Comprehensive Orthopedic Deformity, LLD & Hip Biomechanics Board Review | Part 13
Key Takeaway
ABOS Orthopedic Board Review Part 13 covers advanced deformity correction, limb length discrepancy (LLD) management, and hip biomechanics. Topics include Paley's principles, malunion osteotomy strategies, pelvic support osteotomy (PSO), and distraction osteogenesis, providing critical knowledge for orthopedic specialists and exam preparation.
Question 1
A 50-year-old man with osteonecrosis develops pseudo-subluxation. Radiographs show a 1.5 cm superior migration of the femoral head. This finding directly contributes to which of the following clinical and biomechanical consequences?
View Answer & Explanation
Correct Answer: A
Rationale: The superior migration of the collapsed femoral head directly shortens the effective length of the limb from the hip to the ankle. This creates a functional leg length discrepancy (LLD), which alters gait and can cause secondary problems in the spine and contralateral limb. Superior migration *reduces* the ATD (C).
Question 2
A 10-year-old boy has severe Perthes disease. A surgeon considers a varus derotational osteotomy (VDRO). In the setting of a severely flattened and extruded femoral head, what is the most significant risk of this procedure?
View Answer & Explanation
Correct Answer: C
Rationale: The text warns that in the face of severe collapse, a VDRO can be detrimental. It may drive the flattened, incongruent head into the lateral edge of the acetabulum, creating a fulcrum effect (hinge abduction). This concentrates pressure on the acetabular rim and accelerates degenerative changes, rather than achieving true containment.
Question 3
During the biological process of "creeping substitution" in Perthes disease, the structural integrity of the subchondral bone is compromised. This phase makes the femoral head highly vulnerable to collapse under which type of force?
View Answer & Explanation
Correct Answer: C
Rationale: The text explains that during the vulnerable phase of creeping substitution, the weakened segment collapses under physiological load, which is exacerbated by the forces of walking and muscle contraction. This is the fundamental principle behind offloading treatments like femoropelvic distraction.
Question 4
A 13-year-old with pseudo-subluxation has a standing AP pelvis radiograph showing a significant break in Shenton's line and an increased distance between the medial femoral head and the pelvic teardrop. The increased teardrop distance is a direct radiographic sign of what component of the deformity?
View Answer & Explanation
Correct Answer: D
Rationale: As the femoral head displaces superiorly and laterally, it moves away from the medial wall of the pelvis (the teardrop). This creates an apparent widening of the medial joint space, which is objectively measured as an increased teardrop distance. It is a classic sign of lateralization of the femoral head.
Question 5
A resident is evaluating a patient with a painful limp and abductor lurch. They are measuring the Articulo-Trochanteric Distance (ATD) on an AP radiograph. This distance is measured between the tip of the greater trochanter and the:
View Answer & Explanation
Correct Answer: B
Rationale: The text defines the Articulo-Trochanteric Distance (ATD) as the distance from the tip of the greater trochanter to the superior articular surface of the femoral head. This measurement is a critical indicator of the mechanical lever arm for the hip abductor muscles.
Question 6
A 35-year-old male presents with a painful varus malunion of his mid-shaft tibia following a motorcycle accident 1 year ago. Radiographs demonstrate both varus angulation and lateral translation. When the proximal and distal anatomical axes are drawn, they intersect at a point distal to the original fracture site. What is the correct term for this intersection point?
View Answer & Explanation
Correct Answer: B
Rationale: When both angulation and translation are present, the intersection of the proximal and distal anatomical axes is defined as the angulation-translation CORA (a-t CORA). The standard CORA applies only to pure angular deformities where the axes intersect at the apex of the deformity.
Question 7
A 42-year-old female is undergoing preoperative planning for a femoral malunion with both valgus angulation and medial translation. The surgeon plans to perform a single-cut osteotomy precisely at the a-t CORA. According to the principles of deformity correction, what is the primary geometric outcome of this surgical strategy?
View Answer & Explanation
Correct Answer: C
Rationale: According to Rule 1 of a-t deformity correction, an osteotomy and hinge placed exactly at the a-t CORA will simultaneously correct both the angular and translational components of the deformity through a single rotational movement. This strategy does not, however, eliminate the original cosmetic bump or create a straight canal for nailing.
Question 8
A 28-year-old construction worker has a symptomatic malunion of his tibia with a prominent, painful medial bump. He is very concerned about the cosmetic appearance. The surgeon plans an osteotomy at the point of maximum translation (the original fracture site). Which of the following is the primary advantage of this approach?
View Answer & Explanation
Correct Answer: C
Rationale: Performing the osteotomy at the point of maximum translation allows the surgeon to physically shave down the sclerotic edges and translate the bone to a flush position, completely eliminating the medial bump. The main disadvantage is that it requires sequential correction (translation and angulation) and involves operating in the zone of injury.
Question 9
A 30-year-old patient requires correction of a femoral angulation-translation deformity. The surgeon chooses to perform the osteotomy at the point of maximum translation to facilitate fixation with an intramedullary nail (IMN). What is the major biomechanical advantage of this fixation method in this context?
View Answer & Explanation
Correct Answer: C
Rationale: By re-canalizing the bone at the malunion site, an intramedullary nail can be inserted. IMN offers excellent load-sharing properties, which promotes healing and allows for earlier weight-bearing compared to plates or external fixators. An IMN cannot be used with an osteotomy at the a-t CORA due to the resulting "zig-zag" deformity of the canal.
Question 10
A 55-year-old woman with a tibial malunion has significant varus angulation in the frontal plane but only 4 mm of anterior translation in the sagittal plane. The surgeon plans to correct the varus deformity perfectly but leave the small sagittal translation. Which multi-planar correction strategy does this represent?
View Answer & Explanation
Correct Answer: A
Rationale: Strategy 1, the "Accept and Ignore" approach, is used when one component of a multi-planar deformity is clinically and functionally insignificant. A small sagittal translation (e.g., 4 mm) rarely affects the mechanical axis deviation and can be safely ignored to simplify the surgery and reduce morbidity.
Question 11
A surgeon is planning an osteotomy for a tibial malunion at the a-t CORA. The patient has a history of an open fracture with a compromised, adherent scar over the original malunion site. What is the primary biological advantage of choosing the a-t CORA strategy in this patient?
View Answer & Explanation
Correct Answer: C
Rationale: The most significant advantage of the a-t CORA strategy is biological safety. The a-t CORA is often located away from the original fracture site, allowing the surgeon to operate through pristine, uninjured soft tissues. This drastically reduces the risk of wound breakdown and deep infection, which is a major concern in patients with compromised soft tissues.
Question 12
A 25-year-old athlete has a femoral malunion and desires fixation with an intramedullary nail. The surgeon performs an osteotomy at the point of maximum translation. During the acute intraoperative correction, what is the recommended sequence of maneuvers?
View Answer & Explanation
Correct Answer: B
Rationale: For acute corrections performed at the malunion site, it is highly preferable to perform translation first, then angulation. Translating the bone ends acutely lines up the medullary canal, which then facilitates the angular correction and subsequent insertion of the intramedullary nail. Reversing the order can make canal alignment difficult.
Question 13
A 40-year-old patient is undergoing gradual correction of a tibial angulation-translation deformity using an Ilizarov circular external fixator. The osteotomy was made at the point of maximum translation. What is the recommended sequence of correction when using this gradual method?
View Answer & Explanation
Correct Answer: A
Rationale: For gradual corrections with an external fixator, the reverse of acute correction is true. It is biomechanically safer to perform angulation first, then translation. Angulating first creates a wedge of regenerate bone, which provides a larger surface area and reduces the risk of the bone ends slipping off one another during the subsequent translation.
Question 14
A surgeon performs an osteotomy at the a-t CORA to correct a femoral malunion and fixes it with a locking plate. Postoperatively, the mechanical axis is perfectly restored. What is the most likely patient complaint related to this specific surgical strategy?
View Answer & Explanation
Correct Answer: C
Rationale: A major drawback of the a-t CORA strategy is that the original malunion site is left untouched. This leaves the physical "step-off" or bump of the malunited bone, which can be symptomatic or aesthetically displeasing, especially in subcutaneous locations like the medial tibia.
Question 15
A 33-year-old male has a complex tibial malunion with significant varus angulation, recurvatum, and lateral translation. The surgeon plans to use Strategy 2 (Frontal Plane a-t Point as Primary Apex). After the oblique plane angular correction at this level, which deformity component will be fully corrected?
View Answer & Explanation
Correct Answer: D
Rationale: In Strategy 2, an oblique plane angular correction at the frontal a-t CORA simultaneously corrects both the frontal (varus) and sagittal (recurvatum) components of angulation. Because the cut is at the frontal a-t CORA, the frontal plane translation is also eliminated. The sagittal plane translation is what remains to be corrected.
Question 16
Following the application of Strategy 2 for a multi-planar deformity, a residual sagittal translation remains. The surgeon must now slide the bone fragments to correct this. What is the absolute limiting factor for this translational maneuver?
View Answer & Explanation
Correct Answer: C
Rationale: The limiting factor for any translational correction is maintaining adequate bone-to-bone contact. If the required translation is too large (typically >30-40% of the bone diameter), sliding the fragments will result in a loss of cortical contact, leading to instability and a high risk of non-union.
Question 17
A 45-year-old patient has a severe, multi-planar femoral malunion. The surgeon plans to correct the deformity through the malunion site (Strategy 4) and use an intramedullary nail. This strategy is based on identifying and correcting the deformity in which plane?
View Answer & Explanation
Correct Answer: D
Rationale: Strategy 4 recognizes that a multi-planar deformity (e.g., varus and recurvatum) exists as a single, pure angular deformity in a specific oblique plane. By calculating this true oblique plane axis, the surgeon can perform a single oblique-plane angular correction followed by multi-planar translation, which is ideal for restoring the anatomical canal for IM nailing.
Question 18
A 29-year-old patient presents with a massive tibial deformity with 30 degrees of varus, 25 degrees of procurvatum, and 3 cm of lateral translation. Attempting correction at a single level would result in complete loss of bone contact. Which of the following is the most appropriate surgical strategy?
View Answer & Explanation
Correct Answer: D
Rationale: Strategy 5, the double osteotomy approach, is reserved for massive, complex deformities where a single osteotomy would be biomechanically untenable. By creating two separate osteotomies (e.g., one at the frontal a-t level and one at the sagittal a-t level), the correction is divided into two manageable zones, preserving bone contact and protecting soft tissues. This is almost exclusively managed with a hexapod external fixator.
Question 19
During preoperative planning for a lower extremity malunion, what is the most critical radiographic study required to assess the Mechanical Axis Deviation (MAD)?
View Answer & Explanation
Correct Answer: C
Rationale: The Mechanical Axis Deviation (MAD) is the perpendicular distance from the mechanical axis of the limb (a line from the center of the femoral head to the center of the ankle) to the center of the knee. This can only be accurately assessed on a full-length standing radiograph that visualizes the hip, knee, and ankle joints simultaneously.
Question 20
An osteotomy at the a-t CORA creates a "zig-zag" deformity of the medullary canal. This anatomical change makes which form of fixation mechanically impossible?
View Answer & Explanation
Correct Answer: D
Rationale: The "zig-zag" deformity created by an osteotomy at the a-t CORA involves two opposing kinks in the bone. Passing a straight, rigid intramedullary nail through this S-shaped canal is impossible without iatrogenic fracture. Therefore, this strategy is reserved for plate or external fixation.
Question 21
A 60-year-old diabetic patient with poor skin quality has a tibial malunion. The surgeon is concerned about wound healing and infection. Which osteotomy strategy offers the greatest biological safety margin?
View Answer & Explanation
Correct Answer: B
Rationale: The a-t CORA strategy is biologically safest because the osteotomy is typically performed in a region of healthy bone and soft tissue, away from the compromised "zone of injury" of the original malunion. This is particularly advantageous in patients with risk factors for poor wound healing, such as diabetes or poor skin quality.
Question 22
According to Paley's principles, a mechanical axis deviation (MAD) of what magnitude is considered the threshold for significantly increasing load on the medial compartment of the knee and accelerating osteoarthritis?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that a mechanical axis deviation (MAD) of more than 15 mm into the medial compartment of the knee increases the load on the medial meniscus and articular cartilage exponentially. This is a key threshold used in deformity planning to determine the necessity of correction for joint preservation.
Question 23
A patient has a femoral malunion with varus angulation and medial translation. How does this combination of deformities typically affect the mechanical axis deviation (MAD)?
View Answer & Explanation
Correct Answer: B
Rationale: Varus angulation shifts the mechanical axis medially. Medial translation also shifts the mechanical axis medially. When both occur together, their effects are additive, compounding the deformity and creating a large medial mechanical axis deviation (MAD).
Question 24
A surgeon is planning a multi-planar deformity correction using Strategy 3 (Sagittal Plane a-t Point as Primary Apex). After the oblique plane angular correction, which residual deformity must be addressed by sliding the bone fragments?
View Answer & Explanation
Correct Answer: C
Rationale: Strategy 3 is the inverse of Strategy 2. The osteotomy is performed at the sagittal a-t CORA, which corrects all angulation and the sagittal translation. This leaves a residual translation in the frontal plane (AP radiograph) that must be corrected by physically sliding the bone.
Question 25
A 50-year-old male has a tibial malunion. Preoperative planning reveals an abnormal Medial Proximal Tibial Angle (MPTA). The ultimate goal of deformity correction is to restore both the mechanical axis and the normal joint orientation angles. Why is restoring the MPTA critical even if the MAD is corrected?
View Answer & Explanation
Correct Answer: C
Rationale: Even if the mechanical axis is restored (correcting compressive forces), an abnormal joint orientation angle (like the MPTA) will lead to pathological shear forces across the joint cartilage during the gait cycle. Restoring both the mechanical axis and the joint orientation angles is the only way to fully normalize joint biomechanics and prevent premature osteoarthritis.
Question 26
A 22-year-old patient with a diaphyseal femoral malunion is treated with an osteotomy at the point of maximum translation. The surgeon uses a locking plate for fixation. What is a potential disadvantage of using a plate in this scenario compared to an IM nail?
View Answer & Explanation
Correct Answer: B
Rationale: While locking plates provide excellent rigid fixation, they are load-bearing devices that typically require a larger surgical incision compared to percutaneous nailing techniques. Additionally, the plate itself can be prominent under the skin, especially over a translated segment, which can be a source of irritation for the patient.
Question 27
A 35-year-old female presents with progressive right hip pain and a limp. On examination, she has a positive Trendelenburg sign. Radiographs are obtained for preoperative planning of a proximal femoral osteotomy. The surgeon identifies the line connecting the center of the femoral head to the center of the ankle plafond. This line represents which of the following?
View Answer & Explanation
Correct Answer: B
Rationale: The mechanical axis of the lower extremity is the weight-bearing line connecting the center of the femoral head to the center of the ankle. The anatomic axis (A) follows the medullary canal of the femur. Restoring the mechanical axis is a primary goal of deformity correction.
Question 28
A 28-year-old male with a history of developmental dysplasia of the hip (DDH) is evaluated for a corrective osteotomy. The surgeon measures the angle formed by the mechanical axis of the femur and a line from the tip of the greater trochanter to the center of the femoral head. What is this critical angle called?
View Answer & Explanation
Correct Answer: C
Rationale: The Mechanical Lateral Proximal Femoral Angle (mLPFA) is the cornerstone measurement for proximal femoral deformity analysis, as it defines the relationship of the proximal femur to the weight-bearing axis. The Neck-Shaft Angle (A) is related but is measured against the anatomic, not mechanical, axis.
Question 29
A 17-year-old female is being evaluated for mild hip pain. A standing full-length radiograph of her lower extremities is obtained. Her overall limb alignment is neutral. Measurement of her mechanical Lateral Proximal Femoral Angle (mLPFA) is most likely to fall within which range?
View Answer & Explanation
Correct Answer: B
Rationale: The normal range for the mLPFA is 85° to 95°. Values below this range indicate coxa valga, while values above this range indicate coxa vara. The range of 120° to 135° (D) is typical for the neck-shaft angle, not the mLPFA.
Question 30
A 14-year-old boy presents with a waddling gait and bilateral hip pain. Radiographs reveal a decreased neck-shaft angle of 105°. When measuring his mechanical Lateral Proximal Femoral Angle (mLPFA), what value would be most consistent with this diagnosis of coxa vara?
View Answer & Explanation
Correct Answer: D
Rationale: Coxa vara is characterized by an increased mLPFA, typically greater than 95°. An mLPFA of 110° is a classic finding in coxa vara. A value of 80° (A) would be indicative of coxa valga.
Question 31
A 22-year-old female with cerebral palsy is evaluated for hip instability and pain. Her radiographs demonstrate a neck-shaft angle of 145° and superolateral subluxation of the femoral head. Her mechanical Lateral Proximal Femoral Angle (mLPFA) is expected to be:
View Answer & Explanation
Correct Answer: A
Rationale: Coxa valga, which is common in cerebral palsy and characterized by an increased neck-shaft angle, results in a decreased mLPFA (<85°). An increased mLPFA (C) is seen in coxa vara.
Question 32
A resident is explaining the biomechanics of the hip joint to a medical student. They describe the hip as a class one lever system. In this model, what anatomical structure serves as the fulcrum?
View Answer & Explanation
Correct Answer: B
Rationale: In the class one lever system of the hip, the center of the femoral head acts as the fulcrum. The body weight acts as the load, and the abductor muscle force acts as the effort applied at the greater trochanter (A).
Question 33
During a biomechanics lecture, the Joint Reaction Force (JRF) across the hip during single-leg stance is discussed. The JRF is correctly described as the sum of which two forces?
View Answer & Explanation
Correct Answer: C
Rationale: The total Joint Reaction Force (JRF) across the hip articular cartilage is the sum of the body weight and the force generated by the abductor muscles to keep the pelvis level. Because the abductors have a short moment arm, their force is typically 2-3 times body weight, making the JRF immense.
Question 34
A 30-year-old female with DDH presents with a valgus hip deformity (mLPFA of 75°). How does this deformity primarily affect the biomechanics of her hip abductors?
View Answer & Explanation
Correct Answer: B
Rationale: Coxa valga lateralizes the femoral shaft relative to the head, which critically shortens the horizontal distance from the femoral head (fulcrum) to the greater trochanter (abductor insertion). This shortens the abductor moment arm, forcing the muscles to work much harder and increasing the JRF.
Question 35
A 19-year-old male is diagnosed with severe coxa vara (mLPFA of 115°). This deformity causes a characteristic shift in the overall limb alignment. What is the expected Mechanical Axis Deviation (MAD) in this patient?
View Answer & Explanation
Correct Answer: B
Rationale: The varus alignment of the proximal femur in coxa vara medializes the entire mechanical axis of the lower limb, resulting in a medial Mechanical Axis Deviation (MAD). This places the weight-bearing line medial to the center of the knee.
Question 36
A 26-year-old female with a known history of DDH presents with worsening hip pain and a feeling of instability. On examination, she has a positive Trendelenburg gait. Radiographs reveal a neck-shaft angle of 150° and an mLPFA of 80°. What is the correct diagnosis for her proximal femoral deformity?
View Answer & Explanation
Correct Answer: B
Rationale: The combination of an increased neck-shaft angle (>140°) and a decreased mLPFA (<85°) is the classic definition of coxa valga. Coxa vara (A) would present with a decreased neck-shaft angle and an increased mLPFA.
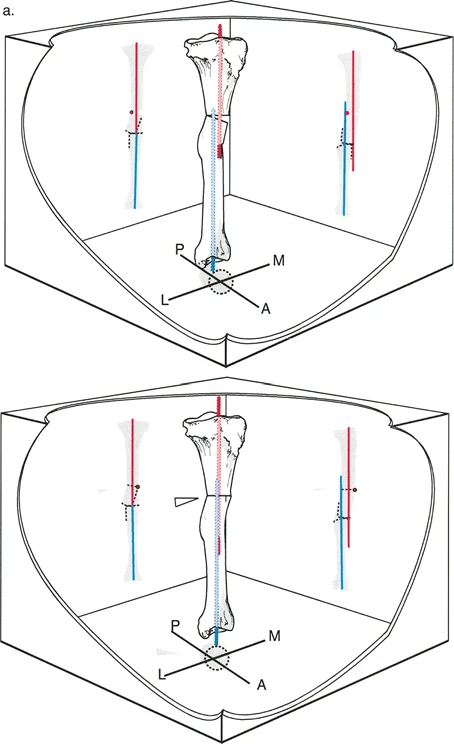
Question 37
A 24-year-old female with a dysplastic acetabulum and coxa valga is shown in the top image. What is the primary biomechanical consequence of her proximal femoral deformity that leads to superolateral subluxation?

View Answer & Explanation
Correct Answer: B
Rationale: The valgus deformity shortens the abductor moment arm, which severely weakens the abductor muscles' ability to stabilize the pelvis and compress the femoral head into the acetabulum. This abductor insufficiency is a primary driver of the superolateral subluxation seen in the image.
Question 38
A surgeon is planning a varus-producing osteotomy for a patient with coxa valga. The diagram illustrates the biomechanical changes. Based on the diagram, what is the primary goal of lateralizing the greater trochanter?

View Answer & Explanation
Correct Answer: C
Rationale: As shown in the transition from the center to the right image, the varus osteotomy lateralizes the greater trochanter. This increases the horizontal distance from the fulcrum (femoral head) to the abductor insertion, thereby lengthening the abductor moment arm. This gives the muscles a mechanical advantage, requiring less force to stabilize the pelvis and thus reducing the overall JRF.
Question 39
A 29-year-old female with DDH and symptomatic coxa valga undergoes the surgical procedure shown. The postoperative radiograph (bottom) demonstrates improved femoral head coverage and containment. Which of the following procedures was most likely performed?
View Answer & Explanation
Correct Answer: C
Rationale: The text specifically describes the Nishio helical dome osteotomy as a powerful solution for coxa valga and anteversion, as seen in the clinical example. The postoperative image shows correction on the femoral side of the joint, making a pelvic osteotomy like a PAO (A) or Salter (B) incorrect. A valgus osteotomy (D) would worsen the deformity.
Question 40
A senior surgeon is teaching a fellow about the technical aspects of the Nishio osteotomy for correcting coxa valga with excessive anteversion. What is the defining geometric characteristic of the bone cut in this procedure?
View Answer & Explanation
Correct Answer: D
Rationale: The Nishio osteotomy is specifically defined by its sophisticated helical or dome-shaped cut made at the base of the femoral neck. This unique geometry allows for simultaneous varus and derotational correction without creating a large bone gap or causing significant shortening.
Question 41
A 31-year-old patient with DDH and coxa valga is a candidate for a varus-producing proximal femoral osteotomy. A surgeon chooses to perform a Nishio osteotomy instead of a traditional lateral closing-wedge osteotomy. What is a major biomechanical advantage of the Nishio technique in this scenario?
View Answer & Explanation
Correct Answer: C
Rationale: A key advantage of the Nishio osteotomy is its ability to correct the deformity while minimizing proximal migration of the greater trochanter. This preserves the physiological length-tension relationship (Blix curve) of the abductor muscles, preventing the iatrogenic weakness often seen with traditional closing-wedge osteotomies.
Question 42
A 25-year-old undergoes a traditional lateral closing-wedge varus osteotomy for coxa valga. Postoperatively, despite a normalized mLPFA, the patient continues to have a significant Trendelenburg gait. This is most likely due to which iatrogenic change?
View Answer & Explanation
Correct Answer: B
Rationale: Traditional closing-wedge osteotomies often cause the greater trochanter to migrate proximally relative to the center of the femoral head. This slackens the abductor muscles, placing them on an unfavorable portion of the Blix curve and causing persistent weakness, even with corrected bony alignment. The Nishio osteotomy is designed to avoid this specific complication.
Question 43
A 27-year-old undergoes a Nishio varus osteotomy for coxa valga. The procedure successfully rotates the femoral shaft medially under the femoral head along the dome-shaped cut. This maneuver has what intended effect on the abductor moment arm?
View Answer & Explanation
Correct Answer: C
Rationale: By medially translating the femoral shaft, the greater trochanter is effectively lateralized relative to the center of the femoral head. This dramatically increases the horizontal distance between the fulcrum and the abductor insertion, thus lengthening the abductor moment arm and improving mechanical efficiency.
Question 44
A 33-year-old patient with painful coxa valga undergoes a successful varus-producing osteotomy that effectively lengthens the abductor moment arm. This surgical correction leads to a direct reduction in which of the following biomechanical forces?
View Answer & Explanation
Correct Answer: C
Rationale: By increasing the abductor moment arm, the abductor muscles need to generate substantially less force to balance the pelvis. Since the Joint Reaction Force (JRF) is the sum of body weight and abductor force, a significant reduction in the required abductor force directly and drastically reduces the overall JRF, protecting the articular cartilage.
Question 45
A 14-year-old girl with a history of a Salter-Harris III fracture of the distal femur presents with a limp. Clinical examination reveals a limb length discrepancy (LLD). According to the principles outlined in the text, LLD is fundamentally defined by which two distinct parameters?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that LLD is a "complex, multi-dimensional deformity defined fundamentally by two distinct parameters: magnitude and direction." Magnitude is the quantitative difference, and direction refers to whether it is shortening or overgrowth and its interaction with other deformities.
Question 46
A 10-year-old boy with fibular hemimelia has a current LLD of 3 cm. The surgeon wishes to predict the discrepancy at skeletal maturity to plan the timing of a future epiphysiodesis. According to the provided text, which method is considered the modern gold standard for this prediction?
View Answer & Explanation
Correct Answer: C
Rationale: The text identifies the Paley Multiplier Method as the "modern gold standard" for predicting LLD at skeletal maturity, noting its speed and accuracy compared to older methods like the Anderson, Green, and Messner charts or the Moseley graph.
Question 47
A 45-year-old man with a 2.5 cm LLD from a healed femoral shaft fracture complains of back pain. During the clinical evaluation, the surgeon places calibrated blocks under the shorter limb until the patient reports feeling level and the iliac crests are aligned. What is the primary purpose of this "functional block test"?
View Answer & Explanation
Correct Answer: B
Rationale: The text emphasizes that the block test is paramount because it "reveals the tolerable correction, which may differ significantly from the radiographic correction," especially in adults with long-standing discrepancies and compensatory mechanisms.
Question 48
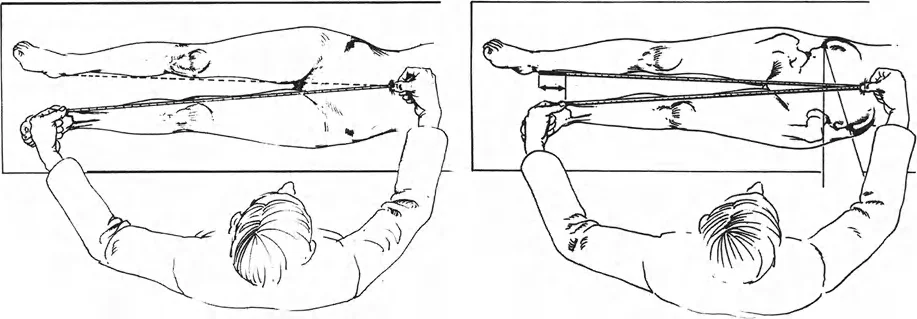
A 16-year-old boy is being evaluated for a gait abnormality. On examination, the measurement from the anterosuperior iliac spine (ASIS) to the medial malleolus (MM) is 88 cm on the right and 85 cm on the left. The measurement from the umbilicus to the MM is 95 cm on the right and 92 cm on the left. What type of limb length discrepancy does this patient have?
View Answer & Explanation
Correct Answer: B
Rationale: The measurement from the ASIS to the MM represents the "True LLD." A difference in this measurement (88 cm vs. 85 cm) indicates a structural difference in bone length. The difference in the umbilicus-to-MM measurement is consistent with this true shortening, not an apparent discrepancy.
Question 49
A 22-year-old woman presents with low back pain and a sensation of having one leg shorter than the other. Clinical measurement from the ASIS to the medial malleolus is equal bilaterally. However, measurement from the umbilicus to the medial malleolus reveals a 2 cm difference. Which of the following is the most likely cause of this finding?
View Answer & Explanation
Correct Answer: C
Rationale: The text defines an "Apparent LLD" as a condition where true bone lengths are equal (equal ASIS-to-MM measurements) but a discrepancy exists from a midline landmark (umbilicus). This is caused by factors like fixed pelvic obliquity, which can result from a hip adduction contracture.
Question 50
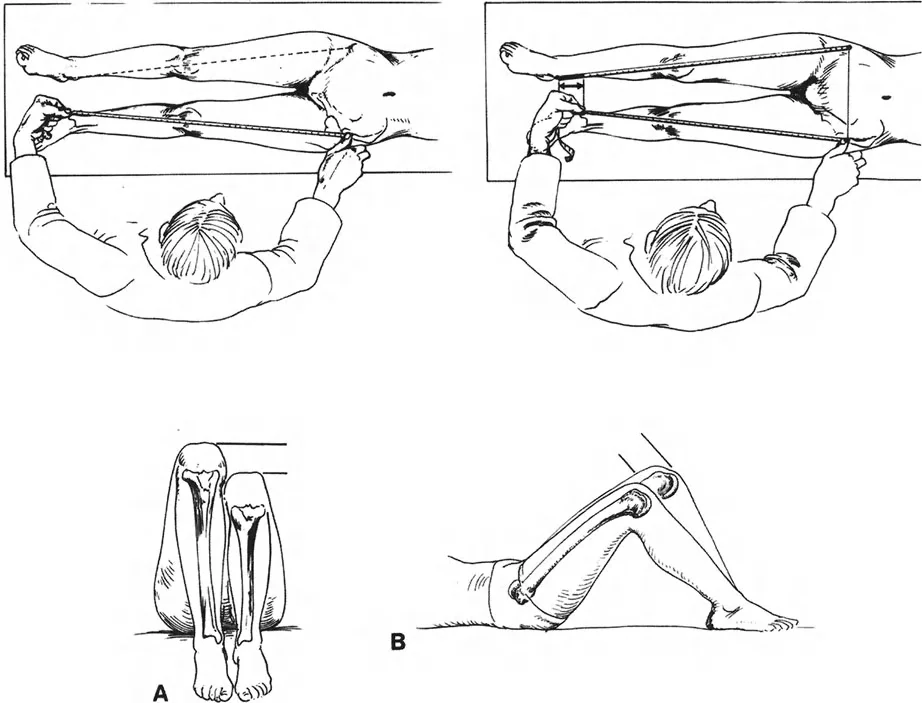
A 5-year-old child is being evaluated for LLD. The patient is placed supine with hips flexed to 45 degrees and knees to 90 degrees, with feet flat on the table. The examiner notes that the left knee is lower than the right knee when viewed from the side. This finding, known as the Galeazzi test, is most indicative of shortening in which bone?
View Answer & Explanation
Correct Answer: C
Rationale: The text describes the Galeazzi test and states, "If one knee is lower, the tibia is short." Since the left knee is lower, this indicates a short left tibia. If the femur were short, the knee would project less anteriorly.
Question 51
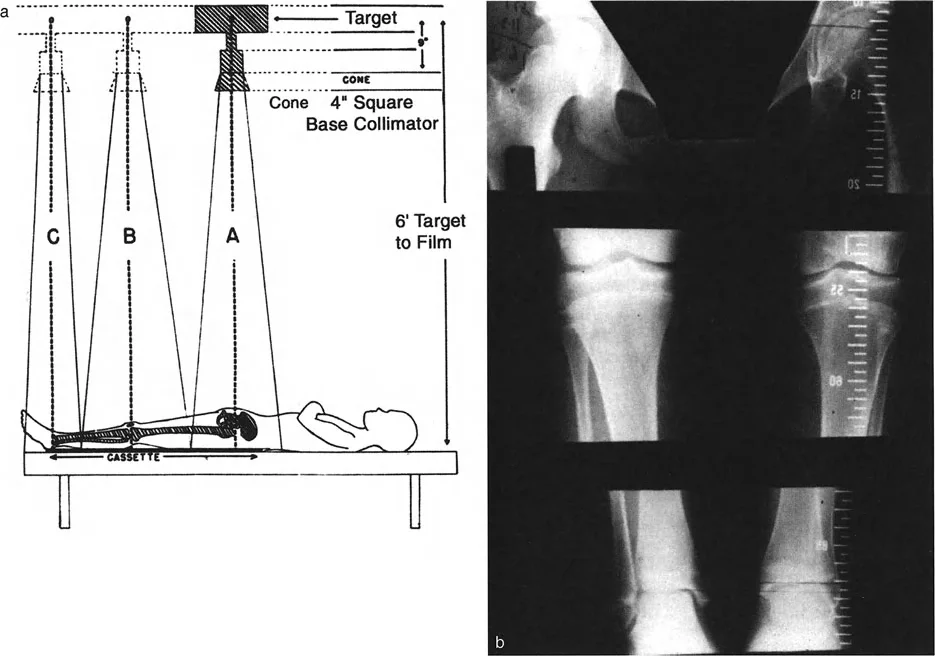
A surgeon orders an orthoroentgenogram (scanogram) to precisely measure a patient's LLD. The technique involves three separate, highly collimated exposures centered over the hip, knee, and ankle. What is the primary advantage of this imaging modality?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that the primary advantage of orthoroentgenograms is "Minimal Magnification" because the central X-ray beam is positioned directly over each joint, eliminating the parallax effect of a divergent beam.
Question 52
A surgeon is planning a complex deformity correction and requires an imaging study that provides both accurate length measurements and a clear depiction of the mechanical axis and joint orientation angles. Which of the following imaging studies is most appropriate for this purpose?
View Answer & Explanation
Correct Answer: C
Rationale: The text explains that teleoroentgenograms are used to overcome the "alignment blindness" of scanograms. A standing teleoroentgenogram exposes the entire limb on a single plate, allowing for a "comprehensive Paley alignment analysis" including mechanical axis deviation (MAD).
Question 53
When obtaining a standing teleoroentgenogram for a patient with a known 3 cm LLD, what is the critical protocol that must be followed to ensure an accurate functional and structural assessment?
View Answer & Explanation
Correct Answer: C
Rationale: The text describes the "Lift Protocol," stating it is "absolutely critical to position a patient with LLD standing on a lift" with a height "approximately equal to their clinically determined LLD" to level the pelvis for an accurate assessment.
Question 54
A digital CT scout film is used to evaluate a patient's LLD. According to the provided text, what is a primary limitation of this imaging modality when compared to a standing teleoroentgenogram?

View Answer & Explanation
Correct Answer: C
Rationale: The text clearly states that while CT scout films are excellent for absolute length, they "are obtained supine. Therefore, they do not demonstrate the dynamic effects of weight-bearing, such as joint space narrowing, ligamentous laxity, or compensatory pelvic tilt."
Question 55
In the context of Paley's principles of deformity correction, the line drawn from the center of the femoral head to the center of the ankle plafond is defined as what?
View Answer & Explanation
Correct Answer: C
Rationale: The text defines the Mechanical Axis of the lower extremity as "a line drawn from the center of the femoral head to the center of the ankle plafond." This is a fundamental concept in Paley's principles.
Question 56
A surgeon is analyzing a long-standing radiograph of a patient with a varus deformity of the proximal tibia. The angle formed by the tibial joint line and the mechanical axis of the tibia is measured. Which of Paley's key joint orientation angles does this represent?
View Answer & Explanation
Correct Answer: B
Rationale: The Medial Proximal Tibial Angle (MPTA) is the angle that determines proximal tibia varus/valgus. The text lists its normal value as 87.2°. The mLDFA relates to the distal femur.
Question 57
According to Paley's osteotomy rules, if a surgeon plans a corrective osteotomy for an angular deformity and places both the osteotomy and the hinge for correction exactly at the Center of Rotation of Angulation (CORA), what is the expected outcome?
View Answer & Explanation
Correct Answer: B
Rationale: This question directly tests Paley's Osteotomy Rule 1, which states: "If the osteotomy and the hinge (axis of correction) are placed exactly at the CORA, the bone will achieve pure angular correction without translation."
Question 58
A 30-year-old patient with a 2.5 cm LLD is skeletally mature and wishes to have the discrepancy corrected in a single surgery with a rapid recovery. The patient is of normal height. Which of the following is the most appropriate treatment option?
View Answer & Explanation
Correct Answer: B
Rationale: The text indicates that acute shortening is a viable option for skeletally mature patients with LLDs between 2 to 3 cm. It is a single-stage procedure. Acute lengthening beyond 2-3 cm is contraindicated due to neurovascular risk, and gradual lengthening is a prolonged process.
Question 59
A surgeon is considering an acute lengthening of the femur for a 4 cm LLD. What is the primary and most significant risk that limits the amount of acute lengthening possible?
View Answer & Explanation
Correct Answer: C
Rationale: The text is unequivocal on this point: "Acute lengthening is highly restricted by the soft tissue envelope. Stretching nerves... and blood vessels acutely beyond 2 to 3 cm carries a severe, unacceptable risk of neuropraxia, compartment syndrome, and vascular compromise."
Question 60
A 17-year-old male requires a 6 cm lengthening of his tibia following a physeal arrest. The surgeon plans for gradual correction using distraction osteogenesis. What is the first phase of this process, immediately following the corticotomy?
View Answer & Explanation
Correct Answer: C
Rationale: The text outlines the parameters of distraction osteogenesis, stating that the "Latency Phase" occurs first. "After the osteotomy, the bone is left to rest for 5 to 7 days" to allow the initial hematoma to form before distraction begins.
Question 61
During the distraction phase of a femoral lengthening, what is the optimal rate and rhythm to promote healthy regenerate bone formation while minimizing soft tissue trauma?
View Answer & Explanation
Correct Answer: D
Rationale: The text specifies the optimal parameters: "The optimal rate is 1 mm per day... this rate is divided into a specific rhythm: typically four 0.25 mm increments spread throughout the 24-hour period."
Question 62
A patient has successfully completed the distraction phase of a 5 cm tibial lengthening. The fixator is now locked, and the patient is waiting for the new bone to harden. What is this phase called, and approximately how long is it expected to last compared to the distraction phase?
View Answer & Explanation
Correct Answer: C
Rationale: The text defines the "Consolidation Phase" as the period when the regenerate bone mineralizes. It explicitly states, "This phase takes roughly twice as long as the distraction phase."
Question 63
A 25-year-old patient is undergoing a femoral lengthening using a magnetically driven intramedullary nail (e.g., PRECICE). What is the most significant advantage of this technology compared to a traditional circular external fixator?
View Answer & Explanation
Correct Answer: B
Rationale: The text highlights several benefits of internal lengthening nails, but the first and most prominent is that they "Eliminate pin-site infections entirely," which is a major source of morbidity with external fixators.
Question 64
A surgeon is performing a corticotomy for a planned tibial lengthening. To preserve the osteogenic potential of the bone, which surgical technique is recommended?
View Answer & Explanation
Correct Answer: C
Rationale: The "Surgical Pearls" table advises to "Perform a multiple drill-hole and osteotome technique (low-energy corticotomy)." It specifically warns, "Never use a high-speed saw, as thermal necrosis will destroy the osteogenic potential of the regenerate."
Question 65
During a planned 7 cm tibial lengthening, the surgeon is concerned about the risk of developing an equinus contracture. Which prophylactic soft tissue procedure might be considered to prevent this complication?
View Answer & Explanation
Correct Answer: C
Rationale: The "Surgical Pearls" table suggests that "intramuscular lengthening of the gastrocnemius may be required to prevent joint contractures during massive lengthenings." An equinus contracture is caused by tightness of the gastrocnemius-soleus complex.
Question 66
A patient undergoing a 4 cm tibial lengthening via an external fixator develops paresthesias in the dorsum of the foot and weakness of ankle dorsiflexion. Which surgical pearl is most relevant to preventing this specific complication?
View Answer & Explanation
Correct Answer: B
Rationale: The symptoms described (sensory changes on the dorsum of the foot and weak dorsiflexion) are classic for common peroneal nerve palsy (foot drop). The text advises, "For tibial lengthenings >3 cm, consider a prophylactic common peroneal nerve decompression at the fibular neck to prevent foot drop."
Question 67
Four weeks into a femoral lengthening, radiographs show dense, mature-appearing bone bridging the distraction gap, preventing further lengthening. What is this complication called?
View Answer & Explanation
Correct Answer: D
Rationale: The text defines "Premature Consolidation" as the complication where "the bone may heal prematurely before the target length is reached." This requires a return to the OR to re-osteotomize the bone.
Question 68
A patient who is a heavy smoker is undergoing tibial lengthening. Radiographs at 6 weeks show a wide distraction gap with thin, wispy regenerate bone. The distraction rate has been 1.5 mm/day. What is the most likely diagnosis and initial management step?
View Answer & Explanation
Correct Answer: C
Rationale: The text describes "Poor Regenerate / Non-Union" as a complication that can occur if the rate is too fast or the biology is compromised (e.g., smoking). The management involves "slowing or reversing the distraction ('accordion technique') to compress the gap and stimulate osteogenesis."
Question 69
A 17-year-old female with a history of neonatal sepsis of the left hip presents with a severe Trendelenburg gait and 6 cm of limb shortening. Radiographs confirm a "flail hip" with complete absence of the femoral head and neck. Her primary complaint is instability and fatigue with walking. According to the provided text, what is the fundamental biomechanical problem that the pelvic support osteotomy (PSO) aims to correct?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that in a chronically dislocated hip, the fulcrum is lost, and the abductors become insufficient. The core rationale of the PSO is to create a new, stable fulcrum by creating a bony abutment against the ischium, thereby restoring abductor function.
Question 70
A 45-year-old male underwent a Girdlestone resection arthroplasty for a periprosthetic joint infection 5 years ago. He now has persistent instability and a painful, lurching gait. He is being considered for a modern, double-level pelvic support osteotomy. Historically, what was the most significant complication of the single-level PSO techniques developed by Hass and Milch that led to their abandonment?
View Answer & Explanation
Correct Answer: B
Rationale: The text clearly states that early single-level PSO techniques were "fraught with complications—most notably, creating severe knee valgus and limb shortening." The modern double-level osteotomy was developed specifically to solve this problem of catastrophic knee malalignment.
Question 71
A surgeon is planning a pelvic support osteotomy for a 22-year-old with sequelae of poliomyelitis. The primary goal is to eliminate the patient's Trendelenburg gait. By creating an extreme valgus deformity at the proximal femur, the PSO establishes a mechanical block. What is the biomechanical principle behind this block?
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "The core rationale of the pelvic support osteotomy is elegantly simple: If the hip cannot adduct, the pelvis cannot drop." The valgus osteotomy creates a bony abutment against the ischium that physically prevents adduction beyond a certain point, thus stabilizing the pelvis.
Question 72
A 19-year-old female with neglected developmental dysplasia of the hip (DDH) undergoes a double-level pelvic support osteotomy. Postoperatively, her abductor strength and function are noted to be dramatically improved. What is the primary mechanism by which the PSO restores the mechanical advantage of the gluteus medius and minimus?
View Answer & Explanation
Correct Answer: C
Rationale: The text explains that the extreme valgus correction "drives the greater trochanter distally and laterally. This effectively tensions the slack abductor muscles, restoring their resting length and dramatically improving their mechanical advantage." This tensioning is a key biomechanical benefit of the procedure.
Question 73
A 30-year-old patient with a "flail hip" from a childhood infection is being evaluated for a PSO. The surgeon explains that the new pivot point created by the osteotomy is biomechanically superior. How does the medialization of the new pivot point on the ischium improve the efficiency of the hip abductors?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "This medialization shortens the body weight lever arm and lengthens the abductor lever arm, further enhancing the mechanical efficiency of the newly reconstructed hip." This is a fundamental principle of hip biomechanics applied in the PSO.
Question 74
A 16-year-old with chronic, unilateral hip dislocation due to L5 spina bifida is a candidate for a PSO. Which of the following conditions is listed in the text as a primary indication for this procedure?
View Answer & Explanation
Correct Answer: D
Rationale: The text provides a table of primary surgical indications. Salvage of a Girdlestone arthroplasty is explicitly listed as an ideal scenario for PSO, especially in cases of chronic infection where implants are undesirable. The other options are typically managed with other procedures.
Question 75
A surgeon is planning a double-level pelvic support osteotomy. The primary innovation introduced by Dr. Paley, which solved the historical failure of the single-level PSO, was the addition of a second, distal osteotomy. What is the principal purpose of this distal osteotomy?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that the historical failure was the creation of massive knee valgus. "Dr. Paley's introduction of a second, distal osteotomy solved this problem." The distal osteotomy's purpose is to create a compensatory varus correction to realign the mechanical axis through the knee center.
Question 76
A resident is performing preoperative planning for a PSO on a patient with no femoral head. They are struggling to define the mechanical axis. According to the Paley method described, what is the correct proximal reference point for drawing the mechanical axis in this situation?
View Answer & Explanation
Correct Answer: C
Rationale: The text is very specific: "In an unstable hip, the femoral head center is absent. Therefore, a new proximal reference point must be established: the new medialized pivot point of the proximal femur against the pelvis." The entire goal is to align the axis from this new point to the ankle, through the knee.
Question 77
A surgeon performs a distal femoral osteotomy for a PSO at a level 3 cm distal to the calculated Center of Rotation of Angulation (CORA). According to Paley Osteotomy Rule 2, what additional maneuver is required during the correction to prevent a parallel shift of the mechanical axis?
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly states Paley Osteotomy Rule 2: "If an osteotomy is performed *away from* the CORA, pure angular correction will cause a parallel shift (translation) of the mechanical axis. To prevent this, a corrective translation must be built into the osteotomy plan."
Question 78
During the final correction of a double-level PSO, the surgeon's goal is to ensure the knee joint is parallel to the ground. What is the target value for the Mechanical Lateral Distal Femoral Angle (mLDFA) that indicates a successful restoration of normal joint orientation?
View Answer & Explanation
Correct Answer: C
Rationale: The text specifies that a goal of the distal osteotomy is to restore normal joint orientation angles. It states, "The Mechanical Lateral Distal Femoral Angle (mLDFA)...should be 87° (± 3°)." This prevents shear forces across the knee.
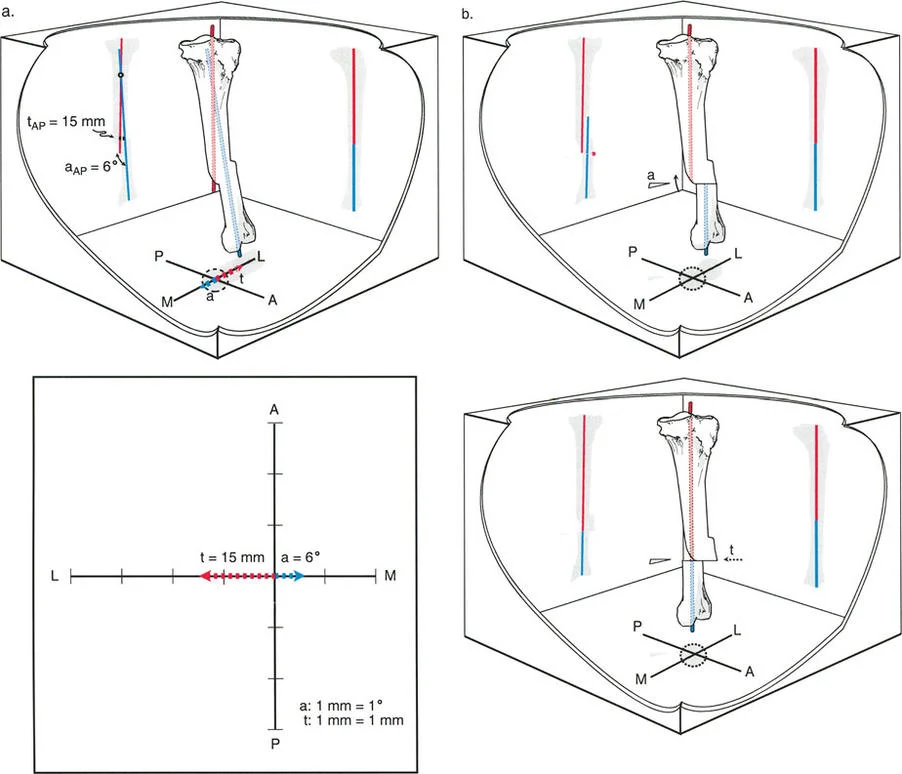
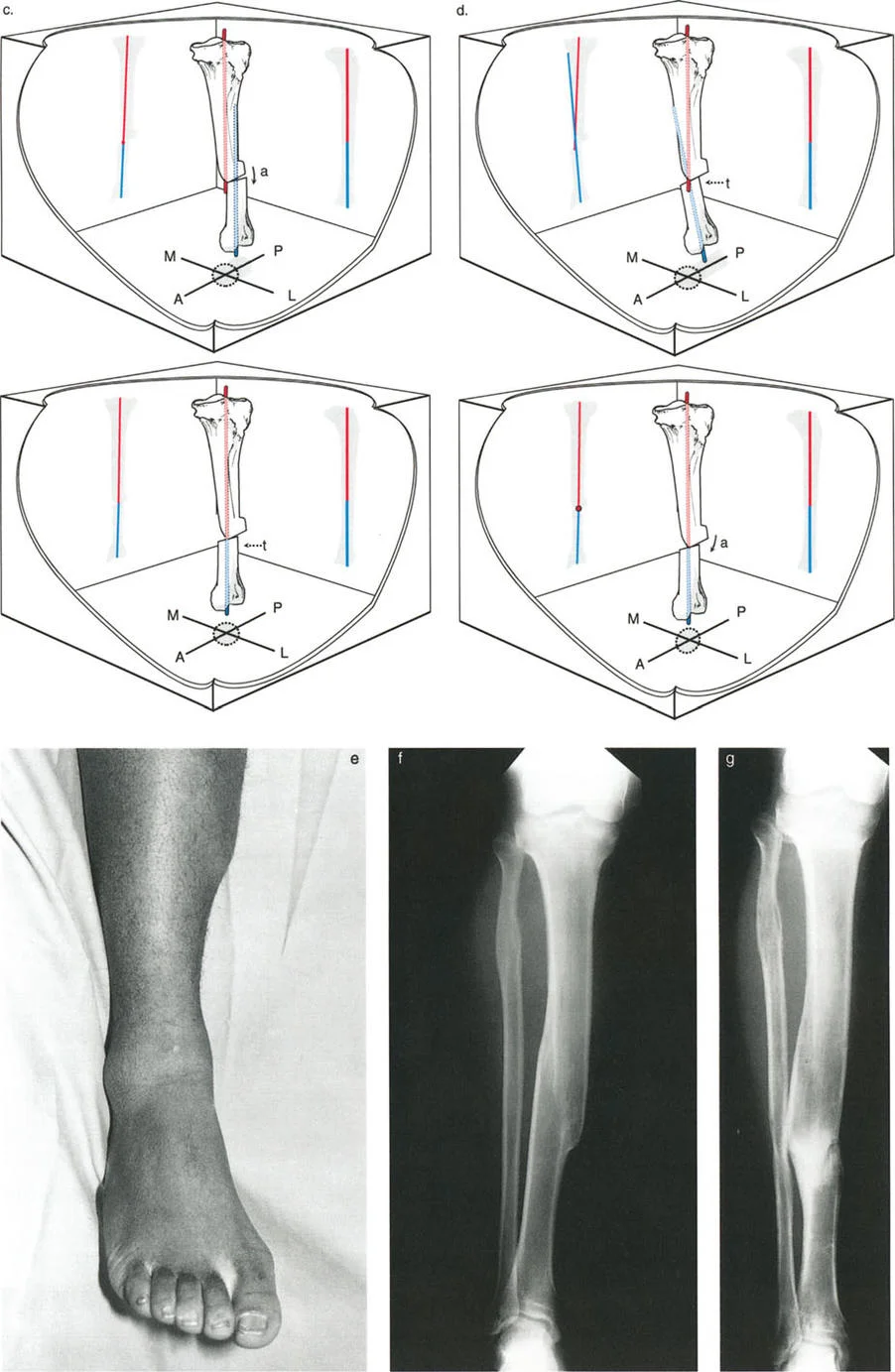
Question 79
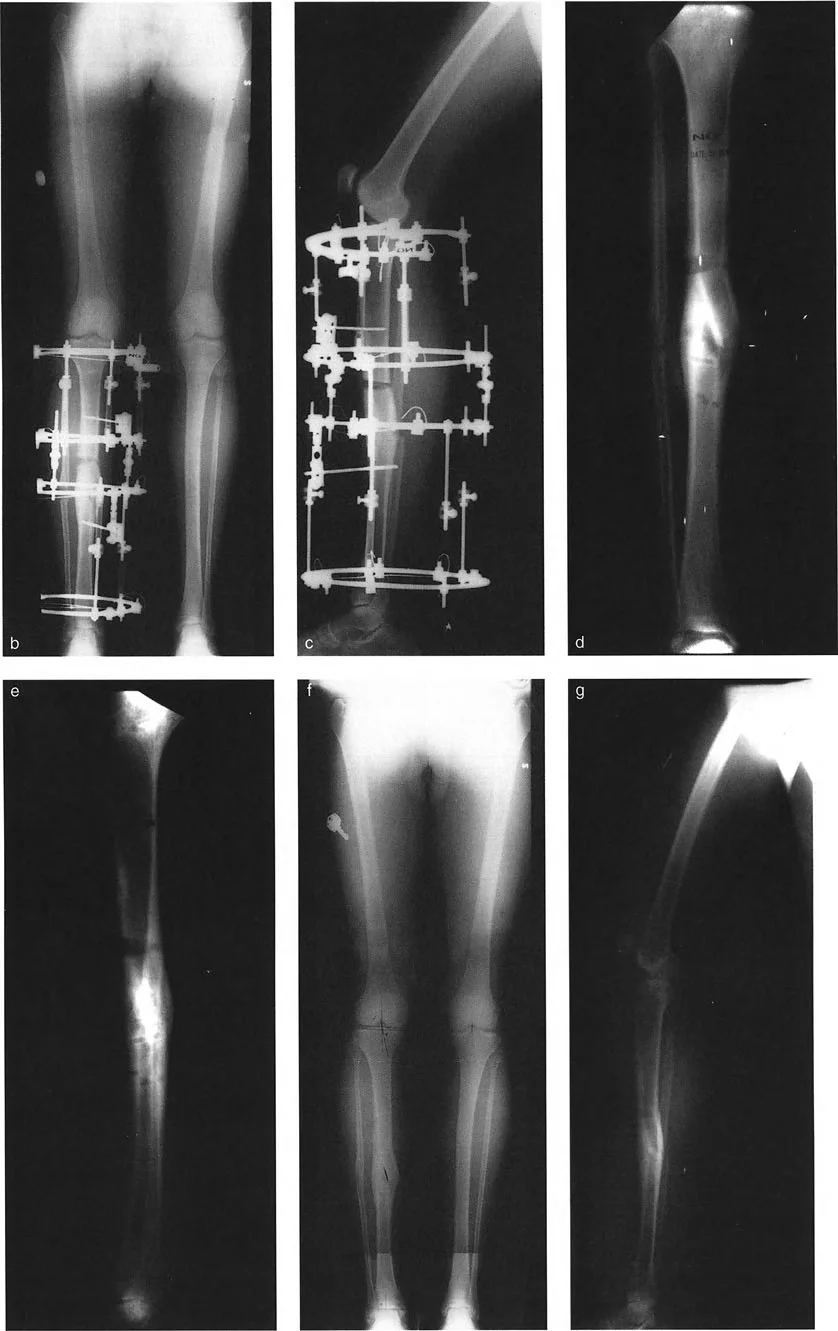
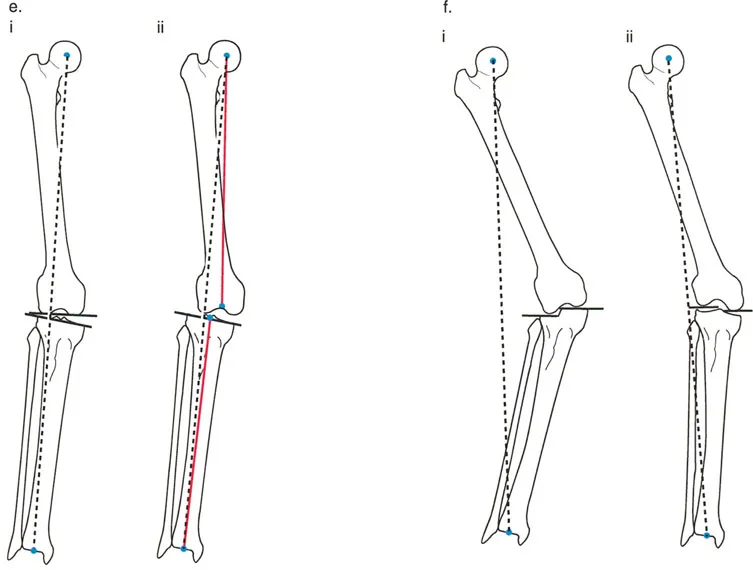
A 25-year-old patient with sequelae of a septic hip is undergoing planning for a double-level PSO. The surgeon is reviewing the principles of the correction. The image provided illustrates the sequential steps of the Paley method. What does diagram (e) primarily demonstrate?

View Answer & Explanation
Correct Answer: C
Rationale: The caption for diagram (e) in the text states: "This diagram shows the initial deformity planning. A single proximal valgus osteotomy has stabilized the hip, but the mechanical axis (red line) is now severely deviated laterally from the knee center, resulting in an abnormal mLDFA." This highlights the problem that the second osteotomy solves.
Question 80
Referring to the same series of diagrams for a double-level PSO, what critical step is depicted as occurring between diagram (f) and diagram (g)?
View Answer & Explanation
Correct Answer: D
Rationale: Diagram (f) shows the limb after lengthening, but with the mechanical axis still deviated. Diagram (g) shows the final corrected state. The text explains this transition: "After lengthening is complete, a varusization at the distal osteotomy site through the lengthening zone has perfectly realigned the limb."
Question 81
A surgeon is preparing for a PSO on a patient with a chronically dislocated hip. To properly plan the magnitude of the proximal valgus osteotomy, two clinical measurements are described as non-negotiable. One is the maximum passive adduction. What is the second essential clinical measurement?
View Answer & Explanation
Correct Answer: B
Rationale: The text identifies two "non-negotiable" clinical measurements for planning the proximal osteotomy: maximum passive adduction and maximum pelvic drop angle. The pelvic drop angle directly quantifies the dynamic instability that the osteotomy must overcome.
Question 82
An orthopedic resident is ordering radiographs for a patient being considered for a PSO. They order a standard AP pelvis and a frog-leg lateral view. The attending surgeon states this is insufficient. Which of the following is described as a mandatory component of the radiographic protocol for PSO planning?
View Answer & Explanation
Correct Answer: C
Rationale: The text lists a specific, mandatory radiographic protocol. A "Full-Length Standing AP Radiograph" is the first item on the list, required to assess overall mechanical alignment and leg length discrepancy, which is essential for planning the double-level correction.
Question 83
During preoperative planning for a PSO, a specific radiograph is obtained to determine the ideal level for the proximal osteotomy. This view demonstrates the precise relationship between the proximal femur and the ischial tuberosity at the limit of adduction. Which radiographic view is this?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states, "The Supine AP Pelvis in Maximum Adduction (Cross-Legged View) is the key radiograph for planning the proximal osteotomy." This view is used to identify the point where the femur crosses the ischial tuberosity line, defining the osteotomy level.
Question 84
A surgeon is using the cross-legged radiograph to plan the proximal osteotomy level for a PSO. A horizontal line is drawn connecting the inferior margins of both ischial tuberosities. How is the exact level of the osteotomy determined relative to this line?
View Answer & Explanation
Correct Answer: C
Rationale: The methodology is described precisely in the text: "The exact point where the medial cortex of the adducted femur crosses this line defines the ideal level for the proximal osteotomy." This ensures the proximal fragment will abut the pelvis correctly.
Question 85
A 20-year-old patient with a chronically dislocated hip is found to have a pelvic drop angle of 35° on single-leg stance. Based on the formula provided in the text for calculating the magnitude of the proximal valgus correction, what is the total planned correction?
View Answer & Explanation
Correct Answer: D
Rationale: The text provides an "unforgiving formula": Total Valgus Correction = (Single Leg Stance Pelvic Drop Angle) + 15° of Overcorrection. Therefore, the calculation is 35° + 15° = 50°.
Question 86
A surgeon is calculating the required proximal valgus correction for a PSO. The formula includes a 15° overcorrection beyond the measured pelvic drop angle. What is the primary purpose of this 15° overcorrection?
View Answer & Explanation
Correct Answer: C
Rationale: The text explains that this "15° of overcorrection is a crucial safety factor. It ensures that the hip remains mechanically locked against adduction even under the high dynamic forces of the gait cycle, completely eliminating the Trendelenburg lurch."
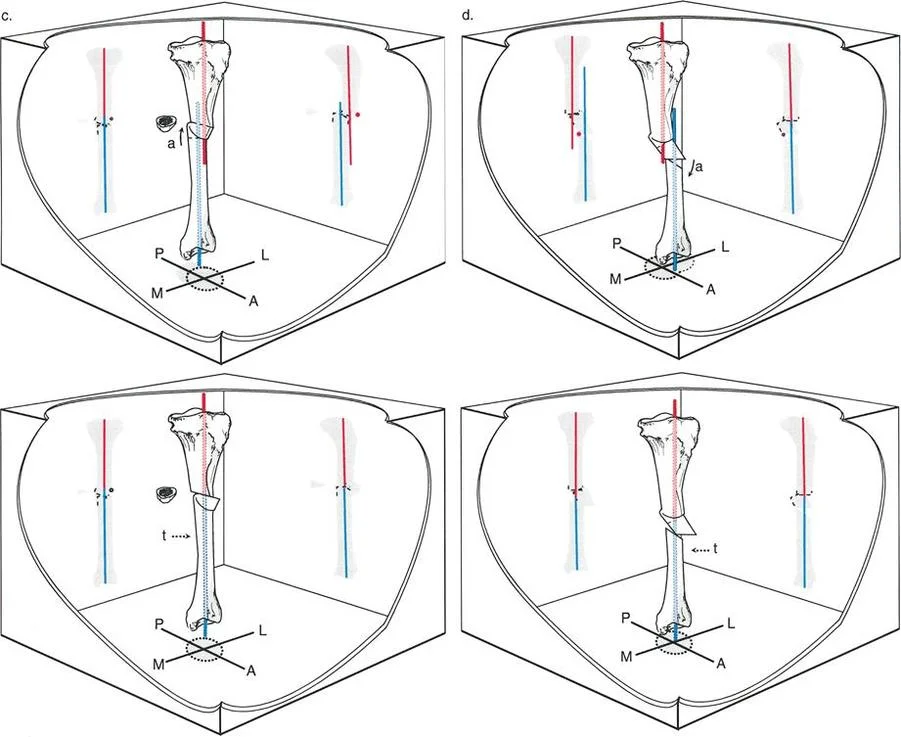
Question 87
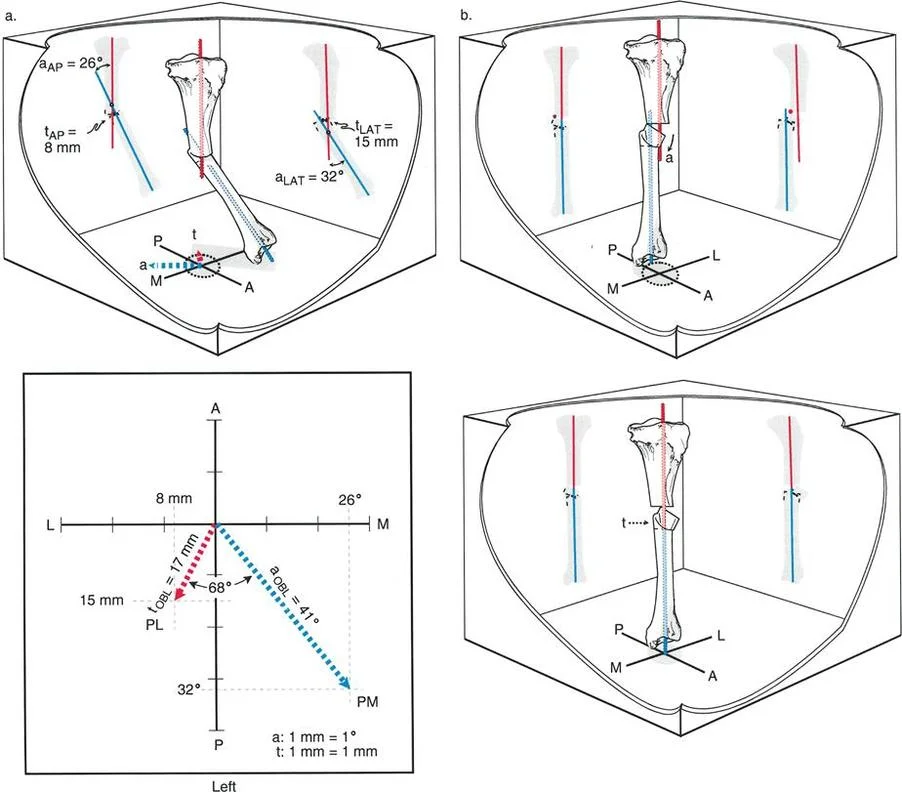
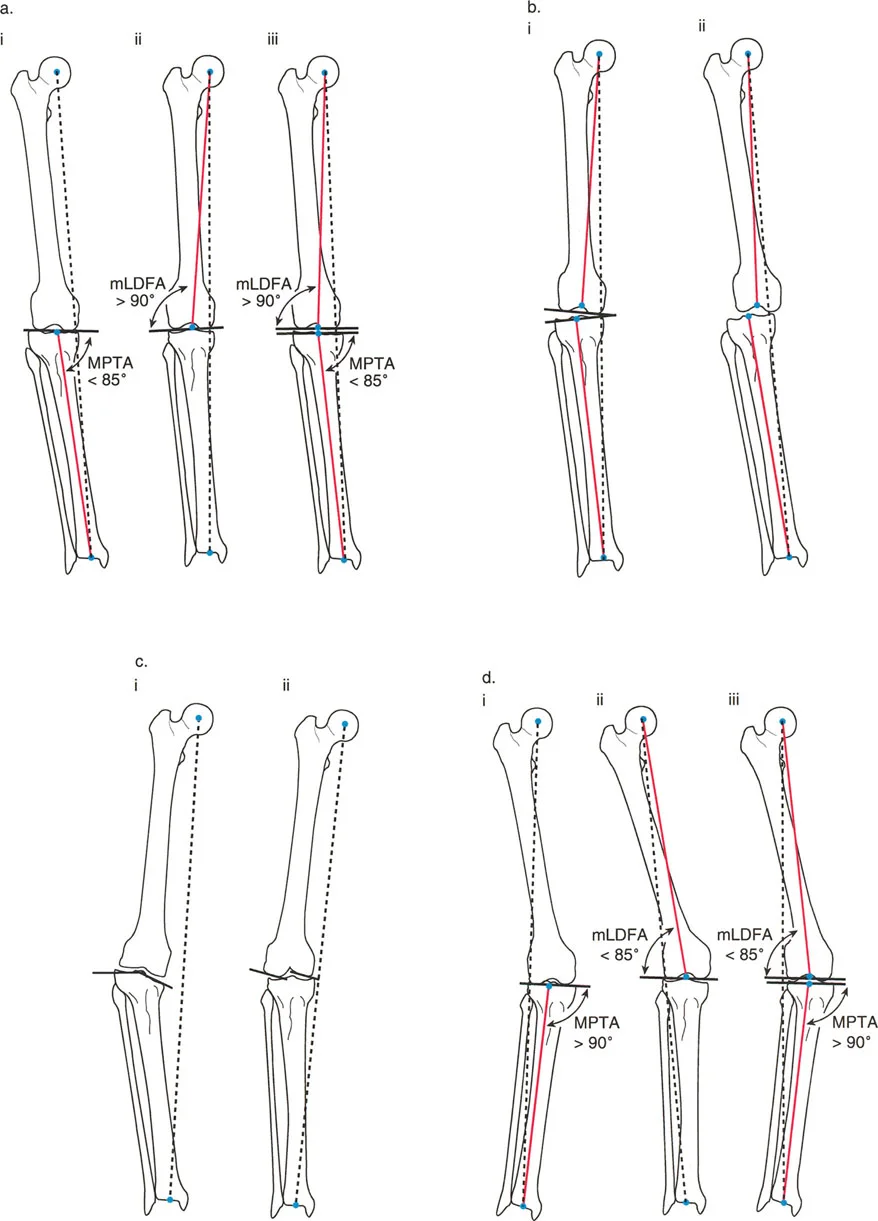
The provided image shows the preoperative planning for a PSO. According to diagram (c), what is the measured single-leg stance pelvic drop for this patient?

View Answer & Explanation
Correct Answer: B
Rationale: The caption for diagram (c) in the text explicitly states: "Measurement of the single-leg stance pelvic drop, which is 40°." This value is then used in the final calculation shown in diagram (d).
Question 88
Based on the complete planning process illustrated in the provided image, what is the final calculated valgus correction for the proximal osteotomy?
View Answer & Explanation
Correct Answer: C
Rationale: Diagram (d) shows the final calculation. The text explains the formula: pelvic drop angle (40° from diagram c) plus an obligatory overcorrection (15°), resulting in a total planned valgus correction of 55°.
Question 89
A 28-year-old patient with a chronically dislocated hip from a tethered cord syndrome also presents with a 20° fixed flexion deformity (FFD) of the hip. During the proximal osteotomy of a PSO, what sagittal plane correction is required to address this deformity and optimize hip function?
View Answer & Explanation
Correct Answer: D
Rationale: The text specifies the sagittal plane correction: "the femur should be extended by the amount of the flexion deformity of the hip **plus an additional 5° of extension**." Therefore, 20° (FFD) + 5° (extra extension) = 25° of total extension.
Question 90
A surgeon is performing a PSO and notes that when the femur is maximally adducted to abut the ischium, it automatically externally rotates. To prevent a postoperative out-toeing gait, what correction must be made in the axial plane at the proximal osteotomy site?
View Answer & Explanation
Correct Answer: B
Rationale: The text highlights this "critical, often-missed biomechanical observation" and states, "the surgeon needs to internally rotate the proximal osteotomy to compensate for this automatic external torsion" to avoid a dysfunctional out-toeing gait.
Question 91
When planning the distal osteotomy for a PSO, the surgeon draws the Proximal Mechanical Axis (PMA) and the Distal Axis Line on a full-length radiograph. What is the geometric definition of the Center of Rotation of Angulation (CORA) in this context?
View Answer & Explanation
Correct Answer: C
Rationale: The text defines the CORA as "the geometric point at the intersection of the proximal and distal axes of a deformed bone." In the planning section for the distal osteotomy, it reiterates that the CORA is "The intersection point of the proximal and distal axis lines."
Question 92
A 45-year-old male undergoes a full-length standing anteroposterior radiograph for evaluation of knee pain. A line is drawn from the center of the femoral head to the center of the tibial plafond at the ankle. Which of the following does this line represent?
View Answer & Explanation
Correct Answer: C
Rationale: The mechanical axis of the lower limb, representing the true line of weight-bearing, is defined as a continuous line from the center of the femoral head to the center of the ankle plafond. The anatomic axis (B) is the mid-diaphyseal line of the bones, which is not a single straight line for the entire limb.
Question 93
A 62-year-old female presents with medial-sided knee pain and a varus thrust on gait. A long-standing radiograph reveals that the mechanical axis of the lower limb passes 25 mm medial to the center of the knee joint. What is the term for this measurement?
View Answer & Explanation
Correct Answer: B
Rationale: The Mechanical Axis Deviation (MAD) is the distance between the mechanical axis line of the lower limb and the center of the knee in the frontal plane. A medial deviation, as described, indicates a varus malalignment. CORA (A) is the intersection point of proximal and distal axis lines used for osteotomy planning.
Question 94
A 58-year-old male is evaluated for asymptomatic lower limbs to establish a baseline for a research study. According to the provided text based on Paley et al. (1994), what is the expected normal Mechanical Axis Deviation (MAD)?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that Paley et al. found the normal MAD to be 9.7 ± 6.8 mm medial to the center of the knee. A value of 0 mm (A) is a common textbook oversimplification but not the clinical reality.
Question 95
A 22-year-old female presents with lateral knee pain and a "knock-kneed" appearance. On her standing alignment radiograph, where would the Mechanical Axis Deviation (MAD) line most likely fall?
View Answer & Explanation
Correct Answer: D
Rationale: A "knock-kneed" appearance corresponds to a valgus malalignment. In valgus, the mechanical axis of the lower limb falls lateral to the center of the knee. A medial MAD (A) would indicate varus malalignment.
Question 96
During preoperative templating for a total knee arthroplasty, a surgeon is discussing alignment with a resident. The resident is asked to define the anatomic tibiofemoral angle. Which of the following is the correct definition?
View Answer & Explanation
Correct Answer: B
Rationale: The anatomic tibiofemoral angle is formed by the intersection of the mid-diaphyseal lines (anatomic axes) of the femur and tibia. The angle between the mechanical axes (A) defines the mechanical tibiofemoral angle.
Question 97
A 35-year-old male with no history of knee injury undergoes a physical examination. When measuring the angle between the anatomic axes of his femur and tibia, what is the expected normal value?
View Answer & Explanation
Correct Answer: D
Rationale: The text states that the normal anatomic tibiofemoral angle, which is commonly referenced in clinical practice, is approximately 6° valgus. The 1.2° varus value (B) corresponds to the normal mechanical tibiofemoral angle.
Question 98
A 50-year-old asymptomatic patient is enrolled in a study on lower limb alignment. Based on the data from Chao et al. and Bhave et al. cited in the text, what is the normal mechanical tibiofemoral angle?
View Answer & Explanation
Correct Answer: D
Rationale: The provided text specifies that the normal mechanical tibiofemoral angle, formed by the mechanical axes of the femur and tibia, is 1.2° to 1.3° varus. The 6° valgus value (A) is the normal anatomic tibiofemoral angle.
Question 99
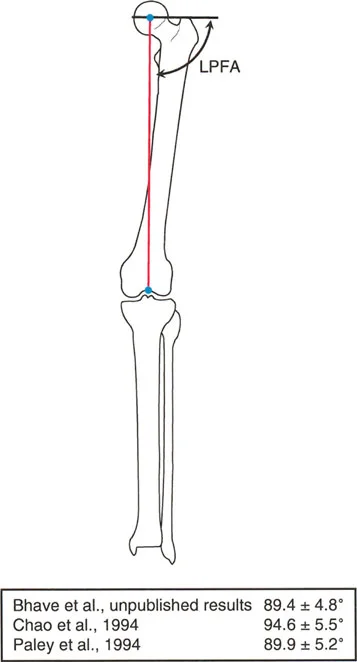
A surgeon is planning a proximal femoral osteotomy for a patient with coxa vara. To assess the frontal plane orientation of the hip, a line is drawn from the tip of the greater trochanter to the center of the femoral head. The angle between this line and the femoral mechanical axis is measured. What is this angle called?
View Answer & Explanation
Correct Answer: C
Rationale: The Lateral Proximal Femoral Angle (LPFA), as described by Paley and Tetsworth, is the angle formed between the femoral mechanical axis and a line from the tip of the greater trochanter to the center of the femoral head. The MNSA (A) involves the axis of the femoral neck, not the trochanteric tip line.
Question 100
A 65-year-old female with no hip pathology is having her contralateral limb templated before a total hip arthroplasty. Based on the pooled institutional data cited, what is the accepted normal value for the Lateral Proximal Femoral Angle (LPFA)?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that based on pooled data, the accepted normal LPFA is 89.9° ± 5.2°, which is often simplified to 90° in practice. The value of 129° (E) is more representative of the anatomic neck-shaft angle.
You Might Also Like
