Master ABOS Board Review: Deformity Correction, Arthroplasty & Pediatric Orthopedics | Part 12
Key Takeaway
ABOS Orthopedic Board Review Part 12 covers advanced principles of limb deformity correction, including guided growth, osteotomies, and external fixation. It details biomechanics of THR and TKR, LLD prediction (Shapiro, Moseley), and pediatric conditions like SCFE and Perthes disease, emphasizing Paley's rules and surgical planning for complex cases.
Question 1
An 8-year-old boy with Blount's disease undergoes proximal tibial hemi-epiphysiodesis. The deformity corrects fully over 12 months, and the hardware is removed. One year later, radiographs show a recurrence of the varus deformity. What is this phenomenon called?
View Answer & Explanation
Correct Answer: A
Rationale: The text specifically mentions that surgeons must monitor for "rebound reangulation" (drifting back to the deformed position) which may occur after staple removal, particularly in younger children or those with underlying conditions like Blount's disease. This may require restapling.
Question 2
A 13-year-old girl is scheduled for guided growth. The foundation for all preoperative planning is a specific type of radiograph. Which of the following imaging studies is considered non-negotiable for this purpose?
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "The foundation of all planning is a full-length, bipedal, weight-bearing anteroposterior radiograph. The patellae must be pointing straight forward to eliminate rotational artifact." This specific view is essential for accurately calculating the MAD and joint orientation angles.
Question 3
A 17-year-old presents with a varus deformity secondary to a healed diaphyseal tibia fracture malunion from 3 years ago. The physes are now closed. Preoperative planning shows the CORA is located in the mid-diaphysis. Why is guided growth not an appropriate treatment option?
View Answer & Explanation
Correct Answer: A
Rationale: The text lists two absolute contraindications present in this case: skeletal maturity (closed physes) and a CORA located far from the physis. Guided growth works by modulating physeal growth, so it is ineffective if the physis is closed or if the deformity's apex is not at the physis.
Question 4
A 14-year-old boy with a 20° genu varum deformity has approximately 18 months of growth remaining. The surgeon opts for a staged intervention. What is the primary benefit of performing a hemi-epiphysiodesis at this stage, knowing a future osteotomy might still be needed?
View Answer & Explanation
Correct Answer: A
Rationale: The text describes a "hybrid strategy" for patients nearing skeletal maturity. Performing a hemi-epiphysiodesis allows the surgeon to gain a partial, "free" correction using the remaining growth. This "significantly reduces the magnitude and surgical morbidity of the final osteotomy." With only 18 months of growth, full correction of a 20° deformity is unlikely (B).
Question 5
When placing a tension-band plate for guided growth, what is the recommended surgical technique regarding the periosteum to preserve local vascularity to the physis?
View Answer & Explanation
Correct Answer: A
Rationale: One of the "High-Yield Surgical Pearls" is to "Respect the Periosteum." The text specifically advises an extra-periosteal placement to preserve the local vascular supply to the physis, avoiding aggressive stripping.
Question 6
A 10-year-old girl undergoes medial proximal tibial hemi-epiphysiodesis for genu valgum. The surgeon is counseling the parents on the follow-up schedule. What is the recommended interval for radiographic monitoring to prevent overcorrection?
View Answer & Explanation
Correct Answer: A
Rationale: The text stresses that guided growth is not a "set it and forget it" procedure and that "Patients must be monitored radiographically every 3 to 4 months." This frequent monitoring is crucial because correction can happen rapidly, especially during growth spurts, and carries a risk of overcorrection.
Question 7
A 9-year-old boy with renal osteodystrophy has developed severe genu valgum. In addition to planning for guided growth surgery, what is the most important concurrent management step?
View Answer & Explanation
Correct Answer: A
Rationale: A key surgical pearl is to "Treat the Underlying Cause." The text advises investigating the underlying etiology (e.g., rickets, renal osteodystrophy) and ensuring metabolic optimization concurrently with surgical treatment. Correcting the deformity without addressing the underlying metabolic bone disease will likely lead to failure or recurrence.
Question 8
A 68-year-old male with a history of a healed mid-shaft femur fracture presents with debilitating knee pain. Radiographs show severe tricompartmental osteoarthritis and a 15° varus deformity with an apex in the femoral diaphysis. When planning a total knee replacement (TKR), what is the most critical initial step in the biomechanical assessment?
View Answer & Explanation
Correct Answer: C
Rationale: The provided text emphasizes that for extra-articular deformities, the foundation of successful planning is understanding the overall limb alignment. Drawing the mechanical axis on a full-length film is mandatory to quantify the MAD and, most importantly, to locate the CORA, which dictates whether an osteotomy is needed. A CT scan (B) is more critical for rotational deformities, particularly in the hip, not the primary tool for coronal plane analysis in this TKR case.
Question 9
A 45-year-old female with developmental dysplasia of the hip (DDH) presents for a total hip replacement (THR). Preoperative planning reveals 55° of femoral anteversion. On physical exam, she has a profound Trendelenburg gait despite having 5/5 abductor strength on manual muscle testing. What is the primary biomechanical reason for her abductor insufficiency?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that excessive femoral anteversion displaces the greater trochanter posteriorly. This dramatically shortens the abductor lever arm, making the abductor muscles mechanically disadvantaged and leading to a Trendelenburg gait even with normal muscle power. Bony impingement (D) may occur, but the primary cause of the gait is the poor mechanical advantage.
Question 10
A surgeon is planning a total knee replacement. To restore neutral mechanical alignment, the distal femoral cut must establish a normal joint orientation angle. What is the target value for the mechanical Lateral Distal Femoral Angle (mLDFA)?
View Answer & Explanation
Correct Answer: B
Rationale: The text specifies that a primary goal of TKR is to re-establish normal joint orientation angles. The normal mLDFA is 87°. An mLDFA of 90° (C) would correspond to the anatomic axis, not the mechanical axis, and would result in a varus alignment.
Question 11
A 52-year-old female with symptomatic hip dysplasia requires a THR. A preoperative CT scan demonstrates 50° of femoral anteversion. According to the principles outlined by Holtgrewe, Hungerford, and Paley, what is the most appropriate surgical plan?
View Answer & Explanation
Correct Answer: C
Rationale: The text strongly advocates for a corrective proximal femoral osteotomy when proximal femoral anteversion exceeds 45°. This approach corrects the deformity at its source, restores abductor mechanics, and is more cost-effective than custom implants. A modular stem (B) is effective for mild to moderate deformities but is insufficient for a severe 50° deformity.
Question 12
A 58-year-old male undergoes a THR with a concurrent subtrochanteric derotational osteotomy for a post-traumatic deformity. Compared to using a highly specialized custom or modular implant to accommodate the deformity, what is a major advantage of performing the osteotomy?
View Answer & Explanation
Correct Answer: C
Rationale: A key advantage of the corrective osteotomy is the restoration of normal biomechanics. By derotating the femur, the posteriorly displaced greater trochanter is brought into a more lateral position, which instantly restores the abductor lever arm and corrects the mechanical Trendelenburg gait. The disadvantages include prolonged healing and increased thigh pain (D), not immediate weight-bearing (A).
Question 13
A 65-year-old female with a severe valgus knee deformity secondary to a malunited proximal tibia fracture is scheduled for a TKR. The CORA is located in the tibial diaphysis, and the deformity is 18° of valgus. The surgeon decides against compensating with intra-articular cuts. What is the most compelling reason for this decision?
View Answer & Explanation
Correct Answer: D
Rationale: The text warns that compensating for a severe deformity located close to the joint is dangerous. To correct an 18° valgus deformity originating in the tibia by altering the femoral and tibial cuts, an extreme amount of bone would need to be resected from the lateral side. This would inevitably compromise the insertion of the LCL on the tibia or the origin on the femur, leading to gross instability. For a varus deformity, the MCL (C) would be at risk.
Question 14
A 55-year-old patient with a chronically dislocated dysplastic hip has a true leg length discrepancy of 4 cm. During a single-stage THR, what is the primary concern that limits acute intraoperative lengthening?
View Answer & Explanation
Correct Answer: B
Rationale: The text establishes a critical "2 cm rule." It states that acute lengthening greater than 2 cm dramatically increases the risk of sciatic nerve palsy. For discrepancies greater than 2 cm, a staged procedure or a femoral shortening osteotomy should be considered to protect the nerve.
Question 15
During a THR, the surgeon encounters a persistent 30° hip flexion contracture after a complete anterior capsulectomy. The hip cannot be brought into full extension on the table. What is the most appropriate next step?
View Answer & Explanation
Correct Answer: B
Rationale: The text outlines a sequential approach to releasing a flexion contracture. After the anterior capsule is excised, the next structure causing a persistent contracture is the iliopsoas tendon. If it is under high tension, it must be released or lengthened. Releasing the IT band (D) addresses an abduction contracture, not flexion.
Question 16
A 72-year-old male with a painful 25° varus knee undergoes a TKR. Intraoperatively, after bone cuts are made, the medial compartment remains tight and cannot be opened with a lamina spreader. Which of the following soft tissue structures is the primary target for release to balance the extension gap?
View Answer & Explanation
Correct Answer: D
Rationale: In a severe varus knee, the medial soft tissues are deeply contracted. The text specifies that balancing requires an extensive medial release, which includes stripping the deep MCL from the tibia and releasing the contracted semimembranosus tendon. The lateral structures (A, B, C) would be stretched and attenuated, not tight.
Question 17
A surgeon performs a subtrochanteric derotational osteotomy and stabilizes it with a long-stemmed femoral component during a THR. To minimize the risk of nonunion and implant toggling, the stem must bypass the osteotomy site and achieve stable fixation in the distal fragment. What is the minimum required length of engagement in the distal fragment?
View Answer & Explanation
Correct Answer: C
Rationale: The surgical pearls section provides a clear rule for fixation: "When using a long stem to bypass an osteotomy, the stem must engage at least two cortical diameters of normal bone past the osteotomy site to prevent toggling and nonunion." This ensures adequate stability for healing.
Question 18
A 63-year-old female presents for a THR consultation. On examination, she has a fixed 25° abduction contracture of the affected hip. When she stands with both legs parallel, she reports her affected leg feels significantly longer, though a tape measure from ASIS to medial malleolus shows equal lengths. What is this phenomenon called?
View Answer & Explanation
Correct Answer: C
Rationale: The text clearly distinguishes between Actual and Apparent LLD. An abduction contracture forces the pelvis into obliquity when the patient tries to stand with legs parallel, creating the sensation of a longer leg on the affected side despite equal bone lengths. This is the definition of an Apparent LLD.
Question 19
A 50-year-old male with a complex, multiapical proximal femoral deformity from a childhood infection requires a THR. The surgeon is concerned about placing a standard stem without causing a fracture. What is the most valuable preoperative planning tool to simulate the osteotomy and implant placement?
View Answer & Explanation
Correct Answer: D
Rationale: The text highlights that for complex, multiapical deformities, CT-guided 3D reconstruction is essential. It allows the surgeon to visualize the deformity in space and perform simulated osteotomies on a virtual or physical model, determining exact wedge sizes and cut angles before surgery. While full-length films (A) are crucial for axis measurement, they do not provide the detailed three-dimensional information needed for this level of complexity.
Question 20
A 66-year-old female undergoes a TKR for a 25° fixed valgus deformity. Postoperatively, she is unable to dorsiflex or evert her foot. During the procedure, extensive lateral soft tissue releases were required. What is the most likely cause of her deficit?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that in severe valgus TKR, the peroneal nerve is at extreme risk during correction and lateral release. A foot drop (inability to dorsiflex/evert) is the classic presentation of a peroneal nerve injury. The text also suggests considering prophylactic isolation and protection of the nerve in such cases.
Question 21
A 25-year-old male presents with knee pain 1 year after a tibial plateau fracture was treated nonoperatively. Radiographs reveal a uniapical deformity of the proximal tibia. The AP view shows 15° of varus, and the lateral view shows 20° of procurvatum. A junior resident refers to this as a "biplanar deformity." According to the principles of deformity correction, what is the most accurate description of this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The provided text emphasizes that a uniapical deformity visible on both AP and lateral radiographs is not a "biplanar" deformity but a single uniplanar deformity existing in an oblique plane. Treating it as two separate deformities (Distractor A) is a fundamental error that can lead to secondary translation or malalignment.
Question 22
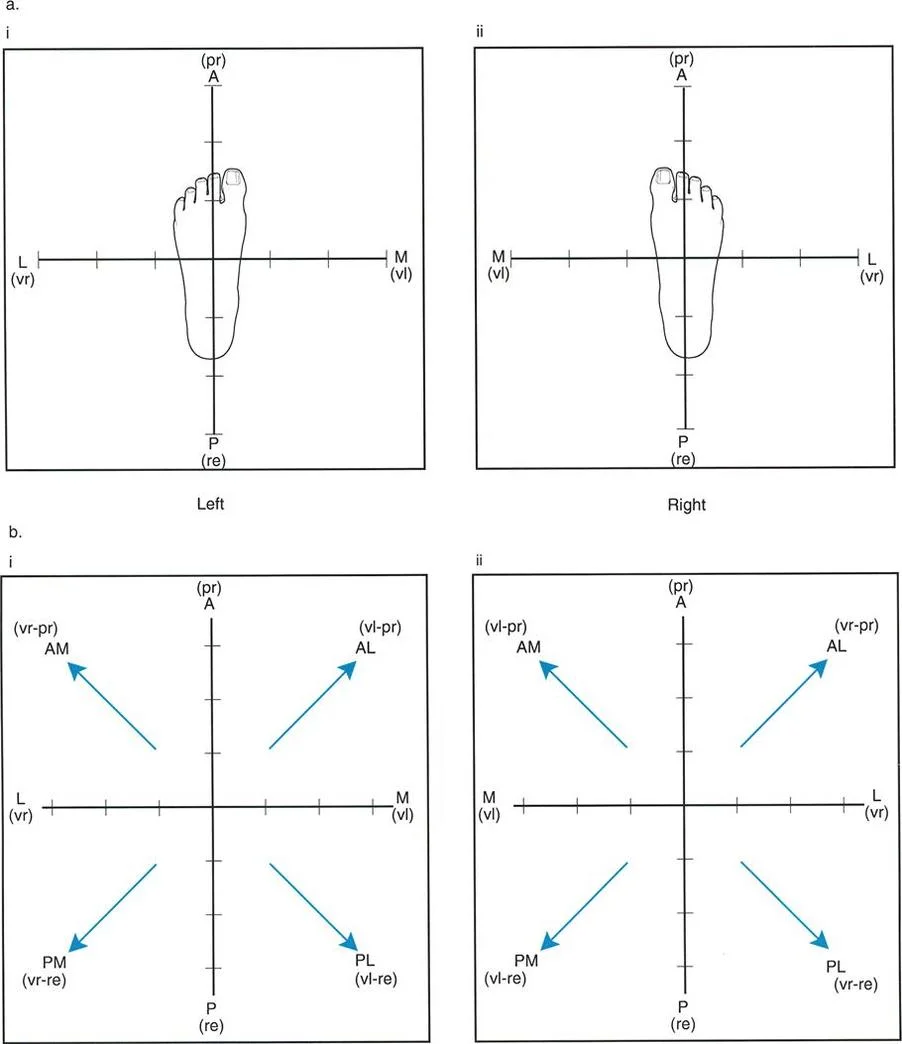
A surgeon is planning an osteotomy for a femoral malunion. The AP radiograph shows 30° of valgus, and the lateral radiograph shows 25° of recurvatum. According to the standard convention for describing oblique plane deformities, what is the correct apical direction?
View Answer & Explanation
Correct Answer: C
Rationale: The convention is to state the sagittal plane direction first, followed by the coronal plane direction. Recurvatum is an apex posterior deformity. Valgus is an apex medial deformity. Therefore, the combined apical direction is Posteromedial (PM). Distractor A (Anteromedial) would correspond to procurvatum and valgus.
Question 23
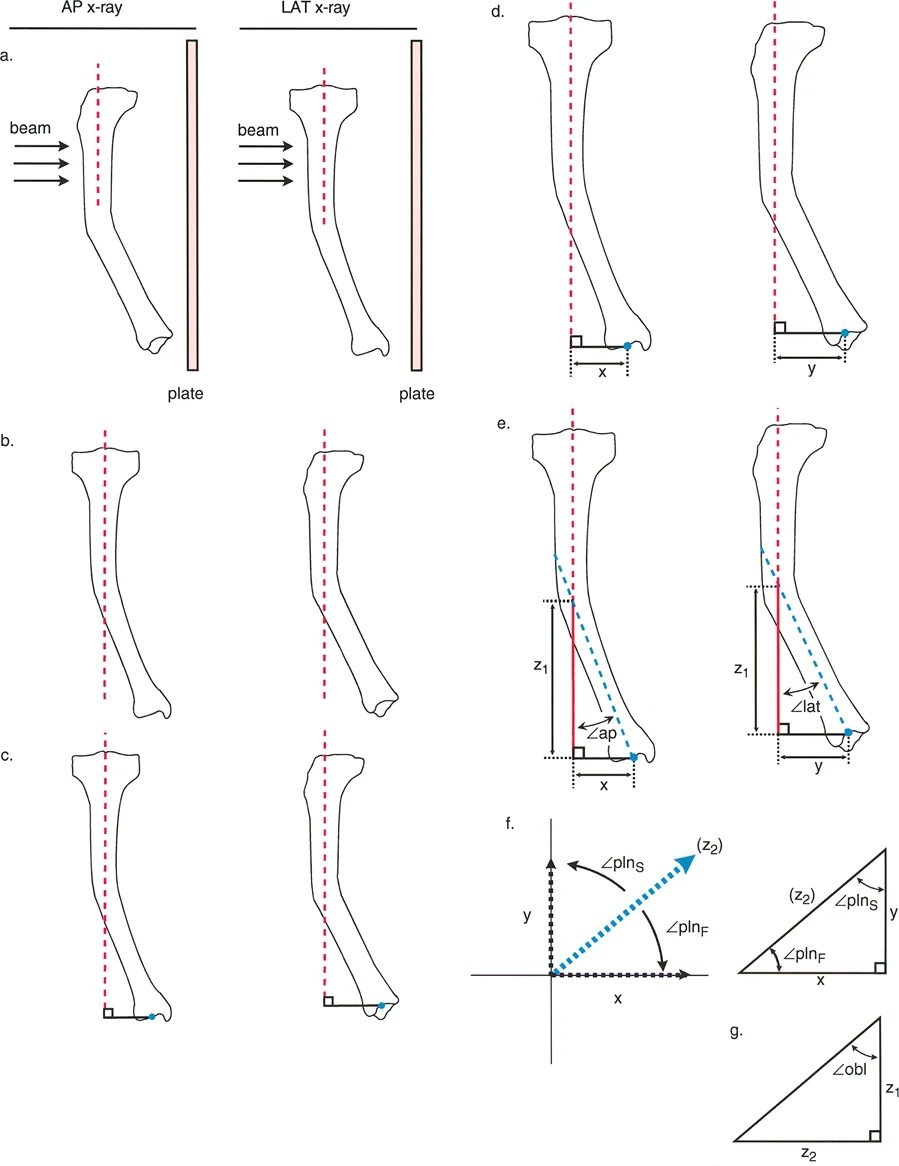
A 40-year-old patient has a distal tibial malunion with 20° of varus (apex lateral) and 20° of procurvatum (apex anterior). A surgeon uses the trigonometric formula $obl = \arctan(\sqrt{\tan^2(ap) + \tan^2(lat)})$ to calculate the true magnitude of the deformity. Which of the following statements is always true regarding the calculated value of $obl$?
View Answer & Explanation
Correct Answer: D
Rationale: A critical rule stated in the text is that the true magnitude of the angulation in the oblique plane ($obl$) is always larger than the magnitude projected in either individual reference plane (AP or lateral). The AP and lateral views show only the "shadow" or projection of the true deformity, which is mathematically always less than or equal to the true magnitude.
Question 24
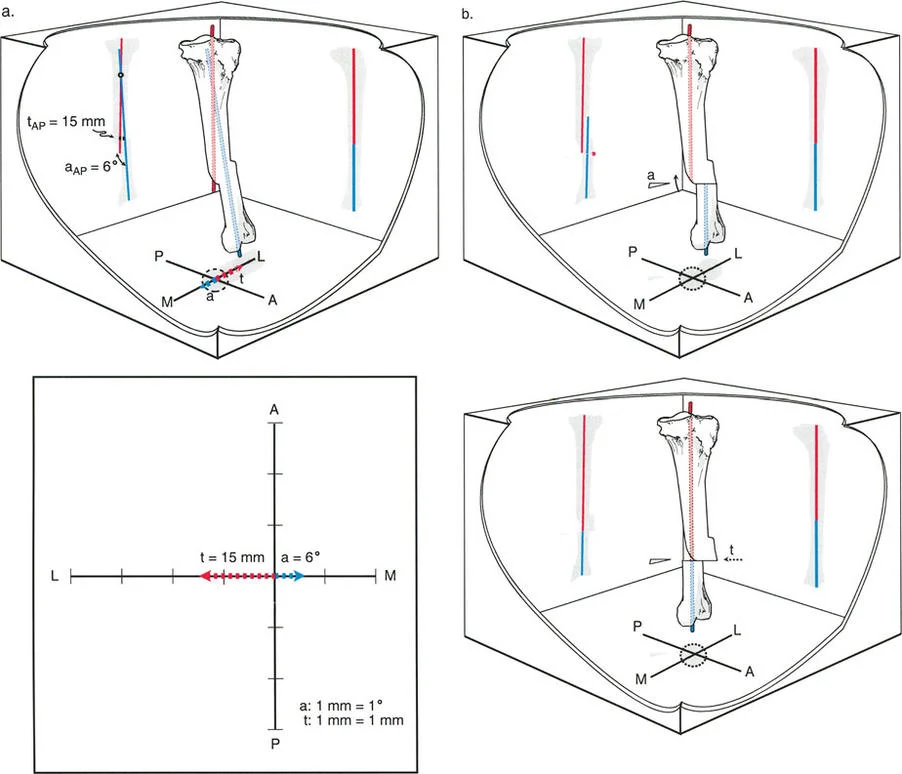
A surgeon is using Paley's Graphic Method to analyze a deformity in a patient's right femur. The deformity consists of varus and procurvatum. When setting up the orthogonal graph, how should the x-axis (coronal plane) be labeled?
View Answer & Explanation
Correct Answer: A
Rationale: The text and accompanying figure specify that when using the Graphic Method, one must imagine looking down at the patient's limb from above. For the right limb, medial is to the right and lateral is to the left on the x-axis. This is a mirror image for the left limb (Distractor B). The y-axis (sagittal plane) labeling is identical for both limbs.
Question 25
When performing Paley's Graphic Method for deformity analysis, what scale is used to plot the angular magnitudes measured from the radiographs onto the orthogonal axes?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that a strict scale of 1 mm = 1 degree must be used when plotting the magnitudes on the graph. This allows the final step of measuring the vector's length in millimeters to directly correspond to the true magnitude of the deformity in degrees, simplifying the process and eliminating the need for further calculation.
Question 26
A 33-year-old female has a mid-shaft tibial malunion. The AP view shows 20° of valgus (apex medial), and the lateral view shows 30° of procurvatum (apex anterior). Using the Graphic Method, a vector is drawn from the origin to the intersection of the plotted points. How is the true magnitude of the oblique plane deformity determined from this graph?
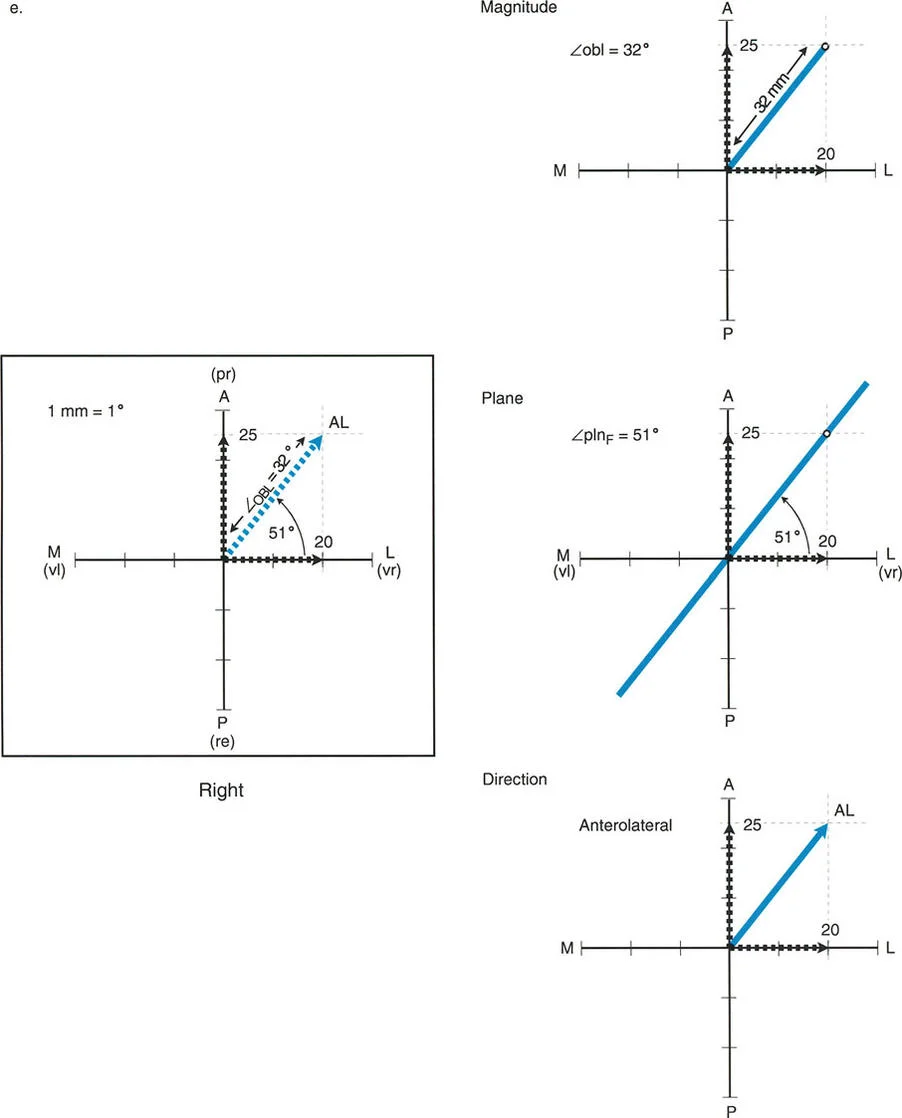
View Answer & Explanation
Correct Answer: C
Rationale: According to Step 5 of the Graphic Method, the true magnitude ($obl$) of the deformity is determined by measuring the length of the resultant vector in millimeters. Because the scale used is 1 mm = 1°, this measurement directly gives the magnitude in degrees. Measuring the angle with the x-axis (Distractor E) determines the orientation of the plane ($pln$), not the magnitude.
Question 27
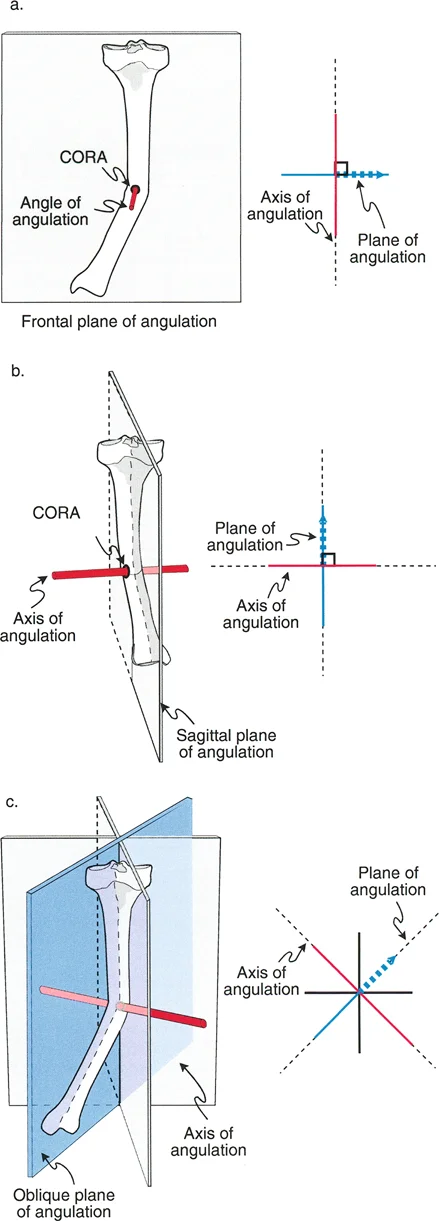
A surgeon is planning a corrective osteotomy for a 28-year-old with a femoral malunion. The true oblique plane of deformity has been calculated. What is the relationship between the plane of angulation and the axis of angulation?
View Answer & Explanation
Correct Answer: B
Rationale: The text states a fundamental principle: "The axis of angulation is always perfectly perpendicular to the plane of angulation." This is crucial for surgical planning, especially for placing hinges for external fixation, which must lie on the axis of correction.
Question 28
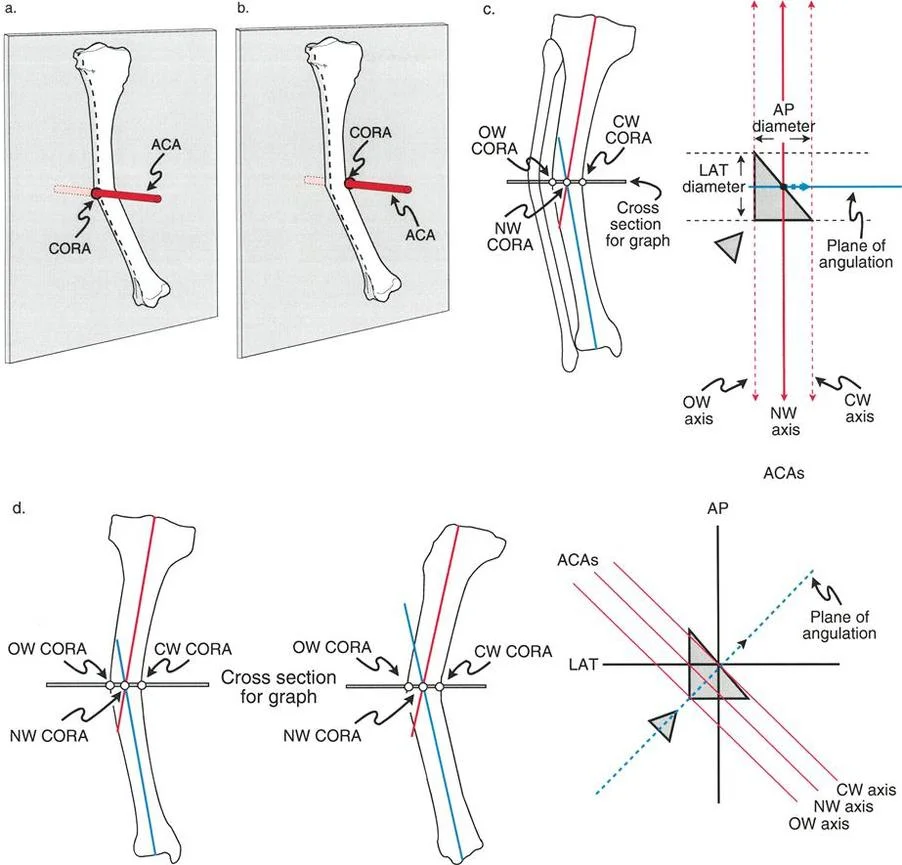
A 19-year-old patient requires correction of an anterolateral tibial deformity using a monolateral external fixator with a single hinge. To achieve pure angular correction without inducing translation, where must the hinge be placed?
View Answer & Explanation
Correct Answer: C
Rationale: For accurate correction with a hinged external fixator, the hinge must be placed exactly on the Axis of Correction of Angulation (ACA). The ACA is perpendicular to the true oblique plane of deformity and passes through the CORA. Placing the hinge parallel to the coronal or sagittal plane (Distractors A and B) would be a common error, leading to incomplete correction and induced translation.
Question 29
The accuracy of Paley's Graphic Method is based on an approximation of trigonometric functions. This method is considered clinically acceptable because the error is minimal for typical deformities. The method is an approximation based on the near-linear behavior of which trigonometric function for angles between 0° and 45°?
View Answer & Explanation
Correct Answer: C
Rationale: The text explains that the Graphic Method works because it simplifies the trigonometric equations by removing the "tan" function. This is a valid approximation because the tangent function is nearly linear for angles less than 45°, which covers the vast majority of clinical deformities. This linearity allows a simple ruler measurement to substitute for a complex trigonometric calculation with minimal error.
Question 30
A surgeon is evaluating a patient with a significant distal femoral malunion where the AP angulation is 50° and the lateral angulation is 55°. When considering the use of Paley's Graphic Method, what is the primary concern regarding the accuracy of the result?
View Answer & Explanation
Correct Answer: B
Rationale: The text states that the accuracy of the Graphic Method is highest when the component deformities are less than 45°. The error is within 4° for combined values less than 45°. When both angulations exceed 45°, the tangent function is no longer linear, and the error of this approximation method increases beyond what may be clinically acceptable, potentially requiring the use of the precise trigonometric formulas instead.
Question 31
A 50-year-old man has a tibial malunion with 30° of varus and 10° of recurvatum. Using Paley's Graphic Method, the surgeon plots 30 mm on the lateral side of the x-axis and 10 mm on the posterior side of the y-axis. A vector is drawn. How is the orientation of the true oblique plane ($pln$) determined from this graph?
View Answer & Explanation
Correct Answer: C
Rationale: Step 5 of the Graphic Method clearly defines how to find the orientation ($pln$). A protractor is used to measure the angle between the resultant vector and the x-axis, which represents the frontal (coronal) plane. This angle defines the orientation of the true oblique plane of deformity. Measuring the vector's length (Distractor A) determines the magnitude, not the orientation.
Question 32
A surgeon is using the Base of Triangle Method (Ilizarov's Method) to analyze a tibial deformity. This method, while accurate, has a significant clinical limitation that makes it less practical than Paley's Graphic Method. What is the primary limitation of the Base of Triangle Method?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that the Base of Triangle method suffers from a severe clinical limitation: "Beam Dependency." It requires the X-ray beam to be perfectly perpendicular to one of the bone segments on both views. This is notoriously difficult to achieve in a deformed limb, and any deviation introduces significant error, making the Paley Graphic Method the preferred clinical standard.
Question 33
A 22-year-old is undergoing acute correction of a posteromedial femoral deformity with an intramedullary nail. To prevent malalignment during nail passage, blocking (Poller) screws are used. To be most effective, how should these screws be oriented relative to the deformity?
View Answer & Explanation
Correct Answer: B
Rationale: The "Surgical Pearls" table indicates that for IM nailing of an oblique deformity, blocking screws must be placed perpendicular to the *true oblique plane* of the deformity. This orientation provides the necessary buttress to guide the nail down the corrected path and prevent it from recreating the original deformity. Placing them relative to the standard AP/LAT planes (Distractors A and C) would be incorrect.
Question 34
A surgeon is planning a closing wedge osteotomy for a varus and procurvatum deformity of the distal femur. The CORA has been identified. To achieve correction without translation, where should the Axis of Correction of Angulation (ACA) be located?
View Answer & Explanation
Correct Answer: B
Rationale: The text specifies the location of the ACA based on the osteotomy type. For a closing wedge osteotomy, the ACA (the hinge of correction) is placed on the concave cortex of the deformity in the true oblique plane. For an opening wedge, it would be on the convex cortex (Distractor A).
Question 35
A 17-year-old patient with a complex tibial deformity is being treated with a hexapod circular external fixator (e.g., Taylor Spatial Frame). The surgeon inputs the AP and lateral deformity parameters into the planning software. What is the primary role of the surgeon in this process, despite the software's computational power?
View Answer & Explanation
Correct Answer: C
Rationale: The surgical pearl regarding hexapod frames highlights that while the software performs the complex calculations, the accuracy of the entire correction is dependent on the surgeon's ability to correctly identify the true CORA and accurately measure the AP and lateral deformity parameters from the radiographs. The principle of "garbage in, garbage out" applies; incorrect inputs will lead to an incorrect correction plan.
Question 36
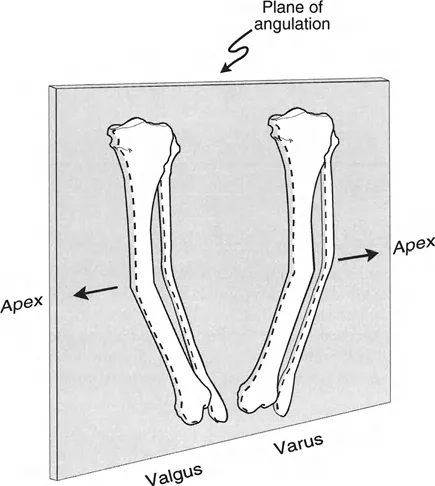
A 35-year-old patient has a tibial deformity characterized by 25° of recurvatum. On the lateral radiograph, this would be described as an apex posterior deformity. How is this deformity defined in the sagittal plane?
View Answer & Explanation
Correct Answer: B
Rationale: The text defines the terminology for anatomic plane deformities. In the sagittal plane, an apex posterior deformity is termed recurvatum. An apex anterior deformity is termed procurvatum (Distractor A). Varus and valgus (Distractors C and D) are coronal plane deformities.
Question 37
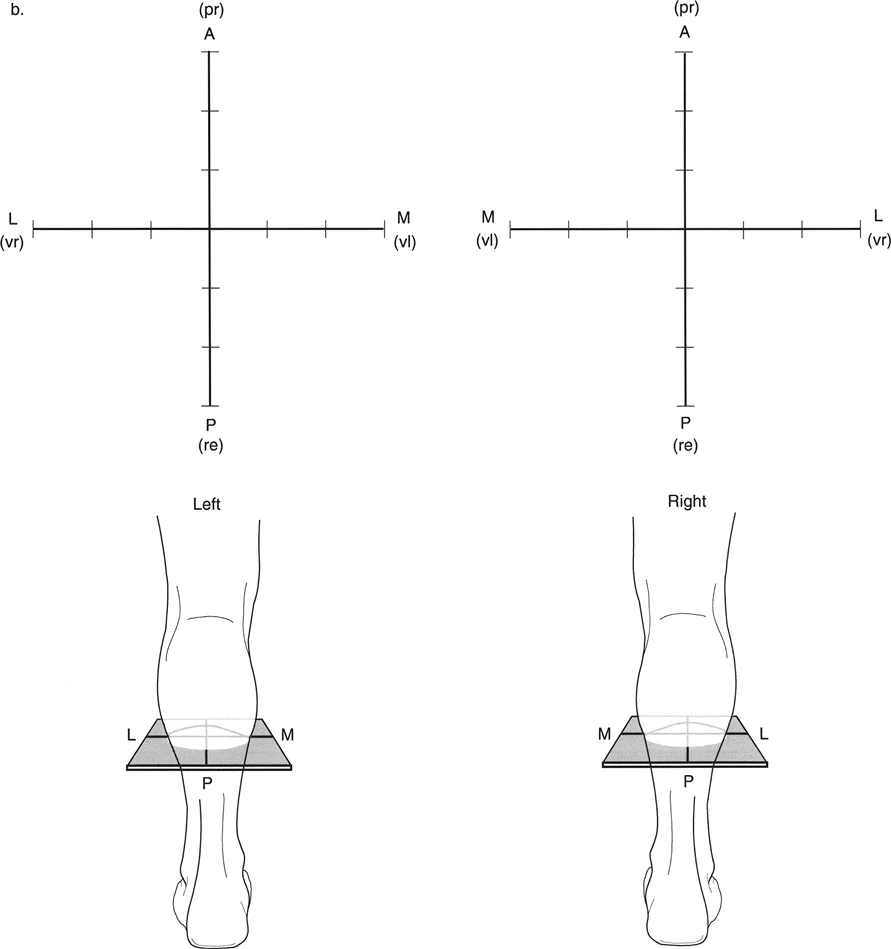
A surgeon is analyzing a deformity of the left tibia using Paley's Graphic Method. The deformity is 15° valgus and 10° procurvatum. How should the axes of the orthogonal graph be labeled for this specific limb?
View Answer & Explanation
Correct Answer: B
Rationale: The text emphasizes that the labeling of the x-axis (coronal plane) is a mirror image for the left limb compared to the right. For the left limb, looking down from above, Lateral is on the right side of the graph and Medial is on the left. The y-axis (sagittal plane) labeling remains consistent, with Anterior up and Posterior down. Distractor A represents the labeling for a right limb.
Question 38
A radiograph is taken of a bone with a 30° anterolateral deformity. If the X-ray beam is oriented perfectly in line with the plane of angulation (i.e., looking "down the barrel" of the deformity), what would be observed on the resulting image?
View Answer & Explanation
Correct Answer: C
Rationale: The text explains this concept with an accompanying figure. A radiograph taken perfectly in line with the plane of angulation would show no deformity because the angulation is occurring directly toward or away from the viewer. Conversely, a radiograph taken perfectly perpendicular to the plane of angulation would show the true, maximum magnitude of the deformity.
Question 39
A 45-year-old female presents with a distal femoral malunion characterized by 20° of valgus and 15° of procurvatum. The surgeon plans to correct this with a single opening wedge osteotomy. What is the primary advantage of correctly identifying this as a uniplanar oblique deformity and making a single cut?
View Answer & Explanation
Correct Answer: B
Rationale: The introduction clearly states that if an oblique plane deformity is incorrectly treated as two separate deformities, the surgeon will "invariably introduce translation, secondary deformities, or mechanical axis deviation (MAD)." Therefore, the main advantage of a single, correctly oriented osteotomy at the CORA is the precise correction of angulation without creating a new problem.
Question 40
A 29-year-old has a tibial malunion with 40° of varus and 15° of recurvatum. Using the Graphic Method, the surgeon plots the points and draws the resultant vector. The length of the vector is measured to be 42.5 mm. What is the true magnitude of the deformity?
View Answer & Explanation
Correct Answer: C
Rationale: The Graphic Method relies on a direct 1:1 scale where 1 mm of vector length equals 1 degree of angulation. Therefore, if the vector measures 42.5 mm, the true magnitude of the oblique plane deformity is 42.5°. This simplicity is the key advantage of the method.
Question 41
A 28-year-old male is evaluated for contralateral hip pain, and as part of the workup, radiographs of the asymptomatic hip are obtained. The angle between the anatomic axis of the femoral shaft and the axis of the femoral neck in the coronal plane is measured. Which of the following represents a normal Neck-Shaft Angle (NSA)?
View Answer & Explanation
Correct Answer: C
Rationale: The normal Neck-Shaft Angle (NSA) is typically 130 degrees, with a normal range of 124–136 degrees. An angle less than 124 degrees is considered coxa vara, while an angle greater than 136 degrees is coxa valga. 170 degrees is the normal Anterior Neck-Shaft Angle (ANSA) in the sagittal plane.
Question 42
A 45-year-old female is undergoing preoperative planning for a corrective osteotomy for genu varum. A full-length standing radiograph is analyzed. The surgeon measures the angle between the mechanical axis of the femur and the joint line of the distal femur. What is the normal value for the mechanical Lateral Distal Femoral Angle (mLDFA)?
View Answer & Explanation
Correct Answer: C
Rationale: The normal mechanical Lateral Distal Femoral Angle (mLDFA) is 87.5 degrees, with a range of 85-90 degrees. This angle is critical for determining if a lower limb deformity originates from the femur or the tibia. A value of 95 degrees would indicate a valgus deformity in the distal femur.
Question 43
A resident is planning a femoral osteotomy and, on a full-length radiograph, draws a straight line connecting the center of the femoral head to the center of the ankle joint. This line is used to assess overall limb alignment. What is this line called?
View Answer & Explanation
Correct Answer: D
Rationale: The mechanical axis of the entire lower limb is a straight line from the center of the femoral head to the center of the ankle joint. The mechanical axis of the femur (distractor C) only runs from the center of the femoral head to the center of the knee, while the anatomic axis follows the mid-diaphyseal line of the bone.
Question 44
A 50-year-old male presents with a femoral shaft malunion. To assess the deformity, the surgeon draws a line following the mid-diaphyseal curve of the femur on an AP radiograph. What axis does this line represent?
View Answer & Explanation
Correct Answer: B
Rationale: The anatomic axis is the mid-diaphyseal line of a bone. In the femur, this line has a natural anterior bow in the sagittal plane and is distinct from the mechanical axis, which is a straight line connecting the centers of the proximal and distal joints.
Question 45
A 33-year-old female with developmental dysplasia of the hip is being evaluated. On her AP pelvis radiograph, the angle between the mechanical axis of the femur and a line from the tip of the greater trochanter to the center of the femoral head is measured to be 105 degrees. What parameter is being assessed, and what does this value indicate?
View Answer & Explanation
Correct Answer: B
Rationale: The Lateral Proximal Femoral Angle (LPFA) is the angle between the femoral mechanical axis and the proximal joint line (trochanter tip to head center). The normal value is approximately 90 degrees. A value of 105 degrees indicates a valgus deformity of the proximal femur. NSA (distractor A) measures the angle with the anatomic axis, not the mechanical axis.
Question 46
A 62-year-old male with a history of a healed intertrochanteric fracture presents with progressive hip pain and a limp. Radiographs reveal a varus malunion with a Neck-Shaft Angle of 100 degrees. According to Pauwels' principles, what is the primary biomechanical consequence of this deformity?
View Answer & Explanation
Correct Answer: B
Rationale: Pauwels' principles state that malalignment, such as coxa vara, alters joint biomechanics by increasing both compressive and shear forces across the articular cartilage. This leads to accelerated cartilage degeneration and osteoarthritis. Coxa vara shortens, not lengthens, the abductor moment arm.
Question 47
A 19-year-old patient with Blount's disease undergoes a standing full-length AP radiograph. The mechanical axis line from the femoral head to the ankle center passes 30mm medial to the center of the knee joint. What is this measurement officially termed?
View Answer & Explanation
Correct Answer: B
Rationale: Mechanical Axis Deviation (MAD) is the measurement of how far the mechanical axis of the lower limb deviates from the center of the knee. A normal MAD is approximately 8mm medial to the knee center. A MAD of 30mm medial indicates a significant varus deformity.
Question 48
A 12-year-old with developmental coxa vara demonstrates a positive Trendelenburg sign. Radiographs show that the tip of the greater trochanter is migrated superiorly relative to the femoral head. Which measurement is most directly correlated with the patient's abductor weakness?
View Answer & Explanation
Correct Answer: C
Rationale: The Articulo-Trochanteric Distance (ATD) is the vertical distance between the femoral head's articular surface and the greater trochanter tip. A decreased or negative ATD shortens the lever arm of the gluteus medius (abductor) muscle, leading to mechanical insufficiency and a positive Trendelenburg sign.
Question 49
A surgeon is planning a corrective osteotomy for a proximal femoral varus deformity. They have drawn the normal mechanical axis of the proximal segment and the normal mechanical axis of the distal segment on a radiograph. The intersection of these two lines defines what critical point for planning?
View Answer & Explanation
Correct Answer: C
Rationale: The Center of Rotation of Angulation (CORA) is the cornerstone of Paley's deformity correction principles. It is precisely defined as the point where the axis of the proximal bone segment intersects with the axis of the distal bone segment. The osteotomy level and hinge point are chosen based on the CORA's location.
Question 50
A 21-year-old has a simple angular deformity in the proximal femur. The surgeon performs a corrective osteotomy where the cut and the axis of correction (hinge) pass directly through the CORA. According to Paley's rules, what is the expected outcome?
View Answer & Explanation
Correct Answer: A
Rationale: This scenario describes Paley's Rule 1. When the osteotomy and hinge are at the CORA, the deformity is corrected by pure angulation, and the proximal and distal axes become collinear without any translational shift. This is the ideal method for correcting a simple angular deformity.
Question 51
A 35-year-old male is undergoing preoperative planning for a complex proximal femoral malunion. The surgeon begins by delineating the fundamental axes of the femur on a long-leg radiograph. According to the principles outlined, how is the mechanical axis of the femur correctly defined?
View Answer & Explanation
Correct Answer: C
Rationale: The provided text explicitly defines the mechanical axis of the femur as "a straight line drawn from the geometric center of the femoral head directly to the center of the intercondylar notch of the knee." This represents the true load-bearing axis. Option A describes the anatomical axis in the coronal plane.
Question 52
A 14-year-old female with a history of developmental dysplasia of the hip is evaluated for a corrective osteotomy. Her radiographs show a significantly increased angle between the femoral neck axis and the anatomical axis of the femoral shaft. Which of the following radiographic parameters is described, and what is its normal range?
View Answer & Explanation
Correct Answer: B
Rationale: The Neck-Shaft Angle (NSA) is defined as the angle between the femoral neck axis and the anatomical axis of the femoral shaft. The normal range is 124° to 136°. A value greater than 136° would be classified as coxa valga, which can be seen in DDH.
Question 53
A 50-year-old male presents with a painful Trendelenburg gait two years after a femoral neck fracture was treated nonoperatively. Radiographs reveal that the tip of his greater trochanter is now 5 mm superior to the center of the femoral head. Which parameter is abnormal, and what is the primary biomechanical consequence?

View Answer & Explanation
Correct Answer: C
Rationale: The Articulotrochanteric Distance (ATD) is the vertical distance from the femoral head center to the trochanter tip. A negative value, as described, indicates a "high-riding trochanter." This severely shortens the abductor lever arm, leading to abductor weakness and a Trendelenburg gait.
Question 54
During preoperative templating for a proximal femoral osteotomy, a surgeon measures the lateral angle formed by the mechanical axis of the femur and a line from the tip of the greater trochanter to the center of the femoral head. The measured value is 75°. Which angle is being measured, and what deformity does this value indicate?

View Answer & Explanation
Correct Answer: C
Rationale: The angle described is the Mechanical Lateral Proximal Femoral Angle (mLPFA). The normal value is 85° to 95°. A value of 75° is below the normal range, indicating a varus deformity of the proximal femur.
Question 55
A 16-year-old male with a malunited Slipped Capital Femoral Epiphysis (SCFE) presents with hip pain and a limp. A standing long-leg radiograph shows the mechanical axis line, drawn from the femoral head to the ankle center, passes 15 mm medial to the center of his knee joint. What is this finding called, and what is its primary long-term risk?
View Answer & Explanation
Correct Answer: B
Rationale: The text states that a varus deformity of the hip (as seen in SCFE) causes the distal femur to shift laterally, resulting in the overall limb mechanical axis deviating medially at the knee. This is termed "medial MAD" and leads to overloading of the medial compartment, predisposing to early osteoarthritis.
Question 56
A surgeon is planning a corrective osteotomy for a 40-year-old with a severe coxa vara deformity. They plan a simple closing wedge osteotomy to restore the Neck-Shaft Angle to 130° without any translation. According to Paley's principles, what is the most likely and dangerous consequence of this specific surgical plan?
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly warns against a pure angular correction (valgus osteotomy) without translation. This maneuver "will swing the distal femur and knee violently laterally," transforming a medial MAD into a severe lateral MAD and transferring destructive forces to the lateral knee compartment.
Question 57
A 13-year-old boy presents with a limp and thigh pain. On examination, he has obligate external rotation with hip flexion. Radiographs are obtained. Based on the typical pathomechanics of Slipped Capital Femoral Epiphysis (SCFE), what is the nature of the displacement?

View Answer & Explanation
Correct Answer: B
Rationale: The text clarifies that in SCFE, the femoral head remains seated in the acetabulum. The deformity occurs as the femoral neck and shaft displace relative to this fixed head. The displacement is superior (creating varus) and anterior (creating extension/retroversion).
Question 58
A resident is evaluating a patient with a chronic, untreated SCFE. The attending surgeon explains that the patient's obligate external rotation is a "rotational illusion." What is the underlying geometric cause of this clinical finding?
View Answer & Explanation
Correct Answer: C
Rationale: The text emphasizes that the apparent rotation is a geometric illusion. The deformity is primarily a single angulation in an oblique plane, combining varus and extension. The angulation around the inclined hinge (ACA) forces the distal limb to swing outwards, creating the appearance of external rotation.
Question 59
A surgeon uses Paley's box diagram to explain a complex proximal femoral deformity to a fellow. The deformity has a 40° varus component in the coronal plane and a 30° extension component in the sagittal plane. What does the Angulation Correction Axis (ACA) represent in this model?

View Answer & Explanation
Correct Answer: C
Rationale: The text and diagram clearly define the Angulation Correction Axis (ACA) as the theoretical hinge pin that is "always perfectly perpendicular to this true oblique plane of deformity." Correcting the angulation around this axis simultaneously addresses both the coronal and sagittal components.
Question 60
A surgeon is planning a proximal femoral osteotomy for a malunited SCFE. They correctly identify the varus and extension components and plan the correction in the true oblique plane. What is the expected outcome regarding the patient's preoperative external rotation deformity if the angular correction is performed perfectly?
View Answer & Explanation
Correct Answer: C
Rationale: This is a key surgical pearl from the text. "If the surgeon perfectly corrects the angulation in the true oblique plane... the apparent rotational deformity will spontaneously and completely correct itself." This understanding prevents an unnecessary and iatrogenic derotational osteotomy.
Question 61
A junior resident is asked to identify the Center of Rotation of Angulation (CORA) for a malunited subcapital fracture. What is the correct definition of the CORA?
View Answer & Explanation
Correct Answer: D
Rationale: The text defines the CORA as "the exact, mathematically defined point where the central axis of the proximal fragment and the central axis of the distal fragment intersect." This is the geometric epicenter of the deformity.
Question 62
A surgeon is templating an osteotomy for the malunited femoral neck fracture shown in the image. They have drawn the anatomical axis of the distal fragment (blue line) and the correct axis of the proximal fragment (red line). Where is the CORA located in this specific case?

View Answer & Explanation
Correct Answer: C
Rationale: The image and accompanying text demonstrate that the CORA is located at the intersection of the proximal and distal axes. In cases of subcapital fractures or SCFE, this point is "located precisely at the level of the physis or the old fracture line."
Question 63
A surgeon plans to correct a severe SCFE deformity by performing a cuneiform osteotomy at the subcapital level, exactly at the CORA. The correction will be hinged at the same location. Which of Paley's osteotomy rules is being applied, and what is the single greatest risk of this procedure?
View Answer & Explanation
Correct Answer: A
Rationale: Performing the osteotomy and hinging the correction at the CORA is Paley's Rule 1. The text explicitly warns that for a subcapital CORA, this approach (like a Dunn osteotomy) "carries a massive risk of devascularizing the femoral head, leading to avascular necrosis (AVN)" due to the tenuous blood supply from the medial circumflex femoral artery.
Question 64
A 45-year-old patient with a painful coxa vara malunion is scheduled for surgery. The surgeon plans an intertrochanteric osteotomy but intends to place the hinge of correction (ACA) at the true CORA, located at the base of the femoral neck. Which of Paley's rules describes this plan, and what is the expected geometric outcome at the osteotomy site?
View Answer & Explanation
Correct Answer: B
Rationale: This scenario describes Paley's Rule 2: the osteotomy is performed away from the CORA (intertrochanteric level), but the ACA is placed at the CORA (femoral neck). The text states this results in the angular deformity being fully corrected, but a "predictable translation will be induced at the osteotomy site."
Question 65
Why is the application of Paley's Rule 2 considered the "workhorse principle" and biomechanically advantageous for correcting coxa vara?
View Answer & Explanation
Correct Answer: B
Rationale: The text highlights two key advantages of Rule 2. First, the osteotomy is performed at the highly vascular intertrochanteric level, far from the femoral head's blood supply, avoiding AVN. Second, the induced medial translation is a "strict biomechanical requirement" to realign the limb's mechanical axis and correct the medial MAD at the knee.
Question 66
During a proximal femoral osteotomy, the surgeon makes the cut at the subtrochanteric level and also places the hinge of correction (ACA) at the subtrochanteric level, despite the true CORA being at the femoral neck. According to Paley's principles, what is the inevitable outcome of this surgical choice?
View Answer & Explanation
Correct Answer: D
Rationale: This describes a Rule 3 osteotomy, where both the cut and the hinge are placed away from the true CORA. The text states that this results in "a massive translation and the creation of a secondary, iatrogenic deformity (a 'Z-deformity' or zigzag alignment)," which will likely misalign the mechanical axis relative to the knee.
Question 67
A surgeon is selecting an implant for a proximal femoral osteotomy in an elderly patient with severe osteoporosis. They desire excellent fixation and versatile screw placement. Which implant, according to the provided text, would be most suitable for this specific clinical challenge?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that "Modern locking plates offer excellent purchase in osteoporotic bone and allow for more versatile screw placement," making them a suitable choice for this patient. A blade plate requires precise insertion and may have less purchase in poor quality bone.
Question 68
A 25-year-old patient with a history of septic arthritis of the hip as a child presents with a severe, rigid proximal femoral deformity and poor bone quality. The surgeon desires the ability to perform a gradual correction and potentially adjust the alignment postoperatively. Which fixation method is ideal for this scenario?

View Answer & Explanation
Correct Answer: D
Rationale: The text identifies external fixation as "Ideal for gradual correction, cases with poor bone quality, or active infection." It also highlights the ability to allow for "postoperative tweaking of the alignment in all six degrees of freedom," which perfectly matches the needs of this complex case.
Question 69
A 6-year-old girl with known fibular hemimelia presents for evaluation of a progressive leg length discrepancy (LLD). Her parents report she has always had a shorter left leg, and the difference seems to be getting larger as she grows. Clinical examination confirms a 4 cm LLD. Serial scanograms over the past two years show a consistent percentage of growth inhibition in the affected limb. According to Shapiro's classification, which pattern of growth inhibition does this clinical scenario most represent?
View Answer & Explanation
Correct Answer: A
Rationale: The Type 1 pattern is defined by a constant, linear progression of the discrepancy due to a fixed percentage of growth inhibition. This is the classic pattern for congenital deficiencies like fibular hemimelia. Type 3 (Upward Slope Plateau) is incorrect as it is characteristic of post-fracture overgrowth, where the discrepancy eventually becomes static.
Question 70
A 7-year-old boy sustained a diaphyseal femur fracture treated with flexible intramedullary nails. At his 1-year follow-up, his parents notice he is limping. A scanogram reveals the fractured limb is now 1.5 cm longer than the contralateral limb. The surgeon counsels the parents that this discrepancy is unlikely to increase further. Which Shapiro pattern of LLD progression does this scenario describe?
View Answer & Explanation
Correct Answer: C
Rationale: The Type 3 pattern is classically associated with the overgrowth phenomenon following a pediatric femoral shaft fracture. The initial hyperemia stimulates growth (upward slope), which then equalizes with the other limb as the fracture heals, causing the discrepancy to plateau. Type 1 is incorrect because the percentage of growth inhibition is not constant; rather, there is a period of overgrowth that ceases.
Question 71
An 8-year-old girl with a history of oligoarticular juvenile idiopathic arthritis (JIA) affecting her right knee presents for evaluation. Initially, her right leg was noted to be 1 cm longer than her left due to chronic hyperemia. Now, at age 12, her right leg is 2 cm shorter than her left. This reversal of the discrepancy is most characteristic of which Shapiro pattern?
View Answer & Explanation
Correct Answer: E
Rationale: The Type 5 pattern is the classic, paradoxical pattern seen in JIA. Initial hyperemia causes overgrowth (upward slope), but persistent inflammation eventually destroys the physis, leading to growth arrest. The once-longer limb then becomes shorter as the contralateral limb continues to grow (downward slope). Type 4 is incorrect as it describes a biphasic worsening of LLD, not a reversal.
Question 72
A 9-year-old boy with a history of Legg-Calvé-Perthes disease of the left hip is being followed annually. His LLD increased from 1 cm to 2.5 cm between ages 6 and 8. The discrepancy then remained stable at 2.5 cm until age 11. Now, at age 12, a new scanogram shows the discrepancy has increased to 3.5 cm. This erratic, multi-phasic progression is best described by which Shapiro pattern?
View Answer & Explanation
Correct Answer: D
Rationale: The Type 4 pattern is characteristic of conditions with delayed or intermittent insults to the physis, classically Legg-Calvé-Perthes disease. It involves an initial period of increasing discrepancy, followed by a plateau, and then a second phase of accelerating discrepancy due to premature physeal arrest. Type 1 is incorrect because the progression is not linear or predictable.
Question 73
In the context of pediatric LLD, the introduction of the fourth dimension, "time," signifies that the condition is:
View Answer & Explanation
Correct Answer: B
Rationale: The text emphasizes that pediatric LLD is a "four-dimensional problem," with time being the critical fourth dimension. This highlights its dynamic nature, where the discrepancy changes over the course of a child's growth, making prediction essential for proper management. A static deformity (A) is characteristic of adult malunions, not growing children.
Question 74
A 5-year-old boy presents with a 3 cm LLD due to a congenital short femur. His parents are anxious about the final discrepancy at maturity. The surgeon explains that because the percentage of growth inhibition is expected to remain constant, they can accurately predict the final LLD. For which Shapiro pattern are standard predictive models, like the Moseley straight-line graph, most reliable?
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly states that the Type 1 (Upward Slope, Proportionate) pattern, with its constant, linear progression, is the only pattern for which standard mathematical prediction models like the Moseley graph are highly accurate. All other patterns have variable rates of progression, making standard prediction unreliable.
Question 75
A 10-year-old girl is being evaluated for LLD. Her growth chart shows an initial rapid increase in the discrepancy, which has now started to slow down. The affected limb appears to be partially "catching up" in growth velocity. Standard prediction models are likely to overestimate the final discrepancy in this patient. This clinical picture is most consistent with which Shapiro pattern?
View Answer & Explanation
Correct Answer: B
Rationale: The Type 2 pattern is defined by an initial increase in discrepancy that then decelerates as the affected limb's growth rate partially recovers. The text notes that standard prediction models will often overestimate the final discrepancy in this less common pattern. Type 1 is incorrect because the rate of inhibition is not constant.
Question 76
When planning treatment for a pediatric LLD, the most crucial parameter for accurately assessing remaining growth potential and timing interventions is:
View Answer & Explanation
Correct Answer: B
Rationale: The text highlights the work of Anderson, Green, and Messner, emphasizing the "absolute superiority of skeletal age over chronological age for assessing remaining growth potential." Skeletal age, determined from a left hand/wrist radiograph, is the cornerstone of all modern LLD prediction methods. Chronological age can be misleading due to variations in maturation.
Question 77
An orthopedic resident is preparing to use the Moseley straight-line graph for a patient with a Type 1 LLD. To do this, she orders a radiograph of the left hand and wrist. The purpose of this radiograph is to compare it to a standardized atlas to determine the patient's:
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states that skeletal age is determined by comparing a left hand and wrist radiograph to the standardized Greulich and Pyle atlas. This is a fundamental step before using any growth prediction chart, including the Moseley graph, as it provides a more accurate measure of skeletal maturity than chronological age.
Question 78
A senior surgeon is explaining the Moseley straight-line graph to a medical student. She points out that the x-axis, representing skeletal age, is not linear. What was the primary reason for Moseley's mathematical manipulation of the x-axis scale?

View Answer & Explanation
Correct Answer: B
Rationale: The text explains that Moseley's "major insight was to mathematically convert this curvilinear growth into a straight line." He achieved this by altering the distance between the age scale on the x-axis, which is why it is non-linear. This allows for simple linear extrapolation to predict growth. The other options are incorrect purposes for this specific design feature.
Question 79
When using the Moseley straight-line graph, the growth of the patient's normal, long leg is plotted as a reference. What is the standard slope of this reference line on the graph?
View Answer & Explanation
Correct Answer: B
Rationale: The text and the accompanying image of the Moseley graph clearly state that the "LONG LEG" line is plotted as a reference at a 45-degree angle. This is a fundamental feature of the graph's design, representing normalized, straightened growth against which the shorter leg's growth is compared.
Question 80
A 7-year-old boy with a post-traumatic physeal arrest of the distal tibia is being evaluated for LLD. The surgeon plans to use the Moseley straight-line graph to predict the discrepancy at maturity and time an epiphysiodesis. What is the minimum number of data points, and the preferred time interval between them, required to reliably use this method?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states a significant limitation of the Moseley method: "It requires at least two to three datum points, preferably obtained at least 1 year apart, to accurately predict LLD." This is necessary to establish a reliable slope for the short leg's growth line. A single data point is insufficient to determine the rate of progression.
Question 81
The foundational longitudinal growth data upon which all modern LLD prediction methods, including the Moseley graph, are based was published by which group of researchers?
View Answer & Explanation
Correct Answer: C
Rationale: The text clearly states, "All modern prediction methods are built upon the seminal, exhaustive longitudinal growth data published by Anderson, Green, and Messner in the mid-20th century." Greulich and Pyle (B) developed the atlas for skeletal age, but the core growth data came from Anderson et al.
Question 82
A 4-year-old girl is diagnosed with hemihypertrophy, causing a progressive LLD of the right lower extremity. Her parents ask why the leg length difference is getting worse over time. The most accurate explanation is that the discrepancy increases because:
View Answer & Explanation
Correct Answer: B
Rationale: Hemihypertrophy/hemiatrophy syndromes typically follow a Shapiro Type 1 pattern. In this pattern, the percentage difference in growth rate between the two limbs is constant. Therefore, as the child undergoes normal growth, the absolute difference in length becomes progressively larger. The short leg does not stop growing (A); it just grows at a slower, fixed percentage rate compared to the long leg.
Question 83
A 13-year-old boy presents with the clinical finding shown in the image. He has a history of a severe proximal tibia fracture at age 8 that resulted in a complete physeal arrest. Which Shapiro pattern of LLD progression would be expected in this patient since the time of his injury?

View Answer & Explanation
Correct Answer: A
Rationale: A stable, complete physeal arrest results in a fixed, constant percentage of growth inhibition (100% inhibition at that physis). This leads to a predictable, linear increase in the LLD as the contralateral limb continues to grow normally, which is the definition of a Shapiro Type 1 pattern. Type 3 is incorrect as it relates to overgrowth from diaphyseal fractures, not growth arrest from physeal injury.
Question 84
The historical method of LLD prediction, popularized by Amstutz, required the surgeon to first determine the patient's growth percentile. How was this accomplished?
View Answer & Explanation
Correct Answer: D
Rationale: The text describes the Amstutz method: "The current long leg femoral and tibial lengths were compared with the measurements presented by Anderson et al. (1964) for the current age and sex of the child. This was done to determine the correct growth percentile for the patient." This cumbersome step was later simplified by the graphical method of Moseley.
Question 85
A 10-year-old girl is shown in the clinical image, requiring a 5 cm block to level her pelvis. She has a diagnosis of congenital short femur. The orthopedic surgeon is planning her treatment. What is the absolute first step in the evaluation and planning process for this patient?

View Answer & Explanation
Correct Answer: B
Rationale: The text states, "Identifying the correct [Shapiro] pattern is the mandatory first step in evaluation, as it determines which predictive models can be reliably applied and which surgical timelines are appropriate." Before any prediction can be made or surgery planned, the surgeon must understand the behavior of the discrepancy over time.
Question 86
The underlying pathophysiology of the initial "upward slope" in a Shapiro Type 3 pattern following a femoral shaft fracture is:
View Answer & Explanation
Correct Answer: D
Rationale: The text explains that for a Type 3 pattern, "the profound hyperemia associated with fracture healing and callus formation stimulates the adjacent physes (especially the distal femur), causing the affected limb to grow faster and longer." This overgrowth creates the initial upward slope. Chronic inflammation (C) is characteristic of Type 5 (JIA).
Question 87
A 9-year-old boy with a history of Legg-Calvé-Perthes disease presents with a worsening limp and groin pain. Radiographs show superior and lateral migration of the femoral head with a break in Shenton's line. The fundamental pathomechanical event that distinguishes this "pseudo-subluxation" from a true subluxation is:
View Answer & Explanation
Correct Answer: C
Rationale: Pseudo-subluxation is defined by the structural failure and collapse *within* the femoral head, causing the femur to migrate with the collapsed segment. True subluxation involves the displacement of an intact, spherical femoral head from the acetabulum, typically due to acetabular dysplasia (B) or capsular laxity (D).
Question 88
A 45-year-old male on long-term steroid therapy develops progressive hip pain. Radiographs reveal flattening of the anterosuperior femoral head and apparent lateral uncoverage. According to the provided text, the two most common conditions leading to hip pseudo-subluxation are severe Legg-Calvé-Perthes disease and:
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that pseudo-subluxation is most commonly observed in severe cases of Legg-Calvé-Perthes disease and advanced osteonecrosis (avascular necrosis) of the hip, both of which compromise the structural integrity of the femoral head. Slipped capital femoral epiphysis (A) is a different pathomechanical entity involving the physis.
Question 89
An 11-year-old boy with severe Perthes disease undergoes preoperative planning. Based on finite element analysis and known vascular anatomy, the predictable three-dimensional vector of femoral head displacement in pseudo-subluxation is:

View Answer & Explanation
Correct Answer: B
Rationale: The anterosuperior and lateral portions of the femoral head are most vulnerable to ischemic insult and subsequent collapse. Consequently, the femoral head predictably displaces along this vector: anteriorly, superiorly, and laterally. The anterior component is often hidden on plain radiographs.
Question 90
A 10-year-old girl presents with a painful limp. Radiographs show a flattened femoral head with a break in Shenton's line and an increased teardrop distance. A CT scan is ordered for further evaluation. The primary reason for obtaining a CT scan in the workup of pseudo-subluxation is to:
View Answer & Explanation
Correct Answer: D
Rationale: The text emphasizes that anterior displacement is the "hidden enemy" in pseudo-subluxation, not visible on conventional 2D radiographs. A CT scan with 3D reconstructions is mandatory to accurately visualize and quantify this anterior migration, which is critical for planning the correct distraction vector. While CT can assess other factors (C), its non-negotiable role here is to define the 3D deformity.
Question 91
A 12-year-old boy with severe, untreated Perthes disease is evaluated. On physical examination, he demonstrates a significant lurching gait. Radiographs show superior migration of the femoral head and a greater trochanter that is level with the center of the femoral head. This gait abnormality is primarily caused by:
View Answer & Explanation
Correct Answer: D
Rationale: The lurching Trendelenburg gait is a hallmark of abductor weakness. In pseudo-subluxation, the superior migration of the collapsed head, combined with relative overgrowth of the greater trochanter, severely reduces or creates a negative Articulo-Trochanteric Distance (ATD). This shortens the abductor lever arm, rendering the gluteus medius and minimus mechanically inefficient. An adduction contracture (A) contributes to the deformity but is not the primary cause of the abductor lurch.
Question 92
An 11-year-old male with a flattened, extruded femoral head from Perthes disease is being considered for surgery. A maximum abduction radiograph is obtained. The view demonstrates that the lateral edge of the deformed head pivots on the acetabular rim, causing the medial joint space to widen. This phenomenon is known as:
View Answer & Explanation
Correct Answer: A
Rationale: Hinge abduction is the term used to describe the fulcrum effect created when a flattened, incongruent femoral head is forced into abduction. The deformed lateral portion of the head cannot enter the acetabulum and instead pivots on the lateral rim, preventing concentric reduction and prying the joint open medially. This finding is a contraindication to traditional containment osteotomies.
Question 93
A surgeon is planning a correction for a 13-year-old with severe pseudo-subluxation. According to Paley's principles of deformity correction, the Center of Rotation of Angulation (CORA) for this condition is located:
View Answer & Explanation
Correct Answer: D
Rationale: The deformity in pseudo-subluxation originates from the collapse and displacement of the femoral head, making it an entirely intra-articular problem. Therefore, the CORA is located inside the hip joint itself. This is the fundamental reason why extra-articular osteotomies (A, B) are biomechanically incorrect for correcting the primary deformity.
Question 94
A 14-year-old with pseudo-subluxation of the left hip is noted to have a 2 cm leg length discrepancy and a bowlegged appearance. A long-leg standing radiograph is obtained. The lateral and superior displacement of the femoral head will cause what predictable change to the mechanical axis at the level of the knee?
View Answer & Explanation
Correct Answer: C
Rationale: The mechanical axis is a line from the center of the femoral head to the center of the ankle. When the femoral head (the starting point) displaces laterally, the entire axis pivots, causing the line to pass more medially at the knee. This increases the medial Mechanical Axis Deviation (MAD), overloads the medial compartment, and can lead to secondary genu varum.
Question 95
A surgeon performs a subtrochanteric varus osteotomy on a patient with severe pseudo-subluxation, hoping to achieve containment. According to the principles outlined in the text, why is this approach likely to fail and potentially worsen the patient's mechanics?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that the CORA is intra-articular. Performing an osteotomy distal to the CORA (e.g., subtrochanteric) violates the fundamental rule of deformity correction. This will correct the angular deformity but will induce an unwanted secondary translation of the femoral shaft, further complicating the limb's mechanical axis. It also risks creating hinge abduction.
Question 96
A 10-year-old boy with Perthes-related pseudo-subluxation complains of pain in his groin that radiates to the inner aspect of his knee. His knee examination is entirely normal. This pattern of referred pain is mediated by which nerve?
View Answer & Explanation
Correct Answer: C
Rationale: The obturator nerve provides sensory innervation to the hip joint as well as a cutaneous branch to the medial aspect of the knee. Irritation or pathology within the hip joint, as seen in this case, frequently refers pain along the distribution of the obturator nerve to the medial knee, which can be a significant clinical confounder.
Question 97
An 11-year-old male with severe Perthes disease is shown in the images below. An intraoperative arthrogram is performed. What is the primary purpose of the arthrogram in this clinical scenario?

View Answer & Explanation
Correct Answer: C
Rationale: In children, the ossific nucleus on a plain radiograph underestimates the true size and shape of the femoral head. An arthrogram is the gold standard for outlining the full cartilaginous surface. It reveals the actual geometry of the head and can be used dynamically under fluoroscopy to confirm the presence of hinge abduction, which is critical for surgical decision-making.
Question 98
A 13-year-old is undergoing preoperative planning for femoropelvic distraction. A physical exam reveals a tight, palpable band in the groin, and the hip cannot be passively abducted beyond 5 degrees. To allow for successful medialization of the femur during distraction, which concomitant procedure is almost always required?
View Answer & Explanation
Correct Answer: C
Rationale: The text identifies the adduction contracture as particularly "pernicious." The tight adductor longus acts as a tether, pulling the femur proximally and laterally, directly opposing the goals of distraction. An aggressive adductor tenotomy is therefore essential to release this constraint and permit the femur to be mobilized distally and medially into the acetabulum.
Question 99
A surgeon is explaining the benefits of femoropelvic distraction to the parents of a child with severe Perthes disease. The primary biological advantage of this technique in the pediatric population is that it:
View Answer & Explanation
Correct Answer: B
Rationale: Femoropelvic distraction works by mechanically offloading the collapsed, necrotic segment of the femoral head. This relieves pressure, restores synovial fluid circulation, and allows the innate plasticity and remodeling potential of the pediatric femoral head to improve its sphericity over time. It does not aim to fuse the joint (D) or force containment through varus (E).
Question 100
A 12-year-old girl is treated for left hip pseudo-subluxation with the device shown. The goal of this treatment is to reverse the pathological displacement. The three vectors of correction applied by this external fixator are:

View Answer & Explanation
Correct Answer: B
Rationale: The treatment aims to reverse the exact path of the pathological displacement. Since the femoral head displaces superiorly, laterally, and anteriorly, the corrective distraction vector must be distal (to restore length), medial (to reduce lateralization), and posterior (to correct the hidden anterior displacement).
You Might Also Like