Orthopedic Board Review MCQs: Set 493 - 100 High-Yield Practice Questions for ABOS & OITE
14 Apr 2026
108 min read
96 Views
Key Takeaway
This page offers Mock Exam Set #493, comprising 100 high-yield orthopedic surgery MCQs. Tailored for ABOS, OITE, and FRCS board exam preparation, these randomized questions help surgeons thoroughly test their knowledge and master key concepts for certification success.
Anterior Transthoracic Approach: Comprehensiv...
00:00
Start Quiz
Question 1High Yield
A 38-year-old man has an enlarging left paraspinal soft-tissue mass. Based on the MRI scans and biopsy specimens shown in Figures 32a through 32e, what is the most likely diagnosis?
Explanation
Explanation
32b 32c 32d 32e Fibromatosis is a benign but aggressive fibrous lesion that principally arises from the connective tissue of muscle and the overlying fascia. The peak incidence is between the ages of 25 and 35 years. Most patients have a deep-seated, firm, poorly circumscribed mass that has grown insidiously and causes little or no pain. MRI is helpful in diagnosing the lesion and in assessing the extent of disease prior to surgical intervention. Histologically, the lesion is poorly circumscribed and infiltrates the surrounding tissue. The lesion appears bland with uniform spindle cells separated by abundant collagen, with little or no cell-to-cell contact. Despite its bland microscopic appearance, the tumor frequently behaves in an aggressive manner. These lesions do not metastasize but have a high incidence of recurrence. Treatment options consist of surgical resection, radiation therapy, chemotherapeutic protocols, hormone modulation, and/or anti-inflammatory medications. Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss's Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 309-337.
References:
- Spear MA, Jennings LC, Mankin HJ, et al: Individualizing management of aggressive fibromatoses. Int J Radiat Oncol Biol Phys 1998;40:637-645.
Question 2High Yield
A 10-year-old boy who has had progressive low back and right buttock pain for the past 3 days is now unable to bear weight on the right side secondary to pain. He has a temperature of 101.3 degrees F (38.5 degrees C). Examination reveals full hip range of motion; but he reports pain on the right side with external rotation. Pain is elicited with compression of the iliac wings and with direct palpation of the right sacroiliac (SI) joint. An MRI scan of the pelvis shows no abscess, but there is inflammation of the SI joint. Management should consist of
Explanation
Explanation
The clinical presentation and MRI findings are consistent with an acute infection of the SI joint. Bed rest and nonsteroidal anti-inflammatory drugs alone are insufficient to treat the problem. Staphylococcus aureus is the causative organism in most of these infections; therefore, unless there is an unusual factor in the history such as IV drug use, immune system compromise, or unusual travel, SI joint aspiration is unnecessary. It is often difficult to enter the SI joint, even under radiographic guidance. Management should consist of hospital admission and IV antibiotics. Blood cultures may be positive and should be obtained prior to starting antibiotics. Surgical fusion of the SI joint is not indicated. Morrissey RT: Bone and Joint Sepsis in Pediatric Orthopaedics. Philadelphia, PA, JB Lippincott, 1990. Beaupre A, Carroll N: The three syndromes of iliac osteomyelitis in children. J Bone Joint Surg Am 1979;61:1087-1092.
References:
- Reilly JP, Gross RH, Emans JB, Yngve DA: Disorders of the sacro-iliac joint in children. J Bone Joint Surg Am 1988;70:31-40.
Question 3High Yield
In Charcot-Marie-Tooth disease a progressive deformity develops in the foot. Which functional muscles predominate in deformity formation?
Explanation
In Charcot-Marie-Tooth disease, the posterior tibialis and peroneus longus tendons remain strong, serving to invert the hindfoot and depress the first metatarsal head thus causing the cavovarus foot associated with this disease. In contrast, the tibialis anterior and peroneus brevis are less functional and therefore cannot dorsiflex the ankle, elevate the first metatarsal, or evert the foot, contributing to the deformity.
Question 4High Yield
A patient undergoes cartilage implantation requiring amplification of donor cells. Which of the following statements best describes the transplants?
Explanation
Chondrocytes are obtained from cartilage harvested from non-weight-bearing areas of the knee. The extracellular matrix is digested, and the chondrocytes are expanded for later transplantation. Cells implanted into a defect are secured with a flap of periosteum. Cells are expanded to obtain 20 to 50 times the original number of cells to transplant at a cell density of 3x10-7 cells/mL. There is a direct relationship between cell number and biosynthetic activity. Osteochondral lesions of up to 8 mm may be treated with autologous transplant alone; larger depth lesions should be bone grafted at the time of harvest. Mesenchymal stem cells differentiate easily into fibrous tissue, bone, and fat; conversion of mesenchymal stem cells into cartilage in vitro currently is difficult to accomplish. Goldberg and Caplan, however, were able to obtain cartilage repair using mesenchymal stem cells transplanted into defects in rabbits in vivo. In animal studies, fluorescent-labeled cells persist for at least 14 weeks, integrate with the surrounding normal margins, and become part of the repaired tissue replete with sulfated proteoglycans and type II collagen. Brittberg M, Peterson L, Sjogren-Jansson E, et al: Articular cartilage engineering with autologous chondrocyte transplantation. J Bone Joint Surg Am 2003;85:109-115.
Question 5High Yield
A 23-year-old college basketball player reports persistent lateral ankle pain after sustaining an inversion injury 6 months ago. Examination reveals pain over the anterolateral ankle, absence of swelling, and no clinical instability. Management consisting of vigorous physical therapy fails to provide relief, and a intra-articular corticosteroid injection provides only temporary relief. Radiographs obtained at the time of injury and subsequent AP and varus stress views are normal. A recent MRI scan fails to show any abnormalities. Management should now include
Explanation
Explanation
Because the patient has failed to respond to appropriate nonsurgical management and imaging studies are normal, the use of arthroscopy not only aids in the diagnosis of chronic ankle pain, but is also helpful in its treatment. In patients with this condition, typical findings include synovitis in the lateral gutter and fibrosis along the talofibular articulation; syndesmosis chondromalacia of the talus and ankle also may be found. In patients with anterior soft-tissue impingement, approximately 84% who have a poor response to nonsurgical management will have a good to excellent response after arthroscopic synovectomy and debridement. Ferkel RD, Fasulo GJ: Arthroscopic treatment of ankle injuries. Orthop Clin North Am 1994;25:17-32.
References:
- Ferkel RD, Karzel RP, Del Pizzo W, Friedman MJ, Fischer SP: Arthroscopic treatment of anterolateral impingement of the ankle. Am J Sports Med 1991;19:440-446.
Question 6High Yield
A 72-year-old woman who was doing well after undergoing total shoulder arthroplasty for arthritis 4 months ago is suddenly unable to elevate her arm. Examination reveals 70 degrees of external rotation compared with 45 degrees on the uninvolved side, and she is unable to lift her hand off her lower back. Radiographs are shown in Figures 43a through 43c. Treatment should consist of


Explanation
Results of treatment of subscapularis rupture are best when immediate repair is performed. When the cause of the anterior instability is the result of rupture of the subscapularis tendon and the component position is acceptable, revising the position of the component is unnecessary. Restoring the coracoacromial arch and subacromial decompression are related to superior instability and rotator cuff pathology, respectively, and would not correct the instability caused by subscapularis rupture. Moeckel BH, Altchek DW, Warren RF, Wickiewicz TL, Dines DM: Instability of the shoulder after arthroplasty. J Bone Joint Surg Am 1993;75:492-497.
Question 7High Yield
A 9-year-old child sustained a fracture-dislocation of C-5 and C-6 with a complete spinal cord injury. What is the likelihood that scoliosis will develop during the remaining years of his growth?
Explanation
Explanation
The incidence of late spinal deformity after complete spinal cord injury in children depends on the level of the spinal cord injury and the age of the patient at the time of injury. If a cervical level injury occurs before age 10 years, paralytic scoliosis will develop in virtually 100% of patients. Brown JC, Swank SM, Matta J, et al: Late spinal deformity in quadriplegic children and adolescents. J Pediatr Orthop 1984;4:456-461. Lancourt JE, Dickson JH, Carter RE: Paralytic spinal deformity following traumatic spinal-cord injury in children and adolescents. J Bone Joint Surg Am 1981;63:47-53.
References:
- Dearolf WW III, Betz RR, Vogel LC, et al: Scoliosis in pediatric spinal cord-injured patients. J Pediatr Orthop 1990;10:214-218.
Question 8High Yield
What region of the spine is most susceptible to changes in the vascular supply to the spinal cord during an anterior approach?
Explanation
The thoracic spinal cord is characterized by a variable and, at times, complicated blood supply. The artery of Adamkiewicz, also known as the great anterior medullary artery, most typically arises off the left side of the aorta between T8 and T12. It represents the sole medullary blood supply to the thoracic spine. When this artery is divided or injured, the blood supply to the thoracic cord may be interrupted. It is important to avoid electocautery of blood vessels within or near the thoracic foramen because this is a site of important, albeit limited, collateral circulation. Sharma M, Anderson FC: Spinal vascular lesions, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 301-306.
Question 9High Yield
Which of the following properties primarily provides the excellent corrosion resistance of metallic alloys such as stainless steel and cobalt-chromium-molybdenum?
Explanation
All of the metals and metallic alloys used in orthopaedic surgery obtain their corrosion resistance from an adherent oxide layer. For stainless steel and cobalt alloy, the addition of chromium as an alloying element ensures the formation of a chromium oxide passive layer that forms on the surface and separates the bulk material from the corrosive body environment. Titanium alloy achieves the same result without chromium by forming an adherent passive layer of titanium oxide. Although these layers can indeed be hard, hardness does not in and of itself provide corrosion resistance. Adding nickel to both metallic alloys adds to strength but does not influence corrosion resistance appreciably. Galvanic potential can influence corrosion but does so by differences in potential between two contacting materials; for example, stainless steel and cobalt alloy have substantially different potentials, and if they were in contact within an aqueous environment, corrosion would commence with the stainless steel becoming the sacrificial anode. Metallic carbides are important in strengthening the alloys but have no role in providing corrosion resistance. Williams DF, Williams RL: Degradative effects of the biological environment on metal and ceramics, in Ratner BD, Hoffman AS, Shoen FJ, et al (eds): Biomaterials Science. San Diego, CA, Academic Press, 1996, pp 260-265. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 190-193.
Question 10High Yield
A 22-year-old professional ballet dancer reports a 3-month history of posterior ankle pain that occurs when she changes from a flat foot to pointe (hyperplantar flexed position). Examination does not elicit the pain with forced passive plantar flexion. A radiograph is shown in Figure 8. What is the most likely cause of the pain?
Explanation
Explanation
The most common causes of posterior ankle pain in ballet dancers are flexor hallucis longus tenosynovitis and os trigonum syndrome. Flexor hallucis longus tenosynovitis differs from a symptomatic os trigonum by the absence of pain with forced plantar flexion and the presence of pain with resisted plantar flexion of the great toe. The pain is often felt in the posterior ankle and can be associated with a snapping or triggering sensation. Os trigonum syndrome commonly occurs in ballet dancers who perform in a position of extreme plantar flexion. The pain occurs from entrapment of the os trigonum between the posterior portion of the talus and calcaneus. Hamilton WG, Geppert MJ, Thompson FM: Pain in the posterior aspect of the ankle in dancers: Differential diagnosis and operative treatment. J Bone Joint Surg Am 1996;78:1491-1500.
References:
- Khan K, Brown J, Way S, et al: Overuse injuries in classical ballet. Sports Med 1995;19:341-357.
Question 11High Yield
Exostoses in which of the following anatomic locations is the most likely to undergo malignant transformation in a patient with multiple hereditary exostosis (MHE)?
Explanation
Explanation
Although osteochondromas can occur in almost every bone in patients with MHE, proximally located lesions are more likely to undergo malignant transformation. Annual radiographs of the shoulder girdles and pelvis are indicated in patients with MHE. Any enlarging osteochondromas are a concern as possible malignancies. Peterson HA: Multiple hereditary osteochondromata. Clin Orthop 1989;239:222.
References:
- McCornack EB: The surgical management of hereditary multiple exostosis. Orthop Rev 1981;10:57.
Question 12High Yield
Which of the following characteristics is seen in patients with osteochondritis dissecans of the elbow?
Explanation
Osteochondritis dissecans occurs in the older child or adolescent (typically older than age 13 years). It involves the lateral compartment. The etiology is felt to be microtraumatic vascular insufficiency from repetitive rotatory and compressive forces. MRI typically shows separation of cartilage from the capitellum and chondral fissuring. Panner's disease is usually seen in children younger than age 10 years, involves the entire capitellar ossific nucleus, and resolves typically with no residual deformity or late sequelae. There is no evidence of ligamentous injury. Defelice GS, Meunier MJ, Paletta GA: Elbow injury in the adolescent athlete, in Altchek DW, Andrews JR (eds): The Athlete's Elbow. New York, NY, Lippincott Williams & Wilkins, 2001, pp 231-248.
Question 13High Yield
What is the most common benign bone tumor in childhood?
Explanation
Explanation
The most common benign bone tumor in childhood is a nonossifying fibroma. It is estimated that 30% of children have a nonossifying fibroma. In most patients, the lesion is not identified until a radiograph is obtained for unrelated reasons. Similarly, most identified cases of fibrous cortical defect are not biopsied because the radiographic and clinical presentations are diagnostic. Aboulafia AJ, Kennon RE, Jelinek JS: Benign bone tumors of childhood. J Am Acad Orthop Surg 1999;7:377-388.
References:
- Biermann JS: Common benign lesions of bone in children and adolescents. J Pediatr Orthop 2002;22:268-273.
Question 14High Yield
Posterior sternoclavicular dislocations are most commonly associated with which of the following complications?
Explanation
Posterior sternoclavicular dislocations are commonly associated with tracheal compression, which can be a life-threatening condition requiring immediate reduction. The other listed complications are less common. Brooks AL, Henning GD: Injury to the proximal clavicular epiphysis, abstracted. J Bone Joint Surg Am 1972;54:1347-1348.
Question 15High Yield
A 10-year-old child has leg discomfort with activity. A radiograph, bone scan, and biopsy specimen are shown in Figures 1a through 1c. What is the most likely diagnosis?
Explanation
Explanation
1b 1c The ground glass appearance on the radiograph, the hot bone scan, and histologic findings of bony spicules without osteoblastic rimming in a background of bland fibrous tissue all suggest fibrous dysplasia. Stress-related pain is common with activity because of the dysplastic bone. Parosteal osteosarcomas are surface lesions. Simple cysts, aneurysmal bone cysts, and eosinophilic granuloma are all possible radiographically; however, the histology is most consistent with fibrous dysplasia. Harris WH, Dudley HR Jr, Barry RS: The natural history of fibrous dysplasia: An orthopaedic, pathological and roentgenographic study. J Bone Joint Surg Am 1962;44:207.
References:
- Campanacci M: Bone and Soft Tissue Tumors. Vienna, Austria, Springer-Verlag, 1990.
Question 16High Yield
What is the reported failure rate for surgical treatment of a Morton's neuroma?
Explanation
Explanation
The reported failure rate is in the range of 15%, which may be the result of incorrect diagnosis, improper web space selection, or formation of a stump neuroma. Therefore, the procedure should be approached with caution, measures should be taken to ensure that the diagnosis is accurate, and nonsurgical options should be exhausted. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111. Beskin JL: Nerve entrapment syndromes of the foot and ankle. J Am Acad Orthop Surg 1997;5:261-269.
References:
- Mann RA, Reynolds JC: Interdigital neuroma: A critical clinical analysis. Foot Ankle 1983;3:238-243.
Question 17High Yield
Which of the following structures may help maintain radial length after a radial head fracture?
Explanation
Explanation
Essex-Lopresti injuries affect axial stability of the forearm. Injury to the interosseous membrane or the triangular fibrocartilage complex can result in proximal migration of the radius. Morrey BF, Chao EY, Hui FC: Biomechanical study of the elbow following excision of the radial head. J Bone Joint Surg Am 1979;61:63-68.
References:
- Coleman DA, Blair WF, Shurr D: Resection of the radial head for fracture of the radial head: Long-term follow-up of seventeen cases. J Bone Joint Surg Am 1987;69:385-392.
Question 18High Yield
A 1-year-old infant has the hand deformities shown in Figure 40. What pathologic process is the most likely cause of these deformities?
Explanation
Streeter's dysplasia is clearly related to rupture of the amnion in utero and is now most commonly referred to as premature amnion rupture sequence. The deformities arise from amniotic bands that wrap about protruding parts and from uterine packing because of the accompanying oligohydramnios. Clubfoot can develop as a result of the latter mechanism. Three limb involvement is most commonly seen, along with syndactyly. Treatment involves resection of bands and Z-plasty of skin. The disease is not genetic and has not been related to teratogen exposure or to iatrogenic influences such as amniocentesis. Developmental field disruption is not seen in this disease, and the growth potential of the involved parts is normal unless neurovascular disruption has arisen from band formation.
Question 19High Yield
Figure 19 shows an arthroscopic view from the anterior lateral portal of the knee looking into the suprapatella pouch. The use of an electrothermal device during this procedure most commonly causes significant postoperative complications by damaging which of the following structures?
Explanation
While it is possible to damage any of these structures, unrecognized intraoperative laceration without adequate coagulation of the superior lateral geniculate artery is common. This can result in significant postoperative hemarthrosis and a return to surgery when bleeding cannot be controlled. Cash JD, Hughston JC: Treatment of acute patella dislocation. Am J Sports Med 1988;16:244-249.
Question 20High Yield
Which of the following staging studies should be obtained for an adult with an 8-cm deep, high-grade malignant fibrous histiocytoma of the extremity?
Explanation
Explanation
MRI is the preferred imaging study to evaluate the local tumor extension for soft-tissue lesions, but CT can be used if MRI is contraindicated (eg, patients with pacemakers). CT of the chest is always recommended in patients with high-grade sarcomas because 80% of metastases occur in the lungs. CT of the abdomen and pelvis is indicated in patients with lower extremity liposarcoma because some patients also have synchronous retroperitoneal liposarcoma. Lymph node metastasis occurs in up to 5% of patients with soft-tissue sarcoma. If the nodes are clinically enlarged, biopsy is indicated. Routine sentinel node biopsy currently is not recommended. Bone scan is not used in the staging of soft-tissue sarcoma as it has not been shown to be cost-effective. Demetri GD, Pollock R, Baker L, Balcerzak S, Casper E, Conrad C, et al: NCCN sarcoma practice guidelines: National Comprehensive Cancer Network. Oncology (Huntingt) 1998;12:183-218.
References:
- Pollack R, Brennan M, Lawrence W, Jr: Society of Surgical Oncology practice guidelines: Soft-tissue sarcoma surgical practice guidelines. Oncology (Huntingt) 1997;11:1327-1332.
Question 21High Yield
A 47-year-old patient has had persistent pain and weakness after undergoing a reamed intramedullary nailing for a midshaft humerus fracture 8 months ago. There is no evidence of infection. Radiographs are shown in Figures 19a and 19b. Management should consist of

Explanation
Compression plating remains the treatment of choice for most established humeral nonunions. Autograft is felt to be superior to allograft. Electrical stimulation has not been found to improve healing rates in patients with nonunion after intramedullary nailing. Retrograde nailing with flexible nails gives inadequate rotational control to promote healing in this patient. Adding cancellous graft alone will not stabilize the nonunion site. Dynamic locking has been successful only in the lower extremity because the bone can be loaded axially. McKee MD, Miranda MA, Riemer BL, et al: Management of humeral nonunion after the failure of locking intramedullary nails. J Orthop Trauma 1996;10:492-499.
Question 22High Yield
A 24-year-old female soccer player has had lateral joint line pain and a recurrent effusion in the left knee after sustaining a twisting injury 6 weeks ago. She reports that symptoms worsen with athletic activities. MRI scans are shown in Figures 2a through 2c. What is the most likely diagnosis?
Explanation
Explanation
2b 2c The MRI scans show the typical findings of a torn discoid lateral meniscus. The average transverse diameter of the lateral meniscus is 11 or 12 mm. A discoid lateral meniscus is suggested when three or more contiguous 5-mm sagittal sections on the MRI scan show continuity of the menicus between the anterior and posterior horns, or when two adjacent peripheral sagittal 5-mm sections show equal meniscal height. Normally the black "bow tie" would be seen on two contiguous sagittal sections. The presence of a discoid meniscus can be further confirmed if coronal views reveal increased width. Jordan MR: Lateral meniscal variants: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:191-200.
References:
- Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 625-630.
Question 23High Yield
Figures 36a and 36b show the radiographs of a 48-year-old woman who smokes cigarettes and sustained a segmental femoral shaft fracture in a motor vehicle accident 9 months ago. Initial management consisted of stabilization with a reamed statically locked intramedullary nail. She now reports lower leg pain that increases with activity. In addition to advising the patient to quit smoking, management should include

Explanation
The patient has an oligotrophic nonunion of the distal femoral fracture. Although the proximal fracture appears incompletely united, it was stable at exchange nailing. The treatment of choice is exchange reamed nailing to at least 2 mm above the nail in place. Bone grafting is debatable. Recent studies have shown a 70% to 75% success rate with exchange nailing only, so in nonhypertrophic nonunions, bone grafting can be considered. Nonsurgical management consisting of observation or external stimulation runs the risk of implant failure. Plate fixation is acceptable but is considered a second choice because of the need to consider stabilization of the proximal fracture until union is achieved. Also, plate fixation definitely requires bone grafting. Webb LX, Winquist RA, Hansen ST: Intramedullary nailing and reaming for delayed union or nonunion of the femoral shaft: A report of 105 consecutive cases. Clin Orthop 1986;212:133-141. Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nailing for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.
Question 24High Yield
Figure 10 shows the radiograph of a 9-year-old girl who injured her left lower leg after being thrown from a horse. Examination reveals no other injuries. Which of the following forms of management will provide the lowest rate of complications and the earliest return to function?
Explanation
Because the patient has a transverse midshaft fracture with no evidence of comminution, the treatment of choice is closed reduction and stabilization with flexible intramedullary nails. Transverse fractures treated with an external fixator heal with poor callus and have a high refracture rate. In addition, the pin tracks produce undesirable and excessive scarring. Femoral pin traction is safe and effective but results in considerable muscle wasting and a slow return to function. Interlocking nails run the risk of greater trochanteric growth disturbance and/or osteonecrosis of the femoral head in this age group. Plate fixation, while effective, requires considerable tissue dissection with large scar formation. It also requires a rather extensive dissection for later plate removal. Ligier JN, Metaizeau JP, Prevot J, Lascombes P: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77.
Question 25High Yield
A 15-year-old girl has left knee pain and an enlarging mass in the distal thigh. AP and lateral radiographs are shown in Figures 52a and 52b, and a biopsy specimen is shown in Figure 52c. What is the most likely diagnosis?
Explanation
Explanation
52b 52c A bone-producing lesion in the metaphysis of an adolescent is most likely an osteosarcoma. The radiographs show a distal femoral bone-producing lesion extending into the surrounding soft tissues. The histologic appearance consists of pleomorphic cells producing osteoid. Ewing's sarcoma and metastatic neuroblastoma do not produce a matrix. Chondrosarcoma is a radiographically destructive lesion with calcification and cartilage cells on histologic section. An osteochondroma is a benign cartilage lesion that is continuous with the medullary cavity of the underlying bone and extends into a bony lesion and covered by a cartilage cap. Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
References:
- Gibbs CP, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 26High Yield
A patient with a cobalt-chromium alloy (Co-Cr) femoral stem has a periprosthetic fracture that is to be fixed with a cable-plate device. The surgeon should make sure that the plate, screws, and cable, respectively, are made of
Explanation
Contact between metals in a biologic environment leads to galvanic corrosion. Reduction potentials of Co-Cr and stainless steel produce the worst combination of metals in commonly used implants. Because the fixation implants are not intended to contact the existing implant, it is not as great a consideration as the plate and the screws and cables that will directly contact each other. Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 119-144.
Question 27High Yield
Figure 9 shows the AP radiograph of a 65-year-old man who has knee pain and swelling. What is the most likely diagnosis?
Explanation
Although all the choices are known causes of joint degeneration (secondary osteoarthritis), only chondrocalcinosis shows distinct linear calcification of the cartilage due to deposition of calcium pyrophosphate crystals. Gout is a recurrent acute arthritis resulting from the deposition of monosodium urate from supersaturated hyperuricemic body fluids. Hemochromotosis is characterized by focal or generalized deposition of iron within body tissues. Arthritis may be present but is less common than other manifestations such as liver cirrhosis, skin pigmentation, diabetes mellitus, and cardiac disease. Rheumatoid arthritis is a nonspecific, usually symmetric inflammation of peripheral joints resulting in destruction of articular and periarticular structures. Ochronosis is a hereditary enzyme deficiency (homogentisic acid oxidase) resulting in deposition of homogentisic acid polymers in articular cartilage. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 188.
Question 28High Yield
A 65-year-old woman with a history of diabetes mellitus and plantar ulcers has an erythematous and swollen right foot and ankle. Despite IV antibiotics, the erythema spreads to her lower calf within 24 hours. She has a systolic blood pressure of 80/55 mm Hg and a pulse rate of 120. Laboratory studies show a creatinine level of 1.5 mg. Initial management should consist of
Explanation
Necrotizing fasciitis is an aggressive and rapidly spreading soft-tissue infection, usually caused by group A beta-hemolytic Streptococcus pyogenes. Presentation is typical of a rapidly ascending cellulitis, recalcitrant to antibiotic treatment. Differentiation between cellulitis and impetigo is difficult, and success depends on a high level of suspicion. The skin and subcutaneous tissues are affected, with sparing of the muscles. Septic shock and multi-organ system failure can be fatal. Treatment is aggressive surgical debridement with broad-spectrum antibiotics. Repeat irrigation and debridement may be necessary. Hyperbaric oxygen studies have shown inconsistent results. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 199-205.
Question 29High Yield
Which of the following infectious organisms may be associated with underlying malignancy?
Explanation
Evidence implicates an association, albeit unexplained, between Clostridium septicum infection and malignancy, particularly hematologic or intestinal malignancy. The malignancy is often at an advanced stage, compromising survival of the patients. A bowel portal of entry is postulated for most patients. In the absence of an external source in the patient with clostridial myonecrosis or sepsis, the cecum or distal ileum should be considered a likely site of infection. Increased awareness of this association between Clostridium septicum and malignancy, and aggressive surgical treatment, may result in improvement in the present 50% to 70% mortality rate. Other organisms associated with malignancy include group Clostridium streptococci that are occasionally associated with upper gastrointestinal malignancies. Schaaf RE, Jacobs N, Kelvin FM, et al: Clostridium septicum infection associated with colonic carcinoma and hematologic abnormality. Radiology 1980;137:625-627.
Question 30High Yield
When performing surgical excision of the lesion shown in the MRI scan in Figure 3, what nerve is most likely at risk?
Explanation
Explanation
The MRI scan shows a large mass (lipoma) in the thenar muscles of the palm. The recurrent motor branch of the median nerve innervates the thenar muscles. The anterior interosseous nerve (AIN) in the proximal forearm innervates the flexor pollicis longus, pronator quadratus, and flexor digitorum pollicis to the index and frequently the middle finger. The terminal branch of the AIN innervates only the wrist capsule. The palmar cutaneous branch of the ulnar nerve is a sensory structure to the hypothenar area. There is no commonly described recurrent branch of the ulnar nerve.
References:
- Kozin SH: The anatomy of the recurrent branch of the median nerve. J Hand Surg Am 1998;23:852-858.
Question 31High Yield
Survival rates for children with soft-tissue sarcoma other than rhabdomyosarcoma are best correlated with
Explanation
In review of 154 patients with nonrhabdomyosarcoma, Rao reported that histologic grade, tumor invasiveness, and adequate surgical margin were the most important prognostic factors. Histologic subtype, use of adjuvant chemotherapy, and patient age were not as important. Size related to degree of invasiveness was not statistically significant. Rao BN: Nonrhabdomyosarcoma in children: Prognostic factors influencing survival. Semin Surg Oncol 1993;9:524-531. Andrassy R, et al: Non-rhabdomyosarcoma Soft-Tissue Sarcomas: Pediatric Surgical Oncology. Philadelphia, PA, WB Saunders, p 221.
Question 32High Yield
Figure 16 shows the radiograph of a 56-year-old man who has neck pain after a rollover accident on his lawnmower. The injury appears to be isolated, and he is neurologically intact. Management of the fracture should consist of
Explanation
The radiograph shows a type IIa Hangman's fracture, and the classic treatment is halo vest immobilization. Traction should be avoided in type IIa injuries because of the risk of overdistraction. A lesser form of immobilization such as a hard collar or a Minerva jacket can be used for nondisplaced (type I) fractures. Surgery generally is reserved for type III fractures (includes C2-3 facet dislocation), or extenuating circumstances such as multiple trauma or other fractures of the cervical spine that require surgical stabilization. Levine AM, Edwards CC: The management of traumatic spondylolisthesis of the axis. J Bone Joint Surg Am 1985;67:217-226.
Question 33High Yield
A 64-year-old man undergoes a primary total knee arthroplasty. Three months after surgery he reports persistent pain, weakness, and difficulty ambulating. Postoperative radiographs are shown in Figures 6a through 6c. What is the best course of action at this time?


Explanation
The Merchant view reveals subluxation of the patellar component. The etiology of maltracking of the patella includes internal rotation of the femoral component, internal rotation of the tibial component, excessive patellar height, and lateralization of the patella component. The treatment of choice in this patient is revision total knee arthroplasty with external rotation of the femoral component. Preoperatively the patient also may require a lateral release, revision of the tibial component if it is internally rotated, and possibly a soft-tissue realignment. Component malalignment needs to be addressed first. Kelly MA: Extensor mechanism complications in total knee arthroplasty. Instr Course Lect 2004;53:193-199. Malkani AL, Karandikar N: Complications following total knee arthroplasty. Sem Arthroplasty 2003;14:203-214.
Question 34High Yield
Which of the following is considered the best method for the prevention of wrong-site surgery?
Explanation
Explanation
The best method of preventing wrong-site surgery is for the surgeon to initial the surgical site in the preoperative holding area after discussion and confirmation of the site with the patient. This should be done before sedating medications are administered. A recent study found that patient noncompliance with specific preoperative instructions to mark the site with a "yes" at home was surprisingly high; only 59% of the patients marked the extremity correctly and 37% made no mark. Noncompliance was higher in those with workers' compensation claims (70%) and those with previous related surgery (51%). DeGiovanni CW, Kang L, Manuel J: Patient compliance in avoiding wrong site surgery. J Bone Joint Surg Am 2003;85:815-819.
References:
- American Academy of Orthopaedic Surgeons. Advisory Statement: Wrong-site Surgery. Document 1015, 2002 Sept. www.aaos.org/wordhtml/papers/advismt/wrong.htm.
Question 35High Yield
Which of the following is the primary mechanism of polyethylene wear in the hip?
Explanation
Explanation
Although previous theories on acetabular wear implicated fatigue cracking and delamination as primary wear mechanisms, these have actually manifested as major modes of polyethylene wear in knees. The primary mechanism of wear in polyethylene acetabular components appears to be adhesion and abrasion. In an analysis of 128 components retrieved at autopsy or revision surgery, wear appeared to occur mostly at the surface of the components and was the result of large strain plastic deformation and orientation of the surface layers into fibrils that subsequently ruptured during multidirectional motion. It was also shown conclusively that 32-mm heads displayed significantly more wear (volumetric wear) than either 22-mm or 26-/28-mm heads (1-mm increase in size increased volumetric wear by 10%). The wear at the articulating surface was characterized by highly worn polished areas superiorly and less worn areas inferiorly separated by a ridge. Abrasion was very common, occurring after adhesion and plastic deformation of polyethylene fibrils, and abrasion secondary to third-body wear. Wear rates decreased with longer survival of components, indicating a "bedding in" phenomenon, arguing against oxidative and fatigue wear. Crevice corrosion occurs in fatigue cracks with low oxygen tension (under screw heads, etc). Oscillatory fretting consists of cyclical abrading of the outer surface from small movements. Fatigue and delamination is predominant in total knee arthroplasty where stresses are maximum just below the surface of the polyethylene component, causing fatigue over time with subsequent delamination. In contrast, hip wear occurs primarily at the surface of the polyethylene component. Jasty M, Goetz DD, Bragdon CR, et al: Wear of polyethylene acetabular components in total hip arthroplasty: An analysis of one hundred and twenty-eight components retrieved at autopsy or revision operations. J Bone Joint Surg Am 1997;79:349-358. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 47-53. Bell CJ, Walker PS, Abeysundera MR, et al: Effect of oxidation on delamination of ultrahigh-molecular-weight polyethylene tibial components. J Arthroplasty 1998;13:280-290.
References:
- Sutula LC, Collier JP, Saum KA, et al: The Otto Aufranc Award: Impact of gamma sterilization on clinical performance of polyethylene in the hip. Clin Orthop 1995;319:28-40.
Question 36High Yield
A 28-year-old woman has left shoulder pain and a tender soft-tissue mass. Based on the MRI scan and biopsy specimens shown in Figures 74a through 74c, what is the most likely diagnosis?


Explanation
Schwannomas (neurilemomas) occur at all ages but are most frequently seen in persons between the ages of 20 and 50 years. MRI features of schwannomas are fairly nonspecific, but when they are associated with a large named nerve, the identification of a mass in continuity with that nerve is highly suggestive of a schwannoma. Most have a fairly homogeneous appearance with a high water content and often fusiform shape. Classically, the histology shows alternating Antoni A (dense spindle cell region) areas and Antoni B (loose myxoid tissue) areas. They also demonstrate uniform intense immunostaining with S-100 protein. Damron TA, Sim FH: Soft-tissue tumors about the knee. J Am Acad Orthop Surg 1997;5:141-152.
Question 37High Yield
A 53-year-old man reports acute, severe left shoulder pain after undergoing abdominal surgery 10 days ago. Initial management, consisting of anti-inflammatory drugs, physical therapy, and a subacromial injection of corticosteroid, fails to provide relief. Reexamination of the shoulder 2 months after the onset of symptoms reveals atrophy of the infraspinous and supraspinous fossa and profound weakness of active abduction and external rotation. His neck is supple with a full range of motion. Plain radiographs and an MRI scan of the shoulder are normal. What diagnostic study should be performed next in the evaluation of this patient?
Explanation
Explanation
Suprascapular nerve palsy is a fairly uncommon yet well-known cause of shoulder pain and weakness. A variety of causes have been described, including compression by a ganglion cyst, an anomalous or thickened superior transverse scapular ligament, a humeral and scapular fracture, and traction or kinking of the nerve in the suprascapular notch. In this patient, the injury is most likely caused by traction or compression of the nerve in the suprascapular notch as the result of positioning during abdominal surgery; therefore, the studies of choice are electromyography and nerve conduction velocity studies. While MRI of the cervical spine may be of some value in ruling out a radiculopathy, the clinical history does not support such a cause for this condition. Rengachary SS, Neff JP, Singer PA, Brackett CE: Suprascapular entrapment neuropathy: A clinical, anatomical, and comparative study. Part 1: Clinical study. Neurosurgery 1979;5:441-446. Rengachary SS, Burr D, Lucas S, Hassanein KM, Mohn MP, Matzke H: Suprascapular entrapment neuropathy: A clinical, anatomical and comparative study. Part 2: Anatomical study. Neurosurgery 1979;5:447-451.
References:
- Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthoscopy 1990;6:301-305.
Question 38High Yield
A 26-year-old man has had hand pain and progressive swelling in the knuckle for the past several months. He denies any trauma to the hand. The ring finger metacarpophalangeal joint is tender, and there is loss of motion in the digit. Figure 32a shows the radiograph and Figures 32b through 32d show the T1-weighted, T2-weighted, and gadolinium MRI scans, respectively. What is the most likely diagnosis?
Explanation
Explanation
32b 32c 32d The radiograph reveals a subchondral lesion in the metacarpophalangeal joint that is lytic and expansile. The MRI scans show a mass that is moderate in intensity on the T2-weighted image and has some gadolinium uptake. There are no cystic components in this lesion. The subchondral location and expansile nature are highly suggestive of giant cell tumor of bone. A lesion with this appearance might also represent an aneurysmal bone cyst, given the amount of expansion present. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 113-118.
References:
- Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 39High Yield
A 31-year-old man sustained a closed injury to his arm in a motor vehicle accident 16 months ago. Treatment of the fracture consisted of intramedullary nailing of the humerus. He now reports pain with minimal activities. Clinical examination and laboratory studies suggest no signs of infection. Radiographs are seen in Figures 12a through 12c. Treatment should now consist of
Explanation
Explanation
12b 12c The use of locked nailing for the treatment of established nonunion of the humerus has produced poor results. Since humeral nailing has already failed, exchange humeral nailing without bone grafting has an even less change of success. To increase the likelihood of achieving bony union, the treatment of choice is removal of the humeral nail, dynamic compression plating, and bone grafting. Zuckerman J, Giordanno C, Rosen H: Treatment of humeral shaft non-unions, in Bigliani L (ed): Complications of shoulder surgery. Baltimore, MD, William & Wilkins, 1993, pp 173-190.
References:
- Jupiter JB: Complex non-union of the humeral diaphysis: Treatment with a medial approach, an anterior plate, and a vascularized fibular graft. J Bone Joint Surg Am 1990;72:701-707.
Question 40High Yield
Which of the following tissues used for anterior cruciate ligament (ACL) reconstruction has the highest maximum load to failure?
Explanation
Explanation
While the patellar tendon ligament is considered by many to be the tissue of choice for ACL reconstruction, more recent studies have shown that the quadruple semitendinosus and gracilis tendon graft has the greatest stiffness and offers the highest maximum load to failure. Hamner DL, Brown CH Jr, Steiner ME, Hecker AT, Hayes WC: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557. Cooper DE, Deng XH, Burstein AL, Warren RF: The strength of the central third patellar tendon graft: A biomechanical study. Am J Sports Med 1993;21:8l8-823. Brown CH Jr, Steiner ME, Carson EW: The use of hamstring tendons for anterior cruciate ligament reconstruction: Technique and results. Clin Sports Med 1993;12:723-756.
References:
- Engebretsen L, Lewis JL: Graft selection and biomechanical considerations in ACL reconstruction. Sports Med Arthroscopy Rev 1996;4:336-341.
Question 41High Yield
Treatment of a cruciate-retaining total knee that is unstable in flexion is best accomplished by
Explanation
Explanation
Pagnano and associates revised 25 painful primary posterior cruciate-retaining total knee arthroplasties for flexion instability. The patients shared typical clinical presentations that included a sense of instability without frank giving way, recurrent knee joint effusion, soft-tissue tenderness involving the pes anserine tendons and the retinacular tissue, posterior instability of 2+ or 3+ with a posterior drawer or a posterior sag sign at 90 degrees of flexion, and above-average motion of the total knee arthroplasty. Twenty-two of the knee replacements were revised to posterior stabilized implants, and three underwent tibial polyethylene liner exchange only. Nineteen of the 22 knee replacements revised to a posterior stabilized implant showed marked improvement after the revision surgery. Only one of the three knee replacements that underwent tibial polyethylene exchange was improved. Flexion instability can be a cause of persistent pain and functional impairment after posterior cruciate-retaining total knee arthroplasty. Revision surgery that focuses on balancing the flexion and extension spaces, in conjunction with a posterior stabilized knee implant, seems to be a reliable treatment for symptomatic flexion instability after posterior cruciate-retaining total knee arthroplasty.
References:
- Pagnano MW, Hanssen AD, Lewallen DG, Stuart MJ: Flexion instability after primary posterior cruciate-retaining total knee arthroplasty. Clin Orthop 1998;356:39-46.
Question 42High Yield
A 28-year-old man was shot in the foot with a .22 caliber handgun approximately 2 hours ago. Examination reveals an entrance wound dorsally and a plantar exit wound. The foot is neurovascularly intact. Radiographs reveal a nondisplaced fracture of the third metatarsal. Soft-tissue management for this injury should consist of
Explanation
The patient has sustained a low-velocity, low-caliber gunshot wound to the foot. Because the injury occurred within a period of 8 hours, this is classified as a type I wound. Several studies support the use of surface debridement, cleansing, and sterile dressings as the treatment of choice. More aggressive measures are reserved for high-velocity injuries and shotgun injuries. Brettler D, Sedlin ED, Mendes DG: Conservative treatment of low velocity gunshot wounds. Clin Orthop 1979;140:26-31. Hampton OD: The indications for debridement of gunshot bullet wounds of the extremities in civilian practice. J Trauma 1961;1:368-372.
Question 43High Yield
What clinical finding is associated with the least favorable prognosis in an adolescent patient who has been diagnosed with a high-grade osteosarcoma of the distal femur?
Explanation
The presence of synchronous bone disease in young patients carries a dismal prognosis, one that is even worse than the presence of resectable pulmonary metastasis. Many osteosarcomas cross the physis; therefore, this has not been shown to be of prognostic importance. Similarly, the presence of the soft-tissue mass has less prognostic significance.
Question 44High Yield
When evaluating articular cartilage, what extracellular matrix component is most closely associated with the deep calcified cartilage zone?
Explanation
Explanation
Collagen type X is produced only by hypertrophic chondrocytes during enchondral ossification (growth plate, fracture callus, heterotopic ossification) and is associated with calcification of cartilage in the deep zone of articular cartilage. Collagen type I is the predominant collagen in bone, ligament, and tendon. Collagen type II is the predominant collagen in articular cartilage. Proteoglycan aggrecan and hyaluronic acid are components of the extracellular matrix and are involved in the compressive strength characteristics of articular cartilage. Buckwalter JA, Mankin HJ: Articular cartilage: Tissue design and chondrocyte matrix interactions. Instr Course Lect 1998;47:477-486.
References:
- Poole AR, Kojima J, Yasuda T, Mwale F, Kobayasai M, Laverty S: Composition and structure of articular cartilage: A template for tissue repair. Clin Orthop 2001;391:S26-S33.
Question 45High Yield
A 39-year-old man has anterior shoulder pain after landing on his abducted left shoulder while playing softball. Examination reveals a stable glenohumeral joint, pain on passive external rotation of greater than 25 degrees, and pain and weakness on belly press (Napoleon's) test. An MRI scan is shown in Figure 32. To provide maximum pain relief and return of function, management should include
Explanation
The examination and MRI scan confirm a subscapularis rupture and dislocation of the long head of the biceps tendon. The greatest return of function will result from repair of the subscapularis and tenodesis of the biceps tendon. Physical therapy alone will result in inadequate healing of the subscapularis and will not address the biceps tendon. While biceps tenotomy is an option, it will not provide the same level of pain relief and return of function as a tenodesis in a young, active man. There is no evidence for a supraspinatus tear. Deutsch A, Altchek DW, Veltri DM, Potter HG, Warren RF: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Question 46High Yield
A 55-year-old man who runs on the weekends reports a 1-year history of continued pain directly posteriorly in the heel. Management consisting of anti-inflammatory drugs, icing techniques, a heel-counter in his shoe split, and physical therapy consisting of stretching, contrast baths, custom orthotics, and iontophoresis has failed to provide relief. Not only is his lifestyle disrupted with respect to running, but he now has pain with normal ambulation with all forms of shoe wear. He is not necessarily concerned with returning to running; he is primarily seeking pain relief. A lateral radiograph and clinical photograph are shown in Figures 32a and 32b. Treatment should now consist of
Explanation
Explanation
32b The patient has severe calcifications at the insertion of the Achilles tendon. Failure to address the Haglund's exostosis and the calcifications will leave the patient with persistent pain. Steroids should not be injected directly into the tendon because of the increased risk of tendon rupture. Shock wave treatment may have some value in treating plantar fasciitis, but its efficacy has not been documented with insertional calcifications and Haglund's exostosis treatment. Brisement is injection of saline solution around the Achilles tendon in an attempt to decompress the peritenon. This may be valuable in intrasubstance Achilles tendinosis or peritendinitis but has no value with insertional disease. Symptoms persisting beyond 6 months are difficult to treat nonsurgically; therefore, the appropriate treatment protocol is aggressive and must address all pathology. The patient may not be able to run at the level achieved prior to surgery, but the goal of the surgery is pain relief. Clain M, Baxter D: Achilles tendinitis. Foot Ankle 1992;13:482-487. Schepsis A, Wagner C, Leach R: Surgical management of Achilles tendon overuse injuries: A long-term follow-up study. Am J Sports Med 1994;22:611-619. Schepsis A, Leach R: Surgical management of Achilles tendinitis. Am J Sports Med 1987;15:308-315.
References:
- Keck S, Kelly P: Bursitis of the posterior part of the heel: Evaluation of surgical treatment of eighteen patients. J Bone Joint Surg Am 1965;47:267-273.
Question 47High Yield
A 58-year-old patient who underwent bilateral hip arthroplasty 12 years ago now reports pain in his hips and difficulty with ambulation to the point where he now uses crutches. A radiograph of the hip and pelvis is shown in Figure 26. What is the best treatment option for this patient?
Explanation
Explanation
The radiographs reveal acetabular component failure with bone loss. There are several treatment options available. The best option for survivorship is a cementless porous-coated acetabular component. This patient may or may not require structural bone graft, which may need to be determined at the time of surgery. Bipolar implants and cemented acetabular components for revision surgery have not demonstrated long-term success. The use of a protrusio ring is reserved primarily for massive bone loss such as a Paprosky type III bone loss with significant superior migration of the acetabular component. The best clinical results for acetabular component revision have been achieved with cementless porous-coated implants. Haddad FS, Masri BA, Garbuz DS, et al: Acetabulum, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 923-936. D'Antonio JA: Periprosthetic bone loss of the acetabulum: Classification and management. Orthop Clin North Am 1992;23:279-290.
References:
- Rubash HE, Sinha RK, Paprosky W, et al: A new classification system for the management of acetabular osteolysis after total hip arthroplasty. Instr Course Lect 1999;48:37-42.
Question 48High Yield
Fixed hyperextension of the metatarsophalangeal joint is associated with
Explanation
Explanation
Claw toe and hammer toe deformities are associated with dorsal subluxation of the interossei, which can no longer serve to flex the metatarsophalangeal joint. The extensor digitorum longus then loses its tenodesing effect on the proximal interphalangeal and distal interphalangeal joints and works unopposed to extend the metatarsophalangeal joint and the proximal phalanx. Without the antagonistic action of the extensor digitorum longus, the extrinsic flexors become unopposed flexors of the proximal and distal interphalangeal joints. Marks RM: Anatomy and pathophysiology of lesser toe deformities. Foot Ankle Clin 1998;3:199-213.
References:
- Myerson MS, Shereff MJ: The pathological anatomy of claw and hammer toes. J Bone Joint Surg Am 1989;71:45-49.
Question 49High Yield
Six weeks after onset, what is the most clearly accepted indication for surgical management for lumbar disk herniation?
Explanation
Explanation
In the absence of a cauda equina syndrome or progressive weakness, the best indication for surgical management is refractory radicular pain. Surgical decision-making should not be based on the size of the herniation. Large extruded herniations tend to resolve more predictably than smaller herniations. Stable motor weakness and numbness resolve similarly in both surgical and nonsurgical management, although surgery hastens the process. When intractable radicular pain is the strict indication for surgery, surgical intervention provides substantial and more rapid pain relief than nonsurgical care. Rhee JM, Schaufele M, Abdu WA: Radiculopathy and the herniated lumbar disc: Controversies regarding pathophysiology and management. J Bone Joint Surg Am 2006;88:2070-2080.
Question 50High Yield
An 8-year-old boy has had pain and swelling around the right knee for the past 4 weeks. He recalls bumping it about 4 weeks ago. He has no pain in other joints, and denies any fevers, chills, or other symptoms. A radiograph is shown in Figure 13. Laboratory studies show a WBC count of 9,700/mm3, an erythrocyte sedimentation rate of 18 mm/h, and a C-reactive protein level of 3.7 mg/L. What is the next most appropriate step in management?
Explanation
Explanation
The history and laboratory findings are consistent with osteomyelitis of the patella. The radiograph reveals bone destruction in the patella; therefore, the next most appropriate step is open biopsy and debridement of the site. Aspiration of the knee joint may be needed to rule out septic arthritis prior to patellar debridement. With this amount of bone destruction, surgical debridement is helpful to obtain cultures and to remove necrotic material. Administering antibiotics without any prior culture increases the risk of negative cultures later and a potentially incorrect choice of antibiotic. A neoplasm should be included in the differential. It would be inappropriate to initiate chemotherapy and radiation therapy without a biopsy-confirmed diagnosis. A bone scan is likely to demonstrate uptake, but radiographs have already localized the abnormality to the patella. Morrisy RT: Bone and joint sepsis, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 466-470.
References:
- Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis, and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Question 51High Yield
A 15-year-old girl who competes in gymnastics has immediate pain and giving way of the left elbow after falling from the uneven parallel bars and landing on her outstretched arms. Examination reveals swelling and tenderness about the elbow, especially over the medial side. Measurement of elbow motion shows 0 degrees to 125 degrees of flexion, and valgus stress at the elbow is painful. AP, lateral, and stress radiographs are shown in Figures 9a through 9c. Management should consist of


Explanation
While many low-demand patients with injuries to the ulnar collateral ligament can be treated nonsurgically, Jobe and associates described two situations in which ulnar collateral ligament reconstruction is indicated: (1) an acute complete rupture in a competitive athlete who uses the upper extremities extensively and who wishes to remain active; and (2) chronic pain or instability that does not improve after at least 3 months of nonsurgical management. Rarely is direct surgical repair of the ligament possible or able to withstand the valgus stresses applied to the elbow. Most authors recommend surgical reconstruction of the ulnar collateral ligament using a palmaris longus, plantaris, or fourth toe extensor tendon from the fourth autograft. Andrews JR, Jelsma RD, Joyce ME, et al: Open surgical procedures for injuries to the elbow in throwers. Oper Tech Sports Med 1994;4:109-133. Jobe FW, Kvitne RS: Elbow instability in the athlete. Instr Course Lect 1991;40:17-23.
Question 52High Yield
Figure 30 shows the MRI scan of a 68-year-old woman who has left hip pain. What is the most appropriate treatment?
Explanation
The patient has a large zone of osteonecrosis of the left femoral head. The wedge-shaped zone of decreased signal intensity on the T1 image in the subchondral region of the femoral head is typical. Based on these findings, total hip arthroplasty is the most appropriate treatment. Open reduction and internal fixation will not help this condition. Incisional biopsy is indicated only if the MRI scan shows a probable neoplasm. Resection of the proximal femur is indicated only for aggressive malignancy. Arthrodesis may be considered in a younger patient but not in a 68-year-old individual. Other treatments, not listed, such as core decompression, vascularized fibular transplant, and osteotomy may be options in selected patients. Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 213-223.
Question 53High Yield
Figure 23 shows the radiograph of a 7 year-old girl with a low thoracic-level myelomeningocele. She has a history of skin ulcers over the apex of the deformity, but her current skin condition is good. Management of the spinal deformity should consist of
Explanation
This form of severe kyphosis results in intractable difficulties with sitting position, compression of internal organs, and chronic skin breakdown. Kyphectomy and posterior fusion with instrumentation, while associated with a high rate of complications, provides one of the best solutions to this clinical dilemma. The other choices are either completely ineffective or inadequate in managing this degree of deformity. Lindseth RE: Spine deformity in myelomeningocele. Instr Course Lect 1991;40:273-279.
Question 54High Yield
A 14-year-old competitive gymnast has had activity-related low back pain for the past month. Examination reveals no pain with forward flexion, but she has some discomfort when resuming an upright position. She also has pain with extension and lateral bending of the spine. The neurologic examination is normal. Popliteal angles measure 20 degrees. AP, lateral, and oblique views of the lumbar spine are negative. What is the next most appropriate step in management?
Explanation
Symptoms of activity-related low back pain, physical findings of pain with extension, lateral bending, and resuming an upright position, and relative hamstring tightness are consistent with spondylolysis. While the initial diagnostic work-up should include plain radiographs of the lumbosacral spine, the findings may be negative because it can take weeks or months for the characteristic changes to become apparent. SPECT has been a useful adjunct in the diagnosis of spondylolysis when plain radiographs are negative. Since the patient's pain is activity related and she is otherwise healthy, evaluation for infection is not indicated. Because the neurologic examination is normal, electromyography, nerve conduction velocity studies, and MRI are not indicated. CT can be used in those instances in which SPECT and bone scans are negative. Ciullo JV, Jackson DW: Pars interarticularis stress reaction, spondylolysis, and spondylolisthesis in gymnasts. Clin Sports Med 1985;4:95-110. Collier BD, Johnson RP, Carrera GF, et al: Painful spondylolysis or spondylolisthesis studied by radiography and single photon emission computed tomography. Radiology 1985;154:207-211. Jackson DW, Wiltse LL, Cirincione RT: Spondylolysis in the female gymnast. Clin Orthop 1976;117:68-73.
Question 55High Yield
A 63-year-old woman with a history of poliomyelitis has a fixed 30-degree equinus contracture of the ankle, rigid hindfoot valgus, and normal knee strength and stability. She reports persistent pain and has had several medial forefoot ulcerations despite a program of stretching, bracing, and custom footwear. What is the next most appropriate step in management?
Explanation
Explanation
The patient has a fixed deformity of the hindfoot and an Achilles tendon contracture; therefore, the treatment of choice is triple arthrodesis with Achilles tendon lengthening. Further bracing will not be helpful. Amputation is not indicated, and ankle arthrodesis will not address the hindfoot deformity. Palliative management would be more appropriate if the knee was unstable or the quadriceps were weak, because the equinus balances the ground reaction force across the knee. Perry J, Fontaine JD, Mulroy S: Findings in post-poliomyelitis syndrome: Weakness of muscles of the calf as a source of late pain and fatigue of muscles of the thigh after poliomyelitis. J Bone Joint Surg Am 1995;77:1148-1153.
References:
- Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
Question 56High Yield
A 68-year-old woman with metastatic breast carcinoma is seen in the emergency department. She appears lethargic, and she reports abdominal pain, nausea, and constipation. An EKG reveals a shortened QT interval. The only physical finding on examination is diffuse hyporeflexia. What is the most appropriate step in management?
Explanation
Explanation
Intravenous fluid administration is the best first step to treat the hypercalcemia of malignancy. Many of these patients are dehydrated, and the increased serum calcium impairs the ability of the kidney to concentrate the urine. The decreased glomerular filtration rate secondary to the hypovolemia also leads to increased tubular resorption of calcium. The establishment of normovolemia will help promote increased urinary excretion of calcium. Lasix can also be used to help promote calciuria. Mithramycin is an antibiotic derived from Streptomyces plicatus. It is part of a group of drugs referred to as chromomycin antibiotics and is the only one of this group used clinically in the United States. It is rarely used in cancer chemotherapy because of its toxicity. A number of drug-related deaths have occurred from the use of mithramycin. Its use is now limited to the treatment of hypercalcemia associated with malignancy where it is used in lower dosage than that used for the treatment of tumors. Methotrexate has no role in the treatment of hypercalcemia of malignancy. While intravenous bisphosphonates are helpful in slowing progression of metastases and may help lower cerum calcium, they are not appropriate in the emergent treatment of hypercalcemia in the metastatic cancer patient.
References:
- Stewart AF: Clinical practice: Hypercalcemia associated with cancer. N Engl J of Med 2005;352:373-379.
Question 57High Yield
A 16-year-old boy with osteochondritis dissecans of the capitellum has intermittent symptoms of catching and locking. Examination is unremarkable. Radiographs reveal a loose body anteriorly with a diameter of 10 mm. To remove the loose body, elbow arthroscopy is being considered. Which of the following procedures would minimize the risk of neurovascular complication during the procedure?
Explanation
Complications of elbow arthroscopy are usually minor or temporary. However, serious complications include nerve injuries. The deep radial nerve is the closest to any of the portals, resting as close as 1 mm away from the scope inserted in the anterolateral portal. The capsule can be displaced anteriorly by distending the joint with about 25 mL of saline solution, thus moving the deep radial nerve approximately 1 cm anteriorly and decreasing the risk of injuring it while establishing the anterolateral portal. Keeping plastic cannulae in the portals may help to diminish fluid extravasation and swelling, which is more of an impediment than a serious complication. The image intensifier has no documented role in guiding loose body removal. While the proximal anteromedial portal is probably the safest anterior portal to establish, it is actually easier to remove a large loose body from this portal while viewing it from an anterolateral position. There is less tendon and muscle bulk to pass through at the site of the proximal anteromedial portal than at the anterolateral portal, making it less likely for the loose body to get stuck in the soft tissues. Techniques have been developed to permit removal of loose bodies as large as 2 cm in diameter without breaking them up into pieces. If it is possible to remove a large loose body intact, doing so greatly simplifies and shortens the procedure. Lynch GJ, Meyers JF, Whipple TL, Caspari RB: Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy 1986;2:190-197.
Question 58High Yield
A 14-year-old boy sustains a right leg injury after being thrown from his motorcycle while racing. He reports diffuse right leg pain starting at his knee and proceeding distally to include his foot. After the injury the patient's mother reports the tibia moving posteriorly then anteriorly while she was supporting the leg. In the emergency department 4 hours after injury, examination reveals a large knee effusion, firm compartments of the leg, a palpable posterior tibialis pulse with a warm, pink foot, and capillary refill of 2 seconds at the toes. His blood pressure is 100/50 mm Hg. Motor examination is intact, but there is decreased sensation in the dorsal first interspace and plantar aspect of the foot. Compartment pressure measurement reveals all four compartments with pressures of 33, 36, 33, and 38 mm Hg respectively. Radiographs are shown in Figure 59a and 59b. The remainder of the skeletal examination is normal. What is the optimal management for this injury?
Explanation
Explanation
59b The patient has a compartment syndrome based on the firm compartments of the leg and the elevated compartment pressures measured at the diastolic pressure reading. Muscle ischemia occurs quickly when compartment pressures are elevated, and within 6 hours irreversible damage can occur. Emergent fasciotomies permit decompression of all four compartments and reestablishment of vascular supply to the muscles. Stabilization of the fracture prevents further soft-tissue injury.
Question 59High Yield
A 12-year-old girl has had lower back pain for the past 6 months that interferes with her ability to participate in sports. She denies any history of radicular symptoms, sensory changes, or bowel or bladder dysfunction. Examination reveals a shuffling gait, restriction of forward bending, and tight hamstrings. Radiographs show a grade III spondylolisthesis of L5 on S1, with a slip angle of 20 degrees. Management should consist of
Explanation
Indications for surgical treatment of spondylolisthesis include pain and/or progression of deformity. Specifically, surgery is necessary when there is persistent pain or a neurologic deficit that fails to respond to nonsurgical therapy, there is significant slip progression, or the slip is greater than 50%. For patients with mild spondylolisthesis, in situ posterolateral L5-S1 fusion is adequate. In patients with more severe slips (greater than 50%), extension of the fusion to L4 offers better mechanical advantage. Postoperative immobilization may be achieved with instrumentation, casting, or both. In patients with a slip angle of greater than 45 degrees, reduction of the lumbosacral kyphosis with instrumentation or casting is desirable to prevent slip progression. Laminectomy alone is contraindicated in a child. Nerve root decompression is indicated if radiculopathy is present clinically. Seitsalo S, Osterman K, Hyvarinen H, Tallroth K, Schlenzka D, Poussa M: Progression of spondylolisthesis in children and adolescents: A long-term follow-up of 272 patients. Spine 1991;16:417-421.
Question 60High Yield
A 25-year-old patient who sustained multiple bilateral rib fractures, a pulmonary contusion, a left nondisplaced transtectal acetabular fracture, and a closed humerus fracture in a motor vehicle accident 2 weeks ago is transferred from another hospital. The humerus fracture has been surgically treated. There are no signs of infection, and the trauma surgeon wants to mobilize the patient as soon as possible. Radiographs are shown in Figures 15a and 15b. Management of the humerus fracture should consist of
Explanation
Explanation
15b The radiographs show a distal third humerus fracture that is angulated, rotated, and not rigidly fixed. Rigid fixation is needed because mobilization is highly desirable to improve pulmonary function. The acetabular fracture is through the weight-bearing dome but is nondisplaced. Nonsurgical management of the acetabular fracture requires at least 6 weeks of touchdown weight bearing to minimize the forces across the hip joint. Open reduction and plate fixation would achieve anatomic reduction and immediate mobilization. A single posterolateral 4.5-mm plate or two 3.5-mm plates at 90 degrees are possible alternatives. Immediate weight bearing on a plated humerus fracture with the use of crutches or a walker has been shown to be safe and would allow touchdown weight bearing, protecting the hip. None of the other options would achieve this goal for this distal fracture.
References:
- Tingstad EM, Wolinsky PR, Shyr Y, Johnson KD: Effect of immediate weightbearing on plated fractures of the humeral shaft. J Trauma 2000;49:278-280.
Question 61High Yield
A patient who underwent total knee arthroplasty now reports a loss of sensation in the area circled in Figure 38. This area is innervated by which of the following nerves?
Explanation
The saphenous nerve follows the saphenous vein, giving off the infrapatellar branch that crosses the knee anteriorly to supply the peripatellar skin. A longitudinal incision can interrupt the nerve, leaving the terminal distribution without sensation.
Question 62High Yield
A 17-year-old high school long distance runner is seeking advice before running a marathon for the first time. What advice should be given regarding his fluid, carbohydrate, and electrolyte intake around the time of the race?
Explanation
Explanation
The goal of fluid replenishment should be to replace the sweat that has been lost. Sweat is mostly water, with a small concentration of salts and other electrolytes. Absorption is enhanced by solutions of low osmolality. Scientific research has also shown that adding carbohydrates to the drink improves athletic performance. Carbohydrates such as glucose and maltodextrins (glucose polymers) stimulate fluid absorption by the intestines. Fructose slows intestinal absorption of fluids. Drinks that are high in fructose, such as orange juice, can lead to gastrointestinal distress and osmotic diarrhea. Kirkendall D: Fluids and electrolytes, in The U.S. Soccer Sports Medicine Book. Baltimore, MD, Williams and Wilkins, 1996.
References:
- Gisolfi CV, Duchman SM: Guidelines for optimal replacement beverages for different athletic events. Med Sci Sports Exerc 1992;24:679-687.
Question 63High Yield
A 34-year-old woman has had painful snapping and popping in the elbow since falling while in-line skating 6 months ago. The popping also occurs when she pushes off with her hands to rise from a seated position. Initial radiographs were normal, and she was told that she had sprained her elbow. Examination reveals few findings except that she is very apprehensive when the forearm is forcefully supinated with the elbow extended or partially flexed. A radiograph taken in that position is shown in Figure 24. Treatment should consist of
Explanation
Explanation
The radiograph reveals posterolateral rotatory subluxation of the radiohumeral and ulnohumeral joints. The space between the ulna and trochlea is enlarged, particularly posteriorly at the olecranon. These findings are diagnostic of posterolateral rotatory instability, which causes recurrent subluxation and reduction as the elbow is flexed from an extended and supinated position with valgus load. The posterolateral rotatory instability apprehension test was performed on this patient and the result was positive. The lateral pivot-shift test causes a clunk as the elbow reduces but is more difficult to perform, even under general anesthesia. The patient does not have isolated subluxation of the radial head, although these findings can be mistakenly diagnosed as such. The radial head is normally shaped and does not represent a congenital dislocation. There are no findings here to suggest osteochondritis dissecans or loose bodies. O'Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446. Burgess RC, Sprague HH: Post-traumatic posterior radial head subluxation: Two case reports. Clin Orthop 1984;186:192-194.
References:
- Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354.
Question 64High Yield
An 18-month-old child with obstetrical palsy has a maximum external rotation as shown in Figure 34. The parents should be advised that without surgical treatment the likelihood that glenoid dysplasia will develop is approximately what percent?
Explanation
Based on the available literature, the probability of development of glenoid dysplasia in the setting of a significant limitation of external rotation is close to 70%. Humeral dysplasia is also likely and can be managed surgically. Efforts are being made to identify procedures that will prevent glenoid dysplasia and help maintain function. Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:659-667. Waters PM, Smith GR, Jaramillo D: Glenohumeral deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:668-677.
Question 65High Yield
A 59-year-old construction worker who is right-hand dominant has had right shoulder pain for the past 9 months with no history of injury. Nonsurgical management consisting of two cortisone injections, physical therapy for 3 months, and nonsteroidal anti-inflammatory drugs has failed to provide lasting relief. Examination reveals tenderness over the acromioclavicular (AC) joint and over the subacromial bursa. He has positive Neer and Hawkins impingement signs and AC joint pain with adduction of the shoulder. Radiographs are shown in Figures 36a and 36b. An MRI scan reveals an intact rotator cuff. Management should now consist of

Explanation
Because the patient has clinical and radiographic signs of AC arthritis and subacromial impingement, the treatment of choice is anterior acromioplasty and distal clavicle excision. Arthroscopic acromioplasty alone would not address the AC arthritis. The rotator cuff is intact; therefore, rotator cuff repair is not indicated. An open Mumford procedure would address the AC arthritis only and not the impingement symptoms. Immobilization might lead to stiffness of the shoulder and is not recommended for treating impingement.
Question 66High Yield
A 73-year-old woman reports a 4-month history of severe left-sided posterior buttock pain and left leg pain. The leg pain radiates into the left lateral thigh and posterior calf with cramping. Examination reveals mild difficulty with a single-leg toe raise on the left side and a diminished ankle reflex. There is also a significant straight leg raise test at 45 degrees which exacerbates symptoms. An MRI scan is shown in Figure 4. What is the most appropriate treatment at this time?
Explanation
Lumbar spinal stenosis with lumbar radiculopathy can be commonly caused by a synovial cyst arising from the facet joints. Lyons and associates reported on the surgical treatment of synovial cysts in 194 patients. Of the 147 with follow-up data, 91% reported good pain relief and 82% had improvement of their motor deficits. Epstein reported a 58% to 63% incidence of good/excellent results and a 38 to 42 point improvement on the SF-36 Physical Function Scale. It was also suggested that since the presence of a synovial cyst indicates facet pathology, possible fusion should be considered in these patients, especially those with underlying spondylolisthesis. Lyons MK, Atkinson JL, Wharen RE, et al: Surgical evaluation and management of lumbar synovial cysts: The Mayo Clinic Experience. J Neurosurg 2000;93:53-57. Khan AM, Synnot K, Cammisa FP, et al: Lumbar synovial cysts of the spine: An evaluation of surgical outcome. J Spinal Disord Tech 2005;18:127-131.
Question 67High Yield
A 13-year-old boy is comatose and has irregular breathing after being struck by a car while riding his bicycle. Auscultation suggests a pneumothorax on the right side and swelling about the right arm and leg. Initial management should consist of
Explanation
Explanation
The first priority is to gain control of the airway with intubation. Following intubation, management should consist of ventilation and placement of a chest tube if needed, vascular access and circulatory stabilization, radiographs of the cervical spine and chest, and CT of the brain. American College of Surgeons Committee on Trauma. Advanced Trauma Life Support Course. Instructor's Manual. Chicago, IL, American College of Surgeons, 1984.
References:
- Eichelberger MR, Randolph JG: Pediatric trauma: An algorithm for diagnosis and therapy. J Trauma 1983;23:91-97.
Question 68High Yield
Figure 2 shows the radiograph of a 72-year-old woman who reports pain after a fall. History includes several years of increasing thigh pain and limb shortening. Management consisting of an extensive work-up for infection reveals normal laboratory studies, a positive bone scan, and a negative hip aspiration. What is the most likely etiology of this complication?
Explanation
The patient has a midstem periprosthetic fracture, which commonly results in loosening of the prosthesis. Patients who have a large amount of bone loss may require an allograft with the surgical reconstruction. Although the patient reported a fall, her history is also consistent with preexisting loosening of the prosthesis. Chronic infection has been shown in up to 16% of these fractures; however, the patient's work-up revealed no infection. Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242. Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Question 69High Yield
A 60-year-old man reports that he has had shoe pressure pain over his right great toe for several years but has minimal discomfort when barefoot or in sandals. A clinical photograph and radiographs are shown in Figures 1a through 1c. Management should consist of
Explanation
Explanation
1b 1c Some patients have minimal symptoms associated with hallux rigidus despite significant radiographic evidence of osteoarthritis. This patient's symptoms are primarily related to shoe pressure from the exostosis and can be managed with extra-depth shoe wear. Smith RW, Katchis SD, Ayson LC: Outcomes in hallux rigidus patients treated nonoperatively: A long-term follow-up study. Foot Ankle Int 2000;21:906-913.
References:
- Shereff MJ, Baumhauer JF: Hallux rigidus and osteoarthrosis of the first metatarsophalangeal joint. J Bone Joint Surg Am 1998;80:898-908.
Question 70High Yield
A superior labrum anterior and posterior (SLAP) lesion doubles the strain in which of the following stabilizing structures?
Explanation
A superior labrum, when intact, stabilizes the shoulder by increasing its ability to withstand excessive external rotational forces by an additional 32%. The presence of a SLAP lesion decreases this restraint and increases the strain in the superior band of the inferior glenohumeral ligament by over 100%. Rodosky MW, Harner CD, Fu FH: The role of the long head of the biceps muscle and superior glenoid labrum in anterior stability of the shoulder. Am J Sports Med 1994;22:121-130.
Question 71High Yield
A 32-year-old amateur bowler has progressive pain in the lateral aspect of the proximal forearm and elbow. Nonsurgical management consisting of a tennis elbow brace, nonsteroidal anti-inflammatory drugs, and activity modification has failed to provide relief. Examination reveals tenderness in the lateral aspect of the proximal forearm and exacerbation of symptoms with resisted finger extension. Radiographs of the elbow reveal no abnormalities. Which of the following studies will aid in diagnosis?
Explanation
It is often difficult to accurately discern between lateral epicondylitis and radial tunnel syndrome. Neither MRI nor a bone scan is likely to reveal abnormalities. Electrodiagnostic studies are often inconclusive, and radial tunnel syndrome often presents without motor weakness. The symptoms of radial tunnel syndrome are expected to improve with an injection of lidocaine into the radial tunnel; therefore, this is the test of choice in this clinical scenario. Radiographs of the wrist will not assist in making the diagnosis. Eversmann WW Jr: Entrapment and compression neuropathies, in Green DP (ed): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingston, 1993, pp 1341-1385.
Question 72High Yield
A 38-year-old man underwent a transtibial amputation for chronic posttraumatic foot and ankle pain and chronic calcaneal osteomyelitis. Postoperative radiographs are seen in Figures 41a and 41b. What is the proposed purpose of the surgical modification seen in the radiographs?

Explanation
The Ertl modification of a below-knee amputation has been proposed to create a more stable "platform" to aid in transferring the load of weight bearing between the residual limb and the prosthetic socket. It is felt that a stable platform allows total contact loading over an enlarged stable surface area. Early studies have suggested that this modification may enhance the patient's perceived functional outcome. Pinzur MS, Pinto MA, Saltzman M, et al: Health-related quality of life in patients with transtibial amputation and reconstruction with bone bridging of the distal tibia and fibula. Foot Ankle Int 2006;27:907-912.
Question 73High Yield
A patient with a below-the-knee amputation is being evaluated for a new prosthesis. He wants to improve his ability to walk on uneven surfaces. What modification to the prosthesis can be made to accommodate this request?
Explanation
Changing from a solid keel to a keel with a sagittal split allows an amputee to navigate uneven terrain more easily. Changing the length of the keel affects the responsiveness of the prosthesis but does not address the surface conditions for ambulation. The SACH is not used as frequently anymore, because overload problems to the nonamputated foot have been observed. Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 31-45.
Question 74High Yield
A 42-year-old man has a symptomatic flatfoot deformity and walks with a slight limp after falling off a scaffold 9 months ago. He also reports that he has had difficulty returning to work. Orthotics have failed to provide relief. Current radiographs are shown in Figures 19a and 19b. To relieve his pain and return the patient to work, treatment should consist of

Explanation
Because the patient has sustained a tarsometatarsal injury with midfoot sag, the treatment of choice is a tarsometatarsal arthrodesis. The cause of his flatfoot deformity is secondary to the tarsometatarsal injury and not from posterior tibialis tendon deficiency. Lateral column lengthening, double arthrodesis, and calcaneal osteotomy are not indicated. Although open reduction and internal fixation may be performed late when arthritis is present, these procedures are less likely to succeed. Komenda GA, Myerson MS, Biddinger KR: Results of arthrodesis of the tarsometatarsal joints after traumatic injury. J Bone Joint Surg Am 1996;78:1665-1676.
Question 75High Yield
After stabilizing a bimalleolar ankle fracture with a plate and lag screws for the fibula and two interfragmental compression screws for the medial malleolus, a syndesmosis screw is indicated in which of the following situations?
Explanation
Explanation
It is imperative to recognize the need for a position screw (syndesmosis screw) to hold the syndesmosis in proper alignment when surgically stabilizing an ankle fracture. Although many different fracture patterns are suspicious for a disrupted syndesmosis, the only sure way to assess the syndesmosis is to stress it with abduction and external rotation of the talus and attempt to displace the fibula from the incisura fibularis. Under fluoroscopy, the talus will move laterally and displace the fibula, show a valgus talar tilt, or show an increase in the medial clear space. If any or all of these signs occur, a syndesmosis screw is inserted after making sure that the fibula is reduced into the incisura fibularis. This screw may traverse three or four cortices but must not act as a lag screw. It usually is inserted with the ankle in maximal dorsiflexion, although this is probably not necessary because it is almost impossible to overcompress the syndesmosis. The diameter of the screw does not make any difference. It may or may not be removed but not before 3 months. Tornetta P III, Spoo JE, Reynolds FA, Lee C: Overtightening of the ankle syndesmosis: Is it really possible? J Bone Joint Surg Am 2001;83:489-492. Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119. Hahn DM, Colton CL: Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
References:
- Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
Question 76High Yield
Figure 8 shows the AP radiograph of a 33-year-old woman who sustained a midshaft clavicle fracture from a motorcycle accident 15 months ago. She continues to have significant pain with activities of daily living. Management should consist of
Explanation
The patient has a symptomatic painful atrophic midclavicular nonunion, and the treatment of choice is rigid internal fixation with a dynamic compression plate and autogenous bone grafting. A tension band effect is desired and achieved by placing the plate superiorly. Excellent success rates of 90% to 100% have been reported using this technique. Intramedullary screw fixation without bone grafting has a decreased success rate. Partial claviculectomy is not a preferred option. Jupiter JB, Leffert RD: Non-union of the clavicle: Associated complications and surgical management. J Bone Joint Surg Am 1987;69:753-760.
Question 77High Yield
A 69-year-old woman has just undergone an uncomplicated total shoulder arthroplasty for glenohumeral osteoarthritis. A press-fit humeral stem and a cemented all-polyethylene glenoid component were placed. At this point, what is the postoperative rehabilitation plan?
Explanation
The patient needs to immediately begin an active assisted range-of-motion program emphasizing forward elevation and external rotation to the side. Sling immobilization without stretching for either 3 or 6 weeks will result in severe stiffness that will compromise her ultimate range of motion. Since she has a good quality subscapularis tendon, there is no need to avoid beginning external rotation to the side. However, starting a strengthening program at 3 weeks risks tearing the subscapularis tendon repair. Active strengthening should not begin for 6 weeks postoperatively to allow the subscapularis tendon repair time to heal. Boardman ND III, Cofield RH, Bengston KA, et al: Rehabilitation after total shoulder arthroplasty. J Arthroplasty 2001;16:483-486.
Question 78High Yield
A 2-year-old child is being evaluated for limb-length and girth discrepancy. As a newborn, the patient was large for gestational age and had hypoglycemia. Current examination shows enlargement of the entire right side of the body, including the right lower extremity and foot. The skin shows no abnormal markings, and the neurologic examination is normal. The spine appears normal. Radiographs confirm a 2-cm discrepancy in the lengths of the lower extremities. Additional imaging studies should include
Explanation
Explanation
The patient may have Beckwith-Wiedemann syndrome (BWS), which consists of exophthalmos, macroglossia, gigantism, visceromegaly, abdominal wall defects, and neonatal hypoglycemia. Hemihypertrophy develops in approximately 15% of patients with BWS. Patients with hemihypertrophy that is the result of BWS have a 40% chance of developing malignancies such as Wilms' tumor or hepatoblastoma; therefore, frequent ultrasound screening is recommended until about age 7 years. The absence of nevi and vascular markings helps to rule out other causes of hemihypertrophy, such as neurofibromatosis, Proteus syndrome, and Klippel-Trenaunay syndrome. Bone age estimations are not accurate at this young age but may become more useful later to help predict the timing of epiphysiodesis procedures. DeBaun MR, Tucker MA: Risk of cancer during the first four years of life in children from The Beckwith-Wiedemann Syndrome Registry. J Pediatr 1998;132:398-400. Ballock RT, Wiesner GL, Myers MT, et al: Hemihypertrophy concepts and controversies. J Bone Joint Surg Am 1997;79:1731-1738.
References:
- Carpenter CT, Lester EL: Skeletal age determination in young children: Analysis of three regions of the hand/wrist film. J Pediatr Orthop 1993;13:76-79.
Question 79High Yield
Which of the following represents a contraindication for interspinous process decompression for the treatment of lumbar spinal stenosis?
Explanation
Kondrashov and associates noted stable good outcomes at 4 years in 14 of 18 patients treated with X-STOP interspinous process decompression as defined as an improvement over preoperative Oswestry scores of 15 points or more. Similar results were seen after 1 year in a European study by Siddiqui and associates. Exclusion and inclusion criteria for these studies varied somewhat, but cauda equina syndrome was the only exclusion criteria listed in both studies. All of the other choices did not represent exclusion criteria in either study. Kondrashov DG, Hannibal M, Hsu KY, et al: Interspinous process decompression with the X-STOP device for lumbar spinal stenosis: A 4-year follow-up study. J Spinal Disord Tech 2006;19:323-327.
Question 80High Yield
Which of the following accurately defines changes in Vitamin D requirements as the result of aging?
Explanation
Explanation
Older individuals ingest less Vitamin D and are unable to generate as much as younger people via the skin in response to ultraviolet exposure; thus, there is a decrease in the levels of serum 25(OH) D. This reduction in 25(OH)D leads to a reduction in calcium absorption. There is also decreased conversion in the kidney of 25(OH)D to 1,25(OH)D. This all leads to an increase in the daily requirements of both calcium and Vitamin D. It also results in a responsive increase in PTH secretion in the elderly, as well as renal function impairment and possible renal resistance to PTH. Dawson-Hughes B, Harris SS, Krall EA, et al: Effect of calcium and vitamin D supplementation on bone density in men and women 65 years of age and older. N Engl J Med 1997;337:670-676. Recker RR, Hinders S, Davies M, et al: Correcting calcium nutritional deficiency prevents spine fractures in elderly women. J Bone Miner Res 1996;11:1961-1966.
References:
- Rosen CJ, Kiel DP: The aging skeleton, in Favus, MJ (ed): Primer on Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 57-59.
Question 81High Yield
A patient with a left-sided C6-7 herniated nucleous pulposis would likely have which of the following constellation of findings?
Explanation
A C6-7 herniation affects the C7 root. The C7 root has the middle finger as its predominant sensory distribution. Its motor function is the triceps, wrist extension, and finger metacarpophalangeal extension. The reflex is the triceps. Magee D: Principles and concepts, in Orthopedic Physical Assessment, ed 3. Philadelphia, PA, WB Saunders, 1997, pp 1-18.
Question 82High Yield
The so-called high ankle sprain from an external rotation mechanism of injury typically involves injury to which of the following structures?
Explanation
Explanation
Ankle sprains most commonly involve injury to the lateral collateral ligaments of the ankle (anterior talofibular, posterior talofibular, and calcaneofibular) from an inversion mechanism of injury. A different entity has been more recently described that involves an external rotation mechanism of injury that widens the ankle mortise and disrupts the anterior inferior tibiofibular ligament. Deltoid ligament and extensor retinaculum injuries do occur, although infrequently, and involve eversion and extreme plantar flexion mechanisms, respectively. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 182. Kaye RA: Stabilization of ankle syndesmosis injuries with a syndesmosis screw. Foot Ankle 1989;9:290-293. Baxter DE: The Foot and Ankle in Sports. St Louis, MO, Mosby-Year Book, 1995, p 30.
References:
- Pfeffer GB (ed): Chronic Ankle Pain in the Athlete. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 11.
Question 83High Yield
A 67-year-old woman has persistent anterior thigh and knee pain after undergoing total knee arthroplasty 1 year ago. Examination and radiographs reveal no problems in the knee, mild hip flexor weakness (grade 4+), and decreased sensation over the anterior thigh including and proximal to the incision. MRI of the lumbar spine will most likely reveal which of the following findings?
Explanation
Explanation
Degenerative spondylolisthesis at L3-4 is the most likely diagnosis. This spondylolisthesis would result in foraminal stenosis affecting the third lumbar root and leading to anterior thigh and knee pain and hip flexor weakness. L4-5 spondylolisthesis would impinge on the L4 root in the foramen. Degenerative disk disease without hypertrophy is unlikely to have root impingement. Posterolateral herniations typically affect the inferior root and are less common in this age group. Hoppenfeld S: Physical Examination of the Spine and Extremities. Upper Saddle River, NJ, Prentice Hall, 1976, p 250.
References:
- Lauerman WC, Goldsmith ME: Spine, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 353-378.
Question 84High Yield
An otherwise healthy 70-year-old man has back and bilateral leg pain in an L5 distribution that is aggravated by standing more than 10 minutes or walking more than 100 feet. He has to sit to get relief. Neurologic and pulse examinations are normal. A radiograph and MRI scan are shown in Figures 4a and 4b. Treatment should consist of
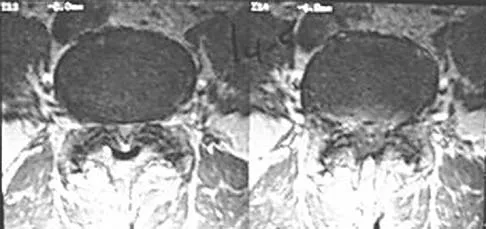
Explanation
The patient has a degenerative spondylolisthesis at L4-5 with associated spinal stenosis. His symptoms are consistent with neurogenic claudication. Based on these findings, the surgical treatment of choice is decompression and posterolateral fusion. Use of instrumentation is controversial. Laminectomy alone is reserved for the patient who is frail medically. There is no role for an anterior approach or for fusion alone without decompression. Fischgrund JS, Mackay M, Herkowitz HN, et al: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 1997;22:2807-2812.
Question 85High Yield
During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following?
Explanation
Explanation
With subscapularis tendon ruptures that have biceps tendon pathology, treatment with tenodesis or tenotomy has improved clinical results. Subluxation or dislocation of the biceps tendon is common with subscapularis rupture. Dislocation of the biceps can occur either beneath the tendon, within the tendon, or extra-articularly. In all cases, the restraints to medial translations of the biceps have been disrupted. Attempts at recentering the biceps have not been successful, and clinical results appear to be improved when tenodesis or tenotomy is employed in the treatment of the unstable biceps associated with subscapularis tears. Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10. Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
References:
- Edwards TB, Walch G, Sirveaux F, et al: Repair of tears of the subscapularis. J Bone Joint Surg Am 2005;87:725-730.
Question 86High Yield
A 23-year-old man is involved in a motor vehicle accident. An AP radiograph is shown in Figure 29a, and axial and sagittal CT scans are shown in Figures 29b and 29c. Neurologic examination shows 1/5 strength of his quadriceps and iliopsoas on the right, with 1/5 quadriceps function on the left. Definitive treatment of his injury should consist of


Explanation
The imaging studies show a fracture-dislocation. Surgical treatment of this injury consists of a decompression reduction, stabilization, and fusion. A posterolateral decompression can also be performed as necessary. An isolated anterior procedure in this type of injury is contraindicated. The anterior longitudinal ligament is most likely intact; therefore, an anterior procedure further destabilizes the spine. Reduction by an anterior approach would also be difficult. Nonsurgical management of the neurologic injury in this patient is not indicated. Theiss SM: Thoracolumbar and lumbar spine trauma, in Stannard JP, Schmidt AH, Kregor PJ (eds): Surgical Treatment of Orthopaedic Trauma. New York, NY, Thieme, 2007, pp 179-207.
Question 87High Yield
The parents of a 10-year-old boy with Down syndrome are seeking sports clearance for participation in the high jump at the Special Olympics. He is asymptomatic, and the neurologic examination is normal. The hips and patellae are clinically stable. Radiographs of the cervical spine in flexion and extension show a maximum atlanto-dens interval (ADI) of 6 mm. Based on these findings, what recommendation should be made?
Explanation
Explanation
In approximately 15% of children with Down syndrome, atlantoaxial instability develops because of ligament laxity, making them susceptible to spinal cord injury with relatively minor trauma. The American Academy of Pediatrics recommends lateral flexion-extension views of the cervical spine in any patient with Down syndrome who wishes to participate in sports. A normal ADI is up to 4 mm. Patients with Down syndrome with an ADI of more than 5 mm should not participate in contact sports or sports with a high risk for neck injury, such as diving, gymnastics, high jump, or butterfly stroke. Cervical fusion has a very high rate of complications in patients with Down syndrome and is recommended only for patients who have myelopathic signs or symptoms. Atlantoaxial instability in Down syndrome: Subject review. American Academy of Pediatrics Committee on Sports Medicine and Fitness. Pediatrics 1995;96:151-154. Tredwell SJ, Newman DE, Lockitch G: Instability of the upper cervical spine in Down syndrome. J Pediatr Orthop 1990;10:602-606.
References:
- Segal LS, Drummond DS, Zanotti RM, et al: Complications of posterior arthrodesis of the cervical spine in patients who have Down syndrome. J Bone Joint Surg Am 1991;73:1547-1554.
Question 88High Yield
A 45-year-old woman has had intense pain in her foot for the last 3 days. She also reports a mild fever and difficulty with shoe wear. Examination reveals a swollen, slightly erythematous warm foot with tenderness at the great toe metatarsophalangeal joint and pain with passive motion of the joint. An AP radiograph is shown in Figure 13. Which of the following will best aid in determining a definitive diagnosis?
Explanation
The patient has gouty arthropathy of the first metatarsophalangeal joint. This definitive diagnosis is achieved with aspiration of the joint and polarized light microscopy that shows needle-shaped negatively birefringent monosodium urate crystals. Differential diagnoses of infectious arthritis and pseudogout are also definitively made through joint aspiration. Although rheumatoid arthritis is a possibility, a serum rheumatoid factor is not always diagnostic and a patient with rheumatoid arthritis may have concomitant gouty arthritis. The radiographic findings are not typical of diabetes mellitus or of a patient with Charcot arthropathy. Wise CM, Agudelo CA: Diagnosis and management of complicated gout. Bull Rheum Dis 1998;47:2-5.
Question 89High Yield
Which of the following findings is a contraindication to isolated percutaneous pinning of a distal radius fracture?
Explanation
Intrafocal pinning allows the Kirschner wires to be placed through a site of comminution and then drilled through intact cortex. Generally Kapandji intrafocal pinning is done for dorsal comminuted extra-articular dorsal bending fractures, but it also may be used to elevate and buttress radial comminution. Simple intra-articular fractures can also be treated with pinning alone. Intrafocal pinning works best as a dorsal or radial buttress to prevent shortening. When there is volar comminution, the fracture is prone to shortening and supplemental external fixation or plating is recommended. Trumble TE, Wagner W, Hanel DP, et al: Intrafocal (Kapandji) pinning of distal radius fractures with and without external fixation. J Hand Surg Am 1998;23:381-394. Choi KY, Chan WS, Lam TP, et al: Percutaneous Kirschner-wire pinning for severely displaced distal radial fractures in children: A report of 157 cases. J Bone Joint Surg Br 1995;77:797-801.
Question 90High Yield
A 63-year-old woman has a femoral neck fracture. A biopsy specimen obtained from the fracture site at the time of her hemiarthroplasty reveals metastatic carcinoma. Seven days after surgery, she becomes confused and lethargic. Which of the following laboratory values is most likely implicated in the patient's symptoms at this time?
Explanation
Explanation
Although many hematologic and electrolyte abnormalities may be present in a patient with advanced metastatic cancer, an elevated serum calcium level is most commonly associated with confusion. Treatment with hydration, diuretics, and bisphosphonates is recommended. Clohishy D: Management of skeletal metastasis in clinical orthopaedics, in Craig E (ed): Operative Orthopaedics. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 994-997.
References:
- Mundy GR: Hypercalcemia of malignancy revisited. J Clin Invest 1988;82:1-6.
Question 91High Yield
What is the most common diagnosis in a patient older than age 40 years with a destructive bony lesion?
Explanation
The most common destructive lesions in a patient older than age 40 years are, in decreasing incidence, metastatic carcinoma, multiple myeloma, lymphoma, and chondrosarcoma. Osteosarcoma is found primarily in younger patients.
Question 92High Yield
Varus deformity after talar fractures is often seen due to collapse of the medial cortex. What artery supplies this portion of the talus?
Explanation
Explanation
The artery of the tarsal canal is a branch of the posterior tibial artery. Among the branches of the artery of the tarsal canal is the deltoid artery. This arterial complex supplies the medial one third of the talar body. Disruption of this artery may lead to osteonecrosis of the medial body and subsequent collapse into varus. This is most commonly seen with talar body fractures but may be seen in Hawkins type 3 talar neck fractures. The artery of the tarsal sinus arises from the dorsalis pedis, lateral malleolar, and perforating peroneal arteries. The peroneal artery anastomoses with the calcaneal branches of the posterior tibial artery to form a plexus of vessels that supplies the posterior tubercle of the talus. Disruption of this artery would not result in collapse of the medial body, and thus would not lead to a varus deformity. Halibruton RA, Sullivan CR, Kelly PJ, et al: The extra-osseous and intra-osseous blood supply of the talus. J Bone Joint Surg Am 1958;40:1115.
References:
- Mulfinger GL, Trueta J: The blood supply of the talus. J Bone Joint Surg Br 1970;52:160-167.
Question 93High Yield
The radiograph shown in Figure 54 reveals that the plate on the second metacarpal is acting in what manner?
Explanation
There are four ways in which a plate acts: compression, tension bend, bridge or spanning, and buttress. Since there is no cortical contact with the large span of comminution, this plate is acting as a bridge plate. A bridge plate is defined as when the plate is used as an extramedullary splint attached to the two main fragments, leaving the comminution untouched.
Question 94High Yield
A patient has a humeral shaft fracture and is scheduled to undergo open reduction and internal fixation with a plate. What surgical approach will provide the greatest amount of exposure?
Explanation
Explanation
The modified posterior approach with elevation of the medial and lateral heads of the triceps can provide exposure of 94% of the humeral shaft. The traditional posterior triceps-splitting approach exposes 55% of the humeral shaft. DeFranco MJ, Lawton JN: Radial nerve injuries associated with humeral fractures. J Hand Surg Am 2006;31:655-663.
References:
- Gerwin M, Hotchkiss RN, Weiland AJ: Alternative operative exposure of the posterior aspect of the humeral diaphysis with reference to the radial nerve. J Bone Joint Surg Am 1996;78:1690-1695.
Question 95High Yield
A distal radius fracture in an elderly man is strongly predictive for what subsequent injury?
Explanation
Fractures of the distal radius increase the relative risk of a subsequent hip fracture significantly more in men than in women. A previous spinal fracture has an equally important impact on the risk of a subsequent hip fracture in both genders.
Question 96High Yield
What cell type causes the bone destruction in metastatic lesions?
Explanation
The main consequence of tumor invading the bone is activation of both osteoblasts and osteoclasts. However, the osteoclastic effect predominates in the majority of tumors early after the invasion of bone by tumor cells, causing resorption of bone. Cramer SF, Fried L, Carter KJ: The cellular basis of metastatic bone disease in patients with lung cancer. Cancer 1981;48:2649-2660.
Question 97High Yield
Which of the following methods of meniscal repair has the highest load to failure strength?
Explanation
Explanation
Numerous experimental studies have shown that vertical suture techniques are superior to all of the other noted methods. In fact, vertical sutures have been shown to be twice as strong as several of these techniques. DeHaven KE: Meniscus repair. Am J Sports Med 1999;27:242-250. Dervin GF, Downing KJ, Keene GC, McBride DG: Failure strengths of suture versus biodegradable arrow for meniscal repair: An in vitro study. Arthroscopy 1997;13:296-300.
References:
- Barber FA: Endoscopic meniscal repair: The T-fix technique. Sports Med Arthroscopy Rev 1999;7:28-33.
Question 98High Yield
A 38-year-old man who is an avid tennis player has had persistent pain over the medial aspect of his knee for the past 6 years. He notes that the pain occurs on a daily basis with any significant activity. Nonsteroidal anti-inflammatory drugs have failed to provide relief. Radiographs are shown in Figures 22a and 22b. What is the best course of action?

Explanation
In a relatively young patient who is an avid tennis player, the treatment of choice is a joint preserving procedure. The radiographs reveal varus alignment with loading of the medial compartment. After all nonsurgical management options have been used, the best treatment option is a medial opening wedge osteotomy. A lateral closing wedge osteotomy of the proximal tibia is also a reasonable option, but it is not one of the choices. A unicompartmental arthroplasty or a total knee arthroplasty would place significant restrictions in this patient. A unispacer may be a temporizing procedure but is controversial and without substantial data in the literature. The knee arthroscopy will not address the medial compartment osteoarthritis. Nagel A, Insall JN, Scuderi GR: Proximal tibial osteotomy: A subjective outcome study. J Bone Joint Surg Am 1996;78:1353-1358. Rinonapoli E, Mancini GB, Corvaglia A, et al: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
Question 99High Yield
Figures 30a and 30b show the MRI scans of a 51-year-old woman who has had an enlarging soft-tissue mass in her right thigh for the past 18 months. Examination reveals no inguinal adenopathy. Results of a biopsy show a high-grade sarcoma. A bone scan is unremarkable, and a CT scan of the chest shows no evidence of pulmonary metastasis. According to the Musculoskeletal Tumor Society (MSTS) staging system, the tumor should be classified as what stage?
Explanation
Explanation
30b According to the MSTS staging system, soft-tissue sarcomas are staged according to the following factors: grade, site, and metastasis. Roman numerals are used to designate malignant tumors, and Arabic numerals are used for benign tumors. Low-grade malignant tumors are staged as I while intermediate- and high-grade tumors are staged as II. Site is defined as intracompartmental (A) or extracompartmental (B). Any metastasis is staged as III. This patient has a high-grade tumor (II), and the MRI scans show that it is confined to a single compartment; therefore, it is staged as IIA. There is no evidence of metastatic disease. Enneking WF, Spanier SS, Goodman MA: A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop 1980;153:106-120. Peabody TD, Monson D, Montag A, Schell MJ, Finn H, Simon MA: A comparison of the prognoses for deep and subcutaneous sarcomas of the extremities. J Bone Joint Surg Am 1994;76:1167-1173. Pisters PW, Leung DH, Woodruff J, Shi W, Brennan MF: Analysis of prognostic factors in 1,041 patients with localized soft tissue sarcomas of the extremities. J Clin Oncol 1996;14:1679-1689.
References:
- Wunder JS, Healey JH, Davis AM, Brennan MF: A comparison of staging systems for localized extremity soft tissue sarcoma. Cancer 2000;88:2721-2730.
Question 100High Yield
Figure 8 shows the radiograph of a 72-year-old man who has had severe pain in the left hip for the past 3 weeks. History reveals alcohol abuse. The next most appropriate step should consist of
Explanation
Explanation
The radiograph reveals destruction of the femoral head with loss of the articular cartilage. These findings are consistent with an infected hip, and aspiration will confirm the diagnosis. Although the patient could have advanced osteonecrosis, typically the cartilage interval is maintained and such destruction is rarely associated with osteonecrosis.
References:
- Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 157-161.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon