Orthopedic Lower Limb Deformity Correction: Biomechanics, Osteotomy & Guided Growth | Part 8

Key Takeaway
Lower limb deformity correction involves precise radiographic planning, understanding biomechanics like the mechanical axis and Center of Rotation of Angulation (CORA), and applying Paley's osteotomy rules for angular and translational corrections. Techniques include high tibial osteotomy, distal femoral osteotomy, and guided growth for pediatric cases, aiming to restore alignment and unload joints.
Question 1
A 16-year-old female with a complex multiapical femoral deformity requires a full-length standing radiograph for preoperative planning. To ensure a true AP projection of the knee and avoid misinterpretation of the deformity, how should the patient's lower extremities be positioned?
View Answer & Explanation
Correct Answer: B
Rationale: For accurate radiographic assessment of lower limb alignment, the standard position is standing with the patellae pointing straight forward (anteriorly). This neutral rotation provides a true AP view of the knee joint. Forcing maximal extension or specific foot positions can introduce rotational artifacts that alter the measured angles and mask or exaggerate the true deformity.
Question 2
A surgeon is performing a deformity analysis on a patient with genu varum. The first step in the mechanical axis planning method is to draw the proximal and distal axes of the bone. How is the proximal mechanical axis of the femur correctly drawn?
View Answer & Explanation
Correct Answer: B
Rationale: The mechanical axis of the femur is defined by a line connecting the center of the femoral head to the center of the knee. This represents the line of weight-bearing force transmission through the femur. The anatomic axis, represented by a line down the medullary canal, is different and has a normal valgus orientation relative to the mechanical axis.
Question 3
A 22-year-old patient has a varus deformity of the distal femur. Preoperative planning is performed on a full-length standing radiograph. The surgeon identifies the intersection of the proximal and distal mechanical axis lines. What does this point of intersection represent?
View Answer & Explanation
Correct Answer: B
Rationale: The center of rotation of angulation (CORA) is the point in space where the proximal axis of a bone segment intersects with the distal axis of that same bone segment. This is the apex of the angular deformity. Identifying the CORA is the fundamental first step in planning an accurate deformity correction.
Question 4
A 55-year-old male with medial compartment knee osteoarthritis and genu varum is undergoing preoperative planning for a high tibial osteotomy (HTO). The surgeon aims to shift the mechanical axis from the medial compartment to a point slightly lateral to the knee center. What is the name of the point on the tibial plateau that is 62% of the way from the medial to the lateral border?
View Answer & Explanation
Correct Answer: C
Rationale: The Fujisawa point is the target for mechanical axis realignment in a high tibial osteotomy for medial compartment osteoarthritis. It is located at 62.5% of the tibial plateau width from the medial edge. Correcting the mechanical axis to pass through this point has been shown to optimally unload the medial compartment and improve clinical outcomes.
Question 5
A surgeon is planning a corrective osteotomy for a distal femoral varus deformity. According to the three rules of osteotomy for angular correction, if the osteotomy is performed at the level of the CORA, what is the required surgical action to achieve perfect correction without creating a secondary translation deformity?

View Answer & Explanation
Correct Answer: A
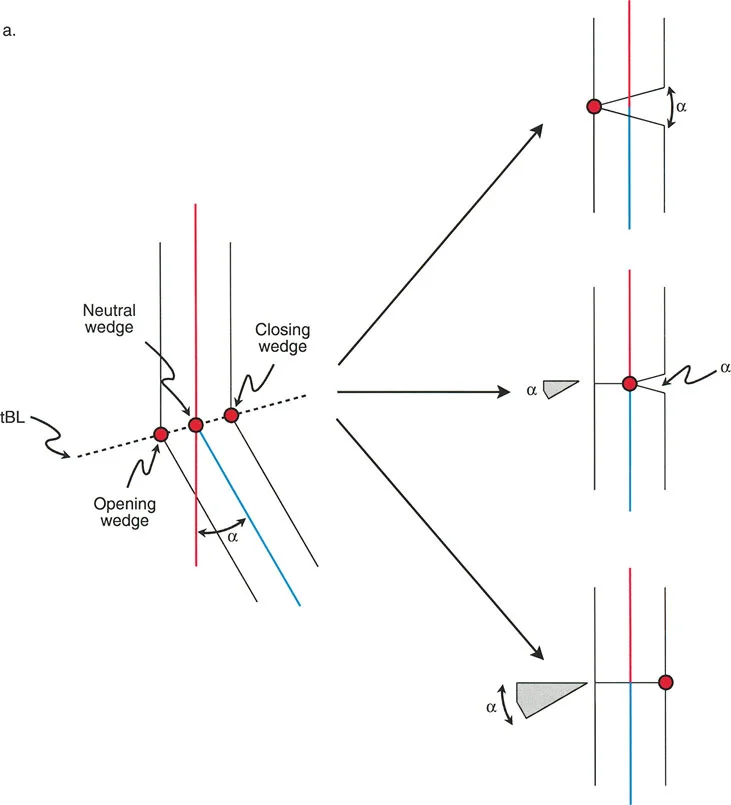
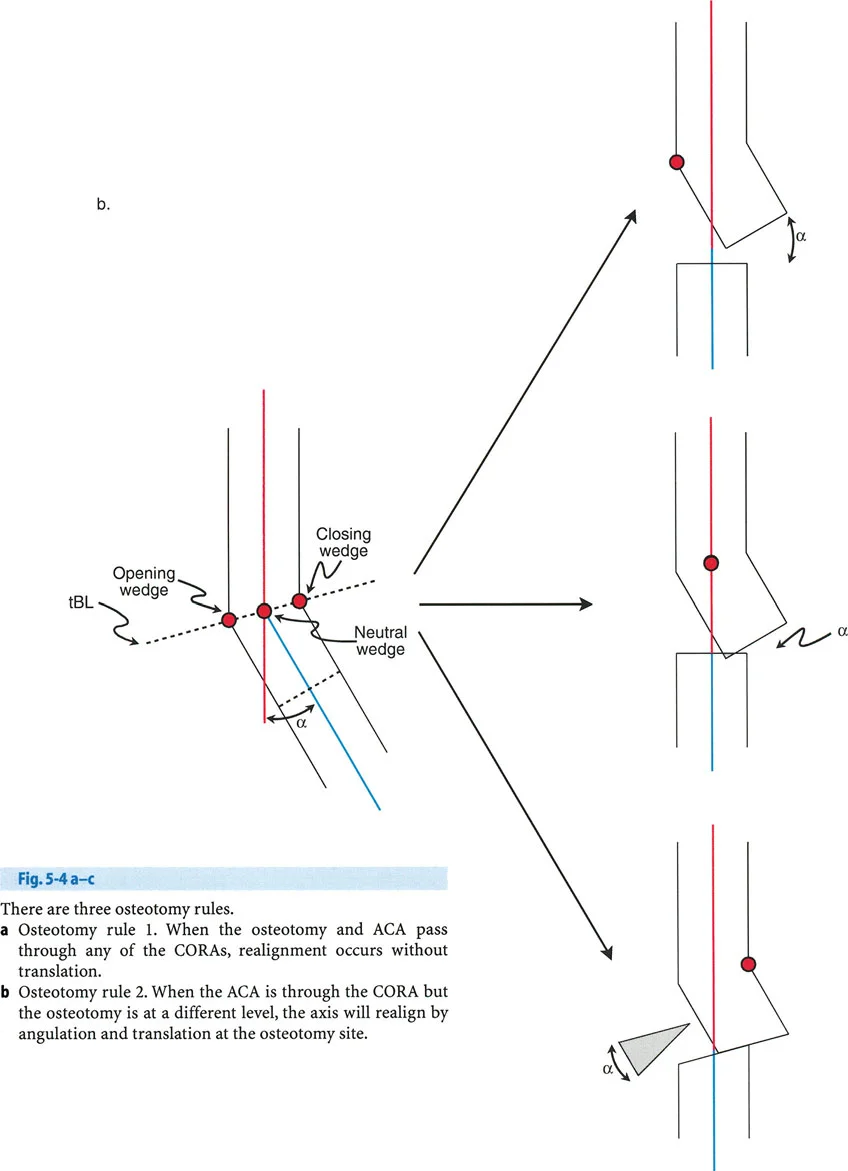
Rationale: Osteotomy Rule 1 states that if the osteotomy is performed at the CORA, only simple angular correction is needed. The bone fragments are simply angulated around the CORA, and the proximal and distal mechanical axes will align perfectly without any need for translation. Performing the osteotomy away from the CORA (Rule 2) necessitates both angulation and translation for perfect correction.
Question 6
A 19-year-old male has a 20° varus deformity of the proximal tibia with the CORA located in the metaphysis. The surgeon plans a closing wedge osteotomy but performs it 2 cm distal to the CORA. To achieve perfect mechanical axis alignment, what additional maneuver is required besides closing the 20° wedge?
View Answer & Explanation
Correct Answer: E
Rationale: Osteotomy Rule 2 states that when an osteotomy for angular correction is performed at a level other than the CORA, a translation is induced. For a varus deformity corrected with a closing wedge osteotomy distal to the CORA, the distal fragment will be translated medially relative to the proximal fragment. To realign the mechanical axis, a compensatory lateral translation of the distal fragment is required.
Question 7
A 28-year-old female has a 15° valgus deformity of the distal femur. The surgeon plans an opening wedge osteotomy proximal to the CORA. After the wedge is opened to correct the angulation, what secondary deformity will be created if no translation is performed?
View Answer & Explanation
Correct Answer: A
Rationale: According to the principles of deformity correction, performing an opening wedge osteotomy for a valgus deformity at a level proximal to the CORA will result in a medial translation of the distal fragment. To achieve perfect axis correction, a compensatory lateral translation would be necessary. Lateral translation would occur if the osteotomy was distal to the CORA.
Question 8
A 40-year-old patient is evaluated for a complex tibial deformity. Radiographs reveal a multiapical deformity in the frontal plane, with a varus CORA in the proximal tibia and a valgus CORA in the distal tibia. Which of the following is the most appropriate strategy for correction?

View Answer & Explanation
Correct Answer: D
Rationale: For a multiapical deformity, correcting the overall malalignment with a single osteotomy will realign the limb but will create a new, compensatory deformity and malorient the joint surfaces. The correct principle is to address each deformity at its apex (CORA) with a separate osteotomy to restore both limb alignment and normal joint orientation.
Question 9
A 25-year-old male has a significant tibial procurvatum deformity. A lateral radiograph is obtained for sagittal plane analysis. The surgeon measures the angle between the proximal tibial anatomic axis and the proximal tibial joint line. What is this angle called, and what is its normal value?

View Answer & Explanation
Correct Answer: B
Rationale: The posterior proximal tibial angle (PPTA) measures the sagittal alignment of the proximal tibia. It is the angle between the anatomic axis of the tibia and the proximal tibial joint line, measured posteriorly. The normal value is 81° (range 77°-84°). A value less than 77° indicates a procurvatum (apex anterior) deformity, while a value greater than 84° indicates a recurvatum (apex posterior) deformity.
Question 10
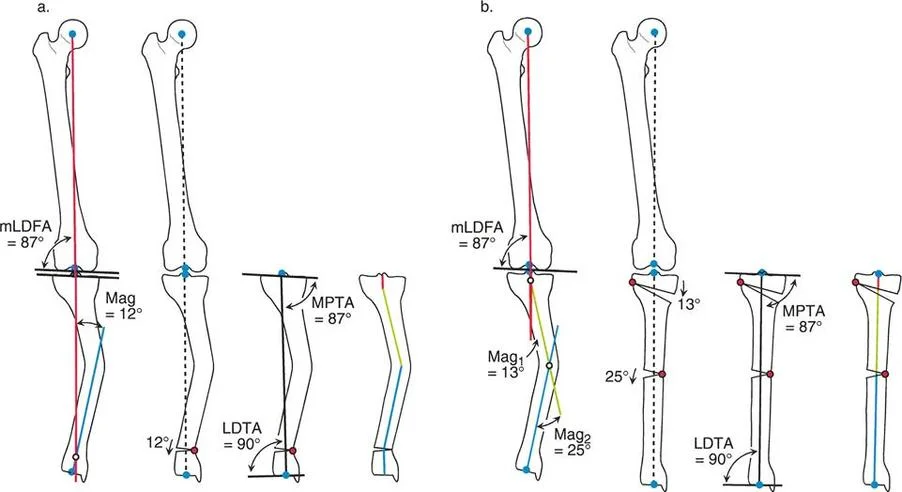
A 33-year-old patient presents with a complex deformity of the tibia involving 15° of varus and 20° of procurvatum. The surgeon is using the graphic method to determine the true magnitude and plane of the deformity. After plotting the varus and procurvatum vectors on an axial grid, what is the next step to find the magnitude of the oblique plane deformity?

View Answer & Explanation
Correct Answer: C
Rationale: The graphic method for oblique plane deformities treats the frontal and sagittal plane angulations as two perpendicular vectors. The true magnitude of the deformity is the hypotenuse of the right triangle formed by these vectors. Therefore, the Pythagorean theorem is used: Magnitude = √(AP_angulation² + LAT_angulation²). In this case, Magnitude = √(20² + 15²) = √625 = 25°.
Question 11
A patient has a pure translational deformity of the mid-diaphysis of the femur, with the distal fragment translated 2 cm medially relative to the proximal fragment. There is no angular deformity. What is the most appropriate osteotomy strategy to correct this deformity?

View Answer & Explanation
Correct Answer: D
Rationale: A pure translation deformity is corrected by creating a bone segment that can be moved into the correct position without changing angulation. This is achieved by making two parallel osteotomies, which isolates a segment of bone. This segment is then translated laterally to realign the bone, and the construct is fixed. A wedge osteotomy is used to correct an angular deformity and would be inappropriate here.
Question 12
A 20-year-old patient has a distal tibial deformity with 20° of varus and 15° of internal rotation. The surgeon plans a single-cut osteotomy to correct both deformities simultaneously. How must the osteotomy plane be oriented relative to the bone to achieve this combined correction?
View Answer & Explanation
Correct Answer: D
Rationale: To correct a combined angular and rotational deformity with a single osteotomy, the osteotomy must be inclined relative to the bone's long axis. The angle of this inclination determines the ratio of angular to rotational correction achieved when the bone is derotated around its long axis. A perpendicular cut can only correct angulation (with a wedge) or rotation (by spinning the fragments), but not both simultaneously with a single maneuver.
Question 13
A 26-year-old male requires a 35° angular correction and 4 cm of lengthening for a complex femoral deformity. Due to the magnitude of the correction and the associated soft-tissue tension, the surgeon is concerned about neurovascular compromise. Which of the following is the safest approach?
View Answer & Explanation
Correct Answer: C
Rationale: For large angular corrections (>30-40°) or when significant lengthening is also required, gradual correction using an external fixator is the safest method. This approach minimizes the risk of neurovascular injury and compartment syndrome that can occur with acute, large-magnitude corrections that place the soft-tissue envelope under excessive tension. The fixator allows for slow, controlled correction of all deformity parameters.
Question 14
A surgeon is performing a percutaneous osteotomy of the proximal tibia using a Gigli saw. To protect the neurovascular structures in the popliteal fossa, the Gigli saw is passed from anteromedial to anterolateral around the posterior cortex. Which structure is most at risk if the saw is passed improperly from the posteromedial side?

View Answer & Explanation
Correct Answer: C
Rationale: The popliteal artery and vein are the most central and vulnerable structures in the popliteal fossa during a proximal tibial osteotomy. The standard technique involves passing instruments from anterior to posterior, staying on the bone, to avoid these structures. Passing a saw from the posteromedial side would place the popliteal artery and vein directly in its path. The common peroneal nerve is more posterolateral and is also at risk, but the popliteal vessels are most central.
Question 15
A 62-year-old male presents with progressive right knee pain. He denies any history of inflammatory arthritis. On examination, he has a varus thrust and tenderness over the medial joint line. Radiographs show isolated medial compartment joint space narrowing. When counseling the patient, you explain the biological limitations of his articular cartilage. Which of the following properties is most responsible for the notoriously limited repair capacity of articular cartilage?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that articular cartilage's capacity for repair is "notoriously limited due to its avascular, aneural, and alymphatic nature." This prevents an inflammatory or cellular healing response. Articular cartilage is primarily Type II collagen (A is incorrect), and it lacks a direct vascular supply (B is incorrect).
Question 16
A 55-year-old woman with a history of a malunited tibial plateau fracture presents with knee pain. There is no morning stiffness, and inflammatory markers are normal. You diagnose her with mechanically-driven, degenerative joint disease. According to the provided text, what is the most pathologically accurate term for this condition?
View Answer & Explanation
Correct Answer: D
Rationale: The text emphasizes that "arthrosis is the preferred terminology for describing the purely degenerative, mechanically driven pathological abnormalities of the joint." It clarifies that inflammation is a secondary cascade, not the primary cause, making "degenerative arthritis" technically inaccurate.
Question 17
A 48-year-old male presents with isolated medial compartment knee pain and a varus deformity. He asks if his cartilage was "bad to begin with." Based on the consensus described in the provided text, which of the following best describes the primary pathogenesis of his condition?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that substantial evidence supports the hypothesis that "malalignment alters stress distribution across the joints...creating eccentric focal overloading that destroys normal cartilage." This refutes the idea that the cartilage is inherently abnormal before the mechanical insult (A is incorrect).
Question 18
A resident is preparing a presentation on lower extremity deformity. They are asked to define the mechanical axis of the lower extremity as pioneered by Friedrich Pauwels. Which of the following is the correct definition?
View Answer & Explanation
Correct Answer: C
Rationale: The text defines the mechanical axis of the lower extremity as "a straight line passing from the center of the ankle (the center of the tibial plafond) to the center of the hip (the center of the femoral head)." The line down the intramedullary canal is the anatomic axis (A is incorrect).
Question 19
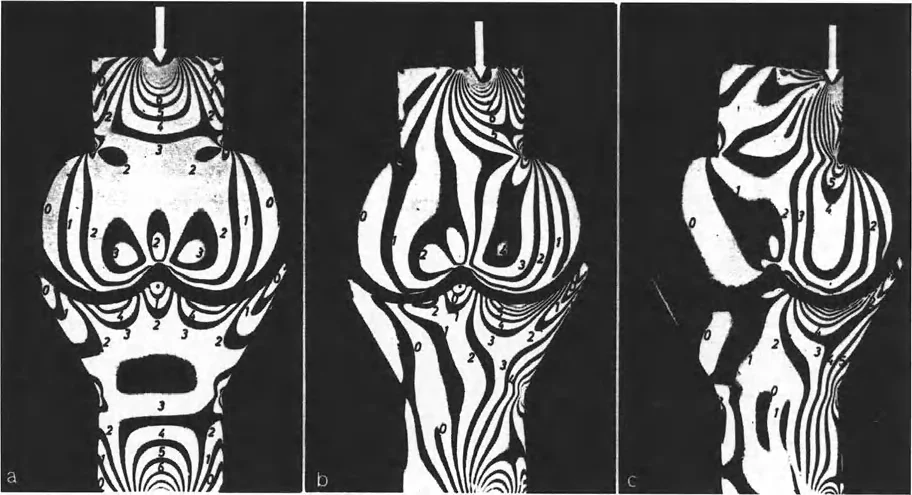
During a conference on high tibial osteotomy, the speaker discusses the historical work of Paul Maquet, who expanded on Pauwels' principles. What was Maquet's primary contribution to understanding the biomechanics of deformity correction?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states, "Paul Maquet later expanded on Pauwels' groundbreaking ideas. He elegantly demonstrated the alteration in stress transmitted across simulated joints using polarized light and photoelastic models." This work provided visual verification of the biomechanical principles of realignment.
Question 20
A 58-year-old active male with significant medial compartment arthrosis and varus malalignment is considering a high tibial osteotomy. He wants to understand the goal of the surgery. What is the primary mechanical objective of performing an osteotomy to place his varus knee into slight valgus?
View Answer & Explanation
Correct Answer: D
Rationale: The text explains that by shifting the mechanical axis, "the surgeon can effectively 'unload' the damaged compartment, providing profound pain relief and delaying the need for arthroplasty." While appearance may improve (A), the primary goal is mechanical unloading to halt the progression of arthrosis.
Question 21
A surgeon is planning a complex multi-level osteotomy. According to the Paley method, two distinct but interrelated concepts must be evaluated: Joint Alignment and Joint Orientation. Which of the following best defines Joint Orientation?
View Answer & Explanation
Correct Answer: B
Rationale: The text defines Joint Orientation as "the position (or angle) of each specific articular surface relative to the mechanical and anatomic axes of the individual limb segments." Joint Alignment refers to the collinearity of the joint centers (A is incorrect).
Question 22
A 45-year-old patient with a suspected femoral deformity is sent for imaging. The referring physician ordered standard AP and lateral views of the knee. For accurate deformity planning, what is the required radiographic study?
View Answer & Explanation
Correct Answer: C
Rationale: The text is unequivocal: "Alignment and orientation can only be accurately judged using standing, long anteroposterior (AP) view radiographs of the entire lower extremity on a single cassette (a 51-inch film). Supine films or short knee films are entirely inadequate for deformity planning."
Question 23
A radiology technician is preparing to take a long-leg alignment radiograph for a patient with a valgus knee. To ensure the coronal plane measurements are valid, how should the patient's leg be positioned?
View Answer & Explanation
Correct Answer: B
Rationale: The text provides a "Surgical Pearl" stating, "The radiograph is only valid if the patella is perfectly centered between the femoral condyles and directed straight forward." It specifically warns against positioning based on the foot (A is incorrect).
Question 24
A 30-year-old patient with significant external tibial torsion is undergoing evaluation for a proximal tibial osteotomy. The technician positions the patient with the foot pointing straight ahead for the alignment radiograph. Why is this technique incorrect?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly warns, "If the patient has external tibial torsion, positioning the foot forward will internally rotate the knee, completely invalidating the coronal plane measurements. Always shoot the X-ray based on the knee (patella forward)."
Question 25
When planning an osteotomy of the tibia, a surgeon must understand the relationship between the bone's mechanical and anatomic axes. Which of the following accurately describes this relationship in the tibia?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "In the tibia, the mechanical axis...and the anatomic axis...are virtually identical. They are parallel and superimposed." The 6-degree difference is characteristic of the femur (A is incorrect).
Question 26
A junior resident is templating a distal femoral osteotomy and is confused about the difference between the femoral mechanical and anatomic axes. Which statement correctly describes the anatomic axis of the femur?
View Answer & Explanation
Correct Answer: C
Rationale: The text defines the anatomic axis of the femur as running "from the piriformis fossa down the medullary canal to the center of the knee." The line from the center of the femoral head to the center of the knee is the mechanical axis of the femur (A is incorrect).
Question 27
During preoperative planning for a total knee arthroplasty using an intramedullary femoral guide, the surgeon must account for the natural relationship between the femur's anatomic and mechanical axes. What is the typical angle subtended between these two axes?
View Answer & Explanation
Correct Answer: C
Rationale: The text clearly states, "Typically, the anatomic axis subtends a 6° angle (range 5° to 7°) to the mechanical axis of the femur." This is a critical value for both deformity correction and arthroplasty.
Question 28
A study is conducted on 100 asymptomatic adult volunteers to establish normative lower limb alignment. A line is drawn from the center of the femoral head to the center of the ankle on long-leg standing radiographs. Where does this line typically pass relative to the center of the knee?
View Answer & Explanation
Correct Answer: B
Rationale: The text notes that while textbooks often show the axis passing through the center, "clinical studies on asymptomatic volunteers reveal a slight physiological variance. A line drawn from the center of the femoral head to the center of the ankle typically passes *immediately medial* to the center of the knee," resulting in about 1.2° to 1.3° of physiological varus.
Question 29
A 50-year-old patient has a varus deformity of the lower limb. The surgeon measures the perpendicular distance from the weight-bearing axis to the center of the knee joint. What is this measurement called?
View Answer & Explanation
Correct Answer: B
Rationale: The text defines Mechanical Axis Deviation (MAD) as the length of a perpendicular line segment extending from the mechanical axis line to the exact geometric center of the knee joint. This value, measured in millimeters, quantifies the magnitude of the malalignment.
Question 30
A surgeon is evaluating a long-leg alignment film. To accurately measure the Mechanical Axis Deviation (MAD), what two points must be identified to draw the primary reference line?
View Answer & Explanation
Correct Answer: B
Rationale: The measurement of MAD begins by drawing the mechanical axis of the lower extremity, which is defined as "a straight line from the center of the femoral head to the center of the tibial plafond." The MAD is then the perpendicular distance from this line to the knee center.
Question 31
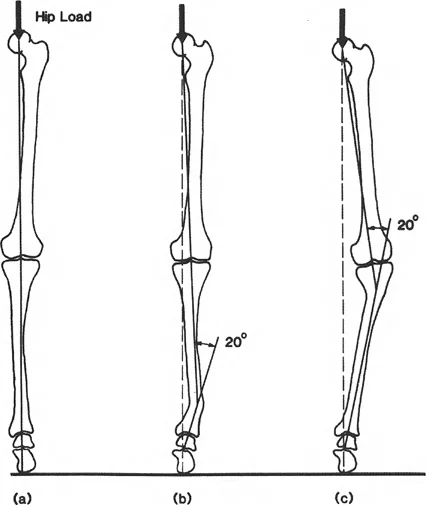
When comparing two patients with 10 degrees of varus deformity, one patient has the deformity in the proximal tibia and the other has it in the mid-femoral diaphysis. The patient with the proximal tibial deformity has significantly more knee pain and arthrosis. This is best explained by which biomechanical principle?
View Answer & Explanation
Correct Answer: C
Rationale: The text describes the Apex Multiplier Effect, stating that "the effect of an angular deformity on the overall mechanical axis increases exponentially as the apex of the deformity approaches the knee joint." Therefore, periarticular deformities are far more destructive than diaphyseal ones of the same magnitude.
Question 32
A 40-year-old patient has a 15-degree varus deformity from a malunited femoral shaft fracture. A second 40-year-old patient has a 15-degree varus deformity from Blount's disease affecting the proximal tibia. According to the principles outlined, which patient is expected to have a larger Mechanical Axis Deviation (MAD) and more severe mechanical consequences at the knee?
View Answer & Explanation
Correct Answer: B
Rationale: This is a clinical application of the Apex Multiplier Effect. The deformity in the proximal tibia is periarticular (closer to the knee), which will produce a much larger MAD and greater mechanical overload compared to the diaphyseal deformity in the femur, even though the angular magnitude is the same.
Question 33
A 34-year-old male presents with a painful varus deformity of the proximal tibia following a malunited fracture. During preoperative planning, the surgeon draws the proximal and distal mechanical axis lines of the tibia. According to the principles of deformity correction, what is the geometric point where these two lines intersect called?
View Answer & Explanation
Correct Answer: B
Rationale: The Center of Rotation of Angulation (CORA) is fundamentally defined as the point of intersection between the proximal mechanical (or anatomic) axis line and the distal mechanical (or anatomic) axis line. The ACA is the hinge point of the correction, which is a surgical choice.
Question 34
A surgeon is planning a corrective osteotomy for a 22-year-old patient with a distal femoral valgus deformity. The surgeon has identified the CORA and is now deciding on the hinge point around which the distal bone segment will rotate to achieve correction. What is this surgically determined hinge point known as?
View Answer & Explanation
Correct Answer: C
Rationale: The Angulation Correction Axis (ACA) represents the hinge point around which the distal bone segment rotates. While the CORA is a fixed property of the deformity, the ACA is a variable under the surgeon's control.
Question 35
A 40-year-old female undergoes a corrective osteotomy for a diaphyseal femoral malunion. Postoperatively, the limb has a corrected mechanical axis, but there is a noticeable "bump" at the osteotomy site, creating a zigzag appearance of the anatomic axis. According to Paley's rules, which scenario most likely occurred?
View Answer & Explanation
Correct Answer: B
Rationale: Paley's Rule 2 states that if the ACA passes through the CORA but the osteotomy is at a different level, the angular deformity is corrected perfectly, but the bone ends translate relative to one another, creating an anatomic "bump." Placing both away from the CORA (Rule 3) would result in residual mechanical axis deviation.
Question 36
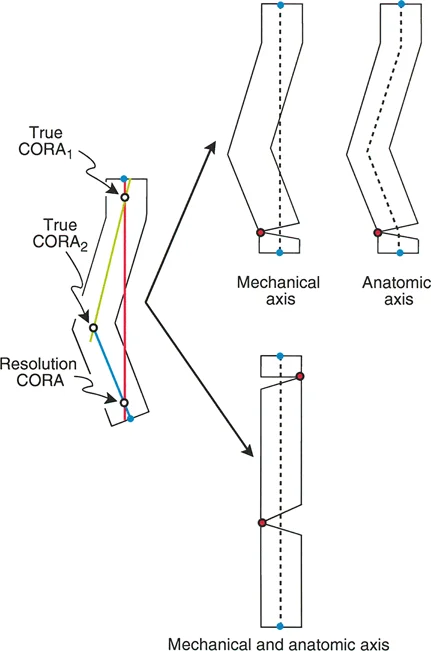
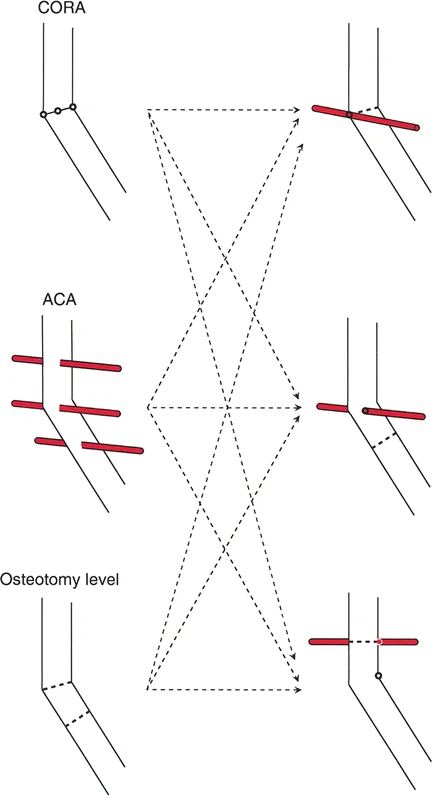
A surgeon is planning a single osteotomy to correct a multiapical femoral deformity in a patient with Paget's disease. The surgeon draws the most proximal axis line and the most distal axis line, ignoring the intermediate bowing, to find their intersection point. What is this specific intersection point called?
View Answer & Explanation
Correct Answer: D
Rationale: The Resolution CORA is the singular point of intersection between the most proximal axis line and the most distal axis line of a multiapical deformed bone. True CORAs are the actual apices of the individual deformities, found by intersecting with a middle axis line.
Question 37
A 28-year-old patient has a post-traumatic varus deformity of the femur. The surgeon plans an opening wedge osteotomy. To achieve a perfect correction with no iatrogenic translation or residual mechanical axis deviation, what is the ideal relationship between the osteotomy, the ACA, and the CORA?
View Answer & Explanation
Correct Answer: A
Rationale: Paley's Rule 1 describes the ideal scenario for perfect correction. When both the osteotomy cut and the Angulation Correction Axis (ACA) pass directly through the CORA, the angular deformity is corrected without inducing any secondary translation, resulting in a perfectly collinear mechanical axis.
Question 38
A 55-year-old male undergoes a high tibial osteotomy for medial compartment arthritis and varus deformity. Postoperative radiographs show that the mechanical axis is now shifted laterally, passing through the lateral tibial spine, and there is significant translation at the osteotomy site. This outcome is most consistent with which surgical error?
View Answer & Explanation
Correct Answer: C
Rationale: Paley's Rule 3 states that if the ACA and the osteotomy are placed away from the CORA, a secondary translation deformity is induced. This results in the mechanical axes becoming parallel but not collinear, causing a residual Mechanical Axis Deviation (MAD). Placing the ACA at the CORA (Option B) would have corrected the mechanical axis perfectly, despite creating an anatomic bump.
Question 39
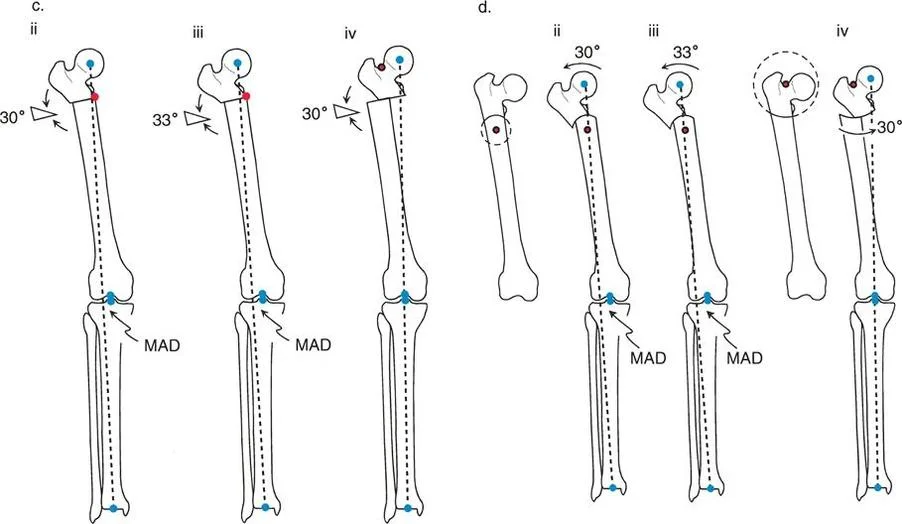
A surgeon is planning a corrective osteotomy for a 30° proximal femoral varus deformity. If the osteotomy is performed distal to the CORA and the ACA (hinge) is placed at the osteotomy line on the lateral cortex, what will be the result of a 30° angular correction?
View Answer & Explanation
Correct Answer: B
Rationale: This scenario violates Paley's rules. By placing the ACA at the osteotomy site, which is away from the CORA, a secondary translation is induced. In this case, the distal femur translates medially, resulting in a residual lateral MAD despite the 30° angular correction.
Question 40
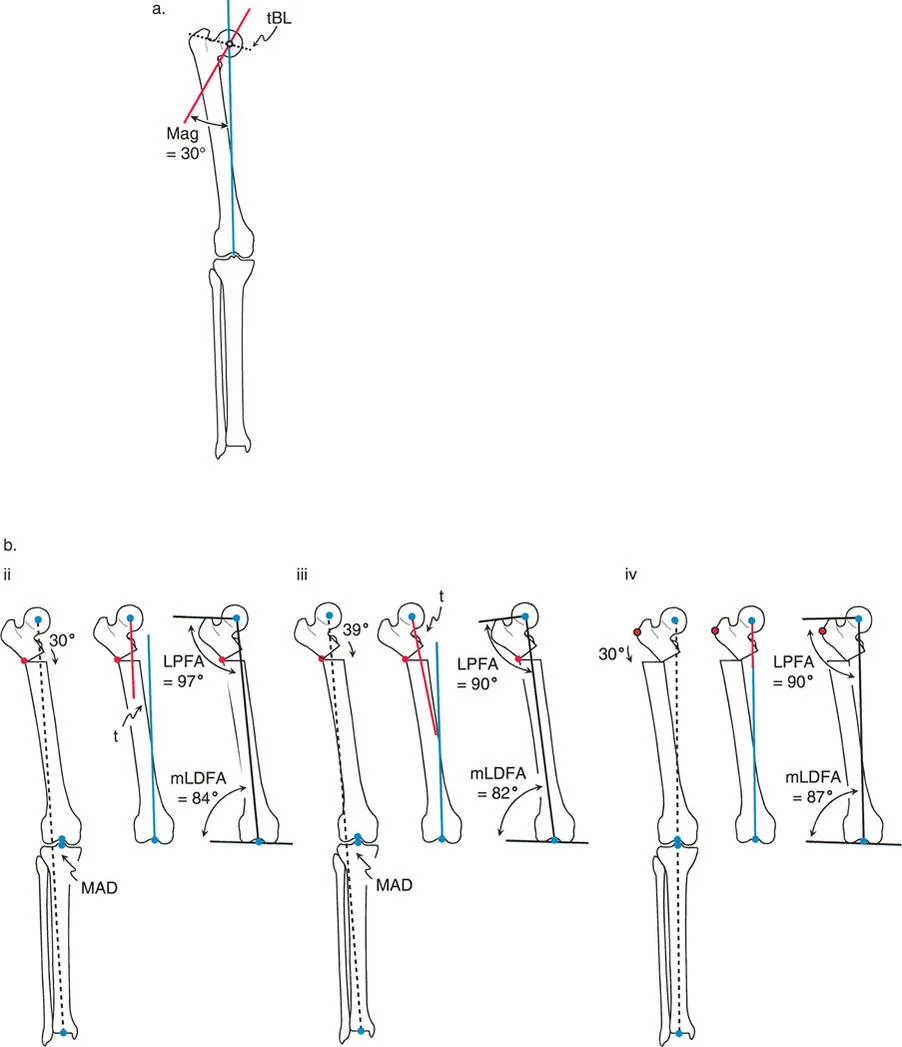
During planning for a proximal femoral varus correction, a surgeon places the osteotomy distal to the CORA with the ACA at the osteotomy site. To achieve a normal mechanical Lateral Proximal Femoral Angle (mLPFA) of 90°, a 39° correction is required for the 30° deformity. What is the primary negative consequence of this 9° overcorrection?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that this overcorrection, required to normalize the hip joint (mLPFA), severely compromises the knee by creating an abnormal valgus orientation and also results in a lateral MAD. The primary goal is to normalize both proximal and distal joint orientation, which this maneuver fails to do.
Question 41
A surgeon plans a focal dome osteotomy to correct a 30° proximal femoral varus deformity. To achieve a perfect correction with normalization of the mechanical axis, anatomic axis, and joint orientations, where must the center of the circular osteotomy cut be placed?
View Answer & Explanation
Correct Answer: D
Rationale: The ideal solution described is the "Focal Dome Osteotomy," where the center of the circular osteotomy cut is placed precisely at the CORA. This allows a pure 30° angular correction to completely eliminate MAD and normalize all axes and joint orientations.
Question 42
A 17-year-old with osteogenesis imperfecta has a multiapical deformity of the femur. The surgeon plans a single osteotomy. Preoperative analysis reveals that the Resolution CORA lies within the bone, between the hip and knee joints. If a single osteotomy with pure angular correction is performed at this Resolution CORA, what is the expected outcome?
View Answer & Explanation
Correct Answer: C
Rationale: When the Resolution CORA is within the bone, a single osteotomy at this point can correct the overall mechanical axis and joint orientations. However, the text clearly states the trade-off: this solution leaves the anatomic axis with residual angulation at multiple levels, creating a "zigzag" appearance.
Question 43
A patient with a complex tibial deformity is evaluated. The proximal and distal mechanical axes are found to be parallel but translated relative to one another. What does this geometric finding imply?
View Answer & Explanation
Correct Answer: B
Rationale: If the proximal and distal axis lines are parallel, they will never intersect. By definition, the CORA is the intersection of these lines. Therefore, there is no Resolution CORA, and the deformity is one of pure translation.
Question 44
A surgeon is planning a multi-level osteotomy for a severe multiapical deformity. To determine the location of the individual osteotomies for a perfect anatomic correction, the surgeon must identify the "True CORAs". How are these points located?
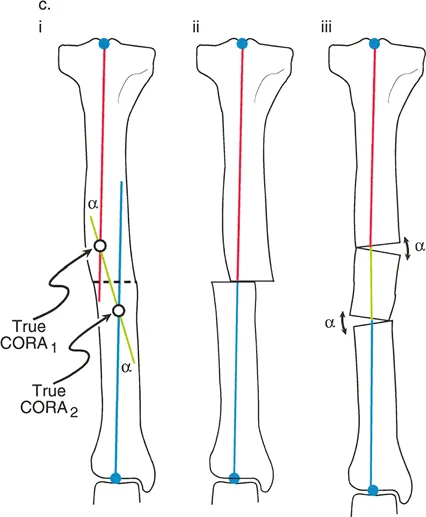
View Answer & Explanation
Correct Answer: C
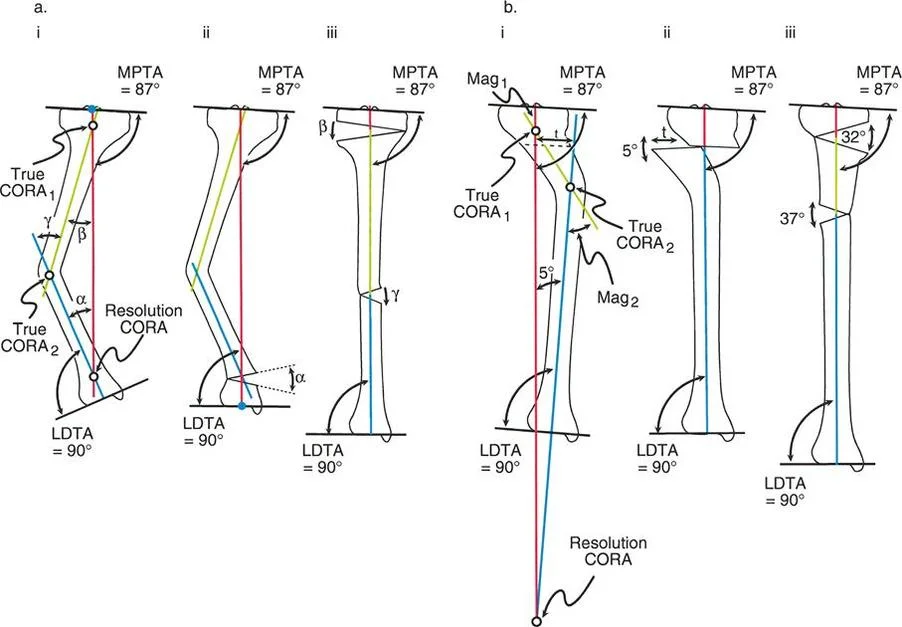
Rationale: The text defines True CORAs as the intersection points created when the proximal axis line and the distal axis line are drawn to intersect with a "true middle axis line" representing the intermediate bone segment. This is the fundamental step in planning a multi-level osteotomy for anatomic correction.
Question 45
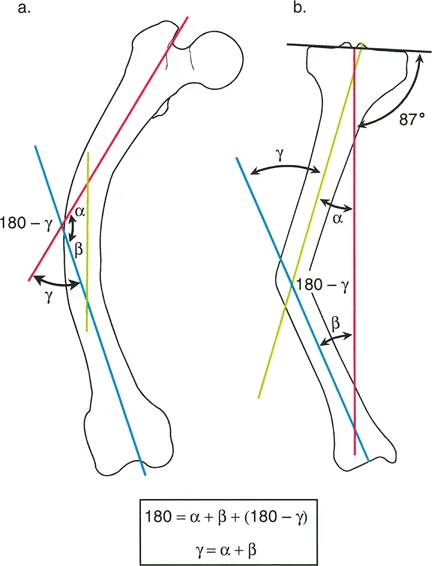
A patient has a multiapical tibial deformity with a 25° varus bow proximally and a 10° valgus bow distally. Using the sign convention where varus is positive and valgus is negative, what is the magnitude of the single resolved angle (γ)?
View Answer & Explanation
Correct Answer: B
Rationale: The formula is Resolved Angle (γ) = Angle 1 (α) + Angle 2 (β). Assigning varus as positive and valgus as negative: γ = (+25°) + (-10°) = +15°. A positive result indicates a net varus deformity of 15°.
Question 46
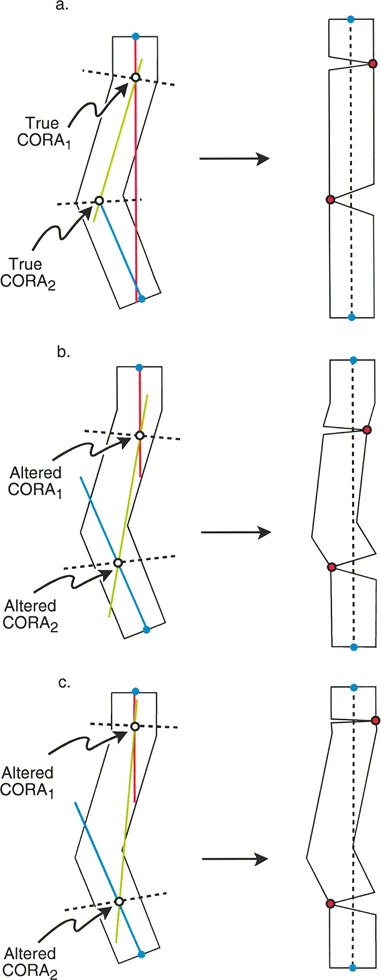
A surgeon identifies the True CORAs for a multiapical deformity, but one True CORA is located in an area with poor soft tissue coverage from a previous open fracture. The surgeon modifies the plan by altering the orientation of the middle axis line to create new intersection points in a healthier location. What are these new, surgically chosen intersection points called?
View Answer & Explanation
Correct Answer: E
Rationale: The text describes this exact technique. When the surgeon manipulates the middle axis line to change the osteotomy levels, the new intersection points are called Altered CORAs. This technique is useful for avoiding compromised areas.
Question 47
A 9-year-old child presents with a severe diaphyseal varus deformity of the tibia due to Streeter's dysplasia. Preoperative planning reveals a 10° valgus deformity in the proximal metaphysis and a 23° varus deformity at the diaphyseal bow. According to the case example, what is the most appropriate surgical solution?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical example for Streeter's dysplasia explicitly describes a multiapical problem with two True CORAs (proximal valgus and diaphyseal varus). The solution presented is a double-level correction: a varus-producing osteotomy proximally to correct the valgus, and a valgus-producing osteotomy in the diaphysis to correct the varus bow.
Question 48
A 2-year-old presents with a congenital posteromedial bow of the tibia. Deformity analysis shows the intersection of the proximal and distal mechanical axes (the Resolution CORA) is located just above the ankle joint. A single-level osteotomy is performed at this Resolution CORA. What is the most likely outcome?
View Answer & Explanation
Correct Answer: A
Rationale: The text describes this exact scenario. A single osteotomy at the Resolution CORA for a multiapical problem like a posteromedial bow will fully correct the MAD and normalize joint orientation. However, it is a single-level solution for a multi-level problem, so it leaves a biomechanically insignificant but visible residual bow in the anatomic axis.
Question 49
A 65-year-old male with genu varum is evaluated. During a relaxed, double-leg stance with feet shoulder-width apart, what percentage of his body weight is supported by each knee joint, assuming symmetrical weight distribution?
View Answer & Explanation
Correct Answer: B
Rationale: The text states that in a relaxed double-leg stance, each knee joint supports approximately 43% of the total body weight. The remaining 7% is the weight of the lower legs and feet. 50% is a common distractor but does not account for the weight of the limbs below the knee.
Question 50
A 45-year-old woman is being evaluated for a lower extremity deformity. A gait analysis is performed. During a normal single-leg stance, the Ground Reaction Vector (GRV) is directed from the foot towards the center of gravity of the "passenger unit." This anatomical landmark corresponds to which vertebral level?

View Answer & Explanation
Correct Answer: D
Rationale: The provided text and diagram explicitly state that the center of gravity for the passenger unit (head, arms, and trunk) is at the T10 vertebra level. S2 is the center of gravity for the entire body, which is a key distinction and a common distractor.
Question 51
A 58-year-old male with severe hip abductor weakness is observed to have a significant lateral trunk and pelvic tilt during the stance phase of gait. This gait pattern is best described as which of the following?
View Answer & Explanation
Correct Answer: C
Rationale: The text describes a Duchenne gait as a significant lateral tilt of the trunk and pelvis to bring the center of gravity directly over the hip during single-leg stance. This is a highly energy-inefficient compensation. While related to Trendelenburg gait (which is the pelvic drop), the text specifically labels the trunk lurch compensation as a Duchenne gait.
Question 52
A biomechanical study is conducted to estimate knee joint loading during normal gait. Based on models using the Ground Reaction Vector (GRV), what is the mean percentage of total weight borne by the medial compartment of a normally aligned knee during single-leg stance?
View Answer & Explanation
Correct Answer: E
Rationale: The text cites Hsu et al. (1990), who estimated that the medial compartment bears a mean of 75% of the total weight borne by the knee during simulated single-leg stance. 68% is the load produced by a 1° mechanical tibiofemoral angle, but 75% is the value cited for the mean load estimation.
Question 53
A 62-year-old female with medial compartment knee osteoarthritis reports her pain is worst just after her heel strikes the ground. During gait analysis, the knee adductor moment is found to be at its maximum. This corresponds to which portion of the stance phase?
View Answer & Explanation
Correct Answer: C
Rationale: The text specifies that the adductor moment around the knee is greatest during the first 10% to 15% of the stance phase, which is the initial stance or loading response. This is when the opposite foot has just left the ground.
Question 54
A surgeon is planning a corrective osteotomy for a 25-year-old male with a post-traumatic tibial varus deformity. The surgeon draws a line from the center of the femoral head to the center of the ankle mortise. The perpendicular distance from this line to the center of the knee joint is measured. What does this measurement represent?
View Answer & Explanation
Correct Answer: C
Rationale: The Mechanical Axis Deviation (MAD) is defined as the perpendicular distance from the center of the knee joint to the mechanical axis line (femoral head center to ankle center). The CORA is the apex of the deformity, not a measure of overall limb alignment deviation.
Question 55
During preoperative planning for a femoral osteotomy, the surgeon identifies the intersection point of the proximal mechanical axis line and the distal mechanical axis line of the femur. According to Paley principles, what is this critical point called?
View Answer & Explanation
Correct Answer: B
Rationale: The Center of Rotation of Angulation (CORA) is precisely defined as the geometric apex of a deformity, where the proximal and distal mechanical axis lines of a bone intersect. Performing the osteotomy at the CORA allows for pure angular correction.
Question 56
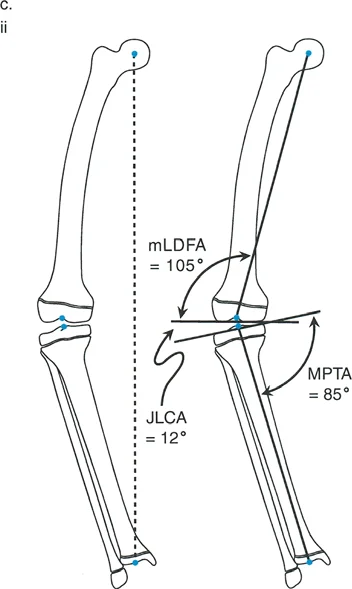
A 30-year-old patient has a valgus deformity of the knee. Radiographic analysis reveals a Mechanical Lateral Distal Femoral Angle (mLDFA) of 94°. Based on this finding, where is the primary source of the deformity?
View Answer & Explanation
Correct Answer: B
Rationale: The normal mLDFA is 85° to 90°. An angle greater than 90° indicates a distal femoral varus deformity (genu varum), not valgus. This question tests the precise definition from the table. The patient's overall valgus alignment must therefore have a more significant compensatory deformity elsewhere, but the mLDFA itself points to femoral varus.
Question 57
A 55-year-old woman with a varus knee deformity undergoes radiographic evaluation. Her Medial Proximal Tibial Angle (MPTA) is measured to be 82°. What does this value indicate?
View Answer & Explanation
Correct Answer: D
Rationale: The normal range for the MPTA is 85° to 90°. A value less than 85°, such as 82°, indicates a proximal tibial varus deformity. This is a key contributor to overall genu varum.
Question 58
A 68-year-old male with long-standing genu varum has standing AP radiographs taken. The angle between the distal femoral articular surface and the proximal tibial articular surface is measured to be 5°. What is this angle called, and what does it primarily suggest in this clinical context?
View Answer & Explanation
Correct Answer: C
Rationale: The Joint Line Convergence Angle (JLCA) measures the angle between the femoral and tibial articular surfaces. A normal JLCA is 0° to 2°. An increased angle, especially in the context of varus deformity, suggests stretching of the lateral collateral ligament (LCL) complex and/or cartilage loss, indicating intra-articular deformity or instability.
Question 59
A 40-year-old female presents with lateral foot pain and a feeling of stiffness in her midfoot during walking. On examination, she has a pronounced hindfoot valgus. What is the most likely compensatory deformity of the forefoot?

View Answer & Explanation
Correct Answer: C
Rationale: As described in the text and shown in the left panel of the image, a valgus hindfoot forces a compensatory supination of the forefoot to keep the first metatarsal head on the ground. Pronation is the compensation for a varus hindfoot.
Question 60
A patient with a hindfoot valgus deformity and compensatory forefoot supination is at an increased risk for stress fractures. This is primarily due to which biomechanical consequence?
View Answer & Explanation
Correct Answer: B
Rationale: The text explains that compensatory forefoot supination locks the transverse tarsal (talonavicular and calcaneocuboid) joints. This transforms the midfoot into a rigid plank, leading to a dramatic loss of shock absorption and transmitting harsh forces up the kinetic chain, increasing stress fracture risk.
Question 61
A 52-year-old male presents with a painful callus under his first metatarsal head and a flexible cavovarus foot. On examination, he has a clear hindfoot varus. What is the expected compensatory position of his forefoot?
View Answer & Explanation
Correct Answer: B
Rationale: As shown in the right panel of the image and described in the text, a varus hindfoot is compensated by pronation of the forefoot. This action brings the medial border of the foot down to the ground, but pathologically overloads the first metatarsal head.
Question 62
A patient with a long-standing, compensated hindfoot varus deformity develops a rigid contracture of the medial longitudinal arch. This is primarily due to chronic contracture of the plantar fascia and which other key soft tissue structures?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that chronic compensation for hindfoot varus (via forefoot pronation) leads to rigid soft tissue contractures, specifically of the plantar fascia, flexor hallucis longus, and abductor hallucis. This transforms a flexible deformity into a rigid one.
Question 63
A surgeon is evaluating a patient's plantar pressure map, which shows a balanced distribution of load between the heel, the first metatarsal head, and the fifth metatarsal head. This pattern is best described by which principle?

View Answer & Explanation
Correct Answer: B
Rationale: The text and accompanying image describe the "Tripod Principle" of plantar loading, where weight is normally distributed across three primary points: the calcaneus, the first metatarsal head, and the lateral border/fifth metatarsal head.
Question 64
A 48-year-old male with a rigid varus hindfoot deformity is observed to walk with a significant out-toeing gait. What is the primary biomechanical advantage of this compensatory rotation?
View Answer & Explanation
Correct Answer: C
Rationale: The text explains that a patient with a varus hindfoot subconsciously externally rotates the limb (out-toeing). This shifts the GRV laterally, closer to the ankle joint center, which dramatically reduces the adduction moment that must be counteracted by the peroneal muscles (evertors).
Question 65
A 35-year-old female with a flexible pes planovalgus deformity and posterior tibial tendon dysfunction is noted to walk with an in-toeing gait. This rotational compensation serves to protect which structure?
View Answer & Explanation
Correct Answer: D
Rationale: In a valgus hindfoot, the GRV passes lateral to the ankle, creating a strong abduction (valgus) moment. The text states that the patient internally rotates (in-toeing) to shift the GRV medially, neutralizing this deforming force and reducing the workload on the primary invertor, the tibialis posterior.
Question 66
A surgeon performs a successful calcaneal osteotomy to correct a patient's hindfoot varus. However, post-operatively, the patient has a severe, fixed out-toeing gait. What is the most likely pre-operative oversight?
View Answer & Explanation
Correct Answer: B
Rationale: The text warns that if a surgeon corrects a coronal deformity (varus) without recognizing the patient's compensatory external rotation, the dynamic compensation can become a fixed, post-operative deformity. The surgeon must assess the transverse plane pre-operatively.
Question 67
A 70-year-old male with severe medial compartment knee osteoarthritis has a varus deformity. Biomechanical analysis reveals that the mechanical axis passes far medial to the knee joint. This significantly increases the lever arm for which of the following?
View Answer & Explanation
Correct Answer: A
Rationale: The text explains that in a varus knee, the medially shifted mechanical axis dramatically lengthens the lever arm of the Ground Reaction Vector. This exponentially increases the adductor moment across the knee, accelerating medial compartment destruction.
Question 68
According to the biomechanical principles described, a varus deformity of only six degrees is sufficient to shift the load on the tibial plateau in what way?
View Answer & Explanation
Correct Answer: C
Rationale: The text makes the startling point that just six degrees of varus deformity can shift the mechanical axis so severely that it produces 100% medial load, effectively unloading the lateral compartment and leading to rapid cartilage destruction.
Question 69
A 66-year-old patient with a chronic varus thrust gait pattern is found to have an increased Joint Line Convergence Angle (JLCA). This finding is a direct result of the chronic stretching of which structure?
View Answer & Explanation
Correct Answer: D
Rationale: The text explains that the chronic varus thrust associated with a varus deformity stretches the lateral collateral ligament (LCL) complex. This ligamentous laxity manifests as an increased JLCA, adding dynamic instability to the bony deformity.
Question 70
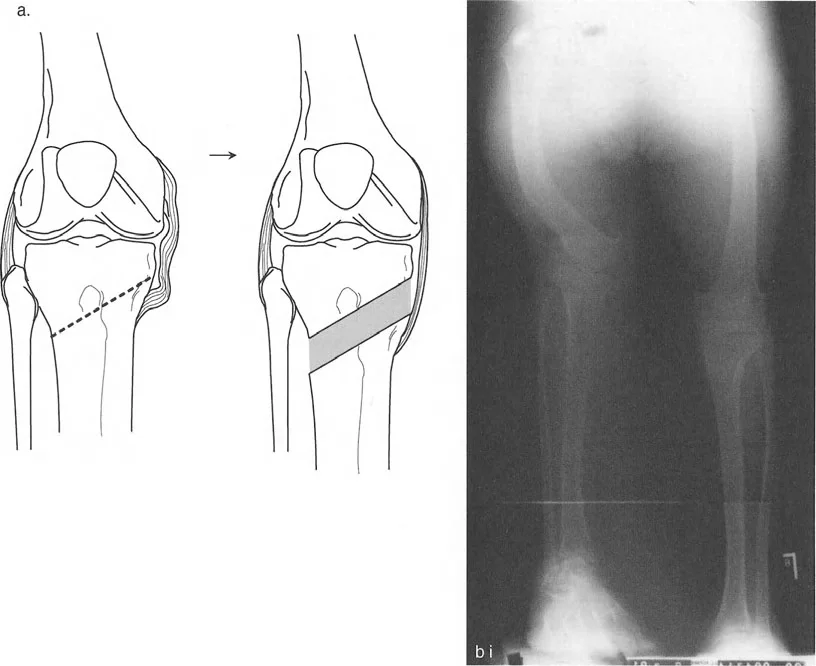
A surgeon is planning a high tibial osteotomy (HTO) for a 58-year-old active male with isolated medial compartment osteoarthritis and a varus deformity. To optimally unload the damaged medial compartment during gait, what is the most appropriate surgical goal for the mechanical axis?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that simply restoring a neutral axis may be insufficient due to the dynamic adductor moment of gait. Therefore, surgeons often aim for a slight overcorrection, shifting the mechanical axis laterally to the 62% coordinate of the tibial plateau (the Fujisawa point), to dynamically unload the medial compartment.
Question 71
A 55-year-old male presents with medial knee pain and a varus deformity. Preoperative planning on a full-length standing radiograph involves drawing a line from the center of the femoral head to the center of the ankle joint. What does this line represent?
View Answer & Explanation
Correct Answer: C
Rationale: The mechanical axis of the lower limb is defined as the straight line from the center of the femoral head to the center of the ankle joint. This line is critical for assessing overall limb alignment and Mechanical Axis Deviation (MAD). The anatomical axis follows the intramedullary canal of the bone.
Question 72
A 28-year-old female has a post-traumatic valgus deformity of her distal femur. During preoperative templating, the surgeon draws the proximal mechanical axis and the distal mechanical axis of the femur. The point where these two lines intersect is best defined as which of the following?
View Answer & Explanation
Correct Answer: B
Rationale: The Center of Rotation of Angulation (CORA) is the geometric point defined by the intersection of the proximal and distal axes of a deformed bone segment. The ACA is the physical hinge of correction, which is ideally placed at the CORA.
Question 73
A surgeon is planning a corrective osteotomy for a tibial deformity. After identifying the CORA, they draw a line that bisects the medial and lateral angles formed by the intersecting axes. According to Paley's principles, what is this line called?
View Answer & Explanation
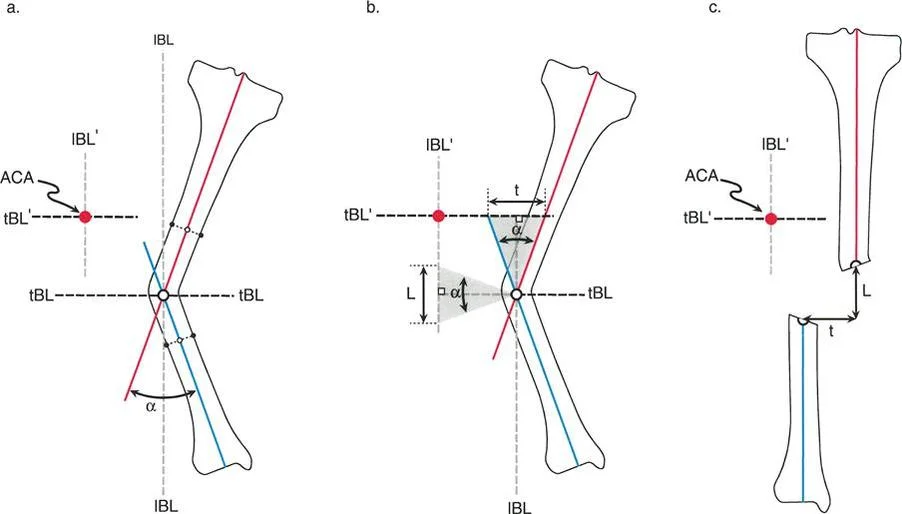
Correct Answer: D
Rationale: The transverse bisector line (tBL) is the line that bisects the medial and lateral angles at the CORA. It represents the plane along which correction can occur without inducing translation of the mechanical axis. The longitudinal bisector line (lBL) bisects the proximal and distal angles.
Question 74
A 45-year-old patient has a varus tibial deformity. During planning, the transverse bisector line (tBL) and longitudinal bisector line (lBL) are drawn at the CORA. What is the geometric relationship between the tBL and the lBL?
View Answer & Explanation
Correct Answer: B
Rationale: By geometric definition, the transverse bisector line (tBL) and the longitudinal bisector line (lBL) are always exactly perpendicular to each other at their intersection point, the CORA.
Question 75
During a medial opening wedge high tibial osteotomy, the surgeon carefully preserves the lateral cortex to act as a hinge. In Paley's terminology, what does this intact lateral cortical hinge physically represent?
View Answer & Explanation
Correct Answer: C
Rationale: The Axis of Correction of Angulation (ACA) is the actual mechanical hinge point around which the bone is physically rotated. In an opening wedge osteotomy with internal fixation, this is the intact opposite cortex. The CORA is the geometric concept; the ACA is the physical reality.
Question 76
A surgeon is planning a corrective osteotomy. According to Paley's principles, collinear realignment of the proximal and distal mechanical axes of a bone will occur if the Axis of Correction of Angulation (ACA) is placed at which location?
View Answer & Explanation
Correct Answer: B
Rationale: A key principle is that collinear realignment of the bone axes occurs whenever the ACA is matched to ANY point on the transverse bisector line (tBL). This allows the surgeon to choose a location on the tBL to achieve different osteotomy types (opening, closing) while still achieving perfect angular correction.
Question 77
A 60-year-old male with a varus knee deformity requires a high tibial osteotomy. The surgeon's goal is to perform a medial opening wedge correction. To achieve this specific type of correction, where must the ACA-CORA be placed?
View Answer & Explanation
Correct Answer: B
Rationale: For an opening wedge osteotomy, the ACA-CORA (the hinge) must be placed on the convex cortex of the deformity. In a varus tibia, the convexity is lateral. Placing the hinge laterally allows the medial (concave) side to be opened. Placing it on the concave cortex would result in a closing wedge.
Question 78
A 35-year-old female has a valgus distal femoral deformity and is also noted to have a 1 cm limb length discrepancy, with the affected limb being longer. To address both issues simultaneously, the surgeon plans a distal femoral osteotomy. Which type of osteotomy is most appropriate?
View Answer & Explanation
Correct Answer: B
Rationale: In a valgus femur, the deformity is concave medially and convex laterally. A medial closing wedge osteotomy will correct the valgus and simultaneously shorten the bone, addressing the limb length discrepancy. An opening wedge would lengthen the already long limb.
Question 79
During the planning of a corrective osteotomy for a diaphyseal deformity, the surgeon places the planned ACA-CORA in the central medullary canal along the transverse bisector line. What is the expected effect on bone length with this technique?
View Answer & Explanation
Correct Answer: C
Rationale: Placing the ACA-CORA in the center of the bone results in a neutral wedge osteotomy. This correction involves a combination of opening on the concave side and closing on the convex side, resulting in a net-zero change in overall bone length.
Question 80
A surgeon performs a corrective osteotomy where the Axis of Correction of Angulation (ACA) is moved proximally along the longitudinal bisector line (lBL), away from the transverse bisector line (tBL). What is the primary biomechanical consequence of this maneuver?
View Answer & Explanation
Correct Answer: C
Rationale: Movement of the ACA along the tBL affects length. In contrast, movement of the ACA along the lBL (proximal or distal to the tBL) results in translation of the bone's axes. The axes can become parallel but will not be collinear.
Question 81
A 25-year-old patient undergoes a corrective osteotomy for a simple, metaphyseal varus deformity of the proximal tibia. The surgeon ensures that the osteotomy cut and the lateral cortical hinge (ACA) are both located precisely at the CORA. According to Paley's rules, what is the expected outcome at the osteotomy site?
View Answer & Explanation
Correct Answer: B
Rationale: This scenario describes Osteotomy Rule 1. When the osteotomy line and the ACA both pass through the same CORA, the bone ends angulate without displacement (translation). This results in a perfect, collinear realignment of the proximal and distal axes.
Question 82
Which of Paley's Three Osteotomy Rules describes the scenario where the osteotomy and the ACA are both located at the CORA, resulting in pure angular correction?
View Answer & Explanation
Correct Answer: A
Rationale: Osteotomy Rule 1 is defined as the "Rule of Pure Angulation." It applies when the osteotomy and the ACA are coincident at the CORA, leading to angular correction without any translation at the osteotomy site.
Question 83
A 40-year-old patient has a valgus deformity with the CORA located just inside the articular surface of the lateral femoral condyle. The surgeon plans to place the ACA at the intra-articular CORA but must make the osteotomy cut in the metaphysis, distal to the CORA. Which of Paley's rules is being applied?
View Answer & Explanation
Correct Answer: B
Rationale: This is the classic scenario for Osteotomy Rule 2. The ACA is placed at the CORA (on the tBL) to ensure proper axis realignment, but the osteotomy is performed at a different level for safety (e.g., to avoid cutting in the joint). This will result in both angulation and translation at the osteotomy site.
Question 84
A surgeon performs a corrective osteotomy for a distal femoral deformity where the CORA is intra-articular. The osteotomy is made in the diaphysis, while the ACA is maintained at the CORA. What is the expected radiographic appearance at the osteotomy site after correction?
View Answer & Explanation
Correct Answer: C
Rationale: This is an application of Osteotomy Rule 2. When the osteotomy and ACA are at different levels, rotation around the ACA causes the bone ends at the cut site to both angulate and translate. This creates a necessary cortical step-off, but the overall proximal and distal axes will become collinear.
Question 85
All of the following are valid clinical reasons to perform an osteotomy at a level different from the CORA (applying Rule 2), EXCEPT:
View Answer & Explanation
Correct Answer: D
Rationale: The primary consequence of applying Rule 2 (cutting away from the CORA) is that it *induces* translation at the osteotomy site. Therefore, a desire to avoid translation would be a reason to use Rule 1, not Rule 2. The other options are all valid reasons to move the osteotomy to a safer location.
Question 86
A post-operative radiograph of a tibial osteotomy shows that the proximal and distal anatomical axes are parallel but not collinear, resulting in a persistent mechanical axis deviation. The angular deformity appears corrected. This outcome is characteristic of which surgical error or advanced technique?
View Answer & Explanation
Correct Answer: C
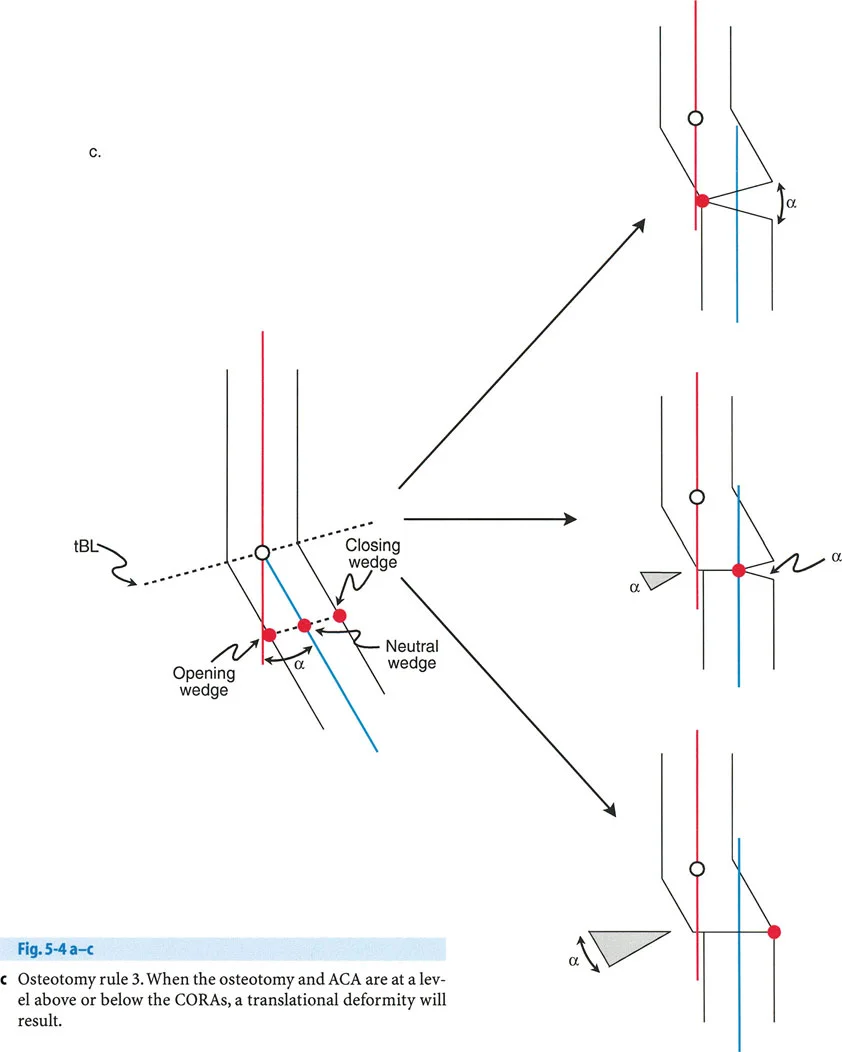
Rationale: Osteotomy Rule 3 occurs when the ACA is not placed on the tBL (i.e., not at a CORA). This results in the correction of angulation but induces a translation of the bone's axes, making them parallel but not collinear. This is often the result of a "Rule 3 Mistake" where the hinge is placed incorrectly.
Question 87
A 30-year-old patient has a malunited diaphyseal femur fracture with both 15 degrees of varus angulation and 10 mm of medial translation. A surgeon plans a single osteotomy to correct both deformities simultaneously. To achieve this, where should the ACA be placed relative to the CORA?
View Answer & Explanation
Correct Answer: C
Rationale: This is an intentional application of Osteotomy Rule 3. To correct a pre-existing translational deformity simultaneously with an angular deformity, the surgeon must intentionally place the ACA off the tBL. This maneuver uses the principles of Rule 3 to induce a corrective translation that counteracts the existing one.
Question 88
The most critical first step in preoperative templating for a lower limb deformity correction is to obtain which of the following imaging studies?
View Answer & Explanation
Correct Answer: C
Rationale: Assessment of the mechanical axis and its deviation is impossible without a full-length standing radiograph. This is the foundational image required to identify the CORA and plan the entire correction based on Paley's principles.
Question 89
A surgeon is performing a medial opening wedge high tibial osteotomy using a locking plate. To prevent catastrophic failure and loss of correction, what is the most critical structure to protect during the osteotomy cut?
View Answer & Explanation
Correct Answer: D
Rationale: In an opening wedge HTO, the intact lateral cortex serves as the physical hinge (ACA). If this hinge is broken, stability is lost, and an unplanned translation (a Rule 3 mistake) can occur, leading to malalignment. The integrity of the hinge is paramount.
Question 90
A 22-year-old patient with a 3 cm limb length discrepancy and a 15-degree valgus deformity of the tibia requires correction. The affected limb is short. Which surgical strategy would be most appropriate to address both problems?
View Answer & Explanation
Correct Answer: C
Rationale: A 3 cm LLD is too large for acute correction with an opening wedge osteotomy, which typically adds only millimeters of length. The optimal solution is to use an external fixator to perform gradual distraction osteogenesis, which can simultaneously correct the angular deformity and lengthen the bone to address the significant LLD.
Question 91
When planning a corrective osteotomy, the point on the transverse bisector line (tBL) that the surgeon chooses to place the physical hinge (ACA) through is specifically termed the:
View Answer & Explanation
Correct Answer: C
Rationale: Since any point on the tBL can serve as a CORA for collinear realignment, the specific point chosen by the surgeon to place the ACA is termed the ACA-CORA. This choice dictates whether the osteotomy will be opening, closing, or neutral.
Question 92
A 58-year-old female with a painful valgus knee undergoes a lateral closing wedge distal femoral osteotomy. What is the primary biomechanical advantage of this type of osteotomy?
View Answer & Explanation
Correct Answer: C
Rationale: A closing wedge osteotomy involves removing a wedge of bone and bringing two broad cancellous surfaces together under compression. This provides a stable environment with excellent bone-to-bone contact, which promotes rapid and reliable healing. Its main disadvantage is bone shortening.
Question 93
A surgeon is using a Taylor Spatial Frame (TSF) to correct a complex, multi-apical tibial deformity. The surgeon must apply Osteotomy Rule 2 because the ideal osteotomy level has poor soft tissue coverage. Which feature of the TSF is particularly advantageous for this situation?
View Answer & Explanation
Correct Answer: D
Rationale: Rule 2 corrections involve both angulation and translation. Hexapod circular fixators like the TSF are ideal because their computer software can precisely calculate the strut adjustments needed to achieve the planned, complex 3D correction, including the necessary translation at the osteotomy site.
Question 94
An 11-year-old skeletally immature girl presents with bilateral genu valgum, causing knee pain and an awkward gait. A clinical photograph is shown. Her parents are concerned about the appearance and potential long-term effects.

View Answer & Explanation
Correct Answer: C
Rationale: Guided growth in a skeletally immature patient utilizes the tension band principle to achieve gradual correction. A plate and screws on the concave side of the deformity (medial side for valgus) tether growth, allowing the convex side to grow and straighten the limb. This is a reversible process. An osteotomy (D) is more invasive and typically reserved for severe deformities or patients near skeletal maturity.
Question 95
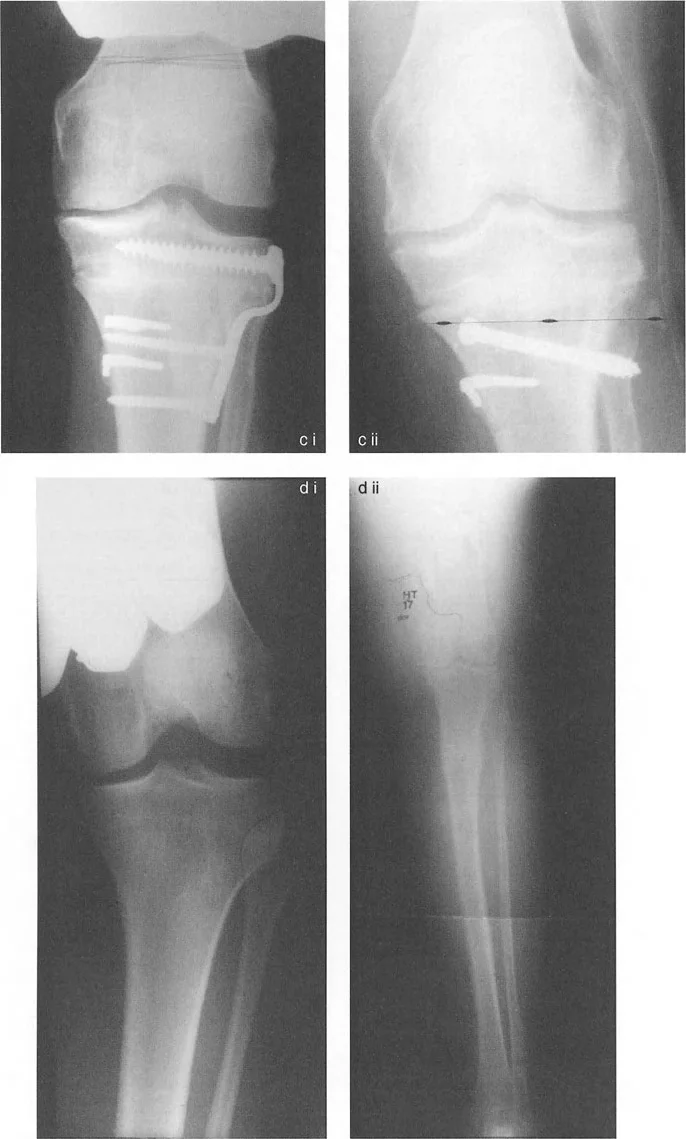
A 12-year-old boy is treated for symptomatic genu varum. Postoperative radiographs are obtained following bilateral distal femoral lateral tension band plating.

View Answer & Explanation
Correct Answer: B
Rationale: The tension band plate, when placed on the convex side of a deformity (lateral side for varus), creates a tether that restricts physeal growth on that side. The continued, unrestricted growth on the concave (medial) side leads to gradual correction of the varus deformity. The plate does not accelerate growth (A, D).
Question 96
A 10-year-old boy with skeletal dysplasia presents with significant genu valgum. His mechanical axis passes 30 mm lateral to the center of the knee joint. Surgical intervention with medial tension band plates is performed on the distal femurs and proximal tibias.

View Answer & Explanation
Correct Answer: C
Rationale: The placement of tension band plates on both the medial distal femur and medial proximal tibia indicates that the genu valgum deformity has components originating from both bones. This is common in certain skeletal dysplasias. Placing plates medially treats valgus, not varus (D).
Question 97
A 9-year-old boy presents with progressive bilateral bowlegs. Clinical examination reveals a varus thrust during gait. A photograph demonstrates the clinical deformity.

View Answer & Explanation
Correct Answer: B
Rationale: The clinical picture shows genu varum (bowlegs). In a 9-year-old with significant growth remaining, the treatment of choice for a femoral-based deformity is guided growth. To correct varus, a tension band must be placed on the lateral side (the convexity) of the distal femur. Medial placement (A) would worsen the varus.
Question 98
A 13-year-old girl with idiopathic genu valgum undergoes bilateral medial distal femoral tension band plating. A postoperative radiograph is shown.

View Answer & Explanation
Correct Answer: C
Rationale: The correct technique for placing an 8-plate or similar tension band device requires one screw to be placed in the epiphysis and the other in the metaphysis, on either side of the physis. This allows the plate to act as a flexible tether across the growth plate. The screws must not cross the physis (A).
Question 99
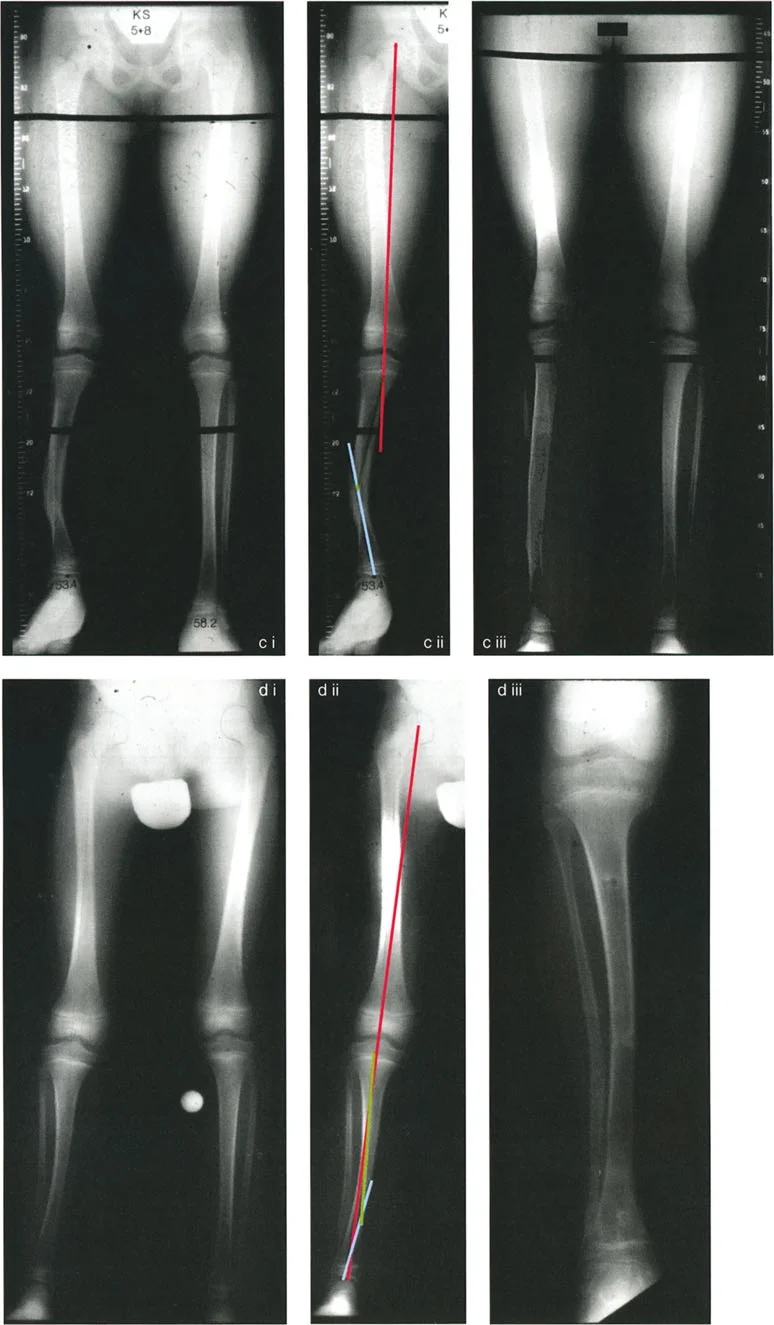
A 7-year-old boy with Blount's disease presents with progressive genu varum. After failing brace treatment, he undergoes surgical correction. The postoperative radiograph is shown.

View Answer & Explanation
Correct Answer: B
Rationale: The radiograph shows tension band plates on the lateral aspect of both the proximal tibia and distal femur. This configuration is used to correct genu varum that has components in both the tibia and femur. Blount's disease often involves a primary tibial varus, but a compensatory femoral varus can also be present, necessitating correction at both levels.
Question 100
A 16-year-old boy with a 3 cm leg length discrepancy (LLD) is evaluated for treatment. His physes are noted to be nearly closed on radiographs. He is interested in the least invasive option to address the LLD.
View Answer & Explanation
Correct Answer: B
Rationale: With nearly closed physes, there is insufficient growth remaining for epiphysiodesis (A) or guided growth (E) to be effective. For a 3 cm LLD, limb lengthening (C) or acute shortening (D) are major surgical options. A shoe lift is the least invasive and most appropriate initial management for a discrepancy of this magnitude in a patient at skeletal maturity.
You Might Also Like
