Orthopedic Board Review MCQs: ABOS, OITE, FRCS Mock Exam Set #975
14 Apr 2026
104 min read
79 Views
Key Takeaway
This page offers 100 high-yield orthopedic board review questions (MCQs) for ABOS, OITE, and FRCS exams. Surgeons can use this practice test (Set 975) to strengthen knowledge, identify weak areas, and master essential concepts for successful exam preparation and certification.
Secure Rotator Cuff Repair: Mastering the Hor...
00:00
Start Quiz
Question 1High Yield
What is the maximum acceptable amount of divergence of the interference screw in the femoral tunnel from the bone plug of a bone-patellar tendon-bone graft in anterior cruciate ligament (ACL) reconstruction before pull-out strength is statistically decreased?
Explanation
In the early 1990s, a transition was made from a two-incision ACL reconstruction to a single-incision ACL reconstruction, and there was concern over divergence of the femoral screws. It was shown radiographically that approximately 5% of the time, divergence of the screw was greater than 15 degrees from the bone plug. In a bovine model, there was significant loss of pull-out strength with an increase in divergence from 15 degrees to 30 degrees. Therefore, attempts should be made to minimize divergence to 15 degrees or less. Lemos MJ, Jackson DW, Lee TO, et al: Assessment of initial fixation of endoscopic interference femoral screws with divergent and parallel placement. Arthroscopy 1995;11:37-41.
Question 2High Yield
A 43-year-old former professional hockey player reports severe pain in his chest after being checked from the side in a pick-up hockey game. An MRI scan and plain radiographs are shown in Figures 25a through 25c. What is the most likely diagnosis?


Explanation
Anterior dislocation is the most common type of sternoclavicular dislocation. The medial end of the clavicle is displaced anterior or anterosuperior to the anterior margin of the sternum. In a study by Omer, 31% of athletic injuries have been known to cause a dislocation of the sternoclavicular joint. The serendipity view can show this dislocation, as will CT of the chest. This view requires the x-ray beam to be aimed at the manubrium with 40 degrees of cephalic tilt. An anterior sternoclavicular joint dislocation will appear superiorly displaced, while a posterior sternoclavicular joint dislocation is inferiorly displaced on the serendipity view. Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 566-572.
Question 3High Yield
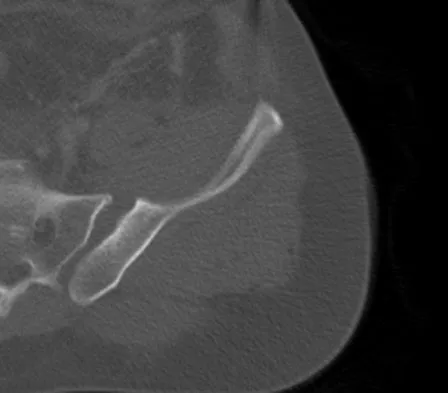
Examination of a 12-year-old girl with a painful flatfoot deformity reveals tenderness in the region of the sinus tarsi and no appreciable subtalar motion. Radiographs are shown in Figures 48a through 48c. Two attempts to relieve her symptoms by cast immobilization fail to relieve the pain. Management should now consist of
Explanation
Explanation
48b 48c Surgical treatment is indicated for a symptomatic tarsal coalition that has failed to respond to nonsurgical management. In this patient, the radiographs reveal a calcaneonavicular coalition and no degenerative changes. The patient is symptomatic, and two attempts at use of a short leg walking cast have failed to provide relief. For calcaneonavicular coalitions, good results have been reported following resection and interposition of the extensor digitorum brevis. A retrospective study of this procedure achieved good to excellent results in 58 of 75 feet (77%). Degenerative arthritis or persistent pain following resection of a coalition is a reasonable indication for a triple arthodesis. A medial closing wedge osteotomy of the calcaneus may be indicated for a rigid flatfoot with severe valgus deformity. There are no studies documenting the long-term effectiveness of a manipulation under general anesthesia for this condition. Gonzalez P, Kumar SJ: Calcaneonavicular coalition treated by resection and interpostion of the extensor digitorum brevis muscle. J Bone Joint Surg Am 1990;72:71-77.
References:
- Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 211-218.
Question 4High Yield
What assay most directly assesses gene expression at the posttranslational level?
Explanation
Explanation
Gene expression at the posttranslational level refers to proteins, as opposed to DNA or RNA. The only assay above that targets protein expression directly is the Western blot. Standard PCR is amplification of targeted DNA segments, regardless of whether or not they are actively expressed. Real-time PCR, Northern blot, and microarray expression profile analysis all quantify RNA as a means to determine posttranscriptional gene expression. Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94.
References:
- Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 19-76.
Question 5High Yield
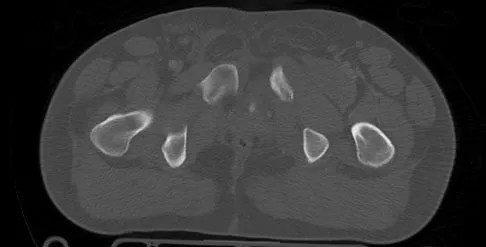
An 18-year-old collegiate basketball player has had a 3-month history of activity-related back pain. She describes isolated low back pain without radiation that increases with training and playing basketball. Her pain resolves with rest. Physical therapy for 6 weeks has failed to provide relief. An axial CT scan is shown in Figure 17a, and Figures 17b and 17c show sagittal CT reconstructions through the right and left lumbar facets, respectively. Further management should consist of which of the following?


Explanation
The sagittal and axial CT scans show a bilateral spondylolysis at L5. The defect is in the pars interarticularis on the right side but at the base of the pedicle on the left. Having failed a trial of physical therapy with only a 3-month history of pain, the next most appropriate step in management should consist of activity modification and bracing in an antilordotic lumbosacral orthosis. Surgical intervention is reserved for patients who have failed to respond to a trial of bracing and activity restriction. Debnath UK, Freeman BJ, Grevitt MP, et al: Clinical outcome of symptomatic unilateral stress injuries of the lumbar pars interarticularis. Spine 2007;32:995-1000.
Question 6High Yield
An 18-year-old hockey player sustains an acute anterior shoulder dislocation that requires manual reduction. At arthroscopy, the lesion shown in Figure 24 will be observed in what percent of patients?
Explanation
Explanation
The clinical photograph shows an acute capsulolabral avulsion from the anterior glenoid, also referred to as a Perthes-Bankart lesion. In patients who sustain an acute dislocation that requires a manual reduction, this pathologic lesion is observed with high frequency. In several research studies, it has been visualized in 80% to 95% of patients at arthroscopy. Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.
References:
- Baker CL, Uribe JW, Whitman C: Arthroscopic evaluation of acute initial anterior shoulder dislocations. Am J Sports Med 1990;18:25-28.
Question 7High Yield
During what phase of the throwing motion is the highest torque measured across the glenohumeral joint?
Explanation
Explanation
Electromyography is used to evaluate muscular firing patterns about the shoulder during the throwing sequence. The rotator cuff muscles and biceps are relatively inactive during the acceleration phase, whereas the pectoralis major, serratus anterior, latissimus dorsi, and subscapularis show highest activity. By contrast, deceleration is accomplished by the rotator cuff musculature and the larger trunk muscles acting in concert to slow down the arm. It is during this phase of follow through that the highest torque is measured secondary to eccentric muscle contraction. Jobe FW, Moynes DR, Tibone JE, Perry J: An EMG analysis of the shoulder in pitching: A second report. Am J Sports Med 1984;12:218-220. Pappas AM, Zawacki RM, Sulliva TJ: Biomechanics of baseball pitching: A preliminary report. Am J Sports Med 1985;13:216-222.
References:
- Altcheck DW, Dines DM: Shoulder injuries in the throwing athlete. J Am Acad Orthop Surg 1995;3:159-165.
Question 8High Yield
A knock-out mouse for the Vitamin D receptor has which of the following phenotypes?
Explanation
A knock-out mouse to the Vitamin D receptor would cause loss of vitamin D function, resulting in rickets. Renal failure would not occur; although Vitamin D is converted from 25 (OH) D to 1,25 (OH) D in the kidney, the active hormone acts on the gut and bone. Osteopetrosis can be seen as the phenotype for the c fos knock-out mouse; the Jansen-type metaphyseal dysplasia phenotype results from overactivation of the PTH/PTHrp receptor. Although compensatory hyperparathyroidism would occur, excessive PTH would not be able to rescue the skeletal loss and instead phosphoturia and phosphotasia would result. Glowacki J, Hurwitz S, Thornhill TS, et al: Osteoporosis and vitamin-D deficiency among postmenopausal women with osteoarthritis undergoing total hip arthroplasty. J Bone Joint Surg Am 2003;85:2371-2377.
Question 9High Yield
What structure is considered the single most important soft-tissue restraint to anterior-posterior stability of the sternoclavicular joint?
Explanation
In a cadaver ligament sectioning study, the posterior capsular ligament was considered the most important structure for anterior-posterior stability of the sternoclavicular joint. The anterior capsular ligament also helps prevent anterior displacement but not to the same degree as the posterior ligament. The interclavicular ligament provides little support for anteroposterior translation. Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Question 10High Yield
Which of the following statements best characterizes polymethylmethacrylate (PMMA) when it is used to secure joint components in bone and to distribute the forces evenly across the bone-implant interface?
Explanation
Explanation
PMMA has no adhesive properties and can be more accurately described as grout than glue. It does not chemically bond to bone or implants; however, mechanical bonding is accomplished with porous or coated components and with cancellous bone. PMMA is approximately three times stronger in compression than in tension. Peak blood levels of monomer are usually seen approximately 3 minutes after the cement is placed. The monomer is cleared by the lungs. Associated hypotension is more closely related to diminished blood volume than to circulating monomer levels. High porosity decreases the tensile and fatigue properties of cement. Manually mixed cement may have porosity as high as 27%. Porosity may be reduced to less than 1% through vacuum mixing or centrifugation of the cement. When adding antibiotics to cement, the compressive and tensile forces are not appreciably decreased, but the overall fatigue strength may be reduced. Canale ST (ed): Campbell's Operative Orthopaedics, ed 9. St Louis, MO, Mosby, 1998, pp 221-224.
References:
- Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 27-33.
Question 11High Yield
Which of the following agents increases the risk for a nonunion following a posterior spinal fusion?
Explanation
Nonsteroidal anti-inflammatory drugs (NSAIDs) have been shown to increase the risk of pseudarthrosis. In a controlled rabbit study, nonunions were reported with the use of toradol and indomethacin. NSAIDs are commonly used medications with the potential to diminish osteogenesis. Studies clearly have demonstrated inhibition of spinal fusion following the postoperative administration of several NSAIDs, including ibuprofen. Cigarette smoking is another potent inhibitor of spinal fusion. Glassman SD, Rose SM, Dimar JR, et al: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Question 12High Yield
During total knee arthroplasty, the patella is noted to subluxate laterally despite a lateral retinacular release. Which of the following methods is most likely to improve patellar stability?
Explanation
Explanation
Slight external rotation of the tibial component will cause a net medialization of the tibial tubercle when the knee is articulated. This will help centralize the extensor mechanism over the trochlear groove and minimize the tendency for lateral subluxation. Internal rotation of the femoral component increases the risk of patellar instability. Anterior translation of the tibial component moves the patellar tendon insertion posteriorly, and may increase force on the patella but should not substantially alter patellar tracking. Clinical studies have shown no patellofemoral benefits to the use of fixed- or mobile-bearing designs. Thicker patellar components will not improve tracking, and may compound the problem. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 207, 323-337 Pagnano MW, Trousdale RT, Stuart MJ, et al: Rotating platform knees did not improve patellar tracking: A prospective, randomized study of 240 primary total knee arthroplasties. Clin Orthop 2004;428:221-227.
References:
- Lotke PA, Garino JP (eds): Revision Total Knee Arthroplasty. Philadelphia PA, Lippincott-Raven, 1999, pp 427-435.
Question 13High Yield
Examination of a 7-year-old boy reveals 20 degrees of valgus following a lawn mower injury to the lateral femoral epiphysis. Treatment consists of total distal femoral epiphyseodesis and varus osteotomy. Following surgery, he has a limb-length discrepancy of 3 cm and 5 degrees of genu valgum. Assuming that he undergoes no further treatment, the patient's predicted limb-length discrepancy at maturity would be how many centimeters?
Explanation
The distal femoral epiphysis grows approximately 1 cm per year and in boys, growth ceases at approximately age 16 years. Therefore, the patient's limb-length discrepancy at maturity would be 12 cm (9 cm plus the 3-cm discrepancy he has from the previous surgery). Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphyseodesis. J Pediatr Orthop 1996;16:173-179.
Question 14High Yield
A 4-year-old girl sustains an isolated spiral femoral fracture after falling from her tricycle. Management should consist of
Explanation
Immediate spica casting is ideal for younger children with uncomplicated femoral fractures that are the result of relatively low-energy injury. Surgical stabilization of pediatric femoral fractures is most commonly performed in children who are older than age 6 years or in children with other factors associated with their femoral fracture, such as concomitant head injury, open fracture, floating knee, severe comminution, or vascular injury. Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659. Sponseller PD: Surgical management of pediatric femoral fractures. Instr Course Lect 2002;51:361-365. Wright JG: The treatment of femoral shaft fractures in children: A systematic overview and critical appraisal of the literature. Can J Surg 2000;43:180-189.
Question 15High Yield
A 16-year-old boy has had thigh pain for the past several months. He denies any history of trauma. Examination reveals a large, deeply fixed, soft-tissue mass in the thigh. Laboratory results show an elevated erythrocyte sedimentation rate (ESR) and leukocytosis. A plain radiograph and MRI scan are shown in Figures 1a and 1b. Biopsy specimens are shown in Figures 1c and 1d. What is the most likely diagnosis?



Explanation
Ewing's sarcoma typically can occur in the diaphysis of the long bones (50% to 55%). It is often accompanied by a large soft-tissue mass. Abnormal findings are common, including a low-grade fever, an elevated ESR, and leukocytosis. The histology is consistent with a small round blue cell tumor. The unique pathology and other findings exclude osteosarcoma. Giant cell tumor and chondrosarcoma have a different histologic appearance and typically are more metaphyseal in location. Chondrosarcoma typically is found in older age groups, has a different histologic pattern, and rarely occurs in the midshaft of the femur.
Question 16High Yield
The photomicrograph in Figure 37 shows a repaired dural tear 4 days after surgery. The material interposed between the dural edges (D) is composed of
Explanation
During the initial healing phases of a dural tear, pia and arachnoid from adjacent nerve roots migrate, fill the dural defect, and create a pia-arachnoid plug. It is this initial plugging of the defect that is believed to prevent further egress of cerebrospinal fluid through the defect. The plug has been shown to develop by the second postoperative day. Fibroblastic proliferation occurs within the dura itself and accounts for the bulbous ends of the dura seen in the photomicrograph. The appearance of the material within the dural edges is inconsistent with the appearance of neural elements, and scar tissue formation occurs later in the healing process. Cain JE Jr, Dryer RF, Barton BR: Evaluation of dural closure techniques: Suture methods, fibrin adhesive sealant, and cyanoacrylate polymer. Spine 1988;13:720-725.
Question 17High Yield
A 6-year-old girl is referred for the elbow injury seen in Figure 2. What is the most appropriate treatment?
Explanation
Explanation
The patient has a displaced lateral condyle fracture; therefore, simple immobilization for 3 to 8 weeks is likely to result in malunion or nonunion. Closed reduction of such injuries is rarely successful. The fracture is unstable, so fixation is required after open reduction. Because the fixation must cross the physis, smooth pins are indicated for the skeletally immature elbow. Open reduction with fixation has been shown to reduce the risk of delayed union and malunion. Beaty JH, Kasser JR: The elbow: Physeal fractures, apophyseal injuries of the distal humerus, avascular necrosis of the trochlea, and T-condylar fractures, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 625-703. Rutherford A: Fractures of the lateral humeral condyle in children. J Bone Joint Surg Am 1985;67:851-856.
References:
- Hasler CC, von Laer L: Prevention of growth disturbances after fractures of the lateral humeral condyle in children. J Pediatr Orthop B 2001;10:123-130.
Question 18High Yield
To preserve blood supply to the fractured bone seen in Figures 12a and 12b, care should be taken when exposing which of the following areas?
Explanation
Explanation
12b The blood supply to the adult capitellum and lateral trochlea comes from posterior vessels arising from the radial recurrent, radial collateral, and interosseous recurrent arteries. These arteries penetrate the distal humerus posterior and superior to the capitellum.
References:
- Yamaguchi K, Sweet FA, Bindra R, et al: The extraosseous and intraosseous arterial anatomy of the adult elbow. J Bone Joint Surg Am 1997;79:1653-1662.
Question 19High Yield
During total knee arthroplasty, what component position aids in proper tracking and stability of the patellar component?
Explanation
Explanation
The femoral component should be implanted with enough external rotation to facilitate patellar tracking. Proper tracking requires a normal Q angle and is affected by axial and rotational alignment of the femur and tibia. An excessive Q angle can result from internal rotation of either component, medialization of the tibial tray, or lateralization of the patellar component. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
References:
- Lonner JH, Lotke PA: Aseptic complications after total knee arthroplasty. J Am Acad Orthop Surg 1999;7:311-324.
Question 20High Yield
A 21-year-old man has had progressive right knee pain for the past 2 months that is exacerbated with weight-bearing activities. A plain radiograph and an MRI scan are shown in Figures 43a and 43b. A biopsy specimen is shown in Figure 43c. According to the Enneking staging system of tumor classification, the lesion should be classified as what stage?
Explanation
Explanation
43b 43c The lesion is an eccentric lytic bone lesion within the epiphyseal-metaphyseal end of the proximal tibia. There is geographic destruction with a "fading border" extending to the articular cartilage. There is no matrix formation or periosteal reaction. The MRI scan shows cortical destruction with extension into the soft tissue. According to the Enneking staging system, benign lesions are stage 1, 2, or 3; malignant lesions are stage I, II, or III. Benign stage 1 lesions are latent; stage 2 are active; and stage 3 are benign aggressive. The histology shows a benign giant cell tumor. Given the cortical breakthrough shown on the MRI scan, the lesion should be classified as stage 3. Enneking WF: Clinical musculoskeletal pathology, in Enneking WF (ed): Appendix A. Gainesville, FL, Storter Publishing, 1986, pp 451-466.
References:
- Aboulafia AJ, Kennon RE, Jelinek JS: Benign bone tumors of childhood. J Am Acad Orthop Surg 1999;7:377-388.
Question 21High Yield
A 35-year-old man reports the development of a painful 2-cm nodule on his dorsal wrist over the past 3 years. A surgeon excised the lesion with a presumptive diagnosis of a ganglion cyst. Histology sections from the excision are shown in Figures 11a and 11b. What is the most likely diagnosis?

Explanation
The histologic appearance of the soft-tissue lesion reveals compact nests of cells with a clear cytoplasm surrounded by a delicate border of fibrocollagenous tissue. There can be scattered multinucleated giant cells. This is consistent with a clear cell sarcoma, also called malignant melanoma of soft parts. This tumor is usually positive for S-100 and HMB45 (a melanoma-associated antigen). These tumors are frequently found around the foot and ankle. Similar to epithelioid sarcoma, it is usually intimately bound to tendons or tendon sheaths. Often the tumors are present for many years. The classic histologic appearance of this lesion differentiates it from the other choices. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 913.
Question 22High Yield
Which of the following structures runs through the site indicated by the arrow in Figure 11?
Explanation
The vertebral artery traverses through the arcuate foramen after exiting the lateral aspect of C1 and before entering the skull. The foramen usually is not fully formed, but a complete foramen such as this one has been reported in up to 18% of patients. Stubbs DM: The arcuate foramen: Variability in distribution related to race and sex. Spine 1992;17:1502-1504.
Question 23High Yield
A 7-year-old boy has a swollen and deformed right arm after falling off his bicycle. Radiographs reveal a completely displaced posterolateral supracondylar humeral fracture. Examination reveals a warm, pink hand and forearm but absent pulses. What is the next most appropriate step in management?
Explanation
Explanation
The incidence of vascular injury in supracondylar humeral fractures is directly related to the degree and direction of displacement. Significant posterior lateral displacement tends to result in brachial artery and median nerve injuries, and posterior medial displacement may lead to radial nerve injury. The brachial artery is always injured at the level of the fracture; therefore, angiography or MRA will not assist in locating the injury. The treatment of choice is surgical reduction and stabilization of the fracture, followed by reassessment of the vascular status. If the hand is pink and warm or pulses can be detected with doppler, it is reasonable to follow the extremity closely after surgery. If the arm becomes pulseless and white, immediate anterior exploration of the arm is indicated. The artery is often entrapped in the fracture and once extricated, will provide adequate blood flow. If the artery is injured, a primary repair or vein graft is needed. Shaw BA: The role of angiography in assessing vascular injuries associated with supracondylar humerus fractures remains controversial. J Pediatr Orthop 1998;18:273. Sabharwal S, Tredwell SJ, Beauchamp RD, et al: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
References:
- Schoenecker PL, Delgado E, Rotman M, et al: Pulseless arm in association with totally displaced supracondylar fracture. J Orthop Trauma 1996;10:410-415.
Question 24High Yield
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?
Explanation
The combination of an elbow dislocation and a fracture of the radial head and coronoid is known as a terrible triad injury. To restore elbow stability, each injury must be addressed. The nonreconstructable radial head fracture requires implant arthroplasty. Open reduction and internal fixation of the coronoid is also necessary as is repair of the lateral collateral ligament complex which is usually avulsed from the lateral epicondyle region. Ring D, Quintero J, Jupiter JB: Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002;84:1811-1815. Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Question 25High Yield
Figures 9a and 9b show the radiographs of a 4-year-old child who sustained an elbow injury. What is the most likely complication resulting from this fracture if treated in a cast?

Explanation
The radiographs show a lateral condyle fracture with 2 mm of displacement. As opposed to other pediatric elbow fractures, lateral condyle fractures have a higher incidence of nonunion. This may be due to minimal metaphyseal bone on the distal fragment, the intra-articular nature of the fracture, or from further displacement when treated nonsurgically. These fractures with 2 mm and greater of displacement should be treated with reduction and stabilization. Osteonecrosis and fishtail deformity may be seen in very rare cases of lateral condyle fractures. The incidence is certainly less than the rates of nonunion seen in nonsurgically treated fractures with 2 mm and greater of displacement. Varus malunion from overgrowth and elbow stiffness are more likely seen in fractures treated surgically. Pirker ME, Weinberg AM, Hollwarth ME, et al: Subsequent displacement of initially nondisplaced and minimally displaced fractures of the lateral humeral condyle in children. J Trauma 2005;58:1202-1207. Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425.
Question 26High Yield
The iliopectineal fascia runs between which of the following structures?
Explanation
Explanation
The sheath of the psoas muscle or the iliopectineal fascia separates the more lateral iliopsoas muscle and the femoral nerve from the more medially located iliac vessels. This fascia has to be taken down to enter the true pelvis. Masquelet AC, McCullough CJ, Tubiana R: An Atlas of Surgical Exposures of the Lower Extremity. Philadelphia, PA, JB Lippincott, 1993. Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Question 27High Yield
An 8-month-old infant has an infection of the fingertip as shown in Figure 22. If neglected, the anticipated path of ascending infection is the fingertip, the flexor sheath, and the
Explanation
Explanation
The flexor sheaths are in continuity with the deep spaces of the hand. The flexor sheaths of the thumb and little finger communicate with the radial and ulnar bursae, respectively, and these two bursae commonly communicate. The central digits do not communicate as readily with deep spaces of the hand but if flexor tendon sheath infection of the index, long, and right fingers is neglected, the potential exists for rupture into the deep midpalmar spaces. Peimer CA (ed): Surgery of the Hand and Upper Extremity: Acute and Chronic Sepsis. New York, NY, Mcgraw Hill, 1996, pp 1735-1741.
References:
- Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow and Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 445-446.
Question 28High Yield
A 25-year-old man sustained the closed injury shown in Figures 22a and 22b. Examination reveals that this is an isolated injury, and he is hemodynamically stable. Treatment should consist of
Explanation
Explanation
22b The treatment of choice for closed diaphyseal femoral fractures in adults is reamed intramedullary nailing with static interlocking. Reaming allows placement of a larger, stronger implant and offers better healing rates than unreamed nailing. Static interlocking ensures that there is no loss of reduction because of underappreciated fracture lines or comminution. Brumback RJ, Virkus WW: Intramedullary nailing of the femur: Reamed versus nonreamed. J Am Acad Orthop Surg 2000;8:83-90.
References:
- Brumback RJ, Ellison TS, Poka A, et al: Intramedullary nailing of femoral shaft fractures: Part III. Long-term effects of static interlocking fixation. J Bone Joint Surg Am 1992;74:106-112.
Question 29High Yield
The wear resistance of ultra-high molecular weight polyethylene can be improved by exposing the polymer to high-energy radiation (eg, gamma or electron beam), followed by a thermal treatment. What is one detrimental side effect of this process?
Explanation
Explanation
Highly cross-linked polyethylene has gained widespread acceptance for joint arthroplasty components because of reported experimental and early clinical accounts of significant reductions in wear. Cross-linking is increased by imparting additional energy into the polymer (above that conventionally used for sterilization). The thermal treatments after cross-linking stabilize the material against oxidative degradation by quenching free radicals and also reduce the elastic modulus. One disadvantage of the increased cross-linking is a reduction in toughness that makes the polyethylene more susceptible to crack initiation and propagation. The reduced toughness raises concerns for gross component fracture and fracture at stress concentrations that can arise with the locking mechanisms used to secure polyethylene inserts into metallic backings. Nonconsolidated polyethylene particles have been associated with increased subsurface density secondary to oxidative degradation in conventional polyethylene implants. The quenching of free radicals by thermal treatment in highly cross-linked polyethylene should prevent this problem. Collier JP, Currier BH, Kennedy FE, et al: Comparison of cross-linked polyethylene materials for orthopaedic applications. Clin Orthop 2003;414:289-304. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 203-208.
References:
- Wright TM, Maher SA: Biomaterials, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 30High Yield
A 21-year-old woman who was wearing a seat belt sustained an injury of the thoracolumbar junction in a motor vehicle accident. The AP radiograph shows widening between the L1 and L2 spinous processes, and the CT scan shows the empty facet sign at this level. The initial evaluation should include
Explanation
The patient has a flexion-distraction injury of the thoracolumbar spine that is often associated with wearing a seat belt. The fracture has a high risk of associated intra-abdominal injury; therefore, the initial evaluation should include a CT of the abdomen. The most common visceral injury is to the bowel. Smith WS, Kaufer H: Patterns and mechanisms of lumbar injuries associated with lap seat belts. J Bone Joint Surg Am 1969;51:239-254.
Question 31High Yield
What is the typical MRI signal intensity of bone marrow affected by acute osteomyelitis?
Explanation
The classic MRI findings of osteomyelitis are a decrease in the normally high signal intensity of marrow on T1-weighted images and normal or increased signal intensity on T2-weighted images. This is the result of replacement of marrow fat by inflammatory cells and edema, which causes lower signal intensity than fat on T1-weighted images and higher signal intensity than fat on T2-weighted images. The addition of gadolinium to a T1-weighted sequence reveals increased signal intensity in the hyperemic marrow. Unger E, Moldofsky P, Gatenby R, et al: Diagnosis of osteomyelitis by MR imaging. Am J Roentgenol 1988;150:605-610. Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Question 32High Yield
What root is most commonly involved with a segmental root level palsy after laminoplasty?
Explanation
The postoperative incidence of C5 root palsy after laminoplasty ranges from 5% to 12%. Other roots also may be affected. The palsies tend to be motor dominant, although sensory dysfunction and radicular pain are also possible. The palsy may arise during the immediate postoperative period or up to 20 days later. C5 may be preferentially involved because it is at the apex of the cervical lordosis. Recovery usually occurs over weeks to months. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 235-249.
Question 33High Yield
Which of the following forms of nonsurgical management is considered best for acute low back pain without radiculopathy?
Explanation
Explanation
Temporary bed rest (less than 4 days) with gradual resumption of activities can be efficacious. Epidural steroid injections may be indicated for acute low back pain with radiculopathy. Acupuncture, facet joint injections, or ligamentous (sclerosant) injections are not indicated. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, Appendix A15.
References:
- Helfgott SM: Sensible approach to low back pain. Bull Rheum Dis 2001;3:50.
Question 34High Yield
A 47-year-old man ruptured his left patellar tendon and twisted his right ankle in a fall. Initial radiographs of the ankle are unremarkable. One week following repair of the left patellar tendon, he reports increased pain with weight bearing in his right ankle. A follow-up radiograph is shown in Figure 38. Management of the ankle injury should consist of
Explanation
Explanation
The radiograph reveals disruption of the syndesmosis with lateral displacement of the talus and widening of the medial ankle clear space. No fibular fracture is noted, although radiographs of the entire tibia and fibula are necessary to rule out a more proximal fibula fracture. There is clear instability of the syndesmosis, and surgical stabilization is needed, either by direct repair of the ligaments or more commonly with surgical stabilization of the fibula to the tibia with screws. Functional rehabilitation and early range of motion are indicated with anterior-lateral ankle sprains but not with true instability of the syndesmosis. In anterior syndesmotic injuries in which there are no signs of instability on plain radiographs or with stressing, cast immobilization and protected weight bearing until tenderness subsides is warranted. Long leg cast immobilization is unlikely to be adequate in maintaining reduction of the syndesmosis. Repair of the talofibular ligaments or fibular osteotomy does not address the pathology at the syndesmosis. Chronic syndesmotic disruption is likely to lead to chronic ankle pain and early arthrosis. Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
References:
- Edwards GS Jr, DeLee JC: Ankle diastasis without fracture. Foot Ankle 1984;4:305-312.
Question 35High Yield
Figure 40 shows the MRI scan of a 23-year-old man with a history of recurrent anterior shoulder instability. What is the most likely diagnosis?
Explanation
The MRI scan shows an ALPSA lesion. This is also known as a medialized Bankart with medial displacement of the torn anterior labrum. During surgical stabilization, the labrum and periosteal sleeve must be mobilized and repaired laterally to reduce recurrent instability. A Perthes lesion is a nondisplaced labral tear. A GLAD lesion represents a nondisplaced anterior labral tear with an associated articular cartilage injury. Neviaser TJ: The anterior labroligamentous periosteal sleeve avulsion lesion: A cause of anterior instability of the shoulder. Arthroscopy 1993;9:17-21.
Question 36High Yield
A 72-year-old woman who sustained a cerebrovascular accident 9 months ago now has a fixed elbow flexion contracture of 80 degrees. Management should consist of
Explanation
Explanation
A flexion contracture of the elbow is commonly seen in hemiplegic patients following cerebrovascular accidents. Spasticity and myostatic contracture of the joint are both causative factors. In patients with a flexion deformity of less than 90 degrees, musculocutaneous neurectomy is recommended, followed by serial casting to treat any residual deformity. At 9 months after injury, physical therapy will not significantly improve motion. Nerve blocks may be used in the early stages of recovery to facilitate therapy and serial casting.
References:
- Waters RL, Keenan ME: Surgical treatment of the upper extremity after stroke, in Chapman MW (ed): Operative Orthopedics. Philadelphia, PA, JB Lippincott, 1988, vol 2, pp 1449-1450.
Question 37High Yield
A 2-year-old boy has been referred for musculoskeletal evaluation. Examination reveals shortened proximal limbs, hip and knee flexion contractures, an abducted thumb, and ear abnormalities. His parents are concerned about his deformed feet. What is the most common foot deformity associated with this patient's diagnosis?
Explanation
The patient has diastrophic dysplasia. Affected individuals have rhizomelic short stature, cauliflower ears, severe joint contractures (especially knees and hips), hitchhiker's thumb, and a cleft palate. The most common foot abnormality is a rigid equinovarus deformity. Surgical results are poorer than those for idiopathic clubfeet and often require bony procedures or talectomy. Ryoppy S, Poussa M, Merikanto J, Marttinen E, Kaitila I: Foot deformities in diastrophic dysplasia: An analysis of 102 patients. J Bone Joint Surg Br 1992;74:441-444.
Question 38High Yield
A 26-year-old man has had hand pain and progressive swelling in the knuckle for the past several months. He denies any trauma to the hand. The ring finger metacarpophalangeal joint is tender, and there is loss of motion in the digit. Figure 32a shows the radiograph and Figures 32b through 32d show the T1-weighted, T2-weighted, and gadolinium MRI scans, respectively. What is the most likely diagnosis?
Explanation
Explanation
32b 32c 32d The radiograph reveals a subchondral lesion in the metacarpophalangeal joint that is lytic and expansile. The MRI scans show a mass that is moderate in intensity on the T2-weighted image and has some gadolinium uptake. There are no cystic components in this lesion. The subchondral location and expansile nature are highly suggestive of giant cell tumor of bone. A lesion with this appearance might also represent an aneurysmal bone cyst, given the amount of expansion present. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 113-118.
References:
- Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 39High Yield
A patient has a humeral shaft fracture and is scheduled to undergo open reduction and internal fixation with a plate. What surgical approach will provide the greatest amount of exposure?
Explanation
Explanation
The modified posterior approach with elevation of the medial and lateral heads of the triceps can provide exposure of 94% of the humeral shaft. The traditional posterior triceps-splitting approach exposes 55% of the humeral shaft. DeFranco MJ, Lawton JN: Radial nerve injuries associated with humeral fractures. J Hand Surg Am 2006;31:655-663.
References:
- Gerwin M, Hotchkiss RN, Weiland AJ: Alternative operative exposure of the posterior aspect of the humeral diaphysis with reference to the radial nerve. J Bone Joint Surg Am 1996;78:1690-1695.
Question 40High Yield
A 72-year-old woman who underwent right total hip arthroplasty 7 years ago now reports right hip pain and limb shortening. Studies for infection are negative. AP and lateral radiographs are shown in Figures 13a and 13b. What is the most appropriate management?
Explanation
Explanation
13b Current literature supports the use of reinforcement cages for the reconstruction of failed, loosened acetabular components associated with major bone loss as seen in this patient. Although results of revision using the so-called jumbo cup with screws generally have been good, the amount of bone loss and medial wall penetration shown here and the likelihood of pelvic discontinuity precludes the use of that technique. With either technique, bone grafting of remaining defects is recommended. Sporer SM, O'Rourke M, Paprosky WG: The treatment of pelvic discontinuity during acetablular revision. J Arthroplasty 2005;20:79-84.
References:
- Paprosky WG, O'Rourke M, Sporer SM: The treatment of acetabular bone defects with an associated pelvic discontinuity. Clin Orthop 2005;441:216-220.
Question 41High Yield
A 32-year-old man has a Glasgow Coma Scale score of 8 and an open pelvic fracture. The patient's family reports that he is a Jehovah's Witness. Initial hemodynamic instability has resolved. In the operating room during a washout, the patient's blood pressure becomes unstable. What is the most appropriate action?
Explanation
Certain medical procedures involving blood are specifically prohibited in the belief system of a Jehovah's Witness whereas others are not doctrinally prohibited. For procedures where there is no specific doctrinal prohibition, a Jehovah's Witness should obtain the details from medical personnel and make his or her own decision. Transfusions of allogeneic whole blood or its constituents or preoperative donated autologous blood are prohibited. Other procedures, while not doctrinally prohibited, are not promoted such as hemodilution, intraoperative cell salvage, use of a heart-lung machine, dialysis, epidural blood patch, plasmapheresis, white blood cell scans (labeling or tagging of removed blood returned to the patient), platelet gel, erythropoietin, or blood substitutes. The patient should not be given blood. Plasma expanders should be used first to restore hemodynamic stability. Cell saver blood from an open would is not recommended nor would there likely be enough from an open tibial fracture to salvage. The patient's family may be expressing their own beliefs rather than the patient's beliefs and it would be better to ask the patient when he or she is more alert to determine what procedures they would allow. A consult with the ethics committee will unnecessarily delay an intervention that should restore hemodynamic stability. Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Question 42High Yield
A 3-year-old child has bilateral genu varum and short stature. Radiographs show physeal widening and generalized osteopenia. The femora and tibiae show anterolateral bowing. Laboratory studies show low normal serum calcium values, significantly decreased serum phosphate levels, and normal parathyroid hormone (PTH), alkaline phosphatase, and vitamin-D levels. These findings are consistent with
Explanation
Children with vitamin D-resistant rickets are short in stature and have genu varum, physeal widening, and generalized osteopenia. The abnormality in inherited vitamin D-resistant rickets is the renal tubule's inability to resorb phosphate leading to hypophosphatemia. Laboratory findings in the condition are normal or near normal serum calcium values, significantly decreased serum phosphate levels, elevated alkaline phosphatase levels, and normal PTH and vitamin-D levels. The most common form is inherited as an X-linked dominant trait. Nutritional rickets has a normal or low serum phosphate levels, normal or low serum calcium values, and decreased levels of 25(OH) vitamin D and 1,25-dihydroxyvitamin D. Hypophosphatasia is a rare condition characterized by a deficiency of alkaline phosphatase in the serum and tissues, leading to generalized abnormal mineralization of bone. Primary hyperparathyroidism usually is caused by a parathyroid adenoma, and the child generally has abdominal problems and hypercalcemic crisis. Laboratory findings include elevated serum calcium values, alkaline phosphatase levels, and PTH levels, and decreased serum phosphate levels. Children with renal osteodystrophy tend to have genu valgum, and laboratory findings include elevated serum phosphate, alkaline phosphatase, and PTH levels, and low serum calcium values. Findings of renal disease include elevated BUN and creatinine. Herring JA: Metabolic and endocrine bone diseases, in Herring JA (ed): Tachdjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, pp 1686-1710.
Question 43High Yield
During a posterior cruciate ligament-sacrificing total knee arthroplasty with anterior referencing, 8 mm of distal femur is resected. It is noted that the flexion gap is tight and the extension gap appears stable. What is the next most appropriate step in management?
Explanation
If the flexion gap is tight and the extension gap is correct, it is preferable to change only the flexion gap and leave the extension gap unchanged; therefore, the treatment of choice is to decrease the size of the femoral component. The smaller component will be smaller in both medial-lateral as well as anterior-posterior dimensions. A smaller anterior-posterior size will allow more space for the flexion gap without significantly affecting the extension gap. Decreasing the size of the tibial polyethylene insert thickness or cutting more proximal tibia will affect both the flexion and extension gaps. Cutting more distal femur will increase the extension gap and not change the flexion gap, making the described situation worse. Cutting both the proximal tibia and distal femur will increase both the flexion and extension gaps.
Question 44High Yield
The superior glenohumeral ligament primarily restrains
Explanation
Explanation
Several cutting studies have evaluated the primary static restraints and the role of the glenohumeral ligaments in providing static stability. With the arm at the side in adduction, the superior glenohumeral ligament and coracohumeral ligament are the primary restraints to inferior translation. The middle glenohumeral ligament functions with the arm in 45 degrees of abduction and resists anterior translation. The inferior glenohumeral ligament is the primary restraint to anterior translation at 90 degrees of abduction. Warner JJ, Deng XH, Warren RF, et al: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
References:
- Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy Orthopaedic Surgeons, 1994, pp 165-177.
Question 45High Yield
Following application of a short leg cast, a patient reports a complete foot drop. A compression injury of the peroneal nerve at the fibular neck is confirmed by electrical studies. Which of the following muscles is expected to be the last to recover function during the ensuing months?
Explanation
The recovery process from peroneal nerve palsy may take many months as axonal regrowth occurs. Of the muscles listed, the extensor hallucis is innervated most distally by the peroneal nerve. The flexor digitorum longus is innervated by the tibial nerve.
Question 46High Yield
Figure 13 shows the radiographs of a 20-year-old intercollegiate basketball player who was injured 6 weeks prior to the start of the season. What is the most appropriate treatment?
Explanation
A Jones fracture occurs at the metaphyseal-diaphyseal junction of the fifth metatarsal. It is often an acute fracture in conjunction with a chronic stress-related injury. It requires either a short leg cast with strict non-weight-bearing or surgical fixation. In the high performance athlete, the need for rapid return to sport activity usually requires surgical intervention, most commonly with an intramedullary screw. Brodsky JW, Krause JO: Stress fractures of the foot and ankle, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, Saunders, 2003, vol 2, pp 2391-2409.
Question 47High Yield
Figures 18a through 18c show the clinical photograph, radiograph, and CT scan of a 21-year-old man who reports persistent pain after injuring his right shoulder 4 months ago. What is the most likely factor associated with this patient's diagnosis?
Explanation
Explanation
18b 18c The more severe the trauma, the higher the rate of subsequent clavicular nonunion. Neither duration nor type of immobilization has been clearly demonstrated to be a causative factor in the development of nonunion. Similarly, closed reduction has not been found to alter the healing course in midshaft clavicular fractures. Lazarus MD, Seon C: Fractures of the clavicle, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, vol 2, pp 1241-1242.
References:
- White RR, Anson PS, Kristiansen T, et al: Adult clavicle fractures: Relationship between mechanism of injury and healing. Orthop Trans 1989;13:514-515.
Question 48High Yield
What is the current 5-year survival rate for patients with classic nonmetastatic, high-grade osteosarcoma of the extremity?
Explanation
Multidisciplinary treatment combining systemic chemotherapy and adequate surgical resection has resulted in a 5-year survival rate of 70% in patients with nonmetastatic osteosarcoma of the extremity . The advent of effective chemotherapy has increased the overall survival rate from 20% to 70% in current studies. Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Question 49High Yield
A patient with a cobalt-chromium alloy (Co-Cr) femoral stem has a periprosthetic fracture that is to be fixed with a cable-plate device. The surgeon should make sure that the plate, screws, and cable, respectively, are made of
Explanation
Contact between metals in a biologic environment leads to galvanic corrosion. Reduction potentials of Co-Cr and stainless steel produce the worst combination of metals in commonly used implants. Because the fixation implants are not intended to contact the existing implant, it is not as great a consideration as the plate and the screws and cables that will directly contact each other. Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 119-144.
Question 50High Yield
Figures 45a through 45c show the radiograph, CT scan, and MRI scan of a 15-year-old boy who has lateral ankle pain. What is the most likely diagnosis?
Explanation
Explanation
45b 45c The elongated anterior process of the calcaneus reaching distally toward the navicular is an abnormal finding. Instead of viewing the rounded, blunt distal anterior process of the calcaneus, a bridge extends to the navicular, albeit incomplete. These findings are consistent with a fibrous coalition. CT can reveal a stress fracture of the calcaneus, arthritis of the subtalar joint with subchondral cysts, or an os peroneal bone disruption in the peroneus longus, but those entities are not shown here. The plantar fascia is intact. Richardson EG: Sesamoids and accessory bones of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 702-732.
References:
- Oestreich AE, Mize WA, Crawford AH, et al: The "anteater nose": A direct sign of calcaneonavicular coalition on the lateral radiograph. J Pediatr Orthop 1987;7:709-711.
Question 51High Yield
A 29-year-old man who lifts weights states that he injured his left shoulder while performing a bench press 2 days ago. The following morning he noted ecchymosis and swelling in the left chest wall. Examination reveals ecchymosis and tenderness and deformity in the left anterior chest wall and axillary fold that is accentuated with resisted adduction of the arm. Passive range of motion beyond 90 degrees of forward flexion and 45 degrees of external rotation is extremely painful. Glenohumeral stability is difficult to assess because of severe guarding. Figure 29 shows an MRI scan. Management should consist of
Explanation
Explanation
Rupture of the pectoralis major tendon most commonly occurs during bench pressing. Wolfe and associates have shown that the most inferiorly located fibers of the sternal head lengthen disproportionately during the final 30 degrees of humeral extension during the bench press. This creates a mechanical disadvantage in the final portion of the eccentric phase of the lift; with forceful flexion of the shoulder these maximally stretched fibers may rupture. In most patients, particularly in young athletes, the treatment of choice is anatomic repair of the ruptured tendon to its insertion in the proximal humerus either with suture anchors or transosseous sutures. Following surgery, most patients experience a near normal return of strength and significant improvement in the cosmetic appearance of the deformity. While more technically challenging, repair of chronic rupture is possible and is indicated in some patients. Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
References:
- Schepsis AA, Grafe MW, Jones HP, Lemos MJ: Rupture of the pectoralis major muscle: Outcome after repair of acute and chronic injuries. Am J Sports Med 2000;28:9-15.
Question 52High Yield
Sudden cardiac death in the young athlete is most frequently caused by
Explanation
Hypertrophic cardiomyopathy is the leading cause of sudden cardiac death in athletes, accounting for 40% of reported cases. Most athletes have no previous symptoms, and sudden death may be the first clinical manifestation. The prevalence of hypertrophic cardiomyopathy in the general population is 1 in 500, with a mortality rate of 2% to 4% in young adults. Athletes with active myocarditis should not engage in sports for up to 6 months, and although they may be at risk for the development of chronic cardiomyopathy, it is rarely a cause of sudden cardiac death. Mitral valve prolapse with an accompanying systolic murmur is common in the general population, but infrequently a cause of sudden cardiac death. Weakening of the aortic wall associated with Marfan syndrome can result in abrupt rupture of the aorta. This accounts for 3% of sudden cardiac deaths in young athletes. Marfan syndrome usually can be detected on preparticipation screenings by its skeletal and ocular manifestations. Atherosclerotic coronary artery disease is the most common cause of sudden cardiac death in older athletes, accounting for 75% of reported cases. However, it is much less common in the young competitive athlete. Burke AP, Farb A, Virmani R, Goodin J, Smialek JE: Sports-related and non-sports-related sudden cardiac death in young adults. Am Heart J 1991;121:568-575.
Question 53High Yield
A patient who underwent a high tibial osteotomy (HTO) is now scheduled to undergo total knee arthroplasty (TKA). When compared with a patient undergoing primary TKA without a prior HTO, the patient should be advised to expect a higher incidence of
Explanation
Explanation
Conversion TKA following a previous HTO can be successful; however, it is associated with poorer clinical results when compared with other primary TKAs. There is an increased likelihood of poor range of motion that is partially affected by patella infera created from the osteotomy. Patella infera also results in difficulty with surgical exposure. There has been no reported increase in the rate of infection, fracture, or loosening.
References:
- Mont MA, Alexander N, Krackow KA, Hungerford DS: Total knee arthroplasty after failed high tibial osteotomy. Orthop Clin North Am 1994;25:515-525.
Question 54High Yield
A 25-year-old man sustained a head injury after being ejected from his car. Examination reveals a Glasgow Coma Scale score of 7 and a swollen right knee. Clinical examination shows that the knee is very unstable, suggesting tears of the medial collateral and anterior and posterior cruciate ligaments, as well as the posterior lateral corner. What is the most appropriate first step to rule out a vascular injury?
Explanation
A knee dislocation carries the potential for an arterial injury and has always brought up the question of need for arteriography to rule out this limb-threatening injury. However, arteriography has an inherent complication rate that may compromise the general care of the patient. In over 240 published cases with documented knee dislocations that were evaluated for vascular injury by physical examination (without imaging studies), not a single missed injury was reported, for a 100% negative predictive value (0% false-negative rate). This degree of accuracy at excluding major vascular injury is unsurpassed by the results obtained with arteriography but with no risk involved and a marked savings in time, equipment, and costs. Therefore, the most appropriate first step to rule out vascular injury is examination of the pedal pulses. If there is any doubt about an arterial injury, another option is the ankle-brachial index (ABI). If the ABI is greater than 0.9, the chance of arterial injury is again nonexistent. However, a positive physical examination or an ABI of less than 0.9 is not 100% predictive of an arterial injury; therefore, arteriography is recommended. Miranda FE, Dennis JW, Veldenz HC, et al: Confirmation of the safety and accuracy of physical examination in the evaluation of knee dislocation for injury of the popliteal artery: A prospective study. J Trauma 2002;52:247-252.
Question 55High Yield
A 63-year-old woman has a femoral neck fracture. A biopsy specimen obtained from the fracture site at the time of her hemiarthroplasty reveals metastatic carcinoma. Seven days after surgery, she becomes confused and lethargic. Which of the following laboratory values is most likely implicated in the patient's symptoms at this time?
Explanation
Explanation
Although many hematologic and electrolyte abnormalities may be present in a patient with advanced metastatic cancer, an elevated serum calcium level is most commonly associated with confusion. Treatment with hydration, diuretics, and bisphosphonates is recommended. Clohishy D: Management of skeletal metastasis in clinical orthopaedics, in Craig E (ed): Operative Orthopaedics. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 994-997.
References:
- Mundy GR: Hypercalcemia of malignancy revisited. J Clin Invest 1988;82:1-6.
Question 56High Yield
Which of the following is considered a contraindication to cement injection techniques, such as kyphoplasty or vertebroplasty, in the treatment of osteoporotic compression fractures?
Explanation
Explanation
When retropulsion of the posterior vertebral wall is present, nothing prohibits the cement from following the path of least resistance into the canal or from pushing a bone fragment further into the canal; most clinicians consider it a contraindication to these techniques. Patient age itself is not a contraindication as long as there are no medical contraindications to surgery. An acute fracture in a patient who remains immobile and hospitalized because of pain may be a good indication for such a technique. Prior compression fracture and older compression fractures are not contraindications, but pain relief may be less predictable. Phillips FM, Pfeifer BA, Leiberman IH, et al: Minimally invasive treatment of osteoporotic vertebral compression fractures: Vertebroplasty and kyphoplasty. Instr Course Lect 2003;52:559-567. Truumees E, Hilibrand A, Vaccaro AR: Percutaneous vertebral augmentation. Spine J 2004;4:218-229.
References:
- Rao RD, Singrakhia MD: Painful osteoporotic vertebral fracture: Pathogenesis, evaluation, and roles of vertebroplasty and kyphoplasty in its management. J Bone Joint Surg Am 2003;85:2010-2022.
Question 57High Yield
For patients undergoing a surgical procedure where the risk of requiring a transfusion is less than 10%, the International Committee of Effective Blood Usage suggests
Explanation
Explanation
Recent studies have shown a high rate of waste of autologous blood. Therefore, the Committee does not recommend autologous blood donation for procedures that carry a transfusion risk of 10% or less. Toy P, Beattie C, Gould S, et al: Transfusion alert: Use of autologous blood. National Heart, Lung, and Blood Institute Expert Panel on the use of autologous blood. Transfusion 1992;35:703-711.
References:
- Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 58High Yield
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of
Explanation
The radiograph shows excessive thoracic kyphosis (normal 20 degrees to 50 degrees) with multiple contiguous vertebral wedging and end plate irregularity, all consistent with the diagnosis of Scheuermann's kyphosis. The patient is skeletally immature; therefore, there is the potential for progression of the kyphotic deformity. Extension bracing has shown efficacy in the treatment of Scheuermann's kyphosis that measures 50 degrees to 74 degrees, and has actually reduced the curvature permanently in some patients. A thoracolumbosacral orthosis may be used if the apex of kyphosis is at T7 or lower. Indications for surgical treatment are controversial, but spinal fusion most likely should not be considered for a painless kyphosis measuring less than 75 degrees. Murray PM, Weinstein SL, Spratt KF: The natural history and long-term follow-up of Scheuermann kyphosis. J Bone Joint Surg Am 1993;75:236-248. Wenger DR, Frick SL: Scheuermann kyphosis. Spine 1999;24:2630-2639.
Question 59High Yield
The majority of severe cervical spine injuries occurring in contact sports evolve during axial loading and flexion of the cervical spine. At what minimum degree of flexion does axial loading place the cervical spine at risk during contact sports?
Explanation
Explanation
The paravertebral musculature, the intervertebral disks, and the normal lordotic curvature of the cervical spine can absorb much of the imparted energy of collision. However, when the neck is flexed approximately 30 degrees, the normal lordotic curvature is flattened and the forces applied to the vertex of the head are directed at a straight segmented column. In this situation, the cervical spine is less able to absorb the applied force. With mounting axial load, compressive deformation occurs within the intervertebral disks, causing angular deformation and buckling. The spine will fail in flexion, with resultant fracture, subluxation, or dislocation. A rotatory component added to axial compression can cause concomitant extension, rotation, and shear injury patterns. The National Football Head and Neck Injury Registry has made two recommendations to the NCAA Football Rules Committee to minimize the risk of such injuries: (1) No player should intentionally strike an opponent with the crown or top of the helmet; and (2) No player should deliberately use his helmet to butt or ram an opponent. Thomas BE, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
References:
- Torg JS, Truex R Jr, Quedenfeld TC, Burstein A, Spealman A, Nichols C III: The National Football Head and Neck Injury Registry: Report and conclusions 1978.
- JAMA 1979;241:1477-1479.
Question 60High Yield
Which of the following is considered an advantage of arthroscopic distal clavicle excision compared with open distal clavicle excision?
Explanation
Arthroscopic versus open distal clavicle excision has the advantage of allowing evaluation of the glenohumeral joint arthroscopically prior to moving into the subclavicular and subacromial space to perform the distal clavicle excision. This can be of value in both confirming the diagnosis as well as avoiding diagnostic errors. Berg and Ciullo showed that in 20 patients who underwent open distal clavicle excision that resulted in failure, 15 of those patients had a superior labral anterior posterior (SLAP) lesion. Of these 15 patients who had the lesion treated surgically, 9 went on to a good to excellent result after the surgery was performed arthroscopically. Fewer complications, lower infection rate, and decreased surgical time have not been documented in the literature. Arthroscopic technique sacrifices the inferior acromioclavicular ligament and preserves the superior acromioclavicular ligament. Berg EE, Ciullo JV: The SLAP lesion: A cause of failure after distal clavicle resection. Arthroscopy 1997;13:85-89.
Question 61High Yield
A 68-year-old woman has been progressing slowly after undergoing humeral head replacement for a four-part fracture 3 months ago. She has not regained active elevation, she feels an audible clunk on attempting elevation, and she reports pain and weakness. She used a sling for 2 weeks in the immediate postoperative period. Radiographs are shown in Figure 37a through 37c. Management should consist of
Explanation
Explanation
37b 37c Immediate repair of the tuberosity and rotator cuff is recommended on identifying the avulsion or nonunion. Revising the humeral component to increase tension and length will overtighten the cuff and increase the chance of tuberosity pull-off. The glenoid is uninvolved and should not be replaced. Attempts to strengthen the rotator cuff will be unsuccessful because the insertions are no longer attached to the humerus when the tuberosities avulse. Brown TD, Bigliani LU: Complications with humeral head replacement. Orthop Clin North Am 2000;31:77-90.
References:
- Muldoon MP, Cofield RH: Complications of humeral head replacement for proximal humeral fractures. Instr Course Lect 1997;46:15-24.
Question 62High Yield
A 12-year-old girl who plays softball has chronic lateral hindfoot aching pain that is aggravated by weight-bearing activity. She reports that the pain has recurred after initial improvement with cast immobilization, and it continues to limit her overall level of activity. Radiographs are seen in Figures 40a through 40c. What is the most appropriate surgical treatment?
Explanation
Explanation
40b 40c The patient has a calcaneonavicular tarsal coalition. Symptoms of calcaneonavicular coalitions typically are seen between the ages of 10 and 14 years. The cause of pain has not been clearly established. It has been postulated that the coalition stiffens with maturity and microfractures can result, producing pain. Resection of a calcaneonavicular coalition generally has been associated with a satisfactory result. Soft-tissue interposition, most commonly using the extensor digitorum brevis muscle, appears to be helpful. A hindfoot arthrodesis (usually triple) would be reserved if coalition resection proves to be unsuccessful. Achilles tendon lengthening and orthotic support, as well as debridement of the sinus tarsi, are not expected to result in a satisfactory outcome. The patient does not have a flatfoot deformity. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 757-765.
Question 63High Yield
Talar compression syndrome in ballet dancers typically involves injury to which of the following structures?
Explanation
Explanation
Talar compression syndrome is also known as os trigonum syndrome or posterior ankle impingement syndrome and occurs in activities involving extreme ankle plantar flexion. It involves pinching of the posterior talus (os trigonum or posterior process of the talus) between the calcaneus and tibia. The flexor hallucis longus also may be impinged. The other structures are not commonly injured in this syndrome. Brodsky AE, Khalil MA: Talar compression syndrome. Am J Sports Med 1986;14:472-476. Wredmark T, Carlstedt CA, Bauer H, Saartok T: Os trigonum syndrome: A clinical entity in ballet dancers. Foot Ankle 1991;11:404-406.
References:
- Marotta JJ, Micheli LJ: Os trigonum impingement in dancers. Am J Sports Med 1992;20:533-536.
Question 64High Yield
A 22-year-old cheerleader who fell from the top of a pyramid now reports anterior and posterior pelvic pain. A radiograph and CT scans are shown in Figures 43a through 43c. What is the best treatment for this injury?
Explanation
Symphyseal widening of greater than 2.5 cm and less than 5 cm denotes an AP II injury and a rotationally unstable pelvis. An AP II pelvic ring injury is best treated with anterior open reduction and internal fixation. Nonsurgical management is reserved for AP I injuries. Pelvic binders are used only acutely and should not be used for definitive management. Iliosacral screws usually are not necessary in the acute management of AP II injuries. Matta JM: Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res 1996;329:88-96. Templeman DC, Schmidt AH, Sems AS, et al: Diastasis of the symphysis pubis: Open reduction internal fixation, in Wiss D (ed): Masters Techniques in Orthopaedic Surgery-Fractures, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 639-648.
Question 65High Yield
A 55-year-old man has had a mass in his right thigh for the past 2 months. An MRI scan and biopsy specimens are shown in Figures 55a through 55c. What is the most likely diagnosis?
Explanation
Explanation
55b 55c The histology shows extraskeletal myxoid chondrosarcoma, characterized by abundant blue myxoid matrix with cords and nests of small tumor cells. Treatment consists of wide resection. Despite the name, hyaline cartilage is not a common component of these tumors. Adult rhabdomyosarcoma and malignant fibrous histiocytoma are highly pleomorphic sarcomas often containing multinucleated giant cells. Myxoid liposarcoma contains a prominent capillary network and lipoblasts. Myxoma is less cellular than extraskeletal myxoid chondrosarcoma and does not have a cord-like arrangement of tumor cells.
References:
- Kawaguchi S, Wada T, Nagoya S, Ikeda T, Isu K, Yamashiro K, et al: Extraskeletal myxoid chondrosarcoma. Cancer 2003;97:1285-1292.
Question 66High Yield
A 16-year-old boy has had a painful ingrown nail on his great toe for the past 3 months. When initial management consisting of soaking the foot in Epsom salts and trimming the nail failed to provide relief, his family physician recommended 2 weeks of oral antibiotics. His symptoms persist, and he is now seeking a second opinion. A clinical photograph is shown in Figure 18. Management should now consist of
Explanation
Explanation
The patient has a chronic ingrown nail on his great toe, which is not an uncommon occurrence in teenagers because of improper nail care. There is local infection and a foreign body reaction because of the nail. Continued conservative management with soaks and antibiotics will not improve the clinical situation. In the presence of local chronic infection, nail matrix ablation is contraindicated. Additionally, in the absence of a history of an ingrown nail, a nail matrix ablation is not medically indicated. The appropriate treatment is partial removal of the nail plate. With nail plate removal, the inflammation and local infection will resolve rapidly. Pettine KA, Cofield RH, Johnson KA, Bussey RM: Ingrown toenail: Results of surgical treatment. Foot Ankle 1988;9:130-134.
References:
- Coughlin MJ, Mann RA: Toenail abnormalities, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 2, pp 1033-1070.
Question 67High Yield
A 45-year-old male karate instructor sustained the injury shown in Figures 40a through 40c while practicing karate. The decision to proceed with surgery depends on which of the following factors?


Explanation
The most important criteria in determining the need for surgery following a nondisplaced or minimally displaced tibial plateau fracture is knee stability to varus/valgus stress. Soft-tissue injury noted on MRI may be addressed at a later time following fracture healing. This fracture pattern is amenable to nonsurgical management. Decisions regarding surgical intervention may be made up to 2 weeks after injury.
Question 68High Yield
A 42-year-old man with a history of renal cell carcinoma has progressive weakness in the lower extremities for the past 3 weeks. The patient desires intervention. A sagittal T2-weighted MRI scan is shown in Figure 9a, and a sagittal contrast enhanced T1-weighted MRI scan is shown in Figure 9b. He currently ambulates minimal distances with a walker. His life expectancy is 8 months. Treatment of the spine lesion should consist of

Explanation
The MRI scans show a metastatic lesion in two contiguous vertebral bodies in the lower thoracic spine. Posterior laminectomy is not indicated because this does not adequately decompress the neural elements and will lead to progressive kyphosis. A posterior fusion may prevent progressive kyphosis but will not decompress the spinal cord. Renal cell carcinoma is not radiosensitive; therefore, radiation therapy would not be helpful in relieving neurologic compression. The lesion should be treated by an anterior corpectomy and reconstruction. This will allow for complete decompression as well as reconstruction of the anterior column. Kyphoplasty is not indicated in a lesion with disruption of the posterior cortex and neurologic impairment. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 351-366.
Question 69High Yield
A 73-year-old man stepped off a street curb and felt a crack in his left hip. He is now unable to bear weight. A radiograph is shown in Figure 54a. Biopsy specimens are shown in Figures 54b and 54c. What is the most likely diagnosis?
Explanation
Explanation
54b 54c The biopsy specimens reveal a high-grade spindle cell lesion adjacent to an area of benign cartilage. This is consistent with a dedifferentiated chondrosarcoma. The radiograph shows a pathologic fracture through a lesion characterized by calcification within the left greater trochanter. Distal to the area of calcification, there is a more osteolytic, destructive appearance. Synovial sarcoma has a biphasic appearance histologically with areas of glandular differentiation that stain positive with keratin. Metastatic prostate cancer, although osteoblastic in appearance, would have a glandular histologic appearance. There is no cartilage in these lesions. Classic low-grade chondrosarcoma does not have an area of high-grade pleomorphic spindle cells within the lesion. A periosteal osteosarcoma is a surface-based lesion with a sunburst radiographic pattern. Although there may be cartilage in the lesion histologically, there are also malignant cells producing osteoid. Dedifferentiated chondrosarcoma is an aggressive, high-grade variant of chondrosarcoma. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 269.
References:
- Mercuri M, Picci P, Campanacci L, et al: Dedifferentiated chondrosarcoma. Skeletal Radiol 1995;24:409-416.
Question 70High Yield
Osteoclasts are primarily responsible for bone resorption of malignancy. Which of the following stimulates osteoclast formation?
Explanation
Explanation
Bone destruction is primarily mediated by osteoclastic bone resorption, and cancer cells stimulate the formation and activation of osteoclasts next to metastatic foci. Increasing evidence suggests that receptor activator of NF-kB ligand (RANKL) is the ultimate extracellular mediator that stimulates osteoclast differentiation into mature osteoclasts. In contrast, OPG inhibits osteoclast development. IL-8 but not IL-5 is known to play a role in osteoclastogenesis. MMP-2 and collagen type I do not have a direct role in osteoclastogenesis. Kitazawa S, Kitazawa R: RANK ligand is a prerequisite for cancer-associated osteolytic lesions. J Pathol 2002;198:228-236.
References:
- Einhorn TA: Metabolic bone diseases, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 71High Yield
A 25-year-old man has chronic back pain that has been slowly worsening. He has no constitutional symptoms, and he denies any previous medical problems. Examination shows a tall lean build with no objective neurologic findings or skin lesions. Figure 32 shows a T2-weighted sagittal MRI scan. What is the most likely diagnosis?
Explanation
The MRI scan shows significant dural ectasia, which is seen in more than 60% of patients with Marfan syndrome. It is also relatively common in patients with neurofibromatosis, but this patient has no skin lesions. It has also been described in Ehlers-Danlos syndrome but is less common. Ahn NU, Sponseller PD, Ahn UM, Nallamshetty L, Kuszyk BS, Zinreich SJ: Dural ectasia is associated with back pain in Marfan' syndrome. Spine 2000;25:1562-1568.
Question 72High Yield
Figure 54 shows the preoperative radiograph of a 45-year-old woman who is considering total hip arthroplasty with her orthopaedic surgeon. What femoral characteristic is a typical concern in this patient?
Explanation
Explanation
Developmental dysplasia of the hip (DDH) leads to early arthritis of the hip as seen in this patient. Although DDH is believed to mostly affect the acetabulum, most patients with DDH also have anatomic aberrations of the femur. Using three-dimensional computer models generated by reconstruction of CT scans, dysplastic femurs were shown to have shorter necks and smaller, straighter canals than the controls. The shape of the canal became more abnormal with increasing subluxation. The studies also have shown that the primary deformity of the dysplastic femur is rotational, with an increase in anteversion of 5 degrees to 16 degrees, depending on the degree of subluxation of the hip. The rotational deformity of the dysplastic femur arises within the diaphysis between the lesser trochanter and the isthmus and is not attributable to a torsional deformity of the metaphysis. Osteopenia is not a concern in a patient with an excellent cortical index (thick cortices and narrow canal). Femoral varus or bowing of the femur is not a typical finding in patients with DDH. Noble PC, Kamaric E, Sugano N, et al: Three-dimensional shape of the dysplastic femur: Implications for THR. Clin Orthop 2003;417:27-40.
References:
- Sugano N, Noble PC, Kamaric E, et al: The morphology of the femur in developmental dysplasia of the hip. J Bone Joint Surg Br 1998;80:711-719.
Question 73High Yield
Posterior lumbar spine arthrodesis may be associated with adjacent segment degeneration cephalad or caudad to the fusion segment. Which of the following is the predicted rate of symptomatic degeneration at an adjacent segment warranting either decompression and/or arthrodesis at mid-range follow-up (5-10 years) after lumbar fusion?
Explanation
The rate of symptomatic degeneration at an adjacent segment warranting either decompression or arthrodesis was predicted to be 16.5% at 5 years and 36.1% at 10 years based on a Kaplan-Meier analysis.
Question 74High Yield
Acute redislocation of the glenohumeral joint is a complication that occurs following a first-time dislocation. This is most often seen with
Explanation
Redislocation following acute dislocation occurs in approximately 3% of patients. This redislocation tends to occur in middle-aged and elderly patients. A higher incidence of redislocation occurs when there are accompanying fractures of the glenoid rim and the greater tuberosity. Robinson CM, Kelly M, Wakefield AE: Redislocation of the shoulder during the first six weeks after a primary anterior dislocation: Risk factors and results of treatment. J Bone Joint Surg Am 2002;84:1552-1559.
Question 75High Yield
Which of the following best describes the function of the notochord?
Explanation
Explanation
The notochord is the anatomic structure that defines the phylum Chordata. The notochord plays a fundamental role in the development of the skeleton, and it exists only for a short period of time. During its temporary existence, the notochord serves as a transient axis of support, provides for the initial axis of orientation of the developing embryo, and most importantly, plays a vital role in the induction of the tissues that eventually form the vertebral column.
References:
- Rosenberg A: Embryology of the skull base and vertebral column, in Harsh G (ed): Chordomas and Chondrosarcomas of the Skull Base and Spine. New York, NY, Thieme, 2003, pp 3-8.
Question 76High Yield
A 46-year-old man has incomplete paraplegia after being involved in a motor vehicle accident. The CT scan shown in Figure 5 reveals marked canal compromise. What is the most appropriate management to improve neurologic status?
Explanation
Explanation
According to a study by the Scoliosis Research Society, the use of anterior decompression is most predictable for improving neurologic status. This is particularly true of bowel and bladder functional loss. Laminectomy is contraindicated because it further destabilizes the spine. Posterior instrumentation and indirect reduction through distraction and ligamentotaxis only incompletely decompress the compromised canal and are successful only if performed within 48 hours of injury. While some improvement may occur with closed management, the amount of recovery is less than that achieved with surgical decompression. A posterior approach and instrumentation may be added to the anterior decompression based on the characteristics of associated injuries to the posterior element. Gertzbein SD: Scoliosis Research Society multicenter spine fracture study. Spine 1992;17:528-540. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-215.
References:
- Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Question 77High Yield
A 7-year-old girl sustains the fracture shown in Figure 29a. Casting results in uneventful healing. Ten months later, the patient has a progressive valgus deformity of the right lower extremity. A radiograph is shown in Figure 29b. Management should now consist of
Explanation
Explanation
29b Although fractures of the proximal tibial metaphysis in young children appear innocuous, development of a progressive valgus deformity is possible despite adequate and appropriate treatment. When treating a child with this injury, it is prudent to warn the parents that a valgus deformity of the tibia may develop. The most likely cause is asymmetric growth of the proximal tibial physis. Because spontaneous angular improvement can be expected in most patients, surgery to correct these deformities should be delayed at least 2 to 3 years and should be limited to patients who have symptoms. There are no studies that document the efficacy of bracing for this deformity. Tuten HR, Keeler KA, Gabos PG, et al: Posttraumatic tibia valga in children: A long-term follow-up note. J Bone Joint Surg Am 1999;81:799-810.
References:
- McCarthy JJ, Kim DH, Eilert RE: Posttraumatic genu valgum: Operative versus nonoperative treatment. J Pediatr Orthop 1998;18:518-521.
Question 78High Yield
Six weeks after onset, what is the most clearly accepted indication for surgical management for lumbar disk herniation?
Explanation
Explanation
In the absence of a cauda equina syndrome or progressive weakness, the best indication for surgical management is refractory radicular pain. Surgical decision-making should not be based on the size of the herniation. Large extruded herniations tend to resolve more predictably than smaller herniations. Stable motor weakness and numbness resolve similarly in both surgical and nonsurgical management, although surgery hastens the process. When intractable radicular pain is the strict indication for surgery, surgical intervention provides substantial and more rapid pain relief than nonsurgical care. Rhee JM, Schaufele M, Abdu WA: Radiculopathy and the herniated lumbar disc: Controversies regarding pathophysiology and management. J Bone Joint Surg Am 2006;88:2070-2080.
Question 79High Yield
A study is designed that examines fractures in children with osteogenesis imperfecta after being treated with bisphosphonates compared with a placebo. A difference is found for which the P value is greater than what is considered to be statistically significant. What is the next appropriate statistical analysis?
Explanation
Explanation
When a study yields a negative result between treatment groups, the next step is to perform a power analysis. The power, by definition, is the probability of rejecting the null hypothesis: in this example the null hypothesis would be that children treated with bisphosphonates would have fewer fractures than the untreated control population. The power analysis helps answer the question as to whether the null hypothesis should be rejected and the finding is real, or whether the sample size was too small or the effect of treatment too subtle to demonstrate a difference between the treatment and control groups. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 7.
References:
- Kocher MS, Zurakowski D: Clinical epidemiology and biostatistics: A primer for orthopaedic surgeons. J Bone Joint Surg Am 2004;86:607-620.
Question 80High Yield
The 5-year outcome for patients with sciatica secondary to lumbar disk herniation shows which of the following results?
Explanation
Explanation
Atlas and associates, in the Maine Lumbar Spine Study, reported that overall, patients treated initially with surgery reported better outcomes. By 5 years, 19% of surgical patients had undergone at least one additional lumbar spine operation, and 16% of nonsurgical patients had opted for at least one lumbar spine operation. At the 5-year follow-up, 70% of patients initially treated surgically reported improvement in their predominant symptom (back or leg pain) versus 56% of those initially treated nonsurgically. They also noted that there was no difference in the proportion of patients receiving disability compensation at the 5-year follow-up.
Question 81High Yield
A positive Froment sign indicates weakness of which of the following muscles?
Explanation
Thumb adduction is powered by the adductor pollicis (ulnar nerve). Testing involves having the patient forcibly hold a piece of paper between the thumb and radial side of the index proximal phalanx. When this muscle is weak or nonfunctioning, the thumb interphalangeal joint flexes with this maneuver, resulting in a positive Froment sign. The paper is held by action of the thumb flexion (flexor pollicis longus and flexor pollicis brevis; median innervated).
Question 82High Yield
A 23-year-old man has had right posterolateral knee pain and occasional lateral calf dysesthesias for the past 8 months. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 62a through 62e. What is the most likely diagnosis?
Explanation
Explanation
62b 62c 62d 62e The radiograph shows an eccentric, cortically based lytic lesion in the proximal fibula. The CT and MRI scans confirm that it is well circumscribed and cortically based with significant surrounding edema. The radiographic differential diagnosis would be a Brodie's abscess or osteoid osteoma. An osteoblastoma would have to be greater than 2 cm in size. A chondroblastoma may also have significant edema around it, but it is an epiphyseal-based lesion, not cortically based. The well-circumscribed nature of the lesion is not consistent with osteosarcoma. The pathology shows a very cellular and vascular stroma with plump, but not atypical osteoblast cells making a matrix of immature woven bone. There are no abundant inflammatory cells or dead bone suggestive of osteomyelitis or a Brodie's abscess. Therefore, the clinical and histologic picture is most consistent with an osteoid osteoma. Percutaneous radiofrequency ablation, usually with CT guidance, has become the preferred method for treating most cases of osteoid osteoma. Rosenthal DI: Radiofrequency treatment. Orthop Clin North Am 2006;37:475-484.
References:
- Ghanem I: The management of osteoid osteoma: Updates and controversies. Curr Opin Pediatr 2006;18:36-41.
Question 83High Yield
Figures 52a and 52b show the radiographs of a left proximal femoral lesion noted serendipitously following minor trauma to the left hip. The patient has no thigh pain and is fully active without limitation. What is the most likely diagnosis of this bony lesion?

Explanation
The radiographs reveal a geographic lesion of the proximal femur with the classic "ground glass" appearance noted in fibrous dysplasia. This intramedullary lesion is modestly expansile, demonstrates some minimal cortical thinning, and has no aggressive features. Chondroblastoma, giant cell tumor, and osteoblastoma are more lytic in appearance, and the location is not typical for giant cell tumor or chondroblastoma. While enchondroma may be considered, the uniform ground glass appearance, lack of punctuate mineralization, and distinct margination of the lesion make that diagnosis less likely.
Question 84High Yield
A 15-year-old boy reports a 2-day history of progressive left buttock pain and severe limping. He denies any history of trauma or radiation of the pain. He has an oral temperature of 100.4 degrees F (38 degrees C). Examination reveals that the lumbar spine and left hip have unguarded motion. The abdomen is nontender. There is moderate tenderness of the left sacroiliac region with no palpable swelling. Pain is elicited when the left lower extremity is placed in the figure-4 position (FABER test). Laboratory studies show a peripheral WBC count of 11,500/mm3 (normal to 10,500/mm3) and an erythrocyte sedimentation rate of 38 mm/h (normal up to 20 mm/h). Radiographs of the pelvis, hips, and lumbar spine are normal. A nucleotide bone scan (posterior view) is shown in Figure 44. Initial management should consist of
Explanation
Explanation
The symptoms, physical findings, and laboratory studies are most consistent with a diagnosis of infectious sacroiliitis, usually caused by Staphylococcus aureus. Initial radiographs will be normal, and the diagnosis of sacroiliitis is often delayed. A technetium Tc 99m bone scan will localize the problem in 90% of patients but may occasionally give a false-negative result in early cases. If suspicion is high, a gallium scan or MRI scan may help confirm the diagnosis of sacroiliitis. Needle aspiration of the sacroiliac joint is difficult; therefore, antibiotic selection is usually empiric or based on blood cultures. Sacroiliitis that is the result of connective tissue inflammatory disease is usually bilateral and without fever or leukocytosis. The lack of hip irritability, spinal rigidity, and abdominal tenderness helps to rule out other causes of limping with fever, such as psoas abscess, diskitis, and septic hip. Aprin H, Turen C: Pyogenic sacroiliitis in children. Clin Orthop 1993;287:98-106.
References:
- Osman AA, Govender S: Septic sacroiliitis. Clin Orthop 1995;313:214-219.
Question 85High Yield
Osteoporotic vertebral compression fractures are associated with
Explanation
Osteoporotic vertebral compression fractures are associated with neurologic complications in less than 1% of patients. After the initial fracture however, patients have a 20% risk of further fractures. The mortality rate of patients with vertebral fractures exceeds that of patients with hip fractures when they are followed beyond 6 months. Gass M, Dawson-Hughs B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11. Lindsay R, Silverman SL, Cooper C, et al: Risk of new vertebral fracture in the year following a fracture. JAMA 2001;285:320-323.
Question 86High Yield
A 45-year-old woman has had right wrist pain for the past 2 months. A radiograph, bone scan, and MRI scan are shown in Figures 66a through 66c, and a photomicrograph is shown in Figure 66d. What is the most likely diagnosis?
Explanation
Explanation
66b 66c 66d The radiograph shows a purely radiolucent lesion without matrix mineralization in the epiphysis of the distal radius. The lesion is "hot" on bone scan, and the MRI scan reveals cortical destruction with a soft-tissue mass. These findings are most consistent with giant cell tumor. The distal radius is a common location for giant cell tumors. The other options would be very uncommon in this location in a 45-year-old patient. The photomicrograph demonstrates multinucleated giant cells in a sea of mononuclear cells. The nuclei of the giant cells and the nuclei of the mononuclear stromal cells are identical. This feature helps distinguish giant cell tumor from other lesions that might contain giant cells. Cheng CY, Shih HN, Hsu KY, et al: Treatment of giant cell tumor of the distal radius. Clin Orthop Relat Res 2001;383:221-228.
References:
- Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 263-284.
Question 87High Yield
A 20-year-old woman has lateral foot and ankle pain after sustaining an inversion injury of the ankle while playing soccer 3 months ago. Activity modifications and physical therapy have failed to provide relief. She describes burning pain that extends from the anterior aspect of the ankle to the foot and lateral two toes. The pain is often worse at night. Plain radiographs, a bone scan, and an MRI scan are normal. Stress examination reveals no instability. What is the most likely diagnosis?
Explanation
Explanation
Persistent pain following an ankle sprain can present a diagnostic dilemma. All of the injuries listed should be considered in the differential diagnosis. The superficial peroneal nerve courses in the lateral compartment and exits the crural fascia 12 to 15 cm above the level of the ankle. Muscle herniation through the fascial defect has been reported to be associated with entrapment of this nerve. The fascial hiatus also may serve as a potential tether in cases of inversion injuries causing injury to the superficial peroneal nerve. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
References:
- Baumhauer JF: Superficial peroneal nerve entrapment. Foot Ankle Clin 1998;3:439-446.
Question 88High Yield
Which of the following clinical findings is commonly associated with symptomatic partial-thickness rotator cuff tears?
Explanation
In symptomatic partial-thickness rotator cuff tears, a painful arc with active range of motion is common, impingement signs are usually positive, and the lift-off test is normal. Active and passive range of motion measurements are often equal, although active range of motion can be painful. External rotation lag signs are often seen with larger full-thickness tears. Hertel R, Ballmer FT, Lambert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-313. McConville OR, Iannotti JP: Partial thickness tears of the rotator cuff: Evaluation and management. J Am Acad Orthop Surg 1999;7:32-43. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Question 89High Yield
A 40-year-old woman has a symptomatic mass on the anterior aspect of the ankle. She reports no constitutional symptoms. An MRI scan is shown in Figure 12. What is the most likely diagnosis?
Explanation
Explanation
The MRI scan reveals a lobular mass that is below the vitamin E tablet marker taped to the skin. This is juxtaposed to the tibialis anterior tendon. It is slightly more enhanced than the surrounding subcutaneous fat and is consistent with a ganglion. Osteosarcoma, aneurysmal bone cyst, or unicameral bone cyst all would demonstrate enhancement or pathology in the bone. This is clearly a well-defined soft-tissue mass. Gouty tophi show low to intermediate signal on T1- and T2-weighted images. Kransdorf MJ, Jelinek JS, Moser RP Jr, et al: Soft tissue masses: Diagnosis using MR imaging. Am J Roentgenol 1989;153:541-547. Wetzel LH, Levine E: Soft-tissue tumors of the foot: Value of MR imaging for specific diagnosis. Am J Roentgenol 1990;155:1025-1030.
References:
- Gerster JC, Landry M, Dufresne L, Meuwly JY: Imaging of tophaceous gout: Computed tomography provide specific images compared with magnetic resonance imaging and ultrasonography. Ann Rheum Dis 2002;61:52-54.
Question 90High Yield
A 28-year-old woman fell on her right wrist while rollerblading 2 days ago. She was seen in the emergency department at the time of injury and was told she had a sprain. Examination now reveals dorsal tenderness in the proximal wrist but no snuffbox or ulnar tenderness. Standard wrist radiographs are normal. What is the next most appropriate step in management?
Explanation
Explanation
When considering the diagnosis of scapholunate ligament injury, standard radiographic views of the hand will not always reveal widening of the scapholunate gap. Although MRI may reveal injury to the ligaments, the PA clenched fist view can be obtained in the office during the initial patient visit. Arthroscopy is not a first-line diagnostic tool. Walsh JJ, Berger RA, Cooney WP: Current status of scapholunate interosseous ligament injuries. J Am Acad Orthop Surg 2002;10:32-42.
References:
- Browner BD, Levine AM, Jupiter JB, et al (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1366-1367.
Question 91High Yield
Figure 35 shows the lateral radiograph of a 15-year-old basketball player who felt a dramatic pop in his knee when landing after a lay-up. The patient reports that he cannot bear weight on the injured extremity. Management should consist of
Explanation
Explanation
Tibial tubercle avulsion is an injury of the adolescent knee that most often occurs just before the end of growth. The fracture usually occurs with jumping, either at push-off or landing. This patient has a type III injury. In type III injuries, the articular surface is disrupted, and meniscal injury and compartment syndrome can occur. Open reduction is the treatment of choice, and anterior fasciotomy should be considered prophylactically at the time of surgery. Although the fracture heals with an anterior epiphysiodesis of the proximal tibia, little growth remains in this patient and no special handling of the physis is warranted. Ogden JA, Tross RB, Murphy MJ: Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-215.
References:
- Pape JM, Goulet JA, Hensinger RN: Compartment syndrome complicating tibial tubercle avulsion. Clin Orthop 1993;295:201-204.
Question 92High Yield
The MRI scan shown in Figure 24 reveals a right-sided herniated nucleus pulposus at L4-5 in a patient with pain in the right leg. Administration of a caudal epidural steroid injection provides immediate relief. Over the next week he notes generalized weakness of the lower extremities and has one episode of urinary incontinence. What is the next most appropriate step in management?
Explanation
Whenever a patient's condition changes following a test or a procedure, the physician must determine the cause. A steroid flare reaction will not cause incontinence or weakness of the lower extremities. An L4-5 diskectomy may alleviate the problem if the right-sided L4-5 disk herniation is the etiology of the symptoms. However, it is unlikely that a right-sided disk herniation alone will cause a cauda equina syndrome. Possible etiologies include a further extrusion of a disk fragment at L4-5 that now obliterates the spinal canal, a disk herniation at another level, or an epidural abscess following injection of corticosteroids through a caudal approach. In the presence of a possible infection, myelography should not be performed from a lumbar puncture. The fastest and least invasive way to make an appropriate diagnosis is to obtain an MRI of the lumbar spine. In this patient, the MRI revealed an epidural abscess that was compressing the cauda equina. Because of the large dose of steroids that were injected, the patient did not manifest symptoms such as fevers and chills until late in the course. Knight JW, Cordingley JJ, Palazzo MG: Epidural abscess following epidural steroid and local anaesthetic injection. Anaesthesia 1997;52:576-578.
Question 93High Yield
A 35-year-old female runner reports progressive vague aching pain involving her midfoot. Her pain is most notable when running. She denies specific injury. Examination reveals minimal swelling and localized tenderness over the dorsal medial midfoot and navicular. Radiographs and an MRI scan are shown in Figures 37a through 37c. What is the most appropriate management?


Explanation
A high index of suspicion is required to identify a possible navicular stress fracture, especially in runners. High pain tolerance in the competitive athlete and often minimal swelling contribute to frequent delays in diagnosis. Localized tenderness over the dorsal navicular (so-called "N spot") in a running athlete should alert the treating physician. In this patient, the radiographs are negative and the MRI scan shows marrow edema within the navicular. This could represent a stress reaction, stress fracture, or osteonecrosis. Appropriate management should include non-weight-bearing immobilization and obtaining a CT scan to determine if a fracture is present. Early surgical treatment may be considered but only if a fracture is identified. Lee A, Anderson R: Stress fractures of the tarsal navicular. Foot Ankle Clin 2004;9:85-104.
Question 94High Yield
During the first 2 years of life, which of the following actions is most responsible for increasing structural stability of the physis?
Explanation
Explanation
The zone of Ranvier provides the earliest increase in strength of the physis. During the first year of life, the zone spreads over the adjacent metaphysis to form a fibrous circumferential ring bridging from the epiphysis to the diaphysis. This ring increases the mechanical strength of the physis. The zone also helps the physis grow latitudinally. In turn, the increased width of the physis helps the physis further resist mechanical forces. The change in shape of the physis to its progressively more undulating form is also a factor in increasing physeal strength, but this occurs over a longer period of time, as the child's activity level increases. The undulations of the physis seen in some growth plates also add to stability but to a lesser extent. The other changes contribute little toward increasing physeal strength. Burkus J, Ogden J: Development of the distal femoral epiphysis: A microscopic morphological investigation of the zone of Ranvier. J Pediatr Orthop 1984;4:661-668.
References:
- Shapiro F, Holtrop ME, Glimcher MJ: Organization and cellular biology of the perichondrial ossification groove of Ranvier: A morphological study in rabbits. J Bone Joint Surg Am 1977;59:703-723.
Question 95High Yield
A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement?
Explanation
The patient has end-stage rotator cuff tear arthropathy. The radiograph shows complete proximal humeral migration (acromiohumeral interval of 0 mm), severe glenohumeral arthritis, and acetabularization of the acromion. In addition, she has "pseudoparalysis" with active elevation of only 30 degrees. Reverse shoulder arthroplasty affords her the best opportunity for pain relief and functional improvement. The other procedures have mixed results but typically are better for pain relief than they are for functional gains. Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Question 96High Yield
Compared to similar patients who do not donate autologous blood, patients with normal baseline hemoglobin who donate autologous blood prior to undergoing primary total hip arthroplasty are likely to
Explanation
Explanation
Billote and associates compared patients with normal baseline hemoglobin levels who did and did not donate autologous blood prior to total hip arthroplasty. No patients received allogeneic blood perioperatively, and the autologous donors had significantly lower hemoglobin levels at the time of surgery and in the recovery room. Of the autologous donors, 69% received an autologous transfusion. The authors concluded that autologous donation was unnecessary in patients undergoing primary total hip arthroplasty who had a normal hemoglobin. Billote D, Glisson SN, Green D, Wixson RL: A prospective, randomized study of preoperative autologous donation for hip replacement surgery. J Bone Joint Surg Am 2002;84:1299-1304.
References:
- Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 47-53.
Question 97High Yield
The modified Brostrom lateral ankle ligamentous reconstruction uses which of the following structures to provide supplementary stabilization?
Explanation
Explanation
The modified Brostrom lateral ankle ligament stabilization procedure uses the remnants of the anterior talofibular and the calcaneofibular ligaments, supplemented by the inferior retinaculum and the transferred talocalcaneal ligament to stabilize the lateral ankle. Chrisman and associates described the use of one half of the peroneus brevis. Watson-Jones and Evans used the entire peroneus brevis. The peroneus longus has been taken by mistake. The plantaris has been used in triligamentous reconstruction. Gould N, Seligson D, Gassman J: Early and late repair of lateral ligament of the ankle. Foot Ankle 1980;1:84-89. Hamilton WG, Thompson FM, Snow SW: The modified Brostrom procedure for lateral ankle instability. Foot Ankle 1993;14:1-7. Chrisman OD, Snook GA: Reconstruction of lateral ligament tears of the ankle: An experimental study and clinical evaluation of seven patients treated by a new modification of the Elmslie procedure. J Bone Joint Surg Am 1969;51:904-912. Evans DL: Recurrent instability of the ankle: My method of surgical treatment. Proc R Soc Med 1953;46:343. Watson-Jones R: Fractures and Joint Injuries, ed 3. Baltimore, MD, Williams and Wilkins, 1946, p 234.
References:
- Liu SH, Baker CL: Comparison of lateral ankle ligamentous reconstruction procedures. Am J Sports Med 1994;22:313-317.
Question 98High Yield
Which of following side effects is most commonly seen in a pediatric patient undergoing ketamine anesthesia?
Explanation
Explanation
The most common deleterious side effect of ketamine is increased salivation and tracheobronchial secretions. For this reason, an antisialagogue agent should be given. While lack of sufficient respiratory depression is one of the major advantages of using ketamine, apnea can occur if the drug is given too rapidly intravenously. Emergence phenomena is common in adults but relatively rare in children. Furman JR: Sedation and analgesia in the child with a fracture, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 62-63. White PF, Way WL, Trevor AJ: Ketamine: Its pharmacology and therapeutic uses. Anesthesiology 1982;56:119-136.
References:
- McCarty EC, Mencio GA, Walker LA, Green NE: Ketamine sedation for the reduction of children's fractures in the emergency department. J Bone Joint Surg Am 2000;82:912-918.
Question 99High Yield
What is the most likely cause of the lesion shown in Figures 35a and 35b?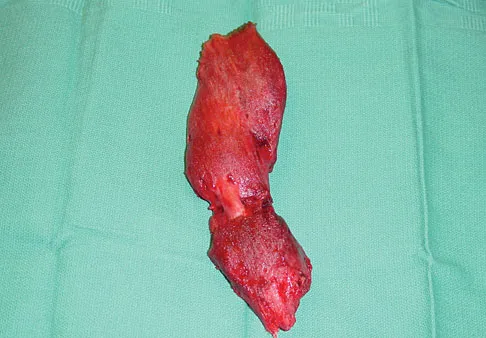

Explanation
The most common cause of myositis ossificans is contusion. Certain regions, including the quadriceps and brachialis, are more commonly affected. The mechanisms of development have not been clearly established. Beiner JM, Jokl P: Muscle contusion injuries: Current treatment options. J Am Acad Orthop Surg 2001;9:227-237.
Question 100High Yield
Which of the following methods is considered effective in decreasing the dislocation rate following a total hip arthroplasty using a posterior approach to the hip?
Explanation
A total hip arthroplasty using the posterior approach has resulted in hip dislocation under certain circumstances. Reconstruction of the external rotator/capsular complex is recognized as a stability-enhancing mechanism for the posterior approach. During the procedure, the acetabular component should be placed in 15 to 20 degrees of anteversion and approximately 45 degrees of abduction. Relative retroversion is a risk factor for posterior dislocation. High abduction angles result in edge loading of the polyethylene and possible early failure, as well as an increased risk of dislocation. Smaller diameter heads and skirted neck extensions used together decrease the range of motion that is allowed before impingement occurs, and this can result in dislocation. Shorter neck lengths generally result in soft-tissue envelope laxity. If laxity occurs, increased offset, neck length, or both can improve stability. Pellicci PM, Bostrom M, Poss R: Posterior approach to total hip replacement using enhanced posterior soft tissue repair. Clin Orthop 1998;355:224-228.
You Might Also Like
Previous ChapterOrthopedic Board Review Set 809: 100 High-Yield MCQs
Next Chapter Orthopedic Board Review: 100 High-Yield MCQs - Set 1065

Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon