Rheumatoid Finger Deformities: Pathomechanics and Surgical Management

Key Takeaway
Rheumatoid arthritis induces complex finger deformities through synovial proliferation, capsular attenuation, and musculotendinous imbalance. This comprehensive guide details the pathomechanics, clinical evaluation, and step-by-step surgical management of intrinsic plus and swan-neck deformities. Key concepts include the Bunnell test for intrinsic tightness, the Nalebuff classification for swan-neck deformities, and evidence-based operative interventions ranging from soft tissue releases and flexor tenodesis to proximal interphalangeal joint arthrodesis and arthroplasty.
Comprehensive Introduction and Patho-Epidemiology
The rheumatoid hand represents one of the most complex biomechanical challenges in the entirety of orthopedic surgery. Finger deformities in rheumatoid arthritis (RA) are rarely the result of a single, isolated structural failure. Rather, they are the culmination of normal physiological forces applied by extrinsic flexors and extensors acting upon joints that have been progressively weakened, attenuated, and destabilized by an aggressive, infiltrative synovitis. The resulting deformities—most notably the intrinsic plus, swan-neck, and boutonniere deformities—are manifestations of a multi-planar collapse pattern that severely compromises hand function, grip strength, and fine motor dexterity.
Rheumatoid arthritis is a systemic autoimmune disease characterized by chronic inflammation of the synovial lining of diarthrodial joints and tendon sheaths. The hypertrophic synovium, or pannus, aggressively proliferates and acts as a locally destructive tissue. It releases a cascade of proteolytic enzymes, matrix metalloproteinases, and inflammatory cytokines (such as TNF-alpha and IL-6) that directly degrade articular cartilage, subchondral bone, and the critical periarticular soft tissue restraints. As the capsuloligamentous structures attenuate, the delicate balance of the digital extensor and flexor mechanisms is irrevocably altered. The pathogenesis is inherently multifactorial, involving tightness of the intrinsic muscles, displacement of the lateral bands of the extensor hood, central slip rupture, or the attenuation and rupture of the long extensor or long flexor tendons.
Furthermore, flexor tenosynovitis frequently produces a mechanical limitation of interphalangeal joint motion that must be meticulously evaluated. In these cases, the range of active flexion of the interphalangeal joints is significantly less than passive flexion. This discrepancy is a critical clinical distinction that dictates surgical decision-making, as it differentiates a primary joint contracture from a tendinous excursion deficit. Epidemiologically, hand and wrist involvement occurs in up to 90% of patients with advanced RA. Despite the advent of biologic disease-modifying antirheumatic drugs (bDMARDs) which have dramatically reduced the incidence of severe end-stage deformities, the orthopedic surgeon must still possess a profound understanding of these pathomechanics to manage the substantial population of patients who either fail medical management or present with established, chronic deformities.
The progressive nature of these deformities necessitates a proactive and highly analytical approach to patient evaluation. The surgeon must decipher whether a deformity is primarily driven by articular destruction, soft tissue contracture, tendinous rupture, or a combination thereof. A failure to accurately identify the primary driver of the deformity will inevitably lead to surgical failure, as addressing a secondary consequence without correcting the primary deforming force guarantees recurrence. Therefore, the mastery of rheumatoid hand surgery relies not merely on technical execution, but on an exhaustive understanding of the underlying patho-epidemiology and the intricate biomechanical interplay of the digits.
Detailed Surgical Anatomy and Biomechanics
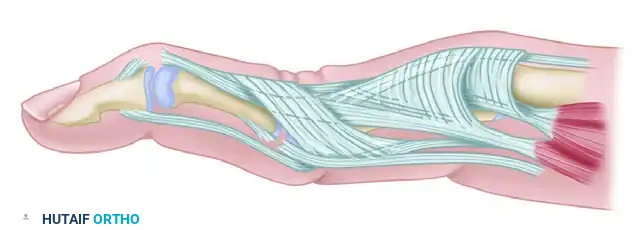
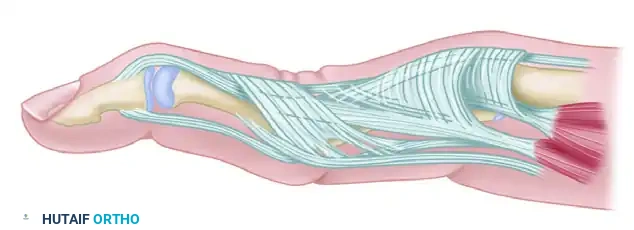
To comprehend the pathomechanics of rheumatoid finger deformities, one must first master the intricate anatomy of the digital extensor and flexor mechanisms, as well as the intrinsic musculature. The extensor mechanism is a highly sophisticated, multi-tendinous aponeurosis that coordinates motion across the metacarpophalangeal (MCP), proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints. The extrinsic extensor tendon (extensor digitorum communis) enters the finger centrally, stabilized by the sagittal bands at the MCP joint. As it traverses distally, it trifurcates into a central slip, which inserts onto the dorsal base of the middle phalanx to extend the PIP joint, and two lateral slips. These lateral slips merge with the intrinsic tendons to form the lateral bands, which continue distally to converge and insert as the terminal tendon on the dorsal base of the distal phalanx, extending the DIP joint.
The intrinsic muscles, comprising the lumbricals and the volar and dorsal interossei, are critical modulators of digital posture. Anatomically, the intrinsic tendons pass volar to the axis of rotation of the MCP joint and dorsal to the axis of rotation of the PIP joint. Consequently, their contraction yields MCP joint flexion and PIP joint extension. The intrinsic tendons fan out into the extensor hood, contributing transverse fibers that flex the MCP joint, and oblique fibers that join the lateral bands to extend the PIP and DIP joints. In the rheumatoid hand, chronic inflammation and spasticity lead to fibrotic contracture of these intrinsic muscles. When contracted, they force the hand into the classic "intrinsic plus" posture. This creates a powerful deforming force that, if left unchecked, contributes significantly to the development of swan-neck deformities and ulnar drift.

The retinacular ligaments play a pivotal role in synchronizing interphalangeal joint motion. The transverse retinacular ligament pulls the lateral bands volarly during PIP flexion, preventing dorsal subluxation. Conversely, the triangular ligament prevents excessive volar subluxation of the lateral bands during PIP extension. The oblique retinacular ligament (ORL), or Landsmeer's ligament, originates from the volar aspect of the proximal phalanx and the flexor tendon sheath, passes volar to the PIP joint axis, and inserts dorsally onto the terminal tendon. This unique trajectory links PIP and DIP joint motion; as the PIP joint extends, the ORL tightens and facilitates DIP joint extension. In rheumatoid swan-neck deformities, attenuation of the transverse retinacular ligament and contracture of the triangular ligament allow the lateral bands to subluxate dorsally, locking the PIP joint in hyperextension and rendering them ineffective at extending the DIP joint.
On the volar aspect, the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons glide within a highly constrained fibro-osseous sheath. The volar plate of the PIP joint is a robust, fibrocartilaginous structure that prevents PIP joint hyperextension. In the rheumatoid patient, aggressive flexor tenosynovitis can attenuate the volar plate and the FDS tendon insertions. The loss of FDS tension, combined with the overpull of the central tendon slip and intrinsic tightness, stretches these volar restraints, initiating the hyperextended swan-neck position. Understanding this delicate balance of forces—where the failure of a single volar restraint or the contracture of a single dorsal structure can precipitate a cascade of multi-joint collapse—is absolute paramount for the reconstructive hand surgeon.
Exhaustive Indications and Contraindications
The surgical management of rheumatoid finger deformities is highly individualized, relying heavily on the flexibility of the deformity, the integrity of the articular surfaces, and the status of the adjacent joints. The Nalebuff classification for swan-neck deformities remains the gold standard for guiding these surgical indications. Type I deformities are characterized by a flexible PIP joint in all positions of the MCP joint, primarily driven by PIP hyperextension with secondary DIP flexion. The indication here is a soft tissue procedure to restrict PIP hyperextension, such as an FDS tenodesis, dermodesis, or ORL reconstruction. Type II deformities exhibit PIP joint flexion limitation exclusively when the MCP joint is extended, indicating intrinsic tightness. The absolute indication for Type II is an intrinsic release, often combined with an FDS tenodesis to address the volar plate laxity.
Type III deformities present a more complex challenge: the PIP joint is stiff and does not allow satisfactory flexion regardless of MCP position, yet radiographs demonstrate a well-preserved PIP joint space without significant cartilaginous destruction. The indication for Type III is an extensive soft tissue reconstruction, including lateral band mobilization, dorsal skin release, and potentially a dorsoproximal interphalangeal capsulotomy. Conversely, Type IV deformities are characterized by fixed PIP joint hyperextension with radiographic evidence of advanced intra-articular destruction, cartilage loss, and erosions. In these cases, soft tissue procedures are strictly contraindicated as they will uniformly fail. The absolute indication for Type IV is osseous stabilization, primarily PIP joint arthrodesis for the index and middle fingers to provide a stable pinch post, or PIP joint arthroplasty for the ring and small fingers to preserve grip span.
Contraindications must be meticulously respected to avoid catastrophic outcomes in this vulnerable patient population. Active, untreated systemic infection or localized soft tissue infection is an absolute contraindication to any elective reconstructive procedure. Furthermore, performing a PIP joint arthroplasty in the presence of an unstable, uncorrected MCP joint or an incompetent flexor mechanism is contraindicated, as the implant will rapidly fail due to unaddressed deforming forces. Poor soft tissue envelope quality, severe vasculitis, or profound osteopenia may also preclude the use of certain hardware or implants, necessitating a shift toward simple arthrodesis or even salvage ray amputation in extreme cases.
| Deformity Classification | Clinical Presentation | Primary Surgical Indications | Absolute / Relative Contraindications |
|---|---|---|---|
| Intrinsic Plus (Isolated) | Positive Bunnell test; flexible joints | Intrinsic release (oblique fiber resection) | Fixed joint contracture (requires capsulotomy) |
| Swan-Neck Type I | Flexible PIP hyperextension; normal MCP | FDS tenodesis, dermodesis, ORL reconstruction | Stiff PIP joint; severe joint destruction |
| Swan-Neck Type II | PIP stiff only with MCP extension | Intrinsic release + FDS tenodesis | Failure to recognize concurrent volar plate laxity |
| Swan-Neck Type III | Stiff PIP; preserved joint space on X-ray | Lateral band mobilization, capsulotomy, manipulation | Joint destruction (Type IV); severe osteopenia |
| Swan-Neck Type IV | Fixed PIP hyperextension; destroyed joint | PIP Arthrodesis (Index/Long) or Arthroplasty (Ring/Small) | Active infection; Arthroplasty contraindicated if MCP is unstable |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning begins with an exhaustive clinical examination to isolate the specific anatomical structures driving the deformity. The Bunnell test (intrinsic tightness test) is the cornerstone of this evaluation. The examiner evaluates the degree of passive PIP joint flexion under two distinct conditions: first, with the MCP joint held in full extension (stretching the intrinsic muscles), and second, with the MCP joint held in full flexion (relaxing the intrinsic muscles). Variable degrees of passive PIP joint flexion loss when the MCP joint is held in extension definitively indicate intrinsic tightness.

A critical clinical pearl when performing the Bunnell test is avoiding false negatives in the presence of ulnar drift. Intrinsic tightness may be predominantly or exclusively present on the ulnar side. To test this accurately, strict axial alignment of the finger with the metacarpal must be maintained by the examiner. Any ulnar deviation at the MCP joint during the test will slacken the intrinsic muscles on the ulnar side of the finger, potentially masking the tightness and confusing the clinical findings. Similarly, the tightness of the oblique retinacular ligament (ORL) must be assessed. The ORL test involves holding the PIP joint in maximal extension and evaluating the resistance to passive flexion of the DIP joint. If DIP flexion is limited with PIP extension but improves with PIP flexion, ORL tightness is confirmed.

Radiographic evaluation is mandatory for all patients presenting with rheumatoid finger deformities. Standard posteroanterior, true lateral, and oblique radiographs of the hand and specific digits are obtained. The surgeon must meticulously evaluate the joint space, the presence of marginal erosions, subchondral cysts, periarticular osteopenia, and the degree of subluxation or dislocation. For patients mapped for PIP joint arthrodesis, pre-operative templating is essential to determine the optimal angle of fusion (typically 25° for the index finger, increasing by 5° for each ulnar digit, up to 40° for the small finger) and to select the appropriate fixation hardware, bearing in mind the often profound osteopenia present in RA patients. If arthroplasty is considered, templating ensures appropriate implant sizing and confirms sufficient bone stock for stem fixation.
Patient positioning is standardized but requires careful attention to detail. The patient is placed supine on the operating table with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the upper arm to ensure a bloodless surgical field, which is critical for the meticulous dissection of delicate tendinous and neurovascular structures. The use of loupe magnification (typically 2.5x to 3.5x) is mandatory for identifying the precise anatomical layers of the extensor mechanism and protecting the digital neurovascular bundles. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation, and the limb is exsanguinated using an Esmarch bandage, unless severe tenosynovitis or a history of deep vein thrombosis dictates elevation exsanguination only.
Step-by-Step Surgical Approach and Fixation Technique
Intrinsic Release
When intrinsic tightness limits function and contributes to progressive deformity (Type II Swan-Neck or isolated Intrinsic Plus), surgical release is indicated. The primary goal is to resect the oblique fibers of the intrinsic wing tendon that extend to the lateral bands, thereby removing the deforming extension force on the PIP joint while strictly preserving the transverse fibers that flex the MCP joint.
The procedure begins with a dorsal longitudinal or curvilinear incision made over the proximal phalanx, ensuring adequate exposure of the extensor hood. The skin flaps are elevated full-thickness to protect the delicate dorsal sensory nerve branches. The extensor mechanism is identified, and the intrinsic tendon is traced as it fans out into the transverse and oblique fibers. Using sharp dissection, a triangular segment of the oblique fibers of the intrinsic expansion is excised bilaterally. In cases where the Bunnell test indicates isolated ulnar intrinsic tightness (common in early ulnar drift), the resection may be performed unilaterally on the ulnar side. Crucially, the surgeon must verify the release intraoperatively; the Bunnell test is repeated on the table. Full passive PIP flexion must now be achievable with the MCP joint fully extended. Failure to achieve this indicates an incomplete release or an unrecognized secondary contracture.
Flexor Digitorum Superficialis (FDS) Tenodesis
For Type I and Type II swan-neck deformities where volar plate attenuation is the primary driver of PIP hyperextension, an FDS tenodesis provides a robust volar tether. A volar Bruner (zig-zag) or mid-lateral incision is made over the PIP joint and proximal phalanx. The neurovascular bundles are identified and gently retracted. The flexor tendon sheath is exposed and carefully opened, strictly preserving the critical A2 and A4 pulleys to prevent secondary flexor tendon bowstringing.
One slip of the FDS tendon (typically the ulnar slip) is identified and divided proximally at the level of the A1 pulley or the proximal edge of the A2 pulley, leaving its distal insertion at the middle phalanx intact. This harvested FDS slip is then routed volarly and prepared for anchoring into the proximal phalanx. A bony trough or drill hole is created in the proximal phalanx, just proximal to the PIP joint articular surface. The tendon is tensioned to hold the PIP joint in approximately 20 to 30 degrees of flexion. Fixation is achieved using a bone anchor, a pull-out suture tied over a dorsal button, or through an intraosseous routing technique. The tension must be precise; over-tensioning will result in a debilitating fixed flexion contracture, while under-tensioning will fail to prevent recurrent hyperextension.
Proximal Interphalangeal Joint Arthrodesis
For Type IV deformities, or severe Type III deformities where soft tissue reconstruction is deemed unreliable, PIP arthrodesis provides definitive correction, stability, and pain relief. A dorsal longitudinal or lazy-S incision is made directly over the PIP joint. The extensor mechanism is incised longitudinally, dividing the central slip, and the collateral ligaments are sharply excised from their proximal origins to fully expose the joint surfaces and allow for complete joint dislocation.

The destroyed articular cartilage and sclerotic subchondral bone are meticulously resected. To maximize bony contact and allow for angular adjustments, a cup-and-cone reamer system is highly recommended, though flat oscillating saw cuts can be utilized if bone stock is severely depleted. The joint is positioned in functional flexion (25° index, 30° middle, 35° ring, 40° small). Fixation in osteopenic rheumatoid bone is notoriously challenging. The 90-90 intraosseous wiring technique combined with a single oblique Kirschner wire offers excellent compression and rotational stability. Alternatively, tension band wiring, dorsal mini-plates, or headless compression subchondral screws can be utilized depending on surgeon preference and bone quality. Once rigid fixation is confirmed fluoroscopically, the extensor mechanism is reapproximated over the hardware to provide a robust soft tissue envelope, and the skin is closed without tension.
Complications, Incidence Rates, and Salvage Management
The surgical management of rheumatoid hand deformities is fraught with potential complications, driven by the inherently compromised nature of the patient's soft tissues, poor bone quality, and systemic immunosuppression. Wound healing complications and superficial infections are relatively common, occurring in 5-10% of cases, exacerbated by chronic corticosteroid use and bDMARD therapy. These are typically managed with oral antibiotics and local wound care, though deep infections requiring operative debridement and hardware removal occur in 1-2% of arthrodesis cases.
A primary complication specific to soft tissue reconstructions, particularly FDS tenodesis, is the development of a progressive PIP joint flexion contracture. This occurs in up to 15% of patients and is almost exclusively the result of intraoperative over-tensioning of the tenodesis slip or prolonged postoperative immobilization. If the contracture exceeds 40 degrees and severely limits function, a salvage surgical release or conversion to a PIP arthrodesis may be necessary. Conversely, recurrent swan-neck deformity occurs in 10-20% of soft tissue procedures over a 5-10 year follow-up period, as the underlying rheumatoid disease continues to stretch out the reconstructed ligaments.
Nonunion is the most dreaded complication following PIP joint arthrodesis, with reported incidence rates ranging from 5% to 15% in the rheumatoid population. The profound periarticular osteopenia and impaired biologic healing capacity contribute significantly to this risk. Asymptomatic nonunions (fibrous unions) that maintain acceptable alignment may be observed. However, symptomatic nonunions with hardware failure, pain, or progressive deformity require revision surgery. Salvage management typically involves hardware removal, autologous bone grafting (often from the distal radius or iliac crest), and revision fixation with a more robust construct, such as a dorsal compression plate. In cases of catastrophic bone loss or recalcitrant infection, a salvage ray amputation may be the most functional and definitive option for the patient.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Progressive Flexion Contracture | 10 - 15% | Over-tensioning of FDS tenodesis; prolonged splinting | Aggressive hand therapy; Surgical release; Conversion to Arthrodesis |
| Recurrent Swan-Neck Deformity | 10 - 20% | Under-tensioning; progressive RA disease activity | Revision soft tissue reconstruction; PIP Arthrodesis |
| PIP Arthrodesis Nonunion | 5 - 15% | Severe osteopenia; inadequate fixation; smoking; steroids | Revision fixation with bone grafting; Dorsal plating; Fibrous union observation |
| Deep Surgical Site Infection | 1 - 2% | Immunosuppression (bDMARDs); poor skin envelope | I&D; Hardware removal; IV antibiotics; potentially Ray Amputation |
| Hardware Prominence / Failure | 5 - 10% | K-wire migration; thin dorsal skin over plates | Hardware removal after clinical union is achieved |
Phased Post-Operative Rehabilitation Protocols
The success of rheumatoid hand reconstruction is inextricably linked to a meticulously executed, phased postoperative rehabilitation protocol. The protocol must be specifically tailored to the procedure performed, balancing the need to protect delicate soft tissue repairs or bony fusions with the imperative to prevent debilitating joint stiffness. Hand therapy should be initiated and guided by a certified hand therapist (CHT) familiar with the unique fragility of the rheumatoid patient.
Protocol for Soft Tissue Reconstructions (Intrinsic Release, FDS Tenodesis):
* Phase I (0 - 2 Weeks): Unlike arthrodesis, soft tissue procedures designed to correct hyperextension (like FDS tenodesis) do not require strict, prolonged immobilization. The primary goal is to prevent severe stiffness while relying on the tenodesis to block terminal extension. The hand is placed in a bulky soft dressing postoperatively. Within 3 to 5 days, a custom dorsal block splint is fabricated, maintaining the PIP joint in 20-30 degrees of flexion to protect the tenodesis. Immediate, controlled active flexion of the PIP and DIP joints is encouraged within the constraints of the splint.
* Phase II (2 - 6 Weeks): Sutures are removed at 14 days. The dorsal block splint is worn continuously between exercise sessions. Active and active-assisted range of motion (ROM) exercises are progressed. The therapist focuses on differential tendon gliding exercises to prevent adhesions between the FDS, FDP, and the reconstructed tissues. Extension is strictly limited to the block provided by the splint.
* Phase III (6+ Weeks): The dorsal block splint is gradually weaned, initially during the day and eventually at night. Gentle passive extension stretching may be initiated if a flexion contracture is developing, but this must be done cautiously to avoid attenuating the tenodesis. Light strengthening exercises and functional use of the hand are incorporated, with a return to full activity typically achieved by 10 to 12 weeks.
Protocol for Proximal Interphalangeal Joint Arthrodesis:
* Phase I (0 - 4 Weeks): Arthrodesis requires strict, uninterrupted immobilization to achieve bony union. The operated digit is placed in a custom static extension splint or cast, protecting the PIP joint. Crucially, active ROM of the adjacent joints—the MCP and DIP joints—is encouraged immediately to prevent secondary stiffness, which develops rapidly in the rheumatoid hand.
* Phase II (4 - 8 Weeks): Clinical and radiographic evaluation is performed at 4 to 6 weeks. If there is evidence of trabecular bridging and no clinical pain at the fusion site, the rigid splint may be transitioned to a buddy tape or a lighter removable splint for protection during heavy activities. ROM exercises for the MCP and DIP joints are intensified.
* Phase III (8+ Weeks): Once solid radiographic union is confirmed, all splinting is discontinued. The focus shifts to maximizing grip strength and optimizing the functional use of the hand with the newly stabilized pinch post. Patients must be counseled that the fused joint will never bend again, and occupational therapy focuses on adaptive strategies for activities of daily living.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for rheumatoid finger deformities is deeply rooted in landmark anatomical and clinical studies. Sterling Bunnell’s original descriptions of the intrinsic musculature and his eponymous test for intrinsic tightness remain the foundational pillars of clinical evaluation. Bunnell accurately identified that the spasticity and contracture of these tiny muscles were the primary culprits in the devastating intrinsic plus deformity, paving the way for targeted surgical releases.
The classification and treatment algorithm for the swan-neck deformity were definitively established by Nalebuff, Millender, and Feldon in the 1970s and 1980s. Their categorization of deformities into Types I through IV based on joint flexibility and radiographic preservation shifted the paradigm from a "one-size-fits-all" approach to a highly specific, pathology-driven treatment algorithm. Their seminal papers demonstrated that performing soft tissue releases on destroyed joints (Type IV) uniformly failed, while performing arthrodesis on flexible joints (Type I) unnecessarily sacrificed motion. This classification system remains universally adopted in contemporary clinical guidelines.
Literature regarding the outcomes of the FDS tenodesis (frequently utilizing the techniques described by Curtis or Beckenbaugh) demonstrates high rates of success in preventing recurrent PIP hyperextension, provided the volar plate attenuation is accurately identified and the tenodesis is not over-tensioned. Long-term follow-up studies indicate that while some degree of stretching occurs over time, the functional improvement in grip and pinch is maintained in the majority of patients.
For PIP joint arthrodesis, the literature extensively debates the optimal fixation method. Studies comparing tension band wiring, 90-90 intraosseous wiring, and headless compression screws in rheumatoid patients generally show comparable union rates (85-95%) when performed meticulously. However, the consensus guidelines emphasize that the choice of implant is secondary to the adequate preparation of the joint surfaces and the precise positioning of the digit in functional flexion. Current clinical guidelines strongly advocate for early surgical intervention in the rheumatoid hand—before fixed contractures and joint destruction occur—to maximize the efficacy of joint-preserving soft tissue reconstructions and maintain the highest possible level of patient function.
