Comprehensive Orthopedic Deformity Planning, Arthroplasty & Biomechanics Review | Part 3

Key Takeaway
Orthopedic deformity correction involves meticulous lower limb alignment analysis using Paley's principles, joint orientation angles (mLDFA, MPTA, JLCA), and mechanical axis deviation (MAD). It integrates biomechanics, gait analysis, and radiographic interpretation to plan complex osteotomies and total joint arthroplasties (TKA, THA), addressing issues like patella baja and rotational malalignment for optimal surgical outcomes.
Question 1
What is the average value for the Medial Proximal Tibial Angle (MPTA) in a normally aligned limb, which serves as a target for the proximal tibial cut in a TKR?
View Answer & Explanation
Correct Answer: B
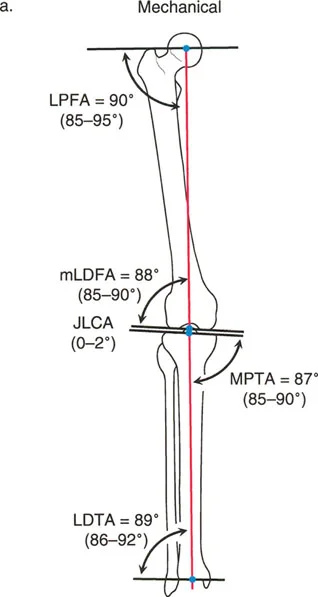
Rationale: The provided table of joint orientation angles lists the normal range for the MPTA as 85° to 90°, with an average value of 87°.
Question 2
A 66-year-old patient undergoes a TKR for a valgus knee with a significant distal femoral deformity. The surgeon successfully corrects the knee alignment. Postoperatively, the patient develops ankle pain. Which joint orientation angle is most important for ensuring the ankle joint remains parallel to the ground after proximal corrections?
View Answer & Explanation
Correct Answer: C
Rationale: The text specifies that the Mechanical Lateral Distal Tibial Angle (mLDTA) "Ensures the ankle joint remains parallel to the ground after proximal corrections, preventing secondary ankle arthrosis."
Question 3
A surgeon is planning a complex TKR and is determining the location of the CORA. How is the CORA geometrically identified on a radiograph?
View Answer & Explanation
Correct Answer: C
Rationale: The text and the associated diagram clearly define the CORA as "the exact intersection point" of the proximal mechanical axis line and the distal mechanical axis line of a deformed bone.
Question 4
A 75-year-old male with Paget's disease has severe bowing of his femur and tibia, resulting in debilitating knee arthritis. His surgeon is planning a TKR. Why is it considered "dangerously insufficient" to rely only on standard short-leg AP and lateral X-rays for preoperative planning in this case?
View Answer & Explanation
Correct Answer: C
Rationale: The text strongly warns that relying on short-leg films is "dangerously insufficient" because a comprehensive deformity analysis, including measurement of the MAD and identification of extra-articular CORAs, requires full-length standing radiographs.
Question 5
What is the average value for the Mechanical Lateral Distal Femoral Angle (mLDFA) that dictates the standard distal femoral valgus cut in a TKR?
View Answer & Explanation
Correct Answer: C
Rationale: The provided table lists the normal range for the mLDFA as 85° to 90°, with an average value of 88°.
Question 6
The fundamental philosophy of applying Paley's principles to arthroplasty is based on a critical paradigm shift for the surgeon. This shift involves evolving from a joint "replacer" to what?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that to succeed in these complex cases, "the orthopedic surgeon must evolve their mindset from a joint 'replacer' to a comprehensive limb 'reconstructor'."
Question 7
A 68-year-old male presents with severe knee pain and a 20-degree varus deformity. A full-length standing radiograph reveals end-stage medial compartment osteoarthritis with significant condylar collapse. The femoral and tibial diaphyses are well-aligned. According to Paley's principles, why is a standard total knee arthroplasty (TKR) with intra-articular bone cuts likely to be successful in correcting this deformity?
View Answer & Explanation
Correct Answer: B
Rationale: The text states that when the CORA is intra-articular, as in cases of severe asymmetric articular wear and condylar collapse, standard arthroplasty cuts follow Paley's Rule 1. This allows for pure angulation to correct the deformity without creating a secondary translation. The location of the CORA, not the magnitude of the deformity, is the key principle.
Question 8
A 62-year-old female with a history of a healed midshaft femoral fracture with 15 degrees of varus malunion presents for TKR. The surgeon plans to correct the overall limb alignment solely by making asymmetric intra-articular bone resections. This approach is a direct violation of which of Paley's Osteotomy Rules and is known as what specific error?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly defines the "Arthroplasty Trap" as a direct violation of Paley's Rule 3. This occurs when an osteotomy (or in this case, arthroplasty cuts) is performed outside the CORA (which is in the midshaft) without translation, creating a secondary "zig-zag" deformity, severe joint line obliquity, and ligament imbalance.
Question 9
A 55-year-old male is undergoing a TKR for a knee with a significant extra-articular varus deformity of the femur. The CORA is located in the distal femoral diaphysis. The surgeon uses a stemmed femoral component with a built-in offset to translate the joint surface medially relative to the diaphyseal fixation. This technique is an application of which of Paley's principles?
View Answer & Explanation
Correct Answer: B
Rationale: The text states that according to Paley's Rule 2, when an osteotomy is performed outside the CORA, the bone ends must be translated to realign the mechanical axis. Using an offset stem in arthroplasty is a direct application of this rule, allowing the surgeon to translate the diaphyseal fixation relative to the joint line.
Question 10
A 70-year-old male undergoes TKR for a severe varus knee secondary to a healed proximal tibial fracture malunion. The surgeon corrects the limb alignment with asymmetric bone cuts, resulting in a joint line that is now oblique to the ground. This will most likely lead to which of the following biomechanical consequences?
View Answer & Explanation
Correct Answer: C
Rationale: The text warns that creating severe joint line obliquity, a consequence of the "Arthroplasty Trap," alters the kinematics of the knee and causes shear stresses on the polyethylene, which can lead to accelerated wear and failure. Distractor D is incorrect; this maneuver creates profound collateral ligament imbalance.
Question 11
A 59-year-old female is being evaluated for conversion of a high tibial osteotomy (HTO) to a TKR. She reports that the original HTO provided no pain relief, and she has a documented history of Complex Regional Pain Syndrome (CRPS). According to the provided text, what is the significance of this history?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that if a patient experienced no relief after the HTO or has a history of CRPS, the prognosis for a successful TKR decreases significantly. It highlights the importance of identifying and managing psychosocial factors preoperatively.
Question 12
A 65-year-old male requires a TKR after a previous HTO was performed through a transverse incision. He also has a scar from a prior arthroscopy. When planning the surgical approach for the TKR, what is the most critical principle to follow to minimize the risk of skin necrosis?
View Answer & Explanation
Correct Answer: B
Rationale: The text emphasizes that the vascular supply to the anterior knee skin is precarious. To avoid catastrophic skin necrosis, the surgeon must utilize the most lateral viable incision and cross previous scars at 90-degree angles when possible. Using the most lateral incision preserves the medial blood supply, which is critical for the standard medial parapatellar approach.
Question 13
A 58-year-old female who underwent a closing wedge valgus-producing HTO 10 years ago now presents for TKR. On examination, she has a foot drop and weakness of ankle dorsiflexion. A thorough preoperative neurologic exam is critical to document a potential injury to which nerve?
View Answer & Explanation
Correct Answer: D
Rationale: The text identifies peroneal nerve palsy as a known complication of proximal tibial osteotomies, especially closing wedge valgus-producing osteotomies that require fibular osteotomy or proximal tibiofibular joint disruption. The clinical finding of a foot drop is classic for a peroneal nerve injury.
Question 14
A 61-year-old male presents with recurrent patellar subluxation after TKR. His TKR was a conversion from a previous HTO. Radiographic analysis reveals that the tibial tubercle is markedly lateralized relative to the trochlear groove. This complication is most likely due to which unaddressed deformity from the original HTO?
View Answer & Explanation
Correct Answer: D
Rationale: The text explains that if the distal tibial fragment heals in excessive external rotation after an HTO, the tibial tubercle becomes mechanically lateralized. This increases the Q-angle and creates a massive lateral vector on the extensor mechanism, leading to inevitable patellar subluxation or dislocation if not addressed during the TKR.
Question 15
During a TKR for a patient with severe post-HTO rotational malalignment and lateralized tibial tubercle, the surgeon finds that a standard lateral retinacular release is insufficient to stabilize the patella. According to the text, what is the most appropriate definitive surgical procedure to correct the patellar tracking in this structural deformity?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that in extreme cases of rotational mismatch and lateralized tubercle, the structural deformity must be addressed with a tibial tubercle medialization procedure (like an Elmslie-Trillat osteotomy). This physically moves the extensor mechanism medially, which soft tissue releases alone cannot accomplish.
Question 16
A surgeon is planning a conversion TKR for a patient with a prior HTO. Preoperative radiographs show retained staples from the HTO located directly in the path of the planned tibial intramedullary (IM) guide. What is the primary implication of this finding for the surgical plan?
View Answer & Explanation
Correct Answer: B
Rationale: The text identifies retained hardware as a critical roadblock. It states that staples, plates, or screws will obstruct the tibial IM canal, preventing the use of IM guides or stemmed components. Therefore, they must be identified for planned removal.
Question 17
A 66-year-old male presents for TKR 15 years after a lateral closing wedge HTO. Radiographs demonstrate a significantly narrowed medial-lateral width of the proximal tibia. What is the most likely surgical challenge this "truncated" metaphysis will present during tibial component sizing?
View Answer & Explanation
Correct Answer: C
Rationale: The text explains that a lateral closing wedge osteotomy truncates the lateral tibial metaphysis, narrowing its M-L width. This makes seating a standard symmetric prosthesis difficult, often leading to dangerous medial overhang (soft tissue irritation) or lateral under-coverage (risk of subsidence).
Question 18
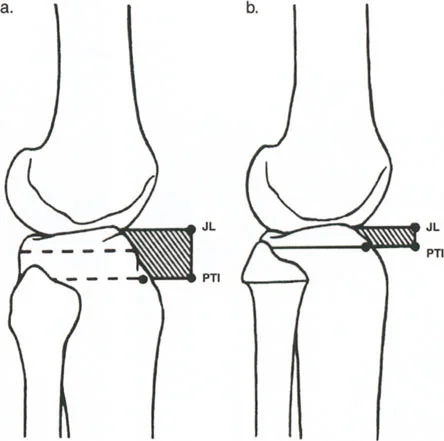
A 57-year-old female who had a closing wedge HTO proximal to the tibial tubercle now requires a TKR. She is found to have iatrogenic patella baja. What is the underlying geometric cause of this condition?
View Answer & Explanation
Correct Answer: B
Rationale: The text and accompanying diagram clearly illustrate that patella baja after a closing wedge HTO is a purely geometric problem. The osteotomy brings the proximal segment (with the joint line) down to the distal segment (with the patellar tendon insertion), fundamentally shortening the distance between these two points and pulling the patella distally.
Question 19
During a TKR conversion in a patient with severe patella baja, the surgeon is unable to subluxate the patella laterally even after a medial parapatellar arthrotomy and a full lateral retinacular release. The tension on the extensor mechanism is moderate. According to the provided surgical hierarchy, what is the next appropriate step to improve exposure?
View Answer & Explanation
Correct Answer: C
Rationale: The table "Surgical Pearls for Managing Patella Baja Exposure" indicates a stepwise approach. For moderate tension when a lateral release is insufficient, the next step is a rectus snip. A V-Y plasty or TTO is reserved for more severe cases.
Question 20
A 60-year-old patient with extreme patella baja and a severely contracted extensor mechanism requires a TKR. The surgeon determines that a rectus snip will be insufficient. Which of the following procedures provides the most significant lengthening of the extensor mechanism but requires a period of postoperative immobilization?
View Answer & Explanation
Correct Answer: D
Rationale: The text describes the V-Y quadricepsplasty as the technique for severe tension and a contracted extensor mechanism. It involves an inverted V incision repaired as a Y to effectively lengthen the mechanism and explicitly notes that it requires postoperative immobilization.
Question 21
A 63-year-old male presents for TKR with a 15-degree valgus deformity that resulted from an over-corrected HTO for previous varus arthritis. Where is the CORA for the current valgus deformity located?
View Answer & Explanation
Correct Answer: C
Rationale: The text highlights that a valgus deformity after an over-corrected HTO is fundamentally different from primary valgus osteoarthritis. The deformity is not intra-articular but is located extra-articularly in the proximal tibial diaphysis/metaphysis, at the site of the previous osteotomy.
Question 22
When performing a TKR on a patient with a severe valgus deformity located in the proximal tibia from a prior HTO, what is the major risk of making a standard distal femoral cut of 5-7 degrees of valgus?
View Answer & Explanation
Correct Answer: B
Rationale: The text describes this as the "Templating Trap." Because the valgus deformity is in the tibia, a standard femoral valgus cut will be additive, placing the knee into even more valgus relative to the already deformed tibia. This would then require a dangerously asymmetric tibial cut to compensate.
Question 23
A 67-year-old patient has a severe, 25-degree extra-articular varus deformity of the proximal tibia. The surgeon determines that correction with intra-articular cuts would lead to catastrophic bone loss and instability. The patient desires a single-stage procedure. What is the most appropriate surgical strategy?
View Answer & Explanation
Correct Answer: B
Rationale: The text presents two advanced solutions for extreme extra-articular deformity. For a patient desiring a single surgery, the concurrent (simultaneous) osteotomy and TKR is the ideal choice. The tibial stem of the TKR can be used as the intramedullary fixation device for the osteotomy, correcting both problems at once.
Question 24
A surgeon performing a complex TKR on a post-HTO knee with severe ligamentous imbalance notes a large flexion gap and instability. Instead of immediately using a highly constrained implant, the surgeon performs an advancement of the medial collateral ligament (MCL) origin. What is the primary advantage of this soft-tissue balancing approach?
View Answer & Explanation
Correct Answer: C
Rationale: The text warns that highly constrained implants transfer massive shear and bending stresses to the bone-implant interface, risking early aseptic loosening. By performing advanced ligamentous procedures like an MCL advancement to restore stability, the surgeon can use a less constrained implant, which reduces these harmful stresses.
Question 25
A 48-year-old female with a history of developmental dysplasia of the hip (DDH) requires a total hip arthroplasty (THA). Preoperative imaging reveals 70 degrees of femoral anteversion. What is the most significant biomechanical consequence of this deformity on the abductor muscles?
View Answer & Explanation
Correct Answer: C
Rationale: The text explains that excessive anteversion rotates the greater trochanter from a lateral to a posterior position. This drastically shortens the abductor lever arm, placing the gluteus medius and minimus at a severe mechanical disadvantage and leading to a Trendelenburg gait.
Question 26
A surgeon is performing a THA on a patient with severe DDH and excessive femoral anteversion. An attempt is made to insert a standard, monoblock, anatomically shaped femoral stem. Which of the following is the most likely immediate complication?
View Answer & Explanation
Correct Answer: D
Rationale: The text describes the dysplastic femur as having a narrow medial-lateral (M-L) dimension, creating a "champagne flute" canal. Forcing a standard stem with a wider M-L profile into this canal will either cause a catastrophic intraoperative fracture or force the stem to follow the bone's native 80-degree anteversion, leading to instability.
Question 27
A 7-year-old boy with spastic diplegic cerebral palsy is evaluated for a gait abnormality. On the examination table with his knee flexed, his ankle can be passively dorsiflexed to 15 degrees. However, during the stance phase of gait, his foot is in a rigid equinus position. Which of the following terms best describes this clinical finding?
View Answer & Explanation
Correct Answer: C
Rationale: The deformity is present during dynamic activity (gait) but is correctable with passive examination, which is the definition of a dynamic deformity. A static deformity or fixed contracture (B) would not be passively correctable on examination.
Question 28
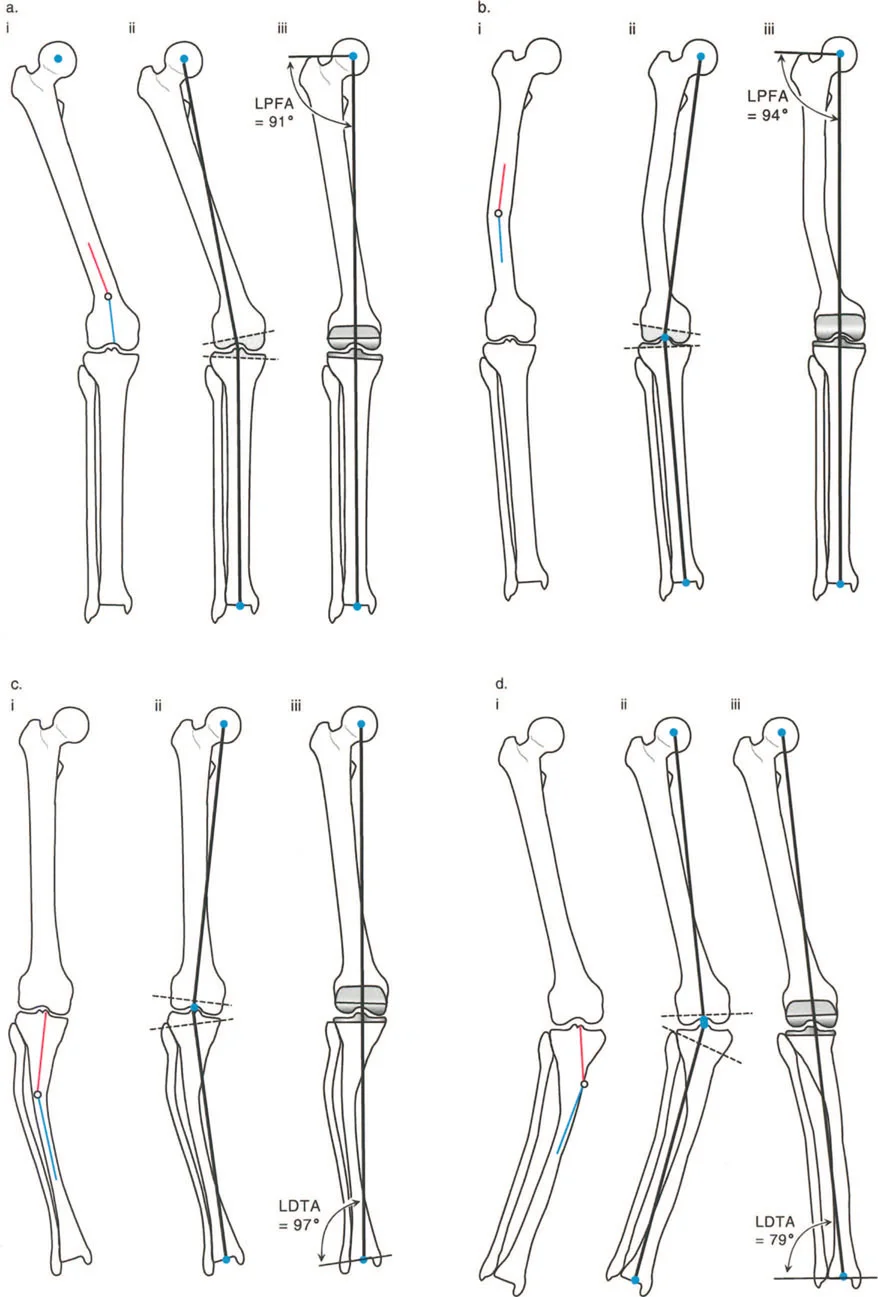
A 14-year-old female presents with a waddling gait and fatigue after walking short distances. Physical examination reveals a positive Trendelenburg sign. Radiographs show a Lateral Proximal Femoral Angle (LPFA) of 75 degrees. Her gluteus medius muscle is confirmed to have 5/5 strength on manual testing. The patient's gait abnormality is primarily due to a deformity in which of the following?
View Answer & Explanation
Correct Answer: C
Rationale: The coxa vara deformity (decreased LPFA) shortens the horizontal distance from the greater trochanter to the femoral head center, effectively shortening the abductor muscle's lever arm. Despite normal muscle strength, the mechanical advantage is lost, leading to functional weakness and a Trendelenburg gait.
Question 29
A resident is preparing a presentation on gait abnormalities in children with cerebral palsy. She describes a condition where internal and external lever arms are distorted due to bone malalignment, leading to inefficient movement. According to the provided text, which term, originally coined by Gage, accurately describes this phenomenon?
View Answer & Explanation
Correct Answer: B
Rationale: The term "lever arm dysfunction" was coined by Gage in 1991 to describe the pathological alteration in leverage relationships due to bone malalignment or contractures, particularly in ambulatory children with cerebral palsy. Mechanical axis deviation (E) is a measurement, not the overarching term for the functional problem.
Question 30
A 45-year-old man with a history of a traumatic brain injury has a long-standing dynamic varus deformity of his foot and ankle due to tibialis posterior spasticity. Over several years, he develops a fixed hindfoot varus that is no longer passively correctable. This progression from a dynamic to a static deformity is best explained by which of the following principles?
View Answer & Explanation
Correct Answer: D
Rationale: Untreated dynamic deformities become static through two primary mechanisms: the development of secondary structural deformities in the bone (Wolff's Law) and the establishment of fixed soft-tissue joint contractures. The Hueter-Volkmann principle (A) relates to growth plate compression and is more relevant in skeletally immature patients.
Question 31
A surgeon is planning a proximal femoral osteotomy for a patient with coxa vara. The patient's gluteus medius has limited potential for strength improvement. To maximize the abductor moment acting on the hip joint, the surgical plan should focus on which of the following biomechanical goals?
View Answer & Explanation
Correct Answer: C
Rationale: A moment is the product of force and the lever arm length. Since the muscle force cannot be significantly increased, the most effective way to increase the moment is to surgically lengthen the lever arm. A valgus-producing osteotomy lateralizes the greater trochanter, achieving this goal.
Question 32
A research fellow is analyzing data from a gait laboratory. The analysis focuses on the ground reaction forces, joint reaction forces, and muscle forces that produce the observed walking pattern. This type of analysis is best described as a study of which of the following?
View Answer & Explanation
Correct Answer: B
Rationale: Kinetics is the study of the forces (e.g., ground reaction forces, muscle forces) that produce or resist motion. Kinematics (A) is the study of motion itself (angles, velocities) without regard to the forces causing it.
Question 33
During a gait analysis study, an orthopedic surgeon uses reflective markers placed on a patient's lower limb to measure joint angles, velocities, and accelerations during walking. This measurement of motion, without consideration for the forces involved, is defined as which of the following?
View Answer & Explanation
Correct Answer: D
Rationale: Kinematics is the study of motion alone, including parameters like angles, velocities, and accelerations, without considering the forces that cause the motion. Kinetics (A) is the study of those forces.
Question 34
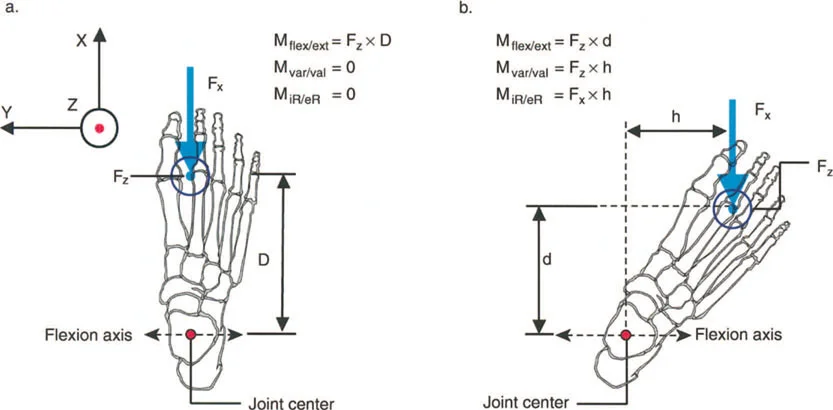
A bioengineer is calculating the varus moment across the knee joint caused by the ground reaction force during single-leg stance. The force is 1500 N and the perpendicular distance from the force vector to the center of the knee is 0.05 meters. What is the magnitude of the moment?
View Answer & Explanation
Correct Answer: B
Rationale: A moment is calculated as the product of force times the perpendicular length of the lever arm. Therefore, Moment = 1500 N * 0.05 m = 75 Nm (Newton-meters). The other options use incorrect units or calculations.
Question 35
A patient has a severe knee flexion contracture of 40 degrees. When the quadriceps muscle contracts to extend the knee, the patellar tendon pulls on the tibial tubercle at an oblique angle rather than perpendicularly. How does this flexion contracture affect the extension moment generated by the quadriceps?
View Answer & Explanation
Correct Answer: C
Rationale: The magnitude of a moment is maximized when the force is applied perpendicularly to the lever. In a flexion contracture, the angle of application is no longer perpendicular, which decreases the effective length of the patellar tendon lever arm and thus reduces the extension moment for a given quadriceps force.
Question 36
An orthopedic surgeon is explaining the biomechanics of walking to a medical student. She states that the forward progression of the body's center of mass is governed by the net external forces acting on the body. This principle is a direct application of which of the following physical laws?
View Answer & Explanation
Correct Answer: A
Rationale: Newton's second law (F = ma) governs translational motion. It states that the net force on a body is equal to the body's mass times the acceleration of its center of mass. This explains the forward progression (translation) of the body during gait. The moment equation (C) governs rotational motion.
Question 37
A 55-year-old woman is evaluated for a Trendelenburg gait. The surgeon explains that during single-leg stance, the hip abductor muscles must counteract the force of body weight to keep the pelvis level. The biomechanical arrangement of the femoral head (fulcrum), body weight (load), and abductor force (effort) is an example of which class of lever?
View Answer & Explanation
Correct Answer: A
Rationale: This is a classic example of a first-class lever. The fulcrum (femoral head) is positioned between the effort (abductor force on the greater trochanter) and the load (body weight acting through the center of gravity). A second-class lever (B) has the load between the fulcrum and effort.
Question 38
A physical therapist is analyzing the "toe-off" phase of gait. The triceps surae pulls on the calcaneus to lift the body, with the foot pivoting on the metatarsophalangeal (MTP) joints. This arrangement, where the MTP joints act as the fulcrum, body weight is the load, and the triceps surae provides the effort, is an example of which class of lever?
View Answer & Explanation
Correct Answer: B
Rationale: This is a second-class lever, where the load (body weight through the ankle) is located between the fulcrum (MTP joints) and the effort (Achilles tendon insertion). This class of lever always provides a mechanical advantage greater than one.
Question 39
A 25-year-old weightlifter performs a biceps curl. The elbow joint serves as the fulcrum, the biceps muscle inserts on the radial tuberosity to provide the effort, and the weight is held in the hand (load). This configuration is the most common type of lever in the human body and is classified as which of the following?
View Answer & Explanation
Correct Answer: C
Rationale: This is a third-class lever, where the effort (biceps insertion) is applied between the fulcrum (elbow joint) and the load (weight in hand). This is the most common lever type in the body, sacrificing mechanical advantage for speed and range of motion.
Question 40
An orthopedic resident is studying biomechanics. She is looking for an example of a lever system in the human body that is designed for power and force production rather than speed, and thus always has a mechanical advantage greater than one. Which of the following clinical examples fits this description?
View Answer & Explanation
Correct Answer: B
Rationale: The foot during toe-off is a second-class lever. The defining characteristic of a second-class lever is that the mechanical advantage is always greater than one, allowing a smaller muscular effort to move a larger load. The elbow (C) and knee (D) are primarily third-class levers with a mechanical advantage less than one.
Question 41
A surgeon is explaining to a patient why a small tear in the biceps tendon can lead to a significant loss of flexion strength. He notes that the biceps acts as a third-class lever. What is the primary biomechanical trade-off inherent to a third-class lever system?
View Answer & Explanation
Correct Answer: C
Rationale: Third-class levers, the most common in the body, always have a mechanical advantage less than one. This means they require large muscular effort to move smaller loads. The benefit of this "disadvantageous" arrangement is that a small, powerful muscle contraction produces a rapid, large-arc movement at the end of the lever (e.g., the hand).
Question 42
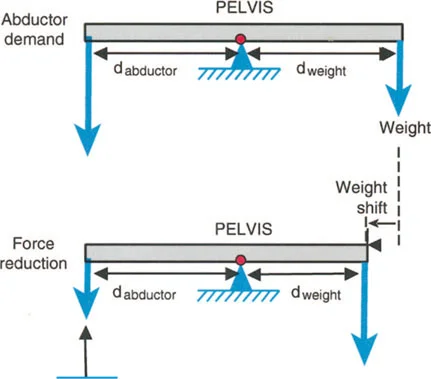
In the first-class lever system of the hip during single-leg stance, the lever arm of the body weight (load) is 10 cm, and the lever arm of the abductor muscles (effort) is 4 cm. What is the mechanical advantage (MA) of the abductor muscles?
View Answer & Explanation
Correct Answer: C
Rationale: Mechanical Advantage (MA) is defined as the ratio of the effort lever arm to the load lever arm (MA = d_effort / d_load). In this case, MA = 4 cm / 10 cm = 0.4. This indicates a mechanical disadvantage, requiring the abductors to generate a force 2.5 times the body weight to maintain a level pelvis.
Question 43
A 25-year-old male with a history of a malunited femoral fracture is being evaluated for a corrective osteotomy. The surgeon orders a 51-inch standing long leg radiograph. According to the Paley method, what is the most critical parameter for standardizing the rotational alignment of the lower limb during image acquisition?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that the "Patella Forward" position is the most critical parameter. Rotation at the hip or ankle can create a pseudo-deformity if the patella is not used as the primary landmark for rotational alignment. Foot position (A) is a common distractor but is incorrect, as patients with torsional deformities may have in-toeing or out-toeing despite a correctly positioned patella.
Question 44
A 45-year-old female presents with right knee pain and a suspected 3 cm leg length discrepancy (LLD). When obtaining a standing long leg radiograph for deformity analysis, what is the correct procedure to compensate for the LLD?
View Answer & Explanation
Correct Answer: B
Rationale: To obtain an accurate Mechanical Axis Deviation (MAD), the pelvis must be leveled. This is achieved by placing calibrated blocks under the shorter limb. Failing to do so causes compensatory hip abduction or adduction, which artificially alters the mechanical axis. Flexing the knee of the longer limb (C) would alter both coronal and sagittal plane alignment.
Question 45
An orthopedic resident is supervising the acquisition of a long leg radiograph for a patient with genu varum. To minimize magnification error and parallax distortion, what is the recommended minimum distance for the x-ray beam source?
View Answer & Explanation
Correct Answer: C
Rationale: The text specifies that the x-ray beam should be centered at the knee from a distance of at least 10 feet (3 meters) to minimize magnification and parallax errors. Shorter distances, like 6 feet (B), are common for standard radiographs but are insufficient for the precision required in deformity planning.
Question 46
A 16-year-old male with Blount's disease is undergoing preoperative planning. The surgeon intends to use digital templating software to measure angles and plan the osteotomy. What must be included in the radiographic field to allow for accurate calibration of the software?
View Answer & Explanation
Correct Answer: C
Rationale: Digital templating software requires a reference object of a known size to calibrate measurements. A radiopaque magnification marker (e.g., a 25mm sphere) placed at the level of the bone (typically the knee) serves this purpose. A ruler on the cassette (D) would be subject to the same magnification error as the bone and would be inaccurate.
Question 47
A surgeon is evaluating a 14-year-old female with a chief complaint of "knock-knees." On physical exam, she has significant femoral anteversion and compensatory external tibial torsion, causing her feet to point straight forward. When positioning her for a long leg AP radiograph, the technician aligns her feet to be perfectly parallel. This action will most likely lead to what measurement error?
View Answer & Explanation
Correct Answer: C
Rationale: The "Patella Forward" rule is paramount. By positioning based on the feet instead of the patella, the femur will be internally rotated on the film. This rotation prevents the posterior femoral condyles from being parallel to the film cassette, which artificially changes the appearance of the distal femoral joint line and leads to an inaccurate mLDFA measurement. This violates the foundational principle of standardized imaging.
Question 48
A 58-year-old male undergoes a successful high tibial osteotomy for varus malalignment. Postoperatively, he complains of lateral foot pain and difficulty walking on uneven surfaces. The surgeon suspects a rigid, compensatory hindfoot deformity that was not addressed. Which specialized radiographic view is mandatory for assessing the mechanical axis of the hindfoot relative to the tibia?
View Answer & Explanation
Correct Answer: E
Rationale: The Saltzman view, a refinement of the Cobey view, is the gold standard for assessing the coronal plane alignment of the hindfoot relative to the distal tibia. It is essential for determining if a hindfoot deformity is primary or compensatory. The other views are used for assessing talar fractures (B), subtalar arthritis (A), or calcaneal fractures (C).
Question 49
A 19-year-old patient presents with knee pain and instability following a traumatic injury. The surgeon suspects a recurvatum deformity of the proximal tibia. Which radiographic view is essential for quantifying this sagittal plane malalignment?
View Answer & Explanation
Correct Answer: B
Rationale: Sagittal plane deformities like procurvatum (anterior bowing) and recurvatum (posterior bowing) are assessed on a standing lateral radiograph that includes the entire femur and tibia. The AP view (A) assesses the coronal plane (varus/valgus).
Question 50
A 33-year-old patient with a varus ankle deformity is being evaluated with a Saltzman hindfoot alignment view. To properly acquire this image, the patient is positioned standing and weight-bearing. At what angle should the x-ray beam be directed toward the floor, aimed at the ankle joint?
View Answer & Explanation
Correct Answer: C
Rationale: The text specifies the technique for the Saltzman view: the x-ray beam is angled 20 degrees downward toward the floor. This specific angle is crucial for projecting the tibial and calcaneal axes correctly for measurement. Other angles would distort the relationship between the tibia and calcaneus.
Question 51
An orthopedic surgeon is templating a distal femoral osteotomy. According to Paley's principles, how is the mechanical axis of the femur correctly defined?
View Answer & Explanation
Correct Answer: C
Rationale: The mechanical axis of the femur represents the line of weight-bearing force and is defined as a straight line from the center of the femoral head to the center of the knee. The line through the diaphysis (A) defines the anatomic axis, which is a critical distinction.
Question 52
During a deformity analysis conference, a senior surgeon asks a resident to identify the Mikulicz line on a long leg radiograph. This line represents which of the following?
View Answer & Explanation
Correct Answer: C
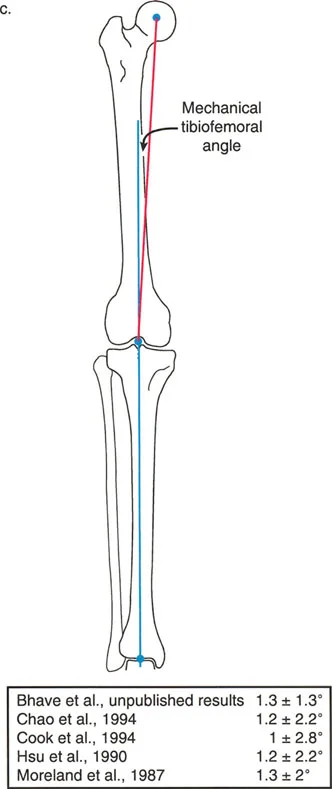
Rationale: The Mikulicz line is the synonym for the mechanical axis of the entire lower limb. It is drawn from the center of the femoral head to the center of the ankle joint and is used to calculate the Mechanical Axis Deviation (MAD) at the knee.
Question 53
A medical student is learning to differentiate the axes of the lower limb. When analyzing the tibia on an AP radiograph, what is the typical relationship between its anatomic and mechanical axes?
View Answer & Explanation
Correct Answer: C
Rationale: Unlike the femur, the tibia is a relatively straight bone. Therefore, its mid-diaphyseal line (anatomic axis) and the line from the knee center to the ankle center (mechanical axis) are essentially the same. The 7-degree divergence (A) is characteristic of the femur.
Question 54
A surgeon is planning a total knee arthroplasty using an intramedullary femoral guide. Understanding the difference between the anatomic and mechanical axes of the femur is critical. In a normal limb, the anatomic axis of the femur diverges from the mechanical axis by an average of how many degrees?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that due to the offset of the femoral neck and the natural bow of the femur, the anatomic axis diverges from the mechanical axis by an average of 7 degrees (in valgus). This is a fundamental value in lower limb alignment and knee arthroplasty.
Question 55
During a total knee arthroplasty, the surgeon inserts a long rod into the femoral canal to guide the distal femoral cutting block. This intramedullary guide naturally follows which axis of the femur?
View Answer & Explanation
Correct Answer: B
Rationale: An intramedullary rod passes down the medullary canal, which by definition represents the anatomic axis of the bone. This is why surgeons must set a 5- to 7-degree valgus cut on the distal femoral cutting block to make the final bone cut perpendicular to the mechanical axis.
Question 56
A 62-year-old male with knee osteoarthritis has a varus deformity. The surgeon performs a malalignment test by drawing the Mikulicz line from the center of the femoral head to the center of the ankle. The line passes 20 mm medial to the center of the knee joint. What does this finding indicate?
View Answer & Explanation
Correct Answer: B
Rationale: The Mechanical Axis Deviation (MAD) is the distance from the center of the knee to the Mikulicz line. When this line passes medial to the knee center, it indicates a varus deformity, which overloads the medial compartment. A line passing lateral would indicate a valgus deformity (A).
Question 57
A 17-year-old female is evaluated for genu valgum. Her long leg radiograph shows the mechanical axis of the lower limb passing 25 mm lateral to the center of the knee. This finding leads to overload of the lateral compartment and stretching of which structure?
View Answer & Explanation
Correct Answer: D
Rationale: A mechanical axis passing lateral to the knee center defines a valgus deformity. This alignment places tensile forces on the medial side of the knee, leading to stretching of the medial collateral ligament (MCL). In varus deformity, the LCL (C) is stretched.
Question 58
In a biomechanically normal, healthy lower limb, where does the mechanical axis (Mikulicz line) typically pass in relation to the center of the knee joint?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that a normal limb has a slight physiologic varus, with the mechanical axis passing 1 to 8 mm medial to the exact center of the knee. This explains why the medial compartment naturally bears more weight (approximately 60%) during gait. A line passing exactly through the center (B) is acceptable but less common than a slightly medial axis.
Question 59
A surgeon is teaching a resident how to define the joint orientation lines for deformity analysis. How is the distal femoral joint line accurately drawn on an AP radiograph?
View Answer & Explanation
Correct Answer: C
Rationale: Precise definition of the joint lines is critical for angle measurement. The distal femoral joint line is defined as the line tangential to the most distal aspects of the two femoral condyles. The line parallel to the tibial plateaus (B) defines the proximal tibial joint line.
Question 60
When measuring the Medial Proximal Tibial Angle (MPTA), the proximal tibial joint line should be drawn tangential to the subchondral bone of the medial and lateral tibial plateaus. Which structure should be specifically ignored to avoid measurement error from osteophytes?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly warns to ignore the intercondylar eminence (tibial spines) when drawing the proximal tibial joint line. This area is frequently distorted by osteophytes in arthritic knees, which can artificially alter the slope of the line and lead to an inaccurate MPTA measurement.
Question 61
A 28-year-old patient is being evaluated for a distal femoral malunion. The surgeon measures the angle between the mechanical axis of the femur and the distal femoral joint line. What is the normal value for the Mechanical Lateral Distal Femoral Angle (mLDFA)?
View Answer & Explanation
Correct Answer: C
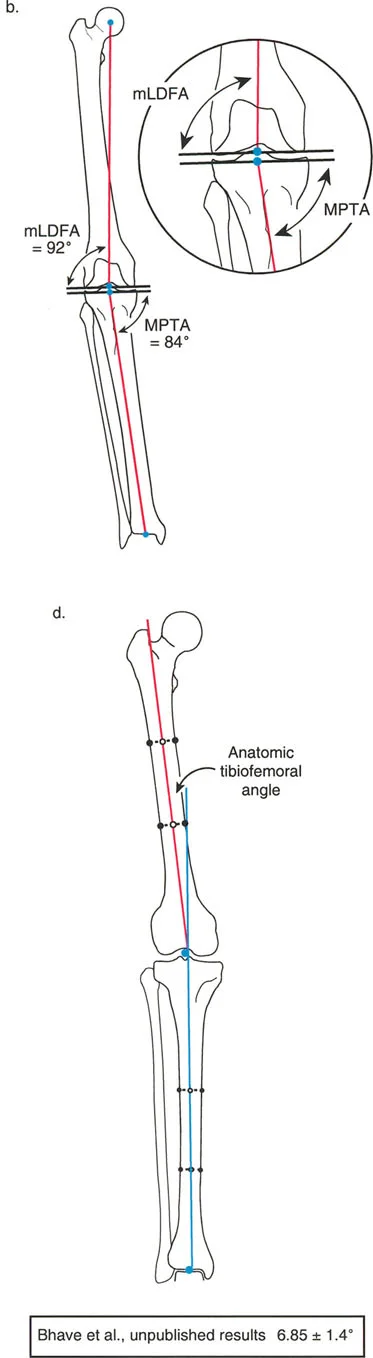
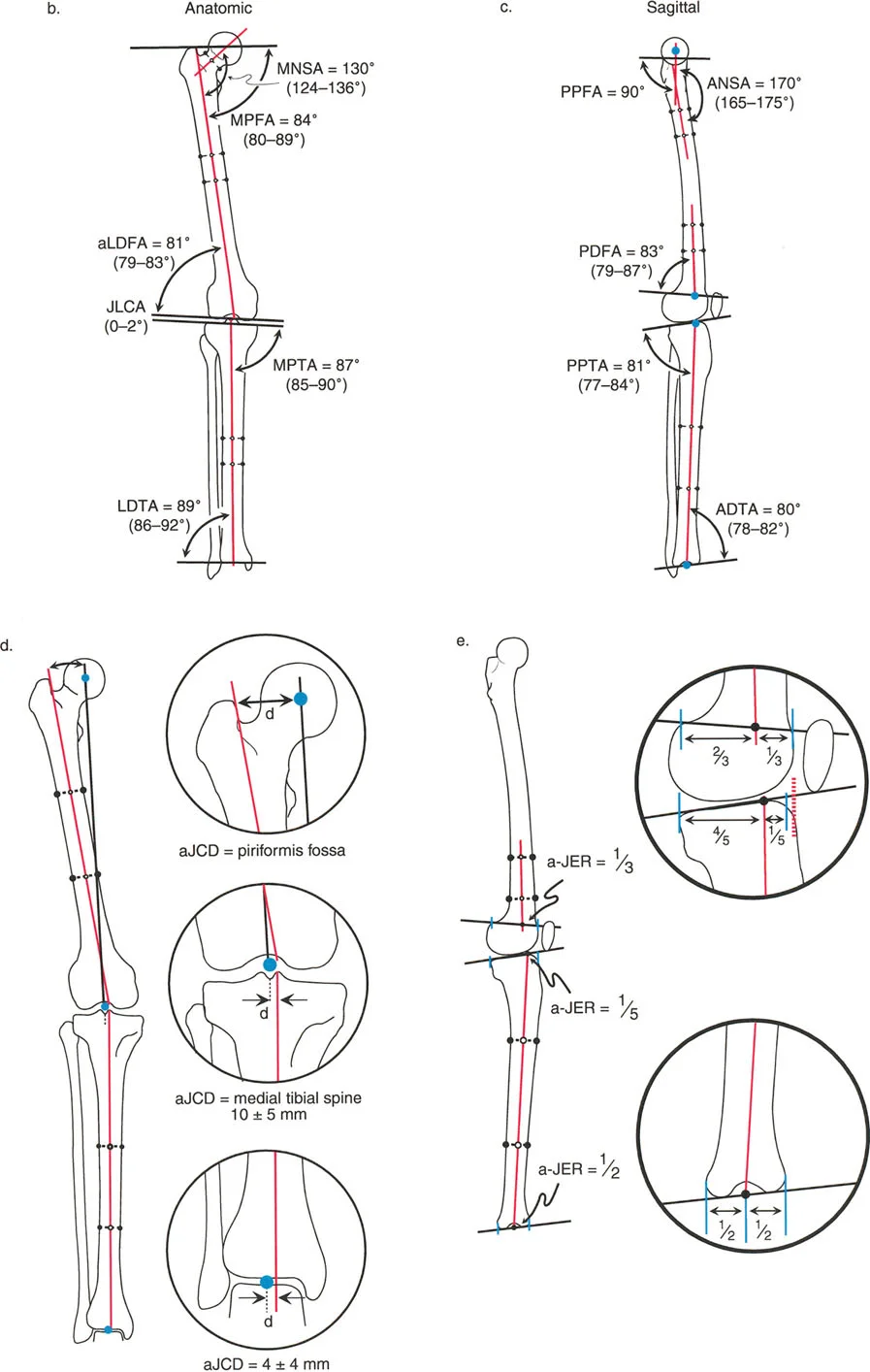
Rationale: The normal mLDFA is 88° (range 85°-90°). This value being less than 90° indicates that the distal femur has a slight physiologic varus relative to its mechanical axis. 81° (A) is the normal aLDFA, and 87° (B) is the normal MPTA.
Question 62
A 40-year-old patient with a proximal tibial malunion presents with knee pain. On a long leg radiograph, the surgeon measures the angle between the mechanical axis of the tibia and the proximal tibial joint line. What is the normal value for the Medial Proximal Tibial Angle (MPTA)?
View Answer & Explanation
Correct Answer: B
Rationale: The normal MPTA is 87° (range 85°-90°). This value being less than 90° indicates that the proximal tibia also has a slight physiologic varus. 89° (C) is the normal mLDTA, and 81° (A) is the normal aLDFA.
Question 63
A resident is asked to explain the difference between the mLDFA and the aLDFA. The aLDFA (Anatomic Lateral Distal Femoral Angle) is normally 81°. This value is approximately 7 degrees less than the normal mLDFA. What does this 7-degree difference represent?
View Answer & Explanation
Correct Answer: D
Rationale: The difference between the mLDFA (88°) and the aLDFA (81°) is a direct reflection of the ~7-degree angle between the femur's mechanical and anatomic axes. Understanding this relationship is key to converting between measurements based on these two different axes.
Question 64
A 45-year-old man presents with medial-sided knee pain. A full-length standing radiograph is obtained to assess his lower limb alignment. When defining the mechanical axis of his entire lower extremity, a line should be drawn connecting the center of the femoral head to which of the following points?
View Answer & Explanation
Correct Answer: B
Rationale: The mechanical axis of the entire lower extremity is a straight line connecting the center of the femoral head to the center of the ankle joint (tibial plafond). This line is fundamental for assessing overall limb alignment and calculating Mechanical Axis Deviation (MAD). The center of the femoral notch is the distal point for the femur's mechanical axis, not the entire limb's.
Question 65
A surgeon is planning a distal femoral osteotomy for a 22-year-old patient with a valgus deformity. To accurately assess the deformity, the surgeon must distinguish between the femur's mechanical and anatomic axes. Which of the following best describes the mechanical axis of the femur?
View Answer & Explanation
Correct Answer: D
Rationale: The mechanical axis of the femur is defined as a straight line from the center of the femoral head to the center of the knee joint, which is specified as the center of the femoral notch. The line down the center of the diaphysis is the anatomic axis.
Question 66
A 58-year-old woman with progressive bow-legged deformity undergoes a standing AP radiograph of her lower extremities. The analysis reveals that the mechanical axis of the limb passes 25 mm medial to the center of the knee joint. What is the name for this measurement?
View Answer & Explanation
Correct Answer: B
Rationale: Mechanical Axis Deviation (MAD) is the perpendicular distance from the mechanical axis of the entire lower limb to the center of the knee joint. A medial deviation, as described, indicates a varus alignment. MPTA and mLDFA are joint orientation angles, not measures of overall alignment.
Question 67
During a preoperative conference, a resident is asked to describe the key difference between the anatomic and mechanical axes of the tibia in the frontal plane. Which statement is most accurate?
View Answer & Explanation
Correct Answer: C
Rationale: In the tibia, the anatomic axis (mid-diaphyseal line) and the mechanical axis (center of plateau to center of plafond) are nearly parallel in the frontal plane. For practical surgical planning, they are often treated as collinear. The 7-degree divergence is characteristic of the femur, not the tibia.
Question 68
A 62-year-old male is evaluated for lateral compartment knee osteoarthritis. His standing radiograph shows the mechanical axis of the lower limb passing 15 mm lateral to the center of the knee. This finding is most consistent with which of the following conditions?
View Answer & Explanation
Correct Answer: B
Rationale: A mechanical axis passing lateral to the center of the knee indicates a valgus alignment (genu valgum), which overloads the lateral compartment of the knee. A mechanical axis passing medial to the knee center indicates varus alignment (genu varum).
Question 69
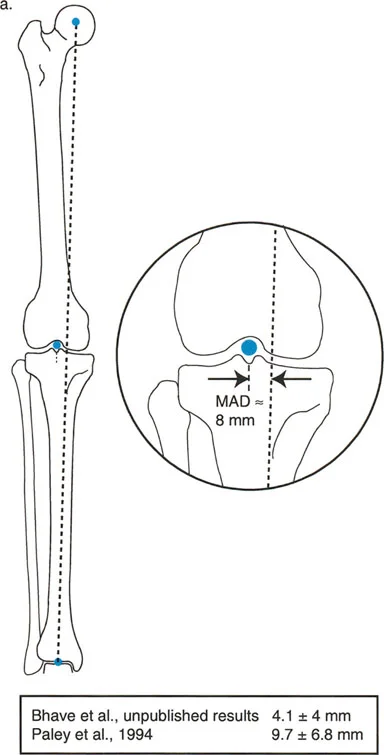
According to Paley's principles, what is the normal range for Mechanical Axis Deviation (MAD) in a healthy adult lower limb?
View Answer & Explanation
Correct Answer: C
Rationale: In a normally aligned limb, the mechanical axis passes slightly medial to the exact center of the knee. The accepted normal value for MAD is approximately 8 mm medial, with a range of ± 7 mm (i.e., 1-15 mm medial).
Question 70
A surgeon is evaluating a patient with a varus malalignment. The MAD is significantly medial. To determine the source of the deformity, the surgeon must now measure the joint orientation angles. What fundamental question does joint orientation answer that alignment (MAD) does not?
View Answer & Explanation
Correct Answer: D
Rationale: Alignment, measured by MAD, tells us *if* the limb is crooked (varus or valgus). Joint orientation, measured by angles like mLDFA and MPTA, tells us *where* (femur, tibia, or both) and *why* the deformity exists. This distinction is critical for correct surgical planning.
Question 71
A 14-year-old with a history of a distal femoral physeal injury presents with a knee deformity. When evaluating the sagittal plane deformity on a lateral radiograph, the surgeon finds it difficult to define the distal femoral joint line due to condylar curvature. Which landmark serves as the best surrogate for the joint orientation line of the distal femur in the sagittal plane?
View Answer & Explanation
Correct Answer: C
Rationale: Blumensaat's line, representing the roof of the intercondylar notch, is a reliable and easily identifiable surrogate for the distal femoral joint orientation line in the sagittal plane. It is particularly useful for measuring the Posterior Distal Femoral Angle (PDFA) to assess for procurvatum or recurvatum.
Question 72
A resident is learning to measure joint orientation angles of the proximal femur. Due to the spherical shape of the femoral head, a direct tangent line cannot be drawn. Which of the following is an accepted method for establishing the hip joint orientation line in the frontal plane?
View Answer & Explanation
Correct Answer: C
Rationale: Because the femoral head is round, surrogate landmarks are used. One standard method is to draw a line from the center of the femoral head to the proximal tip of the greater trochanter. This line represents the hip joint orientation for measuring angles like the mLPFA.
Question 73
Using Paley's standardized nomenclature, a surgeon measures the angle between the mechanical axis of the femur and the distal femoral joint line on the lateral side. What is the correct name for this angle?
View Answer & Explanation
Correct Answer: B
Rationale: Following the formula [Axis] + [Position] + [Location] + [Bone] + Angle: (m)echanical + (L)ateral + (D)istal + (F)emoral + (A)ngle = mLDFA. This is one of the most critical angles in lower limb deformity analysis.
Question 74
When measuring joint orientation angles, the intersection of an axis and a joint line creates two supplementary angles (e.g., a medial and a lateral angle). According to Paley's "less than 90 degrees" rule, which angle is chosen as the standard reference?
View Answer & Explanation
Correct Answer: A
Rationale: To standardize communication, the system designates the angle that is normally acute (less than 90°) as the named angle. For example, the normal mLDFA is 88°, while its supplementary angle (mMDFA) is 92°. Therefore, mLDFA is the standard reference.
Question 75
A surgeon is discussing a case of tibial varus and refers to the "MPTA." A medical student asks why the "m" for mechanical or "a" for anatomic prefix is not used. What is the correct explanation?
View Answer & Explanation
Correct Answer: C
Rationale: Prefixes are omitted when the context is clear or the values are identical. For the tibia in the frontal plane, the mechanical and anatomic axes are parallel, meaning the mMPTA and aMPTA are the same. Therefore, the prefix is unnecessary, and the angle is simply called the MPTA.
Question 76
For which of the following angles is it absolutely mandatory to specify the prefix "m" (mechanical) or "a" (anatomic) to avoid confusion?
View Answer & Explanation
Correct Answer: C
Rationale: The distal femur is the only location where the prefix is mandatory. The femoral anatomic and mechanical axes diverge significantly (by about 7°), resulting in a large difference between the mLDFA (normal 88°) and the aLDFA (normal 81°). Both are less than 90°, so the prefix is required for clarity.
Question 77
A 30-year-old patient with developmental hip dysplasia is being evaluated. The surgeon measures the angle between the anatomic axis of the femur and the femoral neck, finding it to be 115°. What is the common name for this angle, and what condition does this value suggest?
View Answer & Explanation
Correct Answer: B
Rationale: The Medial Neck Shaft Angle (MNSA) is the classic "neck-shaft angle." Its normal value is approximately 130° (range 124-136°). A value of 115° is significantly decreased, which defines coxa vara.
Question 78
During preoperative planning for a high tibial osteotomy, a surgeon measures the Medial Proximal Tibial Angle (MPTA) to be 80°. What is the normal value for the MPTA, and what deformity does an 80° angle represent?
View Answer & Explanation
Correct Answer: D
Rationale: The normal MPTA is 87° (range 85-90°). An angle less than 85° indicates that the proximal tibia is in varus. An MPTA of 80° is a clear indicator of tibial varus, making it a common target for a high tibial osteotomy.
Question 79
A 25-year-old patient has a valgus knee deformity. Radiographic analysis reveals a mechanical Lateral Distal Femoral Angle (mLDFA) of 82°. Based on this finding, what is the source of the patient's deformity?
View Answer & Explanation
Correct Answer: C
Rationale: The normal mLDFA is 88° (range 85-90°). An mLDFA less than 85° indicates a valgus deformity originating from the distal femur. An mLDFA greater than 90° would indicate femoral varus.
Question 80
A 60-year-old patient presents with a severe varus deformity of the knee. The surgeon measures the mLDFA as 88° and the MPTA as 87°. The mechanical axis is deviated 30 mm medially. What is the most likely source of this patient's deformity?
View Answer & Explanation
Correct Answer: D
Rationale: The mLDFA (88°) and MPTA (87°) are both within the normal range. When the joint orientation angles are normal but the overall alignment (MAD) is pathologic, the deformity must be intra-articular. This is indicated by an abnormal Joint Line Convergence Angle (JLCA), often due to severe medial cartilage loss or lateral collateral ligament laxity.
Question 81
What is the normal value for the Joint Line Convergence Angle (JLCA) of the knee, and what does a widened lateral JLCA in a varus knee suggest?
View Answer & Explanation
Correct Answer: B
Rationale: The normal knee JLCA is 0-2°, meaning the distal femoral and proximal tibial joint lines are nearly parallel. In a varus knee, a widened JLCA indicates that the lateral side of the joint is opening up, which is caused by lateral collateral ligament (LCL) laxity or severe medial-sided cartilage loss. An osteotomy alone cannot correct a ligamentous deformity.
Question 82
A surgeon is planning a high tibial osteotomy (HTO) and must consider the sagittal plane alignment to avoid altering knee kinematics. What is the name of the angle that represents the normal posterior slope of the tibial plateau, and what is its average value?
View Answer & Explanation
Correct Answer: C
Rationale: The Posterior Proximal Tibial Angle (PPTA) measures the posterior slope of the tibial plateau relative to the tibial anatomic axis. Its normal value is 81° (range 77-84°). Maintaining this angle during an HTO is critical to prevent iatrogenic stress on the cruciate ligaments.
Question 83
A 19-year-old patient sustained a malunion of a distal tibia fracture. On a lateral radiograph, the Anterior Distal Tibial Angle (ADTA) is measured to be 70°. What is the normal value for the ADTA, and what clinical problem might this deformity cause?
View Answer & Explanation
Correct Answer: D
Rationale: The normal ADTA is 80° (range 78-82°). A decreased ADTA (e.g., 70°) means the tibial plafond is tilted anteriorly, which would limit the space for the talus to move posteriorly during dorsiflexion, thus impairing ankle dorsiflexion.
Question 84
When planning for an antegrade intramedullary nail of the femur, the surgeon uses the piriformis fossa as the starting point. This anatomic landmark corresponds to the intersection of which of the following?
View Answer & Explanation
Correct Answer: B
Rationale: The anatomic axis of the femur intersects the proximal femur precisely at the piriformis fossa. This is the anatomical basis for using the piriformis fossa as the starting point for a straight antegrade femoral nail, as the nail follows the anatomic axis.
Question 85
A surgeon is performing a deformity analysis and needs to locate the intersection of the femoral anatomic axis with the knee joint line in the frontal plane. Where does this intersection typically occur?
View Answer & Explanation
Correct Answer: D
Rationale: Due to the valgus orientation of the femur, its anatomic axis (mid-diaphyseal line) is not collinear with its mechanical axis. The anatomic axis intersects the knee joint line approximately 10 ± 5 mm lateral to the true center of the knee, near the medial aspect of the lateral femoral condyle.
Question 86
In the sagittal plane, the anatomic axis of the tibia intersects the proximal tibial joint line (plateau) at a specific ratio from the anterior edge. What is this anatomic axis to joint edge ratio (aJER) for the proximal tibia?
View Answer & Explanation
Correct Answer: D
Rationale: The aJER for the proximal tibia is 1/5. This means the straight anatomic axis of the diaphysis intersects the tibial plateau very anteriorly, reflecting the significant posterior slope of the plateau relative to the shaft.
Question 87
A 62-year-old male presents with severe right knee pain and a visible varus deformity. A full-length standing radiograph is obtained. The surgeon draws a line from the center of the femoral head to the center of the ankle plafond. The perpendicular distance from this line to the center of the knee joint is measured. What does this measurement represent?
View Answer & Explanation
Correct Answer: B
Rationale: The Mechanical Axis Deviation (MAD) is defined as the perpendicular distance from the center of the knee joint to the mechanical axis line (femoral head center to ankle center). It is the primary metric for assessing global lower extremity alignment. The JLCA measures intra-articular gapping, not overall limb alignment.
Question 88
A 58-year-old female with a history of a healed distal femur fracture presents with debilitating knee pain and a valgus deformity. Preoperative planning on a full-length radiograph reveals a mechanical Lateral Distal Femoral Angle (mLDFA) of 78 degrees. What is the clinical significance of this finding when planning a total knee arthroplasty (TKA)?
View Answer & Explanation
Correct Answer: C
Rationale: The normal mLDFA is 85-90 degrees. A value of 78 degrees indicates a significant valgus deformity originating from the distal femur. This is a clear indicator of an extra-articular femoral-based deformity that cannot be corrected with standard intra-articular TKA resections alone.
Question 89
A 67-year-old male presents with medial-sided knee pain and a varus thrust. Radiographic analysis shows a Medial Proximal Tibial Angle (MPTA) of 80 degrees. The mLDFA is 88 degrees. Based on these findings, where is the primary source of his varus malalignment?
View Answer & Explanation
Correct Answer: B
Rationale: The normal MPTA is 85-90 degrees. An MPTA of 80 degrees indicates a varus deformity originating from the proximal tibia. The mLDFA of 88 degrees is within the normal range, ruling out the distal femur as the primary source of the angular deformity.
Question 90
A 70-year-old female with end-stage osteoarthritis undergoes preoperative planning for a TKA. On her weight-bearing AP radiograph, the angle formed by the convergence of lines drawn along the distal femoral condyles and the tibial plateau measures 8 degrees. What is this angle called, and what does it primarily indicate?
View Answer & Explanation
Correct Answer: C
Rationale: The Joint Line Convergence Angle (JLCA) measures the "gap" between the femoral and tibial joint surfaces on a standing radiograph. A normal JLCA is 0-2 degrees. An elevated value, such as 8 degrees, indicates significant intra-articular deformity (e.g., cartilage loss on one side) or stretching of the collateral ligaments.
Question 91
A 45-year-old male presents with knee arthritis years after a femoral shaft fracture healed with 20 degrees of varus malunion. When planning a combined osteotomy and TKA, what is the single most critical geometric point to identify on the preoperative radiograph?
View Answer & Explanation
Correct Answer: D
Rationale: The CORA is the geometric apex of the deformity, found at the intersection of the proximal and distal mechanical axis lines of the deformed bone. Identifying the CORA is the most critical step because it defines the exact location of the deformity and dictates the strategy for the corrective osteotomy.
Question 92
A surgeon is planning a corrective osteotomy for a simple angular deformity in the distal femur. According to Paley's Osteotomy Rules, what is the outcome if the osteotomy is performed precisely at the CORA and only an angular correction is applied?
View Answer & Explanation
Correct Answer: D
Rationale: This scenario describes Paley's Osteotomy Rule 1. When an osteotomy for a simple angular deformity is performed at the CORA, a pure angular correction (hinge-like motion) realigns the proximal and distal axes perfectly without inducing any translation. This is the most ideal and elegant correction.
Question 93
A surgeon plans to address a 15-degree varus deformity from a mid-diaphyseal femoral malunion by performing a TKA with asymmetric intra-articular bone resections (i.e., resecting more medial distal femur and less lateral). This approach represents a violation of which of Paley's Osteotomy Rules and will most likely result in what complication?
View Answer & Explanation
Correct Answer: C
Rationale: This is a classic violation of Osteotomy Rule 3. The osteotomy (the TKA resection) is performed far from the diaphyseal CORA, and the correction is purely angular without translation. This creates a new deformity at the joint, resulting in an oblique joint line, collateral ligament instability, and inevitable early implant failure.
Question 94
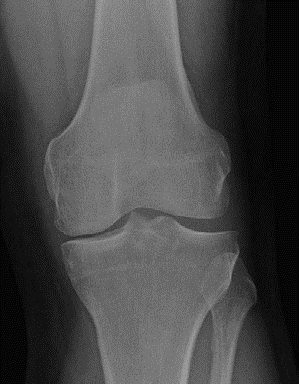
A 68-year-old male presents with bilateral knee pain and difficulty walking. A full-length standing radiograph is shown. Based on a visual assessment of the joint orientation angles in the right knee, what is the most likely primary contributor to his varus deformity?

View Answer & Explanation
Correct Answer: B
Rationale: The image demonstrates significant genu varum. Visually, the joint line of the proximal tibia appears to slope downwards medially, suggesting a decreased Medial Proximal Tibial Angle (MPTA), which is characteristic of a proximal tibial varus deformity. The distal femur does not show an obvious valgus deformity.
Question 95
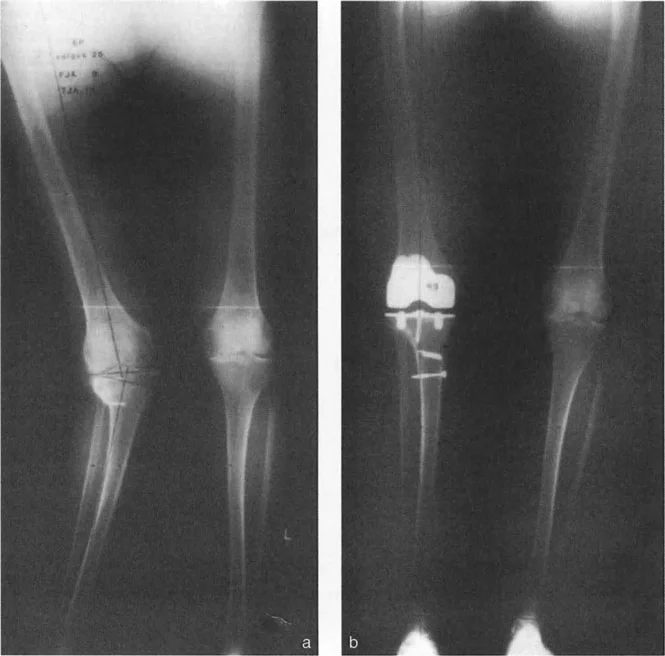
A surgeon is planning a complex TKA for a patient with a valgus deformity originating in the distal femur. The provided image shows the preoperative plan. What procedure is being planned?

View Answer & Explanation
Correct Answer: C
Rationale: The image clearly illustrates a planned osteotomy in the supracondylar region of the femur, which is a distal femoral osteotomy (DFO). This is being done concurrently with a TKA to correct an extra-articular femoral deformity at its CORA, thereby restoring the mechanical axis before implanting the knee components.
Question 96
A 55-year-old patient presents with medial knee pain and varus malalignment. The preoperative plan is shown in the image. Based on the location of the planned osteotomy, what is the most appropriate surgical plan?

View Answer & Explanation
Correct Answer: B
Rationale: The image displays a preoperative plan for correcting a varus deformity originating in the proximal tibia. The osteotomy is marked in the metaphyseal bone of the tibia, consistent with a high tibial osteotomy (HTO). Since this is being planned with a TKA, the correct procedure is a combined TKA and HTO.
Question 97
A 48-year-old patient with a history of a severe tibial plateau and shaft fracture treated with internal fixation presents with pain and deformity. The radiograph is shown. Compared to a primary TKA, what is the most significant challenge in planning this patient's reconstruction?

View Answer & Explanation
Correct Answer: C
Rationale: The image shows a complex post-traumatic condition with malunion at multiple levels (multi-apical) and retained hardware. This presents a profound challenge requiring meticulous preoperative planning to identify all CORAs, plan for hardware removal, and execute a multi-level correction, which is far more complex than a standard TKA.
Question 98
A 59-year-old male has a severe, multiplanar post-traumatic deformity of his lower leg involving 15 degrees of varus, 20 degrees of procurvatum, and 25 degrees of internal rotation. In addition to full-length standing films, which imaging modality is most crucial for accurately quantifying the rotational component of the deformity?
View Answer & Explanation
Correct Answer: C
Rationale: While full-length films are essential for angular deformity in the coronal plane, a CT scan is invaluable and often the only reliable method for precisely measuring complex rotational deformities like femoral or tibial version. MRI is better for soft tissues, not rotational bone profiling.
Question 99
A 65-year-old female with developmental dysplasia of the hip (DDH) presents for a total hip arthroplasty (THA). She has a significant coxa vara deformity. Which joint orientation angle is most critical for evaluating her proximal femoral varus/valgus deformity and planning for appropriate offset restoration?
View Answer & Explanation
Correct Answer: D
Rationale: The mechanical Lateral Proximal Femoral Angle (mLPFA) is the key angle for assessing the alignment of the proximal femur. An abnormal mLPFA is indicative of a varus or valgus deformity of the femoral neck and head relative to the shaft, which is critical for planning stem placement and offset in THA, especially in cases like DDH.
Question 100
A surgeon identifies a CORA for a tibial deformity in a location with poor soft-tissue coverage and compromised bone quality, making an osteotomy at that site risky. According to Paley's Osteotomy Rules, what is an acceptable alternative strategy to restore the mechanical axis?
View Answer & Explanation
Correct Answer: C
Rationale: This scenario describes Paley's Osteotomy Rule 2. When the CORA is in a surgically unfavorable location, the surgeon can perform the osteotomy at a more amenable site. To restore the mechanical axis, this requires both an angular correction and a calculated translation of the bone segments.
You Might Also Like