-body debris?
Explanation
Alumina is the hardest of all the materials listed. Clinical retrieval demonstrates resistance to scratching from third-body debris.
Question 33High Yield
A 70-year-old man has worn through his metal-backed patellar component and sustained damage to the femoral component. Following removal of the components and debridement of the metal-stained synovium, the surgeon finds that the thickness of the remaining patella is 10 mm. Treatment should now include
Explanation
Revision of a failed patellar component can be difficult because of bone loss and damage to the extensor mechanism. Several authors have advised against reinsertion of a patellar component if the residual patellar thickness is 10 mm or less. Leaving an unresurfaced bony remnant in place at the time of revision or reimplantation surgery has been shown to be a reasonable option; however, the results are of a lower quality when compared with revision surgery where the patellar component can be retained or revised. The other treatment options have not been shown to be effective approaches to this problem. Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620. Pagnano MW, Scuderi GR, Insall JN: Patellar component resection in revision and reimplantation total knee arthroplasty. Clin Orthop 1998;356:134-138.
Question 34High Yield
The presence of S100B tumor marker typically corresponds with which of the following as being the most likely source of the metastasis?
Explanation
Advances in development of new tumor markers and techniques of antigen retrieval have enhanced the sensitivity and reliability of identifying the primary source of metastasis. New markers such as CK7, CK20, CA125, and thyroid transcription factor-1 (TTF-1) can help to determine the origin of an adenocarcinoma or aid in the recognition of other tumors. In patients who do not have an obvious primary site of disease or screening radiographs, these new markers can help focus the search for and guide the treatment of the underlying lesion. CA125 is positive in patients with ovarian cancer, CK7 is positive in patients with breast and lung carcinoma, and CK20 is indicative of colon carcinoma if the CK7 marker is negative. Gastrointestinal stromal tumor (GIST) is positive for CD117 (c-kit) and CD34, whereas 75% of bronchogenic carcinomas are positive for TTF-1. Histochemical staining of the S100 protein family has been used for many years in the diagnosis of malignant melanoma. Recent markers HMB-45, MART-1, and Melan-A have proved to be useful in diagnosis of melanoma. S100B protein has been implicated in downregulation of p53 (oncosuppressor gene). Harpio R, Einarsson R: S100 proteins as cancer biomarkers with focus on S100B in malignant melanoma. Clin Biochem 2004;37:512-518.
Question 35High Yield
Figures 28a and 28b show the sagittal and axial lumbar MRI scans of a 72-year-old man who reports dull aching back pain that spreads to his legs, calves, and buttocks. He has had the pain for several years and it is precipitated by standing and walking and relieved by sitting. His symptoms have been worsening over the past year and he notes that he is leaning forward while walking to help relieve his symptoms. He has had no treatment to date. What is his prognosis if he chooses to pursue nonsurgical management for this condition?

Explanation
The patient has lumbar spinal stenosis and the MRI scans reveal the pathology at L4-5, which is secondary to posterior disk bulging and hypertrophy and infolding of the ligamentum flavum, as well as degenerative facet arthrosis. The degree of spinal stenosis is moderate and his symptoms are positional in nature. Tadokoro and associates reported on a prospective study of 89 patients older than 70 years of age who underwent nonsurgical management for lumbar spinal stenosis. They found the prognosis to be relatively good with patients scoring at "excellent" or "good" for activities of daily living at final follow-up. However, they did note that patients with a complete block on myelography did not respond favorably to nonsurgical management. Amundsen and associates reported on a 10-year prospective study comparing surgical care to nonsurgical management. They concluded that, while the long-term results largely favored surgical treatment, more than half of the nonsurgically managed patients had a satisfactory outcome. They also concluded that a delay of surgery for some months did not worsen the prognosis. Therefore, their recommendation was for an initial primarily nonsurgical approach. Amundsen T, Weber H, Nordal HJ, et al: Lumbar spinal stenosis: Conservative or surgical management? A prospective 10-year study. Spine 2000;25:1424-1435. Hilibrand AS, Rand N: Degenerative lumbar stenosis: Diagnosis and management. J Am Acad Orthop Surg 1999;7:239-249.
Question 36High Yield
A 32-year-old powerlifter who was performing a dead lift 3 days ago noted a sharp pain in the front of his dominant right arm just after beginning to lower the weight. He now reports pain in the anterior aspect of the arm that worsens when he opens a door. Examination reveals moderate ecchymosis and swelling of the forearm and tenderness in the antecubital fossa. The MRI scans are shown in Figures 15a and 15b. If the injury is left unrepaired, the greatest functional deficit will most likely be the loss of
Explanation
Explanation
15b A complete tear of the distal biceps brachii most often occurs from a large, rapid eccentric elbow extension load. A pop or tearing sensation usually occurs, and a palpable defect in the antecubital fossa is often present on examination. The treatment of choice is a direct primary repair by a two-incision technique. If left unrepaired, the most disabling consequence is the loss of forearm supination strength. It is unlikely that significant elbow or forearm motion will be lost if the rupture is left unrepaired and early motion exercises are initiated. Elbow flexion strength tends to return with time, but the loss of forearm supination strength remains problematic. D'Alessandro DF, Shields CL Jr, Tibone JE, Chandler RW: Repair of distal biceps tendon ruptures in athletes. Am J Sports Med 1993;21:114-119.
References:
- Agins HJ, Chess JL, Hoekstra DV, Teitge RA: Rupture of the distal insertion of the biceps brachii tendon. Clin Orthop 1988;234:34-38.
Question 37High Yield
Figure 44 shows the radiograph of a 65-year-old man who underwent a revision arthroplasty to remove a loose, cemented femoral stem. When planning the postoperative restrictions, the surgeon should be aware that
Explanation
Explanation
The transfemoral approach, also known as the extended trochanteric osteotomy, is an important technique to master for revision hip surgery. When performed correctly, it allows excellent exposure of the femoral canal and aids in exposure of the acetabulum. As demonstrated in the study cited, however, it markedly reduces the torque that the composite can withstand without failure. This type of basic science study is important to guide postoperative rehabilitation.
References:
- Noble AR, Branham D, Willis M, et al: Mechanical effects of the extended trochanteric osteotomy. J Bone Joint Surg Am 2005;87:521-529.
Question 38High Yield
A 60-year-old man reports that he has had shoe pressure pain over his right great toe for several years but has minimal discomfort when barefoot or in sandals. A clinical photograph and radiographs are shown in Figures 1a through 1c. Management should consist of
Explanation
Explanation
1b 1c Some patients have minimal symptoms associated with hallux rigidus despite significant radiographic evidence of osteoarthritis. This patient's symptoms are primarily related to shoe pressure from the exostosis and can be managed with extra-depth shoe wear. Smith RW, Katchis SD, Ayson LC: Outcomes in hallux rigidus patients treated nonoperatively: A long-term follow-up study. Foot Ankle Int 2000;21:906-913.
References:
- Shereff MJ, Baumhauer JF: Hallux rigidus and osteoarthrosis of the first metatarsophalangeal joint. J Bone Joint Surg Am 1998;80:898-908.
Question 39High Yield
The dorsal (Thompson) approach to the proximal forearm uses which of the following intermuscular intervals?
Explanation
The Thompson posterior approach is used in treatment of fractures of the proximal radius. Dissection is carried out through the interval between the extensor carpi radialis brevis (radial nerve) and the extensor digitorum communis (posterior interosseous nerve). To identify this interval, the forearm is pronated and the mobile lateral wad of muscles (the ulnar-most belly is the extensor carpi radialis brevis) is grasped with the thumb and finger and pulled from the much less mobile mass of the extensor digitorum communis. The furrow created is marked with a skin marker for subsequent skin incision. The skin incision follows a line from the lateral epicondyle of the humerus to a point corresponding to the middle of the posterior aspect of the wrist. Distally, the intermuscular plane is between the extensor carpi radialis brevis and the extensor pollicis longus. Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 128-129. Hoppenfeld S, deBoer P: Posterior approach to the radius, in Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 136-146.
