Orthopedic Board Review: Set 533 - 100 High-Yield MCQs for ABOS, OITE, FRCS
14 Apr 2026
105 min read
81 Views
Key Takeaway
This page features 100 high-yield orthopedic board review multiple-choice questions (MCQs) from Mock Exam Set #533. It helps surgeons preparing for ABOS, OITE, and FRCS exams master critical concepts and assess their readiness with targeted practice.
Pinpoint Root Lesions Involving the Trunk & L...
00:00
Start Quiz
Question 1High Yield
Why is tendon considered an anisotropic material?
Explanation
Explanation
Anisotropic materials have mechanical properties that vary based on the direction of loading. The relative values of Young's modulus for tendon, ligament, and bone are not relevant to isotropy. The mechanical properties of tendon do change with preconditioning, but this change is related to viscoelasticity. The intrinsic mechanical properties of tendon do vary with the rate of loading, but this variance is related to viscoelasticity. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180.
References:
- Lu L, Kaufman KR, Yaszemski MJ: Biomechanics, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 2High Yield
An intoxicated 68-year-old man fell at home. Examination reveals abrasions on his forehead, 2/5 weakness of his hand intrinsics and finger flexors, and 4/5 strength of the deltoid, biceps, and triceps bilaterally. Lower extremity motor function is 5/5. Sensory examination to pain and temperature is diminished in his hands but intact in his lower extremities. Deep tendon reflexes are depressed in all four extremities, but perianal sensation and rectal tone are intact. Foley catheterization yields 700 mL of urine. Radiographs of the cervical spine reveal multilevel spondylosis without fracture or subluxation. An MRI scan reveals high-intensity signal change within the cord substance at C5. What is the most likely diagnosis?
Explanation
Explanation
Central cord syndrome is characterized by greater neurologic involvement of the upper extremities than the lower extremities. This is typically seen in older patients with cervical spondylosis without associated bony injury or joint subluxation. The prognosis for recovery is fair. Patients with Brown-Sequard syndrome have an ipsilateral motor deficit and contralateral loss of pain and temperature. Prognosis for recovery depends on the mechanism of injury, which is often of a penetrating nature. Anterior cord syndrome results from anterior compression such as occurs with a burst or teardrop fracture of the vertebral body; patients have bilateral motor loss, pain, and temperature loss with preservation of proprioception and vibratory sensation (posterior column function). The prognosis for recovery is generally poor. Posterior cord syndrome is rare and is associated with loss of posterior column function (proprioception and vibration). Northrup BE: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 541-549.
References:
- Schneider RC, Thompson JM, Rebin J: The syndrome of acute central cervical spinal cord injury. J Neurol Neurosurg Psychiatry 1958;21:216-227.
Question 3High Yield
What acetabular procedure for developmental dysplasia of the hip does not require a concentric reduction of the femoral head in the acetabulum?
Explanation
Explanation
All of the reorientation innominate osteotomies require a concentric reduction of the hip. The Staheli shelf procedure may be performed even with the hip subluxated, but it is a salvage procedure that covers a portion of the femoral head with capsular fibrocartilage rather than hyaline cartilage. Staheli LT, Chew DE: Slotted acetabular augmentation in childhood adolescence. J Pediatr Orthop 1992;12:569-580.
References:
- Herring JA: Tachdjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 618-650.
Question 4High Yield
A 20-year-old college baseball pitcher reports the insidious onset of medial elbow pain. Examination reveals medial elbow tenderness, a normal neurologic examination, and no obvious valgus laxity. Plain radiographs are normal. MRI scans are shown in Figures 39a and 39b. Management should consist of
Explanation
Explanation
39b Throwers and in particular, pitchers, are prone to high valgus loads to the elbow. A constellation of medial elbow pathology can develop, including medial epicondylitis, ulnar nerve neuritis, medial ulnar collateral ligament injuries, and posteromedial osteophytes of the olecranon. The MRI scans show significant increases in signal intensing as well as fiber disruption of the medial collateral ligament, indicating a complete tear. The common flexor origin shows a homogeneous signal and normal morphology. Therefore, excision of posterior osteophytes and debridement of the common flexor origin are not indicated. Likewise, this patient's symptoms do not indicate ulnar nerve pathology; therefore ulnar nerve transposition is not indicated. Primary repair of medial collateral ligament tears of the elbow lead to unpredictable results with an unacceptable rate of reoperation. The most predictable result in treating this high-demand athlete is reconstruction of the medial collateral ligament with autogenous tissue. Norris TR (ed): Athletic Injuries of the Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 311-323.
References:
- Hyman J, Breazeale NM, Altchek DW: Valgus instability of the elbow in athletes. Clin Sports Med 2001;20:11-24.
Question 5High Yield
A 70-year-old woman has a preoperative anterior interscalene block prior to undergoing a total shoulder arthroplasty. After seating her in the beach chair position, she becomes acutely hypotensive. What is the most likely cause for the hypotension?
Explanation
The beach chair position may cause sudden hypotension and bradycardia as a result of the Bezold-Jarisch reflex. This reflex occurs when venous pooling and increased sympathetic tone induce a low-volume, hypercontractile ventricle, resulting in activation of the parasympathetic nervous system and sympathetic withdrawal. The reported incidence of this phenomenon associated with the sitting position is between 13% to 24%. Left untreated, the result may be cardiac arrest. Pneumothorax or central nervous system toxicity after interscalene block is rare and has an incidence of less than 0.2%. Laryngeal nerve block associated with interscalene nerve block can occur but usually results in hoarseness secondary to ipsilateral vocal cord palsy. Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14:546-556.
Question 6High Yield
Figure 33 shows the MRI scan of a 55-year-old woman who has had a 6-week history of back and leg pain. Which of the following clinical scenarios is most consistent with the MRI scan findings at L4-L5?
Explanation
The MRI scan reveals a L4-L5 foraminal disk herniation originating from the L4-5 disk space that has migrated up into the foramen, compressing the left L4 nerve root. There is normal distribution of the roots in the cerebrospinal fluid, excluding arachnoiditis as a diagnosis, and disk herniation in this location would not result in cauda equina syndrome or myelopathy.
Question 7High Yield
Sterilization of ultra-high molecular weight polyethylene by gamma irradiation in air will degrade its wear performance because of
Explanation
Explanation
Gamma irradiation has long been used as a sterilization method for polyethylene. Exposure to gamma irradiation causes breakage of the chemical bonds in the polyethylene, and oxidation will occur if the material is subsequently exposed to air. The amount of oxidation and decrease in wear performance is also related to the length of time that the gamma-irradiated polyethylene is exposed to oxygen. Collier JP, Sutula LC, Currier BH, et al: Overview of polyethylene as a bearing material: Comparison of sterilization methods. Clin Orthop 1996;333:76-86. McKellop H, Shen FW, Lu B, et al: Effect of sterilization method and other modifications on the wear resistance of acetabular cups made of ultra-high molecular weight polyethylene: A hip-simulator study. J Bone Joint Surg Am 2000;82:1708-1725.
References:
- Sychterz CJ, Young AM, Orishimo K, et al: The relationship between shelf life and in vivo wear for polyethylene acetabular liners. J Arthroplasty 2005;20:168-173.
Question 8High Yield
A collegiate football player who sustained an injury to his neck has significant neck pain and weakness in his extremities. Following immobilization, which of the following steps should be taken prior to transport?
Explanation
Prior to transport, the face mask should be removed so that the airway can be easily accessible. If serious injury is suspected, the helmet and shoulder pads should be left in place until he is assessed at the hospital and radiographs are obtained. Leaving the helmet and shoulder pads in place helps to keep the spine in the most neutral alignment. Removal of the helmet will result in extension of the neck, whereas removal of the shoulder pads will most likely result in flexion of the neck. Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 376. Thomas B, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347. Waninger KN, Richards JG, Pan WT, et al: An evaluation of head movement in backboard-immobilized helmeted football, lacrosse, and ice hockey players. Clin J Sport Med 2001;11:82-86. Donaldson WF III, Lauerman WC, Heil B, et al: Helmet and shoulder pad removal from a player with suspected cervical spine injury: A cadaveric model. Spine 1998;23:1729-1732.
Question 9High Yield
A 42-year-old woman underwent an instrumented posterior spinal fusion at L3-S1 with transforaminal lumbar interbody fusion. She had an excellent clinical result with complete resolution of leg pain. Three months later she now reports increasing back pain and weakness in her legs. Examination reveals weakness in the quadriceps and tibialis anterior. Radiographs show no interval changes in the position of the hardware. MRI scans are shown in Figures 2a through 2c. What is the next most appropriate step in management?


Explanation
The MRI scans reveal a postoperative infection. Observation and antibiotics are not appropriate choices. There is a large fluid collection and this requires decompression because the patient has neurologic changes. There is considerable debate regarding the removal of hardware. Many contend that biofilm on the implants can harbor the infection. However, these complications usually can be treated with serial irrigations, debridements, and IV antibiotics. The incidence of infection has been widely studied with varying rates in fusions with instrumentation. Rates appear to be increased with instrumentation, yet these infections usually can be managed without hardware removal. Glassman SD, Dimar JR, Puno RM, et al: Salvage of instrumental lumbar fusions complicated by surgical wound infection. Spine 1996;21:2163-2169.
Question 10High Yield
Examination of a 5-year-old boy with amyoplasia shows a flexion contracture of 70 degrees of the right knee. The active arc of motion is from 70 degrees to 90 degrees, and the opposite knee has a flexion contracture of 10 degrees. Both hips are dislocated with flexion contractures of 10 degrees, passive hip motion is from 10 degrees to 90 degrees of flexion, and the feet are plantigrade and easily braceable. Despite a daily stretching program, the parents and physical therapists note that it is increasingly difficult for him to walk because of the flexion contracture of the right knee. Management of the knee flexion contracture should now include
Explanation
Most children with amyoplasia are ambulatory and when a decrease in function occurs because of a severe contracture, it must be addressed. A radical posterior soft-tissue release, including the posterior knee capsule and often the collateral ligaments and the posterior cruciate ligament, is needed to obtain extension. After the age of 1 year, aggressive physical therapy will do little to correct a contracture. Botulinum toxin A is indicated for spasticity and is contraindicated with severe contractures. Supracondylar femoral extension osteotomy works well, but will remodel at an average rate of 1 degree per month, which is not considered ideal in a young patient. Gradual correction with a circular ring external fixator is an option, but a soft-tissue release will also most likely be needed for a contracture of this severity. Sarwark JF, MacEwen GD, Scott CI Jr: Amyoplasia (a common form of arthrogryposis). J Bone Joint Surg Am 1990;72:465-469. DelBello DA, Watts HG: Distal femoral extension osteotomy for knee flexion contracture in patients with arthrogryposis. J Pediatr Orthop 1996;16:122-126.
Question 11High Yield
Injury to which of the following structures has been reported following iliac crest bone graft harvest?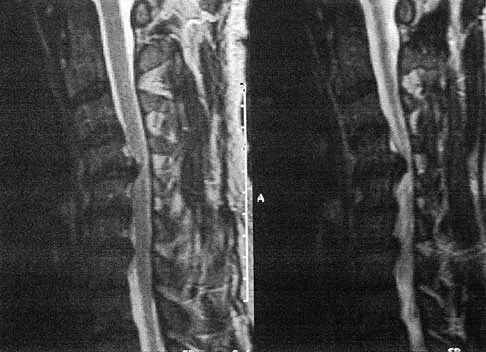
Explanation
Injury to the lateral femoral cutaneous nerve and the ilioinguinal nerve have both been described with an anterior iliac crest bone graft harvest. The lateral femoral cutaneous nerve may be injured from retraction after elevating the iliacus muscle or from direct injury when the nerve actually courses over the crest. A posterior crest harvest can injure the superior gluteal artery if a surgical instrument violates the sciatic notch. Injury to the inferior gluteal artery has not been described; it leaves the pelvis below the piriformis muscle belly and should not be at risk even with a violation of the sciatic notch. Injury to the ilioinguinal nerve has been reported from vigorous retraction of the iliacus muscle after exposing the inner table of the anterior ilium. Cluneal nerve injury may occur with posterior crest harvest, particularly if the skin incision is horizontal or extends more than 8 cm superolateral from the posterior superior iliac spine. Kurz LT, Garfin SR, Booth RE Jr: Iliac bone grafting: Techniques and complications of harvesting, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 323-341.
Question 12High Yield
A 62-year-old woman has back pain and right L2 radicular pain. MRI scans suggest a neoplastic lesion at L2, and a bone scan is negative except at L2. History reveals that she was treated for breast cancer without known metastatic disease 12 years ago and is thought to be free of disease. What is the next most appropriate step in management?
Explanation
Because of the long disease-free interval, it cannot be assumed that this is breast cancer. The lesion could represent metastasis from a new primary tumor or could itself be a primary tumor. CT-guided biopsy will most effectively identify the lesion and guide treatment options. Depending on the specific diagnosis, any of the other options may be appropriate.
Question 13High Yield
A 64-year-old man who was involved in a high-speed motor vehicle accident 6 weeks ago has been in the ICU with a closed head injury. Examination reveals that his range of motion for external rotation to the side is -30 degrees. Radiographs are shown in Figures 28a and 28b. What is the most likely diagnosis?

Explanation
The patient has a posterior shoulder dislocation. The AP radiograph shows overlapping of the humeral head on the glenoid. The scapular Y view shows his humeral articular surface posterior to the glenoid. The posterior shoulder dislocation is frequently missed because the patient is comfortable in the "sling" position with the arm adducted and internally rotated across the abdomen. The marked restriction in external rotation on examination raises the suspicion of a posterior dislocation, adhesive capsulitis, or glenohumeral osteoarthritis. The posterior dislocation is diagnosed based on the radiographic findings. An axillary view or CT is recommended to better evaluate the dislocation. Robinson CM, Aderinto J: Posterior shoulder dislocations and fracture-dislocations. J Bone Joint Surg Am 2005;87:639-650.
Question 14High Yield
What is the most common clinical presentation of a patient with a malignant bone tumor?
Explanation
Explanation
The most common clinical presentation of a patient with a malignant bone tumor is pain. Malignant bone tumors rarely are diagnosed as an incidental finding or pathologic fracture. In patients who have a pathologic fracture on initial presentation, a history of increasing pain prior to the fracture is typical. While 90% of malignant bone tumors are associated with a soft-tissue mass, in many patients the soft-tissue component of the tumor is not clinically apparent. Buckwalter JA: Musculoskeletal neoplasms and disorders that resemble neoplasms, in Weinstein SL, Buckwalter JA (eds): Turek's Orthopaedics: Principles and Their Application, ed 5. Philadelphia, PA, JB Lippincott, 1994, pp 290-295.
References:
- Mehlman CT, Crawford AH, McMath JA: Pediatric vertebral and spinal cord tumors: A retrospective study of musculoskeletal aspects of presentation, treatment, and complications. Orthopedics 1999;22:49-55.
Question 15High Yield
When the iliac apophysis starts ossifying in the normal adolescent, growth of the sitting height or trunk height is characterized by
Explanation
Explanation
Studies by Anderson and associates have resulted in a growth-remaining chart for sitting height that shows an increase of 3 to 5 cm in girls and an increase of 5 to 8 cm in boys. Future growth of the spine may impact brace longevity and fit. Anderson M, Hwang SC, Green WT: Growth of the normal trunk in boys and girls during the second decade of life: Related to age, maturity, and ossification of the iliac epiphyses. J Bone Joint Surg Am 1965;47:1554-1564.
References:
- Zaoussis AL, James JIP: The iliac apophysis and the evolution of curves in scoliosis. J Bone Joint Surg Br 1958;40:442-453.
Question 16High Yield
The teardrop shape marked with an asterisk in Figure 61 represents what anatomic structure?
Explanation
Explanation
The teardrop can be visualized on the obturator outlet view of the pelvis and represents a thick column of bone that runs from the AIIS to the PSIS. Half pins for eternal fixation frames or screws can be inserted into this column for fixation of fractures. Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273. Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
Question 17High Yield
A 13-year-old boy injured his knee playing basketball and is now unable to bear weight. Examination reveals tenderness and swelling at the proximal anterior tibia, with a normal neurologic examination. AP and lateral radiographs are shown in Figures 1a and 1b. Management should consist of
Explanation
Explanation
1b The patient has a displaced intra-articular tibial tuberosity fracture; therefore, the treatment of choice is open reduction and internal fixation. Periosteum is often interposed between the fracture fragments and prevents satisfactory closed reduction. Fortunately, most patients with this injury are close to skeletal maturity and therefore, growth arrest and recurvatum are unusual. Nondisplaced fractures can be treated with a cast, but displaced fractures are best treated with open reduction and internal fixation. Intra-articular fractures can disrupt the joint surface and are sometimes associated with a meniscal tear; therefore, arthroscopy may be needed at the time of open reduction and internal fixation. McKoy BE, Stanitski CL: Acute tibial tubercle avulsion fractures. Orthop Clin North Am 2003;34:397-403.
References:
- Zionts LE: Fractures around the knee in children. J Am Acad Orthop Surg 2002;10:345-355.
Question 18High Yield
Figures 21a and 21b show the radiographs of a 22-year-old man who was shot through the abdomen the previous evening. An exploratory laparotomy performed at the time of admission revealed a colon injury. Current examination reveals no neurologic deficits. Management for the spinal injury should include

Explanation
IV broad-spectrum antibiotics should be administered for 7 days. This regimen, when compared to fragment removal or other antibiotic regimens, has been shown to reduce the incidence of spinal infections and reduce the need for metallic fragment removal with perforation of a viscus. Roffi RP, Waters RL, Adkins RH: Gunshot wounds to the spine associated with a perforated viscus. Spine 1989;14:808-811.
Question 19High Yield
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3, an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Explanation
Examination reveals an irritable hip, creating a differential diagnosis of transient synovitis versus pyogenic hip arthritis. Kocher and associates described four criteria to help predict the presence of infection: inability to bear weight, fever, ESR of more than 40 mm/h, and a peripheral WBC count of more than 12,000/mm3. This patient meets three of the four criteria, with a positive predictive value of 73% to 93% for joint infection. Therefore, aspiration of the hip is warranted, with a high likelihood that emergent hip arthrotomy will be indicated. Ideally, intravenous antibiotics should be administered after culture material has been obtained from needle aspiration of the hip. An urgent bone scan is better indicated as a screening test for sacroiliitis or diskitis. If the arthrocentesis proves negative, CT or MRI of the pelvis may be indicated to rule out a pelvic or psoas abscess. Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422. Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 20High Yield
What is the current 5-year survival rate for patients with classic nonmetastatic, high-grade osteosarcoma of the extremity?
Explanation
Multidisciplinary treatment combining systemic chemotherapy and adequate surgical resection has resulted in a 5-year survival rate of 70% in patients with nonmetastatic osteosarcoma of the extremity . The advent of effective chemotherapy has increased the overall survival rate from 20% to 70% in current studies. Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Question 21High Yield
Figure 37 shows the radiograph of a 21-year-old collegiate basketball player who has had mild midfoot aching for the past 4 months. What is the best course of action?
Explanation
Explanation
A stress fracture of the navicular is considered a high-risk injury because of the incidence of nonunion. If identified early, cast immobilization with no weight bearing is appropriate. However, this patient is a high-caliber athlete who has had symptoms for 4 months. Therefore, surgery is recommended to expedite recovery and optimize the chance of healing. Meyer SA, Saltaman CL, Albright JP: Stress fractures of the foot and ankle. Clin Sports Med 1993;12:395-413. Kahn JM, Fuller PJ, Burkner PD, et al: Outcome of conservative and surgical management of navicular stress fractures in athletes: Eighty-six cases proven with computerized tomography. Am J Sports Med 1992;20:657-666.
References:
- Fitch KD, Blackwell JP, Gillmour WN: Application for non-union stress fractures of the tarsonavicular. J Bone Joint Surg Br 1989;71:105.
Question 22High Yield
A 25-year-old man sustained a head injury after being ejected from his car. Examination reveals a Glasgow Coma Scale score of 7 and a swollen right knee. Clinical examination shows that the knee is very unstable, suggesting tears of the medial collateral and anterior and posterior cruciate ligaments, as well as the posterior lateral corner. What is the most appropriate first step to rule out a vascular injury?
Explanation
A knee dislocation carries the potential for an arterial injury and has always brought up the question of need for arteriography to rule out this limb-threatening injury. However, arteriography has an inherent complication rate that may compromise the general care of the patient. In over 240 published cases with documented knee dislocations that were evaluated for vascular injury by physical examination (without imaging studies), not a single missed injury was reported, for a 100% negative predictive value (0% false-negative rate). This degree of accuracy at excluding major vascular injury is unsurpassed by the results obtained with arteriography but with no risk involved and a marked savings in time, equipment, and costs. Therefore, the most appropriate first step to rule out vascular injury is examination of the pedal pulses. If there is any doubt about an arterial injury, another option is the ankle-brachial index (ABI). If the ABI is greater than 0.9, the chance of arterial injury is again nonexistent. However, a positive physical examination or an ABI of less than 0.9 is not 100% predictive of an arterial injury; therefore, arteriography is recommended. Miranda FE, Dennis JW, Veldenz HC, et al: Confirmation of the safety and accuracy of physical examination in the evaluation of knee dislocation for injury of the popliteal artery: A prospective study. J Trauma 2002;52:247-252.
Question 23High Yield
Figures 16a and 16b show the radiographs of an otherwise healthy 3 1/2-year-old boy who has an isolated deformity of the left leg. Definitive primary treatment of this condition should consist of

Explanation
Treatment of congenital pseudarthrosis of the tibia is problematic. To achieve union, a resection of the pseudarthrosis, stabilization, and bone grafting must be performed. Simple cast immobilization does not yield union. There are various options for the resection, immobilization, and grafting. On the first surgical attempt, retrograde intramedullary nailing offers the best chance for success by transfixing the ankle and subtalar joints with abundant autogenous bone grafting. Distraction osteogenesis and vascularized free fibular graft are reserved as salvage procedures. Gilbert A, Brockman R: Congenital pseudarthrosis of the tibia: Long-term follow-up of 29 cases treated by microvascular bone transfer. Clin Orthop 1995;314:37-44. Boero S, Catagni M, Donzelli O, Facchini R, Frediani PV: Congenital pseudarthrosis of the tibia associated with neurofibromatosis - 1: Treatment with Ilizarov's device. J Pediatr Orthop 1997;17:675-684.
Question 24High Yield
Figures 23a and 23b show the MRI scans of a 50-year-old woman who has increasing gait disturbance. She reports three falls in the past week. Examination reveals hyperreflexia, motor weakness in the biceps and triceps, and a positive Hoffman's sign. What is the most appropriate treatment plan?
Explanation
Explanation
23b The patient has obvious signs of progressive myelopathy. Based on her significant physical examination findings, nonsurgical management will not significantly impact her outcome. Cervical decompression alone is contraindicated in patients with cervical kyphosis such as seen here. Anterior cervical fusion is the best option. Emery SE, Bohlman HH, Bolesta MJ, et al: Anterior cervical decompression and arthrodesis for the treatment of cervical spondylotic myelopathy: Two to seventeen-year follow-up. J Bone Joint Surg Am 1998;80:941-951. Ferguson RJ, Caplan LR: Cervical spondylotic myelopathy. Neurol Clin 1985;3:373-382.
Question 25High Yield
The pathophysiology of a claw toe deformity includes muscular imbalance caused by which of the following relatively strong structures?
Explanation
The dynamic forces acting to maintain the position of the proximal phalanx at the head of the metatarsal are a balance between the extensor digitorum longus and the weaker intrinsic muscles. With hyperextension at the metatarsophalangeal joint, the intrinsic muscles become less efficient as plantar flexors. Consequently, the hyperextension deformity progresses in the metatarsophalangeal joint as the opposition of the intrinsic muscles to the extensor tendon lessens. This is in contrast to the situation in the interphalangeal joints, where the stronger flexors overpower the weaker intrinsic muscles, which act as the extensors. This combination of events leads to hyperextension at the metatarsophalangeal joint and flexion deformities at the interphalangeal joints, resulting in claw toe. Mizel MS, Yodlowski ML: Disorders of the lesser metatarsophalangeal Joints. J Am Acad Orthop Surg 1995;3:166-173.
Question 26High Yield
What is the reported failure rate for surgical treatment of a Morton's neuroma?
Explanation
Explanation
The reported failure rate is in the range of 15%, which may be the result of incorrect diagnosis, improper web space selection, or formation of a stump neuroma. Therefore, the procedure should be approached with caution, measures should be taken to ensure that the diagnosis is accurate, and nonsurgical options should be exhausted. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111. Beskin JL: Nerve entrapment syndromes of the foot and ankle. J Am Acad Orthop Surg 1997;5:261-269.
References:
- Mann RA, Reynolds JC: Interdigital neuroma: A critical clinical analysis. Foot Ankle 1983;3:238-243.
Question 27High Yield
Which of the following lesions is best suited for autologous chondrocyte implantation?
Explanation
Explanation
Articular chondrocyte implantation is best performed for focal chondral defects of one area of the joint. It is not indicated for osteoarthritis. Mandelbaum BR, Brown JE, Fu F, et al: Articular cartilage lesions of the knee. Am J Sports Med 1998;26:853-861. Minas T, Nehrer S: Current concepts in the treatment of articular cartilage defects. Orthopedics 1997;20:525-538.
References:
- Brittberg M, Lindahl A, Nilsson A, Ohlsson C, Isaksson O, Peterson L: Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med 1994;331:889-895.
Question 28High Yield
What is the most accurate description of the relationship between gender and knee loading during landing while playing basketball?
Explanation
Explanation
Ford and associates studied 81 high school basketball players and found that females landed with greater total valgus knee loading and a greater maximum valgus knee angle than male athletes. Hewett and associates reported in a study of 205 female athletes that those with increased dynamic valgus and high abduction loads were at increased risk of anterior cruciate ligament injury. Hewett TE, Myer GD, Ford KR, et al: Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am J Sports Med 2005;33:492-501.
References:
- Ford KR, Meyer GD, Hewett TE: Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exer 2003;35:1745-1750.
Question 29High Yield
A 65-year-old woman with a history of diabetes mellitus and plantar ulcers has an erythematous and swollen right foot and ankle. Despite IV antibiotics, the erythema spreads to her lower calf within 24 hours. She has a systolic blood pressure of 80/55 mm Hg and a pulse rate of 120. Laboratory studies show a creatinine level of 1.5 mg. Initial management should consist of
Explanation
Necrotizing fasciitis is an aggressive and rapidly spreading soft-tissue infection, usually caused by group A beta-hemolytic Streptococcus pyogenes. Presentation is typical of a rapidly ascending cellulitis, recalcitrant to antibiotic treatment. Differentiation between cellulitis and impetigo is difficult, and success depends on a high level of suspicion. The skin and subcutaneous tissues are affected, with sparing of the muscles. Septic shock and multi-organ system failure can be fatal. Treatment is aggressive surgical debridement with broad-spectrum antibiotics. Repeat irrigation and debridement may be necessary. Hyperbaric oxygen studies have shown inconsistent results. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 199-205.
Question 30High Yield
An MRI arthrogram of the elbow is shown in Figure 6. Based on these findings, what is the most likely diagnosis?
Explanation
Explanation
MRI arthrography is the imaging study of choice for evaluation of medial collateral ligament injuries. Carrino JA, Morrison WB, Zou KH, et al: Noncontrast MR imaging and MR arthrography of the ulnar collateral ligament of the elbow: Prospective evaluation of two-dimensional pulse sequences for detection of complete tears. Skeletal Radiol 2001;30:625-632.
References:
- Munshi M, Pretterklieber ML, Chung CB, et al: Anterior bundle of ulnar collateral ligament: Evaluation of anatomic relationships by using MR imaging, MR arthrography, and gross anatomic and histologic analysis. Radiology 2004;231:797-803.
Question 31High Yield
What is the most anatomic location for placement of the femoral tunnel in anterior cruciate ligament reconstruction?
Explanation
It is critical for graft isometry and knee stability that the femoral tunnel be placed as far posterior as possible on the lateral femoral condyle. Superiorly, the graft should be at the one o'clock position on the left knee. Resident's ridge is a false posterior shelf that often seems like the extreme posterior cortex. Abnormal tunnel placement results in a variety of complications, including an unstable knee, early graft failure, and joint stiffness. Johnson RJ, Beynnon BD, Nichols CE, Renstrom PA: The treatment of injuries of the anterior cruciate ligament. J Bone Joint Surg Am 1992;74:140-151.
Question 32High Yield
What is the most common clinically significant preventable complication secondary to the treatment of a displaced talar neck fracture?
Explanation
Explanation
The most important consequence of a displaced talar neck fracture after closed or open treatment is malunion. Because displacement of the talar neck is associated with displacement of the subtalar joint, any malunion leads to intra-articular incongruity or malalignment of the subtalar joint. Varus malunion is common when there is comminution of the medial talar neck. This results in pain, osteoarthritis, and hindfoot deformity that requires further treatment. Because of these complications, it is imperative that all displaced talar neck fractures are reduced anatomically; fragmented fractures may require bone grafting to maintain the length and rotation of the neck. Tile M: Fractures of the talus, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1996, pp 563-588. Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its effect on the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567.
References:
- Raaymakers EL: Complications of talar fractures, in Tscherne H, Schatzker J (eds): Major Fractures of the Pilon, the Talus, and Calcaneus: Current Concepts of Treatment. Berlin, Springer-Verlag, 1993, pp 137-142.
Question 33High Yield
A 28-year-old man who sustained an ankle fracture in a motor vehicle accident underwent open reduction and internal fixation 3 months ago. He continues to report significant ankle pain with ambulation. Radiographs are shown in Figure 26. What is the next most appropriate step in management?
Explanation
The patient sustained a bimalleolar ankle fracture with a syndesmosis disruption. The initial open reduction and internal fixation did not successfully reduce the distal tibiofibular joint. The patient may need a derotational distraction osteotomy of the fibula to reduce the syndesmosis. The other procedures do not address the primary problem of the fibular malunion and syndesmosis malreduction. There is no radiographic evidence of significant arthritis; therefore, ankle arthrodesis is not indicated.
Question 34High Yield
A 50-year-old man with metastatic renal cell carcinoma has right hip pain. A radiograph and CT scan are shown in Figures 48a and 48b. The first step in management should consist of

Explanation
These lesions are extremely vascular and can cause uncontrolled intraoperative bleeding; therefore embolization is the appropriate first treatment. Because the radiograph and CT scan show a lytic lesion in the supra-acetabular region that affects the weight-bearing dome and medial wall, the next step in treatment would most likely be a total hip arthroplasty and acetabular reconstruction. Treatment with bisphosphonates and radiation therapy will not prevent an acetabular fracture. Cementoplasty is an emerging technique in which cement is injected percutaneously into a lesion, but no long-term results have been reported. Radiofrequency ablation of bone metastases is also an emerging technique that provides palliative pain control. Layalle I, Flandroy P, Trotteur G, Dondelinger RF: Arterial embolization of bone metastases: Is it worthwhile? J Belge Radiol 1998;81:223-225.
Question 35High Yield
A 25-year-old tennis player has shoulder pain and weakness to external rotation. MRI scans are shown in Figures 16a and 16b. What is the most likely cause of his weakness?

Explanation
The MRI scans show a paralabral cyst, which is most commonly associated with labral tears. Compression of the suprascapular nerve results in weakness of the supraspinatus and/or infraspinatus depending on the level of compression. Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Question 36High Yield
A 7-year-old girl has had a painful forearm for the past 2 months. Examination reveals fullness on the volar aspect of the forearm. Radiographs and an MRI scan are shown in Figures 42a through 42c. Biopsy specimens are shown in Figures 42d and 42e. What is the most likely diagnosis?




Explanation
The radiographs reveal phleboliths on the volar side of the forearm consistent with hemangioma. The MRI scan reveals a rather well-circumscribed in size, irregular in shape, intramuscular soft-tissue mass in the volar aspect of the distal right forearm within the flexor group musculature. The mass demonstrates heterogeneous mixed signal intensity in both T1- and T2-weighted sequences with increased signal intensity on the T1, suggesting fat within the tumor, typical of hemangioma. The postgadolinium-enhanced sequences demonstrate heterogeneous enhancement. The MRI findings are consistent with a soft-tissue hemangioma. Garzon M: Hemangiomas: Update on classification, clinical presentation and associate anomalies. Cutis 2000;66:325-328.
Question 37High Yield
Figures 4a through 4c show the radiographs, CT scans, and T1-weighted MRI scan of a 19-year old man who has had increasing right hip pain and decreasing range of motion for the past several years. He also reports intermittent "locking" of the hip. What is the most likely diagnosis?
Explanation
Explanation
4b 4c The radiographs reveal small ossified masses around the femoral neck. The CT scans also show these masses and suggest that they are separate from the underlying cortex of the femoral neck, although they abut it. The MRI scan does not reveal significant marrow changes in the proximal femur apart from some mild reactive changes immediately adjacent to the nodules. These findings suggest a synovial or joint-based disorder as opposed to a primary bone tumor. The most likely diagnosis is synovial osteochondromatosis, which is consistent with the patient's mechanical symptoms. Crotty JM, Monu JU, Pope TL Jr: Synovial osteochondromatosis. Radiol Clin North Am 1996;34:327-342.
References:
- Frassica F: Orthopaedic pathology, in Miller M (ed): Review of Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1996, pp 292-335.
Question 38High Yield
A type 2A hangman's fracture, which has the potential to overdistract with traction, has which of the following hallmark findings?
Explanation
Explanation
Type 2A hangman's fractures are thought to have a flexion mechanism rather than extension and axial loading. This allows them to rotate around the anterior longitudinal ligament into flexion. Anterior translation of greater than 3 mm and angulation distinguish type 2 fractures from type 1 fractures. Although there is an association between C1 ring fractures and C2 fractures, this does not factor into the classification. If a C2-3 facet dislocation exists in combination with a C2 pars fracture, it is considered a type 3 fracture. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-217.
References:
- Levine AM, Edwards CC: The management of traumatic spondylolisthesis of the axis. J Bone Joint Surg Am 1985;67:217-226.
Question 39High Yield
An axillary nerve lesion may cause weakness in the deltoid and the
Explanation
While the most prominent functional deficit from axillary nerve lesions occurs from denervation of the deltoid, denervation of the teres minor also occurs.
Question 40High Yield
A 42-year-old athletic trainer has a persistent popping sensation about the lateral ankle associated with weakness and pain following a remote injury. Deficiency in what structure directly leads to this pathology?
Explanation
Explanation
The patient has instability of the peroneal tendon. The superior peroneal retinaculum is the primary retaining structure preventing peroneal subluxation. It is a thickening of fascia that arises off the posterior margin of the distal 1 to 2 cm of the fibula and runs posteriorly to blend with the Achilles tendon sheath. The inferior peroneal retinaculum attaches to the peroneal tubercle of the calcaneus and is not involved in this pathology. A deficient groove in the posterior distal fibula may also be a contributing factor in the development of the condition.
References:
- Maffuli N, Ferran NA, Oliva F, et al: Recurrent subluxation of the peroneal tendons. Am J Sports Med 2006;34:986-992.
Question 41High Yield
An extended head hemiarthroplasty (rotator cuff tear arthropathy head) has what theoretic advantage when compared to a standard hemiarthroplasty?
Explanation
Explanation
The theoretic advantage of a metal-to-bone articulation with the acromion is that there is a greater arc in which a smooth metal surface contacts the glenoid and acromion. This may improve pain and function, but no studies have evaluated this to date. One study showed results comparable to that of a standard hemiarthroplasty. There are no other biomechanic advantages. Visotsky JL, Basamania C, Seebauer L, et al: Cuff tear arthropathy: Pathogenesis, classification, and algorithm for treatment. J Bone Joint Surg Am 2004;86:35-40.
References:
- Zuckerman JD, Scott AJ, Gallagher MA: Hemiarthroplasty for cuff tear arthropathy. J Shoulder Elbow Surg 2000;9:169-172.
Question 42High Yield
A 13-year-old girl sustained an isolated midshaft left femoral fracture in a motor vehicle accident. The fracture was treated with a rigid, antegrade intramedullary nail placed through the piriformis fossa. The fracture healed uneventfully, as shown in Figure 46a; however, at 12 months postoperatively she now reports left hip pain. A current AP radiograph and MRI scan are shown in Figures 46b and 46c. What complication occurred in this patient?
Explanation
Explanation
46b 46c The development of femoral head ischemic necrosis is the iatrogenically created complication in this skeletally immature patient. Placement of a rigid, antegrade intramedullary nail through the piriformis fossa is likely to damage the vascular supply to the femoral head as the vessels ascend the femoral neck on the way to the femoral head. The MRI scan reveals ischemic necrosis with early collapse of the femoral head. The joint space is preserved on the MRI scan, ruling out chondrolysis. Letts M, Jarvis J, Lawton L, et al: Complications of rigid intramedullary rodding of femoral shaft fractures in children. J Trauma 2002;52:504-516. Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop Relat Res 1997;338:60-73.
Question 43High Yield
What inflammatory mediator has been most closely associated with the magnitude of the systemic inflammatory response to trauma and with the development of multiple organ dysfunction syndrome (MODS)?
Explanation
Explanation
Multiple cytokines (inflammatory mediators) are released following trauma, and their levels can be measured in serum. Persistent elevated levels of IL-6 (> 800 pg/mL) indicate an exaggerated systemic inflammatory response to trauma and have been associated with the development of MODS. Recent work has shown that extensive surgical procedures should be avoided when IL-6 levels remain elevated to prevent the precipitation of MODS. In the future, it is likely that this mediator and possibly others will be used to determine timing and techniques of future treatment. Patrick DA, Moore FA, Moore EE, et al: Jack A. Barney Resident Research Award winner: The inflammatory profile of interleukin-6, interleukin-8, and soluble intercellular adhesion molecule-1 in postinjury multiple organ failure. Am J Surg 1996;172:425-429. Pape HC, van Griesven M, Rice J, et al: Major secondary surgery in blunt trauma patients and perioperative cytokine liberation: Determination of the clinical relevance of biochemical markers. J Trauma 2001;50:989-1000.
References:
- Giannoudis PV: When is the safest time to undertake secondary definitive fracture stabilization procedures in multiply injured patients who were initially managed using a strategy of primary temporary skeletal fixation. J Trauma 2002;52:811-812.
Question 44High Yield
A 1-year-old infant has the hand deformities shown in Figure 40. What pathologic process is the most likely cause of these deformities?
Explanation
Streeter's dysplasia is clearly related to rupture of the amnion in utero and is now most commonly referred to as premature amnion rupture sequence. The deformities arise from amniotic bands that wrap about protruding parts and from uterine packing because of the accompanying oligohydramnios. Clubfoot can develop as a result of the latter mechanism. Three limb involvement is most commonly seen, along with syndactyly. Treatment involves resection of bands and Z-plasty of skin. The disease is not genetic and has not been related to teratogen exposure or to iatrogenic influences such as amniocentesis. Developmental field disruption is not seen in this disease, and the growth potential of the involved parts is normal unless neurovascular disruption has arisen from band formation.
Question 45High Yield
A 26-year-old right hand-dominant man has had right shoulder pain for the past 6 months. History reveals that he was the starting pitcher for his high school team. Activity modification, physical therapy, cortisone injection, and anti-inflammatory drugs have failed to improve his symptoms. He has a positive O'Brien's active compression test. What is the next most appropriate step in the diagnosis of this patient?
Explanation
Explanation
MRI-arthrography has been shown to be an accurate technique for assessing the glenoid labrum in patients with suspected labral tears. Often standard MRI technique will not identify labral lesions. The use of MRI-arthrography with an intra-articular injection of gadolinium provides improved visualization of labral lesions. Bencardino and associates demonstrated a sensitivity of 89%, a specificity of 91%, and an accuracy of 90% in detecting labral lesions. SLAP lesions can be visualized on coronal oblique sequences as a deep cleft between the superior labrum and the glenoid that extends well around and below the biceps anchor. Often, contrast will diffuse into the labral fragment, causing it to appear ragged or indistinct. Applegate GR, Hewitt M, Snyder SJ, et al: Chronic labral tears: Value of magnetic resonance arthrography in evaluating the glenoid labrum and labral-bicipital complex. Arthroscopy 2004;20:959-963. Bencardino JT, Beltran J, Rosenberg ZS, et al: Superior labrum anterior-posterior lesions: Diagnosis with MR arthrography of the shoulder. Radiology 2000;214:267-271.
References:
- Nam EK, Snyder SJ: The diagnosis and treatment of superior labrum, anterior and posterior (SLAP) lesions. Am J Sports Med 2003;31:798-810.
Question 46High Yield
An elite skier training for the Olympics sustains an isolated traumatic dislocation of the peroneal tendons that have spontaneously reduced. The games are 9 months away and the athlete does not want to miss them. Treatment should consist of
Explanation
Explanation
Most of these injuries occur in young, active patients. Success rates for nonsurgical management are only marginally better than 50%. The treatment of choice is early surgery for patients who desire a quick return to a sport or active lifestyle. Subluxation of the peroneal tendons leads to longitudinal tears over time. McLennan JG: Treatment of acute and chronic luxations of the peroneal tendons. Am J Sports Med 1980;8:432-436.
References:
- Krause JO, Brodsky JW: Peroneus brevis tendon tears: Pathophysiology, surgical reconstruction, and clinical results. Foot Ankle Int 1998;19:271-279.
Question 47High Yield
A 40-year-old right-handed professional football player reports persistent right wrist pain after falling during a game 5 days ago. A radiograph is shown in Figure 21. Management should consist of
Explanation
Explanation
The radiograph reveals an increased distance between the scaphoid and the lunate, which is indicative of scapholunate disassociation. A ring sign is also present, which represents the distal pole of the scaphoid viewed end on in a palmarly flexed position. In the acute setting, the scapholunate can be repaired. Open repair and percutaneous pinning is the treatment of choice. Dorsal capsulodesis is performed in the chronic setting if such an injury is initially missed. Cohen MS: Ligamentous injuries of the wrist in the athlete. Clin Sports Med 1998;17:533-552.
References:
- Taleisnik J: Carpal instability. J Bone Joint Surg Am 1988;70:1262-1268.
Question 48High Yield
Compared to eumenorrheic athletes, amenorrheic athletes have more frequent occurrences of
Explanation
Explanation
In secondary amenorrhea, women do not receive the estrogen needed to maintain adequate bone mineralization. This hypoestrogenic state affects bone density, and there is evidence that stress fractures are more frequent in amenorrheic than eumenorrheic athletes. The other conditions are not seen with increased frequency in amenorrheic athletes. Warren MP: Health issues for women athletes: Exercise-induced amenorrhea. J Clin Endocrinol Metab 1999;84:1892-1896.
References:
- Rencken ML, Chesnut CH III, Drinkwater BL: Bone density at multiple skeletal sites in amenorrheic athletes. JAMA 1996;276:238-240.
Question 49High Yield
In a retroperitoneal approach to the lumbar spine, what structure runs along the medial aspect of the psoas and along the lateral border of the spine?
Explanation
Explanation
The sympathetic trunk runs longitudinally along the medial border of the psoas. The ilioinguinal nerve emerges along the upper lateral border of the psoas and travels to the quadratus lumborium, and the genitofemoral nerve lies more laterally on the psoas. The ureter is adherent to the posterior peritoneum and falls away from the psoas and the spine in the dissection, as does the aorta. Watkins RG (ed): Surgical Approaches to the Spine. New York, NY, Springer-Verlag, 1983, p 107.
References:
- Johnson R, Murphy M, Sourthwick W: Surgical approaches to the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1559.
Question 50High Yield
Steroids are thought to prevent neurologic deterioration after traumatic spinal cord injury by which of the following mechanisms?
Explanation
Explanation
The proposed mechanisms by which steroids such as methylprednisolone are thought to prevent neurologic deterioration by limiting secondary insult, include: decreasing the area of ischemia in the cord, reducing TNF-alpha expression and NF-kB binding activity, decreasing free radical oxidation and thus stabilizing cell and lysosomal membranes, and checking the influx of calcium into the injured cells, thus reducing cord edema. Slucky AV: Pathomechanics of spinal cord injury. Spine: State Art Rev 1999;13:409-417.
Question 51High Yield
A 47-year-old woman has had a 1-month history of left hip and medial thigh pain that is exacerbated by sitting. Laboratory studies show a total protein level of 8.2 g/dL (normal 6.0 to 8.0) and an immunoglobulin G (IGG) level of 2,130 mg/dL (normal 562 to 1,835). A radiograph, CT scan, and biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
Explanation
38b 38c The laboratory studies and histology are both consistent with myeloma. Infection should show white blood cells other than plasma cells on histology. Lymphoma would show lymphocytes, not plasma cells. The lack of bone formation on the imaging studies and the lack of osteoid on histology rule out osteosarcoma. The cells have too much cytoplasm and nuclear chromatin to be Ewing's sarcoma cells.
References:
- Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989, vol 2, ch 16.
Question 52High Yield
Figure 24 shows the radiograph of a 47-year-old woman who has severe right hip pain and a limp. Management should consist of
Explanation
Femoral shortening osteotomy for a Crowe type IV hip dislocation has been shown to provide superior results with minimal complications. Cementless fixation of the stem allows for modular implants that greatly simplify the reconstruction.
Question 53High Yield
Figure 18a shows the initial lateral radiograph of a 6-year-old girl who sustained a fracture in a motor vehicle accident and was treated in a cast 1 year ago. She now has the valgus deformity seen in Figure 18b. Treatment should consist of

Explanation
Proximal tibial metaphyseal fractures may result in late genu valgum as a result of asymmetric growth of the proximal tibia. These patients are best treated with observation because the deformity is likely to remodel. Osteotomy is not indicated and potentially will lead to recurrence. Stapling of the medial tibial physis is appropriate in patients who have a severe and progressive deformity. Cozen L: Knock-knee deformity in children: Congenital and acquired. Clin Orthop 1990;258:191-203. Jackson DW, Cozen L: Genu valgum as a complication of proximal tibial metaphyseal fractures in children. J Bone Joint Surg Am 1971;53:1571-1578. Brammar TJ, Rooker GD: Remodeling of valgus deformity secondary to proximal metaphyseal fracture of the tibia. Injury 1998;29:558-560. Ogden JA, Ogden DA, Pugh L, et al: Tibia valga after proximal metaphyseal fractures in childhood: A normal biologic response. J Pediatr Orthop 1995;15:489-494.
Question 54High Yield
A 45-year-old woman has had right wrist pain for the past 2 months. A radiograph, bone scan, and MRI scan are shown in Figures 66a through 66c, and a photomicrograph is shown in Figure 66d. What is the most likely diagnosis?
Explanation
Explanation
66b 66c 66d The radiograph shows a purely radiolucent lesion without matrix mineralization in the epiphysis of the distal radius. The lesion is "hot" on bone scan, and the MRI scan reveals cortical destruction with a soft-tissue mass. These findings are most consistent with giant cell tumor. The distal radius is a common location for giant cell tumors. The other options would be very uncommon in this location in a 45-year-old patient. The photomicrograph demonstrates multinucleated giant cells in a sea of mononuclear cells. The nuclei of the giant cells and the nuclei of the mononuclear stromal cells are identical. This feature helps distinguish giant cell tumor from other lesions that might contain giant cells. Cheng CY, Shih HN, Hsu KY, et al: Treatment of giant cell tumor of the distal radius. Clin Orthop Relat Res 2001;383:221-228.
References:
- Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 263-284.
Question 55High Yield
An otherwise healthy 45-year-old woman reports the onset of severe right leg pain. Figure 20a shows an axial MRI scan of the L4-5 level, and Figure 20b shows a sagittal view with the arrow at the L4-5 level. What nerve root is the most likely source of her pain?
Explanation
Explanation
20b The scans show a disk herniation in the far lateral region of the disk. In particular, the sagittal view shows the herniation adjacent to the exiting L4 nerve root. Disk herniations in this area that cause symptoms are more likely to compress the nerve exiting at the same level rather than the next most caudal level. McCulloch JA: Microdiscectomy, in Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, vol 2, pp 1765-1783.
References:
- Hodges SD, Humphreys SC, Eck JC, Covington LA: The surgical treatment of far lateral L3-L4 and L4-L5 disc herniations: A modified technique and outcomes analysis of 25 patients. Spine 1999;24:1243-1246.
Question 56High Yield
The dorsal (Thompson) approach to the proximal forearm uses which of the following intermuscular intervals?
Explanation
The Thompson posterior approach is used in treatment of fractures of the proximal radius. Dissection is carried out through the interval between the extensor carpi radialis brevis (radial nerve) and the extensor digitorum communis (posterior interosseous nerve). To identify this interval, the forearm is pronated and the mobile lateral wad of muscles (the ulnar-most belly is the extensor carpi radialis brevis) is grasped with the thumb and finger and pulled from the much less mobile mass of the extensor digitorum communis. The furrow created is marked with a skin marker for subsequent skin incision. The skin incision follows a line from the lateral epicondyle of the humerus to a point corresponding to the middle of the posterior aspect of the wrist. Distally, the intermuscular plane is between the extensor carpi radialis brevis and the extensor pollicis longus. Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 128-129. Hoppenfeld S, deBoer P: Posterior approach to the radius, in Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 136-146.
Question 57High Yield
A 38-year-old man has an enlarging left paraspinal soft-tissue mass. Based on the MRI scans and biopsy specimens shown in Figures 32a through 32e, what is the most likely diagnosis?
Explanation
Explanation
32b 32c 32d 32e Fibromatosis is a benign but aggressive fibrous lesion that principally arises from the connective tissue of muscle and the overlying fascia. The peak incidence is between the ages of 25 and 35 years. Most patients have a deep-seated, firm, poorly circumscribed mass that has grown insidiously and causes little or no pain. MRI is helpful in diagnosing the lesion and in assessing the extent of disease prior to surgical intervention. Histologically, the lesion is poorly circumscribed and infiltrates the surrounding tissue. The lesion appears bland with uniform spindle cells separated by abundant collagen, with little or no cell-to-cell contact. Despite its bland microscopic appearance, the tumor frequently behaves in an aggressive manner. These lesions do not metastasize but have a high incidence of recurrence. Treatment options consist of surgical resection, radiation therapy, chemotherapeutic protocols, hormone modulation, and/or anti-inflammatory medications. Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss's Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 309-337.
References:
- Spear MA, Jennings LC, Mankin HJ, et al: Individualizing management of aggressive fibromatoses. Int J Radiat Oncol Biol Phys 1998;40:637-645.
Question 58High Yield
A 22-year-old competitive volleyball player has shoulder pain, and rest and a cortisone injection have failed to provide relief. Examination reveals atrophy along the posterior scapula, but an MRI scan does not reveal a rotator cuff tear or labral cyst. What is the most likely cause for the shoulder weakness?
Explanation
Explanation
Repetitive overhead slams and serves may produce a traction injury to the distal branch of the suprascapular nerve. Bankart, biceps, and superior labrum anterior and posterior injuries can occur but usually do not produce visible atrophy. Muscle avulsion is uncommon. Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
References:
- Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthroscopy 1990;6:301-305.
Question 59High Yield
The insurance carrier of a patient who underwent total knee arthroplasty 4 days ago is now demanding that the patient be discharged from the hospital. However, examination reveals that the patient has a range of motion of only 10 degrees to 55 degrees, and the patient is concerned whether she will ever move her knee normally. The insurance company representative should be advised that
Explanation
Explanation
Examination findings that show flexion of only 55 degrees at discharge should alert the surgeon that the patient will require close scrutiny and follow-up. Mauerhan and associates examined the records of 745 patients who had a primary total knee arthroplasty from 1993 to 1996. At their institution, development and implementation of clinical pathways resulted in a significant decrease in the average length of stay, beginning in 1993 with 6.4 days +/- 1.8 days and progressively decreasing to 4.4 days +/- 1.0 days in 1996. The rate of manipulation (patients manipulated at 6 weeks/total number of patients receiving total knee arthroplasty) was 6.0% in 1993, 11.3% in 1994, 13.5% in 1995, and 12.0% in 1996. In the period of 1993 to 1996, patients requiring manipulation consistently had a lower range of motion of 69.0 degrees +/- 10 degrees at the time of discharge compared with patients not requiring manipulation who had a range of motion of 80.7 degrees +/- 10.6 degrees. In this era of outpatient services, however, another solution would be to arrange for outpatient physical therapy on a more frequent basis and to see the patient more frequently in the office until an acceptable range of motion is established.
References:
- Mauerhan DR, Mokris JG, Ly A, Kiebzak GM: Relationship between length of stay and manipulation rate after total knee arthroplasty. J Arthroplasty 1998;13:896-900.
Question 60High Yield
Following a chevron bunionectomy performed through a dorsal approach, a patient has persistent numbness on the dorsal and medial aspect of the hallux. What nerve has most likely been injured?
Explanation
Explanation
The dorsomedial cutaneous nerve of the hallux, which is a distal branch of the superficial peroneal nerve, supplies sensation to the skin on the dorsal and medial half of the hallux and may be injured during a chevron bunionectomy. Injury to the nerve leads to particularly painful neuromas that directly impinge on the shoe. For this reason, direct medial approaches are typically preferred for access to the medial aspect of the metatarsophalangeal joint.
References:
- Miller SD: Dorsomedial cutaneous nerve syndrome: Treatment with nerve transection and burial into bone. Foot Ankle Int 2001;22:198-202.
Question 61High Yield
A 36-year-old woman is brought to the emergency department intubated and sedated following a motor vehicle accident. She is moving her upper and lower extremities spontaneously. She cannot follow commands. CT scans are shown in Figures 7a through 7c. The initial survey does not reveal any other injuries. Initial management of the cervical injury should consist of immediate
Explanation
Explanation
7b 7c The patient has a bilateral facet dislocation of C6-C7 with preservation of at least some neurologic function. Urgent reduction is necessary. However, because she is sedated and unable to follow commands, an MRI scan is necessary before any closed or open posterior reduction to look for an associated disk herniation. If a disk herniation is present, it must be removed prior to any reduction maneuver to prevent iatrogenic neurologic injury. It is very unlikely that this injury can be reduced with an open anterior procedure alone. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 189-199.
Question 62High Yield
Figures 28a and 28b show the sagittal and axial lumbar MRI scans of a 72-year-old man who reports dull aching back pain that spreads to his legs, calves, and buttocks. He has had the pain for several years and it is precipitated by standing and walking and relieved by sitting. His symptoms have been worsening over the past year and he notes that he is leaning forward while walking to help relieve his symptoms. He has had no treatment to date. What is his prognosis if he chooses to pursue nonsurgical management for this condition?

Explanation
The patient has lumbar spinal stenosis and the MRI scans reveal the pathology at L4-5, which is secondary to posterior disk bulging and hypertrophy and infolding of the ligamentum flavum, as well as degenerative facet arthrosis. The degree of spinal stenosis is moderate and his symptoms are positional in nature. Tadokoro and associates reported on a prospective study of 89 patients older than 70 years of age who underwent nonsurgical management for lumbar spinal stenosis. They found the prognosis to be relatively good with patients scoring at "excellent" or "good" for activities of daily living at final follow-up. However, they did note that patients with a complete block on myelography did not respond favorably to nonsurgical management. Amundsen and associates reported on a 10-year prospective study comparing surgical care to nonsurgical management. They concluded that, while the long-term results largely favored surgical treatment, more than half of the nonsurgically managed patients had a satisfactory outcome. They also concluded that a delay of surgery for some months did not worsen the prognosis. Therefore, their recommendation was for an initial primarily nonsurgical approach. Amundsen T, Weber H, Nordal HJ, et al: Lumbar spinal stenosis: Conservative or surgical management? A prospective 10-year study. Spine 2000;25:1424-1435. Hilibrand AS, Rand N: Degenerative lumbar stenosis: Diagnosis and management. J Am Acad Orthop Surg 1999;7:239-249.
Question 63High Yield
Which of the following activities can improve posterior capsular contractures?
Explanation
Posterior capsule stretching is performed in the cross-chest and behind the back positions. Stretching in internal rotation in the abducted shoulder will further stretch the posterior capsule. Wide grip stretch, and anterior capsule and strengthening exercises will not necessarily stretch the capsule. Ellenbacher TS: Shoulder internal and external rotation strength and range of motion of highly-skilled junior tennis players. Isokinetic Exercise Sci 1992;2:1-8.
Question 64High Yield
A 20-year-old male lacrosse player sustains an anterior dislocation of the shoulder. He is extremely concerned about recurrent dislocations. Which of the following treatments has been shown to reduce the risk of recurrent dislocation?
Explanation
Recent evidence has shown that the position of immobilization of the shoulder after a dislocation influences the reduction of the Bankart lesion. In an MRI study in patients who sustained an anterior dislocation, the Bankart lesion was reduced to the glenoid anatomically with the arm in 30 degrees of external rotation. Subsequently, a clinical follow-up study has shown a reduction in recurrence rates when the arm is immobilized in external rotation compared to internal rotation. Itoi E, Hatakeyama Y, Kido T, et al: A new method of immobilization after traumatic anterior dislocation of the shoulder: A preliminary study. J Shoulder Elbow Surg 2003;12:413-415.
Question 65High Yield
A 36-year-old woman was injured in a train derailment. She has a significant open depressed skull fracture with active bleeding, a hemopneumothorax, and blood in the left upper quadrant and colic gutter by Focused Assessment with Sonography for Trauma (FAST) examination. Additionally, she has the pelvic injury seen on the CT scans in Figures 18a and 18b. The mortality rate for this patient approaches

Explanation
Mortality following trauma that requires surgical intervention for head, chest, and abdominal injury exceeds 90%. The type of pelvic fracture is a predictor of associated injury, blood requirements, and overall mortality. AP III pelvic fractures require the most blood, and are associated with significant abdominal trauma and shock. Lateral compression pelvic fractures are more associated with head, chest, and occasionally abdominal trauma, and mortality often occurs from associated injuries. Dalal SA, Burgess AR, Siegel JH, et al: Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resuscitative requirements and outcome. J Trauma 1989;29:981-1000. Eastridge BJ, Burgess AR: Pedestrian pelvic fractures: 5-year experience of a major urban trauma center. J Trauma 1997;42:695-700.
Question 66High Yield
The arrow in Figure 39 is pointing to which of the following ligaments?
Explanation
The lunotriquetral interosseous ligament stabilizes the lunotriquetral joint. The scapholunate interosseous ligament stabilizes the scapholunate joint. The ulnolunate ligament originates from the base of the ulnar styloid and inserts in the lunate. The ulnotriquetral ligament originates from the base of the ulnar styloid and inserts on the triquetrum. The ulnolunate and the ulnotriquetral ligaments are important stabilizers to the ulnar side of the wrist. The short radiolunate ligament originates on the volar ulnar margin of the distal radius and inserts in the ulnar margin of the lunate. Berger RA: Ligament anatomy, in Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist, Diagnosis and Operative Management. St Louis, MO, Mosby, 1998, pp 73-105.
Question 67High Yield
With a full-thickness articular cartilage injury, the body's healing response produces cartilage mainly composed of what type of collagen?
Explanation
With a full-thickness articular cartilage injury, a healing response is initiated with hematoma, stem cell migration, and vascular ingrowth. This response produces type I collagen and resultant fibrous cartilage rather than desired hyaline cartilage as produced by chondrocytes. This repair cartilage has diminished resiliency, stiffness, poor wear characteristics, and the predilection for arthritis. Type I collagen is also found in the annulus of intervertebral disks, tendon, bone, meniscus, and skin. Type II is found in articular cartilage and nucleus pulposus of intervertebral disks. Type III is found in skin and blood vessels, type IV is found in basement membranes, and type X is found in the calcified layer of cartilage. Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 19-28.
Question 68High Yield
A 28-year-old hockey player has a shoulder deformity after being checked into the boards. Examination reveals that swelling has improved, but there is tenderness along the distal clavicle. Radiographs reveal a grade II acromioclavicular joint separation. Initial management should consist of
Explanation
The most common shoulder injury in hockey players is to the acromioclavicular joint. Early rest and control of pain and inflammation is the preferred management. Surgery is reserved for patients with significant coracoclavicular disruption that has failed to respond to nonsurgical management. Cross-chest stretches and overhead exercises may increase symptoms. A cortisone injection within the glenohumeral joint will have little effect. Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Question 69High Yield
Figures 17a and 17b show the AP and lateral radiographs of a 75-year-old woman who reports giving way and shifting of the knee, particularly when she is descending stairs or ambulating on level surfaces. History reveals a total knee replacement 5 years ago. Treatment should consist of

Explanation
The radiographs show well-fixed components of a posterior cruciate-retaining total knee replacement. The relative position of the femoral component is anteriorly subluxated relative to the tibial component. The AP radiograph shows that the articular space is markedly asymmetric, indicating either failure or fracture of the polyethylene or subluxation of the femur relative to the tibia. The patient's symptoms suggest a failure of the posterior cruciate ligament that is consistent with the radiographic findings; therefore, the treatment of choice is revision to a posterior cruciate-substituting implant.
Question 70High Yield
A 40-year-old man reports an enlarging soft-tissue mass in his right shoulder. Based on the MRI scan and biopsy specimens shown in Figures 40a through 40c, what is the most likely diagnosis?


Explanation
Nodular fasciitis is a pseudosarcomatous, self-limiting reactive process composed of fibroblasts and myofibroblasts. Most patients give a history of a rapidly growing mass that has been present for only a few weeks. Many have pain associated with the mass and can recall a specific traumatic event predating the presence of the lesion. It can occur at any age but is most commonly seen in adults who are 20 to 40 years of age. Histologically, the lesion is composed of predominantly plump, immature-appearing fibroblasts that bear a close resemblance to the fibroblasts found in granulation tissue. Characteristically, the fibroblasts are arranged in short, irregular bundles and fascicles and are adjacent to collagen and reticulin. The lesions can appear to be more myxoid or more fibrotic in nature and this correlates to the duration of symptoms. The lesions with a short duration of symptoms have a more myxoid appearance in contrast to those of longer duration characterized by hyaline fibrosis. Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss's Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 250-266.
Question 71High Yield
A patient with a previously pain-free knee replacement now reports a sudden inability to ambulate. Radiographs of the knee are shown in Figures 33a and 33b. Management should consist of
Explanation
Explanation
33b The radiographs show a patellar tendon rupture following a total knee replacement. This infrequent, but serious, complication is reported to occur in 0.17% to 1.4% of patients after total knee arthroplasty. Although the radiographs show concerning features such as incomplete tibial and femoral periprosthetic lucencies, it is most important for the surgeon to recognize extensor mechanism disruption. Insall J, Salvati E: Patella position in the normal knee joint. Radiology 1971;101:101-104. Lynch AF, Rorabeck CH, Bourne RB: Extensor mechanism complications following total knee arthroplasty. J Arthroplasty 1987;2:135-140.
References:
- Rand JA, Morrey BF, Bryan RS: Patellar tendon rupture after total knee arthroplasty. Clin Orthop 1989;244:233-238.
Question 72High Yield
A 66-year-old man reports a 2-week history of worsening low back and leg pain. He reports that his pain is aggravated by lying down and relieved by standing and walking. He notes that he has been losing weight recently and that his pain has been awakening him during the night. His medical history is significant for hypertension, coronary artery disease, and prostate cancer. His physical examination is essentially unremarkable. Lumbar radiographs are within normal limits. What is the most appropriate management for this patient?
Explanation
In the initial assessment of acute low back pain in adults, no diagnostic testing is indicated during the first 4 weeks in the absence of "red flags" for a serious underlying condition. The purpose of the initial assessment of acute low back pain in adults is to rule out serious underlying conditions presenting as low back pain. The Agency for Healthcare Policy and Research, in its 1994 clinical practice guideline, identified four serious conditions that may present with low back pain, including fracture, tumor, infection, and cauda equina syndrome. This patient has five "red flags" for a spinal tumor as a possible etiology of his low back pain, including age of older than 50 years, constitutional symptoms (recent weight loss), pain worse when supine, severe nighttime pain, and a history of cancer. Of these, his history of cancer is most significant, as greater than 90% of spinal tumors are metastatic. In order of frequency, breast, prostate, lung, and kidney make up approximately 80% of all secondary spread to the spine. In the presence of "red flags" for tumor or infection, it is recommended that the clinician obtain a CBC count, ESR, and a urinalysis. If these are within normal limits and suspicions still remain, consider consultation or seek further evidence with a bone scan, radiographs, or additional laboratory studies. Negative radiographs alone are insufficient to rule out disease. If radiographs are positive, the anatomy can be better defined with MRI. Agency for Health Care Policy and Research, Bigos SJ (ed): Acute Low Back Problems in Adults. Rockville, MD, US Department of Health and Human Services, AHCPR Publication 95-0642, Clinical Practice Guideline #14, 1994.
Question 73High Yield
A 48-year-old man has recurrent right knee pain. Figure 52a shows the sagittal proton density T2-weighted MRI scan, and Figure 52b shows the sagittal T2-weighted MRI scan at the same level. The arrow is pointing to a

Explanation
Meniscal tears have many configurations and locations. The normal medial meniscus has a bow-tie configuration on the two most medial consecutive sagittal views. Toward the center of the joint the anterior and posterior horns have a triangular shape. These images show an abnormal intra-articular low-signal structure located anterior to the intact posterior cruciate ligament. This most likely represents a torn and displaced posterior horn of the medial meniscus, sometimes called "double PCL sign". A popliteal cyst and ligaments of Wrisberg and Humphry are not visible on these figures. Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Question 74High Yield
Figure 3a shows the preoperative radiograph of a 5-year-old girl who achieved complete correction with valgus osteotomies. Figure 3b shows a radiograph obtained 2 years later. What is the cause of the recurrent deformity on the right side?
Explanation
Explanation
3b Although inadequate correction, obesity, patient age of older than 5 years and an increased metaphyseal-diaphyseal angle are all associated with a poorer outcome, the radiographs show a growth arrest of the medial tibial physis. If not recognized and treated with early surgery, progressive genu varum will occur with continued growth of the lateral physis. In addition to repeat osteotomy, options for treating the arrest include physeal bar resection or, as necessary, completion of the growth arrest by epiphyseodesis of the lateral physes, followed by a limb equalization procedure at a later date. Brooks WC, Gross RH: Genu varum in children: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:326-335. Herring JA: Tachdjian's Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, pp 840-950.
References:
- Schoenecker PL, Rich MM: The lower extremity, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 1068-1073.
Question 75High Yield
Figure 33 shows the venogram of a patient who has a long history of alcohol abuse. Warfarin should be used cautiously because of the interaction with which of the following factors?
Explanation
Warfarin acts by inhibiting clotting factors II, VII, IX, X. The actual mechanism of action is by inhibition of hepatic enzymes, vitamin K epoxide, and perhaps vitamin K reductase. This inhibition results in lack of carboxylation of vitamin K-dependent proteins (II, VII, IX, X). The anticoagulant effect of warfarin can be reversed with vitamin K or fresh-frozen plasma. The use of alcohol may lead to liver dysfunction and an even more limited margin of available factors. Lieberman JR, Wollaeger J, Dorey F, et al: The efficacy of prophylaxis with low-dose warfarin for prevention of pulmonary embolism following total hip arthroplasty. J Bone Joint Surg Am 1997;79:319-325.
Question 76High Yield
A 46-year-old man has incomplete paraplegia after being involved in a motor vehicle accident. The CT scan shown in Figure 5 reveals marked canal compromise. What is the most appropriate management to improve neurologic status?
Explanation
Explanation
According to a study by the Scoliosis Research Society, the use of anterior decompression is most predictable for improving neurologic status. This is particularly true of bowel and bladder functional loss. Laminectomy is contraindicated because it further destabilizes the spine. Posterior instrumentation and indirect reduction through distraction and ligamentotaxis only incompletely decompress the compromised canal and are successful only if performed within 48 hours of injury. While some improvement may occur with closed management, the amount of recovery is less than that achieved with surgical decompression. A posterior approach and instrumentation may be added to the anterior decompression based on the characteristics of associated injuries to the posterior element. Gertzbein SD: Scoliosis Research Society multicenter spine fracture study. Spine 1992;17:528-540. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-215.
References:
- Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Question 77High Yield
When performing a total knee arthroplasty using modular components, what is the minimum recommended thickness of an ultra-high molecular weight polyethylene insert for a tibial component?
Explanation
Explanation
Polyethylene wear has been identified as a major contributor to failure of total knee implants, of which thickness is an important factor. Several studies have shown that the minimum thickness should be 6 to 8 mm. While Wright and Bartel have shown that 6 to 8 mm has been recommended as the minimum thickness of an ultra-high molecular weight polyethylene insert for a tibial component in total knee arthroplasty, more recent work by Meding and associates and Worland and associates has verified the clinical efficacy of 4 mm of polyethylene in compression-molded anatomic graduated nonmodular components. Bartel DL, Bicknell VL, Wright TM: The effect of conformity, thickness, and material on stresses in ultra-high molecular weight components for total joint replacement. J Bone Joint Surg Am 1986;68:1041-1051. Wright TM, Bartel DL: The problem of surface damage in polyethylene total knee components. Clin Orthop 1991;273:261-263. Meding JB, Ritter MA, Faris PM: Total knee arthroplasty with 4.4 mm of tibial polyethylene: 10-year followup. Clin Orthop 2001;388:112-117.
References:
- Worland RL, Johnson G, Alemparte J, Jessup DE, Kennan J, Norambuena N: Ten to fourteen year survival and functional analysis of the AGC total knee replacement system. Knee 2002;9:133-137.
Question 78High Yield
A 38-year-old man sustains a complete avulsion with retraction of the ischial attachment of the hamstring muscles in a fall while water skiing. He indicates that he is an aggressive athlete who participates regularly in multiple running and cutting-type sports, and he strongly desires to continue his athletic competition. Management should consist of
Explanation
Several studies have identified a complete proximal avulsion of the hamstring muscles as an injury that leads to significant long-term disability, with a high percentage of athletes who must permanently restrict their activities following nonsurgical management. Early surgical repair and prolonged rehabilitation have yielded consistently better results than nonsurgical management. Orava S, Kujala UM: Rupture of the ischial origin of the hamstring muscles. Am J Sports Med 1995;23:702-705.
Question 79High Yield
The vascularity of the digital flexor tendons is significantly richer in what cross-sectional region?
Explanation
The vascularity of the dorsal portion of the digital flexor tendons is considerably richer than the volar portion. The other regions are not preferentially more vascular. Hunter JM, Scheider LH, Makin EJ (eds): Tendon Surgery in the Hand. St Louis, MO, Mosby, 1987, pp 91-99.
Question 80High Yield
A 45-year-old woman with stage II posterior tibial tendinitis has failed to respond to nonsurgical management. Recommended treatment now includes posterior tibial tendon debridement and medial calcaneal displacement osteotomy along with transfer of what tendon?
Explanation
Explanation
The flexor digitorium longus is the commonly accepted tendon transfer for posterior tibial tendon insufficiency. The flexor hallucis longus has to be carefully rerouted to avoid crossing the neurovascular bundle and has not been shown clinically to provide superior results to flexor digitorum longus transfer. Use of the peroneus longus results in loss of plantar flexion strength of the first metatarsal, contributing to the flatfoot deformity. The anterior tibial tendon is in the anterior compartment and fires out of phase with the posterior tibial tendon. Sitler DF, Bell SJ: Soft tissue procedures. Foot Ankle Clin 2003;8:503-520.
References:
- Guyton GP, Jeng C, Krieger LE, et al: Flexor digitorum longus transfer and medial displacement calcaneal osteotomy for posterior tibial tendon dysfunction: A middle-term clinical follow-up. Foot Ankle Int 2001;22:627-632.
Question 81High Yield
A 2-week-old infant has had diminished movement of the right upper extremity since birth. Examination reveals weakness of shoulder abduction and external rotation, elbow flexion, and forearm supination. Both pupils are equally round and responsive to light. The remainder of the examination is normal. Radiographs of the upper limb show a healing middle-third clavicle fracture. Management should consist of
Explanation
Explanation
The patient has a classic Erb's palsy with weakness of the muscles innervated by the fifth and sixth cervical roots. Horner syndrome, a poor prognostic indicator for recovery, is absent in this infant. All infants with brachial plexus birth palsies initially should be monitored for spontaneous recovery during the first 3 to 6 months of life. During this period of observation, glenohumeral motion, especially external rotation, should be maintained. Many infants will begin to show recovery within the first 6 to 8 weeks after birth and continue on to normal function. The timing of microsurgery is controversial. A recent study found that the outcome of microsurgical repair in patients who had no recovery of biceps function within 3 months after birth was similar compared to those who had recovery of biceps function between 3 and 6 months and no microsurgical repair. The author concluded that microsurgical repair was effective in improving function in those infants who had no evidence of recovery of biceps function within the first 6 months of life. Waters PM: Comparison of the natural history, the outcome of microsurgical repair, and the outcome of operative reconstruction in brachial plexus birth palsy. J Bone Joint Surg Am 1999;81:649-659.
References:
- Greenwald AG, Schute PC, Shiveley JL: Brachial plexus birth palsy: A 10-year report on the incidence and prognosis. J Pediatr Orthop 1984;4:689-692.
Question 82High Yield
A 24-year-old man who works at a local oyster and clam farm sustained a laceration on his hand at work. Examination reveals a cellulitic index finger without evidence of tenosynovitis. After appropriate irrigation and debridement, what antibiotic is most appropriate?
Explanation
Explanation
Injuries involving brackish water and shellfish can have devastating consequences caused by Vibrio vulnificus infections. Patients may have a severe invasive infection, with three main clinical features: primary septicemia, wound infection, and gastroenteritis. Antibiotic administration is crucial because mortality rates of up to 50% have been observed with Vibrio septicemia. The current recommendation is to give a third-generation cephalosporin such as ceftazadime. Chiang SR, Chuang YC: Vibrio vulnificus infection: Clinical manifestations, pathogenesis, and antimicrobial therapy. J Microbiol Immunol Infect 2003;36:81-88.
References:
- Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 240-259.
Question 83High Yield
Figure 25 shows the clinical photograph of a 48-year-old man who has had a forefoot ulcer for the past 4 months. History reveals that he has had type II diabetes mellitus for the past 10 years. Examination reveals sensory and motor neuropathy, with weak ankle dorsiflexion. The ankle cannot be passively dorsiflexed past a neutral position. Initial management should consist of
Explanation
Explanation
Foot deformity and decreased joint motion have been associated with increased plantar pressures and an increased risk of ulceration. In a partial-thickness ulcer without exposed bone or tendon, total contact casting is highly effective. Concomitant Achilles tendon lengthening increases the likelihood that healing of the ulcer can be obtained and perhaps more importantly, maintained. Lin SS, Lee TH, Wapner KL: Plantar forefoot ulceration with equinus deformity of the ankle in diabetic patients: The effect of tendo-Achilles lengthening and total contact casting. Orthopedics 1996;19:465-475.
References:
- Armstrong DG, Stacpoole-Shea S, Nguyen H, Harkless LB: Lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot. J Bone Joint Surg Am 1999;81:535-538.
Question 84High Yield
Figures 34a and 34b show the clinical photographs of a 46-year-old woman who has a painful deformity of the second toe. Surgical treatment consisting of metatarsophalangeal capsulotomy and proximal interphalangeal joint resection arthroplasty resulted in satisfactory correction, but the toe remains unstable at the metatarsophalangeal joint. What is the next most appropriate step?

Explanation
Crossover second toes are attributed to attenuation or rupture of the plantar plate and lateral collateral ligament and are associated with varying degrees of instability. Flexor-to-extensor transfer (Girdlestone/Taylor procedure) can provide intrinsic stability to the toe. Although plantar metatarsal head condylectomy can increase stability by resulting in scarring of the plantar plate, excision of the entire second metatarsal head carries a high risk of transfer metatarsalgia. Removal of the base of the proximal phalanx destabilizes the toe and should be reserved as a salvage procedure. Simple flexor tenotomy alone will not improve stability, and arthrodesis of the second metatarsophalangeal joint will limit motion and impair function. Coughlin MJ: Crossover second toe deformity. Foot Ankle 1987;8:29-39.
Question 85High Yield
Compared with cobalt-chromium, the biomechanical properties of titanium on polyethylene articulation in total hip replacement result in
Explanation
The surface hardness of titanium is low compared with that of cobalt-chromium alloys. Titanium articulations are easily scratched, resulting in a significantly increased rate of wear and debris production. The wear and resulting lysis can also result in an increased rate of loosening. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486. Agins HJ, Alcock NW, Bansal M, et al: Metallic wear in failed titanium-alloy total hip replacements: A histological and quantitative analysis. J Bone Joint Surg Am 1988;70:347-356.
Question 86High Yield
Figure 13 shows the clinical photograph of a 66-year-old man who has had an increasingly painful right foot deformity for the past 3 years. Examination reveals that the subtalar joint is fixed in 15 degrees of valgus, and forefoot supination can be corrected to 10 degrees from neutral. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
Explanation
The most important determining factor for correction of an adult flatfoot without an arthrodesis is the flexibility of the subtalar and transverse tarsal joints. Rigid deformities cannot be corrected with a medial sliding calcaneal osteotomy with FDL transfer or a subtalar arthroereisis. Isolated subtalar or talonavicular arthrodesis does not correct the deformities entirely. If the patient has forefoot supination that can be corrected to less than 7 degrees, an isolated subtalar fusion is a possible alternative.
References:
- Mann RA: Flatfoot in adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 757-784.
Question 87High Yield
Which of the following accurately describes the biosynthetic materials tricalcium phosphate (TCP) and hydroxyapatite?
Explanation
Explanation
TCP is resorbed more rapidly, at a rate of 10 to 20 times faster than hydroxyapatite, partially because its larger pore size makes it a weaker substance. It provides significantly less compressive strength than hydroxyapatite. It does partially convert to hydroxyapatite, thus slowing its resorption rate. The absorbing cell of hydroxyapatite is the foreign body giant cell, not the osteoclast. Optimum pore size appears to be between 150 and 500 um. Lane JM, Bostrom MP: Bone grafting and new composite biosynthetic graft materials. Instr Course Lect 1998;47:525-534.
References:
- Walsh WR, Chapman-Sheath PJ, Cain S, et al: A resorbable porous ceramic composite bone graft substitute in a rabbit metaphyseal defect model. J Orthop Res 2003;21:655-661.
Question 88High Yield
Figure 21 shows the AP radiograph of a 41-year-old patient who sustained a closed bicolumnar fracture of the distal humerus that resulted in a painful nonunion. What is the best initial construct for rigid stabilization of this fracture pattern?
Explanation
The dual plate fixation construct is significantly stronger than single plate or "Y" plate fixation. Two-plate constructs at right angles, the ulnar plate medially and the lateral plate posteriorly, would appear to be biomechanically optimal. This approach usually is feasible at the time of surgery. Clinically, dual 3.5-mm reconstruction or dynamic compression plates are superior to one third tubular plate fixation. Supplementary external fixation is not considered a better treatment option. Failure of fixation and nonunion are often the result of inadequate fixation and osteoporosis. Helfet DL, Hotchkiss RN: Internal fixation of the distal humerus: A biomechanical comparison of methods. J Orthop Trauma 1990;4:260-264.
Question 89High Yield
A biopsy of the involved physis in a patient with slipped capital femoral epiphysis (SCFE) would most likely reveal
Explanation
Vascular invasion, histologically similar to granulation tissue, has been noted between the columns in the zone of hypertrophy, leading to the theory of microtrauma as an etiology. SCFE is also associated with conditions that increase the height of the zone of hypertrophy, including the adolescent growth spurt and endocrinopathies. The perichondral ring has been shown to decrease in thickness with age. Normal undulations in the growth plate also decrease during this time, possibly further destabilizing the physis. Abnormal accumulations of proteoglycan have been reported. Chung SM, Batterman SC, Brighton CT: Shear strength of the human femoral capital epiphyseal plate. J Bone Joint Surg Am 1976;58:94-103.
Question 90High Yield
A 25-year-old woman undergoes surgical treatment of a displaced proximal humeral fracture via a deltopectoral approach. At the first postoperative visit, she reports a tingling numbness along the anterolateral aspect of the forearm. What structure is most likely injured?
Explanation
Explanation
Sensation along the anterolateral aspect of the forearm is supplied by the lateral antebrachial cutaneous nerve, the terminal branch of the musculocutaneous nerve. The musculocutaneous nerve can be injured by proximal humeral fractures or dislocations, and is also at risk during surgical exposure if excessive retraction is placed on the conjoint tendon. The musculocutaneous nerve enters the conjoint tendon 1 cm to 5 cm distal to the coracoid process. McIlveen SJ, Duralde XA, D'Alessandro DF, et al: Isolated nerve injuries about the shoulder. Clin Orthop 1994;306:54-63.
References:
- Warner JP: Frozen shoulder: Diagnosis and management. J Am Acad Orthop Surg 1997;5:130-140.
Question 91High Yield
A 29-year-old man who lifts weights states that he injured his left shoulder while performing a bench press 2 days ago. The following morning he noted ecchymosis and swelling in the left chest wall. Examination reveals ecchymosis and tenderness and deformity in the left anterior chest wall and axillary fold that is accentuated with resisted adduction of the arm. Passive range of motion beyond 90 degrees of forward flexion and 45 degrees of external rotation is extremely painful. Glenohumeral stability is difficult to assess because of severe guarding. Figure 29 shows an MRI scan. Management should consist of
Explanation
Explanation
Rupture of the pectoralis major tendon most commonly occurs during bench pressing. Wolfe and associates have shown that the most inferiorly located fibers of the sternal head lengthen disproportionately during the final 30 degrees of humeral extension during the bench press. This creates a mechanical disadvantage in the final portion of the eccentric phase of the lift; with forceful flexion of the shoulder these maximally stretched fibers may rupture. In most patients, particularly in young athletes, the treatment of choice is anatomic repair of the ruptured tendon to its insertion in the proximal humerus either with suture anchors or transosseous sutures. Following surgery, most patients experience a near normal return of strength and significant improvement in the cosmetic appearance of the deformity. While more technically challenging, repair of chronic rupture is possible and is indicated in some patients. Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
References:
- Schepsis AA, Grafe MW, Jones HP, Lemos MJ: Rupture of the pectoralis major muscle: Outcome after repair of acute and chronic injuries. Am J Sports Med 2000;28:9-15.
Question 92High Yield
An otherwise healthy 78-year-old woman has low back and buttock pain. Rectal examination reveals a large sacral mass. Figures 7a and 7b show a CT scan and a sagittal MRI scan of the lumbosacral spine. A biopsy specimen is shown in Figure 7c. What is the most likely diagnosis?


Explanation
A chordoma is a malignant neoplasm originating from remnants of the notochord. It is usually localized to the midline with 50% at the sacrococcygeal area, 35% at the skull base, and 15% at the mobile portion of the spine. Large vacuolated cells (physaliferous cells) are a characteristic of the tumor. Mindell ER: Chordoma. J Bone Joint Surg Am 1981;63:501-505.
Question 93High Yield
A 55-year-old woman who underwent a left total hip arthroplasty 8 months ago using a modified Hardinger approach reports a persistent painless limp. Examination reveals that when she is not using a cane, she lurches to the left during weight bearing on the left lower extremity. An AP radiograph is shown in Figure 29. Which of the following hip muscle groups should be strengthened to improve the gait abnormality?
Explanation
Explanation
The modified Hardinger approach includes a partial anterior trochanteric osteotomy creating a trochanteric wafer (as seen on the radiograph) that is displaced anterior and medial in continuity with the gluteus medius and vastus lateralis. Failure of abductor reattachment, migration of the trochanter, nonunion of the osteotomy site, and excessive splitting of the gluteus medius muscle causing injury to the inferior branch of the superior gluteal nerve can result in weakness of the abductor mechanism. Abductor strength should be evaluated with the patient lying on the opposite side and elevating the affected limb. Although slight weakness may manifest itself as a limp only after prolonged muscular activity, significant weakness results in a constant limp without associated discomfort. Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 512-526.
References:
- Kasser JR (ed): Orthopedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 389-426.
Question 94High Yield
What is the optimum position of immobilization of the foot and ankle immediately after Achilles tendon repair to maximize skin perfusion?
Explanation
Explanation
Achilles tendon tension is not affected by knee position when the ankle is in 20 degrees to 25 degrees of plantar flexion. Skin perfusion overlying the Achilles tendon is maximal in 20 degrees of plantar flexion and is reduced beyond 20 degrees of plantar flexion. Neutral flexion or any amount of dorsiflexion compromises the repair.
References:
- Poynton AR, O'Rourke K: An analysis of skin perfusion over the Achilles tendon in varying degrees of plantar flexion. Foot Ankle Int 2001;22:572-574.
Question 95High Yield
A 32-year-old professional football player has disabling left arm pain in the C7 dermatome that has been increasing in severity for the past 2 months. Examination shows a positive Spurling test on the left side, but no changes in motor, sensory, or deep tendon reflexes. Because nonsurgical management has failed to provide relief, he has chosen surgery to allow him to complete his season. The MRI scan and myelogram shown in Figures 19a and 19b show minimal disk bulge, but a root cutoff is noted at the left C7 foramen. Electromyography demonstrates C7 nerve root irritation. Which of the following procedures will best optimize his chances for completing the season?

Explanation
Because the patient has chronic pain, a possible lateral recess stenosis of the C7 root, and no neurologic deficits, keyhole foraminotomy is the treatment of choice for decompressing the exiting nerve root and offering an early return to play, especially when using a muscle-splitting posterior approach. Henderson and associates reported excellent results with posterolateral foraminotomy in patients with radicular symptoms. Although anterior cervical diskectomy and fusion is equally effective in the long term, a period of 6 to 12 weeks is required to allow the anterior fusion to heal prior to a return to play. Chen and associates reported that keyhole foraminotomy maintains cervical motion segment dynamics better than compared to anterior limited diskectomy and foraminotomy or anterior diskectomy with fusion. Henderson, CM, Hennessy RG, Shuey HM Jr, Shackelford EG: Posterior-lateral foraminotomy as an exclusive operative technique for cervical radiculopathy: A review of 846 consecutively operated cases. Neurosurgery 1983;13:504-512. Dillin W, Booth R, Cuckler J, Balderston R, Simeone F, Rothman R: Cervical radiculopathy: A review. Spine 1986;11:988-991.
Question 96High Yield
The main blood supply to the lateral two thirds of the talar body is provided by the
Explanation
Explanation
The main blood supply to the lateral two thirds of the talar body is derived from the artery of the tarsal canal, a branch of the posterior tibial artery. The peroneal artery helps form a vascular plexis over the posterior tubercle and combines with other arteries to form the artery of the sinus tarsi, which is the principal blood supply of the intrasinus structures of the talus. The anterior tibial arteries send branches to the superior surface of the talar head and give rise to the anterolateral malleolar artery, which may anastomose with other vessels to form the artery of the tarsal sinus. Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1465-1518.
References:
- Haliburton RA, Sullivan CR, Kelly PJ, et al: The extra-osseous and intra-osseous blood supply of the talus. J Bone Joint Surg Am 1958;40:1115-1120.
Question 97High Yield
Which of the following is most commonly associated with an open clavicular fracture?
Explanation
Explanation
Open clavicular fractures are rare and result from high-energy trauma. In a series of 20 patients with open clavicular fractures, 13 (65%) sustained a closed head injury. Fifteen (75%) had associated pulmonary injuries and 35% had a cervical or thoracic spine fracture. Only one demonstrated scapulothoracic dissociation. Screening for pulmonary and closed head injuries should be considered in the setting of traumatic open clavicular fractures.
Question 98High Yield
A 21-year-old collegiate track athlete increased her training 4 months ago in anticipation of starting the season. Two months into her training program, she reported pain followed by a 1-month history of diffuse pain in the first metatarsophalangeal joint that was aggravated by weight bearing. A removable walker boot partially relieved the pain, and she was able to complete the season. Her pain has now returned; however, she denies any history of injury. Examination reveals tenderness over the medial sesamoid but no deformities. A radiograph and bone scan are shown in Figures 22a and 22b. What is the best treatment option at this time?
Explanation
Explanation
22b The radiograph reveals either a fractured or bipartite sesamoid. The bone scan shows asymmetrically increased uptake over the medial sesamoid. Given the history and physical examination, a stress fracture is the most likely diagnosis. Medial sesamoidectomy reliably improves pain, and athletes return to sports on an average of 7 weeks after excision. Immobilization typically requires more than 4 to 8 weeks and is not always successful; however, it would be appropriate management for a patient who is not an elite athlete. Sanders R: Fractures of the midfoot and forefoot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1601-1603.
References:
- Saxena A, Krisdakumtorn T: Return to activity after sesamoidectomy in athletically active individuals. Foot Ankle Int 2003;24:415-419.
Question 99High Yield
A 37-year-old woman has had intermittent paresthesias and numbness in the plantar foot for the past 6 months. She reports that the symptoms are worse with activity, and the paresthesias are beginning to awaken her at night. MRI scans are shown in Figures 6a and 6b. What is the most likely diagnosis?

Explanation
The symptoms are consistent with tarsal tunnel syndrome. Ganglion cysts are a well-known cause of tarsal tunnel syndrome. The MRI scans show a high intensity, well-circumscribed mass in the tarsal tunnel that is consistent with a fluid-filled cyst. Patients usually respond well to excision of the ganglion and resolution of the tarsal tunnel symptoms. The surrounding fat is a different signal intensity on the MRI scans, which rules out a lipoma. Synovial cell sarcoma has a heterogeneous appearance on an MRI scan. Metastatic tumors are most commonly found in the osseous structures of the foot, not the soft tissues. Rozbruch SR, Chang V, Bohne WH, et al: Ganglion cysts of the lower extremity: An analysis of 54 cases and review of the literature. Orthopedics 1998;21:141-148. Llauger J, Palmer J, Monill JM, et al: MR imaging of benign soft-tissue masses of the foot and ankle. Radiographics 1998;18:1481-1498.
Question 100High Yield
A 53-year-old man has had a long history of multiple joint symptoms, and he notes that the worst pain is from his left shoulder. A radiograph and MRI scan are shown in Figures 13a and 13b. Prior to surgical treatment of the shoulder, what is the most appropriate work-up?
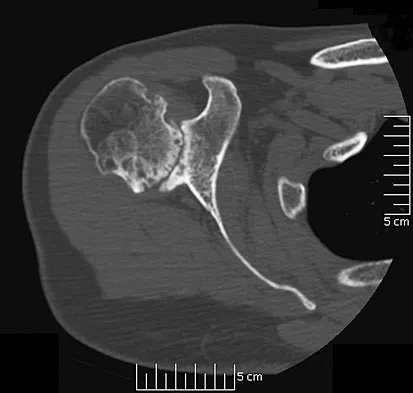
Explanation
Rheumatoid arthritis is sometimes associated with radiographic evidence of instability of the cervical spine. In a study by Grauer and associates, radiographs of the cervical spine of patients with rheumatoid arthritis who had undergone total joint arthroplasty over a 5-year period were retrospectively reviewed. Nearly one half of the patients had radiographic evidence of cervical instability on the basis of traditional measurements. While radiographic evidence of cervical instability was not infrequent in this population of patients who underwent total joint arthroplasty for rheumatoid arthritis, radiographic predictors of paralysis were much less common. MRI prior to surgery may also be a consideration if the radiographic appearance of the rotator cuff alters the consideration of surgical treatment. In a series of patients undergoing prosthetic arthroplasty for a variety of shoulder disorders, the presence of a rotator cuff tear has been shown to be associated with a less favorable outcome. Most often, the presence of a rotator cuff tear was associated with a diagnosis of rheumatoid or other inflammatory arthritis and the tears were large and generally irreparable. Some case series demonstrated a higher prevalence of loosening of the glenoid component in patients with a large rotator cuff tear associated with superior migration of the humeral head. However, obtaining an MRI scan of the shoulder is not considered the best response since failure to determine cervical instability may result in anesthetic death. Whereas MRI may be helpful in planning reconstruction, it would be a less important priority. Grauer JN, Tingstad EM, Rand N, et al: Predictors of paralysis in the rheumatoid cervical spine in patients undergoing total joint arthroplasty. J Bone Joint Surg Am 2004;86:1420-1424.
You Might Also Like
Previous ChapterOrthopedic Board Review: 100 High-Yield MCQs - Mock Exam Se…
Next Chapter Orthopedic Surgery Board Review: 100 High-Yield MCQs | Mock…

Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon