Orthopedic Board Review: 100 High-Yield MCQs (Mock Exam Set 890)
14 Apr 2026
104 min read
94 Views
Key Takeaway
This page offers 100 high-yield orthopedic surgery multiple-choice questions (MCQs) for ABOS, OITE, and FRCS board exam preparation. As Mock Exam Set 890, it helps surgeons assess their knowledge, reinforce critical concepts, and confidently prepare for their certifying examinations. Master challenging topics.
Antiprotrusio Cage Revision: Solving Acetabul...
00:00
Start Quiz
Question 1High Yield
In an acute closed boutonniere injury, what is the most appropriate splinting technique for the proximal interphalangeal joint?
Explanation
Rupture of the central slip of the extensor mechanism and a varying degree of lateral band volar migration are the pathologic entities in an acute boutonniere injury. Splinting the proximal interphalangeal joint in full extension allows reapproximation of the central slip to the base of the middle phalanx. Distal interphalangeal joint flexion is permitted to allow movement of the lateral bands distally and dorsally, preventing contracture. Newport ML: Extensor tendon injuries in the hand. J Am Acad Orthop Surg 1997;5:59-66.
Question 2High Yield
An 83-year-old man has a painful mass of the great toe. Radiographs and a biopsy specimen are seen in Figures 22a and 22b. What is the most likely diagnosis?
Explanation
Explanation
22b Gouty arthritis, pseudogout, and infection can all present with inflammatory arthritis and periarticular erosions. Strongly negative birefringent crystals are seen in gout. The histologic image shows elongated "needle-like" crystals of gout. Epidermal inclusion cysts are rarely painful and usually have a history of localized penetrating trauma. Hamilton W, Breedman KB, Haupt HM, Lackman R: Knee pain in a 40-year-old man. Clin Orthop 2001;383:282-285,290-292.
References:
- Mizel M, Miller R, Scioli M (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 301-302.
Question 3High Yield
A 35-year-old woman who is training for a triathlon has had a 2-month history of heel pain with weight bearing and is unable to run. History reveals that she is amenorrheic. Examination reveals that she is thin and has pain over the heel that is exacerbated with medial and lateral compression. Range of motion and motor and sensory function are normal. Radiographs are normal. What is the most likely diagnosis?
Explanation
Explanation
The most likely diagnosis is a stress fracture of the calcaneus and is supported by the history of running, female gender, and amenorrhea. Reproducing pain with medial and lateral compression of the heel also supports the diagnosis. A bone scan or MRI would most likely confirm the diagnosis. Plantar fasciitis would result in pain on the bottom of the heel with point tenderness. The lack of other areas of involvement or other symptoms does not support a seronegative inflammatory arthritis. Tarsal tunnel syndrome and peripheral neuropathy are unlikely because of the normal neurologic examination. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
References:
- Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 179-191.
Question 4High Yield
A 16-year-old cheerleader reports an ache in the right shoulder and arm that is worse after activity. She denies any history of acute trauma. Examination reveals a positive sulcus sign and an AP glide test with a posterior and anterior apprehension sign. To confirm a diagnosis of multidirectional instability, which of the following imaging studies is most appropriate?
Explanation
Multidirectional instability is a common finding in young female athletes. The anatomic structures are all intact but are hypermobile; therefore, CT and bone scans and scapular Y-views are often normal. Obtaining a weighted or AP stress view while applying downward traction on the arm will document instability and hypermobility of the joint. MRI generally is not indicated in this condition. Ultrasound is used primarily for rotator cuff pathology. Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Question 5High Yield
Second impact syndrome (SIS) after head injury is characterized by which of the following?
Explanation
SIS is a devastating but preventable complication of head injury. It occurs when return to activities is allowed prior to complete resolution of the symptoms of the first head injury. A second, sometimes trivial, head injury can lead to a devastating series of events that can result in sudden death. The symptoms tend to progress rapidly and often involve the brain stem. The prognosis is poor. Cantu RC: Second-impact syndrome. Clin Sports Med 1998;17:37-44. Saunders RL, Harbaugh RE: Second impact in catastrophic contact-sports head trauma. JAMA 1984;252:538-539.
Question 6High Yield
A patient has a displaced midshaft transverse fracture of the humerus and is neurologically intact. Following closed reduction and application of a coaptation splint, the patient cannot dorsiflex the wrist or the fingers at the metacarpophalangeal joints of the hand. What is the next most appropriate step in management?
Explanation
Explanation
The answer to this question is controversial. All of the standard textbooks state that development of a radial nerve palsy during initial fracture management may represent a laceration or injury of the nerve by bone fragments at the time of manipulation; therefore, surgery should be considered. However, it appears that there is no scientific basis for this decision. A review of the available literature shows that the results were the same for patients who were observed as for those who underwent radial nerve exploration. The indications for surgical exploration include palsies associated with open fractures, irreducible closed fractures, and vascular injuries. The only other relative indication for surgical exploration is following manipulation of a Holstein-Lewis fracture (a distal third fracture of the humerus with a lateral spike). In this type of fracture, exploration may be necessary if a closed reduction leads to radial nerve palsy because the spike may lacerate or compress the nerve. Observation for return of nerve function may be appropriate for 3 months or longer prior to considering late exploration. Bostman O, Bakalim G, Vainionpaa S, Wilppula E, Patiala H, Rokkanen P: Radial palsy in shaft fracture of the humerus. Acta Orthop Scand 1986;57:316-319. Shaz JJ, Bhatti NA: Radial nerve paralysis associated with the fractures of the humerus: A review of 62 cases. Clin Orthop 1983;172:171-176.
References:
- Holstein A, Lewis GB: Fractures of the humerus with radial nerve paralysis. J Bone Joint Surg Am 1963;458:1382-1388.
Question 7High Yield
A 68-year-old woman who sustained a closed distal tibia fracture 2 years ago was initially treated with an external fixator across the ankle for 12 weeks, followed by intramedullary nailing of the fibula and lag screw fixation of the tibia. She continued to report persistent pain so she was treated with a brace and a bone stimulator. She now reports pain in her ankle. Examination reveals ankle range of motion of 8 degrees of dorsiflexion to 25 degrees of plantar flexion. She is neurovascularly intact. Current radiographs are shown in Figures 9a through 9c. What is the next most appropriate step in management?


Explanation
The patient has a nonunion of the distal fifth of the tibia. The nonunion appears to be oligotrophic, somewhere between atrophic and hypertrophic. Management requires stabilization and stimulation of the local biology, which can be accomplished with open reduction and internal fixation with bone grafting. Bracing or casting does not provide enough stability. Ultrasound bone stimulation has been shown to speed fresh fracture repair but is not indicated in nonunions. The distal segment is too short for intramedullary nailing. A fibular osteotomy alone would increase instability and, even with prolonged casting, would be unlikely to lead to successful repair. Carpenter CA, Jupiter JB: Blade plate reconstruction of metaphyseal nonunion of the tibia. Clin Orthop 1996;332:23-28. Lonner JH, Siliski JM, Jupiter JB, Lhowe DW: Posttraumatic nonunion of the proximal tibial metaphysis. Am J Orthop 1999;28:523-528. Stevenson S: Enhancement of fracture healing with autogenous and allogeneic bone grafts. Clin Orthop 1998;355:S239-S246.
Question 8High Yield
Figure 25 shows an arthroscopic thermal capsular shrinkage device being used in the anterior inferior quadrant of a patient with a subluxating shoulder. Which of the following neurologic complications is most frequently reported with this technique?
Explanation
The axillary nerve lies within millimeters of the anterior inferior capsule. The inferior capsule is of varying thickness, and thermal energy used in shortening the ligament can cause damage to the sensory fibers of the axillary nerve. Clinically, this is manifested as a burnt skin sensation in the axillary nerve distribution area. The motor branch of the axillary nerve is usually spared. The suprascapular nerve and the radial nerve are far from the shrinkage zone. The musculocutaneous nerve, frequently at risk with open procedures, lies well anterior. Fanton GS: Arthroscopic electrothermal surgery of the shoulder. Op Tech Sports Med 1998;6:157-160.
Question 9High Yield
What structure provides the major blood supply to the humeral head?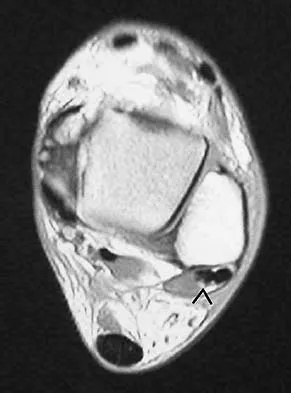
Explanation
The ascending branch of the anterior circumflex humeral artery provides the major blood supply to the humeral head. The posterior circumflex humeral artery supplies a much smaller portion of the proximal humerus. The nutrient humeral artery is the main blood supply for the humeral shaft. The thoracoacromial artery is primarily a muscular branch. The rotator cuff insertions contribute some blood supply to the tuberosities but not a major contribution. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Question 10High Yield
What mechanism is associated with the spontaneous resorption of herniated nucleus pulposus?
Explanation
Explanation
Nonsurgical modalities remain the mainstay for treatment of herniated disks. Spontaneous resorption of herniated disks frequently is detected by MRI. Marked infiltration by macrophages and neovascularization are observed on histologic examination of herniated disks, and the resorption is believed to be related to this process. Many cytokines such as vascular endothelial growth factor, tumor necrosis factor-alpha, and metalloproteinases have been implicated in this process, but none has been found to be singularly responsible. Haro H, Kato T, Kamori H, et al: Vascular endothelial growth factor (VEGF)-induced angiogenesis in herniated disc resorption. J Orthop Res 2002;20:409-415.
References:
- Doita M, Kanatani T, Ozaki T, et al: Influence of macrophage infiltration of herniated disc tissue on the production of matrix metalloproteinases leading to disc resorption. Spine 2001;26:1522-1527.
Question 11High Yield
Figure 14 shows the AP radiograph of a patient who underwent prosthetic arthroplasty 8 years ago and has now become symptomatic again over the past 18 months. A WBC count and erythrocyte sedimentation rate are within normal limits, and aspiration of the glenohumeral joint yields a negative Gram stain and cultures. Which of the following procedures will most likely provide the best pain relief and function?
Explanation
Explanation
Simple removal of the loose glenoid component or removal of the loose component followed by implantation of a new glenoid component are both appropriate treatment choices, depending on the remaining glenoid bone stock. However, removal and reimplantation appears to provide the most predictable pain relief and better function than removal alone. Antuna SA, Sperling JW, Cofield RH, et al: Glenoid revision surgery after total shoulder arthroplasty. J Shoulder Elbow Surg 2001;10:217-224.
References:
- Rodosky MW, Bigliani LU: Surgical treatment of non-constrained glenoid component failure. Oper Tech Orth 1994;4:226-236.
Question 12High Yield
Which of the following statements best describes synovial fluid?
Explanation
Synovial tissue is composed of vascularized connective tissue that lacks a basement membrane. Two cell types (type A and type B) are present: type B cells produce synovial fluid. Synovial fluid is made of hyaluronic acid and lubricin, proteinases,and collagenases. It is an ultrafiltrate of blood plasma added to fluid produced by the synovial membrane. It does not contain erythrocytes, clotting factors, or hemoglobin. It lubricates articular cartilage and provides nourishment via diffusion. Synovial fluid exhibits non-Newtonian flow characteristics. The viscosity coefficient is not a constant, the fluid is not linearly viscous, and its viscosity increases as the shear rate decreases.
Question 13High Yield
A 56-year-old woman sustained the fracture shown in Figures 30a and 30b in a motor vehicle accident. What mechanism is most likely responsible for the injury?

Explanation
The CT scans show a burst fracture that results from an axial load injury. The radiographic hallmark of a burst fracture is compression of the posterior cortex of the vertebral body with retropulsion of bone into the spinal canal. AP radiographs often show widening of the interpedicular distance with a fracture of the lamina. Theiss SM: Thoracolumbar and lumbar spine trauma, in Stannard JP, Schmidt AH, Kregor PJ (eds): Surgical Treatment of Orthopaedic Trauma. New York, NY, Thieme, 2007, pp 179-207.
Question 14High Yield
An 18-year-old football halfback reports that he had immediate right knee pain after being tackled 1 week ago. Examination now reveals moderate tenderness over the proximal medial tibia and lateral joint and normal cruciate stability. In evaluating the integrity of the posterolateral knee structures, what is the most reliable examination finding?
Explanation
Explanation
The most reliable test for a relatively isolated posterolateral complex (PLC) injury is the asymmetric tibial external rotation or "dial test." It can be performed with the patient prone or supine. When greater than 10 degrees of external rotation at 30 degrees of flexion is present when compared with the opposite knee, it indicates significant damage to the posterolateral structures. Asymmetric external rotation, which is also present at 90 degrees of flexion, indicates injury to the posterior cruciate ligament (PCL) as well. Varus laxity may indicate significant damage to both the PLC and PCL. Approximately 35% of the normal population may have a reverse pivot shift when examined under anesthesia; therefore, it is considered a less specific test. The external rotation/recurvatum and posterolateral drawer tests are adjunctive in assessing isolated posterolateral laxity but are not thought to be as reliable. Veltri DM, Warren RF: Isolated and combined posterior cruciate injuries. J Am Acad Orthop Surg 1993;1:67-75.
References:
- Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont IL, American Academy of Orthopaedic Surgeons, 2002, pp 489-511.
Question 15High Yield
Figure 18a shows the initial lateral radiograph of a 6-year-old girl who sustained a fracture in a motor vehicle accident and was treated in a cast 1 year ago. She now has the valgus deformity seen in Figure 18b. Treatment should consist of

Explanation
Proximal tibial metaphyseal fractures may result in late genu valgum as a result of asymmetric growth of the proximal tibia. These patients are best treated with observation because the deformity is likely to remodel. Osteotomy is not indicated and potentially will lead to recurrence. Stapling of the medial tibial physis is appropriate in patients who have a severe and progressive deformity. Cozen L: Knock-knee deformity in children: Congenital and acquired. Clin Orthop 1990;258:191-203. Jackson DW, Cozen L: Genu valgum as a complication of proximal tibial metaphyseal fractures in children. J Bone Joint Surg Am 1971;53:1571-1578. Brammar TJ, Rooker GD: Remodeling of valgus deformity secondary to proximal metaphyseal fracture of the tibia. Injury 1998;29:558-560. Ogden JA, Ogden DA, Pugh L, et al: Tibia valga after proximal metaphyseal fractures in childhood: A normal biologic response. J Pediatr Orthop 1995;15:489-494.
Question 16High Yield
Which of the following tendons is the primary antagonist of the posterior tibialis tendon?
Explanation
The primary action of the posterior tibialis tendon is inversion of the foot; secondarily, it plantar flexes the ankle. The anterior tibialis tendon also inverts the foot and only partially antagonizes the posterior tibialis tendon. The primary action of the peroneus longus is plantar flexion of the first ray. It secondarily everts the posterior tibialis tendon. The action of the flexor digitorum longus tendon is synergistic with the posterior tibialis tendon. The primary action of the peroneus brevis tendon is eversion; therefore, it is the primary antagonist of the posterior tibialis tendon. Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 550-551.
Question 17High Yield
Osteophyte formation at the posteromedial olecranon and olecranon articulation in high-caliber throwing athletes is most often the result of underlying
Explanation
Explanation
During the late acceleration phase of throwing, the triceps forcibly contracts, extending the elbow as the ball is released. Normally, this force is absorbed by the anterior capsule and the brachialis and biceps muscles. However, if the ulnar collateral ligament is insufficient, the elbow will be in a subluxated position during extension and cause impaction of the olecranon and the olecranon fossa posteromedially. Over time, osteophyte formation is likely to occur. Conway JE, Jobe FW, Glousman RE, Pink M: Medial instability of the elbow in throwing athletes: Treatment by repair or reconstruction of the ulnar collateral ligament. J Bone Joint Surg Am 1992;74:67-83.
References:
- Wilson FD, Andrews, JR, Blackburn TA, McCluskey G: Valgus extension overload in the pitching elbow. Am J Sports Med 1983;11:83-88.
Question 18High Yield
A 10-year-old boy with spastic diplegic cerebral palsy walks in a crouched position with the hips and knees flexed. Maximum knee flexion is 15 degrees during early swing phase. Instrumented gait analysis shows quadriceps activity from terminal stance throughout swing phase. Treatment should consist of
Explanation
Explanation
The rectus femoris muscle spans two joints and is active during running, sprinting, and walking at a fast pace during the preswing and early swing phase of gait. In these situations, the muscle helps to generate power to initiate hip flexion while absorbing or controlling the rate of knee flexion during early swing phase. Quadriceps activity, including the rectus femoris, is not normally needed when walking at a routine cadence. However, rectus femoris activity is commonly noted during preswing and the swing phase in patients with cerebral palsy, particularly those with diplegia. In an effort to initiate swing phase, the rectus femoris is "overactive." As a result, the knee flexion that commonly occurs at terminal stance and initial swing is restricted. Instead of achieving the normal 50 to 60 degrees of flexion during early swing, this patient's knee flexion is limited to 15 degrees. The goal of treatment is to retain rectus femoris activity for initiation of hip flexion but to diminish its restraint on knee flexion. Studies have shown that transfer of the distal rectus femoris tendon provides more flexion of the knee during the swing phase of gait than simply releasing the tendon. V-Y lengthening of the quadriceps tendon or a Z lengthening of the patellar tendon causes too much weakening of the quadriceps muscle and worsens the crouch deformity. In addition to transfer of the rectus femoris tendon, other procedures are often done concomitantly to obtain the best balance and realignment of hip-knee-ankle activity. Aiona MD: Guidelines for managing lower extremity problems in cerebral palsy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1534-1541. Chambers H, Laure A, Kaufman K, Cardelia M, Sutherland D: Prediction of outcome after rectus femoris surgery in cerebral palsy: The role of cocontraction of the rectus femoris and vastus lateralis. J Pediatr Orthop 1998;18:703-711.
References:
- Ounpuu S, Muik E, Davis RB, Gage JR, Deluca PA: Rectus femoris surgery in children with cerebral palsy. J Pediatr Orthop 1993;13:331-335.
Question 19High Yield
A 52-year-old man has shoulder pain and stiffness after undergoing a "mini-lateral" rotator cuff repair 6 months ago. Examination reveals that he is afebrile with normal vital signs. There is slight erythema but no drainage from the incision. Range of motion is limited in all planes, and there is weakness with resisted external rotation and abduction. Radiographs show a well-positioned metal implant within the greater tuberosity. Laboratory studies reveal a WBC count of 8,400/mm3 (normal 3,500 to 10,500/mm3) and an erythrocyte sedimentation rate of 63 mm/h (normal up to 20 mm/h). What is the next most appropriate step in management?
Explanation
Explanation
Deep sepsis of the shoulder following rotator cuff repair is an uncommon problem. Patients with infections of this type typically report persistent pain and are not systemically ill. They may have signs of local wound problems such as erythema, drainage, and dehiscence. Laboratory studies can be helpful in making an accurate diagnosis. Most patients will not show a significant elevation of the WBC count; however, an elevated erythrocyte sedimentation rate is nearly always present and should alert the clinician to the presence of infection. Aspiration of both subacromial and glenohumeral joint spaces is necessary to confirm the diagnosis. The most effective treatment for deep shoulder sepsis following rotator cuff repair involves extensive surgical debridement, removing all suspicious soft tissue as well as implants. Administration of appropriate antibiotic therapy is needed for complete control of the infection. Mirzayan R, Itamura JM, Vangsness CT, et al: Management of chronic deep infection following rotator cuff repair. J Bone Joint Surg Am 2000;82:1115-1121. Settecerri JJ, Pitnu MA, Rock MG, et al: Infection after rotator cuff repair. J Shoulder Elbow Surg 1994;8:105.
References:
- Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Question 20High Yield
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by
Explanation
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by the use of a direct lateral approach to the ankle. The superficial peroneal nerve and its branches exit the fascial hiatus approximately 9 cm to 10 cm proximal to the tip of the distal fibula with a range of 4 cm to 13 cm, and their course is typically anterior to the midlateral plane of the fibula. However, small branches may course across the surgical plane directly laterally. A posterior-lateral approach diminishes the risk of injury to the superficial peroneal nerve and its branches; however, by moving farther posterior, the sural nerve and its branches may be at increased risk. Cast immobilization may injure the cutaneous nerves about the ankle; however, the risks are greater with surgical intervention. A medial or anterior-medial approach to the ankle will not injure the superficial peroneal nerve at the ankle level. Redfern DJ, Sauve PS, Sakellariou A: Investigation of incidence of superficial peroneal nerve injury following ankle fracture. Foot Ankle Int 2003;24:771-774.
Question 21High Yield
When comparing surgical and nonsurgical extremities in patients who underwent anterior cruciate ligament (ACL) reconstruction using patellar tendon or hamstrings autografts, isokinetic strength measurements obtained 6 months after the surgery would most likely reveal
Explanation
Follow-up examination at 6 months revealed no statistically significant differences in quadricep or hamstring strength when comparing surgical versus nonsurgical extremities isokinetically. Therefore, the selection of autogenous hamstring or patellar tendon for ACL reconstruction should not be based solely on the assumption of the graft tissue source altering the recovery of quadricep and/or hamstring strength. Carter TR, Edinger S: Isokinetic evaluation of anterior cruciate ligament reconstruction: Hamstring versus patellar tendon. Arthroscopy 1999;15:169-172 Howell SM, Taylor MA: Brace-free rehabilitation, with early return to activity, for knees reconstructed with a double-looped semitendinosus and gracilis graft. J Bone Joint Surg Am 1996;78:814-825.
Question 22High Yield
Which of the following structures are found in the anterior tarsal tunnel?
Explanation
The contents of the anterior tarsal tunnel are the extensor hallucis longus, tibialis anterior, extensor digitorum longus, dorsalis pedis artery, and the deep peroneal nerve. The term "anterior tarsal tunnel syndrome" is used to specifically describe the compression of the deep peroneal nerve under the inferior extensor retinaculum. With nerve compression, patients report a burning sensation across the dorsum of the foot with paresthesias in the first web space. There also may be wasting and weakness of the extensor digitorum brevis. Kuritz HM: Anterior entrapment syndromes. J Foot Surg 1976;15:143-148.
Question 23High Yield
What type of exercise is used early in the rehabilitation process to safely stimulate co-contraction of the scapular and rotator cuff muscles?
Explanation
Explanation
Closed kinetic chain exercises are used early in the rehabilitation process. The distal segment is fixed, and an axial load is applied which provides glenohumeral compression and reduces the demand on the rotator cuff. These exercises stimulate co-contractions of the scapular and rotator cuff muscles, load scapular stabilizers, and facilitate active motion. Facilitated active motion exercises use proximal segment motion to stimulate and facilitate motion in the target tissue. These exercises are often performed in diagonal movements. Resistive active motion exercises are used later in the rehabilitation process. These are typically open kinetic chain exercises that involve active glenohumeral motion with extrinsic loads such as weights or exercise tubing. During the later stages of upper extremity rehabilitation, plyometrics are added. These exercises help to prepare the athlete for return to sport. When performed at slower speeds, these exercises emphasize stabilization and control. As the speeds increase, muscles begin to work in the stretch-shortening sequence associated with sports participation. Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 129-136.
References:
- Kibler WB: Shoulder rehabilitation: Principles and practice. Med Sci Sports Exerc 1998;30:S40-50.
Question 24High Yield
A 10-year-old boy has activity-related knee pain that is poorly localized. He denies locking, swelling, or giving way. Examination shows mild tenderness at the medial femoral condyle and painless full range of motion without ligamentous instability. Radiographs are shown in Figures 2a through 2c. What is the best course of action?


Explanation
The radiographs show an osteochondritis dissecans (OCD) lesion in the medial femoral condyle of a skeletally immature patient. The lesion is not displaced from its bed. Nonsurgical management of a stable OCD lesion in a patient with open physes consists of a period of activity limitation and occasional immobilization. Unstable lesions, loose bodies, and patients with closed physes require more aggressive treatment. Most of the surgical procedures can be done arthroscopically. Because the radiographic appearance is typical, biopsy is unnecessary. The radiographs do not show an osteocartilaginous loose body, and the patient reports no catching or locking; therefore, removal of the loose body is not indicated. Linden B: Osteochondritis dissecans of the femoral condyles: A long term follow-up study. J Bone Joint Surg Am 1977;59:769-776. Cahill BR: Osteochondritis dissecans of the knee: Treatment of juvenile and adult forms. J Am Acad Orthop Surg 1995;3:237-247.
Question 25High Yield
In patients without spondylolisthesis or scoliosis undergoing laminectomy for lumbar spinal stenosis, spinal fusion is generally recommended if
Explanation
Explanation
With the notable exception of fusion for degenerative spondylolisthesis and scoliosis, there is a paucity of evidence on the indications for spinal fusion in patients undergoing laminectomy for spinal stenosis. However, it is generally recommended that if the spine is destabilized (for example by removal of one complete facet joint or by an iatrogenic pars fracture), spinal fusion should be considered. Although fusion can be considered for a very long laminectomy, a two-level laminectomy does not represent, by itself, a clear indication for the addition of a spinal fusion. The repair of a dural tear and the use of nicotine by the patient play no role in the determination of whether or not to add fusion to a laminectomy procedure. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 299-409.
Question 26High Yield
Figure 23 shows the postoperative radiograph of a patient who underwent an anterior cruciate ligament (ACL) reconstruction (with bone-patella tendon-bone autograft) that failed. He initially had loss of flexion postoperatively. What is the most likely cause of this failure?
Explanation
Explanation
The key to this question is the fact that the patient initially lost flexion postoperatively and this relates to anterior placement of the femoral tunnel, thus capturing the knee. The bone plug seen on the radiograph is actually from the tibial tunnel, but this occurred as the patient forced flexion until failure of the ACL graft and pullout of the plug from the tunnel. Although it could be argued that better tibial fixation would have prevented this failure, poor placement of the femoral tunnel led to the failure of this ACL reconstruction. Fu FH, Bennett CH, Latterman C, et al: Current trends in anterior cruciate ligament reconstruction: Part 1. Biology and biomechanics of reconstruction. Am J Sports Med 1999;27:821-830.
References:
- Fu FH, Bennett CH, Ma CB, et al: Current trends in anterior cruciate ligament reconstruction: Part II. Operative procedures and clinical correlations. Am J Sports Med 2000;28:124-130.
Question 27High Yield
A 68-year-old woman undergoes a complicated four-level anterior cervical diskectomy and fusion at C3-7 with iliac crest bone graft and instrumentation for multilevel cervical stenosis. Surgical time was approximately 6 hours and estimated blood loss was 800 mL. Neuromonitoring was stable throughout the procedure. The patient's history is significant for smoking. The most immediate appropriate postoperative management for this patient should include
Explanation
Explanation
Airway complications after anterior cervical surgery can be a catastrophic event necessitating emergent intubation for airway protection. Multilevel surgeries requiring long intubation and prolonged soft-tissue retraction as well as preexisting comorbidities may predispose a patient to postoperative airway complications. Sagi and associates reported that surgical times greater than 5 hours, blood loss greater than 300 mL, and multilevel surgery at or above C3-4 are risk factors for airway complications. In surgical procedures with the aforementioned factors, serious consideration should be given to elective intubation for 1 to 3 days to avoid urgent reintubation. Sagi HC, Beutler W, Carroll E, et al: Airway complications associated with surgery on the anterior cervical spine. Spine 2002;27:949-953. Epstein NE, Hollingsworth R, Nardi D, et al: Can airway complications following multilevel anterior cervical surgery be avoided? J Neurosurg 2001;94:185-188.
Question 28High Yield
Based on the findings seen in the radiograph in Figure 26, emergent management should consist of
Explanation
Explanation
The radiograph shows a volarly dislocated lunate. Initial emergent treatment of perilunate dislocations should consist of closed reduction and splinting, especially if the patient exhibits median nerve compression. Open reduction and pinning or ligament repair are necessary but are not emergent. A dorsal approach is sometimes required for ligament repair or bony visualization; however, this can be done in a more semi-elective manner. Isenberg J, Prokop A, Schellhammer F, et al: Palmar lunate dislocation. Unfallchirurg 2002;105:1133-1138.
References:
- Ruby LK: Fractures and dislocations of the carpus, in Browner BD, Jupiter JB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1367-1372.
Question 29High Yield
A 29-year-old woman was injured in a high-speed motor vehicle accident 3 hours ago. Radiographs are shown in Figures 7a through 7e. Her right foot injury is open and contaminated. Her associated injuries include a closed head injury and a ruptured spleen requiring resection. She has had 6 units of packed red blood cells and the trauma surgeon has turned her care over to you. Her current base deficit is 10 and her urinary output has averaged 0.4 mL/kg for the last 2 hours. What is the best treatment at this time?
Explanation
Explanation
7b 7c 7d 7e The patient appears to be a borderline or unstable surgical patient following her initial trauma and spleenectomy (high base excess and low urine output). She needs continued resuscitation and minimal additional blood loss. This is best accomplished with irrigation and debridement of the ankle, external fixation of the ankle, foot, and femur, and splinting of the forearm. A traction pin for the femoral fracture will not control bleeding as well as an external fixator. Intramedullary nailing of the femur and open reduction and internal fixation of the forearm would be appropriate in patients that are euvolemic and stable. Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461. Taeger G, Ruchholtz S, Waydhas C, et al: Damage control orthopedics in patients with multiple injuries is effective, time saving, and safe. J Trauma 2005;59:409-416. Harwood PJ, Giannoudis PV, van Griensven M, et al: Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J Trauma 2005;58:446-452.
Question 30High Yield
What process is often found associated with other neoplasms?
Explanation
Aneurysmal bone cyst may be either a "pattern" or a "diagnosis." Therefore, aneurysmal bone cyst should be viewed as a diagnosis of exclusion. Hemorrhage into a variety of primary bone lesions (eg, giant cell tumor of bone, chondroblastoma, osteoblastoma, fibrous dysplasia, osteosarcoma, or vascular neoplasms) may result in intralesional, membrane-bone blood-filled cysts. Such secondary changes may be confused with aneurysmal bone cyst, resulting in inappropriate therapy because assessment should be focused on identifying the underlying primary process. The entire specimen should be examined histologically in an effort to locate an underlying primary bone tumor. Bonakdarpour A, Levy WM, Aegerter E: Primary and secondary aneurysmal bone cyst: A radiological study of 75 cases. Radiology 1978;126:75-83. Levy WM, Miller AS, Bonakdarpour A, Aegerter E: Aneurysmal bone cyst secondary to other osseous lesions: Report of 57 cases. Am J Clin Pathol 1975;63:1-8.
Question 31High Yield
A 42-year-old woman underwent an instrumented posterior spinal fusion at L3-S1 with transforaminal lumbar interbody fusion. She had an excellent clinical result with complete resolution of leg pain. Three months later she now reports increasing back pain and weakness in her legs. Examination reveals weakness in the quadriceps and tibialis anterior. Radiographs show no interval changes in the position of the hardware. MRI scans are shown in Figures 2a through 2c. What is the next most appropriate step in management?


Explanation
The MRI scans reveal a postoperative infection. Observation and antibiotics are not appropriate choices. There is a large fluid collection and this requires decompression because the patient has neurologic changes. There is considerable debate regarding the removal of hardware. Many contend that biofilm on the implants can harbor the infection. However, these complications usually can be treated with serial irrigations, debridements, and IV antibiotics. The incidence of infection has been widely studied with varying rates in fusions with instrumentation. Rates appear to be increased with instrumentation, yet these infections usually can be managed without hardware removal. Glassman SD, Dimar JR, Puno RM, et al: Salvage of instrumental lumbar fusions complicated by surgical wound infection. Spine 1996;21:2163-2169.
Question 32High Yield
What is the most reproducible landmark for the accurate anatomic placement of the tibial tunnel for an anterior cruciate ligament (ACL) reconstruction?
Explanation
Explanation
The anterior border of the PCL is the most accurate and reproducible landmark for appropriate placement of the tibial tunnel for an ACL reconstruction. The central sagittal insertion point of the ACL is consistently 10 to 11 mm anterior to the anterior border of the PCL ligament. The anterior border of the tibia is not well visualized and does not serve as a reference point. While the posterior border of the anterior horn of the lateral meniscus could be used as a reference point, it has twice the variability of the PCL reference point. The posterior border of the tibia is difficult to identify and has greater variability than the PCL relative to the AP dimension of the proximal tibial surface. The anterior horn of the medial meniscus is also more variable than the PCL. Hutchinson MR, Bae TS: Reproducibility of anatomic tibial landmarks for anterior cruciate ligament reconstructions. Am J Sports Med 2001;29:777-780.
References:
- McGuire DA, Hendricks SD, Sanders HM: The relationship between anterior cruciate ligament reconstruction tibial tunnel location and the anterior aspect of the posterior cruciate ligament insertion. Arthroscopy 1997;13:465-473.
Question 33High Yield
A collegiate rower reports the sudden onset of right chest pain while rowing. The athlete states that the pain is worse with deep inspiration and coughing. Examination reveals localized tenderness over the posterolateral corner of the eighth rib. What is the most likely diagnosis?
Explanation
Explanation
A rib stress fracture, the most common injury to the thorax in rowing athletes, generally occurs during periods of intense training with a low stroke rate and heavy loads. It is characterized by the sudden onset of sharp, localized chest pain while rowing. The fifth through the ninth rib is generally affected, and the diagnosis is best established with a bone scan. An intercostal muscle strain generally has an insidious onset and may be poorly localized. Costochondritis affects the anterior costochondral junction. A pneumothorax and an empyema can cause nonlocalized chest pain but are associated with respiratory distress and systemic physical findings. Karlson KA: Rib stress fractures in elite rowers. Am J Sports Med 1998;26:516-520.
References:
- Holden DL, Jackson DW: Stress fractures of the ribs in female rowers. Am J Sports Med 1985;13:342-348.
Question 34High Yield
A 32-year-old woman sustained an injury to her left upper extremity in a motor vehicle accident. Examination reveals a 2-cm wound in the mid portion of the dorsal surface of the upper arm and deformities at the elbow and forearm; there are no other injuries. Her vital signs are stable, and she has a base deficit of minus 1 and a lactate level of less than 2. Radiographs are shown in Figures 9a and 9b. In addition to urgent debridement of the humeral shaft fracture, management should include

Explanation
With a severe injury to the upper extremity, the best opportunity for achieving a good functional result for a floating elbow is immediate debridement of the open fracture, followed by internal fixation of the fractures. The ability to do this depends on the patient's physiologic status. In this patient, the procedure is acceptable because she has normal vital signs and no chest or abdominal injuries, and normal physiologic parameters (base excess and lactate) show adequate peripheral perfusion. The surgical approaches will be determined by the associated injury patterns and open wounds. In this patient, the humerus was debrided and stabilized through a posterior approach as was the medial condyle fracture. The ulna was fixed through an extension of the posterior incision and the radius through a separate dorsal approach. Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Question 35High Yield
Figure 54 shows the preoperative radiograph of a 45-year-old woman who is considering total hip arthroplasty with her orthopaedic surgeon. What femoral characteristic is a typical concern in this patient?
Explanation
Explanation
Developmental dysplasia of the hip (DDH) leads to early arthritis of the hip as seen in this patient. Although DDH is believed to mostly affect the acetabulum, most patients with DDH also have anatomic aberrations of the femur. Using three-dimensional computer models generated by reconstruction of CT scans, dysplastic femurs were shown to have shorter necks and smaller, straighter canals than the controls. The shape of the canal became more abnormal with increasing subluxation. The studies also have shown that the primary deformity of the dysplastic femur is rotational, with an increase in anteversion of 5 degrees to 16 degrees, depending on the degree of subluxation of the hip. The rotational deformity of the dysplastic femur arises within the diaphysis between the lesser trochanter and the isthmus and is not attributable to a torsional deformity of the metaphysis. Osteopenia is not a concern in a patient with an excellent cortical index (thick cortices and narrow canal). Femoral varus or bowing of the femur is not a typical finding in patients with DDH. Noble PC, Kamaric E, Sugano N, et al: Three-dimensional shape of the dysplastic femur: Implications for THR. Clin Orthop 2003;417:27-40.
References:
- Sugano N, Noble PC, Kamaric E, et al: The morphology of the femur in developmental dysplasia of the hip. J Bone Joint Surg Br 1998;80:711-719.
Question 36High Yield
Figures 20a and 20b show lateral and AP radiographs of a 49-year-old man who sustained a gunshot wound through the left shoulder. He reports neck pain and examination reveals weakness in all four extremities. What is the priority of evaluation?
Explanation
Explanation
20b The projectile entered the left shoulder and traveled to the right neck; therefore, a high incidence of suspicion must be directed to the airway, great vessels of the neck, and contents of the mediastinum. Immediate assessment of airway, breathing, and circulation takes priority, followed by examination of the neurologic status and other systems, as determined by the examination findings. Subcommittee on ATLS of the American College of Surgeons Committee on Trauma 1993-1997, Spine and Spinal Cord Trauma; Advanced Trauma Life Support Student Manual, ed 6, 1997. International Standards for Neurological and Functional Classification of Spinal Cord Injury. American Spinal Injury Association and International Medical Society of Paraplegia (ASIA/IMSOP).
Question 37High Yield
The anterolateral (Watson-Jones) approach to the hip exploits the intermuscular interval between the
Explanation
The Watson-Jones approach to the hip uses the intermuscular interval between the gluteus medius and the tensor fascia lata. This is not a true internervous plane, as both muscles are supplied by the superior gluteal nerve. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 316-332.
Question 38High Yield
A 3-year-old girl has had wrist pain, a fever, and has refused to move her right wrist for the past 10 days. She has an oral temperature of 102 degrees F (38.7 degree C). Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h, a WBC count of 11,000/mm3, and a left shift. AP and lateral radiographs are shown in Figures 57a and 57b. What is the most likely diagnosis?
Explanation
Explanation
57b The most likely diagnosis is acute osteomyelitis. She may also have a septic wrist; however, the lytic lesion in the distal radius has the typical presentation and radiographic appearance of metaphyseal osteomyelitis. In this area of sluggish vascular flow, low oxygen tension, and low pH, bacterial seeding is common and is the usual origin of metaphyseal osteomyelitis. Leukemia and Ewing's sarcoma can present as a lytic lesion with an elevated erythrocyte sedimentation rate, but they are much less common than osteomyelitis and are less focal and more destructive in appearance. Nonossifying fibroma is typically metaphyseal and eccentric; however, it is well circumscribed and uncommon in the upper extremity. Eosinophilic granuloma does not typically present with inflammatory indicies. Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis and treatment. J Am Acad Orthop Surg 1994;2:333-341.
References:
- Song KM, Sloboda JF: Acute hematogenous osteomyelitis in children. J Am Acad Orthop Surg 2001;9:166-175.
Question 39High Yield
A 6-year-old boy with spastic diplegic cerebral palsy has a crouched gait. Examination reveals hip flexion contractures of 15 degrees and popliteal angles of 70 degrees. Equinus contractures measure 10 degrees with the knees extended. Which of the following surgical procedures, if performed alone, will worsen the crouching?
Explanation
Children with spastic diplegic cerebral palsy often have contractures of multiple joints. Because the gait abnormalities can be complex, isolated surgery is rarely indicated. To avoid compensatory deformities at other joints, it is preferable to correct all deformities in a single operation. Isolated heel cord lengthening in the presence of tight hamstrings and hip flexors will lead to progressive flexion at the hips and knees, thus worsening a crouched gait. Split posterior tibial tendon transfer is used for patients with hindfoot varus, which is not present in this patient. Gage JR: Distal hamstring lengthening/release and rectus femoris transfer, in Sussman MD (ed): The Diplegic Child. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1992, pp 324-326.
Question 40High Yield
A 48-year-old man has recurrent right knee pain. Figure 52a shows the sagittal proton density T2-weighted MRI scan, and Figure 52b shows the sagittal T2-weighted MRI scan at the same level. The arrow is pointing to a

Explanation
Meniscal tears have many configurations and locations. The normal medial meniscus has a bow-tie configuration on the two most medial consecutive sagittal views. Toward the center of the joint the anterior and posterior horns have a triangular shape. These images show an abnormal intra-articular low-signal structure located anterior to the intact posterior cruciate ligament. This most likely represents a torn and displaced posterior horn of the medial meniscus, sometimes called "double PCL sign". A popliteal cyst and ligaments of Wrisberg and Humphry are not visible on these figures. Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Question 41High Yield
Where is the watershed zone for tarsal navicular vascularity?
Explanation
Explanation
The central one third has been established as the watershed zone by angiographic studies, and has been borne out in clinical conditions involving the navicular, such as stress fractures and osteonecrosis. These findings account for the susceptibility to injury at this level. Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 239-242.
References:
- Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983, pp 299-302.
Question 42High Yield
A 35-year-old woman reports an 8-week history of neck pain radiating to her right upper extremity. She denies any history of trauma or provocative event. Examination reveals decreased pinprick sensation in her right middle finger, otherwise sensation is intact bilaterally. Finger flexors and interossei demonstrate 5/5 motor strength bilaterally. Finger extensors are 4/5 on the right and 5/5 on the left. The triceps reflex is 1+ on the right and 2+ on the left. The most likely diagnosis is a herniated nucleus pulposus at what level?
Explanation
The patient's neurologic examination is consistent with a C7 radiculopathy on the right side. In a patient with this symptom complex in the absence of trauma, a cervical disk herniation is the most common etiology for a C7 radiculopathy. There are eight cervical nerve roots and the C7 nerve exits at the C6-7 disk space and is most frequently impinged by a disk herniation at this level. Houten JK, Errico TJ: Cervical spondylotic myelopathy and radiculopathy: Natural history and clinical presentation, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 985-990.
Question 43High Yield
A 16-year-old high school pitcher notes acute pain on the medial side of his elbow during a pitch. Examination that day reveals medial elbow tenderness, pain with valgus stress, mild swelling, and loss of extension. Plain radiographs show closed physes and no fracture. Which of the following diagnostic studies will best reveal his injury?
Explanation
The history and findings are consistent with a diagnosis of a sprain of the medial collateral ligament (MCL) of the elbow; therefore, contrast-enhanced MRI is considered the most sensitive and specific study for accurately showing this injury. Arthroscopic visualization of the MCL is limited to the most anterior portion of the anterior bundle only; complete inspection of the MCL using the arthroscope is not possible. CT without the addition of contrast is of no value in this situation. Use of a technetium Tc 99m bone scan is limited to aiding in the diagnosis of occult fracture, a highly unlikely injury in this patient. There are no clinical indications for electromyography. Timmerman LA, Andrews JR: Undersurface tear of the ulnar collateral ligament in baseball players: A newly recognized lesion. Am J Sports Med 1994;22:33-36. Timmerman LA, Schwartz ML, Andrews JR: Preoperative evaluation of the ulnar collateral ligament by magnetic resonance imaging and computed tomography arthrography: Evaluation of 25 baseball players with surgical confirmation. Am J Sports Med 1994;22:26-32.
Question 44High Yield
A 23-year-old man has had right posterolateral knee pain and occasional lateral calf dysesthesias for the past 8 months. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 62a through 62e. What is the most likely diagnosis?
Explanation
Explanation
62b 62c 62d 62e The radiograph shows an eccentric, cortically based lytic lesion in the proximal fibula. The CT and MRI scans confirm that it is well circumscribed and cortically based with significant surrounding edema. The radiographic differential diagnosis would be a Brodie's abscess or osteoid osteoma. An osteoblastoma would have to be greater than 2 cm in size. A chondroblastoma may also have significant edema around it, but it is an epiphyseal-based lesion, not cortically based. The well-circumscribed nature of the lesion is not consistent with osteosarcoma. The pathology shows a very cellular and vascular stroma with plump, but not atypical osteoblast cells making a matrix of immature woven bone. There are no abundant inflammatory cells or dead bone suggestive of osteomyelitis or a Brodie's abscess. Therefore, the clinical and histologic picture is most consistent with an osteoid osteoma. Percutaneous radiofrequency ablation, usually with CT guidance, has become the preferred method for treating most cases of osteoid osteoma. Rosenthal DI: Radiofrequency treatment. Orthop Clin North Am 2006;37:475-484.
References:
- Ghanem I: The management of osteoid osteoma: Updates and controversies. Curr Opin Pediatr 2006;18:36-41.
Question 45High Yield
A 13-year-old boy has had a painless mass in the arm for the past 2 months. An MRI scan and biopsy specimens are shown in Figures 46a through 46c. What is the most likely diagnosis?
Explanation
Explanation
46b 46c Nodular fasciitis is a benign soft-tissue lesion that usually arises from the fascia and is often misdiagnosed as a sarcoma. Desmoid tumors (aggressive fibromatosis) are also benign tumors with a greater tendency for local recurrence. Desmoid tumors have more spindle-shaped fibroblasts in an abundant collagenous matrix. Malignant fibrous histiocytoma is a hypercellular pleomorphic sarcoma more commonly found in adults. The histology is not consistant with a fatty tumor.
References:
- Bernstein KE, Lattes R: Nodular (pseudosarcomatous) fasciitis, a nonrecurrent lesion: Clinicopathologic study of 134 cases. Cancer 1982;49:1668-1678.
Question 46High Yield
Figures 25a and 25b show the radiographs of a 66-year-old man who has had a long history of bilateral painful flatfoot deformities. Examination reveals that his foot is partially correctable passively, albeit with discomfort, and he has an Achilles tendon contracture. An ankle-foot orthosis has failed to provide relief. Treatment should now consist of

Explanation
The patient has a pronounced deformity with pain and degenerative arthritis; therefore, triple arthrodesis is the treatment of choice. Gastrocnemius or Achilles tendon lengthening may be a necessary adjunct to the triple arthrodesis, but alone is inadequate to allow for correction. Because the ankle-foot orthosis has failed to provide relief, a UCBL is not likely to help. Osteotomy procedures are designed for lesser deformities and well-preserved joints. Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 115-120.
Question 47High Yield
What is the most likely complication following treatment of the humeral shaft fracture shown in Figure 6?
Explanation
Explanation
The humerus was treated with an intramedullary nail. Findings from two prospective randomized studies of intramedullary nailing or compression plating of acute humeral fractures have shown approximately a 30% incidence of shoulder pain with antegrade humeral nailing. This is the most common complication in both of these series. Nonunions are present in approximately 5% to 10% of humeral fractures treated with an intramedullary nail. Infection has an incidence of approximately 1%. Elbow injury is unlikely unless the nail is excessively long. Rarely, injury to the radial nerve is possible if it is trapped in the intramedullary canal. Chapman JR, Henley MB, Agel J, et al: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
References:
- McCormack RG, Brien D, Buckley RE, et al: Fixation of fractures of the shaft of the humerus by dynamic compression plate or intramedullary nail: A prospective, randomised trial. J Bone Joint Surg Br 2000;82:336-339.
Question 48High Yield
A 27-year-old man was struck by a taxi cab and sustained comminuted right distal third tibia and fibula fractures; treatment consisted of placement of an intramedullary nail in the tibia the following morning. At his 6-month follow-up, he has clawing of all five toes. Examination reveals flexion deformities of the distal and proximal interphalangeal joints that are flexible with plantar flexion and rigid with dorsiflexion. Calluses are present on the dorsum and tip of the toes. Single heel rise is normal. He has a mild equinus contracture (relative to the left leg) that is not relieved with knee flexion. What is the most appropriate treatment option?
Explanation
Explanation
This is an example of tethering of the flexor hallucis longus/flexor digitorum longus (FHL/FDL) to the fracture site. Additional time and/or physical therapy and bracing would not be expected to be of benefit. Release of the FHL and FDL from the fracture site or retromalleolar lengthening will address the posttraumatic claw toe deformity and Achilles tendon lengthening will address the mild equinus. Posterior tibial tendon transfer is not appropriate as the patient demonstrates a normal heel rise. Midfoot releases and hallux fusion are also not indicated. Feeny MS, Williams RL, Stephens MM: Selective lengthening of the proximal flexor tendon in the management of acquired claw toes. J Bone Joint Surg Br 2001;83:335-338.
References:
- Clawson DK: Claw toes following tibial fracture. Clin Orthop Relat Res 1974;103:47-48.
Question 49High Yield
A 63-year-old woman who sustained a distal radial fracture 2 months ago now reports that she is unable to achieve active extension of the thumb at the interphalangeal joint. What type of trauma may lead to this clinical finding?
Explanation
Nondisplaced distal radial fractures have a higher rate of spontaneous rupture of the extensor pollicis longus tendon. The extensor mechanism is felt to impinge on the tendon following a nondisplaced fracture and causes either a mechanical attrition of the tendon or a local area of ischemia in the tendon. Helal B, Chen SC, Iwegbu G: Rupture of the extensor pollicis longus tendon in undisplaced Colles' type of fracture. Hand 1982;14:41-47.
Question 50High Yield
Figures 45a and 45b show the radiographs of a 40-year-old woman with rheumatoid arthritis who is unable to straighten her ring and little fingers. Examination reveals that the fingers can be passively corrected, but she is unable to actively maintain the fingers in extension. Management should consist of

Explanation
The patient has extensor tendon ruptures at the level of the wrist that are the result of synovitis at the distal radioulnar joint (Vaughn-Jackson syndrome). Extensor indius proprius transfer appropriately matches strength and excursion of the ruptured extensor digiti quinti and extensor digitorum communis tendons. An extensor tenosynovectomy with distal radioulnar joint resection decreases the synovitis, which if left untreated may cause additional tendon ruptures. Radial head resection is used for posterior interosseous nerve compression secondary to radial head synovitis, and in this patient only two fingers are involved, which rules out this diagnosis. Dynamic splinting is not indicated for ruptured tendons. Metacarpophalangeal arthroplasties and imbrication of the sagittal bands are used for metacarpophalangeal arthritis and extensor tendon subluxation. If this was the problem, the patient should be able to maintain the fingers in extension after they are passively extended. Total wrist arthrodesis prevents the tenodesis effect, thus limiting effective tendon excursion and making the proposed transfer less effective. Feldon P, Terrono AL, Nalebuff EA, et al: Rheumatoid arthritis and other connective tissue diseases: Tendon ruptures, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 1669-1684. Moore JR, Weiland AJ, Valdata L: Tendon ruptures in the rheumatoid hand: Analysis of treatment and functional results in 60 patients. J Hand Surg Am 1987;12:9-14.
Question 51High Yield
Design and manufacturing of a metal-on-metal articulation has an important influence on the tribology. Which of the following statements best characterizes the type of contact that is best for metal-on-metal articulations?
Explanation
It is important that the radii of a metal-on-metal head to cup articulation be such that there is polar contact. As the radii become closer to equal, conditions favor higher frictional torque and equatorial seizing. The "bedding in" of metal-on-metal surfaces and their stiffness are both components of the properties considered in the design of polar contact surfaces.
Question 52High Yield
A 35-year-old man sustained a 1-inch stab incision in his proximal forearm while trying to use a screwdriver 2 weeks ago. The laceration was routinely closed, and no problems about the incision site were noted. He now reports that he has been unable to straighten his fingers or thumb completely since the injury. Clinical photographs shown in Figures 30a and 30b show the man passively flexing the wrist. What is the most appropriate management?

Explanation
The clinical photographs indicate that the tenodesis effect of digit flexion with passive wrist extension and digit extension with passive wrist flexion is intact, indicating no discontinuity of the extensor or flexor tendons. The most likely injury is a laceration of the posterior interosseous nerve.
Question 53High Yield
A 35-year-old man is seen for evaluation of his left ankle following multiple previous ankle sprains and frequent episodes of the ankle giving way. Examination reveals marked laxity about the lateral ankle with associated tenderness along the peroneal tendons. Physical therapy, anti-inflammatory drugs, and supportive bracing have failed to provide relief. An MRI scan shows peroneal tenosynovitis and a possible tear. He elects to undergo a peroneal tendon repair and lateral ligament reconstruction. Which of the following best describes the structure labeled "A" in Figure 45?
Explanation
The structure labeled "A" is a peroneus quartus, a supernumary muscle arising most commonly from the peroneus brevis. The presence of peroneus quartus is not uncommon, with an incidence of up to 21%, and is associated with lateral ankle pain and peroneal tendon symptoms, theoretically as a result of mass effect within the peroneal tendon sheath. Zammit J, Singh D: The peroneus quartus muscle: Anatomy and clinical relevance. J Bone Joint Surg Br 2003;85:1134-1137.
Question 54High Yield
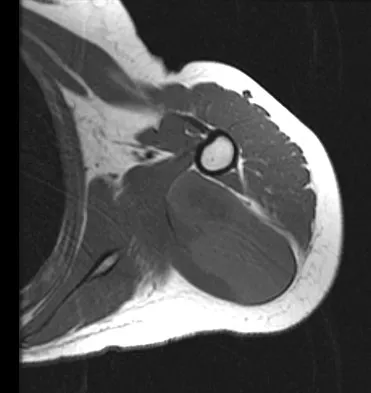
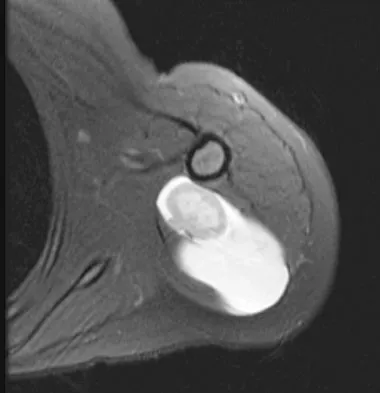
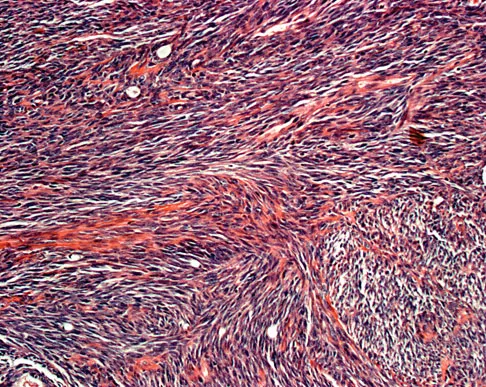
A 16-year-old girl has had painless swelling in her posterior left arm for the past 4 months. A radiograph, MRI scans, and an incisional biopsy specimen are shown in Figures 43a through 43d. What is the cytogenetic translocation most commonly associated with this tumor?
Explanation
This is a case of synovial sarcoma. The radiograph shows some soft-tissue swelling in the upper arm. The MRI scans show a lesion that has increased signal on T2-weighted images and low signal on T1-weighted images. There is a suggestion of a large cystic component to this lesion. The pathology shows a biphasic population of cells, a spindle cell component, and an epithelioid component. Up to 20% of synovial cell sarcomas have areas of cyst formation. The most common cytogenetic translocation with synovial cell sarcoma is X; 18. The 11; 22 translocation is most commonly associated with Ewing's sarcomas; the 12; 22 translocation is most commonly associated with clear cell sarcomas; the 2; 13 translocation is most commonly associated with alveolar rhabdomyosarcomas, and the 12; 16 translocation is most commonly associated with myxoid liposarcomas. Kawai A, Woodruff J, Healey JH, et al: SYT-SSX gene fusion as a determinant of morphology and prognosis in synovial sarcoma. New Engl J Med 1998;338:153-160.
Question 55High Yield
A 22-year-old professional ballet dancer reports a 3-month history of posterior ankle pain that occurs when she changes from a flat foot to pointe (hyperplantar flexed position). Examination does not elicit the pain with forced passive plantar flexion. A radiograph is shown in Figure 8. What is the most likely cause of the pain?
Explanation
Explanation
The most common causes of posterior ankle pain in ballet dancers are flexor hallucis longus tenosynovitis and os trigonum syndrome. Flexor hallucis longus tenosynovitis differs from a symptomatic os trigonum by the absence of pain with forced plantar flexion and the presence of pain with resisted plantar flexion of the great toe. The pain is often felt in the posterior ankle and can be associated with a snapping or triggering sensation. Os trigonum syndrome commonly occurs in ballet dancers who perform in a position of extreme plantar flexion. The pain occurs from entrapment of the os trigonum between the posterior portion of the talus and calcaneus. Hamilton WG, Geppert MJ, Thompson FM: Pain in the posterior aspect of the ankle in dancers: Differential diagnosis and operative treatment. J Bone Joint Surg Am 1996;78:1491-1500.
References:
- Khan K, Brown J, Way S, et al: Overuse injuries in classical ballet. Sports Med 1995;19:341-357.
Question 56High Yield
Figures 35a and 35b show the axial T2-weighted and coronal T1-weighted MRI scans of a patient who has enlargement of the right thigh. What is the most likely diagnosis?
Explanation
Explanation
35b The images show a large, almost circumferential, mass surrounding the diaphysis of the femur. The intramedullary signal is normal with minimal cortical destruction, both findings that should be abnormal in conventional osteosarcoma and Ewing's sarcoma. There are very low-signal striations representing osteoid formation that would have a sunburst radiographic pattern. This indicates an osteogenic lesion. Myositis ossificans is not indicated because studies would reveal zonal ossification starting in the periphery rather than the more central pattern seen in this patient. This appearance is typical for periosteal osteosarcoma.
References:
- El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 176.
Question 57High Yield
Figure 42 shows the sagittal T2-weighted MRI scan of a patient's right knee. These findings are most commonly seen with a complete tear of the
Explanation
Explanation
The MRI scan reveals disruption of the lateral capsule and ligaments with fluid in the soft tissues laterally. Additionally, there is a large bone bruise on the medial femoral condyle. This combination indicates injury to the posterolateral complex. These injuries often have coexisting anterior and/or posterior cruciate ligament injuries. Failure to recognize the posterolateral corner injury can lead to failure of anterior or posterior cruciate ligament reconstructions. LaPrade RF, Gilbert TJ, Bollom TS, et al: The magnetic resonance imaging appearance of individual structures of the posterolateral knee: A prospective study of normal knees and knees with surgically verified grade III injuries. Am J Sports Med 2000;28:191-199.
References:
- Ross G, Chapman AW, Newberg AR, et al: Magnetic resonance imaging for the evaluation of acute posterolateral complex injuries of the knee. Am J Sports Med 1997;25:444-448.
Question 58High Yield
Figure 7 shows a sagittal T1-weighted MRI scan. What muscle/tendon is identified by the arrow?
Explanation
Explanation
The sagittal T1-weighted MRI scan is useful for interpreting the quality of muscle. The arrow is pointing to the teres minor. Goutallier D, Postel JM, Gleyze P, et al: Influence of cuff muscle fatty degeneration on anatomic and functional outcomes after simple suture of full-thickness tears. J Shoulder Elbow Surg 2003;12:550-554.
References:
- Agur AM (ed): Grant's Atlas of Anatomy, ed 9. Baltimore, MD, Lippincott Williams & Wilkins, 1991, p 394.
Question 59High Yield
Figure 41 shows the MRI scan of a 38-year-old weightlifter. What does the arrow on the MRI scan indicate?
Explanation
Explanation
Pectoralis major ruptures typically occur in avid weightlifters (often on supplements) and typically while bench-pressing. Clinically there is significant discoloration/bruising over the pectoralis and into the axilla. MRI helps confirm the diagnosis and may help determine if the tear is in the muscle belly or at the bone-tendon junction. Bal GK, Basamania CJ: Pectoralis major tendon ruptures: Diagnosis and treatment. Tech Shoulder Elbow Surg 2005;6:128-134.
References:
- Aarimaa V, Rantanen J, Heikkila J, et al: Ruptures of the pectoralis major muscle. Am J Sports Med 2004;32:1256-1262.
Question 60High Yield
What is the most common diagnosis in a patient older than age 40 years with a destructive bony lesion?
Explanation
The most common destructive lesions in a patient older than age 40 years are, in decreasing incidence, metastatic carcinoma, multiple myeloma, lymphoma, and chondrosarcoma. Osteosarcoma is found primarily in younger patients.
Question 61High Yield
A 20-year-old man involved in a motor vehicle accident is brought to the emergency department with a C6-7 unilateral facet dislocation. His neurologic examination reveals a focal left-sided C7 nerve root palsy. He is awake and cooperative with questioning and has no other obvious traumatic injuries. What is the most appropriate treatment at this time?
Explanation
In the patient who is neurologically intact or has an incomplete injury from a cervical facet dislocation, a closed reduction with weighted tong traction is appropriate when the patient is awake, alert, and cooperative. Although there is a risk that a cervical facet dislocation could occur with an underlying cervical disk herniation, Vaccaro and associates have shown that closed reduction can be safely carried out in the awake, responsive patient. Closed reduction can be performed in the emergency department with traction with skull tongs or a halo ring. A slow stepwise application of weight is added until a reduction is achieved. Any worsening of the neurologic status of the patient requires immediate termination of the closed reduction and further diagnostic imaging before proceeding with further treatment. Vaccaro AR, Falatyn SP, Flanders AE, et al: Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine 1999;24:1210-1217. Hart RA: Cervical facet dislocation: When is magnetic resonance imaging indicated? Spine 2002;27:116-117.
Question 62High Yield
Outcome measures should have established psychometric properties of reliability, validity, and responsiveness. Reliability refers to which of the following?
Explanation
Explanation
The recent JBJS article by Kocher and associates defines the different psychometric properties that are used in outcome measures. Reliability is a measure of how reproducible a test is. This can be interobserver reliability (ie, reliability between people), or intraobserver reliability (ie, reliability for the same person doing the outcome measure at different occasions).
References:
- Kocher MS, Horan MP, Briggs KK, et al: Reliability, validity, and responsiveness of the American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability, rotator cuff disease, and glenohumeral arthritis. J Bone Joint Surg Am 2005;87:2006-2011.
Question 63High Yield
A 32-year-old man notes increasing back pain and progressive paraparesis over the past few weeks. He is febrile, and laboratory studies show a WBC of 12,500/mm3. MRI scans are shown in Figures 6a and 6b. Management should consist of

Explanation
Indications for surgery in spinal infections include progressive destruction despite antibiotic treatment, an abscess requiring drainage, neurologic deficit, need for diagnosis, and/or instability. This patient has a progressive neurologic deficit. Debridement performed at the site of the abscess should effect canal decompression. Once the debridement is complete back to viable bone, the defect can be reconstructed with a strut graft. Additional posterior stabilization is used as deemed necessary by the degree of anterior destruction. CT-guided needle aspiration, while occasionally useful in the earliest phases of an infection, produces frequent false-negative results and would provide little useful information in the management of this patient. Emery SE, Chan DP, Woodward HR: Treatment of hematogenous pyogenic vertebral osteomyelitis with anterior debridement and primary bone grafting. Spine 1989;14:284-291. Lifeso RM: Pyogenic spinal sepsis in adults. Spine 1990;15:1265-1271.
Question 64High Yield
A right-handed 14-year-old pitcher has had a 3-month history of shoulder pain while pitching. Examination reveals full range of motion, a mildly positive impingement sign, pain with rotational movement, and no instability. Plain AP radiographs of both shoulders are shown in Figures 25a and 25b. Management should consist of
Explanation
Explanation
25b The patient has the classic signs of Little Leaguer's shoulder, with findings that include pain localized to the proximal humerus during the act of throwing and radiographic evidence of widening of the proximal humeral physis. Examination usually reveals tenderness to palpation over the proximal humerus, but the presence of any swelling, weakness, atrophy, or loss of motion is unlikely. The treatment of choice is rest from throwing for at least 3 months, followed by a gradual return to pitching once the shoulder is asymptomatic. Carson WG Jr, Gasser SI: Little Leaguer's shoulder: A report of 23 cases. Am J Sports Med 1998;26:575-580.
References:
- Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in adolescent baseball pitchers. A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 65High Yield
A 21-year-old man has had posterior neck discomfort for the past 6 months. A whole-body bone scan and a cervical single-photon emission CT reveal increased activity at the C7 spinous process. MRI reveals multifocal involvement of the spinous process lamina and facet of C7. A CT-directed needle biopsy reveals osteoblastoma. What is the best course of action?
Explanation
Explanation
En bloc excision is the recommended treatment of osteoblastoma. Treatment should consist of en bloc removal of the lamina, facet, and spinous process. Facet removal would necessitate fusion. Radiation therapy is not recommended. Intralesional curettage has a high rate of recurrence. Bridwell KH, Ogilvie JW: Primary tumors of the spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery. Philadelphia, PA, JB Lippincott, 1991, vol 2, pp 1143-1174.
References:
- Ozaki T, Liljenquist U, Hillmann A, et al: Osteoid osteoma and osteoblastoma of the spine: Experience with 22 patients. Clin Orthop 2002;397:394-402.
Question 66High Yield
An axillary nerve lesion may cause weakness in the deltoid and the
Explanation
While the most prominent functional deficit from axillary nerve lesions occurs from denervation of the deltoid, denervation of the teres minor also occurs.
Question 67High Yield
A 57-year-old woman with diabetes mellitus has purulent drainage from a lateral incision after undergoing open reduction and internal fixation of a displaced ankle fracture 10 days ago. Examination reveals moderate erythema and a foul odor coming from the wound. Cultures are obtained. What is the next most appropriate step in management?
Explanation
Early postoperative wound infections after open reduction and internal fixation should be treated with aggressive debridement and maintenance of stability of the fracture. If infection persists following healing of the fracture, the hardware should be removed. Carragee EJ, Csongradi JJ, Bleck EE: Early complications in the operative treatment of ankle fractures: Influence of delay before operation. J Bone Joint Surg Br 1991;73:79-82.
Question 68High Yield
What is the most common reason for reoperation in total knee arthroplasty?
Explanation
Patellar problems currently constitute the largest number of complications after total knee arthroplasty, affecting between 8% and 35% of patients. These problems include patellar instability, fracture, component loosening, surface erosion, and pain. Malalignment, as an isolated reason for revision, is uncommon, yet it contributes to accelerated wear of the components. Joint instability affects up to 6% of patients, and the infection rate in knee arthroplasty is around 1% to 2%. Blasier RB, Matthews LS: Complications of prosthetic knee arthroplasty, in Epps CH (ed): Complications in Orthopaedic Surgery. Philadelphia, PA, JP Lippincott, 1994, pp 1066-1069. Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620.
Question 69High Yield
A patient has a humeral shaft fracture and is scheduled to undergo open reduction and internal fixation with a plate. What surgical approach will provide the greatest amount of exposure?
Explanation
Explanation
The modified posterior approach with elevation of the medial and lateral heads of the triceps can provide exposure of 94% of the humeral shaft. The traditional posterior triceps-splitting approach exposes 55% of the humeral shaft. DeFranco MJ, Lawton JN: Radial nerve injuries associated with humeral fractures. J Hand Surg Am 2006;31:655-663.
References:
- Gerwin M, Hotchkiss RN, Weiland AJ: Alternative operative exposure of the posterior aspect of the humeral diaphysis with reference to the radial nerve. J Bone Joint Surg Am 1996;78:1690-1695.
Question 70High Yield
A 48-year-old man reports localized plantar forefoot pain. Examination reveals a discrete callus (intractable plantar keratosis) with well-localized tenderness beneath the second metatarsal head. The callus most likely lies beneath what structure?
Explanation
Explanation
A discrete or focal callus is a response to excessive weight-bearing stress beneath the lateral (fibular) condyle of a lesser metatarsal head (most commonly second). The other structures generally have not been associated with a discrete callus. Coughlin MJ, Mann RA: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 413-465.
References:
- Cracchiolo A: Surgical procedures of the lateral metatarsals, in Jahss MH (ed): Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991, pp 1269-1283.
Question 71High Yield
Varus intertrochanteric osteotomy for coxa valga commonly produces which of the following results?
Explanation
Explanation
The greater trochanter is raised as a by-product of varus osteotomy, and a temporary abductor lag and lurch is common for 6 months following surgery. In the absence of hip joint subluxation, varus intertrochanteric osteotomy has no effect on the center edge angle of Wiberg. Varus osteotomy typically increases femoral offset, thereby improving the abductor lever arm and reducing the hip joint reaction force. Even without taking a wedge, varus osteotomy always produces some degree of shortening.
References:
- Millis MB, Murphy SB, Poss R : Osteotomies about the hip for the prevention and treatment of osteoarthrosis. Instr Course Lect 1996;45:209-226.
Question 72High Yield
Progressive paralysis is most likely to be seen in association with what type of congenital vertebral abnormality?
Explanation
Explanation
Anterior failure of formation results in a progressive kyphosis that may lead to cord compression and progressive neurologic deficit. Anterior failure of segmentation can also produce progressive kyphosis but usually is not severe enough to cause cord compression. Posterior failure of formation is seen in conditions such as myelomeningocele in which the neurologic deficit is generally stable. Lateral abnormalities and posterior failure of segmentation are rarely associated with progressive neurologic deficit. McMaster MJ, Singh H: Natural history of congenital kyphosis and kyphoscoliosis: A study of one hundred and twelve patients. J Bone Joint Surg Am 1999;81:1367-1383.
References:
- Dubousset J: Congenital kyphosis and lordosis, in Weinstein SL (ed): The Pediatric Spine: Principles and Practice, ed 1. New York, NY, Raven Press, 1994, pp 245-258.
Question 73High Yield
The injury seen in the CT scan shown in Figure 56 is related to or associated with injury to which of the following structures?
Explanation
Explanation
The right syndesmosis appears disrupted on the CT scan when compared to the normal left side. CT can be helpful in determining injury to the syndesmosis, especially with occult clinical findings. Ebraheim NA, Lu J, Yang H, et al: The fibular incisure of the tibia on CT scan: A cadaver study. Foot Ankle Int 1998;19:318-321. Ebraheim NA, Lu J, Yang H, et al: Radiographic and CT evaluation of tibiofibular syndesmotic diastasis: A cadaver study. Foot Ankle Int 1997;18:693-698.
References:
- Harper MC: Delayed reduction and stabilization of the tibiofibular syndesmosis. Foot Ankle Int 2001;22:15-18.
Question 74High Yield
Figure 16 shows the clinical photograph of a 3-month-old infant with a foot deformity that has been nonprogressive since birth. Examination reveals that the deformity corrects actively and with passive manipulation. There is no associated equinus. Management should consist of
Explanation
The patient has bilateral metatarsus adductus deformities. In a long-term follow-up study by Farsetti and associates, deformities that were passively correctable spontaneously resolved and no treatment was required. More rigid deformities were successfully treated with serial manipulation, with good results in 90%. There were no poor results. Therefore, observation is the management of choice for passively correctable deformities. In feet that are more rigid, serial manipulation and casting is the management of choice.
Question 75High Yield
A patient with a documented allergy to nickel requires a total knee arthroplasty. Which of the following prostheses is most likely to provide long-term success in this individual?
Explanation
Explanation
Nickel allergy is not an infrequent preoperative finding. The ramifications of such allergies in arthroplasty patients are poorly understood at this time. Stainless steel and cobalt-chromium alloys contain relatively high concentrations of nickel. Titanium, oxidized zirconium, and polyethylene do not contain significant amounts of nickel. Titanium is not a good surface for the articulating portion of the femoral component because of its propensity for metallosis. Oxidized zirconium is the only suitable femoral component for patients allergic to nickel. A modular titanium tibial component or an all-polyethylene tibial component would be satisfactory for these patients. Laskin RS: An oxidized Zr ceramic surfaced femoral component for total knee arthroplasty. Clin Orthop 2003;416:191-196.
References:
- Nasser S, Campbell PA, Kilgus D, et al: Cementless total joint arthroplasty prostheses with titanium-alloy articular surfaces: A human retrieval analysis. Clin Orthop 1990;261:171-185.
Question 76High Yield
A 30-year-old man who sustained a tibial fracture with a peroneal nerve palsy 2 years ago now has a drop foot and weak eversion of the foot. He reports success with stretching exercises, but he catches his toes when his foot tires. Examination reveals that the foot is plantigrade and supple. What is the next most appropriate step in management?
Explanation
Explanation
The patient has a supple plantigrade foot that would benefit from a drop foot brace to prevent catching of the toes. Tendon transfer should not be considered until the patient has undergone bracing. Achilles tendon lengthening is not necessary because the foot is plantigrade and flexible. Nerve grafting is not indicated because of the length of time the peroneal nerve palsy has been present. Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
References:
- Santi MD, Botte MJ: Nerve injury and repair in the foot and ankle. Foot Ankle Int 1996;17:425-439.
Question 77High Yield
A 66-year-old woman who previously underwent hemiarthroplasty 2 years ago for a fracture continues to have severe pain and loss of motion despite undergoing physical therapy. A radiograph is shown in Figure 2. What is the most likely reason that this patient has failed to improve her motion?
Explanation
The radiograph shows tuberosity malposition. The effect of improper prosthetic placement has also been associated with poor outcomes. However, the malposition of the tuberosity seen on the radiograph clearly explains loss of motion in this patient. It has been demonstrated that the functional results after hemiarthroplasty for three- and four-part proximal humeral fractures appear to be directly associated with tuberosity osteosynthesis. The most significant factor associated with poor and unsatisfactory postoperative functional results was malposition and/or migration of the tuberosities. Factors associated with a failure of tuberosity osteosynthesis in a recent study were poor initial position of the prosthesis, poor position of the greater tuberosity, and women older than age 75 years (most likely with osteopenic bone). Greater tuberosity displacement has been identified by Tanner and Cofield as being the most common complication after prosthetic arthroplasty for proximal humeral fractures. Furthermore, Bigliani and associates examined the causes of failure after prosthetic replacement for proximal humeral fractures and found that although almost all failed cases had multiple causes, the most common single identifiable reason was greater tuberosity displacement. Bigliani LU, Flatow EL, McCluskey G, et al: Failed prosthetic replacement for displaced proximal humeral fractures. Orthop Trans 1991;15:747-748. Boileau P, Krishnan SG, Tinsi L, et al: Tuberosity malposition and migration: Reasons for poor outcomes after hemiarthroplasty for displaced fractures of the proximal humerus. J Shoulder Elbow Surg 2002;11:401-412.
Question 78High Yield
Figures 42a through 42c show the clinical photographs and radiograph of a patient with diabetes mellitus who lives independently. The patient was admitted to the hospital late yesterday afternoon with clinical signs of sepsis. Parenteral antibiotic therapy resolved the sepsis, and blood glucose levels are now well controlled. The patient has no palpable pulses. The ankle-brachial index is 0.70. Laboratory studies show a WBC count of 8,500/mm3, a serum albumin of 1.9 g/dL, and a total lymphocyte count of 1,500/mm3. What treatment has the best potential to optimize his survival and independence?
Explanation
Explanation
42b 42c The patient was admitted to the hospital with sepsis. The sepsis has resolved, leaving the patient with a negative nitrogen balance. Now that the patient is stable, metabolic support should be used to optimize his nutrition. If the serum albumin can be increased to 2.5 g/dL, he has an excellent potential to heal an amputation at the Syme ankle disarticulation level; a level that will optimize his functional independence. Pinzur MS, Stuck RR, Sage R, et al: Syme ankle disarticulation in patients with diabetes. J Bone Joint Surg Am 2003;85:1667-1672.
Question 79High Yield
Patients who have osteonecrosis of the humeral head and who have the best prognosis are those with which of the following conditions?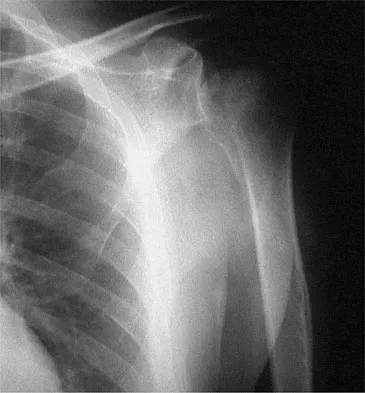
Explanation
The natural history of nontraumatic osteonecrosis varies greatly, so it is difficult to predict which patients will have severe arthrosis develop. Patients with sickle cell disease tend to have the most benign course. The most commonly reported cause of nontraumatic osteonecrosis is corticosteroid therapy. Fortunately, the incidence of osteonecrosis among patients treated with long-term systemic corticosteroids has fallen from more than 25% to less than 5% in recent years, owning to judicious steroid use and dosing. The interval between corticosteroid administration and the onset of shoulder symptoms is also variable, ranging from 6 to 18 months in one large series. This is comparable to the interval leading up to the onset of hip symptoms, which ranges from 6 months to 3 years or longer. The incidence of humeral head involvement has not been shown to vary with the underlying indication for steroid use. Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg 2002;11:281-298.
Question 80High Yield
A 1-year-old infant has the hand deformities shown in Figure 40. What pathologic process is the most likely cause of these deformities?
Explanation
Streeter's dysplasia is clearly related to rupture of the amnion in utero and is now most commonly referred to as premature amnion rupture sequence. The deformities arise from amniotic bands that wrap about protruding parts and from uterine packing because of the accompanying oligohydramnios. Clubfoot can develop as a result of the latter mechanism. Three limb involvement is most commonly seen, along with syndactyly. Treatment involves resection of bands and Z-plasty of skin. The disease is not genetic and has not been related to teratogen exposure or to iatrogenic influences such as amniocentesis. Developmental field disruption is not seen in this disease, and the growth potential of the involved parts is normal unless neurovascular disruption has arisen from band formation.
Question 81High Yield
In revision total hip arthroplasty, an acetabular reconstruction cage is best indicated for which of the following patterns of bone loss?
Explanation
Explanation
Acetabular cage reconstruction is indicated in severe disruption of acetabular bone stock when a cementless acetabular component cannot be stabilized in intimate contact with a sufficient bed of structurally sound and viable host bone, with or without a structural graft. Cages are used in pelvic discontinuity where they provide a bridge between the ilium and the ischium, while supporting a cemented cup. All of the other scenarios are amenable to achieving an adequate rim fit for a cementless component, using a jumbo cup if necessary. Whiteside LA: Selection of acetabular component, in Steinberg ME, Garino JP (eds): Revision Total Hip Arthroplasty. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 209-220.
References:
- Berry DJ, Muller ME: Revision arthroplasty using an anti-protrusio cage for massive acetabular bone deficiency. J Bone Joint Surg Br 1992;74:711-715.
Question 82High Yield
What is the most common location for localized pigmented villonodular synovitis (PVNS) to occur?
Explanation
Localized PVNS is a form of the disease in which synovial proliferation is restricted to one area of a joint and causes the formation of a small mass-like lesion. The true incidence of this is unknown but is probably less common than the diffuse form of the disease. PVNS presents as a usually painful discrete mass. The anterior compartment of the knee is the most common location. Tyler WK, Vidal AF, Williams RJ, et al: Pigmented villonodular synovitis. J Am Acad Orthop Surg 2006;14:376-385.
Question 83High Yield
A patient with rheumatoid arthritis has a rupture of the extensor digitorum communis to 4 and 5. You are planning to perform an extensor indicis proprius (EIP) tendon transfer. What effect will this have on index finger extension?
Explanation
EIP transfer results in no functional deficit. If the tendon is cut proximal to the sagittal band, there will be no extensor deficit. Browne EX, Teague MA, Snyder CC: Prevention of extensor lag after indicis proprius transfer. J Hand Surg Am 1979;4:168-172.
Question 84High Yield
What is the function of the rotator cuff during throwing?
Explanation
Explanation
The coupled action of the rotator cuff prevents superior migration and controls anterior and posterior translation by depressing the humeral head. Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
References:
- Abrams JS: Special shoulder problems in the throwing athlete: Pathology, diagnosis, and nonoperative management. Clin Sports Med 1991;10:839-861.
Question 85High Yield
An infant is born with a mass that involves both the volar and dorsal compartments of the left arm. A clinical photograph and biopsy specimen are shown in Figures 41a and 41b. What is the best initial course of action?
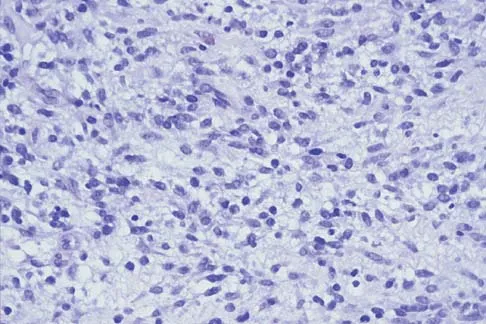
Explanation
The patient has infantile fibrosarcoma. For unresectable lesions, the treatment of choice is chemotherapy with vincristine, actinomycin-D, and cyclophosphamide, followed by excision if there is an adequate decrease in the size of the lesion.
Question 86High Yield
Which of the following patients with cerebral palsy is considered the ideal candidate for a selective dorsal rhizotomy?
Explanation
The enthusiasm with which dorsal rhizotomy was received led to the broadening of selection criteria with poorer results. The ideal candidate is an ambulatory 4- to 8-year-old child with spastic diplegia who does not use assistive devices or have joint contractures. The child must be old enough to actively participate in the rigorous postoperative physical therapy program. The use of the procedure in an ambulatory 16-year-old patient is less desirable because joint contractures will most likely have developed to a varying degree. The hemiplegic child is best treated by orthopaedic interventions. Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29. Renshaw TS, Green NE, Griffin PP, Root L: Cerebral palsy: Orthopaedic management. J Bone Joint Surg Am 1995;77:1590-1606.
Question 87High Yield
Which of the following results cannot be achieved with an in-shoe orthosis?
Explanation
Explanation
Depending on the type of materials used, an orthotic can be fabricated to achieve a variety of results. While a rigid fixed deformity can be stabilized or cushioned, an orthotic will not correct a deformity that is not passively correctable. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 55-64. Bono CM, Berberian WS: Orthotic devices: Degenerative disorders of the foot and ankle. Foot Ankle Clin 2001;6:329-340.
References:
- Buonomo LJ, Klein JS, Keiper TL: Orthotic devices: Custom-made, prefabricated, and material selection. Foot Ankle Clin 2001;6:249-252.
Question 88High Yield
An 11-year-old female gymnast has had gradually increasing right wrist pain for the past 6 months. Examination reveals normal range of motion and strength. Moderate tenderness is present over the distal radius. AP radiographs will most likely show
Explanation
Distal radial physeal stress syndrome has been reported in up to 25% of nonelite gymnasts showing premature closure of the distal radial physis and distal ulnar overgrowth, producing positive ulnar variance. The diagnosis should be suspected when there is tenderness at the distal radial physis in a young gymnast. The pathology is thought to be the result of repetitive compressive stresses caused by upper extremity weight-bearing forces. The recommended treatment is 3 to 6 months of rest. Salter-Harris fractures with a distal radial epiphyseal slip are unlikely, especially in the absence of a specific traumatic event. Mandelbaum BR, Bartolozzi AR, Davis CA, Teurlings L, Bragonier B: Wrist pain syndrome in the gymnast: Pathogenetic, diagnostic, and therapeutic consideration. Am J Sports Med 1989;17:305-317.
Question 89High Yield
A 43-year-old woman has an enlarging mass in the left groin. A radiograph, CT scan, and a biopsy specimen are shown in Figures 42a through 42c. Treatment should consist of


Explanation
The patient has a pelvic chondrosarcoma. The radiograph shows a lytic bone lesion emanating from the left inferior pubic ramus and extending into the soft tissues. Punctate calcifications are revealed on the radiograph and CT scan. The histology is consistent with a malignant cartilage lesion. Appropriate treatment for a pelvic chondrosarcoma is wide resection. In this location, wide resection of the ischiopelvic region (type 3 internal hemipelvectomy) is the treatment of choice. A type 2 internal hemipelvectomy involves resection of the periacetabular region. A type 1 internal hemipelvectomy involves resection of the ilium. No reconstruction is required for a type 3 resection. A classic hemipelvectomy is not necessary because the tumor can be removed with an adequate margin while maintaining the neurovascular structures and hip joint. Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642. Sheth DS, Yasko AW, Johnson ME, Ayala AG, Murray JA, Romsdahl MM: Chondrosarcoma of the pelvis: Prognostic factors for 67 patients treated with definitive surgery. Cancer 1996;78:745-750.
Question 90High Yield
A 26-year-old man is brought to the emergency department unresponsive and intubated after being found lying on the side of the road. He has a Glasgow Coma Scale score of 6. A chest tube has been inserted on the right side of the chest for a pneumothorax. An abdominal CT scan reveals a small liver laceration and minimal intraperitoneal hematoma. A pneumatic antishock garment (PASG) is on but not inflated. He has bilateral tibia fractures. A pelvic CT scan shows an anterior minimally displaced left sacral ala fracture and left superior and inferior rami fractures. He has received 2 L of saline solution and 4 units of blood but remains hemodynamically unstable. What is the next most appropriate step in management?
Explanation
Explanation
There is no identifiable thoracic, abdominal, or long bone source of ongoing bleeding. The patient has a lateral compression Burgess-Young type I pelvic ring injury. This injury does not increase the pelvic volume because it is not unstable in external rotation. Application of a PASG, a pelvic clamp, or an external fixator may be helpful if the patient has a pelvic injury that is unstable in external rotation or translation but would be of little use in this injury pattern. Persistent hemodynamic instability after administration of 4 units of blood is the decision point where most authors would recommend angiography and embolization. If the pelvis is unstable in external rotation or translation, inflation of the PASG trousers or application of an external fixator is recommended before angiography. Attributing the hemodynamic instability to the head injury before ruling out the pelvis as a source is not indicated. Burgess AR, Eastridge BJ, Young JW, et al: Pelvic ring disruptions: Effective classification system and treatment protocols. J Trauma 1990;30:848-856. Evers BM, Cryer HM, Miller FB: Pelvic fracture hemorrhage: Priorities in management. Arch Surg 1989;124:422-424.
References:
- Flint L, Babikian G, Anders M, Rodriguez J, Steinberg S: Definitive control of mortality from severe pelvic fracture. Ann Surg 1990;211:703-707.
Question 91High Yield
A 50-year-old woman who underwent a joint replacement of the hallux metatarsophalangeal joint 6 months ago now has pain and swelling about the great toe. Radiographs are shown in Figures 39a and 39b. What is the next most appropriate step in management?

Explanation
The radiographs show displacement of the prosthesis, and there has been large amounts of bone resected to insert the implant. Arthrodesis is indicated with interposition bone graft to stabilize the joint and restore length to the first ray.
Scientific References
- :
Question 92High Yield
A 55-year-old woman who underwent a left total hip arthroplasty 8 months ago using a modified Hardinger approach reports a persistent painless limp. Examination reveals that when she is not using a cane, she lurches to the left during weight bearing on the left lower extremity. An AP radiograph is shown in Figure 29. Which of the following hip muscle groups should be strengthened to improve the gait abnormality?
Explanation
Explanation
The modified Hardinger approach includes a partial anterior trochanteric osteotomy creating a trochanteric wafer (as seen on the radiograph) that is displaced anterior and medial in continuity with the gluteus medius and vastus lateralis. Failure of abductor reattachment, migration of the trochanter, nonunion of the osteotomy site, and excessive splitting of the gluteus medius muscle causing injury to the inferior branch of the superior gluteal nerve can result in weakness of the abductor mechanism. Abductor strength should be evaluated with the patient lying on the opposite side and elevating the affected limb. Although slight weakness may manifest itself as a limp only after prolonged muscular activity, significant weakness results in a constant limp without associated discomfort. Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 512-526.
References:
- Kasser JR (ed): Orthopedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 389-426.
Question 93High Yield
Which of the following is an advantage of unreamed nailing of the tibia compared to reamed nailing?
Explanation
Explanation
The debate between reamed versus unreamed intramedullary nailing of the tibia continues. Although unreamed nailing was proposed for open fractures to minimize infection, its simplicity made it appealing for closed fractures. However, most studies to date show that the only advantage of unreamed nailing is less surgical time. All studies show higher nonunion rates with increased hardware failure and increased time to union for unreamed nailing. Even in open fractures graded up to Gustilo Grade IIIA, the reamed tibial nail performs better. Larsen LB, Madsen JE, Hoiness PR, et al: Should insertion of intramedullary nails for tibial fractures be with or without reaming? A prospective, randomized study with 3.8 years' follow-up. J Orthop Trauma 2004;18:144-149.
References:
- Blachut PA, O'Brien PJ, Meek RN, et al: Interlocking intramedullary nailing with or without reaming for the treatment of closed fractures of the tibial shaft: A prospective randomized study. J Bone Joint Surg Am 1997;79:640-646.
Question 94High Yield
Osteoporosis is best diagnosed by
Explanation
Explanation
Risk factors can suggest the existence of osteoporosis. However, definitive testing, based on the use of bone densitometry measurements, uses the T score in which an average score is taken from a normal population of young women. The presence of increased osteoid in lamellar bone is seen in osteomalacia but not osteoporosis. The presence of fractures is evidence of a risk factor for osteoporosis and can predict future fractures, but it does not definitively confirm the diagnosis. The Singh index is a radiographic finding that is not as accurate as bone mineral density scores.
References:
- Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 141-154.
Question 95High Yield
Figure 11 shows the anatomic dissection of the medial side of the knee joint after removal of the superficial fascia. The arrow is pointing to what structure?
Explanation
Explanation
The semitendinosus and gracilis tendons lie beneath the superficial fascia and superficial to the medial collateral ligament. The semitendinosus is located more inferior to the gracilis tendon. The sartorius is more posterior and distal as is the medial collateral ligament. The semimembranosus is posterior. Pagnani MJ, Warner JJ, O'Brien SJ, Warren RF: Anatomic considerations in harvesting the semitendinosus and gracilis tendons and a technique of harvest. Am J Sports Med 1993;21:565-571.
References:
- Warren LF, Marshall JL: The supporting structures and layers on the medial side of the knee: An anatomical analysis. J Bone Joint Surg Am 1979;61:56-62.
Question 96High Yield
Osteonecrosis of the large joints may develop in patients with which of the following conditions?
Explanation
Osteonecrosis of major joints can occur in patients exposed to corticosteroids, alcohol, and antiseizure medications, as well as patients with hemaglobulinopathy, such as sickle cell anemia. In addition, patients with primary APS who had not taken corticosteroids were also found to be at high risk for osteonecrosis of the hip. In one study of 30 patients with primary APS, asymptomatic osteonecrosis was evident in 20%. A recent article has also found a high association between idiopathic osteonecrosis of the hip and collagen II mutation. None of the other conditions has been shown to be associated with a higher risk of osteonecrosis. Tektonidou MG, Malagari K, Vlachoyiannopoulos PG, et al: Asymptomatic avascular necrosis in patients with primary antiphospholipid syndrome in the absence of corticosteroid use: A prospective study by magnetic resonance imaging. Arthritis Rheum 2003;48:732-736.
Question 97High Yield
A 20-year-old man reports painless snapping about the lateral aspect of the right hip. He denies any history of trauma. Examination reveals no limp or tenderness. Hip range of motion is full, and there is good strength. Radiographs are normal. What anatomic structure is most likely causing these symptoms?
Explanation
Coxa saltans (snapping hip syndrome) can occur in two forms: external/lateral or interior/medial/anterior. This patient has the external/lateral form. The external/lateral form involves the iliotibial band, tensor fascia, or gluteus medius, which snaps over the greater trochanter. The external form usually can be treated with physical therapy alone; however, several recent studies report satisfactory results with surgical treatment. Faraj and associates reported good results from surgical Z-plasty in a series of 10 patients. White and associates reported good results in a series of 16 patients with 17 hips who underwent surgical release of an external snapping hip. The interior/medial/anterior form can involve the iliopsoas tendon, acetabular labrum, subluxation of the hip, and loose bodies. White RA, Hughes MS, Burd T, et al: A new operative approach in the correction of external coxa saltans: The snapping hip. Am J Sports Med 2004;32:1504-1508. Faraj AA, Moulton A, Sirivastava VM: Snapping iliotibial band: Report of ten cases and review of the literature. Acta Orthop Belg 2001;67:19-23.
Question 98High Yield
In children with isolated zone II lacerations of the flexor tendon, poor digital motion is best correlated with
Explanation
In a recent study on restoration of motion following zone I and zone II flexor tendon repairs in children, age was found to have no effect on the results of zone II tendon repairs. Early passive motion offered no better results than immobilization for 3 weeks. Immobilization for more than 4 weeks correlated with poorer results.
Question 99High Yield
Which of the following is considered the best method to measure limb-length discrepancy in a patient with a knee flexion contracture?
Explanation
Explanation
The most effective way to measure a limb-length discrepancy in a patient with a knee flexion contracture is a lateral CT scanogram. All the other methods listed provide inaccurate results with a knee flexion contracture because the measurements are made in the coronal plane. Aaron A, Weinstein D, Thickman D, et al: Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg Am 1992;74:897-902.
References:
- Tachdjian MO: Clinical Pediatric Orthopaedics: The Art of Diagnosis and Principles of Management. Stamford, CT, Appleton and Lange, 1997, pp 237-240.
Question 100High Yield
A 55-year-old man underwent cementless total hip arthroplasty for advanced painful osteoarthritis of the hip 2 years ago. The follow-up radiograph shown in Figure 30 shows
Explanation
The radiograph shows a well-osseointegrated tapered stem with a metaphyseal porous coating, spot welds in the porous region, and calcar rounding. Trochanteric stress shielding and distal cortical hypertrophy are also signs of ingrown stems but are seen more frequently in association with extensively porous-coated stems exhibiting diaphyseal ingrowth. There is no evidence of lucent lines or a pedestal, signs that suggest instability. Femoral stem subsidence can be determined only by a review of sequential radiographs. Engh CA, Massin P, Suthers KE: Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop 1990;257:107-128.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon