Orthopedic Surgery Mock Exam 249: 100 High-Yield MCQs for ABOS, OITE, FRCS
14 Apr 2026
106 min read
111 Views
Key Takeaway
This page presents 100 high-yield orthopedic surgery multiple-choice questions (MCQs) for ABOS, OITE, and FRCS board exams. Test your knowledge and prepare confidently with this comprehensive practice set, designed to help surgeons master key concepts and excel in their certification.
Optimizing the Anteromedial Approach for Dist...
00:00
Start Quiz
Question 1High Yield
A patient who was involved in a motor vehicle accident 2 weeks ago now reports neck pain. Work-up reveals no evidence of nerve root involvement or acute radiographic abnormality. The patient appears to have a hyperextension soft-tissue injury of the neck (whiplash). What is the best course of treatment at this time?
Explanation
Early mobilization and resumption of normal activities immediately after neck sprain has been shown to improve functional outcome and decrease subjective symptoms as measured 6 months after injury. Borchgrevink GE, Kaasa A, McDonagh D, Stiles TC, Haraldseth O, Lereim I: Acute treatment of whiplash neck injuries: A randomized trial during the first 14 days after a car accident. Spine 1998;23:25-31.
Question 2High Yield
A 7-year-old girl has pain and swelling of the right elbow after falling off her bicycle. Radiographs are shown in Figure 31. What is the most appropriate initial step in management?
Explanation
Explanation
Lateral condylar fractures are challenging to treat because of late displacement and development of a nonunion that may lead to valgus instability, pain, or tardy ulnar nerve palsy. Fractures such as this one with more than 2 mm of displacement on any radiographic view are prone to nonunion and should be stabilized. Fractures with less than 2 mm of displacement usually are stable and may be treated nonsurgically. In these patients, careful follow-up is recommended within several days of casting to check for fracture displacement. Arthrography or MRI may be helpful in these minimally displaced fractures. Fractures with an intact articular cartilage surface, such as noted on these studies, are unlikely to displace further. Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425. Attarian DE: Lateral condyle fractures: Missed diagnoses in pediatric elbow injuries. Mil Med 1990;155:433-434. Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
References:
- Badelon O, Bensahel H, Mazda K, et al: Lateral humeral condylar fractures in children: A report of 47 cases. J Pediatr Orthop 1988;8:31-34.
Question 3High Yield
A 53-year-old man with a history of severe left hip pain has a significant limp that is the result of a 5-cm limb-length discrepancy. An AP radiograph is shown in Figure 48. The underlying etiology is most likely related to a history of
Explanation
Radiographic abnormalities such as coxa magna, coxa breva secondary to growth arrest, and coxa plana and acetabular deformities are associated with healed Legg-Calve-Perthes disease. Femoral heads that were flat yet congruent with the acetabulum are at risk for disabling arthritis in the sixth decade of life in 50% of these untreated patients. As the normal ball-and-socket joint deforms to a flattened cylinder, the hip loses abduction and rotation capability, while retaining flexion and extension potential. If the femoral head is flat and is not concentric with the acetabulum, early severe arthritis occurs. Hinge abduction and anterior impingement are known sequelae of a flat, incongruent femoral head.
Question 4High Yield
A 13-year-old boy sustains a valgus stress injury to the knee while playing football, and he is unable to bear weight after the injury. Examination reveals tenderness medially superior to the joint line. The knee is held in flexion, and he has a large effusion and localized medial swelling. Plain radiographs show no obvious fracture. What is the next diagnostic step?
Explanation
Explanation
In the skeletally mature individual, this mechanism of injury will often result in a sprain of the medial collateral ligament. In skeletally immature patients, the same mechanism can cause a fracture of the distal femoral physis. If the fracture is nondisplaced, the plain radiographs may show only soft-tissue swelling or effusion. While the MRI scan may show edema in the soft tissues on the medial side of the knee and even an abnormality of the physis, stress radiographs provide a quicker and less expensive means of making the diagnosis. Arthroscopy and arthrography would not be helpful in making the diagnosis. Arthroscopy may result in further displacement of the injury. Smith L: Concealed injury to the knee. J Bone Joint Surg Am 1962;44:1659-1660.
References:
- Beaty JH, Kumar A: Fractures about the knee in children. J Bone Joint Surg Am 1994;76:1870-1880.
Question 5High Yield
A 78-year-old patient undergoing revision total knee arthroplasty has bone loss throughout the knee at the time of revision. A distal femoral augment is used to restore the joint line. One month after surgery, the patient reports pain and is unable to ambulate. A lateral radiograph is shown in Figure 34. What is the most likely etiology of this problem?
Explanation
Instability is a leading cause of failure following total knee arthroplasty. Instability can present as global instability, extension gap (varus/valgus) instability, or flexion gap (anterior/posterior) instability. Treatment options are numerous based on the exact pathology. The radiograph reveals anterior/posterior instability with dislocation consistent with flexion gap instability. A loose flexion gap can allow the femoral component to ride above the tibial cam post mechanism, resulting in dislocation. Distal femoral augments treat extension gap instability, whereas tibial augments can treat both flexion and extension gap instability. Posterior condyle augments at the distal femur can also be used to treat flexion gap instability. Flexion gap instability is further aggravated by extension mechanism incompetence. Note the excessively thin patella on the lateral radiograph. Pagnano MW, Hanssen AD, Lewallen DG, et al: Flexion instability after primary cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46. McAuley J, Engh GA, Ammeen DJ: Treatment of the unstable total knee arthroplasty. Inst Course Lect 2004;53:237-241.
Question 6High Yield
A 56-year-old man with a history of chronic lower back pain from lumbar spondylosis reports a 2-day history of acute incapacitating back pain. He denies any history of acute trauma, although he reports the pain starting after a coughing spell. He also reports difficulty urinating and some fecal incontinence. Examination reveals generalized lower extremity weakness, saddle paresthesia, hyporeflexia in the lower extremities, and loss of rectal tone. What is the most appropriate management at this time?
Explanation
Explanation
Cauda equina syndrome is a medical emergency that must be quickly diagnosed and treated to avoid long-term complications. Cauda equina syndrome typically presents with low back pain, unilateral or usually bilateral sciatica, saddle sensory disturbances, bladder and bowel dysfunction, and variable lower extremity motor and sensory loss. Although a number of pathologies can cause cauda equina syndrome, in a patient with a history of chronic back pain, disk pathology is the most common cause of acute onset cauda equina syndrome. Whereas radiographs may be useful in a traumatic onset of symptoms, MRI is the most appropriate study. Cauda equina syndrome should be evaluated on an emergent basis and admission for work-up is appropriate. Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522.
Question 7High Yield
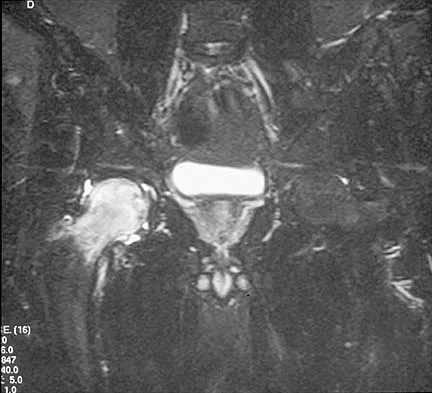
Figures 10a through 10c show the plain radiograph and MRI scans of a 41-year-old man who has right hip pain. What is the most likely diagnosis?

Explanation
Transient osteoporosis is a self-limited painful but reversible disorder. Although first described in pregnant women, it is more common in young to middle-aged men. The radiograph shows loss of mineralization in the right hip relative to the left side. There is no osseous destruction or cortical expansion typical of metastasis or giant cell tumor. The process is confined to the femoral side of the joint unlike rheumatoid arthritis, which would be centered in the joint. Osteonecrosis is better defined with sharp but irregularly shaped margins, and there is no double-line sign. The MRI scans reveal diffuse edema in the femoral head and neck that is atypical for osteonecrosis. Transient osteoporosis may recur in the same or opposite hip.
Question 8High Yield
Figure 1 shows the radiograph of a patient who underwent a total knee revision with a posterior stabilized mobile-bearing prosthesis and now has recurrent knee dislocations. What is the most likely cause?
Explanation
Explanation
The patient has a posterior stabilized total knee revision, and the femoral component has dislocated over the tibial polyethylene cam/post. This usually indicates a loose flexion gap, or "flexion instability." A loose flexion gap can occur due to undersizing of the femoral component, anteriorization of the femoral component, excessive distal augmentation of the distal femur, or collateral ligament insufficiency, especially if combined with posterior capsular insufficiency. Isolated laxity of the extension gap (with a well-balanced flexion gap) causes varus/valgus instability, but it rarely causes the femoral component to "jump" the tibial cam of a posterior stabilized tibial insert. Malrotation of the components may cause patellar instability or a rotational instability of the tibiofemoral joint but should not cause a frank posterior dislocation of the tibia, unless combined with other errors of balancing. Although a mobile-bearing total knee arthroplasty may be more sensitive to errors in balancing than a fixed-bearing total knee arthroplasty, this complication does not reflect a faulty prosthetic design. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 339-365. Lotke PA, Garino JP: Revision Total Knee Arthroplasty. New York, NY, Lippincott-Raven, 1999, pp 173-186, 227-249.
References:
- Clarke HD, Scuderi GR: Flexion instability in primary total knee replacement. J Knee Surg 2003;16:123-128.
Question 9High Yield
A patient with a 5-cm synovial sarcoma located in the distal portion of the rectus femoris muscle undergoes excision of the mass. The procedure is performed through a 10-cm longitudinal incision. Only a portion of the rectus femoris is removed; the vast majority of the muscle is preserved. The plane of dissection is beyond the reactive zone, and the pathology reveals that the margins are negative. This procedure is classified as
Explanation
Explanation
The patient underwent a wide resection, which involves excision of the tumor along with a cuff of normal tissue that completely surrounds the tumor. The plane of resection is beyond the reactive zone. A radical resection involves removal of the entire affected muscle from origin to insertion. In a marginal excision, the plane of dissection is through the reactive zone of the tumor. A marginal excision is generally considered inadequate surgery for high-grade sarcomas. In an intralesional resection, the plane of dissection is through the tumor. Excision within the reactive zone but beyond the tumor is the same as a marginal excision. Enneking WF: Staging of musculoskeletal neoplasms, in Current Concepts of Diagnosis and Treatment of Bone and Soft Tissue Tumors. Heidelberg, Germany, Springer-Verlag, 1984.
References:
- Simon MA, Springfield D: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998.
Question 10High Yield
A 27-year-old woman with Down syndrome has a severe bunion with pain and deformity in the left forefoot. Nonsurgical management has failed to provide relief. She does not use any assistive ambulatory devices. A radiograph is shown in Figure 21. Treatment should now consist of
Explanation
The patient requires an arthrodesis of the first metatarsophalangeal joint because of the abnormal neuromuscular forces. The more traditional bunionectomies such as a distal chevron bunionectomy, a proximal first metatarsal osteotomy, and a double osteotomy have a high failure rate because of the underlying Down syndrome. The Keller procedure is indicated for older, sedentary individuals and has little role in the management of a neuromuscular bunion. Coughlin MJ, Abdo RV: Arthodesis of the first metatarsophalangeal joint with Vitallium plate fixation. Foot Ankle Int 1994;15:18-28.
Question 11High Yield
A 12-month-old boy has right congenital fibular intercalary hemimelia with a normal contralateral limb. A radiograph of the lower extremities shows a limb-length discrepancy of 2 cm. All of the shortening is in the right tibia. Assuming that no treatment is rendered prior to skeletal maturity, the limb-length discrepancy will most likely
Explanation
Explanation
Many congenital limb deficiencies and bowing deformities result in growth retardation. If unilateral, a gradually progressive limb-length discrepancy will result; however, the proportional lengths of the lower extremities will remain at a relatively constant ratio. For example, if the right foot is at the level of the left knee at birth, this will still be true at maturity. This concept can be useful for early prediction of limb-length discrepancy by using a "multiplier method," as described by Paley and associates. This method can facilitate early treatment decisions, such as the need for amputation, without having to wait for serial scanography measurements. Paley D, Bhave A, Herzenberg JE, et al: Multiplier method for predicting limb-length discrepancy. J Bone Joint Surg Am 2000;82:1432-1446.
References:
- Moseley CF: A straight-line graph for leg length discrepancies. Clin Orthop 1978;136:33-40.
Question 12High Yield
Examination of a 45-year-old man with Charcot-Marie-Tooth disease reveals a cavus foot, a tight Achilles tendon, and forefoot callus formation. Radiographs reveal advanced degenerative changes in the hindfoot. Shoe wear modifications have failed to provide relief. Treatment should now consist of
Explanation
Explanation
The patient has the typical end stage residuals from long-standing Charcot-Marie-Tooth disease. Initial management consisting of shoe wear modifications and orthotic devices is preferred, but these are not successful when the disease process has progressed. Surgical correction with calcaneal osteotomy or Achilles tendon lengthening and Steindler stripping is not indicated in the presence of significant hindfoot arthritis. Because this patient has findings consistent with hindfoot arthritis, a triple arthrodesis with correction of the cavus deformity is the preferred treatment. Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth disease. J Bone Joint Surg Br 1989;71:17-20.
References:
- Wetmore RS, Drennan JC: Long-term results of triple arthrodesis in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 1989;71:417-422.
Question 13High Yield
What is the most common indication for revision following unconstrained elbow arthroplasty?
Explanation
Instability following unconstrained elbow arthroplasty occurs in 10% of patients. Subluxation is twice as common as frank dislocation; however, only 20% of these patients undergo revision. Instability following unconstrained elbow arthroplasty can be caused by component malposition or ligament insufficiency. King GJ, Itoi E, Niebur GL, et al: Motion and laxity of the capitellocondylar total elbow prosthesis. J Bone Joint Surg Am 1994;76:1000-1008.
Question 14High Yield
Which of the following clinical disorders is the result of a mutation in fibroblast growth factor recepter 3 (FGFR3)?
Explanation
Explanation
Camptomelic dysplasia is caused by a heterozygous loss of function of the Sox9 gene. The alternatives have genetic causes, but are not linked to Sox9. Cleidocranial dysplasia is related to a defect in Cbfa-1 (Osf-2, Runx2). Schmid metaphyseal chondrodysplasia is related to Type X collagen. Fibrous dysplasia is related to a defect in the alpha subunit of stimulatory guanine-nucleotide-binding protein (Gs). Achondroplasia is related to a defect in fibroblast growth factor receptor 3. Wagner T, Wirth J, Meyer J, et al: Autosomal sex reversal and camptomelic dysplasia are caused by mutations in and around the SRY-related gene SOX9. Cell 1994;79:1111-1120. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 111-131.
References:
- Dietz FR, Murray JC: Update on the genetic bases of disorders with orthopaedic manifestations, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 15High Yield
A 12-year-old girl falls in gymnastics and sustains comminuted midshaft radius and ulna fractures. Closed reduction and cast immobilization are attempted but fracture redisplacement with 20 degrees of angulation occurs. Surgical treatment includes closed reduction and intramedullary fixation of both bones. What is the most common long-term complication for this fracture?
Explanation
Explanation
Healing of forearm fractures in skeletally immature patients is the usual outcome. The use of intramedullary fixation has been reported to result in a lower frequency of refractures when compared to plate osteosynthesis due to the absence of diaphyseal holes after plate removal, which are considered stress risers. Regardless of implant technique, malunion and infection are infrequent. Loss of forearm pronation and supination is a common occurrence in surgically treated fractures due to the higher degree of soft-tissue injury, and periosteal stripping leads to fracture site instability and fracture comminution. Luhmann SJ, Gordon JE, Schoenecker PL: Intramedullary fixation of unstable both-bone forearm fractures in children. J Pediatr Orthop 1998;18:451-456.
Question 16High Yield
A 13-year-old boy has a mild deformity of the left sternoclavicular joint after being involved in a rollover accident while riding an all-terrain vehicle. Examination in the emergency department reveals that he is hemodynamically stable, and his neurovascular examination is normal. The CT scan shown in Figure 22 was obtained because radiographs were inconclusive. Management should consist of
Explanation
Explanation
The CT scan reveals a completely displaced physeal fracture of the medial clavicle with marked posterior displacement of the distal fragment. This fracture pattern is associated with potential injury to the vascular structures of the mediastinum. Reduction should be performed for this fracture and generally can be done closed with shoulder retraction and upward pull on the clavicle with a towel clip. Once reduced, the fracture is relatively stable and typically will heal in good position. Reduction should be performed in the operating room in the event that a vascular injury is detected once compression is removed from the clavicle. Open reduction may be necessary if closed reduction is not possible; however, pinning or ligament reconstruction usually is not necessary. Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, p 581.
References:
- Wirth MA, Rockwood CA Jr: Acute and chronic traumatic injuries of the sternoclavicular joint. J Am Acad Orthop Surg 1996;4:268-278.
Question 17High Yield
Figure 33 shows the CT scan of a 40-year-old man who injured his left shoulder while skiing. What structure is attached to the bony fragment?
Explanation
Explanation
The scan reveals a bony Bankart lesion. The anterior band of the inferior glenohumeral ligament is the major restraint to anterior translation of the humeral head and is usually injured with anterior shoulder dislocations. It inserts onto the glenoid labrum at the anteroinferior aspect of the glenoid rim. The labrum most frequently avulses from the glenoid (Bankart lesion), but occasionally the bony attachment is avulsed. O'Brien SJ, Neves MC, Arnoczky SP, et al: The anatomy and histology of the inferior glenohumeral ligament complex of the shoulder. Am J Sports Med 1990;18:449-456.
References:
- Warner JP: The gross anatomy of the joint surfaces, ligaments, labrum and capsule, in Matsen FA, Fu FF, Hawkins RJ (eds): The Shoulder: A Balance of Mobility and Stability. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1992, pp 7-28.
Question 18High Yield
A 12-year-old girl who is Risser stage 3 has had intermittent mild midback pain for the past 4 weeks. The pain is worse after prolonged sitting and after carrying a heavy backpack at school. She occasionally takes acetaminophen, but the pain does not limit sport activities. Examination reveals a mild right rib prominence during forward bending. Neurologic examination is normal. Radiographs show a 20-degree right thoracic scoliosis with no congenital anomalies or lytic lesions. Management should consist of
Explanation
Mild scoliosis is not a painful condition, but it usually presents during adolescence. Intermittent back pain is reported by 25% to 30% of adolescents whether or not scoliosis is present. Such pain is often attributed to muscle strain from tight muscles, poor posture, or heavy school backpacks. The clinician must distinguish typical pain (mild, intermittent, nonlimiting) from atypical pain. The latter requires more careful examination and imaging studies (bone scan or MRI) to determine the source of pain. The patient's age and right thoracic curve pattern are typical for idiopathic scoliosis; therefore, imaging of the neuroaxis is not necessary to look for cord syrinx, tethering, or tumor. Brace treatment is not required for this small curve unless future progression is demonstrated. Ramirez N, Johnston CE, Browne RH: The prevalence of back pain in children who have idiopathic scoliosis. J Bone Joint Surg Am 1997;79:364-368. Hollingworth P: Back pain in children. Br J Rheum 1996;35:1022-1028.
Question 19High Yield
What is the typical axial plane transverse angulation of the thoracic pedicles?
Explanation
Explanation
Thoracic pedicles typically are angled 25 degrees medially at T1 so the starting point is more lateral. T2 angles about 15 degrees, and then the pedicles average about 5 to 7 degrees down to T10. At T11 and 12, the angulation is minimal. Weinstein L: Pediatric Spine Principles and Practice. New York, NY, Raven Press, 1994, pp 1659-1681.
Question 20High Yield
An elite gymnast injured her ankle in an awkward dismount 36 hours ago. Examination reveals weakness on single leg step-up. A clinical photograph of the medial ankle is shown in Figure 15. Plain radiographs are normal. To help confirm the diagnosis, the next step in evaluation should consist of
Explanation
Explanation
Ecchymosis on the medial side of the ankle is distributed in the posterior tibialis tendon sheath location, posterior to the medial malleolus, and extending inferiorly to the tendon's attachment on the navicular. MRI is the imaging study of choice to determine the extent of tendon damage. MRI will also help assess the deltoid ligament. Bone scans and CT are helpful in identifying osteochondral fractures and occult fractures; however, these studies are not indicated for this patient. Peroneal tendons are located lateral on the ankle. Arthroscopy of the ankle joint would not be helpful in assessing the posterior tibial tendons. Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 307-317.
References:
- Rosenberg ZS, Cheung Y, Jahss MH, Noto AM, Norman A, Leeds NE: Rupture of the posterior tibial tendon: CT and MR imaging with surgical correlation. Radiology 1988;169:229-235.
Question 21High Yield
A 35-year-old man is seen for evaluation of his left ankle following multiple previous ankle sprains and frequent episodes of the ankle giving way. Examination reveals marked laxity about the lateral ankle with associated tenderness along the peroneal tendons. Physical therapy, anti-inflammatory drugs, and supportive bracing have failed to provide relief. An MRI scan shows peroneal tenosynovitis and a possible tear. He elects to undergo a peroneal tendon repair and lateral ligament reconstruction. Which of the following best describes the structure labeled "A" in Figure 45?
Explanation
The structure labeled "A" is a peroneus quartus, a supernumary muscle arising most commonly from the peroneus brevis. The presence of peroneus quartus is not uncommon, with an incidence of up to 21%, and is associated with lateral ankle pain and peroneal tendon symptoms, theoretically as a result of mass effect within the peroneal tendon sheath. Zammit J, Singh D: The peroneus quartus muscle: Anatomy and clinical relevance. J Bone Joint Surg Br 2003;85:1134-1137.
Question 22High Yield
Examination of an 18-year-old professional soccer player who was forcefully kicked across the shin while attempting a slide tackle reveals a marked effusion and limited motion of the knee. The tibia translates 12 mm posterior to the femoral condyles when the knee is held in 90 degrees of flexion. There is no posteromedial or posterolateral instability. Management should consist of
Explanation
The patient has an acute grade III posterior cruciate ligament injury. The majority of grade I and II injuries can be treated with protected weight bearing and quadriceps rehabilitation, and most patients can return to sports within 2 to 4 weeks. In contrast, grade III injuries require immobilization in full extension for 2 to 4 weeks to protect the posterior cruciate ligament and the other posterolateral structures presumed to be damaged. The mainstay of postinjury rehabilitation for all posterior cruciate ligament injuries is quadriceps strengthening exercises, which have been shown to counteract posterior tibial subluxation. Miller MD, Bergfeld JA, Fowler PJ, Harner CD, Noyes FR: The posterior cruciate ligament injured knee: Principles of evaluation and treatment. Instr Course Lect 1999;48:199-207.
Question 23High Yield
A 16-year-old high school football player sustains an injury to the left hip. The avulsed fragment identified by the arrow in Figure 34 represents the origin of which of the following structures?
Explanation
The avulsed fragment represents the origin of the rectus femoris from the anterior inferior iliac spine and the brim of the acetabulum. Avulsion of the anterior inferior iliac spine is much less common than avulsion of the anterior superior iliac spine with its origin of the sartorius. The origin of the gluteus minimus is from the outer cortex of the iliac wing and has not been reported as a source of bony avulsion. The hip capsule is composed of the ischiofemoral and pubofemoral ligaments, in addition to the iliofemoral ligament. The pelvic attachment of the ischiofemoral ligament is from the ischial part of the acetabulum posteriorly, while the pubofemoral ligament attaches to the pubic portion inferiorly. Technically, ligaments do not have origins and insertions as muscle tendon groups do, but have attachment sites. Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Question 24High Yield
What is the most frequent complication of both lateral closing wedge high tibial osteotomy and medial opening wedge osteotomy?
Explanation
Explanation
Scuderi and associates reported on patellar height after a high tibial osteotomy. Eighty-nine percent of the patellae, as measured by the Insall-Salvati index, and 76.3 percent, as measured by the Blackburne-Peel index, were observed to be lowered. More recently, Wright and associates reported a 64% incidence of patella baja in patients undergoing a medial opening wedge osteotomy. The incidence of intra-articular fracture during medial opening wedge osteotomy has been reported to be as high as 11% by Hernigou and associates, whereas the incidence of intra-articular fracture during lateral closing wedge high tibial osteotomy has been reported to be 10% to 20% by Matthews and associates. The incidence of peroneal nerve palsy with a lateral closing wedge high tibial osteotomy ranges from 0% to 20%, according to Marti and associates, whereas the incidence of peroneal palsy following a medial opening wedge osteotomy has been reported to be 15.7% by Flierl and associates. The exact incidence of compartment syndrome after a high tibial osteotomy is not known; however, it does not reach the level of patella baja. The incidence of deep infection after a lateral closing wedge high tibial osteotomy ranges from 0% to 4% according to Billings and associates. Scuderi GR, Windsor RE, Insall JN: Observations on patellar height after proximal tibial osteotomy. J Bone Joint Surg Am 1989;71:245-248. Wright JM, Crockett HC, Slawski DP, et al: High tibial osteotomy. J Am Acad Orthop Surg 2005;13:279-289. Hernigou P, Medevielle D, Debeyre J, et al: Proximal tibial osteotomy for osteoarthritis with varus deformity: A ten to thirteen-year follow-up study. J Bone Joint Surg Am 1987;69:332-354. Matthews LS, Goldstein SA, Malvitz TA, et al: Proximal tibial osteotomy: Factors that influence the duration of satisfactory function. Clin Orthop 1988;229:193-200. Marti CB, Gautier E, Wachtl SW, et al: Accuracy of frontal and sagittal plane correction in open-wedge high tibial osteotomy. Arthroscopy 2004;20:366-372. Marti RK, Verhigan RA, Kerkhoffs GM, et al: Proximal tibial varus osteotomy: Indications, technique, and five to twenty-one-year results. J Bone Joint Surg Am 2001;83:164-170. Flierl S, Sabo D, Hornig K, et al: Open wedge high tibial osteotomy using fractioned drill osteotomy: A surgical modification that lowers the complication rate. Knee Surg Sports Traumatol Arthrosc 1996;4:149-153.
References:
- Billings A, Scott DF, Camargo MP, et al: High tibial osteotomy with a calibrated osteotomy guide, rigid internal fixation, and early motion: Long-term follow-up. J Bone Joint Surg Am 2000;82:70-79.
Question 25High Yield
Figure 35 shows the lateral radiograph of a 15-year-old basketball player who felt a dramatic pop in his knee when landing after a lay-up. The patient reports that he cannot bear weight on the injured extremity. Management should consist of
Explanation
Explanation
Tibial tubercle avulsion is an injury of the adolescent knee that most often occurs just before the end of growth. The fracture usually occurs with jumping, either at push-off or landing. This patient has a type III injury. In type III injuries, the articular surface is disrupted, and meniscal injury and compartment syndrome can occur. Open reduction is the treatment of choice, and anterior fasciotomy should be considered prophylactically at the time of surgery. Although the fracture heals with an anterior epiphysiodesis of the proximal tibia, little growth remains in this patient and no special handling of the physis is warranted. Ogden JA, Tross RB, Murphy MJ: Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-215.
References:
- Pape JM, Goulet JA, Hensinger RN: Compartment syndrome complicating tibial tubercle avulsion. Clin Orthop 1993;295:201-204.
Question 26High Yield
An otherwise healthy 57-year-old man has persistent, severe hip pain after undergoing total hip arthroplasty 3 months ago. What is the next most appropriate step in management?
Explanation
Any patient who is severely symptomatic this quickly after surgery must be evaluated for infection. Loosening is also a possible cause, but infection must be ruled-out. Bone scans are not helpful at this early postoperative stage. Normal laboratory values argue strongly against infection, but when abnormal, need to be supplemented with a hip aspiration. Aspiration remains the most selective and sensitive measure, especially when linked to a WBC count of the synovial tissues in the joint. There is no indication for an antiobiotic trial because it may make future culture sensitivity more difficult. Drancourt M, Stein A, Argenson JN, et al: Oral rifampin plus ofloxacin for treatment of staphylococcus-infected orthopedic implants. Antimicrob Agents Chemother 1993;37:1214-1218. Duncan CP, Beauchamp C: A temporary antibiotic-loaded joint replacement system for the management of complex infections involving the hip. Orthop Clin North Am 1993; 24: 751-759.
Question 27High Yield
Reconstruction of the posterior cruciate ligament (PCL) via the inlay technique involves exposure of the PCL tibial insertion site by a posterior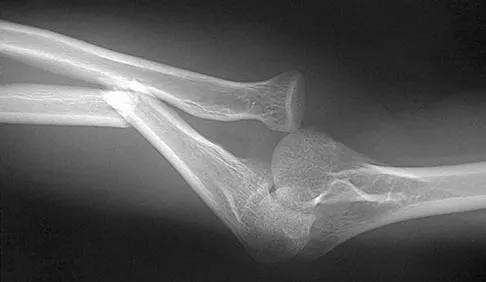
Explanation
The posterior medial approach through the semimembranosus/medial gastrocnemius interval is used in the inlay technique for PCL reconstruction. Exposure of the posterior capsule of the knee through this interval provides the greatest margin of safety to avoid injury to the tibial nerve, motor branch of the medial gastrocnemius, and the peroneal nerve. The direct posterior approach using the medial sural cutaneous nerve allows exposure of the popliteal neurovascular structures, but deep dissection through this interval places the motor branch of the medial gastrocnemius at risk. The interval between the semitendinosus and semimembranosus is used in accessory incisions with medial meniscus repairs but does not allow exposure of the PCL insertion. Berg EE: Posterior cruciate tibial inlay reconstruction. Arthroscopy 1995;11:69-76.
Question 28High Yield
Figure 4a shows the radiograph of a 20-year-old man who has an injury to the right shoulder. Figure 4b shows an arthroscopic view (posterior portal). The arrow points to a
Explanation
Explanation
4b The radiograph shows an anterior dislocation of the shoulder. A frequently encountered sequela of this is a compression fracture of the posterolateral humeral head, commonly referred to as a Hill-Sachs defect. The arthroscopic view of the glenohumeral joint visualizes the posterior aspect of the humeral head. In the image, the area devoid of cartilage to the right is the bare area. The indentation seen to the left is a Hill-Sachs defect. Matsen FA, Thomas SC, Rockwood CA, et al: Glenohumeral instability, in Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 611-754.
References:
- Mazzocca AD, Noerdlinger M, Cole B, et al: Arthroscopy of the shoulder: Indications and general principals of techniques, in McGinty JB (ed): Operative Arthroscopy, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 412-427.
Question 29High Yield
A 75-year-old patient returns for follow-up after undergoing bilateral total hip arthroplasty (THA). The right hip is a hybrid THA performed 12 years ago, whereas the left hip is a cementless THA performed 10 years ago. Both acetabular components are the same type, same size, and from the same manufacturer. Both femoral heads are 28-mm cobalt-chromium components. What is the most likely explanation for the advanced polyethylene wear in one hip?
Explanation
Explanation
Over the past three decades, gamma irradiation and air has been the most common method of sterilizing polyethylene used in total joint arthroplasty. This method of sterilization results in breakage of the chemical bonds within the polymer. While this promotes cross-linking, it also leaves the polyethylene vulnerable to oxidation, especially if packaged in an air environment. Oxidation has been shown to decrease polyethylene's molecular weight, ultimate tensile strength, elongation, and toughness which results in a stiffer, more brittle material that is less resistant to wear. Severity of oxidation and a decrease in mechanical properties have been shown to be related to the length of time that the component is exposed to air (the shelf life). Currier and associates studied the clinical performance of gamma irradiated in air polyethylene components that had been shelf aged. They demonstrated that for the first 5 years of shelf life, polyethylene oxidized rather slowly. However, polyethylene components with a shelf life of more than 5 years would be expected to have minimal mechanical toughness and would likely fail rapidly if implanted. Bohl and associates evaluated 135 patients who had undergone total knee arthroplasty. Survivorship at 5 years was 100% for components with a shelf life of less than 4 years, 89% for components with a shelf life of 4 to 8 years, and 79% for components with a shelf life of more than 8 years. Sychterz and associates reported no correlation between shelf life and true wear rates for components with a shelf life of less than 3 years. In summary, both in vivo and in vitro data suggest that shelf life in excess of 3 to 5 years has a direct effect on wear of polyethylene. Currier BH, Currier JH, Collier JP, et al: Shelf life and in vivo duration: Impacts on performance of tibial bearings. Clin Orthop 1997;342:111-122. Bohl JR, Bohl WR, Postak PD, et al: The Coventry Award: The effects of shelf life on clinical outcome for gamma sterilized polyethylene tibial components. Clin Orthop 1999;367:28-38.
References:
- Sychterz CJ, Young AM, Orishimo K, et al: The relationship between shelf life and in vivo wear for polyethylene acetabular liners. J Arthroplasty 2005;20:168-173.
Question 30High Yield
A 39-year-old man reports low back pain, lower extremity numbness, and urinary retention after being injured in a motor vehicle accident 1 day ago. He is able to walk but is in pain. A straight leg raise results in increased back pain, and examination reveals that perianal sensation is decreased. Placement of a urinary catheter results in 500 mL of urine. What is the next most appropriate step in management?
Explanation
Explanation
Acute cauda equina syndrome, including saddle hypesthesia and bowel/bladder incontinence, is a red flag that demands emergent evaluation with MRI and urgent surgery if compression is confirmed. Results appear to be improved if surgery is performed within 48 hours. The other treatment approaches listed are not indicated if a cauda equina syndrome is present. Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522. Shapiro S: Medical realities of cauda equina syndrome secondary to lumbar disc herniation. Spine 2000;25:348-351.
References:
- Kostuik JP, Harrington I, Alexander D, et al: Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am 1986;68:386-391.
Question 31High Yield
The anticoagulant effect of the low-molecular-weight heparins (LMWH) is mediated by the binding affinity of antithrombin III to which of the following coagulation factors?
Explanation
Standard heparin mediates its anticoagulant effect largely through its interaction with antithrombin III. A conformational change in antithrombin III occurs that markedly accelerates its ability to inactivate the coagulation enzymes thrombin factor (II), factor Xa, and factor IXa. In contrast, LMWHs do not contain the necessary saccharide units to bind thrombin and antithrombin III simultaneously. The anticoagulant effect of LMWHs involves binding of antithrombin III to factor Xa.
Question 32High Yield
A 15-year-old girl has had a painful mass on the medial aspect of her left thigh for the past 5 years. The pain is present only when she is performing athletic activities and is completely relieved with rest. A radiograph and MRI scan are shown in Figures 29a and 29b. The patient and her parents would like to have the mass removed. What further diagnostic studies are required prior to considering surgical resection?
Explanation
Explanation
29b The radiograph and MRI scan show a pedunculated lesion arising from the medial aspect of the distal femoral metaphysis. The cortex of the lesion is contiguous with the cortex of the underlying normal bone. Similarly, the medullary canal of the lesion is contiguous with that of the normal bone. These findings are diagnostic of osteochondroma. Rarely a secondary chondrosarcoma can arise in a preexisting osteochondroma. This diagnosis is suggested by identifying a cartilage cap that is greater than 1.5-cm thick in a skeletally mature patient. MRI is the best study to rule out a secondary chondrosarcoma. CT also may be used for this purpose but is not indicated in this patient because an MRI has already been obtained. A bone scan is not useful to identify a secondary chondrosarcoma. Similarly, there is no role for biopsy in this patient. No further tests are needed. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
References:
- Murphey MD, Choi JJ, Kransdorf, MJ, et al: Imaging of osteochondroma: Variants and complications with radiologic-pathologic correlation. Radiographics 2000;20:1407-1434.
Question 33High Yield
Evaluation of the percent of necrosis in the resected specimen after preoperative chemotherapy is of prognostic value for what type of sarcoma?
Explanation
Explanation
To date, only the percent of necrosis after induction chemotherapy in high-grade osteosarcomas seems to be of prognostic value. The value in soft-tissue sarcoma and rhabdomyosarcoma is being evaluated but has not been substantiated. Chondrosarcomas and parosteal osteosarcomas are not treated with chemotherapy. Rosen G, Marcove RC, Caparros B, Nirenberg A, Kosloff C, Huvos AG: Primary osteogenic sarcoma: The rationale for pre-operative chemotherapy and delayed surgery. Cancer 1979,43:2163-2177. Davis AM, Bell RS, Goodwin PJ: Prognostic factors in osteosarcoma: A critical review. J Clin Oncol 1994;12:423-431.
References:
- Wunder JS, Paulian G, Huvos AG, Heller G, Meyers PA, Healey JH: The histological response to chemotherapy as a predictor of the oncological outcome of operative treatment of Ewing sarcoma. J Bone Joint Surg Am 1998;80:1020-1033.
Question 34High Yield
A 26-year-old man falls off a motorcycle and injures his left wrist. There are no open wounds and the neurovascular examination is normal. Radiographs are shown in Figures 10a and 10b. Definitive management should consist of
Explanation
Explanation
10b The patient has a high-energy injury with resultant comminution of the distal radius metaphysis. Cast immobilization is likely to lead to radial shortening and angulation due to the comminution. Similarly, while external fixation and pinning has been successful in the past, some loss of radial length and volar angulation is typically noted. Present plate fixation devices for the distal radius employing locking screw technology have a superior ability to resist radial shortening and dorsal angulation. Fixation of the ulnar styloid is warranted when there is distal radioulnar joint instability or significant displacement of the styloid. This is more likely to occur with a fracture at the base of the styloid. In this instance, the distal radioulnar joint does not appear to be disrupted. May MM, Lawton JN, Blazar PE: Ulnar styloid fractures associated with distal radius fractures: Incidence and implications for distal radioulnar joint instability. J Hand Surg Am 2002;27:965-971.
Question 35High Yield
A 42-year-old woman who observes traditional Muslim practices is seen in your office accompanied by her physician husband to discuss possible elective bunion correction. In considering the treatment of this patient, what is one of the most important considerations?
Explanation
Explanation
In considering faith-based issues regarding treatment of this patient, the presence of her husband for the office visit would imply an agreement with her decision to have surgery. It also may facilitate her examination. Her role as caregiver, dietary concerns, and cleansing rituals are less important considerations with an outpatient-based procedure. Privacy concerns remain paramount to Muslim women, which include limited exposure during examination, during surgery, and in subsequent follow-up visits.
Question 36High Yield
Figures 17a through 17c show the radiographs of a 38-year-old man following a motorcycle accident. The posterior portion of the talus extruded through a posterolateral wound. The extruded talar body is visible in the wound along with some road debris. Management should now consist of surgical irrigation, debridement, and
Explanation
Explanation
17b 17c The extruded talus should be placed in sterile bacitracin solution, irrigated thoroughly, gently debrided, and immediately replanted in the OR. Open reduction and internal fixation of the talar fracture may be attempted immediately depending on the soft-tissue envelope, or delayed after soft-tissue stabilization with an external fixator. A retrospective study of 19 patients with an extruded talus reported that 12 patients had no subsequent surgery after definitive fixation, 7 had subsequent procedures, and 2 patients developed infections that were treated successfully at an average of 42-month follow-up. Successful outcome in this series was attributed to multiple debridements, soft-tissue stabilization, and primary wound closure. Smith CS, Nork SE, Sangeorzan BJ: The extruded talus: Results of reimplantation. J Bone Joint Surg Am 2006;88:2418-2424. Brewster NT, Maffulli N: Reimplantation of the totally extruded talus. J Orthop Trauma 1997;11:42-45.
References:
- Marsh JL, Saltzman CL, Iverson M, et al: Major open injuries of the talus. J Orthop Trauma 1995;9:371-376.
Question 37High Yield
Figures 12a and 12b show the radiographs of a 50-year-old patient who reports acute knee pain after sustaining a twisting injury while playing tennis. Examination is unremarkable. The next most appropriate step in management should consist of

Explanation
The radiographs show localized diffuse cortical thickening that is characteristic of melorheostosis. The condition may be monostotic or it may involve many bones in one extremity (monomelic) in the distribution of a sclerotome. Bone scans will show increased uptake at the site or sites of skeletal involvement. Long tubular bones are most commonly involved. Melorheostosis is usually asymptomatic and requires no treatment. On rare occasions, there may be associated soft-tissue contractures. Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby Inc, 1998, pp 1105-1107. Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
Question 38High Yield
Which of the following best characterizes bone mineralization?
Explanation
Mineralization occurs at the site of hole zones between the collagen fibrils. Crystals begin from the necessary ions of the lattice that come together with the correct orientation to form the first stable crystal. Formation of this critical nucleus is the most energy-demanding step of crystallization. Enzymes within the extracellular matrix vesicles degrade inhibitors such as adenosine triphosphate, pyrophosphate, and proteoglycans found in the surrounding extracellular matrix. Bone mineral consists of numerous impurities (carbonate, magnesium) that are more soluble, allowing the bone to act as a reservoir for calcium, phosphate, and magnesium ions. Crystals may form by addition of ions or ion clusters to the critical nucleus in many directions, with 'kink' sites forming to branch and exponentially proliferate the crystals. Macromolecules facilitate formation of the critical nucleus and increasing local concentrations of necessary ions. Once the crystals are formed and proliferating, macromolecules bind to the surface and block the growth of the crystal, regulating size, shape, and number of crystals. Lian JB, Stein GS, Canalis E, et al: Bone formation: Osteoblast lineage cells, growth factors, matrix proteins, and the mineralization process, in Favus MJ (ed): Primer on Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 14-29.
Question 39High Yield
Which of the following is not a characteristic of synovial sarcomas?
Explanation
Explanation
Synovial sarcomas have a number of features that differentiate them from other soft-tissue sarcomas. They often have small areas of calcifications within the lesion. They occur in a younger patient population than most soft-tissue sarcomas. A subset of patients with synovial sarcoma tend to be chemosensitive. They often contain the SYT-SSX translocation. Although they can occur intra-articular, this is rare, despite their name. Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 1109-1126.
References:
- Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Question 40High Yield
The space available for the cord is an important determinant in neurologic recovery. Recent analysis suggests that the most reliable radiographic predictor for neurologic recovery after surgery in patients with rheumatoid arthritis and paralysis is a preoperative
Explanation
Boden and associates' recent article presents significant evidence that patients with rheumatoid arthritis, neurologic deterioration, and C1-2 instability are more likely to improve after surgery if the posterior alanto-odontoid interval is greater than 10 mm preoperatively. The accepted safe range for the posterior atlanto-odontoid interval is 14 mm. This measurement is believed to better represent the space available for the cord than the anterior alanto-odontoid interval. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 273-279. Boden SD, Dodge LD, Bohlman HH, Rechtine GR: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Question 41High Yield
Figure 11 shows a consecutive sequence of MRI scans obtained in a 12-year-old boy who has had increasing lateral knee pain and catching for the past 6 months. Examination reveals pain localized to the lateral joint line. Range-of-motion testing reveals a 5-degree lack of full extension on the involved side. Plain radiographs and laboratory values are within normal limits. What is the most appropriate management?
Explanation
Discoid menisci are rare causes of lateral knee pain in children. Various etiologies have been proposed, including failure of central absorption of the developing meniscus and hereditary transmission. Patients with discoid menisci have pain, clicking, and locking with a loss of active extension on range-of-motion testing. Classification of discoid menisci according to the Watanabe classification include complete, incomplete, and Wrisberg ligament type. The Wrisberg variant contains an abnormal posterior meniscal attachment. MRI is the diagnostic tool of choice, revealing a thick, flat meniscus generally seen in three consecutive MRI images. Symptomatic knees are often associated with a meniscal tear or degeneration and are managed with arthroscopic partial excision to a more normal shape (saucerization). Vandermeer RD, Cunningham FK: Arthroscopic treatment of the discoid lateral meniscus: Results of long-term follow-up. Arthroscopy 1989;5:101-109.
Question 42High Yield
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3, an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Explanation
Examination reveals an irritable hip, creating a differential diagnosis of transient synovitis versus pyogenic hip arthritis. Kocher and associates described four criteria to help predict the presence of infection: inability to bear weight, fever, ESR of more than 40 mm/h, and a peripheral WBC count of more than 12,000/mm3. This patient meets three of the four criteria, with a positive predictive value of 73% to 93% for joint infection. Therefore, aspiration of the hip is warranted, with a high likelihood that emergent hip arthrotomy will be indicated. Ideally, intravenous antibiotics should be administered after culture material has been obtained from needle aspiration of the hip. An urgent bone scan is better indicated as a screening test for sacroiliitis or diskitis. If the arthrocentesis proves negative, CT or MRI of the pelvis may be indicated to rule out a pelvic or psoas abscess. Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422. Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 43High Yield
Initial postoperative management after repair of an acute rotator cuff tear includes
Explanation
Explanation
In the immediate postoperative period following repair of an acute rotator cuff tear, passive forward elevation and external rotation should be performed within the safe zone determined at surgery. Early active range of motion (prior to tendon healing), internal rotation behind the back, and resistive exercises increase the risk of rupture of the repair. Iannotti JP: Full-thickness rotator cuff tear: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
References:
- Bigliani LU, Cordasco FA, McIlveen ST, et al: Operative repair of massive rotator cuff tears: Long-term result. J Shoulder Elbow Surg 1992;1:120-130.
Question 44High Yield
Figure 13 shows the radiographs of a 56-year-old woman who has pain and varus knee deformity after undergoing total knee arthroplasty 8 years ago. Aspiration and studies for infection are negative. During revision surgery, management of the tibial bone loss is best achieved by
Explanation
Explanation
Massive bone loss encountered in revision total knee arthroplasty remains a significant challenge. Recent reports have shown high success rates using structural allograft to reconstruct massive bone defects. Custom and hinged prostheses in this setting are no longer favored. The defect shown is segmental and is too large to be filled with cement or iliac crest bone graft. Mow CS, Wiedel JD: Structural allografting in revision total knee arthroplasty. J Arthroplasty 1996;11:235-241. Engh GA, Herzwurm PJ, Parks NL: Treatment of major defects of bone with bulk allografts and stemmed components during total knee arthroplasty. J Bone Joint Surg Am 1997;79:1030-1039.
References:
- Clatworthy MG, Ballance J, Brick GW, Chandler HP, Gross AE: The use of structural allograft for uncontained defects in revision total knee arthroplasty: A minimum five-year review. J Bone Joint Surg Am 2001;83:404-411.
Question 45High Yield
A 36-year-old man has a moderate-sized left paracentral L5-S1 disk herniation with compression of the S1 nerve. Examination will most likely reveal sensory changes at what location?
Explanation
Explanation
Because the left paracentral L5-S1 disk herniation is compressing the left S1 nerve root, the patient will have numbness along the lateral border and plantar surface of the foot. Numbness along the anterior thigh stopping at the knee is consistent with an L3 radiculopathy. Sensory changes at the dorsum of the foot and great toe normally signify an L5 distribution; the medial leg signifies an L4 distribution. Perianal numbness involves the S2-S5 nerve roots. Wisneski RJ, Garfin SR, Rothman RH, Lutz GE: Lumbar disk disease, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman and Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, vol 1, pp 629-634.
References:
- Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton- Century-Crofts, 1976, pp 249-254.
Question 46High Yield
A 15-year-old girl with a midshaft fibular lesion has histologic findings consistent with Ewing's sarcoma. Following induction chemotherapy, local control typically consists of
Explanation
Explanation
The current treatment regimen for Ewing's sarcoma typically involves induction chemotherapy followed by local control and further chemotherapy. Local control consists of surgery only, radiation therapy only, or a combination of the two. In bones that are easily resectable (expendable) with wide margins, surgery is usually recommended. For areas that cannot be resected (ie, large bulky pelvic tumors), radiation therapy alone is sometimes the preferred method of local control. If surgery is chosen and the margins are close, radiation therapy can be used as an adjuvant treatment. Amputation is rarely required for an isolated fibular lesion. Observation without adequate local control results in local recurrence. Nesbit ME Jr, Gehan EA, Burgert EO Jr, et al: Multimodality therapy for the treatment of primary, non-metastatic Ewing's sarcoma of the bone: A long-term follow-up of the first intergroup study. J Clin Oncol 1990;8:1664-1674.
References:
- Simon M, Springfield D, et al: Ewing's Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 296.
Question 47High Yield
A patient with rheumatoid arthritis with both ankle and subtalar involvement was treated as shown in Figures 11a and 11b. What complication is unique to this type of fixation?
Explanation
Explanation
11b The interlocking screws at the proximal end of the rod can act as a stress riser and lead to fracture. Postoperative pain at this level should prompt inclusion of this diagnosis in the differential. Removing the screws following bone union can decrease the chances of this occurring. A short rod that avoids the diaphyseal area may also be beneficial. Rotatory deformity is controlled by the perpendicularly oriented distal transfixion screws. Talar osteonecrosis would be unusual since the dissection can be minimized with an intramedullary rod. Any type of hardware can fail if the construct does not lead to a solid arthrodesis. Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 236-237. Thordarson DB, Chang D: Stress fractures and tibial cortical hypertrophy after tibiotalocalcaneal arthrodesis with an intramedullary nail. Foot Ankle Int 1999;20:497-500.
References:
- Hammett R, Hepple S, Forster B, et al: Tibiotalocalcaneal (hindfoot) arthrodesis by retrograde intramedullary nailing using a curved locking nail: The results of 52 procedures. Foot Ankle Int 2005;26:810-815.
Question 48High Yield
A 57-year-old man involved in a motor vehicle accident sustains an injury to his right shoulder. A spot AP radiograph is shown in Figure 34. What is the next most appropriate step in the orthopaedic management of this patient?
Explanation
Explanation
The next step in the management of this injury is completion of the shoulder trauma series. An axillary radiograph, which can be quickly performed in the emergency department, must be obtained to accurately assess the humeral head relationship to the glenoid. If difficulty is encountered, a "Velpeau" axillary may be substituted. If that fails to elucidate the status of the glenohumeral joint, a CT scan should be obtained.
Question 49High Yield
A 47-year-old woman has a right bunion that has been symptomatic despite modifications in shoe wear. She requests surgical correction. An AP radiograph is shown in Figure 37. Treatment should consist of
Explanation
Explanation
Because the radiograph reveals an intermetatarsal angle of greater than 15 degrees and an incongruent metatarsophalangeal joint, the treatment of choice is a proximal first metatarsal osteotomy with distal soft-tissue realignment. A distal chevron procedure would not correct this degree of deformity. A Keller procedure is reserved for a less active elderly individual. Arthrodesis is appropriate for a patient with advanced arthritis of the metatarsophalangeal joint. The double osteotomy is reserved for the congruent metatarsophalangeal joint with hallux valgus. Coughlin MJ, Carlson RE: Treatment of hallux valgus with an increased distal metatarsal articular angle: Evaluation of double and triple first ray osteotomies. Foot Ankle Int 1999;20:762-770.
References:
- Coughlin MJ: Hallux valgus. Instr Course Lect 1997;46:357-391.
Question 50High Yield
Which of the following best describes the resultant forces on an increased offset stem when compared with a standard offset stem?
Explanation
Explanation
The increased emphasis on restoring offset in total hip arthroplasty has implications for the forces applied to the components and the fixation interfaces. Static analysis has shown that with an increased affect, joint reaction force on the articulation is decreased. When the resultant load on the hip is "out of plane" (ie, directed anterior to posterior), there is increased torsion where the stem is turned into more retroversion. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180. Hurwitz DE, Andriaacchi TP: Biomechanics of the hip, in Callaghan J, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven , 1998.
References:
- Pauwels F: Biomechanics of the Normal and Diseased Hip. New York, NY, Springer-Verlag, 1976.
Question 51High Yield
A 33-year-old woman reports a mass on the right hand that has been enlarging for 1 year. An intraoperative photograph is shown in Figure 28a, and a biopsy specimen is shown in Figure 28b. What is the most likely diagnosis?
Explanation
Explanation
28b Giant cell tumor of the tendon sheath is the most common solid soft-tissue mass in the hand. These tumors are slow-growing and may be present for months or years before coming to medical attention. Patients usually report mechanical difficulties because of the size or position of the tumor. The gross appearance is that of a lobulated mass that may be multicolored; typically yellow, brown, red, and gray. Histologically the lesion consists of multinucleated giant cells, polygonal mononuclear cells, and histiocytes that may contain abundant hemosiderin or lipid. Walsh EF, Mechrefe A, Akelman E, et al: Giant cell tumor of tendon sheath. Am J Orthop 2005;34;116-121.
References:
- Weiss SW, Goldblum JR (eds): Enzinger and Weiss's Soft Tissue Tumors, ed 4. St Louis, MO, Mosby, 2001, pp 1038-1047.
Question 52High Yield
Which of the following is considered the preferred approach to resect a lesion in the posterior one third of the proximal humerus?
Explanation
Explanation
At least 8 cm of the posterior aspect of the proximal region of the humeral diaphyseal cortex can be exposed through the interval between the lateral head of the triceps and the deltoid muscle. No nerves or blood vessels need to be exposed in the dissection. The deltoid muscle is innervated by the axillary nerve and the triceps muscle by the radial nerve. This is a true internervous plane.
References:
- Berger RA, Buckwalter JA: A posterior surgical approach to the proximal part of the humerus. J Bone Joint Surg Am 1989;71:407-410.
Question 53High Yield
A 28-year-old woman has had pain in her hand and mild swelling of the little finger for the past 2 months. A radiograph is shown in Figure 41a, and the biopsy specimen is shown in Figures 41b and 41c. What is the most likely diagnosis?
Explanation
Explanation
41b 41c The radiographic appearance shows a slightly expansile lesion in the proximal phalanx of the fifth digit typical of an enchondroma. There is a stippled appearance within the bone and no evidence of cortical destruction. The biopsy reveals a cartilage lesion with basophilic cytoplasm. There are some hypercellular areas but no evidence of pleomorphism. Enchondromas in the tubular bones of the hand are usually more cellular than their counterparts in the femur and humerus and should not be considered malignant. No other lesions are noted in the radiograph, so a diagnosis of Ollier's disease cannot be made. An osteochondroma is a benign surface cartilage tumor. Brown tumor and osteomyelitis can be differentiated from enchondroma based on the histology. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 225.
References:
- McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 227.
Question 54High Yield
When performing the exposure for an anterior approach to the cervical spine, excessive retraction of the trachea and esophagus should be avoided to prevent injury of the
Explanation
Explanation
The recurrent laryngeal nerve lies between the trachea and the esophagus and is subject to stretch injury if excessive retraction is applied. The vagus nerve lies in the carotid sheath. The sympathetic trunk lies anterior to the longus colli muscles. The hypoglossal nerve and superior laryngeal nerve are both at risk during the exposure but are not located between the trachea and esophagus. An HS: Principles and Techniques of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1998, chapter 2.
References:
- Flynn TB: Neurologic complication of anterior cervical interbody fusion. Spine 1982;7:536-539.
Question 55High Yield
An obese 10-year-old boy has had left groin pain and a limp for the past 2 months. Examination reveals decreased abduction and internal rotation. Laboratory studies show normal renal function and an elevated thyroid-stimulating hormone (TSH) level. AP and frog lateral radiographs of the pelvis are shown in Figures 30a and 30b. What is the best course of action?

Explanation
The radiographs show a grade I slipped capital femoral epiphysis (SCFE) that is classified as stable because the child is able to bear weight. The elevated TSH level indicates possible hypothyroidism. SCFE usually occurs in boys age 12 to 14 years. Because of the patient's young age and hypothyroidism, he is at increased risk for slippage of the contralateral hip; therefore, prophylactic pinning of the uninvolved side also should be considered. Because of the risk of slip progression, crutch treatment and nonsteroidal anti-inflammatory drugs are not indicated. Realignment osteotomy is not indicated for grade I SCFE. Traction to reduce the slip, followed by pinning, has been advocated for unstable slips but is not indicated here. Loder RT, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
Question 56High Yield
Which of the following is considered the best method to measure limb-length discrepancy in a patient with a knee flexion contracture?
Explanation
Explanation
The most effective way to measure a limb-length discrepancy in a patient with a knee flexion contracture is a lateral CT scanogram. All the other methods listed provide inaccurate results with a knee flexion contracture because the measurements are made in the coronal plane. Aaron A, Weinstein D, Thickman D, et al: Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg Am 1992;74:897-902.
References:
- Tachdjian MO: Clinical Pediatric Orthopaedics: The Art of Diagnosis and Principles of Management. Stamford, CT, Appleton and Lange, 1997, pp 237-240.
Question 57High Yield
A 28-year-old painter has had increasing pain in his hand and forearm after sustaining a paint injection wound to the tip of his left index finger 24 hours ago. Management should consist of
Explanation
Explanation
The clinical presentation soon after injury may be surprisingly innocuous, but all high-pressure injection injuries of various materials are best treated by emergent surgical debridement of all foreign material from the flexor tendon sheath as well as the subcutaneous tissues. Subsequent hospital admission, IV antibiotics, and possible repeat debridements usually are necessary. The use of antibiotics alone is inadequate treatment of this severe injury. Pinto MR, Turkula-Pinto LE, Cooney WP, Wood MB, Dobyns JH: High-pressure injection injuries of the hand: Review of 25 patients managed by open wound technique. J Hand Surg Am 1993;18:125-130. Urbaniak JR, Evans JP, Bright DS: Microvascular management of ring avulsion injuries. J Hand Surg Am 1981;6:25-30. Tsai TM, Manstein C, DuBou R, Wolff T, Kutz JE, Kleinert HE: Primary microsurgical repair of ring avulsion amputation injuries. J Hand Surg Am 1984;9:68-72. Kay S, Werntz J, Wolff T: Ring avulsion injuries: Classification and prognosis. J Hand Surg Am 1989;14:204-213.
References:
- Schnall SB, Mirzayan R: High-pressure injection injuries to the hand, in Kozin SH (ed): Hand Clinics: Upper Extremity Trauma. Philadelphia, PA, 1999, pp 245-248.
Question 58High Yield
What is the structure indicated by the letter "A" in Figure 21?
Explanation
The ligaments shown are the components of the lateral collateral ligament complex, and the structure indicated by the letter "A" is the radial collateral ligament. The lateral ulnar collateral ligament is the structure indicated by the letter "C" and the annular ligament is indicated by the letter "B." The transverse ligament is a component of the medial collateral ligament complex. Morrey BF: Anatomy of the elbow joint, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1993, p 30.
Question 59High Yield
A 42-year-old man reports a 12-month history of a painful fusiform swelling of the Achilles tendon. Physical therapy, heel lifts, and anti-inflammatory drugs have failed to provide relief. MRI scans are shown in Figures 44a and 44b. What is the treatment of choice?

Explanation
The area of the tendon degeneration is greater than 50% of the width so a supplemental tendon transfer is needed. Debridement and repair alone do not provide adequate strength. Injection risks tendon rupture. Brisement is indicated for peritendinitis, not tendinosis. Nonsurgical management is unlikely to be of benefit after 12 months. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 94-95.
Question 60High Yield
Compared with cobalt-chromium, the biomechanical properties of titanium on polyethylene articulation in total hip replacement result in
Explanation
The surface hardness of titanium is low compared with that of cobalt-chromium alloys. Titanium articulations are easily scratched, resulting in a significantly increased rate of wear and debris production. The wear and resulting lysis can also result in an increased rate of loosening. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486. Agins HJ, Alcock NW, Bansal M, et al: Metallic wear in failed titanium-alloy total hip replacements: A histological and quantitative analysis. J Bone Joint Surg Am 1988;70:347-356.
Question 61High Yield
A 53-year-old man has a 4- x 5-cm high-grade soft-tissue sarcoma in the midthigh. As part of the staging evaluation, regional nodes should be assessed by
Explanation
In general, soft-tissue metastases to regional nodes are a relatively rare occurrence (less than 5% overall). The incidence of lymphatic metastasis is highest for synovial sarcoma, rhabdomyosarcoma, clear cell sarcoma, and epithelioid sarcoma. Regional nodes should be assessed clinically. CT is not used to routinely assess regional nodes. Evaluation of a sentinal node is not indicated because of the low incidence of regional nodal involvement. Fine needle aspiration may be indicated to assess clinically suspicious nodes. Prophylactic inguinal node dissection is contraindicated because it may lead to unnecessary complications such as lymphedema.
Question 62High Yield
A 21-year-old patient has had pain and a marked decrease in active and passive shoulder motion after having had a seizure 2 months ago as the result of alcohol abuse. Current AP and axillary radiographs and a CT scan are shown in Figures 26a through 26c. Management should consist of


Explanation
Open reduction and subscapularis and lesser tuberosity transfer into the defect is the treatment of choice in young individuals who have defects that involve between 20% to 45% of the head. Disimpaction and bone grafting is an option in injuries that are less than 3 weeks old. Closed reduction 2 to 3 months after injury usually is unsuccessful and increases the risk of fracture or neurovascular injury. Total shoulder arthroplasty is reserved for defects of greater than 50% or with associated glenoid surface damage. Hemiarthroplasty should be avoided in young individuals unless 50% or more of the head is involved. Gerber C: Chronic locked anterior and posterior dislocations, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997, pp 99-113.
Question 63High Yield
An 18-year-old collegiate basketball player has had a 3-month history of activity-related back pain. She describes isolated low back pain without radiation that increases with training and playing basketball. Her pain resolves with rest. Physical therapy for 6 weeks has failed to provide relief. An axial CT scan is shown in Figure 17a, and Figures 17b and 17c show sagittal CT reconstructions through the right and left lumbar facets, respectively. Further management should consist of which of the following?


Explanation
The sagittal and axial CT scans show a bilateral spondylolysis at L5. The defect is in the pars interarticularis on the right side but at the base of the pedicle on the left. Having failed a trial of physical therapy with only a 3-month history of pain, the next most appropriate step in management should consist of activity modification and bracing in an antilordotic lumbosacral orthosis. Surgical intervention is reserved for patients who have failed to respond to a trial of bracing and activity restriction. Debnath UK, Freeman BJ, Grevitt MP, et al: Clinical outcome of symptomatic unilateral stress injuries of the lumbar pars interarticularis. Spine 2007;32:995-1000.
Question 64High Yield
A 10-year-old boy has activity-related knee pain that is poorly localized. He denies locking, swelling, or giving way. Examination shows mild tenderness at the medial femoral condyle and painless full range of motion without ligamentous instability. Radiographs are shown in Figures 2a through 2c. What is the best course of action?


Explanation
The radiographs show an osteochondritis dissecans (OCD) lesion in the medial femoral condyle of a skeletally immature patient. The lesion is not displaced from its bed. Nonsurgical management of a stable OCD lesion in a patient with open physes consists of a period of activity limitation and occasional immobilization. Unstable lesions, loose bodies, and patients with closed physes require more aggressive treatment. Most of the surgical procedures can be done arthroscopically. Because the radiographic appearance is typical, biopsy is unnecessary. The radiographs do not show an osteocartilaginous loose body, and the patient reports no catching or locking; therefore, removal of the loose body is not indicated. Linden B: Osteochondritis dissecans of the femoral condyles: A long term follow-up study. J Bone Joint Surg Am 1977;59:769-776. Cahill BR: Osteochondritis dissecans of the knee: Treatment of juvenile and adult forms. J Am Acad Orthop Surg 1995;3:237-247.
Question 65High Yield
Commotio cordis is best treated with
Explanation
Explanation
Commotio cordis is a rare but catastrophic condition that is caused by blunt chest trauma. It results in cardiac fibrillation and is universally fatal unless immediate defibrillation is performed. Although case reports of successful use of the chest thump maneuver exist, the best method of treatment is cardiac defibrillation. IV fluids, epinephrine, and albuterol inhalers are used to treat dehydration, anaphylactic shock, and bronchospasm respectively, and are not effective in the treatment of commotio cordis. McCrory P: Commotio cordis. Br J Sports Med 2002;36:236-237.
References:
- Boden BP, Tacchetti R, Mueller FO: Catastrophic injuries in high school and college baseball players. Am J Sports Med 2004;32:1189-1196.
Question 66High Yield
A quarterback sustains a rough tackle after which he appears confused, has a dazed look on his face and an unsteady gait on standing. He denies loss of consciousness. Reexamination within 10 minutes is normal, the patient is lucid, and he wants to return to play. The coach and the player should be advised that he may
Explanation
The patient has a grade I (mild) concussion that can result in confusion and disorientation, without loss of consciousness. This concussion syndrome is completely reversible, with no long-term sequelae. Athletes who sustain a grade I concussion may return to play after 15 minutes if there are no lingering symptoms, such as headache or vertigo. A grade II concussion is characterized by loss of consciousness of less than 5 minutes. With this type of injury, the athlete can return to play in 1 week, if asymptomatic. If a grade III (severe) concussion is sustained, the athlete should avoid contact for a minimum of 1 month before considering a return to competition. A grade III concussion is characterized by a loss of consciousness of greater than 5 minutes or posttraumatic amnesia of greater than 24 hours. A CT scan is not indicated in a grade I injury. An athlete who sustains three grade I or grade II concussions, or two grade III concussions may not return to play for the season. Torg JS, Gennarelli TA: Head and cervical spine injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine Principles & Practice. Philadelphia, PA, WB Saunders, 1994, vol 1, pp 417-462.
Question 67High Yield
Figure 3 shows the AP radiograph of a patient with diabetes mellitus who has knee pain. A semiconstrained knee prosthesis was used in this patient to prevent which of the following complications?
Explanation
The radiographic appearance of the joint is highly suspicious for neuropathic joint (Charcot's joint). Evidence of bone loss on both the tibial and the femoral sides may necessitate the use of metal and/or bone augments. Patients with a neuropathic joint often have excellent range of motion, and postoperative stiffness is not a problem. The main problem with these patients is instability that occurs secondary to ligamentous laxity. Use of a semiconstrained prosthesis prevents the latter complication. Parvizi J, Marrs J, Morrey BF: Total knee arthroplasty for neuropathic (Charcot) joints. Clin Orthop 2003;416:145-150.
Question 68High Yield
Based on the MR arthrogram of the elbow shown in Figure 8, which of the following structures is torn?
Explanation
Based on the MR arthrogram in which gadolinium (bright on T1-weighted images) was injected into the joint space prior to imaging, the study shows a tear of the anterior band of the ulnar collateral ligament (UCL). The disruption in the distal end of the UCL is outlined by contrast. A small collection of contrast extravasation into the flexor musculature further confirms the presence of a tear. The UCL has a broad-based attachment on the medial epicondyle and has a pointed or tapered attachment distally on the ulna. Most UCL tears occur distally at the ulnar (coronoid) attachment. MR arthrography provides improved sensitivity compared to conventional MRI, without contrast, for the detection of UCL pathology, particularly in the subacute or chronic setting. After the soft-tissue edema and joint fluid associated with the injury have resolved, the torn end of the ligament may lie in contact with its adjacent attachment and create a false-negative appearance. In this patient, a noncontrasted MR arthrogram showed no tear, yet the tear is apparent with intra-articular contrast and distention. MR arthrography of the elbow also may be useful in detecting intra-articular bodies or in evaluation for loose osteochondral fragments or flaps. Morrey BF: Acute and chronic instability of the elbow. J Am Acad Orthop Surg 1996;4:117-128.
Question 69High Yield
Thoracic disk herniations are most frequently found in what area of the spine?
Explanation
Explanation
Although thoracic disk herniations have been reported at all levels of the thoracic spine, more than two thirds are found at T9-T12, which is the more mobile lower third of the thoracic region. Belanger TA, Emery SE: Thoracic disc disease and myelopathy, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 855-864.
References:
- Bohlman HH, Zdeblick TA: Anterior excision of herniated thoracic discs. J Bone Joint Surg Am 1988;70:70-77.
Question 70High Yield
Which of the following is an advantage of unreamed nailing of the tibia compared to reamed nailing?
Explanation
Explanation
The debate between reamed versus unreamed intramedullary nailing of the tibia continues. Although unreamed nailing was proposed for open fractures to minimize infection, its simplicity made it appealing for closed fractures. However, most studies to date show that the only advantage of unreamed nailing is less surgical time. All studies show higher nonunion rates with increased hardware failure and increased time to union for unreamed nailing. Even in open fractures graded up to Gustilo Grade IIIA, the reamed tibial nail performs better. Larsen LB, Madsen JE, Hoiness PR, et al: Should insertion of intramedullary nails for tibial fractures be with or without reaming? A prospective, randomized study with 3.8 years' follow-up. J Orthop Trauma 2004;18:144-149.
References:
- Blachut PA, O'Brien PJ, Meek RN, et al: Interlocking intramedullary nailing with or without reaming for the treatment of closed fractures of the tibial shaft: A prospective randomized study. J Bone Joint Surg Am 1997;79:640-646.
Question 71High Yield
Figures 45a through 45c show the radiograph, CT scan, and MRI scan of a 15-year-old boy who has lateral ankle pain. What is the most likely diagnosis?
Explanation
Explanation
45b 45c The elongated anterior process of the calcaneus reaching distally toward the navicular is an abnormal finding. Instead of viewing the rounded, blunt distal anterior process of the calcaneus, a bridge extends to the navicular, albeit incomplete. These findings are consistent with a fibrous coalition. CT can reveal a stress fracture of the calcaneus, arthritis of the subtalar joint with subchondral cysts, or an os peroneal bone disruption in the peroneus longus, but those entities are not shown here. The plantar fascia is intact. Richardson EG: Sesamoids and accessory bones of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 702-732.
References:
- Oestreich AE, Mize WA, Crawford AH, et al: The "anteater nose": A direct sign of calcaneonavicular coalition on the lateral radiograph. J Pediatr Orthop 1987;7:709-711.
Question 72High Yield
A 45-year-old man seen in the emergency department reports a 1-week history of worsening low back pain and a progressive neurologic deficit in the S1 distribution. Examination reveals 2/5 strength in the gastrocnemius. Laboratory studies show a WBC count of 13,500/mm3 and an erythrocyte sedimentation rate of 74 mm/h. Radiographs of the lumbosacral spine show narrowing of the L5-S1 disk space, with irregularity of the end plates. A sagittal T2-weighted MRI scan is shown in Figure 8. Definitive management should consist of
Explanation
The history, physical examination, laboratory, and radiographic findings are most consistent with an infectious process. When there are signs of neurologic compromise, surgery is generally recommended. This is an anterior process, and anterior column debridement is necessary, followed by stabilization. Anterior or posterior stabilization is a reasonable option, but posterior decompression alone is unlikely to adequately reverse the process and may lead to segmental kyphosis. Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 165-189.
Question 73High Yield
Figures 21a and 21b show the radiographs of a 22-year-old man who was shot through the abdomen the previous evening. An exploratory laparotomy performed at the time of admission revealed a colon injury. Current examination reveals no neurologic deficits. Management for the spinal injury should include

Explanation
IV broad-spectrum antibiotics should be administered for 7 days. This regimen, when compared to fragment removal or other antibiotic regimens, has been shown to reduce the incidence of spinal infections and reduce the need for metallic fragment removal with perforation of a viscus. Roffi RP, Waters RL, Adkins RH: Gunshot wounds to the spine associated with a perforated viscus. Spine 1989;14:808-811.
Question 74High Yield
A 12-year-old girl has progressive development of cavus feet. Examination reveals slightly diminished vibratory sensation on the bottom of the foot. Reflexes are 1+ at the knees and ankles. Motor examination shows that all muscles are 5/5 in the foot, except the peroneal and anterior tibial muscles are rated as 4+/5. Which of the following studies is considered most diagnostic?
Explanation
The patient most likely has a form of Charcot-Marie-Tooth disease, or hereditary motor sensory neuropathy (HMSN). The most common varieties can now be diagnosed by DNA testing. Mutations have been detected in the peripheral myelin protein-22 (PMP-22) gene in HMSN type IA and in the connexin gene in the x-linked HMSN. Specific DNA diagnosis is useful in genetic counseling. Routine chromosomal testing most likely would not detect these mutations. Nerve conduction velocity study results are normal in some types of HMSN, and delayed nerve conduction, when found, indicates a peripheral neuropathy but does not specify the type or inheritance pattern. Biopsy of the sural nerve or of the quadriceps can be informative in some patients, but is not as specific as DNA testing. These procedures are most often reserved for patients with negative DNA test results. Chance PF: Molecular genetics of hereditary neuropathies. J Child Neurol 1999;14:43-52.
Question 75High Yield
A 19-year-old football player who sustained three traumatic anterior shoulder dislocations underwent surgery to repair a Bankart lesion. Nine months after surgery, examination reveals stability, elevation to 150 degrees, external rotation to 0 degrees with the elbow at his side and to 50 degrees at 90 degrees of abduction, and internal rotation to T12. If his range of motion does not improve, he is at most risk for
Explanation
Loss of external rotation can lead to degenerative joint disease following an anterior stabilization procedure. A tight anterior capsule will prevent internal impingement. Risk of thoracic outlet syndrome should not be increased. Subscapularis detachment is a risk following open anterior repair; however, a gain in external rotation would be noted. In time, this patient's shoulder may show increased posterior glenohumeral wear but should not have symptoms of recurrent subluxation unless multidirectional instability is present. Hawkins RJ, Angelo RL: Glenohumeral osteoarthrosis: A late complication of the Putti-Platt repair. J Bone Joint Surg Am 1990;72:1193-1197.
Question 76High Yield
An elite skier training for the Olympics sustains an isolated traumatic dislocation of the peroneal tendons that have spontaneously reduced. The games are 9 months away and the athlete does not want to miss them. Treatment should consist of
Explanation
Explanation
Most of these injuries occur in young, active patients. Success rates for nonsurgical management are only marginally better than 50%. The treatment of choice is early surgery for patients who desire a quick return to a sport or active lifestyle. Subluxation of the peroneal tendons leads to longitudinal tears over time. McLennan JG: Treatment of acute and chronic luxations of the peroneal tendons. Am J Sports Med 1980;8:432-436.
References:
- Krause JO, Brodsky JW: Peroneus brevis tendon tears: Pathophysiology, surgical reconstruction, and clinical results. Foot Ankle Int 1998;19:271-279.
Question 77High Yield
A 36-year-old woman has pain and swelling of the anterior arm after undergoing arthroscopic shoulder surgery 8 months ago. At the time of the procedure, extensive debridement and synovectomy of the anterior aspect of the joint was performed to remove scar tissue that had formed after an open rotator cuff repair. Examination reveals a golf ball-sized swelling just lateral to the coracoid. The area is not warm and shows no other signs of infection. An MRI scan is shown in Figure 1. Management should now consist of
Explanation
Explanation
Deficiency of the rotator cuff interval may be acquired or congenital. In this patient, extensive debridement of the rotator cuff interval capsule at the time of arthroscopy most likely is the cause of the defect seen on the MRI scan. Surgical closure of the defect is the treatment of choice. During the repair, the shoulder should be placed in 30 degrees of external rotation to avoid overtightening. Care should be taken to include the leading edge of both the supraspinatus and subscapularis tendons in the repair because the rotator cuff interval capsular tissue is likely to be of poor quality. Cole BJ, Rodeo SA, O'Brien SJ, et al: The anatomy and histology of the rotator interval capsule of the shoulder. Clin Orthop 2001;390:129-137.
References:
- Jost B, Koch PP, Gerber C: Anatomy and functional aspects of the rotator interval. J Shoulder Elbow Surg 2000;9:336-341.
Question 78High Yield
Anabolic steroid use has which of the following effects on serum lipoprotein levels?
Explanation
The use of anabolic steroids causes a decrease in high-density lipoprotein levels but has no effect on low-density lipoprotein levels. An abnormally low high-density lipoprotein level should alert the physician to the possibility of steroid use in an athlete. Hartgens F, Rietjens G, Keizer HA, et al: Effects of androgenic-anabolic steroids on apolipoproteins and lipoprotein (a). Br J Sports Med 2004;38:253-259.
Question 79High Yield
Which of the following agents have been shown to reduce the incidence of skeletal events in patients with multiple myeloma?
Explanation
Bisphosphonates are a class of drugs that act to inhibit osteoclast resorption of bone. It has been shown that patients with multiple myeloma who are treated with bisphosphonates have fewer pathologic fractures than patients who are not treated with bisphosphonates. Vitamin D and calcium are considered appropriate for patients who are at risk for the development of osteoporosis, as is estrogen in selected women. Chelating agents and progesterones have no use in the treatment of patients with multiple myeloma or osteoporosis. Berenson JR: Bisphosphonates in multiple myeloma. Cancer 1997;15:1661-1667.
Question 80High Yield
Ulnohumeral distraction interposition arthroplasty is considered the most appropriate treatment for which of the following patients?
Explanation
Distraction interposition arthroplasty is indicated for the treatment of both rheumatoid and posttraumatic arthritis and is reserved for younger patients who are not suitable candidates for total elbow arthroplasty. Although less reliable than prosthetic replacement, distraction interposition arthroplasty is a useful option in the treatment of young, high-demand patients with elbow arthritis. It is rarely indicated in the presence of polyarticular inflammatory arthritis but may be of value in those patients in whom the disease is limited primarily to the elbow. Isolated radiocapitellar arthritis can be successfully treated with radial head resection, although caution should be exercised if there is evidence of instability. Osteoarthritis is best treated with ulnohumeral arthroplasty. Cheng SL, Morrey BF: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Question 81High Yield
A 21-year-old right hand-dominant male collegiate swimmer reports painful clicking in the right shoulder. He states that he can occasionally feel his shoulder "slip out" when he is working out. AP, true AP, and axillary radiographs are shown in Figures 39a through 39c. What is the next most appropriate step in management?


Explanation
The radiographs show glenoid hypoplasia. The common radiographic findings of glenoid hypoplasia include an inferior and posterior glenoid deficiency, enlargement of the distal end of the clavicle, and sometimes an indentation in the glenoid. It is usually bilateral and rarely associated with other syndromes; therefore, an echocardiogram, abdominal ultrasound, or a skeletal survey is unnecessary unless the patient has stigmata of a syndrome such as Holt-Oram or Apert's. Although posterior instability has been reported, the results of glenoid osteotomy have been variable and should not be considered initially. Physical therapy is the mainstay of initial management, but the patient should be counseled that this may be a recurrent problem with early osteoarthritis developing in many patients. Radiographs of the contralateral side should be obtained because this is usually bilateral. Wirth MA, Lyons FR, Rockwood CA Jr: Hypoplasia of the glenoid: A review of sixteen patients. J Bone Joint Surg Am 1993;75:1175-1184.
Question 82High Yield
Figures 19a through 19c show radiographs of the cervical spine of an asymptomatic patient with Down syndrome who wants to participate in a Special Olympics running event. The neurologic examination is normal. Management should consist of
Explanation
Explanation
19b 19c An atlanto-dens interval (ADI) of up to 4 mm in children is considered normal. Children with Down syndrome have increased ligamentous laxity, with atlantoaxial instability occurring in as many as 15% to 20% of patients. These patients are at risk for catastrophic injury following minor trauma and should be routinely screened for instability, generally beginning when the patient starts to walk. Patients with an ADI of greater than 5 mm should avoid contact sports and high-risk activities such as gymnastics, diving, the high jump, and the butterfly stroke. The American Academy of Pediatrics Committee of Sports Medicine and Fitness guidelines recommend that lateral views of the cervical spine in neutral, flexion, and extension should be obtained in all children with Down syndrome who wish to participate in sports. Patients with normal radiographs and examinations do not need repeat radiographs, although some authors suggest that instability increases with age, and therefore recommend repeat radiographs every 5 years. Cervical spine fusion in patients with Down syndrome has a high rate of complications and should be performed only on patients with symptoms and evidence of myelopathy. American Academy of Pediatrics Committee of Sports Medicine and Fitness: Atlantoaxial instability in Down syndrome. Pediatrics 1995;96:151-154. Copley LA, Dormans JP: Cervical spine disorders in infants and children. J Am Acad Orthop Surg 1998;6:204-214.
References:
- Tredwell SJ, Newman DE, Lockitch G: Instability of the upper cervical spine in Down syndrome. J Pediatr Orthop 1990;10:602-606.
Question 83High Yield
What is the most common cause of rotator cuff injury in high school athletes?
Explanation
Explanation
A large number of etiologies of rotator cuff injury have been proposed. Both intrinsic and extrinsic mechanisms have been suggested. In the young athlete the common underlying mechanism is overuse. Contributing factors include increased laxity, anatomic variation in the coracoacromial arch, and altered kinematics. Wilkins KE: Shoulder injuries: Epidemiology, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 175-182.
References:
- Sher JS: Anatomy, biomechanics, and pathophysiology of rotator cuff disease, in Iannnotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 3-30.
Question 84High Yield
A Trendelenburg gait is most likely to be seen in association with
Explanation
A Trendelenburg gait results from weakness of the gluteus medius, which is innervated by the L5 nerve root. A paracentral disk herniation at L4-L5 most commonly results in an L5 radiculopathy and thus weakness of the gluteus medius. A paracentral herniation at L5-S1 most commonly affects the S1 nerve root. A paracentral herniation at L3-L4, a central herniation at L3-L4, and a far lateral herniation at L4-L5 all affect the L4 root. Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Question 85High Yield
A 55-year-old woman has slowly increasing pain at the distal end of her little finger that is exacerbated by cold temperatures. She denies any history of trauma to her hands and is employed as a school teacher. The histology of the resected specimen is shown in Figure 71. What is the most likely diagnosis?
Explanation
Explanation
Glomus tumors are rare vascular lesions typically occurring about the nail of the distal phalanx of the hand. The diagnostic "triad" of glomus tumors consists of local pain, sensitivity to cold, and paroxysmal pain. They tend to present with pain as the most typical symptom and this can be exacerbated by changes in temperature that is felt to cause a vascular response within the lesion. The biopsy specimen confirms a glomus tumor showing the typical vascular spaces surrounded by glomus epithelioid glomus cells. Zook EG, Brown RE: The perionychium, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 1353-1380.
References:
- McDermott EM, Weiss AP: Glomus tumors. J Hand Surg Am 2006;31:1397-1400.
Question 86High Yield
A 46-year-old patient with cervical myelopathy undergoes a multilevel posterior cervical laminectomy from C3 to C7. The risk of postlaminectomy kyphosis is greatest with removal of which of the following structures?
Explanation
Removal of more than 50% of a facet joint can lead to segmental instability and compromises the overall strength of the joint. Removal of the lamina, interspinous ligament, and ligamentum flavum are standard features of a cervical laminectomy. Most surgeons favor fusion with instrumentation of a laminectomized cervical spine. If the anterior part of the spine is already ankylosed from previous surgery or from degenerative conditions, or a posterior fusion with instrumentation is included, then the risk of kyphosis or instability is reduced.
Question 87High Yield
What mechanism contributes to strength gains during conditioning of the preadolescent athlete?
Explanation
Prepubescent athletes gain strength through neurogenic adaptations, including recruitment of motor units, reduced inhibition, and learned motor skills. Myogenic adaptations (muscle hypertrophy) occur after puberty and include increased contractile proteins, thickening of the connective tissue, and increased short-term energy sources such as creatine phosphate. Grana WA: Strength training, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 520-526.
Question 88High Yield
Which of the following properties apply to the human meniscus when compared with articular cartilage?
Explanation
The meniscal cartilage, like articular cartilage, possesses viscoelastic properties. The extracellular matrix is a biphasic structure composed of a solid phase (collagen, proteoglycan) that acts as a fiber-reinforced porous-permeable composite, and a fluid phase that may be forced through the solid matrix by a hydraulic pressure gradient. Although these properties are shared with articular cartilage, the meniscus is more elastic and less permeable than articular cartilage. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 3-23.
Question 89High Yield
What is the most common bone tumor in the hand?
Explanation
The most common bone tumor in the hand is an enchondroma. Forty-two percent of these lesions occur in the small tubular bones. They frequently present with a fracture in these locations. Fractures are usually treated nonsurgically. Indications for surgery include patients with symptomatic lesions or those who are considered high risk for recurrent fracture. The histologic appearance of an enchondroma in the hand is more cellular than enchondromas found in the long bones. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 103.
Question 90High Yield
Which of the following anatomic structures is often difficult to visualize during elbow arthroscopy?
Explanation
The ulnar collateral ligament is often difficult to visualize during elbow arthroscopy. It can be seen clearly in only 10% to 30% of elbow arthroscopies. All of the other structures should be easily and thoroughly seen and palpated during elbow arthroscopy. Johnson LL: Arthroscopic Surgery: Principles and Practice. St Louis, MO, CV Mosby, 1988.
Question 91High Yield
A previously asymptomatic 40-year-old man injures his shoulder in a fall. Examination shows that he is unable to lift the hand away from his back while maximally internally rotated. An axial MRI scan of the shoulder is shown in Figure 14. What is the most likely diagnosis?
Explanation
The MRI scan shows detachment of the subscapularis from its insertion on the lesser tuberosity. The examination finding is consistent with a positive lift-off test, also indicating a tear of the subscapularis. Lyons RP, Green A: Subscapularis tendon tears. J Am Acad Orthop Surg 2005;13:353-363.
Question 92High Yield
What nerve is at the highest risk for injury with a percutaneous repair of an Achilles tendon injury?
Explanation
Cadaver and clinical studies have shown that the sural nerve is at the highest risk for injury with a percutaneous repair of the Achilles tendon.
Question 93High Yield
A 58-year-old patient who underwent bilateral hip arthroplasty 12 years ago now reports pain in his hips and difficulty with ambulation to the point where he now uses crutches. A radiograph of the hip and pelvis is shown in Figure 26. What is the best treatment option for this patient?
Explanation
Explanation
The radiographs reveal acetabular component failure with bone loss. There are several treatment options available. The best option for survivorship is a cementless porous-coated acetabular component. This patient may or may not require structural bone graft, which may need to be determined at the time of surgery. Bipolar implants and cemented acetabular components for revision surgery have not demonstrated long-term success. The use of a protrusio ring is reserved primarily for massive bone loss such as a Paprosky type III bone loss with significant superior migration of the acetabular component. The best clinical results for acetabular component revision have been achieved with cementless porous-coated implants. Haddad FS, Masri BA, Garbuz DS, et al: Acetabulum, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 923-936. D'Antonio JA: Periprosthetic bone loss of the acetabulum: Classification and management. Orthop Clin North Am 1992;23:279-290.
References:
- Rubash HE, Sinha RK, Paprosky W, et al: A new classification system for the management of acetabular osteolysis after total hip arthroplasty. Instr Course Lect 1999;48:37-42.
Question 94High Yield
A 15-year-old girl who plays high school basketball has had worsening forefoot pain and swelling that is aggravated by activity for the past 5 weeks. She denies any history of an injury. Examination reveals no deformities. A radiograph is shown in Figure 38. Initial management should consist of
Explanation
Explanation
Freiberg's infraction is believed to be an osteochondrosis of the second metatarsal head. It is the only osteochondrosis that has a predilection for females. The typical patient is an athletically active adolescent female. The radiograph shows stage II disease wherein reossification is occurring; it is at this time that the second metatarsal head is most susceptible to deformation. Therefore, initial management should consist of a short leg walking cast.
References:
- Mann RA, Coughlin MJ: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 413-415.
Question 95High Yield
A previously healthy 13-year-old girl has had thigh pain for the past 3 weeks. The radiograph shown in Figure 47a reveals a lesion in the right femur. A bone scan and CT scan of the chest show no evidence of other lesions. A biopsy specimen is shown in Figure 47b. What is the most likely diagnosis?

Explanation
The patient has Langerhans cell histiocytosis that may be solitary (eosinophilic granuloma) or associated with systemic illness (Hand-Schuller-Christian disease and Letterer-Siwe disease). The solitary form of the disease, eosinophilic granuloma, typically affects patients in the first three decades of life. Radiographically, it is characterized as a well-defined, lytic, "punched out" intramedullary lesion. Histologically, two cell types, eosinophils and Langerhans cells, are seen. The Langerhans cells are seen as mononuclear histiocyte-like cells with oval nuclei with well-defined round or oval cytoplasm. A prominent nuclear groove can be seen in most of the nuclei (coffee bean nuclei). A mixture of inflammatory cells and lipid-laden foam cells with nuclear debris may be present as well. The lack of nuclear atypia and atypical mitoses excludes malignant conditions such as Ewing's sarcoma, lymphoma of bone, and metastatic neuroblastoma. The lack of acute inflammatory cells excludes the diagnosis of osteomyelitis. The eosinophils have bi-lobed nuclei and granular eosinophilic cytoplasm. Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby, 1988.
Question 96High Yield
What procedure can eliminate a sulcus sign?
Explanation
A sulcus sign represents inferior subluxation of the shoulder. The elimination of this sign and correction of the inferior subluxation is best achieved through either an open or arthroscopic rotator interval closure. A SLAP repair stabilizes the biceps anchor but does not affect the sulcus sign. A Bankart repair, which corrects anterior-inferior laxity, is not sufficient to eliminate a sulcus sign. Subacromial decompression and supraspinatus repairs have no effect on inferior subluxation. Field LD, Warren RF, O'Brien SJ, et al: Isolated closure of rotator interval defects for shoulder instability. Am J Sports Med 1995;23:557-563.
Question 97High Yield
The injection shown in Figures 1a and 1b would most benefit a patient who reports which of the following symptoms?

Explanation
The images demonstrate a L5 selective root block as it exits the L5-S1 foramen. This root block best helps relieve pain or paresthesias in the L5 distribution, which is the dorsal first web space and the great toe. The lateral foot is an S1 distribution and would need to be blocked through the posterior first sacral foramen. The anterior shin and thigh represent the L4 root which exits a level above this at the L4-5 foramen. A stocking distribution is nonanatomic and not indicative of a specific root. Magee D: Principles and concepts, in Orthopaedic Physical Assessment, ed 3. Philadelphia, PA, WB Saunders, 1997, pp 1-18.
Question 98High Yield
What is the most common bacteria cultured from dog and cat bites to the upper extremity?
Explanation
To define bacteria responsible for dog and cat bite infections, a prospective study yielded a median of five bacterial isolates per culture. Pasteurella is most common from both dog bites (50%) and cat bites (75%). Pasteurella canis was the most frequent pathogen of dog bites, and Pasteurella multocida was the most common isolate of cat bites. Other common aerobes included streptococci, staphylococci, moraxella, and neisseria.
Question 99High Yield
A 25-year-old woman who fell on her outstretched hand reports chronic pain over the hypothenar eminence region and some dorsal ulnar wrist pain. She also notes difficulty playing golf and tennis. Plain radiographs of the hand and wrist are unremarkable. A CT scan is shown in Figure 36. What is the next most appropriate step in management?
Explanation
The CT scan reveals a hook of the hamate nonunion with irregular resorption at the fracture site, which is at the base of the hamate. Symptomatic relief of the pain and discomfort has been well documented after excision of the hook of the hamate. Ultrasound therapy will not provide long-term symptomatic relief or induce nonunion healing. MRI for further soft-tissue evaluation is inappropriate because this is a bony problem; the bony architecture of the wrist is best visualized by CT. Open reduction and internal fixation of the hook of the hamate does not provide the symptomatic relief that is found with excision of the hook of the hamate. In addition, the technical difficulties and relative risk of persistent nonunion after open reduction and internal fixation are not merited when hamate excision can be effected easily and causes no long-term untoward effects. Electrodiagnostic evaluation is inappropriate because there is no history of the persistent numbness and tingling that is found in peripheral compression neuropathies. Stark HH, Chao EK, Zemel NP, Rickard TA, Ashworth CR: Fracture of the hook of the hamate. J Bone Joint Surg Am 1989;71:1206-1207. Failla JM: Hook of hamate vascularity: Vulnerability to osteonecrosis and nonunion. J Hand Surg Am 1993;18:1075-1079. Carter PR, Easton RG, Littler JW: Ununited fracture of the hook of the hamate. J Bone Joint Surg Am 1977;59:583-588.
Question 100High Yield
An 8-month-old infant has an infection of the fingertip as shown in Figure 22. If neglected, the anticipated path of ascending infection is the fingertip, the flexor sheath, and the
Explanation
Explanation
The flexor sheaths are in continuity with the deep spaces of the hand. The flexor sheaths of the thumb and little finger communicate with the radial and ulnar bursae, respectively, and these two bursae commonly communicate. The central digits do not communicate as readily with deep spaces of the hand but if flexor tendon sheath infection of the index, long, and right fingers is neglected, the potential exists for rupture into the deep midpalmar spaces. Peimer CA (ed): Surgery of the Hand and Upper Extremity: Acute and Chronic Sepsis. New York, NY, Mcgraw Hill, 1996, pp 1735-1741.
References:
- Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow and Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 445-446.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon