Orthopedic Board Review: 100 High-Yield MCQs - Mock Exam Set 712
14 Apr 2026
98 min read
104 Views
Key Takeaway
This page offers 100 high-yield orthopedic board review questions (MCQs) to help surgeons and residents prepare for ABOS, OITE, and FRCS exams. Mock Exam Set 712 is designed to test knowledge, identify critical areas, and build confidence for mastering certification and recertification assessments.
Evaluation of Nerve Root Lesions: Pinpoint Tr...
00:00
Start Quiz
Question 1High Yield
What is the most frequent location of entrapment of the deep peroneal nerve?
Explanation
Explanation
The most frequently described entrapment of the deep peroneal nerve is the anterior tarsal tunnel syndrome. This syndrome refers to entrapment of the deep peroneal nerve under the inferior extensor retinaculum. Entrapment can also occur as the nerve passes under the tendon of the extensor hallucis brevis. Compression by underlying dorsal osteophytes of the talonavicular joint and an os intermetatarseum (between the bases of the first and second metatarsals) have previously been described in runners. Kopell HP, Thompson WA: Peripheral entrapment neuropathies of the lower extremity. N Engl J Med 1960;262:56-60.
References:
- Schon LC, Mann RA: Diseases of the nerves, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 1, pp 675-677.
Question 2High Yield
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50?
Explanation
The image shows a view of the radiocapitellar joint from an anterior medial portal. The radial nerve lies on the elbow capsule at the midportion of the capitellum. It is at risk for injury when capsular excision is performed in this region. Field LD, Altchek DW, Warren RF, et al: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Question 3High Yield
A 65-year-old man who underwent cemented right total hip arthroplasty 6 years ago now reports acute pain for the past week. He denies any trauma, recent illnesses, or symptoms other than pain. Plain radiographs show possible loosening of the femoral component. A normal result from which of the following studies will most specifically rule out infection?
Explanation
Explanation
A patient with an infected total hip arthroplasty may lack the symptoms of fever, chills, redness, or increased warmth typical of septic arthritis. Sensitivity for ESR and CRP ranges from 61% to 96%, and specificity ranges from 85% to 100%. Technetium Tc 99m bone scans are costly and time-consuming and will not differentiate between septic and aseptic loosening. Hip aspiration has a false-positive rate of up to 15%, although it may be useful in this patient to further complement the clinical picture if the ESR and CRP are elevated. The WBC count is rarely elevated in infected total hip arthroplasty. MRI is expensive and is not indicated for the diagnosis; however, it can aid in identifying intrapelvic extension of a periprosthetic abscess. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
References:
- Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 137-148.
Question 4High Yield
A 23-year-old baseball pitcher reports pain in the posterior aspect of his dominant shoulder during the late cocking phase of throwing. With the dominant shoulder positioned in 90 degrees of abduction from the body and with the scapula stabilized, examination reveals 135 degrees of external rotation and 20 degrees of internal rotation. Examination of the opposite shoulder reveals 100 degrees of external rotation and 75 degrees of internal rotation. Both shoulders are stable on examination. Radiographs and MRI scans are unremarkable. What is the primary cause of his pain?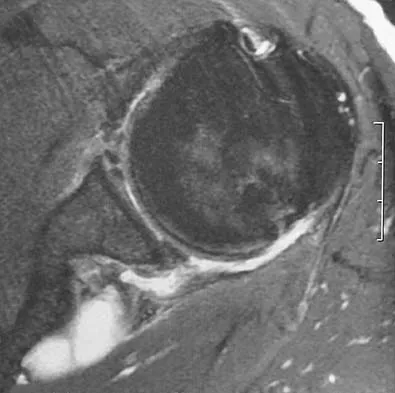
Explanation
Internal impingement of the shoulder is a leading cause of shoulder pain in the throwing athlete. The primary lesion in pathologic internal impingement is excessive tightening of the posterior band of the inferior glenohumeral ligament complex. To obtain an accurate assessment of true glenohumeral rotation, the scapula is stabilized during examination. A loss of 20 degrees or more of internal rotation, as measured with the shoulder positioned in 90 degrees of abduction, indicates excessive tightness of the posterior band of the inferior glenohumeral ligament complex. Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part I: Pathoanatomy and biomechanics. Arthroscopy 2003;19:404-420.
Question 5High Yield
Which of the following surgical devices employed for stabilization of the sternoclavicular joint is associated with the highest incidence of life-threatening complications?
Explanation
Explanation
Numerous reports have documented serious complications including death from migration of intact or broken Kirschner wires or Steinmann pins into hilar structures such as the heart, pulmonary artery, and the aorta. Gilot GJ, Wirth MA, Rockwood CA: Injuries to the sternoclavicular joint, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott, Williams and Wilkins, 2006, vol 2, pp 1373-1374.
References:
- Lyons FA, Rockwood CA Jr: Migration of pins used in operations of the shoulder. J Bone Joint Surg Am 1990;72:1262-1267.
Question 6High Yield
A 22-year-old professional baseball catcher has posterior shoulder pain and severe external rotation weakness with the arm in adduction. Radiographs are normal. MRI scans are shown in Figures 15a through 15c. Management should consist of
Explanation
Explanation
15b 15c The MRI scans reveal a large posterior paralabral cyst associated with a posterior-superior labral tear. The cyst appears as a well-defined, smoothly marginated mass with low signal intensity on T1-weighted MRI scans and with high signal intensity on T2-weighted MRI scans. MRI also reveals changes in the supraspinatus and infraspinatus muscles secondary to denervation, including decreased muscle bulk and fatty infiltration. MRI has the added advantage, compared with other imaging modalities, of detecting intra-articular lesions, such as labral tears, which are frequently associated with ganglion cysts of the shoulder. In this case of a professional baseball player with a space-occupying lesion causing nerve compression with an associated labral tear, the treatment of choice is arthroscopic decompression of the cyst and repair of the tear. Acromioplasty would not address the primary pathology in this patient. Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
References:
- Martin SD, Warren RF, Martin TL, et al: Suprascapular neuropathy: Results of non-operative treatment. J Bone Joint Surg Am 1997;79:1159-1165.
Question 7High Yield
A 20-year-old woman has had wrist pain for the past 5 months. A radiograph, MRI scans, and biopsy specimen are shown in Figures 46a through 46d. The patient is then treated with intralesional surgery. The patient should be counseled that her risk of developing lung metastasis is approximately what percent?
Explanation
Explanation
46b 46c 46d Giant cell tumor of bone has about a 2% risk of benign pulmonary metastasis in all cases and 6% risk in recurrent cases. The radiograph and MRI scans show a lytic destructive lesion in the distal radius with no matrix mineralization. The lesion extends up to the subchondral bone. In a young woman, the most likely diagnosis is giant cell tumor of bone, which is supported by the pathology results that show monotonous fibrovascular stroma with numerous multinucleated giant cells where the nuclei that make up the giant cells are identical to the nuclei that make up the background stromal cells. Athanasian EA, Wold LE, Amadio PC: Giant cell tumors of the bones in the hand. J Hand Surg Am 1997;22:91-98.
References:
- Siebenrock KA, Unni KK, Rock MC: Giant-cell tumor of bone metastasizing to the lungs: A long-term follow-up. J Bone Joint Surg Br 1998;80:43-47.
Question 8High Yield
A 25-year-old man sustained the closed injury shown in Figures 22a and 22b. Examination reveals that this is an isolated injury, and he is hemodynamically stable. Treatment should consist of
Explanation
Explanation
22b The treatment of choice for closed diaphyseal femoral fractures in adults is reamed intramedullary nailing with static interlocking. Reaming allows placement of a larger, stronger implant and offers better healing rates than unreamed nailing. Static interlocking ensures that there is no loss of reduction because of underappreciated fracture lines or comminution. Brumback RJ, Virkus WW: Intramedullary nailing of the femur: Reamed versus nonreamed. J Am Acad Orthop Surg 2000;8:83-90.
References:
- Brumback RJ, Ellison TS, Poka A, et al: Intramedullary nailing of femoral shaft fractures: Part III. Long-term effects of static interlocking fixation. J Bone Joint Surg Am 1992;74:106-112.
Question 9High Yield
A 65-year-old man has a painful right hip mass that has been growing for several years. A radiograph, CT scan, and photomicrograph are shown in Figures 56a through 56c. What is the most appropriate treatment?


Explanation
This is a conventional chondrosarcoma. The radiograph and the CT scan show a lesion arising from the inferior pubic ramus with a large soft-tissue mass. Abundant punctate, stippled, or "popcorn-like" calcification is present. The photomicrograph demonstrates hypercellular cartilage. Surgical resection is the only effective treatment. Whereas chemotherapy might play a role in the treatment of a dedifferentiated chondrosarcoma, it has no role in the treatment of a conventional chondrosarcoma. Chondrosarcomas are relatively radioresistant. Donati D, El Ghoneimy A, Bertoni F, et al: Surgical treatment and outcome of conventional pelvic chondrosarcoma. J Bone Joint Surg Br 2005;87:1527-1530. Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome. J Bone Joint Surg Am 1999;81:326-338.
Question 10High Yield
The load versus deformation curve of the functional spinal unit (FSU) is made up of the neutral zone, the elastic zone, and the plastic zone. What is the plastic zone of the curve believed to represent?
Explanation
Explanation
Plastic deformation of viscoelastic tissues represents deformation of the soft tissues to the point of failure. The lining up of collagen fibers would be in the "toe region" of the curve, which, in the case of the FSU, would be mainly in the neutral zone. Elastin is a minor contributor to the composition of the ligaments and would be protected by the stiffer collagen fibers. The transition between flexion and extension occurs in the neutral zone, and reversible elongation occurs in the elastic zone. Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 15-23.
References:
- Panjabi MM, White AA: Physical properties and functional biomechanics of the spine, in White AA, Panjabi MM: Clinical Biomechanics of the Spine, ed 2. Philadelphia, PA, JB Lippincott, 1990, pp 1-83.
Question 11High Yield
Cell signaling through the activation of a transmembrane receptor complex formed by serine/threonine kinase receptors occurs with which of the following growth factors?
Explanation
Explanation
Cell activation and transcription varies with the target cell, the growth factor-receptor combination, and the biologic state of the cell. The growth factors in the transforming growth factor-beta (TGF-ß) superfamily signal through serine/threonine kinase receptors. Fibroblast growth factors, insulin-like growth factors, and platelet-derived growth factors signal through tyrosine kinase receptors. Growth hormone is released by the pituitary and circulates to the liver where target cells are stimulated to release insulin-like growth factor. Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044.
References:
- Schmitt JM, Hwang K, Winn SR, et al: Bone morphogenetic proteins: An update on basic biology and clinical relevance. J Orthop Res 1999;17:269-278.
Question 12High Yield
Which of the following factors is associated with the worst prognosis in soft-tissue sarcomas?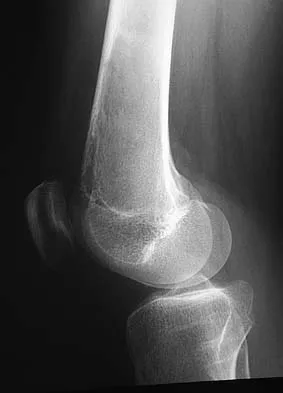
Explanation
Although factors such as a high-grade tumor and large size are associated with decreased survival, the presence of metastases carries the worst prognosis. Good results are very rare when metastases are present. Soft-tissue sarcomas, as a whole, respond poorly to chemotherapy, leading to a poor prognosis when metastases are present. Collin C, Goobold J, Hadju SI, Brennan MF: Localized extremity soft tissue sarcoma: An analysis of factors affecting survival. J Clin Oncol 1987;5:601-612.
Question 13High Yield
The illustration shown in Figure 19 shows a Chamberlain line. What is the most likely diagnosis?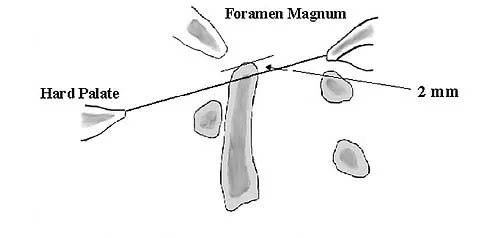
Explanation
Basilar invagination is best defined as vertical or compressive instability at the occiput-C1 joint. Such invaginations most commonly occur in patients with rheumatoid arthritis but also can occur secondary to trauma or tumor. A Chamberlain line is used as a method to determine basilar invagination. The odontoid tip should not be more than 5 mm above a Chamberlain line. Wiesel SW, Rothman RH: Occipito-atlantal hypermobility. Spine 1979;4:187-191.
Question 14High Yield
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
Explanation
Explanation
Subscapularis tears can be associated with disruption of the transverse ligament supporting the biceps. The remaining aspects of the rotator cuff, superior labrum, and capsule can be intact with this injury. Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
References:
- Gerber C, Sebesta A: Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: A preliminary report. J Shoulder Elbow Surg 2000;9:483-490.
Question 15High Yield
A 30-year-old man who underwent an anterior lumbar diskectomy and fusion at L4-5 and L5-S1 through an anterior retroperitoneal approach 1 month ago now reports he is unable to obtain and maintain an erection. The most likely cause of this condition is
Explanation
Sexual dysfunction is a common condition after extensive anterior lumbar surgical dissection. Erectile dysfunction usually is nonorganic but may be related to parasympathetic injury. The parasympathetic nerves are deep in the pelvis at the level of S2-3 and S3-4 and usually are not involved in the surgical field for anterior L4-5 and L5-S1 procedures. Retrograde ejaculation is the result of injury to the sympathetic chain on the anterior surface of the major vessels crossing the L4-5 level and at the L5-S1 interspace. Erectile function and orgasm are not affected by sympathetic injury. The pudendal nerve is primarily a somatic nerve and is not located in the surgical field. Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492.
Question 16High Yield
A patient with deficient anteroinferior bone stock undergoes a Latarjet procedure that transfers a portion of the coracoid to the glenoid rim and secures it with two screws. After surgery, the patient reports numbness on the anterolateral forearm. To verify the diagnosis, what muscle should be tested for strength?
Explanation
Explanation
A Latarjet procedure is similar to a Bristow procedure, but with the Latarjet procedure a larger portion of the coracoid is transferred to the scapular neck at the anteroinferior glenoid. As in a Bristow procedure, if the fragment is pulled or twisted during the dissection or during fixation, the musculocutaneous nerve can be injured. With loss of biceps function, elbow flexion and forearm supination will be weaker. Ho E, Cofield RH, Balm MR, Hattrup SJ, Rowland CM: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270. Boardman ND 3rd, Cofield RH: Neurologic complications of shoulder surgery. Clin Orthop 1999;368:44-53.
References:
- Allain J, Goutallier D, Glorion C: Long-term results of the Latarjet procedure for the treatment of anterior instability of the shoulder. J Bone Joint Surg Am 1998;80:841-852.
Question 17High Yield
A 15-year-old boy who participates in track reports acute pain along the left iliac crest during a sprint. Examination reveals that the anterior superior iliac spine is nontender. The most likely diagnosis is an injury to the
Explanation
Explanation
The patient has iliac apophysitis. The radiographic findings are easily overlooked but usually reveal slight asymmetric widening of the iliac crest apophysis. The apophysis is the most vulnerable structure, as it is three to five times weaker than the tendon. This is not an epiphyseal site, and injury to the muscle or the tendinous insertion to bone (enthesis) is unlikely. Clancy WG Jr, Foltz AS: Iliac apophysitis and stress fractures in adolescent runners. Am J Sports Med 1976;4:214-218. Waters PM, Millis MB: Hip and pelvic injuries in the young athlete, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 279-293. Lombardo SJ, Retting AC, Kerlan RK: Radiographic abnormalities of the iliac apophysis in adolescent athletes. J Bone Joint Surg Am 1983;65:444-446.
References:
- Paletta GA Jr, Andrish JT: Injuries about the hip and pelvis in the young athlete. Clin Sports Med 1995;14:591-628.
Question 18High Yield
Which of the following statements correctly describes the results of gamma irradiation of musculoskeletal allograft?
Explanation
Explanation
Low dose gamma irradiation (less than 3.0 megarads) with antibiotic soaks is one of the most common techniques for secondary sterilization. Elimination of HIV with gamma irradiation requires doses estimated to be greater than 3.5 megarads. Gamma irradiation levels of 4 megarads have been shown to alter the mechanical properties of human infrapatellar tendons. Ethylene oxide, also used for allograft sterilization, has been associated with a chronic inflammatory process that resolved after graft removal. Jackson DW, Windler GE, Simon TM: Intraarticular reaction associated with the use of freeze-dried, ethylene oxide-sterilized bone-patella tendon-bone allografts in the reconstruction of the anterior cruciate ligament. Am J Sports Med 1990;18:1-10. Conway B, Tomford W, Mankin HJ, et al: Radiosensitivity of HIV-1: Potential application to sterilization of bone allografts. AIDS 1991;5:608-609.
References:
- Rasmussen TJ, Feder SM, Butler DL, et al: The effects of 4 Mrad of gamma irradiation on the initial mechanical properties of bone-patellar tendon-bone grafts. Arthroscopy 1994;10:188-197.
Question 19High Yield
Figures 25a and 25b show the clinical photographs of a 19-year-old baseball outfielder who has shoulder pain after sliding headfirst into second base. He reports pain while batting, sliding, and catching. Examination reveals a posterior prominence during midranges of forward elevation, which then disappears with a palpable clunk during terminal elevation and abduction. What is the most likely diagnosis?
Explanation
Explanation
25b A headfirst slide with the arm extended can injure the posterior shoulder. Winging of the scapula is dynamic and is considered a compensatory effort to prevent subluxation; it is not related to nerve injury. Posterior glenohumeral subluxation can be present during the initiation of a bat swing. Rotator cuff function, interval tears, and superior labrum tears can be painful but do not produce winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
References:
- Fiddian NJ, Kling RJ: The winged scapula. Clin Orthop 1984;185:228-236.
Question 20High Yield
Flexion and extension of the elbow occur about an axis of rotation that
Explanation
Explanation
The elbow mimics a true hinge and flexes and extends around an axis that is centered in the centers of the trochlea and capitellum. The medial epicondyle is not perfectly isometrically placed; rather the axis of rotation passes through a point on the anteroinferior aspect of the medial epicondyle. Application of a hinged external fixator is possible because of the fact that there is a single axis of rotation. Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 53-54. London JT: Kinematics of the elbow. J Bone Joint Surg Am 1981;63:529-535.
References:
- Morrey BF, Chao EY: Passive motion of the elbow joint. J Bone Joint Surg Am 1976;58:501-508.
Question 21High Yield
Which of the following is considered the most common long-term effect on the spine of a professional race horse jockey?
Explanation
Explanation
Horseback riding is a sport that directly affects the jockey's spine. Tsirikos and associates reported the results of a study of 32 jockeys. They found that equestrian sports, especially professional horseback riding, apart from the increased risk of direct spinal injury caused by a fall from the horse, can lead to progressive spinal degeneration as a result of repetitive trauma and increased physical stress on the spine. It is associated with spondylosis of the cervical spine and lumbar spine. Tsirikos A, Papagelopoulos PJ, Giannakopoulos PN, et al: Degenerative spondyloarthropathy of the cervical and lumbar spine in jockeys. Orthop 2001;24:561-564.
References:
- Hordegen KM: The spine and horseback riding. Schweiz Med Wochenschr 1975;105:668-675.
Question 22High Yield
Atraumatic neuropathy of the suprascapular nerve usually occurs at what anatomic location?
Explanation
Explanation
The suprascapular nerve passes through the suprascapular notch and the spinoglenoid notch before innervating the infraspinatus muscle. At both locations, the suprascapular nerve is prone to nerve compression, which often results from a ganglion cyst. The other anatomic locations are not associated with suprascapular nerve impingement. Romeo AA, Rotenberg DD, Bach BR: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
References:
- Post M, Mayer J: Suprascapular nerve entrapment: Diagnosis and treatment. Clin Orthop 1987;223:126-136.
Question 23High Yield
Acetaminophen is an antipyretic medication. It exerts its pharmacologic effects by inhibiting which of the following enzymes?
Explanation
Acetaminophen inhibits prostaglandin E2 production via IL-1 B, without affecting cyclooxygenase-2 enzymatic activity. The therapeutic concentrations of acetaminophen induce an inhibition of IL-1 B-dependent NF-kappa B nuclear translocation. The selectivity of this effect suggests the existence of an acetaminophen-specific activity at the transcriptional level that may be one of the mechanisms through which the drug exerts its pharmacologic effects. Acetaminophen does not affect any of the other enzymes named above.
Question 24High Yield
A 25-year-old woman has significant pain and swelling in her left ankle after falling off her bicycle. Examination reveals that she is neurovascularly intact. Radiographs are shown in Figures 33a through 33c. What is the next most appropriate step in management?


Explanation
The radiographs show a displaced ankle fracture with widening of the syndesmosis. Open reduction and internal fixation is indicated with fixation of the mortise with syndesmotic screws. Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Question 25High Yield
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with
Explanation
Explanation
27b An isolated avulsion of the lesser tuberosity occurs very rarely and usually is found in 12- and 13-year-old adolescents. The MRI scans reveal a tear of the humeral attachment of the inferior glenohumeral ligament, a so-called HAGL lesion. This injury to the inferior glenohumeral ligament occurs much less commonly than the classic Bankart lesion (anterior inferior labral tear). A tear of the subscapularis occurs with a similar mechanism of injury but generally occurs in older individuals. Bokor DJ, Conboy VB, Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br 1999;81:93-96.
References:
- Wolf EM, Cheng JC, Dickson K: Humeral avulsion of the inferior glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607.
Question 26High Yield
Which of the following primary prognostic factors best predicts the outcome of the knee lesion shown in Figure 22?
Explanation
The patient has osteochondritis dissecans. While location, size, and knee stability are all relevant to the overall prognosis, studies have shown that younger patients with open growth plates have a better prognosis of healing when compared with patients who have closed growth plates. The degree of pain is also relevant to treatment, but it is subjective rather than objective and is not as reliable of a prognostic indicator as age. Stanitski CL: Osteochondritis dissecans of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, vol 3, pp 387-405. Cahill B: Treatment of juvenile osteochondritis dissecans and osteochondritis dissecans of the knee. Clin Sports Med 1985;4:367-384.
Question 27High Yield
Flexion-distraction injuries of the thoracolumbar spine are most frequently associated with injury to what organ system?
Explanation
In patients with flexion-distraction injuries of the thoracolumbar spine, 50% have associated, potentially life-threatening, visceral injuries that occasionally are diagnosed hours or even days after admission. Based on these findings, consultation with a general surgeon is recommended. Blunt and penetrating injuries to the cardiopulmonary system or aorta sometimes can be seen with this type of injury, but they are no more common than with other types of thoracolumbar fractures because of the relatively mild bony injury anteriorly. Neurologic trauma with this type of fracture is also somewhat rare. Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 351-360.
Question 28High Yield
What pharmacologic agents are preferred for the treatment of symptomatic active Paget's disease?
Explanation
Recent medical literature supports the use of bisphosphonates as the treatment of choice for active Paget's disease.
Question 29High Yield
A 21-year-old college student reports hearing a pop and has acute pain laterally over the ankle after twisting it during a recreational basketball game. Examination 1 hour after the injury reveals minimal swelling and ecchymosis. The anterior drawer sign is positive. Radiographs reveal no evidence of a fracture. What is the best course of action?
Explanation
Even though the patient has a grade 3 ankle ligament injury, studies have shown that 95% of patients with a grade 3 injury that may include a complete tear of the ligaments will heal successfully with conservative functional management. Extensive diagnostic evaluation with stress radiographs, CT, and MRI is not indicated. Surgical reconstruction is not indicated because of the overwhelming success of conservative management; however, in the few patients where late instability develops, surgical reconstruction offers an excellent outcome. Carne P: Nonsurgical treatment of ankle sprains using the modified Sarmiento brace. Am J Sports Med 1989;17:253-257.
Question 30High Yield
What are the optimal conditions for leaving the acetabular shell in place, replacing the acetabular liner, and grafting the osteolytic defect shown in Figure 39?
Explanation
Explanation
Dense pods of ingrowth into the porous coating of cementless ingrowth sockets are seen. Channels through the non-ingrown portion allow access to the trabecular bone of the ilium. Polyethylene wear debris can enter these areas through screw holes. Expansile, lytic lesions can result, which can become large without compromising implant fixation. Loosening is late and results from catastrophic loss of bone. A well-fixed acetabular component with a modular design, a well-designed locking mechanism, and a good survivorship history is a candidate for exchange of the liner and grafting of the osteolytic lesion. Ries MD: Complications in primary total hip arthroplasty: Avoidance and management. Wear. Instr Course Lect 2003;52:257-265. Dumbleton JH, Manley MT, Edidin AA: A literature review of the association between wear rate and osteolysis in total hip arthroplasty. J Arthroplasty 2002;17:649-661.
References:
- Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180.
Question 31High Yield
A 38-year-old man underwent a transtibial amputation for chronic posttraumatic foot and ankle pain and chronic calcaneal osteomyelitis. Postoperative radiographs are seen in Figures 41a and 41b. What is the proposed purpose of the surgical modification seen in the radiographs?

Explanation
The Ertl modification of a below-knee amputation has been proposed to create a more stable "platform" to aid in transferring the load of weight bearing between the residual limb and the prosthetic socket. It is felt that a stable platform allows total contact loading over an enlarged stable surface area. Early studies have suggested that this modification may enhance the patient's perceived functional outcome. Pinzur MS, Pinto MA, Saltzman M, et al: Health-related quality of life in patients with transtibial amputation and reconstruction with bone bridging of the distal tibia and fibula. Foot Ankle Int 2006;27:907-912.
Question 32High Yield
A 21-year-old woman who was wearing a seat belt sustained an injury of the thoracolumbar junction in a motor vehicle accident. The AP radiograph shows widening between the L1 and L2 spinous processes, and the CT scan shows the empty facet sign at this level. The initial evaluation should include
Explanation
The patient has a flexion-distraction injury of the thoracolumbar spine that is often associated with wearing a seat belt. The fracture has a high risk of associated intra-abdominal injury; therefore, the initial evaluation should include a CT of the abdomen. The most common visceral injury is to the bowel. Smith WS, Kaufer H: Patterns and mechanisms of lumbar injuries associated with lap seat belts. J Bone Joint Surg Am 1969;51:239-254.
Question 33High Yield
Creatine is currently being used by athletes as a dietary supplement in an attempt to enhance performance. What is the physiologic basis for its use?
Explanation
Creatine is currently used as a nutritional supplement in an attempt to enhance athletic performance. The physiologic basis for its use is based on its conversion by CK to PCr, which acts as an energy reservoir in muscle cells for the production of ATP. A number of studies that examined the effect of creatine supplementation on performance concluded that while creatine does not increase peak force production, it can increase the amount of work done in the first few anaerobic short duration, maximal effort trials. The mechanism for this enhancement of work is unknown, but it is most likely secondary to the increase in the available PCr pool. Greenhaff PL: Creatine and its application as an ergogenic aid. Int J Sport Nutr 1995;5:S100-S110. Greenhaff PL, Casey A, Short AH, Harris R, Soderlund K, Hultman E: Influence of oral creatine supplementation on muscle torque during repeated bouts of maximal voluntary exercise in man. Clin Sci 1993;84:565-571. Trump ME, Heigenhauser GJ, Putman CT, Spriet LL: Importance of muscle phosphocreatine during intermittent maximal cycling. J Appl Physiol 1996;80:1574-1580.
Question 34High Yield
In the preoperative planning of revision acetabular reconstruction, the surgeon should identify significant posterior column deficiency by noting which of the following radiographic features?
Explanation
Proximal and medial migration of the femoral head usually indicates deficiencies of the dome or anterior column. Wear of the polyethylene may result in osteolysis and impingement, which are not indicative of any major bone deficiency. A significant osteolytic lesion in the ischium may represent a major posterior column deficiency that can create a technical challenge during the reconstruction. Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: Acetabular technique. Clin Orthop 1994;298:147-155.
Question 35High Yield
A 55-year-old woman with type I diabetes mellitus has a chronic ulcer over the dorsum of her right foot and reports forefoot pain. Examination reveals 1- x 2-cm nondraining ulcer over the dorsum of the foot. The patient has 1-2+ pain with compression of the foot and ankle. She has a weakly palpable posterior tibial pulse and an absent dorsalis pedis pulse. There is no erythema, cellulitis, or drainage. Radiographs are normal. Which of the following diagnostic studies should be obtained?
Explanation
The presence of a dorsal ulcer in the presence of weak or absent pulses strongly suggests the possibility of arterial insufficiency. The best initial noninvasive study to assess for ischemia is the Doppler arterial study. A determination of the vascular status is of a greater priority than an assessment for infection or neuropathy because of the location and presentation of the ulcer. If ankle pressures are less than 45 mm Hg, there is a high risk that these lesions will not heal without revascularization. Wagner FW Jr: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981;2:64-122.
Question 36High Yield
Figure 36 shows an AP radiograph of a 65-year-old man who reports activity-related groin pain. History reveals that he underwent total hip arthroplasty 12 years ago. What is the most likely diagnosis?
Explanation
Explanation
The AP radiograph demonstrates extensive periacetabular osteolysis. The central hole eliminator has dissociated from the shell and migrated into a lytic defect in the ischium. In a retrieval study, most periacetabular osteolytic lesions had a clear communication pathway with the joint space. Lesions with communication to the joint via several pathways or through a central dome hole (as in this patient) were larger and more likely to be associated with cortical erosion. Although periprosthetic tumors have been described, they are rare and particle-induced inflammation around a prosthesis does not seem to increase the risk for carcinogenesis. Visuri T, Pulkkinen P, Paavolainen P: Malignant tumors at the site of total hip prosthesis: Analytic review of 46 cases. J Arthroplasty 2006;21:311-323. Bezwada HP, Shah AR, Zambito K, et al: Distal femoral allograft reconstruction for massive osteolytic bone loss in revision total knee arthroplasty. J Arthroplasty 2006;21:242-248.
References:
- Kitamura N, Naudie DD, Leung SB, et al: Diagnostic features of pelvic osteolysis on computed tomography: The importance of communication pathways. J Bone Joint Surg Am 2005;87:1542-1550.
Question 37High Yield
Which of the following factors is most critical to the success of a meniscal allograft transplantation?
Explanation
Explanation
Success of a meniscal allograft transplantation is strongly dependent on accurate graft sizing, typically within 5% of the native meniscus. Previous studies have established that donor cell viability is not mandatory for the survival of these grafts since they are replaced by the recipient's cells (at least peripherally) within several weeks. Thus, cryopreservation of the graft to ensure cell viability is not necessary. There is a limited immune response to musculoskeletal allografts; therefore, immunosuppression, as is required for visceral organ transplantation, is not indicated. Wirth CA, Kohn D: Meniscal transplantation and replacement, in Fu FH, Harner CD, Vince JG (eds): Knee Surgery. Baltimore, MD, Williams & Wilkins, 1994, vol 1, pp 631-641. Brautigan BE, Johnson DL, Caborn DM, et al: Allograft tissues, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 205-213.
References:
- Shaffer B, Kennedy S, Klimkiewicz J, et al: Preoperative sizing of meniscal allografts in meniscus transplantation. Am J Sports Med 2000;28:524-533.
Question 38High Yield
Which of the following statements best describes synovial fluid?
Explanation
Synovial tissue is composed of vascularized connective tissue that lacks a basement membrane. Two cell types (type A and type B) are present: type B cells produce synovial fluid. Synovial fluid is made of hyaluronic acid and lubricin, proteinases,and collagenases. It is an ultrafiltrate of blood plasma added to fluid produced by the synovial membrane. It does not contain erythrocytes, clotting factors, or hemoglobin. It lubricates articular cartilage and provides nourishment via diffusion. Synovial fluid exhibits non-Newtonian flow characteristics. The viscosity coefficient is not a constant, the fluid is not linearly viscous, and its viscosity increases as the shear rate decreases.
Question 39High Yield
A patient who underwent closed reduction of the hips as an infant now reports pain. An abduction internal rotation view shows an incongruous joint. Based on the findings shown in Figure 3, what is the most appropriate type of pelvic osteotomy for the right hip?
Explanation
Pelvic osteotomies that redirect hyaline cartilage over the femoral head offer the potential for long-term preservation of the hip; however, salvage procedures such as the Chiari osteotomy are indicated in patients without a concentrically reducible hip. Ito and associates reported that moderate dysplasia and moderate subluxation without complete obliteration of the joint space and a preoperative center-edge angle of at least minus 10 degrees are desirable selection criteria. Ohashi H, Hirohashi K, Yamano Y: Factors influencing the outcome of Chiari pelvic osteotomy: A long-term follow-up. J Bone Joint Surg Br 2000;82:517-525.
Question 40High Yield
Which of the following nerves is most commonly injured during ankle arthroscopy?
Explanation
The superficial peroneal nerve, which is adjacent to the location of the lateral arthroscopic portal is most commonly injured. Ferkel RD, Heath DD, Guhl JF: Neurological complications of ankle arthroscopy. Arthroscopy 1996;12:200-208.
Question 41High Yield
Which of the following best describes the resultant forces on an increased offset stem when compared with a standard offset stem?
Explanation
Explanation
The increased emphasis on restoring offset in total hip arthroplasty has implications for the forces applied to the components and the fixation interfaces. Static analysis has shown that with an increased affect, joint reaction force on the articulation is decreased. When the resultant load on the hip is "out of plane" (ie, directed anterior to posterior), there is increased torsion where the stem is turned into more retroversion. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180. Hurwitz DE, Andriaacchi TP: Biomechanics of the hip, in Callaghan J, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven , 1998.
References:
- Pauwels F: Biomechanics of the Normal and Diseased Hip. New York, NY, Springer-Verlag, 1976.
Question 42High Yield
Figures 20a and 20b show the sagittal and coronal T1-weighted MRI scans of a patient's left knee. Abnormal findings include

Explanation
The MRI scans show meniscal tissue extending across the entire lateral compartment, revealing a discoid lateral meniscus. The increased signal within the lateral meniscal tissue indicates a tear. Discoid lateral menisci are congenital variants that often present with mechanical symptoms in adolescents. The other structures in the knee are normal. Ahn JH, Shim JS, Hwang CH, et al: Discoid lateral meniscus in children: Clinical manifestations and morphology. J Pediatr Orthop 2001;21:812-816.
Question 43High Yield
Figures 35a through 35c show the clinical photograph and radiographs of a 15-year-old boy who stubbed his toe 1 day ago while walking barefoot in the yard. Management should consist of
Explanation
Explanation
35b 35c The patient has an open fracture of the physis of the distal phalanx with a portion of the nail bed interposed in the physis. Seymour initially described this injury in the distal phalanges of fingers. Optimal treatment consists of removing the interposed tissue, irrigating the fracture, and a short course of antibiotics. The nail should be preserved to provide stability. Kensinger DR, Guille JT, Horn BD, et al: The stubbed great toe: Importance of early recognition and treatment of open fractures of the distal phalanx. J Pediatr Orthop 2001;21:31-34. Pinckney LE, Currarino G, Kennedy LA: The stubbed great toe: A cause of occult compound fracture and infection. Radiology 1981;138:375-377.
References:
- Seymour N: Juxta-epiphysial fracture of the terminal phalanx of the finger. J Bone Joint Surg Br 1966;48:347-349.
Question 44High Yield
A 12-year-old girl has had lower back pain for the past 6 months that interferes with her ability to participate in sports. She denies any history of radicular symptoms, sensory changes, or bowel or bladder dysfunction. Examination reveals a shuffling gait, restriction of forward bending, and tight hamstrings. Radiographs show a grade III spondylolisthesis of L5 on S1, with a slip angle of 20 degrees. Management should consist of
Explanation
Indications for surgical treatment of spondylolisthesis include pain and/or progression of deformity. Specifically, surgery is necessary when there is persistent pain or a neurologic deficit that fails to respond to nonsurgical therapy, there is significant slip progression, or the slip is greater than 50%. For patients with mild spondylolisthesis, in situ posterolateral L5-S1 fusion is adequate. In patients with more severe slips (greater than 50%), extension of the fusion to L4 offers better mechanical advantage. Postoperative immobilization may be achieved with instrumentation, casting, or both. In patients with a slip angle of greater than 45 degrees, reduction of the lumbosacral kyphosis with instrumentation or casting is desirable to prevent slip progression. Laminectomy alone is contraindicated in a child. Nerve root decompression is indicated if radiculopathy is present clinically. Seitsalo S, Osterman K, Hyvarinen H, Tallroth K, Schlenzka D, Poussa M: Progression of spondylolisthesis in children and adolescents: A long-term follow-up of 272 patients. Spine 1991;16:417-421.
Question 45High Yield
A teenager is undergoing a correction of deformity and lengthening of the femur. Distractions are proceeding as expected; however, during his 6-week follow-up examination, the patient reports that the distraction motors have become harder to turn over for the past 2 to 3 days. Figures 37a and 37b show current radiographs. What is the most likely complication being encountered?
Explanation
Explanation
37b Premature consolidation is a complication that is unique to gradual bone lengthening after corticotomy. Causes include excessive latency period, inadequate distraction rate, exuberant bone formation, patient compliance problems, and mechanical failure of the distraction apparatus. The femur and fibula are most commonly involved. This patient did not have an incomplete corticotomy, as initial distraction occurred before the distraction device was noted to seize up. The radiographs show bowing of the Ilizarov wires and mature regenerate bone, both suggestive of premature consolidation. No wire breakage or joint subluxation is seen on the radiographs. Treatment for premature consolidation includes continuing distraction until the consolidation bridge ruptures, or additional surgery may include closed rotational osteoclasis or repeat corticotomy. Paley D: Problems, obstacles and complications of limb lengthening, in Maiocchi AB, Aronson J (eds): Operative Principles of Ilizarov. Baltimore, MD, Williams & Wilkins, 1991, p 360.
References:
- Herring JA: Limb length discrepancy, in Herring JA (ed): Tachdjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, p 1088.
Question 46High Yield
Posterior sternoclavicular dislocations are most commonly associated with which of the following complications?
Explanation
Posterior sternoclavicular dislocations are commonly associated with tracheal compression, which can be a life-threatening condition requiring immediate reduction. The other listed complications are less common. Brooks AL, Henning GD: Injury to the proximal clavicular epiphysis, abstracted. J Bone Joint Surg Am 1972;54:1347-1348.
Question 47High Yield
In addition to radiographs of the primary lesion and chest, MRI of the primary lesion, and CT of the chest, staging studies for Ewing's sarcoma should include which of the following?
Explanation
Explanation
A bone scan and bone marrow biopsy are part of the staging studies for Ewing's sarcoma. Whole body MRI and PET scans are investigational and show promise of greater sensitivity than a bone scan. Schleiermacher G, Peter M, Oberlin O, Philip T, Rubie H, Mechinaud F, et al: Increased risk of systemic relapses associated with bone marrow micrometastasis and circulating tumor cells in localized ewing tumor. J Clin Oncol 2003;21:85-91.
References:
- Daldrup-Link HE, Franzius C, Link TM, Laukamp D, Sciuk J, Jurgens H, et al: Whole-body MR imaging for detection of bone metastases in children and young adults: Comparison with skeletal scintigraphy and FDG PET. Am J Roentgenol 2001;177:229-236.
Question 48High Yield
A patient who sustained injuries in a motorcycle accident 30 minutes ago has significant motor and sensory deficits corresponding to a C6 level of injury. A lateral radiograph obtained during the initial on-scene evaluation reveals bilateral jumped facets at C5-C6; this appears to be an isolated injury. The patient is awake and alert. The next step in management of the dislocation should consist of
Explanation
Surgical open reduction may increase the neurologic deficit if a disk herniation exists. Evidence from animal studies suggests that rapid decompression of the spinal cord may improve recovery. Serially increasing traction weight to reduce the dislocation has been shown to be safe when used in patients who are awake. Indications for MRI include patients who are unable to cooperate with serial examinations, the need for open reduction, and progression of deficit during awake reduction. Delamarter RB, Sherman J, Carr JB: Pathophysiology of spinal cord injury: Recovery after immediate and delayed decompression. J Bone Joint Surg Am 1995;77:1042-1049. Star AM, Jones AA, Cotler JM, Balderston RA, Sinha R: Immediate closed reduction of cervical spine dislocations using traction. Spine 1990;15:1068-1072.
Question 49High Yield
What is the most common malignancy involving the hand?
Explanation
Skin cancers far outnumber primary musculoskeletal malignancies of the hand and the most common of these is squamous cell carcinoma. Metatastic lung carcinoma, while classic for the carcinoma that metastasizes to the hand, does so at an extremely low rate. Fink JA, Akelman E: Nonmelanotic malignant skin tumors of the hand. Hand Clin 1995;11:255-264.
Question 50High Yield
Ewing's sarcoma of bone most commonly occurs in which of the following locations?
Explanation
Explanation
Ewing's sarcoma typically occurs in the major long tubular bones, with the femur the most common location. The flat bones of the pelvis are the second most common location. Ewing's sarcoma occurs in the fibula but with a lower incidence than that seen in the major tubular bones. Ewing's sarcoma infrequently occurs in the metacarpals or the vertebral bodies. Simon M, Springfield D, et al: Ewing's Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 287.
References:
- Wold LA, et al: Ewing's Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 210-211.
Question 51High Yield
Which of the following is considered the treatment of choice for a 3-cm chondroblastoma of the distal femoral epiphysis with no intra-articular extension?
Explanation
Curettage and bone grafting typically are the preferred treatment of chondroblastoma, yielding acceptable local recurrence rates of less than 10%. Some surgeons advocate adjuvant therapies such as phenol, liquid nitrogen, or argon beam coagulation. Untreated, these lesions can destroy bone and invade the joint to a significant degree. Large intra-articular lesions may require major joint reconstruction. Wide local excision is rarely required to control the tumor. Radiation therapy is indicated only in unresectable lesions. Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748.
Question 52High Yield
Which of the following ligaments is the primary static restraint against inferior translation of the arm when the shoulder is in 0 degrees of abduction?
Explanation
The superior glenohumeral ligament (SGHL) and coracohumeral ligament serve as primary static restraints against inferior translation of the arm when the shoulder is in 0 degrees of abduction. Of these, the coracohumeral ligament has been shown to have a greater cross-sectional area, greater stiffness, and greater ultimate load than the SGHL. The inferior glenohumeral ligament plays a greater stabilizing role with increasing abduction of the arm. The coracoacromial ligament may help provide superior stability, especially when the rotator cuff is deficient. The coracoclavicular ligaments stabilize the acromioclavicular joint. Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Question 53High Yield
A 60-year-old man with diabetes mellitus is referred for evaluation of nonhealing ulcers of his left foot. Nonsurgical management has failed to provide relief, and a below-the-knee amputation is being considered. Which of the following studies best predicts successful amputation wound healing?
Explanation
Explanation
The TcPO2 measures the O2 delivering capacity of the local vasculature. Values above 40 mm Hg have been shown to correlate with positive healing potential. The hemoglobin A1c is a good indicator of long-term glucose levels; however, it has no direct correlation with wound healing potential. Serum albumin is an indirect measure of nutritional status, and deficiencies in nutrition must be addressed before any surgery. Adequate hemoglobin levels are also necessary to promote adequate oxygenation to the amputation site. The ankle-brachial index may be falsely elevated as a result of calcified vessels in patients with diabetes mellitus. Wyss CR, Harrington RM, Burgess EM, et al: Transcutaneous oxygen tension as a predictor of success after amputation. J Bone Joint Surg Am 1988;70:203-207.
References:
- Dwars BJ,van den Broek TA, Rauwerda JA, et al: Criteria for reliable selection of the lowest level of amputation in peripheral vascular disease. J Vasc Surg 1992;15:536-542.
Question 54High Yield
A 12-year-old girl has had right knee pain for the past 3 months. Radiographs and a coronal T2-weighted MRI scan are shown in Figures 10a through 10c. A biopsy specimen is shown in Figure 10d. What is the most appropriate treatment for this lesion?
Explanation
Explanation
10b 10c 10d The radiographs show a lytic lesion in the right proximal tibia that has a high fluid content based on the MRI findings. The radiographic appearance is consistent with either telangiectatic osteosarcoma or aneurysmal bone cyst. Low-magnification histology shows a lesion resembling an aneurysmal bone cyst, with blood lakes separated by cellular septa. However, high-magnification shows severe cytologic atypia, indicative of a telangiectatic osterosarcoma. The appropriate treatment is neoadjuvant chemotherapy followed by wide resection and reconstruction of the lesion. Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
References:
- Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Question 55High Yield
A 30-year-old man has had a 3-day history of severe, incapacitating lower back pain without radiation. He reports improvement with rest. He denies any history of trauma, has no constitutional symptoms, and his neurologic examination is normal. What is the best course of action?
Explanation
There are no red flags in the history or examination to warrant MRI. Limited bed rest (less than 3 days) has been shown to be more beneficial to early recovery compared with prolonged bed rest (more than 7 days). No data support the use of epidural or facet steroid injections for acute low back pain.
Question 56High Yield
What is the incidence and significance of anterior cruciate ligament laxity following tibial eminence fractures in skeletally immature individuals?
Explanation
Explanation
Measurable anterior cruciate ligament laxity, while frequently seen after tibial eminence fractures, usually does not cause symptoms. It is found even in patients whose fractures have been anatomically reduced and fixed, leading to speculation that it is due to stretching of the ligament at the time of injury. Willis R, Blokker C, Stall TM, et al: Long-term follow-up of anterior eminence fractures. J Pediatr Orthop 1993;13:361-364.
References:
- Smith JB: Knee instability after fracture of the intercondylar eminence of the tibia. J Pediatr Orthop 1984;4:462-464.
Question 57High Yield
A 63-year-old woman with a history of poliomyelitis has a fixed 30-degree equinus contracture of the ankle, rigid hindfoot valgus, and normal knee strength and stability. She reports persistent pain and has had several medial forefoot ulcerations despite a program of stretching, bracing, and custom footwear. What is the next most appropriate step in management?
Explanation
Explanation
The patient has a fixed deformity of the hindfoot and an Achilles tendon contracture; therefore, the treatment of choice is triple arthrodesis with Achilles tendon lengthening. Further bracing will not be helpful. Amputation is not indicated, and ankle arthrodesis will not address the hindfoot deformity. Palliative management would be more appropriate if the knee was unstable or the quadriceps were weak, because the equinus balances the ground reaction force across the knee. Perry J, Fontaine JD, Mulroy S: Findings in post-poliomyelitis syndrome: Weakness of muscles of the calf as a source of late pain and fatigue of muscles of the thigh after poliomyelitis. J Bone Joint Surg Am 1995;77:1148-1153.
References:
- Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
Question 58High Yield
Figure 17 shows the radiograph of a 2-year-old girl who sustained a fracture of the femur in a fall while walking with her parents. History reveals that this is her third long bone fracture, having sustained a humerus fracture 1 year ago and a fracture of the opposite femur 9 months ago. There is no family history of any similar problem. Examination reveals distinctly blue sclerae, normal appearing teeth, and no skin lesions. What is the most likely cause of this patient's disorder?
Explanation
Explanation
Osteogenesis imperfecta (OI) is a genetically determined disorder of type I collagen synthesis that is characterized by bone fragility. This patient has had three fractures of the long bones by age 2 years, with the last one occurring after relatively minor trauma. The patient's history and clinical features are consistent with a diagnosis of Sillence type IA OI. Type I OI is the mildest and most common form. Inheritance is autosomal-dominant; however, as in this patient, new mutations are frequent. Type I is subclassified into the A type (absence of dentinogenesis imperfecta) and B type (presence of dentinogenesis imperfecta). The sclerae are blue, and the first fractures usually occur in the preschool years after walking has begun. Cells from individuals with type I OI largely demonstrate a quantitative defect of type I collagen; they synthesize and secrete about half the normal amount of type I procollagen. Qualitative mutations that lead to an abnormal type I procollagen molecule result in more severe types of the disorder. There are no indications that this child has been abused. Radiographs of the femur show no evidence of rickets, pyknodysostosis, or osteopetrosis. Morquio syndrome, characterized by excess excretion of keratin sulfate in the urine, is not associated with bone fragility. Kocher MS, Shapiro F: Osteogenesis imperfecta. J Am Acad Orthop Surg 1998;6:225-236. Sillence DO, Senn A, Danks DM: Osteogenesis imperfecta: An expanding panorama of variants. Clin Orthop 1981;159:11-25.
References:
- Cole WG: Etiology and pathogenesis of heritable connective tissue diseases. J Pediatr Orthop 1993;13:392-403.
Question 59High Yield
A 45-year-old man reports right shoulder pain with overhead activities only. Figures 47a through 47d show the radiographs, bone scan, and MRI scan of a lesion of the proximal shoulder. What is the most appropriate treatment?
Explanation
Explanation
47b 47c 47d The figures show a lesion of the proximal humerus consistent with an enchondroma. The lesion is calcified on the radiographs. There is no cortical destruction, significant endosteal scalloping, or soft-tissue mass. The bone scan shows mild uptake in the area of the proximal humerus, and the T2-weighted MRI scan shows a lesion with high uptake, suggesting a lesion with high water content. A CT scan could also be obtained to rule out bone destruction or periosteal reaction. Pain with overhead activities is likely related to the rotator cuff. A biopsy is unlikely to add information because of inherent difficulties interpreting low-grade cartilaginous lesions. Curettage and grafting and en bloc resection are excessive treatments for a benign lesion that is apparently asymptomatic. Observation with a follow-up radiograph in 3 to 6 months is appropriate. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
References:
- Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
Question 60High Yield
An adult with a distal humeral fracture underwent open reduction and internal fixation. What is the most common postoperative complication?
Explanation
Most patients lose elbow range of motion after open reduction and internal fixation of a distal humeral fracture. Ulnar nerve dysfunction, nonunion, and infection all occur less commonly. Webb LX: Distal humerus fractures in adults. J Am Acad Orthop Surg 1996;4:336-344.
Question 61High Yield
In surgically treating hand and finger infections in patients with diabetes mellitus, what factor is associated with higher amputation rates?
Explanation
Patients with diabetes mellitus are prone to infection, and surgical treatment of their infections frequently requires multiple procedures. The triad of poor wound healing, chronic neuropathy, and vascular disease contributes to the increased infection rate. Studies have demonstrated increased amputation rates in patients with diabetes mellitus who have renal failure or deep polymicrobial or gram-negative infections. Gonzalez MH, Bochar S, Novotny J, et al: Upper extremity infections in patients with diabetes mellitus. J Hand Surg Am 1999;24:682-686. Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 62High Yield
Figure 12 shows a lateral radiograph of the elbow. What is the most likely diagnosis?
Explanation
Explanation
The figure shows a supracondylar process, which is a normal anatomic variant. An osteochondroma tends to occur more toward the end of bones, and the medullary space of the underlying bone extends into the base of the osteochondroma. The presence of a supracondylar process is usually asymptomatic. However, the ligament of Struthers that always extends from the supracondylar process to the medial epicondyle can result in median nerve entrapment secondary to trauma. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 132-133.
References:
- Keats TE, Anderson MW: Atlas of Normal Roentgen Variants That May Simulate Disease, ed 7. St Louis, MO, Mosby Inc, 2001, p 497.
Question 63High Yield
When treating osteoporosis with alendronate, what is the most common side effect?
Explanation
Explanation
Alendronate is a second-generation bisphosphonate, and it can cause epigastric distress in up to 30% of patients. This side effect can be minimized by gradually building up to therapeutic doses over a period of 4 to 8 weeks. Marshall JK, Rainsford KD, James C, et al: A randomized controlled trial to assess alendoronate-associated injury of the upper gastrointestinal tract. Aliment Pharmacol Ther 2000;14:1451-1457.
References:
- Lane JM, Sandhu HS: Osteoporosis of the spine, in Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 227-234.
Question 64High Yield
An eversion mechanism of injury is associated with which of the following ankle conditions?
Explanation
An inversion ankle injury typically involves ligamentous damage to the lateral ligaments of the ankle to include the anterior talofibular ligament and calcaneofibular ligament. Acute and particularly chronic ankle sprains also can have associated injuries. The inversion mechanism has been implicated in osteochondral and transchondral talar dome lesions, producing splits in the peroneus tendons, and in the development of meniscoid and soft-tissue impingement lesions in the anterolateral ankle. An inversion mechanism can also stretch the superficial peroneal nerve, leading to pain and paresthesias along its distribution. A fracture of the anterior colliculus is typically the result of an eversion mechanism resulting in a bony avulsion of the deltoid ligament from the anterior colliculus of the medial malleolus. Casillas MM: Ligament injuries of the foot and ankle in the athlete, in DeLee JC, Drez D, Miller MD (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2323-2357.
Question 65High Yield
A 21-year-old woman has a nontraumatic rupture of the Achilles tendon. Which of the following commonly prescribed medications has been associated with this condition?
Explanation
Explanation
Fluoroquinolones have been associated with increased rates of tendinitis, with special predilection for the Achilles tendon. Tenocytes in the Achilles tendon have exhibited degenerative changes when viewed microscopically after fluoroquinolone administration. Recent clinical studies have shown an increased relative risk of Achilles tendon rupture of 3.7. The other listed drugs have no known increase in tendon rupture rates nor tendinitis. van der Linden PD, van de Lei J, Nab HW, et al: Achilles tendinitis associated with fluoroquinolones. Br J Clin Pharmacol 1999;48:433-437. Bernard-Beaubois K, Hecquet C, Hayem G, et al: In vitro study of cytotoxicity of quinolones on rabbit tenocytes. Cell Biol Toxicol 1998;14:283-292.
References:
- Maffulli N: Rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036.
Question 66High Yield
A 7-year-old boy is seen in the emergency department with an isolated and displaced supracondylar humerus fracture and absent radial and ulnar pulses. Despite a moderately painful attempt at realignment, examination reveals that his hand remains pulseless. What is the next most appropriate step in management?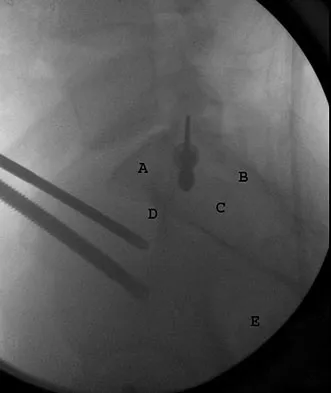
Explanation
Displaced supracondylar humerus fractures in children may have associated vascular compromise. Decreased blood flow may be due to vessel injury, entrapment within the fracture site, kinking from fracture displacement, or from vessel spasm. Optimal initial treatment in the emergency department includes gentle realignment of the limb and vascular assessment. Angiography is not required in isolated injuries as the level of the vessel compromise is always at the site of the fracture. When blood flow is not restored, the next best step in treatment is to proceed urgently to the operating room. A formal closed reduction and pinning is performed, and then the vascular status is reassessed. Exploration and vascular repair is required if the hand is cool, white, and without pulses. Ay S, Akinci M, Kamiloglu S, et al: Open reduction of displaced pediatric supracondylar humeral fractures through the anterior cubital approach. J Pediatr Orthop 2005;25:149-153. Sabharwal S, Tredwell SJ, Beauchamp RD, et al: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Question 67High Yield
Figure 12 shows the radiograph of a patient who has anterior knee pain. History reveals a femoral fracture at age 5 years. What is the most likely cause of the deformity?
Explanation
Explanation
The radiograph shows a recurvatum deformity of the proximal tibia with growth arrest of the tibial tubercle apophysis. This deformity has been described in association with femoral shaft fractures in children and has been attributed to a clinically silent, concommitant injury to the proximal tibial physes and also to iatrogenic injury associated with a proximal tibial traction pin. Overlengthened hamstrings and rupture of the posterior cruciate ligament may lead to knee hyperextension; however, these problems should not cause bone deformity. Osgood-Schlatter disease occurs when growth is nearly complete and usually leads to prominence of the tibial tubercle. Patellar tendon rupture is rare in children and would not cause this deformity unless the repair was performed with screws across the apophysis. Hresko MT, Kasser JR: Physeal arrest about the knee associated with non-physeal injuries of the lower extremity. J Bone Joint Surg Am 1989;71:698-703.
References:
- Bowler JR, Mubarak SJ, Wenger DR: Tibial physeal closure and genu recurvatum after femoral fracture: Occurrence without a tibial traction pin. J Pediatric Orthop 1990;10:653-657.
Question 68High Yield
A 50-year-old man who underwent an arthroscopic rotator cuff repair 5 days ago now returns for an early postoperative follow-up because of increasing pain in his shoulder. He reports increasing malaise and has a low-grade fever. Examination reveals no redness or swelling, but he has scant serous drainage from the posterior portal. An emergent Gram stain is positive for gram-positive cocci. The next most appropriate step in management should consist of
Explanation
An infection of the shoulder is considered a surgical emergency unless there are medical reasons that a patient cannot be taken to the operating room. If cultures of wound drainage are in question, then an aspiration should be done emergently, not several days later. The hallmark of infection in any major joint is increasing pain out of proportion to what is expected. Drainage occurring 1 to 2 days after an arthroscopic procedure is not normal, and it should be aggressively treated. Delay in diagnosis can result in sepsis and on a delayed basis, postinfectious arthritis. Both the glenohumeral joint and the subacromial space require debridement and irrigation, followed by antibiotics after both areas are cultured. Mansat P, Cofield RH, Kersten TE, Rowland CM: Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213. Settecerri JJ, Pitner MA, Rock MG, Hanssen AD, Cofield RH: Infection after rotator cuff repair. J Shoulder Elbow Surg 1999;8:1-5. Ward WG, Eckardt JJ: Subacromial/subdeltoid bursa abscesses: An overlooked diagnosis. Clin Orthop 1993;288:189-194.
Question 69High Yield
A 65-year-old woman sustained an axial load on the arm followed by an abduction injury after falling on ice. Treatment in the emergency department consisted of reduction of an anterior dislocation. She now has a positive drop arm sign and a positive lift-off test. An MRI scan is shown in Figure 9. Based on these findings, management should consist of
Explanation
Dislocation of the long head of the biceps tendon is the result of a defect in the region of the rotator cuff interval, coracohumeral ligament-superior glenohumeral ligament pulley, or an associated tear of the medial insertion of the subscapularis tendon. In the case of an intra-articular dislocation of the long head of the biceps tendon associated with a tear of the subscapularis tendon, stabilization of the biceps tendon is difficult in this situation; therefore, biceps release or tenodesis and repair of the subscapularis tendon is the treatment of choice. Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310. Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Question 70High Yield
A 10-year-old girl who is Risser stage 0 has back deformity associated with neurofibromatosis type 1 (NF1). She has no back pain. Examination shows multiple cafe-au-lait nevi with normal lower extremity neurologic function and reflexes. Standing radiographs of the spine show a short 50-degree right thoracic scoliosis with a kyphotic deformity of 55 degrees (apex T8). A 10-degree progression in scoliosis has occurred during the past 1 year. There is no cervical deformity. MRI shows mild dural ectasia, primarily in the upper lumbar region. Management should consist of
Explanation
Explanation
Scoliotic deformities in patients with NF1 are often dysplastic with short, angular curves. Posterior arthrodesis is made more difficult by the presence of kyphosis and of weak posterior elements caused by dural ectasia. Combined anterior and posterior spinal arthrodesis is generally preferred for progressive dysplastic curves to maximize deformity correction and to decrease the risk of pseudarthrosis. Anterior fusion may also prevent crankshaft phenomenon in young children. Brace treatment is not effective for large, rigid, or dysplastic curves. Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
References:
- Funasaki H, Winter RB, Lonstein JB, et al: Pathophysiology of spinal deformities in neurofibromatosis: An analysis of seventy-one patients who had curves associated with dystrophic changes. J Bone Joint Surg Am 1994;76:692-700.
Question 71High Yield
The anticoagulant effect of the low-molecular-weight heparins (LMWH) is mediated by the binding affinity of antithrombin III to which of the following coagulation factors?
Explanation
Standard heparin mediates its anticoagulant effect largely through its interaction with antithrombin III. A conformational change in antithrombin III occurs that markedly accelerates its ability to inactivate the coagulation enzymes thrombin factor (II), factor Xa, and factor IXa. In contrast, LMWHs do not contain the necessary saccharide units to bind thrombin and antithrombin III simultaneously. The anticoagulant effect of LMWHs involves binding of antithrombin III to factor Xa.
Question 72High Yield
When planning revision of a total hip arthroplasty where an acetabular reconstruction will be required, what prerequisite is important to ensure long-term success of a cementless component?
Explanation
In bone defects where host bone support is less than 50%, the failure rate is 70% at 5.1 years. The presence or absence of columns or hip position is of relatively little importance if the supportive bone is not present in at least 50% of the surface area around the future acetabular implant.
Question 73High Yield
In the upright standing position, approximately what percent of the vertical load is borne by the lumbar spine facet joints?
Explanation
Direct measurement and finite element modeling results show that approximately 20% of the vertical load is borne by the posterior structures of the lumbar spine in the upright position. Adams MA, Hutton WC: The effect of posture on the role of the apophyseal joints in resisting intervertebral compressive forces. J Bone Joint Surg Br 1980;62:358-362.
Question 74High Yield
A 16-year-old girl injured her hip in a fall. Radiographs are shown in Figures 14a and 14b. She denies any history of pain prior to the fall and is currently asymptomatic. A bone scan, MRI scan, and biopsy specimens are shown in Figures 14c through 14f. What is the most likely diagnosis?





Explanation
Although the classic radiographic appearance of fibrous dysplasia is one of a central metaphyseal lesion with ground glass matrix, it is not unusual to see either a more radiodense-appearing lesion or a more peripheral location. The histologic finding of spicules of woven bone without osteoblastic rimming in a bland fibrous background is diagnostic of fibrous dysplasia. The imaging studies could be consistent with low-grade osteosarcoma, osteoblastoma, or osteomyelitis, but all have a very different histologic picture. Observation is indicated in the absence of symptoms, impending fracture, or deformity. Fibrous dysplasia most commonly occurs in the proximal femur. Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 30-43.
Question 75High Yield
Figure 24 shows the radiograph of a 47-year-old woman who has severe right hip pain and a limp. Management should consist of
Explanation
Femoral shortening osteotomy for a Crowe type IV hip dislocation has been shown to provide superior results with minimal complications. Cementless fixation of the stem allows for modular implants that greatly simplify the reconstruction.
Question 76High Yield
Which of the following findings is a relative contraindication to primary total knee arthroplasty?
Explanation
Explanation
Contraindications to primary total knee arthroplasty include active infection, an incompetent extensor mechanism, compromised vascularity in the extremity, and local neurologic disruption affecting the competence of the musculature about the knee. Anterior cruciate, posterior cruciate, or lateral ligament incompetence can be managed with primary total knee arthroplasty. Mild flexion contracture and previous high tibial valgus osteotomy are not contraindications to primary total knee arthroplasty.
References:
- Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 513-536.
Question 77High Yield
A 55-year-old woman who underwent a left total hip arthroplasty 8 months ago using a modified Hardinger approach reports a persistent painless limp. Examination reveals that when she is not using a cane, she lurches to the left during weight bearing on the left lower extremity. An AP radiograph is shown in Figure 29. Which of the following hip muscle groups should be strengthened to improve the gait abnormality?
Explanation
Explanation
The modified Hardinger approach includes a partial anterior trochanteric osteotomy creating a trochanteric wafer (as seen on the radiograph) that is displaced anterior and medial in continuity with the gluteus medius and vastus lateralis. Failure of abductor reattachment, migration of the trochanter, nonunion of the osteotomy site, and excessive splitting of the gluteus medius muscle causing injury to the inferior branch of the superior gluteal nerve can result in weakness of the abductor mechanism. Abductor strength should be evaluated with the patient lying on the opposite side and elevating the affected limb. Although slight weakness may manifest itself as a limp only after prolonged muscular activity, significant weakness results in a constant limp without associated discomfort. Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 512-526.
References:
- Kasser JR (ed): Orthopedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 389-426.
Question 78High Yield
Figures 3a and 3b show the MRI scans of a patient with neck pain. What is the most likely diagnosis?

Explanation
Muliple neurofibromas result in marked foraminal enlargement as seen on the sagittal MRI scan. Collagen disorders leading to dural ectasia may show similar enlargement, but none of these is listed as a possible answer. Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Question 79High Yield
The thickest bone in the occiput is located
Explanation
Explanation
Anatomic studies have shown that the thickest bone of the occiput is at the level of the external occipital protuberance. It ranges from 11.5 mm to 15.1 mm in men and from 9.7 mm to 12 mm in women. In general, the bone thins as it extends distally from the external occipital protuberance and it also moves laterally from the midline. The structures at risk during screw placement include the venous sinuses. Nadim Y, Lu J, Sabry FF, et al: Occipital screws in occipitocervical fusion and their relation to the venous sinuses: An anatomic and radiographic study. Orthopedics 2000;23:717-719.
References:
- Ebraheim N, Lu J, Biyani A, et al: An anatomic study of the thickness of the occipital bone: Implications for occipitocervical instrumentation. Spine 1996;21:1725-1729.
Question 80High Yield
Figures 37a and 37b show the clinical photographs of a 43-year-old patient with type I diabetes mellitus who has a stump ulcer after undergoing successful transtibial amputation 1 year ago. Which of the following is considered the most predictable method of healing the ulcer and preventing recurrent ulceration?
Explanation
Explanation
37b The ulcer occurred as the result of a mismatch between the shape of the residual limb and the prosthetic socket. With the mismatch, the residual limb pistoned and the tissue failed because of the applied shear forces. The most predictable short- and long-term solution is reconstruction of the residual limb. Refraining from use of the prosthesis will prevent the patient from walking for months. It is unlikely that prosthetic socket modification will allow resolution of this large ulcer.
References:
- Hadden W, Marks R, Murdoch G, et al: Wedge resection of amputation stumps: A valuable salvage procedure. J Bone Joint Surg Br 1987;69:306-308.
Question 81High Yield
A 37-year-old man who works in a factory has isolated, lateral unicompartmental pain about his knee with activities. Nonsurgical management has failed to provide relief. The radiograph shown in Figure 45 reveals a tibiofemoral angle of approximately 15 degrees which is clinically correctable to neutral. What is the best surgical option in this patient?
Explanation
Explanation
Patients with a valgus alignment about the knee can have lateral compartment arthritis. Similar to a high tibial osteotomy, a supracondylar femoral osteotomy is indicated in younger patients who have a more active lifestyle and isolated unicompartmental disease. In this young patient who works in a factory and has a valgus knee, a medial closing wedge supracondylar femoral osteotomy is the treatment of choice. The role of arthroplasty is limited in younger patients. Mathews J, Cobb AG, Richardson S, et al: Distal femoral osteotomy for lateral compartment osteoarthritis of the knee. Orthopedics 1998;21:437-440.
References:
- Cameron HU, Botsford DJ, Park YS: Prognostic factors in the outcome of supracondylar femoral osteotomy for lateral compartment osteoarthritis of the knee. Can J Surg 1997;40:114-118.
Question 82High Yield
A 16-year-old boy sustains a twisting injury to the left knee while wrestling. MRI scans are shown in Figures 22a through 22c. What is the most likely diagnosis?
Explanation
Explanation
22b 22c The MRI scans show a displaced bucket-handle medial meniscus tear that can be visualized on coronal, sagittal, and axial views. The sagittal view shows the typical "double posterior cruciate ligament sign," in which the low-signal bucket-handle fragment parallels the normal low-signal posterior cruciate ligament. The coronal and axial images both show the displaced medial meniscus in the notch. Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
References:
- Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 83High Yield
Figures 35a and 35b show the radiographs of a patient who underwent debridement of a chronically infected, fully constrained knee prosthesis and now reports pain and instability despite bracing. History reveals that the patient has had no drainage since undergoing the last debridement 6 months ago. A C-reactive protein level and aspiration are negative for infection. Treatment should now consist of

Explanation
The radiographs show a significant loss of the proximal anterior tibial cortex, consistent with an extensively damaged or deficient extensor mechanism. Such a deficit precludes insertion of another knee arthroplasty. Arthrodesis is the treatment of choice for this patient and is indicated for loss of the extensor mechanism and knee instability. A recent report on arthrodesis following removal of an infected prosthesis showed a union rate of 91% using a short intramedullary nail. Insertion of an antibiotic-impregnated PMMA spacer is not indicated because the rationale for using a spacer is to maintain a space for reinsertion of another prosthesis. Reconstruction of the extensor mechanism would not address the loss of the joint. Amputation is the final treatment option if the arthrodesis fails. Rand JA: Alternatives to reimplantation for salvage of the total knee arthroplasty complicated by infection. J Bone Joint Surg Am 1993;75:282-289. Lai KA, Shen WJ, Yang CY: Arthrodesis with a short Huckstep nail as a salvage procedure for failed total knee arthroplasty. J Bone Joint Surg Am 1998;80:380-388.
Question 84High Yield
The quadrilateral space in the shoulder contains which of the following structures?
Explanation
The quadrilateral or quadrangular space of the shoulder is formed laterally by the humerus, proximally by the subscapularis (and teres minor viewed from posterior), distally by the teres major, and medially by the long head of triceps. The posterior humeral circumflex artery and axillary nerve pass through it. The axillary artery is more proximal. The radial nerve and profunda brachii pass through a triangular space more inferior. The circumflex scapular artery passes through a triangular space more medial. Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, pp 205-206.
Question 85High Yield
Figure 11a shows the clinical photograph of a 46-year old woman who reports a 3-week history of pain and a "lump" at the base of her neck. She is otherwise in good health and denies any trauma. A 3-D reconstruction CT is shown in Figure 11b. What is the most likely diagnosis?
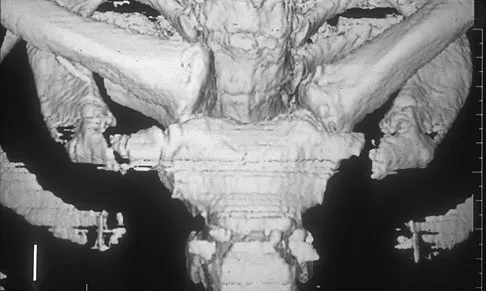
Explanation
Spontaneous subluxation of the sternoclavicular joint occurs without any significant trauma. It is usually accentuated by placing the extremity in an overhead position. Discomfort usually resolves within 4 to 6 weeks with nonsurgical management. Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1078-1079.
Question 86High Yield
A 53-year-old man reports a 5-week history of worsening low back pain accompanied by bilateral knee and ankle pain and swelling. He also reports a lesser degree of neck and left elbow pain. He denies any history of trauma or provocative episodes. His medical history is significant for Reiter's syndrome more than 25 years ago, with no subsequent exacerbations. Furthermore, he has recently returned from a vacation in Costa Rica and noted the development of infectious gastroenteritis with diarrhea within 1 week of his return. This was treated with a 10-day course of oral antibiotics and has since resolved. He denies any significant bowel or urinary symptoms at this time. His neurologic examination is essentially within normal limits, but is somewhat limited by his low back and leg pain. What further investigation is most appropriate at this time?
Explanation
Explanation
The patient has pain involving the cervical and lumbar spine as well as pain and swelling in both the knees and ankles. As such, this can be classified as polyarticular arthritis. The presence of multiple joint symptoms in the lower extremities, the absence of a history of trauma, and the multiple joints involved direct attention away from the spine as the etiology of this patient's pain. Radiographs of the involved joints are not likely to yield much useful information to assist with a diagnosis. Likewise, an MRI scan of the lumbar spine is not likely to provide much information regarding the etiology of the patient's condition. When a rheumatologic illness is suspected, the selective use of confirmatory laboratory testing can aid in arriving at a correct diagnosis. A presumed case of gout or chondrocalcinosis can be confirmed by the presence of the appropriate crystals in a joint-fluid aspiration. Because of the patient's recent trip to Costa Rica and the subsequent gastroenteritis, a CBC count, ESR, and CRP should be ordered to rule out infectious and inflammatory versus noninflammatory conditions. Rheumatoid factor (RF) in general should only be ordered for patients with polyarticular joint inflammation for more than 6 weeks. The presence of rheumatoid factor does not indicate rheumatoid arthritis. Antinuclear antibodies (ANA) should be ordered when a connective tissue disease such as systemic lupus erythematosus (SLE) is suspected on the basis of specific history and physical examination findings, such as inflammatory arthritis. Human leukocyte antigen-B27 (HLA-B27) should be ordered only when the patient's history is compatible with ankylosing spondylitis or Reiter's syndrome and this patient had a history of Reiter's syndrome. Gardner GC, Kadel NJ: Ordering and interpreting rheumatologic laboratory tests. J Am Acad Orthop Surg 2003;11:60-67.
Question 87High Yield
A 55-year-old man has had progressive right shoulder pain for the past 2 years. Examination reveals active elevation to 120 degrees, external rotation to 20 degrees, and internal rotation to the sacrum. AP and axillary radiographs are shown in Figures 23a and 23b. Which of the following procedures would result in the most predictable long-term pain relief?
Explanation
Explanation
23b Total shoulder arthroplasty yields excellent pain relief and function in patients with osteoarthritis. It is favored over humeral arthroplasty, especially when there is asymmetric posterior glenoid wear and posterior humeral subluxation as shown on the axillary radiograph. Arthroscopic debridement of the glenohumeral joint may be helpful in delaying the need for arthroplasty when the arthritic changes are mild to moderate but is not indicated for advanced osteoarthritis. Cofield RH, Frankle MA, Zuckerman JD: Humeral head replacement for glenohumeral arthritis. Semin Arthroplasty 1995;6:214-221. Levine WN, Djurasovic M, Glasson JM, Pollock RG, Flatow EL, Bigliani LU: Hemiarthroplasty for glenohumeral osteoarthritis: Results correlated to degree of glenoid wear. J Shoulder Elbow Surg 1997;6:449-454.
References:
- Matsen FA III: Early effectiveness of shoulder arthroplasty for patients who have primary glenohumeral degenerative joint disease. J Bone Joint Surg Am 1996;78:260-264.
Question 88High Yield
When performing a bunionectomy with a release of the lateral soft-tissue structures, the surgeon is cautioned against releasing the conjoined tendon that inserts along the lateral base of the proximal phalanx of the great toe. This conjoined tendon is made up of what two muscles?
Explanation
Owens and Thordardson cautioned surgeons not to release the conjoined tendon from the base of the proximal phalanx of the great toe because of an increased risk of iatrogenic hallux varus. Release of the transverse and oblique heads of the adductor hallucis is largely accomplished by releasing the soft tissue adjacent to the lateral sesamoid, without releasing tissue from the base of the proximal phalanx. The conjoined tendon is made up of the flexor hallucis brevis and the adductor hallucis. Owens S, Thordardson DB: The adductor hallucis revisited. Foot Ankle Int 2001;22:186-191.
Question 89High Yield
A 12-year-old girl has bilateral developmentally dislocated hips. History reveals no previous treatment, and she reports no discomfort. Good long-term clinical results are most likely to occur with
Explanation
Explanation
The natural history of complete developmental dislocation of the hip is dependent on two factors: bilaterality and the presence or absence of a false acetabulum. Patients with bilateral dislocations may have low back pain because of hyperlordosis, but they tend to have less disability than patients with unilateral dislocations who have secondary problems related to limb-length inequality. Degenerative joint disease and clinical disability are most likely to develop in patients with completely dislocated hips and well-developed false acetabula. In a 12-year-old child who has bilateral developmental hip dislocations, it would be difficult to obtain surgical treatment results that are better than the natural history of the disorder. Abductor strengthening exercises are unlikely to influence the long-term outcome in this disorder. Surface replacements are not indicated in young asymptomatic patients. Weinstein SL: Natural history of congenital hip dislocation (CDH) and hip dysplasia. Clin Orthop 1987;225:62-76.
References:
- Wedge JH, Wasylenko MJ: The natural history of congenital dislocation of the hip: A critical review. Clin Orthop 1978;137:154-162.
Question 90High Yield
Figure 17 shows the radiograph of a 25-year-old professional football player who has superior shoulder pain that prevents him from sports participation. History reveals that he sustained a shoulder injury that was treated with closed reduction and temporary pinning 3 years ago. The best course of action should be
Explanation
The radiograph shows a complete acromioclavicular separation. Because the patient is a professional athlete who is unable to participate, surgery is indicated. Chronic separations, especially those with previous trauma from joint pinning, should be treated with resection of the distal clavicle and stabilization to the coracoid. Some type of biologic reconstruction of the coracoclavicular ligaments is generally recommended. Open repair of the ligaments is generally not possible in such a delayed fashion. Screw fixation alone will not provide a lasting solution as the screws usually need to be removed, leaving no fixation in place. Reconstruction using the coracoacromial ligament is generally recommended with coracoclavicular fixation to protect the repair while it heals. Nuber GW, Bowen MK: Disorders of the acromioclavicular joint: Pathophysiology, diagnosis and management, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999.
Question 91High Yield
Examination of a 23-year-old female college basketball player who has had anterior knee pain for the past 3 weeks reveals tenderness and fullness over the inferior patella and proximal patellar tendon. There is no patellofemoral crepitus, patella apprehension sign, or anterior or posterior instability. Initial management should include
Explanation
The patient has patellar tendinitis (jumper's knee). It is a common overuse condition seen in runners, volleyball players, soccer players, and jumpers but can be seen in any activity in which repeated extension of the knee is required. In the acute setting, the pain is well localized and there is tenderness and sometimes swelling of the tendon. MRI is recommended for evaluating chronic cases and for surgical planning. In the acute phases, ice, rest, and avoidance of the offending activity are recommended. Weakness of the quadriceps and hamstring muscle are thought to contribute to this problem; therefore, stretching and isometric exercise in a limited range of motion are important. Complete rest and intratendinous injections of steroids are detrimental to tendon physiology. Stanish WD, Rubinovich RM, Curwin S: Eccentric exercise in chronic tendinitis. Clin Orthop 1986;208:65-68.
Question 92High Yield
Which of the following is considered the cause of Milwaukee shoulder, a joint disease similar to rotator cuff arthropathy?
Explanation
Neer and associates focused on mechanical and nutritional factors as the etiology of rotator cuff arthropathy. McCarty and associates, in describing a similar syndrome known as Milwaukee shoulder, focused on an inflammatory cause in proposing the pathogenic role of hydroxyapatite, a basic calcium phosphate. Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-1244.
Question 93High Yield
Figures 3a through 3c show the radiographs and bone scan of a patient who reports increasing pain associated with activity for the past several months. Laboratory studies show an erythrocyte sedimentation rate of 14 mm/h and a C-reactive protein level of 0.4. Aspiration is negative for infection. Management should consist of
Explanation
Explanation
3b 3c The radiographs show polyethylene wear, but exchange of this will not necessarily provide pain relief. The presence of pain suggests the possibility of occult loosening, and the surgeon must be prepared for this option intraoperatively. There is little evidence of infection. Rand JA, Peterson LF, Bryan RS, Ilstrup DM: Revision total knee arthroplasty, in Anderson LD (ed): Instructional Course Lectures XXXV. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1986, pp 305-318.
References:
- Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 317-322.
Question 94High Yield
A 13-year-old girl was riding on an all-terrain vehicle when the driver struck a tree. She sustained the injury shown in Figures 45a through 45d. This injury is best described as what type of acetabular fracture pattern?
Explanation
Explanation
45b 45c 45d The fracture is a both-column fracture in the Judet/Letournel classification and a C3 in the AO classification. There is extension into the sacroiliac joint along the pelvic brim and comminution along the posterior column above the sciatic notch. Both the anterior and posterior columns are separately broken and displaced. However, the defining feature of a both-column pattern, as seen in this patient, is that all articular fragments are on fracture fragments and no joint surface is left intact to the axial skeleton above. The use of three-dimensional images makes it easier to view the location of the fracture fragments and the amount and direction of displacement. Helfet DL, Beck M, Gautier E, et al: Surgical techniques for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 533-603. Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
References:
- Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 95High Yield
When compared with a patient who has a subluxated hip, a patient with a dislocated hip who is undergoing acetabular reconstruction for developmental dysplasia of the hip will most likely have
Explanation
Explanation
The rate of revision has been found to be significantly increased in patients with a dislocated hip preoperatively compared with patients with a subluxated hip. This may be the result of compromised acetabular bone stock. The rate of nerve palsy may be increased because of the greater degree of lengthening required to reduce the reconstructed hip. Numair J, Joshi AB, Murphy JC, Porter ML, Hardinge K: Total hip arthroplasty for congenital dysplasia or dislocation of the hip: Survivorship analysis and long-term results. J Bone Joint Surg Am 1997;79:1352-1360.
References:
- Schmalzried TP, Noordin S, Amstutz HC: Update on nerve palsy associated with total hip replacement. Clin Orthop 1997;344:188-206.
Question 96High Yield
Which of the following findings is a prerequisite for a high tibial valgus osteotomy for medial compartment gonarthrosis?
Explanation
Explanation
The indications for high tibial valgus osteotomy include a physiologically young age, arthritis confined to the medial compartment, 10 to 15 degrees of varus alignment on weight-bearing radiographs, a preoperative arc of motion of at least 90 degrees, flexion contracture of less than 15 degrees, and a motivated, compliant patient. Contraindications include lateral compartment narrowing of the articular cartilage, lateral tibial subluxation of greater than 1 cm, medial compartment bone loss, ligamentous instability, and inflammatory arthritis. Naudie D, Bourne RB, Rorabeck CH, Bourne TT: The Insall Award: Survivorship of the high tibial valgus osteotomy. A 10- to 22-year followup study. Clin Orthop 1999;367:18-27.
References:
- Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 255-264.
Question 97High Yield
What is the first ossification center to appear radiographically in the pediatric elbow?
Explanation
Explanation
The first ossification center to appear in the pediatric elbow is the capitellum. This ossification center generally appears between the first month and the 11th month in girls and between the first month and the 26th month in boys. The other ossification centers in the elbow appear in the following progression: radial head (3.8 to 4.5 years), medial epicondyle (5 to 6 years), olecranon (6 to 7 years), trochlea (9 to 10 years), and the lateral epicondyle (10 years). Wilkins KE, Beaty JH, Chambers HG, et al: Fractures and dislocation of the elbow region, in Rockwood CA, Green DP, Bucholz RW, et al (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 657-662.
References:
- Haraldsson S: On osteochondrosis deformans juvenilis capituli humeri including investigation of the intra-osseous vasculature in the distal humerus. Acta Orthop Scand 1959;38:1-232.
Question 98High Yield
During cemented total hip arthroplasty, peak pulmonary embolization of marrow contents occurs when the
Explanation
Peak embolization is observed during femoral stem insertion. Embolization is also observed during acetabular preparation and hip reduction. Lewallen DG, Parvizi J, Ereth MH: Perioperative mortality associated with hip and knee arthroplasty, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 119-127.
Question 99High Yield
Figure 9 shows the AP radiograph of a 65-year-old man who has knee pain and swelling. What is the most likely diagnosis?
Explanation
Although all the choices are known causes of joint degeneration (secondary osteoarthritis), only chondrocalcinosis shows distinct linear calcification of the cartilage due to deposition of calcium pyrophosphate crystals. Gout is a recurrent acute arthritis resulting from the deposition of monosodium urate from supersaturated hyperuricemic body fluids. Hemochromotosis is characterized by focal or generalized deposition of iron within body tissues. Arthritis may be present but is less common than other manifestations such as liver cirrhosis, skin pigmentation, diabetes mellitus, and cardiac disease. Rheumatoid arthritis is a nonspecific, usually symmetric inflammation of peripheral joints resulting in destruction of articular and periarticular structures. Ochronosis is a hereditary enzyme deficiency (homogentisic acid oxidase) resulting in deposition of homogentisic acid polymers in articular cartilage. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 188.
Question 100High Yield
A 24-year-old man has right forearm pain after sliding head first into home plate. Examination reveals that the arm is swollen, but there are no neurovascular deficits or skin lacerations. Radiographs reveal a both-bone forearm fracture. The ulna has an oblique fracture with a 30% butterfly fragment, and the radius is comminuted over 75% of its circumference. In addition to reduction and plate fixation of both bones, management should consist of
Explanation
Explanation
The patient has a both-bone fracture with a comminuted radial shaft. Open reduction and internal fixation of both bones is the treatment of choice. In the past, Chapman and associates recommended bone grafting radial shaft fractures with more than 30% comminution of the circumference. This has remained the recommendation in most textbooks. More recent studies, where modern biologic plating techniques were used, found that the addition of bone graft to comminuted fractures was not necessary because the union rate did not differ from that of nongrafted comminuted fractures. Anderson LD, Sisk TD, Tooms RE, Park WI III: Compression-plate fixation in acute diaphyseal fractures of the radius and ulna. J Bone Joint Surg Am 1975;57:287-297. Chapman MW, Gordon JE, Zissimos AG: Compression-plate fixation of acute fractures of the diaphyses of the radius and ulna. J Bone Joint Surg Am 1989;71:159-169. Wright RR, Schmeling GJ, Schwab JP: The necessity of acute bone grafting in diaphyseal forearm fractures: A retrospective review. J Orthop Trauma 1997;11:288-294.
References:
- Wei SY, Born CT, Abene A, Ong A, Hayda R, Delong WG Jr: Diaphyseal forearm fractures treated with and without bone graft. J Trauma 1999;46:1045-1048.
You Might Also Like

Previous ChapterOrthopedic Board Review: Set 533 - 100 High-Yield MCQs for …
Next Chapter Orthopedic Surgery Board Review: 100 High-Yield MCQs | Mock…

Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon