Orthopedic Deformity Correction & Gait Biomechanics Review | Paley's Principles | Part 6
Key Takeaway
Orthopedic deformity correction involves applying Paley's principles to realign mechanical axes, using various osteotomy techniques like opening/closing wedges and domes. Critical elements include identifying the CORA and ACA, understanding their relationship, and analyzing gait biomechanics to restore physiological Ground Reaction Vector pathways, minimizing joint overload and metabolic cost.
Question 1
A 48-year-old male undergoes a dome osteotomy of the distal tibia for a varus malunion. During the correction, the bone segments pivot smoothly. The inherent Angulation Correction Axis (ACA) of any dome osteotomy is located at what point?
View Answer & Explanation
Correct Answer: C
Rationale: The dome osteotomy functions by rotating two cylindrical surfaces against each other. The axis of this rotation, and therefore the ACA, is inherently the central axis of the cylinder from which the cut is derived. In 2D, this is the center of the circle that forms the arc of the osteotomy.
Question 2
A 62-year-old female with medial compartment arthritis and genu varum undergoes a classic Maquet high tibial dome osteotomy. When analyzed using Paley's principles, what is the critical geometric flaw of this procedure?
View Answer & Explanation
Correct Answer: C
Rationale: The classic Maquet osteotomy is a concave-distal dome. While the apex of the cut may be near the CORA, the geometric center of the circle (the ACA) is located far distally. This mismatch between the ACA and CORA is a violation of deformity correction principles and leads to secondary translation.
Question 3
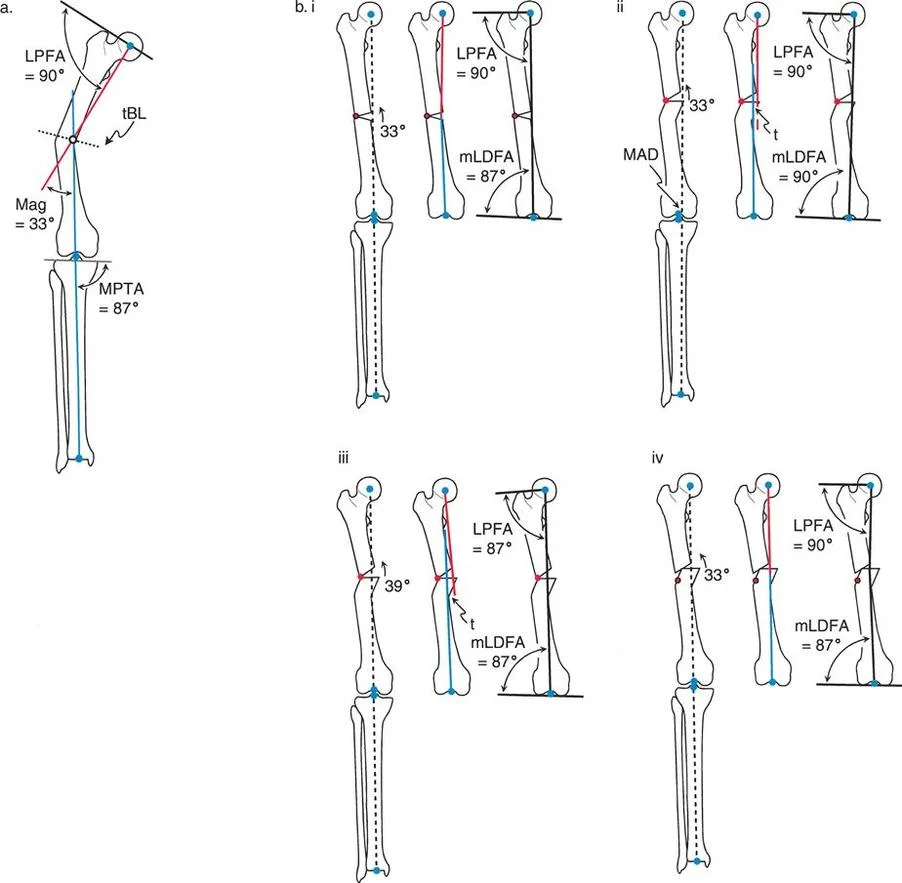
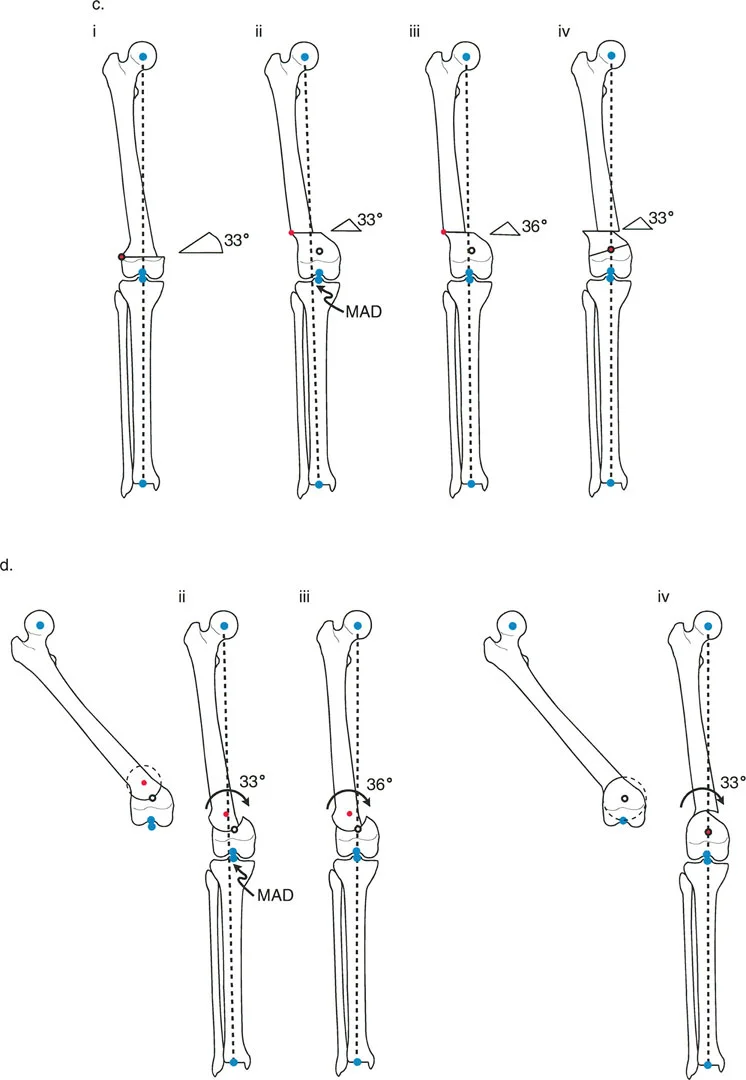
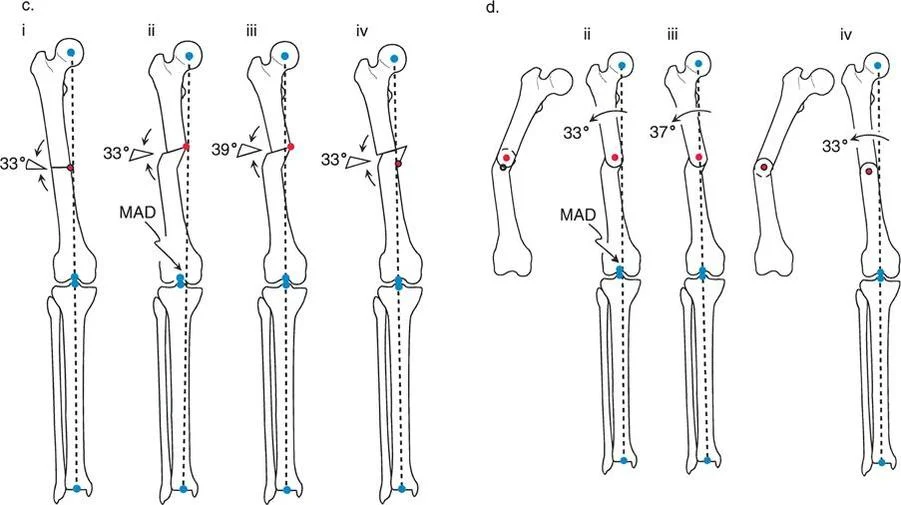
The provided image illustrates the geometric problem with the classic Maquet osteotomy for a varus tibia. Based on the diagram, why does correcting the angular deformity result in a secondary translation of the mechanical axis?
View Answer & Explanation
Correct Answer: B
Rationale: The image clearly shows that the CORA is located near the joint line, while the center of the circular cut (the ACA) is located far distally in the tibial diaphysis. Because the bone is hinged around an ACA that is not at the CORA, a secondary translation deformity is created (Paley's Rule 3).
Question 4
A surgeon performs a classic Maquet high tibial osteotomy for a 10-degree varus deformity. The angular correction is performed precisely to 10 degrees. According to Paley's principles, what is the most likely outcome regarding the mechanical axis?
View Answer & Explanation
Correct Answer: C
Rationale: Because the Maquet osteotomy violates Rule 3 (ACA is not at the CORA), correcting the angular deformity alone will not fully correct the mechanical axis. A secondary medial translation is induced, resulting in a residual medial Mechanical Axis Deviation (MAD).
Question 5
During a Maquet-style high tibial osteotomy for varus deformity, a surgeon corrects the angulation but notices the mechanical axis is still deviated medially. To eliminate this residual MAD, the surgeon must perform what compensatory maneuver?
View Answer & Explanation
Correct Answer: B
Rationale: To compensate for the secondary translation created by the incorrect ACA placement in a Maquet osteotomy, the surgeon is forced to overcorrect the angular deformity. This pushes the distal limb segment further laterally, shifting the mechanical axis back to the center of the knee, but at the cost of creating an abnormal joint orientation angle.
Question 6
A 45-year-old male presents with medial knee pain. A full-length standing radiograph shows the mechanical axis line passing 20 mm medial to the center of the knee joint. Which of the following terms best describes this finding?
View Answer & Explanation
Correct Answer: B
Rationale: The mechanical axis is a line from the center of the femoral head to the center of the ankle. When this line passes medial to the knee center, it indicates a varus deformity, which is quantified as medial Mechanical Axis Deviation (MAD). Valgus malalignment would result in the axis passing lateral to the knee center.
Question 7
A 28-year-old female undergoes preoperative planning for a distal femoral osteotomy. Her surgeon measures the angle between the femoral mechanical axis and the knee joint line on the lateral side. A value of 80° is recorded. What is the name of this angle, and what deformity does it indicate?
View Answer & Explanation
Correct Answer: C
Rationale: The mechanical Lateral Distal Femoral Angle (mLDFA) is the angle between the femoral mechanical axis and the distal femoral joint line. The normal value is 87°. A value less than 85° (e.g., 80°) indicates a valgus deformity of the distal femur. An mLDFA greater than 90° would indicate varus.
Question 8
During preoperative planning for a femoral malunion, the proximal mechanical axis (PMA) and distal mechanical axis (DMA) are drawn on a long-leg radiograph. These two lines intersect at a single point in the mid-diaphysis. What is this intersection point called?
View Answer & Explanation
Correct Answer: D
Rationale: The Center of Rotation of Angulation (CORA) is the geometric apex of a deformity, defined as the point where the proximal and distal mechanical axis lines intersect. The ACA is the surgically created hinge point for correction, which may or may not be at the same location as the CORA.
Question 9
A surgeon is correcting a mid-diaphyseal femoral varus deformity. The osteotomy is performed precisely at the CORA, and the hinge for correction (ACA) is also placed at the CORA. According to Paley's rules, what is the expected outcome regarding the anatomic axis?
View Answer & Explanation
Correct Answer: B
Rationale: This scenario describes Paley's Osteotomy Rule 1. When the osteotomy and the ACA are both located at the CORA, a pure angular correction is achieved. This results in perfect realignment of both the mechanical and anatomic axes without any translation.
Question 10
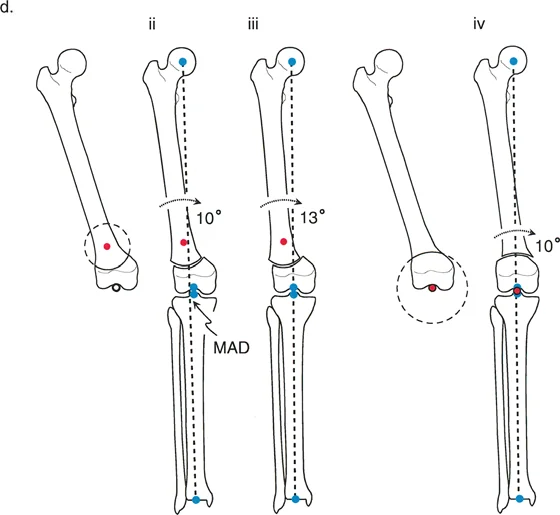
A 19-year-old has a distal femoral valgus deformity where the CORA is located within the knee joint. To preserve the joint, the surgeon performs an osteotomy in the distal femoral metaphysis but places the axis of correction (ACA) at the CORA. Which of Paley's rules is being applied, and what is the expected result?
View Answer & Explanation
Correct Answer: B
Rationale: This is the classic application of Paley's Osteotomy Rule 2. The ACA is at the CORA, but the osteotomy is at a different level. This correctly realigns the mechanical axis and joint orientation but necessarily creates a translation of the bone segments at the osteotomy site.
Question 11
A surgeon corrects a 20° distal femoral valgus deformity. The CORA is at the joint line. The surgeon performs a closing wedge osteotomy 4 cm proximal to the joint and places the hinge (ACA) at the osteotomy level, not at the CORA. What is the most likely outcome?
View Answer & Explanation
Correct Answer: C
Rationale: This describes a violation of Rule 2, which is an application of Paley's Osteotomy Rule 3. When both the osteotomy and the ACA are placed at a level different from the CORA, a secondary translational deformity is created, and the mechanical axis is not fully restored, resulting in residual MAD.
Question 12
A 25-year-old patient with a 15° femoral varus deformity requires a corrective osteotomy that will also lengthen the limb by 1.5 cm. Which type of osteotomy is most appropriate, and where should the ACA be placed?
View Answer & Explanation
Correct Answer: B
Rationale: An opening wedge osteotomy inherently lengthens the bone on the side of the wedge. For a varus (bow-legged) deformity, the convexity is lateral. The hinge of correction (ACA) for an opening wedge is placed on the convex side to pivot the bone open correctly.
Question 13
A 50-year-old patient with significant osteoporosis has a varus malunion of the tibia. The surgeon desires maximum bone-on-bone contact for stability and faster healing, and a slight limb shortening is acceptable. Which osteotomy technique is most suitable?
View Answer & Explanation
Correct Answer: C
Rationale: A closing wedge osteotomy involves removing a wedge of bone and closing the gap, which provides excellent cortical contact and inherent stability, promoting faster healing. It also causes limb shortening, which is acceptable in this case. Opening wedges have a gap that needs to be filled and are less stable acutely.
Question 14
A surgeon plans a focal dome osteotomy for a diaphyseal deformity. For this technique to achieve pure angular correction without inducing translation or residual MAD, where must the center of the circular osteotomy cut be located?
View Answer & Explanation
Correct Answer: C
Rationale: The key principle of a focal dome osteotomy is that the center of rotation of the cut must be coincident with the CORA. When this is achieved, the bone segments can slide along the curved path, resulting in perfect angular correction without altering the mechanical axis alignment or creating translation.
Question 15
A 17-year-old presents with a 10° distal femoral valgus deformity with the CORA located at the knee joint line. A medial opening wedge osteotomy is planned in the metaphysis. To achieve a perfect mechanical axis, what is the most critical step according to Paley's principles?
View Answer & Explanation
Correct Answer: C
Rationale: This is a Rule 2 scenario. Since the CORA is in the joint, the osteotomy must be done elsewhere (metaphysis). To restore the mechanical axis perfectly, the ACA must be placed at the CORA. This will cause the distal fragment to translate medially, which is a necessary and planned consequence of the correction.
Question 16
A 22-year-old has a severe 33° distal femoral valgus deformity with the CORA at the old physeal scar. The surgeon performs an osteotomy proximal to the CORA and places the ACA at the osteotomy level. If a 33° correction is made, what is the expected outcome for the mechanical axis?
View Answer & Explanation
Correct Answer: C
Rationale: This is a common error (Rule 3). By placing the ACA at the osteotomy level instead of the true CORA, correcting the deformity angle (33°) will not fully realign the limb. The mechanical axis will not pass through the knee center, leaving residual MAD. To fix the MAD, one would have to overcorrect the angle, which would then malorient the joints.
Question 17
A patient presents with a "golf club" deformity of the femur after a previous varus osteotomy for valgus. The PMA and DMA lines are nearly parallel. This appearance is the classic result of which surgical error?
View Answer & Explanation
Correct Answer: C
Rationale: A "golf club" deformity is a pure or near-pure translational deformity. It occurs when an angular correction is performed at a level remote from the CORA without accounting for the necessary translation (i.e., placing the ACA at the osteotomy site). This is an application of Rule 3, which creates a secondary translational deformity.
Question 18
A 16-year-old male undergoes gradual correction of a distal femoral valgus deformity using an Ilizarov circular external fixator. The hinges of the frame are placed at the level of the knee joint, while the osteotomy is performed in the metaphysis. This setup is designed to execute which principle?
View Answer & Explanation
Correct Answer: B
Rationale: The Ilizarov frame's hinges act as the ACA. By placing them at the CORA (the knee joint) while cutting the bone at a different level (metaphysis), the frame forces the bone to angulate and translate simultaneously. This is a perfect mechanical execution of Paley's Rule 2.
Question 19
A surgeon is using the Fixator-Assisted Nailing (FAN) technique for a distal femoral valgus deformity. What is the primary role of the temporary external fixator in this procedure?
View Answer & Explanation
Correct Answer: C
Rationale: In the FAN technique, the external fixator is used as a temporary reduction tool. It allows the surgeon to precisely correct the angulation and translation and hold that correction securely while the definitive internal fixation (the intramedullary nail) is placed. The fixator is then removed.
Question 20
A 35-year-old male has a 33° varus deformity in the mid-diaphysis of his femur. The CORA is easily accessible. The surgeon plans an osteotomy at the CORA stabilized with an intramedullary nail. Why is this scenario considered ideal for applying Paley's Rule 1?
View Answer & Explanation
Correct Answer: B
Rationale: Rule 1 (osteotomy and ACA at the CORA) is ideal for diaphyseal deformities because the CORA is located in the shaft of the bone, far from the complexities of a joint. This allows the surgeon to cut directly at the apex of the deformity, achieving a pure angular correction without the need for a compensatory translation.
Question 21
A 30-year-old male has a hypertrophic varus nonunion of the femur. Preoperative planning reveals the CORA is located medial to the actual bone. What is the correct interpretation of this finding?
View Answer & Explanation
Correct Answer: C
Rationale: Due to the normal neck-shaft angle of the femur, the mechanical axis line runs medial to the femoral diaphysis. Therefore, when the PMA and DMA lines are drawn for a diaphyseal deformity, their intersection point (CORA) can correctly fall outside the physical boundary of the bone. This is not an error.
Question 22
When performing an acute deformity correction of the femoral diaphysis with an intramedullary nail, what is the purpose of using Poller (blocking) screws?
View Answer & Explanation
Correct Answer: D
Rationale: An intramedullary nail will tend to follow the path of least resistance down the canal, which can cause it to re-create the deformity. Poller screws are placed strategically to act as a buttress, effectively narrowing the canal and steering the nail along the desired, corrected path, thereby holding the reduction.
Question 23
According to the surgical pearls provided, why is it crucial to draw both the anatomic and mechanical axes during preoperative planning for a femoral deformity?
View Answer & Explanation
Correct Answer: B
Rationale: In the femur, due to the neck-shaft angle, the anatomic and mechanical axes are not the same (they differ by about 7°). A surgeon who only straightens the anatomic axis (the "look" of the bone) may fail to correct the mechanical axis, leading to persistent joint malalignment and abnormal loading.
Question 24
A 55-year-old man with medial compartment knee osteoarthritis is evaluated. Observational gait analysis reveals a distinct lateral bowing of the knee during the loading response of the stance phase. This clinical sign is a dynamic manifestation of the underlying deformity. What is this pathognomonic gait finding called?
View Answer & Explanation
Correct Answer: D
Rationale: A varus thrust is a visible, dynamic lateral bowing of the knee during the stance phase. It is a glaring sign of a medially shifted Ground Reaction Vector (GRV) due to varus deformity, which overloads the medial compartment and stretches the lateral ligamentous structures.
Question 25
A 45-year-old woman undergoes a distal tibial osteotomy for a procurvatum deformity. Postoperatively, she complains of difficulty walking and a feeling of being "blocked" during midstance. Which of the three rockers of gait is most likely compromised by her original deformity?
View Answer & Explanation
Correct Answer: B
Rationale: A procurvatum (apex-anterior) deformity of the distal tibia decreases the Anterior Distal Tibial Angle (ADTA) and functions like a fixed equinus contracture. This physically blocks the tibia from advancing over the talus, obliterating the second (ankle) rocker, which is essential for forward progression during midstance.
Question 26
A 62-year-old male presents with severe knee pain. A full-length standing radiograph is obtained for deformity analysis. The surgeon draws a line from the center of the femoral head to the center of the ankle mortise. This line passes 25 mm medial to the center of the knee joint. What does this measurement represent?
View Answer & Explanation
Correct Answer: C
Rationale: The Mechanical Axis Deviation (MAD) is the perpendicular distance from the center of the knee joint to the mechanical axis (a line from the femoral head center to the ankle center). A medial MAD indicates a varus deformity and predicts medial compartment overload during gait.
Question 27
During preoperative planning for a high tibial osteotomy, the surgeon identifies the intersection point of the proximal and distal mechanical axes of the tibia. According to Paley's principles, what is the geometric term for this critical point?
View Answer & Explanation
Correct Answer: C
Rationale: The Center of Rotation of Angulation (CORA) is the specific geometric point where the proximal and distal mechanical axis lines of a deformed bone intersect. Locating the CORA is the single most important step in preoperative planning, as it dictates where the surgical correction should be centered.
Question 28
A surgeon is planning a corrective osteotomy for a tibial deformity. The plan involves placing the osteotomy cut and the corrective hinge at a location distant from the CORA. According to Paley's osteotomy rules, what is the inevitable and biomechanically flawed outcome of this surgical plan?
View Answer & Explanation
Correct Answer: E
Rationale: This scenario describes Paley's Osteotomy Rule Three. When both the osteotomy and the hinge are located away from the CORA, the mechanical axes become parallel but not collinear. This leaves a residual translation deformity and a persistent Mechanical Axis Deviation (MAD), which is biomechanically flawed and compromises the gait outcome.
Question 29
A 30-year-old patient has a 20° fixed flexion deformity (FFD) of the right knee. During gait, the Ground Reaction Vector (GRV) is consistently posterior to the knee joint center. Which muscle group must work excessively throughout the stance phase to prevent the knee from buckling?
View Answer & Explanation
Correct Answer: B
Rationale: In the presence of a knee flexion deformity, the GRV passes posterior to the knee, creating a constant external flexion moment. This must be balanced by an internal extension moment produced by the quadriceps muscle to maintain stability. This leads to rapid quadriceps fatigue and is one of the most metabolically expensive deformities.
Question 30
A 60-year-old woman with a history of ankle trauma presents with a stiff ankle and gait disturbance. A pedobarographic analysis is performed. The surgeon notes that the center of pressure fails to progress past the heel during the entire stance phase. This finding indicates a catastrophic failure of which specific gait mechanisms?

View Answer & Explanation
Correct Answer: C
Rationale: The image shows intense, prolonged loading on the heel, with a complete failure of the center of pressure to progress anteriorly. This indicates a functional heel rocker (initial contact) but a catastrophic absence of the second (ankle) and third (forefoot) rockers, which are responsible for advancing the tibia and providing propulsion, respectively.
Question 31
A 22-year-old male has a valgus deformity of his left knee. During midstance, where does the Ground Reaction Vector (GRV) pass relative to the knee joint center, and what is the resulting pathological moment?
View Answer & Explanation
Correct Answer: B
Rationale: In a valgus (knock-kneed) deformity, the mechanical axis and thus the GRV are shunted lateral to the center of the knee. This creates a powerful external abduction moment, which overloads the lateral compartment and places chronic tensile stress on the medial collateral ligament (MCL).
Question 32
A surgeon is evaluating a full-length standing radiograph of a patient with a tibial deformity. The Medial Proximal Tibial Angle (MPTA) is measured to be 78°. What is the clinical significance of this finding?
View Answer & Explanation
Correct Answer: C
Rationale: The normal Medial Proximal Tibial Angle (MPTA) is 85° to 90°. An MPTA less than 85° indicates a tibial varus deformity. This is the most frequent cause of medial compartment overload during midstance.
Question 33
A 14-year-old girl presents with a "knock-kneed" appearance. Radiographic analysis reveals a Mechanical Lateral Distal Femoral Angle (mLDFA) of 95°. The MPTA is normal at 88°. Based on these findings, where is the primary source of the patient's valgus deformity?
View Answer & Explanation
Correct Answer: D
Rationale: The normal mLDFA is 85° to 90°. An mLDFA greater than 90° indicates a valgus deformity originating from the distal femur. Since the MPTA is normal, the tibia is not contributing to the overall valgus alignment.
Question 34
A 40-year-old patient has a history of a malunited tibial shaft fracture. The surgeon plans an osteotomy and places the corrective hinge exactly at the CORA, but performs the bone cut in the diaphysis for better healing potential. Which of Paley's osteotomy rules is being applied?
View Answer & Explanation
Correct Answer: B
Rationale: Paley's Osteotomy Rule Two describes the scenario where the axis of correction (hinge) is placed at the CORA, but the osteotomy is performed at a different level. This results in perfect angular correction and collinear mechanical axes, but creates a mandatory translation at the osteotomy site, which must be accounted for.
Question 35
Which joint orientation angle is most critical for the successful execution of the second (ankle) rocker of gait, and what is its normal range?
View Answer & Explanation
Correct Answer: D
Rationale: The Anterior Distal Tibial Angle (ADTA) is a sagittal plane angle that is crucial for gait. A normal ADTA (78°-82°) is absolutely necessary for the 10°-15° of dorsiflexion required for the tibia to advance over the foot, which defines the functional second (ankle) rocker.
Question 36
A 28-year-old patient with a 3 cm leg length discrepancy (LLD) on the right side is observed walking. To compensate for the short limb, the patient ambulates on the toes of their right foot. What is this classic gait compensation called?
View Answer & Explanation
Correct Answer: C
Rationale: Walking in equinus (on the toes) is a classic gait compensation for a leg length discrepancy on the short side. This maneuver functionally lengthens the shorter limb to help level the pelvis during the stance phase.
Question 37
In a physiologically normal limb during midstance, the Ground Reaction Vector (GRV) passes slightly anterior to the knee joint center. What is the biomechanical advantage of this alignment?
View Answer & Explanation
Correct Answer: B
Rationale: The GRV passing slightly anterior to the knee creates a mild external extension moment. This is a marvel of biomechanical efficiency, as it is easily counteracted by passive tension in the posterior capsule of the knee with minimal active muscular effort, thus conserving metabolic energy.
Question 38
A 58-year-old man with a painful gait undergoes pedobarographic analysis. The force-time graph for his affected left foot (red line) is sharply shortened and more erratic compared to the smooth, longer curve of his right foot (blue line). What is the most likely clinical interpretation of this finding?
View Answer & Explanation
Correct Answer: B
Rationale: An asymmetrical, sharply shortened stance time is the hallmark of an antalgic (pain-avoiding) or mechanically unstable gait. The patient is instinctively minimizing the time spent on the affected limb to avoid pain or a feeling of instability, which is a direct consequence of the underlying pathology.
Question 39
The first rocker of gait begins at initial contact and is critical for shock absorption. Which muscle group is primarily responsible for controlling this phase through eccentric contraction?
View Answer & Explanation
Correct Answer: D
Rationale: During the first (heel) rocker, the pretibial muscles, primarily the tibialis anterior, contract eccentrically. This controlled firing decelerates the foot's plantarflexion ("foot slap") and pulls the tibia forward, initiating knee flexion for shock absorption.
Question 40
The third rocker of gait is responsible for providing the massive propulsive thrust to drive the limb into the swing phase. This mechanism is centered on which anatomical fulcrum?
View Answer & Explanation
Correct Answer: C
Rationale: The third (forefoot) rocker uses the metatarsophalangeal (MTP) joints as its fulcrum. As the heel lifts off the ground, the powerful triceps surae complex contracts concentrically, pivoting over the MTP joints to provide the propulsion needed for terminal stance and preswing.
Question 41
A surgeon is performing a massive valgus-producing osteotomy of the proximal tibia to correct a severe varus deformity. What prophylactic procedure should be strongly considered to prevent a common iatrogenic complication?
View Answer & Explanation
Correct Answer: C
Rationale: Large angular corrections that produce valgus at the proximal tibia can place the common peroneal nerve under significant tension. Prophylactic decompression of the nerve as it winds around the fibular neck is a crucial step to prevent a stretch neuropraxia, which can result in a debilitating foot drop.
Question 42
A 19-year-old patient has a distal tibial recurvatum deformity following a physeal injury. How would this deformity affect the Anterior Distal Tibial Angle (ADTA) and the stance phase of gait?
View Answer & Explanation
Correct Answer: B
Rationale: Recurvatum (apex-posterior) of the distal tibia increases the ADTA. This places the ankle in relative dorsiflexion, causing the tibia to advance too quickly over the foot. The result is a premature heel-off and a shortened, highly inefficient stance phase.
Question 43
During a preoperative evaluation, the single most reliable clinical sign of pain, instability, or mechanical insufficiency on an affected limb is observed during the "Hallway Test." What is this sign?
View Answer & Explanation
Correct Answer: B
Rationale: A shortened stance time on the affected limb is the most reliable clinical sign of a problem. Patients instinctively spend as little time as possible bearing weight on a limb that is painful, unstable, or mechanically inefficient, a phenomenon clearly visible during observational gait analysis.
Question 44
A 65-year-old patient with severe knee osteoarthritis has a 10° Joint Line Convergence Angle (JLCA) on weight-bearing radiographs, which reduces to 1° on varus stress views. What does the large JLCA on the standing film primarily represent?
View Answer & Explanation
Correct Answer: D
Rationale: The Joint Line Convergence Angle (JLCA) quantifies the angle between the distal femoral and proximal tibial articular surfaces. A widened JLCA (normal is 0-2°) on weight-bearing films that is correctable on stress views indicates dynamic instability from ligamentous laxity or, more commonly, severe asymmetrical cartilage wear in one compartment.
Question 45
A surgeon plans a distal femoral osteotomy for a valgus deformity. The CORA is located in the metaphysis. The surgeon chooses to perform the osteotomy and place the corrective hinge exactly at the CORA. According to Paley's rules, what is the expected result at the osteotomy site?
View Answer & Explanation
Correct Answer: A
Rationale: This scenario describes Paley's Osteotomy Rule One, the anatomic ideal. When the osteotomy cut and the axis of correction (hinge) are both placed exactly at the CORA, pure angular correction is achieved. The bone ends angulate seamlessly without any translation, and the mechanical axes become perfectly collinear.
Question 46
A 35-year-old patient has a 25° fixed flexion deformity (FFD) of both knees and stiff ankles. To maintain a plantigrade foot during stance, what compensatory posture will this patient most likely adopt?
View Answer & Explanation
Correct Answer: C
Rationale: With bilateral FFD >20° and stiff ankles, the patient cannot use ankle dorsiflexion or equinus to compensate. Instead, they will increase hip flexion and lean the trunk forward. This posture allows them to place the foot flat on the ground but dramatically increases the workload on the gluteus maximus to maintain an upright posture.
Question 47
What is the primary, overriding goal of any lower extremity realignment surgery, such as a high tibial osteotomy, from a biomechanical perspective?
View Answer & Explanation
Correct Answer: C
Rationale: The ultimate objective of deformity correction is the restoration of dynamic biomechanical function. The primary goal of a realignment surgery is to redirect the GRV back to its physiological, energy-conserving pathway, thereby normalizing joint moments, reducing cartilage wear, and minimizing the metabolic cost of walking.
Question 48
A 50-year-old patient with a varus malunion of the distal tibia is evaluated. Radiographs show a Lateral Distal Tibial Angle (LDTA) of 80°. How will this deformity affect loading across the ankle joint during gait?
View Answer & Explanation
Correct Answer: A
Rationale: The normal LDTA is 87° to 91°. An LDTA less than 87° represents a varus deformity of the distal tibia. This causes the center of pressure to shift dangerously medially across the talar dome, leading to medial edge-loading and predisposing the patient to rapid ankle arthritis.
Question 49
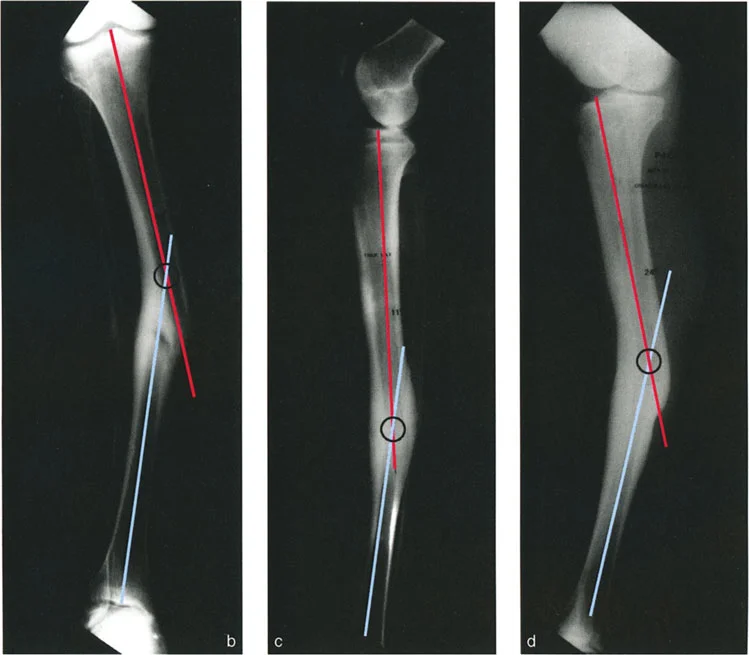
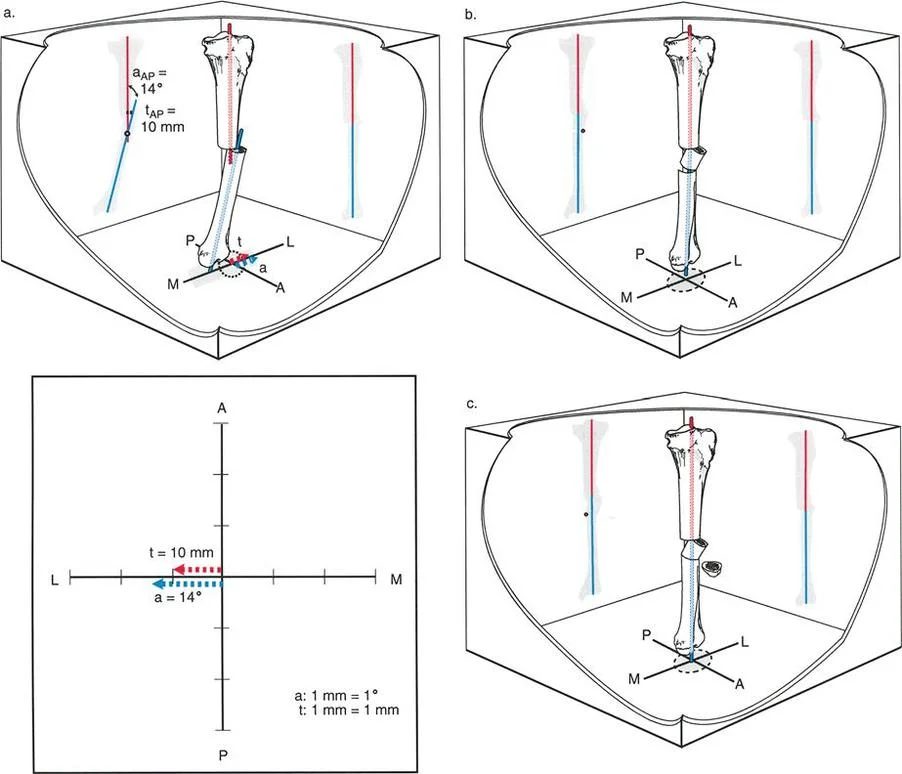
A 35-year-old male presents with a left tibial malunion. The anteroposterior (AP) radiograph shows pure valgus angulation with no translation. The lateral (LAT) radiograph shows pure anterior translation with no angulation. According to the principles of deformity analysis, what is the relationship between the plane of angulation and the plane of translation?
View Answer & Explanation
Correct Answer: C
Rationale: The vignette describes a deformity where angulation exists purely in one anatomic plane (frontal) and translation exists purely in the other anatomic plane (sagittal). These planes are, by definition, perpendicular (90° apart). This corresponds to Variant 1 described in the text.
Question 50
A 40-year-old female has a tibial malunion where the angulation is confined to the frontal plane. In this specific scenario, where is the Center of Rotation of Angulation (CORA) located on the anteroposterior (AP) view?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "The CORA is at the level of the fracture because there is no translation in the plane of angulation." Since the angulation is in the frontal plane and there is no translation in that same plane, the CORA must be at the fracture level on the AP view.
Question 51
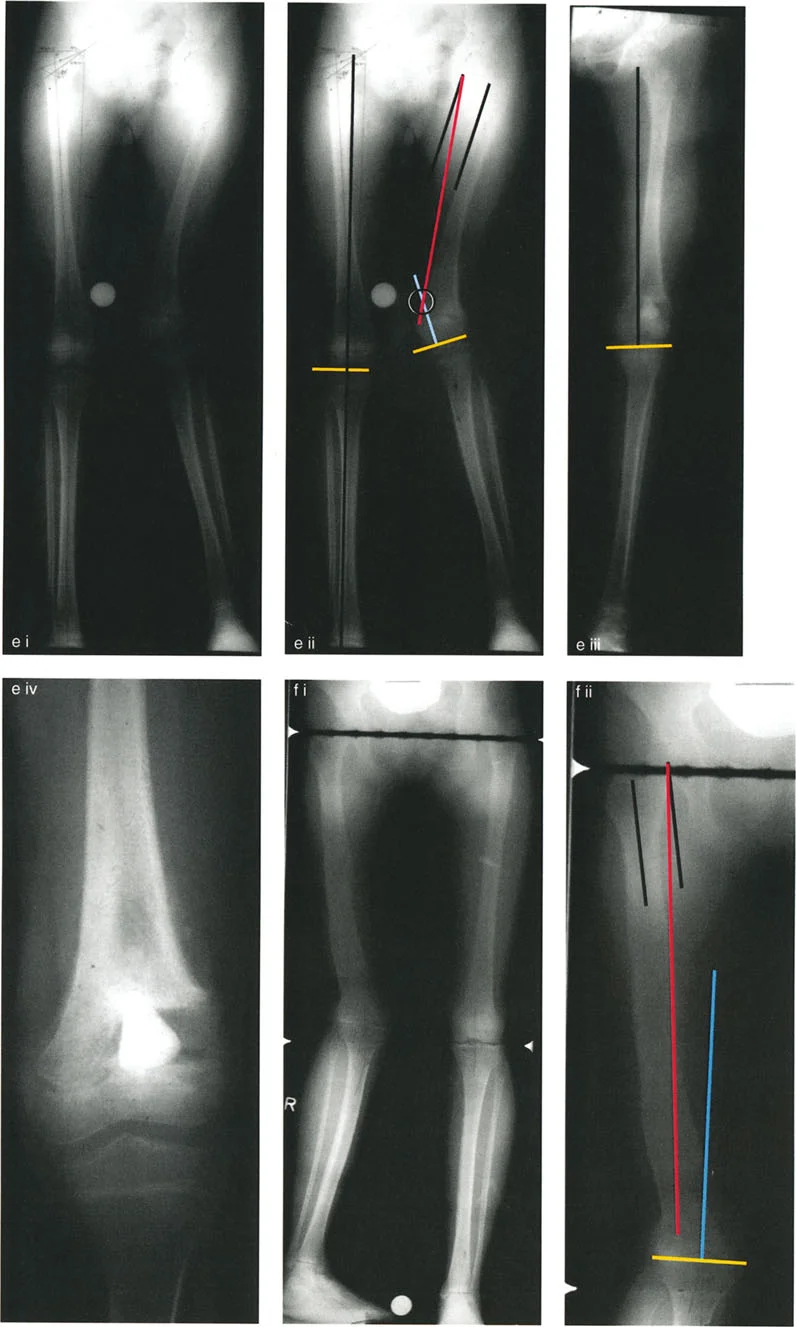
A 50-year-old male sustained a tibial fracture 30 years ago, which healed with a pure lateral translation deformity in the frontal plane and no angulation. He now presents with knee pain and radiographs show isolated lateral compartment osteoarthritis. What is the most likely cause of his arthritis?

View Answer & Explanation
Correct Answer: C
Rationale: The provided text explicitly notes an example case where a patient developed lateral compartment osteoarthritis due to lateral MAD from lateral translation deformity alone. This demonstrates that MAD, whether from angulation or translation, can lead to degenerative joint changes.
Question 52
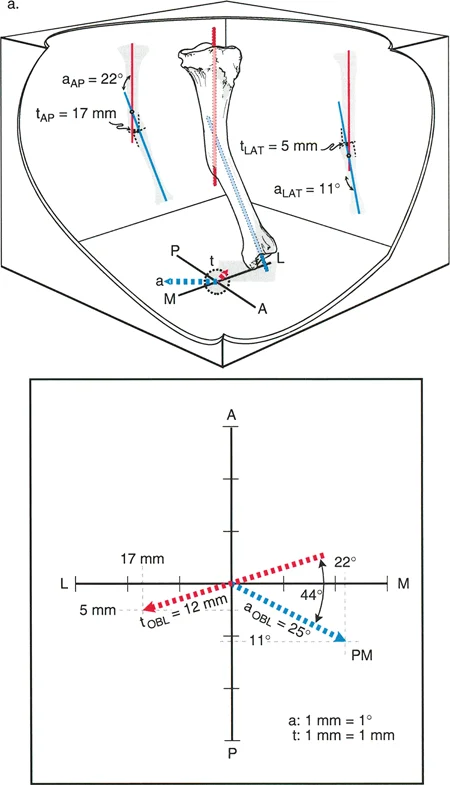
A surgeon is analyzing a tibial malunion. The AP radiograph shows both varus angulation and lateral translation. The LAT radiograph shows both procurvatum angulation and posterior translation. The CORA on the AP view is proximal to the fracture, while the CORA on the LAT view is distal. What does the differing level of the CORAs indicate?

View Answer & Explanation
Correct Answer: B
Rationale: The text states, "The CORAs' being at different level is the hallmark that angulation and translation are in different planes." This situation is characteristic of deformities where both angulation and translation exist in oblique planes (Variant 2 or 4).
Question 53
A 28-year-old patient has a tibial malunion with angulation and translation in different oblique planes that are 90° apart (Variant 2). What would be expected on an oblique radiograph taken perpendicular to the plane of maximum angulation?
View Answer & Explanation
Correct Answer: B
Rationale: For a Variant 2 deformity, where the planes of angulation and translation are 90° apart, an oblique radiograph can be obtained that is perfectly aligned with the plane of angulation. This view, by definition, is perpendicular to the plane of translation, and would therefore show "angulation with no translation."
Question 54
A patient presents with the tibial deformity shown in the diagram, where angulation is in the frontal plane (x-axis) and translation is in the sagittal plane (y-axis). This represents a Variant 1 deformity. Which statement is true regarding the CORA in the sagittal plane?

View Answer & Explanation
Correct Answer: D
Rationale: The Center of Rotation of Angulation (CORA) is a concept that applies to angular deformities. In a plane where there is pure translation and no angulation (the sagittal plane in this case), the CORA is undefined or irrelevant. The text focuses on the CORA being at the fracture level in the plane of angulation when there is no translation in that same plane.
Question 55
A 45-year-old male has a tibial malunion. The AP radiograph shows valgus angulation and medial translation. The LAT radiograph shows only posterior translation with no angulation. How would this deformity be classified?
View Answer & Explanation
Correct Answer: C
Rationale: This scenario fits the description of Variant 3. The text states for this variant: "AP radiograph shows angulation and translation and LAT radiograph shows translation only." Because translation appears on both views (medial on AP, posterior on LAT), the plane of translation is oblique. Because angulation appears only on the AP view, the plane of angulation is anatomic (frontal). The planes are therefore different and less than 90° apart.
Question 56
A patient has a complex tibial malunion where both AP and LAT radiographs show angulation and translation. The CORAs are at different levels. An oblique radiograph obtained to show maximum angulation still demonstrates some translational deformity. An orthogonal oblique view shows no angulation but still has some translation. What is the relationship between the planes of angulation and translation?
View Answer & Explanation
Correct Answer: D
Rationale: This describes a Variant 4 deformity. The key finding is that no single radiographic plane can isolate one deformity component from the other. The text explains: "there is no plane in which the radiographic projection does not show the presence of either angulation or translation," which occurs when both deformities are in different oblique planes that are less than 90° apart.
Question 57
When planning an osteotomy for a tibial malunion with angulation and translation in the same anatomic plane, the correction is planned at the a-t CORA. If an opening wedge osteotomy is performed at this level, what is the expected outcome regarding the translational component of the deformity?
View Answer & Explanation
Correct Answer: B
Rationale: The text states that when correcting at the a-t CORA with a single angular maneuver (like an opening or closing wedge), "The fracture site is not disturbed; the bump from the translation is therefore left on the bone." The primary correction is angular; the translation itself is not directly addressed by this specific technique.
Question 58
A 33-year-old patient has a tibial malunion. The AP radiograph shows only lateral translation. The LAT radiograph shows only recurvatum angulation. This deformity is depicted in the provided clinical example. Which statement accurately describes this deformity?
View Answer & Explanation
Correct Answer: B
Rationale: This is a classic example of a Variant 1 deformity. Translation is purely in the frontal (anatomic) plane, and angulation is purely in the sagittal (anatomic) plane. The two planes are different and are 90° apart.
Question 59
The hallmark of a deformity where angulation and translation are in different planes is that the CORA on the AP view is at a different level than the CORA on the LAT view. This is characteristic of which two deformity variants?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states for both Variant 2 and Variant 4 that "The CORA on the AP radiograph is at a level different from that of the CORA on the LAT radiograph" or "the CORAs on the AP and LAT radiographs are at different levels." This is because in both variants, the deformity components are in different (and typically oblique) planes.
Question 60
A patient has a tibial malunion consistent with Variant 2 (angulation and translation in different oblique planes, 90° apart). An oblique radiograph is obtained that shows the plane of maximum translation. What angular deformity is expected on this specific view?
View Answer & Explanation
Correct Answer: C
Rationale: For a Variant 2 deformity, the planes of angulation and translation are orthogonal (90° apart). Therefore, the oblique radiograph that is perfectly aligned with the plane of maximum translation will be, by definition, perpendicular to the plane of angulation, and will show "translation with no angulation."
Question 61
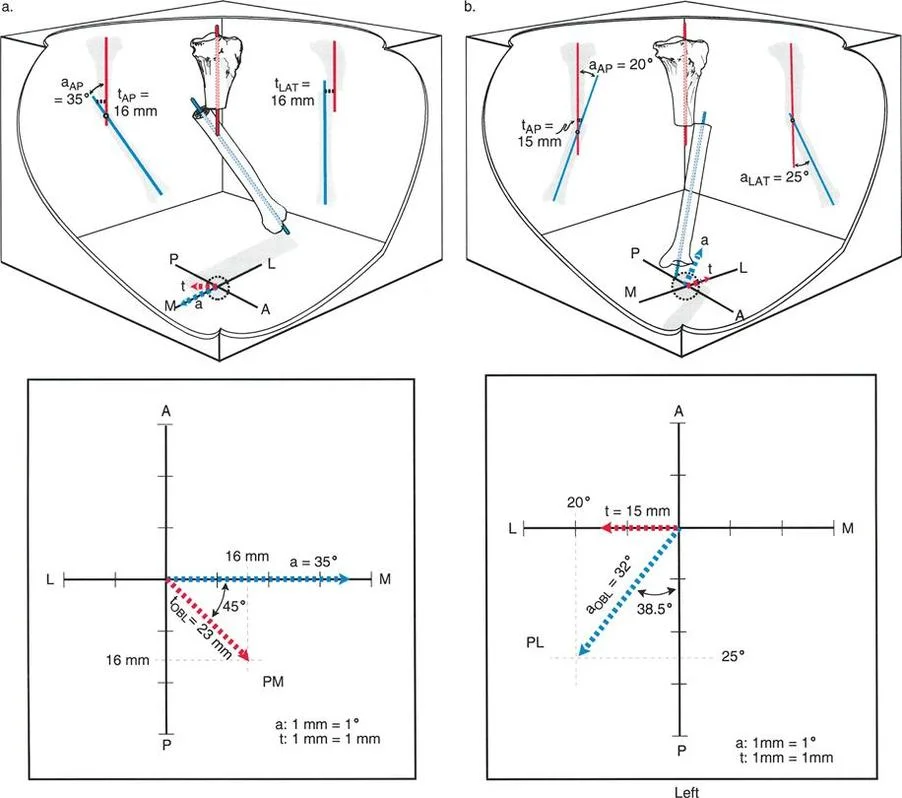
A 25-year-old presents with the tibial malunion shown. AP view shows 20° varus and lateral translation. LAT view shows 25° procurvatum and posterior translation. An oblique view reveals a 32° angulation. What is the significance of the 32° measurement?
View Answer & Explanation
Correct Answer: B
Rationale: The text, referencing this specific case, states: "The oblique plane angulation measures 32°, which is greater than the angulation on the AP and LAT views." This demonstrates that for an oblique plane deformity, the true magnitude of angulation is only seen on an oblique view aligned with that plane, and it will be greater than the components seen on the standard AP and LAT views.
Question 62
In the analysis of a Variant 3 deformity, the AP radiograph shows only medial translation, while the LAT radiograph shows both recurvatum and posterior translation. Which component of the deformity lies in an oblique plane?
View Answer & Explanation
Correct Answer: B
Rationale: The text explains that if a deformity component (angulation or translation) appears on both AP and LAT radiographs, it is in an oblique plane. In this case, translation is seen on both views (medial on AP, posterior on LAT), so translation is in an oblique plane. Angulation (recurvatum) is only seen on the LAT view, so it is in an anatomic (sagittal) plane.
Question 63
A surgeon is evaluating a tibial malunion. The AP view shows varus angulation and medial translation. The LAT view shows anterior translation but no angulation. Which statement correctly describes the planes of deformity?
View Answer & Explanation
Correct Answer: B
Rationale: This is an example of a Variant 3 deformity. Angulation (varus) is seen only on the AP view, so its plane is anatomic (frontal). Translation is seen on both views (medial on AP, anterior on LAT), so its plane is oblique. The text provides this exact example: "The plane of angulation is therefore in the frontal plane whereas the plane of translation is in an oblique plane."
Question 64
For a Variant 4 deformity (angulation and translation in different oblique planes, <90° apart), what is the expected finding on an oblique radiograph that shows the maximum translation?
View Answer & Explanation
Correct Answer: C
Rationale: The text explains for Variant 4: "The oblique radiograph that shows the maximum translation would also show some angular deformity of lesser magnitude to the actual oblique plane angulation." This is because the planes are not orthogonal, so they cannot be completely isolated from each other on any 2D projection.
Question 65
A patient has a tibial malunion with valgus angulation and lateral translation seen on the AP view, and recurvatum angulation and posterior translation on the LAT view. The CORAs are at different levels. This deformity is classified as Variant 4. What distinguishes this from a Variant 2 deformity?
View Answer & Explanation
Correct Answer: C
Rationale: Both Variant 2 and Variant 4 can present with angulation and translation on both AP and LAT views with CORAs at different levels. The key differentiator is the relationship between the planes. In Variant 2, the planes are 90° apart, allowing for oblique views with pure deformity. In Variant 4, the planes are less than 90° apart, meaning no oblique view can completely isolate one deformity from the other.
Question 66
A surgeon performs a closing wedge osteotomy at the a-t CORA for a malunion where angulation and translation are in the same plane. The goal is to correct a varus deformity. What is a known consequence of this specific corrective strategy?
View Answer & Explanation
Correct Answer: C
Rationale: The text clearly states for both opening and closing wedge osteotomies performed at the a-t CORA: "The deformity is corrected by a single angular maneuver. The fracture site is not disturbed; the bump from the translation is therefore left on the bone."
Question 67
A 55-year-old male with a history of degenerative disc disease presents with low back pain and a forward-stooped posture. On examination, he has a 25-degree fixed flexion deformity (FFD) of his right hip. His gait analysis reveals an exaggerated lumbar lordosis but otherwise normal knee and ankle kinematics. According to Paley principles, what does this finding represent?
View Answer & Explanation
Correct Answer: B
Rationale: The text states that the primary line of defense against a hip FFD is increasing lumbar lordosis. This allows the patient to maintain an upright posture and horizontal visual axis. Mass flexion (A) occurs when lumbar mobility is compromised, and pseudo equinus (C) occurs when the deformity is even more severe.
Question 68
A 68-year-old female with a history of a T10-S1 spinal fusion for scoliosis develops a progressive 30-degree fixed flexion deformity of her left hip. She complains of severe anterior knee pain and profound quadriceps fatigue after walking short distances. Her gait is characterized by a crouched posture. What is the most likely biomechanical cause of her knee symptoms?
View Answer & Explanation
Correct Answer: D
Rationale: Due to her spinal fusion, the patient cannot compensate for her hip FFD with lumbar lordosis. She is forced into mass flexion, which involves forced knee flexion. This posture places the knee's extensor mechanism under a continuous, high-tensile load throughout stance, leading to quadriceps fatigue and anterior knee pain. Lumbar lordosis (B) is not possible due to her fusion.
Question 69
A 22-year-old male with cerebral palsy presents with a severe, crouched gait and bilateral 50-degree hip fixed flexion deformities. He walks exclusively on his toes. On physical examination, his ankle can be passively dorsiflexed to 15 degrees when his hip and knee are flexed. What is the most appropriate initial surgical management?
View Answer & Explanation
Correct Answer: C
Rationale: The patient's toe walking is a pseudo equinus, a compensation for the severe proximal hip FFD. The ability to passively dorsiflex the ankle with the hip/knee flexed confirms this. The Paley treatment principle is to correct the primary CORA, which is at the hip. A proximal femoral extension osteotomy addresses the cause. Achilles lengthening (A) would be a catastrophic error, removing his last point of stability.
Question 70
A 45-year-old patient with a right hip FFD is observed to be toe-walking on the right side. A surgeon suspects pseudo equinus. Which clinical test would most strongly support this diagnosis?
View Answer & Explanation
Correct Answer: E
Rationale: The text explicitly lists two key differentiators for pseudo equinus. The Silfverskiöld test will be negative because the ankle has full passive motion when the proximal compensatory chain is relaxed. Additionally, the patient can get their heel down if they flex their trunk, which shifts the center of gravity forward, negating the need for the distal compensation. A positive Thomas test (D) confirms the hip FFD but doesn't differentiate the cause of the toe walking.
Question 71
A 70-year-old male with ankylosing spondylitis and a rigid spine has a 40-degree hip FFD. He is forced into a mass flexion gait pattern. This compensatory strategy is designed to achieve what primary goal?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that mass flexion is an "obligate strategy designed solely to keep the center of gravity from falling anterior to the base of support." It is a metabolically expensive (B) and mechanically destructive strategy that does not improve gait efficiency (A) and severely loads, rather than offloads, the patellofemoral joint (D).
Question 72
The diagram below illustrates the progression of sagittal plane compensation for a hip FFD. The patient on the right has exhausted their ability to compensate with knee flexion and ankle dorsiflexion. What is the term for this patient's gait pattern?

View Answer & Explanation
Correct Answer: D
Rationale: The diagram and accompanying text explain that when a hip FFD is so severe that it exceeds the compensatory range of knee flexion and ankle dorsiflexion, the patient is forced into obligate toe walking. This is termed pseudo equinus. Mass flexion (A) is the preceding compensatory stage shown on the left.
Question 73
A 40-year-old laborer underwent a right hip arthrodesis in optimal position 15 years ago. He now presents with severe left knee and low back pain. His gait is characterized by rising on the toes of his fused right leg during its stance phase. What is this compensatory maneuver called?
View Answer & Explanation
Correct Answer: C
Rationale: To clear the contralateral (swinging) limb, a patient with a fused hip must use compensatory strategies. Vaulting is specifically defined as rising up forcefully on the toes of the stance limb to create clearance for the swing limb. Hip hiking (B) and circumduction (A) are other compensations used, but the description matches vaulting.
Question 74
A gait analysis study compares two patient cohorts: one with hip fusions and one with ankle fusions. Both groups have a similar average walking velocity. Based on advanced biomechanical principles, which group would be expected to have a significantly higher oxygen consumption per meter traveled?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that the oxygen consumption and overall energy expenditure are "drastically higher in the hip fusion patient." This is a direct consequence of losing the pelvic drop mechanism, which forces the body's center of gravity through a much higher, more abrupt, and metabolically punishing vertical arc.
Question 75
The scatter plot below demonstrates the relationship between two biomechanical variables during gait. A patient with a hip fusion would typically fall in the upper right quadrant of this plot. What does this indicate?

View Answer & Explanation
Correct Answer: D
Rationale: The plot shows that increased vertical displacement of the center of gravity (x-axis) directly correlates with higher oxygen consumption/energy expenditure (y-axis). A patient with a hip fusion has a highly inefficient gait with large vertical displacement due to vaulting and hip hiking, placing them in the upper right quadrant, representing high values for both variables.
Question 76
What critical component of energy-efficient normal gait is completely obliterated by a hip arthrodesis, leading to compensatory vaulting and hip hiking?
View Answer & Explanation
Correct Answer: C
Rationale: The text emphasizes that in normal gait, a "gradual, controlled pelvic drop on the swinging side" is crucial for minimizing vertical excursion and allowing foot clearance. When a hip is fused, the pelvis becomes a rigid extension of the femur, and this elegant, energy-saving mechanism is "entirely obliterated."
Question 77
A 25-year-old female has a 3 cm leg length discrepancy (LLD), with the right leg being shorter. She compensates by walking on the toes of her right foot. This compensation requires adequate strength of which muscle group?
View Answer & Explanation
Correct Answer: D
Rationale: Compensating for an LLD with an equinus posture on the short side requires the patient to toe-walk. This position must be held against the body's weight during the stance phase, which necessitates robust plantar flexor (gastrocnemius-soleus complex) strength. Weakness would cause the ankle to collapse into dorsiflexion.
Question 78
A 65-year-old male with a 4 cm LLD (left leg longer) has been compensating for years by flexing his left knee during gait. He now presents with new-onset, debilitating anterior left knee pain, forcing him to use a cane. What is the most likely cause of his new symptoms?
View Answer & Explanation
Correct Answer: C
Rationale: Compensating for LLD by flexing the long-side knee places the ground reaction vector posterior to the knee, creating a massive flexion moment that requires intense quadriceps contraction. This "exponentially increases patellofemoral joint reactive forces," leading to pain and accelerated degeneration, which is a common reason older patients abandon this strategy.
Question 79
A patient with a 3 cm LLD (left leg shorter) is unable to compensate with an equinus posture due to a stiff ankle. To compensate via pelvic tilt, which combination of muscular actions is required?
View Answer & Explanation
Correct Answer: B
Rationale: The text specifies that for the pelvis to tilt downward on the short side, two actions are essential: "hip abduction on the short side and hip adduction on the long side." An adduction contracture on the short leg would mechanically block this compensation.
Question 80
A 17-year-old female presents with bilateral knee pain. Examination reveals increased femoral anteversion and compensatory external tibial torsion. Her foot progression angle during gait appears relatively normal. What is the classic term for this condition?
View Answer & Explanation
Correct Answer: C
Rationale: Miserable malalignment syndrome is the classic orthopedic term for the combination of increased femoral anteversion (internal rotation of the femur) and compensatory external tibial torsion. This creates a rotational conflict at the knee, leading to patellofemoral pain, despite a potentially normal foot progression angle.
Question 81
During the stance phase of gait, the knee is flexed approximately 20 degrees and the "screw-home mechanism" is engaged. What is the approximate range of axial rotation available at the knee in this position?
View Answer & Explanation
Correct Answer: A
Rationale: The text states that during the load-bearing stance phase, as the knee approaches full extension, the screw-home mechanism locks the joint, "permitting a mere 3 degrees of tibial rotation." This is why the knee is structurally incapable of effectively compensating for rotational deformities during weight-bearing.
Question 82
A patient has internal tibial torsion combined with excessive femoral anteversion. How is this type of multi-segmental rotational deformity best classified?
View Answer & Explanation
Correct Answer: B
Rationale: An additive deformity is when both the femoral and tibial segments are rotated in the same direction (in this case, internally). This results in a compounding, clinically obvious in-toeing gait. A compensatory deformity (A, C) is when the rotations oppose each other.
Question 83
A 30-year-old patient with a 6 cm LLD is evaluated in the gait lab. Without a shoe lift, the vertical excursion of his center of gravity is measured. Compared to a normal individual's excursion of 5 cm, what is the expected excursion for this patient?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that in the presence of a significant LLD, the normal vertical excursion of the center of gravity (5 cm) "can double, increasing by as much as 10 cm if left uncompensated." This massive increase in vertical displacement leads to a spike in energy consumption.
Question 84
A patient with a "short leg gait" due to a 2.5 cm LLD is observed. Which of the following is a characteristic finding of this gait pattern compared to normal gait?
View Answer & Explanation
Correct Answer: D
Rationale: A short leg gait is characterized by reduced stance time and reduced stride length on the short side, along with an increased cadence. This is distinct from an antalgic gait, where stride length is reduced on the normal side to get off the painful limb quickly.
Question 85
A 72-year-old patient with a history of polio has profound quadriceps weakness and a 3 cm LLD (right leg longer). Which compensatory mechanism for the LLD will this patient be unable to utilize effectively?
View Answer & Explanation
Correct Answer: C
Rationale: Compensating by flexing the knee on the long side is highly demanding on the quadriceps. The text states, "If the quadriceps are weak... the patient cannot adopt this posture due to a fear of the knee collapsing." Therefore, this patient's quadriceps weakness prevents the use of this specific mechanism.
Question 86
Why is a casual observation of the foot progression angle potentially misleading in a patient with miserable malalignment syndrome?
View Answer & Explanation
Correct Answer: C
Rationale: In miserable malalignment, the internal rotation from femoral anteversion is opposed by the external tibial torsion. The text notes that in this compensatory scenario, "the final foot progression angle may appear deceptively normal to a casual observer," masking the severe rotational conflict occurring at the knee.
Question 87
A 60-year-old female with a left hip FFD and a fused lumbar spine presents with a crouched gait. This "mass flexion" pattern involves forced knee flexion and what corresponding motion at the ankle?
View Answer & Explanation
Correct Answer: B
Rationale: The text defines the two components of mass flexion: 1. Forced Knee Flexion and 2. Forced Ankle Dorsiflexion. The ankle must dorsiflex to accommodate the flexed knee while keeping the foot flat on the ground.
Question 88
A 45-year-old male undergoes a gait analysis, which is determined to be normal and energy-efficient. During the initial contact (heel strike) phase of his gait, what is the position of the Ground Reaction Vector (GRV) relative to the knee joint center and the resulting external moment?

View Answer & Explanation
Correct Answer: B
Rationale: During initial contact, the GRV passes anterior to the knee joint center. This creates an external extension moment, which passively stabilizes the knee and minimizes the need for quadriceps activation. A GRV posterior to the knee (Option A) is characteristic of a knee flexion deformity and creates a destabilizing flexion moment.
Question 89
A 30-year-old female is evaluated for a normal gait pattern. Her biomechanics demonstrate optimal muscle function. During initial contact to mid-stance, the Ground Reaction Vector (GRV) passes anterior to her hip joint. This requires counteraction by which of the following muscle groups to prevent collapse?
View Answer & Explanation
Correct Answer: D
Rationale: When the GRV passes anterior to the hip joint center, it creates an external flexion moment. This moment must be counteracted by the powerful hip extensor muscles, such as the gluteus maximus and hamstrings, to maintain an upright posture. The hip flexors (Option A) would exacerbate the flexion moment.
Question 90
A 55-year-old patient demonstrates a highly efficient gait with minimal energy expenditure. The key to this efficiency is passive stability during terminal stance. This is achieved when the Ground Reaction Vector (GRV) shifts to what position relative to the hip joint?
View Answer & Explanation
Correct Answer: E
Rationale: The hallmark of energy efficiency in terminal stance is the posterior shift of the GRV relative to the hip joint. This creates a powerful external extension moment that is passively resisted by the tension in the anterior hip capsule and the iliofemoral ligament (Y-ligament of Bigelow), requiring virtually no active muscle contraction. An anterior GRV (Option A) requires active hip extensor muscle firing.
Question 91
A 14-year-old boy with cerebral palsy presents with a crouched gait and complains of severe anterior thigh fatigue after walking short distances. A gait analysis confirms a fixed knee flexion deformity. During the stance phase, where is the Ground Reaction Vector (GRV) located relative to his knee joint?

View Answer & Explanation
Correct Answer: B
Rationale: In a fixed knee flexion deformity, the GRV falls far posterior to the knee's center of rotation throughout the stance phase. This creates a massive, relentless external flexion moment that constantly tries to buckle the knee. An anterior GRV (Option A) is seen in normal gait and genu recurvatum, which creates a stabilizing extension moment.
Question 92
A 68-year-old female with a 20-degree fixed knee flexion contracture reports debilitating fatigue. Biomechanically, this fatigue is a direct result of the high metabolic cost required to prevent the knee from collapsing. Which muscle group is forced into a continuous, high-force isometric contraction to counteract the abnormal external moment?
View Answer & Explanation
Correct Answer: C
Rationale: The posterior position of the GRV in a knee flexion deformity creates a constant external flexion moment. To prevent the knee from buckling into further flexion, the patient must fire their quadriceps muscle continuously and with maximum force. This prolonged isometric contraction is metabolically exhausting and explains the patient's fatigue. The hamstrings (Option A) are knee flexors and would worsen the collapse.
Question 93
A 16-year-old male with post-traumatic genu recurvatum is observed to "lock" his knee in maximum hyperextension during stance. This compensatory strategy relies on which structures to provide stability against the anteriorly shifted mechanical axis?

View Answer & Explanation
Correct Answer: D
Rationale: In genu recurvatum, the GRV passes far anterior to the knee, creating a strong extension (hyperextension) moment. To prevent further collapse, the patient relies entirely on the passive tension of the posterior soft tissues, primarily the posterior capsule and the cruciate ligaments (ACL and PCL). The quadriceps (Option A) would exacerbate the hyperextension.
Question 94
A 72-year-old male has a significant hip flexion deformity secondary to osteoarthritis. During gait, he is unable to achieve adequate hip extension in terminal stance. This biomechanical failure prevents the Ground Reaction Vector (GRV) from passing posterior to the hip joint. What is the primary consequence of this?

View Answer & Explanation
Correct Answer: C
Rationale: The inability to achieve terminal hip extension means the GRV never passes posterior to the hip. Consequently, the patient completely loses the passive energy storage and release mechanism provided by the tensioning of the iliofemoral (Y) ligament. This forces a more metabolically costly, purely muscular gait. Over-reliance on quadriceps (Option A) is characteristic of a knee flexion deformity.
Question 95
A 9-year-old child with a spastic equinus deformity makes initial contact with the forefoot instead of the heel. According to the principles of gait rockers, this deformity completely destroys which rocker?
View Answer & Explanation
Correct Answer: A
Rationale: The first rocker, or heel rocker, is the period from initial contact to foot flat, where the body rolls over the rounded calcaneus. Ankle equinus forces a forefoot or midfoot initial contact, completely bypassing and thus destroying the heel rocker. This eliminates the normal shock-absorbing mechanism of heel strike.
Question 96
A 25-year-old patient with a rigid ankle equinus deformity is noted to have a significantly shortened step length with the contralateral limb. This is a direct consequence of the equinus deformity blocking which critical event during the stance phase?
View Answer & Explanation
Correct Answer: C
Rationale: The primary reason equinus reduces contralateral step length is its interference with the second (ankle) rocker. The second rocker is defined by the forward progression of the tibia over the fixed foot, which requires ankle dorsiflexion. Since equinus blocks dorsiflexion, tibial advancement is halted, which in turn limits how far the opposite leg can swing forward.
Question 97
A patient with a knee flexion deformity is observed to walk with a forward trunk lean. What is the biomechanical purpose of this compensation?
View Answer & Explanation
Correct Answer: C
Rationale: In a knee flexion deformity, the GRV is posterior to the knee, creating a large flexion moment that the quadriceps must fight. By leaning the trunk forward, the patient shifts their overall center of mass anteriorly. This moves the GRV forward, shortening the lever arm of the external flexion moment and providing some relief to the overworked quadriceps.
Question 98
The passive, metabolic-free "boost" that helps initiate hip flexion for the swing phase is generated by the release of stored elastic potential energy from which structure?
View Answer & Explanation
Correct Answer: C
Rationale: During terminal stance, full hip extension places the powerful iliofemoral ligament (Y-ligament of Bigelow) under immense tension, storing elastic potential energy like a spring. As the limb transitions to pre-swing, this energy is released, providing a passive boost that helps initiate hip flexion, significantly reducing the work required by the iliopsoas muscle.
Question 99
A 17-year-old patient with Charcot-Marie-Tooth disease exhibits a high-steppage gait. This gait modification is a necessary swing-phase compensation for what underlying problem?

View Answer & Explanation
Correct Answer: B
Rationale: A high-steppage gait, characterized by exaggerated hip and knee flexion during the swing phase, is a classic compensation to ensure the foot clears the ground. It is most commonly seen in conditions that cause foot drop or an equinus deformity, where passive ankle dorsiflexion is insufficient to prevent the toes from dragging.
Question 100
According to the provided text, the Ground Reaction Vector (GRV) is the embodiment of which physical law as applied to human locomotion?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that the GRV is the literal embodiment of Newton's third law of motion. As the foot exerts a force (action) on the ground, the ground exerts an equal and opposite force (reaction) back onto the foot. This reactive force is the GRV.
You Might Also Like
