ABOS Orthopedic Board Review: Lower Extremity Deformity, Gait & Hip Biomechanics | Part 10

Key Takeaway
Orthopedic deformity correction involves restoring normal lower extremity alignment and function. Key principles include gait biomechanics analysis, understanding joint orientation angles like PDFA and MPTA, and applying Paley's methods for osteotomy planning. Procedures like pelvic support osteotomy address complex hip instability and limb length discrepancies, crucial for ABOS board review.
Question 1
During a clinical gait assessment, a surgeon observes excessive pelvic rotation and "hip hiking" on the right side during the swing phase. This is a classic compensation for what underlying biomechanical problem?
View Answer & Explanation
Correct Answer: B
Rationale: Hip hiking is a strategy to increase clearance for the swinging leg. It is used when the limb is functionally too long to clear the ground with normal hip and knee flexion, such as in cases of an ankle fused in equinus or a stiff knee.
Question 2
The metabolic efficiency of normal human ambulation is largely dependent on the smooth, sequential function of the three foot rockers. What is the primary purpose of this rocker system?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that the elegance of human ambulation lies in its metabolic efficiency, which is achieved by the foot rocker system. This system allows for a smooth, rolling transition that conserves energy by minimizing abrupt accelerations and decelerations.
Question 3
A 45-year-old male presents with a 15° fixed flexion deformity (FFD) of his left knee following a remote injury. He complains of significant anterior knee pain and quadriceps fatigue after walking short distances. During the mid-stance phase of his gait, what is the relationship between the Ground Reaction Vector (GRV) and his knee's transverse axis of rotation?
View Answer & Explanation
Correct Answer: B
Rationale: In a knee with an FFD, full extension is not possible. This forces the GRV to pass posterior to the knee's center of rotation during mid-stance, creating a powerful flexion moment that must be constantly counteracted by the quadriceps. Option A describes the biomechanically efficient state of a normal knee.
Question 4
A 22-year-old female is evaluated for a knee flexion deformity after a malunited distal femur fracture. A full-length, weight-bearing lateral radiograph is obtained for surgical planning. Her Posterior Distal Femoral Angle (PDFA) is measured to be 95°. According to Paley's principles, what is the normal value for the PDFA and what does her measurement indicate?
View Answer & Explanation
Correct Answer: B
Rationale: The normal PDFA is 83°. An increased PDFA (>83°), such as 95°, signifies a distal femoral procurvatum (an apex-anterior bow), which is a bony cause of a knee flexion deformity. A PDFA within the normal range would suggest a soft tissue or intra-articular cause.
Question 5
A 16-year-old boy with a history of Blount's disease presents with a crouched gait and bilateral knee flexion deformities. Radiographic analysis of his right leg reveals a Posterior Proximal Tibial Angle (PPTA) of 92°. What is the primary structural deformity indicated by this finding?
View Answer & Explanation
Correct Answer: C
Rationale: The normal PPTA is 81°. An increased PPTA (>81°), such as 92°, indicates a proximal tibial procurvatum (apex-anterior bowing of the proximal tibia). This is a common bony contributor to a fixed flexion deformity. Options D and E are soft tissue causes, which would not be diagnosed by an abnormal PPTA.
Question 6
A 58-year-old woman with a 20° knee flexion deformity is being evaluated. Her PDFA is 83° and her PPTA is 81°. On physical examination, she has a firm endpoint to passive extension. What is the most likely source of her deformity?
View Answer & Explanation
Correct Answer: D
Rationale: The patient's sagittal plane joint orientation angles (PDFA and PPTA) are normal. This rules out a significant bony procurvatum deformity in the femur or tibia as the cause of her FFD. Therefore, the etiology must be a soft tissue contracture involving structures like the posterior capsule or hamstrings.
Question 7
A surgeon is planning a corrective osteotomy for a 30-year-old patient with a post-traumatic, apex-anterior deformity of the distal femur. To achieve a precise correction, the surgeon must identify the intersection of the proximal and distal mid-diaphyseal axes on a lateral radiograph. What does this intersection point represent?
View Answer & Explanation
Correct Answer: B
Rationale: The CORA is the geometric point at the apex of a bony deformity, found by the intersection of the proximal and distal axial lines. Identifying the CORA is the foundational step in Paley's principles for planning an accurate corrective osteotomy. The MAD is a measure of overall limb alignment, not the location of the deformity's apex.
Question 8
A 12-year-old girl with a mild 10° knee flexion deformity is observed walking. She is able to keep her foot flat on the ground during the stance phase. The diagram shown illustrates the primary biomechanical events occurring. Which statement best describes her compensatory gait pattern?
View Answer & Explanation
Correct Answer: C
Rationale: The diagram shows that for a mild FFD, the body compensates by increasing ankle dorsiflexion to maintain a plantigrade foot. Despite this compensation, the flexed knee forces the GRV (yellow/green line) to pass posterior to the knee's center of rotation (blue dot), creating a flexion moment that requires quadriceps activity.
Question 9
A 17-year-old male has a severe, 40° knee flexion deformity. His ankle has a maximum passive dorsiflexion of 20°. Based on the geometric constraints illustrated in the provided image, what is the inevitable consequence during the stance phase of gait?

View Answer & Explanation
Correct Answer: C
Rationale: As the image on the right demonstrates, when the magnitude of the knee FFD (40°) exceeds the ankle's capacity to compensate with dorsiflexion (20°), it is geometrically impossible to keep the foot flat. The heel must lift off the ground, resulting in an obligate toe-walking or equinus gait.
Question 10
A 65-year-old man with a 25° knee flexion deformity also has a rigid ankle fusion in a neutral position from a prior trauma. Which of the following compensatory mechanisms will be most pronounced in his gait?

View Answer & Explanation
Correct Answer: C
Rationale: With a stiff ankle, the primary distal compensatory mechanism for an FFD is lost. To achieve a plantigrade foot position and advance the body's center of mass, the patient must shift all compensation proximally. This results in a characteristic posture of exaggerated hip flexion and a significant anterior lean of the trunk, as depicted in the diagram.
Question 11
A 35-year-old patient with a chronic 20° knee FFD undergoes gait analysis. The study confirms a persistent flexion moment at the knee throughout the stance phase. What is the most direct physiological consequence of this abnormal moment?
View Answer & Explanation
Correct Answer: B
Rationale: The posterior GRV in an FFD creates a constant flexion moment that threatens to buckle the knee. To prevent collapse, the patient must maintain a sustained, energy-draining isometric contraction of the quadriceps muscle throughout stance. This leads to rapid fatigue, pain, and eventual patellofemoral degeneration. The "screw-home" mechanism (Option E) is lost with an FFD.
Question 12
A surgeon is analyzing a full-length lateral radiograph of a patient with a knee flexion deformity. A plumb line is dropped from the center of the femoral head. In this patient, the line passes 30 mm anterior to the center of the knee joint. What does this measurement represent?
View Answer & Explanation
Correct Answer: D
Rationale: The sagittal mechanical axis is a line from the femoral head to the ankle center. In an FFD, the knee is held in a flexed, anteriorly displaced position relative to this line. The distance from the plumb line (representing the weight-bearing axis) to the knee center in the sagittal plane is the anterior sagittal MAD. Correcting this deviation is a key surgical goal.
Question 13
A 19-year-old male presents with the clinical appearance shown in the image, characterized by bilateral knee flexion deformities and an inability to stand fully upright. This gait pattern is most accurately described as which of the following?

View Answer & Explanation
Correct Answer: B
Rationale: The image displays a classic crouched gait, which is characterized by excessive flexion at the hips and knees, often accompanied by ankle dorsiflexion. This pattern is common in patients with bilateral severe FFDs, such as those with spastic diplegic cerebral palsy, and is extremely energy-inefficient.
Question 14
A 25-year-old female has a 30° fixed flexion deformity of her left knee. When she stands, her left pelvis drops significantly, as shown in the clinical photograph. This occurs due to what phenomenon?

View Answer & Explanation
Correct Answer: C
Rationale: A knee flexion deformity functionally shortens the vertical height of the limb during the stance phase, even if the bone lengths are equal. This creates a functional leg length discrepancy, causing the pelvis to drop on the affected side to allow the foot to reach the ground. This is distinct from a true LLD (Option A) where the bones are different lengths, or a Trendelenburg gait (Option B) caused by abductor weakness.
Question 15
A 14-year-old with arthrogryposis is examined on the table and is unable to achieve the final degrees of passive knee extension, as shown in the image. Radiographs reveal a PDFA of 84° and a PPTA of 82°. Which structures are the most likely primary cause of this fixed flexion deformity?

View Answer & Explanation
Correct Answer: C
Rationale: The patient's PDFA and PPTA are essentially normal, ruling out a significant bony deformity as the primary cause. The clinical image shows a clear restriction to passive extension. This combination strongly points to a soft tissue contracture, where the posterior structures (capsule, hamstrings, gastrocnemius origins) act as a tether, preventing full extension.
Question 16
In a normal, energy-efficient gait, the quadriceps muscle is largely inactive during mid-stance. What biomechanical principle allows for this passive knee stability?
View Answer & Explanation
Correct Answer: B
Rationale: The brilliance of normal gait mechanics is that the GRV passes slightly anterior to the knee's axis in mid-stance. This generates a passive extension moment, which is stabilized by the posterior capsuloligamentous structures and the "screw-home" mechanism, requiring minimal to no quadriceps activity. An FFD reverses this, forcing the GRV posterior (Option A).
Question 17
A surgeon is planning a distal femoral extension osteotomy to correct a procurvatum deformity. The goal is to restore the Posterior Distal Femoral Angle (PDFA) to its normal value. What is the target angle for the PDFA post-correction?
View Answer & Explanation
Correct Answer: C
Rationale: According to Paley's principles, the normal value for the PDFA is 83°. The goal of a corrective osteotomy for distal femoral procurvatum is to restore this normal joint orientation angle to realign the limb and normalize gait mechanics. 81° is the normal PPTA, and 80° is the normal ADTA.
Question 18
A 40-year-old man has a 15° FFD. He has noticed that he no longer strikes the ground with his heel first when he walks. This loss of a normal heel strike is a direct consequence of which aspect of the deformity?
View Answer & Explanation
Correct Answer: A
Rationale: Normal heel strike requires the knee to be at or near full extension at the end of the swing phase. A fixed flexion deformity makes this impossible. The foot, therefore, approaches the ground in a more plantar-flexed or flat position, leading to a "foot slap" or forefoot-first contact pattern and altering shock absorption.
Question 19
The Anterior Distal Tibial Angle (ADTA) is an important measurement in the overall sagittal plane analysis of the lower limb. What is its normal value and what is its primary role in the context of a knee flexion deformity?
View Answer & Explanation
Correct Answer: D
Rationale: The normal ADTA is 80°. While located at the ankle, this angle is crucial for assessing the ankle joint's orientation and, by extension, its ability to dorsiflex. A mobile ankle with a normal ADTA is essential for the body's primary distal compensatory strategy for a knee FFD.
Question 20
A patient with a 25° knee FFD is described as having "quadriceps burnout." This clinical finding is a direct result of the muscle working to counteract which force during the stance phase?
View Answer & Explanation
Correct Answer: C
Rationale: The FFD forces the GRV to pass posterior to the knee's axis of rotation. This creates a powerful, pathological flexion moment that constantly tries to buckle the knee. The quadriceps must fire continuously and isometrically to resist this moment, leading to extreme energy expenditure, fatigue, and eventual "burnout."
Question 21
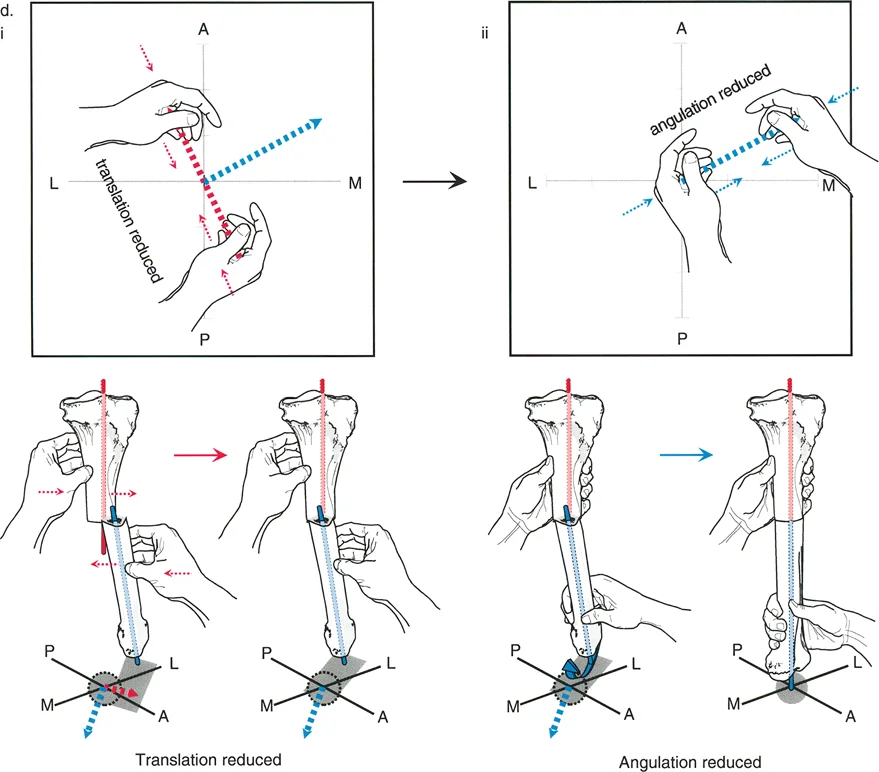
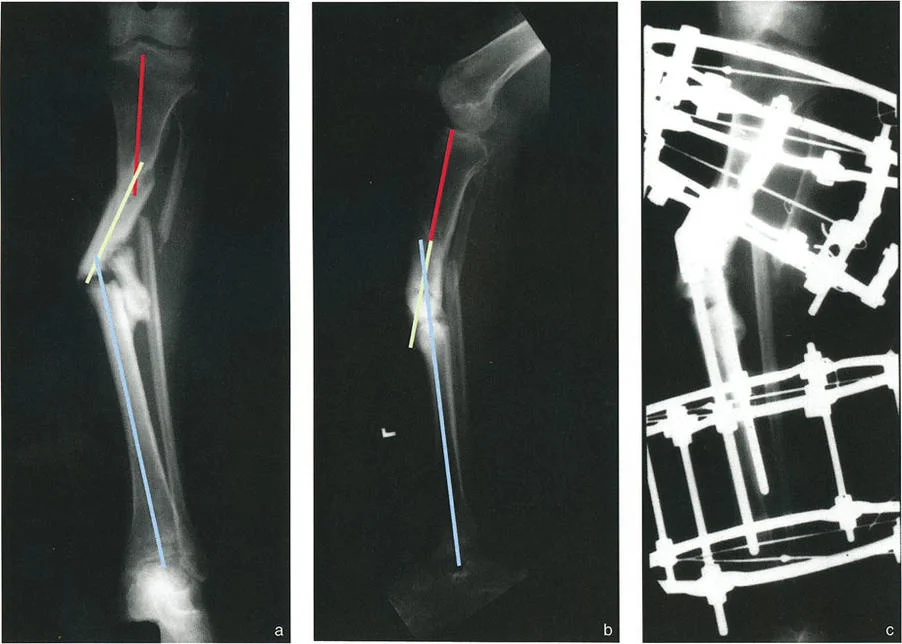
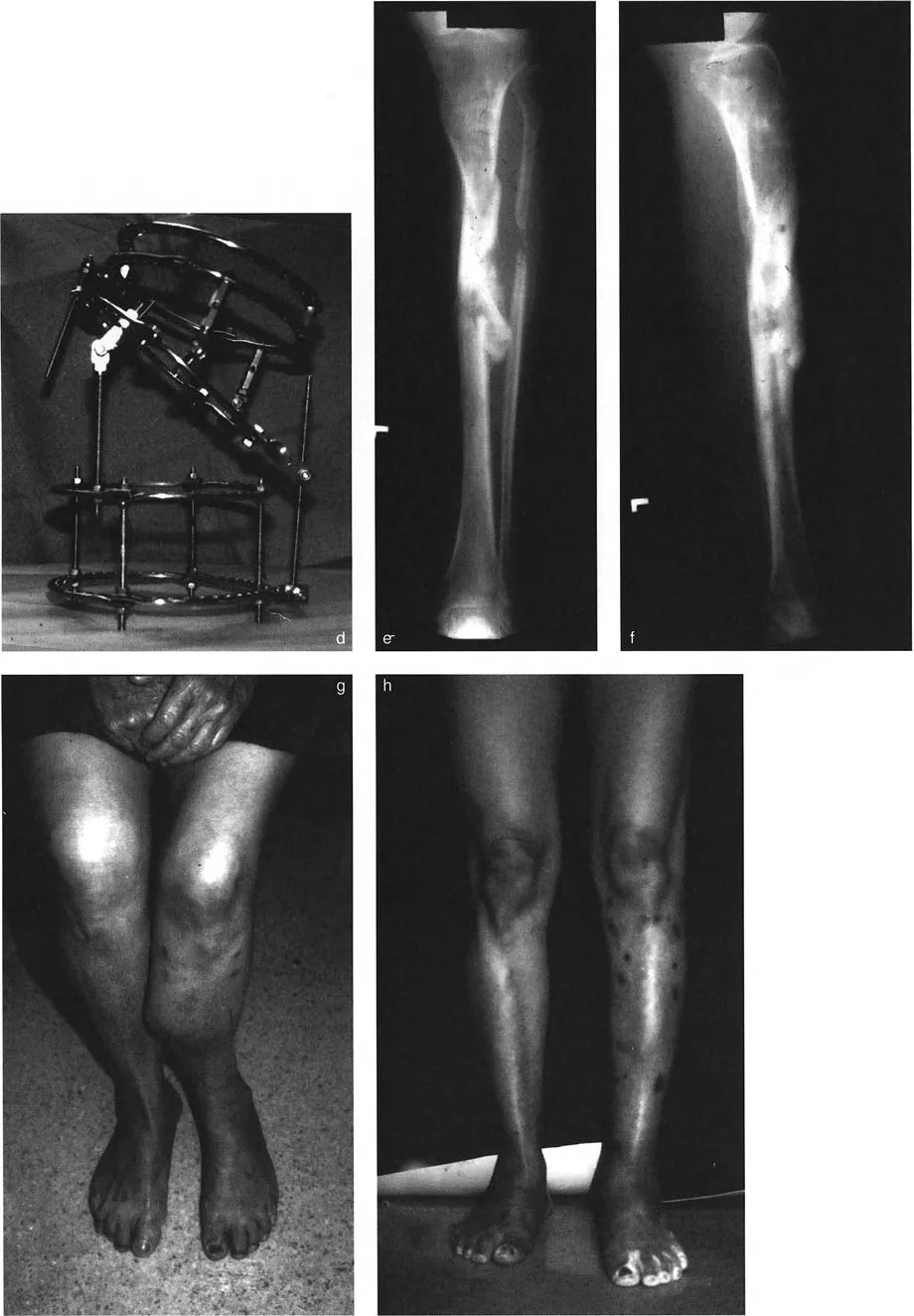
A 45-year-old male presents with a painful tibial nonunion one year after a mid-shaft fracture. Anteroposterior (AP) and lateral (LAT) radiographs are obtained. The AP view demonstrates varus angulation and lateral translation.
View Answer & Explanation
Correct Answer: D
Rationale: The provided text and images (Fig. 8-18e, f) illustrate a case where angulation and translation are in different oblique planes. This results in the AP CORA and the LAT CORA being on opposite sides of the nonunion. The presence of translation displaces the CORA from the nonunion site itself.
Question 22
A 38-year-old female presents with a tibial malunion characterized by procurvatum and posterior translation on the lateral radiograph, and varus with lateral translation on the AP radiograph. During open reduction, what is the first manipulative step to facilitate correction?
View Answer & Explanation
Correct Answer: D
Rationale: As stated in the caption for Figure 8-18d, the strategy for reduction is to correct translation first, then angulation. Placing hands along the plane of translation to reduce it simplifies the subsequent correction of the angular deformity.
Question 23
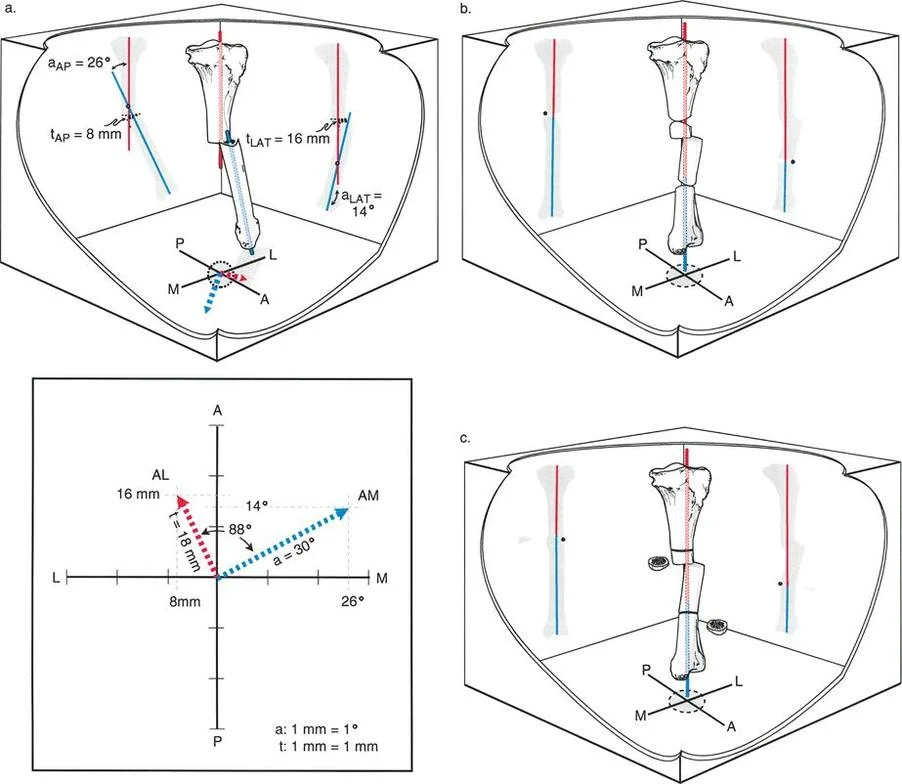
A 50-year-old male has a complex tibial malunion where the AP view shows a CORA medial to the bone and the lateral view shows a CORA posterior to the bone, with the two apices separated by 7 cm. The surgeon plans a two-level osteotomy correction. What is this approach called in the provided text?
View Answer & Explanation
Correct Answer: C
Rationale: Strategy 5 is described for deformities where angulation and translation are in different planes, causing the AP and LAT CORAs to be distantly separated. This strategy treats the deformity as a double-level biplanar angular deformity, with one osteotomy at the AP a-t CORA and another at the LAT a-t CORA.
Question 24
A surgeon is planning a correction for a tibial malunion using Strategy 5, which involves two separate osteotomies for distantly separated CORAs. What is a known potential cosmetic consequence of this "bypass" technique?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that in considering all bypass options, including Strategy 5, "one must take into consideration that a bump may remain despite accurate realignment." This is because the osteotomies are not at the true, single apex of the combined deformity.
Question 25
A 29-year-old patient has a segmental tibial fracture with a proximal malunion and a distal mal-nonunion. The distal deformity consists of valgus angulation and lateral translation. On radiographic planning, the CORA on the AP and LAT views for this distal deformity is at the same level. What does this finding imply?
View Answer & Explanation
Correct Answer: C
Rationale: The text accompanying Figure 8-20b states, "Note that the CORA for the second fracture is at the same level on the AP and LAT views, because angulation and translation are in the same plane." This simplifies correction, often allowing for a single oblique plane correction at that level.
Question 26
A 33-year-old male presents with the segmental tibial deformity shown, including a proximal varus malunion and a distal hypertrophic mal-nonunion with valgus and procurvatum. Based on the case presented, what is the most appropriate treatment for the distal hypertrophic nonunion?
View Answer & Explanation
Correct Answer: D
Rationale: The explanation for Figure 8-20e states that the distal level was "treated by distraction through the hypertrophic nonunion." This technique, often performed with an external fixator like the Ilizarov frame, uses the principle of distraction osteogenesis to achieve both union and deformity correction.
Question 27
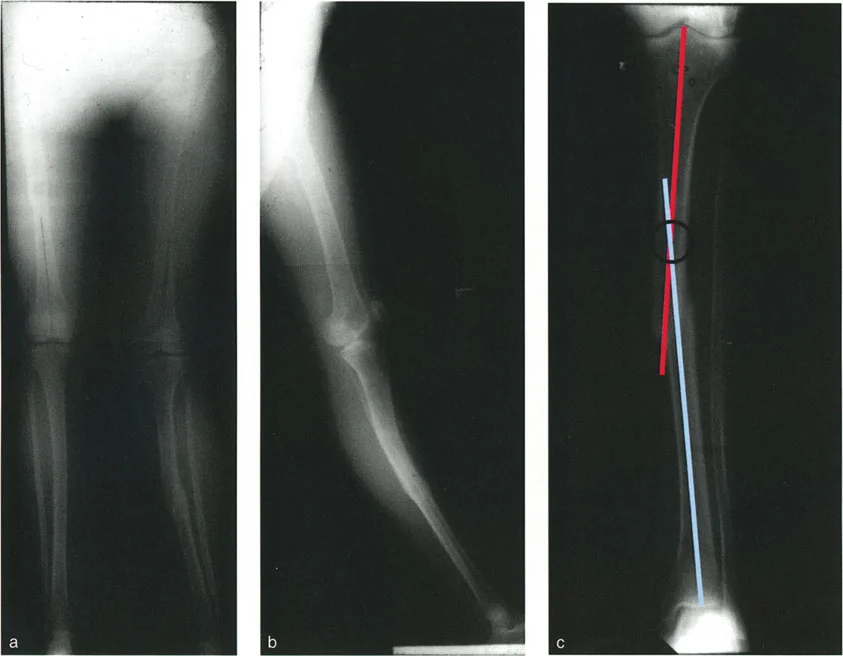
A 25-year-old patient undergoes correction of a segmental tibial malunion. Postoperatively, the mechanical axis is corrected, but a residual bump is noted on the medial side of the tibia. Radiographs confirm the osteotomy was performed at a single "resolution point." What is the most likely reason for the residual bump?
View Answer & Explanation
Correct Answer: B
Rationale: The text for Figure 8-21e explicitly states, "...there is a residual bump on the medial side of the tibia, due to the osteotomy's being at the resolution point and not at the fracture level." A resolution point is a location for a single osteotomy to correct a multi-apical deformity, but it is a bypass osteotomy, which can leave a residual bump.
Question 28
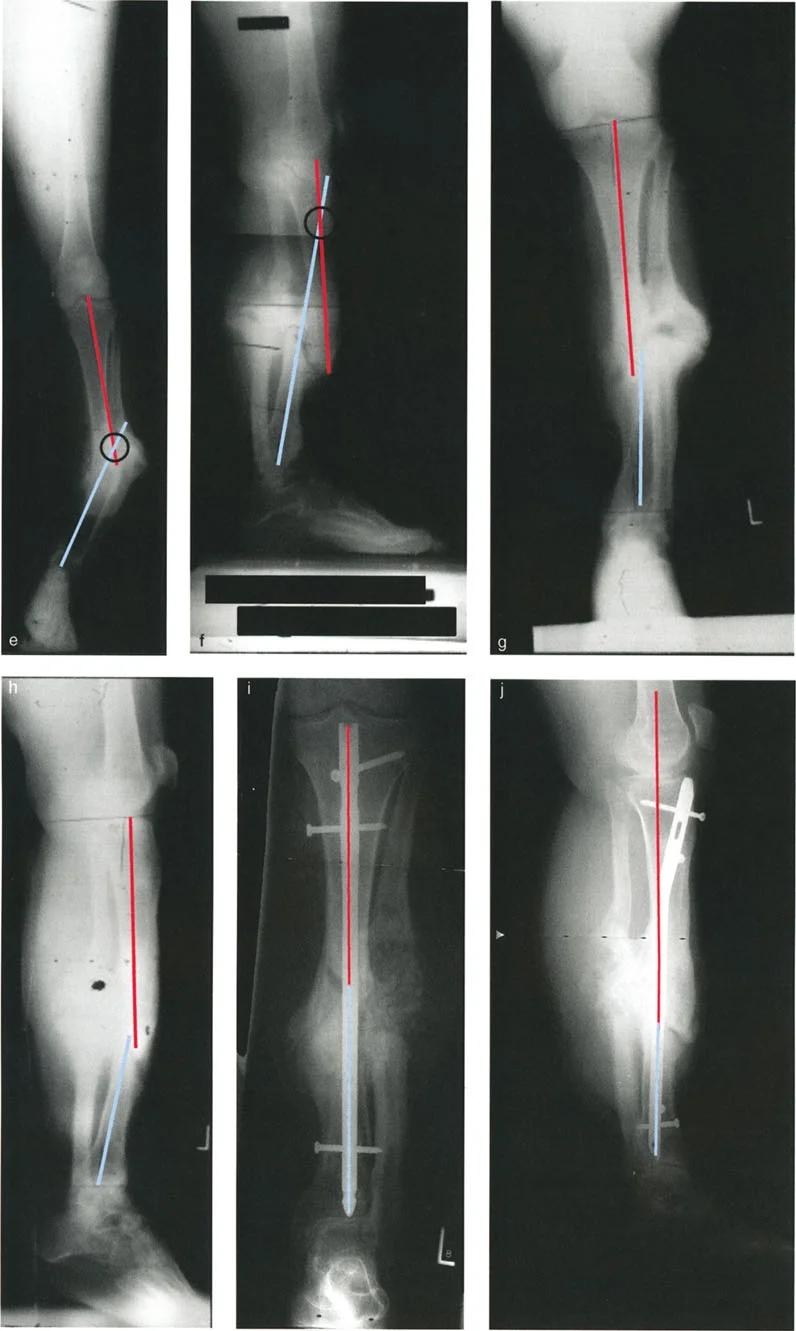
A 41-year-old male has a tibial malunion with valgus angulation and lateral translation at the distal end of a healed segmental fracture. How does the presence of lateral translation affect the location of the CORA on the AP view?
View Answer & Explanation
Correct Answer: B
Rationale: As described in the caption for Figure 8-21c, "Because of the translation deformity, the CORA is displaced proximally." For a valgus deformity with lateral translation, the intersection of the axes (the CORA) moves proximally from the level of the malunion.
Question 29
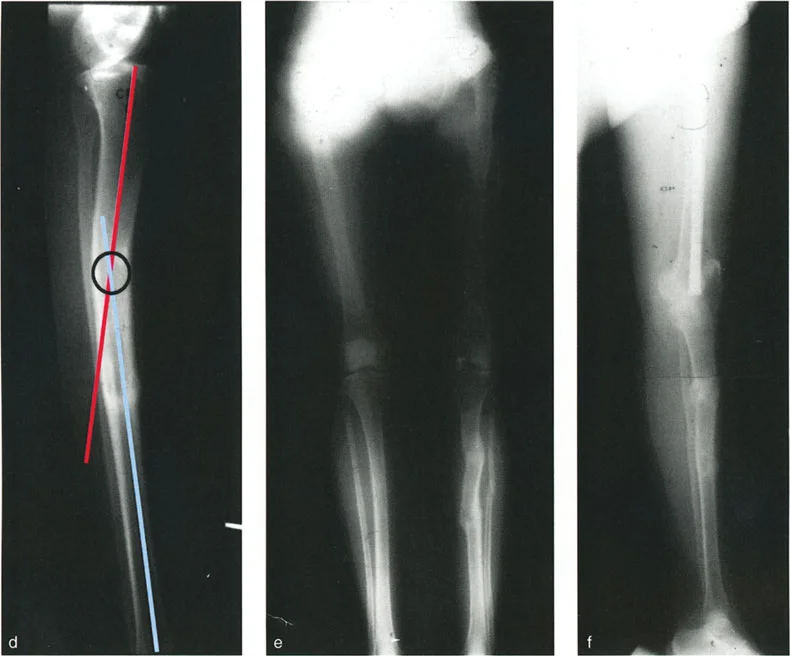
A patient presents with a tibial nonunion. The AP radiograph shows varus angulation with lateral translation, and the lateral radiograph shows procurvatum with posterior translation. After initial distraction fails to achieve union, an intramedullary nail (IMN) is used. What was the final outcome described in the case?
View Answer & Explanation
Correct Answer: C
Rationale: The text accompanying Figure 8-18i and j states, "Because the deformity was almost completely reduced, the nonunion was treated by IMN, fully correcting the deformity. Union was obtained... Complete realignment through the original fracture site was achieved."
Question 30
In the context of Strategy 5 for correcting a complex deformity, an osteotomy is made at the AP a-t CORA. What is the specific purpose of the correction performed at this level?
View Answer & Explanation
Correct Answer: B
Rationale: The description of Strategy 5 (Fig. 8-19) specifies that the deformity is treated as two single-level uniplanar deformities. It states, "Angulation at the former osteotomy [AP a-t CORA] is performed for frontal plane correction only."
Question 31
A 30-year-old patient is shown before and after correction of a segmental tibial deformity. The preoperative clinical photograph shows a prominent bump on the subcutaneous border of the tibia. The postoperative photograph shows a straight leg with no bump. How was this cosmetic result achieved?
View Answer & Explanation
Correct Answer: B
Rationale: The case in Figure 8-20 demonstrates a multi-level correction where the proximal osteotomy and distal distraction were performed at the levels of the deformities. The caption for Fig. 8-20h notes, "The leg is straight, and the bump is gone." This contrasts with the case in Fig. 8-21, where a bypass osteotomy at a resolution point left a residual bump.
Question 32
A 28-year-old male has a segmental tibial fracture malunion. The long LAT view shows a significant recurvatum deformity. Planning radiographs of the tibia show this deformity originates from the proximal end of the segmental fracture. What is the associated deformity at the distal end on the LAT view in this specific case?
View Answer & Explanation
Correct Answer: D
Rationale: The caption for Figure 8-21d, which corresponds to this case, states that the LAT view shows "recurvatum malunion at the proximal end of the segmental fracture, and neither angulation nor translation at the distal end of the segmental fracture."
Question 33
When planning a deformity correction with an Ilizarov frame for a multi-level deformity, as shown in Figure 8-20, what is the ideal orientation of each ring block relative to the bone segment it is fixed to?
View Answer & Explanation
Correct Answer: C
Rationale: The caption for Figure 8-20c describes the Ilizarov frame application: "...with each ring block perpendicular to the axis of each segment." This orthogonal placement is a fundamental principle that allows for predictable and controlled correction of the deformity between the blocks.
Question 34
A 42-year-old patient has a tibial malunion with varus angulation and no translation at a proximal level, and valgus angulation with lateral translation at a distal level. This represents what type of deformity?
View Answer & Explanation
Correct Answer: C
Rationale: The case presented in Figure 8-20 is described as a "multilevel fracture deformity" with distinct deformities at two separate levels (proximal and distal). This is the definition of a multiapical deformity, as there are two separate apices of angulation.
Question 35
A 58-year-old male presents with progressive right knee pain and a "bow-legged" appearance. His standing radiograph shows significant medial joint space narrowing. According to the principles outlined, what is the most fundamental concept that dictates the increased loading on his medial compartment during gait?
View Answer & Explanation
Correct Answer: B
Rationale: The provided text establishes the core concept that static alignment directly dictates dynamic joint loading. The varus malalignment shifts the mechanical axis medially, concentrating force on the medial compartment, which is the primary driver of his pathology.
Question 36
A 45-year-old woman with a history of a poorly healed tibial fracture complains of knee pain. During gait analysis, her body is divided into two functional units for biomechanical assessment. Which of the following structures are all components of the "passenger unit"?
View Answer & Explanation
Correct Answer: B
Rationale: The text defines the passenger unit as the head, arms, and trunk (HAT). The locomotor unit consists of the lower extremities and the pelvis. This distinction is critical for understanding how the body's mass is carried during gait.
Question 37
A surgeon is planning a complex lower extremity reconstruction for a patient with multi-level deformities. To understand the effect of trunk position on gait, the surgeon must focus on the center of gravity of the passenger unit. At which vertebral level is this center of gravity located?
View Answer & Explanation
Correct Answer: D
Rationale: The text specifically states that while the global center of gravity is at S2, the clinically paramount center of gravity for the passenger unit (comprising ~70% of body mass) is located at the level of the tenth thoracic vertebra (T10).
Question 38
A 62-year-old male with severe right-sided genu varum demonstrates a significant leftward trunk lean during the stance phase of gait on his right leg. According to the provided text and biomechanical principles, what is the primary effect of this compensatory trunk lean on the ground reaction vector (GRV)?

View Answer & Explanation
Correct Answer: E
Rationale: As illustrated in the provided image and text, a lateral trunk lean (away from the affected side) shifts the passenger unit's center of gravity (T10) laterally. This physically "drags" the GRV laterally, which decreases the lever arm for the knee adduction moment, paradoxically offloading the painful medial compartment at the cost of overloading other structures like the hip abductors.
Question 39
A 66-year-old woman with end-stage medial compartment osteoarthritis and a varus deformity adopts a chronic lateral trunk sway. While this gait modification may reduce her medial knee pain, what is a significant negative biomechanical consequence of this compensation?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that a lateral trunk lean, used to shift the GRV, comes at a "steep physiological price." This includes a drastic increase in the workload on the hip abductors (ipsilateral to the stance limb) to maintain pelvic stability against the shifted center of mass.
Question 40
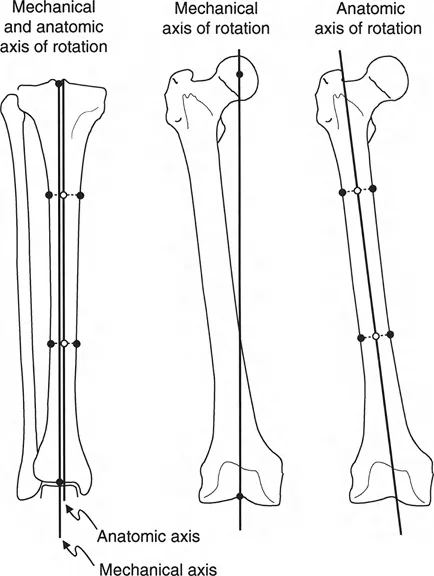
A surgeon is evaluating a full-length standing radiograph of a 55-year-old patient to plan a high tibial osteotomy. How is the mechanical axis of the lower extremity correctly defined?
View Answer & Explanation
Correct Answer: C
Rationale: The text provides a precise definition: the mechanical axis is a straight line drawn from the center of the femoral head to the center of the ankle joint (tibial plafond). This is the cornerstone of knee deformity analysis in the Paley method.
Question 41
A 30-year-old patient with a perfectly aligned lower extremity undergoes a biomechanical gait analysis. In a normal limb, where does the mechanical axis typically pass relative to the center of the knee joint, creating the physiologic Mechanical Axis Deviation (MAD)?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that in a normal, healthy lower limb, the mechanical axis passes slightly medial to the center of the knee joint, creating a physiologic Mechanical Axis Deviation (MAD) of approximately 8 mm medial to the center of the tibial plateau.
Question 42
A 60-year-old male presents with a painful valgus (knock-kneed) deformity of his left knee. On his long-leg alignment radiograph, where would the Mechanical Axis Deviation (MAD) be located?
View Answer & Explanation
Correct Answer: C
Rationale: The text defines a valgus deformity as a condition where the mechanical axis is shifted laterally, causing the MAD to fall lateral to the center of the knee joint. This overloads the lateral compartment.
Question 43
In a biomechanically normal knee, the physiologic medial deviation of the mechanical axis results in a natural adduction moment during gait. What is the approximate load distribution between the medial and lateral compartments of the knee during the stance phase?
View Answer & Explanation
Correct Answer: D
Rationale: The text specifies that in a normally aligned knee, approximately 68% of the joint reactive force is transmitted through the medial compartment, with the remaining 32% transmitted through the lateral compartment.
Question 44
A 59-year-old patient has developed a progressive varus deformity. Biomechanical studies have shown that the relationship between the degree of malalignment and the shift in compartmental loading is not linear. A varus malalignment of just 6 degrees can shift what percentage of dynamic joint loading to the medial compartment?
View Answer & Explanation
Correct Answer: D
Rationale: The text highlights the exponential effect of malalignment, stating the "shocking clinical reality" that a mere 6 degrees of varus malalignment can shift nearly 100% of the dynamic joint loading entirely to the medial compartment.
Question 45
During a physical exam, a 63-year-old male with medial knee pain is observed to walk with a significant "toe-out" gait. According to biomechanical principles, what is the primary purpose of this subconscious gait modification?
View Answer & Explanation
Correct Answer: B
Rationale: The text explains that a "toe-out" gait, achieved through external rotation, physically places the ground reaction vector (GRV) closer to the center of the knee joint. This effectively reduces the adductor moment arm and, consequently, the painful load on the medial compartment.
Question 46
A 55-year-old woman with a varus knee deformity is noted to have a "toe-in" gait. How does this rotational compensation affect the biomechanics of her knee during the stance phase?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that, conversely to a toe-out gait, a "toe-in" gait (internal rotation) places the GRV further away from the center of the knee joint. This drastically increases the adductor moment arm and the painful load on the medial compartment.
Question 47
A 68-year-old male has progressive genu varum. In this condition, the medial compartment undergoes massive compressive overload. What is the corresponding pathological process that occurs in the lateral soft tissue envelope?
View Answer & Explanation
Correct Answer: C
Rationale: The text describes a predictable cascade where medial collapse leads to lateral "gapping." To compensate, the lateral structures (LCL, IT band, PLC) are subjected to chronic, repetitive tensile overload, which leads to structural attenuation (stretching) and functional laxity.
Question 48
A surgeon is reviewing radiographs of a patient with severe varus knee deformity. The surgeon measures the angle between a line tangential to the distal femoral articular surface and a line tangential to the proximal tibial articular surface. What is this critical angle called?
View Answer & Explanation
Correct Answer: D
Rationale: This describes the exact definition of the Joint Line Congruency Angle (JLCA) provided in the text. It is a direct measure of joint incongruity resulting from asymmetric cartilage loss and/or ligamentous laxity.
Question 49
An orthopedic resident is evaluating a patient with a varus knee. The attending surgeon points out that the Joint Line Congruency Angle (JLCA) is 8 degrees. What is the most important clinical implication of this finding?
View Answer & Explanation
Correct Answer: D
Rationale: The normal JLCA is 0° to 2°. An increased angle, such as 8°, is a "massive red flag" indicating severe joint incongruity. The text directly links this to asymmetric cartilage loss and, critically, significant lateral ligamentous laxity.
Question 50
A 70-year-old woman with end-stage genu varum is examined. During the stance phase of her gait, her knee is observed to bow outwards dynamically. What is this clinical sign called, and what does it represent?
View Answer & Explanation
Correct Answer: D
Rationale: The text defines this visible, dynamic lateral and outward bowing of the knee during weight-bearing as a varus thrust. It explicitly states that this sign manifests clinically when lateral tibial subluxation occurs and represents the end-stage of biomechanical joint failure.
Question 51
A 65-year-old male presents with a chief complaint of right knee pain from a severe varus deformity. On physical exam, he demonstrates a profound drop of the left pelvis when standing on his right leg. Classically, this gait is associated with hip pathology. What is the "infra-pelvic" cause for this gait abnormality described in the text?
View Answer & Explanation
Correct Answer: B
Rationale: The text introduces the critical and often-missed concept of an "infra-pelvic Trendelenburg." It explains that severe genu varum can be the root cause of a Trendelenburg gait, even in the presence of a healthy hip joint.
Question 52
A patient with a large genu varum deformity develops a Trendelenburg gait despite having a normal superior gluteal nerve and healthy hip abductor muscles. What is the compensatory kinematic change at the hip that leads to this gait pattern?

View Answer & Explanation
Correct Answer: D
Rationale: As shown in the image and explained in the text, to place the foot flat on the ground and maintain a stable base of support, a patient with genu varum must subconsciously compensate by abducting the femur at the hip joint. This is the primary kinematic change that initiates the biomechanical cascade leading to the Trendelenburg gait.
Question 53
A 58-year-old male with a 20-degree varus deformity of his right knee exhibits a Trendelenburg lurch. The compensatory femoral abduction required for him to walk has what direct effect on his gluteus medius muscle?
View Answer & Explanation
Correct Answer: B
Rationale: The text explains this using the Blix length-tension curve. Compensatory femoral abduction drastically reduces the distance between the gluteus medius origin (ilium) and insertion (greater trochanter). This functionally shortens and slackens the muscle, pushing it onto the inefficient descending limb of the curve and rendering it unable to generate sufficient force.
Question 54
A 61-year-old patient with severe genu varum and a secondary Trendelenburg gait undergoes a successful high tibial osteotomy (HTO) that corrects his coronal alignment. Postoperatively, his Trendelenburg gait resolves completely. Why does this occur without any direct hip surgery?
View Answer & Explanation
Correct Answer: C
Rationale: This is the central thesis of the "infra-pelvic Trendelenburg." Correcting the knee deformity eliminates the need for compensatory femoral abduction. The femur returns to its normal adducted position during stance, which restores the optimal length and tension of the gluteus medius, allowing it to function effectively again.
Question 55
A surgeon is analyzing a standing AP radiograph to determine the location of a varus deformity. The angle between the mechanical axis of the femur and the joint line of the distal femur is measured. What is this angle called?
View Answer & Explanation
Correct Answer: B
Rationale: The text and its associated table define the Mechanical Lateral Distal Femoral Angle (mLDFA) as the angle that determines distal femoral coronal alignment. It is measured between the femoral mechanical axis and the distal femoral joint line.
Question 56
An orthopedic surgeon measures the Medial Proximal Tibial Angle (MPTA) on a patient's radiograph and finds it to be 80°. What is the significance of this measurement?

View Answer & Explanation
Correct Answer: C
Rationale: The normal MPTA is 85° to 90°. As shown in the provided image and explained in the text, a low MPTA (<85°), such as 80°, indicates tibia vara. This definitively locates the source of the varus deformity to the proximal tibia.
Question 57
A 45-year-old bioengineer is designing a prosthetic limb. She wants to maximize the rotational power of an artificial muscle actuator at a joint. According to fundamental biomechanical principles, the moment generated by this actuator is a product of which two variables?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly defines a moment (M) as the product of the muscle's force (F) and its lever arm (d), which is the perpendicular distance from the joint's center of rotation to the muscle's line of action (M = F × d). Option A describes power, not moment.
Question 58
A 22-year-old ballet dancer presents with posterior ankle pain. An MRI and biomechanical analysis are performed. The analysis reveals a dynamic change in the Achilles tendon's lever arm during plantarflexion and dorsiflexion, as depicted in the provided diagram. What is the primary physiological benefit of this mechanism?

View Answer & Explanation
Correct Answer: B
Rationale: The text explains that as the triceps surae shortens during plantarflexion, it becomes weaker according to the length-tension curve. The simultaneous increase in its lever arm compensates for this reduced force production, helping to maintain a constant propulsive moment. Option A is incorrect; muscle force decreases as the muscle shortens from its optimal length.
Question 59
A 58-year-old male with a history of a malunited calcaneal fracture complains of a weak and inefficient gait. He struggles to push off during walking. This patient's primary difficulty corresponds to a disruption of which phase of the gait cycle?

View Answer & Explanation
Correct Answer: C
Rationale: The third (forefoot) rocker is the primary power-generating phase responsible for propulsion or "push-off." A calcaneal malunion can shorten the lever arm of the triceps surae, catastrophically impairing its ability to generate the necessary moment for this phase. The first rocker involves controlled plantarflexion after heel strike.
Question 60
A 15-year-old female with developmental dysplasia of the hip is noted to have a femoral neck-shaft angle of 150 degrees (coxa valga). According to the principles of lever arm mechanics, what is the most significant biomechanical consequence of this deformity on the hip abductor muscles?

View Answer & Explanation
Correct Answer: B
Rationale: As illustrated in the diagram and explained in the text, coxa valga medializes the greater trochanter relative to the femoral head's center of rotation. This action directly shortens the perpendicular distance (lever arm) for the abductor muscles, forcing them to generate much higher forces to create the same stabilizing moment.
Question 61
A 55-year-old man is evaluated for a painful, lurching gait. He is observed to lean his upper body significantly over his right leg during the single-leg stance phase. This gait modification is a compensation designed to achieve what biomechanical goal?

View Answer & Explanation
Correct Answer: B
Rationale: The abductor lurch (Duchenne gait) is a compensatory mechanism. By leaning the trunk over the stance limb, the patient shifts their center of gravity closer to the hip joint (the fulcrum). This shortens the lever arm of the body weight, thereby reducing the external adduction moment that the weakened or mechanically disadvantaged abductors must counteract.
Question 62
A 68-year-old male presents with worsening medial-sided right knee pain and a bow-legged appearance. A long-leg standing radiograph is obtained. The line drawn from the center of the femoral head to the center of the ankle passes 25 mm medial to the center of the knee. What does this measurement represent?

View Answer & Explanation
Correct Answer: C
Rationale: The text defines the Mechanical Axis Deviation (MAD) as the pathological displacement of the mechanical axis (femoral head center to ankle center) from the center of the knee. A medial deviation, as described, indicates a varus deformity and an increased external adduction moment on the knee.
Question 63
A 17-year-old male with a history of a malunited slipped capital femoral epiphysis (SCFE) presents with a painless limp. His radiographs demonstrate a significantly shortened femoral neck (coxa breva). From a biomechanical standpoint, this condition is most analogous to which other deformity?

View Answer & Explanation
Correct Answer: C
Rationale: The text and accompanying figure explicitly state that coxa breva (short femoral neck) has the same devastating biomechanical effect as coxa valga. Both conditions reduce the perpendicular distance from the greater trochanter to the hip's center of rotation, shortening the abductor lever arm and compromising the abductor mechanism.
Question 64
During the second rocker of gait, the tibia advances over a plantigrade foot. The triceps surae is active during this phase. What is the primary function of the triceps surae during this specific phase?
View Answer & Explanation
Correct Answer: B
Rationale: The text describes the second (ankle) rocker as the phase where the body's momentum carries the tibia forward. The triceps surae works eccentrically (acting as a brake) to control this forward progression and decelerate the body. Concentric contraction for propulsion occurs in the third rocker.
Question 65
A 62-year-old female is being evaluated for a total hip arthroplasty. Preoperative planning focuses on restoring the abductor mechanism. If the abductor lever arm is reduced by 50% due to poor component placement, by what factor must the abductor muscle force increase to generate the same pelvic-stabilizing moment?
View Answer & Explanation
Correct Answer: C
Rationale: This is a direct application of the moment equation (M = F × d). If the moment (M) must remain constant and the lever arm (d) is halved (0.5d), the force (F) must be doubled (2F) to maintain the equality (M = 2F × 0.5d). Therefore, the force must increase by a factor of 2.0.
Question 66
A 65-year-old woman with gluteus medius insufficiency is examined. When she stands on her affected right leg, her left pelvis drops. What is the name of this clinical sign?
View Answer & Explanation
Correct Answer: D
Rationale: The text defines the Trendelenburg sign as the dropping of the pelvis on the contralateral (swing) side during single-leg stance on the affected side. This indicates failure of the stance-limb abductors to stabilize the pelvis. The Duchenne sign refers to the compensatory trunk lurch, not the pelvic drop itself.
Question 67
A patient with a flexible flatfoot deformity complains of rapid fatigue during long walks. The deformity causes a collapse of the medial longitudinal arch during the push-off phase of gait. How does this disrupt the third rocker?
View Answer & Explanation
Correct Answer: B
Rationale: The text emphasizes that for the third rocker to be effective, the foot must function as a rigid lever to propel the body forward. A flexible flatfoot deformity prevents the foot from becoming rigid, causing energy to be dissipated within the collapsing arch rather than being used for propulsion, leading to an inefficient gait.
Question 68
A 70-year-old male with severe genu valgum (knock-kneed) deformity is evaluated for a high tibial osteotomy. A standing long-leg radiograph would be expected to show the mechanical axis falling in which location relative to the knee joint?
View Answer & Explanation
Correct Answer: C
Rationale: As described in the text and shown in the diagram, a valgus deformity shifts the mechanical axis laterally. This lateral Mechanical Axis Deviation (MAD) increases the lever arm of the ground reaction force, creating a large external abduction moment that overloads the lateral compartment of the knee.
Question 69
A 12-year-old boy is recovering from Legg-Calve-Perthes disease of the right hip. He has developed coxa breva and coxa magna. His parents are concerned about his prominent limp. The biomechanical deficit leading to his limp is primarily caused by a reduction in the:
View Answer & Explanation
Correct Answer: D
Rationale: The text clearly states that coxa breva (a short femoral neck), a common sequela of Perthes disease, severely compromises the abductor lever arm. This mechanical disadvantage of the gluteus medius is the primary cause of the abductor lurch or Trendelenburg gait.
Question 70
The function of two-joint muscles like the hamstrings is biomechanically efficient during complex movements like a sit-to-stand maneuver. What is the primary reason for this efficiency?
View Answer & Explanation
Correct Answer: B
Rationale: The text explains this compensatory mechanism. During a sit-to-stand, the hamstrings shorten at the hip (hip extension) while lengthening at the knee (knee extension). This concurrent action results in minimal net change in muscle length, allowing the muscle to operate at a more favorable, powerful point on its length-tension curve throughout the movement.
Question 71
A 72-year-old male with the clinical appearance shown in the image presents with severe right knee pain that is worse with walking. Based on the deformity pictured, which compartment of his knee is most likely experiencing overload due to an increased external moment?

View Answer & Explanation
Correct Answer: A
Rationale: The clinical image shows a significant varus (bow-legged) deformity. In varus, the mechanical axis shifts medially, which increases the lever arm for the ground reaction force relative to the knee's center. This creates a large external adduction moment that disproportionately loads and wears down the medial compartment.
Question 72
In the context of the foot and ankle during gait, the first (heel) rocker is primarily controlled by the eccentric action of which muscle group?
View Answer & Explanation
Correct Answer: D
Rationale: The text states that the first rocker occurs at initial contact and involves the pretibial muscles working eccentrically to control the descent of the forefoot to the ground. This action prevents "foot slap" and absorbs shock. The triceps surae is primarily active in the second and third rockers.
Question 73
A surgeon is performing a valgus-producing intertrochanteric osteotomy to treat hip dysplasia with coxa valga. What is the primary biomechanical goal of laterally displacing the greater trochanter during this procedure?
View Answer & Explanation
Correct Answer: C
Rationale: Coxa valga is characterized by a medialized greater trochanter and a short abductor lever arm. A key goal of corrective surgery is to move the greater trochanter laterally, away from the center of the femoral head. This directly increases the abductor lever arm, improving the mechanical advantage of the gluteus medius and reducing the force required to stabilize the pelvis.
Question 74
The image depicts the foot acting as a second-class lever during the third rocker of gait. In this lever system, what anatomical structure serves as the fulcrum?
View Answer & Explanation
Correct Answer: C
Rationale: The diagram and text clearly identify the components of the second-class lever during the third rocker. The effort is the pull of the triceps surae, the load is the body weight acting through the ankle, and the fulcrum (pivot point) is at the metatarsal heads, over which the foot pivots to propel the body forward.
Question 75
A 30-year-old patient with a history of a femoral neck fracture malunion develops a painful limp. Radiographs confirm coxa breva. The patient is counseled that without surgical correction, the constant mechanical disadvantage of the abductors will most likely lead to what long-term consequence?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that the constant mechanical disadvantage imposed by a shortened lever arm leads to rapid muscle fatigue, a painful limp, and eventually, abductor failure and early joint degeneration. The muscles are chronically overloaded, not hypertrophied.
Question 76
The classic length-tension curve for skeletal muscle dictates that a muscle's force production capacity is greatest at its optimal resting length. How does the body's musculoskeletal design often compensate for the fact that muscles weaken as they shorten during a contraction?
View Answer & Explanation
Correct Answer: C
Rationale: The text introduces this as a primary compensatory mechanism. The example of the triceps surae is used, where the lever arm increases as the muscle shortens during plantarflexion. This increase in the lever arm (d) helps to offset the decrease in force (F), maintaining the overall moment (M = F × d).
Question 77
A 19-year-old male presents with a painful, lurching gait and a 7 cm limb length discrepancy following neonatal septic arthritis of his left hip. On physical examination, he demonstrates a profound drop of the right pelvis when standing on his left leg. This compensatory lurch is necessary to shift his center of gravity over the affected limb. What is the underlying biomechanical failure causing this gait pattern?
View Answer & Explanation
Correct Answer: B
Rationale: The text states that in severe proximal femoral deficiency, the anatomical fulcrum (the femoral head articulating with the acetabulum) is lost. This initiates the biomechanical cascade of abductor insufficiency and pelvic drop, leading to the Trendelenburg gait. Adductor contracture is a separate issue and does not cause the primary instability.
Question 78
A 22-year-old female with a history of post-traumatic massive bone loss of the proximal femur presents with a disabling Trendelenburg gait and 6 cm of shortening. She is an active individual who finds her current disability intolerable. Radiographs confirm the absence of the femoral head and neck. Given her age and the catastrophic bone loss, what is the most appropriate reconstructive procedure described?

View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly identifies the Paley Pelvic Support Osteotomy as a transformative solution for young, active patients with catastrophic loss of the proximal femur for whom standard THA is impossible and arthrodesis is functionally undesirable. A Girdlestone procedure would result in a poor functional outcome and would not address the instability or limb length discrepancy.
Question 79
A 25-year-old patient with sequelae of poliomyelitis has a flail hip with complete absence of abductor muscle function confirmed by physical exam and EMG. The patient has a high-riding femur and significant limb length discrepancy. When considering a Paley Pelvic Support Osteotomy, the lack of abductor function represents what?
View Answer & Explanation
Correct Answer: C
Rationale: The text clearly lists "Absent or denervated abductor musculature" as an absolute contraindication. The procedure restores the biomechanics for the muscles to work; it cannot create function if the muscles are absent or denervated. A relative contraindication, such as severe osteoporosis, might be manageable, but absent abductors preclude a successful outcome.
Question 80
A surgeon is planning an Ilizarov hip reconstruction for a 17-year-old with chronic, irreducible developmental dysplasia of the hip. To accurately define the surgical parameters and capture the dynamic instability of the hip, which radiographic view is described as unequivocally the most important?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "This is unequivocally the most important initial image in the planning phase. The patient must stand solely on the affected leg *without any external support*". This view is essential to assess the maximum proximal femoral migration and plan the osteotomy level.
Question 81
A 20-year-old undergoes a Paley Pelvic Support Osteotomy. The procedure involves creating a complex, double-level femoral deformity. What is the primary biomechanical goal of creating the proximal osteotomy shelf?

View Answer & Explanation
Correct Answer: B
Rationale: The text explains that the ultimate goal is to surgically break the vicious cycle of instability. It achieves this "By creating a new, stable, bony fulcrum (the proximal osteotomy shelf)," which allows the pelvis to rest securely on the femur. While the procedure does affect the mechanical axis, its primary purpose is to re-establish a fulcrum.
Question 82
A resident is learning about hip biomechanics in preparation for a deformity correction case. During a normal single-leg stance, the hip joint functions as a balanced, dynamic lever system. According to the provided text, how is this system classified?
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly states, "During a normal single-leg stance... the hip functions as a finely balanced, dynamic first-class lever system." It defines the fulcrum (femoral head), load (body weight), and effort (abductors) consistent with this classification.
Question 83
A 16-year-old with complete destruction of the right femoral head from a childhood infection is examined. When she stands on her right leg, her left pelvis drops significantly. According to the biomechanical cascade described, what is the most direct cause of this pelvic drop?
View Answer & Explanation
Correct Answer: C
Rationale: The text outlines a "vicious cycle" where the loss of the fulcrum leads to abductor insufficiency because the muscles lose their resting tension. This functional powerlessness of the abductors directly results in the inability to support the pelvis, causing it to drop on the contralateral side. Fixed pelvic obliquity is a potential long-term consequence, not the direct cause of the dynamic drop.
Question 84
A 28-year-old patient presents with a painful Trendelenburg gait due to a chronic irreducible hip dislocation. Clinical measurement and scanogram reveal a limb length discrepancy of 5.5 cm. Based on the typical indications mentioned in the text, does this patient's LLD meet the criteria for considering a Paley Pelvic Support Osteotomy?
View Answer & Explanation
Correct Answer: C
Rationale: The text lists "significant limb length discrepancy (usually >4 cm)" as a key clinical symptom and indication for the procedure. A 5.5 cm LLD falls squarely within this range. The text also states that patients should ideally be skeletally mature.
Question 85
A 30-year-old patient with severe proximal femoral deficiency is a potential candidate for an Ilizarov hip reconstruction. However, the patient has a documented history of poor compliance with medical treatments and struggles with the cognitive understanding of a complex, multi-month external fixator protocol. How would this psychosocial issue be classified as a contraindication?
View Answer & Explanation
Correct Answer: B
Rationale: The table of contraindications lists "Severe cognitive or psychosocial issues" as a relative contraindication. The rationale is that the patient must be able to comply with the demanding external fixator and pin-care regimen. It is not absolute, as with sufficient social support it might be overcome, but it is a significant concern.
Question 86
A 21-year-old patient with an unsalvageable hip from post-infectious destruction is considering surgical options. Historically, a Girdlestone resection arthroplasty was an option. Compared to the Girdlestone procedure, what is the primary advantage of the Paley Pelvic Support Osteotomy?
View Answer & Explanation
Correct Answer: C
Rationale: The text describes the Girdlestone procedure as offering a "poor functional outcome." The Paley osteotomy, in contrast, is designed to create a stable pseudo-joint, eliminate the Trendelenburg gait, and equalize limb length, thereby restoring function. A Girdlestone procedure exacerbates instability and shortening.
Question 87
A 15-year-old female presents with a severe limp and pain. The radiograph shown is taken. Based on the principles discussed in the text, what is the primary biomechanical problem demonstrated by the proximal migration of the left femur?
View Answer & Explanation
Correct Answer: C
Rationale: The image shows severe proximal femoral migration, which signifies the loss of the femoral head's articulation with the acetabulum. The text explains this as the "Loss of Fulcrum," which leads to the abductor muscles losing their normal insertion-to-origin distance and resting tension, rendering them insufficient.
Question 88
The postoperative radiograph of a patient who underwent an Ilizarov hip reconstruction is shown. The valgus osteotomy in the proximal femur is designed to create a specific biomechanical structure to support the pelvis. What is this structure called?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states that the surgery works by "creating a new, stable, bony fulcrum (the proximal osteotomy shelf)." This shelf, created by the valgus subtrochanteric osteotomy, is what allows the pelvis to rest securely on the proximal femur.
Question 89
A 72-year-old female with a history of chronic irreducible hip dislocation and severe, medically-documented osteoporosis presents with a painful Trendelenburg gait. She is otherwise healthy. Why would she be considered a poor candidate for a Paley Pelvic Support Osteotomy?
View Answer & Explanation
Correct Answer: B
Rationale: The text lists "Severe osteoporosis" as a relative contraindication. The clinical rationale provided is that "Poor bone stock severely compromises the purchase and stability of the Ilizarov external fixator half-pins and wires." While her age is also a factor, the specific contraindication mentioned in the text is the poor bone quality.
Question 90
During a discussion of normal hip biomechanics, a surgeon describes the hip as a first-class lever. In this system, the body weight acts as the load and the femoral head acts as the fulcrum. What anatomical structure provides the "Effort" to counterbalance the load?
View Answer & Explanation
Correct Answer: C
Rationale: The text clearly defines the components of the first-class lever system of the hip: "The Effort: The hip abductor muscle complex (primarily the gluteus medius and minimus), contracting to exert a powerful counterbalancing upward force on the greater trochanter."
Question 91
A patient with a destroyed left hip demonstrates a positive Trendelenburg sign, with the right side of the pelvis dropping during left single-leg stance. To prevent falling, the patient must rapidly shift their upper body. What is this characteristic compensatory maneuver called?
View Answer & Explanation
Correct Answer: D
Rationale: The text defines the Trendelenburg gait as the compensatory maneuver for the Trendelenburg sign. It states, "To prevent falling over, the patient must rapidly shift their entire upper body torso and center of gravity laterally over the affected limb. This compensatory maneuver is the characteristic, energy-inefficient Trendelenburg gait."
Question 92
A 24-year-old has chronic irreducible developmental dysplasia of the hip (DDH) with a completely absent true acetabulum and a severely distorted proximal femur. According to the text, why is a standard total hip arthroplasty (THA) often technically impossible in such cases?
View Answer & Explanation
Correct Answer: C
Rationale: The introductory paragraph states that the Paley osteotomy is considered when "standard total hip arthroplasty is technically impossible due to catastrophic bone stock loss or active infection history." The text implies that the severe anatomical distortion and deficiency of bone make stable placement of prosthetic components unfeasible.
Question 93
A 31-year-old patient with post-infectious destruction of the proximal femur is evaluated for a pelvic support osteotomy. The physical exam reveals a chronic, actively draining sinus tract over the greater trochanter, and MRI confirms active osteomyelitis. Why is this finding an absolute contraindication?
View Answer & Explanation
Correct Answer: B
Rationale: The contraindication table lists "Active, uncontrolled deep bone infection" as absolute. The rationale provided is: "External fixation pins passing through infected tissue can lead to catastrophic sepsis and frame failure." This risk is unacceptable.
Question 94
A 34-year-old female with a history of developmental dysplasia of the hip (DDH) presents with a painful limp and functional leg length discrepancy. When initiating preoperative planning for a proximal femoral osteotomy, what is considered the most reliable and stable horizontal reference line on an AP pelvis radiograph?
View Answer & Explanation
Correct Answer: C
Rationale: The line connecting the inferior aspects of the SI joints is the gold standard because the SI joints are robust, centrally located, and minimally affected by the dysplastic changes that often distort other pelvic landmarks like the iliac crests or acetabula in pathologies like DDH.
Question 95
A 7-year-old boy with no prior surgical history presents with coxa vara. For preoperative planning of a valgus osteotomy, which landmark provides an excellent and easily identifiable horizontal reference line on his AP pelvis radiograph?
View Answer & Explanation
Correct Answer: C
Rationale: In a skeletally immature patient with an unoperated pelvis, the triradiate cartilage is a highly reliable and easily visible landmark for establishing the pelvic horizontal line. The SI joints are also reliable but the triradiate cartilage is often preferred in this specific population.
Question 96
A 9-year-old girl with a history of a prior Pemberton pelvic osteotomy for hip dysplasia presents with a residual proximal femoral deformity. The surgeon notes that the triradiate cartilages appear asymmetric on the AP pelvis radiograph. What is the most appropriate horizontal reference line to use for planning her femoral correction?
View Answer & Explanation
Correct Answer: D
Rationale: When a prior pelvic osteotomy has been performed, the triradiate cartilages can become asymmetric and are no longer reliable. The surgeon must revert to the universally applicable adult landmarks, the inferior SI joints or sacral foramina, which are insulated from such iatrogenic changes.
Question 97
A surgeon is meticulously planning a proximal femoral osteotomy for a varus deformity. After establishing the pelvic horizontal line, the next step is to draw the Proximal Mechanical Axis (PMA). How is the PMA correctly defined and drawn?
View Answer & Explanation
Correct Answer: C
Rationale: The PMA represents the ideal, corrected orientation of the proximal femur. It is defined biomechanically relative to a level pelvis, not by the patient's existing deformed anatomy. It is always drawn 90 degrees to the pelvic horizontal line through the hip center.
Question 98
During a preoperative assessment for a complex lower limb deformity, a surgeon needs to determine the existing alignment of the distal limb segment. How is the Distal Mechanical Axis (DMA) accurately constructed on a full-length standing radiograph?
View Answer & Explanation
Correct Answer: C
Rationale: The DMA represents the actual, existing alignment of the distal lower extremity. It is defined by a line connecting the center of the ankle and knee joints, which is then extended proximally toward the hip to identify any deviation from the ideal axis.
Question 99
A 25-year-old male has a post-traumatic varus deformity of the proximal femur. The surgeon has drawn the Proximal Mechanical Axis (PMA) and the Distal Mechanical Axis (DMA). According to Paley's principles, how is the Center of Rotation of Angulation (CORA) for this deformity identified?
View Answer & Explanation
Correct Answer: D
Rationale: The CORA is the precise mathematical epicenter of an angular deformity. For hip and proximal femoral deformities, it is defined as the exact intersection point of the idealized PMA and the actual DMA. This point is critical for planning a mechanically sound osteotomy.
Question 100
A 19-year-old patient presents with a severe adduction deformity of the left hip. The preoperative radiograph is shown in the left panel. What is the most accurate interpretation of the tilted yellow pelvic line?

View Answer & Explanation
Correct Answer: B
Rationale: The image demonstrates a classic apparent LLD. The fixed adduction deformity forces the pelvis to elevate on the affected side to allow the foot to clear the ground, creating pelvic obliquity. This is a functional, not a structural, shortening. The goal of surgery is to level the pelvis by correcting the angle.
You Might Also Like
