Orthopedic Board Review: 100 High-Yield MCQs - Set 1065
14 Apr 2026
102 min read
122 Views
Key Takeaway
This page provides 100 high-yield orthopedic board review questions, randomized for comprehensive exam preparation. Surgeons can utilize this extensive multiple-choice question set, Mock Exam 1065, to master crucial concepts and confidently pass ABOS, OITE, and FRCS board certification exams.
Mastering Acromioclavicular Joint Reduction: ...
00:00
Start Quiz
Question 1High Yield
A 48-year-old man has had pain and swelling of the hallux metatarsophalangeal joint for the past 9 months. A rocker bottom stiff-soled shoe has failed to provide relief; however, two cortisone injections have temporarily alleviated his symptoms. The radiographs shown in Figures 20a and 20b reveal diffuse arthritis of the entire hallux metatarsophalangeal joint. What is the most definitive surgical treatment?

Explanation
Because the radiographs demonstrate severe arthritis, hallux metatarsophalangeal arthrodesis is the treatment of choice. Cheilectomy alone will not relieve pain because the entire joint is degenerative. Joint replacement has not been shown to be a long-term solution. Keller resection arthroplasty is not indicated in younger active patients. Hallux valgus correction will not address arthritis of the joint and could stiffen the joint further. Smith RW, Joanis TL, Maxwell PD: Great toe metatarsophalangeal joint arthrodesis: A user-friendly technique. Foot Ankle 1992;13:367-377.
Question 2High Yield
Figures 43a and 43b show the clinical photographs of a 4-month-old child with bilateral popliteal pterygium. The fixed knee contractures measure 100 degrees bilaterally. What future treatment is most likely to successfully correct this deformity?
Explanation
Explanation
43b Congenital popliteal webbing with contractures of 60 degrees is a difficult deformity to correct. The anatomy of the web is of considerable importance. MRI can delineate the extent of the posterior fibrous band that often stretches from the ischium to the calcaneus. The sciatic nerve, usually shortened, most often runs just anterior to this fibrous band. For mild contractures of less than 20 degrees, nonsurgical management is usually adequate. Hamstring lengthening and postoperative splinting are usually sufficient for contractures of 20 degrees to 40 degrees. Moderate contractures of up to 60 degrees usually require Z-plasties in the popliteal fossa and postoperative serial casting to avoid undue tension on neurovascular structures. Contractures of more than 60 degrees require a femoral shortening osteotomy or gradual correction with an external fixator. However, rapid recurrence following fixator removal is common if formal soft-tissue procedures and postoperative splinting are not performed. Parikh SN, Crawford AH, Do TT, et al: Popliteal pterygium syndrome: Implications for orthopaedic management. J Pediatr Orthop B 2004;13:197-201.
References:
- Brunner R, Hefti F, Tgetgel JD: Arthrogrypotic joint contracture at the knee and foot: Correction with a circular frame. J Pediatr Orthop B 1997;6:192-197.
Question 3High Yield
Figures 5a and 5b show the radiographs of a 56-year-old man who was seen in the emergency department following a twisting injury to his left ankle. Examination in your office 3 days later reveals marked swelling and diffuse tenderness to palpation about the ankle and leg. What is the next most appropriate step in management?
Explanation
Explanation
5b The radiographs show an isolated posterior malleolus fracture which, given the injury mechanism, is highly suspicious for a Maisonneuve injury. As with any suspected extremity injury, radiographs including the joints above and below the level of injury are acutely indicated. Although MRI may reveal a ligamentous injury to the ankle and CT may show asymmetry of the ankle mortise or syndesmosis, both studies are considerably more costly and are not indicated in the absence of a complete radiographic work-up. Technetium bone scan is nonspecific and would be of limited value in this instance, as would repeat radiographs of the ankle. Walling AK, Sanders RW: Ankle fractures, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 1973-2016.
References:
- Marsh JL, Saltzman CL: Ankle fractures, in Bucholz RW, Heckman JD, Court-Brown C (eds): Rockwood and Green's Fractures in Adults, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, vol 2, pp 2147-2247.
Question 4High Yield
Compared to similar patients who do not donate autologous blood, patients with normal baseline hemoglobin who donate autologous blood prior to undergoing primary total hip arthroplasty are likely to
Explanation
Explanation
Billote and associates compared patients with normal baseline hemoglobin levels who did and did not donate autologous blood prior to total hip arthroplasty. No patients received allogeneic blood perioperatively, and the autologous donors had significantly lower hemoglobin levels at the time of surgery and in the recovery room. Of the autologous donors, 69% received an autologous transfusion. The authors concluded that autologous donation was unnecessary in patients undergoing primary total hip arthroplasty who had a normal hemoglobin. Billote D, Glisson SN, Green D, Wixson RL: A prospective, randomized study of preoperative autologous donation for hip replacement surgery. J Bone Joint Surg Am 2002;84:1299-1304.
References:
- Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 47-53.
Question 5High Yield
A 20-year-old football player sustains a dorsiflexion external rotation injury to his right ankle. During sideline evaluation, which of the following findings best indicates a syndesmosis ankle sprain without diastasis?
Explanation
Explanation
The inability to single leg hop is considered the best indicator of a syndesmosis ankle sprain without diastasis. Tenderness along the syndesmosis, the deltoid, or over the anterior talofibular ligament or anterior distal tibia/fibula may present later, following the initial injury. The squeeze test and tenderness with dorsiflexion and external rotation may be positive but often are not present initially. The best determinant for prediction of return to play is the amount of tenderness along the syndesmosis, measured from the distal fibula up the syndesmosis. Nussbaum ED, Hosea TM, et al: Prospective evaluation of syndesmosis ankle sprains without diastasis. Am J Sports Med 2001;29:31-35. Miller CD, Shelton WR, Barrett GR, et al: Deltoid and syndesmosis ligament injury of the ankle without fracture. Am J Sports Med 1985;23:746-750.
References:
- Amendola A: Controversies in diagnosis and management of syndesmosis injuries of the ankle. Foot Ankle 1992;13:44-50.
Question 6High Yield
A 10-year-old girl has been unable to walk for the past 5 days because of bilateral hip pain. Administration of IV morphine has provided some pain relief. She is afebrile. History reveals that she had an upper respiratory tract infection 3 weeks ago that resolved uneventfully. Examination reveals moderate pain with internal rotation and abduction, while log rolling maneuvers do not cause significant pain. An MRI scan shows a small effusion of one hip; however, a bone scan and plain radiographs are normal. Initial laboratory studies showed a markedly elevated WBC count, which subsequently declined to normal levels with IV antibiotics. Current studies show an erythrocyte sedimentation rate (ESR) of 100 mm/h. Aspiration of the hip obtains 3 mL of fluid; Gram stain is negative for bacteria, but a cell count shows a WBC count of 16,500/mm3. Streptozyme titer of the peripheral blood is 200 units (normal is less than 100 units). Management should now consist of
Explanation
Explanation
This clinical situation requires careful analysis because some data suggest infection and some a noninfectious inflammatory process. Bilateral hip involvement, the absence of significant fluid collection or fever, the streptozyme level, and the history of upper respiratory infection all suggest poststreptococcal toxic synovitis as the most likely cause for the clinical presentation. In the first 24 hours, this type of presentation might warrant incision and drainage given uncertainty of the diagnosis and the risks associated with missing an infection. However, 5 days after onset, surgery is not warranted, especially given that the patient remains afebrile and her symptoms are improving. Cardiology consultation would be appropriate. There is no evidence to suggest slipped capital femoral epiphysis. Treatment with antibiotics is not advised because there is no bacteriologic data on which to base treatment. De Cunto CL, Giannini EH, Fink CW, et al: Prognosis of children with poststreptococcal reactive arthritis. J Pediatr Infect Dis 1988;7:683-686.
References:
- Haueisen DC, Weiner DS, Weiner SD: The characterization of "transient synovitis of the hip" in children. J Pediatr Orthop 1986;6:11-17.
Question 7High Yield
A 22-year-old wrestler who underwent an open anterior shoulder reconstruction to repair a dislocated shoulder 6 months ago now reports shoulder pain after attempting a takedown. Examination reveals external rotation that is 15 degrees greater than the contralateral side. He has pain associated with abduction and external rotation but no apprehension. Which of the following tests would most likely reveal positive findings?
Explanation
Postoperative subscapularis detachment can be identified with a positive lift-off test that reveals weakness in internal rotation. This complication does not necessarily compromise the anterior capsule repair. The load-and-sift maneuver and articular contrast studies may be normal. Supraspinatus tests for impingement and weakness should be negative. Gerber C, Krushell RJ: Isolated ruptures of the tendon of the subscapularis muscle: Clinical fractures in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Question 8High Yield
What structure is most at risk for injury from a retractor against the tracheoesophageal junction during an anterior approach to the cervical spine?
Explanation
Although any of these structures can be injured by pressure from the medial blade of a self-retaining retractor, the recurrent laryngeal nerve runs cephalad in the interval between the esophagus and trachea and is vulnerable to pressure if caught between the retractor and an inflated endotracheal tube balloon. Ebraheim NA, Lu J, Skie M, et al: Vulnerability of the recurrent laryngeal nerve in the anterior approach to the lower cervical spine. Spine 1997;22:2664-2667.
Question 9High Yield
Which of the following is the strongest contraindication to unicompartmental knee arthroplasty (UKA)?
Explanation
Explanation
UKA prostheses cannot substitute for an absent ACL, and if arthroplasty is indicated, these patients should receive a total knee arthroplasty rather than a UKA. Age is not an absolute contraindication, and the procedure has been advocated for young patients as well as older patients if they meet the appropriate indications for an arthroplasty. Varus deformities of the mechanical axis of up to 10 degrees generally are not a contraindication to unicompartmental arthroplasty, as long as the knee can be properly balanced at the time of surgery. Modest chondromalacia of the patellofemoral joint, especially if asymptomatic, is not a contraindication to UKA. Lotke PA (ed): Knee Arthroplasty: Master Techniques in Orthopaedic Surgery. New York, NY, Raven Press, 1995, pp 275-293. Insall JN, Windsor RE, Scott WN, et al (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 805-814.
References:
- Tabor OB Jr, Tabor OB: Unicompartmental arthroplasty: A long-term follow-up study. J Arthroplasty 1998;13:373-379.
Question 10High Yield
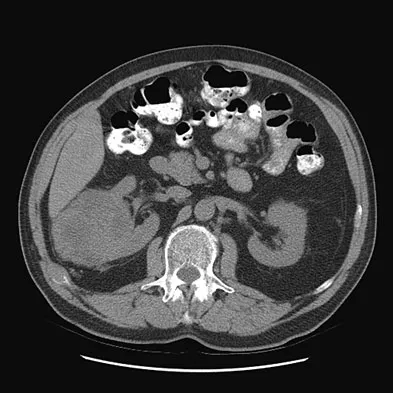
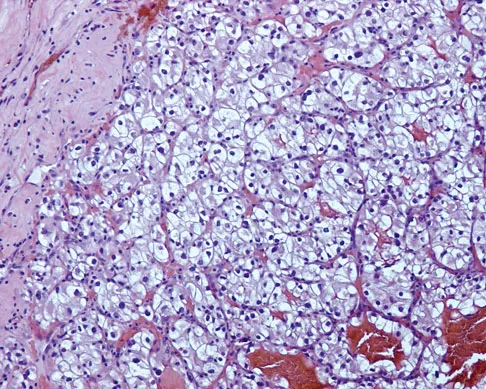
Figures 20a and 20b show the AP and lateral radiographs of a 62-year-old man who has had hip pain for the past 3 weeks. Figure 20c shows a CT scan of the abdomen and pelvis. A needle biopsy specimen is shown in Figure 20d. Preoperative management should include which of the following?

Explanation
The histology shows findings consistent with metastatic renal cell carcinoma. Renal cell carcinoma metastases are extremely vascular. Preoperative embolization helps minimize the amount of blood loss during curettage of these lesions. Chatziioannou AN, Johnson ME, Pneumaticos SG, et al: Preoperative embolization of bone metastases from renal cell carcinoma. Eur Radiol 2000;10:593-596.
Question 11High Yield
Figure 21 shows the AP radiograph of a 41-year-old patient who sustained a closed bicolumnar fracture of the distal humerus that resulted in a painful nonunion. What is the best initial construct for rigid stabilization of this fracture pattern?
Explanation
The dual plate fixation construct is significantly stronger than single plate or "Y" plate fixation. Two-plate constructs at right angles, the ulnar plate medially and the lateral plate posteriorly, would appear to be biomechanically optimal. This approach usually is feasible at the time of surgery. Clinically, dual 3.5-mm reconstruction or dynamic compression plates are superior to one third tubular plate fixation. Supplementary external fixation is not considered a better treatment option. Failure of fixation and nonunion are often the result of inadequate fixation and osteoporosis. Helfet DL, Hotchkiss RN: Internal fixation of the distal humerus: A biomechanical comparison of methods. J Orthop Trauma 1990;4:260-264.
Question 12High Yield
What is the single most important nutritional factor affecting athletic performance?
Explanation
Maintenance of adequate hydration is the single most important factor affecting athletic performance. While carbohydrate loading may be beneficial for some endurance athletes, the consumption of carbohydrates during exercise does not appear to be beneficial for athletes engaged in events that last less than 1 hour. In general, athletes consuming a balanced diet do not need electrolyte supplementation. Maughan RJ, Noakes TD: Fluid replacement and exercise stress: A brief review of studies on fluid replacement and some guidelines for the athlete. Sports Med 1991;12:16-31.
Question 13High Yield
Figure 12 shows the radiograph of a 15-year-old boy with cerebral palsy who has pain at the first metatarsophalangeal joints. He is a community ambulator. Management consisting of accommodative shoes has failed to provide relief. What is the treatment of choice?
Explanation
While other surgeries have provided some success, first metatarsophalangeal joint arthrodesis has the highest overall success rate compared to other surgeries in ambulatory and nonambulatory children with cerebral palsy. The recurrence rate is unacceptably high with the other procedures listed above. In contrast, neurologically normal children are amenable to osteotomies and soft-tissue procedures. Davids JR, Mason TA, Danko A, et al: Surgical management of hallux valgus deformity in children with cerebral palsy. J Pediatr Orthop 2001;21:89-94.
Question 14High Yield
What type of cementless femoral fixation results in the highest rate of distal femoral osteolysis?
Explanation
Explanation
Despite the relatively few problems with porous-coated cementless stems, stress shielding and thigh pain do occur. One design feature of proximally coated stems that has been associated with a higher incidence of distal osteolysis is the presence of noncircumferential proximal porous coating. Tapered, modular with sleeve, and hydroxyapatite proximally porous-coated stems have all performed well. Fully porous-coated straight stems have a high survivorship rate as well. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
References:
- Emerson RH Jr, Sanders SB, Head WC, Higgins L: Effect of circumferential plasma-spray porous coating on the rate of femoral osteolysis after total hip arthroplasty. J Bone Joint Surg Am 1999;81:1291-1298.
Question 15High Yield
What is the most common cause of mechanical failure of an orthopaedic biomaterial during clinical use?
Explanation
Explanation
In most orthopaedic applications, the materials are strong enough to withstand a single cycle of loading in vivo. However, these loads may be large enough to initiate a small crack in the implant that can grow slowly over thousands or millions of cycles, eventually leading to gross failure. Such fatigue failure has occurred with virtually every type of implant, including stainless steel fracture plates and screws, bone cement in joint arthroplasty, and polyethylene inserts in total knee arthroplasty. Lewis G: Fatigue testing and performance of acrylic bone-cement materials: State-of-the-art review. J Biomed Mater Res Br 2003;66:457-486. Stolk J, Verdonschot N, Huiskes R: Stair climbing is more detrimental to the cement in hip replacement than walking. Clin Orthop 2002;405:294-305.
References:
- Wright TM, Maher SA: Biomaterials, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 16High Yield
What term best describes the process involved when a growth factor produced by an osteoblast stimulates the differentiation of an adjacent undifferentiated mesenchymal cell during fracture repair?
Explanation
Explanation
Growth factors are proteins secreted by cells that can act on target cells to produce certain biologic actions. These actions can be described as autocrine, paracrine, and endocrine. Autocrine actions are those in which the growth factor influences an adjacent cell of its origin or identical phenotype. Paracrine actions are those in which the protein influences an adjacent cell that is different in its origin or phenotype. Endocrine actions are those in which the factor influences a cell located at a distant anatomic site. Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044.
References:
- Zuscik MJ, Drissi MH, Reynolds PR, et al: Molecular and cell biology in orthopaedics, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 17High Yield
Figures 29a and 29b show a clinical photograph and radiographs of a patient who sustained an open calcaneus fracture in a motor vehicle accident. The patient received immediate IV antibiotics and an emergent irrigation and debridement. The swelling has subsided by 3 weeks and the medial wound is clean. What do you tell the patient about the likelihood of infection if a formal open reduction and internal fixation via a lateral approach is performed?
Explanation
Explanation
29b Multiple authors have shown similar infection rates for grade 1 and 2 open medial fractures and closed fractures that have been treated with an extensile lateral approach and open reduction and internal fixation. Patients only need IV antibiotics for 2 to 3 days after surgery. Formal open reduction and internal fixation is not recommended for grade 3 medial wounds and most lateral wounds. Heier KA, Infante AF, Walling AK, et al: Open fractures of the calcaneus: Soft-tissue injury determines outcome. J Bone Joint Surg Am 2003;85:2276-2282.
Question 18High Yield
A 66-year-old woman who requires a cane for ambulation now notes increasing difficulty in using the cane after undergoing total elbow arthroplasty 3 months ago. AP and lateral radiographs are shown in Figures 15a and 15b. What is the most likely diagnosis?

Explanation
The lateral radiograph reveals a triceps avulsion with a small portion of bone. Triceps weakness and insufficiency can be a symptomatic problem after total elbow arthroplasty and is probably underreported. Ulnar nerve neuritis, aseptic loosening, instability, and infection are all complications of total elbow arthroplasty but would not account for the radiographic findings. Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orhthopaedic Surgeons, 2002, pp 323-327.
Question 19High Yield
A 43-year-old man has had right groin pain for the past 3 months. A radiograph, CT scan, and biopsy specimen are shown in Figures 18a through 18c. What is the most likely diagnosis?


Explanation
The radiographic appearance of the lesion is lytic with calcifications in the supra-acetabular region. The CT scan shows bone destruction and periosteal reaction, which rules out an enchondroma. The histologic appearance is that of cellular cartilage, with a high cytoplasmic:nuclear ratio and basophilic appearance to the cytoplasm; these findings rule out chordoma and metastatic renal cell carcinoma. In addition, chordomas are most frequently found in the sacrum and base of the skull. Because there is no high-grade spindle cell component to suggest dedifferentiation, the most likely diagnosis is chondrosarcoma. Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Question 20High Yield
Figures 5a and 5b show axial and coronal MRI images of the left ankle of a patient with lateral ankle pain. What is the most likely diagnosis?

Explanation
The figures show a longitudinal split within the peroneus brevis tendon as it courses posterior to the fibula. The peroneus longus tendon has been driven between the medial and lateral components of the peroneus brevis tendon. Peroneal split syndrome is a cause of lateral ankle pain but may be less asymptomatic in the elderly. It may be associated with tendon subluxation following a tear of the superior peroneal retinaculum.
Question 21High Yield
Which of the following factors is associated with decreases in active periprosthetic osteolysis in total hip arthroplasty?
Explanation
Explanation
A 32-mm head design results in less linear wear but more volumetric wear particles. Modular components that allow motion between the polyethylene insert and the shell can result in backside wear. The oxidative degradation of gamma-irradiated polyethylene stored in air leads to increased wear. All of these factors lead to a greater particulate load and more osteolysis. Circumferential porous coating blocks ingrowth of particle-laden fluid and decreases osteolysis. Bartel DL, Bicknell VL, Wright TM: The effect of conformity, thickness, and material on stresses in ultra-high molecular weight components for total joint replacement. J Bone Joint Surg Am 1986;68:1041-1051. Fisher J, Hailey JL, Chan KL, et al: The effect of aging following irradiation on the wear of UHMWPE. Trans Orthop Res Soc 1995;20:12.
References:
- Archibeck MJ: The basic science of periprosthetic osteolysis. Instr Course Lect 2001;50:185-195.
Question 22High Yield
Figure 14 shows the AP radiograph of a patient who underwent prosthetic arthroplasty 8 years ago and has now become symptomatic again over the past 18 months. A WBC count and erythrocyte sedimentation rate are within normal limits, and aspiration of the glenohumeral joint yields a negative Gram stain and cultures. Which of the following procedures will most likely provide the best pain relief and function?
Explanation
Explanation
Simple removal of the loose glenoid component or removal of the loose component followed by implantation of a new glenoid component are both appropriate treatment choices, depending on the remaining glenoid bone stock. However, removal and reimplantation appears to provide the most predictable pain relief and better function than removal alone. Antuna SA, Sperling JW, Cofield RH, et al: Glenoid revision surgery after total shoulder arthroplasty. J Shoulder Elbow Surg 2001;10:217-224.
References:
- Rodosky MW, Bigliani LU: Surgical treatment of non-constrained glenoid component failure. Oper Tech Orth 1994;4:226-236.
Question 23High Yield
What is the most important feature in choosing an outcome instrument to assess shoulder disorders?
Explanation
There has been a recent increase in the use of outcome instruments to document and measure effects of treatment of medical conditions, including shoulder disorders. The most important feature of an instrument is whether it actually measures what it purports to measure; this is defined as its validity. Leggin BG, Iannotti JP: Shoulder outcome measurement, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, p 1027.
Question 24High Yield
Figure 42 shows the radiograph of a patient with spinal muscular atrophy. Examination reveals good upper extremity function, and she can tie her shoes and propel a manual wheelchair. Posterior instrumentation and fusion may result in
Explanation
Explanation
Spinal muscular atrophy is caused by an abnormal survival motor neuron gene that prevents apoptosis of the motor nerves. Spinal fusion results in better sitting balance, stabilized or improved pulmonary function, and high parental satisfaction, but it may result in at least temporary loss of upper extremity function. Bentley G, Haddad F, Bull TM, Seingry D: The treatment of scoliosis in muscular dystrophy using modified Luque and Harrington-Luque instrumentation. J Bone Joint Surg Br 2001;83:22-28. Furumasu J, Swank SM, Brown JC, Gilgoff I, Warath S, Zeller J: Functional activities in spinal muscular atrophy patients after spinal fusion. Spine 1989;14:771-775.
References:
- Granata C, Cervellati S, Ballestrazzi A, Corbascio M, Merlini L: Spine surgery in spinal muscular atrophy: Long-term results. Neuromuscul Disord 1993;3:207-215.
Question 25High Yield
A 50-year-old electrician who is right-hand dominant has had right shoulder pain and stiffness after sustaining an electric shock 2 months ago. An AP radiograph obtained at the time of injury was considered negative, and the patient was diagnosed with a shoulder sprain. The patient now reports continued shoulder pain and restricted motion. AP and axillary radiographs and a CT scan are shown in Figures 41a through 41c. Management should consist of


Explanation
Open reduction and transfer of the subscapularis and lesser tuberosity into the humeral head defect is the treatment of choice for chronic posterior dislocations in which the articular defect consists of 20% to 40% of the articular surfaces. Closed reduction can be used if the dislocation is recognized early and the articular defect is less than 20% of the articular surface. Humeral arthroplasty is reserved for patients with an articular defect that is greater than 45% to 50% of the head. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 26High Yield
A 62-year-old man has a severe pes planus and pain in the hindfoot. Radiographs show advanced degenerative changes at the talonavicular and subtalar joints with good preservation of the ankle joint. What is the most appropriate surgical procedure to alleviate his pain?
Explanation
Explanation
Once degenerative changes have occurred, soft-tissue procedures are not indicated. Triple arthrodesis is the treatment of choice for adult-acquired flatfoot. Isolated fusion of the subtalar or talonavicular joint will not be sufficient to correct the problem. Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 269-282.
References:
- Graves SC, Stephenson K: The use of subtalar and triple arthrodesis in the treatment of posterior tibial tendon dysfunction. Foot Ankle Clin 1997;2:319.
Question 27High Yield
A 10-year-old girl reports activity-related bilateral arm pain. Examination reveals no soft-tissue masses in either arm, and she has full painless range of motion in both shoulders and elbows. The radiograph and bone scan are shown in Figures 20a and 20b, and biopsy specimens are shown in Figures 20c and 20d. What is the most likely diagnosis?



Explanation
Based on these findings, the most likely diagnosis is fibrous dysplasia. Twenty percent of patients with fibrous dysplasia have multifocal disease. The lesions show a typical ground glass appearance. Fibrous dysplasia frequently involves the diaphysis of the long bones. There is no associated soft-tissue mass and no periosteal reactions to these lesions, suggesting a benign lesion. The histology shows proliferating fibroblasts in a dense collagen matrix. Trabeculae are arranged in an irregular or "Chinese letter" appearance. Osteogenic sarcoma and Ewing's sarcoma have a much different radiographic appearance of malignant osteoid and small round blue cells. Periosteal chondroma does occur in the proximal humerus but is not typically multifocal. It appears as a surface lesion with saucerization of the underlying bone and a bony buttress adjacent to the lesion. Some patients with multifocal lesions have associated endocrine abnormalities (McCune-Albright syndrome). Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 118-119.
Question 28High Yield
Portions of which of the following normal structures help compose the spiral cord seen in Dupuytren's contracture?
Explanation
The normal fascial components that become diseased and compose the spiral cord include the pretendinous band, spiral band, lateral digital sheet, and Grayson's ligament. Cleland's ligament lies dorsal and is not involved with spiral cord formation. The intrinsic muscle and tendon, the natatory ligament, and the intermetacarpal ligament are well proximal to the digit and are not involved in spiral cord formation. McGrouther D: Dupuytren's contracture, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 1, pp 565-569.
Question 29High Yield
Which of the following bearing surface combinations has shown the lowest in vivo wear rates in total hip arthroplasty?
Explanation
Explanation
Ceramic bearings, made of alumina, have the lowest in vivo wear rates of any bearing combination, 0.5 to 2.5 Mm per component per year. Laboratory wear rates for metal-on-metal are lower than those for metal-on-polyethylene bearings, ranging from 2.5 to 5.0 Mm per year. Titanium used for bearing surfaces has a high failure rate because of a poor resistance to wear and notch sensitivity. Wear rates for ceramic-on-polyethylene bearings have varied, ranging from 0 to 150 Mm. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 47-53.
References:
- Jazrawi LM, Kummer FJ, DiCesare PE: Alternative bearing surfaces for total joint arthroplasty. J Am Acad Orthop Surg 1998;6:198-203.
Question 30High Yield
A 45-year-old tennis player undergoes surgery for chronic lateral epicondylitis. After returning to play, he notes increasing lateral elbow pain with mechanical catching and locking. Examination shows positive supine posterolateral rotatory instability. What ligament has been injured?
Explanation
The patient has sustained an iatrogenic injury to the lateral ulnar collateral ligament. This injury has been reported after lateral approaches to the elbow. The orbicular, annular, and lateral radial collateral ligaments have a much less important role in lateral elbow stability. The anterior band of the ulnar collateral ligament is on the medial side of the elbow and is important for valgus stability. O'Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
Question 31High Yield
A 24-year-old man sustains an injury to his right elbow after falling 10 feet. Radiographs are shown in Figures 41a and 41b. Treatment should consist of
Explanation
Explanation
41b Transolecranon fracture-dislocations are most effectively managed with open reduction and internal fixation, followed by early aggressive range of motion. Concomitant injury to the collateral ligament is rare, and stability is achieved by anatomic reconstruction of the olecranon fracture with rigid fixation. The need for collateral ligament repair or a hinged external fixator is uncommon in this fracture pattern.
References:
- Ring D, Jupiter JB, Sanders RW, et al: Transolecranon fracture-dislocation of the elbow. J Orthop Trauma 1997;11:545-550.
Question 32High Yield
A 52-year-old man has shoulder pain and stiffness after undergoing a "mini-lateral" rotator cuff repair 6 months ago. Examination reveals that he is afebrile with normal vital signs. There is slight erythema but no drainage from the incision. Range of motion is limited in all planes, and there is weakness with resisted external rotation and abduction. Radiographs show a well-positioned metal implant within the greater tuberosity. Laboratory studies reveal a WBC count of 8,400/mm3 (normal 3,500 to 10,500/mm3) and an erythrocyte sedimentation rate of 63 mm/h (normal up to 20 mm/h). What is the next most appropriate step in management?
Explanation
Explanation
Deep sepsis of the shoulder following rotator cuff repair is an uncommon problem. Patients with infections of this type typically report persistent pain and are not systemically ill. They may have signs of local wound problems such as erythema, drainage, and dehiscence. Laboratory studies can be helpful in making an accurate diagnosis. Most patients will not show a significant elevation of the WBC count; however, an elevated erythrocyte sedimentation rate is nearly always present and should alert the clinician to the presence of infection. Aspiration of both subacromial and glenohumeral joint spaces is necessary to confirm the diagnosis. The most effective treatment for deep shoulder sepsis following rotator cuff repair involves extensive surgical debridement, removing all suspicious soft tissue as well as implants. Administration of appropriate antibiotic therapy is needed for complete control of the infection. Mirzayan R, Itamura JM, Vangsness CT, et al: Management of chronic deep infection following rotator cuff repair. J Bone Joint Surg Am 2000;82:1115-1121. Settecerri JJ, Pitnu MA, Rock MG, et al: Infection after rotator cuff repair. J Shoulder Elbow Surg 1994;8:105.
References:
- Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Question 33High Yield
A 13-year-old girl injures her ankle playing soccer. Radiographs reveal a displaced Tillaux fracture. CT scans are shown in Figure 25. What is the most important consideration for appropriate management?
Explanation
Tillaux and triplane fractures occur in adolescents as the result of an external rotation injury of the ankle. As seen on the CT scan, the growth plate starts to close during adolescence; therefore, growth arrest resulting in limb-length discrepancy or angulation is less of a concern in this age group than achieving joint congruity. The joint should be surgically reduced if displacement is greater than 2 mm to minimize the chances of late arthrosis. Kay RM, Matthys GA: Pediatric ankle fractures: Evaluation and treatment. J Am Acad Orthop Surg 2001;9:268-278. Kling TF Jr: Operative treatment of ankle fractures in children. Orthop Clin North Am 1990;21:381-392.
Question 34High Yield
A patient undergoes excision of a 3- x 3-cm soft-tissue sarcoma. The final histology results show tumor at the surgical margin. The surgical procedure performed is classified as
Explanation
Explanation
Surgical margins are classified according to the plane of dissection in relation to the tumor. An intralesional procedure is where the plane of dissection passes through the tumor. A marginal resection involves a resection where the plane of dissection is through the reactive zone of the tumor. A wide resection is through completely normal tissue outside of the reactive zone. A radical resection removes all of the muscles and/or bone of the compartment that are involved by the tumor.
References:
- Enneking WF, Spanier SS, Goodman MA: A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop 1980;153:106-120.
Question 35High Yield
A 74-year-old man reports progressive left hip pain with weight-bearing activities. A radiograph is shown in Figure 30. What is the most likely underlying diagnosis?
Explanation
Explanation
The radiograph shows enlargement of the bone, coarse trabeculation, a blastic appearance, and thickening of the cortex, revealing the classic appearance of Paget's disease in the sclerotic phase, the most common presentation. While lymphoma may present as a blastic lesion, it will not have the same enlargement, coarse trabeculation of bone, and the significant sclerosis seen here. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 211-215.
References:
- Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 1947-2000.
Question 36High Yield
Figure 10 shows the radiograph of an 18-year-old woman who sustained a spinal cord injury in a motor vehicle accident. Based on the radiographic findings, her injury is best described as
Explanation
The Allen and Ferguson mechanistic classification system is a useful tool for evaluating cervical spine injuries. Cervical fractures are classified as compressive extension, distractive extension, compressive flexion, distractive flexion, vertical compression, and lateral flexion. The patient has a distractive flexion injury.
Question 37High Yield
A 38-year-old left hand-dominant bodybuilder reports ecchymosis in the left axilla and anterior brachium after sustaining an injury while bench pressing 3 weeks ago. Coronal and axial MRI scans are shown in Figures 16a and 16b. What treatment method yields the best long-term results?
Explanation
Explanation
16b The MRI scans show a rupture of the sternocostal portion of the pectoralis major tendon. This is the most common site of rupture and bench pressing is the most common etiology. Surgical repair yields better functional outcomes and patient satisfaction for tears not only at the tendon/bone interface but also at the myotendinous junction. Bak K, Cameron EA, Henderson IJ: Rupture of the pectoralis major: A meta-analysis of 112 cases. Knee Surg Sports Traumatol Arthrosc 2000;8:113-119.
References:
- Hanna CM, Glenny AB, Stanley SN, et al: Pectoralis major tears: Comparison of surgical and conservative treatment. Br J Sports Med 2001;35:202-206.
Question 38High Yield
Which of the following are considered appropriate nonsurgical bracing/orthotic options for a supple adult-acquired flatfoot deformity with forefoot abduction, secondary to posterior tibial tendon insufficiency?
Explanation
Explanation
The initial stages of posterior tibial tendon insufficiency, where the deformity remains supple, may be treated with bracing or an orthotic for pain relief. The Arizona brace was introduced in 1988, and assists in pain relief and deformity correction by minimizing hindfoot valgus alignment, lateral calcaneal displacement, and medial ankle collapse. It is particularly helpful in those patients with advanced disease that cannot tolerate an ankle-foot orthosis. All other choices are incorrect because of the addition of lateral posting, which is not advantageous in valgus deformities. The addition of medial posting to any of the above choices would render them correct alternatives. A heel lift is applicable in Achilles tendon disorders, not posterior tibial tendon disorders. Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
References:
- Imhauser CW, Abidi NA, Frankel DZ, et al: Biomechanical evaluation of the efficacy of external stabilizers in conservative treatment of acquired flat foot deformity. Foot Ankle Int 2002;23:727-737.
Question 39High Yield
A 40-year-old man has intractable pain following 2 years of nonsurgical management for high-grade spondylolisthesis. What is the best surgical option?
Explanation
Circumferential fusion is the preferred choice for patients undergoing revision surgery following failed posterolateral fusions for isthmic spondylolisthesis as well as for those patients having primary surgery for high-grade isthmic spondylolisthesis.
Question 40High Yield
For halo traction, what is the preferred site for anterior pin placement?
Explanation
The safe zone for anterior halo pin insertion is marked laterally by the anterior border of the temporalis muscle (to avoid penetration of this muscle and relative thin cortex of the skull). Medially, the pin should be placed 4.5 cm lateral to the midline to avoid injury to the supraorbital nerve or the frontal sinus. The safe area is marked superiorly by the head equator to avoid cephalad migration of the pin and inferiorly by the supraorbital ridge to prevent displacement or penetration into the orbit.
Question 41High Yield
The mother of a 24-month-old girl reports that the child cannot rotate her right forearm. She also notes delayed development, with the child first walking at 18 months. The child has a five-word vocabulary and has not begun using simple phrases. Examination reveals that the right forearm is fixed in 80 degrees of pronation. The remainder of the examination of both upper extremities is otherwise normal. A radiograph is shown in Figure 41. Which of the following studies will best aid in diagnosis?
Explanation
Explanation
The patient has classic radioulnar synostosis. Patients with this disorder frequently have duplication of sex chromosomes. Synostosis is often seen in females with 48-XXXX or 49-XXXXX in association with delayed development and mental retardation. In males, it can be associated with 48-XXXY or 49-XXXXY. Radioulnar synostosis is not usually associated with muscle disorders, congenital heart disease, or renal anomalies. MRI of the forearm can reveal other soft-tissue anomalies, but this information is not particularly helpful in planning therapy. Osteotomy is sometimes indicated to improve rotational position of the wrist, but this patient's rotation is quite functional for everyday tasks, and rotational osteotomy is not indicated.
References:
- Rimoin DL, Connor JM, Pyeritz RE, Korf BR: Emery & Rimoin's Principles and Practice of Medical Genetics, ed 4. New York, NY, Churchill Livingstone, 2002, pp 1196-1197.
Question 42High Yield
A follow-up examination of a patient 6 weeks after knee surgery reveals a range of motion from 5 degrees to 55 degrees of flexion. Which of the following statements best summarizes the role of manipulation under anesthesia for this patient?
Explanation
Esler and associates evaluated the use of manipulation under anesthesia in 47 knees. Manipulation was considered when intensive physical therapy failed to increase flexion to more than 80 degrees. The mean time from arthroplasty to manipulation was 11.3 weeks, and the mean active flexion before manipulation was 62 degrees. One year later, the mean gain was 33 degrees. Definite sustained gains in flexion were achieved even when manipulation was performed 4 or more months after arthroplasty. An additional 21 patients who met the criteria for manipulation declined the procedure, and despite continued physical therapy, they showed no significant increase in knee flexion.
Question 43High Yield
Which of the following methods is effective in correcting recurrent dislocation following total hip arthroplasty?
Explanation
Explanation
Recurrent dislocation following total hip arthroplasty is a difficult problem to correct. Studies conducted by the Mayo Clinic show a failure rate of close to 40% with surgical treatment. A variety of methods have been successful, but no specific approach has been reported to be the most predictably successful. To select and institute the proper treatment option, the cause of the dislocation must be identified. Surgical options fall into several broad categories that include increasing soft-tissue tension (trochanteric advancement or longer neck lengths) or more stable articulation (larger diameter head component, bipolar prosthesis, or a constrained component). In a series of total hip arthroplasties done with a constrained cup, the loosening rates of the cup and the stem were reported to be 6% each, comparable to a reported series of complex revision total hip arthroplasties at a similar follow-up interval. Woo RY, Morrey BF: Dislocations after total hip arthroplasty. J Bone Joint Surg Am 1982;64:1295-1306.
References:
- Goetz DD, Capello WN, Callaghan JJ, Brown TD, Johnston RC: Salvage of a recurrently dislocating total hip prosthesis with use of a constrained acetabular component: A retrospective analysis of fifty-six cases. J Bone Joint Surg Am 1998;80:502-509.
Question 44High Yield
Figures 27a through 27c show the AP radiograph, MRI scan, and biopsy specimen of an otherwise healthy man who has a painful wrist. Serum chemistry studies are normal. What is the most likely diagnosis?
Explanation
Explanation
27b 27c The osseous sites most frequently involved by giant cell tumor of bone are the distal femur, proximal tibia, and distal radius with approximately 10% of giant cell tumors involving the distal radius. The goals of treatment are to remove the tumor completely and to preserve maximum function of the extremity.
References:
- Vander Griend RA, Funderburk CH: The treatment of giant-cell tumors of the distal part of the radius. J Bone Joint Surg Am 1993;75:899-908.
Question 45High Yield
A 27-year-old woman has a bilateral C5-C6 facet dislocation and quadriparesis after being involved in a motor vehicle accident. Initial management consisted of reduction with traction, but she remains a Frankel A quadriplegic. To facilitate rehabilitation, surgical stabilization and fusion is planned. From a biomechanical point of view, which of the following techniques is the LEAST stable method of fixation?
Explanation
In two different biomechanical studies performed in both bovine and human cadaveric spines, all posterior techniques of stabilization were found to be superior to anterior plating in flexion-distraction injuries of the cervical spine. These injuries usually have an intact anterior longitudinal ligament that allows posterior fixation to function as a tension band. Anterior plating with grafting destroys this last remaining stabilizing structure and does not allow for a tension band effect because all of the posterior stabilizing structures have been destroyed with the injury. In clinical practice, however, anterior plating can be effective in the treatment of this injury with appropriate postoperative orthotic management. Sutterlin CE III, McAfee PC, Warden KE, et al: A biomechanical evaluation of cervical spine stabilization methods in a bovine model: Static and cyclical loading. Spine 1988;13:795-802.
Question 46High Yield
A 32-year-old man has an open comminuted humeral shaft fracture. Examination reveals absence of sensation in the first web space and he is unable to fully extend the thumb, fingers, and wrist. What is the recommended treatment following irrigation and debridement of the fracture?
Explanation
There is a high incidence of partial or complete laceration of the radial nerve with high-energy open fractures of the humeral shaft. The recommended treatment is irrigation and debridement of the fracture followed by open reduction and internal fixation and exploration of the radial nerve. If the nerve is completely lacerated, primary repair may be performed but poor outcomes have been reported. If a large zone of nerve injury is identified, delayed nerve grafting is advocated. Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high energy humeral shaft fractures. J Hand Surg 2004;29:144-147. Foster RJ, Swiontkowski MR, Bach AW, et al: Radial nerve palsy caused by open humeral shaft fractures. J Hand Surg Am 1993;18:121-124.
Question 47High Yield
A 14-year-old girl reports a 3-week history of anterior thigh pain and a palpable mass after sustaining a soccer-related injury. Examination reveals a tender, firm mass in the midportion of the rectus femoris. MRI scans are shown in Figures 39a through 39c. What is the most appropriate management?


Explanation
The history, examination, and MRI scan findings are consistent with a midsubstance partial rupture of the rectus femoris muscle. This is an injury masquerading as a "pseudo tumor." The lack of an appreciable mass effect on the T1-weighted MRI scan, the defined fluid signal on the T2-weighted scans, and the lack of significant contrast enhancement after gadolinium are all most consistent with injury rather than a neoplasm. Most of these injuries respond to nonsurgical management; a few will benefit from late debridement and repair if symptoms fail to resolve in 3 to 6 months. The treatment of choice is nonsurgical management with a follow-up MRI scan to verify that the findings are resolving. Hughes C IV, Hasselman CT, Best TM, et al: Incomplete, intrasubstance strain injuries of the rectus femoris muscle. Am J Sports Med 1995;23:500-506.
Question 48High Yield
A 12-year-old boy sustained a grade III open tibial fracture 1 week ago and underwent multiple debridements and fracture fixation. He now has a soft-tissue defect that measures 6 cm x 6 cm, with an area of exposed bone and muscle on the distal medial leg that is a few centimeters proximal to the ankle. Management of the soft-tissue defect should now consist of
Explanation
The soft-tissue defect is in a very difficult position - the distal tibia. The defect is too distal for a gastrocnemius flap, and the exposed bone precludes an immediate skin graft. A free flap and skin graft would be required for closure. VAC is very effective in soft-tissue defects such as this one. Healthy granulation tissues form quickly. VAC can be the definitive treatment, or it can be used before skin grafting. Wet-to-dry dressings could promote granulation, but the process is hastened substantially by VAC. Amputation is not a consideration because there are no signs of infection or fracture healing problems at this time. Mooney JF III, Argenta LC, Marks MW, et al: Treatment of soft tissue defects in pediatric patients using the V.A.C. system. Clin Orthop 2000;376:26-31.
Question 49High Yield
Figures 56a through 56c show the radiograph, CT scan, and biopsy specimen of a 44-year-old man who underwent chemotherapy and radiation therapy for lymphoma of the distal femur 20 years ago. His current problem is most likely related to
Explanation
Explanation
56b 56c The patient has changes consistent with radiation therapy to the femur, including osteopenia and an aggressive appearing neoplasm. The tumor is most likely a radiation-induced sarcoma. This is more likely than recurrent lymphoma at this late date. It is not related to steroid use or a primary lung tumor. Mirra J (ed): Bone Tumors: Clinical, Radiologic and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, p 353.
References:
- Huvos A, Woodard H, Cahan W, et al: Postradiation osteogenic sarcoma of bone and soft tissue. A clinical pathologic study of 66 Patients. Cancer 1985;55:1244.
Question 50High Yield
A 53-year-old man with a history of severe left hip pain has a significant limp that is the result of a 5-cm limb-length discrepancy. An AP radiograph is shown in Figure 48. The underlying etiology is most likely related to a history of
Explanation
Radiographic abnormalities such as coxa magna, coxa breva secondary to growth arrest, and coxa plana and acetabular deformities are associated with healed Legg-Calve-Perthes disease. Femoral heads that were flat yet congruent with the acetabulum are at risk for disabling arthritis in the sixth decade of life in 50% of these untreated patients. As the normal ball-and-socket joint deforms to a flattened cylinder, the hip loses abduction and rotation capability, while retaining flexion and extension potential. If the femoral head is flat and is not concentric with the acetabulum, early severe arthritis occurs. Hinge abduction and anterior impingement are known sequelae of a flat, incongruent femoral head.
Question 51High Yield
Where is the underlying defect in a rhizomelic dwarf with the findings shown in Figure 5?
Explanation
The radiograph shows the typical findings of achondroplasia. The defect is in fibroblast growth factor receptor 3. The pedicles narrow distally in the lumbar spine. The pelvis is low and broad with narrow sciatic notches and ping-pong paddle-shaped iliac wings. This is often called a champagne glass pelvis. Type I collagen abnormalities are typically found in osteogenesis imperfecta, and type II collagen defects are found in spondyloepiphyseal dysplasia and Kneist syndrome. COMP is defective in multiple epiphyseal dysplasia. Sulfate transport defects are seen in diastrophic dysplasia. Johnson TR, Steinbach LS: Essentials of Musculoskeletal Imaging. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 809-812.
Question 52High Yield
A 36-year-old woman has pain and swelling of the anterior arm after undergoing arthroscopic shoulder surgery 8 months ago. At the time of the procedure, extensive debridement and synovectomy of the anterior aspect of the joint was performed to remove scar tissue that had formed after an open rotator cuff repair. Examination reveals a golf ball-sized swelling just lateral to the coracoid. The area is not warm and shows no other signs of infection. An MRI scan is shown in Figure 1. Management should now consist of
Explanation
Explanation
Deficiency of the rotator cuff interval may be acquired or congenital. In this patient, extensive debridement of the rotator cuff interval capsule at the time of arthroscopy most likely is the cause of the defect seen on the MRI scan. Surgical closure of the defect is the treatment of choice. During the repair, the shoulder should be placed in 30 degrees of external rotation to avoid overtightening. Care should be taken to include the leading edge of both the supraspinatus and subscapularis tendons in the repair because the rotator cuff interval capsular tissue is likely to be of poor quality. Cole BJ, Rodeo SA, O'Brien SJ, et al: The anatomy and histology of the rotator interval capsule of the shoulder. Clin Orthop 2001;390:129-137.
References:
- Jost B, Koch PP, Gerber C: Anatomy and functional aspects of the rotator interval. J Shoulder Elbow Surg 2000;9:336-341.
Question 53High Yield
A 17-year-old football player is injured during a play and reports abdominal pain that is soon followed by nausea and vomiting. What organ has most likely been injured?
Explanation
Explanation
The spleen is the most common organ injured in the abdomen as the result of blunt trauma. It is also the most common cause of death because of an abdominal injury. The liver is the second most commonly injured organ. Injury to the other organs is rare. The diagnosis can be made with CT. Treatment ranges from observation to splenectomy, depending on the severity of injury. Green GA: Gastrointestinal disorders in the athlete. Clin Sports Med 1992;11:453-470.
References:
- Kibler WB (ed): ACSM's Handbook for Team Physician. Philadelphia, PA, Williams & Wilkins, 1996, p 151.
Question 54High Yield
In Dupuytren's disease, the retrovascular cord typically displaces the radial proper digital nerve of the ring finger in what direction?
Explanation
Explanation
Retrovascular cords are common in Dupuytren's disease and commonly require surgical treatment. Nerve injury in Dupuytren's surgery is an infrequent complication that occurs partly because the digital nerves can be displaced from their normal anatomic relationships by retrovascular cords. The nerves are displaced superficially, toward the center of the digit (palmarly and ulnarly). This displacement is typically seen at the level of the metacarpophalangeal joint.
References:
- Rayan GM: Palmar fascial complex anatomy and pathology in Dupuytren's disease. Hand Clin 1999;15:73-86.
Question 55High Yield
Based on the type of articulation shown in Figure 32, wear is not affected by which of the following factors?
Explanation
Explanation
Wear in total hip arthroplasty is a very complex phenomenon. The radial mismatch of the femoral head to the acetabular component has been shown in multiple studies to be a significant factor in wear. The mismatch can neither be too small nor too large. When the mismatch is too small, seizing of the implants can occur. When the mismatch is too large, contact stresses increase and produce exceptionally high wear. The ideal radial mismatch should be approximately 50 microns. Surface roughness and ball sphericity are two items that are extremely important with respect to wear. High carbon content has been shown to decrease wear. This device has a very large head-to-neck ratio, so impingement-related wear is unlikely. Amstutz HC, Grigoris P: Metal on metal bearings in hip arthroplasty. Clin Orthop 1996;329:S11-S34. Amstutz HC, Campbell P, McKellop H, et al: Metal on metal total hip replacement workshop consensus document. Clin Orthop 1996;329:S297-S303.
References:
- McKellop H, Park SH, Chiesa R, et al: In vivo wear of three types of metal on metal hip prostheses during two decades of use. Clin Orthop 1996;329:S128-S140.
Question 56High Yield
Which of the following statements regarding conus medullaris syndrome is most accurate?
Explanation
Conus medullaris syndrome most frequently occurs as a result of trauma or with a disk herniation at L1, resulting in a lower motor neuron syndrome but with a poor prognosis for recovery of bowel and bladder dysfunction. The conus region, as the termination of the spinal cord, contains the motor cell bodies of the sacral roots. The syndrome is usually a sacral level neural injury; therefore, lower extremity weakness is uncommon. Haher TR, Felmly WT, O'Brien M: Thoracic and lumbar fractures: Diagnosis and management, in Bridwell KH, Dewald RL, Hammerberg KW, et al (eds): The Textbook of Spinal Surgery, ed 2. New York, NY, Lippincott Williams & Wilkins, 1977, pp 1773-1778.
Question 57High Yield
Figure 29a shows the clinical photograph of a 26-year-old woman who has had the leg deformity since birth. She reports difficulty with walking and weight bearing and notes increased discomfort and swelling when the leg is dependent. She denies any history of trauma or family history of a similar disorder. Examination reveals a fixed equinovarus deformity of the foot but no evidence of a limb-length discrepancy. No other cutaneous findings or soft-tissue masses are noted. Sagittal and axial T1- and T2-weighted MRI scans are shown in Figures 29b and 29c. What is the most likely diagnosis?


Explanation
Because the MRI scans show marked dilation and proliferation of lymphatic channels that completely involve all the leg muscles and the clinical photograph shows the severe swelling associated with this disease, the most likely diagnosis is lymphangiomatosis. Poliomyelitis affects the anterior horn cells and manifests as muscle atrophy. Neurofibromatosis can have a similar clinical appearance but usually is associated with other systemic and cutaneous findings. Congenital band syndrome results in amputated or shortened extremities. Chronic venous stasis disease usually is not associated with joint contractures, and typically it affects older individuals. Surgical excision is the only known treatment; this patient underwent an above-knee amputation. Berquist TH (ed): MRI of the Musculoskeletal System, ed 3. Philadelphia, PA, Lippincott Raven, 1997, p 771.
Question 58High Yield
A 45-year-old man has severe pain in both feet after his boots become wet while hunting. Examination 3 hours after the onset of symptoms reveals that his feet are cold to touch and the skin appears blanched. Management should consist of
Explanation
Explanation
The patient has frostbite involving both feet. Rapid rewarming in a protected environment is the initial treatment. A footbath with water at 104.0 degrees F to 107.6 degrees F (40 degrees C to 42 degrees C) is ideal. This facilitates a uniform rewarming of the involved tissue. The other choices are less than ideal. Appliances such as heating pads provide uneven heating and may actually burn the skin. Pinzur MS: Frostbite: Prevention and treatment. Biomechanics 1997;4:14-21.
References:
- Fritz RL, Perrin DH: Cold exposure injuries: Prevention and treatment. Clin Sports Med 1989;8:111-128.
Question 59High Yield
A 12-year-old boy sustained a both bone forearm fracture 10 weeks ago and underwent closed reduction and casting. Examination now reveals that the injury is healed, but he is unable to extend his little and ring fingers of the injured hand with his wrist extended. Full extension is possible with the wrist flexed. A radiograph and clinical photograph are shown in Figures 15a and 15b. The remainder of his hand and wrist examination and neurologic evaluation in the hand are normal. What is the most likely diagnosis?

Explanation
In this patient, examination reveals an inability to extend the fingers with the wrist extended, but full extension is possible with wrist flexion. These findings demonstrate isolated tenodesis of the flexor digitorum to the ring and little fingers. These findings are not consistent with compartment syndrome or nerve injury. Scarring or entrapment of tendons in forearm fractures can occur. Watson PA, Blair W: Entrapment of the index flexor digitorum profundus tendon after fracture of both forearm bones in a child. Iowa Orthop J 1999;19:127-128. Shaw BA, Murphy KM: Flexor tendon entrapment in ulnar shaft fractures. Clin Orthop 1996;330:181-184. Kolkman KA, van Niekerk JL, Rieu PN, et al: A complicated forearm greenstick fracture: Case report. J Trauma 1992;32:116-117.
Question 60High Yield
What is the most common foot and ankle deformity in patients with arthrogryposis?
Explanation
Explanation
Clubfoot (talipes equinovarus) in patients with arthrogryposis is a rigid and resistant deformity. However, multiple studies document limited success with nonsurgical management. Manipulation and casting are generally a preliminary treatment before surgery; successful correction will most like require a talectomy. Guidera KJ, Drennan JC: Foot and ankle deformities in arthrogryposis multiplex congenita. Clin Orthop 1985;194:93-98. Handelsman JE, Badalamente MA: Neuromuscular studies in clubfoot. J Pediatr Orthop 1981;1:23-32.
References:
- Dias LS, Stern LS: Talectomy in the treatment of resistant talipes equinovarus deformity in myelomeningocele and arthrogryposis. J Pediatr Orthop 1987;7:39-41.
Question 61High Yield
A 45-year-old man has had left thigh pain for the past 4 months. An AP radiograph, bone scan, MRI scans, and biopsy specimens are shown in Figures 6a through 6f. What is the most appropriate treatment?





Explanation
The radiograph demonstrates thickened trabeculae and thickened cortices in the left proximal femur compared to the right, and the bone scan shows increased uptake in this area. The MRI scans show thickened trabeculae with normal marrow signal. These findings are diagnostic of Paget's disease. Medical treatment, including bisphosphonates and calcitonin, is indicated for painful bone lesions. Hadjipavlou AG, Gaitanis IN, Kontakis GM: Paget's disease of the bone and its management. J Bone Joint Surg Br 2002;84:160-169.
Question 62High Yield
Figure 10 shows the MRI scan of a 56-year-old woman with metastatic breast cancer who now reports progressive paraparesis. Her general health remains good. Treatment should consist of
Explanation
If the patient's medical condition and prognosis remain good in the presence of significant and progressive neurologic deficit from cord compression, then the most reliable means of restoring function is via surgical decompression and fusion. Decompression should be directed toward the compressing structure (eg, anteriorly if the compression is from the anterior side). This procedure can be done via a posterolateral technique, such as costotransversectomy in some cases.
Question 63High Yield
A 78-year-old man being seen for routine follow-up studies reports mild to moderate pain in his left arm. The patient has a history of lung cancer and severe heart disease. A radiograph and a bone scan are shown in Figures 36a and 36b. Treatment should consist of

Explanation
The patient has lung cancer metastatic to the left humerus that is mildly to moderately symptomatic. Radiographically, the lesion is small and is not associated with significant cortical destruction. Metastatic lesions in the upper extremity have a lower incidence of pathologic fracture than lesions in the lower extremity.
Question 64High Yield
Retrograde ejaculation is most commonly associated with what surgical approach?
Explanation
Explanation
Retrograde ejaculation is the sequela of an injury to the superior hypogastric plexus. This structure needs protection, especially during anterior exposure of the lumbosacral junction. Although the superior hypogastric plexus can be injured with anterior or anterolateral spine surgery at any lumbar level, it is most at risk with anterior transperitoneal approaches to the lumbosacral junction. To avoid this complication, the use of monopolar electrocautery should be avoided during deep dissection in this region. The ideal anterior exposure starts with blunt dissection just to the medial aspect of the left common iliac vein sweeping the prevertebral tissues toward the patient's right side. Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492. Watkins RG (ed): Surgical Approaches to the Spine. New York, NY, Springer-Verlag, 1983, p 107.
Question 65High Yield
What part of the glenoid labrum has the least vascularity?
Explanation
Explanation
The glenoid labrum receives its blood supply from the suprascapular, posterior humeral circumflex, and circumflex scapular arteries. The labral vessels arise from the capsular and periosteal vessels that penetrate the periphery of the labrum. The bone does not appear to be a source of vascularity. The posterior/superior and inferior labrum have a fairly robust vascular supply, whereas the anterior/superior labrum has relatively poor vascularity, which may influence the success of superior lateral repairs.
References:
- Cooper DE, Arnoczky SP, O'Brien SJ, et al: Anatomy, histology and vascularity of the glenoid labrum: An anatomical study. J Bone Joint Surg Am 1992;74:46-52.
Question 66High Yield
Based on the MRI scan shown in Figure 6, the abnormal signal is seen in what carpal bone?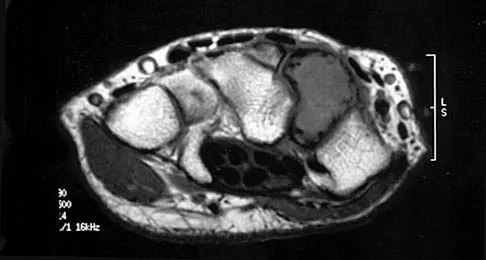
Explanation
The MRI scan reveals an abnormal signal in the trapezoid, which lies adjacent to the capitate in the distal carpal row. The tumor is a giant cell tumor of bone. Cooney WP, Linscheid RL, Dobyns JH: The Wrist: Diagnosis and Operative Treatment. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 278-282. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2238-2240. bar based on these measurements is shown in Figure 54d. Initial treatment should consist of 1- bony bar resection and distal fibula epiphysiodesis. 2- bony bar resection and corrective osteotomy. 3- bony bar resection and physiodesis of the opposite distal tibial physis. 4- corrective osteotomy and a limb-lengthening procedure. 5- corrective osteotomy and physiodesis of the opposite distal tibial physis. 2 54a 54b 54c 54d Mapping of a physeal bar from biplane polytomography or CT helps to identify lesions that should be treated surgically and aids in planning the surgical approach and resection. Criteria for surgical excision are at least 2 years of longitudinal growth remaining and involvement of no more than 50% of the physis. Osteotomy is required if angular deformity is greater than 20 degrees. Although this physeal bar is large, it is slightly less than 50% of the total area of the physis. Limb lengthening in this case should be reserved for failure of bar resection. Physiodesis of the opposite distal tibia at this age would result in disproportionate shortening of both tibiae. Carlson WO, Wenger DR: A mapping method to prepare for surgical excision of a partial physeal arrest. J Pediatr Orthop 1984;4:232-238.
Question 67High Yield
A 79-year-old woman reports a history of left leg pain with walking. Her pain is exacerbated with walking and stair climbing, and her symptoms are improved by standing after she stops walking. Lumbar flexion does not provide any significant improvement of the symptoms and sitting does not significantly change symptoms. Her leg pain is worse at night and she obtains relief by hanging her leg over the side of the bed. The neurologic examination is essentially normal. Examination of the lower extremities demonstrates mild early trophic changes, and her pulses distally are palpable but are diminished bilaterally. Radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management?
Explanation
Explanation
15b The patient has symptoms that are more consistent with vascular claudication than with the pseudoclaudication anticipated from lumbar spinal stenosis. Therefore, the patient is a candidate for further vascular work-up. The radiographs reveal early spinal stenosis and spondylolisthesis at L4-5 but also show significant calcification of the iliac arteries, suggestive of peripheral vascular disease. Vascular claudication is a manifestation of peripheral vascular disease and presents with crampy leg pain that is exacerbated by physical exertion. The pain is easily relieved by standing still or sitting. Unlike pseudoclaudication, a forward-flexed posture and/or sitting does not improve the symptoms. Night pain is common in vascular claudication due to the elevation of the extremities and patients often report pain improvement by hanging their extremities in a dependent position. In evaluation of a patient with suspected vascular claudication, the five "P's" of vascular insufficiency should be monitored, including pulselessness, paralysis, paresthesia, pallor, and pain. While pain and paresthesias can be common in both vascular claudication and pseudoclaudication, the presence of any of the remaining symptoms is suggestive of vascular disease. Aufderheide TP: Peripheral arteriovascular disease, in Rosen P, Barkin R (eds): Emergency Medicine: Concepts and Clinical Practice, ed 4. St Louis, MO, Mosby, 1998, pp 1826-1844.
Question 68High Yield
The view from an anterosuperior portal of the right shoulder shown in Figure 12 reveals which of the following findings?
Explanation
Explanation
The arthroscopic view shows a HAGL lesion. With the arthroscope directed anteroinferiorly, muscular striations of the subscapularis can be visualized through the avulsion site. In vitro strain studies indicate that glenohumeral ligament failure on the humeral side occurs in approximately 25% of patients, while clinically this lesion has been reported in approximately 9% of patients with shoulder instability. Failure to recognize and treat this lesion leads to persistent anterior instability. An ALPSA lesion, a Bankart variant, occurs on the glenoid side and is characterized by a sleeve-like medial retraction and inferior rotation. A Bankart lesion is the classic avulsion of the glenohumeral ligament from the glenoid rim. The subscapularis tendon and the rotator interval are not shown in the figure. Wolf EM, Cheng JC, Dickson K: Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607. Bigliani LU, Pollack RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
References:
- Warner JJ, Beim GM: Combined Bankart and HAGL lesion associated with anterior shoulder instability. Arthroscopy 1997;13:749-752.
Question 69High Yield
A 2-year-old girl was born with the toe deformity shown in Figure 2. She has difficulty wearing shoes despite having adequate room in the toe box. Management at this time should consist of
Explanation
Explanation
The patient has a congenital curly toe deformity of the third toe, and tenotomy of the toe flexors is highly effective for this problem. Stretching and taping are ineffective for this deformity. The position of the second toe is secondary; therefore, procedures on that toe are unnecessary and ineffective. The flexor to extensor transfer is a more complicated procedure that produces negligible results, or may even worsen the deformity. Resection arthroplasty is contraindicated because it causes abnormal growth of the toes. Hamer AJ, Stanley D, Smith TW: Surgery for curly toe deformity: A double-blind, randomized, prospective trial. J Bone Joint Surg Br 1993;75:662-663. Ross ER, Menelaus MB: Open flexor tenotomy for hammer toes and curly toes in childhood. J Bone Joint Surg Br 1984;66:770-771.
References:
- Sullivan JA: The child's foot, in Morrissy RT, Weinstein SL (eds): Lovell & Winter's Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1077-1135.
Question 70High Yield
A 36-year-old woman is brought to the emergency department intubated and sedated following a motor vehicle accident. She is moving her upper and lower extremities spontaneously. She cannot follow commands. CT scans are shown in Figures 7a through 7c. The initial survey does not reveal any other injuries. Initial management of the cervical injury should consist of immediate
Explanation
Explanation
7b 7c The patient has a bilateral facet dislocation of C6-C7 with preservation of at least some neurologic function. Urgent reduction is necessary. However, because she is sedated and unable to follow commands, an MRI scan is necessary before any closed or open posterior reduction to look for an associated disk herniation. If a disk herniation is present, it must be removed prior to any reduction maneuver to prevent iatrogenic neurologic injury. It is very unlikely that this injury can be reduced with an open anterior procedure alone. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 189-199.
Question 71High Yield
Which of the following is considered the most important factor in eliminating infection in chronic osteomyelitis?
Explanation
Explanation
The most important factor in eliminating infection in chronic osteomyelitis is a complete debridement of the compromised bone and soft tissue. Antibiotics should be used in conjunction with surgical debridement. However, the foundation of treating infected bone is removal of the diseased tissue. Cierny G III, Cook WG, Mader JT: Ankle arthrodesis in the presence of ongoing sepsis: Indications, methods, and results. Orthop Clin North Am 1989;20:709-721. Cierny G, Zorn EZ: Arthrodesis of the tibiotalar joint for sepsis. Foot Ankle Clin 1996;1:177-197.
References:
- Richter D, Hahn MP, Laun RA, Ekkernkamp A, Muhr G, Osterman PA: Arthrodesis of the infected ankle and subtalar joint: Technique, indications and results of 45 consecutive cases. J Trauma 1999;47:1072-1078.
Question 72High Yield
A 46-year-old man sustains a calcaneal fracture in a fall off a scaffold. During surgical reconstruction using an extended lateral incision, the fracture is reduced and fixed with a plate and screws. One of the posterior facet screws is found to be 5 mm out of the bone on the Harris view. What structure is most likely at risk because of this finding?
Explanation
Explanation
The abductor hallucis muscle is the most medial structure. The posterior tibial tendon and the flexor digitorum longus tendon lie more cephalad to the sustentaculum tali. There is a groove under the sustentaculum for the flexor hallucis longus tendon. Subchondral lag screws placed across the posterior facet exit the medial side of the calcaneus in this groove. Just medial to the flexor hallucis longus tendon is the neurovascular bundle. A screw that is out of the bone a short distance can cause triggering of the flexor hallucis longus tendon. Patients will report loss of great toe excursion in the early postoperative period. Accurate measurement of subchondral lag screw length avoids this complication. Hollinshead WH: Anatomy for Surgeons, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 802-852. Rosenberg AS, Cheung Y: Diagnostic imaging of the ankle and foot, in Jahss MH (ed): Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991, pp 109-154.
References:
- Waggoner AM, Smith JW: Internal fixation of calcaneus fractures: An anatomical study of structures at risk. J Orthop Trauma 1995;9:107-112.
Question 73High Yield
A 12-year-old girl has had pain in her right knee for 1 month that started as activity-related and progressed to night pain. Radiographs are shown in Figures 16a and 16b, and a biopsy specimen is shown in Figure 16c. What is the recommended treatment?
Explanation
Explanation
16b 16c This is a classic appearance for an osteosarcoma. The radiographs reveal a mixed osteolytic and osteoblastic lesion in a skeletally immature patient in the distal right femoral metaphysis. The pain pattern with progressive symptoms leading to the presence of night pain is also typical for this condition. The biopsy specimen reveals pleomorphic cells and the presence of osteoid. The current standard of care in the treatment of osteosarcoma is neoadjuvant chemotherapy followed by surgical resection or amputation followed by additional postoperative chemotherapy. Osteosarcoma is not radiosensitive. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
References:
- McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 205.
Question 74High Yield
What is the most common reason for reoperation in total knee arthroplasty?
Explanation
Patellar problems currently constitute the largest number of complications after total knee arthroplasty, affecting between 8% and 35% of patients. These problems include patellar instability, fracture, component loosening, surface erosion, and pain. Malalignment, as an isolated reason for revision, is uncommon, yet it contributes to accelerated wear of the components. Joint instability affects up to 6% of patients, and the infection rate in knee arthroplasty is around 1% to 2%. Blasier RB, Matthews LS: Complications of prosthetic knee arthroplasty, in Epps CH (ed): Complications in Orthopaedic Surgery. Philadelphia, PA, JP Lippincott, 1994, pp 1066-1069. Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620.
Question 75High Yield
A patient who underwent an L5-S1 diskectomy 18 months ago has persistent pain in the left leg. Figures 9a and 9b show postoperative axial T1-weighted MRI scans at the L5-S1 level without and with gadolinium. What is the most likely diagnosis?
Explanation
Explanation
9b Persistent or recurrent symptoms after lumbar diskectomy are troublesome and can be difficult to assess. Gadolinium-enhanced MRI scans may be helpful. The images show enhancement about the left S1 root, a finding that is most consistent with perineural (epidural) fibrosis. The root itself does not enhance. Root enhancement has been associated with compressive radicular symptoms. A disk herniation does not enhance with gadolinium. A neurilemmoma enhances with gadolinium, but the involved root would be enlarged. There is no evidence of a fluid collection which would be consistent with an epidural abscess. Babar S, Saifuddin A: MRI of the post-discectomy lumbar spine. Clin Radiol 2002;57:969-981. Kikkawa I, Sugimoto H, Saita K, et al: The role of Gd-enhanced three-dimensional MRI fast low-angle shot (FLASH) in the evaluation of symptomatic lumbosacral nerve roots. J Orthop Sci 2001;6:101-109.
References:
- Vroomen PC, Van Hapert SJ, Van Acker RE, et al: The clinical significance of gadolinium enhancement of lumbar disc herniations and nerve roots on preoperative MRI. Neuroradiology 1998;40:800-806.
Question 76High Yield
A 40-year-old patient who has a type II odontoid fracture is placed in a halo vest for 12 weeks; however, current radiographs show no evidence of healing. The next most appropriate step in management should consist of
Explanation
Because nonsurgical managment has failed and a significant number of type II odontoid fractures will go on to a nonunion, the salvage treatment of choice is posterior fusion at C1-2. Odontoid screws are contraindicated in patients with a chronic nonunion, which this patient has at the end of 3 months. Montesano PX: Anterior and posterior screw and plate techniques used in the cervical spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1996, vol 2, pp 1743-1761. Bohler J: Anterior stabilization for acute fractures and non-unions of the dens. J Bone Joint Surg Am 1982;64:18-27.
Question 77High Yield
A 32-year-old laborer reports left ankle pain and deformity. History reveals that he sustained a left ankle fracture 2 years ago and was treated with closed reduction and casting. Radiographs are shown in Figures 25a through 25c. What is the most appropriate management?


Explanation
Corrective osteotomy of fibular malunions, with appropriate lengthening, even in the presence of early arthritis, has been shown to decrease ankle pain and increase stability. Reduction and bone grafting of the medial malleolar nonunion is also needed. There is no evidence supporting the use of intra-articular steroids or hyaluronic acid in the ankle joint. Lateral talar displacement of even 1 mm has been reproducibly shown to decrease tibiotalar contact by 40% to 42%, causing a predisposition to arthritis. Weber D, Friederich NF, Muller W: Lengthening osteotomy of the fibula for post-traumatic malunion: Indication, technique and results. Int Orthop 1998;22:149-152. Lloyd J, Elsayed S, Hariharan K, et al: Revisiting the concept of talar shift in ankle fractures. Foot Ankle Int 2006;27:793-796. Offierski CM, Graham JD, Hall JH, et al: Later revision of fibular malunion in ankle fractures. Clin Orthop Relat Res 1982;171:145-149.
Question 78High Yield
A 30-year-old elite marathon runner reports chronic pain over the lateral aspect of the distal right leg and dysesthesia over the dorsum of the foot with active plantar flexion and inversion of the foot. Examination reveals a tender soft-tissue fullness approximately 10 cm proximal to the lateral malleolus. The pain is exacerbated by passive plantar flexion and inversion of the ankle. There is also a positive Tinel's sign over the site of maximal tenderness. There is no motor weakness, and deep tendon reflexes are normal. Radiographs and MRI of the leg are normal. What is the next most appropriate step in management?
Explanation
Explanation
The patient has entrapment of the superficial peroneal nerve against its fascial opening in the distal leg. It is typically exacerbated by passive or active plantar flexion and inversion of the foot, which leads to traction of the nerve as it exits this opening. Treatment involves release of the fascial opening to reduce this traction phenomenon. Closure of the defect will only aggravate the condition and potentially result in an exertional compartment syndrome. A four-compartment fasciotomy is only indicated for an established compartment syndrome of the leg. Styf J: Diagnosis of exercise-induced pain in the anterior aspect of the lower leg. Am J Sports Med 1988;16:165-169. Sridhara CR, Izzo KL: Terminal sensory branches of the superficial peroneal nerve: An entrapment syndrome. Arch Phys Med Rehabil 1985;66:789-791.
References:
- Styf J: Entrapment of the superficial peroneal nerve: Diagnosis and results of decompression. J Bone Joint Surg Br 1989;71:131-135.
Question 79High Yield
An 83-year-old woman with a long history of her foot slowly and progressively "turning out" now reports significant ankle pain. History reveals that she has significant cardiac disease and exercise-induced angina. Examination reveals a deficiency in the posterior tibial tendon; however, the hindfoot remains moderately supple. Radiographs reveal a valgus tilt of the tibiotalar joint and early arthrosis. What is the most appropriate orthotic management?
Explanation
The patient will continue to have pain secondary to the ankle arthrosis with both the UCBL and the molded articulated ankle-foot orthosis. The total contact orthotic does not provide enough hindfoot control to support the progressive collapse of the ankle into valgus positioning. A molded leather gauntlet will not only control tibiotalar motion but also control hindfoot motion and allow support of the longitudinal arch.
Question 80High Yield
A 29-year-old woman reports dysesthesias and burning after undergoing bunion surgery that consisted of a proximal crescentic first metatarsal osteotomy 6 months ago. Examination reveals a positive Tinel's sign at the proximal aspect of the healed incision. What injured nerve is responsible for her continued symptoms?
Explanation
Painful incisional neuromas after bunion surgery frequently involve the dorsomedial cutaneous branch of the superficial peroneal nerve. This is the medial branch of the superficial peroneal nerve that terminates as the dorsomedial cutaneous nerve to the hallux. Branches of the deep peroneal nerve to this area are rare, and no branches to this area exist from the sural nerve. The saphenous nerve branches are generally more proximal, and the medial plantar nerve lies plantarly. Kenzora JE: Sensory nerve neuromas: Leading to failed foot surgery. Foot Ankle 1986;7:110-117.
Question 81High Yield
Spontaneous entrapment of the posterior interosseous nerve most commonly occurs in which of the following locations?
Explanation
The extensor carpi radialis brevis, supinator muscle, arcade of Frohse, and leash of Henry are potential sites of compression for the posterior interosseous nerve. The most common location of spontaneous entrapment is the arcade of Frohse. The lateral intermuscular septum is a site of compression for the radial nerve.
Question 82High Yield
Figure 24 shows the radiograph of an otherwise healthy 56-year-old patient who reports hip pain after undergoing a primary cementless hip replacement 4 months ago. The next most appropriate step should consist of
Explanation
Periosteal new bone formation is a warning sign of prosthetic infection. Indomethacin may prevent heterotopic ossification if given early enough; however, it is irrelevant in this patient. A C-reactive protein and a sed rate are useful screening studies that add to the predictive value of the radiographs and may be performed routinely if sepsis is suspected. A bone scan obtained 4 months after surgery would show increased uptake in all cases. If results of a sed rate and C-reactive protein are normal, then a biopsy should be considered to rule out a neoplasm.
Question 83High Yield
Storage of musculoskeletal allografts by cryopreservation is achieved by
Explanation
Cryopreservation uses chemicals to remove cellular water and controlled rate freezing to prevent ice crystal formation. The tissue is procured, cooled to wet ice temperature for quarantine, and then stored in a container with cryoprotectant solution of dimethyl sulfoxide or glycerol which displaces the cellular water. The controlled rate freezing is then done to prevent ice crystal formation. Fresh allografts are not frozen in order to maintain maximum cellular viability, and this process limits the shelf life of osteochondral allografts. Freeze-drying involves replacement of water in the tissue with alcohol to a moisture level of 5% and then uses a vacuum process to remove the alcohol from the tissue. Preparation of fresh frozen grafts involves freezing the graft twice and packaging the tissue without solution at minus 80 degrees C. American Association of Tissue Banks: Standards for Tissue Banking. MacLean, VA, American Association of Tissue Banks, 1999. Vangsness CT Jr, Triffon MJ, Joyce MJ, et al: Soft tissue allograft reconstruction of the human knee: A survey of the American Association of Tissue Banks. Am J Sports Med 1996;24:230-234.
Question 84High Yield
The scoring system for impending pathologic fractures devised by Mirels involves assessment of which of the following factors?
Explanation
Explanation
The scoring system published by Mirels in 1989 is based on the following characteristics: the location of the lesion, the amount of pain the patient is experiencing, the type of lesion (either lucent, mixed, or blastic), and the lesion size. The tumor is scored from 1 to 3 in each category and a total score is obtained that correlates to fracture risk. Prophylactic fixation is advised for lesions with scores of higher than 8, and consideration for stabilization should be strongly considered for scores of 8. The Mirels scoring system can be useful as an adjunct to clinical decision making. Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. 1989. Clin Orthop Relat Res 2003;415:S4-S13.
References:
- Damron TA, Morgan H, Prakash D, et al: Critical evaluation of Mirels' rating system for impending pathologic fractures. Clin Orthop Relat Res 2003;415:S201-S207.
Question 85High Yield
Which of the following nerves is most likely responsible for symptoms associated with plantar fasciitis?
Explanation
The first branch of the lateral calcaneal nerve innervates the abductor digiti minimi. It is reported to be trapped at the interval between the abductor hallucis and the quadratus plantae muscles.
Question 86High Yield
A female cross-country runner has an insidious onset of right groin pain. Radiographs of the right hip reveal a tension-side stress fracture. History reveals that she was treated for a "foot" fracture 1 year ago. In addition to performing internal fixation of the femoral neck, which of the following should be obtained?
Explanation
Explanation
Stress fractures in female long distance runners are frequently associated with the Female Athletic Triad. The triad consists of osteoporosis, amenorrhea, and altered eating habits. A thorough menstrual history, including age of menarche, history of amenorrhea, and use of oral contraceptives, is imperative. Amenorrhea leads to osteoporosis and predisposes the athlete to fractures. An MRI of the hip is not necessary because a fracture is evident on the radiograph. Serum calcium levels are normal in osteoporosis, a family history would be noncontributory, and it is highly unlikely that a contralateral hip radiograph will yield useful information. Bennell KL, Malcolm SA, Thomas SA, et al: Risk factors for stress fractures in track and field athletes: A twelve-month prospective study. Am J Sports Med 1996;24:810-818.
References:
- Barrow GW, Saha H: Menstrual irregularity and stress fractures in collegiate female distance runners. Am J Sports Med 1988;16:209-216.
Question 87High Yield
A 25-year-old professional baseball pitcher reports a 4-month history of gradually increasing medial elbow pain that occurs during the late cocking and acceleration phases of throwing. The pain occasionally refers distally along the ulnar aspect of the forearm. He denies any weakness; however, he notes occasional paresthesias. A nerve conduction velocity study demonstrates increased latency across the cubital tunnel. Management consisting of 6 weeks of rest and rehabilitation fails to provide relief as the symptoms returned when he resumed throwing. What is the best course of action?
Explanation
In the thrower's elbow, ulnar neuritis is felt to result from both chronic compression and traction on the nerve that occurs during the throwing motion. Occasionally, subluxation of the nerve also can lead to symptoms. If nonsurgical management fails to provide relief, transposition of the nerve to an anterior subcutaneous location is the surgical procedure of choice. The nerve is held in its new position by one or two fascial slings created from the fascia of the common flexor origin. Schickendantz MS: Diagnosis and treatment of elbow disorders in the overhead athlete. Hand Clin 2002;18:65-75.
Question 88High Yield
A 62-year-old woman reports diffuse aches and pains of the hip and pelvis. She denies any significant trauma but does have a history of chronic anemia. Figure 17a shows a radiograph of the pelvis, and Figures 17b and 17c show T2-weighted MRI scans. What is the most likely diagnosis?
Explanation
Explanation
17b 17c The radiograph reveals diffuse osteopenia and areas in the proximal femora that are moth-eaten in appearance. The extent of the marrow-replacing process is evident on the MRI scans, which reveal signal abnormality throughout the entire pelvis and both proximal femora. This represents a marrow-packing process, of which multiple myeloma is the best choice. This diagnosis is also supported by the anemia noted on the patient's history. Metastatic carcinoma and lymphoma also may have a similar presentation.
References:
- Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 2189-2216.
Question 89High Yield
Figures 15a through 15c show the radiographs of a 23-year-old football player who was injured when another player fell on his flexed and planted foot. He reports severe pain in the midfoot with a feeling of numbness on the dorsum of the foot, and he is unable to bear weight on the limb. Examination reveals mild swelling. Management should consist of


Explanation
Myerson and associates studied the outcomes of 19 patients with tarsometatarsal joint injuries during athletic activity. Injuries were classified as first- or second-degree sprains of the tarsometatarsal joint or a third-degree sprain with diastasis between the metatarsals or cuneiforms. Poor functional results were seen in those with a delay in diagnosis and with inadequate treatment. For patients with third-degree sprains, poor results were obtained with nonsurgical management. These patients required open reduction and internal fixation for optimal return to function. The anatomic reduction is critical to the outcome; therefore, open reduction is preferred. Baxter DE: The Foot and Ankle in Sport, ed 1. St Louis, MO, Mosby, 1995, pp 107-123. Curtis MJ, Myerson M, Szura B: Tarsometatarsal joint injuries in the athlete. Am J Sports Med 1993;21:497-502. Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Question 90High Yield
The blood supply to the anterior cruciate ligament is primarily derived from what artery?
Explanation
Explanation
Microvascular studies have shown that the majority of the blood supply to the cruciate ligaments comes from the middle geniculate artery, although there is collateral flow through the other geniculates and from bone. Arnoczky SP: Blood supply to the anterior cruciate ligament and supporting structures. Orthop Clin North Am 1985;16:15-28.
References:
- Arnoczky SP, Rubin RM, Marshall JL: Microvasculature of the cruciate ligaments and its response to injury. J Bone Joint Surg Am 1979;61:1221-1229.
Question 91High Yield
A 23-year-old man who was the restrained driver in a car involved in a high-speed motor vehicle accident sustained the closed injury shown in Figures 32a through 32c. Which of the following factors has the greatest impact on the risk of osteonecrosis?
Explanation
Explanation
32b 32c The incidence of osteonecrosis following displaced talar neck fractures is most related to the extent of initial fracture displacement. With increasing fracture displacement, the tenuous vascular supply to the talar body is more at risk for damage, thereby increasing the risk of osteonecrosis. Although displaced talar neck fractures have historically been considered a surgical emergency, recent studies have shown that the timing of surgical intervention bears no impact on the development of osteonecrosis. While nicotine use has an influence on fracture healing, it has never been shown to be a factor in osteonecrosis, nor has posterior-to-anterior screw fixation or the quality of fracture reduction. Lindvall E, Haidukewych G, Dipasquale T, et al: Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am 2004;86:2229-2234.
Question 92High Yield
A collegiate football player who sustained an injury to his neck has significant neck pain and weakness in his extremities. Following immobilization, which of the following steps should be taken prior to transport?
Explanation
Prior to transport, the face mask should be removed so that the airway can be easily accessible. If serious injury is suspected, the helmet and shoulder pads should be left in place until he is assessed at the hospital and radiographs are obtained. Leaving the helmet and shoulder pads in place helps to keep the spine in the most neutral alignment. Removal of the helmet will result in extension of the neck, whereas removal of the shoulder pads will most likely result in flexion of the neck. Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 376. Thomas B, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347. Waninger KN, Richards JG, Pan WT, et al: An evaluation of head movement in backboard-immobilized helmeted football, lacrosse, and ice hockey players. Clin J Sport Med 2001;11:82-86. Donaldson WF III, Lauerman WC, Heil B, et al: Helmet and shoulder pad removal from a player with suspected cervical spine injury: A cadaveric model. Spine 1998;23:1729-1732.
Question 93High Yield
A 24-year-old professional football player underwent surgery for a symptomatic cervical disk herniation with radiculopathy 9 months ago. A current radiograph is shown in Figure 17. He has normal neurologic findings, no pain, and full range of motion. A CT scan shows a solid fusion. When can he expect to return to play?
Explanation
Explanation
The radiograph shows that the two-level anterior cervical diskectomy and fusion has healed. In addition, the patient has good range of motion and the neurologic examination is normal. Based on these findings, the patient can return to play immediately. Patients with one- or two-level anterior cervical diskectomies and fusions that have healed fully can return to play. Any loss of motion, persistent neurologic deficit, or significant adjacent segment degeneration may preclude a player from returning. Thomas B, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
References:
- Torg JS, Ramsey-Emrhein JA: Management guidelines for participation in collision activities with congenital, developmental, or post-injury lesions involving the cervical spine. Clin Sports Med 1997;16:501-530.
Question 94High Yield
Where does the median nerve pass in the proximal forearm?
Explanation
Explanation
The median nerve passes through the pronator teres and deep to the flexor digitorum superficialis. The ulnar artery passes deep to both. Anderson JE (ed): Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Williams and Wilkins, 1978, pp 6-55.
References:
- Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 120.
Question 95High Yield
A healthy 16-year-old boy has had increasing pain in the right knee for the past 3 months. Examination reveals warmth and swelling around the distal femur. Radiographs and an MRI scan are shown in Figures 51a through 51c, and a biopsy specimen is shown in Figure 51d. What is the most likely diagnosis?


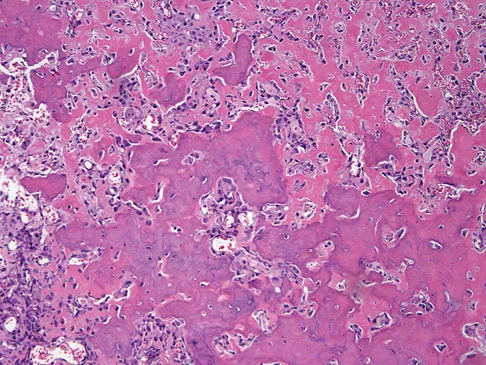
Explanation
The radiographs show a bone-producing lesion in the distal femoral metaphysis in this case of classic osteosarcoma presenting in the most common location, the distal femur. The coronal MRI scan reveals a marrow-occupying lesion with extension into the soft tissues. The histology shows osteoid production by pleomorphic cells consistent with an osteosarcoma. Ewing's sarcoma is a bone tumor characterized by uniform small blue cells on histology. Rhabdomyosarcoma is the most common childhood soft-tissue sarcoma. Osteomyelitis has an inflammatory appearance on histology. Malignant fibrous histiocytoma of bone has a lytic radiographic appearance and a pleomorphic storiform pattern without osteoid on histology. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
Question 96High Yield
Lumbar instability may be surgically induced by
Explanation
In cadaveric studies, unilateral facetectomy, or excision of 50% or more of both facets, significantly decreases the biomechanic integrity of the motion segment and may increase the risk of iatrogenic instability. Sacrifice of the spinous process, interspinous ligaments, and ligamentum flavum weakens the motion segment but does not increase the risk for instability. Facetectomy, even unilateral, predisposes the patient toward lumbar instability.
Question 97High Yield
A 66-year-old woman who previously underwent hemiarthroplasty 2 years ago for a fracture continues to have severe pain and loss of motion despite undergoing physical therapy. A radiograph is shown in Figure 2. What is the most likely reason that this patient has failed to improve her motion?
Explanation
The radiograph shows tuberosity malposition. The effect of improper prosthetic placement has also been associated with poor outcomes. However, the malposition of the tuberosity seen on the radiograph clearly explains loss of motion in this patient. It has been demonstrated that the functional results after hemiarthroplasty for three- and four-part proximal humeral fractures appear to be directly associated with tuberosity osteosynthesis. The most significant factor associated with poor and unsatisfactory postoperative functional results was malposition and/or migration of the tuberosities. Factors associated with a failure of tuberosity osteosynthesis in a recent study were poor initial position of the prosthesis, poor position of the greater tuberosity, and women older than age 75 years (most likely with osteopenic bone). Greater tuberosity displacement has been identified by Tanner and Cofield as being the most common complication after prosthetic arthroplasty for proximal humeral fractures. Furthermore, Bigliani and associates examined the causes of failure after prosthetic replacement for proximal humeral fractures and found that although almost all failed cases had multiple causes, the most common single identifiable reason was greater tuberosity displacement. Bigliani LU, Flatow EL, McCluskey G, et al: Failed prosthetic replacement for displaced proximal humeral fractures. Orthop Trans 1991;15:747-748. Boileau P, Krishnan SG, Tinsi L, et al: Tuberosity malposition and migration: Reasons for poor outcomes after hemiarthroplasty for displaced fractures of the proximal humerus. J Shoulder Elbow Surg 2002;11:401-412.
Question 98High Yield
Figure 19 shows the radiograph of a 6-month-old infant who has limited hip motion. History reveals no complications during pregnancy or delivery. Examination reveals that hip abduction is 45 degrees in flexion bilaterally. The neurologic examination is normal. What is the best course of action?
Explanation
Explanation
Diminished hip abduction can occur in normal children and is not always associated with hip pathology; therefore, initial management should consist of observation.
References:
- Castelein RM, Korte J: Limited hip abduction in the infant. J Pediatr Orthop 2001;21:668-670.
Question 99High Yield
When the great toe deviates into a valgus position, the action of the abductor hallucis muscle becomes one of
Explanation
Explanation
The abductor hallucis muscle inserts together with the medial tendon of the flexor hallucis brevis into the medial base of the proximal phalanx of the great toe. When the hallux assumes a valgus position, the action of the abductor becomes one of flexion and pronation of the first metatarsal. Resch S: Functional anatomy and topography of the foot and ankle, in Myerson M (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 1, pp 25-49.
Question 100High Yield
A 4-year-old boy sustained a nondisplaced, but complete, fracture of the left proximal tibial metaphysis 1 year ago. The fracture healed uneventfully in an anatomic position. Examination of the injured extremity now reveals 18 degrees of valgus compared with 3 degrees of valgus on the opposite side. Management should now include
Explanation
The development of a valgus deformity after this type of fracture is a well-known occurrence, and the patient's parents should be informed about this risk. In a patient who is age 4 years, the natural history is one of gradual correction by the development of a physiologic varus deformity at the distal tibial physis; therefore, no active intervention is needed at this time. Bracing has no effect on the deformity, and the child is too young for any procedure on the growth plate. Proximal tibial osteotomy is reserved until the patient nears skeletal maturity because of the risk of recurrence of the deformity. Lateral stapling can be done near skeletal maturity if the deformity persists, but this is unlikely to be necessary. Zionts LE, MacEwen GD: Spontaneous improvement of posttraumatic tibia valga. J Bone Joint Surg Am 1986;68:680-687.
You Might Also Like

Previous ChapterOrthopedic Board Review Set 809: 100 High-Yield MCQs
Next Chapter Orthopedic Board Review MCQs: ABOS, OITE, FRCS Mock Exam Se…

Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon