ABOS Orthopedic Board Review: Lower Limb Deformity Correction, Gait, & Guided Growth | Part 11
Key Takeaway
Lower extremity deformity correction involves understanding Paley's rules, CORA, mechanical axis deviation, and sagittal plane analysis. Key aspects include gait biomechanics, joint orientation angles (mLDFA, MPTA), and pediatric guided growth principles like Heuter-Volkmann and Wolff's laws for effective surgical planning and outcomes.
Question 1
A surgeon is performing a simple, uniapical varus correction in the proximal femur. To achieve a perfect correction where the mechanical axis is restored to a straight line without any displacement, which of Paley's rules must be followed?
View Answer & Explanation
Correct Answer: C
Rationale: This describes Paley's Rule One, the ideal correction. When the osteotomy and the axis of correction are both located at the CORA, the angular deformity is corrected, and the proximal and distal mechanical axes become perfectly collinear without any translation.
Question 2
A 40-year-old patient has a proximal femoral deformity with the CORA located in a region of poor, osteopenic bone. The surgeon decides to perform the osteotomy 3 cm distal to the CORA where the bone quality is better. To achieve a perfectly collinear mechanical axis, what must be done?
View Answer & Explanation
Correct Answer: B
Rationale: This is an application of Paley's Rule Two. When the osteotomy is not at the CORA, the mechanical axis can still be restored, but only if the hinge of correction remains at the CORA. This maneuver necessitates an intentional, mathematically planned translation of the bone fragments at the osteotomy site.
Question 3
A patient undergoes a subtrochanteric osteotomy for a varus deformity. Postoperatively, the limb appears visually straight, but a full-length radiograph reveals that the mechanical axis passes through the hip and ankle centers but deviates medially, missing the center of the knee. This "dog-leg" deformity is known as Mechanical Axis Deviation (MAD). What is the most likely surgical error?
View Answer & Explanation
Correct Answer: C
Rationale: This describes the common pitfall outlined in Paley's Rule Three. When both the cut and the hinge are placed away from the CORA (e.g., "eyeballing" the correction), an unplanned, iatrogenic translation is created. The axes become parallel but not collinear, resulting in a persistent MAD.
Question 4
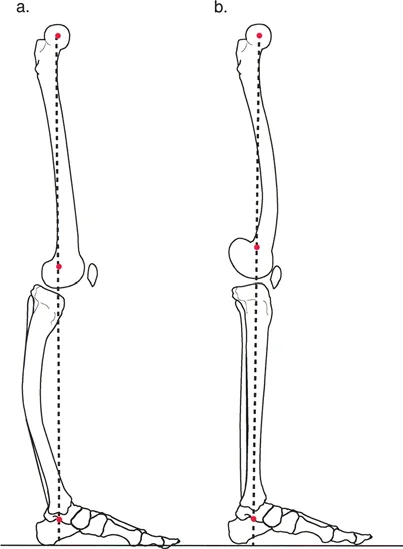
A 65-year-old male is evaluated for gait instability. During the stance phase, his quadriceps are observed to be continuously firing. A long-leg lateral radiograph is obtained with the knee in terminal extension. Which of the following radiographic findings would best explain the need for constant quadriceps activation during stance?
View Answer & Explanation
Correct Answer: B
Rationale: The sagittal mechanical axis must pass anterior to the knee's center of rotation to create a passive extension moment, allowing the knee to "lock" and the quadriceps to relax during stance. If the axis passes posteriorly, a flexion moment is created, requiring continuous quadriceps firing to prevent buckling. Option A describes the normal, efficient state.
Question 5
A 45-year-old female with a history of poliomyelitis presents with a gait disturbance. She ambulates by thrusting her hip forward to achieve knee stability. This compensatory mechanism is designed to manipulate the ground reaction force and sagittal mechanical axis. What is the primary biomechanical goal of this gait pattern?
View Answer & Explanation
Correct Answer: B
Rationale: Patients with quadriceps paralysis rely on passive skeletal locking for stability. By thrusting the hip forward, they move their body's center of gravity and the sagittal mechanical axis anterior to the knee's center of rotation. This creates an extension moment that passively locks the knee, preventing collapse without active quadriceps function. Option A would cause knee buckling.
Question 6
A 28-year-old male sustains a tibial shaft fracture that heals with an apex posterior deformity (recurvatum). He is able to walk with a near-normal gait pattern despite the significant bony deformity seen on radiographs. Which compensatory mechanism is he most likely utilizing?
View Answer & Explanation
Correct Answer: C
Rationale: Recurvatum (apex posterior) deformities are compensated for by flexing the knee. This action moves the distal limb segment anteriorly, effectively neutralizing the bony deformity and restoring a more normal overall sagittal mechanical axis. Option D would exacerbate the deformity's effect.
Question 7
A 35-year-old female presents with a distal femoral procurvatum deformity following a malunited fracture. To compensate and maintain a functional limb alignment, which joint motion is required?
View Answer & Explanation
Correct Answer: B
Rationale: A procurvatum (apex anterior) deformity shifts the distal segment posteriorly. To compensate and bring the foot back under the body's center of gravity, the knee must hyperextend. This is less well-tolerated than the compensation for recurvatum because the knee's capacity for hyperextension is anatomically limited. Option A is the compensation for recurvatum.
Question 8
A 70-year-old patient from a culture where deep squatting is a daily activity undergoes a total knee arthroplasty. During the procedure, significant cartilage loss is noted. Based on biomechanical studies of knee joint loading, where are these osteoarthritic lesions most likely to be predominantly located?
View Answer & Explanation
Correct Answer: B
Rationale: Biomechanical studies show that maximum knee joint loading occurs at 15° to 20° of flexion and is exacerbated in deep squatting. This leads to a higher prevalence of early and severe osteoarthritic lesions on the posterior aspect of the femoral condyles. Option A is incorrect as the anterior condyles are loaded less intensely.
Question 9
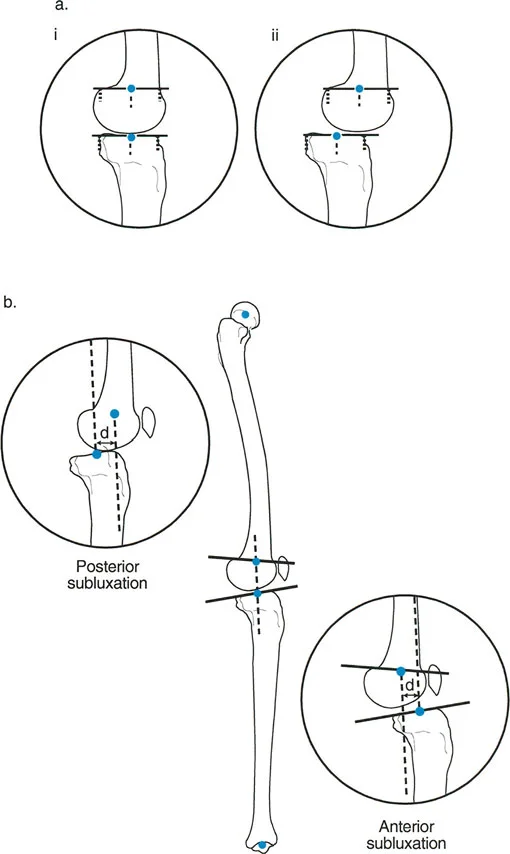
A 55-year-old male with chronic knee instability is evaluated with a lateral radiograph in full extension. The surgeon measures the distance between the mid-sagittal line of the lateral femoral condyle and the mid-sagittal line of the tibial plateau. A measurement of 5 mm is recorded, with the tibia displaced anteriorly. What is the correct diagnosis?
View Answer & Explanation
Correct Answer: B
Rationale: According to the "3mm Rule," a displacement greater than 3 mm between the mid-sagittal lines of the femur and tibia indicates pathologic subluxation. Since the tibia is displaced anteriorly relative to the femur, this is defined as anterior subluxation. Option C is incorrect because the displacement is anterior, not posterior.
Question 10
A surgeon is performing a sagittal plane Malalignment Test (MAT) on a patient with a suspected deformity. A long lateral radiograph is taken with the knee in maximum passive extension. The test is positive for flexion malalignment. What does this finding signify?
View Answer & Explanation
Correct Answer: B
Rationale: Flexion malalignment is defined as a state where the sagittal mechanical axis fails to pass anterior to the knee's center of rotation when the knee is in maximum extension. This indicates that the passive knee locking mechanism is compromised. Option A describes normal alignment. Option C defines extension malalignment.
Question 11
An orthopedic resident is evaluating a patient with a significant distal femoral procurvatum deformity. The standing lateral radiograph, however, shows a relatively normal overall limb alignment. Why is the sagittal Malalignment Test (MAT) often considered misleading in such cases?
View Answer & Explanation
Correct Answer: B
Rationale: The primary limitation of the sagittal MAT is that the hip, knee, and ankle can move to compensate for a bony deformity. A patient with femoral procurvatum can hyperextend their knee, and a patient with tibial recurvatum can flex their knee, making the overall limb alignment appear normal on a static standing radiograph and hiding the true malalignment. This is why the Malorientation Test (MOT) is necessary.
Question 12
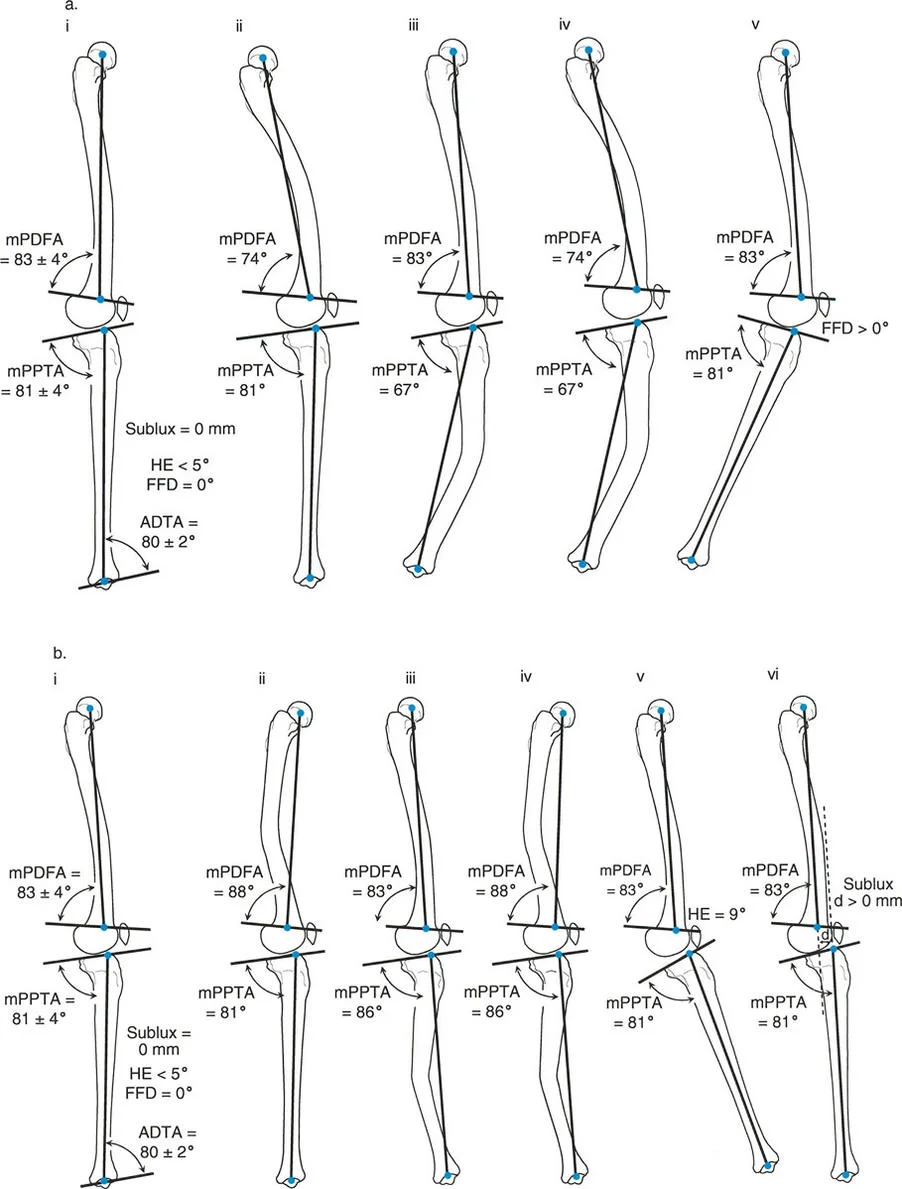
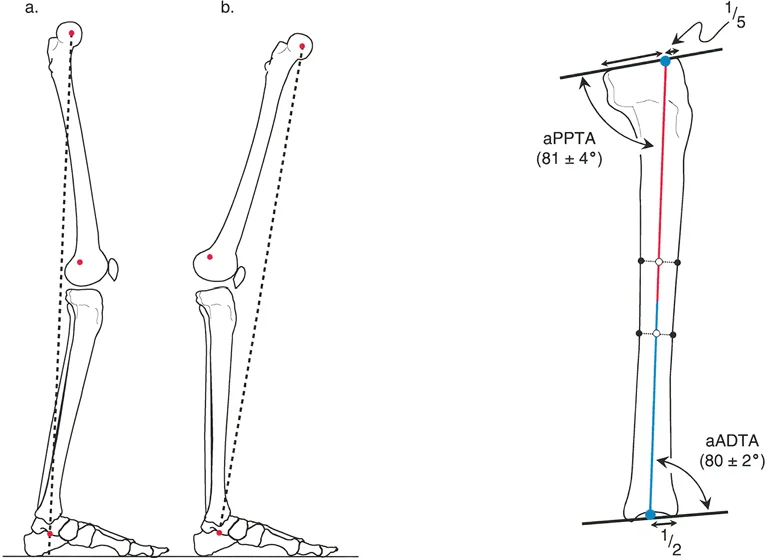
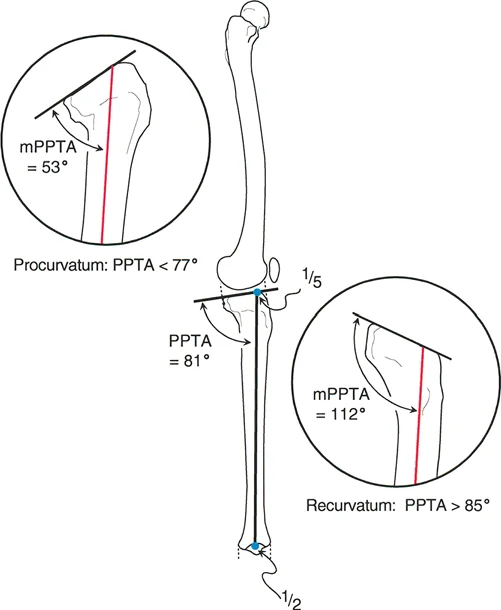
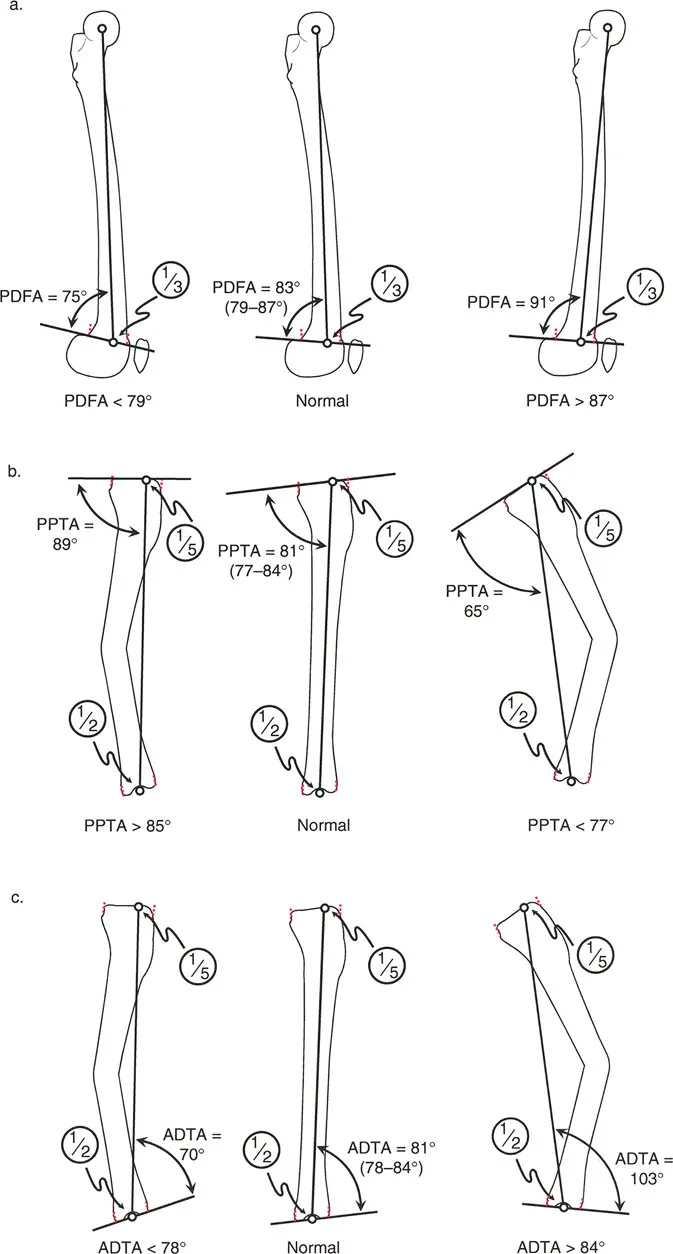
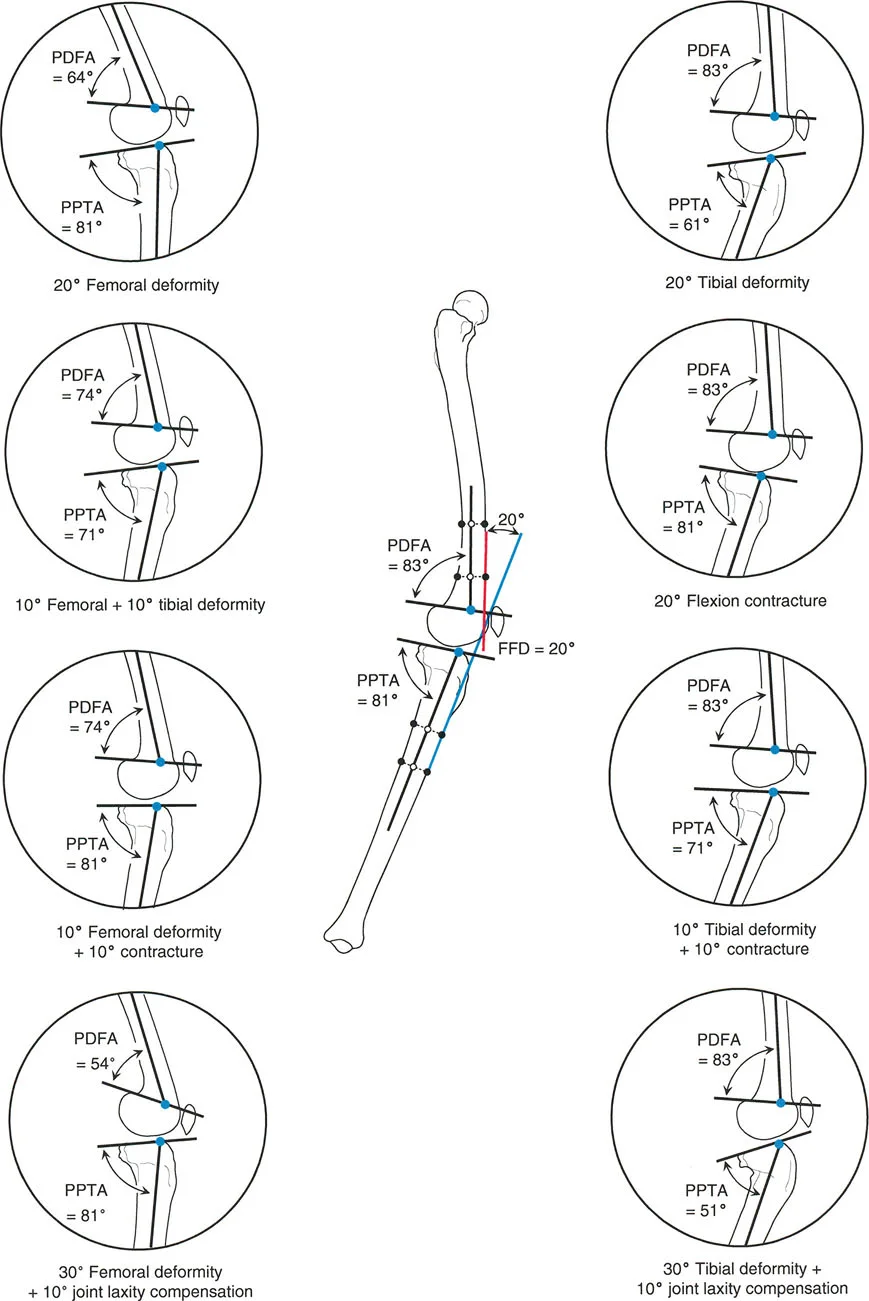
When performing a sagittal plane Malorientation Test (MOT) of the proximal tibia, the anatomic posterior proximal tibial angle (aPPTA) is measured. What is the normal range for this angle?
View Answer & Explanation
Correct Answer: B
Rationale: The normal value for the anatomic posterior proximal tibial angle (aPPTA) is 81° ± 4°. This angle measures the posterior slope of the tibial plateau relative to the tibial anatomic axis. Option C is the normal value for the aPDFA (distal femur).
Question 13
A surgeon is evaluating a lateral radiograph of a distal femur to assess for sagittal plane deformity. The anatomic posterior distal femoral angle (aPDFA) is measured. What is the normal value for this angle?
View Answer & Explanation
Correct Answer: C
Rationale: The normal value for the anatomic posterior distal femoral angle (aPDFA) is 83° ± 4°. This angle is measured between the sagittal distal femoral joint line and the mid-diaphyseal line of the distal femur. Option A is the normal aADTA, and Option B is the normal aPPTA.
Question 14
A 22-year-old patient has a healed tibial fracture with a suspected sagittal plane deformity. A Malorientation Test (MOT) is performed. The measured anatomic posterior proximal tibial angle (aPPTA) is 72°. What does this measurement indicate?
View Answer & Explanation
Correct Answer: B
Rationale: The normal aPPTA is 81° ± 4° (range 77°-85°). A value of 72° is significantly less than the normal range. A decreased aPPTA signifies an increased posterior slope, which corresponds to a procurvatum (apex anterior) deformity. Option C would be indicated by an aPPTA greater than 85°.
Question 15
A 40-year-old male has a malunited distal femur fracture. On the lateral radiograph, his anatomic posterior distal femoral angle (aPDFA) is measured to be 92°. How is this deformity best described?
View Answer & Explanation
Correct Answer: B
Rationale: The normal aPDFA is 83° ± 4° (range 79°-87°). A value of 92° is significantly greater than the normal range. An increased aPDFA signifies a recurvatum (apex posterior) deformity of the distal femur. Option A would be indicated by an aPDFA less than 79°.
Question 16
A surgeon is performing an overall sagittal plane Malorientation Test (MOT) for the femur in a patient with a mid-shaft deformity. The modified posterior distal femoral angle (mPDFA) is measured to be 75°. What is the correct interpretation of this finding?
View Answer & Explanation
Correct Answer: B
Rationale: The threshold for overall femoral procurvatum using the modified mechanical axis is an mPDFA of less than 79°. Since the measured value is 75°, this indicates an overall procurvatum deformity of the femur. Recurvatum would be indicated by an mPDFA greater than 87°.
Question 17
An overall sagittal plane MOT of the tibia is performed on a patient with a complex post-traumatic deformity. The modified posterior proximal tibial angle (mPPTA) is calculated to be 90°. What does this value signify?
View Answer & Explanation
Correct Answer: C
Rationale: The threshold for overall tibial recurvatum using the modified mechanical axis is an mPPTA of greater than 85°. A value of 90° is well above this threshold, indicating an overall recurvatum (apex posterior) deformity of the tibia. Procurvatum would be indicated by an mPPTA less than 77°.
Question 18
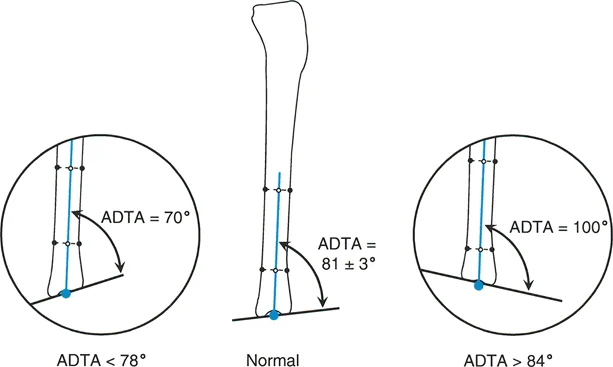
During a preoperative evaluation for a supramalleolar osteotomy, a surgeon measures the anatomic anterior distal tibial angle (aADTA) on a lateral radiograph. The measured angle is 75°. What deformity is present?
View Answer & Explanation
Correct Answer: B
Rationale: The normal aADTA is 80° ± 2° (range 78°-82°). A value less than 78° indicates a recurvatum (apex posterior) deformity of the distal tibia. A value of 75° falls into this category. Procurvatum would be indicated by an aADTA greater than 84°.
Question 19
According to Paley's 4-step protocol for sagittal deformity analysis, what is the first step in quantifying the clinical deformity?
View Answer & Explanation
Correct Answer: C
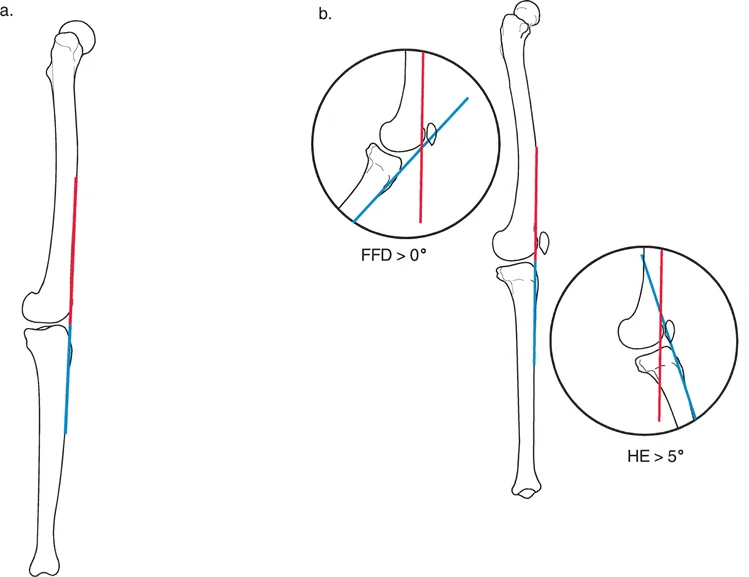
Rationale: Step 1 of the protocol is to measure the overall clinical deformity, which is the Fixed Flexion Deformity (FFD) or Hyperextension (HE). This is done by measuring the angle between the anterior cortical line of the distal femur and the anterior cortical line of the proximal tibia on a radiograph taken in maximal knee extension. While assessing for subluxation is important, it is not Step 1 of this specific 4-step protocol.
Question 20
A 30-year-old patient has a 20° fixed flexion deformity (FFD) on clinical exam. Radiographic analysis reveals a distal femoral procurvatum of 12° (aPDFA = 71°) and a proximal tibial procurvatum of 8° (aPPTA = 73°). Using Paley's reconciliation formula, what is the contribution of soft tissue to this deformity?
View Answer & Explanation
Correct Answer: C
Rationale: The formula is `Difference = FFD - (Total Bony Procurvatum) + (Total Bony Recurvatum)`. Total bony procurvatum is 12° (femur) + 8° (tibia) = 20°. The FFD is 20°. So, `Difference = 20 - 20 + 0 = 0`. A difference of 0 means the bony deformity exactly accounts for the clinical deformity, and there is no soft tissue contracture.
Question 21
A patient presents with a clinical 30° fixed flexion deformity (FFD). The sagittal MOT reveals a 15° femoral procurvatum and a 5° tibial procurvatum. There is no recurvatum deformity. Based on the 4-step reconciliation protocol, what is the underlying soft tissue pathology?
View Answer & Explanation
Correct Answer: B
Rationale: Total bony procurvatum = 15° + 5° = 20°. The clinical FFD is 30°. Using the formula `Difference = FFD - (Total Bony Procurvatum)`, we get `Difference = 30 - 20 = 10`. A positive difference (> 0) indicates that the bony deformity does not fully account for the FFD, meaning a soft tissue knee flexion contracture of 10° is also present.
Question 22
A 42-year-old male has a clinical fixed flexion deformity (FFD) of 10°. Radiographic analysis shows a 15° distal femoral procurvatum and a 5° proximal tibial procurvatum. What is the correct interpretation of these findings?
View Answer & Explanation
Correct Answer: D
Rationale: Total bony procurvatum = 15° + 5° = 20°. The clinical FFD is only 10°. Using the formula `Difference = FFD - (Total Bony Procurvatum)`, we get `Difference = 10 - 20 = -10`. A negative difference (< 0) means there is more bony deformity than clinical deformity. This is only possible if the patient has compensatory knee joint hyperextension laxity (in this case, 10°) that is masking the full extent of the bony problem.
Question 23
A patient is evaluated for knee hyperextension (HE) of 15°. The sagittal MOT shows a 10° femoral recurvatum and a 5° tibial recurvatum. There is no procurvatum. What is the soft tissue contribution to this deformity?
View Answer & Explanation
Correct Answer: E
Rationale: The formula for HE is `Difference = HE - (Total Bony Recurvatum) + (Total Bony Procurvatum)`. Total bony recurvatum = 10° + 5° = 15°. The clinical HE is 15°. So, `Difference = 15 - 15 + 0 = 0`. A difference of 0 indicates that the bony recurvatum exactly accounts for the clinical hyperextension, with no additional soft tissue pathology.
Question 24
A 25-year-old patient has a clinical knee hyperextension (HE) of 20°. Radiographic analysis reveals a total bony recurvatum of 12° and no procurvatum. According to Paley's reconciliation protocol, what is the soft tissue diagnosis?
View Answer & Explanation
Correct Answer: B
Rationale: Using the formula `Difference = HE - (Total Bony Recurvatum)`, we get `Difference = 20 - 12 = 8`. A positive difference (> 0) in the context of hyperextension indicates that the bony deformity does not fully account for the clinical HE. Therefore, pathologic soft tissue knee hyperextension laxity of 8° must be present.
Question 25
A 55-year-old male undergoes gait analysis for progressive right knee pain. At a normal walking speed, the analysis reveals that the time from his right heel strike to the subsequent right heel strike is 1.0 second. What is the approximate duration of the stance phase for his right leg?
View Answer & Explanation
Correct Answer: D
Rationale: The stance phase constitutes approximately 62% of a normal gait cycle. Therefore, for a 1.0-second gait cycle, the stance phase would be 0.62 seconds. The swing phase would be 0.38 seconds (B), which is the primary distractor.
Question 26
A 30-year-old runner is evaluated for anterior shin pain. Physical examination reveals weakness of the tibialis anterior muscle. Dysfunction of this muscle would most directly impair which phase of the gait cycle?

View Answer & Explanation
Correct Answer: A
Rationale: The first (heel) rocker involves controlled plantarflexion of the foot after heel strike, which is mediated by the eccentric contraction of the tibialis anterior. Weakness leads to an uncontrolled "foot slap." The third rocker (C) is primarily powered by the gastroc-soleus complex.
Question 27
A 62-year-old female with severe ankle arthritis presents for evaluation. Her gait is characterized by an inability to advance her tibia over her planted foot. To maintain forward progression, she forcefully drives her ipsilateral knee into hyperextension during mid-stance. This compensatory pattern indicates a failure of which rocker mechanism?
View Answer & Explanation
Correct Answer: B
Rationale: The second (ankle) rocker is responsible for the forward progression of the tibia over the talus. When this is blocked (e.g., by arthritis or deformity), the body compensates by creating a recurvatum thrust at the knee. Failure of the third rocker (C) would impair push-off.
Question 28
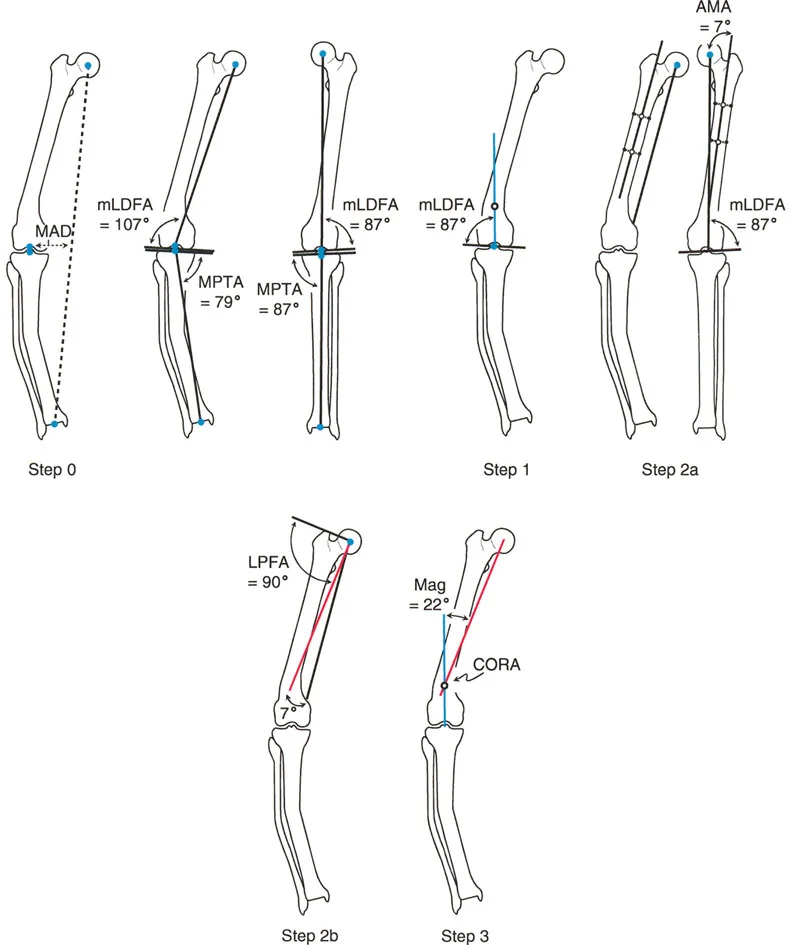
A surgeon is planning a distal femoral osteotomy for a 45-year-old male with a valgus deformity. Preoperative planning on a full-length standing radiograph shows the line from the center of the femoral head to the center of the ankle passes 25 mm lateral to the center of the knee. This measurement is defined as the:
View Answer & Explanation
Correct Answer: B
Rationale: Mechanical Axis Deviation (MAD) is the perpendicular distance from the center of the knee to the mechanical axis of the lower extremity. A lateral MAD indicates a valgus deformity. The mLDFA (D) is an angle measuring joint orientation, not overall limb alignment.
Question 29
A 58-year-old female presents with medial-sided knee pain and a varus deformity. A standing radiograph demonstrates that the mechanical axis passes medial to the knee center. This alignment creates which pathological force across the knee during the single limb stance phase?
View Answer & Explanation
Correct Answer: B
Rationale: In a varus deformity, the ground reaction force passes medial to the knee's center of rotation, creating an adduction moment that overloads the medial compartment. An abduction moment (A) is seen in valgus deformities.
Question 30
A 25-year-old patient has a 20-degree procurvatum deformity of the distal tibia. To achieve a plantigrade foot for standing, the patient must sacrifice motion at the adjacent ankle joint. What is the specific motion that is consumed by this compensation?

View Answer & Explanation
Correct Answer: B
Rationale: A procurvatum (anterior bow) of the tibia tilts the ankle plafond anteriorly. To bring the foot flat to the ground, the ankle joint must dorsiflex by an amount equal to the deformity (20 degrees). This motion is therefore consumed before gait even begins. Plantarflexion (A) would be consumed by a recurvatum deformity.
Question 31
During preoperative planning for a tibial osteotomy, the surgeon identifies the point where the proximal mechanical axis intersects the distal mechanical axis. According to Paley's principles, what is this critical point called?
View Answer & Explanation
Correct Answer: C
Rationale: The Center of Rotation of Angulation (CORA) is the geometric epicenter of a bone deformity, defined as the intersection of the proximal and distal mechanical axis lines. The MAD (A) is a measure of overall limb alignment, not the location of the deformity itself.
Question 32
A surgeon performs a proximal tibial osteotomy for a varus deformity. The osteotomy and the hinge of correction are both placed precisely at the CORA. According to Paley's osteotomy rules, what is the expected outcome?
View Answer & Explanation
Correct Answer: A
Rationale: Paley's Rule 1 states that when the osteotomy and hinge are at the CORA, pure angular correction is achieved. The bone ends angulate without translating. If the osteotomy is performed away from the CORA (B), translation will occur.
Question 33
A 19-year-old male with a history of a malunited clubfoot deformity presents with a limp. His gait is characterized by a long step with his affected leg and a noticeably short, hurried step with his normal, contralateral leg. This gait asymmetry is most directly caused by:
View Answer & Explanation
Correct Answer: C
Rationale: The length of the swing phase of the normal leg is determined by the duration of the terminal stance phase of the affected leg. A blocked ankle rocker on the affected side cuts this phase short, which in turn truncates the swing phase of the contralateral leg, resulting in a short step.
Question 34
A 65-year-old female has a severe valgus deformity of her left knee. Radiographic analysis reveals a Mechanical Lateral Distal Femoral Angle (mLDFA) of 78 degrees. What is the normal range for this angle?
View Answer & Explanation
Correct Answer: C
Rationale: The normal mLDFA is approximately 87 degrees, with a typical range of 85 to 90 degrees. A value of 78 degrees represents significant femoral valgus, contributing to the overall limb malalignment.
Question 35
A 40-year-old male is evaluated for a painful varus ankle. His radiographs show a Mechanical Lateral Distal Tibial Angle (mLDTA) of 80 degrees. How does this malorientation primarily affect his gait?
View Answer & Explanation
Correct Answer: B
Rationale: The normal mLDTA is 89 degrees (range 86-92). A decreased angle (varus) orients the ankle plafond such that the patient bears weight on the lateral aspect of the foot, disrupting all three rocker mechanisms. While it contributes to overall limb malalignment, its most direct effect is on foot posture during stance.
Question 36
A gait analysis is performed on a healthy 28-year-old. The period when both feet are in contact with the ground simultaneously during weight transfer is measured. According to normative data, what percentage of the total gait cycle does one of these "double stance support" periods occupy?

View Answer & Explanation
Correct Answer: A
Rationale: The gait cycle contains two periods of double stance support, one at the beginning and one at the end of the stance phase. Each of these periods lasts for approximately 12% of the total gait cycle. 38% (C) is the duration of single limb stance or the entire swing phase.
Question 37
A 50-year-old patient with limited ankle motion due to a previous pilon fracture requires a minimum of 10 degrees of ankle dorsiflexion for normal gait. This motion is biomechanically essential for the successful completion of which rocker mechanism?
View Answer & Explanation
Correct Answer: B
Rationale: The second (ankle) rocker requires a minimum of 10 degrees of ankle dorsiflexion to allow the tibia to advance smoothly over the fixed, plantigrade foot. Insufficient dorsiflexion blocks this critical phase of forward progression.
Question 38
A 60-year-old male with a valgus knee deformity is shown in the clinical image. This alignment results in an overload of the lateral compartment of the knee. This pathological loading is caused by which of the following biomechanical forces?

View Answer & Explanation
Correct Answer: B
Rationale: The image shows a varus deformity, not valgus. However, the question asks about a valgus deformity. A valgus deformity is characterized by a mechanical axis that passes lateral to the knee center (lateral MAD). This creates an abduction moment, which overloads the lateral compartment and stretches the medial collateral ligament. An adduction moment (A) is seen in varus deformities.
Question 39
A surgeon plans a tibial osteotomy but places the osteotomy and the corrective hinge 3 cm distal to the CORA. To avoid creating a secondary deformity, what additional surgical maneuver must be performed?
View Answer & Explanation
Correct Answer: D
Rationale: According to Paley's Rule 3, if both the osteotomy and hinge are placed away from the CORA, a secondary translation deformity is created. To achieve proper alignment of the mechanical axis and joint lines, this translation must be calculated and intentionally performed as part of the correction.
Question 40
A 22-year-old female presents with posterior knee pain and instability. Her clinical gait is shown in the image. This gait pattern is a classic secondary compensation for a primary pathology that has exhausted motion at which joint?

View Answer & Explanation
Correct Answer: B
Rationale: The image displays a genu recurvatum (hyperextension) thrust during stance. This is a pathognomonic compensatory mechanism for a blocked second (ankle) rocker, where the ankle lacks sufficient dorsiflexion to allow the tibia to advance. The force is transmitted proximally, causing the knee to hyperextend.
Question 41
A 48-year-old male has a varus deformity primarily located in his proximal tibia. Preoperative radiographic assessment reveals a Mechanical Proximal Tibial Angle (MPTA) of 78 degrees. What is the average normal value for the MPTA?
View Answer & Explanation
Correct Answer: C
Rationale: The average normal MPTA is 87 degrees, with a range of 85-90 degrees. A value of 78 degrees indicates significant tibial varus, which is a primary driver of knee malalignment and medial compartment overload.
Question 42
The powerful, explosive push-off that initiates the swing phase is the primary function of which rocker mechanism and is powered mainly by which muscle group?
View Answer & Explanation
Correct Answer: C
Rationale: The third (forefoot) rocker occurs during terminal stance and involves the heel lifting off the ground as weight rolls onto the metatarsal heads. This is powered by a strong concentric contraction of the gastroc-soleus complex, providing propulsion. The first rocker (A) is controlled by the tibialis anterior.
Question 43
A 60-year-old patient with knee osteoarthritis has a standing radiograph showing that the femoral and tibial articular surfaces are not parallel, with the joint space widened laterally. The angle between the tangent to the femoral condyles and the tangent to the tibial plateau measures 5 degrees. This measurement defines the:
View Answer & Explanation
Correct Answer: E
Rationale: The Joint Line Congruency Angle (JLCA) measures intra-articular deformity or ligamentous laxity. A normal JLCA is 0-2 degrees. An increased value, as in this case, indicates joint instability or incongruity, which can contribute to a "wobble" during gait.
Question 44
The fundamental objective of lower extremity deformity correction is to restore normal biomechanics. For physiological gait, the articular surfaces of the hip, knee, and ankle should be oriented in what way relative to the ground during the single-limb stance phase?
View Answer & Explanation
Correct Answer: B
Rationale: A key principle of deformity correction is restoring normal joint orientation. During the single-limb stance phase, the joint surfaces of the hip, knee, and ankle must be parallel to the ground to ensure even load distribution and smooth kinematic function.
Question 45
A 35-year-old male has a 15-degree procurvatum deformity of the distal tibia. He complains of anterior ankle pain, especially when trying to walk uphill. The physical "hard stop" to his compensatory ankle dorsiflexion is caused by impingement between which two structures?
View Answer & Explanation
Correct Answer: C
Rationale: In compensating for a procurvatum deformity, the ankle is forced into extreme dorsiflexion. The anatomical limit of this motion is reached when the anterior lip of the distal tibial articular surface physically impacts the neck of the talus, causing anterior osseous impingement.
Question 46
A surgeon performs an osteotomy for a tibial deformity at a level different from the CORA, but places the hinge of correction at the CORA. According to Paley's Rule 2, what will be the result at the osteotomy site?
View Answer & Explanation
Correct Answer: B
Rationale: Paley's Rule 2 states that if the osteotomy is not at the CORA but the hinge is, the overall mechanical axis will be corrected, but this will be accompanied by a translation of the bone fragments at the osteotomy site. Rule 1 (A) applies when both are at the CORA.
Question 47
A 58-year-old male presents with progressive right knee pain and a noticeable "bow-legged" appearance. A full-length standing radiograph demonstrates a significant medial Mechanical Axis Deviation (MAD). According to the principles of deformity correction, what is the primary biomechanical consequence of this finding?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that a medial MAD (varus deformity) overloads the medial compartment, exponentially increasing joint reactive forces and accelerating osteoarthritis. Lateral compartment overload (A) would occur in a valgus deformity. Medial collateral ligament attenuation (B) is associated with valgus, not varus.
Question 48
A 65-year-old female undergoes a total knee arthroplasty (TKA). Postoperatively, she has persistent medial knee pain. Radiographs reveal a well-fixed TKA but a previously unrecognized 15-degree varus deformity in the distal femur. Failure to correct this extra-articular deformity most commonly leads to which complication?
View Answer & Explanation
Correct Answer: B
Rationale: The provided text highlights that failing to correct extra-articular frontal plane deformities in the context of TKA leads to eccentric loading and early catastrophic failure of the polyethylene liner. While aseptic loosening (A) can occur, liner failure due to point loading is the more direct and common consequence.
Question 49
An orthopedic resident is learning to perform preoperative planning for a limb deformity. They are asked to define the mechanical axis of the lower limb. Which of the following descriptions is the most accurate?
View Answer & Explanation
Correct Answer: B
Rationale: The text defines the mechanical axis of the lower limb as "a straight line drawn from the center of the femoral head to the center of the ankle joint." The line down the medullary canal (A) describes the anatomic axis.
Question 50
A 45-year-old patient with a post-traumatic malunion of the tibia is being evaluated. On a full-length standing radiograph, the line from the femoral head to the ankle center passes 30 mm medial to the center of the knee. What is the correct term for this finding?
View Answer & Explanation
Correct Answer: D
Rationale: The deviation of the mechanical axis from the center of the knee joint is defined as Mechanical Axis Deviation (MAD). In this case, it is a 30 mm medial MAD, indicating a varus deformity.
Question 51
A 22-year-old female presents with lateral knee pain and instability. Her clinical examination and radiographs are consistent with a significant valgus deformity of the lower limb. Chronic malalignment in this pattern leads to progressive strain and attenuation of which structure?
View Answer & Explanation
Correct Answer: A
Rationale: The text states that chronic malalignment stretches collateral ligaments. In a valgus ("knock-kneed") deformity, the medial side of the joint is under tension, leading to stretching and attenuation of the medial collateral ligament. The lateral collateral ligament (B) would be under strain in a varus deformity.
Question 52
A 19-year-old with a history of metabolic bone disease has a long, sweeping varus bow of his femur. During preoperative planning (Step 3 of the Paley method), the surgeon draws a single proximal anatomic axis line and a single distal anatomic axis line. They do not accurately represent the curvature of the bone. What does this indicate?
View Answer & Explanation
Correct Answer: B
Rationale: The text explains that if a single proximal and distal line do not accurately capture the bone's curvature, the deformity is multiapical. This requires drawing additional mid-diaphyseal lines to identify multiple CORAs.
Question 53
A surgeon is planning a correction for a femoral deformity as shown in the image. A proximal axis line and a distal axis line have been drawn to represent the two main segments of the bone.
The point where these two lines intersect is best defined as the:
View Answer & Explanation
Correct Answer: A
Rationale: According to the Paley method, the intersection of the proximal and distal axis lines of a deformed bone segment defines the Center of Rotation of Angulation (CORA), which is the apex of the deformity.
Question 54
A 30-year-old patient has a complex tibial deformity, and the preoperative plan is shown in the image. The plan involves two separate osteotomies.
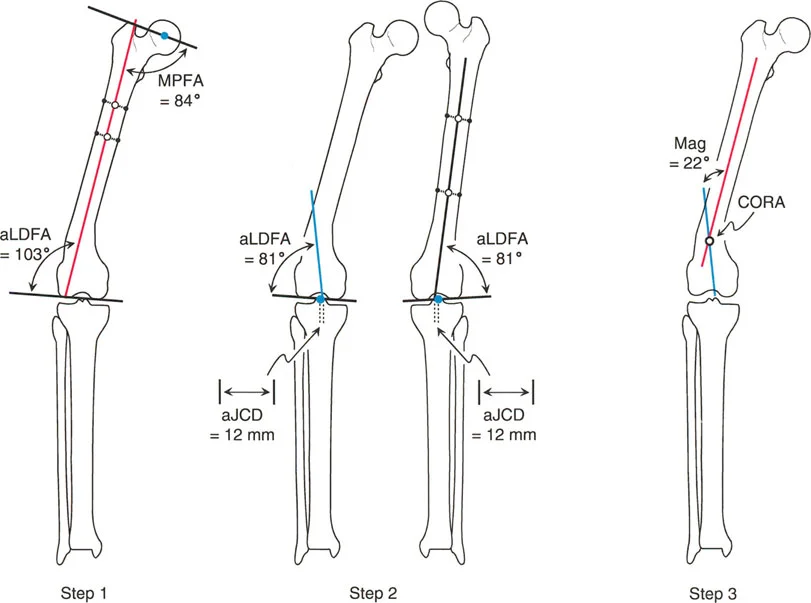
What is the most likely reason for planning two osteotomies instead of one?
View Answer & Explanation
Correct Answer: B
Rationale: The image and text describe a multiapical deformity. Attempting to correct a multiapical deformity with a single osteotomy would induce a large, unacceptable translation. Therefore, each apex (CORA) must be corrected with its own osteotomy.
Question 55
A surgeon misinterprets a multiapical femoral varus deformity as uniapical. They perform a single, large angular correction at the distal CORA only. What is the most predictable iatrogenic consequence of this action?
View Answer & Explanation
Correct Answer: B
Rationale: The text warns that attempting to correct a multiapical deformity with a single osteotomy will result in a massive translation, creating an unacceptable "zig-zag" appearance and pulling the bone out of the soft tissue envelope.
Question 56
During deformity planning for a tibia with a complex bow, a surgeon draws a proximal anatomic axis line, a distal anatomic axis line, and one additional mid-diaphyseal anatomic axis line to accurately map the bone's shape. According to the "Rule of Intersecting Lines," how many CORAs and magnitudes of angulation will be identified?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "For each additional anatomic axis line drawn, there will be one additional CORA and magnitude." Starting with a proximal and distal line (one CORA), adding one mid-diaphyseal line creates a second intersection point, resulting in a total of two CORAs.
Question 57
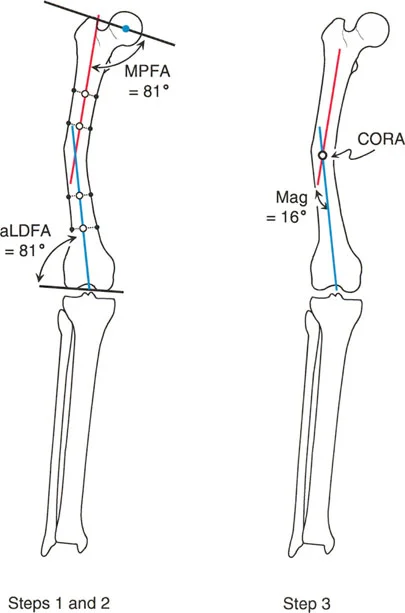
A surgeon is performing preoperative planning for a femoral osteotomy. They note that the line representing the center of the medullary canal and the line from the femoral head center to the knee center are not parallel. What is the term for the angle of divergence between these two lines?
View Answer & Explanation
Correct Answer: C
Rationale: The text defines the divergence between the anatomic axis (medullary canal) and the mechanical axis (head center to knee center) in the femur as the Anatomic-Mechanical Angle (AMA), which is typically around 7 degrees.
Question 58
When performing frontal plane deformity planning for the tibia, what is the typical relationship between the anatomic axis and the mechanical axis?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that in the tibia, the anatomic and mechanical axes are "essentially parallel (usually only 0 to 1 degree of difference)." This is in stark contrast to the femur, where they diverge significantly.
Question 59
A surgeon is comparing the CORA derived from mechanical axis planning versus anatomic axis planning for a femoral deformity. In which region of the femur will the locations of the mechanical CORA and anatomic CORA be the farthest apart?
View Answer & Explanation
Correct Answer: E
Rationale: The text explains that in the proximal femur, the mechanical and anatomic axes diverge the most. Consequently, the CORAs derived from the two methods will be the farthest apart in this region.
Question 60
In the provided image, a surgeon is analyzing the intersection of proximal and distal axis lines for a femoral deformity. A dotted line is shown cutting the angle of deformity exactly in half.
According to Paley's principles, what does this dotted line represent?
View Answer & Explanation
Correct Answer: C
Rationale: The image and text identify the line that cuts the angle of deformity in half as the bisector line. This line is critical because it defines the true transverse level of the angulation and is the key to planning osteotomies that are not located at the CORA.
Question 61
During preoperative planning for a distal femoral varus deformity, a surgeon identifies both the mechanical CORA and the anatomic CORA, which are in slightly different locations. To determine the true transverse level of the angulation for planning the osteotomy, which geometric construct should be prioritized?
View Answer & Explanation
Correct Answer: C
Rationale: The text emphasizes that "it is the bisector line of the deformity—not any individual CORA point—that defines the true transverse level of the angulation." This principle is fundamental to accurate osteotomy placement, especially when the cut is not at the CORA.
Question 62
A 40-year-old male has a 20-degree varus deformity in his distal femur. A surgeon is deciding between mechanical and anatomic axis planning. According to the provided text, what is the relationship between the bisector lines generated by these two methods for a distal femoral deformity?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "In distal femoral deformities, the difference between the mechanical and anatomic bisector lines is negligible." This means either method can be used to accurately identify the level of the CORA in this location.
Question 63
A 35-year-old patient requires a corrective osteotomy for a femoral malunion. The surgeon plans to use a locked intramedullary nail for fixation. Which method of preoperative planning is most advantageous in this scenario?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly notes that anatomic axis planning is easier or superior when using an intramedullary nail, as the nail must traverse the anatomic medullary canal. The anatomic axis dictates the path of the reamer and implant.
Question 64
An orthopedic surgeon is teaching a resident the principles of mechanical axis planning for a femoral deformity. How is the Mechanical CORA correctly defined?
View Answer & Explanation
Correct Answer: B
Rationale: The text provides a clear definition: "Mechanical CORA: Defined by the intersection of the Proximal Mechanical Axis (PMA) and the Distal Mechanical Axis (DMA)." The intersection of anatomic axes (A) defines the Anatomic CORA.
Question 65
A 15-year-old male with a history of a malunited proximal femur fracture presents with a limp and knee pain. On examination, a line drawn from the center of his femoral head to the center of his ankle joint passes 25 mm medial to the center of his knee. What does this line represent?
View Answer & Explanation
Correct Answer: B
Rationale: The text defines the mechanical axis as a straight line from the center of the femoral head to the center of the ankle joint. The anatomic axis (A) follows the intramedullary canal of the bone, which is incorrect. The other options are specific angles, not the primary load-bearing line.
Question 66
A 45-year-old female presents with progressive right knee pain. Radiographs reveal a significant proximal femoral varus deformity. Her mechanical axis is found to pass 30 mm medial to the knee center. What is the correct term for this finding?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that a structural deformity in the proximal femur creates a Mechanical Axis Deviation (MAD) by shifting the spatial position of the femoral head. In a normal limb, the axis passes just medial to the knee center (physiologic valgus), but a 30 mm deviation is pathologic MAD.
Question 67
A surgeon is evaluating a standing, full-length radiograph of a healthy 25-year-old athlete with no complaints. In a normally aligned lower limb, where should the mechanical axis pass relative to the center of the knee joint?
View Answer & Explanation
Correct Answer: C
Rationale: The guide explicitly states that in a perfectly aligned limb, the mechanical axis passes "just medial to the center of the knee joint (typically 8 ± 7 mm medial to the center), creating a slight, physiologic valgus alignment." A lateral deviation (D) would represent a pathologic varus limb alignment.
Question 68
A 12-year-old with developmental coxa vara presents for evaluation. Radiographs confirm a neck-shaft angle of 105°. According to the provided text, what is the primary biomechanical consequence of this deformity on the knee joint?
View Answer & Explanation
Correct Answer: D
Rationale: The text clearly explains that in coxa vara, the mechanical axis shifts medially, resulting in a varus alignment of the entire limb. This "exponentially increasing the contact forces and load on the medial compartment of the knee," leading to medial compartment osteoarthritis. A lateral shift (E) is characteristic of coxa valga.
Question 69
A 50-year-old patient with a history of untreated coxa vara now has severe medial-sided knee pain and imaging consistent with advanced osteoarthritis. This clinical scenario is a direct result of which biomechanical principle?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that coxa vara shifts the overall mechanical axis of the limb medially, leading to a varus alignment and subsequent medial compartment knee failure. A laterally deviated axis (A) is associated with coxa valga. While JLCA may increase as a result, the primary cause is the medial MAD.
Question 70
A 16-year-old female with cerebral palsy has developed bilateral coxa valga with neck-shaft angles of 150°. She now complains of lateral knee pain. What is the expected finding on a full-length standing radiograph?
View Answer & Explanation
Correct Answer: C
Rationale: The guide specifies that in coxa valga, the femoral head moves superiorly and laterally, which "shifts the mechanical axis laterally." This results in a valgus alignment (knock-kneed appearance) and overloads the lateral compartment of the knee. A medial shift (A) is seen in coxa vara.
Question 71
A patient with long-standing, uncorrected coxa valga is being evaluated. Which of the following is a direct biomechanical consequence of this deformity?
View Answer & Explanation
Correct Answer: A
Rationale: The text states that coxa valga results in a valgus alignment of the limb, "pathologically overloading the lateral compartment of the knee and stretching the medial collateral ligament (MCL)." It does not increase compressive forces on the MCL (B); it places it under tension.
Question 72
A surgeon is planning a proximal femoral osteotomy for a 19-year-old with a complex deformity. The surgeon measures the angle between the femoral head/neck complex and the true mechanical axis of the femur. What is this cornerstone angle called?
View Answer & Explanation
Correct Answer: C
Rationale: The mLPFA is explicitly defined in the text as "the absolute cornerstone angle of hip deformity planning" and represents the relationship between the femoral head/neck complex and the true mechanical axis of the femur. The NSA (A) relates to the anatomic axis and can be misleading.
Question 73
A preoperative radiograph of a 30-year-old male shows a Mechanical Lateral Proximal Femoral Angle (mLPFA) of 75°. What does this value indicate?
View Answer & Explanation
Correct Answer: C
Rationale: The provided table states the normal range for mLPFA is 85-95°. It specifies that "a value below 85° indicates a varus deformity." A value above 95° would indicate a valgus deformity (B).
Question 74
During preoperative planning for a patient with a severe diaphyseal femur deformity, the surgeon is unable to accurately draw the mechanical axis. Which angle serves as the most vital fallback measurement in this scenario?
View Answer & Explanation
Correct Answer: B
Rationale: The text highlights the aMPFA as a "vital fallback measurement when severe diaphyseal deformity makes the true mechanical axis difficult or impossible to draw accurately" because it relates the head/neck to the more reliable anatomic axis (intramedullary canal).
Question 75
A resident is measuring angles on a proximal femur radiograph. They measure the angle between the femoral head/neck complex and the anatomic axis of the proximal femur. What is the normal range for this angle?
View Answer & Explanation
Correct Answer: E
Rationale: The angle described is the Anatomic Medial Proximal Femoral Angle (aMPFA). The table lists its normal range as 80-89°. The range 85-95° (A) is for the mLPFA, and 124-136° (B) is for the NSA.
Question 76
A 40-year-old patient has a post-traumatic deformity of the hip. The surgeon notes that the Neck Shaft Angle (NSA) appears normal at 130°, but the mLPFA is pathologically low. Why is the mLPFA considered biomechanically more important than the NSA for complex deformity planning?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that the NSA "can be highly misleading in complex deformity planning because it fails to account for the femur's natural anterior bow and lateral sweep." The mLPFA is superior because it relates directly to the true load-bearing mechanical axis.
Question 77
A 22-year-old female presents with a painful, non-weightbearing gait. On examination, she has a profound Trendelenburg gait. Radiographs show that the tip of her greater trochanter is 5 mm superior to the center of the femoral head. Which measurement is abnormal?
View Answer & Explanation
Correct Answer: D
Rationale: The Articulo Trochanteric Distance (ATD) is the vertical distance between the trochanteric tip and the femoral head center. The text states a decreased or negative ATD (trochanter higher than the head) "dramatically shortens the abductor lever arm," leading to abductor weakness and a Trendelenburg gait.
Question 78
During surgical planning for a valgus intertrochanteric osteotomy, the surgeon aims to restore a normal abductor lever arm. What is the target normal range for the Articulo Trochanteric Distance (ATD)?
View Answer & Explanation
Correct Answer: D
Rationale: The table of joint orientation angles clearly lists the normal range for the Articulo Trochanteric Distance (ATD) as 10-25 mm. This distance is critical for proper abductor muscle function.
Question 79
A 55-year-old male with a proximal femoral varus deformity is being evaluated. Standing radiographs show that the angle between the distal femoral joint line and the proximal tibial joint line is 6°. What does this measurement represent?
View Answer & Explanation
Correct Answer: C
Rationale: The Joint Line Convergence Angle (JLCA) is the angle between the knee joint lines. A value of 6° is abnormal (normal is 0-2°) and, as the text explains, "strongly indicates that the knee has developed secondary ligamentous laxity or asymmetric cartilage wear as a compensatory mechanism."
Question 80
A surgeon is planning a proximal femoral osteotomy to correct a valgus deformity. Preoperative assessment reveals a Joint Line Convergence Angle (JLCA) of 8°. What is the clinical significance of this finding?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that a large JLCA in the presence of a proximal femoral deformity indicates secondary compensatory changes in the knee (ligamentous laxity or cartilage wear). This "may necessitate a concurrent or staged knee surgery." It is not a contraindication (D) but a critical factor in overall limb reconstruction planning.
Question 81
A resident is learning the Paley methodology for deformity correction. How is the Center of Rotation of Angulation (CORA) geometrically defined?
View Answer & Explanation
Correct Answer: B
Rationale: The guide provides a precise definition: "The CORA is defined as the geometric apex of the deformity. It is the specific point... where the normal proximal axis of the bone intersects the abnormal distal axis of the bone." The other options describe different anatomical or surgical landmarks.
Question 82
When planning a correction for a complex, multi-planar proximal femoral deformity, how is the coronal plane CORA located on a radiograph?
View Answer & Explanation
Correct Answer: C
Rationale: The text gives a specific graphical method: "you find the coronal plane CORA by drawing the normal proximal mechanical axis... and intersecting it with the mechanical axis of the distal femoral shaft." This process identifies the apex of the angular deformity in that plane.
Question 83
A surgeon is planning a closing wedge osteotomy for a femoral neck non-union where the CORA is located precisely within the planned osteotomy site in the mid-neck. The surgeon performs the cut and angulates the fragments around a hinge at the osteotomy site. Which of Paley's Osteotomy Rules is being applied?
View Answer & Explanation
Correct Answer: A
Rationale: Osteotomy Rule One is defined by performing the osteotomy exactly at the level of the CORA and angulating around an axis (ACA) that also passes through the CORA. This results in perfect realignment with pure angulation and no translation, as described in the vignette.
Question 84
A surgeon is performing a femoral neck osteotomy according to Paley's Rule One. What is the expected result if this rule is followed perfectly?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that when applying Rule One, "the deformity is completely corrected with pure angulation" and results in "perfect, seamless realignment... with absolutely no translation required." A combination of angulation and translation (B) is characteristic of Rule Two.
Question 85
Despite being the "anatomic ideal," why is an osteotomy performed at the CORA in the femoral neck (Rule One) rarely advisable in the proximal femur?
View Answer & Explanation
Correct Answer: D
Rationale: The guide is emphatic on this point, stating that the CORA is often in an intracapsular region with a tenuous blood supply. Performing an osteotomy there "carries an unacceptably high, often catastrophic risk of causing Avascular Necrosis (AVN) of the femoral head."
Question 86
A surgeon plans a valgus-producing intertrochanteric osteotomy to correct coxa vara. The CORA is located in the femoral head. The osteotomy is performed distally in the intertrochanteric region. To achieve a perfect correction of the mechanical axis, the axis of correction (ACA) must pass through which point?
View Answer & Explanation
Correct Answer: D
Rationale: This scenario describes Osteotomy Rule Two. The principle states that when the cut is different from the CORA, the ACA must still be designed to pass "through the CORA" to achieve perfect realignment. Placing the ACA at the osteotomy site (A) is the error described in Rule Three.
Question 87
A surgeon is performing a valgus intertrochanteric osteotomy for coxa vara, applying Paley's Rule Two. The osteotomy is performed distal to the CORA. What additional maneuver is mathematically required at the osteotomy site besides angulation?
View Answer & Explanation
Correct Answer: C
Rationale: The text explains that under Rule Two, correction requires both angulation and translation. It provides a specific example: "when performing a valgus-producing osteotomy to correct coxa vara, the distal shaft must be intentionally translated medially." Lateral translation (D) would worsen the mechanical axis deviation.
Question 88
A 10-year-old boy presents with progressively worsening bowlegs. On examination, he has significant genu varum. Radiographs confirm the deformity, and the mechanical axis passes medial to the knee. According to the Heuter-Volkmann law, what is the primary biological driver of this progressive deformity?
View Answer & Explanation
Correct Answer: A
Rationale: The Heuter-Volkmann law states that increased compression inhibits physeal growth. In genu varum, the mechanical axis shifts medially, increasing compressive forces on the medial physes of the distal femur and proximal tibia, which suppresses their growth and allows the deformity to worsen. Option C is incorrect because Wolff's law describes bone remodeling in response to altered stress, which is a secondary effect, not the primary driver of the physeal deformity progression.
Question 89
A 12-year-old girl undergoes successful guided growth for genu valgum. Over 18 months, her mechanical axis normalizes. Which biological principle is primarily responsible for the subsequent remodeling of the femoral and tibial metaphyses to align with the new, corrected mechanical axis?
View Answer & Explanation
Correct Answer: A
Rationale: Wolff's law states that bone adapts to the loads under which it is placed. As the mechanical axis is corrected, the stress patterns across the metaphysis and diaphysis change, leading to osteoclastic resorption and osteoblastic deposition that remodels the bone to the new, corrected alignment. The Heuter-Volkmann law (B) governs the physeal growth modulation that drives the initial angular correction, not the subsequent bone remodeling.
Question 90
A surgeon is evaluating a full-length, weight-bearing AP radiograph of a 9-year-old boy with knock-knees. To quantify the overall severity of the lower extremity malalignment, a line is drawn from the center of the femoral head to the center of the ankle mortise. What is this measurement called?
View Answer & Explanation
Correct Answer: A
Rationale: The Mechanical Axis Deviation (MAD) is the perpendicular distance from the mechanical axis line (femoral head center to ankle center) to the center of the knee joint. It is the single most important initial measurement for assessing overall lower extremity alignment. The other options are specific angles used to locate the source of the deformity (D) or define its apex (E).
Question 91
An 11-year-old girl presents with genu valgum. Her full-length radiograph shows a Mechanical Axis Deviation (MAD) of 30 mm lateral to the knee center. Measurement of her joint orientation angles reveals a mechanical Lateral Distal Femoral Angle (mLDFA) of 80°. The Medial Proximal Tibial Angle (MPTA) is 88°. What is the primary location of her deformity?
View Answer & Explanation
Correct Answer: A
Rationale: The normal mLDFA is 85°-90°. A decreased angle (<85°) indicates femur valgum. In this patient, the mLDFA of 80° is the source of the valgus deformity. The MPTA of 88° is within the normal range (85°-90°), ruling out the proximal tibia as the primary source.
Question 92
A 13-year-old boy has a varus deformity of his lower limb. Radiographic analysis shows a normal mLDFA of 87° but a Medial Proximal Tibial Angle (MPTA) of 80°. What is the correct interpretation of these findings?
View Answer & Explanation
Correct Answer: A
Rationale: The normal MPTA is 85°-90°. A decreased angle (<85°) indicates tibia vara. The patient's MPTA of 80° points to the proximal tibia as the source of the varus deformity. The mLDFA is normal, ruling out a femoral deformity.
Question 93
During preoperative planning for a developmental genu varum deformity in an 8-year-old, the surgeon identifies the intersection point of the proximal and distal mechanical axes of the tibia. What does this point represent?
View Answer & Explanation
Correct Answer: A
Rationale: The CORA is the geometric apex of the deformity, defined as the intersection of the proximal and distal mechanical axes of the deformed bone. In developmental deformities, the CORA is typically located at the physis, which is the ideal location for correction via guided growth.
Question 94
A 16-year-old female with nearly closed physes presents with a painful 20° genu valgum deformity. She has significant remaining growth predicted to be less than 0.5 cm. What is the most appropriate surgical treatment?
View Answer & Explanation
Correct Answer: A
Rationale: Guided growth (hemi-epiphysiodesis) is contraindicated in patients with closed or nearly closed physes as there is insufficient remaining growth to achieve correction. An osteotomy is the definitive treatment for significant angular deformities in skeletally mature or near-mature patients. Options B and C would be ineffective.
Question 95
A 7-year-old boy with idiopathic genu valgum is being considered for guided growth. His parents are concerned about the procedure being permanent. Which of the following is a key advantage of using modern tension-band plates or staples for hemi-epiphysiodesis?
View Answer & Explanation
Correct Answer: A
Rationale: A major advantage of modern guided growth with plates or staples is its reversibility. Once the desired correction is achieved, the hardware can be removed, and normal physeal growth typically resumes. This is in contrast to permanent techniques like the Phemister bone block epiphysiodesis. Correction is gradual, not instantaneous (B).
Question 96
A surgeon is planning a hemi-epiphysiodesis for a 9-year-old child. To accurately predict the remaining growth and properly time the intervention and subsequent hardware removal, which of the following is most critical?
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly states that surgical planning *must* be based on a skeletal age assessment to accurately predict remaining growth. Chronological age can be misleading as it does not always correlate with physiological maturity. The amount of remaining growth is the engine of correction, making its accurate prediction paramount.
Question 97
A 4-year-old child presents with a significant genu valgum deformity. The surgeon is hesitant to perform a hemi-epiphyseal stapling. What is the primary technical concern with performing this procedure in a very young child, as described in the text?
View Answer & Explanation
Correct Answer: A
Rationale: The text identifies a relative contraindication in very young children (<5 years) due to "technical difficulties in getting satisfactory staple fixation... because of the highly cartilaginous nature of the epiphysis, leading to pull-out." Modern evidence has shown the risk of permanent growth arrest (B) is low if implants are removed in a timely manner.
Question 98
A 12-year-old undergoes guided growth for a 15° femoral varus deformity. A follow-up radiograph 6 months later shows the tines of the staple have spread apart slightly. What is the clinical significance of this "tine spread"?
View Answer & Explanation
Correct Answer: A
Rationale: The text describes "tine spread" as evidence of the immense strain of growth (estimated at 450 psi) causing sub-failure yielding of the implant. This is a visual cue that the biological engine is working and applying corrective force, not necessarily a sign of failure requiring revision.
Question 99
Two 11-year-old patients have identical 15° valgus deformities and similar growth rates. Patient A's deformity is in the distal femur (wider physis), and Patient B's deformity is in the distal tibia (narrower physis). Both are treated with hemi-epiphysiodesis. Which patient's deformity is expected to correct more quickly, and why?
View Answer & Explanation
Correct Answer: A
Rationale: The rate of angular correction is a function of physeal growth rate and physeal width. The text explains that a larger width growth plate has a greater "turning radius" and is less "agile," meaning it corrects more slowly than a smaller width growth plate growing at the same rate. Therefore, the narrower distal tibial physis will correct faster.
Question 100
A surgeon is performing a lateral distal femoral hemi-epiphysiodesis using a tension-band plate for genu varum. To minimize the risk of secondary deformities, what is the most critical aspect of implant placement as seen on the lateral radiograph?
View Answer & Explanation
Correct Answer: A
Rationale: The text emphasizes that the implant must be perfectly centered over the physis on the lateral view. Anterior malpositioning will induce a genu recurvatum deformity, while posterior malpositioning will induce a genu flexum deformity. The text also recommends extra-periosteal placement (E) to preserve blood supply, but central placement is most critical for avoiding secondary plane deformity.
You Might Also Like