Question 40High Yield
A 66-year-old woman who requires a cane for ambulation now notes increasing difficulty in using the cane after undergoing total elbow arthroplasty 3 months ago. AP and lateral radiographs are shown in Figures 15a and 15b. What is the most likely diagnosis?

Explanation
The lateral radiograph reveals a triceps avulsion with a small portion of bone. Triceps weakness and insufficiency can be a symptomatic problem after total elbow arthroplasty and is probably underreported. Ulnar nerve neuritis, aseptic loosening, instability, and infection are all complications of total elbow arthroplasty but would not account for the radiographic findings. Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orhthopaedic Surgeons, 2002, pp 323-327.
Question 41High Yield
Figure 17 shows the radiograph of a 25-year-old professional football player who has superior shoulder pain that prevents him from sports participation. History reveals that he sustained a shoulder injury that was treated with closed reduction and temporary pinning 3 years ago. The best course of action should be
Explanation
The radiograph shows a complete acromioclavicular separation. Because the patient is a professional athlete who is unable to participate, surgery is indicated. Chronic separations, especially those with previous trauma from joint pinning, should be treated with resection of the distal clavicle and stabilization to the coracoid. Some type of biologic reconstruction of the coracoclavicular ligaments is generally recommended. Open repair of the ligaments is generally not possible in such a delayed fashion. Screw fixation alone will not provide a lasting solution as the screws usually need to be removed, leaving no fixation in place. Reconstruction using the coracoacromial ligament is generally recommended with coracoclavicular fixation to protect the repair while it heals. Nuber GW, Bowen MK: Disorders of the acromioclavicular joint: Pathophysiology, diagnosis and management, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999.
Question 42High Yield
The carpal tunnel canal is narrowest (smallest cross-sectional area) at what level?
Explanation
Explanation
The carpal tunnel canal has an hourglass shape in the coronal plane and is narrowest at the level of the hook of the hamate. Cobb TK, Dalley BK, Posteraro RH, et al: Anatomy of the flexor retinaculum. J Hand Surg Am 1993;18:91-99.
References:
- Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow and Shoulder. Rosemont, IL, American Society of Surgery of the Hand, 2003, p 300.
Question 43High Yield
Based on the findings seen at C5-6 in Figure 30, the most likely deficit for this patient will be weakness of the
Explanation
Explanation
A herniated cervical disk at C5-6 causes a C6 radiculopathy. There are eight cervical nerve roots and seven cervical vertebrae, and C8 exits between the C7 and T1 vertebrae. The C6 nerve root typically innervates the biceps and wrist extensor. The deltoid is predominantly innervated by C5. The wrist flexor and triceps are predominantly innervated by C7. Grip strength is predominantly a function of C8.
References:
- Hoppenfeld S: Evaluation of nerve root lesions involving the upper extremity, in Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-23.
Question 44High Yield
What is the most common foot deformity associated with myelomeningocele?
Explanation
Explanation
All of the above can be associated with myelomeningocele, but talipes equinovarus occurs in 50% to 90% of patients with myelomeningocele. Congenital vertical talus is rarely associated with any neuromuscular diseases other than myelomeningocele but is not the most common deformity in myelomeningocele. Stans AA, Kehl DK: The pediatric foot, in Baratz ME, Watson AD, Imbriglia JE (eds): Orthopaedic Surgery: The Essentials. New York, NY, Thieme, 1999, pp 702-703.
References:
- Lindseth RE: Myelomeningocele, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott, Williams & Wilkins, 2001, pp 622-628.
Question 45High Yield
A 30-year-old patient has had severe left hip pain and difficulty ambulating, necessitating the use of a cane, for the past 6 months. A photomicrograph of the femoral head sectioned at the time of surgery is shown in Figure 31. What is the most likely diagnosis?
Explanation
The photomicrograph demonstrates a wedge-shaped infarct with femoral head collapse; therefore, the diagnosis is osteonecrosis of the femoral head. Perthes disease and osteoarthritis do not involve a wedge-shaped defect. Tuberculosis of the hip joint results in greater destruction of the articular cartilage. Basset LW, Mirra JM, Cracchiolo A III: Ischemic necrosis of the femoral head: Correlation between magnetic resonance imaging and histologic sections. Clin Orthop 1987;223:181-187.
Question 46High Yield
Which of the following nutraceuticals has been associated with perioperative bleeding?
Explanation
Ginkgo biloba is a popular nutraceutical for patients who have early dementia, intermittent claudication secondary to peripheral vascular disease, vertigo, and tinnitus. It is reported to improve mental alertness and cognitive deficiency. It has antiplatelet properties as a result of one of its components, ginkgolide B, which displaces platelet-activating factor from its receptor binding sight. Rowin and Lewis reported on spontaneous bilateral subdural hematomas associated with chronic ginkgo biloba ingestion. Vale also reported on subarachnoid hemorrhage associated with ginkgo biloba. Bebbington and associates reported on persistent postoperative bleeding after total hip arthroplasty secondary to ginkgo biloba usage. Furthermore, the use of ginkgo biloba with aspirin or other antiplatelet agents or anticoagulants represents a relative contraindication. Physicians should be aware not only of prescribed medications but also alternative nutraceuticals that are used by the patient. Rowin J, Lewis SL: Spontaneous bilateral subdural hematomas associated with chronic ginkgo biloba ingestion. Neurology 1996;46:1775-1776. Vale S: Subarachnoid hemorrhage associated with ginkgo biloba. Lancet 1998;352:36.
Question 47High Yield
When compared with cobalt-chromium and stainless steel implants, a titanium implant has what biomechanical properties?
Explanation
Explanation
Titanium implants are commonly used in spinal surgery, especially when MRI may be needed after implantation. Titanium implants have a lower modulus of elasticity when compared with cobalt-chromium and stainless steel implants. This is felt to allow less stress shielding for these types of implants. The other properties do not apply to titanium implants.
References:
- Buckwalker JA, Einhorn TA, Simon SR (ed): Orthopedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 182-215.
Question 48High Yield
A patient has a displaced midshaft transverse fracture of the humerus and is neurologically intact. Following closed reduction and application of a coaptation splint, the patient cannot dorsiflex the wrist or the fingers at the metacarpophalangeal joints of the hand. What is the next most appropriate step in management?
Explanation
Explanation
The answer to this question is controversial. All of the standard textbooks state that development of a radial nerve palsy during initial fracture management may represent a laceration or injury of the nerve by bone fragments at the time of manipulation; therefore, surgery should be considered. However, it appears that there is no scientific basis for this decision. A review of the available literature shows that the results were the same for patients who were observed as for those who underwent radial nerve exploration. The indications for surgical exploration include palsies associated with open fractures, irreducible closed fractures, and vascular injuries. The only other relative indication for surgical exploration is following manipulation of a Holstein-Lewis fracture (a distal third fracture of the humerus with a lateral spike). In this type of fracture, exploration may be necessary if a closed reduction leads to radial nerve palsy because the spike may lacerate or compress the nerve. Observation for return of nerve function may be appropriate for 3 months or longer prior to considering late exploration. Bostman O, Bakalim G, Vainionpaa S, Wilppula E, Patiala H, Rokkanen P: Radial palsy in shaft fracture of the humerus. Acta Orthop Scand 1986;57:316-319. Shaz JJ, Bhatti NA: Radial nerve paralysis associated with the fractures of the humerus: A review of 62 cases. Clin Orthop 1983;172:171-176.
References:
- Holstein A, Lewis GB: Fractures of the humerus with radial nerve paralysis. J Bone Joint Surg Am 1963;458:1382-1388.
Question 49High Yield
A 13-year-old boy sustains a valgus stress injury to the knee while playing football, and he is unable to bear weight after the injury. Examination reveals tenderness medially superior to the joint line. The knee is held in flexion, and he has a large effusion and localized medial swelling. Plain radiographs show no obvious fracture. What is the next diagnostic step?
Explanation
Explanation
In the skeletally mature individual, this mechanism of injury will often result in a sprain of the medial collateral ligament. In skeletally immature patients, the same mechanism can cause a fracture of the distal femoral physis. If the fracture is nondisplaced, the plain radiographs may show only soft-tissue swelling or effusion. While the MRI scan may show edema in the soft tissues on the medial side of the knee and even an abnormality of the physis, stress radiographs provide a quicker and less expensive means of making the diagnosis. Arthroscopy and arthrography would not be helpful in making the diagnosis. Arthroscopy may result in further displacement of the injury. Smith L: Concealed injury to the knee. J Bone Joint Surg Am 1962;44:1659-1660.
References:
- Beaty JH, Kumar A: Fractures about the knee in children. J Bone Joint Surg Am 1994;76:1870-1880.
Question 50High Yield
Figures 31a and 31b show the radiograph and MRI scan of an otherwise normal 3-month-old infant who has a spinal deformity. MRI reveals no intraspinal anomalies. What is the next step in management?

Explanation
Congenital scoliosis in an infant warrants evaluation of the renal, cardiac, and neurologic systems because frequently there is concurrent pathology. Progression in this instance is possible but not certain; therefore, progression must be documented prior to any surgical intervention. Close observation with serial radiographs every 4 to 6 months is appropriate. All of the surgical options listed may be reasonable choices in the future, but cardiac evaluation is the most important issue at this time. Basu PS, Elsebaie H, Noordeen MH: Congenital spinal deformity: A comprehensive assessment at presentation. Spine 2002;27:2255-2259.
Question 51High Yield
Analysis of primary total hip arthroplasty using press-fit acetabular components without supplementary screw fixation reveals that screw fixation
Explanation
Using mechanical failure of fixation as the end point, Udomkiat and associates demonstrated a 12-year survivorship of 99.1% for titanium press-fit acetabular components without supplementary screw fixation. This study suggests that it is unlikely that the use of supplementary screws would lead to improved results. In addition, polyethylene wear debris tends to migrate through screw holes and along the course of screws. Screw holes also decrease the available surface for bone ingrowth. Screws that back up may be a source of backside polyethylene wear. This suggests that screw holes and the use of screws should be avoided when they are unnecessary for cup fixation.
Question 52High Yield
Atraumatic neuropathy of the suprascapular nerve usually occurs at what anatomic location?
Explanation
Explanation
The suprascapular nerve passes through the suprascapular notch and the spinoglenoid notch before innervating the infraspinatus muscle. At both locations, the suprascapular nerve is prone to nerve compression, which often results from a ganglion cyst. The other anatomic locations are not associated with suprascapular nerve impingement. Romeo AA, Rotenberg DD, Bach BR: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
References:
- Post M, Mayer J: Suprascapular nerve entrapment: Diagnosis and treatment. Clin Orthop 1987;223:126-136.
Question 53High Yield
A 36-year-old skier sustains a grade III posterior cruciate ligament (PCL) tear. Where will increased contact pressures develop over time?
Explanation
Complete rupture of the PCL leads to increased contact pressures in the patellofemoral and medial compartments of the knee. However, whether degenerative arthritis will develop and in which compartments still remains controversial.
Question 54High Yield
Initial postoperative management after repair of an acute rotator cuff tear includes
Explanation
Explanation
In the immediate postoperative period following repair of an acute rotator cuff tear, passive forward elevation and external rotation should be performed within the safe zone determined at surgery. Early active range of motion (prior to tendon healing), internal rotation behind the back, and resistive exercises increase the risk of rupture of the repair. Iannotti JP: Full-thickness rotator cuff tear: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
References:
- Bigliani LU, Cordasco FA, McIlveen ST, et al: Operative repair of massive rotator cuff tears: Long-term result. J Shoulder Elbow Surg 1992;1:120-130.
Question 55High Yield
Manipulation under anesthesia for resistant frozen shoulder should be avoided in patients with
Explanation
Severe osteoporosis is a contraindication to manipulation under anesthesia in patients with a resistant frozen shoulder because of the higher risk of humeral fracture. Manipulation is considered for frozen shoulder in patients who are symptomatic despite undergoing a reasonable course of appropriate physical therapy. Harryman DT II: Shoulder: Frozen and stiff. Instr Course Lect 1997;42:247-257.
Question 56High Yield
In revision total hip arthroplasty, an acetabular reconstruction cage is best indicated for which of the following patterns of bone loss?
Explanation
Explanation
Acetabular cage reconstruction is indicated in severe disruption of acetabular bone stock when a cementless acetabular component cannot be stabilized in intimate contact with a sufficient bed of structurally sound and viable host bone, with or without a structural graft. Cages are used in pelvic discontinuity where they provide a bridge between the ilium and the ischium, while supporting a cemented cup. All of the other scenarios are amenable to achieving an adequate rim fit for a cementless component, using a jumbo cup if necessary. Whiteside LA: Selection of acetabular component, in Steinberg ME, Garino JP (eds): Revision Total Hip Arthroplasty. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 209-220.
References:
- Berry DJ, Muller ME: Revision arthroplasty using an anti-protrusio cage for massive acetabular bone deficiency. J Bone Joint Surg Br 1992;74:711-715.
Question 57High Yield
What is the best initial screening test for a patient with a limb-length discrepancy?
Explanation
Explanation
With the patient standing, add blocks under the short leg until the pelvis is level, then measure the blocks to determine the discrepancy. This method is an accurate, simple, and inexpensive way to assess limb-length discrepancy. Differences of less than 2 cm need no treatment. Increasing discrepancy in a growing child should be followed clinically. Radiographic examination can include scanography, CT scanography, or a standing pelvic radiograph with the pelvis leveled. CT scanography is the most accurate diagnostic test when hip, knee, or ankle contractures are present. Herring JA: Tachdjian's Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, pp 1041-1045. Schoenecker PL, Rich MM: The lower extremity, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 1120-1122. Stanitski DF: Limb-length inequality: Assessment and treatment options. J Am Acad Orthop Surg 1999;7:143-153.
References:
- Aaron A, Weinstein D, Thickman D, Eilert R: Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg Am 1992;74:897-902.
Question 58High Yield
A 68-year-old woman who sustained a closed distal tibia fracture 2 years ago was initially treated with an external fixator across the ankle for 12 weeks, followed by intramedullary nailing of the fibula and lag screw fixation of the tibia. She continued to report persistent pain so she was treated with a brace and a bone stimulator. She now reports pain in her ankle. Examination reveals ankle range of motion of 8 degrees of dorsiflexion to 25 degrees of plantar flexion. She is neurovascularly intact. Current radiographs are shown in Figures 9a through 9c. What is the next most appropriate step in management?


Explanation
The patient has a nonunion of the distal fifth of the tibia. The nonunion appears to be oligotrophic, somewhere between atrophic and hypertrophic. Management requires stabilization and stimulation of the local biology, which can be accomplished with open reduction and internal fixation with bone grafting. Bracing or casting does not provide enough stability. Ultrasound bone stimulation has been shown to speed fresh fracture repair but is not indicated in nonunions. The distal segment is too short for intramedullary nailing. A fibular osteotomy alone would increase instability and, even with prolonged casting, would be unlikely to lead to successful repair. Carpenter CA, Jupiter JB: Blade plate reconstruction of metaphyseal nonunion of the tibia. Clin Orthop 1996;332:23-28. Lonner JH, Siliski JM, Jupiter JB, Lhowe DW: Posttraumatic nonunion of the proximal tibial metaphysis. Am J Orthop 1999;28:523-528. Stevenson S: Enhancement of fracture healing with autogenous and allogeneic bone grafts. Clin Orthop 1998;355:S239-S246.
Question 59High Yield
Which of the following is an advantage of unreamed nailing of the tibia compared to reamed nailing?
Explanation
Explanation
The debate between reamed versus unreamed intramedullary nailing of the tibia continues. Although unreamed nailing was proposed for open fractures to minimize infection, its simplicity made it appealing for closed fractures. However, most studies to date show that the only advantage of unreamed nailing is less surgical time. All studies show higher nonunion rates with increased hardware failure and increased time to union for unreamed nailing. Even in open fractures graded up to Gustilo Grade IIIA, the reamed tibial nail performs better. Larsen LB, Madsen JE, Hoiness PR, et al: Should insertion of intramedullary nails for tibial fractures be with or without reaming? A prospective, randomized study with 3.8 years' follow-up. J Orthop Trauma 2004;18:144-149.
References:
- Blachut PA, O'Brien PJ, Meek RN, et al: Interlocking intramedullary nailing with or without reaming for the treatment of closed fractures of the tibial shaft: A prospective randomized study. J Bone Joint Surg Am 1997;79:640-646.
Question 60High Yield
The injury shown in Figure 24 was most likely caused by what mechanism of injury?
Explanation
Explanation
The CT cut shows a fracture through the posterior portion of the iliac wing or a crescent fracture. This occurs after a laterally directed force is applied to the anterior part of the involved iliac wing.
Question 61High Yield
What process is often found associated with other neoplasms?
Explanation
Aneurysmal bone cyst may be either a "pattern" or a "diagnosis." Therefore, aneurysmal bone cyst should be viewed as a diagnosis of exclusion. Hemorrhage into a variety of primary bone lesions (eg, giant cell tumor of bone, chondroblastoma, osteoblastoma, fibrous dysplasia, osteosarcoma, or vascular neoplasms) may result in intralesional, membrane-bone blood-filled cysts. Such secondary changes may be confused with aneurysmal bone cyst, resulting in inappropriate therapy because assessment should be focused on identifying the underlying primary process. The entire specimen should be examined histologically in an effort to locate an underlying primary bone tumor. Bonakdarpour A, Levy WM, Aegerter E: Primary and secondary aneurysmal bone cyst: A radiological study of 75 cases. Radiology 1978;126:75-83. Levy WM, Miller AS, Bonakdarpour A, Aegerter E: Aneurysmal bone cyst secondary to other osseous lesions: Report of 57 cases. Am J Clin Pathol 1975;63:1-8.
Question 62High Yield
A 23-year-old professional baseball pitcher reports shoulder pain and decreased velocity while pitching. Physical examination reveals a side-to-side internal rotation deficit of 25 degrees. The O'Brien sign is negative; Neer and Hawkins signs are negative. Rotator cuff strength is full. Radiographs are unremarkable. What is the next step in management?
Explanation
Explanation
Throwing athletes with symptomatic internal rotation deficits often benefit from an intensive posterior capsular stretching program. Patients that fail to respond to nonsurgical management may benefit from an arthroscopic posterior capsular release. Wilk KE, Meister K, Andrews JR: Current concepts in rehabilitation of the overhead throwing athlete. Am J Sports Med 2002;30:136-151.
References:
- Myers JB, Laudner KG, Pasquale MR, et al: Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingement. Am J Sports Med 2006;34:385-391.
Question 63High Yield
Which of the following is considered the most useful screening method for the evaluation of protective foot sensation in a patient with diabetes mellitus?
Explanation
Patients with diabetes mellitus should be screened for the presence of protective foot sensation. In the absence of protective foot sensation, patients are at increased risk for the development of neuropathic ulcerations and neuropathic arthropathy. The most reliable screening tool for the presence of protective sensation is the ability to feel the 5.07 Semmes-Weinstein monofilament. Pinzur MS, Shields N, Trepman E, Dawson P, Evans A: Current practice patterns in the treatment of Charcot foot. Foot Ankle Int 2000;21:916-920.
Question 64High Yield
Figure 21 shows the tomogram of a 26-year-old woman who sustained an axial load injury to her neck in a fall off a horse. What ligament is injured?
Explanation
Levine and Edwards, in their description of the classic C1 burst (Jefferson) fracture, noted that spread of the lateral masses of more than 7 mm is indicative of a transverse ligament rupture. Long-term C1-C2 instability, however, has not been described with this fracture pattern. Although long-term traction followed by halo vest immobilization has been described as the best technique for achieving an ideal result, treatment of this injury remains somewhat controversial. Levine AM, Edwards CC: Fractures of the atlas. J Bone Joint Surg Am 1991;73:680-691.
Question 65High Yield
Figures 28a through 28d show the radiographs and MRI scans of a 20-year-old basketball player who sustained an inversion injury to his right ankle. Management should consist of
Explanation
Explanation
28b 28c 28d Osteochondral fractures involving the talar dome have been classified based on radiographic and MRI findings. A nondisplaced and incomplete fracture may be treated effectively with a short leg cast and no weight bearing for 6 weeks. This patient has a complete, separated, and displaced osteochondral fragment involving the midlateral talar dome that will most likely cause pain, mechanical symptoms, and effusion if treated nonsurgically. In addition, there is very little bone remaining on the fragment, making the likelihood of healing with open reduction and internal fixation problematic. The treatment of choice includes arthroscopy, removal of the loose fragment, curettage or drilling of the base, and a rehabilitation program that emphasizes peroneal strengthening, range of motion, and proprioceptive training. Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
References:
- Baker CL, Morales RW: Arthroscopic treatment of tranchondral talar dome fractures: A long-term follow-up study. Arthroscopy 1999;15:197-202.
Question 66High Yield
A 28-year-old man who sustained an ankle fracture in a motor vehicle accident underwent open reduction and internal fixation 3 months ago. He continues to report significant ankle pain with ambulation. Radiographs are shown in Figure 26. What is the next most appropriate step in management?
Explanation
The patient sustained a bimalleolar ankle fracture with a syndesmosis disruption. The initial open reduction and internal fixation did not successfully reduce the distal tibiofibular joint. The patient may need a derotational distraction osteotomy of the fibula to reduce the syndesmosis. The other procedures do not address the primary problem of the fibular malunion and syndesmosis malreduction. There is no radiographic evidence of significant arthritis; therefore, ankle arthrodesis is not indicated.
Question 67High Yield
Examination of a 7-year-old boy reveals 20 degrees of valgus following a lawn mower injury to the lateral femoral epiphysis. Treatment consists of total distal femoral epiphyseodesis and varus osteotomy. Following surgery, he has a limb-length discrepancy of 3 cm and 5 degrees of genu valgum. Assuming that he undergoes no further treatment, the patient's predicted limb-length discrepancy at maturity would be how many centimeters?
Explanation
The distal femoral epiphysis grows approximately 1 cm per year and in boys, growth ceases at approximately age 16 years. Therefore, the patient's limb-length discrepancy at maturity would be 12 cm (9 cm plus the 3-cm discrepancy he has from the previous surgery). Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphyseodesis. J Pediatr Orthop 1996;16:173-179.
Question 68High Yield
Figure 38 shows the radiograph of a 75-year-old woman who has had right shoulder pain, difficulty sleeping on the affected arm, and difficulties performing activities of daily living for the past 6 weeks. Initial nonsurgical management includes analgesics, a subacromial cortisone injection, and gentle range-of-motion exercises. However, these modalities have failed to provide relief, and the patient reports that she is unable to elevate her arm. Her pain is worse and she would like the most reliable treatment method for pain relief and functional improvement. What is the best surgical treatment?
Explanation
The authors of several studies conducted in Europe have reported promising results in the short- and medium-term with use of a reversed or inverted shoulder implant. The most recent investigation, a multicenter study in Europe in which 77 patients (80 shoulders) with glenohumeral osteoarthritis and a massive rupture of the rotator cuff were treated with the Delta III prosthesis, described an improvement in the mean constant score of 42 points, an increase of 65 degrees in forward elevation, and minimal or no pain in 96% of the patients. Hemiarthroplasty, the "nonconstrained" option, has long been the standard of care for rotator cuff tear arthropathy. However, careful examination of the literature reveals that the results have not been uniform. Favard L, Lautmann S, Sirveaux F, et al: Hemiarthroplasty versus reverse arthroplasty in the treatment of osteoarthritis with massive rotator cuff tear, in Walch G, Boileau P, Mole D (eds): 2000 Shoulder Prosthesis Two to Ten Year Follow-Up. Montpellier, France, Sauramps Medical, 2001, pp 261-268. Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Question 69High Yield
Based on the radiographic findings shown in Figure 41, which of the following wrist ligaments is most likely disrupted?
Explanation
The radiograph shows a diastasis of the scapholunate interval, caused by certain failure of the scapholunate interosseous ligament. The lunotriquetral interosseous ligament stabilizes the lunotriquetral joint. The long radiolunate ligament originates in the volar radius and inserts in the lunate. The short radiolunate ligament originates on the ulnar margin of the radius and inserts on the ulnar margin of the lunate. The ulnolunate ligament originates at the ulnar styloid base and inserts on the volar aspect of the lunate. Linscheid RL, Dobyns JH, Beabout JW, et al: Traumatic instability of the wrist: Diagnosis, classification, and pathomechanics. J Bone Joint Surg Am 1972;54:1612-1632. Mayfield JK, Johnson RP, Kilcoyne RK: Carpal dislocations: Pathomechanics and progressive perilunar instability. J Hand Surg Am 1980;5:226-241.
Question 70High Yield
Figure 2 shows the radiograph of a 26-year-old auto mechanic who injured his right dominant elbow in a fall during a motocross race. Examination reveals pain and catching that limits his range of motion to 45 degrees of supination and 20 degrees of pronation. The interosseous space and distal radioulnar joint are stable. Management should consist of
Explanation
Explanation
The radial head is an important secondary stabilizer of the elbow, helping to resist valgus forces. There has been a movement toward open reduction and internal fixation of the radial head when technically feasible, especially in a relatively high-demand athlete or laborer. The examination and radiograph suggest that displacement of the fragment is great enough to create a mechanical block. Extended splinting would only serve to encourage arthrofibrosis. Early range of motion is appropriate if there is minimal displacement of the radial head fragement, it is stable, and there is no mechanical block to motion. Fragments larger than one third of the joint surface should be excised only if it is not possible to reduce and repair the fragment. Primary excision of the radial head should be avoided if possible. Complications after excision of the radial head include muscle weakness, wrist pain, valgus elbow instability, heterotopic ossification, and arthritis. Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
References:
- Esser RD, Davis S, Taavao T: Fractures of the radial head treated by internal fixation: Late results in 26 cases. J Orthop Trauma 1995;9:318-323.
Question 71High Yield
A 24-year-old man was thrown from a car and is seen in the emergency department with a Glasgow Coma Scale (GCS) score of 8. A CT scan of the head shows no significant bleeding. The patient is hemodynamically stable. The left femur has the closed injury shown on the radiographs in Figures 53a and 53b. What is the best treatment for this patient?
Explanation
Explanation
53b Treatment of patients with a closed head injury and a femoral fracture remains controversial but recent data suggest that intramedullary nails done acutely with avoidance of intraoperative hypotension did not compromise the outcome related to the head injury. This was especially true for high-level GCS scores. A GCS score of lower than 8 and intraoperative hypotension have been associated with worsening outcomes following acute intramedullary nailing of the femur. Skin traction and distal femur skeletal traction in a young adult man with a femoral fracture is not well tolerated secondary to spasm and pain. External fixation is an option but an unnecessary step in the treatment of this patient. Ventriculostomy is not necessary in stable patients with no significant bleeding on a CT scan of the head. Starr AJ, Hunt JL, Chason DP, et al: Treatment of femur fracture with associated head injury. J Orthop Trauma 1998;12:38-45. Nau T, Kutscha-Lissberg F, Muellner T, et al: Effects of a femoral shaft fracture on multiply injured patients with a head injury. World J Surg 2003;27:365-369. McKee MD, Schemitsch EH, Vincent LO, et al: The effect of a femoral fracture on concomitant closed head injury in patients with multiple injuries. J Trauma 1997;42:1041-1045.
Question 72High Yield
In hip arthroplasty, the location of the medial femoral circumflex artery is best described as
Explanation
Explanation
The obturator artery lies closest to the transverse acetabular ligament. The femoral artery is closest to the anterior rim of the acetabulum. No named vessel lies within the substance of the gluteus minimus or superior to the piriformis tendon. The medial femoral circumflex artery lies medial or deep to the quadratus femoris muscle. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 1. Philadelphia, PA, JB Lippincott, 1984, Figure 7-53, p 346.
References:
- Callaghan JJ, Rosenberg AG, Rubash HE: The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, p 705.
Question 73High Yield
A 20-year-old woman has lateral foot and ankle pain after sustaining an inversion injury of the ankle while playing soccer 3 months ago. Activity modifications and physical therapy have failed to provide relief. She describes burning pain that extends from the anterior aspect of the ankle to the foot and lateral two toes. The pain is often worse at night. Plain radiographs, a bone scan, and an MRI scan are normal. Stress examination reveals no instability. What is the most likely diagnosis?
Explanation
Explanation
Persistent pain following an ankle sprain can present a diagnostic dilemma. All of the injuries listed should be considered in the differential diagnosis. The superficial peroneal nerve courses in the lateral compartment and exits the crural fascia 12 to 15 cm above the level of the ankle. Muscle herniation through the fascial defect has been reported to be associated with entrapment of this nerve. The fascial hiatus also may serve as a potential tether in cases of inversion injuries causing injury to the superficial peroneal nerve. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
References:
- Baumhauer JF: Superficial peroneal nerve entrapment. Foot Ankle Clin 1998;3:439-446.
Question 74High Yield
A 64-year-old man with a history of diabetes mellitus underwent open reduction and internal fixation of a displaced ankle fracture 8 weeks ago. Examination now reveals recent onset erythema, warmth, and swelling of the midfoot. Radiographs are shown in Figures 23a through 23d. What is the most likely reason for the swelling of the foot?



Explanation
A Charcot flare in adjacent joints is not uncommon in patients with neuropathy who undergo surgery or other trauma. Venous thrombosis would present with swelling of the entire leg, while infection would present earlier in the postoperative period. The radiographs are pathognomonic of Charcot arthropathy, not an unrecognized fracture or gout. A compartment syndrome this late after injury is extremely rare, and there would be no bony distraction associated with compartment syndrome.
Question 75High Yield
A 27-year-old man has neck pain after being involved in a motor vehicle accident. A lateral cervical radiograph is shown in Figure 21. What would be the most common neurologic finding?
Explanation
Explanation
The radiographic findings are consistent with a type II Hangman's fracture or traumatic spondylolisthesis of C2. This occurs with more than 3 mm of displacement according to the classification of Levine and Edwards. Even though the radiograph reveals significant displacement, the overall space available for the neural elements is increased, therefore minimizing the risk of neural compromise. Neurologic injury is most frequently encountered in type III injuries that are associated with bilateral facet dislocations of C2 on C3 but is infrequent in type I (less than 3 mm displacement) and type II traumatic spondylolisthesis. When neurologic deficits are associated with type II injuries, it is usually the result of an associated head injury. Cruciate paralysis occurs as a result of the crossover of the motor and sensory tracts at different levels of the cord at the C1-C2 junction. This results in normal sensation but complete loss of motor function. Levine AM: Traumatic spondylolisthesis of the axis (Hangman's fracture), in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 287-288.
References:
- Francis WR, Fielding JW, Hawkins RJ, Pepin J, Hensinger R: Traumatic spondylolisthesis of the axis. J Bone Joint Surg Br 1981;63:313-318.
Question 76High Yield
A 58-year-old patient who underwent bilateral hip arthroplasty 12 years ago now reports pain in his hips and difficulty with ambulation to the point where he now uses crutches. A radiograph of the hip and pelvis is shown in Figure 26. What is the best treatment option for this patient?
Explanation
Explanation
The radiographs reveal acetabular component failure with bone loss. There are several treatment options available. The best option for survivorship is a cementless porous-coated acetabular component. This patient may or may not require structural bone graft, which may need to be determined at the time of surgery. Bipolar implants and cemented acetabular components for revision surgery have not demonstrated long-term success. The use of a protrusio ring is reserved primarily for massive bone loss such as a Paprosky type III bone loss with significant superior migration of the acetabular component. The best clinical results for acetabular component revision have been achieved with cementless porous-coated implants. Haddad FS, Masri BA, Garbuz DS, et al: Acetabulum, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 923-936. D'Antonio JA: Periprosthetic bone loss of the acetabulum: Classification and management. Orthop Clin North Am 1992;23:279-290.
References:
- Rubash HE, Sinha RK, Paprosky W, et al: A new classification system for the management of acetabular osteolysis after total hip arthroplasty. Instr Course Lect 1999;48:37-42.
Question 77High Yield
A 25-year-old man has a mass on the medial aspect of the left knee. He reports that the mass has been present for several years, but a recent increase in physical activity has resulted in periodic tenderness. Radiographs are shown in Figures 13a and 13b. What is the most likely diagnosis?
Explanation
Explanation
13b The radiographs reveal a sessile lesion projecting from the medial aspect of the distal femur. The lesion shares the cortex with the bone and the base communicates with the medullary space of the femur. This is the classic appearance of an osteochondroma, the most common benign tumor of bone. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
References:
- Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 78High Yield
What is the primary indication for performing an arthroscopic synovectomy on a patient with hemophilia that is the result of factor VIII deficiency?
Explanation
Explanation
Improved medical management has changed musculoskeletal outcomes for individuals with hemophilia. Patients with severe hemophilia receiving prophylactic administration of factor VIII may never develop a target joint that requires further orthopaedic intervention. Patients with moderate hemophilia and those patients with severe hemophilia not receiving prophylactic treatment will still develop joints that have recurrent hemarthroses. When recurrent hemarthrosis continues despite optimal medical management, synovectomy is indicated. While synovectomy is predictable in its ability to decrease joint bleeding, it does not necessarily improve joint range of motion or prevent the development of hemophilic arthropathy over time. It will not reverse articular damage to the joint once it has developed. Dunn AL, Busch MT, Wyly JB; et al: Arthroscopic synovectomy for hemophilic joint disease in a pediatric population. J Pediatr Orthop 2004;24:414-426.
References:
- Journeycake JM, Miller KL, Anderson AM, et al: Arthroscopic synovectomy in children and adolescents with hemophilia. J Pediatr Hematol Oncol 2003;25:726-731.
Question 79High Yield
Figures 24a through 24c show the coronal T1-weighted, T2-weighted fat-saturated, and T1-weighted fat-saturated gadolinium MRI scans of the proximal thigh of a 52-year-old woman who reports a mass in the medial thigh and groin area. She notes that the fullness has grown in size over the course of many months. Based on these findings, what is the most likely diagnosis?
Explanation
Explanation
24b 24c The images show a complex, lobular lesion of the thigh that has signal characteristics that follow fat. The size of the lesion, the areas of stranding within the mass, along with mild uptake on the gadolinium sequences and the mild edema within the lesion on the T2-weighted image make liposarcoma the most likely diagnosis and simple intramuscular lipoma far less likely. All other diagnoses listed would not follow fat characteristics shown on the MRI sequences.
References:
- Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Question 80High Yield
What is the most common long-term complication of the fracture shown in Figure 32?
Explanation
Explanation
The fracture pattern shown in the radiograph involves both a talar neck fracture and a talar body fracture. The body fracture propagates into the subtalar joint, with significant risk for the development of arthritis in that surface even with an anatomic reduction. In addition, Canale and Kelly reported a 25% incidence of malunion of talar neck fractures, with varus angulation occurring most frequently. Of these patients, 50% required a secondary surgical procedure because of the development of degenerative joint disease of the subtalar joint. Canale ST, Kelly FB Jr: Fractures of the neck of the talus: Long-term evaluation of seventy-one cases. J Bone Joint Surg Am 1978;60:143-156.
References:
- Higgins TF, Baumgaertner MR: Diagnosis and treatment of fractures of the talus: A comprehensive review of the literature. Foot Ankle Int 1999;20:595-605.
Question 81High Yield
To adequately expose the volar plate of the proximal interphalangeal joint of the finger, which of following pulleys is typically incised?
Explanation
Explanation
Full exposure of the volar plate of the proximal interphalangeal joint of the finger is best accomplished by incision of the distal C1, A3, and proximal C2 pulleys; followed by gentle retraction of the flexor digitorum superficialis and profundus tendons. Sacrifice of the A3 pulley, although associated with some biomechanic disadvantage, can be tolerated without causing functionally limiting bowstringing of the flexor tendon. Sacrifice of even a portion of the A2 or A4 pulleys can decrease the biomechanic leverage provided by the flexor tendon sheath, leading to bowstringing of the flexor tendons. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 176-186. Strickland J: Flexor tendon-acute injuries, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 2, pp 1853-1855.
References:
- Lin GT, Amadio PC, An KN, et al: Functional anatomy of the human digital flexor pulley system. J Hand Surg Am 1989;14:949-956.
Question 82High Yield
In the anterior forearm approach to the distal radius (Henry approach), the radial artery is located between what two structures?
Explanation
The standard approach to the volar aspect of the distal radius is the Henry approach. Following incision of the skin and subcutaneous tissues, the forearm fascia is incised. The radial artery and venae comitantes lie in the interval between the tendons of the flexor carpi radialis muscle and the brachioradialis muscle. This interval is developed, and the radial artery and veins are retracted in a radial direction. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 83High Yield
Figure 8a shows the clinical photograph of an 83-year-old woman who has an enlarging left forearm mass. MRI scans are shown in Figures 8b and 8c. What is the next most appropriate step in management?
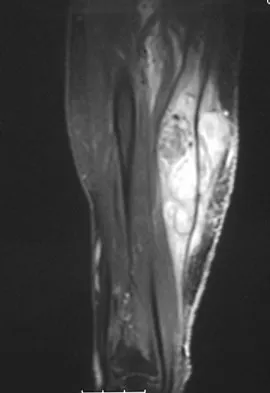
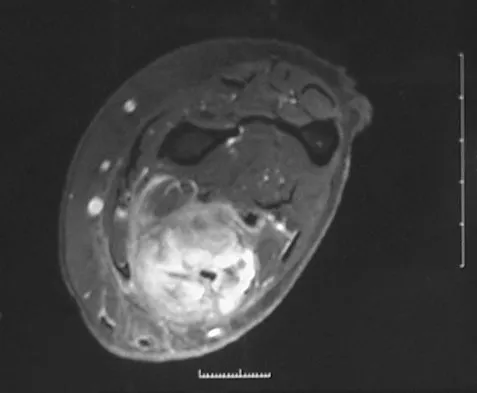
Explanation
Any large (greater than 5 cm), deep, heterogeneous mass in the extremities should be considered a sarcoma until proven otherwise. Sarcomas are rare, and without a high index of suspicion, the lesions may be misdiagnosed or there may be a delay in diagnosis. Needle biopsies can obtain sufficient tissue for diagnosis and are associated with less morbidity than open biopsy. Marginal resections or excisional biopsies should be reserved for a few select benign lesions and locations. Damron TA, Beauchamp CP, Rougraff BT, et al: Soft-tissue lumps and bumps. Instr Course Lect 2004;53:625-637.
Question 84High Yield
A 10-year-old child with cerebral palsy undergoes bilateral hamstring lengthening for severe knee flexion contractures, and knee immobilizers are applied postoperatively. Examination at the initial postoperative check 2 hours after surgery reveals that she can dorsiflex her toes on the right foot, but not on the left foot. The physician should now
Explanation
Explanation
Children with cerebral palsy are often difficult to examine. However, this patient clearly has a peroneal nerve deficit, most likely from the acute stretch after the hamstring lengthening. The nerve has the best chance of recovery if it is relaxed by flexing the knee. Once the nerve has recovered, gradual knee extension can be accomplished. Aspden RM, Porter RW: Nerve traction during correction of knee flexion deformity: A case report and calculation. J Bone Joint Surg Br 1994;76:471-473.
References:
- Heydarian K, Akbarnia BA, Jabalameli M, Tabador K: Posterior capsulotomy for the treatment of severe flexion contractures of the knee. J Pediatr Orthop 1984;4:700-704.
Question 85High Yield
Figures 5a and 5b show axial and coronal MRI images of the left ankle of a patient with lateral ankle pain. What is the most likely diagnosis?

Explanation
The figures show a longitudinal split within the peroneus brevis tendon as it courses posterior to the fibula. The peroneus longus tendon has been driven between the medial and lateral components of the peroneus brevis tendon. Peroneal split syndrome is a cause of lateral ankle pain but may be less asymptomatic in the elderly. It may be associated with tendon subluxation following a tear of the superior peroneal retinaculum.
Question 86High Yield
A 28-year-old woman sustained an injury to her dominant right arm after falling off her porch. Examination reveals a deformity at the elbow. She is neurovascularly intact. Figures 46a and 46b show the radiographs obtained before closed reduction, and postreduction radiographs are shown in Figure 46c and 46d. What is the most likely early complication?
Explanation
Explanation
00 46a 46b 46c 46d The patient has a complex fracture-dislocation of the elbow. The radial head is fractured, and there is a displaced coronoid fracture. These associated fractures indicate that the elbow is at high risk for recurrent instability after initial treatment. To prevent this complication, surgical treatment will most likely be required and will consist of some or all of the following: radial head open reduction and internal fixation or replacement, coronoid open reduction and internal fixation, medial and lateral ligament repairs, and even articulated external fixation. This patient was treated with open reduction and internal fixation of the radial head, and the elbow redislocated postoperatively. Ring D, Jupiter JB: Reconstruction of posttraumatic elbow instability. Clin Orthop 2000;370:44-56. O'Driscoll SW: Classification and evaluation of recurrent instability of the elbow. Clin Orthop 2000;370:34-43.
References:
- O'Driscoll SW, Morrey BF, Korinek S, An KN: Elbow subluxation and dislocation. Clin Orthop 1992;280:186-197.
Question 87High Yield
A 45-year-old man with a painful varus knee is being considered for an upper tibial osteotomy. Which of the following factors is considered the most compelling argument against this procedure?
Explanation
Proximal tibial osteotomy is appropriate for the younger and/or athletic patient who has mild to moderate medial compartment osteoarthritis. Relative contraindications include limited range of motion (eg, flexion contracture of 15 degrees), anatomic varus of greater than 10 degrees, advanced patellofemoral arthritis, and tibial subluxation. Inflammatory arthritides involve all the compartments and are a contraindication to osteotomies around the knee.
Question 88High Yield
A 12-year-old boy who has had a 1-month history of right thigh pain and a limp reports worsening of the pain after a fall, and he can no longer walk or bear weight on the involved extremity. Radiographs of the pelvis reveal a slipped capital femoral epiphysis with moderate to severe displacement. While positioning the patient on the fracture table for screw fixation, partial reduction of the slip is achieved. No further reduction maneuvers are attempted, and the epiphysis is stabilized with a single cannulated screw. What complication is most likely to develop following this procedure?
Explanation
Explanation
Traditional classification of slipped capital femoral epiphyses is based on the following temporal criteria: acute (symptoms that persist for less than 3 weeks); chronic (symptoms that persist for more than 3 weeks); or acute on chronic (acute exacerbation of long-standing symptoms). A newer classification differentiates between a stable slip where weight bearing is possible, and an unstable slip if it is not. Reduction of an unstable slip often occurs unintentionally with induction of anesthesia and positioning of the patient for surgery. The rate of satisfactory results is lower primarily because of a much higher incidence of osteonecrosis following internal fixation of an unstable slip. Loder RT, Richards BS, Shapiro PS, Reznick LR, Aronson DD: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
References:
- Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 151-159.
Question 89High Yield
A 29-year-old man undergoes surgery for a grade I isthmic spondylolisthesis at L5. Following surgery, what type of brace will best immobilize the L5-S1 motion segment?
Explanation
Explanation
The thoracolumbosacral orthosis with thigh extension best immobilizes the lumbosacral junction. Fidler and Plasmans have demonstrated increased motion at the lumbosacral junction with the standard chairback-type brace. Connolly PJ, Grob D: Bracing of patients after fusion for degenerative problems of the lumbar spine: Yes or no? Spine 1998;23:1426-1428.
References:
- Fidler MW, Plasmans CM: The effect of four types of support on the segmental mobility of the lumbosacral spine. J Bone Joint Surg Am 1983;65:943-947.
Question 90High Yield
A 20-year-old football player has immediate pain in the midfoot and is unable to bear weight after an opposing player lands on the back of his plantar flexed foot. AP and lateral radiographs are shown in Figures 4a and 4b. Management should consist of
Explanation
Explanation
4b The history and radiographs indicate a Lisfranc fracture-dislocation of the foot. The radiographs show the classic "fleck sign," which is an avulsion of the Lisfranc ligament from the base of the second metatarsal. Most authors recommend open reduction and internal fixation of this injury. Closed reduction can be attempted, but anatomic reduction is unlikely because of the interposed bone fragments and soft tissues. Standard radiographs are not reliable in identifying 1 to 2 mm of subluxation of the tarsometatarsal joint. The tarsometatarsal joint has a poor tolerance to even mild subluxation, and the resulting decrease in joint contact area increases the likelihood of posttraumatic arthritis. Open reduction with the joint visible allows more anatomic reduction and internal fixation of larger osteochondral fragments or excision of smaller interposed fragments. Bellabarba C, Sanders R: Dislocations of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 2, pp 1539-1558.
References:
- Murphy GA: Fractures and dislocations of the foot, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 9. St Louis, MO, Mosby, 1998, vol 2, pp 1956-1960.
Question 91High Yield
When 6 weeks of noninvasive nonsurgical management fails to provide relief for a lumbar disk herniation, a trial of epidural steroid injections is likely to yield which of the following results?
Explanation
Explanation
Lumbar epidural steroid injections appear to play a role in management of a lumbar disk herniation that has failed to respond to at least 6 weeks of nonsurgical treatment. Approximately 42% to 56% of patients report significant pain relief compared with 92% to 98% of those patients treated with diskectomy. Patients with extruded or sequestered herniations report the greatest and most rapid relief. Similarly, those with well-hydrated disk fragments report rapid relief of symptoms. A smaller percentage of patients report symptom relief compared with those having surgery, but the degree of improvement is similar for both groups and the improvement lasts up to 3 years. Butterman GR: Treatment of lumbar disc herniation: Epidural steroid injection compares with discectomy: A prospective, randomized study. J Bone Joint Surg Am 2004;86:670-679.
References:
- Butterman GR: Lumbar disc herniation regression after successful epidural steroid injection. J Spinal Disord Tech 2002;15:469-476.
Question 92High Yield
Figures 21a and 21b show the radiographs of a 22-year-old man who has had progressive pain and swelling about the knee for the past 6 weeks. Examination reveals limited range of motion and fullness about the knee. What is the most likely diagnosis?
Explanation
Explanation
21b The radiographs reveal a destructive lesion in the metaphysis of the distal femur with periosteal changes and an associated soft-tissue mass with subtle mineralization. This suggests an aggressive malignant process. In this age group, the most likely diagnosis is osteosarcoma. Giant cell tumor, which usually is in a more subchondral location, is not typically so aggressive. Aneurysmal bone cyst is usually more geographic, with a well-marginated reactive rim. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
References:
- Resnick D, Kyriakos M, Greenway GD: Tumors and tumor-like lesions of bone: Imaging and pathology of specific lesions, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 3800-3833.
Question 93High Yield
What is the most frequent complication following primary total hip arthroplasty?
Explanation
Thromboembolic disease can occur in up to 58% of unprotected patients and up to 20% of protected patients depending on the type of prophylaxis used, even though most thrombi are small and have little clinical consequence. The primary goal of prophylaxis is to prevent symptomatic deep venous thrombosis and fatal pulmonary emboli. Dislocation has been reported in up to 10% of primary cases, but generally acceptable rates of less than 5% are the norm. Component loosening following primary total hip arthroplasty is rare prior to a 10-year follow-up, and 90% to 95% of patients should reach the 10-year follow-up without the need for revision for any reason. Metal hypersensitivity is unusual, and nickel found in cobalt-chromium alloys is the most common offending agent. Infection of primary total hip arthroplasty is less than 1%. Eftekhar N: Total Hip Arthroplasty. St Louis, MO, Mosby,1993, pp 1445-1676.
Question 94High Yield
A 36-year-old man sustains a traumatic spondylolisthesis of L5 on S1. Surgical stabilization requires pedicular fixation into the sacrum. If the screw is placed in a medial to lateral direction and penetrates the sacral ala, what nerve root is at risk?
Explanation
Explanation
The L5 nerve root lies directly over the superior and anterior alae. If the screw is directed approximately 20 degrees laterally and bicortical purchase is achieved, there is the risk of injuring the L5 nerve root. If the screw is directed medially into the body of S1, there is little risk of injury. The same root is at risk during placement of an iliosacral screw. Ebraheim NA, et al: Lumbosacral nerve and dorsal screw placement. Orthopedics 2000;23:245-247. Ebraheim NA, Mermer M, Xu R, Yeasting RA: Radiological evaluation of S1 dorsal screw placement. J Spinal Disord 1996;9:527-535.
References:
- Routt ML Jr, Nork SE, Mills WJ: Percutaneous fixation of pelvic ring disruptions. Clin Orthop 2000;375:15-29.
Question 95High Yield
A 2-year-old child has marked hypotonia and depressed reflexes. History reveals that the child was normal at birth and developed normally for the first year. The child also began to ambulate, but lost this ability during the next 6 months. Laboratory studies show a creatine phosphokinase level that is within the normal range. DNA testing confirms a deletion in the survival motor neuron (SMN) gene. What is the most likely diagnosis?
Explanation
The patient has spinal muscular atrophy, type 2. This type is intermediate in severity between the Werdnig-Hoffmann type (type 1) and the Kugelberg-Welander type (type 3). It normally manifests itself between the ages of 3 and 15 months. Survival until adolescence is common. All three types of spinal muscular atrophy have been linked to the SMN gene at the 5q12.2-13.3 locus. DNA testing is available and is preferred to muscle biopsy because it is less invasive and more definitive. Biros I, Forrest S: Spinal muscular atrophy: Untangling the knot? J Med Genet 1999;36:1-8.
Question 96High Yield
Figure 24 shows the radiograph of a 4-year-old girl with spina bifida. Examination reveals an L3 motor level, excellent sitting and standing balance, and satisfactory range of motion at the hips. Management should consist of
Explanation
Explanation
Children with spina bifida and bilateral symmetrical dislocation of the hips usually do not require treatment. A level pelvis and good range of motion of the hips are more important for ambulation than reduction of bilateral hip dislocations. Because the patient has good sitting and standing balance and good range of motion, maintenance of that range of motion and symmetry is more important than reduction. Surgery is not recommended.
References:
- Heeg M, Broughton NS, Menelaus MB: Bilateral dislocation of the hip in spina bifida: A long-term follow-up study. J Pediatr Orthop 1998;18:434-436.
Question 97High Yield
Figures 36a and 36b show the radiographs of a 48-year-old woman who smokes cigarettes and sustained a segmental femoral shaft fracture in a motor vehicle accident 9 months ago. Initial management consisted of stabilization with a reamed statically locked intramedullary nail. She now reports lower leg pain that increases with activity. In addition to advising the patient to quit smoking, management should include

Explanation
The patient has an oligotrophic nonunion of the distal femoral fracture. Although the proximal fracture appears incompletely united, it was stable at exchange nailing. The treatment of choice is exchange reamed nailing to at least 2 mm above the nail in place. Bone grafting is debatable. Recent studies have shown a 70% to 75% success rate with exchange nailing only, so in nonhypertrophic nonunions, bone grafting can be considered. Nonsurgical management consisting of observation or external stimulation runs the risk of implant failure. Plate fixation is acceptable but is considered a second choice because of the need to consider stabilization of the proximal fracture until union is achieved. Also, plate fixation definitely requires bone grafting. Webb LX, Winquist RA, Hansen ST: Intramedullary nailing and reaming for delayed union or nonunion of the femoral shaft: A report of 105 consecutive cases. Clin Orthop 1986;212:133-141. Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nailing for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.
Question 98High Yield
A 10-month-old girl has the spinal deformity shown in Figures 55a and 55b with no apparent neurologic finding. The next step in evaluation should be to obtain
Explanation
Explanation
55b Approximately 60% of patients with a congenital spine abnormality have associated malformations outside the spinal column. Genitourinary abnormalities are probably the most common, occurring in up to 37% of patients. These are usually anatomic anomalies, such as renal agenesis, duplication, fusion, and ectopia. A genitourinary ultrasound is the least invasive screening tool. Other associated anomalies include cervical vertebral abnormalities, VATER syndrome, and intraspinal abnormalities such as diastematomyelia. An MRI scan is not recommended as part of the screening examination; however, if the patient had neurologic signs or symptoms, an MRI scan would be indicated. Beals RK, Robbins JR, Rolfe B: Anomalies associated with vertebral malformations. Spine 1993;18:1329-1332.
References:
- Bradford DS, Heithoff KB, Cohen M: Intraspinal abnormalities and congenital spine deformities: A radiographic and MRI study. J Pediatr Orthop 1991;11:36-41.
Question 99High Yield
Figure 17 shows the radiograph of an 11-year-old boy with Duchenne muscular dystrophy who has been nonambulatory for the past 2 years. Management of the spinal deformity should consist of
Explanation
Explanation
The presence of any curve greater than 20 degrees in a nonambulatory patient with Duchenne muscular dystrophy is an indication for posterior fusion with instrumentation. Because of progressive cardiomyopathy and pulmonary deficiency, waiting until the curve is larger can increase the risk of pulmonary or cardiac complications during or following surgery. There is some disagreement as to whether all such fusions must extend to the pelvis. Bracing or other nonsurgical management is ineffective and is not indicated in this situation. Sussman M: Duchenne muscular dystrophy. J Am Acad Orthop Surg 2002;10:138-151.
References:
- Mubarek SJ, Morin WD, Leach J: Spinal fusion in Duchenne muscular dystrophy: Fixation and fusion to the sacropelvis? J Pediatr Orthop 1993;13:752-757.
Question 100High Yield
A 21-year-old college defensive lineman sustains a minimally displaced (less than 1 mm) midthird scaphoid fracture during the first game of the season. Management should consist of
Explanation
Explanation
The union rate for minimally displaced midthird scaphoid fractures is quite high with cast immobilization while allowing a return to sports. Inadequate immobilization results in a much higher nonunion rate. Early fixation and rehabilitation have been proposed for sports or positions that are not amenable to cast immobilization. While immobilization of a nondisplaced fracture results in an acceptably high union rate, there is no advantage to fixation in conjunction with immobilization in the course of healing. With adequate immobilization and protection, play restrictions until healing has occurred are unnecessary. Rettig AC, Kollias SC: Internal fixation of acute stable scaphoid fractures in the athlete. Am J Sports Med 1996;24:182-186. Rettig AC, Weidenbener EJ, Gloyeske R: Alternative management in midthird scaphoid fractures in the athlete. Am J Sports Med 1994;22:711-714.
References:
- Riester JN, Baker BE, Mosher JF, Lowe D: A review of scaphoid fracture healing in competitive athletes. Am J Sports Med 1985;13:159-161.
You Might Also Like
Previous ChapterOrthopedic Board Exam Set 787: 100 High-Yield MCQs for ABOS…
Next Chapter Orthopedic Board Review: Mock Exam Set 405 – 100 High-Yield…

Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon