Orthopedic Board Review MCQs: Practice Exam Set 563 – 100 Questions
14 Apr 2026
98 min read
127 Views
Key Takeaway
This page offers 100 high-yield orthopedic surgery Multiple Choice Questions (MCQs) for ABOS, OITE, and FRCS board exams. Practice Set #563 helps surgeons test their knowledge, identify weaknesses, and master key concepts to ace their certification exams.
Comprehensive Guide to the Direct Lateral App...
00:00
Start Quiz
Question 1High Yield
Figure 39 shows the AP radiograph of a 62-year-old man with degenerative osteoarthritis secondary to trauma. History reveals that he underwent total elbow arthroplasty 3 years ago. He continues to report instability and constant pain. A complete work-up, including aspiration and cultures, is negative. Treatment should consist of removal of the components and
Explanation
An unconstrained prosthesis dislocation is a disconcerting problem that is not easily resolved; however, revision to a semiconstrained prosthesis would best achieve both pain relief and stability. Removal of the components and distraction arthroplasty or conversion to a resection arthroplasty are options, but the results would be unpredictable with regards to pain relief, postoperative motion, or elbow stability. Arthrodesis is poorly tolerated. With revision to another unconstrained prosthesis, there is the risk of continued redislocation because of chronic ligamentous insufficiency. Linscheid RL: Resurfacing elbow replacement arthroplasty: Rationale, technique and results, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 602-610.
Question 2High Yield
Nutritional rickets is associated with which of the following changes in chemical blood level?
Explanation
Nutritional rickets is associated with decreased dietary intake of Vitamin D, resulting in low levels of Vitamin D that result in decreased intestinal absorption of calcium and low to normal serologic levels of calcium. To boost serum calcium levels, there is a compensatory increase in PTH and bone resorption, leading to increased alkaline phosphatase levels. Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94. Pettifor J: Nutritional and drug-induced rickets and osteomalacia, in Farrus MJ (ed): Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 399-466.
Question 3High Yield
An inverted radial reflex is associated with
Explanation
Explanation
An inverted radial reflex is a hypoactive brachioradialis reflex in combination with involuntary finger flexion. It is a spinal cord "release" sign and is associated with upper motor neuron pathology as seen in cervical stenosis with myelopathy. Radiculopathy is characterized by a diminished reflex but no finger flexion. Peripheral neuropathy is not associated with any reflex change. Parsonage-Turner syndrome is an idiopathic brachial neuritis. Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 762.
References:
- Vaccaro AR, Betz RR, Zeidman SM (eds): Principles and Practice of Spine Surgery. St Louis, MO, Mosby, 2002, p 323.
Question 4High Yield
A 24-year-old baseball pitcher reports pain over the posterior aspect of his shoulder that occurs only during throwing. He notes that the discomfort is greatest during the late cocking and early acceleration phases. Examination reveals localized tenderness with palpation over the external rotators and posterior glenoid. Radiographs are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
Explanation
38b 38c The radiographs show a posterior glenoid osteophyte, often termed a "thrower's exostosis." These exostoses are best visualized on the Stryker notch view and may be missed on other more standard radiographic views of the shoulder. CT and MRI scans may be used, but usually add little information to the radiographic findings. Arthroscopic examination of patients with this condition commonly reveals undersurface tearing of the rotator cuff and posterior labrum. Treatment of this condition remains somewhat controversial, with avocation of both nonsurgical and surgical techniques. Meister K, Andrews JR, Batts J, Wilk K, Baumgarten T, Baumgartner T: Symptomatic thrower's exostosis: Arthroscopic evaluation and treatment. Am J Sports Med 1999;27:133-136. Ferrari JD, Ferrari DA, Coumas J, Pappas AM: Posterior ossification of the shoulder: The Bennett lesion. Etiology, diagnosis, and treatment. Am J Sports Med 1994;22:171-176.
References:
- Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posteriorsuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
Question 5High Yield
What is the most common site of metastases from a soft-tissue sarcoma?
Explanation
The most common site of metastases from a soft-tissue sarcoma is the lungs and occurs in 40% to 60% of patients. The second most common site of metastases in soft-tissue sarcomas is the lymph nodes. Nodal metastases are seen with regularity in synovial sarcoma, epithelioid sarcoma, and rhabdosarcoma. The liver, brain, bone, and muscle are occasional sites of spread, but the occurrence is very rare. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Question 6High Yield
An 86-year-old woman sustained a fracture of the humerus and underwent surgical fixation 8 weeks ago. There was no radial nerve function below the elbow after surgery. Radiographs are shown in Figures 51a and 51b. What is the most appropriate management at this time?
Explanation
Explanation
51b Most radial nerve palsies associated with closed fractures of the humerus resolve spontaneously, including Holstein-Lewis lesions (radial nerve palsy associated with oblique distal third fractures of the humerus). Initial sign of recovery at the brachioradialis may not occur for 4 months. There has been no evidence of deleterious effects occurring during this observation period. There are advocates of early exploration of the nerve. Exploration in the intermediate period between 1 and 4 months is not supported. As overall alignment of the fracture is acceptable, there is no need for hardware exchange until nonunion is clearly identified. Shao YC, Harwood P, Grotz MR, et al: Radial nerve palsy associated with fractures of the shaft of the humerus: A systematic review. J Bone Joint Surg Br 2005;87:1647-1652.
Question 7High Yield
A 37-year-old laborer falls 12 feet and sustains a comminuted tibial plafond fracture. Three years after treatment using standard techniques, what will be the most likely outcome?
Explanation
Two recent studies by Pollak and associates and Marsh and associates have focused on function after high-energy tibial plafond fractures. Findings are unfavorable even when anatomic reduction is performed in the best centers and patients are provided excellent rehabilitation. Function improves up to 2 years after injury, but even basic walking skills remain adversely affected. Virtually all patients have long-term adverse general health effects compared to their gender and age-matched peers. Posttraumatic degenerative arthritis is present in most ankles. Patients should be told early about the long-term prognosis, and early vocational/psychological counseling should be given. Despite these adverse outcomes, only a minority of patients require fusion or arthroplasty. Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Question 8High Yield
A 30-year-old patient has had severe left hip pain and difficulty ambulating, necessitating the use of a cane, for the past 6 months. A photomicrograph of the femoral head sectioned at the time of surgery is shown in Figure 31. What is the most likely diagnosis?
Explanation
The photomicrograph demonstrates a wedge-shaped infarct with femoral head collapse; therefore, the diagnosis is osteonecrosis of the femoral head. Perthes disease and osteoarthritis do not involve a wedge-shaped defect. Tuberculosis of the hip joint results in greater destruction of the articular cartilage. Basset LW, Mirra JM, Cracchiolo A III: Ischemic necrosis of the femoral head: Correlation between magnetic resonance imaging and histologic sections. Clin Orthop 1987;223:181-187.
Question 9High Yield
An extended head hemiarthroplasty (rotator cuff tear arthropathy head) has what theoretic advantage when compared to a standard hemiarthroplasty?
Explanation
Explanation
The theoretic advantage of a metal-to-bone articulation with the acromion is that there is a greater arc in which a smooth metal surface contacts the glenoid and acromion. This may improve pain and function, but no studies have evaluated this to date. One study showed results comparable to that of a standard hemiarthroplasty. There are no other biomechanic advantages. Visotsky JL, Basamania C, Seebauer L, et al: Cuff tear arthropathy: Pathogenesis, classification, and algorithm for treatment. J Bone Joint Surg Am 2004;86:35-40.
References:
- Zuckerman JD, Scott AJ, Gallagher MA: Hemiarthroplasty for cuff tear arthropathy. J Shoulder Elbow Surg 2000;9:169-172.
Question 10High Yield
A 60-year-old woman reports a painful hip arthroplasty after undergoing surgery 18 months ago. Radiographs show stable cementless implants without signs of ingrowth. Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h. Management should now consist of
Explanation
Explanation
Significant elevation of the erythrocyte sedimentation rate in a patient with a painful hip arthroplasty mandates a complete work-up for infection prior to considering revision surgery. Reproducibility and reliability of ultrasonography as a diagnostic test still needs clarification. Aspiration is the easiest and most cost-effective test and should be performed prior to nuclear imaging. The latter is most valuable if the results are negative, strongly predicting the absence of infection. Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
References:
- McAuley JP, Moreau G: Sepsis: Etiology, prophylaxis, and diagnosis, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 1295-1306.
Question 11High Yield
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should
Explanation
The risk of intraoperative fracture in osteopenic rheumatoid bone is significant. Fractures may occur with dislocation of the head and canal reaming, especially while extending and externally rotating the shoulder. If the fracture occurs at the distal tip of the prosthesis, the use of a long-stemmed prosthesis to bypass the fracture site and supplementation with wire cables has been reported with good results. Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346. Boyd AD Jr, Thornhill TS, Barnes CL: Fractures adjacent to humeral protheses. J Bone Joint Surg Am 1992;74:1498-1504.
Question 12High Yield
Figures 9a and 9b show the radiographs of a 75-year-old man who underwent a revision total knee arthroplasty with a long-stemmed tibial component. In rehabilitation, he reports fullness and tenderness in the proximal medial leg (at the knee). The strategy that would best limit this postoperative problem is use of
Explanation
Explanation
9b The problem with this reconstruction is the medial protrusion of the base plate. The use of a base plate with an offset stem can prevent the protrusion and thus the impingement and pain. Allograft bone or smoothing the outline with cement would be just as prominent and likely to cause pain. An ingrowth surface may improve soft-tissue attachment but would still leave the implant protruding medially and likely to cause pain. A nonstemmed tibial base plate would lead to less medial protrusion but at the expense of a smaller area for load carriage on the proximal tibia.
References:
- Gustke K: Cemented tibial stems are not requisite in revision. Orthopedics 2004;27:991-992.
Question 13High Yield
A 59-year-old woman underwent open reduction and internal fixation (ORIF) of her ankle 6 months ago, with subsequent hardware removal 3 months later. She now reports persistent, diffuse ankle pain, swelling, and limited range of motion. Figure 48 shows an oblique radiograph of the ankle. What is the next most appropriate step in management?
Explanation
Explanation
The radiographs demonstrate persistent widening of the medial clear space with an ossicle. This represents soft-tissue interposition-scar tissue, the deltoid ligament, or the posterior tibialis tendon. Physical therapy will not improve the symptomatic malalignment. Hardware removal would be indicated for pain localized to the lateral fibula. Repeat syndesmotic screw fixation alone will not reduce the malalignment. Deltoid ligament repair may be necessary but will need to be combined with debridement of the medial ankle and syndesmosis, as well as repeat placement of one or more syndesmotic screws to maintain the reduction. Weening B, Bhandari M: Predictors of functional outcome following transsyndesmotic screw fixation of ankle fractures. J Orthop Trauma 2005;19:102-108.
Question 14High Yield
A 38-year-old left hand-dominant bodybuilder reports ecchymosis in the left axilla and anterior brachium after sustaining an injury while bench pressing 3 weeks ago. Coronal and axial MRI scans are shown in Figures 16a and 16b. What treatment method yields the best long-term results?
Explanation
Explanation
16b The MRI scans show a rupture of the sternocostal portion of the pectoralis major tendon. This is the most common site of rupture and bench pressing is the most common etiology. Surgical repair yields better functional outcomes and patient satisfaction for tears not only at the tendon/bone interface but also at the myotendinous junction. Bak K, Cameron EA, Henderson IJ: Rupture of the pectoralis major: A meta-analysis of 112 cases. Knee Surg Sports Traumatol Arthrosc 2000;8:113-119.
References:
- Hanna CM, Glenny AB, Stanley SN, et al: Pectoralis major tears: Comparison of surgical and conservative treatment. Br J Sports Med 2001;35:202-206.
Question 15High Yield
A 21-year-old football player had severe pain and immediate swelling in the left anteromedial chest wall while bench pressing near maximal weights several days ago. Examination at the time of injury revealed a mass on the anteromedial chest wall. Follow-up examination now reveals decreased swelling, and axillary webbing is observed. The patient has weakness to adduction and forward flexion. The injured muscle originates from the
Explanation
The patient has a pectoralis major rupture, an injury that occurs most commonly during weight lifting. Grade III injuries represent complete tears of either the musculotendinous junction or an avulsion of the tendon from the humerus, the most common injury site. Examination will most likely reveal ecchymoses and swelling in the proximal arm and axilla, and strength testing will show weakness with internal rotation and in adduction and forward flexion. Axillary webbing, caused by a more defined inferior margin of the anterior deltoid as the result of rupture of the pectoralis, can be seen as the swelling diminishes. Surgical repair is the treatment of choice for complete ruptures. Nonsurgical treatment is associated with significant losses in adduction, flexion, internal rotation, strength, and peak torque. The pectoralis major originates from the proximal clavicle and the border of the sternum, including ribs two through six. The pectoralis major inserts (rather than originates) on the humerus. The coracoid process is the insertion site for the pectoralis minor, as well as the origin for the conjoined tendon. The pectoralis major has no attachment or origin from the scapula. The anterior deltoid originates from the lateral one third of the clavicle and the anterior acromion. Miller MD, Johnson DL, Fu FH, Thaete FL, Blanc RO: Rupture of the pectoralis major muscle in a collegiate football player: Use of magnetic resonance imaging in early diagnosis. Am J Sports Med 1993;21:475-477.
Question 16High Yield
A 14-year-old football player has had right knee pain for the past 2 months; however, he denies any history of trauma. Examination shows an abductor lurch and increased external rotation of the right lower extremity. The best course of action should be to
Explanation
Explanation
Slipped capital femoral epiphysis is the most common pathology involving the hip in adolescents. While patients with acute slips may report severe pain and are unable to ambulate, those with chronic slips often have pain during ambulation, a limp, and increased external rotation of the hip. While 60% of the patients specifically report hip pain, the remainder have pain in the thigh or knee. The initial diagnostic study of choice is AP and frog-lateral radiographs of the pelvis; bilateral involvement is frequently seen. Boyer DW, Mickelson MR, Ponseti IV: Slipped capital femoral epiphysis: Long-term follow-up study of one hundred and twenty-one patients. J Bone Joint Surg Am 1981;63:85-95.
References:
- Stasikelis PJ, Sullivan CM, Philips WA, Polard JA: Slipped capital femoral epiphysis: Prediction of contralateral involvement. J Bone Joint Surg Am 1996;78:1149-1155.
Question 17High Yield
Figure 8 shows the CT scan of an 11-year-old boy who has had a 1-year history of worsening painful flatfeet. He reports pain associated with physical education at school, especially with running and jumping. Management consisting of activity restriction, anti-inflammatory drugs, and casting has failed to provide relief. Treatment should now consist of
Explanation
In most patients with symptomatic talocalcaneal coalition involving less than 50% of the subtalar joint, resection with fat graft interposition is preferred over a subtalar or triple arthrodesis, especially if reasonable range of motion can be achieved. This patient has a synchondrosis that is partially cartilaginous. Although patients may have a residual gait abnormality, most report pain relief after surgery. Scranton PE Jr: Treatment of symptomatic talocalcaneal coalition. J Bone Joint Surg Am 1987;69:533-539. Kitaoka HB, Wikenheiser MA, Schaughnessy WJ, et al: Gait abnormalities following resection of talocalcaneal coalition. J Bone Joint Surg Am 1997;79:369-374.
Question 18High Yield
In addition to pain, which of the following factors are considered most predictive of the risk of pathologic fracture?
Explanation
While guidelines for predicting fracture risk are at best imprecise, the scoring system by Mirels (pain, anatomic location, and pattern of bony destruction) has been shown to be most predictive of fracture risk. Functional pain, peritrochanteric location, and lytic bone destruction are the greatest risk factors for pathologic fracture. The factors of patient weight, age, soft-tissue mass, and location within bone are all of lesser importance. Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Question 19High Yield
Which of the following best describes the relationship of the median nerve to the flexor carpi radialis tendon just proximal to the carpal canal?
Explanation
Explanation
The median nerve has an intimate association with the palmaris longus and the flexor carpi radialis at the proximal aspect of the carpal canal. The median nerve lies just ulnar and dorsal to the flexor carpi radialis tendon. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
References:
- Henry A: Extensile Exposure, ed 3. Edinburgh, UK, Churchill Livingstone, 1995, pp 100-107.
Question 20High Yield
Figure 9 shows the AP radiograph of a 65-year-old man who has knee pain and swelling. What is the most likely diagnosis?
Explanation
Although all the choices are known causes of joint degeneration (secondary osteoarthritis), only chondrocalcinosis shows distinct linear calcification of the cartilage due to deposition of calcium pyrophosphate crystals. Gout is a recurrent acute arthritis resulting from the deposition of monosodium urate from supersaturated hyperuricemic body fluids. Hemochromotosis is characterized by focal or generalized deposition of iron within body tissues. Arthritis may be present but is less common than other manifestations such as liver cirrhosis, skin pigmentation, diabetes mellitus, and cardiac disease. Rheumatoid arthritis is a nonspecific, usually symmetric inflammation of peripheral joints resulting in destruction of articular and periarticular structures. Ochronosis is a hereditary enzyme deficiency (homogentisic acid oxidase) resulting in deposition of homogentisic acid polymers in articular cartilage. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 188.
Question 21High Yield
A 43-year-old woman has had pain in the left hip for the past 2 months. A radiograph, CT scan, MRI scan, and biopsy specimens are shown in Figures 16a through 16e. What is the most likely diagnosis?
Explanation
Explanation
16b 16c 16d 16e The imaging studies are consistent with a chondrosarcoma. The radiograph shows a radiolucent lesion in the pelvis, and there are stippled calcifications on the CT scan. The histology shows a low-grade cellular hyaline cartilage neoplasm with stellate, occasionally binucleated chondrocytes. Enchondroma has a more benign histologic appearance.
References:
- Mirra JM, Gold R, Downs J, Eckardt JJ: A new histologic approach to the differentiation of enchondroma and chondrosarcoma of the bones: A clinicopathologic analysis of 51 cases. Clin Orthop 1985;201:214-237.
Question 22High Yield
Which of the following best describes the most common anatomic variation seen in the glenoid labrum and the middle glenohumeral ligament in the anterosuperior quadrant of the shoulder??
Explanation
Explanation
Wide variations in the anatomy of the anterosuperior portion of the labrum and the middle glenohumeral ligament have been reported and are more common than previously thought. The labrum attached to the glenoid rim and a flat/broad middle glenohumeral ligament is the most common "normal" variation. A cord-like middle glenohumeral ligament is often associated with the presence of a sublabral hole. An anterosuperior labrum confluent with a cord-like middle glenohumeral ligament and no labral attachment to bone is the configuration of the Buford complex. The prevalence of each variation from one recent study is as follows: #1: 86.6%; #2: 3.3%; #3: 8.6%; and #4: 1.5%. Rao AG, Kim TK, Chronopoulos E, et al: Anatomical variants in the anterosuperior aspect of the glenoid labrum. J Bone Joint Surg Am 2003;85:653-659. Ilahi OA, Labbe MR, Cosculluela P: Variants of the anterosuperior glenoid labrum and associated pathology. Arthroscopy 2002;18:882-886.
References:
- Williams MM, Snyder SJ, Buford D: The Buford complex-The "cord-like" middle glenohumeral ligament and absent anterosuprior labrum complex: A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 23High Yield
When using a two-incision approach for open reduction and internal fixation of a Hawkins III talar fracture-dislocation involving the talar neck and body, what anatomic structure must be preserved to optimize outcome?
Explanation
Explanation
A Hawkins III fracture-dislocation generally presents with posteromedial displacement with the deltoid ligament intact. Therefore, the only remaining blood supply is the deltoid branch of the artery of the tarsal canal originating from the posterior tibial artery. Often, the medial malleolus is fractured, assisting in reduction and visualization of fracture reduction. If the medial malleolus is intact, a medial malleolus osteotomy allows visualization of the reduction without compromising the last remaining blood supply to the talus. Mulfinger GL, Trueta J: The blood supply of the talus. J Bone Joint Surg Br 1970;52:160-167.
References:
- Vallier HA, Nork SE, Barei DP, et al: Talar neck fractures: Results and outcomes. J Bone Joint Surg Am 2004;86:1616-1624.
Question 24High Yield
A 35-year-old man who is an avid weight lifter competing in local tournaments reports new onset pain and loss of motion in his dominant right shoulder. Examination reveals joint line tenderness, active elevation to 100 degrees, and external rotation to 10 degrees. His contralateral shoulder reveals 170 degrees forward elevation and 50 degrees external rotation. Radiographs are shown in Figures 46a and 46b. What is the next most appropriate step in management?
Explanation
Explanation
46b New onset pain and stiffness in the young arthritic shoulder is a difficult problem to treat. Initial management should be aimed at reducing pain and improving motion in all planes. This patient's activities and age preclude a shoulder arthroplasty at this time. If nonsurgical management fails to provide relief, then arthroscopic debridement and capsular release may be beneficial. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 257-266.
References:
- Skedros JG, O'Rourke PJ, Zimmerman JM, et al: Alternatives to replacement arthroplasty for glenohumeral arthritis, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 485-499.
Question 25High Yield
What is the most common diagnosis in a patient older than age 40 years with a destructive bony lesion?
Explanation
The most common destructive lesions in a patient older than age 40 years are, in decreasing incidence, metastatic carcinoma, multiple myeloma, lymphoma, and chondrosarcoma. Osteosarcoma is found primarily in younger patients.
Question 26High Yield
A 40-year-old man has intractable pain following 2 years of nonsurgical management for high-grade spondylolisthesis. What is the best surgical option?
Explanation
Circumferential fusion is the preferred choice for patients undergoing revision surgery following failed posterolateral fusions for isthmic spondylolisthesis as well as for those patients having primary surgery for high-grade isthmic spondylolisthesis.
Question 27High Yield
The need for postoperative allogeneic blood transfusions after total hip arthroplasty has been shown to be reduced when using
Explanation
In a prospective study, 216 patients were randomized into three groups consisting of low-dose preoperative erythropoietin, high-dose preoperative erythropoietin, and placebo control. All patients were treated for 4 weeks prior to total hip arthroplasty. Both the low- and high-dose erythropoietin groups had a significantly lower rate of blood transfusions (p < 0.001) after surgery. Waddell JP: Evidence-based orthopedics. J Bone Joint Surg Am 2001;83:788.
Question 28High Yield
A 63-year-old woman has a femoral neck fracture. A biopsy specimen obtained from the fracture site at the time of her hemiarthroplasty reveals metastatic carcinoma. Seven days after surgery, she becomes confused and lethargic. Which of the following laboratory values is most likely implicated in the patient's symptoms at this time?
Explanation
Explanation
Although many hematologic and electrolyte abnormalities may be present in a patient with advanced metastatic cancer, an elevated serum calcium level is most commonly associated with confusion. Treatment with hydration, diuretics, and bisphosphonates is recommended. Clohishy D: Management of skeletal metastasis in clinical orthopaedics, in Craig E (ed): Operative Orthopaedics. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 994-997.
References:
- Mundy GR: Hypercalcemia of malignancy revisited. J Clin Invest 1988;82:1-6.
Question 29High Yield
Figure 14 shows a lateral radiograph of a knee joint. The bony structure indicated by the arrow is a sesamoid bone that resides in what tendon?
Explanation
Explanation
The radiograph shows a fabella, a sesamoid bone that is usually found within the tendon of the lateral head of the gastrocnemius. It can be confused with a loose body on radiographs. It occurs in 18% of patients and is often bilateral. Anderson JE (ed): Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Williams & Wilkins, 1978, pp 4-69.
References:
- Weissman BNW, Sledge CB (ed): Orthopaedic Radiology. Philadelphia, PA, WB Saunders, 1986, p 514.
Question 30High Yield
What is the primary mechanism of injury for the fracture shown in Figures 33a and 33b?

Explanation
The radiographs show a triplane fracture of the ankle. In adolescence, closure of the distal tibial physis starts peripherally at the anteromedial aspect of the medial malleolus and extends posteriorly and laterally. The anterolateral quadrant of the physis is the last to close, making this region the most susceptible to separation. When the foot is twisted into external rotation, the anterolateral portion of the epiphysis is avulsed by the pull of the anterior tibiofibular ligament. When this fragment alone is avulsed, the result is a juvenile Tillaux fracture. When the fracture extends to involve the remainder of the physis and posterior metaphysis, as in this patient, the result is a triplane fracture. Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 267-272. Dias LS, Giegerich CR: Fractures of the distal tibial epiphysis in adolescence. J Bone Joint Surg Am 1983;65:438-444.
Question 31High Yield
A 40-year-old woman with no history of back problems has a symptomatic L4-5 disk herniation with an L5 radiculopathy that has failed to respond to 12 weeks of nonsurgical management. In the preoperative discussion, the surgeon advises the patient that the chance of recurrence of the herniation after successful diskectomy is what percent?
Explanation
The incidence of recurrent disk herniation after a successful diskectomy is approximately 5% to 10%. Indications for surgical diskectomy for a recurrence are the same as for a primary diskectomy. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 685-698.
Question 32High Yield
At the time of the revision surgery shown in Figure 14, the acetabular component was found to be stable. Polyethylene exchange with a standard ultra-high molecular weight polyethylene liner and grafting was performed. The patient is at significantly increased risk for
Explanation
Explanation
Maloney and associates reported a 35% increased risk of pelvic osteolysis after total hip arthroplasty with a porous-coated acetabular component without cement. All components were stable at the time of revision. Only liners were exchanged and debridement of the granuloma with or without bone graft was performed. No defects progressed and one third of the lesions were no longer visible on radiographs, regardless of bone grafting. Unfortunately, despite the technical ease of many of these types of revisions, the dislocation rate for these cases is significant. Precautions should be taken postoperatively, and patients should be educated about this risk preoperatively. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 411-424. Boucher HR, Lynch C, Young AM, et al: Dislocation after polyethylene liner exchange in total hip arthroplasty. J Arthroplasty 2003;18:654-657.
References:
- Maloney WJ, Herzwurm P, Paprosky W, et al: Treatment of pelvic osteolysis associated with a stable acetabular component inserted without cement as part of a total hip replacement. J Bone Joint Surg Am 1997;79:1628-1634.
Question 33High Yield
A 40-year-old woman has a symptomatic mass on the anterior aspect of the ankle. She reports no constitutional symptoms. An MRI scan is shown in Figure 12. What is the most likely diagnosis?
Explanation
Explanation
The MRI scan reveals a lobular mass that is below the vitamin E tablet marker taped to the skin. This is juxtaposed to the tibialis anterior tendon. It is slightly more enhanced than the surrounding subcutaneous fat and is consistent with a ganglion. Osteosarcoma, aneurysmal bone cyst, or unicameral bone cyst all would demonstrate enhancement or pathology in the bone. This is clearly a well-defined soft-tissue mass. Gouty tophi show low to intermediate signal on T1- and T2-weighted images. Kransdorf MJ, Jelinek JS, Moser RP Jr, et al: Soft tissue masses: Diagnosis using MR imaging. Am J Roentgenol 1989;153:541-547. Wetzel LH, Levine E: Soft-tissue tumors of the foot: Value of MR imaging for specific diagnosis. Am J Roentgenol 1990;155:1025-1030.
References:
- Gerster JC, Landry M, Dufresne L, Meuwly JY: Imaging of tophaceous gout: Computed tomography provide specific images compared with magnetic resonance imaging and ultrasonography. Ann Rheum Dis 2002;61:52-54.
Question 34High Yield
A patient undergoes excision of a 3- x 3-cm soft-tissue sarcoma. The final histology results show tumor at the surgical margin. The surgical procedure performed is classified as
Explanation
Explanation
Surgical margins are classified according to the plane of dissection in relation to the tumor. An intralesional procedure is where the plane of dissection passes through the tumor. A marginal resection involves a resection where the plane of dissection is through the reactive zone of the tumor. A wide resection is through completely normal tissue outside of the reactive zone. A radical resection removes all of the muscles and/or bone of the compartment that are involved by the tumor.
References:
- Enneking WF, Spanier SS, Goodman MA: A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop 1980;153:106-120.
Question 35High Yield
For patients undergoing a surgical procedure where the risk of requiring a transfusion is less than 10%, the International Committee of Effective Blood Usage suggests
Explanation
Explanation
Recent studies have shown a high rate of waste of autologous blood. Therefore, the Committee does not recommend autologous blood donation for procedures that carry a transfusion risk of 10% or less. Toy P, Beattie C, Gould S, et al: Transfusion alert: Use of autologous blood. National Heart, Lung, and Blood Institute Expert Panel on the use of autologous blood. Transfusion 1992;35:703-711.
References:
- Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 36High Yield
A professional baseball player has had intermittent, mild shoulder pain for the past 2 years. Nonsurgical management has consisted of anti-inflammatory drugs. Examination reveals atrophy of the infraspinatus muscle but not the supraspinatus. There is weakness in external rotation with the arm at his side but not at 90 degrees of abduction. He has no weakness or pain with resisted abduction. Electromyography confirms an isolated lesion of the suprascapular nerve branch to the infraspinatus. He is otherwise neurologically intact. An MRI scan of the shoulder shows no cysts but confirms atrophy of the infraspinatus muscle. What is the next most appropriate step in management?
Explanation
Explanation
Suprascapular nerve injuries are more commonly seen in athletes who participate in overhead activities. When a patient is evaluated for posterior shoulder pain and infraspinatus muscle weakness or atrophy, electrodiagnostic studies are an essential part of the evaluation. In addition, imaging studies are indicated to exclude other diagnoses that can mimic a suprascapular nerve injury. Initial management should consist of cessation of the aggravating activity along with an organized shoulder rehabilitation program. If nonsurgical management fails to provide relief within 6 months to 1 year, surgical exploration of the suprascapular nerve should be considered. Release of the spinoglenoid ligament with resultant suprascapular nerve decompression may result in pain relief and a return of normal shoulder function. In this patient, who has a chronic neuropathy and mild symptoms, surgery is indicated only if nonsurgical management fails to provide relief and he is unable to perform at his position. Cummins CA, Bowen M, Anderson K, et al: Suprascapular nerve entrapment at the spinoglenoid notch in a professional baseball pitcher. Am J Sports Med 1999;27:810-812. Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
References:
- Ferretti A, De Carli A, Fontana M: Injury of the suprascapular nerve at the spinoglenoid notch: The natural history of infraspinatus atrophy in volleyball players. Am J Sports Med 1998;26:759-763.
Question 37High Yield
A 68-year-old man embarks on a 24-week strength training program. He trains at 80% of his single repetition maximum for both the upper and lower extremities. Which of the following changes can be anticipated?
Explanation
Consistent, long-term exercise training in older athletes has proven very beneficial in reversing both endurance and strength losses that traditionally have been seen with aging. This patient's program will lead to a significant increase in the strength, cross-sectional area, and capillary density of the trained muscles. No major changes in aerobic capacity are anticipated. Strength improvements of up to 5% per day, similar to those for younger athletes, have been identified in this population in one study. Kirkendall DT, Garrett WE Jr: The effects of aging and training on skeletal muscle. Am J Sports Med 1998;26:598-602.
Question 38High Yield
A 23-year-old soccer player sustains a grade III complete posterior cruciate ligament (PCL) tear after colliding with another player. In reconstructing the PCL, it is optimal to reconstruct the
Explanation
The PCL is a nonisometric structure with nonuniform tension during knee motion, with maximum tension at 90 degrees of flexion. While the posteromedial PCL fibers have been found to be the most isometric, the anterolateral fibers represent the bulk of the ligament. Studies have suggested that anterior placement of the femoral tunnel is superior to placement in an isometric position. The anterolateral bundle tightens as the knee flexes; therefore, it is optimal to tension the graft at 90 degrees of flexion. Harner CD, Xerogeanes JW, Livesay GA, et al: The human posterior cruciate ligament complex: An interdisciplinary study. Ligament morphology and biomechanical evaluation. Am J Sports Med 1995;23:736-745.
Question 39High Yield
An 8-year-old boy sustains nondisplaced midshaft fractures of the tibia and fibula after being struck by a car while he was riding his bicycle. No other injuries are noted, but the patient reports pain with passive motion of his toes. His neurovascular examination is otherwise normal. What is the best course of action?
Explanation
Pain with passive motion of the toes is a recognized early sign of increased compartment pressures. At a minimum, a baseline evaluation of the leg compartment pressures should be obtained. While it is normal for the patient to have pain related to the associated muscle contusions, any significant concerns should be addressed immediately in light of the severe consequences likely when a compartment syndrome occurs. Mubarak SJ, Owen CA, Hargens AR, et al: Acute compartment syndromes: Diagnosis and treatment with the aid of the wick catheter. J Bone Joint Surg Am 1978;60:1091-1095.
Question 40High Yield
A Trendelenburg gait is most likely to be seen in association with
Explanation
A Trendelenburg gait results from weakness of the gluteus medius, which is innervated by the L5 nerve root. A paracentral disk herniation at L4-L5 most commonly results in an L5 radiculopathy and thus weakness of the gluteus medius. A paracentral herniation at L5-S1 most commonly affects the S1 nerve root. A paracentral herniation at L3-L4, a central herniation at L3-L4, and a far lateral herniation at L4-L5 all affect the L4 root. Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Question 41High Yield
A 10-year-old boy with a history of retinoblastoma now reports right knee pain. AP and lateral radiographs are shown in Figures 3a and 3b. What is the most likely diagnosis?
Explanation
Explanation
3b The radiographs show a bone-producing lesion in the femoral diaphysis. The radiographic appearance of small round cell tumors is more permeative with an elevated periosteum and no matrix production. The appearance of this lesion is most consistent with osteosarcoma. Patients who carry the Rb gene are predisposed to osteosarcoma. However, Ewing's sarcoma, primitive neuroectodermal tumor, and osteomyelitis can all occur in this location. Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
References:
- Chauveinc L, Mosseri V, Quintana E, Desjardins L, Schlienger P, Doz F, Dutrillaux B: Osteosarcoma following retinoblastoma: Age at onset and latency period. Ophthalmic Genet 2001;22:77-88.
Question 42High Yield
An 18-year-old rugby player has had pain in his ring finger after missing a tackle 1 week ago. Examination reveals tenderness in the distal palm, and he is unable to actively flex the distal interphalangeal (DIP) joint. Radiographs are normal. What is the most appropriate management?
Explanation
Explanation
Flexor digitorum profundus rupture or "rugger jersey finger" often occurs in the ring finger after the player misses a tackle and catches the digit on the shirt of the opposing player. Surgical repair is required for zone I-type injuries. Moiemen NS, Elliot D: Primary flexor tendon repair in zone I. J Hand Surg Br 2000;25:78-84.
References:
- Strickland JW: Flexor tendon injuries: I. Foundations of treatment. J Am Acad Orthop Surg 1995;3:44-54.
Question 43High Yield
Which of the following findings is considered a poor prognostic factor for postoperative neurologic recovery in patients with rheumatoid arthritis?
Explanation
When markedly diminished space available for the cord (demonstrated by a posterior atlantoaxial interval of less than 10 mm) is seen, there is a poor prognosis for recovery (25% of Ranawat class IIIb patients) following surgery. A posterior atlantoaxial interval of 14 mm or less is a predictor of increased risk of paralysis, but patients with an interval between 10 mm and 14 mm have a greater chance of recovery. Space available for the cord that is at least 14 mm is not associated with an increased risk of neurologic deficit. Boden SD, Dodge LD, Bohlman HH, et al: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Question 44High Yield
A 25-year-old woman has had continuous pain after falling on her outstretched wrist 12 weeks ago. A current radiograph is shown in Figure 11. Management should consist of
Explanation
The patient has a scaphoid fracture with cystic resorption of the distal aspect of the midthird of the scaphoid. This fracture is unlikely to heal without intervention. Percutaneous pinning, closed manipulation, and bone grafting will not restore alignment. Treatment requires restoration of scaphoid length, bone grafting, and internal fixation to obtain healing with normal alignment. Cooney WP, Linscheid RL, Dobyns JH, Wood MB: Scaphoid nonunion: Role of anterior interpositional bone grafts. J Hand Surg Am 1988;13:635-650. Fernandez DL: A technique for anterior wedge-shaped grafts for scaphoid nonunions with carpal instability. J Hand Surg Am 1984;9:733-737. Stark HH, Rickard TA, Zemel NP, Ashworth CR: Treatment of ununited fractures of the scaphoid by illiac bone grafts and Kirschner-wire fixation. J Bone Joint Surg Am 1988;70:982-991.
Question 45High Yield
What property of titanium alloys accounts for their high corrosion resistance in vivo?
Explanation
Explanation
In both room temperature air and physiologic fluids, titanium alloys self-passivate or spontaneously form a layer of titanium oxide very rapidly. This layer makes titanium alloys resistant to surface breakdown. Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, Lippincott, 2003, vol 1, pp 269-278.
References:
- Lemons JE: Metallic alloys, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 19-27.
Question 46High Yield
A 14-year-old boy has an asymptomatic mass on the right arm. MRI scans and biopsy specimens are shown in Figures 51a through 51d. Immunostaining is positive for desmin. Additional staging studies should include



Explanation
The patient has rhabdomyosarcoma. Axilliary node and bone marrow biopsy are part of the staging because about 12% of patients with rhabdomyosarcoma of the extremity have evidence of lymph nodes metastases at presentation. Bone marrow metastases have been shown to portend a worse prognosis. Lawrence W, Jr., Hays DM, Heyn R, Tefft M, Crist W, Beltangady M, et al: Lymphatic metastases with childhood rhabdomyosarcoma: A report from the Intergroup Rhabdomyosarcoma Study. Cancer 1987;60:910-915.
Question 47High Yield
A 56-year-old man sustained a nondisplaced extra-articular fracture of the proximal aspect of the third metatarsal after dropping a heavy object on his left foot. Management should consist of
Explanation
This injury pattern is one of a direct trauma to the mid aspect of the foot. Without additional forces involved, capsular ligamentous injury is not anticipated; therefore, the injury should be a stable pattern. Treatment should consist of protected weight bearing as tolerated in a walking boot or walking cast. Surgical intervention with open reduction and internal fixation, percutaneous pinning, or open reduction and internal fixation with primary tarsometatarsal joint fusion is not indicated with this pattern of injury. The use of external bone stimulation in this acute fracture setting is not indicated. With injuries to the midfoot area where the exact mechanism of injury is uncertain, there should be a high index of suspicion for an associated injury to the tarsometatarsal joint, and standing radiographs or stress radiographs should be obtained. Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1265-1296.
Question 48High Yield
A 66-year-old man reports a 2-week history of worsening low back and leg pain. He reports that his pain is aggravated by lying down and relieved by standing and walking. He notes that he has been losing weight recently and that his pain has been awakening him during the night. His medical history is significant for hypertension, coronary artery disease, and prostate cancer. His physical examination is essentially unremarkable. Lumbar radiographs are within normal limits. What is the most appropriate management for this patient?
Explanation
In the initial assessment of acute low back pain in adults, no diagnostic testing is indicated during the first 4 weeks in the absence of "red flags" for a serious underlying condition. The purpose of the initial assessment of acute low back pain in adults is to rule out serious underlying conditions presenting as low back pain. The Agency for Healthcare Policy and Research, in its 1994 clinical practice guideline, identified four serious conditions that may present with low back pain, including fracture, tumor, infection, and cauda equina syndrome. This patient has five "red flags" for a spinal tumor as a possible etiology of his low back pain, including age of older than 50 years, constitutional symptoms (recent weight loss), pain worse when supine, severe nighttime pain, and a history of cancer. Of these, his history of cancer is most significant, as greater than 90% of spinal tumors are metastatic. In order of frequency, breast, prostate, lung, and kidney make up approximately 80% of all secondary spread to the spine. In the presence of "red flags" for tumor or infection, it is recommended that the clinician obtain a CBC count, ESR, and a urinalysis. If these are within normal limits and suspicions still remain, consider consultation or seek further evidence with a bone scan, radiographs, or additional laboratory studies. Negative radiographs alone are insufficient to rule out disease. If radiographs are positive, the anatomy can be better defined with MRI. Agency for Health Care Policy and Research, Bigos SJ (ed): Acute Low Back Problems in Adults. Rockville, MD, US Department of Health and Human Services, AHCPR Publication 95-0642, Clinical Practice Guideline #14, 1994.
Question 49High Yield
A previously healthy 30-year-old woman has neck pain and bilateral hand and lower extremity tingling with weakness after falling down stairs. She is alert and oriented. Examination reveals incomplete quadriplegia at the C6 level that remains unchanged throughout her evaluation and initial treatment. Radiographs show a bilateral facet dislocation of C6 on C7 without fracture. Attempts at reduction with halo cervical traction up to her body weight are unsuccessful. What is the next most appropriate step?
Explanation
Explanation
A facet dislocation that cannot be reduced in an alert, awake patient with some preservation of cord function requires MRI to evaluate the disk prior to a reduction under anesthesia. The presence or absence of a disk herniation must be assessed, as this factor may influence the method of reduction. Vaccaro AR, Falatyn SP, Flanders AE, et al: Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine 1999;24:1210-1217. Fardon DF, Garfin SR, Abitbol J (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 247-262. Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets. J Bone Joint Surg Am 1991;73:1555-1560.
References:
- Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.
Question 50High Yield
When compared with cobalt-chromium and stainless steel implants, a titanium implant has what biomechanical properties?
Explanation
Explanation
Titanium implants are commonly used in spinal surgery, especially when MRI may be needed after implantation. Titanium implants have a lower modulus of elasticity when compared with cobalt-chromium and stainless steel implants. This is felt to allow less stress shielding for these types of implants. The other properties do not apply to titanium implants.
References:
- Buckwalker JA, Einhorn TA, Simon SR (ed): Orthopedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 182-215.
Question 51High Yield
Figures 34a and 34b show the clinical photographs of a 46-year-old woman who has a painful deformity of the second toe. Surgical treatment consisting of metatarsophalangeal capsulotomy and proximal interphalangeal joint resection arthroplasty resulted in satisfactory correction, but the toe remains unstable at the metatarsophalangeal joint. What is the next most appropriate step?

Explanation
Crossover second toes are attributed to attenuation or rupture of the plantar plate and lateral collateral ligament and are associated with varying degrees of instability. Flexor-to-extensor transfer (Girdlestone/Taylor procedure) can provide intrinsic stability to the toe. Although plantar metatarsal head condylectomy can increase stability by resulting in scarring of the plantar plate, excision of the entire second metatarsal head carries a high risk of transfer metatarsalgia. Removal of the base of the proximal phalanx destabilizes the toe and should be reserved as a salvage procedure. Simple flexor tenotomy alone will not improve stability, and arthrodesis of the second metatarsophalangeal joint will limit motion and impair function. Coughlin MJ: Crossover second toe deformity. Foot Ankle 1987;8:29-39.
Question 52High Yield
Figure 30 shows an axial T1-weighted MRI scan of a patient's right shoulder. The arrows are pointing to what normal structure?
Explanation
Explanation
Tears of the pectoralis major tendon are frequently missed during examination. MRI provides excellent visualization of the tendon if the study extends low enough down the arm. The pectoralis major tendon inserts on the crest of the greater tubercle of the humerus, just lateral to the long head of the biceps tendon. The latissimus dorsi tendon inserts medial to the long head of the biceps tendon on the lesser tubercle. The subscapularis tendon inserts on the lesser tuberosity more proximally. The deltoid insertion is more distal. Connell DA, Potter HG, Sherman MF, et al: Injuries of the pectoralis major muscle: Evaluation with MR imaging. Radiology 1999;210:785-791. Carrino JA, Chandnanni VP, Mitchell DB, et al: Pectoralis major muscle and tendon tears: Diagnosis and grading using magnetic resonance imaging. Skeletal Radiol 2000;29:305-313.
References:
- Ohashi K, El-Khoury GY, Albright JP, et al: MRI of complete rupture of the pectoralis major muscle. Skeletal Radiol 1996;25:625-628.
Question 53High Yield
A 6-year-old boy presents with a mass and a lucent lesion involving the tibial shaft as seen in Figure 17a. The mass is mildly tender to palpation. The bone scan is focally hot in the tibia. Biopsy specimens are shown in Figures 17b and 17c. What is the most likely diagnosis?
Explanation
Explanation
17b 17c Osteofibrous dysplasia frequently presents at a very young age, usually less than 10 years. In most patients, it involves the anterior cortex of the tibial shaft and minor anterior bowing of the tibia is frequently seen. The lesion is unpredictable in nature, but local recurrence is very high in patients who undergo surgery before 15 years of age. Campanacci M, Laus M: Osteofibrous dysplasia of the tibia and fibula. J Bone Joint Surg Am 1981;63:367-375.
References:
- McCaffery M, Letts M, Carpenter B, et al: Osteofibrous dysplasia: A review of the literature and presentation of an additional 3 cases. Am J Orthop 2003;32:479-486.
Question 54High Yield
Free flap coverage for severe trauma to the upper extremity has the fewest complications when performed within what time period after injury?
Explanation
Explanation
Flap necrosis and infection rates are lowest if free flap coverage is performed within 72 hours of injury. Delays beyond 72 hours are associated with a higher rate of complications. Godina M: Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78:285-292.
References:
- Manske PR (ed): Hand Surgery Update. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 31-37.
Question 55High Yield
A 27-year-old man has neck pain after being involved in a motor vehicle accident. A lateral cervical radiograph is shown in Figure 21. What would be the most common neurologic finding?
Explanation
Explanation
The radiographic findings are consistent with a type II Hangman's fracture or traumatic spondylolisthesis of C2. This occurs with more than 3 mm of displacement according to the classification of Levine and Edwards. Even though the radiograph reveals significant displacement, the overall space available for the neural elements is increased, therefore minimizing the risk of neural compromise. Neurologic injury is most frequently encountered in type III injuries that are associated with bilateral facet dislocations of C2 on C3 but is infrequent in type I (less than 3 mm displacement) and type II traumatic spondylolisthesis. When neurologic deficits are associated with type II injuries, it is usually the result of an associated head injury. Cruciate paralysis occurs as a result of the crossover of the motor and sensory tracts at different levels of the cord at the C1-C2 junction. This results in normal sensation but complete loss of motor function. Levine AM: Traumatic spondylolisthesis of the axis (Hangman's fracture), in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 287-288.
References:
- Francis WR, Fielding JW, Hawkins RJ, Pepin J, Hensinger R: Traumatic spondylolisthesis of the axis. J Bone Joint Surg Br 1981;63:313-318.
Question 56High Yield
A 22-month-old girl has cerebral palsy. Which of the following findings is a good prognostic indicator of the child's ability to walk in the future?
Explanation
For the parachute test, the examiner holds the child prone and then lowers the child rapidly toward the floor. The parachute reaction is normal or positive if the child reaches toward the floor. The Moro or startle reflex should not be present beyond age 6 months. Asymmetric tonic neck reflex, extensor thrust, and absent foot placement are abnormal findings at any age. Bleck EE: Orthopaedic Management in Cerebral Palsy. Lavenham, Suffolk, The Lavenham Press, 1987, pp 121-139.
Question 57High Yield
What structure (arrow) is shown in Figure 24?
Explanation
The structure illustrated is the sympathetic chain viewed from an anterolateral view of the lower lumbar spine. It descends along the anterolateral aspect of the spine into the pelvis closely adherent to the vertebral column. The spinal nerves, including L5, can be seen exiting from the foramen. The ureters descend from the kidneys and cross anterior to the iliac vessels to the bladder. Onibokun A, Khoo LT, Holly L: Anterior retroperitoneal approach to the lumbar spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 101-105.
Question 58High Yield
Figures 15a and 15b show the radiographs of an 18-year-old mountain biker who came off of a 15-foot ramp and sustained an injury to his ankle. Because the local rural hospital had no orthopaedic surgeon available, he was transported to a Level 1 emergency department 10 hours after his initial injury. Examination reveals that the injury remains closed. Management should consist of
Explanation
Explanation
15b High-energy tibial pilon fractures involve disruption of the soft-tissue envelope with significant lower extremity edema. Definitive reconstruction of the comminuted distal tibia should be delayed for at least 7 days to allow edema to dissipate, lowering the risk of skin necrosis. An external fixator is the best method to keep the ankle at anatomic length while preventing skin necrosis. Ligamentotaxis will hold the fragments reduced to allow the edema to dissipate. CT may be obtained in traction to localize the individual fragments and plan surgical incisions and subsequent fixation. Short leg casting will not provide adequate ligamentotaxis to hold the fragments reduced and prevent skin compromise. Primary fusion of the ankle in an unstable tibial pilon fracture is prone to a poor result from nonunion or malunion. Tornetta P III, Weiner L, Bergman M, et al: Pilon fractures: Treatment with combined internal and external fixation. J Orthop Trauma 1993;7:489-496.
References:
- Sirkin M, Sanders R, DiPasquale T, Herscovici D Jr: A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma 1999;13:78-84.
Question 59High Yield
A 30-year-old woman has pain in her right hand. The radiograph, CT scan, and biopsy specimen are seen in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
Explanation
38b 38c An enchondroma is the most common primary tumor of the long bones of the hand. The lesion is usually asymptomatic and often is detected when there is a pathologic fracture. Shimizu K, Kotoura Y, Nishijima N, Nakamura T: Enchondroma of the distal phalanx of the hand. J Bone Joint Surg Am 1997;79:898-900.
References:
- Takigawa K: Chondroma of the bones of the hand: A review of 110 cases. J Bone Joint Surg Am 1971;53:1591-1600.
Question 60High Yield
Figures 25a and 25b show the clinical photographs of a 19-year-old baseball outfielder who has shoulder pain after sliding headfirst into second base. He reports pain while batting, sliding, and catching. Examination reveals a posterior prominence during midranges of forward elevation, which then disappears with a palpable clunk during terminal elevation and abduction. What is the most likely diagnosis?
Explanation
Explanation
25b A headfirst slide with the arm extended can injure the posterior shoulder. Winging of the scapula is dynamic and is considered a compensatory effort to prevent subluxation; it is not related to nerve injury. Posterior glenohumeral subluxation can be present during the initiation of a bat swing. Rotator cuff function, interval tears, and superior labrum tears can be painful but do not produce winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
References:
- Fiddian NJ, Kling RJ: The winged scapula. Clin Orthop 1984;185:228-236.
Question 61High Yield
The plate seen in Figure 48a was applied to the fracture seen in Figure 48b, and is functioning in what capacity?

Explanation
A Weber type B ankle fracture occurs with a supination external rotation mechanism of injury. The fibula generally fails with a spiral fracture pattern. The lag screws provide compression, and the plate acts to neutralize rotational and angular bending forces. A buttress plate resists vertical shear forces. A tension band is used over areas that may fail in tension, such as an olecranon fracture. Compression is provided by the lag screws, and distraction is again resisted by the lag screws.
Question 62High Yield
The most common mechanism of injury to the triangular fibrocartilage complex (TFCC) involves
Explanation
TFCC tears are common in athletes. As the athlete braces for a fall, the wrist is most commonly in an extended position and the forearm is pronated. Cohen MS: Ligamentous injuries of the wrist in the athlete. Clin Sports Med 1998;17:533-552.
Question 63High Yield
What preoperative factor correlates best with the outcome of rotator cuff repair?
Explanation
Explanation
The size of the rotator cuff tear in both anteroposterior and mediolateral dimensions has been found to correlate best with outcome. Older patient age and rupture of the long head of the biceps tend to be associated with larger tears and, therefore, may be associated indirectly with a poorer outcome. Iannotti JP: Full-thickness rotator cuff tears: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
References:
- Iannotti JP, Bernot MP, Kuhlman JR, Kelley MJ, Williams GR: Postoperative assessment of shoulder function: A prospective study of full-thickness rotator cuff tears. J Shoulder Elbow Surg 1996;5:449-457.
Question 64High Yield
A 10-year-old boy has a painful thigh mass. A radiograph, MRI scan, and biopsy specimen are shown in Figures 42a through 42c. What is the most likely diagnosis?


Explanation
A destructive mixed lytic and blastic metaphyseal lesion with a large soft-tissue mass in an adolescent is most likely an osteosarcoma until proven otherwise. The epicenter of the tumor is on the surface of the bone, most likely involves the periosteum, and is more likely to be chondroblastic in nature. Parosteal osteosarcoma is a low-grade tumor, much more radiodense, usually smaller, and found in the posterior distal femur of middle-aged patients. Chondrosarcomas are distinctly rare in childhood.
Question 65High Yield
Figure 29a shows the clinical photograph of a 26-year-old woman who has had the leg deformity since birth. She reports difficulty with walking and weight bearing and notes increased discomfort and swelling when the leg is dependent. She denies any history of trauma or family history of a similar disorder. Examination reveals a fixed equinovarus deformity of the foot but no evidence of a limb-length discrepancy. No other cutaneous findings or soft-tissue masses are noted. Sagittal and axial T1- and T2-weighted MRI scans are shown in Figures 29b and 29c. What is the most likely diagnosis?


Explanation
Because the MRI scans show marked dilation and proliferation of lymphatic channels that completely involve all the leg muscles and the clinical photograph shows the severe swelling associated with this disease, the most likely diagnosis is lymphangiomatosis. Poliomyelitis affects the anterior horn cells and manifests as muscle atrophy. Neurofibromatosis can have a similar clinical appearance but usually is associated with other systemic and cutaneous findings. Congenital band syndrome results in amputated or shortened extremities. Chronic venous stasis disease usually is not associated with joint contractures, and typically it affects older individuals. Surgical excision is the only known treatment; this patient underwent an above-knee amputation. Berquist TH (ed): MRI of the Musculoskeletal System, ed 3. Philadelphia, PA, Lippincott Raven, 1997, p 771.
Question 66High Yield
A 25-year-old woman has significant pain and swelling in her left ankle after falling off her bicycle. Examination reveals that she is neurovascularly intact. Radiographs are shown in Figures 33a through 33c. What is the next most appropriate step in management?


Explanation
The radiographs show a displaced ankle fracture with widening of the syndesmosis. Open reduction and internal fixation is indicated with fixation of the mortise with syndesmotic screws. Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Question 67High Yield
What process is often found associated with other neoplasms?
Explanation
Aneurysmal bone cyst may be either a "pattern" or a "diagnosis." Therefore, aneurysmal bone cyst should be viewed as a diagnosis of exclusion. Hemorrhage into a variety of primary bone lesions (eg, giant cell tumor of bone, chondroblastoma, osteoblastoma, fibrous dysplasia, osteosarcoma, or vascular neoplasms) may result in intralesional, membrane-bone blood-filled cysts. Such secondary changes may be confused with aneurysmal bone cyst, resulting in inappropriate therapy because assessment should be focused on identifying the underlying primary process. The entire specimen should be examined histologically in an effort to locate an underlying primary bone tumor. Bonakdarpour A, Levy WM, Aegerter E: Primary and secondary aneurysmal bone cyst: A radiological study of 75 cases. Radiology 1978;126:75-83. Levy WM, Miller AS, Bonakdarpour A, Aegerter E: Aneurysmal bone cyst secondary to other osseous lesions: Report of 57 cases. Am J Clin Pathol 1975;63:1-8.
Question 68High Yield
In patients older than age 40 years who sustain a first-time anterior dislocation of the shoulder, prolonged morbidity is most commonly associated with
Explanation
In the study done by Pevny and associates, 35% of patients older than age 40 years sustained rotator cuff tears and 8% had axillary nerve palsies. All of the patients with axillary nerve palsy also had rotator cuff tears. Imaging of the rotator cuff is indicated in this age group. The incidence of recurrent instability in patients older than age 40 years is 10% to 15%. Pevny T, Hunter RE, Freeman JR: Primary traumatic anterior shoulder dislocation in patients 40 years of age and older. Arthroscopy 1998;14:289-294. Sonnabend DH: Treatment of primary anterior shoulder dislocation in patients older than 40 years of age: Conservative versus operative. Clin Orthop 1994;304:74-77.
Question 69High Yield
When an acute infection of a total elbow arthroplasty is managed with irrigation and debridement, which of the following organisms is associated with the highest risk of persistent infection?
Explanation
Explanation
Salvage of a total elbow arthroplasty is possible with early aggressive management of acute infection (symptoms for less than 30 days) with serial irrigation and debridement and antibiotic bead placement. This form of treatment is indicated when there are no radiographic or intraoperative signs of loosening. However, successful treatment is largely dependent on the organism. Staphylococcus epidermidis is associated with persistent infection because it is an encapsulating organism, and it is best treated with implant removal and IV antibiotics. Yamaguchi K, Adams RA, Morrey BF: Infection after total elbow arthroplasty. J Bone Joint Surg Am 1998;80:481-491.
References:
- Schoifet SD, Morrey BF: Treatment of infection after total knee arthroplasty by debridement with retention of the components. J Bone Joint Surg Am 1990;72:1383-1390.
Question 70High Yield
An 11-year-old boy sustained an ankle injury while playing football. Figure 20 shows an AP radiograph obtained the day of injury. Treatment should consist of
Explanation
Explanation
The child has an injury involving both the growth plate and the articular surface of the ankle. Because of the significant displacement, open reduction and internal fixation is indicated to realign the physis and joint surface. The best method of fixation to avoid growth arrest is one that does not cross the physis. This is usually achieved by a transverse epiphyseal screw parallel to the physis. If the metaphyseal fragment was large enough, a transverse metaphyseal screw could be used instead. The incidence of growth arrest following physeal ankle injuries is as high as 50%, and long-term follow-up is indicated. Cass JR, Peterson HA: Salter-Harris Type-IV injuries of the distal tibial epiphyseal growth plate, with emphasis on those involving the medial malleolus. J Bone Joint Surg Am 1983;65:1059-1070.
References:
- Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibia physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-739.
Question 71High Yield
When performing a total knee arthroplasty using modular components, what is the minimum recommended thickness of an ultra-high molecular weight polyethylene insert for a tibial component?
Explanation
Explanation
Polyethylene wear has been identified as a major contributor to failure of total knee implants, of which thickness is an important factor. Several studies have shown that the minimum thickness should be 6 to 8 mm. While Wright and Bartel have shown that 6 to 8 mm has been recommended as the minimum thickness of an ultra-high molecular weight polyethylene insert for a tibial component in total knee arthroplasty, more recent work by Meding and associates and Worland and associates has verified the clinical efficacy of 4 mm of polyethylene in compression-molded anatomic graduated nonmodular components. Bartel DL, Bicknell VL, Wright TM: The effect of conformity, thickness, and material on stresses in ultra-high molecular weight components for total joint replacement. J Bone Joint Surg Am 1986;68:1041-1051. Wright TM, Bartel DL: The problem of surface damage in polyethylene total knee components. Clin Orthop 1991;273:261-263. Meding JB, Ritter MA, Faris PM: Total knee arthroplasty with 4.4 mm of tibial polyethylene: 10-year followup. Clin Orthop 2001;388:112-117.
References:
- Worland RL, Johnson G, Alemparte J, Jessup DE, Kennan J, Norambuena N: Ten to fourteen year survival and functional analysis of the AGC total knee replacement system. Knee 2002;9:133-137.
Question 72High Yield
Figure 12 shows the radiograph of a 55-year-old man who has severe, painful osteoarthritis of the left hip and is scheduled to undergo a left total hip arthroplasty. History reveals that he underwent a right total hip arthroplasty 5 years ago that remains pain-free. Based on the preoperative radiograph, the patient is at greatest risk for what complication?
Explanation
Explanation
The patient is at increased risk for limb-length discrepancy because the radiograph shows that the left leg is already longer than the right leg. To restore the proper biomechanics of the left hip, the left leg may have to be lengthened, further increasing the limb-length discrepancy. Intraoperative fracture, deep vein thrombosis, sciatic nerve palsy, and thigh pain are commonly associated with total hip arthroplasty, but the patient is not at increased risk for these complications.
References:
- Ranawat CS, Rodriguez JA: Functional leg-length inequality following total hip arthroplasty. J Arthroplasty 1997;12:359-364.
Question 73High Yield
A 55-year-old woman with type I diabetes mellitus has a chronic ulcer over the dorsum of her right foot and reports forefoot pain. Examination reveals 1- x 2-cm nondraining ulcer over the dorsum of the foot. The patient has 1-2+ pain with compression of the foot and ankle. She has a weakly palpable posterior tibial pulse and an absent dorsalis pedis pulse. There is no erythema, cellulitis, or drainage. Radiographs are normal. Which of the following diagnostic studies should be obtained?
Explanation
The presence of a dorsal ulcer in the presence of weak or absent pulses strongly suggests the possibility of arterial insufficiency. The best initial noninvasive study to assess for ischemia is the Doppler arterial study. A determination of the vascular status is of a greater priority than an assessment for infection or neuropathy because of the location and presentation of the ulcer. If ankle pressures are less than 45 mm Hg, there is a high risk that these lesions will not heal without revascularization. Wagner FW Jr: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981;2:64-122.
Question 74High Yield
Figure 43 shows the lateral radiograph of a patient who underwent anterior cruciate ligament reconstruction. Based on the tunnel placement shown in the radiograph, evaluation of postoperative knee range of motion will most likely show
Explanation
The radiograph shows the correct tibial tunnel and anterior femoral tunnel; therefore, range of motion will most likely show loss of flexion. Brown CH Jr, Carson EW: Revision anterior cruciate ligament surgery. Clin Sports Med 1999;18:109-171.
Question 75High Yield
Which of the following statements best describes the outcome of the routine use of continuous passive motion (CPM) machines after total knee arthroplasty (TKA)?
Explanation
Although CPM machines are used widely in the United States for patients undergoing TKA, the benefit seems to be marginal, if any. Numerous randomized trials have shown that final outcomes after total knee arthroplasty are unaffected by the use of CPM machines postoperatively. Some studies have suggested that use of CPM may improve flexion in the first few weeks, but any short-term benefit from the machine was lost by intermediate-term follow-up. Aside from potential improvement in flexion within the first few postoperative weeks, there does not appear to be any benefit from the machines. There is no improvement in pain, ambulation, or extension. The cost-effectiveness of these machines has been questioned by many authors. Pellicci PM, Tria AJ, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 287-293. McInnes J, Larson MG, Daltroy LH, et al: A controlled evaluation of continuous passive motion in patients undergoing total knee arthroplasty. JAMA 1992;268:1423-1428.
Question 76High Yield
A 6-year-old African-American boy with sickle cell disease has had pain and limited use of his right arm for the past 3 days. History reveals that he sustained a humeral fracture approximately 3 years ago. A lateral radiograph is shown in Figure 25. Based on these findings, a presumptive diagnosis of chronic osteomyelitis is made. What are the two most likely organisms?
Explanation
The risk of Salmonella osteomyelitis is much greater in patients with sickle cell disease than the general population. The exact reason for this increased risk is still unclear, but it appears to be associated with an increased incidence of gastrointestinal microinfarcts and abscesses. Both Staphylococcus aureus and Salmonella have been mentioned as the most prevalent causative organisms. Piehl FC, David RJ, Prugh SI: Osteomyelitis in sickle cell disease. J Pediatr Orthop 1993;13:225-227. Givner LB, Luddy RE, Schwartz AD: Etiology of osteomyelitis in patients with major sickle hemoglobinopathies. J Pediatr 1981;99:411-413. Epps CH Jr, Bryant DD III, Coles MJ, Castro O: Osteomyelitis in patients who have sickle-cell disease: Diagnosis and management. J Bone Joint Surg Am 1991;73:1281-1294.
Question 77High Yield
What part of the glenoid labrum has the least vascularity?
Explanation
Explanation
The glenoid labrum receives its blood supply from the suprascapular, posterior humeral circumflex, and circumflex scapular arteries. The labral vessels arise from the capsular and periosteal vessels that penetrate the periphery of the labrum. The bone does not appear to be a source of vascularity. The posterior/superior and inferior labrum have a fairly robust vascular supply, whereas the anterior/superior labrum has relatively poor vascularity, which may influence the success of superior lateral repairs.
References:
- Cooper DE, Arnoczky SP, O'Brien SJ, et al: Anatomy, histology and vascularity of the glenoid labrum: An anatomical study. J Bone Joint Surg Am 1992;74:46-52.
Question 78High Yield
Cementation technique has a definite influence on the long-term survival of cemented femoral components. Both clinical and autopsy studies support the use of a cement mantle with a thickness of how many millimeters?
Explanation
Explanation
Long-term radiographic analysis of cemented total hips supports the creation of a 2- to 5-mm cement mantle in the proximal medial region. Autopsy studies have shown that the incidence of crack formation was greatest when the cement mantle was less than 2 mm. Ebramzadeh E, Sarmiento A, McKellop HA, Llinas A, Gogan W: The cement mantle in total hip arthroplasty: Analysis of long-term radiographic results. J Bone Joint Surg Am 1994;76:77-87. Jasty M, Maloney WJ, Bragdon CR, O'Connor DO, Haire T, Harris WH: The initiation of failure in cemented femoral components of hip arthroplasty. J Bone Joint Surg Br 1991;73:551-558.
References:
- Maloney WJ III: The cemented femoral component, in Callaghan JJ, Rubash HE, Rosenberg AG (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 965-966.
Question 79High Yield
On MRI, a nonsanguinous effusion has what appearance?
Explanation
Nonbloody effusions that are greater than 1 mL are readily detected by MRI. They appear black on T1-weighted images and white on T2-weighted images. A sanguinous effusion is seen as white on T1-weighted images and black on T2-weighted images. Resnick D, Kang HS: Synovial joints, in Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 49-53.
Question 80High Yield
A 7-year-old girl reports foot pain and has difficulty ambulating. History reveals that she fell off a scooter 1 week ago, and there is possible exposure to a tick bite. A radiograph is shown in Figure 29. What is the best course of action?
Explanation
The child has Kohler's disease. This is a self-limiting osteochondritis of the navicular. It is treated symptomatically with initial cast immobilization for 6 to 12 weeks, followed possibly by orthotic management. Findings shown in the radiograph usually will normalize within 1 year, and there are no long-term sequelae. Borges JL, Guille JT, Bowen JR: Kohler's bone disease of the tarsal navicular. J Pediatr Orthop 1995;15:596-598.
Question 81High Yield
What bilateral surgical intervention is considered inappropriate based on the findings shown in the radiograph in Figure 52?
Explanation
The radiograph reveals osteonecrosis of both femoral heads with reasonably maintained joint surfaces. There may be some slight flattening of the femoral heads. Hip arthrodesis is difficult to perform because of the necrotic bone. Its use in patients with osteonecrotic hips is limited because of the 80% bilaterality; therefore, it is not an acceptable alternative. All the other options are acceptable interventions. Mont MA, Jones LC, Sotereanos DG, et al: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect 2000;49:169-185.
Question 82High Yield
A 55-year-old man has had a mass in his right thigh for the past 2 months. An MRI scan and biopsy specimens are shown in Figures 55a through 55c. What is the most likely diagnosis?
Explanation
Explanation
55b 55c The histology shows extraskeletal myxoid chondrosarcoma, characterized by abundant blue myxoid matrix with cords and nests of small tumor cells. Treatment consists of wide resection. Despite the name, hyaline cartilage is not a common component of these tumors. Adult rhabdomyosarcoma and malignant fibrous histiocytoma are highly pleomorphic sarcomas often containing multinucleated giant cells. Myxoid liposarcoma contains a prominent capillary network and lipoblasts. Myxoma is less cellular than extraskeletal myxoid chondrosarcoma and does not have a cord-like arrangement of tumor cells.
References:
- Kawaguchi S, Wada T, Nagoya S, Ikeda T, Isu K, Yamashiro K, et al: Extraskeletal myxoid chondrosarcoma. Cancer 2003;97:1285-1292.
Question 83High Yield
Venous thrombolembolism is a common complication following total hip and total knee arthroplasty; therefore, prophylaxis is deemed efficacious. Several studies on low-molecular-weight heparin (LMWH) have shown which of the following findings?
Explanation
Prophylactic LMWH is associated with a risk of bleeding complications, especially if administered too soon after surgery. The risk of major bleeding is 0.3% for control, 0.4% for aspirin, 1.3% for warfarin, 1.8% for LMWH, and 2.6% for unfractionated heparin. Colwell and associates conducted a prospective, randomized trial on over 1,500 total hip arthroplasty patients. Overall, the risk of clinically apparent venous thrombolembolism was 3.6% for LMWH and 3.7% for warfarin. LMWH acts in several sites of the coagulation cascade, with its principal action being inhibition of factor 10a. Thrombocytopenia is less common with LMWH than with unfractionated heparin. The use of LMWH is a relative contraindication with indwelling epidural anesthesia. Colwell CW Jr, Collis DK, Paulson R, et al: Comparison of enoxaparin and warfarin for the prevention of venous thromboembolic disease after total hip arthroplasty:. Evaluation during hospitalization and three months after discharge. J Bone Joint Surg Am 1999;81:932-940.
Question 84High Yield
A 55-year-old woman with a long history of low back and left lower extremity pain has failed to respond to exhaustive nonsurgical management. MRI scans show bulging and degeneration at L3-4 and L4-5 as well as a normal disk at L2-3 and L5-S1. She undergoes provocative lumbar diskography at L3-4, L4-5, and L5-S1. Post-diskography axial CT images of L3-4 and L4-5 are shown in Figures 6a and 6b, respectively. The injections at L3-4 and L4-5 produce no pain. The injection at L5-S1 produces 10/10 concordant back pain with radiation to the lower extremity. What is the most appropriate recommendation at this time?

Explanation
The results of this patient's lumbar diskography are equivocal at best. The two disks most likely to be her pain generators, based on their MRI appearance, produced 10/10 pain, however it was nonconcordant and did not reproduce any of her typical left-sided radicular symptoms. The only disk that produced concordant back pain was the normal disk at the L5-S1 level and it reproduced radicular symptoms on the side opposite of her typical pain. Based on these findings, it would be difficult to select a level or levels to include in a lumbar fusion. As such, continued nonsurgical management is the safest treatment option at the current time. Brox and associates reported on a randomized clinical trial comparing lumbar fusion to cognitive intervention and exercise and found similar results in both groups, with significantly less risk in the latter. Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Question 85High Yield
Which of the following acetabular cup designs has shown the greatest survivorship at 10 years in patients younger than age 60 years?
Explanation
Explanation
Poor survivorship of cemented sockets in young patients has lead to the development of a variety of cementless designs. Of these, smooth metal-backed sockets have not performed as well as porous-coated designs. Threaded metal-backed sockets showed a 6% to 25% revision rate secondary to aseptic loosening at a mean follow-up of 4.5 to 6 years. Despite some early failed designs, cementless porous-coated metal-backed sockets have shown the best survivorship in long-term studies. Smith SE, Harris WH: Total hip arthroplasty performed with insertion of the femoral component with cement and the acetabular component without cement: Ten to thirteen-year study. J Bone Joint Surg Am 1997;79:1827-1833.
References:
- Pellicci PM, Tria AJ Jr, Garvin KL, (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 195-206.
Question 86High Yield
A 16-year-old boy has a symptomatic flatfoot deformity that is causing pain, skin breakdown, and shoe wear problems. Shoe modification and an orthosis have failed to provide relief. Examination reveals hindfoot valgus, talonavicular sag, and forefoot abduction that are all passively correctable. Treatment should consist of
Explanation
Explanation
The patient has a supple planovalgus deformity that is passively fully correctable, and nonsurgical management has failed to provide relief. Lateral column lengthening with medial soft-tissue tightening will correct the deformity and maintain a flexible foot. Arthrodesis is not recommended for a supple, correctable deformity because of loss of motion and long-term degeneration of surrounding joints. Medial displacement calcaneal osteotomy is generally reserved for an adult-acquired flexible flatfoot. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 613-631. Evans D: Calcaneo-valgus deformity. J Bone Joint Surg Br 1975;57:270-278.
References:
- Mosca VS: Calcaneal lengthening for valgus deformity of the hindfoot: Results in children who had severe, symptomatic flatfoot and skewfoot. J Bone Joint Surg Am 1995;77:500-512.
Question 87High Yield
A 77-year-old man with diabetes mellitus has had a nonhealing Wagner grade I ulcer under the medial sesamoid for the past 3 months. He smokes tobacco regularly. He has undergone several debridements and total contact casting. Examination reveals no palpable pulses. He has no erythema or purulence, and he is afebrile. Radiographs reveal no abnormalities. What is the best initial diagnostic test to help determine why the ulcer has failed to heal?
Explanation
Explanation
The best initial test for this patient is to assess the vascular supply to the foot. An elderly smoker with diabetes mellitus has a high risk of peripheral vascular disease. Decreased weight bearing has not been successful. Although a bone scan might be helpful, it would take secondary consideration to the patient's vascular supply, especially in the absence of any acute infection. Monofilament testing would help diagnosis neuropathy, which is a root cause behind the ulcer forming, but does not prevent it from healing. The Thompson's test is used to diagnosis an Achilles tendon rupture.
References:
- Brodsky JW: Evaluation of the diabetic foot. Instr Course Lect 1999;48:289-303.
Question 88High Yield
A 30-year-old patient has acetabular dysplasia and moderate secondary osteoarthrosis. Which of the following studies will best help predict the success of periacetabular osteotomy?
Explanation
Improvement in the appearance of the hip joint on functional radiographic evaluation (abduction/adduction views) has been shown to be predictive of outcome following joint preserving surgery. CT and MRI findings have not been shown to be predictive of outcome.
Question 89High Yield
Degenerative spondylolisthesis of the cervical spine is most commonly seen at which of the following levels?
Explanation
Degenerative spondylolisthesis of the cervical spine is seen almost exclusively at C3-4 and C4-5; this is in contrast to degenerative changes, which are most commonly seen at C5-6 and C6-7. Tani T, Kawasaki M, Taniguchi S, et al: Functional importance of degenerative spondylolisthesis in cervical spondylotic myelopathy in the elderly. Spine 2003;28:1128-1134.
Question 90High Yield
A 32-year-old woman sustained an injury to her left upper extremity in a motor vehicle accident. Examination reveals a 2-cm wound in the mid portion of the dorsal surface of the upper arm and deformities at the elbow and forearm; there are no other injuries. Her vital signs are stable, and she has a base deficit of minus 1 and a lactate level of less than 2. Radiographs are shown in Figures 9a and 9b. In addition to urgent debridement of the humeral shaft fracture, management should include

Explanation
With a severe injury to the upper extremity, the best opportunity for achieving a good functional result for a floating elbow is immediate debridement of the open fracture, followed by internal fixation of the fractures. The ability to do this depends on the patient's physiologic status. In this patient, the procedure is acceptable because she has normal vital signs and no chest or abdominal injuries, and normal physiologic parameters (base excess and lactate) show adequate peripheral perfusion. The surgical approaches will be determined by the associated injury patterns and open wounds. In this patient, the humerus was debrided and stabilized through a posterior approach as was the medial condyle fracture. The ulna was fixed through an extension of the posterior incision and the radius through a separate dorsal approach. Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Question 91High Yield
A 20-year-old patient has foot pain. A radiograph and T1-weighted MRI scan are shown in Figures 8a and 8b. A biopsy specimen is shown in Figure 8c. Treatment should consist of

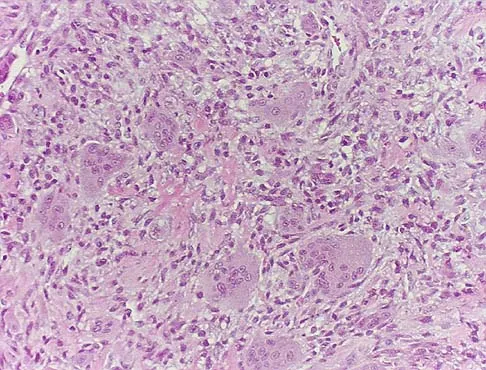
Explanation
Giant cell tumors occur near articular surfaces in young adults. The histology shows abundant giant cells with nuclei resembling the surrounding cells. Although the MRI scan shows soft-tissue involvement, curettage is still the preferred treatment. Chemotherapy is not necessary for benign lesions, and amputation is too aggressive. Cementation, phenol, and cryosurgery (liquid nitrogen) are all acceptable local adjuvants to curettage. Packing the cavity with bone graft rather than cement is also acceptable. Dahlin DC, Unni KK: Bone Tumors: General Aspects and Data on 8,542 Cases. Springfield, IL, Charles C. Thomas, 1986.
Question 92High Yield
The diagnosis of an infection after total knee arthroplasty is most reliably proven based on what single study?
Explanation
Explanation
In a study of 52 patients with infected total knee arthroplasties, Windsor and associates showed that the average leukocyte count was 8,300/mm3 and that aspirated knee fluid was positive in all patients except one. Knee radiographs can be unclear in showing infection, which may be present without radiographic signs of loosening. Technetium Tc 99m and gallium bone scans may not conclusively show the presence of infection, particularly in the first 3 years after knee arthroplasty. Windsor RE, Bono JV: Infected total knee replacements. J Am Acad Orthop Surg 1994;2:44-53.
References:
- Windsor RE, Insall JN, Urs WK, et al: Two-stage reimplantation for the salvage of total knee arthroplasty complicated by infection: Further follow-up and refinement of indications. J Bone Joint Surg Am 1990;72:272-278.
Question 93High Yield
A 40-year-old laborer sustains the injury shown in the radiograph and CT scan in Figures 56a and 56b. What is the most common complication associated with surgical intervention?

Explanation
The patient has a severe Sanders type 4 calcaneus fracture. By far the most common complication associated with surgical treatment of calcaneus fractures is wound dehiscence. Sanders R: Displaced intra-articular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250.
Question 94High Yield
Figure 19 shows the radiograph of a 12-year-old boy who sustained an injury to his hand when another child fell on him. Management should consist of
Explanation
Explanation
The patient has a Salter-Harris type III fracture of the proximal phalanx of the thumb. It is usually caused by an abduction injury where the ulnar collateral ligament avulses a fragment away from the proximal epiphysis and is the most common childhood gamekeeper's injury. If there is greater than 1 mm of separation or a significant articular step-off, an open reduction, performed through an extensor aponeurosis-splitting approach, is required to reestablish joint congruity and stability. Percutaneous or closed methods of reduction are usually ineffective. The dorsal approach avoids the volar neurovascular structures. Since the ulnar collateral ligament is still attached, this area does not need to be visualized. The major goal is to reestablish joint congruity and bony stability. This can be easily performed via the dorsal approach. Carey TP: Fracture and dislocations of the phalanges, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 435-436.
References:
- Ogden JA: Skeletal Injury in the Child. New York, NY, Springer-Verlag, 2000, p 668.
Question 95High Yield
A 32-year-old runner has pain in the medial arch that radiates into the medial three toes. He reports the presence of pain only when running. Examination reveals normal hindfoot alignment. There is a weakly positive Tinel's sign over the posterior tibial nerve. Tenderness is noted with palpation over the plantar medial area in the vicinity of the navicular tuberosity. What is the most likely diagnosis?
Explanation
The examination findings reveal that there is specific involvement of the medial plantar nerve by the distribution of the pain medially. The symptoms exclude the possibility of plantar fasciitis and anterior tibial tendinitis. Sinus tarsi syndrome would produce anterolateral symptoms rather than medial symptoms. Rask MR: Medial plantar neurapraxia (jogger's foot): Report of three cases. Clin Orthop 1978;134:193-195. Murphy PC, Baxter DE: Nerve entrapment of the foot and ankle in runners. Clin Sports Med 1985;4:753-763.
Question 96High Yield
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3, an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Explanation
Examination reveals an irritable hip, creating a differential diagnosis of transient synovitis versus pyogenic hip arthritis. Kocher and associates described four criteria to help predict the presence of infection: inability to bear weight, fever, ESR of more than 40 mm/h, and a peripheral WBC count of more than 12,000/mm3. This patient meets three of the four criteria, with a positive predictive value of 73% to 93% for joint infection. Therefore, aspiration of the hip is warranted, with a high likelihood that emergent hip arthrotomy will be indicated. Ideally, intravenous antibiotics should be administered after culture material has been obtained from needle aspiration of the hip. An urgent bone scan is better indicated as a screening test for sacroiliitis or diskitis. If the arthrocentesis proves negative, CT or MRI of the pelvis may be indicated to rule out a pelvic or psoas abscess. Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422. Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 97High Yield
The posterior circumflex humeral artery and the axillary nerve usually lie in a space bordered superiorly by the
Explanation
Explanation
The quadrangular space is bordered superiorly by the teres minor, medially by the long head of the triceps, laterally by the humerus, and inferiorly by the teres major. The posterior circumflex humeral artery and the axillary nerve lie in this space. Rockwood CA Jr, Matsen FA III: The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 70-71.
References:
- Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, pp 401-402, 407.
Question 98High Yield
Figure 28 shows an AP radiograph of a 54-year-old woman who underwent lumbar laminectomy and fusion at the L4 and L5 levels with placement of a bone stimulator 8 years ago. She also underwent a left total hip arthroplasty 2 years ago; aspiration of that joint now reveals that it is infected with a gram-positive cocci organism. History is also significant for IV drug use and human immunodeficiency virus (HIV). The patient reports fever, chills, and left flank and abdominal pain. Examination reveals significant pain with resisted left hip flexion and passive hip extension. She also has lumbar hyperlordosis. Which of the following studies would best identify the underlying cause of her infection?
Explanation
Explanation
The patient's clinical signs (fever and flank, hip, and abdominal pain) suggest a primary iliopsoas abscess. With an increased patient population who abuse drugs and/or who are HIV-positive, iliopsoas abscess may be more prevalent because of systemic bacterial seeding and may be potentially unrecognized. Diagnostic imaging studies provide a better understanding of the anatomic magnitude of the infection, give concrete confirmation of the diagnosis, and may suggest an underlying cause. Neither standard abdominal radiographs nor ultrasound studies are sensitive enough to be diagnostic of this disease process. CT has been established as the standard study for identifying the underlying cause of this abscess. The hip infection has most likely developed as a result of hematogenous spread from an infected skin lesion from the patient's IV drug use. Santaella RO, Fishman EK, Lipsett PA: Primary vs secondary iliopsoas abscess: Presentation, microbiology, and treatment. Arch Surg 1995;130:1309-1313.
References:
- Malhotra R, Singh KD, Bhan S, Dave PK: Primary pyogenic abscess of the psoas muscle. J Bone Joint Surg Am 1992;74:278-284.
Question 99High Yield
A 55-year-old man sustained an elbow dislocation in a fall. Postreduction radiographs are shown in Figures 40a and 40b. What is the best course of management?

Explanation
The radiographs show an elbow dislocation associated with a comminuted radial head fracture. In the setting of comminution and instability, factures of the radial head are best managed with an arthroplasty rather than open reduction and internal fixation. Resection of the radial head will worsen the instability and is not recommended. Silastic radial head replacements are contraindicated. Hildebrand KA, Patterson SD, King GJ: Acute elbow dislocations: Simple and complex. Orthop Clin North Am 1999;30:63-79.
Question 100High Yield
During the first 2 years of life, which of the following actions is most responsible for increasing structural stability of the physis?
Explanation
Explanation
The zone of Ranvier provides the earliest increase in strength of the physis. During the first year of life, the zone spreads over the adjacent metaphysis to form a fibrous circumferential ring bridging from the epiphysis to the diaphysis. This ring increases the mechanical strength of the physis. The zone also helps the physis grow latitudinally. In turn, the increased width of the physis helps the physis further resist mechanical forces. The change in shape of the physis to its progressively more undulating form is also a factor in increasing physeal strength, but this occurs over a longer period of time, as the child's activity level increases. The undulations of the physis seen in some growth plates also add to stability but to a lesser extent. The other changes contribute little toward increasing physeal strength. Burkus J, Ogden J: Development of the distal femoral epiphysis: A microscopic morphological investigation of the zone of Ranvier. J Pediatr Orthop 1984;4:661-668.
References:
- Shapiro F, Holtrop ME, Glimcher MJ: Organization and cellular biology of the perichondrial ossification groove of Ranvier: A morphological study in rabbits. J Bone Joint Surg Am 1977;59:703-723.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon