100 Orthopedic Board Review MCQs: Mock Exam Set #280
14 Apr 2026
101 min read
141 Views
Key Takeaway
This page offers 100 high-yield orthopedic board review questions, specifically Mock Exam Set 280, designed to help surgeons master the ABOS, OITE, and FRCS exams. Sharpen your knowledge of surgical anatomy and critical concepts through challenging multiple-choice questions for ultimate success.
Comprehensive Surgical Anatomy of the Thigh: ...
00:00
Start Quiz
Question 1High Yield
A patient who is an observant Jehovah's Witness requires major surgery for scoliosis that will likely result in significant blood loss. Which of the following might the patient consider allowing the surgical team to use?
Explanation
Explanation
Jehovah's Witnesses will not accept the transfusion of blood or blood products such as packed red or white cells, platelets, or plasma. However, many Jehovah's Witnesses will accept the use of a cell saver in a "closed circuit." Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Question 2High Yield
A 40-year-old man with amyloidosis injured his left knee while walking. Figure 17a shows an AP radiograph that was obtained 2 weeks after the injury. The radiograph shown in Figure 17b was obtained after the patient wore a hinged knee brace for 3 months. A clinical photograph is shown in Figure 17c. What is the most likely diagnosis?
Explanation
Explanation
17b 17c The patient has a Charcot arthropathy of the knee, which is associated with amyloidosis. The rapid joint destruction shown in the radiographs is most consistent with that diagnosis. Drennan D, Fahey J, Maylahn D: Important factors in achieving arthrodesis of the Charcot knee. J Bone Joint Surg Am 1971;53:1180-1193. Soudry M, Binazzi R, Johanson N, et al: Total knee arthroplasty in Charcot and Charcot like joints. Clin Orthop 1986;208:199-204.
References:
- Buxbaum JN: The systemic amyloidoses. Curr Opin Rhemutol 2004;16:67-75.
Question 3High Yield
Figures 8a and 8b show the clinical photograph and radiograph of a 4-month-old infant who has a left foot deformity. Examination reveals that the foot deformity is an isolated entity, and the infant has no known neuromuscular conditions or genetic syndromes. Which of the following studies will best confirm the diagnosis?

Explanation
The clinical photograph shows a rocker-bottom deformity, and the lateral radiograph suggests a congenital vertical talus deformity. A lateral radiograph of the foot in maximum plantar flexion is needed to demonstrate the fixed position of the deformity with malalignment of the talar-metatarsal axis. A fixed dislocation of the navicular on the talus differentiates a congenital vertical talus from the oblique talus with talonavicular subluxation. Kumar SJ, Cowell HR, Ramsey PL: Vertical and oblique talus. Instr Course Lect 1982;31:235-251. Kodros SA, Dias LS: Single-stage correction of congenital vertical talus. J Pediatr Orthop 1999;19:42-48.
Question 4High Yield
What type of nerve palsy is most common following elbow arthroscopy?
Explanation
Transient ulnar nerve palsy is the most common palsy following elbow arthroscopy. The ulnar nerve is most frequently affected, followed by the radial nerve. Injury to the other nerves has been reported but less frequently. Kelly EW, Morrey BF, O'Driscoll SW: Complications of elbow arthroscopy. J Bone Joint Surg Am 2001;83:25-34.
Question 5High Yield
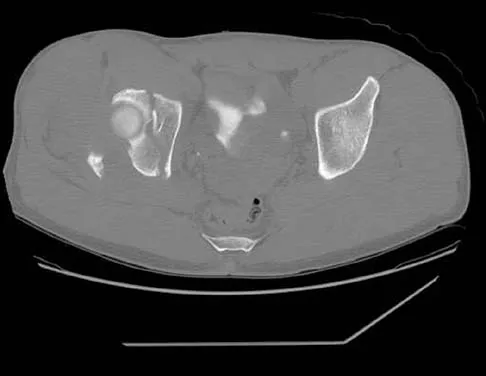
The radiographs and CT scan seen in Figures 28a through 28d reveal what type of acetabular fracture pattern?


Explanation
The AP, obturator oblique, and iliac oblique views of the pelvis reveal a fracture that disrupts the iliopectineal and ilioischial lines, indicating a fracture that involves both anterior and posterior columns. However, it does not have the other features of anterior or posterior column fracture patterns. A displaced posterior wall fracture is also present, best seen on the obturator oblique view. The anterior to posterior directed fracture line on the CT scan indicates a transverse fracture; therefore, the patient has a transverse with posterior wall fracture pattern. A T-type fracture would be similar but would have a break into the obturator ring. Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Question 6High Yield
A 22-year-old female collegiate javelin thrower has shoulder pain. She notes that her pain is primarily located in the posterior aspect of her shoulder, is exacerbated with throwing, and she experiences maximal tenderness in the extreme cocking phase of the throwing cycle. On examination, she reports deep posterior shoulder pain when the arm is abducted 90 degrees and maximally externally rotated to 110 degrees. This reproduces her symptoms precisely. Shoulder radiographs are normal. What is the most likely diagnosis?
Explanation
Explanation
The patient has internal impingement. Internal impingement is commonly seen in overhead throwing athletes. When positioned in the extreme cocking phase of the throwing cycle, the posterior glenoid impacts the articular surface of the infraspinatus and posterior fibers of the supraspinatus tendon. This impact can cause partial-thickness rotator cuff tearing and posterosuperior labral lesions. She has no evidence of anterior shoulder instability, and her range of motion is excellent which rules out adhesive capsulitis. Subacromial impingement is identified with anterolateral shoulder pain with internal rotation in the abducted position. A full-thickness rotator cuff tear in a 22-year-old individual would require significant trauma and would likely result in pain at rest and with lifting. Meister K, Buckley B, Batts J: The posterior impingement sign: Diagnosis of rotator cuff and posterior labral tears secondary to internal impingement in overhand athletes. Am J Orthop 2004;33:412-415.
References:
- Kaplan LD, McMahon PJ, Towers J, et al: Internal impingement: Findings on magnetic resonance imaging and arthroscopic evaluation. Arthroscopy 2004;20:701-704.
Question 7High Yield
During a retroperitoneal approach to the L4-5 disk, what structure must be ligated to safely mobilize the common iliac vessels toward the midline from laterally and gain exposure?
Explanation
To mobilize the common iliac vessels across the midline, the iliolumbar vein must be ligated. It has a short trunk and can be torn if mobilization is attempted without ligation. It is the only branch off the common iliacs (there are no arterial branches) prior to the terminal branches, the internal (hypogastric) and external iliacs. The middle sacral vessels run distally from the axilla of the bifurcation and are a factor when accessing the L5-S1 disk. Baker JK, Reardon PR, Reardon MJ, et al: Vascular injury in anterior lumbar surgery. Spine 1993;18:2227-2230.
Question 8High Yield
A 17-year-old girl has multidirectional instability of the shoulder. What is the most appropriate initial management?
Explanation
Explanation
Multidirectional instability of the shoulder is defined as symptomatic instability in two or more directions (anterior, posterior) but must include a component of inferior instability. Initial treatment should always include physical therapy and instruction in a home exercise program that emphasizes periscapular and rotator cuff strengthening to improve the dynamic stability of the glenohumeral joint. Immobilization has not been shown to be effective. Open capsular shift and arthroscopic capsular plication remain the surgical options when appropriate nonsurgical management fails (typically a minimum of 6 months of dedicated therapy and home program). Thermal capsulorrhaphy remains controversial but is not recommended by many clinicians because of reported complications including recurrent instability, axillary nerve injury, chondrolysis, and capsular injury. Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908. D'Alessandro DF, Bradley JP, Fleischli JE, et al: Prospective evaluation of thermal capsulorrhaphy for shoulder instability: Indications and results, two- to five-year follow-up. Am J Sports Med 2004;32:21-33. Levine WN, Clark AM Jr, D'Alessandro DF, et al: Chondrolysis following arthroscopic thermal capsulorrhaphy to treat shoulder instability: A report of two cases. J Bone Joint Surg Am 2005;87:616-621.
References:
- Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 278-279.
Question 9High Yield
In Dupuytren's disease, the retrovascular cord typically displaces the radial proper digital nerve of the ring finger in what direction?
Explanation
Explanation
Retrovascular cords are common in Dupuytren's disease and commonly require surgical treatment. Nerve injury in Dupuytren's surgery is an infrequent complication that occurs partly because the digital nerves can be displaced from their normal anatomic relationships by retrovascular cords. The nerves are displaced superficially, toward the center of the digit (palmarly and ulnarly). This displacement is typically seen at the level of the metacarpophalangeal joint.
References:
- Rayan GM: Palmar fascial complex anatomy and pathology in Dupuytren's disease. Hand Clin 1999;15:73-86.
Question 10High Yield
Ulnohumeral distraction interposition arthroplasty is considered the most appropriate treatment for which of the following patients?
Explanation
Distraction interposition arthroplasty is indicated for the treatment of both rheumatoid and posttraumatic arthritis and is reserved for younger patients who are not suitable candidates for total elbow arthroplasty. Although less reliable than prosthetic replacement, distraction interposition arthroplasty is a useful option in the treatment of young, high-demand patients with elbow arthritis. It is rarely indicated in the presence of polyarticular inflammatory arthritis but may be of value in those patients in whom the disease is limited primarily to the elbow. Isolated radiocapitellar arthritis can be successfully treated with radial head resection, although caution should be exercised if there is evidence of instability. Osteoarthritis is best treated with ulnohumeral arthroplasty. Cheng SL, Morrey BF: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Question 11High Yield
Following a vertebroplasty of L2, cement is noted to protrude directly anterior to the L2 vertebral body. The cement is closest to which of the following structures?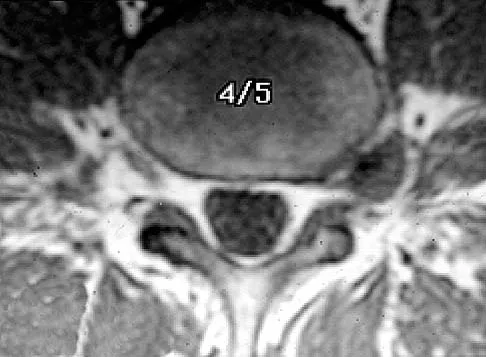
Explanation
At the level of L2, the liver and the vena cava lie to the right. The pancreas and duodenum are anterior to the aorta. The aorta lies in the midline just in front of the vertebral body. Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3. Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 331.
Question 12High Yield
A 35-year-old man sustained a 1-inch stab incision in his proximal forearm while trying to use a screwdriver 2 weeks ago. The laceration was routinely closed, and no problems about the incision site were noted. He now reports that he has been unable to straighten his fingers or thumb completely since the injury. Clinical photographs shown in Figures 30a and 30b show the man passively flexing the wrist. What is the most appropriate management?

Explanation
The clinical photographs indicate that the tenodesis effect of digit flexion with passive wrist extension and digit extension with passive wrist flexion is intact, indicating no discontinuity of the extensor or flexor tendons. The most likely injury is a laceration of the posterior interosseous nerve.
Question 13High Yield
Which of the following prophylactic regimens for the prevention of deep venous thrombosis after knee arthroplasty has received a grade 1A recommendation in favor of its use from the American College of Chest Physicians (ACCP) in the 2004 guidelines?
Explanation
Explanation
In the 2004 ACCP guidelines, there were three prophylactic regimens that received a grade 1A favorable recommendation. These included low-molecular-weight heparin, warfarin, or fondaparinux, as long as they are used for at least 10 days. If warfarin is used, the target INR should be 2.0 to 3.0, according to the guidelines. Pneumatic compression sleeves have gained popularity in the orthopaedic community but have not received a grade 1A rating from the ACCP at this time. Use of aspirin by itself is discouraged by the ACCP.
References:
- Geerts WH, Pineo GF, Heit JA, et al: Prevention of venous thromboembolism: The seventh ACCP Conference on antithrombotic and thrombolytic therapy. Chest 2004;126:338S-400S.
Question 14High Yield
A 48-year-old woman with rheumatoid arthritis reports increasing elbow pain for the past 6 months. History reveals that she underwent total elbow arthroplasty 7 years ago. A peripheral WBC count, erythrocyte sedimentation rate, and C-reactive protein studies are normal. An AP radiograph is shown in Figure 5. What is the next most appropriate step in management?
Explanation
Explanation
Pain relief is excellent after total elbow arthroplasty and is comparable to the results found with hip and knee arthroplasty. The failure of total elbow arthroplasty in the treatment of rheumatoid arthritis can be the result of infection, aseptic loosening, instability, and bearing surface wear. The radiographic findings shown here are consistent with bushing wear in a linked device. The bushings can be changed before continued wear results in osteolysis and implant loosening. If the implants become loose, then reimplantation is necessary. Resection arthroplasty is not indicated if the components are well fixed. Elbow arthrodesis is not indicated in patients with rheumatoid arthritis. Gill DR, Morrey BF: The Coonrad-Morrey total elbow arthroplasty in patients who have rheumatoid arthritis: A ten to fifteen-year follow-up study. J Bone Joint Surg Am 1998;80:1327-1335.
References:
- Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 333-341.
Question 15High Yield
Figures 6a through 6d show the radiographs and biopsy specimens of an 8-year-old girl with leg pain. Management of the lesion should consist of

Explanation
The biopsy specimens show a chondromyxoid fibroma with varying amounts of cartilage, benign fibrous tissue, giant cells, and loose myxoid areas. Chondromyxoid fibroma is a benign active bone lesion that is best treated with aggressive curettage and bone grafting. Although recurrences are common, more aggressive treatment is not warranted initially. Wilson AJ, Kyriakos M, Ackerman LV: Chondromyxoid fibroma: Radiographic appearance in 38 cases and in a review of the literature. Radiology 1991;179:513-518.
Question 16High Yield
A 58-year-old patient who underwent bilateral hip arthroplasty 12 years ago now reports pain in his hips and difficulty with ambulation to the point where he now uses crutches. A radiograph of the hip and pelvis is shown in Figure 26. What is the best treatment option for this patient?
Explanation
Explanation
The radiographs reveal acetabular component failure with bone loss. There are several treatment options available. The best option for survivorship is a cementless porous-coated acetabular component. This patient may or may not require structural bone graft, which may need to be determined at the time of surgery. Bipolar implants and cemented acetabular components for revision surgery have not demonstrated long-term success. The use of a protrusio ring is reserved primarily for massive bone loss such as a Paprosky type III bone loss with significant superior migration of the acetabular component. The best clinical results for acetabular component revision have been achieved with cementless porous-coated implants. Haddad FS, Masri BA, Garbuz DS, et al: Acetabulum, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 923-936. D'Antonio JA: Periprosthetic bone loss of the acetabulum: Classification and management. Orthop Clin North Am 1992;23:279-290.
References:
- Rubash HE, Sinha RK, Paprosky W, et al: A new classification system for the management of acetabular osteolysis after total hip arthroplasty. Instr Course Lect 1999;48:37-42.
Question 17High Yield
A patient reports persistent anterior shoulder pain following a forceful external rotation injury to the shoulder. An MRI scan is shown in Figure 4. The patient remains symptomatic despite 3 months of nonsurgical management. Treatment should now consist of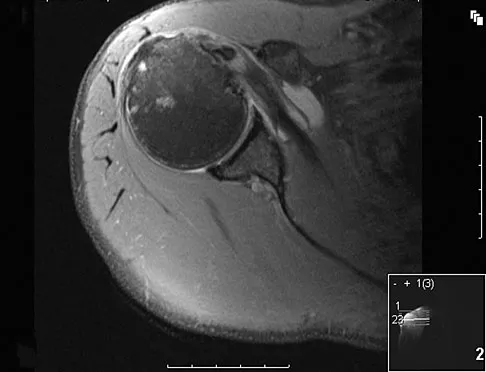
Explanation
The MRI scan reveals a subscapularis tear with a biceps that is out of the groove. Treatment in this patient is most predictable if the subscapularis is repaired. The biceps should either be tenodesed or tenotomized since it is unstable. Recentering of the biceps has been found to be unpredictable. Treatment of these lesions has been shown to have better results if the biceps is either released or tenodesed. This prevents recurrent biceps symptoms that can be source of surgical failure. Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10. Deutsch A, Altcheck DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Question 18High Yield
Figure 4a shows the radiograph of a 20-year-old man who has an injury to the right shoulder. Figure 4b shows an arthroscopic view (posterior portal). The arrow points to a
Explanation
Explanation
4b The radiograph shows an anterior dislocation of the shoulder. A frequently encountered sequela of this is a compression fracture of the posterolateral humeral head, commonly referred to as a Hill-Sachs defect. The arthroscopic view of the glenohumeral joint visualizes the posterior aspect of the humeral head. In the image, the area devoid of cartilage to the right is the bare area. The indentation seen to the left is a Hill-Sachs defect. Matsen FA, Thomas SC, Rockwood CA, et al: Glenohumeral instability, in Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 611-754.
References:
- Mazzocca AD, Noerdlinger M, Cole B, et al: Arthroscopy of the shoulder: Indications and general principals of techniques, in McGinty JB (ed): Operative Arthroscopy, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 412-427.
Question 19High Yield
Which of the following findings is seen in the chest radiograph shown in Figure 13?
Explanation
Explanation
Orthopaedic surgeons are often responsible for interpreting radiographs of general examinations such as the chest radiograph shown. For accurate interpretation, it is important to systematically review all of the information available on the radiograph. Using this approach, the fracture of the left proximal humerus is readily recognized. Linear air soft-tissue density at the lung periphery would suggest a pneumothorax, but this finding is not shown on the radiograph. The upper thoracic spine is well aligned. The sternoclavicular and distal clavicles are normal.
References:
- Bone LB: Emergency treatment of the injured patient, in Browner BD, Jupiter JB, Levine AM, Trafton PG (eds): Skeletal Trauma. Philadelphia, PA, WB Saunders, 1992, pp 133-138.
Question 20High Yield
A patient who underwent an L5-S1 diskectomy 18 months ago has persistent pain in the left leg. Figures 9a and 9b show postoperative axial T1-weighted MRI scans at the L5-S1 level without and with gadolinium. What is the most likely diagnosis?
Explanation
Explanation
9b Persistent or recurrent symptoms after lumbar diskectomy are troublesome and can be difficult to assess. Gadolinium-enhanced MRI scans may be helpful. The images show enhancement about the left S1 root, a finding that is most consistent with perineural (epidural) fibrosis. The root itself does not enhance. Root enhancement has been associated with compressive radicular symptoms. A disk herniation does not enhance with gadolinium. A neurilemmoma enhances with gadolinium, but the involved root would be enlarged. There is no evidence of a fluid collection which would be consistent with an epidural abscess. Babar S, Saifuddin A: MRI of the post-discectomy lumbar spine. Clin Radiol 2002;57:969-981. Kikkawa I, Sugimoto H, Saita K, et al: The role of Gd-enhanced three-dimensional MRI fast low-angle shot (FLASH) in the evaluation of symptomatic lumbosacral nerve roots. J Orthop Sci 2001;6:101-109.
References:
- Vroomen PC, Van Hapert SJ, Van Acker RE, et al: The clinical significance of gadolinium enhancement of lumbar disc herniations and nerve roots on preoperative MRI. Neuroradiology 1998;40:800-806.
Question 21High Yield
A 71-year-old woman undergoes a posterior lumbar decompression and fusion from L4-S1. Thirty-six hours after the procedure, she reports severe right-sided chest pain and shortness of breath. Doppler ultrasound reveals a clot proximal to the knee within the femoral vein. A large pulmonary embolus is confirmed by CT angiography. The next most appropriate step in management should consist of
Explanation
Explanation
In a review of 13,000 spinal procedures, nine patients were treated with heparin following development of pulmonary emboli. Of these patients, six had serious complications ranging from wound drainage to paralysis. Heparin therapy instituted within 10 days of the surgical procedure resulted in a 100% complication rate. Vena cava filter placement has a complication rate of 0.12% to 10.1%. Removable filters are currently in clinical trials. Cain JE Jr, Major MR, Lauerman WC, et al: The morbidity of heparin therapy after development of pulmonary embolus in patients undergoing thoracolumbar or lumbar spinal fusion. Spine 1995;20:1600-1603. Roberts AC: Venous imaging and inferior vena cava filters. Curr Opin Radiol 1992;4:88-96.
References:
- Becker DM, Philbrick JT, Selby JB: Inferior vena cava filters. Arch Intern Med 1992;152:1985-1994.
Question 22High Yield
A 21-year-old soccer player reports pain and is unable to straighten his knee following an acute injury during a game. He is unable to continue to play. An MRI scan is shown in Figure 3. What is the next most appropriate step in management?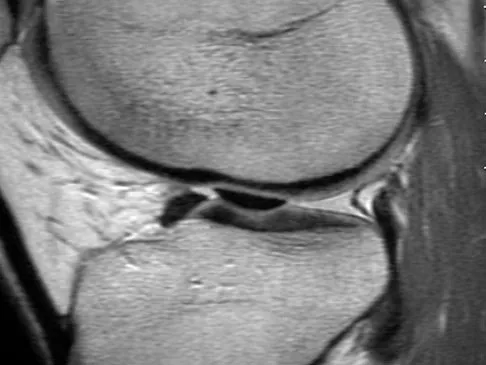
Explanation
The patient has a locked knee that cannot be fully extended. This is most likely the result of the mechanical block of a bucket-handle tear that has flipped into the notch. Also, the pain may be so severe that the muscle spasm prevents the knee from straightening out. When the patient is anesthetized, the muscle spasm relaxes and the meniscus can be reduced out of the notch. Arthroscopy is the treatment of choice. A meniscal repair is usually possible in large bucket-handle tears because the meniscus is torn in the red-red zone where most of the vascular supply is located. If the handle portion is badly frayed or damaged, a partial meniscectomy should be performed. The classic finding on MRI is a "double PCL sign." This is due to the flipped portion of the meniscus in the notch. Critchley IJ, Bracey DJ: The acutely locked knee: Is manipulation worthwhile? Injury 1985;16:281-283.
Question 23High Yield
In performing an opening wedge high tibial osteotomy at the tibial tubercle, the osteotome extends 5 mm posteriorly and centrally out of the bone as shown in Figures 17a and 17b. What is the first structure it enters?

Explanation
The major risk of performing a high tibial osteotomy is neurovascular injury. The new version of the high tibial osteotomy makes a transverse osteotomy at the level of the tibial tubercle. The osteotome is protected by the oblique belly of the popliteus muscle. The popliteal artery and vein and tibial nerve all lie posterior to the muscle. The soleus muscle originates below this level. Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3. Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 422.
Question 24High Yield
A 14-year-old boy sustained a 100% displaced distal radius Salter-Harris type II fracture. Neurologic examination demonstrates normal motor examination and two-point discrimination. He undergoes fracture reduction to the anatomic position with the application of a long arm cast. Postreduction he reports increasing hand and wrist pain with diminution of two-point discrimination to 10 mm over the index and middle fingers over the next several hours after surgery. The cast is bivalved and the padding released relieving all external pressure over the arm. Reevaluation reveals increasing sensory deficit over the affected area. What is the next most appropriate management intervention?
Explanation
The patient has an evolving acute carpal tunnel syndrome. Initial management for this injury is to relieve all external pressure that may elevate the neural compression. Surgical decompression of the median nerve at the carpal tunnel is the optimal intervention. Further nonsurgical interventions (cast removal or further bivalving) are insufficient to alleviate the neural compression. Waters PM, Mih AD: Fractures of the distal radius and ulna, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, p 361.
Question 25High Yield
A patient undergoes the procedure shown in Figure 19. An important part of this procedure is preservation of what wrist ligament?
Explanation
Proximal row carpectomy is a salvage wrist procedure that yields a surprisingly stable construct. This has been attributed to two factors: 1) the congruency of the head of the capitate in the lunate fossa (this articulation is less congruent than the native lunate/lunate fossa relationship, but surprisingly stable), and 2) preservation of the radioscaphocapitate ligament, the most radial of the palmar extrinsic ligaments, which prevents ulnar subluxation after proximal row carpectomy.
Question 26High Yield
A 46-year-old woman reports pain and a shortened appearance of her toe after undergoing a Keller resection arthroplasty 2 years ago for hallux rigidus. Examination reveals mild swelling and motion limited to 25 degrees at the metatarsophalangeal joint. Radiographs show large dorsal osteophytes on the first metatarsal head, 50% resection of the proximal phalanx, and complete loss of the metatarsophalangeal joint space. Which of the following is considered the most reliable procedure to improve her pain and the appearance of her toe?
Explanation
Because the patient has significant arthritis, arthrodesis is the treatment of choice. Adding a bone graft will prevent further shortening and add length to her toe, resulting in improved cosmesis. A cheilectomy will not alleviate her arthritis pain. The toe is too short for an effective Moberg phalangeal dorsiflexion osteotomy. A Waterman first metatarsal dorsal osteotomy will not address the degenerative joint disease or shortening. Silastic arthroplasty may help, but there is the risk of additional problems with foreign body reaction and a significant risk of failure known to occur with Silastic materials. Myerson MS, Schon LC, McGuigan FX, Oznur A:Result of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int 2000;21:297-306. Mann RA, Coughlin MJ: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 252-253.
Question 27High Yield
An 82-year-old man has had episodic right thigh pain after undergoing a total hip arthroplasty 10 years ago. Initial postoperative radiographs are shown in Figures 26a and 26b, and current radiographs are shown in Figures 26c and 26d. What is the most likely cause of his pain?
Explanation
Explanation
26b 26c 26d These radiographs are dominated by the subsidence of the femoral component. There is also evidence of polyethylene wear and femoral osteolysis in the region of the greater trochanter. There is no evidence of proximal (calcar) stress shielding, and there is a thick distal pedestal. Engh and associates defined two major signs of osseointegration - the absence of radiolucent lines around the porous-surfaced portion of the implant and new bone bridging the gap between the endosteal surface and the porous portion of the implant. Implant migration indicates failure of ingrowth. Osteolysis is a periprosthetic loss of bone secondary to particulate debris and it is often clinically silent unless it is accompanied by pathologic fracture. It is often globular. Acetabular loosening is based on radiolucent lines and implant migration. The current radiographs demonstrate subsidence of the stem with pedestal formation. Engh CA, Massin P, Suthers KE: Roentgenographic assessment of biologic fixation of porous-surface femoral components. Clin Orthop Relat Res 1990;257:107-128.
References:
- Engh CA, Hooten JP, Zettl-Schaffer KF, et al: Evaluation of bone ingrowth in proximally and extensively porous-coated anatomic medullary locking prostheses retrieved at autopsy. J Bone Joint Surg Am 1995;77:903-910.
Question 28High Yield
A 35-year-old man who snowboards sustained the injury shown in Figures 4a through 4c. What is the mechanism of injury?
Explanation
Explanation
4b 4c Fractures of the lateral process of the talus in snowboarders have been thought to result from pure dorsiflexion, inversion, and axial loading. In a cadaveric study, 10 cadavers were placed in fixed dorsiflexion and inversion with an axial load. This was combined with or without external rotation. No fractures occurred after axial loading in the dorsiflexed-inverted position. Fractures of the lateral process of the talus occurred in 75% of the specimens with the addition of external rotation. Boon AJ, Smith J, Zobitz ME, et al: Snowboarder's talus fracture: Mechanism of injury. Am J Sports Med 2001;29:333-338.
References:
- Kirkpatrick DP, Hunter RE, Janes PC, et al: The snowboarder's foot and ankle. Am J Sports Med 1998;26:271-277.
Question 29High Yield
A 14-year-old boy sustained a femoral neck fracture in a fall from a tree and underwent open reduction and internal fixation 6 months ago. Follow-up examination now reveals an antalgic Trendelenburg gait and painful range of motion. A radiograph is shown in Figure 23, and a CT scan shows a nonunion. Treatment should consist of
Explanation
The coxa vara deformity and fracture nonunion should be treated simultaneously; therefore, the treatment of choice is curettage of the nonunion, intertrochanteric valgus osteotomy, and revision internal fixation. In addition, valgus osteotomy will convert the shear forces across the nonunion to compression, aiding in healing of the nonunion. None of the other procedures addresses both issues, and hip fusion is inappropriate under these conditions. Lam SF: Fractures of the neck of the femur in children. J Bone Joint Surg Am 1971;53:1165-1179.
Question 30High Yield
A 47-year-old woman has an asymptomatic pelvic mass that was discovered on routine gynecologic examination. A radiograph, CT scan, MRI scan, and biopsy specimen are shown in Figures 7a through 7d. Metastatic work-up is negative. Treatment should consist of
Explanation
Explanation
7b 7c 7d The imaging studies show a chondrosarcoma; therefore, surgical treatment is indicated. There is no role for intralesional treatment of an exophytic lesion, particularly in the pelvis. Even obtaining a biopsy specimen risks intrapelvic contamination, although many surgeons would still perform a biopsy prior to a resection to confirm the diagnosis. Chondrosarcoma is considered resistant to both radiation therapy and chemotherapy; therefore, radiation therapy generally is not used except for unresectable lesions. Chemotherapy would be used only for metastatic disease or in patients with high-grade chondrosarcoma. The grade would not be known until after resection, and in this patient, the histology slide showed a grade I neoplasm. Chemotherapy would not be used preoperatively because a cartilage tumor is unlikely to shrink, and in this patient, the lesion is resectable. Springfield DS, Gebhardt MS, Mcguire MH: Chondrosarcoma: A review. J Bone Joint Surg Am 1996;78:141-149.
References:
- Marco RA, Gitelis S, Brebach GT, Healey JH: Cartilage tumors: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:292-304.
Question 31High Yield
A 38-year-old marathon runner has had Achilles tendon pain for the past 2 months. Examination reveals that the tendon is thickened and tender proximal to the calcaneal insertion. The tendon sheath is not thickened or tender. The pathophysiology of the tendon is best described as
Explanation
Explanation
Atraumatic Achilles tendon disease can be differentiated into Achilles tendinosis and peritendinitis. Thickening and tenderness of the Achilles tendon are present in both, but thickening and tenderness of the tendon sheath indicates peritendinitis. Histologic examination of Achilles tendinosis reveals an absence of acute and chronic inflammatory cells. Radiologists often diagnose partial tendon rupture by MRI and there may be microscopic longitudinal tears present, but there is no mechanical compromise as would be implied by a partial rupture. The thickening typically occurs in the portion of the tendon with the poorest blood supply, and biochemical analysis detects high levels of lactate and other products of anaerobic glycolysis. Astrom M, Rausing A: Chronic Achilles tendinopathy: A survey of surgical and histopathologic findings. Clin Orthop 1995;316:151-164. Ohberg L, Lorentzon R, Alfredson H: Neovascularisation in Achilles tendons with painful tendinosis but not in normal tendons: An ultrasonographic investigation. Knee Surg Sports Traumatol Arthrosc 2001;9:233-238.
References:
- Alfredson H, Bjur D, Thorsen K, et al: High intratendinous lactate levels in painful chronic Achilles tendinosis: An investigation using microdialysis technique. J Orthop Res 2002;20:934-938.
Question 32High Yield
Which of the following statements best describes the location of the nerve that is at risk in a direct posterior approach to the Achilles tendon?
Explanation
The sural nerve lies lateral to the Achilles tendon at the level of the foot but follows an oblique course proximally to lie directly over the tendon as it heads to the popliteal fossa. It is at risk with any proximal dissection from a direct posterior approach and in particular with procedures done at the musculotendinous junction. The nerve crosses over the lateral border of the Achilles tendon at an average of 9.8 cm above its insertion. Webb J, Moorjani N, Radford M: Anatomy of the sural nerve and its relation to the Achilles tendon. Foot Ankle Int 2000;21:475-477.
Question 33High Yield
What is the most common primary malignant tumor of bone in childhood?
Explanation
Osteosarcoma is the most common primary malignant tumor of bone in childhood, followed by Ewing's sarcoma. Rhabdomyosarcoma is a soft-tissue sarcoma of childhood. Chondrosarcoma rarely occurs in childhood. Osteochondroma is a benign tumor of bone. Simon MA, Springfield DS, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 266.
Question 34High Yield
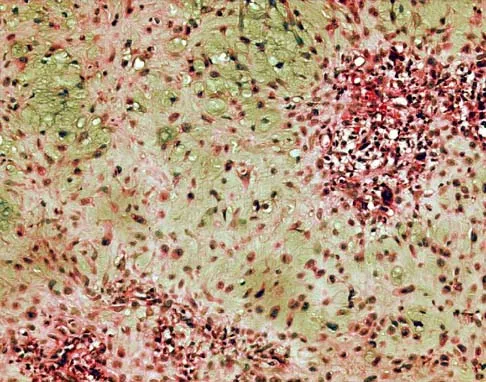
The biopsy specimens seen in Figures 55a and 55b are from a lytic lesion in the sacrum of a 58-year-old man. What is the most likely diagnosis?

Explanation
The lesion is a chordoma and the other listed choices can be eliminated based on the histology. Many tumors can occur in the sacrum including chordoma, multiple myeloma, giant cell tumor, aneurysmal bone cyst, and metastatic disease. The histology in this patient shows a lobulated lesion on low power with fibrous septae separating the lobules. At higher magnification, the cells have eosinophilic vacuolated cytoplasm and are called physaliferous cells. Chordoma is a low-grade neoplasm that most commonly occurs in the sacrum and rarely in the base of the skull. The diagnosis is often delayed. Chordoma is thought to originate from notochordal remnants. Chordoma typically occurs in the midline and has an associated soft-tissue mass. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 372. Fuchs B, Dickey ID, Yaszemski MJ, et al: Operative management of sacral chordoma. J Bone Joint Surg Am 2005;87:2211-2216.
Question 35High Yield
A 28-year-old woman fell on her right wrist while rollerblading 2 days ago. She was seen in the emergency department at the time of injury and was told she had a sprain. Examination now reveals dorsal tenderness in the proximal wrist but no snuffbox or ulnar tenderness. Standard wrist radiographs are normal. What is the next most appropriate step in management?
Explanation
Explanation
When considering the diagnosis of scapholunate ligament injury, standard radiographic views of the hand will not always reveal widening of the scapholunate gap. Although MRI may reveal injury to the ligaments, the PA clenched fist view can be obtained in the office during the initial patient visit. Arthroscopy is not a first-line diagnostic tool. Walsh JJ, Berger RA, Cooney WP: Current status of scapholunate interosseous ligament injuries. J Am Acad Orthop Surg 2002;10:32-42.
References:
- Browner BD, Levine AM, Jupiter JB, et al (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1366-1367.
Question 36High Yield
A 13-year-old boy has had a painless mass in the arm for the past 2 months. An MRI scan and biopsy specimens are shown in Figures 46a through 46c. What is the most likely diagnosis?
Explanation
Explanation
46b 46c Nodular fasciitis is a benign soft-tissue lesion that usually arises from the fascia and is often misdiagnosed as a sarcoma. Desmoid tumors (aggressive fibromatosis) are also benign tumors with a greater tendency for local recurrence. Desmoid tumors have more spindle-shaped fibroblasts in an abundant collagenous matrix. Malignant fibrous histiocytoma is a hypercellular pleomorphic sarcoma more commonly found in adults. The histology is not consistant with a fatty tumor.
References:
- Bernstein KE, Lattes R: Nodular (pseudosarcomatous) fasciitis, a nonrecurrent lesion: Clinicopathologic study of 134 cases. Cancer 1982;49:1668-1678.
Question 37High Yield
A 26-year-old man has had a 2-year history of pain and stiffness after sustaining a comminuted olecranon fracture. Treatment at the time of injury consisted of open reduction and internal fixation with tension band wiring. Examination reveals motion of 45 degrees to 110 degrees and pain throughout the arc of motion. Resisted flexion and extension are painful. Forearm rotation is normal. Radiographs are shown in Figure 51. Treatment should consist of
Explanation
The patient has posttraumatic arthritis of the elbow; therefore, the treatment of choice is hardware removal and soft-tissue releases with splinting to avoid recurrence of contractures. The combination of pain and stiffness in an elbow that has sustained significant joint surface damage renders it unresponsive to simple soft-tissue releases and heterotopic bone excision. Joint distraction and interposition arthroplasty offer the possibility of maintaining motion and relieving pain as a later salvage procedure. Joint replacement should not be performed in young, active, strong individuals because the prosthesis will fail quickly and complications will develop. Synovectomy and radial head excision are not indicated. Morrey BF: Distraction arthroplasty: Clinical applications. Clin Orthop 1993;293:46-54.
Question 38High Yield
A 30-year-old woman who runs approximately 30 miles a week has had right hip and groin pain for the past 3 weeks. Examination reveals an antalgic gait, limited motion of the right hip, and pain, especially with internal and external rotation. Plain radiographs are normal, and an MRI scan is shown in Figure 21. Management should consist of
Explanation
Explanation
A stress fracture of the hip is a relatively common problem in endurance sports. These fractures are classified as compression-side, tension-side, and displaced femoral neck fractures. The MRI scan shows a compression-side stress fracture. Compression-side fractures usually occur in the inferior or calcar area of the proximal femur, and non-weight-bearing crutch ambulation for 6 to 7 weeks will most likely result in healing. Once the patient is walking without pain or a limp, activities can be slowly increased. Because tension-side fractures have a high risk of displacement, treatment should consist of immediate internal fixation. Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 239-253.
References:
- Fullerton LR Jr, Snowdy HA: Femoral neck stress fractures. Am J Sports Med 1988;16:365-377.
Question 39High Yield
Figures 8a through 8c show the lateral radiograph and T1- and T2-weighted MRI scans of a 14-year-old soccer player who reports aching thigh pain. The next most appropriate step in management should consist of


Explanation
Although the MRI findings could be misinterpreted as an aggressive soft-tissue process, the periosteal-based ossification on the radiograph in an athlete most likely suggests myositis ossificans. The radiograph should be repeated to see further maturation of the ossification with a typical "zoning" pattern. The zoning pattern is one of peripheral ossification. This is often best seen on a CT scan. King JB: Post-traumatic ectopic calcification in the muscles of athletes: A review. Br J Sports Med 1998;32:287-290.
Question 40High Yield
During a posterior approach to the glenoid with retraction as shown in Figure 33, care should be taken during superior retraction to avoid injury to which of the following structures?
Explanation
Explanation
During a posterior approach to the shoulder for either a scapular fracture, glenoid fracture, or posterior shoulder pathology, the interval between the teres minor and infraspinatus is split. Excessive superior retraction on the infraspinatus, or excessive dissection superomedially under the infraspinatus muscle and tendon can cause injury to the suprascapular nerve and/or artery. During dissection in this interval, the axillary artery and axillary nerve are well protected. A branch of the circumflex scapular artery ascends between the teres minor and infraspinatus muscle, but it is at risk during dissection on the scapula in the mid portion of the interval and not during superior retraction. The profunda brachii artery is not present in this interval. Jerosch JJ, Greig M, Peuker ET, et al: The posterior subdeltoid approach: A modified access to the posterior glenohumeral joint. J Shoulder Elbow Surg 2001;10:265-268. Judet R: Surgical treatment of scapular fractures. Acta Orthop Belg 1964;30:673-678.
References:
- Kavanagh BF, Bradway JK, Cofield RH: Open reduction and internal fixation of displaced intra-articular fractures of the glenoid fossa. J Bone Joint Surg Am 1993;75:479-484.
Question 41High Yield
A 7-year-old boy is seen in the emergency department with an isolated and displaced supracondylar humerus fracture and absent radial and ulnar pulses. Despite a moderately painful attempt at realignment, examination reveals that his hand remains pulseless. What is the next most appropriate step in management?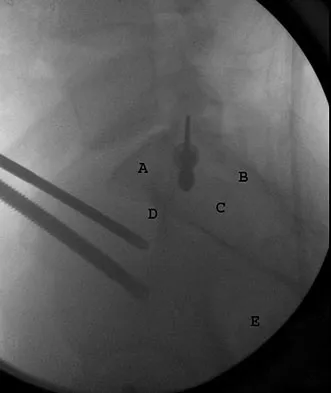
Explanation
Displaced supracondylar humerus fractures in children may have associated vascular compromise. Decreased blood flow may be due to vessel injury, entrapment within the fracture site, kinking from fracture displacement, or from vessel spasm. Optimal initial treatment in the emergency department includes gentle realignment of the limb and vascular assessment. Angiography is not required in isolated injuries as the level of the vessel compromise is always at the site of the fracture. When blood flow is not restored, the next best step in treatment is to proceed urgently to the operating room. A formal closed reduction and pinning is performed, and then the vascular status is reassessed. Exploration and vascular repair is required if the hand is cool, white, and without pulses. Ay S, Akinci M, Kamiloglu S, et al: Open reduction of displaced pediatric supracondylar humeral fractures through the anterior cubital approach. J Pediatr Orthop 2005;25:149-153. Sabharwal S, Tredwell SJ, Beauchamp RD, et al: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Question 42High Yield
A 74-year-old woman with rheumatoid arthritis reports shoulder pain that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 23a and 23b. Examination reveals active forward elevation to 120 degrees and external rotation to 30 degrees. What treatment option results in the most predictable pain relief and function?
Explanation
Explanation
23b Most studies have shown that total shoulder arthroplasties yield better pain relief and improved forward elevation when compared to hemiarthroplasty in patients with rheumatoid arthritis. Although rotator cuff tears are more common in this patient population, this patient has good forward elevation and no significant superior migration of the humeral head; therefore, a reverse arthroplasty is not indicated. The arthritis is too advanced in this patient to consider arthroscopy, but in less advanced cases it can improve range of motion and decrease pain. Metal-backed glenoid components have shown higher rates of loosening. Collin DN, Harryman DT II, Wirth MA: Shoulder arthroplasty for the treatment of inflammatory arthritis. J Bone Joint Surg Am 2004;86:2489-2496. Baumgarten KM, Lashgari CM, Yamaguchi K: Glenoid resurfacing in shoulder arthroplasty: Indications and contraindications. Instr Course Lect 2004;53:3-11.
References:
- Martin SD, Zurakowski D, Thornhill TS: Uncemented glenoid component in total shoulder arthroplasty: Survivorship and outcomes. J Bone Joint Surg Am 2005;87:1284-1292.
Question 43High Yield
A 38-year-old man underwent a transtibial amputation for chronic posttraumatic foot and ankle pain and chronic calcaneal osteomyelitis. Postoperative radiographs are seen in Figures 41a and 41b. What is the proposed purpose of the surgical modification seen in the radiographs?

Explanation
The Ertl modification of a below-knee amputation has been proposed to create a more stable "platform" to aid in transferring the load of weight bearing between the residual limb and the prosthetic socket. It is felt that a stable platform allows total contact loading over an enlarged stable surface area. Early studies have suggested that this modification may enhance the patient's perceived functional outcome. Pinzur MS, Pinto MA, Saltzman M, et al: Health-related quality of life in patients with transtibial amputation and reconstruction with bone bridging of the distal tibia and fibula. Foot Ankle Int 2006;27:907-912.
Question 44High Yield
A 30-year-old woman injured her ankle playing soccer 3 months ago. She now reports popping and pain over the lateral side of her ankle. An MRI scan is shown in Figure 33. What structure needs to be repaired to alleviate the popping?
Explanation
Explanation
The symptoms and MRI scan indicate dislocated peroneal tendons. In this patient, the structure that needs to be repaired is the superior peroneal retinaculum. If the popping was coming from a torn peroneal tendon, repair would involve the peroneal longus or brevis tendon, but this is not shown in the MRI scan. The anterior talofibular ligament or the calcaneofibular ligament would need to be repaired if the patient had ankle instability due to an ankle sprain. Jones DC: Tendon disorders of the foot and ankle. J Am Acad Orthop Surg 1993;1:87-94.
Question 45High Yield
The need for postoperative allogeneic blood transfusions after total hip arthroplasty has been shown to be reduced when using
Explanation
In a prospective study, 216 patients were randomized into three groups consisting of low-dose preoperative erythropoietin, high-dose preoperative erythropoietin, and placebo control. All patients were treated for 4 weeks prior to total hip arthroplasty. Both the low- and high-dose erythropoietin groups had a significantly lower rate of blood transfusions (p < 0.001) after surgery. Waddell JP: Evidence-based orthopedics. J Bone Joint Surg Am 2001;83:788.
Question 46High Yield
Creatine is currently being used by athletes as a dietary supplement in an attempt to enhance performance. What is the physiologic basis for its use?
Explanation
Creatine is currently used as a nutritional supplement in an attempt to enhance athletic performance. The physiologic basis for its use is based on its conversion by CK to PCr, which acts as an energy reservoir in muscle cells for the production of ATP. A number of studies that examined the effect of creatine supplementation on performance concluded that while creatine does not increase peak force production, it can increase the amount of work done in the first few anaerobic short duration, maximal effort trials. The mechanism for this enhancement of work is unknown, but it is most likely secondary to the increase in the available PCr pool. Greenhaff PL: Creatine and its application as an ergogenic aid. Int J Sport Nutr 1995;5:S100-S110. Greenhaff PL, Casey A, Short AH, Harris R, Soderlund K, Hultman E: Influence of oral creatine supplementation on muscle torque during repeated bouts of maximal voluntary exercise in man. Clin Sci 1993;84:565-571. Trump ME, Heigenhauser GJ, Putman CT, Spriet LL: Importance of muscle phosphocreatine during intermittent maximal cycling. J Appl Physiol 1996;80:1574-1580.
Question 47High Yield
Which of the following findings is likely to be pathologic in a thin, well-conditioned endurance athlete?
Explanation
Explanation
Left ventricular hypertrophy by voltage is a nonspecific diagnosis, especially in athletes with an asthenic body habitus. High vagal tone in endurance athletes may result in first degree or even type I second degree (ie, Wenckebach) AV block in endurance athletes. High vagal tone results in resting sinus bradycardia in many trained athletes. A I-II/IV systolic ejection murmur is occasionally found in healthy athletes; however, when the murmur increases in intensity with maneuvers that decrease ventricular filling, such as standing or the Valsalva maneuver, dynamic obstruction that is the result of hypertrophic obstructive cardiomyopathy should be suspected. Nonspecific STT wave changes in the lateral leads on ECG are not uncommon in highly trained athletes; thus, they are nonspecific for ischemic heart disease. Pelliccia A, Maron BJ, Culasso F, DiPaolo FM, et al: Clinical significance of abnormal electrocardiographic patterns in trained athletes. Circulation 2000;102:278-284.
References:
- Maron BJ, Thompson PD, Puffer JC, McGrew CA: Cardiovascular preparticipation screening of competitive athletes: A statement for health professionals from the Sudden Death Committee (Clinical Cardiology) and Congenital Cardiac Defects Committee (Cardiovascular Disease in the Young), American Heart Association. Circulation 1996;94:850-856.
Question 48High Yield
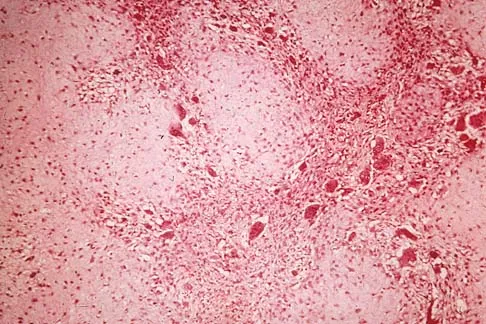
A 54-year-old woman reports worsening pain in her buttock, especially when sitting for long periods of time. She has occasional pain and paresthesias radiating down her posterior leg. She has no significant medical history. MRI scans are shown in Figures 15a and 15b and a biopsy specimen is shown in Figure 15c. What is the most likely diagnosis?
Explanation
Explanation
15b 15c The biopsy specimen shows a wavy collagenous matrix with elongated cells; this is most consistent with neurofibroma. The patient has a mass in the region of the sciatic nerve. Imaging characteristics, homogeneous and very low signal on T1-weighted and very high signal on the T2-weighted sequences, are consistent with a myxoid-type lesion. These include myxoma, myxoid sarcomas, and nerve sheath tumors. Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 1135-1136
References:
- Menendez LR: Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL American Academy of Orthopaedic Surgeons, 2002, p 251.
Question 49High Yield
When performing knee arthroplasty, which of the following procedures provides the most consistent fixation for the tibial component?
Explanation
Explanation
All of the options, except cementing the metaphyseal portion and press fitting the keel of the tibial component, have been shown to create strong and long-lasting constructs; however, cementing of both the platform and the keel offers the most predictable solution. Cementing the platform and not the keel has been shown to have a higher loosening rate than the more traditional methods of fully cementing or using screws to augment fixation.
References:
- Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 457-468.
Question 50High Yield
A 72-year-old woman has had progressively increasing pain in the right knee for the past 6 months. She denies any trauma and has no pain in any other joints, but she notes occasional swelling in the knee and a catching sensation. Figures 31a and 31b show the plain radiographs and Figure 31c shows the MRI scan. Treatment should consist of
Explanation
Explanation
31b 31c The plain radiographs show a defect in the lateral femoral condyle and narrowing of the lateral joint space. The MRI scan shows a lesion consistent with osteonecrosis of the lateral femoral condyle. The treatment alternatives for this condition are an osteotomy or a total knee replacement, but a total knee replacement is the treatment of choice for a 72-year-old patient. Arthroscopy or an osteochondral bone graft will not address her symptoms. A valgus osteotomy will exacerbate the problem by overloading the lateral joint, which is already diseased. Lotke PA, Ecker ML: Osteonecrosis of the knee. J Bone Joint Surg Am 1988;70:470-473.
References:
- Ecker ML, Lotke PA: Osteonecrosis of the medial part of the tibial plateau. J Bone Joint Surg Am 1995;77:596-601.
Question 51High Yield
An axial T1-weighted MRI scan of the pelvis is shown in Figure 35. Which of the following structures is enclosed by the circle?
Explanation
The obturator vessels and nerve pass along the lateral pelvic wall along the true pelvic brim (nerve lies anterior to the vessels and lies on the obturator internus muscle) and descend into the obturator groove at the upper portion of the obturator foramen. Higuchi T: Normal anatomy and magnetic resonance appearance of the pelvis, in Takahashi HE, Morita T, Hotta T, et al (eds): Operative Treatment of Pelvic Tumors. Tokyo, Japan, Springer-Verlag, 2003, pp 4-21.
Question 52High Yield
A 14-year-old girl has had mild pain and nail deformity of the great toe for the past 4 months. A radiograph is shown in Figure 50. What is the most likely etiology of the lesion?
Explanation
Explanation
The lesion is typical of a subungual exostosis, which is most often found on the medial aspect of the great toe in children and young adults. The diagnosis is confirmed on radiographs and usually requires excision for relief. Lokiec F, Ezra E, Krasin E, Keret D, Wientraub S: A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop 2001;21:76-79. Letts M, Davidson D, Nizalik E: Subungual exostosis: Diagnosis and treatment in children. J Trauma 1998;44:346-349.
References:
- Davis DA, Cohen PR: Subungual exostosis: Case report and review of the literature. Pediatr Dermatol 1996;13:212-218.
Question 53High Yield
A 73-year-old man reports increasing back and lower extremity pain. A bone scan is shown in Figure 31. What is the most likely diagnosis?
Explanation
Explanation
The bone scan reveals lesions throughout the skeleton. The patient's age, gender, and pain pattern are consistent with metastatic prostate cancer. Multiple myeloma typically does not have enough osteoblastic activity to produce this bone scan. The patient's age is not consistent with metastatic neuroblastoma (a pediatric disease). Polyostotic fibrous dysplasia may involve multiple active lesions in younger patients but does not have such a widespread distribution of lesions. Hodgkin's lymphoma can involve bone, but the widespread discrete appearance on this bone scan is most consistent with metastatic prostate cancer. In a patient with widespread bone metastases from prostate cancer, bisphosphonates may play a critical role in treatment by decreasing pain and the number of fractures. Roudier MP, Vesselle H, True LD, Higano CS, Ott SM, King SH, Vessella RL: Bone histology at autopsy and matched bone scintigraphy findings in patients with hormone refractory prostate cancer: The effect of bisphosphonate therapy on bone scintigraphy results. Clin Exp Metastasis 2003;20:171-180.
References:
- Sartor O: Radioisotopic treatment of bone pain from metastatic prostate cancer. Curr Oncol Rep 2003;5:258-262.
Question 54High Yield
A 45-year-old man has persistent hindfoot pain that is aggravated by weight-bearing activities. History reveals that he sustained a calcaneus fracture 2 years ago, and he underwent a subtalar fusion 1 year ago. Examination reveals tenderness in the sinus tarsi and across the transverse tarsal joint. A plain radiograph and a CT scan are shown in Figures 24a and 24b. A technetium Tc 99m bone scan reveals uptake at the subtalar joint and at the transverse tarsal joints. Management should now consist of
Explanation
Explanation
24b The patient has a nonunion at the subtalar joint because of poor preparation of the arthrodesis site with incomplete removal of the articular cartilage. Clinically, he has arthritis at the transverse tarsal joint. Casting with a bone stimulator is not expected to result in a union of the subtalar arthrodesis. To address both the subtalar nonunion and the transverse tarsal joint arthritis, revision of the subtalar arthrodesis and conversion to a triple arthrodesis is the preferred option. Graves SC, Mann RA, Graves KO: Triple arthrodesis in older adults: Results after long-term follow-up. J Bone Joint Surg Am 1993;75:355-362. Haddad SL, Myerson MS, Pell RF IV, Schon LC: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499. Sangeorzan BJ, Smith D, Veith R, Hansen ST Jr: Triple arthrodesis using internal fixation in treatment of adult foot disorders. Clin Orthop 1993;294:299-307. Sangeorzan BJ: Salvage procedures for calcaneus fractures. Instr Course Lect 1997;46:339-346.
References:
- Wapner KL: Triple arthrodesis in adults. J Am Acad Orthop Surg 1998;6:188-196.
Question 55High Yield
Total hip arthroplasty in a patient with a long-standing hip fusion on the contralateral side is most likely to result in
Explanation
Explanation
Contralateral total hip arthroplasty in patients with hip fusions results in a 40% higher rate of mechanical failure and loosening. During gait, motion of the contralateral hip is increased and more time is spent bearing weight on that hip. In patients with hip fusions, gait efficiency is only 53%, with a greater rate of oxygen consumption. Garvin KL, Pellicci PM, Windsor RE, et al: Contralateral total hip arthroplasty or ipsilateral total hip arthroplasty in patients who have long-standing fusion of the hip. J Bone Joint Surg Am 1989;71:1355-1362. Gore DR, Murray MP, et al: Walking patterns of men with unilateral surgical hip fusion. J Bone Joint Surg Am 1975;57:759-765.
References:
- Romness DW, Morrey BF: Total knee arthroplasty in patients with prior ipsilateral hip fusion. J Arthroplasty 1992;7:63-70.
Question 56High Yield
A full-term newborn has webbing at the knees, rigid clubfeet, a Buddha-like posture of the lower extremities, and no voluntary or involuntary muscle action at and below the knees. Radiographs of the spine and pelvis reveal an absence of the lumbar spine and sacrum. What maternal condition is associated with this diagnosis?
Explanation
The history, physical examination, and radiographic findings are consistent with type IV sacral agenesis or caudal regression syndrome. These children are born with no lumbar spine or sacrum. The T12 vertebra is often prominent posteriorly. Popliteal webbing and knee flexion contractures are common with this diagnosis. There is a higher incidence of this diagnosis when the mother has diabetes mellitus. Maternal drug abuse and alcoholism can produce phenotypically unique children but without the findings described here. Maternal idiopathic scoliosis is not associated with caudal regression syndrome. Chan BW, Chan KS, Koide T, et al: Maternal diabetes increases the risk of caudal regression caused by retinoic acid. Diabetes 2002;51:2811-2816.
Question 57High Yield
An 18-year old man has a simple oblique fracture of the humeral shaft that requires surgical stabilization to maintain reduction and facilitate mobilization. Which of the following methods will provide the best outcome?
Explanation
Explanation
The patient has a simple fracture pattern that can be reduced anatomically and stabilized with absolute stability by interfragmental compression and protection plating. This will guarantee a 95% to 98% union rate with no radial nerve palsy. Intramedullary nailing does not equal these results in a simple fracture pattern in the humerus. Bridge plating is indicated for multifragmented fracture patterns when anatomic reduction and absolute stability cannot be achieved. External fixation is reserved for severe open fractures. Chapman JR, Henley MP, Agel J, Benca PJ: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166. Farragos AF, Schemitsch EH, McKee MD: Complications of intramedullary nailing for fractures of the humeral shaft: A review. J Orthop Trauma 1999;13:258-267.
References:
- Modabber M, Jupiter JB: Operative management of diaphyseal fractures of the humerus: Plate versus nail. Clin Orthop 1998;347:93-104.
Question 58High Yield
What is the most common complaint in patients with a developmental radial head dislocation?
Explanation
Explanation
Developmental dislocation of the radial head most frequently presents as a painless mass over the posterior aspect of the elbow. Patients do not have feelings of elbow subluxation but may report pain or clicking. Limitation of motion is most frequently found in the pronation and supination arc rather than in flexion and extension. Lloyd-Roberts GC, Bucknill TM: Anterior dislocation of the radial head in children-etiology: Natural history and management. J Bone Joint Surg Am 1977;58:402.
References:
- Hamilton W, Parks JC II: Isolated dislocation of the radial head without fracture of the ulna. Clin Orthop Relat Res 1973;97:94-96.
Question 59High Yield
A 10-year-old child with cerebral palsy undergoes bilateral hamstring lengthening for severe knee flexion contractures, and knee immobilizers are applied postoperatively. Examination at the initial postoperative check 2 hours after surgery reveals that she can dorsiflex her toes on the right foot, but not on the left foot. The physician should now
Explanation
Explanation
Children with cerebral palsy are often difficult to examine. However, this patient clearly has a peroneal nerve deficit, most likely from the acute stretch after the hamstring lengthening. The nerve has the best chance of recovery if it is relaxed by flexing the knee. Once the nerve has recovered, gradual knee extension can be accomplished. Aspden RM, Porter RW: Nerve traction during correction of knee flexion deformity: A case report and calculation. J Bone Joint Surg Br 1994;76:471-473.
References:
- Heydarian K, Akbarnia BA, Jabalameli M, Tabador K: Posterior capsulotomy for the treatment of severe flexion contractures of the knee. J Pediatr Orthop 1984;4:700-704.
Question 60High Yield
What is the most common organism found following a nail puncture wound through tennis shoes in a host without immunocompromise?
Explanation
The association of a nail puncture wound with a gram-negative infection (Pseudomonas aeruginosa) has been attributed to the local environmental factors in shoes. Osteomyelitis is rare, occurring only in about 1% of patients. Tetanus prophylaxis should be given if it is not up to date. While the remaining organisms listed are periodically involved, they are more common in patients who are immunocompromised or who have diabetes mellitus. Therefore, obtaining a culture of the infected wound is appropriate in such individuals because of the multifactorial nature of the infection. Green NE, Bruno J III: Pseudomonas infections of the foot after puncture wounds. South Med J 1980;73:146-149.
Question 61High Yield
When using highly cross-linked ultra-high molecular weight polyethylene as an articulating surface for total knee arthroplasty, what property of the material raises concern?
Explanation
Explanation
The decreased mobility of the polymer chains from cross-linking leads to decreased volumetric wear but also to decreases in ductility and fatigue resistance. Stresses at the knee are higher and varied in the point of application, leading to the concern for fatigue resistance and fracture.
References:
- Koval KJ (ed): Orthopaedic Knowlegde Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 193-199.
Question 62High Yield
When standing, dorsiflexion of the great toe will accentuate
Explanation
Explanation
Dorsiflexion of the great toe will accentuate rigidity of the transverse tarsal articulation. Through the windlass mechanism, dorsiflexion of the great toe tightens the plantar fascia, stabilizing the longitudinal arch and placing the foot in supination. Supination makes the talonavicular and calcaneocuboid joints nonparallel, accentuating the rigidity of the transverse tarsal articulation. The heel also tends to go into varus, resulting in obligatory external tibial rotation. Mann RA: Biomechanics of the foot and ankle, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 1-44.
References:
- Hicks JH: The mechanics of the foot: II. The plantar aponeurosis and the arch. J Anat 1954;88:25.
Question 63High Yield
A patient has had a locked posterior dislocation of the shoulder for the past 6 months. After undergoing total shoulder arthroplasty that includes adequate anterior releases and posterior capsulorrhaphy, the patient still exhibits posterior instability intraoperatively. The postoperative rehabilitation regimen should include
Explanation
Achieving stability in chronic locked posterior dislocations of the shoulder remains a difficult challenge. Intraoperative measures include decreased humeral retroversion, anterior releases, and posterior capsular tightening. Postoperative rehabilitation is of equal importance. Immobilization in an external rotation brace (10 degrees to 15 degrees) with the arm at the side for 4 to 6 weeks is recommended to decrease tension in the posterior capsule. When passive range-of-motion exercises are instituted, they should be performed in the plane of the scapula to avoid stress posteriorly. Internal rotation and supine elevation should be avoided for similar reasons. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 64High Yield
A 16-year-old high school football player sustains an injury to the left hip. The avulsed fragment identified by the arrow in Figure 34 represents the origin of which of the following structures?
Explanation
The avulsed fragment represents the origin of the rectus femoris from the anterior inferior iliac spine and the brim of the acetabulum. Avulsion of the anterior inferior iliac spine is much less common than avulsion of the anterior superior iliac spine with its origin of the sartorius. The origin of the gluteus minimus is from the outer cortex of the iliac wing and has not been reported as a source of bony avulsion. The hip capsule is composed of the ischiofemoral and pubofemoral ligaments, in addition to the iliofemoral ligament. The pelvic attachment of the ischiofemoral ligament is from the ischial part of the acetabulum posteriorly, while the pubofemoral ligament attaches to the pubic portion inferiorly. Technically, ligaments do not have origins and insertions as muscle tendon groups do, but have attachment sites. Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Question 65High Yield
Figures 35a and 35b show the axial T2-weighted and coronal T1-weighted MRI scans of a patient who has enlargement of the right thigh. What is the most likely diagnosis?
Explanation
Explanation
35b The images show a large, almost circumferential, mass surrounding the diaphysis of the femur. The intramedullary signal is normal with minimal cortical destruction, both findings that should be abnormal in conventional osteosarcoma and Ewing's sarcoma. There are very low-signal striations representing osteoid formation that would have a sunburst radiographic pattern. This indicates an osteogenic lesion. Myositis ossificans is not indicated because studies would reveal zonal ossification starting in the periphery rather than the more central pattern seen in this patient. This appearance is typical for periosteal osteosarcoma.
References:
- El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 176.
Question 66High Yield
A 42-year-old athletic trainer has a persistent popping sensation about the lateral ankle associated with weakness and pain following a remote injury. Deficiency in what structure directly leads to this pathology?
Explanation
Explanation
The patient has instability of the peroneal tendon. The superior peroneal retinaculum is the primary retaining structure preventing peroneal subluxation. It is a thickening of fascia that arises off the posterior margin of the distal 1 to 2 cm of the fibula and runs posteriorly to blend with the Achilles tendon sheath. The inferior peroneal retinaculum attaches to the peroneal tubercle of the calcaneus and is not involved in this pathology. A deficient groove in the posterior distal fibula may also be a contributing factor in the development of the condition.
References:
- Maffuli N, Ferran NA, Oliva F, et al: Recurrent subluxation of the peroneal tendons. Am J Sports Med 2006;34:986-992.
Question 67High Yield
A 55-year-old man reports increasing weakness in his arms that has progressed to his lower limbs, resulting in frequent tripping and falling. Examination reveals weakness in shoulder abduction and external and internal rotation bilaterally. Fasciculation is noted. He also has weakness in elbow flexion and extension bilaterally, and his grip strength is diminished. An electromyogram and nerve conduction velocity studies show decreased amplitude of compound motor action potential, slightly slowed motor conduction velocity, and denervation signs with decreased recruitment in all extremities. The sensory study is normal. Based on these findings, what is the most likely diagnosis?
Explanation
Explanation
The major determinant of ALS (Lou Gehrig disease) is progressive loss of motor neurons. The loss usually begins in one area, is asymmetrical, and later becomes evident in other areas. The first signs of ALS may include either upper or lower motor neuron loss. Recognition of upper motor neuron involvement depends on clinical signs, but electromyography and nerve conduction velocity studies can help identify lower motor neuron involvement. Electrodiagnostic abnormalities in three or more areas are required to make a definitive diagnosis. The motor unit potentials (MUPs) changes in ALS include impaired MUPs recruitment, unstable MUPs, and abnormal MUPs size and configuration. A number of abnormal spontaneous discharges can occur with ALS, especially fibrillation potentials and fasciculation potentials. In ALS, the motor nerve conduction study will be abnormal, but a co-existing normal sensory study is definitive for this disease. de Carvalho M, Johnsen B, Fuglsang-Frederiksen A: Medical technology assessment: Electrodiagnosis in motor neuron diseases and amyotrophic lateral sclerosis. Neurophysiol Clin 2001;31:341-348. Daube JR: Electrodiagnostic studies in amyotrophic lateral sclerosis and other motor neuron disorders. Muscle Nerve 2000;23:1488-1502.
References:
- Troger M, Dengler R: The role of electromyography (EMG) in the diagnosis of ALS. Amyotroph Lateral Scler Other Motor Neuron Disord 2000;1:S33-S40.
Question 68High Yield
A fracture of the radial head is surgically exposed using a posterolateral approach to the elbow. Once the radial head is exposed, how should the arm be positioned to best protect the posterior interosseous nerve from injury?
Explanation
As long as the dissection stays proximal to the annular ligament, the posterior interosseous nerve is not at risk for injury. However, to ensure that the nerve is as far removed from the surgical field as possible, the forearm should be placed in pronation. Forearm supination of any degree will bring the nerve toward the surgical field. A neutral position of the forearm or elbow extension with wrist extension will not protect the posterior interosseous nerve. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, p 100.
Question 69High Yield
A 20-year-old man sustained an isolated displaced type II odontoid fracture in a motor vehicle accident. He is neurologically intact. Treatment consists of placement in halo traction, and the fracture is reduced. What is the next most appropriate step in treatment?
Explanation
The traditional treatment of a reduced type II fracture is a halo vest. A 20-year-old man will tolerate a halo vest better than the elderly or women. Anterior screw fixation has gained increasing support; however, it too has risks and requires a significant learning curve. More recently, C1 lateral mass screws have become more popular. The long-term results and benefits have not yet been determined. Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 193. Kiovikko MP, Kiuru MJ, Koskinen SK, et al: Factors associated with nonunion in conservatively-treated type-II fractures of the odontoid process. J Bone Joint Surg Br 2004;86:1146-1151. Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, p 1091.
Question 70High Yield
Figure 3 shows the radiograph of an asymptomatic 10-year-old boy. Management should consist of
Explanation
Asymptomatic spondylolysis in a child or adolescent should be observed for the possible development of spondylolisthesis, but no other active intervention is needed. The initial treatment of choice for symptomatic spondylolysis includes rest and activity modifications, nonsteroidal anti-inflammatory drugs, physical therapy, bracing, and casting. Immobilization with a TLSO or pantaloon spica cast may permit healing of an acute pars fracture. Rarely, surgical treatment may be necessary. Surgical options include posterolateral L5-S1 fusion or direct repair of the pars defect. Pizzutillo PD, Hummer CD III: Nonoperative treatment for painful adolescent spondylolysis or spondylolisthesis. J Pediatr Orthop 1989;9:538-540.
Question 71High Yield
A 21-year-old woman who was wearing a seat belt sustained an injury of the thoracolumbar junction in a motor vehicle accident. The AP radiograph shows widening between the L1 and L2 spinous processes, and the CT scan shows the empty facet sign at this level. The initial evaluation should include
Explanation
The patient has a flexion-distraction injury of the thoracolumbar spine that is often associated with wearing a seat belt. The fracture has a high risk of associated intra-abdominal injury; therefore, the initial evaluation should include a CT of the abdomen. The most common visceral injury is to the bowel. Smith WS, Kaufer H: Patterns and mechanisms of lumbar injuries associated with lap seat belts. J Bone Joint Surg Am 1969;51:239-254.
Question 72High Yield
Figure 40 shows the radiograph of a 30-year-old woman who has a painful elbow. Examination reveals a deformed skull, multiple cafe-au-lait spots, and bone deformities. What is the most likely diagnosis?
Explanation
Findings in patients with McCune-Albright syndrome include polyostotic fibrous dysplasia, multiple cafe-au-lait spots, and precocious puberty. The bone changes in NF-1 resemble nonossifying fibromas, not fibrous dysplasia. NF-2 has little bony change with typical ocular abnormalities. Paget's disease occurs in older individuals and does not present with cafe-au-lait spots. Ollier's disease (multiple enchondromatosis) may show bone changes but not the other findings. Albright F, Butler AM, Hampton AO, et al: Syndrome characterized by osteitis fibrosa disseminata, areas of pigmentation and endocrine dysfunction with precocious puberty in females. N Engl J Med 1937;216:727-746. Danon M, Robboy SJ, Kim S, Scully R, Crawford JD: Cushing syndrome, sexual precocity, and polyostotic fibrous dysplasia (Albright syndrome) in infancy. J Pediatr 1975;87:917-921.
Question 73High Yield
Figure 17 shows the AP radiograph of a 5-year old child who has mild short stature and a painless bilateral gluteus medius lurch. Initial work-up should include
Explanation
Explanation
Bilateral flattening of the femoral heads suggests multiple epiphyseal dysplasia; therefore, a skeletal survey is indicated to look for involvement of other epiphyses. Unilateral flattening of the femoral head would suggest Legg-Perthes disease. Sponseller PD: Skeletal dysplasias, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 269-270.
References:
- Herring JA: Tachdjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 689-691.
Question 74High Yield
When performing a bunionectomy with a release of the lateral soft-tissue structures, the surgeon is cautioned against releasing the conjoined tendon that inserts along the lateral base of the proximal phalanx of the great toe. This conjoined tendon is made up of what two muscles?
Explanation
Owens and Thordardson cautioned surgeons not to release the conjoined tendon from the base of the proximal phalanx of the great toe because of an increased risk of iatrogenic hallux varus. Release of the transverse and oblique heads of the adductor hallucis is largely accomplished by releasing the soft tissue adjacent to the lateral sesamoid, without releasing tissue from the base of the proximal phalanx. The conjoined tendon is made up of the flexor hallucis brevis and the adductor hallucis. Owens S, Thordardson DB: The adductor hallucis revisited. Foot Ankle Int 2001;22:186-191.
Question 75High Yield
Figures 13a and 13b show the MRI scans of a 70-year-old patient who has a posterior calf mass. Examination reveals that the mass extends to the midcalf level. A biopsy specimen reveals a high-grade soft-tissue sarcoma. Metastatic work-up shows no lesions. Management should consist of

Explanation
Soft-tissue sarcomas generally are treated with radiation therapy and wide surgical resection. In this patient, involvement of most of the posterior calf compartment and circumferential involvement of the posterior tibial and peroneal neurovascular bundle makes limb salvage impractical. Any attempt at wide surgical resection would leave a poorly functioning limb with questionable surgical margins. A high below-knee amputation would be the best option. Radiation therapy alone is contraindicated. Lindberg RD, Martin RG, Romsdahl MM, et al: Conservative surgery and post-operative radiotherapy in 300 adults with soft tissue sarcoma. Cancer 1981;47:2391-2397. Sim FT, Frassica FS, Frassica DA: Soft tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 76High Yield
What structure is most at risk for injury from a retractor against the tracheoesophageal junction during an anterior approach to the cervical spine?
Explanation
Although any of these structures can be injured by pressure from the medial blade of a self-retaining retractor, the recurrent laryngeal nerve runs cephalad in the interval between the esophagus and trachea and is vulnerable to pressure if caught between the retractor and an inflated endotracheal tube balloon. Ebraheim NA, Lu J, Skie M, et al: Vulnerability of the recurrent laryngeal nerve in the anterior approach to the lower cervical spine. Spine 1997;22:2664-2667.
Question 77High Yield
Examination of a 5-year-old boy with amyoplasia shows a flexion contracture of 70 degrees of the right knee. The active arc of motion is from 70 degrees to 90 degrees, and the opposite knee has a flexion contracture of 10 degrees. Both hips are dislocated with flexion contractures of 10 degrees, passive hip motion is from 10 degrees to 90 degrees of flexion, and the feet are plantigrade and easily braceable. Despite a daily stretching program, the parents and physical therapists note that it is increasingly difficult for him to walk because of the flexion contracture of the right knee. Management of the knee flexion contracture should now include
Explanation
Most children with amyoplasia are ambulatory and when a decrease in function occurs because of a severe contracture, it must be addressed. A radical posterior soft-tissue release, including the posterior knee capsule and often the collateral ligaments and the posterior cruciate ligament, is needed to obtain extension. After the age of 1 year, aggressive physical therapy will do little to correct a contracture. Botulinum toxin A is indicated for spasticity and is contraindicated with severe contractures. Supracondylar femoral extension osteotomy works well, but will remodel at an average rate of 1 degree per month, which is not considered ideal in a young patient. Gradual correction with a circular ring external fixator is an option, but a soft-tissue release will also most likely be needed for a contracture of this severity. Sarwark JF, MacEwen GD, Scott CI Jr: Amyoplasia (a common form of arthrogryposis). J Bone Joint Surg Am 1990;72:465-469. DelBello DA, Watts HG: Distal femoral extension osteotomy for knee flexion contracture in patients with arthrogryposis. J Pediatr Orthop 1996;16:122-126.
Question 78High Yield
Following an episode of transient quadriplegia in contact sports, an athlete's return to play is absolutely contraindicated when
Explanation
Return to play decisions after traumatic spinal or spinal cord injury are not always clear-cut and often must be made on a patient-by-patient basis. The Torg ratio has been found to have low sensitivity in patients with large vertebral bodies. Abnormal electromyographic studies can persist in the face of normal function and do not define spinal injury. Duration of quadriplegia is not related to anatomic pathology. Findings on MRI scans or contrast-enhanced CT scans consistent with stenosis include lack of a significant cerebrospinal fluid signal around the cord, bony or ligament hypertrophy, or disk encroachment. Based on these findings, return to play should be avoided. Cantu RC, Bailes JE, Wilberger JE Jr: Guidelines for return to contact or collision sport after a cervical spine injury. Clin Sports Med 1998;17:137-146. Herzog RJ, Wiens JJ, Dillingham MF, Sontag MJ: Normal cervical spine morphometry and cervical stenosis in asymptomatic professional football players: Plain film radiography, multiplanar computer tomography, and magnetic resonance imaging. Spine 1991;16:178-186.
Question 79High Yield
Figures 9a and 9b show the radiographs of a 28-year-old woman who sustained a head injury and a closed injury, without soft-tissue compromise, to her right lower extremity in a motor vehicle accident. Appropriate management of the foot injury should include
Explanation
Explanation
9b The displaced talar neck fracture should be treated with open reduction and internal fixation using screws. Closed reduction and casting will not maintain position, and percutaneous pinning is not able to maintain reduction to allow union. External fixation and amputation are not necessary for this injury unless there is severe soft-tissue loss.
References:
- Adelaar RS: Fractures of the talus. Instr Course Lect 1990;39:147-156.
Question 80High Yield
The plate seen in Figure 48a was applied to the fracture seen in Figure 48b, and is functioning in what capacity?

Explanation
A Weber type B ankle fracture occurs with a supination external rotation mechanism of injury. The fibula generally fails with a spiral fracture pattern. The lag screws provide compression, and the plate acts to neutralize rotational and angular bending forces. A buttress plate resists vertical shear forces. A tension band is used over areas that may fail in tension, such as an olecranon fracture. Compression is provided by the lag screws, and distraction is again resisted by the lag screws.
Question 81High Yield
To avoid an injury to the L5 nerve root when placing an S1 sacroiliac screw, what area of the sacrum should be avoided on the lateral C arm image shown in Figure 21?
Explanation
Explanation
Safe placement of a sacroiliac screw depends on excellent imaging of and understanding of pelvic anatomy. There are variations in the anatomy of the upper sacrum. Patients with dysplasia of the sacrum can have "in-out-in" screws placed that exit the ilium, pass anterior to the sacral ala, and injure the L5 nerve root. To make sure that this does not occur, a lateral image of the sacrum is used to ensure that the starting point is in the "safe zone." The starting point needs to be below the iliac cortical density (ICD) which parallels the sacral alar slope. This will prevent placing screws into the recessed ala of patients with a dysplastic sacrum. The triangular area anterior to the ICD is labeled A in the figure, B represents the sacral canal, C is S2, D is the anterior border of the sacrum, and E represents the greater sciatic notches. Routt ML Jr, Simonian PT, Agnew SG, et al: Radiographic recognition of the sacral alar slope for optimal placement of iliosacral screws: A cadaveric and clinical study. J Orthop Trauma 1996;10:171-177.
Question 82High Yield
Figure 40 shows the AP radiograph of a 55-year-old man who reports left knee pain. Which of the following conditions is least likely to produce this radiographic presentation?
Explanation
The radiograph reveals densities within the articular cartilage of the knee commonly referred to as chondrocalcinosis. The term chondrocalcinosis refers to the presence of calcium-containing crystals detected as radiodensities in cartilage. Calcium-containing crystals other than calcium pyrophosphate dihydrate may also deposit in articular cartilage and menisci, producing both radiographically detectable densities in cartilage and joint inflammation or degeneration. Hemochromatosis, alkaptonuria (ochronosis), and Wilson's disease are characterized by cellular deposition of iron, calcium, and copper ions, respectively, into various tissues including articular cartilage and can give this appearance. Septic arthritis does not usually cause chondrocalcinosis. Klippel JH (ed): Primer on the Rheumatic Diseases, ed 11. Atlanta, GA, Arthritis Foundation, 1997, pp 226-229 and 328-331.
Question 83High Yield
A patient who underwent closed reduction of the hips as an infant now reports pain. An abduction internal rotation view shows an incongruous joint. Based on the findings shown in Figure 3, what is the most appropriate type of pelvic osteotomy for the right hip?
Explanation
Pelvic osteotomies that redirect hyaline cartilage over the femoral head offer the potential for long-term preservation of the hip; however, salvage procedures such as the Chiari osteotomy are indicated in patients without a concentrically reducible hip. Ito and associates reported that moderate dysplasia and moderate subluxation without complete obliteration of the joint space and a preoperative center-edge angle of at least minus 10 degrees are desirable selection criteria. Ohashi H, Hirohashi K, Yamano Y: Factors influencing the outcome of Chiari pelvic osteotomy: A long-term follow-up. J Bone Joint Surg Br 2000;82:517-525.
Question 84High Yield
An 18-month-old boy has 45 degrees of kyphosis in the thoracolumbar spine secondary to type I congenital kyphosis. Examination reveals that he is neurologically intact, and an MRI scan shows no evidence of intraspinal pathology. Management should consist of
Explanation
Explanation
Surgery is indicated for congenital kyphosis once the deformity reaches a certain size or if significant progression is documented. In a young patient with a relatively small deformity, the treatment of choice is isolated in situ posterior fusion and postoperative immobilization. If an adequate posterior fusion can be obtained, an epiphyseodesis effect can be generated, allowing the remaining anterior growth to cause some correction. Because there is no evidence of neurologic compression and the deformity is less than 50 degrees, anterior surgery is not indicated. There is no role for bracing in the management of congenital kyphosis. Winter RB: Congenital Deformities of the Spine. New York, NY, Thieme-Stratton, 1983, pp 229-261.
References:
- Winter RB, Moe JH: The results of spinal arthrodesis for congenital spinal deformity in patients younger than five years old. J Bone Joint Surg Am 1982;64:419-432.
Question 85High Yield
Which of the following is considered the best cementless acetabular reconstruction method when planning for total hip arthroplasty in a patient with developmental dysplasia of the hip (DDH)?
Explanation
Anatomic positioning of the acetabular component has been shown to be the optimal position for reconstruction of the acetabulum in total hip arthroplasty for DDH. The use of medialized component positioning has been shown to be successful at maximizing the host bone coverage and minimizing the use of bone graft to structurally support the acetabular component. A small acetabular component can be used successfully as long as the femoral head is also reduced in size to maintain the thickness of the acetabular polyethylene. High and lateral positioning for the acetabular reconstruction will result in an increase in the joint reaction forces. In addition, a high and lateral placement will not provide adequate bone to stabilize the reconstruction. Numair J, Joshi AB, Murphy JC, Porter ML, Hardinge K: Total hip arthroplasty for congenital dysplasia or dislocation of the hip: Survivorship analysis and long-term results. J Bone Joint Surg Am 1997;79:1352-1360. Dorr LD, Tawakkol S, Moorthy M, Long W, Wan Z: Medial protrusio technique for placement of a porous-coated, hemispherical acetabular component without cement in a total hip arthroplasty in patients who have acetabular dysplasia. J Bone Joint Surg Am 1999;81:83-92.
Question 86High Yield
What is the most common secondary malignancy arising in pagetic bone?
Explanation
The incidence of malignant transformation or the formation of a secondary malignancy in pagetic bone is estimated to be less than 1%. Osteosarcoma is the most common secondary malignancy, followed by fibrosarcoma and chondrosarcoma. Ewing's sarcoma arising in pagetic bone has not been reported. Grimer RJ, Carter SR, Tillman RM, et al: Osteosarcoma of the pelvis. J Bone Joint Surg Br 1999;81:796-802.
Question 87High Yield
A 19-year-old college student reports a 1-week history of wrist pain following an intramural rugby match. A PA radiograph is shown in Figure 6. He denies any prior wrist injury. What is the best course of action?
Explanation
The patient has a scaphoid fracture involving the proximal pole. Surgical treatment is recommended for such fractures because of the prolonged period of cast immobilization necessary and the increased risk of delayed union, nonunion, and/or osteonecrosis with nonsurgical management. A cannulated compression screw, inserted in the central scaphoid via a dorsal approach, is biomechanically advantageous and provides greater stability for fracture healing than Kirschner wires. Recently, good outcomes have been reported with arthroscopic-assisted percutaneous fixation of nondisplaced or minimally displaced scaphoid fractures. Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210. Chan KW, McAdams TR: Central screw placement in percutaneous screw scaphoid fixation: A cadaveric comparison of proximal and distal techniques. J Hand Surg Am 2004;29:74-79. Bedi A, Jebson PJ, Hayden RJ, et al: Internal fixation of acute non-displaced scaphoid waist fractures via a limited dorsal approach: An assessment or radiographic and functional outcomes. J Hand Surg Am 2007;32:326-333.
Question 88High Yield
A 25-year-old carpenter falls on his outstretched arm. What physical finding best correlates with the lesion seen on the MRI scan shown in Figure 3?
Explanation
Explanation
The MRI scan shows disruption of the subscapularis muscle. Subscapularis rupture is associated with weakness in internal rotation as shown with a positive lift-off test as described by Gerber and Krushell. The belly press test also has been shown to be a useful clinical test for this problem. Weakness in external rotation and abduction is more consistent with supraspinatus and infraspinatus tears. Deltoid atrophy is associated with an axillary nerve injury. Loss of biceps contour is associated with rupture of the long head of the biceps. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
References:
- Greis PE, Kuhn JE, Schultheis J, et al: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Question 89High Yield
A 22-month-old child has scrapes and bruises on his head and a severe deformity of the forearm after being thrown from a car as an unrestrained passenger in a motor vehicle accident. Examination reveals a Glasgow Coma Scale score of 12. Prior to treatment of the forearm, management should include
Explanation
Explanation
As CT scanning has become available, the use of radiographs of the skull has decreased in importance for evaluation of head trauma. The indications for CT scanning for suspected head trauma include any degree of obtundation, focal neurologic deficit, history of a high-velocity injury, amnesia for the injury, progressive headache, persistent vomiting, children younger than age 2 years, serious facial injury, posttraumatic seizure, skull penetration, or a Glasgow Coma Scale score of 13 or less. Evidence of improved outcome with use of steroids in head trauma is lacking. Steroids are useful for increased intracranial pressure caused by brain tumors or abscesses. High-dose IV methylprednisolone is indicated for spinal cord trauma and improves the ultimate degree of recovery of function. When herniation is suspected in a patient with asymmetric neurologic findings or the patient's condition is deteriorating rapidly, a mannitol infusion may be used. Hall DE: Head injuries, in Hoekelman RA (ed): Primary Pediatric Care. St Louis, Mo, Mosby, 1997, pp 1709-1712. Nelson WE, Behrman RE, Kliegman RM (eds): Nelson Essentials of Pediatrics. Philadelphia, Pa, WB Saunders, 1998, p 712.
References:
- Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 123-130.
Question 90High Yield
Figure 20 shows the radiograph of a 21-year-old college basketball player who jammed his left index finger on the rim. He reports pain and tenderness over the dorsum of the distal interphalangeal (DIP) joint. Examination reveals that he is unable to actively extend the DIP joint; however, the skin is intact. Management should consist of
Explanation
Explanation
Mallet fingers without DIP joint subluxation can be treated with extension splinting. Surgical fixation may be necessary in bony mallet injuries when the joint is subluxated. Size of the bony fragment, while often correlating with stability, is not always an indication for fixation. Buddy taping allows motion; therefore, the fragment will not heal in the appropriate position. Intermittent splinting with range-of-motion exercises also will not allow the fragment to heal in the appropriate position. Crawford GP: The molded polyethylene splint for mallet finger deformities. J Hand Surg Am 1984;9:231-237.
References:
- Wehbe MA, Schneider LH: Mallet fractures. J Bone Joint Surg Am 1984;66:658-669.
Question 91High Yield
A 61-year-old man has a symptomatic bunionette that is refractory to nonsurgical management. A radiograph is shown in Figure 6. What is the optimal surgical correction?
Explanation
The patient has a bunionette with a large 4-5 intermetatarsal angle. This requires not only ostectomy of the lateral prominence but metatarsal osteotomy to decrease the intermetatarsal angle. Excising the head results in a flail joint and creates the possibility of a transfer lesion. Condylectomy can reduce plantar pressures but does not address the bunionette. The joint surface is well maintained, thus there are no indications for resection. Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Question 92High Yield
Based on the radiographic findings shown in Figure 41, which of the following wrist ligaments is most likely disrupted?
Explanation
The radiograph shows a diastasis of the scapholunate interval, caused by certain failure of the scapholunate interosseous ligament. The lunotriquetral interosseous ligament stabilizes the lunotriquetral joint. The long radiolunate ligament originates in the volar radius and inserts in the lunate. The short radiolunate ligament originates on the ulnar margin of the radius and inserts on the ulnar margin of the lunate. The ulnolunate ligament originates at the ulnar styloid base and inserts on the volar aspect of the lunate. Linscheid RL, Dobyns JH, Beabout JW, et al: Traumatic instability of the wrist: Diagnosis, classification, and pathomechanics. J Bone Joint Surg Am 1972;54:1612-1632. Mayfield JK, Johnson RP, Kilcoyne RK: Carpal dislocations: Pathomechanics and progressive perilunar instability. J Hand Surg Am 1980;5:226-241.
Question 93High Yield
Based on the radiograph shown in Figure 4, the innervation of what muscle is most at risk with total hip arthroplasty?
Explanation
The radiograph reveals a Crowe IV deformity in a patient with developmental dysplasia of the hip. If hip arthroplasty is performed, then some degree of limb lengthening is anticipated. Excessive limb lengthening can result in sciatic nerve palsy in these patients. The peroneal branch of the sciatic nerve is most often affected. Of the muscles listed, only the extensor hallucis longus is innervated by the peroneal branch of the sciatic nerve. Eggli S, Hankemayer S, Muller ME: Nerve palsy after leg lengthening in total replacement arthroplasty for developmental dysplasia of the hip. J Bone Joint Surg Br 1999;81:843-845.
Question 94High Yield
The posterior circumflex artery provides blood supply to what portion of the proximal humerus?
Explanation
Explanation
The posterior circumflex artery provides blood supply only to the posterior portion of the greater tuberosity and a small posteroinferior portion of the humeral head. The humeral head is supplied primarily by the anterolateral ascending branch of the anterior circumflex artery; the terminal branch of this artery is termed the arcuate artery. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 267-274.
References:
- Gerber C, Schneeberger AG, Vinh TS: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
Question 95High Yield
The 5-year outcome for patients with sciatica secondary to lumbar disk herniation shows which of the following results?
Explanation
Explanation
Atlas and associates, in the Maine Lumbar Spine Study, reported that overall, patients treated initially with surgery reported better outcomes. By 5 years, 19% of surgical patients had undergone at least one additional lumbar spine operation, and 16% of nonsurgical patients had opted for at least one lumbar spine operation. At the 5-year follow-up, 70% of patients initially treated surgically reported improvement in their predominant symptom (back or leg pain) versus 56% of those initially treated nonsurgically. They also noted that there was no difference in the proportion of patients receiving disability compensation at the 5-year follow-up.
Question 96High Yield
Acetaminophen is an antipyretic medication. It exerts its pharmacologic effects by inhibiting which of the following enzymes?
Explanation
Acetaminophen inhibits prostaglandin E2 production via IL-1 B, without affecting cyclooxygenase-2 enzymatic activity. The therapeutic concentrations of acetaminophen induce an inhibition of IL-1 B-dependent NF-kappa B nuclear translocation. The selectivity of this effect suggests the existence of an acetaminophen-specific activity at the transcriptional level that may be one of the mechanisms through which the drug exerts its pharmacologic effects. Acetaminophen does not affect any of the other enzymes named above.
Question 97High Yield
A 45-year-old man who is a smoker has a significant hemothorax and bilateral closed femoral fractures. On insertion of a chest tube, 1,100 mL of blood was returned. He has had 75 mL of chest tube output over the last 2 hours while being resuscitated in the ICU. His base deficit is now 2 and his urine output has been 3 mL/kg over the last hour. What is the next most appropriate step in management?
Explanation
Explanation
Although this patient had a hemothorax, the bleeding has stopped and he has been resuscitated to a euvolemic status with a small base deficit and good urine output. External fixation of both femurs is an option but an unnecessary step in the treatment algorithm. Nork SE, Agel J, Russell GV, et al: Mortality after reamed intramedullary nailing of bilateral femur fractures. Clin Orthop Relat Res 2003;415:272-278.
Question 98High Yield
Venous thrombolembolism is a common complication following total hip and total knee arthroplasty; therefore, prophylaxis is deemed efficacious. Several studies on low-molecular-weight heparin (LMWH) have shown which of the following findings?
Explanation
Prophylactic LMWH is associated with a risk of bleeding complications, especially if administered too soon after surgery. The risk of major bleeding is 0.3% for control, 0.4% for aspirin, 1.3% for warfarin, 1.8% for LMWH, and 2.6% for unfractionated heparin. Colwell and associates conducted a prospective, randomized trial on over 1,500 total hip arthroplasty patients. Overall, the risk of clinically apparent venous thrombolembolism was 3.6% for LMWH and 3.7% for warfarin. LMWH acts in several sites of the coagulation cascade, with its principal action being inhibition of factor 10a. Thrombocytopenia is less common with LMWH than with unfractionated heparin. The use of LMWH is a relative contraindication with indwelling epidural anesthesia. Colwell CW Jr, Collis DK, Paulson R, et al: Comparison of enoxaparin and warfarin for the prevention of venous thromboembolic disease after total hip arthroplasty:. Evaluation during hospitalization and three months after discharge. J Bone Joint Surg Am 1999;81:932-940.
Question 99High Yield
In a postganglionic brachial plexus lesion at Erb's point (point of formation of the upper trunk by the C5 and C6 nerve roots), which of the following nerves will still function normally?
Explanation
Explanation
In a postganglionic injury to the brachial plexus, the rhomboid muscle, innervated by the dorsal scapular nerve, would still be expected to function. This is a useful clinical sign that the brachial plexus lesion is postganglionic as opposed to preganlionic. The musculocutaneous, axillary, and suprascapular nerves are all located distal to Erb's point (the most common location of an upper nerve root brachial plexus injury), and all contain fibers from the C5 and C6 nerve roots. Therefore, these nerves are not expected to function normally following a postganglionic C5 and C6 nerve root injury. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System: Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, pp 28-29.
References:
- Zimmerman NB, Weiland AJ: Assessment and monitoring of brachial plexus injury in the adult, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, JB Lippincott, 1991, vol 2, pp 1273-1283.
Question 100High Yield
Torsional moments about the longitudinal axis of a total hip arthroplasty show what change during stair climbing compared with walking?
Explanation
Explanation
The magnitudes of out-of-plane loads on a total hip replacement during activities of daily living can be substantial. Bergmann and associates studied these forces about two instrumented hip prostheses. They noted that the torsional moment about the hip during stair climbing is twice as high as during slow walking and that similar moments are generated during slow jogging. Higher loads were noted when the patients stumbled without falling. They also noted that the torsional moments observed in vivo were close to or even exceeded the experimentally determined limits of the torsional strength of implant fixations. Hurwitz DE, Andriacchi TP: Biomechanics of the hip, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott Raven, 1998, pp 75-85.
References:
- Bergmann G, Graichen F, Rohlmann A: Is staircase walking a risk for the fixation of hip implants? J Biomech 1995;28:535-553.
You Might Also Like

Previous ChapterOrthopedic Board Review: 100 ABOS, OITE, FRCS MCQs (Mock Ex…
Next Chapter Orthopedic Board Exam Set 703: 100 High-Yield Ortho MCQs

Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon