Orthopedic Board Review Set 809: 100 High-Yield MCQs
14 Apr 2026
103 min read
81 Views
Key Takeaway
This page presents Mock Exam Set #809, featuring 100 randomized, high-yield Orthopedic Surgery Multiple Choice Questions (MCQs) designed for ABOS, OITE, and FRCS board exam preparation. Surgeons can utilize these practice questions to assess knowledge, identify gaps, and master critical concepts for exam success.
Femur Anterograde Intramedullary Nailing: A C...
00:00
Start Quiz
Question 1High Yield
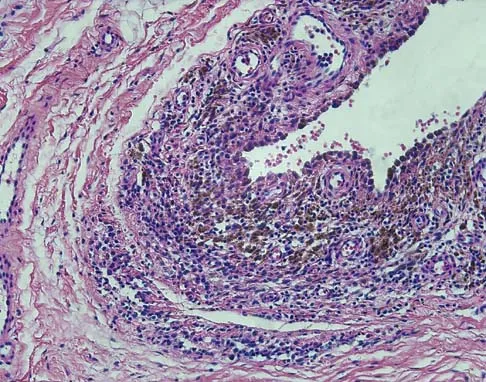
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function?
Explanation
Explanation
31b The radiograph and intraoperative photograph show osteonecrosis with near complete head loss/collapse. A stemmed implant is more appropriate in this patient because there is very little bone to support a resurfacing implant. In a younger patient, a glenoid implant should be delayed as long as possible because of the eventual need for revision secondary to glenoid loosening and wear, especially in a young active male. The hemiarthroplasty may be converted to a total shoulder arthroplasty in the future. Levy O, Copeland SA: Cementless surface replacement arthroplasty of the shoulder: 5- to 10-year results with the Copeland mark-2 prosthesis. J Bone Joint Surg Br 2001;83:213-221.
References:
- Burroughs PL, Gearen PF, Petty WR, et al: Shoulder arthroplasty in the young patient. J Arthroplasty 2003;18:792-798.
Question 2High Yield
A 60-year-old man with diabetes mellitus is referred for evaluation of nonhealing ulcers of his left foot. Nonsurgical management has failed to provide relief, and a below-the-knee amputation is being considered. Which of the following studies best predicts successful amputation wound healing?
Explanation
Explanation
The TcPO2 measures the O2 delivering capacity of the local vasculature. Values above 40 mm Hg have been shown to correlate with positive healing potential. The hemoglobin A1c is a good indicator of long-term glucose levels; however, it has no direct correlation with wound healing potential. Serum albumin is an indirect measure of nutritional status, and deficiencies in nutrition must be addressed before any surgery. Adequate hemoglobin levels are also necessary to promote adequate oxygenation to the amputation site. The ankle-brachial index may be falsely elevated as a result of calcified vessels in patients with diabetes mellitus. Wyss CR, Harrington RM, Burgess EM, et al: Transcutaneous oxygen tension as a predictor of success after amputation. J Bone Joint Surg Am 1988;70:203-207.
References:
- Dwars BJ,van den Broek TA, Rauwerda JA, et al: Criteria for reliable selection of the lowest level of amputation in peripheral vascular disease. J Vasc Surg 1992;15:536-542.
Question 3High Yield
Figure 16a shows the radiograph of a 34-year-old woman who sustained a basicervical fracture of the femoral neck. The fracture was treated with a compression screw and side plate. Seven months postoperatively, she continues to have significant hip pain and cannot bear full weight on her hip. A recent radiograph is shown in Figure 16b. Management should now consist of

Explanation
The patient sustained a high-angle femoral neck fracture. The follow-up clinical findings and radiograph show that she now has a nonunion with failed internal fixation. The joint appears preserved. In a healthy, young patient, arthroplasty of the femoral head, although possible, is not ideal. Excellent healing and function can be obtained in 70% to 80% of patients with femoral neck nonunion with a valgus intertrochanteric osteotomy. Marti RK, Schuller HM, Raaymakers EL: Intertrochanteric osteotomy for non-union of the femoral neck. J Bone Joint Surg Br 1989;71:782-787.
Question 4High Yield
A 32-year-old runner has pain in the medial arch that radiates into the medial three toes. He reports the presence of pain only when running. Examination reveals normal hindfoot alignment. There is a weakly positive Tinel's sign over the posterior tibial nerve. Tenderness is noted with palpation over the plantar medial area in the vicinity of the navicular tuberosity. What is the most likely diagnosis?
Explanation
The examination findings reveal that there is specific involvement of the medial plantar nerve by the distribution of the pain medially. The symptoms exclude the possibility of plantar fasciitis and anterior tibial tendinitis. Sinus tarsi syndrome would produce anterolateral symptoms rather than medial symptoms. Rask MR: Medial plantar neurapraxia (jogger's foot): Report of three cases. Clin Orthop 1978;134:193-195. Murphy PC, Baxter DE: Nerve entrapment of the foot and ankle in runners. Clin Sports Med 1985;4:753-763.
Question 5High Yield
A 25-year-old left hand-dominant man has severe left shoulder pain after being involved in a high-speed motor vehicle accident. Examination reveals that he is unable to move the left shoulder. His neurovascular status is intact in the entire left upper extremity. A radiograph is shown in Figure 19. What is the most appropriate surgical management of this injury?
Explanation
Explanation
In this young patient, every attempt must be made to retain the native proximal humerus; therefore, open reduction and internal fixation should be attempted of both the articular segment and tuberosities to the humeral shaft. This is best accomplished through an open approach. Shoulder arthroplasty should be reserved for the elderly and for failed internal fixation. Ko JY, Yamamoto R: Surgical treatment of complex fractures of the proximal humerus. Clin Orthop Relat Res 1996;327:225-237.
References:
- Aschauer E, Resch H: Four-part proximal humeral fractures: ORIF, in Warner JP, Iannotti JP, Flatow EL (eds): Complex and Revision Problems in Shoulder Surgery, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 289-309.
Question 6High Yield
A 30-year-old patient reports chronic medial knee pain and swelling. Figure 9a shows an articular cartilage lesion observed during arthroscopy. The surgeon decides to treat the lesion with the microfracture technique seen in Figure 9b. A biopsy of the repaired tissue 1 year after treatment is likely to show which of the following findings?
Explanation
Explanation
9b Microfracture is a marrow stimulation technique where stem cells from the underlying subchondral bone marrow can form at the base of the lesion. The rationale for this technique is based on these cells differentiating into cells that will produce an articular cartilage repair. Biopsy findings in animals and humans have demonstrated primarily a fibrocartilagenous repair tissue and not articular cartilage. The collagen type found in hyaline or articular cartilage is of the type II variety. Fibrocartilage possesses mostly type I and III cartilage. Buckwalter JA, Mankin HJ: Articular cartilage: Degeneration and osteoarthritis, repair, regeneration, and transplantation. Instr Course Lect 1998;47:487-504.
References:
- Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 471-488.
Question 7High Yield
The spring ligament of the foot connects what two bones?
Explanation
Explanation
The spring ligament is also known as the calcaneonavicular ligament and connects the calcaneus to the navicular. This ligament supports the talar head and is an important anatomic supporting structure of the medial longitudinal arch of the foot. Choi K, Lee S, Otis JC, et al: Anatomical reconstruction of the spring ligament using peroneus longus tendon graft. Foot Ankle Int 2003;24:430-436.
Question 8High Yield
A 42-year-old man reports a 12-month history of a painful fusiform swelling of the Achilles tendon. Physical therapy, heel lifts, and anti-inflammatory drugs have failed to provide relief. MRI scans are shown in Figures 44a and 44b. What is the treatment of choice?

Explanation
The area of the tendon degeneration is greater than 50% of the width so a supplemental tendon transfer is needed. Debridement and repair alone do not provide adequate strength. Injection risks tendon rupture. Brisement is indicated for peritendinitis, not tendinosis. Nonsurgical management is unlikely to be of benefit after 12 months. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 94-95.
Question 9High Yield
A patient with a left-sided C6-7 herniated nucleous pulposis would likely have which of the following constellation of findings?
Explanation
A C6-7 herniation affects the C7 root. The C7 root has the middle finger as its predominant sensory distribution. Its motor function is the triceps, wrist extension, and finger metacarpophalangeal extension. The reflex is the triceps. Magee D: Principles and concepts, in Orthopedic Physical Assessment, ed 3. Philadelphia, PA, WB Saunders, 1997, pp 1-18.
Question 10High Yield
A 23-year-old college basketball player reports persistent lateral ankle pain after sustaining an inversion injury 6 months ago. Examination reveals pain over the anterolateral ankle, absence of swelling, and no clinical instability. Management consisting of vigorous physical therapy fails to provide relief, and a intra-articular corticosteroid injection provides only temporary relief. Radiographs obtained at the time of injury and subsequent AP and varus stress views are normal. A recent MRI scan fails to show any abnormalities. Management should now include
Explanation
Explanation
Because the patient has failed to respond to appropriate nonsurgical management and imaging studies are normal, the use of arthroscopy not only aids in the diagnosis of chronic ankle pain, but is also helpful in its treatment. In patients with this condition, typical findings include synovitis in the lateral gutter and fibrosis along the talofibular articulation; syndesmosis chondromalacia of the talus and ankle also may be found. In patients with anterior soft-tissue impingement, approximately 84% who have a poor response to nonsurgical management will have a good to excellent response after arthroscopic synovectomy and debridement. Ferkel RD, Fasulo GJ: Arthroscopic treatment of ankle injuries. Orthop Clin North Am 1994;25:17-32.
References:
- Ferkel RD, Karzel RP, Del Pizzo W, Friedman MJ, Fischer SP: Arthroscopic treatment of anterolateral impingement of the ankle. Am J Sports Med 1991;19:440-446.
Question 11High Yield
What percent of patients initially diagnosed with classic, high-grade osteosarcoma of the extremity have visible evidence of pulmonary metastasis on CT of the chest?
Explanation
CT studies show that approximately 10% to 20% of patients with high-grade osteosarcoma have pulmonary metastases at diagnosis. Although not visible on current staging studies, it is believed that up to 80% of patients have micrometastatic disease that requires systemic chemotherapy. Because it is not possible to identify those patients who do not have disseminated micrometastatic disease, most patients are treated presumptively with chemotherapy. Kaste SC, Pratt CB, Cain AM, et al: Metastases detected at the time of diagnosis of primary pediatric extremity osteosarcoma at diagnosis: Imaging features. Cancer 1999;86:1602-1608.
Question 12High Yield
A 14-year-old boy sustained a femoral neck fracture in a fall from a tree and underwent open reduction and internal fixation 6 months ago. Follow-up examination now reveals an antalgic Trendelenburg gait and painful range of motion. A radiograph is shown in Figure 23, and a CT scan shows a nonunion. Treatment should consist of
Explanation
The coxa vara deformity and fracture nonunion should be treated simultaneously; therefore, the treatment of choice is curettage of the nonunion, intertrochanteric valgus osteotomy, and revision internal fixation. In addition, valgus osteotomy will convert the shear forces across the nonunion to compression, aiding in healing of the nonunion. None of the other procedures addresses both issues, and hip fusion is inappropriate under these conditions. Lam SF: Fractures of the neck of the femur in children. J Bone Joint Surg Am 1971;53:1165-1179.
Question 13High Yield
In the radiograph shown in Figure 42, the fracture pattern around this well-fixed stem is classified as Vancouver type
Explanation
The Vancouver classifications describes periprosthetic hip fractures in the following way. Type A fractures are in the trochanteric region. Type B1 fractures occur around the stem or at the tip in the face of a well-fixed stem. These are usually treated with open reduction and internal fixation, usually including struts, cable, and/or cable plates. Type B2 fractures occur in the same region with a loose stem. Type B3 fractures occur with a loose stem where the proximal bone is of poor quality and/or severely comminuted. Type C fractures occur well below the stem. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 149-154. Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol for proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.
Question 14High Yield
Which of the following is considered an important component in treating the lesion shown in Figure 56?
Explanation
Explanation
Mucoid cysts are commonly associated with DIP joint arthritis. Two treatment options are commonly used: (1) aspiration/drainage and injection of corticosteroid and (2) surgical excision. When performing the surgery, excision of the bony osteophytes about the DIP joint is helpful in achieving a cure. There are no reports of significant benefit with nail removal or partial ligament or extensor tendon resection. Some authors have advocated skin excision and rotational flaps for wound coverage, but this is somewhat controversial. Rizzo M, Beckenbaugh RD: Treatment of mucous cysts of the fingers: Review of 134 cases with minimum 2-year follow-up evaluation. J Hand Surg Am 2003;28:519-524.
References:
- Eaton RG, Dobranski AI, Littler JW: Marginal osteophyte excision in treatment of mucous cysts. J Bone Joint Surg Am 1973;55:570-574.
Question 15High Yield
What is the most common donor site complication following a free vascularized fibular graft for osteonecrosis of the femoral head?
Explanation
Urbaniak and Harvey reported donor site morbidity following free vascularized fibular graft in 198 consecutive patients. At a 5-year follow-up, they reported overall complications in 24% of the patients. The most common complication was a sensory deficit (11.8%), followed by motor weakness (2.7%), flexor hallucis longus contracture (2%), and deep venous thrombosis (less than 1%).
Question 16High Yield
A 39-year-old man has had persistent right shoulder pain for the past 6 months. A formal physical therapy program has failed to provide relief, and an injection several months ago provided only short-term relief. Examination reveals a positive Neer and Hawkins test. There is no instability and the neurovascular examination is normal. Arthroscopy reveals a partial rotator cuff tear on the bursal side measuring 60% of the tendon thickness. What is the next most appropriate step in management?
Explanation
Although arthroscopic debridement with or without subacromial decompression is a reasonable response, the patient has positive impingement signs. Several recent studies regarding the surgical treatment of partial rotator cuff tears have demonstrated good to excellent results after repair of tears involving more than 50% of the tendon thickness. This was shown specifically for bursal-sided tears and joint-side tears. Biceps tenotomy is not indicated in a young patient. Matava MJ, Purcell DB, Rudzki JR: Partial-thickness rotator cuff tears. Am J Sports Med 2005;33:1405-1417.
Question 17High Yield
Oxidation of polyethylene after sterilization occurs most rapidly when the implant undergoes
Explanation
The use of gamma radiation to sterilize polyethylene will result in the formation of free radicals in the material that increase the susceptibility of the material to oxidation and wear. The packaging can also have an impact. If the polyethylene is packaged in air, the oxygen in the packaging can significantly oxidize the material on the shelf prior to clinical use. Gas plasma and ethylene oxide sterilization do not appear to increase oxidation of polyethylene. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486. Wright TM: Ultra-high molecular weight polyethylene, in Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 37-46.
Question 18High Yield
A 35-year-old woman who is training for a triathlon has had a 2-month history of heel pain with weight bearing and is unable to run. History reveals that she is amenorrheic. Examination reveals that she is thin and has pain over the heel that is exacerbated with medial and lateral compression. Range of motion and motor and sensory function are normal. Radiographs are normal. What is the most likely diagnosis?
Explanation
Explanation
The most likely diagnosis is a stress fracture of the calcaneus and is supported by the history of running, female gender, and amenorrhea. Reproducing pain with medial and lateral compression of the heel also supports the diagnosis. A bone scan or MRI would most likely confirm the diagnosis. Plantar fasciitis would result in pain on the bottom of the heel with point tenderness. The lack of other areas of involvement or other symptoms does not support a seronegative inflammatory arthritis. Tarsal tunnel syndrome and peripheral neuropathy are unlikely because of the normal neurologic examination. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
References:
- Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 179-191.
Question 19High Yield
When compared to smokers who do not quit, an improvement in the rate of lumbar fusion is seen in patients who cease smoking for at least how many months postoperatively?
Explanation
Explanation
The effects of cigarette smoking and smoking cessation on spinal fusion have been studied extensively. Although permanent smoking cessation is ideal, significant improvements in fusion rates are seen in patients who avoid smoking for greater than 6 months postoperatively.
Question 20High Yield
Human tendons are made up primarily of what collagen type (~95%)?
Explanation
Explanation
Tendons are dense, primarily collagenous tissues that attach muscle to bone. Collagen content of the dry weight is slightly greater than that found in ligaments and is predominantly type I. Type III collagen makes up the remaining ~5% of total collagen content. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 10-12. Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 21-37.
References:
- Frank CB, Shrive NG, Lo IK, et al: Form and function of tendon and ligament, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 21High Yield
What is the most accurate description of the relationship between gender and knee loading during landing while playing basketball?
Explanation
Explanation
Ford and associates studied 81 high school basketball players and found that females landed with greater total valgus knee loading and a greater maximum valgus knee angle than male athletes. Hewett and associates reported in a study of 205 female athletes that those with increased dynamic valgus and high abduction loads were at increased risk of anterior cruciate ligament injury. Hewett TE, Myer GD, Ford KR, et al: Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am J Sports Med 2005;33:492-501.
References:
- Ford KR, Meyer GD, Hewett TE: Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exer 2003;35:1745-1750.
Question 22High Yield
A 10-year-old boy who is active in soccer has had activity-related heel pain for the past 3 months. Examination reveals tenderness over the posterior heel and a tight Achilles tendon. Radiographs demonstrate a 2-cm cyst in the anterior body of the calcaneus. His physes have not closed. Based on these findings, what is the most appropriate management?
Explanation
Explanation
The most likely diagnosis is Sever's disease, which is considered either an apophysitis or a para-apophyseal stress fracture. It is common in athletic children and is associated with a tight Achilles tendon. Cast immobilization may be necessary if activity reduction fails. Calcaneal cysts are quite common and do not require any further diagnostic testing or treatment unless they occupy the full width of the calcaneus or one third of the length of the calcaneus. Ogden JA, Ganey TM, Hill JD, et al: Sever's injury: A stress fracture of the immature calcaneal metaphysis. J Ped Orthop 2004;24:488-492.
References:
- Pogoda P, Priemel M, Linhart W, et al: Clinical relevance of calcaneal bone cysts: A study of 50 cysts in 47 patients. Clin Orthop Relat Res 2004;424:202-210.
Question 23High Yield
When performing an arthroscopic subacromial decompression, bleeding can be encountered when dividing the coracoacromial ligament because of injury to what artery?
Explanation
The acromial branch of the thoracoacromial trunk courses along the coracoacromial ligament. This artery enters the ligament approximately 5 mm below the acromial edge. Division of the ligament at its insertion on the acromion minimizes the risk of bleeding. Esch JC, Baker CL: Arthroscopic anatomy and normal variations, in Whipple TL (ed): Surgical Arthroscopy: The Shoulder and Elbow. Philadelphia, PA, JB Lippincott, 1993, pp 63-76.
Question 24High Yield
A 6-year-old child has a fixed flexion deformity of the interphalangeal (IP) joint of the right thumb. The thumb is morphologically normal, with a nontender palpable nodule at the base of the metacarpophalangeal joint. Clinical photographs are shown in Figures 42a and 42b. Based on these findings, what is the treatment of choice?

Explanation
The child has a trigger thumb deformity. A trigger thumb is a developmental mechanical problem rather than a congenital deformity. The anomaly generally is not noted at birth. A fixed flexion deformity of the IP joint of the thumb most commonly occurs in children in the first 2 years of life. A stretching and splinting program may correct the deformity in the first year of life, but nonsurgical management after age 3 years results in a success rate of only 50%. Release of the proximal annular pulley of the flexor sheath is recommended at this age. Tan AH, Lam KS, Lee EH: The treatment outcome of trigger thumb in children. J Pediatric Orthop B 2002;11:256-259. Slakey JB, Hennrikus WL: Acquired thumb flexion contracture in children: Congenital trigger thumb. J Bone Joint Surg Br 1996;78:481-483.
Question 25High Yield
Which of the following statements best describes synovial fluid?
Explanation
Synovial tissue is composed of vascularized connective tissue that lacks a basement membrane. Two cell types (type A and type B) are present: type B cells produce synovial fluid. Synovial fluid is made of hyaluronic acid and lubricin, proteinases,and collagenases. It is an ultrafiltrate of blood plasma added to fluid produced by the synovial membrane. It does not contain erythrocytes, clotting factors, or hemoglobin. It lubricates articular cartilage and provides nourishment via diffusion. Synovial fluid exhibits non-Newtonian flow characteristics. The viscosity coefficient is not a constant, the fluid is not linearly viscous, and its viscosity increases as the shear rate decreases.
Question 26High Yield
Figures 43a and 43b show the clinical photographs of a 4-month-old child with bilateral popliteal pterygium. The fixed knee contractures measure 100 degrees bilaterally. What future treatment is most likely to successfully correct this deformity?
Explanation
Explanation
43b Congenital popliteal webbing with contractures of 60 degrees is a difficult deformity to correct. The anatomy of the web is of considerable importance. MRI can delineate the extent of the posterior fibrous band that often stretches from the ischium to the calcaneus. The sciatic nerve, usually shortened, most often runs just anterior to this fibrous band. For mild contractures of less than 20 degrees, nonsurgical management is usually adequate. Hamstring lengthening and postoperative splinting are usually sufficient for contractures of 20 degrees to 40 degrees. Moderate contractures of up to 60 degrees usually require Z-plasties in the popliteal fossa and postoperative serial casting to avoid undue tension on neurovascular structures. Contractures of more than 60 degrees require a femoral shortening osteotomy or gradual correction with an external fixator. However, rapid recurrence following fixator removal is common if formal soft-tissue procedures and postoperative splinting are not performed. Parikh SN, Crawford AH, Do TT, et al: Popliteal pterygium syndrome: Implications for orthopaedic management. J Pediatr Orthop B 2004;13:197-201.
References:
- Brunner R, Hefti F, Tgetgel JD: Arthrogrypotic joint contracture at the knee and foot: Correction with a circular frame. J Pediatr Orthop B 1997;6:192-197.
Question 27High Yield
During the evaluation of a patient suspected of having a lumbar disk herniation, T1- and T2-weighted MRI scans reveal a hyperintence lobular, well-defined lesion in the L2 vertebral body. What is the most likely diagnosis?
Explanation
The findings are characteristic of hemangioma. When the hemangioma is large enough, vertical striations may be visible on plain radiographs. Axial CT scans commonly reveal a speckled appearance. Metastatic lesions are typically hypointense on T1-weighted images because they replace the fatty marrow. Bony islands, like cortical bone, are dark on T1- and T2-weighted images. Intravertebral disk herniation would have characteristics similar to the disk and be in continuity with the disk. Osteoporosis is more diffuse. Ross JS, Masaryk TJ, Modic MT, Carter JR, Mapstone T, Dengel FH: Vertebral hemangiomas: MR imaging. Radiology 1987;165:165-169.
Question 28High Yield
Figures 32a and 32b show the radiographs of a 13-year-old right hand-dominant boy who sustained a closed Salter-Harris type II fracture of the proximal humerus during a hockey game. The shoulder has significant swelling, but is neurovascularly intact. What treatment offers the best chance of reestablishing normal shoulder motion?

Explanation
The patient has a significantly angulated proximal humerus fracture with a high degree of varus angulation, and rotational malalignment is likely. Failure to correct the varus angulation will result in permanent loss of shoulder abduction because the patient's age limits bony remodeling. These fractures are inherently unstable due to the inability to control the proximal fracture alignment. Shoulder spica casts have a high rate of redisplacement after treatment. Adequate open or closed reduction and pin fixation in the operating room optimizes alignment and all but eliminates the chance of redisplacement. Dobbs MB, Luhmann SJ, Gordon JE, et al: Severely displaced proximal humerus epiphyseal fractures. J Pediatr Orthop 2003;23:208-215. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, p 701.
Question 29High Yield
An 11-year-old girl sustained an injury to her right foot when a 500-lb headstone fell on it. The headstone was removed after 3 minutes. Radiographs show multiple midfoot fractures. Examination reveals severe pain that is worse with passive toe motion. Clinical photographs are shown in Figure 28. Management should consist of
Explanation
The patient has a classic history and examination for an acute compartment syndrome of the foot. CT, MRI, or stress radiographs are not necessary prior to emergent fasciotomies of the foot. These studies can be performed after the initial fasciotomies to determine the best long-term management of the fractures. There are nine compartments in the foot. These are decompressed through three incisions (two on the dorsal foot and one medially). A short leg cast does not address the compartment syndrome and could be limb threatening with excessive swelling in a circumferential cast. It is preferable to splint severe crush injuries rather than apply a cast. Fulkerson E, Razi A, Tejwani N: Review: Acute compartment syndrome of the foot. Foot Ankle Int 2003;24:180-187.
Question 30High Yield
Examination of a hand with compartment syndrome is most likely to reveal which of the following?
Explanation
In a study of 19 patients with compartment syndrome of the hand, all had tense swollen hands with elevated compartment pressures. Most patients were neurologically compromised so pain with passive stretch may be difficult to illicit. Arterial inflow is present in the arch and thus pallor is not present. The typical posture of the hand is not clenched, rather it is an intrinsic minus posture of metacarpophalangeal joint extension and flexion of the proximal and distal interphalangeal joints. Oullette EA, Kelly R: Compartment syndromes of the hand. J Bone Joint Surg Am 1996;78:1515-1522.
Question 31High Yield
A 65-year-old woman fell onto her outstretched right arm and immediately had pain. She has a history of osteoporosis. Examination of the right arm reveals lateral arm swelling, ecchymosis, and she is unable to move the elbow due to pain. Her neurovascular status is intact. Radiographs are shown in Figures 14a and 14b. Appropriate treatment should include

Explanation
Comminuted, displaced radial head fractures (Hotchkiss type 3) require anatomic metallic radial head arthroplasty to regain function. Radial head excision has led to catastrophic sequelae including chronic wrist pain, elbow instability, and proximal radius migration. Immobilization, internal fixation, or anconeus arthroplasty are not recommended at this time because of the potentially poorer outcomes. Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
Question 32High Yield
A 66-year-old man reports a 2-week history of worsening low back and leg pain. He reports that his pain is aggravated by lying down and relieved by standing and walking. He notes that he has been losing weight recently and that his pain has been awakening him during the night. His medical history is significant for hypertension, coronary artery disease, and prostate cancer. His physical examination is essentially unremarkable. Lumbar radiographs are within normal limits. What is the most appropriate management for this patient?
Explanation
In the initial assessment of acute low back pain in adults, no diagnostic testing is indicated during the first 4 weeks in the absence of "red flags" for a serious underlying condition. The purpose of the initial assessment of acute low back pain in adults is to rule out serious underlying conditions presenting as low back pain. The Agency for Healthcare Policy and Research, in its 1994 clinical practice guideline, identified four serious conditions that may present with low back pain, including fracture, tumor, infection, and cauda equina syndrome. This patient has five "red flags" for a spinal tumor as a possible etiology of his low back pain, including age of older than 50 years, constitutional symptoms (recent weight loss), pain worse when supine, severe nighttime pain, and a history of cancer. Of these, his history of cancer is most significant, as greater than 90% of spinal tumors are metastatic. In order of frequency, breast, prostate, lung, and kidney make up approximately 80% of all secondary spread to the spine. In the presence of "red flags" for tumor or infection, it is recommended that the clinician obtain a CBC count, ESR, and a urinalysis. If these are within normal limits and suspicions still remain, consider consultation or seek further evidence with a bone scan, radiographs, or additional laboratory studies. Negative radiographs alone are insufficient to rule out disease. If radiographs are positive, the anatomy can be better defined with MRI. Agency for Health Care Policy and Research, Bigos SJ (ed): Acute Low Back Problems in Adults. Rockville, MD, US Department of Health and Human Services, AHCPR Publication 95-0642, Clinical Practice Guideline #14, 1994.
Question 33High Yield
Figure 12 shows a lateral radiograph of the elbow. What is the most likely diagnosis?
Explanation
Explanation
The figure shows a supracondylar process, which is a normal anatomic variant. An osteochondroma tends to occur more toward the end of bones, and the medullary space of the underlying bone extends into the base of the osteochondroma. The presence of a supracondylar process is usually asymptomatic. However, the ligament of Struthers that always extends from the supracondylar process to the medial epicondyle can result in median nerve entrapment secondary to trauma. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 132-133.
References:
- Keats TE, Anderson MW: Atlas of Normal Roentgen Variants That May Simulate Disease, ed 7. St Louis, MO, Mosby Inc, 2001, p 497.
Question 34High Yield
Figures 13a and 13b show the MRI scans of a 70-year-old patient who has a posterior calf mass. Examination reveals that the mass extends to the midcalf level. A biopsy specimen reveals a high-grade soft-tissue sarcoma. Metastatic work-up shows no lesions. Management should consist of

Explanation
Soft-tissue sarcomas generally are treated with radiation therapy and wide surgical resection. In this patient, involvement of most of the posterior calf compartment and circumferential involvement of the posterior tibial and peroneal neurovascular bundle makes limb salvage impractical. Any attempt at wide surgical resection would leave a poorly functioning limb with questionable surgical margins. A high below-knee amputation would be the best option. Radiation therapy alone is contraindicated. Lindberg RD, Martin RG, Romsdahl MM, et al: Conservative surgery and post-operative radiotherapy in 300 adults with soft tissue sarcoma. Cancer 1981;47:2391-2397. Sim FT, Frassica FS, Frassica DA: Soft tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 35High Yield
A 35-year-old man sustained a 10% compression fracture of the C5 vertebra in a diving accident. Radiographs show good alignment, and examination reveals no neurologic compromise. An MRI scan reveals no significant soft-tissue disruption posteriorly. Management should consist of
Explanation
Explanation
The patient has a stable flexion-compression injury of the cervical spine. The fracture occurs as a result of compression failure of the vertebral body. If the force continues, a tension failure of the posterior structures occurs, leading to potential dislocation. Immobilization in a rigid cervical orthosis will allow this fracture to heal. Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 457-464.
References:
- Allen GL, Ferguson RL, Lehmann TR, O'Brien RP: A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27.
Question 36High Yield
A 68-year-old man fell off a 20-foot mountain cliff and was seen in the emergency department the following morning. A radiograph is shown in Figure 12. He is a nonsmoker with medical comorbidities of hypertension and hypercholesterolemia that is well controlled with medicine and diet. Capillary refill and sensation are intact distally and the patient is able to move his toes with mild discomfort. Serosanguinous fracture blisters are present laterally, and the foot is swollen and red. What is the most appropriate management?
Explanation
Whereas a patient age of older than 50 years used to be a contraindication for open reduction and internal fixation of displaced intra-articular calcaneal fractures, new data suggest that the presence of associated medical comorbidities that affect wound healing such as smoking, diabetes mellitus, and peripheral vascular disease are more relevant to postoperative functional outcome. Surgical treatment of Sanders II and III displaced intra-articular calcaneal fractures with initial Bohler angles of > 15 degrees results in better outcomes as compared to nonsurgical management. Indications for primary fusion might include Sanders IV fractures in which articular congruity or Bohler angles cannot be restored. Given the condition of the soft tissues at presentation, delayed fixation is recommended. Herscovici D Jr, Widmaier J, Scaduto JM, et al: Operative treatment of calcaneal fractures in elderly patients. J Bone Joint Surg Am 2005;87:1260-1264. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Question 37High Yield
A 25-year-old student sustains the injury shown in Figures 13a through 13c after falling off a curb. Initial management should consist of
Explanation
Explanation
13b 13c The radiographs reveal a fracture entering the 4-5 intermetatarsal articulation, consistent with a zone 2 injury. This classically is also referred to as a Jones fracture. The history and radiographic findings indicate this is an acute fracture, which guides management. A zone 1 fracture enters the fifth tarsometatarsal joint, and a zone 3 fracture is a proximal diaphyseal fracture distal to the 4-5 articulation. Initial management is usually nonsurgical and consists of non-weight-bearing in a short leg cast. This method has been shown to result in a better healing rate compared to weight bearing as tolerated. Rosenberg GA, Sterra JJ: Treatment strategies for acute fractures and nonunions of the proximal fifth metatarsal. J Am Acad Orthop Surg 2000;8:332-338.
References:
- Lawrence SJ, Botte MJ: Jones' fracture and related fractures of the proximal fifth metatarsal. Foot Ankle 1993;14:358-365.
Question 38High Yield
Which of the following represents a contraindication for interspinous process decompression for the treatment of lumbar spinal stenosis?
Explanation
Kondrashov and associates noted stable good outcomes at 4 years in 14 of 18 patients treated with X-STOP interspinous process decompression as defined as an improvement over preoperative Oswestry scores of 15 points or more. Similar results were seen after 1 year in a European study by Siddiqui and associates. Exclusion and inclusion criteria for these studies varied somewhat, but cauda equina syndrome was the only exclusion criteria listed in both studies. All of the other choices did not represent exclusion criteria in either study. Kondrashov DG, Hannibal M, Hsu KY, et al: Interspinous process decompression with the X-STOP device for lumbar spinal stenosis: A 4-year follow-up study. J Spinal Disord Tech 2006;19:323-327.
Question 39High Yield
An 11-year-old girl has wrist pain. Figure 4a shows the radiograph, and Figures 4b and 4c show the low- and medium-power photomicrographs of a lesion in the distal radius. What is the most likely diagnosis?
Explanation
Explanation
4b 4c The radiograph shows an osteolytic eccentric lesion in the metaphyseal-diaphyseal region of the bone, and the photomicrographs show an aneurysmal bone cyst. The low-power photomicrograph shows large empty spaces with fibrous stroma and multinucleated giant cells. The red area in the center is hemorrhage in the stroma. The large empty spaces are cysts, which would be filled with blood in vivo. The medium-power photomicrograph shows a large cyst-like space and hemorrhage in the surrounding stoma. Giant cell tumors have "sheets" of giant cells. A nonossifying fibroma would have spindle cells, and a unicameral bone cyst may have a few giant cells, but blood is rare. Springfield DS, Gebhardt MC: Bone and soft tissue tumors, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 540-542.
References:
- Herring JA: Tachdjian's Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, pp 1906-1909.
Question 40High Yield
Figures 49a and 49b show MRI scans of the shoulder. What is the most likely diagnosis?

Explanation
The supraspinatus tendon shows clear detachment and retraction from its greater tuberosity attachment by the absence of the normal dark subacromial signal extending to the attachment on the greater tuberosity. There is no anterior inferior glenoid labral detachment that usually is seen in a Bankart lesion. The acromioclavicular joint shows no evidence of separation. The humeral head is migrated cranially, indicating a chronic rotator cuff tear. Iannotti JP, Zlatkin MB, Esterhai JL, Kressel HY, Dalinka MK, Spindler KP: Magnetic resonance imaging of the shoulder: Sensitivity, specificity, and predictive value. J Bone Joint Surg Am 1991;73:17-29. Seeger LL, Gold RH, Bassett LW, Ellman H: Shoulder impingement syndrome: MR findings in 53 shoulders. Am J Roentgenol 1988;150:343-347.
Question 41High Yield
Which of the following forms of nonsurgical management is considered best for acute low back pain without radiculopathy?
Explanation
Explanation
Temporary bed rest (less than 4 days) with gradual resumption of activities can be efficacious. Epidural steroid injections may be indicated for acute low back pain with radiculopathy. Acupuncture, facet joint injections, or ligamentous (sclerosant) injections are not indicated. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, Appendix A15.
References:
- Helfgott SM: Sensible approach to low back pain. Bull Rheum Dis 2001;3:50.
Question 42High Yield
A 22-year-old skier reports painful range of motion in the left thumb after falling forward on his outstretched hand while holding his ski pole. Examination of the left thumb reveals increased AP laxity and 45 degrees of valgus laxity at the metacarpophalangeal (MCP) joint. Examination of the right thumb shows 25 degrees of valgus laxity at the MCP joint. Radiographs are normal. Management should consist of
Explanation
Explanation
The patient has a complete tear of the ulnar collateral ligament as defined by MCP joint laxity of greater than 30 degrees (or 15 degrees greater laxity compared with the opposite side). Primary repair is the treatment of choice because displacement of the ligament superficial to the adductor aponeurosis (Stener lesion) must be corrected. Any volar plate injury can be addressed during repair of the ulnar collateral ligament.
References:
- Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint. J Am Acad Orthop Surg 1997;5:224-229.
Question 43High Yield
A 10-year-old child has leg discomfort with activity. A radiograph, bone scan, and biopsy specimen are shown in Figures 1a through 1c. What is the most likely diagnosis?
Explanation
Explanation
1b 1c The ground glass appearance on the radiograph, the hot bone scan, and histologic findings of bony spicules without osteoblastic rimming in a background of bland fibrous tissue all suggest fibrous dysplasia. Stress-related pain is common with activity because of the dysplastic bone. Parosteal osteosarcomas are surface lesions. Simple cysts, aneurysmal bone cysts, and eosinophilic granuloma are all possible radiographically; however, the histology is most consistent with fibrous dysplasia. Harris WH, Dudley HR Jr, Barry RS: The natural history of fibrous dysplasia: An orthopaedic, pathological and roentgenographic study. J Bone Joint Surg Am 1962;44:207.
References:
- Campanacci M: Bone and Soft Tissue Tumors. Vienna, Austria, Springer-Verlag, 1990.
Question 44High Yield
Figure 54 shows the preoperative radiograph of a 45-year-old woman who is considering total hip arthroplasty with her orthopaedic surgeon. What femoral characteristic is a typical concern in this patient?
Explanation
Explanation
Developmental dysplasia of the hip (DDH) leads to early arthritis of the hip as seen in this patient. Although DDH is believed to mostly affect the acetabulum, most patients with DDH also have anatomic aberrations of the femur. Using three-dimensional computer models generated by reconstruction of CT scans, dysplastic femurs were shown to have shorter necks and smaller, straighter canals than the controls. The shape of the canal became more abnormal with increasing subluxation. The studies also have shown that the primary deformity of the dysplastic femur is rotational, with an increase in anteversion of 5 degrees to 16 degrees, depending on the degree of subluxation of the hip. The rotational deformity of the dysplastic femur arises within the diaphysis between the lesser trochanter and the isthmus and is not attributable to a torsional deformity of the metaphysis. Osteopenia is not a concern in a patient with an excellent cortical index (thick cortices and narrow canal). Femoral varus or bowing of the femur is not a typical finding in patients with DDH. Noble PC, Kamaric E, Sugano N, et al: Three-dimensional shape of the dysplastic femur: Implications for THR. Clin Orthop 2003;417:27-40.
References:
- Sugano N, Noble PC, Kamaric E, et al: The morphology of the femur in developmental dysplasia of the hip. J Bone Joint Surg Br 1998;80:711-719.
Question 45High Yield
A 60-year-old woman reports anterior knee pain 2 years after undergoing primary total knee arthroplasty for rheumatoid arthritis. A Merchant view of the patella is shown in Figure 16. What is the most likely cause of her pain?
Explanation
Patellar complications commonly occur after primary total knee arthroplasty; therefore, proper component positioning is critical in obtaining a successful result. This patient has lateral tilting and subluxation of the patellar component. Internal rotation of the femoral component has the most deleterious effect on patellar tracking. Lateral placement of the femoral component, medial placement of the patellar component, and external rotation of the tibial component have beneficial effects on patellar tracking. Elevation of the joint line, if not excessive, should not impact patellar tracking. Rand JA: Patellar resurfacing in total knee arthroplasty. Clin Orthop 1990;260:110-117.
Question 46High Yield
What is the primary benefit of using rhBMP-2 instead of autogenous bone graft inside an anterior spinal fusion cage?
Explanation
Radiographic fusion success rates are best described as slightly rather than substantially improved. Hospital stay and time to fusion also are not substantially decreased. Use of BMP does eliminate the need for autograft harvest for anterior lumbar interbody fusion/cage. The need for postoperative bracing is not altered based on graft choice. Early studies of posterolateral fusion applications appear to show a greater potential benefit of rhBMP-2 over autograft. Not all BMP formulations perform the same with regard to safety and effectiveness. Other osteoinductive proteins in clinical trials (BMP-7, GDF-5) will require individual analysis of these properties.
Question 47High Yield
A 23-year-old man sustained an injury to his left foot when a forklift rolled over it at work. Examination reveals marked swelling of the midfoot and forefoot, with tenderness to palpation over the medial hindfoot and dorsomedial forefoot. The distal dorsalis pedis pulse is audible on Doppler examination, and his sensation is intact to touch. Radiographs are shown in Figures 33a and 33b. Management should consist of

Explanation
The best results after dislocations of the tarsometatarsal joints are seen with anatomic reduction; this is best achieved by open reduction and maintained with internal fixation with either pins or screws. Open reduction provides a means of debriding small bony fragments from the joint and allowing direct inspection of the reduction. Associated crush or shearing fractures of the cuboid or tarsal navicula are signs that suggest a Lisfranc injury. Because patients can function quite well despite the development of arthrosis in the Lisfranc joint, primary arthrodesis is not indicated in the management of this injury. Resch S, Stenstrom A: The treatment of tarsometatarsal injuries. Foot Ankle 1990;11:117-123. Schenck RC Jr, Heckman JD: Fractures and dislocations of the forefoot: Operative and nonoperative treatment. J Am Acad Orthop Surg 1995;3:70-78.
Question 48High Yield
Figure 26 shows the radiograph of an otherwise healthy Caucasian 5-year-old boy who has a painless limp. What is the best treatment option?
Explanation
The prognosis of Legg-Perthes disease in children younger than age 6 years is good. There is no indication that surgical treatment will improve the outcome. Range-of-motion exercises to prevent contracture may be helpful. Herring JA, Kim HT, Browne R: Legg-Calve-Perthes disease: Prospective multicenter study of the effect of treatment on outcome. J Bone Joint Surg Am 2004;86:2121-2134.
Question 49High Yield
What arterial vessel is most prone to injury during posterior iliac crest bone graft harvest?
Explanation
The superior gluteal artery is most at risk with a posterior iliac crest bone graft harvest. The artery leaves the pelvis through the sciatic notch and can be injured by retractors or other sharp instruments entering the sciatic notch area. The deep circumflex iliac, iliolumbar, and fourth lumbar arteries supply the iliacus and iliopsoas muscles and can be damaged during anterior bone graft harvest. The ascending branch of the lateral femoral circumflex artery is at risk during the anterior approach to the hip. Guyer RD, Delmarter RB, Fulp T, Small SD: Complications of cervical spine surgery, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 547. Kurz LT, Garfin SR, Booth RE Jr: Iliac bone grafting: Techniques and complications of harvesting, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 330-331.
Question 50High Yield
A distal radius fracture in an elderly man is strongly predictive for what subsequent injury?
Explanation
Fractures of the distal radius increase the relative risk of a subsequent hip fracture significantly more in men than in women. A previous spinal fracture has an equally important impact on the risk of a subsequent hip fracture in both genders.
Question 51High Yield
A 20-year-old athlete sustains a 2- x 3-cm grade IV chondral injury to the right knee. After failure of nonsurgical management, which of the following procedures would ensure the highest percentage of hyaline-like cartilage?
Explanation
Explanation
Autologous chondrocyte implantation was first reported by Brittberg in 1994 and has resulted in predominantly type II collagen (hyaline-like articular cartilage) in the repair tissue. The extracellular matrix in articular cartilage is made up primarily of type II collagen, proteoglycans, and water. Arthroscopic chondroplasty, microfracture, drilling, and abrasion arthroplasty all result eventually in fibrocartilage fill of the defect (predominantly type I collagen). Brittberg M, Lindahl A, Nilsson A, et al: Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med 1994;331:889-895.
References:
- Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 787-804.
Question 52High Yield
A 14-year-old boy reports pain in the distal thigh. He denies any history of trauma. Examination reveals tenderness and swelling of the distal thigh without effusion. A radiograph and CT scan are shown in Figures 10a and 10b. A biopsy specimen is shown in Figure 10c. Management should consist of
Explanation
Explanation
10b 10c Based on these findings, the patient has an aneurysmal bone cyst. Frequently, fluid-fluid levels can be detected on MRI or CT images. The histologic results show a lesion that consists of cavernous spaces filled with blood. The lining of the cavity contains spindle cells, multinucleated giant cells, and reactive bone. Curettage and bone grafting is the preferred treatment method. Without treatment, these lesions can become quite large and destructive. Radiation therapy is not recommended for resectable lesions. Chemotherapy is not required for these benign lesions. Simon MA, Springfield DS, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-200.
References:
- Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, p 232.
Question 53High Yield
Figure 26 shows the radiograph of a 48-year-old woman who has right arm pain and hematuria. A bone scan reveals increased uptake in the left ribs and thoracic spine. A needle biopsy specimen shows that the lesion is highly keratin positive and composed primarily of clear cells. What is the best course of action?
Explanation
The lesion has the typical "blown out" lytic radiographic appearance that is most commonly found in thyroid or renal cell metastases. Given the history of hematuria and histology findings, the most likely diagnosis is metastatic renal cell carcinoma. This tumor is relatively resistant to chemotherapy. Radiation therapy is used as a postoperative adjuvant treatment with varying response rates. Surgery should be performed after preoperative embolization to decrease the risk of intraoperative bleeding, as no tourniquet can be used in this location. Patients with metastatic renal cell carcinomas may survive for years, resulting in a higher likelihood of local tumor progression with ineffective adjuvant therapy. Intramedullary fixation combined with curettage and cementation will provide the best chance of local control while maintaining the patient's native shoulder and elbow joints. A total humeral resection is an extensive surgery with considerable morbidity and is not indicated for this patient because less extensive surgery is likely to be effective. Harrington KD, Sim FH, Enis JE, Johnston JO, Diok HM, Gristina AG: Methylmethacrylate as an adjunct in internal fixation of pathological fractures: Experience with three hundred and seventy-five cases. J Bone Joint Surg Am 1976;58:1047-1054. Sun S, Lang EV: Bone metastases from renal cell carcinoma: Preoperative embolization. J Vasc Interv Radiol 1998;9:263-269.
Question 54High Yield
A 20-year-old man with fascioscapulohumeral dystrophy has severe scapular winging of both shoulders. He can no longer abduct above 80 degrees, and it affects his activities of daily living. A clinical photograph is shown in Figure 26. Definitive management should consist of
Explanation
The patient's history is typical of patients with severe fascioscapulohumeral dystrophy. The scapular winging can be so pronounced that there is significant loss of function of the upper extremity. The surgical options include transfer of the pectoralis major muscle with a tendon graft or scapulothoracic fusion. The latter is a technically demanding procedure but can provide a very stable platform for the upper extremity. Most patients will see increased elevation of the extremity once the scapula is stabilized. Pectoralis minor transfer has not been described and would not be effective. Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Question 55High Yield
A 62-year-old man who underwent total knee arthroplasty 6 months ago now reports pain after falling on the anterior portion of the knee. Examination reveals weakness of knee extension but no extensor lag. Flexion that had once measured 115 degrees is now limited to 70 degrees because of pain. A radiograph is shown in Figure 25. Management should now consist of
Explanation
The patient has a type IIIB patellar fracture (inferior pole fracture with an intact patellar tendon). Nonsurgical management is the treatment of choice if there is little displacement and the extensor mechanism is intact. Brown TE, Diduch DR: Fractures of the patella, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2, pp 1290-1312.
Question 56High Yield
A 19-year-old man who plays college volleyball undergoes a routine preparticipation physical examination. Figure 35 shows a posterior view of his dominant shoulder. An electromyogram shows that this is a chronic injury, and an MRI scan shows no abnormalities. The best course of action should be
Explanation
Explanation
Isolated palsy of the infraspinatus portion of the suprascapular nerve is common in volleyball players and is seen frequently in the throwing arm of baseball players. The exact cause is not known, but it may be the result of either tethering or traction on the nerve at the spinoglenoid notch. Synovial cysts in the spinoglenoid notch also can be a cause, but the patient's negative MRI findings rule out that entity. Because many isolated nerve palsies of the infraspinatus branch are asymptomatic, initial management should always be nonsurgical. Surprisingly, many athletes with this injury can participate fully in sports. Surgical treatment with decompression at the notch is unpredictable and generally is indicated only if nonsurgical management fails. Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
References:
- Martin SD, Warren RF, Martin TL, Kennedy K, O'Brien SJ, Wickiewicz TL: Suprascapular neuropathy: Results of non-operative treatment. J Bone Joint Surg Am 1997;79:1159-1165.
Question 57High Yield
Which of the following is considered the best measure of the adequacy of resuscitation in the first 6 hours after injury?
Explanation
The end point of resuscitation is adequate tissue perfusion and oxygenation. Blood lactate is the end point of anaerobic metabolism. The level of blood lactate reflects global hypoperfusion and is directly proportional to oxygen debt. Two separate prospective studies have verified a significant difference in mortality when blood lactate was used as a measure of resuscitation when compared to traditional parameters (mean arterial pressure, urine output, central venous pressure, and heart rate). Base deficit is a direct measure of metabolic acidosis and an indirect measure of blood lactate levels. It correlates well with organ dysfunction, mortality, and adequacy of resuscitation. It is easy to measure, can be obtained rapidly, and is an excellent assessment of the adequacy of resuscitation. Porter JM, Ivatury RR: In search of the optimal end points of resuscitation in trauma patients: A review. J Trauma 1998;44:908-914.
Question 58High Yield
A 75-year-old woman began a walking program 2 months after undergoing right total knee arthroplasty. She had to stop the program after 4 weeks because of hindfoot pain and ankle swelling. Radiographs are shown in Figures 42a and 42b. What is the most likely diagnosis?

Explanation
It is often tempting to assign a diagnosis of plantar fasciitis in patients with hindfoot pain. In this patient, the radiographs confirm a diagnosis of a calcaneal insufficiency fracture. The dense condensation of bone on the lateral view confirms the diagnosis. There is no radiographic evidence of a heel spur, osteochondral lesions, or chondrocalinosis. Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA, WB Saunders, 1995, p 2591. Kearon C: Natural history of venous thromboembolism. Semin Vasc Med 2001;1:27-37.
Question 59High Yield
Figures 24a through 24c show the coronal T1-weighted, T2-weighted fat-saturated, and T1-weighted fat-saturated gadolinium MRI scans of the proximal thigh of a 52-year-old woman who reports a mass in the medial thigh and groin area. She notes that the fullness has grown in size over the course of many months. Based on these findings, what is the most likely diagnosis?
Explanation
Explanation
24b 24c The images show a complex, lobular lesion of the thigh that has signal characteristics that follow fat. The size of the lesion, the areas of stranding within the mass, along with mild uptake on the gadolinium sequences and the mild edema within the lesion on the T2-weighted image make liposarcoma the most likely diagnosis and simple intramuscular lipoma far less likely. All other diagnoses listed would not follow fat characteristics shown on the MRI sequences.
References:
- Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Question 60High Yield
A 72-year-old woman who fell on her right shoulder while using a treadmill is now unable to elevate her right arm. An MRI scan is shown in Figure 7. What is the most likely diagnosis?
Explanation
Explanation
The MRI scan reveals a large chronic rotator cuff tear with retraction and fatty infiltration atrophy of the supraspinatus and infraspinatus tendons. This tear is responsible for the patient's severe weakness and inability to elevate the arm.
References:
- Gerber C, Myer DC, Schneeberger RP, et al: Effect of tendon release and delayed repair on the structure of the muscles of the rotator cuff: An experimental study in sheep. J Bone Joint Surg Am 2004;86:1973-1982.
Question 61High Yield
A 16-year-old girl has a painful foot mass. A radiograph, MRI scan, and biopsy specimens are shown in Figures 35a through 35d. What is the most likely diagnosis?
Explanation
Synovial sarcoma should always be considered in the differential diagnosis of a foot mass; however, the histopathology shows a typical example of PVNS, with hemosiderin, giant cells, and synovium. Synovial chondromatosis would have metaplastic cartilage in the synovium. The radiograph shows subtle erosion of the lateral cortex of the cuboid, and the MRI scan shows a soft-tissue mass. Ghert MA, Scully SP, Harrelson JM: Pigmented villonodular synovitis of the foot and ankle: A review of six cases. Foot Ankle Int 1999;20:326-330. Jones BC, Sundaram M, Kransdorf MJ: Synovial sarcoma: MR imaging findings in 34 patients. Am J Roentgenol 1993;161:827-830. Sartoris DJ, Resnick D: Magnetic resonance imaging of pediatric foot and ankle disorders. J Foot Surg 1990;29:489-494.
Question 62High Yield
What is the main benefit of using metal-backed tibial components in total knee arthroplasty?
Explanation
In a normal knee, the hard subchondral bone helps to distribute loads across the joint surface. A metal-backed tibial component in total knee arthroplasty decreases the compressive stresses on the underlying, softer cancellous bone by distributing the load over a larger surface area, particularly when one condyle is loaded. Although metallic base plates also increase the tensile forces on the other condyle when one is loaded and may decrease the thickness of the polyethylene tray, these are not benefits. Compressive forces on the polyethylene tray are increased with metal backing. The conformity of the articular surfaces is not affected by metal backing of the tibial component.
Question 63High Yield
If a laminectomy for spinal stenosis is performed, which of the following is an indication for concomitant arthrodesis at that level?
Explanation
Explanation
A prospective randomized study of patients with degenerative spondylolisthesis and spinal stenosis by Herkowitz and Kurz showed significantly improved clinical outcomes in patients who also received a lumbar arthrodesis. Patients with a laminectomy at an adjacent level do not have improved outcomes with an arthrodesis. Minimal lumbar scoliosis does not require arthrodesis. Arthrodesis is indicated in cases where there is removal of more than 50% of the facets bilaterally but not with an associated foraminal stenosis. Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-807.
References:
- Garfin SR, Rauschning W: Spinal stenosis. Instr Course Lect 2001;50:145-152.
Question 64High Yield
Patients who have osteonecrosis of the humeral head and who have the best prognosis are those with which of the following conditions?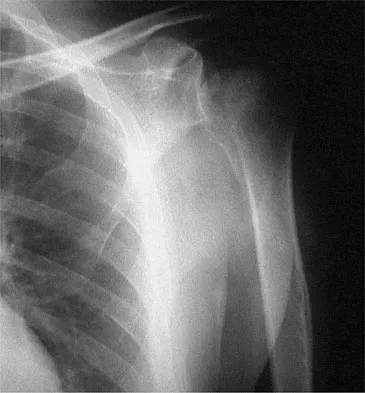
Explanation
The natural history of nontraumatic osteonecrosis varies greatly, so it is difficult to predict which patients will have severe arthrosis develop. Patients with sickle cell disease tend to have the most benign course. The most commonly reported cause of nontraumatic osteonecrosis is corticosteroid therapy. Fortunately, the incidence of osteonecrosis among patients treated with long-term systemic corticosteroids has fallen from more than 25% to less than 5% in recent years, owning to judicious steroid use and dosing. The interval between corticosteroid administration and the onset of shoulder symptoms is also variable, ranging from 6 to 18 months in one large series. This is comparable to the interval leading up to the onset of hip symptoms, which ranges from 6 months to 3 years or longer. The incidence of humeral head involvement has not been shown to vary with the underlying indication for steroid use. Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg 2002;11:281-298.
Question 65High Yield
A patient is scheduled to undergo total knee arthroplasty (TKA) following failure of nonsurgical management. History reveals that she underwent a patellectomy as a teenager as the result of a motor vehicle accident. Examination reveals normal ligamentous stability. For the most predictable outcome, which of the following implants should be used?
Explanation
Explanation
Paletta and Laskins performed a retrospective study of the results of TKA with cement in 22 patients who had a previous patellectomy. Nine of the patients had insertion of a posterior cruciate ligament-substituting implant. Thirteen patients had insertion of a posterior cruciate ligament-sparing implant. The 5-year postoperative knee scores were 89 for the posterior cruciate ligament-substituting knee versus 67 for the posterior cruciate ligament-sparing knee (P < 0.01). The patella functions to increase the lever arm of the extensor mechanism and to position the quadriceps tendon and the patellar ligament roughly parallel to the anterior cruciate ligament and posterior cruciate ligament, respectively. The patellar ligament thereby provides a strong reinforcing structure that functions to prevent excessive anterior translation of the femur during flexion of the knee. The absence of the patella results in the patellar ligament and the quadriceps tendon being relatively in line with one another. After a patellectomy, the resultant quadriceps force is no longer parallel to the posterior cruciate ligament. This results in loss of the reinforcing function of the patellar ligament. The authors believe this loss of reinforcing function may place increased stresses on the posterior cruciate ligament and posterior aspect of the capsule, which may result in stretching of these structures over time. They found a high rate of anteroposterior instability, a high prevalence of recurvatum, and a high rate of loss of full active extension compared with passive extension in the posterior cruciate ligament-sparing group, which supports their theory. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
References:
- Paletta GA Jr, Laskins RS: Total knee arthroplasty after a previous patellectomy. J Bone Joint Surg Am 1995;77:1708-1712.
Question 66High Yield
Which of the following nutraceuticals has been associated with perioperative bleeding?
Explanation
Ginkgo biloba is a popular nutraceutical for patients who have early dementia, intermittent claudication secondary to peripheral vascular disease, vertigo, and tinnitus. It is reported to improve mental alertness and cognitive deficiency. It has antiplatelet properties as a result of one of its components, ginkgolide B, which displaces platelet-activating factor from its receptor binding sight. Rowin and Lewis reported on spontaneous bilateral subdural hematomas associated with chronic ginkgo biloba ingestion. Vale also reported on subarachnoid hemorrhage associated with ginkgo biloba. Bebbington and associates reported on persistent postoperative bleeding after total hip arthroplasty secondary to ginkgo biloba usage. Furthermore, the use of ginkgo biloba with aspirin or other antiplatelet agents or anticoagulants represents a relative contraindication. Physicians should be aware not only of prescribed medications but also alternative nutraceuticals that are used by the patient. Rowin J, Lewis SL: Spontaneous bilateral subdural hematomas associated with chronic ginkgo biloba ingestion. Neurology 1996;46:1775-1776. Vale S: Subarachnoid hemorrhage associated with ginkgo biloba. Lancet 1998;352:36.
Question 67High Yield
A 64-year-old man who underwent total shoulder arthroplasty 4 weeks ago is making satisfactory progress in physical therapy, but his therapist notes limitations in external rotation to neutral. A stretching program is started, and the patient suddenly gains 90 degrees of external rotation but now reports increased pain and weakness. What is the best course of action?
Explanation
Explanation
Nearly all approaches to shoulder arthroplasty require detachment of the subscapularis tendon from the humerus and subsequent repair. Healing of this tenotomy is one of the limiting factors in postoperative recovery. Failure of the tenotomy repair must be recognized and treated early with repeat repair or pectoralis muscle transfer for optimal results. Failure of the subscapularis is diagnosed clinically as excessive external rotation and weakness, especially in the lift-off or belly press position. Muscle testing can be difficult in the postoperative period and may not be possible to assess in those positions. Although MRI might be useful to confirm the diagnosis, studies may be limited by artifact. CT or electromyography would not be diagnostic. Wirth MA, Rockwood CA Jr: Complications of total shoulder-replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
References:
- Miuer SL, Hazrati Y, Klepps S, et al: Loss of subscapularis function after shoulder replacement: A seldom recognized problem. J Shoulder Elbow Surg 2003;12:29-34.
Question 68High Yield
A 64-year-old man who was involved in a high-speed motor vehicle accident 6 weeks ago has been in the ICU with a closed head injury. Examination reveals that his range of motion for external rotation to the side is -30 degrees. Radiographs are shown in Figures 28a and 28b. What is the most likely diagnosis?

Explanation
The patient has a posterior shoulder dislocation. The AP radiograph shows overlapping of the humeral head on the glenoid. The scapular Y view shows his humeral articular surface posterior to the glenoid. The posterior shoulder dislocation is frequently missed because the patient is comfortable in the "sling" position with the arm adducted and internally rotated across the abdomen. The marked restriction in external rotation on examination raises the suspicion of a posterior dislocation, adhesive capsulitis, or glenohumeral osteoarthritis. The posterior dislocation is diagnosed based on the radiographic findings. An axillary view or CT is recommended to better evaluate the dislocation. Robinson CM, Aderinto J: Posterior shoulder dislocations and fracture-dislocations. J Bone Joint Surg Am 2005;87:639-650.
Question 69High Yield
A 39-year-old competitive cyclist sustains an injury to her left hip in a fall. Gadolinium arthrography, with an accompanying MRI scan, is shown in Figure 31. A cleft, or defect, identified by the arrow, indicates a detachment of the
Explanation
The area indicated by the arrow represents gadolinium contrast extending into a separation between the lateral labrum and its acetabular attachment. This can be a traumatic detachment, but occasionally a cleft may be present as a normal variant of the labral morphology. The capsular attachment of the iliofemoral ligament is peripheral to the labrum. The pulvinar is the common name applied to the fat and overlying synovium contained within the acetabular fossa above the ligamentum teres. The zona orbicularis is a circumferential thickening of the capsule around the femoral neck, and the retinacular vessels travel within the capsular synovium up the femoral neck to supply the femoral head. Petersilge CA, Haque MA, Petersilge WJ, Lewin JS, Lieberman JM, Buly R: Acetabular labral tears: Evaluation with MR arthrography. Radiology 1996;200:231-235. Czerny C, Hofmann S, Neuhold A, et al: Lesions of the acetabular labrum: Accuracy of MR imaging and MR arthrography in detection and staging. Radiology 1996;200:225-230.
Question 70High Yield
A knock-out mouse for the Vitamin D receptor has which of the following phenotypes?
Explanation
A knock-out mouse to the Vitamin D receptor would cause loss of vitamin D function, resulting in rickets. Renal failure would not occur; although Vitamin D is converted from 25 (OH) D to 1,25 (OH) D in the kidney, the active hormone acts on the gut and bone. Osteopetrosis can be seen as the phenotype for the c fos knock-out mouse; the Jansen-type metaphyseal dysplasia phenotype results from overactivation of the PTH/PTHrp receptor. Although compensatory hyperparathyroidism would occur, excessive PTH would not be able to rescue the skeletal loss and instead phosphoturia and phosphotasia would result. Glowacki J, Hurwitz S, Thornhill TS, et al: Osteoporosis and vitamin-D deficiency among postmenopausal women with osteoarthritis undergoing total hip arthroplasty. J Bone Joint Surg Am 2003;85:2371-2377.
Question 71High Yield
A 40-year-old woman sustains a flexion injury to her neck. Physical examination is normal. A lateral radiograph of the cervical spine is shown in Figure 57a. MRI scans of the cervical spine are shown in Figures 57b and 57c. Treatment should include
Explanation
Explanation
57b 57c This is a classic bilateral facet dislocation. When there is no evidence of a disk herniation, treatment should include careful skeletal traction, closed reduction, and posterior fusion. There is no role for anterior procedures. These fractures are unstable and require surgical intervention. Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 1120-1128.
Question 72High Yield
A 40-year-old woman with no history of back problems has a symptomatic L4-5 disk herniation with an L5 radiculopathy that has failed to respond to 12 weeks of nonsurgical management. In the preoperative discussion, the surgeon advises the patient that the chance of recurrence of the herniation after successful diskectomy is what percent?
Explanation
The incidence of recurrent disk herniation after a successful diskectomy is approximately 5% to 10%. Indications for surgical diskectomy for a recurrence are the same as for a primary diskectomy. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 685-698.
Question 73High Yield
A 68-year-old woman undergoes a complicated four-level anterior cervical diskectomy and fusion at C3-7 with iliac crest bone graft and instrumentation for multilevel cervical stenosis. Surgical time was approximately 6 hours and estimated blood loss was 800 mL. Neuromonitoring was stable throughout the procedure. The patient's history is significant for smoking. The most immediate appropriate postoperative management for this patient should include
Explanation
Explanation
Airway complications after anterior cervical surgery can be a catastrophic event necessitating emergent intubation for airway protection. Multilevel surgeries requiring long intubation and prolonged soft-tissue retraction as well as preexisting comorbidities may predispose a patient to postoperative airway complications. Sagi and associates reported that surgical times greater than 5 hours, blood loss greater than 300 mL, and multilevel surgery at or above C3-4 are risk factors for airway complications. In surgical procedures with the aforementioned factors, serious consideration should be given to elective intubation for 1 to 3 days to avoid urgent reintubation. Sagi HC, Beutler W, Carroll E, et al: Airway complications associated with surgery on the anterior cervical spine. Spine 2002;27:949-953. Epstein NE, Hollingsworth R, Nardi D, et al: Can airway complications following multilevel anterior cervical surgery be avoided? J Neurosurg 2001;94:185-188.
Question 74High Yield
When performing a flexor tendon repair of a digit other than the thumb, what structures of the flexor tendon sheath should be preserved?
Explanation
Explanation
The A2 and A4 pulleys are considered the most important parts of the pulley system. If these two structures are preserved, 80% of finger flexion can be maintained. If the pulley system is not left intact or is not reconstructed, "bow-stringing" of the flexor tendons occurs with loss of full flexion. The A2 pulley is over the proximal phalanx and the A4 pulley is over the middle phalanx. Doyle JR: Anatomy of the finger flexor tendon sheath and pulley system. J Hand Surg Am 1988;13:473-484.
References:
- Strickland JW: Flexor tendon injuries: I. Foundations of treatment. J Am Acad Orthop Surg 1995;3:44-54.
Question 75High Yield
A 20-year-old football player sustains a dorsiflexion external rotation injury to his right ankle. During sideline evaluation, which of the following findings best indicates a syndesmosis ankle sprain without diastasis?
Explanation
Explanation
The inability to single leg hop is considered the best indicator of a syndesmosis ankle sprain without diastasis. Tenderness along the syndesmosis, the deltoid, or over the anterior talofibular ligament or anterior distal tibia/fibula may present later, following the initial injury. The squeeze test and tenderness with dorsiflexion and external rotation may be positive but often are not present initially. The best determinant for prediction of return to play is the amount of tenderness along the syndesmosis, measured from the distal fibula up the syndesmosis. Nussbaum ED, Hosea TM, et al: Prospective evaluation of syndesmosis ankle sprains without diastasis. Am J Sports Med 2001;29:31-35. Miller CD, Shelton WR, Barrett GR, et al: Deltoid and syndesmosis ligament injury of the ankle without fracture. Am J Sports Med 1985;23:746-750.
References:
- Amendola A: Controversies in diagnosis and management of syndesmosis injuries of the ankle. Foot Ankle 1992;13:44-50.
Question 76High Yield
A 45-year-old woman with stage II posterior tibial tendinitis has failed to respond to nonsurgical management. Recommended treatment now includes posterior tibial tendon debridement and medial calcaneal displacement osteotomy along with transfer of what tendon?
Explanation
Explanation
The flexor digitorium longus is the commonly accepted tendon transfer for posterior tibial tendon insufficiency. The flexor hallucis longus has to be carefully rerouted to avoid crossing the neurovascular bundle and has not been shown clinically to provide superior results to flexor digitorum longus transfer. Use of the peroneus longus results in loss of plantar flexion strength of the first metatarsal, contributing to the flatfoot deformity. The anterior tibial tendon is in the anterior compartment and fires out of phase with the posterior tibial tendon. Sitler DF, Bell SJ: Soft tissue procedures. Foot Ankle Clin 2003;8:503-520.
References:
- Guyton GP, Jeng C, Krieger LE, et al: Flexor digitorum longus transfer and medial displacement calcaneal osteotomy for posterior tibial tendon dysfunction: A middle-term clinical follow-up. Foot Ankle Int 2001;22:627-632.
Question 77High Yield
A 78-year-old woman falls onto her nondominant left elbow and sustains the injury shown in Figure 5. What treatment option allows her the shortest recovery time and highest likelihood of good function and range of motion?
Explanation
Total elbow arthroplasty has become the treatment of choice for complex, comminuted distal humeral fractures in patients older than age 70 years. It yields a faster recovery with more predictable functional outcomes, although limitations of lifting weight of more than 5 pounds must be followed to avoid loosening. Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement. J Bone Joint Surg Am 2004;86:940-947.
Question 78High Yield
A 56-year-old man with a history of chronic lower back pain from lumbar spondylosis reports a 2-day history of acute incapacitating back pain. He denies any history of acute trauma, although he reports the pain starting after a coughing spell. He also reports difficulty urinating and some fecal incontinence. Examination reveals generalized lower extremity weakness, saddle paresthesia, hyporeflexia in the lower extremities, and loss of rectal tone. What is the most appropriate management at this time?
Explanation
Explanation
Cauda equina syndrome is a medical emergency that must be quickly diagnosed and treated to avoid long-term complications. Cauda equina syndrome typically presents with low back pain, unilateral or usually bilateral sciatica, saddle sensory disturbances, bladder and bowel dysfunction, and variable lower extremity motor and sensory loss. Although a number of pathologies can cause cauda equina syndrome, in a patient with a history of chronic back pain, disk pathology is the most common cause of acute onset cauda equina syndrome. Whereas radiographs may be useful in a traumatic onset of symptoms, MRI is the most appropriate study. Cauda equina syndrome should be evaluated on an emergent basis and admission for work-up is appropriate. Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522.
Question 79High Yield
Figures 21a and 21b show the radiograph and CT scan of a 14-year-old patient with thigh pain. The next most appropriate step in management should consist of

Explanation
The radiographs show increased density and reactive bone formation. A faint nidus can be seen on the radiograph but is obvious on the CT scan. The initial therapy for an osteoid osteoma should be oral anti-inflammatory drugs. A biopsy or SPECT bone scan is not indicated because the osteoid osteoma is clearly seen on the CT scan. If the patient fails to respond to nonsurgical therapy, CT-guided radiofrequency ablation or surgical excision is indicated depending on the anatomic location. Frassica FJ, Waltrip RL, Sponseller PD, Ma LD, McCarthy EF Jr: Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 1996;27:559-574. Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid osteoma. J Bone Joint Surg Am 1992;74:179-185.
Question 80High Yield
Which of the following is considered an advantage of arthroscopic distal clavicle excision compared with open distal clavicle excision?
Explanation
Arthroscopic versus open distal clavicle excision has the advantage of allowing evaluation of the glenohumeral joint arthroscopically prior to moving into the subclavicular and subacromial space to perform the distal clavicle excision. This can be of value in both confirming the diagnosis as well as avoiding diagnostic errors. Berg and Ciullo showed that in 20 patients who underwent open distal clavicle excision that resulted in failure, 15 of those patients had a superior labral anterior posterior (SLAP) lesion. Of these 15 patients who had the lesion treated surgically, 9 went on to a good to excellent result after the surgery was performed arthroscopically. Fewer complications, lower infection rate, and decreased surgical time have not been documented in the literature. Arthroscopic technique sacrifices the inferior acromioclavicular ligament and preserves the superior acromioclavicular ligament. Berg EE, Ciullo JV: The SLAP lesion: A cause of failure after distal clavicle resection. Arthroscopy 1997;13:85-89.
Question 81High Yield
Examination of a 12-year-old girl with bilateral anterior knee pain reveals excessive femoral anteversion and excessive external tibial torsion. The patient has no patellofemoral instability. Nonsurgical management consisting of muscle strengthening and nonsteroidal medication has failed to relieve the patient's pain. Treatment should now consist of
Explanation
Children with symptomatic severe torsional malalignment of the lower extremity and patellofemoral pathology show excessive femoral anteversion and external tibial torsion on physical examination and analysis of gait. The functional effect of this torsional malalignment is centered about the knee joint. If nonsurgical management fails to alleviate patellofemoral pain, definitive surgical treatment should consist of corrective osteotomies, including internal rotation of the distal part of the tibia or external rotation of the femur, or both. Patients with surgical correction by osteotomy show an improved gait pattern and appearance of the extremity and a marked decrease in knee pain. External rotation of the distal part of the tibia or internal rotation of the distal part of the femur worsens the torsional malalignment. No additional soft-tissue realignment procedures, including retinacular release or patellar realignment, are required.
Question 82High Yield
A 20-year-old basketball player has tenderness and bruising after sustaining a blow to the knee. A radiograph is shown in Figure 15. What is the most likely diagnosis?
Explanation
Explanation
The patient has a bipartite patella. The line between the fragment and the main patella is smooth and sclerotic, indicating a chronic, not acute, entity. The location is classic for a bipartite patella, not a tumor. Schmidt DR, Henry JH: Stress injuries of the adolescent extensor mechanism. Clin Sports Med 1989;8:343-355.
References:
- Weaver JK: Bipartite patellae as a cause of disability in the athlete. Am J Sports Med 1977;5:137-143.
Question 83High Yield
The husband of a 22-year-old woman has hypophosphatemic rickets. The woman has no orthopaedic abnormalities, but she is concerned about her chances of having a child with the same disease. What should they be told regarding this disorder?
Explanation
Hypophosphatemia is a rare genetic disease usually inherited as an X-linked dominant trait. The fact that the woman has no skeletal manifestations would indicate that the husband has the X-linked mutation. The disease is more severe in boys than it is in girls. The husband will not transmit the disease to his sons. However, all of their daughters will be affected either with the disease or as carriers. If the woman has the disease or the trait, there is a 50% chance that her sons will inherit the disease and a 50% chance that her daughters will be carriers or have a milder form of the disease. Parents should be advised to have genetic counseling so they can be informed when deciding whether to have children. Herring JA: Metabolic and endocrine bone diseases, in Tachdjian's Pediatric Orthopaedics, ed 3. New York, NY, WB Saunders, 2002, pp 1685-1743. Sillence DO: Disorders of bone density, volume, and mineralization, in Rimoin DL, Conner JM, Pyerite RE, et al (eds): Principles and Practice of Medical Genetics, ed 4. New York, NY, Churchill Livingstone, 2002.
Question 84High Yield
Which of the following assessment tools most accurately reflects outcomes of well-being, daily function, and general health in a patient treated for cervical myelopathy?
Explanation
Explanation
The short-form 36 is an excellent tool for measuring the patient's perception of treatment outcome because it is a patient-generated, validated assessment of physical, social, and role function, emotional and mental health, energy/fatigue, pain, health perception, and health change. The Nurick criteria is an evaluation of physical function with gradations of ambulation and daily function. The Japanese Orthopaedic Association score gives points for function in activities of daily living but does not assess perception of general health. The neck disability index assesses the impact of neck pain on daily life, and the Odom criteria are the surgeon's evaluations of degree of radicular pain and deficit. Albert TJ, Mesa JJ, Eng K, McIntosh TC, Balderston RA: Health outcome assessment before and after lumbar laminectomy for radiculopathy. Spine 1996;21:960-963. Swiontkowski MF, Buckwalter JA, Keller RB, Haralson R: The outcomes movement in orthopaedic surgery: Where we are and where we should go. J Bone Joint Surgery Am 1999;81:732-740.
References:
- Ludwig SC, Albert TJ: Measuring outcomes in cervical myelopathy and radiculopathy. Instr Course Lect 1999;48:417-421.
Question 85High Yield
The brachialis muscle is innervated by what two nerves?
Explanation
The brachialis is innervated by two nerves: medially, the musculocutaneous nerve; laterally, the radial nerve. The muscle is split longitudinally to approach the humerus anteriorly. Henry AK: The distal part of the humerus and front of the forearm, in Henry AK (ed): Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 90-115.
Question 86High Yield
A 53-year-old woman has severe neck and left shoulder pain after a rollover motor vehicle accident. Radiographs and a CT scan of the cervical spine are shown in Figures 34a through 34c. Management should consist of
Explanation
Explanation
34b 34c The plain radiographs show a horizontal orientation of the C5 facet joint. The CT scan through C5 reveals an ipsilateral pedicle and lamina fracture (floating facet). This injury involves two adjacent motion segments and is extremely unstable. Lateral mass plates, with or without the purchase of the "floating facet," provide the best means of stabilization and should include the facet above (C4) and below (C6) the level of injury. Orthotic immobilization is insufficient for this particular injury. Halo vest treatment does not control the subaxial spine well and is of limited value. While simple midline (Rogers) wiring provides some tension band restoration, it is not optimal for rotational control. The use of lateral mass plates provides rotational stability. Another option would be anterior fusion and plating, which would save cervical segments. Levine AM, Mazel C, Roy-Camille R: Management of fracture separations of the articular mass using posterior cervical plating. Spine 1992;17:S447-S454. Levine AM: Facet fractures and dislocations, in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 360-362. Whitehill R, Richman JA, Glaser JA: Failure of immobilization of the cervical spine by the halo vest: A report of five cases. J Bone Joint Surg Am 1986;68:326-332.
References:
- Garvey TA, Eismont FJ, Roberti LJ: Anterior decompression, structural bone grafting, and Caspar plate stabilization for unstable cervical spine fractures and/or dislocations. Spine 1992;17:S431-S435.
Question 87High Yield
Acute redislocation of the glenohumeral joint is a complication that occurs following a first-time dislocation. This is most often seen with
Explanation
Redislocation following acute dislocation occurs in approximately 3% of patients. This redislocation tends to occur in middle-aged and elderly patients. A higher incidence of redislocation occurs when there are accompanying fractures of the glenoid rim and the greater tuberosity. Robinson CM, Kelly M, Wakefield AE: Redislocation of the shoulder during the first six weeks after a primary anterior dislocation: Risk factors and results of treatment. J Bone Joint Surg Am 2002;84:1552-1559.
Question 88High Yield
A 15-year-old girl who competes in gymnastics has immediate pain and giving way of the left elbow after falling from the uneven parallel bars and landing on her outstretched arms. Examination reveals swelling and tenderness about the elbow, especially over the medial side. Measurement of elbow motion shows 0 degrees to 125 degrees of flexion, and valgus stress at the elbow is painful. AP, lateral, and stress radiographs are shown in Figures 9a through 9c. Management should consist of


Explanation
While many low-demand patients with injuries to the ulnar collateral ligament can be treated nonsurgically, Jobe and associates described two situations in which ulnar collateral ligament reconstruction is indicated: (1) an acute complete rupture in a competitive athlete who uses the upper extremities extensively and who wishes to remain active; and (2) chronic pain or instability that does not improve after at least 3 months of nonsurgical management. Rarely is direct surgical repair of the ligament possible or able to withstand the valgus stresses applied to the elbow. Most authors recommend surgical reconstruction of the ulnar collateral ligament using a palmaris longus, plantaris, or fourth toe extensor tendon from the fourth autograft. Andrews JR, Jelsma RD, Joyce ME, et al: Open surgical procedures for injuries to the elbow in throwers. Oper Tech Sports Med 1994;4:109-133. Jobe FW, Kvitne RS: Elbow instability in the athlete. Instr Course Lect 1991;40:17-23.
Question 89High Yield
A 27-year-old woman with Down syndrome has a severe bunion with pain and deformity in the left forefoot. Nonsurgical management has failed to provide relief. She does not use any assistive ambulatory devices. A radiograph is shown in Figure 21. Treatment should now consist of
Explanation
The patient requires an arthrodesis of the first metatarsophalangeal joint because of the abnormal neuromuscular forces. The more traditional bunionectomies such as a distal chevron bunionectomy, a proximal first metatarsal osteotomy, and a double osteotomy have a high failure rate because of the underlying Down syndrome. The Keller procedure is indicated for older, sedentary individuals and has little role in the management of a neuromuscular bunion. Coughlin MJ, Abdo RV: Arthodesis of the first metatarsophalangeal joint with Vitallium plate fixation. Foot Ankle Int 1994;15:18-28.
Question 90High Yield
Examination of a 10-year-old girl with a hypoplastic breast and atrophic pectoralis major may also reveal which of the following findings?
Explanation
Explanation
Poland's syndrome has four main features: 1) short digits as the result of absence or shortening of the middle phalanx; 2) syndactyly of the short digits usually consisting of a simple, complete type; 3) hypoplasia of the hand and forearm; and 4) absence of the sternocostal head of the pectoralis major on the same side. Wilson MR, Louis DS, Stevenson TR: Poland's syndrome: Variable expression and associated anomalies. J Hand Surg 1988;13:880-882.
References:
- Poland A: Deficiency of the pectoralis muscle. Guys Hosp Rep 1841;6:191.
Question 91High Yield
Which of the following is considered a potential advantage in prophylaxis for the prevention of deep venous thrombosis associated with the use of low-molecular weight heparin (LMWH) as compared with fixed-dose unfractionated heparin?
Explanation
One possible reason for improved efficacy of LMWHs is the relative improved bioavailability compared with that of unfractionated heparin. This is, in part, the result of a more predictable dose response and a longer half-life. There is no alteration of venous flow, and the rate of bleeding complications is the same or slightly higher than that of other prophylactic agents. Colwell CW Jr, Spiro TE, Trowbridge AA: Use of enoxaparin, a low-molecular weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14. Bara L, Billaud E, Kher A, Samama M: Increased anti-Xa bioavailability for a low-molecular weight heparin (PK 10169) compared with unfractionated heparin. Semin Thromb and Hemost 1985;11:316-317.
Question 92High Yield
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5 degrees of angulation. When the MCP joint is flexed 30 degrees, a radially directed stress produces 45 degrees of angulation. Radiographs are otherwise normal. Management should consist of
Explanation
Injuries to the ulnar collateral ligament of the MCP joint of the thumb commonly occur in recreational skiers. Historically, this injury has been referred to as "gamekeeper's thumb." The ligament consists of the proper collateral ligament and the more volar accessory collateral ligament. In extension, the accessory ligament is taut, and in flexion, the proper ligament is taut. For a complete tear of the ligament complex to occur, there must be laxity in full extension. Incomplete tears respond well to thumb spica splinting or casting for 2 to 3 weeks and gradual resumption of range of motion. Prolonged immobilization of incomplete injuries leads to higher rates of MCP joint stiffness. Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Question 93High Yield
The incidence of osteosarcoma is highest in what age group?
Explanation
The peak incidence of osteosarcoma occurs in the second decade, followed by the third decade. Up to 75% of all cases of osteosarcoma occur in patients between 10 and 25 years. It rarely occurs after age 30. Affected women tend to be younger than affect men. Osteosarcoma associated with Paget's disease or in radiation-induced osteosarcoma occurs in an older population. Simon M, Springfield D, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 266. Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989.
Question 94High Yield
In Gustilo type III open tibial diaphyseal fractures, which of the following factors is associated with an increased risk of a poor functional outcome?
Explanation
Explanation
According to the published outcomes analyses from the Lower Extremity Assessment Project (LEAP) study group of patients prospectively followed for 2 to 7 years, definitive fixation with an intramedullary nail has shown improved outcomes when compared to definitive external fixation. The findings showed that the timing of wound debridement (within 6 hours from injury as compared to within 6 to 24 hours), the timing of soft-tissue coverage (3 days or less from injury as compared to more than 3 days), and the timing of bone grafting after injury (within or after 3 months) did not impact the infection or union rates and had no effect on functional outcome. The LEAP study has shown at 7-year follow-up that patients who are definitively treated with external fixation have a significantly longer time to union, poorer functional outcomes, longer time to achieve full weight bearing, and more time in the hospital.
Question 95High Yield
A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow 9 years ago. Over the past year the patient has had increasing pain and elbow instability. There is no clinical evidence of infection, and radiographs show no new bony process. What is the best option for this patient?
Explanation
Explanation
In a series reported by Blaine and associates, 12 patients were converted from interposition to total elbow arthroplasty. This procedure was successful in 10 out of 12 patients. Blaine TA, Adams R, Morrey BF: Total elbow arthroplasty after interposition arthroplasty for elbow arthritis. J Bone Joint Surg Am 2005;87;286-292.
References:
- Cheng SL, Morrey FB: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Question 96High Yield
A 14-year-old boy sustains a right leg injury after being thrown from his motorcycle while racing. He reports diffuse right leg pain starting at his knee and proceeding distally to include his foot. After the injury the patient's mother reports the tibia moving posteriorly then anteriorly while she was supporting the leg. In the emergency department 4 hours after injury, examination reveals a large knee effusion, firm compartments of the leg, a palpable posterior tibialis pulse with a warm, pink foot, and capillary refill of 2 seconds at the toes. His blood pressure is 100/50 mm Hg. Motor examination is intact, but there is decreased sensation in the dorsal first interspace and plantar aspect of the foot. Compartment pressure measurement reveals all four compartments with pressures of 33, 36, 33, and 38 mm Hg respectively. Radiographs are shown in Figure 59a and 59b. The remainder of the skeletal examination is normal. What is the optimal management for this injury?
Explanation
Explanation
59b The patient has a compartment syndrome based on the firm compartments of the leg and the elevated compartment pressures measured at the diastolic pressure reading. Muscle ischemia occurs quickly when compartment pressures are elevated, and within 6 hours irreversible damage can occur. Emergent fasciotomies permit decompression of all four compartments and reestablishment of vascular supply to the muscles. Stabilization of the fracture prevents further soft-tissue injury.
Question 97High Yield
Figure 22 shows the radiographs of a 16-year-old boy who injured his elbow in a fall 1 year ago. Although he has no pain, he reports restricted forearm rotation and elbow flexion. What is the most likely diagnosis?
Explanation
Congenital dislocation of the radial head is often confused with posttraumatic dislocation. The distinguishing feature here is the dome-shaped radial head. Some patients with congenital anomalies fail to recognize their limitations until an injury occurs. Soft-tissue contractures do not cause radial head dislocation nor do they usually cause this pattern of motion restriction (mainly flexion and rotation without significant loss of extension). There is no deformity of the ulna to suggest an old Monteggia lesion. Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 196.
Question 98High Yield
Figures 29a and 29b show the radiograph and CT scan of a 48-year-old man who has diffuse spinal pain. What is the most likely diagnosis?
Explanation
Explanation
29b The studies show marginal syndesmophyte formation characteristic of ankylosing spondylitis. These patients typically have diffuse ossification of the disk space without large osteophyte formation. DISH typically presents with large osteophytes, referred to as nonmarginal syndesmophytes. In this patient, the zygoapophyseal joints are fused rather than degenerative as would be seen in rheumatoid arthritis, and the costovertebral joints are also fused. Osteopetrosis does not normally ankylose the disk space. McCullough JA, Transfeldt EE: Macnab's Backache, ed 3. Baltimore, MD, Williams and Wilkins, 1997, pp 190-194.
References:
- Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott, Williams and Wilkins, 2003, pp 141-151.
Question 99High Yield
For patients undergoing a surgical procedure where the risk of requiring a transfusion is less than 10%, the International Committee of Effective Blood Usage suggests
Explanation
Explanation
Recent studies have shown a high rate of waste of autologous blood. Therefore, the Committee does not recommend autologous blood donation for procedures that carry a transfusion risk of 10% or less. Toy P, Beattie C, Gould S, et al: Transfusion alert: Use of autologous blood. National Heart, Lung, and Blood Institute Expert Panel on the use of autologous blood. Transfusion 1992;35:703-711.
References:
- Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 100High Yield
A 13-year-old boy has had pain and swelling in his ankle for the past several months. Based on the radiograph, MRI scan, and biopsy specimen shown in Figures 77a through 77c, what is the best course of action?
Explanation
Explanation
77b 77c Chondroblastomas are benign cartilage lesions frequently seen in adolescents or young adults. They are found in the epiphyseal or apophyseal regions of bones. The radiograph shows a radiolucent lesion with mineralization and a well-marginated rim of reactive bone. The lesion is composed of sheets of immature chondroblasts (polygonal cells with a clear, bluish cytoplasm and a small round central nucleus). In some regions, classic "chicken-wire" matrix calcifications and a "cobblestone" pattern of cell arrangement may be seen. Treatment consists of curettage and bone grafting. Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 247-264.
References:
- Lin PP, Thenappan A, Deavers MT, et al: Treatment and prognosis of chondroblastoma. Clin Orthop Relat Res 2005;438:103-109.
You Might Also Like
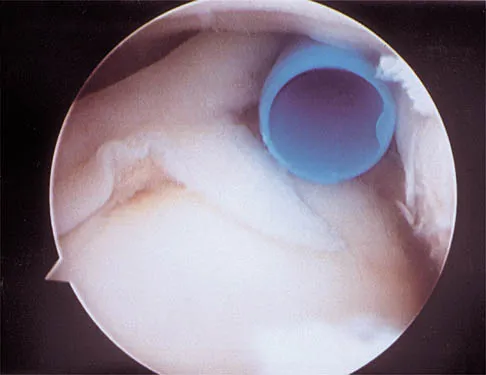
Previous ChapterOrthopedic Board Review MCQs: ABOS, OITE, FRCS Mock Exam Se…
Next Chapter AAOS Orthopedic MCQs (Set 1): Neurofibromatosis & Genetic S…

Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon