Orthopedic Board Review: 100 High-Yield MCQs - Set 501
14 Apr 2026
107 min read
94 Views
Key Takeaway
This page provides 100 high-yield orthopedic surgery multiple-choice questions (MCQs) for ABOS, OITE, and FRCS board review. Test your knowledge across core orthopedics, including advanced fracture management. This practice exam helps surgeons master essential concepts and optimize their preparation.
Advanced Surgical Management of Pelvic & Acet...
00:00
Start Quiz
Question 1High Yield
Figures 21a and 21b show the radiograph and CT scan of a 14-year-old patient with thigh pain. The next most appropriate step in management should consist of

Explanation
The radiographs show increased density and reactive bone formation. A faint nidus can be seen on the radiograph but is obvious on the CT scan. The initial therapy for an osteoid osteoma should be oral anti-inflammatory drugs. A biopsy or SPECT bone scan is not indicated because the osteoid osteoma is clearly seen on the CT scan. If the patient fails to respond to nonsurgical therapy, CT-guided radiofrequency ablation or surgical excision is indicated depending on the anatomic location. Frassica FJ, Waltrip RL, Sponseller PD, Ma LD, McCarthy EF Jr: Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 1996;27:559-574. Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid osteoma. J Bone Joint Surg Am 1992;74:179-185.
Question 2High Yield
Which of the following findings is a prerequisite for a high tibial valgus osteotomy for medial compartment gonarthrosis?
Explanation
Explanation
The indications for high tibial valgus osteotomy include a physiologically young age, arthritis confined to the medial compartment, 10 to 15 degrees of varus alignment on weight-bearing radiographs, a preoperative arc of motion of at least 90 degrees, flexion contracture of less than 15 degrees, and a motivated, compliant patient. Contraindications include lateral compartment narrowing of the articular cartilage, lateral tibial subluxation of greater than 1 cm, medial compartment bone loss, ligamentous instability, and inflammatory arthritis. Naudie D, Bourne RB, Rorabeck CH, Bourne TT: The Insall Award: Survivorship of the high tibial valgus osteotomy. A 10- to 22-year followup study. Clin Orthop 1999;367:18-27.
References:
- Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 255-264.
Question 3High Yield
Figure 46 shows the AP radiograph of a patient with right shoulder pain. What is the most likely diagnosis?
Explanation
Posttraumatic osteolysis of the distal portion of the clavicle is a condition that can be a complication of acute or repetitive trauma. The distal end of the clavicle is frayed and resorbed. Resorption may occur after weeks or months. The end of the clavicle may reconstitute over a period of months, or the acromioclavicular joint may remain widened. The differential diagnosis for distal clavicular erosion also includes rheumatoid arthritis, hyperparathyroidism, neoplastic destruction, cleidocranial dysplasia, and pyknodysostosis. Acutely, a type 2 acromioclavicular joint injury does not result in erosion or resorption of the clavicle. Periosteal sleeve injuries radiographically mimic acromioclavicular joint dislocation. Rickets occurs only in childhood.
Question 4High Yield
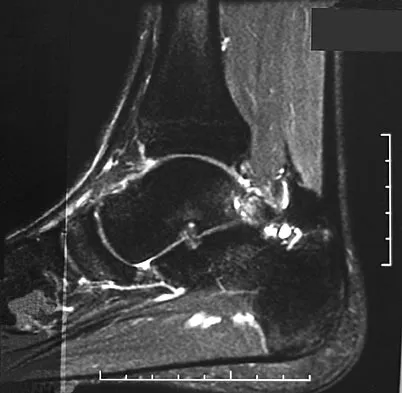
Figures 28a through 28d show the radiographs and MRI scans of a 20-year-old basketball player who sustained an inversion injury to his right ankle. Management should consist of
Explanation
Explanation
28b 28c 28d Osteochondral fractures involving the talar dome have been classified based on radiographic and MRI findings. A nondisplaced and incomplete fracture may be treated effectively with a short leg cast and no weight bearing for 6 weeks. This patient has a complete, separated, and displaced osteochondral fragment involving the midlateral talar dome that will most likely cause pain, mechanical symptoms, and effusion if treated nonsurgically. In addition, there is very little bone remaining on the fragment, making the likelihood of healing with open reduction and internal fixation problematic. The treatment of choice includes arthroscopy, removal of the loose fragment, curettage or drilling of the base, and a rehabilitation program that emphasizes peroneal strengthening, range of motion, and proprioceptive training. Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
References:
- Baker CL, Morales RW: Arthroscopic treatment of tranchondral talar dome fractures: A long-term follow-up study. Arthroscopy 1999;15:197-202.
Question 5High Yield
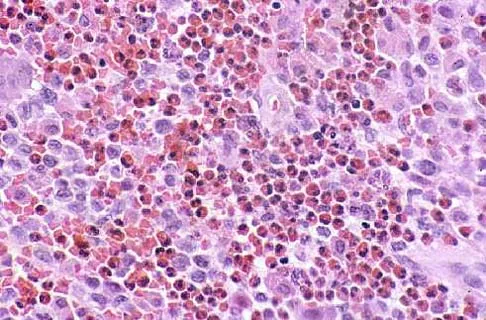
A 12-year-old girl has had progressive left knee pain for the past 4 months. She reports that the pain is unrelated to activity, and she has no history of fever or recent infections. Examination reveals full range of motion of the knee but tenderness along the medial joint line. Plain radiographs and MRI scans are shown in Figures 39a through 39d. A biopsy specimen of the lesion is shown in Figure 39e. Treatment should include
Explanation
Explanation
39b 39c 39d 39e The lesion is a chondroblastoma. The plain radiographs show a well-defined radiolucent lesion in the distal femoral epiphysis of a skeletally immature patient. The margins are well defined, suggesting a benign growth. The epiphysis is an unusual location for bone tumors, except for chondroblastomas. Of all chondroblastomas, 95% are located within the epiphysis. The MRI scans show a punctate appearance that is commonly seen in cartilage lesions. The biopsy specimen shows a chondroid lesion with polygonal chondrocytes. These findings are consistent with a chondroblastoma. The natural history of chondroblastomas is for continued growth and bone destruction if left untreated. Treatment should consist of curettage, with or without the use of physical or chemical adjuvants, and bone grafting.
References:
- Springfield DS, Capanna R, Gherlinzoni F, Picci P, Campanacci M: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Question 6High Yield
Figure 31 shows the AP and lateral radiographs of the elbow of a 56-year-old man with chronic polyarticular rheumatoid arthritis. His function continues to be limited by pain with activities of daily living. Examination shows that his total arc of motion is 110 degrees. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
Explanation
A semiconstrained prosthesis can provide excellent results in carefully selected patients. Because the radiographs show extensive joint destruction with loss of the capitellum and trochlea, a capitellocondylar total elbow (unconstrained) prosthesis is contraindicated. Elbow fusion is poorly accepted, and the radiographs show too much articular destruction for a radial head excision, synovectomy, or interposition arthroplasty to be effective. Ewald FC, Simmons ED Jr, Sullivan JA, et al: Capitellocondylar total elbow replacement in rheumatoid arthritis: Long-term results. J Bone Joint Surg Am 1993;75:498-507.
References:
- Morrey BF, Adams RA: Capitellocondylar total elbow replacement in rheumatoid arthritis. J Bone Joint Surg Am 1992;74:479-490.
Question 7High Yield
Based on the radiographic findings shown in Figure 41, which of the following wrist ligaments is most likely disrupted?
Explanation
The radiograph shows a diastasis of the scapholunate interval, caused by certain failure of the scapholunate interosseous ligament. The lunotriquetral interosseous ligament stabilizes the lunotriquetral joint. The long radiolunate ligament originates in the volar radius and inserts in the lunate. The short radiolunate ligament originates on the ulnar margin of the radius and inserts on the ulnar margin of the lunate. The ulnolunate ligament originates at the ulnar styloid base and inserts on the volar aspect of the lunate. Linscheid RL, Dobyns JH, Beabout JW, et al: Traumatic instability of the wrist: Diagnosis, classification, and pathomechanics. J Bone Joint Surg Am 1972;54:1612-1632. Mayfield JK, Johnson RP, Kilcoyne RK: Carpal dislocations: Pathomechanics and progressive perilunar instability. J Hand Surg Am 1980;5:226-241.
Question 8High Yield
Figure 12 shows the lumbar CT scan of a 24-year-old man who was injured in a snowmobile accident. What is the mechanism of injury?
Explanation
A true compression fracture is a single-column injury that does not create canal compromise. A burst fracture is a two- or three-column injury that disrupts the middle column and thereby narrows the spinal canal. This patient has a burst fracture. The mechanism of injury is usually vertical compression or flexion compression. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-217.
Question 9High Yield
A 59-year-old man reports moderate shoulder pain and very restricted range of motion after undergoing humeral arthroplasty for osteoarthritis 1 year ago. An AP radiograph is shown in Figure 32. Management should now consist of
Explanation
Explanation
The radiograph reveals that an insufficient amount of the proximal humerus was excised in the index procedure, resulting in malalignment of the humeral component, overstuffing of the glenohumeral joint, and glenoid arthritis. It is unlikely that physical therapy or soft-tissue releases alone will be adequate. Revision of the humeral component, recutting of the proximal humerus to allow a more anatomic alignment of the humeral component, appropriate soft-tissue releases, and glenoid arthroplasty will offer the best chance of improvement in this difficult situation. Neer CS II, Kirby RM: Revision of humeral head and total shoulder arthroplasties. Clin Orthop 1982;170:189-195.
References:
- Petersen SA, Hawkins RJ: Revision of failed total shoulder arthroplasty. Orthop Clin North Am 1998;29:519-533.
Question 10High Yield
A 26-year-old man has recurrent right knee pain. Figures 9a and 9b show consecutive sagittal T2-weighted MRI scans, and Figure 9c shows a coronal T1-weighted MRI scan. What is the most likely diagnosis?


Explanation
A discoid meniscus is a large disk-like meniscus. It is seen in the lateral meniscus in 3% of the population; a discoid medial meniscus is much less common. It can be identified on the coronal view by noting meniscal tissue extending into the tibial spine at the intercondylar notch. The average width of a normal meniscus is less than 11 mm. A bow-tie appearance should not be seen on more than two consecutive sagittal images because the conventional thickness of the sagittal slices is 3 mm and the interval between two consecutive slices is 1.5 mm. Two sagittal slices will cover a 9-mm thickness. A discoid meniscus can be diagnosed on the sagittal views by noting a bow-tie appearance on more than two consecutive images. Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Question 11High Yield
New painful paresthesias near the site of the incision after an ulnar nerve transposition is the result of injury to what nerve?
Explanation
Explanation
Branches of the medial antebrachial cutaneous nerve can often be identified during routine ulnar nerve surgery crossing the medial aspect of the elbow. It should be preserved to avoid development of painful paresthesias.
References:
- Dellon AL, Mackinnon SE: Injury to the medial antebrachial cutaneous nerve during cubital tunnel surgery. J Hand Surg Br 1985;10:33-36.
Question 12High Yield
A 42-year-old woman is brought to the emergency department following a motor vehicle accident. She has sustained multiple injuries, and she is intubated and pharmacologically paralyzed. Sagittal cervical CT scans through the right cervical facets, the left cervical facets, and the midline are shown in Figures 12a through 12c, respectively. Definitive management of her cervical injury should consist of
Explanation
Explanation
12b 12c The CT scans reveal an occipital-cervical dissociation with subluxation of the occipitocervical joints bilaterally. Definitive management should consist of an occipital-cervical fusion with instrumentation. Immobilization in a Philadelphia collar is inadequate for this highly unstable injury, and halo immobilization, while affording adequate temporary immobilization, is not appropriate definitive management for this ligamentous injury. The patient does not have an injury at C4-C5 or C6-C7. Jackson RS, Banit DM, Rhyne AL III, et al: Upper cervical spine injuries. J Am Acad Orthop Surg 2002;10:271-280.
Question 13High Yield
Figure 36 shows the radiograph of a 28-year-old man who injured his shoulder in a motocross race. Management should consist of
Explanation
Explanation
Fractures of the distal one third of the clavicle have a high incidence of delayed union (45% to 67%) and nonunion (22% to 33%) with nonsurgical management. Surgical stabilization with tension band techniques or a combination of plate and screw techniques is indicated, especially in young, active patients. In this patient, significant displacement of the fracture implies injury to the coracoclavicular ligaments with a higher risk of delayed union or nonunion. Various surgical treatments have been recommended, but the use of smooth wires is not indicated because of the potential for hardware migration. Jupiter JB, Ring D: Fractures of the clavicle, in Ianotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott, Williams and Wilkins, 1999, pp 709-736.
References:
- Kona J, Bosse MJ, Staehli JW, Rosseau RL: Type II distal clavicle fractures: A retrospective review of surgical treatment. J Orthop Trauma 1990;4:115-120.
Question 14High Yield
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of
Explanation
The radiograph shows excessive thoracic kyphosis (normal 20 degrees to 50 degrees) with multiple contiguous vertebral wedging and end plate irregularity, all consistent with the diagnosis of Scheuermann's kyphosis. The patient is skeletally immature; therefore, there is the potential for progression of the kyphotic deformity. Extension bracing has shown efficacy in the treatment of Scheuermann's kyphosis that measures 50 degrees to 74 degrees, and has actually reduced the curvature permanently in some patients. A thoracolumbosacral orthosis may be used if the apex of kyphosis is at T7 or lower. Indications for surgical treatment are controversial, but spinal fusion most likely should not be considered for a painless kyphosis measuring less than 75 degrees. Murray PM, Weinstein SL, Spratt KF: The natural history and long-term follow-up of Scheuermann kyphosis. J Bone Joint Surg Am 1993;75:236-248. Wenger DR, Frick SL: Scheuermann kyphosis. Spine 1999;24:2630-2639.
Question 15High Yield
A 28-year-old woman has had pain in her hand and mild swelling of the little finger for the past 2 months. A radiograph is shown in Figure 41a, and the biopsy specimen is shown in Figures 41b and 41c. What is the most likely diagnosis?
Explanation
Explanation
41b 41c The radiographic appearance shows a slightly expansile lesion in the proximal phalanx of the fifth digit typical of an enchondroma. There is a stippled appearance within the bone and no evidence of cortical destruction. The biopsy reveals a cartilage lesion with basophilic cytoplasm. There are some hypercellular areas but no evidence of pleomorphism. Enchondromas in the tubular bones of the hand are usually more cellular than their counterparts in the femur and humerus and should not be considered malignant. No other lesions are noted in the radiograph, so a diagnosis of Ollier's disease cannot be made. An osteochondroma is a benign surface cartilage tumor. Brown tumor and osteomyelitis can be differentiated from enchondroma based on the histology. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 225.
References:
- McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 227.
Question 16High Yield
Figure 17 shows the radiograph of an 11-year-old boy with Duchenne muscular dystrophy who has been nonambulatory for the past 2 years. Management of the spinal deformity should consist of
Explanation
Explanation
The presence of any curve greater than 20 degrees in a nonambulatory patient with Duchenne muscular dystrophy is an indication for posterior fusion with instrumentation. Because of progressive cardiomyopathy and pulmonary deficiency, waiting until the curve is larger can increase the risk of pulmonary or cardiac complications during or following surgery. There is some disagreement as to whether all such fusions must extend to the pelvis. Bracing or other nonsurgical management is ineffective and is not indicated in this situation. Sussman M: Duchenne muscular dystrophy. J Am Acad Orthop Surg 2002;10:138-151.
References:
- Mubarek SJ, Morin WD, Leach J: Spinal fusion in Duchenne muscular dystrophy: Fixation and fusion to the sacropelvis? J Pediatr Orthop 1993;13:752-757.
Question 17High Yield
A 45-year-old man who is a smoker has a significant hemothorax and bilateral closed femoral fractures. On insertion of a chest tube, 1,100 mL of blood was returned. He has had 75 mL of chest tube output over the last 2 hours while being resuscitated in the ICU. His base deficit is now 2 and his urine output has been 3 mL/kg over the last hour. What is the next most appropriate step in management?
Explanation
Explanation
Although this patient had a hemothorax, the bleeding has stopped and he has been resuscitated to a euvolemic status with a small base deficit and good urine output. External fixation of both femurs is an option but an unnecessary step in the treatment algorithm. Nork SE, Agel J, Russell GV, et al: Mortality after reamed intramedullary nailing of bilateral femur fractures. Clin Orthop Relat Res 2003;415:272-278.
Question 18High Yield
A 40-year-old man has a palpable mass over the dorsum of the ankle. He reports no history of direct trauma but notes that he sustained a laceration to the middle of his leg 6 weeks ago. Examination reveals a 4-cm x 1-cm mass. T1- and T2-weighted MRI scans are shown in Figures 12a and 12b. An intraoperative photograph and biopsy specimen are shown in Figures 12c and 12d. What is the most likely diagnosis?


Explanation
The findings are most consistent with a rupture of the anterior tibial tendon. The damaged area of tendon should be resected, followed by tendon reconstruction or tenodesis. The histology is not consistent with giant cell tumor of the tendon sheath, gout, or synovial sarcoma. Fibromatosis is characterized by a large number of spindle cells within the collagen background. Otte S, Klinger HM, Loreaz F, Haerer T: Operative treatment in case of closed rupture of the anterior tibial tendon. Arch Orthop Traum Surg 2002;122:188-190.
Question 19High Yield
A 15-year-old boy reports feeling a pop and notes sudden giving way of the left knee while playing basketball. He has immediate pain and swelling in the knee. An AP radiograph is shown in Figure 32. A small avulsion fragment from the lateral tibial margin is the only finding. What is the most likely diagnosis?
Explanation
Explanation
An avulsion fracture from the lateral tibial margin carries the eponym Segond fracture and is pathognomonic for an anterior cruciate ligament (ACL) tear. The fragment is located posterior to Gerdy's tubercle and is superior and anterior to the fibular head. It represents an avulsion of the lateral capsular ligament of the knee and is caused by the same mechanism that causes the ACL tear. The pes anserinus is the insertion point of the medial hamstrings and would not be affected in a lateral avulsion injury. The posterior cruciate ligament may be seen on a lateral view if associated with an avulsion fragment, but a tear of the PCL generally cannot be diagnosed on an AP view. The insertion of the iliotibial band is broad and is unlikely to produce an avulsion injury such as that seen in the radiograph. This view is not consistent with the appearance of a lateral collateral ligament injury. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 533-557.
References:
- Larson RL, Tailon M: Anterior cruciate ligament insufficiency: Principles of treatment. J Am Acad Orthop Surg 1994;2:26-35.
Question 20High Yield
The parents of a previously healthy 3-year-old child report that she refused to walk on awakening. Examination later in the day reveals that the patient can walk but with a noticeable limp. She has a temperature of 99.5 degrees F (37.5 degrees C). Range of motion measurements are shown in Figure 50. An AP pelvis radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3 and an erythrocyte sedimentation rate of 10 mm/h. Management should consist of
Explanation
Explanation
The patient has the typical history and presentation of transient synovitis of the hip, a condition that is more common in children age 2 to 5 years but which may affect children up to 12 years. The discomfort typically is noted on awakening, and the child will refuse to walk. Later in the day, the pain commonly improves and the child can walk but will have a limp. Mild to moderate restriction of hip abduction is the most sensitive range-of-motion restriction. The extent of the evaluation for transient synovitis depends on the intensity and duration of symptoms. Because she has been afebrile for the past 24 hours, observation is the management of choice. In the differential diagnosis of suspected transient synovitis, septic arthritis of the hip is the primary disorder to exclude. Osteomyelitis of the proximal femur also should be considered. In most patients, clinical examination will differentiate of these disorders to a reasonable certainty. Plain radiographs are normal in the early stage of an infectious process. Ultrasonography shows increased fluid in the hip joint in both transient synovitis and septic arthritis. MRI can differentiate the two conditions; however, this test would require general anesthesia and is not required in most patients in this age group. If a child with transient synovitis has a concurrent infectious process such as an upper respiratory tract infection or otitis media, the temperature will most likely be elevated. In this situation, a full evaluation for an infectious process and initiation of IV antibiotics should be considered. This would include radiographs, CBC count, erythrocyte sedimentation rate, blood cultures, aspiration of the hip joint, and IV antibiotics. Del Beccaro MA, Champoux AN, Bockers T, Mendelman PM: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Annals Emerg Med 1992;21:1418-1422.
References:
- Kehl DK: Developmental coxa vara, transient synovitis, and idiopathic chondrolysis of the hip, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 1035-1058.
Question 21High Yield
You are interested in learning a new technique for minimally invasive total knee arthroplasty. The Keyhole Genuflex system seems appealing to you because the instrumentation comes with wireless controls. Which of the following represents an acceptable arrangement?
Explanation
Both the AAOS and AdvaMed, the medical device manufacturer's trade organization, have written guidelines that address potential conflicts of interest regarding interactions between physicians and manufacturer's representatives when it comes to patients' best interest. The AAOS feels that the orthopaedic profession exists for the primary purpose of caring for the patient and that the physician-patient relationship is the central focus of all ethical concerns. When an orthopaedic surgeon receives anything of significant value from industry, a potential conflict of interest exists. The AAOS believes that it is acceptable for industry to provide financial and other support to orthopaedic surgeons if such support has significant educational value and has the purpose of improving patient care. All dealings between orthopaedic surgeons and industry should benefit the patient and be able to withstand public scrutiny. A gift of any kind from industry should in no way influence the orthopaedic surgeon in determining the most appropriate treatment for his or her patient. Orthopaedic surgeons should not accept gifts or other financial support with conditions attached. Subsidies by industry to underwrite the costs of educational events where CME credits are provided can contribute to the improvement of patient care and are acceptable. A corporate subsidy received by the conference's sponsor is acceptable; however, direct industry reimbursement for an orthopaedic surgeon to attend a CME educational event is not appropriate. Special circumstances may arise in which orthopaedic surgeons may be required to learn new surgical techniques demonstrated by an expert or to review new implants or other devices on-site. In these circumstances, reimbursement for expenses may be appropriate. AAOS Standard of Professionalism -Orthopaedist -Industry Conflict of Interest (Adopted 4/18/07), Mandatory Standard numbers 6, 9, 12-15. www3.aaos.org/member/profcomp/SOPConflictsIndustry.pdf The Orthopaedic Surgeon's Relationship with Industry, in Guide to the Ethical Practice of Orthopaedic Surgery, ed 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007. www.aaos.org/about/papers/ethics/1204eth.asp
Question 22High Yield
What joint always remains uninvolved in all stages of scapholunate advanced collapse (SLAC) deformity of the wrist?
Explanation
The development of arthritis in SLAC wrist follows a consistent pattern. Beginning at the radial styloid to the scaphoid articulation, it progresses through the entire radioscaphoid joint and the midcarpal joint. In all stages, the radiolunate joint is spared, which is the basis for a scaphoid excision and four-corner fusion performed as a motion-sparing procedure for treatment of this condition. Wyrick JD: Proximal row carpectomy and intercarpal arthrodesis for the management of arthritis. J Am Acad Orthop Surg 2003;11:277-281. Watson HK, Ballett FL: The SLAC wrist: Scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg Am 1984;9:358-365.
Question 23High Yield
During primary total knee arthroplasty, the trial components are in place. The extensor space is tight, but the flexion space is normal. What is the best gap balancing solution?
Explanation
The first rule of total knee arthroplasty is to restore the joint line to its original location. This will ensure optimal patellofemoral biomechanics and will facilitate ligament balancing. Changes on the tibial side affect both the flexion and extension gaps equally. Changes in femoral component sizing or position affect the flexion gap only. Tibial changes affect both the flexion and extension gaps. To convert a tight extension gap to a normal flexion gap, more distal femur needs to be resected. Vince KG: Revision knee arthroplasty technique. Instr Course Lect 1993;42:325-339.
Question 24High Yield
The first branch of the lateral plantar nerve innervates the
Explanation
The first branch of the lateral plantar nerve innervates the abductor digiti quinti, and more distal branches of the lateral plantar nerve supply the quadratus plantae and the interossei. The medial plantar nerve supplies the abductor hallucis brevis and the flexor digitorum brevis. Pansky B, House EH: Review of Gross Anatomy, ed 3. New York, NY, Macmillan, 1975, pp 464-476.
Question 25High Yield
An 18-year-old high school football player sustains a left posterior hip dislocation that is reduced in the emergency department under IV sedation. Postreduction radiographs reveal a concentric reduction with no evidence of fracture or loose bodies within the joint. What is the most common complication of hip dislocations?
Explanation
Explanation
Traumatic dislocation of the hip in sports injuries is uncommon, and 85% to 92% occur in a posterior direction. In dislocations without fractures, osteonecrosis is the most common complication occurring in 10% to 20% of patients. MRI should be performed at 3 months postreduction to rule out osteonecrosis. Nerve injuries are rare in this setting, and recurrent dislocations are unusual without acetabular fractures. Chondrolysis has been reported as a rare occurrence. Anderson K, Strickland S, Warren R: Hip and groin injures in athletes. Am J Sports Med 2001;29:521-533.
References:
- Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 407-416.
Question 26High Yield
Following a vertebroplasty of L2, cement is noted to protrude directly anterior to the L2 vertebral body. The cement is closest to which of the following structures?
Explanation
At the level of L2, the liver and the vena cava lie to the right. The pancreas and duodenum are anterior to the aorta. The aorta lies in the midline just in front of the vertebral body. Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3. Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 331.
Question 27High Yield
A 22-year-old professional ballet dancer reports a 3-month history of posterior ankle pain that occurs when she changes from a flat foot to pointe (hyperplantar flexed position). Examination does not elicit the pain with forced passive plantar flexion. A radiograph is shown in Figure 8. What is the most likely cause of the pain?
Explanation
Explanation
The most common causes of posterior ankle pain in ballet dancers are flexor hallucis longus tenosynovitis and os trigonum syndrome. Flexor hallucis longus tenosynovitis differs from a symptomatic os trigonum by the absence of pain with forced plantar flexion and the presence of pain with resisted plantar flexion of the great toe. The pain is often felt in the posterior ankle and can be associated with a snapping or triggering sensation. Os trigonum syndrome commonly occurs in ballet dancers who perform in a position of extreme plantar flexion. The pain occurs from entrapment of the os trigonum between the posterior portion of the talus and calcaneus. Hamilton WG, Geppert MJ, Thompson FM: Pain in the posterior aspect of the ankle in dancers: Differential diagnosis and operative treatment. J Bone Joint Surg Am 1996;78:1491-1500.
References:
- Khan K, Brown J, Way S, et al: Overuse injuries in classical ballet. Sports Med 1995;19:341-357.
Question 28High Yield
A 5-year-old girl sustains an isolated injury to the right shoulder area after falling off the monkey bars. Examination reveals intact neurovascular function in the extremity distally, but she is quite uncomfortable. An AP radiograph of the proximal humerus is shown in Figure 24. Her parents state that she is a very talented gymnast. Considering her age and potential athletic career, management should consist of
Explanation
Explanation
In this age group, bayonet apposition can produce very good results. Healing occurs rapidly, and remodeling usually is complete in less than 1 year. All of the other methods have significant risks of complications and are unnecessary for this fracture. Martin RF: Fractures of the proximal humerus and humeral shaft, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 144-148.
References:
- Sanders JO, Rockwood CA Jr, Curtis RJ: Fractures and dislocation of the humeral shaft and shoulder, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 937-939.
Question 29High Yield
Figure 28 shows an AP radiograph of a 54-year-old woman who underwent lumbar laminectomy and fusion at the L4 and L5 levels with placement of a bone stimulator 8 years ago. She also underwent a left total hip arthroplasty 2 years ago; aspiration of that joint now reveals that it is infected with a gram-positive cocci organism. History is also significant for IV drug use and human immunodeficiency virus (HIV). The patient reports fever, chills, and left flank and abdominal pain. Examination reveals significant pain with resisted left hip flexion and passive hip extension. She also has lumbar hyperlordosis. Which of the following studies would best identify the underlying cause of her infection?
Explanation
Explanation
The patient's clinical signs (fever and flank, hip, and abdominal pain) suggest a primary iliopsoas abscess. With an increased patient population who abuse drugs and/or who are HIV-positive, iliopsoas abscess may be more prevalent because of systemic bacterial seeding and may be potentially unrecognized. Diagnostic imaging studies provide a better understanding of the anatomic magnitude of the infection, give concrete confirmation of the diagnosis, and may suggest an underlying cause. Neither standard abdominal radiographs nor ultrasound studies are sensitive enough to be diagnostic of this disease process. CT has been established as the standard study for identifying the underlying cause of this abscess. The hip infection has most likely developed as a result of hematogenous spread from an infected skin lesion from the patient's IV drug use. Santaella RO, Fishman EK, Lipsett PA: Primary vs secondary iliopsoas abscess: Presentation, microbiology, and treatment. Arch Surg 1995;130:1309-1313.
References:
- Malhotra R, Singh KD, Bhan S, Dave PK: Primary pyogenic abscess of the psoas muscle. J Bone Joint Surg Am 1992;74:278-284.
Question 30High Yield
A 23-year-old woman with a history of bilateral recurrent ankle sprains, progressive cavovarus feet, and a family history of high arches and foot deformities is seen for evaluation. Management consisting of bracing and physical therapy has been poorly tolerated. Heel varus is partially corrected with a Coleman block. There are thick calluses under the first metatarsal heads. Sensation to touch and Weinstein monofilament is normal. Tibialis anterior and peroneus brevis are weak but present. What is the most appropriate management?
Explanation
The history and presentation are consistent with type I Charcot-Marie-Tooth (CMT), the most common form of hereditary peripheral motor sensory neuropathy. Type I CMT is the most common, occurring in 50% of patients with CMT, and is characterized by marked slowing of motor neuron velocities, and inconsistent slowing of sensory neuron velocities. Peroneus longus to brevis transfer is indicated to release the overpull of the peroneus longus, and restore the eversion and dorsiflexion function of the peroneus brevis. A lateralizing calcaneal osteotomy with proximal translation is indicated to correct heel varus given that the Coleman block only allows for partial correction of heel varus. Proximal translation of the posterior tuber corrects for the increased calcaneal dorsiflexion, improving the lever arm for the triceps surae. A medial column closing wedge osteotomy is often required to correct a rigid, or semirigid plantar flexed first ray to allow for a balanced, plantigrade foot. Triple arthrodesis is indicated for rigid, arthritic hindfoot deformities. Transfer of the posterior tibial tendon to the tibialis anterior is not indicated since it is an out-of-phase transfer. Transfer of the posterior tibial tendon, when performed, should be to the lateral aspect of the foot. A medializing calcaneal osteotomy would accentuate the heel varus. There is no indication for Botox in CMT; Botox injection of the calf would further weaken push-off during gait. Bracing of a progressive semirigid or rigid deformity is not recommended. Younger AS, Hansen ST Jr: Adult cavovarus foot. J Am Acad Orthop Surg 2005;13:302-315. Sammarco GJ, Taylor R: Cavovarus foot treated with combined calcaneus and metatarsal ostetotomies. Foot Ankle Int 2001;22:19-30.
Question 31High Yield
A 15-year-old girl has left knee pain and an enlarging mass in the distal thigh. AP and lateral radiographs are shown in Figures 52a and 52b, and a biopsy specimen is shown in Figure 52c. What is the most likely diagnosis?
Explanation
Explanation
52b 52c A bone-producing lesion in the metaphysis of an adolescent is most likely an osteosarcoma. The radiographs show a distal femoral bone-producing lesion extending into the surrounding soft tissues. The histologic appearance consists of pleomorphic cells producing osteoid. Ewing's sarcoma and metastatic neuroblastoma do not produce a matrix. Chondrosarcoma is a radiographically destructive lesion with calcification and cartilage cells on histologic section. An osteochondroma is a benign cartilage lesion that is continuous with the medullary cavity of the underlying bone and extends into a bony lesion and covered by a cartilage cap. Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
References:
- Gibbs CP, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 32High Yield
What is the most common short-term complication following femoral impaction grafting for revision total hip arthroplasty?
Explanation
Explanation
Impaction grafting is an alternative for severe femoral bone deficiency; however, stem subsidence is commonly observed during the first few months. Slight subsidence is felt to be integral to the success of the procedure. Predictable bone graft incorporation and stable stem fixation have been reported in the medium-term. The incidence of periprosthetic fractures has been reported as high as 24%. Mikhail MWE, Weidenhielm L, Jazrawi LM, et al: Collarless, polished, tapered stem failure. J Bone Joint Surg Am 2000;82:1513-1514.
References:
- Leopold SS, Rosenberg AG: Current status of impaction allografting for revision of a femoral component. Instr Course Lect 2000;49:111-118.
Question 33High Yield
Ganglion cysts about the wrist most commonly arise from what structure?
Explanation
Ganglion cysts are the most common mass or mass-like lesions seen in the hand and wrist. They arise in a variety of locations, including synovial joints or tendon sheaths. The most common location is the dorsal/radial wrist arising from the dorsal scapholunate interosseous ligament.
Question 34High Yield
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms?
Explanation
Explanation
Traumatic posterior instability is a common finding in football players, especially in the blocking positions as well as in the defensive linemen and linebackers. A traumatic blow to the outstretched arm results in posterior glenohumeral forces. Labral detachment at the glenoid rim is common. Patients report slipping or pain with posteriorly directed pressure. Rarely do these patients have true dislocations that require reduction; however, recurrent episodes of subluxation or pain are not uncommon. Posterior repair has been shown to be successful in the treatment of traumatic instability. Bottoni CR, Franks BR, Moore JH, et al: Operative stabilization of posterior shoulder instability. Am J Sports Med 2005;33:996-1002. Williams RJ III, Strickland S, Cohen M, et al: Arthroscopic repair for traumatic posterior shoulder instability. Am J Sports Med 2003;31:203-209.
References:
- Kim SH, Ha KI, Park JH, et al: Arthroscopic posterior labral repair and capsular shift for traumatic unidirectional recurrent posterior subluxation of the shoulder. J Bone Joint Surg Am 2003;85:1479-1487.
Question 35High Yield
Which of the following clinical scenarios represents an appropriate indication for convex hemiepiphysiodesis/hemiarthrodesis in the treatment of a child with a congenital spinal deformity?
Explanation
Convex hemiarthrodesis and hemiepiphysiodesis are procedures designed to gradually reduce curve magnitude in congenital scoliosis because of hemivertebrae. They are used to surgically create an anterior and posterior bar to arrest growth on the convexity of the existing deformity. Success of the technique is predicated on continued growth on the concave side of the deformity. Prerequisites for this procedure include curves of limited length (less than or equal to five vertebrae), curves of reasonable magnitude (less than 70 degrees), absence of kyphosis, concave growth potential, and appropriate age (younger than age 5 years).
Question 36High Yield
When performing the exposure for an anterior approach to the cervical spine, the surgical dissection should not enter the plane between the trachea and the esophagus and excessive retraction should be avoided to prevent injury to the
Explanation
The recurrent laryngeal nerve lies between the trachea and the esophagus. The vagus nerve lies in the carotid sheath. The sympathetic trunk lies anterior to the longus colli muscles. The hypoglossal and superior laryngeal nerves are both at risk during the exposure but are not located between the trachea and the esophagus. Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Question 37High Yield
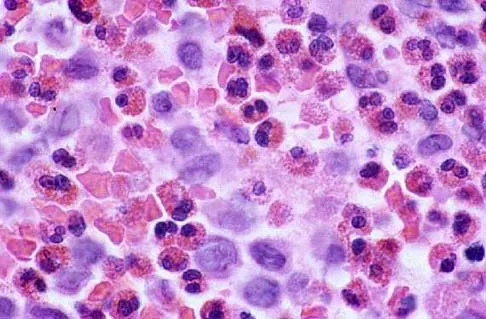
Figures 47a through 47f show the AP radiograph, bone scan, CT scan, MRI scan, and biopsy specimens of a 30-year-old woman who has had vague left shoulder pain for 1 year. Management should consist of



Explanation
The histology shows eosinophils with a background of larger cells (Langerhans' cells). This is consistent with eosinophilic granuloma. Localized sites are best treated with curettage, steroid injection, or observation. Chemotherapy is used only if there is systemic involvement. Mirra JM: Eosinophilic granuloma, in Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. London, England, Lea and Febiger, 1989, pp 1023-1060. Sessa S, Sommelet D, Lascombes P, Prevot J: Treatment of Langerhans-cell histiocytosis in children: Experience at the Children's Hospital of Nancy. J Bone Joint Surg Am 1994;76:1513-1525.
Question 38High Yield
A 7-year-old girl who sustained a type III posteromedial extension supracondylar fracture underwent a closed reduction at the time of injury. Figure 27a shows the position of the fracture fragments prior to percutaneous medial and lateral pin fixation. Following surgery, healing was uneventful and the patient regained a full painless range of motion. Fifteen months after the injury, she now reports loss of elbow motion and moderate pain with activity. A current AP radiograph is shown in Figure 27b. What is the most likely cause of her symptoms?
Explanation
Explanation
27b The patient sustained a very distal supracondylar fracture of the humerus. Fractures in this area can disrupt the blood vessels supplying the lateral ossification center of the trochlea. With disturbance of the blood supply in this area, local osteonecrosis occurs and disrupts the support for the overlying articular surface, producing joint incongruity and localized degenerative arthritis. Haraldsson S: The interosseous vasculature of the distal end of the humerus with special reference to the capitellum. Acta Orthop Scand 1957;27:81-93.
References:
- Morrissy RT, Wilkins KE: Deformities following distal humeral fracture in childhood. J Bone Joint Surg Am 1984;66:557-562.
Question 39High Yield
A 77-year-old woman who underwent a cemented total hip arthroplasty 10 years ago now reports groin pain. Examination reveals a loosened acetabular component and a well-fixed femoral component. Treatment should consist of revision of
Explanation
Recent literature supports retention of well-fixed cemented femoral components when revising loosened cemented acetabular components. Current literature also supports the use of cementless components for revision of loosened cemented acetabular components. Peters CL, Kull L, Jacobs JJ, Rosenberg AG, Galante JO: The fate of well fixed cemented femoral components left in place at the time of revision of the acetabular component. J Bone Joint Surg Am 1997;79:701-706. Poon ED, Lachiewicz PF: Results of isolated acetabular revisions: The fate of the unrevised femoral component. J Arthroplasty 1998;13:42-49. Moskal JT, Shen FH, Brown TE: The fate of stable femoral components retained during isolated acetabular revision: A six- to twelve-year follow-up study. J Bone Joint Surg Am 2002;84:250-255.
Question 40High Yield
What mechanism is associated with the spontaneous resorption of herniated nucleus pulposus?
Explanation
Explanation
Nonsurgical modalities remain the mainstay for treatment of herniated disks. Spontaneous resorption of herniated disks frequently is detected by MRI. Marked infiltration by macrophages and neovascularization are observed on histologic examination of herniated disks, and the resorption is believed to be related to this process. Many cytokines such as vascular endothelial growth factor, tumor necrosis factor-alpha, and metalloproteinases have been implicated in this process, but none has been found to be singularly responsible. Haro H, Kato T, Kamori H, et al: Vascular endothelial growth factor (VEGF)-induced angiogenesis in herniated disc resorption. J Orthop Res 2002;20:409-415.
References:
- Doita M, Kanatani T, Ozaki T, et al: Influence of macrophage infiltration of herniated disc tissue on the production of matrix metalloproteinases leading to disc resorption. Spine 2001;26:1522-1527.
Question 41High Yield
A 20-year-old woman has lateral foot and ankle pain after sustaining an inversion injury of the ankle while playing soccer 3 months ago. Activity modifications and physical therapy have failed to provide relief. She describes burning pain that extends from the anterior aspect of the ankle to the foot and lateral two toes. The pain is often worse at night. Plain radiographs, a bone scan, and an MRI scan are normal. Stress examination reveals no instability. What is the most likely diagnosis?
Explanation
Explanation
Persistent pain following an ankle sprain can present a diagnostic dilemma. All of the injuries listed should be considered in the differential diagnosis. The superficial peroneal nerve courses in the lateral compartment and exits the crural fascia 12 to 15 cm above the level of the ankle. Muscle herniation through the fascial defect has been reported to be associated with entrapment of this nerve. The fascial hiatus also may serve as a potential tether in cases of inversion injuries causing injury to the superficial peroneal nerve. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
References:
- Baumhauer JF: Superficial peroneal nerve entrapment. Foot Ankle Clin 1998;3:439-446.
Question 42High Yield
A 28-year-old professional dancer reports a 3-month history of progressive pain in the posterior aspect of the left ankle. Her symptoms are worse when she assumes the en pointe position. Examination reveals tenderness to palpation at the posterolateral aspect of the ankle posterior to the peroneal tendons which is made worse with passive plantar flexion. There is no nodularity, fluctuance, or tenderness of the Achilles tendon. The neurovascular examination is unremarkable. A lateral radiograph and MRI scan are shown in Figures 16a and 16b, respectively. Management should consist of
Explanation
The imaging studies reveal findings typical of the os trigonum syndrome. This condition results from inflammation between the os trigonum and the adjacent talus. The symptoms of posterior ankle pain are exacerbated by plantar flexion, which stresses the fibrous union between these two bones. Definitive management of the high-level athlete involves excision of the os trigonum from a medial approach, although arthroscopic excision has also been described. The os trigonum is not an intra-articular structure; therefore, ankle arthroscopy is neither diagnostic nor therapeutic. Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057. Mouhsine E, Crevoisier X, Leyvraz P, et al: Post-traumatic overload or acute syndrome of the os trigonum: A possible cause of posterior ankle impingement. Knee Surg Sports Traumatol Arthrosc 2004;12:250-253.
Question 43High Yield
A positive Froment sign indicates weakness of which of the following muscles?
Explanation
Thumb adduction is powered by the adductor pollicis (ulnar nerve). Testing involves having the patient forcibly hold a piece of paper between the thumb and radial side of the index proximal phalanx. When this muscle is weak or nonfunctioning, the thumb interphalangeal joint flexes with this maneuver, resulting in a positive Froment sign. The paper is held by action of the thumb flexion (flexor pollicis longus and flexor pollicis brevis; median innervated).
Question 44High Yield
Figures 35a and 35b show the radiographs of a patient who underwent debridement of a chronically infected, fully constrained knee prosthesis and now reports pain and instability despite bracing. History reveals that the patient has had no drainage since undergoing the last debridement 6 months ago. A C-reactive protein level and aspiration are negative for infection. Treatment should now consist of

Explanation
The radiographs show a significant loss of the proximal anterior tibial cortex, consistent with an extensively damaged or deficient extensor mechanism. Such a deficit precludes insertion of another knee arthroplasty. Arthrodesis is the treatment of choice for this patient and is indicated for loss of the extensor mechanism and knee instability. A recent report on arthrodesis following removal of an infected prosthesis showed a union rate of 91% using a short intramedullary nail. Insertion of an antibiotic-impregnated PMMA spacer is not indicated because the rationale for using a spacer is to maintain a space for reinsertion of another prosthesis. Reconstruction of the extensor mechanism would not address the loss of the joint. Amputation is the final treatment option if the arthrodesis fails. Rand JA: Alternatives to reimplantation for salvage of the total knee arthroplasty complicated by infection. J Bone Joint Surg Am 1993;75:282-289. Lai KA, Shen WJ, Yang CY: Arthrodesis with a short Huckstep nail as a salvage procedure for failed total knee arthroplasty. J Bone Joint Surg Am 1998;80:380-388.
Question 45High Yield
Which is the best initial study for the diagnostic evaluation of diskogenic low back pain?
Explanation
Explanation
Radiography is the best initial study for the evaluation of diskogenic low back pain. The normal degenerative process can be evaluated. Vacuum phenomenon may be found within the disk space. Other possible sources for back pain should also be evaluated. The other tests may be beneficial but represent later imaging options.
Question 46High Yield
A neurologic injury at T11-L2 with loss of bowel and bladder control is best described as what syndrome?
Explanation
Explanation
Conus medullaris syndrome describes isolated loss of bowel and bladder function, usually at T12-L1 but can include T11-L2. In central cord syndrome, lower extremity motor function is better than upper extremity function. Cauda equina syndrome generally involves injury at the lumbar levels, with some degree of lower extremity motor loss. Posterior cord syndrome is characterized by preservation of motor function below the level of injury and position/vibratory sensory loss. In anterior cord syndrome, the lower extremity findings include loss of light touch, sharp/dull, and temperature sensations below the level of injury, as well as motor function. Apple DF Jr: Spinal cord injury rehabilitation, in Rothman RH, Simeone FA (eds): The Spine, ed 3. Philadelphia, PA, WB Saunders, 1992, Chapter 31.
References:
- Weisberg LA: Neurologic localization: Lesions below foramen magnum, in Weisberg LA, Strub RL, Garcia CA (eds): Adult Neurology, ed 2. St. Louis, MO, Mosby, 1993.
Question 47High Yield
An elite skier training for the Olympics sustains an isolated traumatic dislocation of the peroneal tendons that have spontaneously reduced. The games are 9 months away and the athlete does not want to miss them. Treatment should consist of
Explanation
Explanation
Most of these injuries occur in young, active patients. Success rates for nonsurgical management are only marginally better than 50%. The treatment of choice is early surgery for patients who desire a quick return to a sport or active lifestyle. Subluxation of the peroneal tendons leads to longitudinal tears over time. McLennan JG: Treatment of acute and chronic luxations of the peroneal tendons. Am J Sports Med 1980;8:432-436.
References:
- Krause JO, Brodsky JW: Peroneus brevis tendon tears: Pathophysiology, surgical reconstruction, and clinical results. Foot Ankle Int 1998;19:271-279.
Question 48High Yield
A patient with a below-the-knee amputation is being evaluated for a new prosthesis. He wants to improve his ability to walk on uneven surfaces. What modification to the prosthesis can be made to accommodate this request?
Explanation
Changing from a solid keel to a keel with a sagittal split allows an amputee to navigate uneven terrain more easily. Changing the length of the keel affects the responsiveness of the prosthesis but does not address the surface conditions for ambulation. The SACH is not used as frequently anymore, because overload problems to the nonamputated foot have been observed. Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 31-45.
Question 49High Yield
Figures 4a through 4c show the radiographs of a 43-year-old woman who sustained a twisting injury to her right ankle. She has ankle pain and tenderness medially and laterally. To help determine the optimal treatment, an external rotation stress radiograph of the ankle is obtained. This test is designed to evaluate the integrity of what structure?


Explanation
In the presence of a supination external rotation-type fracture of the distal fibula (Weber type B), stability of the ankle is best assessed by performing an external rotation stress AP view of the ankle. This test is used to assess the integrity of the deltoid ligament. The presence of a deltoid ligament rupture results in instability and generally is best managed surgically. The gravity stress test can also be used. Egol KA, Amirtharajah M, Tejwani NC, et al: Ankle stress test for predicting the need for surgical fixation of isolated fibular fractures. J Bone Joint Surg Am 2004;86:2393-2398. McConnell T, Creevy W, Tornetta P III: Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am 2004;86:2171-2178.
Question 50High Yield
A 12 1/2-year-old boy reports intermittent knee pain and limping that interferes with his ability to participate in sports. He actively participates in football, basketball, and baseball. He denies any history of injury. Examination shows full range of motion without effusion. Radiographs reveal an osteochondritis dissecans (OCD) lesion on the lateral aspect of the medial femoral condyle. MRI scans are shown in Figures 14a and 14b. Initial treatment should consist of

Explanation
This skeletally immature patient has a small OCD lesion that appears stable, and he has not undergone any treatment. Therefore, a trial of immobilization until pain resolves is the best initial choice. Thereafter, cessation of sport activities for 4 to 6 months may allow healing of the lesion. Surgical treatment of juvenile OCD lesions is reserved for unstable lesions, patients who have not shown radiographic evidence of healing and are still symptomatic after 6 months of nonsurgical management, or patients who are approaching skeletal maturity. Good results with stable in situ lesions that have failed to respond to nonsurgical management have been reported with both transarticular and retroarticular drilling. Results after excision alone are poor at 5-year follow-up, and it is unclear if microfracture will improve the long-term outcome. Mosaicplasty may be the next best option for patients who remain or become symptomatic after excision of the fragment and microfracture. Wall E, Von Stein D: Juvenile osteochondritis dissecans. Orthop Clin North Am 2003;34:341-353.
Question 51High Yield
Figure 18 shows the radiograph of a patient with a total hip arthroplasty dislocation. During revision, increasing the diameter of the femoral head while maintaining the ratio of head-to-neck diameter constant has the effect of
Explanation
Explanation
Although there is strong clinical and laboratory evidence that suggests smaller head size is linked with lower rates of polyethylene wear, moving to the use of 22-mm heads from larger sizes would tend to increase the dislocation rate. The key premise to this argument is that the absolute size of the femoral neck remains unchanged. While neck diameters were appropriate for the early monoblock femoral components, the use of modular femoral stems allows the surgeon to place 22-mm heads onto the same neck and trunion as used by larger heads. This has the effect of lessening the head-to-neck diameter ratio, which then accentuates the rate of impingement and dislocation. Reducing the neck diameter in proportion to the head diameter would eliminate the range-of-motion penalty accompanying head size reduction. Scifert and associates used a three-dimensional finite element model to study various combinations of femoral head size and neck ratios. They found that increasing the diameter of the femoral head while maintaining a constant head-to-neck diameter had the effect of significantly increasing the resisting moment necessary to induce a dislocation. The higher the head-to-neck ratio, the greater the range of motion until impingement and the greater the range of motion to dislocation.
References:
- Scifert CF, Brown TD, Pedersen DR, Callaghan JJ: A finite element analysis of factors influencing total hip dislocation. Clin Orthop 1998;355:152-162.
Question 52High Yield
A 14-year-old boy has an asymptomatic mass on the right arm. MRI scans and biopsy specimens are shown in Figures 51a through 51d. Immunostaining is positive for desmin. Additional staging studies should include



Explanation
The patient has rhabdomyosarcoma. Axilliary node and bone marrow biopsy are part of the staging because about 12% of patients with rhabdomyosarcoma of the extremity have evidence of lymph nodes metastases at presentation. Bone marrow metastases have been shown to portend a worse prognosis. Lawrence W, Jr., Hays DM, Heyn R, Tefft M, Crist W, Beltangady M, et al: Lymphatic metastases with childhood rhabdomyosarcoma: A report from the Intergroup Rhabdomyosarcoma Study. Cancer 1987;60:910-915.
Question 53High Yield
A posterolateral approach to the tibial plafond proceeds between what two muscles?
Explanation
A posterolateral approach to the posterior malleolus proceeds between the lateral and deep posterior compartments. Distally, the peroneus brevis muscle lies most medially within the lateral compartment, and the flexor hallucis longus lies most laterally in the deep posterior compartment. Henry AK: Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 269-270.
Question 54High Yield
Patients with patellar clunk syndrome are best managed by which of the following methods?
Explanation
Patellar clunk syndrome is usually the result of a fibrous nodule that forms on the undersurface of the distal quadriceps tendon. It may get entrapped in the intercondylar notch of the femoral component during flexion, and lead to a sudden snap as the nodule is pulled out of the notch during active extension. Nonsurgical management is rarely successful. Surgical debridement is usually curative, with only rare recurrence. More aggressive procedures such as realignment, revision, or patellectomy are usually not necessary, and are reserved for cases resistant to soft-tissue debridement. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 329. Diduch DR, Scuderi GR, Scott WN, et al: The efficacy of arthroscopy following total knee replacement. Arthroscopy 1997;13:166-171.
Question 55High Yield
Reconstruction of the posterior cruciate ligament (PCL) via the inlay technique involves exposure of the PCL tibial insertion site by a posterior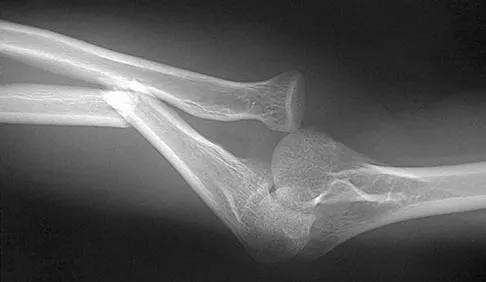
Explanation
The posterior medial approach through the semimembranosus/medial gastrocnemius interval is used in the inlay technique for PCL reconstruction. Exposure of the posterior capsule of the knee through this interval provides the greatest margin of safety to avoid injury to the tibial nerve, motor branch of the medial gastrocnemius, and the peroneal nerve. The direct posterior approach using the medial sural cutaneous nerve allows exposure of the popliteal neurovascular structures, but deep dissection through this interval places the motor branch of the medial gastrocnemius at risk. The interval between the semitendinosus and semimembranosus is used in accessory incisions with medial meniscus repairs but does not allow exposure of the PCL insertion. Berg EE: Posterior cruciate tibial inlay reconstruction. Arthroscopy 1995;11:69-76.
Question 56High Yield
A 35-year-old man sustained a 10% compression fracture of the C5 vertebra in a diving accident. Radiographs show good alignment, and examination reveals no neurologic compromise. An MRI scan reveals no significant soft-tissue disruption posteriorly. Management should consist of
Explanation
Explanation
The patient has a stable flexion-compression injury of the cervical spine. The fracture occurs as a result of compression failure of the vertebral body. If the force continues, a tension failure of the posterior structures occurs, leading to potential dislocation. Immobilization in a rigid cervical orthosis will allow this fracture to heal. Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 457-464.
References:
- Allen GL, Ferguson RL, Lehmann TR, O'Brien RP: A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27.
Question 57High Yield
A 15-year-old boy with epilepsy who is treated with phenytoin sustains a vertebral compression fracture during a breakthrough seizure. Radiographs of the spine reveal generalized osteopenia. What is the most likely cause of the osteopenia?
Explanation
Explanation
As a side effect of treatment, phenytoin induces osteomalacia, or rickets, in growing children, through interference with metabolism of vitamin D. Oral supplementation of vitamin D can minimize this effect in patients who are undergoing prolonged treatment with phenytoin.
References:
- Chung S, Ahn C: Effects of anti-epileptic drug therapy on bone mineral density in ambulatory epileptic children. Brain Dev 1994;16:382-385.
Question 58High Yield
What is the best surgical approach for the scapular fracture shown in Figure 46?
Explanation
Explanation
Indications for open reduction of glenoid intra-articular fractures include those fractures with a 5-mm articular surface displacement or when the humeral head is subluxated with the fracture fragment. Kavanaugh and associates and Leung and Lam have shown that the posterior approach with plate fixation is best for most glenoid fractures, including the Ideberg type II fracture shown here. The anterior approach is best used for anterior rim and transverse fractures. Kavanagh BF, Bradway JK, Cofield RH: Open reduction and internal fixation of displaced intra-articular fractures of the glenoid fossa. J Bone Joint Surg Am 1993;75:479-484. Leung KS, Lam TP: Open reduction and internal fixation of ipsilateral fractures of the scapular neck and clavicle. J Bone Joint Surg Am 1993;75:1015-1018.
References:
- Ideberg R: Unusual glenoid fractures: A report on 92 cases. Acta Orthop Scand 1995;66:395-397.
Question 59High Yield
A football player sustains a traumatic anterior inferior dislocation of the shoulder in the last game of the season. It is reduced 20 minutes later in the locker room. The patient is neurologically intact and has regained motion. If the patient undergoes arthroscopic evaluation, what finding is seen most consistently?
Explanation
Explanation
In an acute first-time dislocation, arthroscopy has been shown to reveal a Bankart lesion in most shoulders. The classic finding of labral detachment from the anterior inferior glenoid along with occasional hemorrhage within the inferior glenohumeral ligament is the most common sequelae of a traumatic anterior inferior dislocation. Acute treatment, if chosen, is repair of the labral tissue back to the glenoid plus or minus any capsular plication to address potential plastic deformation of the glenohumeral ligament. Acute treatment of a patient sustaining a first-time dislocation remains controversial. The potential indications may be patients whose dislocation occurs at the end of a season and when the desire to minimize risk of future instability outweighs the risks of surgical intervention. Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311. DeBerardino TM, Arciero RA, Taylor DC, et al: Prospective evaluation of arthroscopic stabilization of acute, initial anterior shoulder dislocations in young athletes: Two- to five-year follow-up. Am J Sports Med 2001;29:586-592.
References:
- Bottoni CR, Wilckens JH, DeBerardino TM, et al: A prospective, randomized evaluation of arthroscopic stabilization versus nonoperative treatment in patients with acute, traumatic, first-time shoulder dislocations. Am J Sports Med 2002;30:576-580.
Question 60High Yield
A collegiate football player who sustained an injury to his neck has significant neck pain and weakness in his extremities. Following immobilization, which of the following steps should be taken prior to transport?
Explanation
Prior to transport, the face mask should be removed so that the airway can be easily accessible. If serious injury is suspected, the helmet and shoulder pads should be left in place until he is assessed at the hospital and radiographs are obtained. Leaving the helmet and shoulder pads in place helps to keep the spine in the most neutral alignment. Removal of the helmet will result in extension of the neck, whereas removal of the shoulder pads will most likely result in flexion of the neck. Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 376. Thomas B, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347. Waninger KN, Richards JG, Pan WT, et al: An evaluation of head movement in backboard-immobilized helmeted football, lacrosse, and ice hockey players. Clin J Sport Med 2001;11:82-86. Donaldson WF III, Lauerman WC, Heil B, et al: Helmet and shoulder pad removal from a player with suspected cervical spine injury: A cadaveric model. Spine 1998;23:1729-1732.
Question 61High Yield
A baseball pitcher has intractable posterior and superior shoulder pain. The arthroscopic view seen in Figure 25 shows no Bankart or Hill-Sachs lesion and a negative drive-through sign. There are no signs of ligamentous laxity, but active compression and anterior slide tests are positive. Treatment should consist of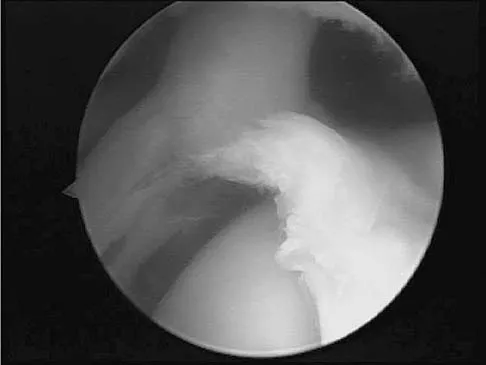
Explanation
According to Morgan and associates, a type II SLAP lesion can create or is associated with a superior instability pattern. They suggest that this can exist without a co-existing anteroinferior instability pattern. They reported that repair of the SLAP lesion alone resulted in satisfactory outcomes in 90% of patients and a return to throwing in more than 90% of pitchers. The arthroscopic findings in this patient do not support a diagnosis of anteroinferior laxity or instability; therefore, thermal capsular shift or capsular placation is not necessary. Morgan CD, Burkhart SS, Palmeri M, et al: Type II SLAP lesions: Three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy 1998;14:553-565. Mileski RA, Snyder RJ: Superior labral lesions in the shoulder: Pathoanatomy and surgical management. J Am Acad Orthop Surg 1998;6:121-131.
Question 62High Yield
Osteophyte formation at the posteromedial olecranon and olecranon articulation in high-caliber throwing athletes is most often the result of underlying
Explanation
Explanation
During the late acceleration phase of throwing, the triceps forcibly contracts, extending the elbow as the ball is released. Normally, this force is absorbed by the anterior capsule and the brachialis and biceps muscles. However, if the ulnar collateral ligament is insufficient, the elbow will be in a subluxated position during extension and cause impaction of the olecranon and the olecranon fossa posteromedially. Over time, osteophyte formation is likely to occur. Conway JE, Jobe FW, Glousman RE, Pink M: Medial instability of the elbow in throwing athletes: Treatment by repair or reconstruction of the ulnar collateral ligament. J Bone Joint Surg Am 1992;74:67-83.
References:
- Wilson FD, Andrews, JR, Blackburn TA, McCluskey G: Valgus extension overload in the pitching elbow. Am J Sports Med 1983;11:83-88.
Question 63High Yield
Figures 44a and 44b show the radiographs of a 28-year-old woman who has had progressive hip pain for the past 3 months. What is the most likely diagnosis?

Explanation
The patient has multiple hereditary exostoses and a secondary chondrosarcoma arising from a proximal femoral exostosis. The radiograph of the knee shows multiple osteochondromas typical in a patient with multiple hereditary exostoses. Patients with this diagnosis are at an increased risk for malignant degeneration of an osteochondroma. The lateral radiograph of the hip shows a bony lesion emanating from the anterior aspect of the femoral neck that is not well defined in the surrounding soft tissues. There are punctate calcifications and a large soft-tissue mass. The most likely diagnosis is a secondary chondrosarcoma developing from a benign osteochondroma. An enchondroma is an intramedullary benign cartilage lesion. Ollier's disease and Maffucci's syndrome involve multiple enchondromas. Scarborough M, Moreau G: Benign cartilage tumors. Orthop Clin North Am 1996;27:583-589.
Question 64High Yield
A 16-year-old girl was involved in a motorcycle accident that resulted in a significant right tibial fracture with soft-tissue loss over the distal 4 cm of the anterior medial tibia. The patient has had two irrigations and debridements and recently had an intramedullary nail placed for the skeletal injury. Vacuum-assisted closure (VAC) has been used to cover the defect since the injury. The risk of infection developing in the tibia is
Explanation
The risk of infection in a 3B open tibia fracture is most directly related to the timing of the soft-tissue coverage and less related to the size or location of the wound. The wound VAC does not lower or raise the risk of infection in open fractures. It does appear to increase the window of time to obtain coverage without increasing the risk of infection. Additionally, the wound VAC may decrease the probability of needing free tissue coverage. Intramedullary nailing has not been shown to lower the risk of infection in 3B fractures. Godina M: Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78:285-292. Dedmond BT, Kortesis B, Punger K, et al: The use of negative-pressure wound therapy (NPWT) in the temporary treatment of soft-tissue injuries associated with high-energy open tibia shaft fractures. J Orthop Trauma 2007;21:11-17.
Question 65High Yield
Figures 23a and 23b show the AP and lateral radiographs of the elbow of a 30-year-old professional pitcher. The pathology shown in these studies is most consistent with which of the following conditions?
Explanation
Explanation
23b The radiographs show the osteophytic build-up of the posteromedial corner of the elbow that occurs with valgus extension overload in the pitching elbow. This is the result of excessive valgus forces during the acceleration and deceleration phases of throwing. These forces, coupled with medial elbow stresses, cause a wedging of the olecranon into the medial wall of the olecranon fossa. Valgus instability of the elbow may further stimulate osteophyte formation. Repetitive impact of a spur within the olecranon fossa may cause fragmentation and eventual formation of loose bodies. Azar FM, Wilk KE: Nonoperative treatment of the elbow in throwers. Oper Tech Sports Med 1996;4:91-99. Field LD, Savoie FJ: Common elbow injuries in sport. Sports Med 1988;26:193-205.
References:
- Wilson FD, Andrews JR, Blackburn TA, et al: Valgus extension overload in the pitching elbow. Am J Sports Med 1983;11:83-88.
Question 66High Yield
A 22-year-old college baseball pitcher reports the recent onset of anterior and posterosuperior shoulder pain in his throwing shoulder. Examination shows a 15-degree loss of internal rotation, tenderness over the coracoid, and a positive relocation test. Radiographs are normal, and an MRI scan without contrast shows no definitive lesions. A rehabilitation program is prescribed. Which of the following regimens should be initially employed?
Explanation
Explanation
Throwing athletes, particularly pitchers, have a high incidence of shoulder pain. Recent evidence suggests that posteroinferior capsular tightness and scapular dyskinesis may play a substantial role in the pathologic cascade, culminating in the development of articular surface rotator cuff tears and tearing of the posterosuperior labrum. These patients have posterosuperior shoulder pain primarily. Furthermore, these athletes are susceptible to a muscular fatigue syndrome, the SICK (Scapular malposition, Inferior medial border prominence, Coracoid pain and malposition, and dysKinesis of scapular movement) scapula syndrome. This patient has an internal rotation deficit and tenderness over the coracoid. The internal rotation deficit is addressed by stretching the posterior capsule. The tenderness over the coracoid has been attributed to a contracture of the pectoralis minor tendon secondary to scapular malposition. The initial phase of the rehabilitation regimen is directed at stretching the posterior capsule and pectoralis minor tendon. Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part III. Arthroscopy 2003;19:641-661.
References:
- Kibler WB, McMullen J: Scapular dyskinesis and its relationship to shoulder pain. J Am Acad Orthop Surg 2003;11:142-151.
Question 67High Yield
When using a two-incision approach for open reduction and internal fixation of a Hawkins III talar fracture-dislocation involving the talar neck and body, what anatomic structure must be preserved to optimize outcome?
Explanation
Explanation
A Hawkins III fracture-dislocation generally presents with posteromedial displacement with the deltoid ligament intact. Therefore, the only remaining blood supply is the deltoid branch of the artery of the tarsal canal originating from the posterior tibial artery. Often, the medial malleolus is fractured, assisting in reduction and visualization of fracture reduction. If the medial malleolus is intact, a medial malleolus osteotomy allows visualization of the reduction without compromising the last remaining blood supply to the talus. Mulfinger GL, Trueta J: The blood supply of the talus. J Bone Joint Surg Br 1970;52:160-167.
References:
- Vallier HA, Nork SE, Barei DP, et al: Talar neck fractures: Results and outcomes. J Bone Joint Surg Am 2004;86:1616-1624.
Question 68High Yield
Figures 20a and 20b show lateral and AP radiographs of a 49-year-old man who sustained a gunshot wound through the left shoulder. He reports neck pain and examination reveals weakness in all four extremities. What is the priority of evaluation?
Explanation
Explanation
20b The projectile entered the left shoulder and traveled to the right neck; therefore, a high incidence of suspicion must be directed to the airway, great vessels of the neck, and contents of the mediastinum. Immediate assessment of airway, breathing, and circulation takes priority, followed by examination of the neurologic status and other systems, as determined by the examination findings. Subcommittee on ATLS of the American College of Surgeons Committee on Trauma 1993-1997, Spine and Spinal Cord Trauma; Advanced Trauma Life Support Student Manual, ed 6, 1997. International Standards for Neurological and Functional Classification of Spinal Cord Injury. American Spinal Injury Association and International Medical Society of Paraplegia (ASIA/IMSOP).
Question 69High Yield
What type of nerve palsy is most common following elbow arthroscopy?
Explanation
Transient ulnar nerve palsy is the most common palsy following elbow arthroscopy. The ulnar nerve is most frequently affected, followed by the radial nerve. Injury to the other nerves has been reported but less frequently. Kelly EW, Morrey BF, O'Driscoll SW: Complications of elbow arthroscopy. J Bone Joint Surg Am 2001;83:25-34.
Question 70High Yield
A 47-year-old woman underwent a bunionectomy and hallux valgus correction a few years ago. She now has the complication shown in Figures 38a and 38b. She has no pain with motion of the metatarsophalangeal or interphalangeal joints. What is the best reconstructive option in this setting?
Explanation
Explanation
38b The patient has a flexible hallux varus that is a complication of the bunion surgery. With joints that are not arthritic and still flexible, a medial release is necessary to realign the joint. The extensor hallucis longus split transfer helps maintain position and still preserve motion at the interphalangeal joint level. Arthrodesis is a salvage procedure. Soft-tissue releases alone are most likely inadequate. Excision of the lateral sesamoid is contraindicated because that further compromises the forces resisting hallux varus. Phalangeal osteotomy would not address the medial subluxation at the metatarsophalangeal joint. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 27-32.
Question 71High Yield
A 69-year-old man sustains a traumatic amputation to the distal phalanx of his little finger while working with power tools. Radiographs are shown in Figures 27a and 27b. The patient was instructed how to perform wet-to-dry dressing changes in the emergency department. Clinical pictures taken in the office are shown in Figures 27c through 27e. What is the most appropriate management of this soft-tissue wound?
Explanation
Explanation
27b 27c 27d 27e The clinical photographs and radiographs reveal a distal phalangeal amputation with soft-tissue coverage over nonexposed bone. This is an ideal circumstance to allow healing by secondary intention with wet-to-dry dressing changes. There are few complications and the aesthetics surpass that of any soft-tissue reconstruction procedure. Volar advancement flaps (Moberg flaps) are limited to small defects about the thumb. A thenar flap will provide good coverage; however, the results are not comparable to simple dressing changes. A V-Y flap is useful when there is more tissue loss dorsally. Jebson PL, Louis DS: Amputations, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green's Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 1947.
Question 72High Yield
A 78-year-old woman falls onto her nondominant left elbow and sustains the injury shown in Figure 5. What treatment option allows her the shortest recovery time and highest likelihood of good function and range of motion?
Explanation
Total elbow arthroplasty has become the treatment of choice for complex, comminuted distal humeral fractures in patients older than age 70 years. It yields a faster recovery with more predictable functional outcomes, although limitations of lifting weight of more than 5 pounds must be followed to avoid loosening. Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement. J Bone Joint Surg Am 2004;86:940-947.
Question 73High Yield
An 18-year-old rugby player has had pain in his ring finger after missing a tackle 1 week ago. Examination reveals tenderness in the distal palm, and he is unable to actively flex the distal interphalangeal (DIP) joint. Radiographs are normal. What is the most appropriate management?
Explanation
Explanation
Flexor digitorum profundus rupture or "rugger jersey finger" often occurs in the ring finger after the player misses a tackle and catches the digit on the shirt of the opposing player. Surgical repair is required for zone I-type injuries. Moiemen NS, Elliot D: Primary flexor tendon repair in zone I. J Hand Surg Br 2000;25:78-84.
References:
- Strickland JW: Flexor tendon injuries: I. Foundations of treatment. J Am Acad Orthop Surg 1995;3:44-54.
Question 74High Yield
A 62-year-old woman has back pain and right L2 radicular pain. MRI scans suggest a neoplastic lesion at L2, and a bone scan is negative except at L2. History reveals that she was treated for breast cancer without known metastatic disease 12 years ago and is thought to be free of disease. What is the next most appropriate step in management?
Explanation
Because of the long disease-free interval, it cannot be assumed that this is breast cancer. The lesion could represent metastasis from a new primary tumor or could itself be a primary tumor. CT-guided biopsy will most effectively identify the lesion and guide treatment options. Depending on the specific diagnosis, any of the other options may be appropriate.
Question 75High Yield
A 42-year-old patient has had a fever and low back pain for several days. Laboratory studies show an elevated erythrocyte sedimentation rate and a WBC count of 9,500 mm3 with 75% neutrophils. A CT scan is shown in Figure 15. Examination will most likely reveal what other findings?
Explanation
The CT scan reveals a left-sided psoas abscess. Irritation of the saphenous division of the femoral nerve can cause paresthesias along the medial aspect of the knee. Pain is usually improved with hip flexion. Cellier C, Gendre JP, Cosnes J, et al: Psoas abscess complication Crohn's disease. Gastroenterol Clin Biol 1992;16:235-238.
Question 76High Yield
Which of the following best describes the relative content of the components of articular cartilage in decreasing order?
Explanation
Explanation
Water is the most abundant component of articular cartilage with a wet weight of 65% to 80%. Of the water, 80% is at the surface and 65% at the deep zone. Collagen accounts for 10% to 20% of the wet weight, with type II collagen accounting for 90% to 95% of the total collagen content. Small amounts of types V, VI, IX, X, and XI collagen are also present. Proteoglycans comprise 10% to 15% of the wet weight of collagen. The remainder of the wet weight is made up of other collagens, noncollagenous proteins, and chondrocytes.
References:
- Schiller AL: Pathology of osteoarthritis, in Kuettner KE, Goldberg VM: Osteoarthritic Disorders. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 95-101.
Question 77High Yield
Following reconstruction of the anterior cruciate ligament (ACL), which of the following rehabilitation exercises has the greatest potential to harm the graft?
Explanation
Isometric quadriceps contraction between 15 and 30 degrees of flexion creates significant strain in the ACL and potential damage to the reconstructed graft. Isolated quadriceps contraction with knee flexion of greater than 60 degrees, hamstring contraction at any angle of knee flexion, and active knee motion between 35 and 90 degrees of flexion create substantially less strain in the properly implanted ACL graft. Beynnon BD, Gleming BC, Johnson RL, Nichols CE, Renstrom PA, Pope MH: Anterior cruciate ligament strain behavior during rehabilitation exercises in vivo. Am J Sports Med 1995;23:24-34.
Question 78High Yield
Figure 6 shows the radiograph of a 14-year-old baseball player who felt a pop and had an immediate onset of pain in his elbow after a hard throw from the outfield. The best course of action should be to
Explanation
The valgus stress at the elbow caused by throwing strains the medial collateral ligament. The medial epicondyle, on which the ligament inserts, is the last ossification center to fuse to the distal humerus, and acute avulsion of the medial epicondyle can occur in adolescents. If the elbow is allowed to heal in a displaced position, valgus instability and loss of elbow extension may result. Valgus instability is especially problematic for the throwing athlete. Surgical treatment with rigid internal fixation is the treatment of choice for displaced medial epicondyle avulsion fractures. Valgus instability is prevented, and the rigid fixation allows for early range of motion. Case SL, Hennrikus WL: Surgical treatment of displaced medial epicondyle fractures in adolescent athletes. Am J Sports Med 1997;25:682-686.
Question 79High Yield
When compared with fresh-frozen bone allograft, freeze-dried bone allograft (FDBA) is characterized by
Explanation
The compaction of FDBA is faster than that of fresh-frozen bone. The maximal stiffness reached by both materials when tested was the same (55 MPa), but the FDBA required fewer impactions to achieve that stiffness. Because it is easier to impact, the FDBA may be mechanically more efficient than the fresh-frozen bone in surgical conditions. The brittleness of irradiated FDBA, caused by loss of the capacity to absorb energy in a plastic way, increases the compactness and stiffness of morcellized grafts. The failure rate of fusion in adolescent idiopathic scoliosis has been shown to be much higher in FDBA than in either iliac crest bone graft or composite autograft with demineralized bone matrix. There is a greater erosive surface response to allograft when compared to autograft or frozen allograft, with a larger number of osteoclast and osteoblast nuclei seen microscopically. Cornu O, Libouton X, Naets B, et al: Freeze-dried irradiated bone brittleness improves compactness in an impaction bone grafting model. Acta Orthop Scand 2004;75:309-314. Price CT, Connolly JF, Carantzas AC, et al: Comparison of bone grafts for posterior spinal fusion in adolescent idiopathic scoliosis. Spine 2003;28:793-798.
Question 80High Yield
Figure 53 shows the arteriogram of a 45-year-old man who has severe vasculitis. What do the findings show?
Explanation
Explanation
The arterial supply to the hand is abundant and normally duplicated. The deep palmar arch as shown in this arteriogram typically receives its primary contribution from the radial artery which travels deep to the first dorsal compartment tendons and then returns to the volar aspect of the palm through the first web space. The superficial palmar arch receives its supply from the ulnar artery and is not visualized in this patient.
References:
- Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist: Diagnosis and Operative Treatment. Philadephia, PA, Mosby-Year Book, 1998, p 110.
Question 81High Yield
Figure 17 shows the clinical photograph of a 45-year-old female tennis player who has right arm pain and weakness with elevation after undergoing a cervical biopsy several months ago. The cause of her shoulder weakness is damage to the
Explanation
The patient has primary scapulotrapezius winging caused by surgical damage to the spinal accessory nerve during a lymph node biopsy. Other causes include blunt trauma, traction, and penetrating injuries. With spinal accessory palsy, the shoulder appears depressed and laterally translated because of unopposed serratus anterior muscle function. With primary serratus anterior winging that is the result of long thoracic nerve palsy, the scapula assumes a position of elevation and medial translation with the inferior angle rotated medially. The thoracodorsal nerve innervates the latissimus dorsi and is not associated with scapular winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 82High Yield
Which of the following changes occur in the spinal cord and the spinal canal when the cervical spine moves from neutral to full flexion?
Explanation
Explanation
The spinal cord and spinal canal undergo dynamic changes during neck flexion and extension. In neck flexion, the spinal cord initially unfolds and then undergoes elastic deformation with full flexion; the spinal canal lengthens. This may explain the presence of Lhermitte's sign as the cord is pulled anteriorly over an anterior osteophyte or disk, generating a compressive force on the spinal cord. During neck extension, the spinal cord relaxes (folding like an accordion) and the spinal canal shortens. Breig A: Biomechanics of the Central Nervous System: Some Basic Normal and Pathologic Phenomena. Stockholm, Sweden, Almquist and Wiksell, 1960.
References:
- Ghanayem AJ, Zdeblick TA, Panjabi MM: Biomechanics of nonacute cervical spine trauma, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 103-105.
Question 83High Yield
The radiographic feature seen in Figure 37 that best indicates a slow-growing process is the
Explanation
Explanation
For the fibula (or any bone) to bow, a long-standing process needs to be present. Pressure from a rapid process would cause erosion, not allowing the bone to remodel. The other features are helpful confirmatory findings but also may be associated with aggressive processes. In this patient, the fibular deformity is caused by a sessile osteochondroma of the tibia. Lodwick GS, Wilson AJ, Farrell C, Virtama P, Dittrich F: Determining growth rates of focal lesions of bone from radiographs. Radiology 1980;134:577-583.
References:
- Moser RP Jr, Madewell JE: An approach to primary bone tumors. Radiol Clin North Am 1987;25:1049-1093.
Question 84High Yield
A 21-year-old professional ballet dancer reports a painful popping sensation over her right hip joint. Examination reveals that symptoms are reproduced with hip flexion and external rotation. Which of the following studies will best confirm the diagnosis?
Explanation
The patient has snapping hip syndrome of the internal type, which is more common in ballet dancers. It is caused by the iliopsoas tendon gliding over the iliopectineal line or the femoral head. The diagnosis usually can be made by the history and physical examination. Snapping is reproduced by hip flexion and extension or flexion with external rotation and abduction. Conventional and dynamic ultrasonography will confirm the snapping structure. Radiographs occasionally show calcifications near the lesser trochanter. MRI can be used to rule out other diagnoses that can simulate snapping hip. Gruen GS, Scioscia TN, Lowenstein JE: The surgical treatment of internal snapping hip. Am J Sports Med 2002;30:607-613.
Question 85High Yield
An 8-month-old infant has an infection of the fingertip as shown in Figure 22. If neglected, the anticipated path of ascending infection is the fingertip, the flexor sheath, and the
Explanation
Explanation
The flexor sheaths are in continuity with the deep spaces of the hand. The flexor sheaths of the thumb and little finger communicate with the radial and ulnar bursae, respectively, and these two bursae commonly communicate. The central digits do not communicate as readily with deep spaces of the hand but if flexor tendon sheath infection of the index, long, and right fingers is neglected, the potential exists for rupture into the deep midpalmar spaces. Peimer CA (ed): Surgery of the Hand and Upper Extremity: Acute and Chronic Sepsis. New York, NY, Mcgraw Hill, 1996, pp 1735-1741.
References:
- Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow and Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 445-446.
Question 86High Yield
A 6-year-old child sustained a closed nondisplaced proximal tibial metaphyseal fracture 1 year ago. She was treated with a long leg cast with a varus mold, and the fracture healed uneventfully. She now has a 15-degree valgus deformity. What is the next step in management?
Explanation
The tibia has grown into valgus secondary to the proximal fracture. This occurs in about one half of these injuries, and maximal deformity occurs at 18 months postinjury. The deformity gradually improves over several years, with minimal residual deformity. Therefore, treatment at this age is unnecessary as there is a high rate of recurrence and complications regardless of technique. The valgus deformity is not a result of physeal injury or growth arrest. Medial proximal tibial hemiepiphysiodesis is an excellent method of correcting the residual deformity but is best reserved until close to the end of growth. Brougham DI, Nicol RO: Valgus deformity after proximal tibial fractures in children. J Bone Joint Surg Br 1987;69:482. McCarthy JJ, Kim DH, Eilert RE: Posttraumatic genu valgum: Operative versus nonoperative treatment. J Pediatr Orthop 1998;18:518-521.
Question 87High Yield
When comparing the failure load of an evenly tensioned four-stranded hamstring tendon anterior cruciate ligament autograft to a 10-mm bone-patellar tendon-bone autograft, the hamstring graft will fail at a tension
Explanation
The failure load of an evenly tensioned four-stranded hamstring tendon autograft has been reported to be 4,500 Newtons. The failure load of a 10-mm patellar tendon autograft has been estimated at 2,600 Newtons. The intact anterior cruciate ligament failure load has been calculated at 1,725 Newtons. Corry IS, Webb JM, Clingeleffer AJ, Pinczewski LA: Arthroscopic reconstruction of the anterior cruciate ligament: A comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am J Sports Med 1999;27:448-454. Hamner DL, Brown CH Jr, Steiner ME, et al: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557.
Question 88High Yield
At the L4-5 level, what is the location of the S2-5 nerve roots in relationship to the L5 and S1 nerve roots?
Explanation
Explanation
The nerve roots of S2-5 are positioned dorsally and in the midline relative to the L5 and S1 nerve roots. The L5 nerve root is located lateral to S1 as it prepares to exit under the L5 pedicle. The S1 nerve root is located lateral and ventral to the S2-5 nerve roots. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 3-17.
References:
- Cohen MS, Wall EJ, Olmarker K, Rydevik BL, Garfin SR: Anatomy of the spinal nerve roots in the lumbar and lower thoracic spine, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman and Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, vol 1, pp 84-86.
Question 89High Yield
A 16-year-old boy has had thigh pain for the past several months. He denies any history of trauma. Examination reveals a large, deeply fixed, soft-tissue mass in the thigh. Laboratory results show an elevated erythrocyte sedimentation rate (ESR) and leukocytosis. A plain radiograph and MRI scan are shown in Figures 1a and 1b. Biopsy specimens are shown in Figures 1c and 1d. What is the most likely diagnosis?



Explanation
Ewing's sarcoma typically can occur in the diaphysis of the long bones (50% to 55%). It is often accompanied by a large soft-tissue mass. Abnormal findings are common, including a low-grade fever, an elevated ESR, and leukocytosis. The histology is consistent with a small round blue cell tumor. The unique pathology and other findings exclude osteosarcoma. Giant cell tumor and chondrosarcoma have a different histologic appearance and typically are more metaphyseal in location. Chondrosarcoma typically is found in older age groups, has a different histologic pattern, and rarely occurs in the midshaft of the femur.
Question 90High Yield
A 38-year-old man has winging of the ipsilateral scapula after undergoing a transaxillary resection of the first rib 3 weeks ago. What is the most likely cause of this finding?
Explanation
During transaxillary resection of the first rib, the long thoracic nerve is at risk as it passes either through or posterior to the middle scalene muscle. Injury to this nerve may occur as the result of overly aggressive retraction of the middle scalene during the procedure. Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Question 91High Yield
A 22-year-old patient sustained a jamming injury to the right little finger. The lateral radiograph shown in Figure 18 reveals comminution of the base of the middle phalanx, with palmar and dorsal metaphyseal cortical involvement. The articular surface also is disrupted. Management should consist of
Explanation
This fracture, known as a pilon fracture, represents comminution of the base of the middle phalanx with both palmar and dorsal cortical disruption. The treatment method that allows the best function and fewest complications is indirect reduction achieved through specific dynamic splinting or the use of specifically designed proximal interphalangeal joint external fixators. Early mobilization can be achieved by either of these techniques. Volar plate arthroplasty is indicated for a simple fracture-dislocation of the proximal interphalangeal joint with comminution of the volar fracture fragment and dorsal dislocation of the remaining articular surface. Open reduction and internal fixation or percutaneous pinning adds surgical risks and scarring and typically will not provide added stability. Cast immobilization will not achieve the goal of early range of motion. Stern PJ, Roman RJ, Kiefhaber TR, McDonough JJ: Pilon fractures of the proximal interphalangeal joint. J Hand Surg Am 1991;16:844-850.
Question 92High Yield
When compared to traditional open repair through a posterior incision, percutaneous Achilles tendon repair clearly results in a reduction of what complication?
Explanation
Prospective studies, including randomized and randomized multicenter reports, have shown that percutaneous or mini-open acute Achilles tendon repair has comparable functional results when compared to traditional open techniques. Calder and Saxby reported one superficial infection out of 46 patients with a mini-open repair; Assal and associates and Cretnik and associates had no wound complications or infections. The other complications have not proved to be less likely with the mini-open or percutaneous technique. Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures: A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am 2002;84:161-170. Calder JD, Saxby TS: Early, active rehabilitation following mini-open repair of Achilles tendon rupture: A prospective study. Br J Sports Med 2005;39:857-859.
Question 93High Yield
A 4-month-old infant is referred for evaluation of congenital scoliosis. The child has no congenital heart anomalies, and a renal ultrasound shows that he has one kidney. Examination reveals mild scoliosis and a large hairy patch on the child's back. Neurologic evaluation is normal for his age. A clinical photograph and radiograph are shown in Figures 19a and 19b. Initial management should consist of
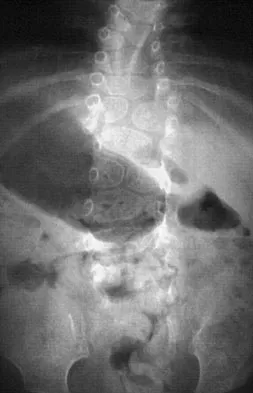
Explanation
Congenital anomalies of the spine, including failure of formation and failure of segmentation, are associated with other anomalies in other organ systems that develop at the same time. These include anomalies in the genitourinary system, cardiac anomalies, Sprengel's deformity, radial hypoplasia, and gastrointestinal anomalies including imperforate anus and trachealesophageal fistula. Spinal dysraphism is the most common associated abnormality. McMaster found an 18% incidence before the common use of MRI. Bradford and associates reported on 16 of 42 patients with congenital spinal anomalies and spinal dysraphism using MRI. Neural axis lesions may be associated with visible midline abnormalities such as a hairy patch or nevus. The child has already had a cardiac and renal work-up, and based on the findings of the hairy patch and congenital vertebral anomalies, MRI of the entire spine is prudent at this time. Spinal fusion is indicated for progressive congenital scoliosis or kyphosis. Physical therapy does not affect the natural history of congenital scoliosis. McMaster MJ: Occult intraspinal anomalies and congenital scoliosis. J Bone Joint Surg Am 1984;66:588-601. Bradford DS, Heithoff KB, Cohen M: Intraspinal abnormalities and congenital spine deformities: A radiographic and MRI study. J Pediatr Orthop 1991;11:36-41.
Question 94High Yield
A 19-year-old man has had intermittent progressive knee pain with ambulation and pain at night following a rodeo accident 4 weeks ago. Figures 4a through 4e show the radiographs, a bone scan, CT scan, and T2-weighted MRI scan. What is the most likely diagnosis?




Explanation
The imaging studies reveal a predominantly blastic lesion in the distal femur with posterolateral periosteal changes. The bone scan shows increased uptake in the distal femur, beyond that expected with radiography. Cross-sectional imaging confirms the presence of a soft-tissue mass extending from the lateral aspect of the femur, with diffuse intramedullary signal changes. This aggressive presentation, particularly in this location and in a patient of this age, is most consistent with osteosarcoma. The mineralization in the soft tissue strongly suggests neoplasm, not the reactive bony changes seen in an infectious process. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
Question 95High Yield
A 60-year-old woman has a mass in the right scapula. Figures 25a and 25b show a CT scan and a biopsy specimen. The cells are lymphocyte common antigen positive, Ewing's specific antigen (CD99) negative, and keratin negative. What is the next step in management?

Explanation
The clinical history, CT scan, and histology are most consistent with a lymphoma of bone. An important part of the staging is bone marrow aspiration and biopsy. The other studies listed are not indicated. Lymphoma of bone, when localized, is usually treated with chemotherapy and radiation therapy and has excellent survival rates. Widespread lymphoma has a worse prognosis. Finiewicz K, van Biesen K: Non-Hodgkins lymphoma, in Golomb H, Vokes E (eds): Oncologic Therapies, ed 2. Berlin, Germany, Springer, 2003, pp 295-318.
Question 96High Yield
A 17-year-old high school football player is seen for follow-up after sustaining an injury 3 days ago. He reports that he tackled a player, felt numbness throughout his body, and could not move for approximately 15 seconds. A spinal cord injury protocol was initiated on the field. Evaluation in the emergency department revealed a normal neurologic examination and full painless neck motion. He states that he has no history of a similar injury. An MRI scan of the cervical spine is normal. During counseling, the patient and his family should be informed that he has sustained
Explanation
The long-term effect of transient quadriplegia is unknown. Based on a history of one brief episode of transient quadriplegia and normal examination and MRI findings, the risk of permanent spinal cord injury with a return to play is low. There is a risk of recurrent episodes of transient quadriplegia after the initial episode. Morganti C, Sweeney CA, Albanese SA, et al: Return to play after cervical spine injury. Spine 2001;26:1131-1136. Odor JM, Watkins RG, Dillin WH, et al: Incidence of cervical spinal stenosis in professional and rookie football players. Am J Sports Med 1990;18:507-509. Torg JS, Naranja RJ Jr, Palov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Question 97High Yield
Glenohumeral inferior stability in the adducted shoulder position is primarily a function of the
Explanation
Explanation
When the arm is adducted, the superior structures, including the superior glenohumeral ligament, are responsible in limiting the inferior translation. With the arm abducted, the inferior glenohumeral ligament complex is responsible for limiting inferior subluxation. Rotator cuff activity can actually depress the humeral head and does not play a role in preventing inferior subluxation. The long head of the biceps and the posterior glenohumeral ligament do not play a role in protecting the shoulder from inferior instability. Warner JJ, Deng XH, Warren RF, Torzilli PA: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
References:
- Harryman DT II, Sidles JA, Harris SL, Matsen FA III: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
Question 98High Yield
A newborn with myelomeningocele has no movement below the waist and has bilateral hips that dislocate with provocative flexion and adduction. What is the best treatment option for the hip instability?
Explanation
Explanation
The status of the hips (located or dislocated) in children with thoracic-level myelomeningocele has no effect on the functional outcome of these patients. Management of unstable hips in this population should be limited to treatment of the contractures that may lead to poor limb positioning in either braces or a wheelchair. The use of the Pavlik harness and/or spica cast is contraindicated because they would promote flexion and abduction contractures. In the past, open reduction either through an anterior or medial approach had been performed with a high incidence of redislocation and other complications, with little functional gain for the child. Gabriel KG: Natural history of hip deformity in spina bifida, in Sarwark JR, Lubicky JP (eds): Caring for the Child With Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 89-103.
References:
- Schoenecker PL: Surgical management of hip problems in children with myelomeningocele, in Sarwark KR, Lubicky JP (eds): Caring for the Child With Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 117-131.
Question 99High Yield
Osteoclasts are primarily responsible for bone resorption of malignancy. Which of the following stimulates osteoclast formation?
Explanation
Explanation
Bone destruction is primarily mediated by osteoclastic bone resorption, and cancer cells stimulate the formation and activation of osteoclasts next to metastatic foci. Increasing evidence suggests that receptor activator of NF-kB ligand (RANKL) is the ultimate extracellular mediator that stimulates osteoclast differentiation into mature osteoclasts. In contrast, OPG inhibits osteoclast development. IL-8 but not IL-5 is known to play a role in osteoclastogenesis. MMP-2 and collagen type I do not have a direct role in osteoclastogenesis. Kitazawa S, Kitazawa R: RANK ligand is a prerequisite for cancer-associated osteolytic lesions. J Pathol 2002;198:228-236.
References:
- Einhorn TA: Metabolic bone diseases, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 100High Yield
Following a radial nerve neurapraxia at or above the elbow, return of muscle function can be expected to start at the brachioradialis and return along which of the following progressions?
Explanation
Explanation
Following a radial nerve neurapraxia above the elbow, muscle recovery can be expected in a predictable pattern. Although variations will occur, the return of function or reinnervation usually occurs in the following order: brachioradialis, extensor carpi radialis longus, supinator, extensor carpi radialis brevis, extensor carpi ulnaris, extensor digitorum comminus, extensor digiti minimi, extensor indicis proprious, extensor pollicis longus, abductor pollicis longus, and extensor pollicis brevis. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, p 53.
References:
- Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 428-429.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon