Upper Extremity Burn & Contracture Reconstruction: An Intraoperative Masterclass
Key Takeaway
This masterclass guides you through acute and reconstructive surgical techniques for upper extremity thermal and electrical injuries. We'll meticulously cover comprehensive anatomy, preoperative planning, real-time intraoperative execution of escharotomy, fasciotomy, and complex tissue rearrangements like the "jumping man" Z-plasty. Emphasis is placed on neurovascular preservation, managing compartment syndrome, and optimizing functional outcomes for these challenging cases.
Alright fellows, gather 'round. Welcome to the operating theater. Today, we're tackling a complex and critical area of orthopaedic surgery: the acute management and secondary reconstruction of thermal and electrical injuries to the distal upper extremity. These are not merely skin problems; they represent a profound challenge to form and function, often leading to debilitating contractures that demand meticulous surgical intervention and long-term rehabilitation. Our goal today is to restore not just appearance, but vital hand and forearm function, preventing the tragic sequelae of untreated burn injury.
Understanding the Injury: Pathogenesis and Clinical Presentation
Before we even consider an incision, we must deeply understand the pathology. Burns and electrical injuries to the hand and forearm present a spectrum of surgical problems, from acute, life-threatening conditions to chronic, disabling contractures.
Electrical Burns: The Hidden Damage
High-voltage electrical injury, defined as involving a power source greater than 600 volts, is particularly insidious. Unlike thermal burns, the visible cutaneous injury often belies extensive "hidden" deep tissue damage. This occurs primarily through two mechanisms:
- Thermal Injury: As electrical current traverses tissues, resistance generates heat, causing direct thermal damage along its path. Tissues with high electrical resistance, such as skin and bone, generate more heat, leading to more profound destruction of themselves and surrounding structures.
- Electroporation: This is cellular damage induced by the electric field itself. The severity of electroporation is determined by the cell's size and its transmembrane potential. Myocytes, with their larger surface area, are particularly prone to this injury. Furthermore, myocytes near bone may experience increased transmembrane potential due to architectural and orientation factors, leading to greater damage in these areas.
This combination of thermal injury and electroporation often results in extensive deep tissue and muscle necrosis, predisposing the patient to acute compartment syndrome.
Thermal Burns and Contractures
Thermal burns, particularly circumferential or near-circumferential full-thickness burns, can also lead to acute compartment syndrome. The inelastic burned tissue, or eschar, acts as a tourniquet, compromising venous return and capillary perfusion, leading to distal tissue ischemia.
Long-term, both thermal and electrical burns frequently result in severe contractures. Normal skin pliability is lost as scar tissue replaces healthy dermis after second- and third-degree burns. This leads to increased and disorganized deposition of collagen fibers, forming compact, shortened scars. Inflammation, pain, and edema in the acute phase promote immobility, often in the "position of comfort," which unfortunately is the "position of deformity." This rapid formation of contractures typically produces the classic "clawing deformity" with a flexed wrist and proximal interphalangeal (PIP) joints, extended distal interphalangeal (DIP) and metacarpophalangeal (MCP) joints, and adducted web spaces.
Classic deformities associated with severe hand burn, with flexed PIP and extended MCP/DIP joints.
Despite aggressive acute care, splinting, and therapy, long-term hand and wrist deformities are common.
Comprehensive Surgical Anatomy: Forearm and Hand Compartments
Understanding the intricate anatomy of the forearm and hand is paramount, especially when dealing with compartment syndrome and contractures. These are tightly constrained spaces, and any increase in volume can rapidly compromise neurovascular structures.
Forearm Compartments
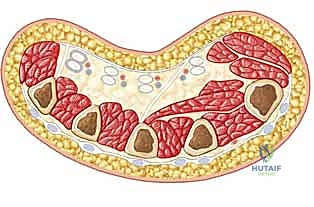
The forearm is meticulously divided into three primary fascial compartments, each with its own neurovascular supply and muscle groups.
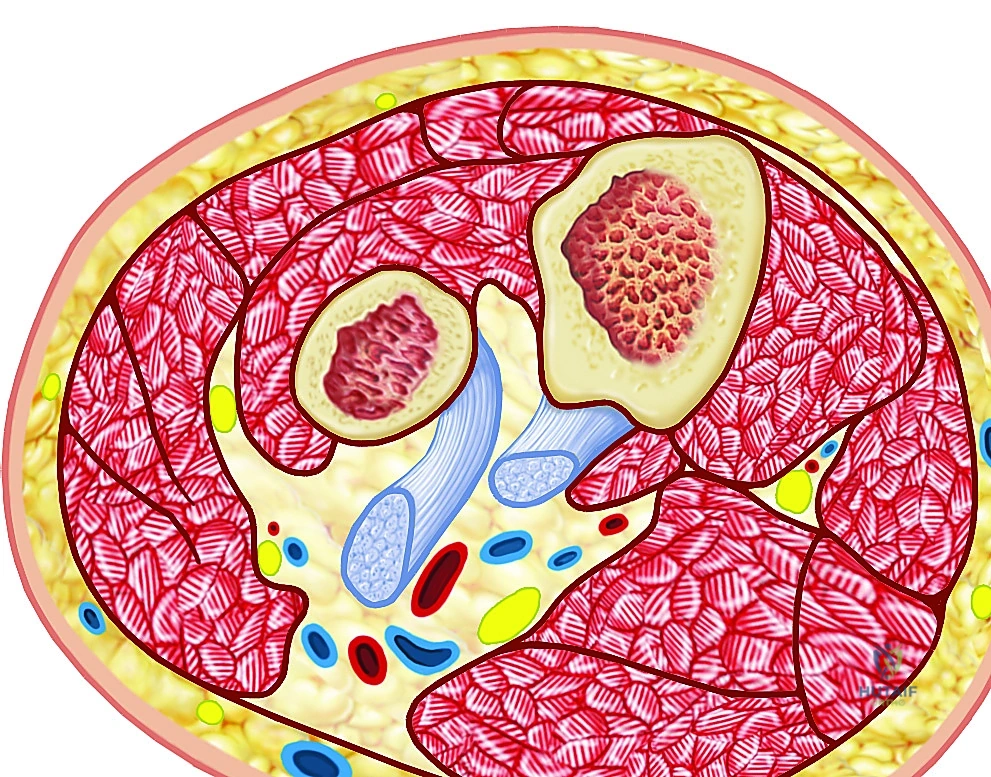

Cross-sections illustrating the forearm compartments.
-
Volar Compartment: This is the largest and most complex compartment.
- Muscles: Contains the superficial flexors (pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, flexor carpi ulnaris) and deep flexors (flexor digitorum profundus, flexor pollicis longus, pronator quadratus).
- Neurovascular Structures: The median nerve (runs between FDS and FDP proximally, then superficial to FDP distally) and the ulnar nerve (runs with the ulnar artery, medial to FCU) are critical structures here. The radial artery and ulnar artery also traverse this compartment. Damage to these nerves results in severe functional deficits, including loss of sensation and motor control to critical hand muscles.
- Risk: This compartment is most commonly affected by compartment syndrome due to the large muscle mass and dense fascial envelope.
-
Dorsal Compartment:
- Muscles: Houses the extensor muscles of the wrist and digits (extensor digitorum, extensor digiti minimi, extensor carpi ulnaris, extensor pollicis longus, extensor pollicis brevis, abductor pollicis longus, extensor indicis).
- Neurovascular Structures: The posterior interosseous nerve (deep branch of the radial nerve) and the posterior interosseous artery are found here.
- Risk: While less common than volar compartment syndrome, it can occur and compromise extensor function.
-
Mobile Wad (Lateral Compartment):
- Muscles: Comprises the brachioradialis, extensor carpi radialis longus, and extensor carpi radialis brevis.
- Neurovascular Structures: The radial nerve (superficial branch) runs deep to the brachioradialis.
- Risk: Typically less involved in compartment syndrome but still requires release if pressures are elevated.
Hand Compartments
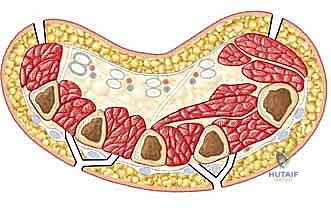
The hand itself is divided into several intrinsic fascial compartments.


Cross-sections of the hand showing intrinsic fascial compartments.
- Dorsal Interosseous Compartments (4): Located between the metacarpals, housing the dorsal interossei muscles, which abduct the fingers. Innervated by the deep ulnar nerve.
- Volar Interosseous Compartments (3): Also between metacarpals, housing the volar interossei muscles, which adduct the fingers. Innervated by the deep ulnar nerve.
- Thenar Compartment: Houses the thenar muscles (abductor pollicis brevis, flexor pollicis brevis, opponens pollicis) responsible for thumb movement. Innervated primarily by the recurrent motor branch of the median nerve.
- Hypothenar Compartment: Houses the hypothenar muscles (abductor digiti minimi, flexor digiti minimi, opponens digiti minimi) for small finger movement. Innervated by the deep ulnar nerve.
- Adductor Compartment: Houses the adductor pollicis muscle. Innervated by the deep ulnar nerve.
Osteology: The radius, ulna, carpal bones, metacarpals, and phalanges form the bony framework. Burn contractures can affect the joint capsules and ligaments surrounding these bones, leading to fixed deformities. Heterotopic ossification, an abnormal bone formation in soft tissues, can further complicate joint mobility.
Compartment Syndrome: The Race Against Time
Compartment syndrome is a serious, limb-threatening sequela that warrants immediate surgical attention. In burns, vascular permeability leads to massive edema of the soft tissues, particularly the muscles. The inelastic fascia housing each compartment does not allow the edematous muscles to expand, leading to a rapid elevation of intracompartmental pressure. This increased pressure eventually interrupts arterial inflow to the muscles, following the arteriovenous gradient theory.
- Myonecrosis: Classic studies have shown that myonecrosis occurs after 6 hours of ischemia. Beyond 8 to 12 hours, irreversible functional damage is almost guaranteed.
- Volkmann's Ischemic Contracture: If left untreated, the result is the devastating Volkmann’s ischemic contracture, where muscles and nerves die and are replaced by dense, fibrous, non-functional tissue.
Crucially, compartment syndrome can occur not only within fascial compartments but also beneath full- or near-full-thickness burns where the inelastic skin itself limits underlying soft tissue expansion.
Preoperative Planning: Setting the Stage for Success
Fellows, meticulous preoperative planning is the bedrock of successful outcomes in these complex cases. We leave nothing to chance.
Patient Assessment and Resuscitation
For acute burn injuries, especially high-voltage or large body surface area burns:
- ABCs First: Always prioritize airway, breathing, and circulation. These patients often require trauma and critical care consultation to evaluate for other life-threatening injuries.
- Fluid Resuscitation: Aggressive fluid resuscitation is paramount. Be prepared for massive edema within 36 hours of injury.
- Mechanism of Injury: A detailed history of the burn mechanism is crucial – high-voltage, enclosed space, explosion – as this dictates the potential for deeper, hidden damage.
- Blood Products: Burn débridements can incur significant blood loss. Ensure blood products (packed red blood cells, fresh frozen plasma) are readily available intra- and perioperatively.
Physical Examination: The Cornerstone of Diagnosis
Your clinical judgment is paramount.
-
Acute Compartment Syndrome:
- Clinical Presentation: Severe edema and tightness of the hand, wrist, and forearm distal to the burn.
- Pain: Progressive pain despite immobilization, especially pain with passive muscle stretch. This is the most sensitive early sign of muscle ischemia.
- Nerve Ischemia: Diminished sensation (light touch, two-point discrimination) and muscle weakness are late, ominous signs. Remember, absent or diminished pulse is a very late finding in compartment syndrome; do not wait for it.
- Palpation: Compartments will feel tender and firm, or "wood-like," to palpation.
- Capillary Refill: Delayed capillary refill may suggest increased soft tissue or compartment pressure. Quickened capillary refill can suggest venous congestion, also a sign of impending compromise.
-
Secondary Burn Reconstruction:
- Range of Motion (ROM): A complete hand examination, focusing on active and passive ROM of affected joints, is essential.
- MCP ROM:
- Type I: Mild limitation in MCP flexion with wrist flexion, >30 degrees of flexion with wrist in extension.
- Type II: Severe limitation in MCP flexion with wrist in flexion, <30 degrees of flexion with wrist in extension.
- Type III: Severe limitation in MCP flexion with wrist in extension.
- Pearls: Types II and III suggest underlying joint and ligamentous pathology requiring more than just soft tissue release.
- PIP ROM:
- Type I: Near-normal PIP extension with MCP in flexion.
- Type II: Moderately limited PIP extension with MCP in flexion.
- Type III: Fixed PIP flexion regardless of MCP position.
- Pearls: Types II and III again indicate underlying joint and ligamentous involvement.
- MCP ROM:
- Scar Quality: Examine the scar for hyperemia and pliability. Immature scars (usually within 6 months) may still respond to nonoperative management.
- Skin Coverage: Assess for poor or unstable skin coverage, which might necessitate distant flap coverage.
- Deformity Analysis: Appreciate the specific structures involved in the deformity – skin, subcutaneous tissue, fascia, joint capsule, ligaments, tendons.
- Range of Motion (ROM): A complete hand examination, focusing on active and passive ROM of affected joints, is essential.
Imaging and Diagnostic Studies
- Compartment Pressure Measurement: This is critical for objective confirmation.
- Technique: A simple setup can be made with an 18- or 20-gauge needle attached to a syringe containing saline and a pressure transducer, connected via a three-way stopcock. Alternatively, commercially available devices are excellent.
- Procedure: Zero the transducer at the level of the soft tissue. Insert the needle into the subcutaneous tissue or muscle compartment. Inject a small amount (0.2–0.5 mL) of saline to establish a water column. Open the transducer to the needle for monitoring.
- Thresholds:
- Normotensive Patients: Pressure >30 mm Hg.
- Hypotensive Patients: Compartment pressure within 20 mm Hg of the diastolic pressure.
- Caveat: While helpful, remember that clinical judgment remains paramount. If there's any doubt, intervene.
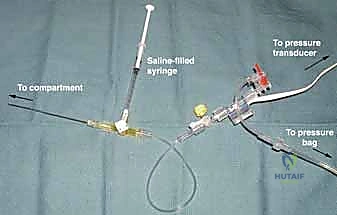
Pressure transducer adapted for measurement of compartment pressure.
* Plain Radiographs: For secondary reconstruction, obtain radiographs to evaluate joint condition and check for heterotopic ossification, which requires different management.
* No Imaging for Acute Pressure: Currently, no imaging modality can reliably detect acute increases in compartment pressure.
Differential Diagnosis
Always consider other causes of limb pain and dysfunction:
- Nerve injury (direct trauma, compression)
- Arterial insufficiency or injury
- Venous thrombosis
- Intrinsic joint disease (e.g., arthritis)
- Other scarring or contracture phenomena (e.g., Dupuytren's disease)
Nonoperative Management
For immature scars (hyperemic, within 6 months of injury), conservative measures can be effective:
- Pressure Garments: Must be worn for several months to control hypertrophic scarring.
- Silicone Dressing: Also aids in scar maturation and reduction.
- Physical Therapy: Aggressive range-of-motion exercises.
- Splinting: In an antideforming posture (e.g., volar intrinsic-plus splint with the thumb in palmar abduction) to prevent debilitating contractures.


Immature burn scars amenable to conservative treatment. A volar intrinsic-plus splint with the thumb in palmar abduction to prevent debilitating postburn contractures.
Preoperative Setup and Positioning
Alright team, let's get the patient ready.
- Positioning: The patient will be supine with the affected arm extended on a specialized hand table or arm board. This allows full access to the hand, wrist, and forearm. Ensure the arm is securely padded and positioned to prevent iatrogenic nerve compression.
- Tourniquet: A pneumatic tourniquet will be applied to the proximal arm. We will inflate this to appropriate pressures (e.g., 250 mmHg for normotensive patients) to provide a bloodless field, crucial for precise dissection and identification of vital structures. Be mindful of tourniquet time; we'll track it diligently.
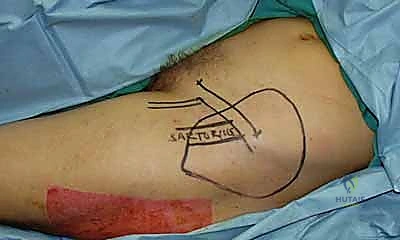
- Draping: Standard sterile draping, ensuring the entire upper extremity, from shoulder to fingertips, is exposed for comprehensive access, especially if we anticipate needing a pedicled flap.
- Fluoroscopy: While not always necessary for every step, have the C-arm draped and ready, particularly if we anticipate joint releases requiring K-wire stabilization or if heterotopic ossification is suspected.
- Instrumentation: Ensure all standard hand sets are available, along with fine microsurgical instruments for flap elevation and specialized instruments for joint releases (e.g., small osteotomes, rongeurs, K-wires).
Intraoperative Execution: The Masterclass
Now, let's get down to business. Remember, every cut, every dissection, every decision is made with precision and purpose.
Indications for Surgical Management
- Acute Burns & Compartment Syndrome:
- High-Voltage Injury: This is an immediate indication for fasciotomy and burn débridement, as the extent of deep thermal damage is often difficult to assess clinically. We operate early and aggressively.
- Thermal/Low-Voltage Injury: Patients require closed monitoring. If increased soft tissue or compartment pressure is suspected or confirmed (pressure >30 mmHg or within 20 mmHg of diastolic), immediate escharotomy or fasciotomy is indicated. Otherwise, débridement may be delayed 48-72 hours to allow for demarcation of burned areas.
- Inadequate Escharotomy Release: If elevated compartment pressure is not relieved by escharotomy, a full fasciotomy is necessary.
- Secondary Burn Reconstruction:
- Significant functional impairment due to contracture, especially MCP/PIP Type II or III contractures, indicating joint and ligamentous pathology.
- Unstable or poor skin coverage requiring flap reconstruction.
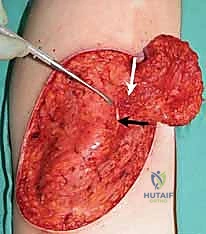
Step 1: Escharotomy (When Indicated)
For acute circumferential burns causing a tourniquet effect, an escharotomy is the first line of defense.
- Technique: "Scalpel, #15 blade please." We'll make full-thickness incisions through the
Additional Intraoperative Imaging & Surgical Steps











REFERENCES
-
The flap is divided, thinned, and inset 3 to 4 weeks after the index procedure.
-
Beasley RW. Secondary repair of burned hands. Clin Plast Surg 1981; 8:141–162.
-
Dente CJ, Feliciano DV, Rozycki GS, et al. A review of upper extremity fasciotomies in a level I trauma center. Am Surg 2004;70:1088– 1093.
-
Esselman PC, Thombs BD, Magyar-Russell G, et al. Burn rehabilitation: State of the science. Am J Phys Med Rehabil 2006;85:383– 413.
-
Graham TJ, Stern PJ, True MS. Classification and treatment of postburn metacarpophalangeal joint extension contractures in children. J Hand Surg Am 1990;15:450–456.
-
Hargens AR, Romine JS, Sipe JC, et al. Peripheral nerve-conduction block by high muscle-compartment pressure. J Bone Joint Surg Am 1979;61A:192–200.
-
Larson DL, Abston S, Willis B, et al. Contracture and scar formation in the burn patient. Clin Plast Surg 1974;1:653–666.
-
Lee RC, Zhang D, Hannig J. Biophysical injury mechanism in electrical shock trauma. Annu Rev Biomed Eng 2000;2:477–509.
-
Matsen FA III. Compartmental syndrome: an unified concept. Clin Orthop Relat Res 1975;113:8–14.
-
Mubarak SJ, Owen CA, Hargens AR, et al. Acute compartment syndromes: Diagnosis and treatment with the aid of the wick catheter. J Bone Joint Surg Am 1978;60:1091–1095.
-
Sheridan GW, Matsen FA 3rd. Fasciotomy in the treatment of the acute compartment syndrome. J Bone Joint Surg Am 1976;58:112– 115.
-
Stern PJ, Neale HW, et al. Classification and treatment of postburn proximal interphalangeal joint flexion contractures in children. J Hand Surg Am 1987;12:450–457. 12. von Volkmann R. Ischaemic muscle paralyses and contractures. Clin Orthop Relat Res 1967;50:5–6.
OUTCOMES
- When adequately done, the outcome after fasciotomy, in any location, is closely related to its timing. In fasciotomy performed within 12 hours of onset of compartment syndrome, normal function has been reported in 68% of patients. The number decreases sharply, to 8%, if fasciotomy is delayed beyond 12 hours. 10
-
Approximately 30% of fasciotomy wounds can be closed primarily. The rest require skin grafting. 2
-
Several articles describing various local tissue rearrangement procedures for contracture release document low complication rates and good results.
-
Our experience agrees with published series that pedicled groin flaps provide stable soft tissue coverage of upper extremity defects with low complication rates.
COMPLICATIONS
- Complications for escharotomy and fasciotomy include:
-
Bleeding
-
Inadequate release
-
Complications for local tissue rearrangement for contracture release include:
-
Partial skin necrosis
-
Dehiscence
-
Recurrence
-
Injury to neurovascular bundle
-
Flap necrosis
-
Avulsion
-
Excessive bulk requiring revisions
You Might Also Like