Excision of Dorsal and Volar Wrist Ganglions: A Comprehensive Surgical Guide
Key Takeaway
Wrist ganglion excision requires meticulous dissection to prevent recurrence and neurovascular injury. For dorsal ganglions, the stalk is typically traced to the scapholunate interval. Volar ganglions require careful mobilization of the radial artery and protection of the palmar cutaneous branch of the median nerve. Complete excision of the cyst complex, including its capsular origin, is the gold standard for minimizing recurrence rates in both approaches.
Comprehensive Introduction and Patho-Epidemiology
Ganglion cysts represent the most ubiquitous soft-tissue neoplastic-like masses of the hand and wrist, comprising an overwhelming 50% to 70% of all such clinical presentations. These benign, mucin-filled pseudocysts typically arise in intimate association with adjacent joint capsules, intrinsic carpal ligaments, or tendon sheaths. Epidemiologically, they demonstrate a pronounced predilection for the female demographic, with a female-to-male ratio approaching 3:1, and most frequently manifest during the second to fourth decades of life. Despite their prevalence, the precise pathophysiological mechanisms governing their genesis remain a subject of rigorous academic debate and histological investigation within the orthopedic community.
The prevailing pathophysiological paradigm posits that ganglions are not true cysts—as they lack a definitive epithelial or synovial cellular lining—but rather represent the sequelae of mucoid degeneration within periarticular connective tissues. This fibroblastic proliferation and subsequent hyaluronic acid elaboration are thought to be catalyzed by repetitive microtrauma or underlying capsular laxity. A critical biomechanical component of this theory is the "check-valve" mechanism: a unidirectional, micro-fistulous tract connecting the underlying radiocarpal or midcarpal joint space to the main cyst body. This anatomical anomaly allows synovial fluid to be pumped outward into the periarticular tissues during extreme ranges of wrist motion, where it subsequently concentrates, thickens, and coalesces into the highly viscous, jelly-like mucin characteristic of these masses.
Histologically, the cyst wall is composed of densely packed, randomly oriented collagen fibers interspersed with a sparse population of fibroblasts and fibrocytes. The mucinous fluid contained within the cyst is rich in glucosamine, globulins, and predominantly, high-molecular-weight hyaluronic acid. This biochemical composition explains the high viscosity and translucent, gelatinous appearance of the fluid upon aspiration or surgical rupture. Understanding this structural lack of a true secretory lining is paramount; it underscores why simple aspiration or cyst wall fenestration is plagued by unacceptably high recurrence rates, as the underlying capsular defect and check-valve mechanism remain completely unaddressed.
Clinically, wrist ganglions are broadly categorized by their anatomical epicenter: dorsal and volar. Dorsal wrist ganglions are overwhelmingly the most common, accounting for approximately 60% to 70% of wrist ganglions, and predominantly originate from the dorsal scapholunate interosseous ligament (SLIL) interval. Conversely, volar wrist ganglions, comprising roughly 20% to 30%, typically arise from the radiocarpal joint (specifically the radioscaphoid interval) or the scaphotrapezial (ST) joint. While a significant proportion of these masses remain asymptomatic and may even undergo spontaneous resolution via cyst wall rupture and fluid resorption, surgical excision is definitively indicated for patients experiencing persistent, intractable pain, mechanical impingement, secondary compressive neuropathies, or significant cosmetic deformity that has proven refractory to conservative modalities.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional spatial awareness of wrist anatomy is the absolute prerequisite for the safe and definitive extirpation of ganglion cysts. The surgical approach, whether dorsal or volar, must meticulously navigate a highly complex topography of neurovascular bundles, gliding tendinous structures, and biomechanically critical intrinsic ligaments.
Dorsal Wrist Extensor Compartments and Ligamentous Anatomy
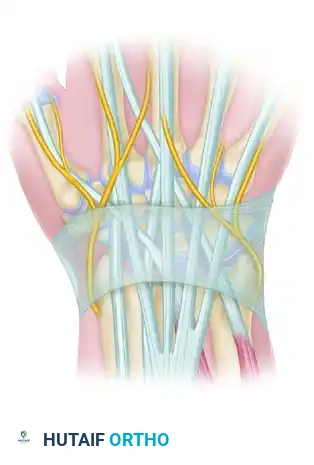
The dorsal aspect of the radiocarpal and midcarpal joints is organized into six distinct extensor compartments, segregated by vertical septa descending from the extensor retinaculum to the underlying distal radius and ulna. A dorsal ganglion classically presents as a lobulated mass emerging through the retinacular fibers, typically localizing precisely between the third and fourth extensor compartments. The third compartment houses the Extensor Pollicis Longus (EPL) tendon, which executes a sharp radial turn around Lister's tubercle. The fourth compartment contains the multiple slips of the Extensor Digitorum Communis (EDC) and the Extensor Indicis Proprius (EIP). The surgical interval between the EPL and EDC provides the most direct and anatomically sound trajectory to the dorsal joint capsule.
Deep to these tendinous structures lies the dorsal wrist capsule and the critical intrinsic carpal ligaments. The stalk of a dorsal ganglion almost universally originates from the capsule directly overlying the Scapholunate Interosseous Ligament (SLIL). The SLIL is a C-shaped ligamentous complex composed of dorsal, proximal (membranous), and volar regions. The dorsal band of the SLIL is the thickest, most robust, and biomechanically paramount stabilizer of the scapholunate articulation, possessing a yield strength significantly higher than its volar counterpart. The surgeon must possess the anatomical acumen to differentiate the redundant, pathologically distended dorsal capsule—which must be excised—from the underlying transversely oriented, taut fibers of the dorsal SLIL, which must be scrupulously preserved.
Furthermore, the superficial neurovascular anatomy demands meticulous attention. The superficial branch of the radial nerve (SRN) courses radially, providing sensation to the dorsal-radial aspect of the hand, while the dorsal cutaneous branch of the ulnar nerve (DCBUN) supplies the ulnar dorsum. Deep within the operative field, the terminal sensory branch of the posterior interosseous nerve (PIN) resides within the floor of the fourth extensor compartment. This nerve provides nociceptive innervation to the dorsal wrist capsule. In cases of chronic, painful dorsal ganglions, some surgeons advocate for a concomitant prophylactic PIN neurectomy to alleviate capsular pain, though this remains a topic of surgeon preference.
Volar Wrist Flexor Compartments and Neurovascular Topography
The anatomical landscape of the volar wrist is inherently more hazardous, demanding an even higher degree of surgical precision. Volar ganglions are intimately associated with the radial artery and the flexor tendon sheaths. The mass is classically situated just radial to, or immediately beneath, the Flexor Carpi Radialis (FCR) tendon. The FCR tendon sheath often serves as a superficial boundary, and retracting the FCR ulnarly is a standard maneuver to expose the deeper capsular origins.
The most critical structure in this surgical theater is the radial artery. The artery courses distally along the volar aspect of the radius, passing directly over the radioscaphoid joint—a frequent site of volar ganglion origin. The radial artery frequently becomes intimately entwined with the lobulations of the ganglion cyst, with the cyst wall adhering tenaciously to the arterial adventitia. In severe cases, the cyst may completely encircle the artery, necessitating painstaking micro-dissection to liberate the vessel without inducing vasospasm, intimal tearing, or catastrophic hemorrhage.
Equally treacherous is the Palmar Cutaneous Branch of the Median Nerve (PCBMN). This delicate sensory nerve typically arises from the radial aspect of the median nerve approximately 5 cm proximal to the distal wrist crease. It travels distally in the interval between the FCR and the Palmaris Longus (PL), before piercing the antebrachial fascia to provide sensation to the base of the thenar eminence and the proximal palm. The PCBMN is notoriously unforgiving; iatrogenic traction, contusion, or transection frequently results in a devastating, recalcitrant neuroma that can render the hand functionally impaired due to severe neuropathic pain.
Exhaustive Indications and Contraindications
The decision-making algorithm for the surgical excision of wrist ganglions must be rooted in a comprehensive assessment of the patient's symptomatology, functional demands, and the natural history of the pathology. Because a substantial percentage of ganglions may spontaneously resolve, particularly in pediatric populations, a period of watchful waiting is almost universally recommended as the initial management strategy for asymptomatic masses.
When conservative measures—such as observation, immobilization, or image-guided aspiration combined with corticosteroid injection—fail to yield durable relief, surgical intervention becomes the definitive treatment pathway. The primary indication for surgical excision is persistent, localized pain that significantly limits activities of daily living, occupational duties, or athletic participation. Mechanical symptoms, such as a palpable "clunking," restricted range of motion (particularly terminal wrist flexion for dorsal cysts and extension for volar cysts), or a subjective sense of weakness, are also robust indications for operative management.
Furthermore, ganglions can occasionally precipitate secondary compressive neuropathies. A volar ganglion extending proximally into the carpal tunnel may compress the median nerve, mimicking carpal tunnel syndrome. Similarly, a cyst extending into Guyon's canal can cause ulnar nerve entrapment, while a dorsal cyst may compress the terminal branches of the PIN, leading to a deep, aching dorsal wrist pain. In these scenarios, surgical excision serves a dual purpose: extirpation of the mass and decompression of the compromised neural structures. Aesthetic concerns, while subjective, are a valid indication for surgery, provided the patient is thoroughly counseled regarding the inevitable surgical scar and the inherent, albeit small, risk of postoperative recurrence.
Contraindications to surgical excision are relatively few but must be strictly respected. Absolute contraindications include the presence of active, localized soft-tissue infection or overlying cellulitis, which could seed the radiocarpal joint leading to septic arthritis. Vascular compromise is a critical relative contraindication, particularly for volar ganglions. An abnormal preoperative Allen test, indicating inadequate ulnar collateral perfusion to the superficial and deep palmar arches, should give the surgeon extreme pause. In such cases, the risk of iatrogenic radial artery injury during cyst dissection could result in catastrophic digital ischemia, necessitating complex vascular reconstruction or bypass.
| Category | Specific Clinical Scenarios | Rationale / Considerations |
|---|---|---|
| Absolute Indications | Compressive neuropathy (Median, Ulnar, or PIN) | Urgent decompression required to prevent irreversible axonal degeneration and motor/sensory loss. |
| Absolute Indications | Intractable pain failing conservative management | Chronic nociceptive signaling from capsular distension; requires excision of the capsular stalk. |
| Relative Indications | Significant mechanical block to ROM | Excision restores normal radiocarpal and midcarpal kinematics. |
| Relative Indications | Severe cosmetic deformity | Patient-driven indication; requires extensive preoperative counseling regarding scarring and recurrence. |
| Absolute Contraindications | Active overlying cellulitis or deep infection | High risk of iatrogenic septic arthritis via capsular penetration. |
| Relative Contraindications | Abnormal Allen Test (Volar Ganglions) | Indicates poor ulnar collateral flow; high risk of hand ischemia if radial artery is injured or requires ligation. |
| Relative Contraindications | Asymptomatic cysts in low-demand patients | Natural history favors observation; surgical risks (scar, stiffness, neuroma) outweigh benefits. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative preparation is the cornerstone of a successful, complication-free ganglion excision. The clinical evaluation must begin with a meticulous physical examination. Transillumination of the mass with a penlight in a darkened room is a classic and highly reliable diagnostic maneuver; the mucin-filled cyst will brightly transilluminate, differentiating it from solid neoplastic masses such as giant cell tumors of the tendon sheath, lipomas, or fibromas. A comprehensive neurovascular examination is mandatory, with specific attention paid to two-point discrimination in the median, ulnar, and radial nerve distributions, and a rigorously performed Allen test prior to any volar approach.
Imaging modalities, while not always necessary for classic, easily palpable cysts, play a vital role in surgical planning and ruling out concomitant pathology. Standard posteroanterior (PA), lateral, and scaphoid-view radiographs of the wrist are mandatory. These plain films are essential to exclude underlying osseous abnormalities that can mimic or accompany ganglions, such as a carpal boss (an osteophyte at the base of the 2nd/3rd metacarpal), advanced radiocarpal or midcarpal osteoarthritis, or signs of carpal instability like Scapholunate Advanced Collapse (SLAC). In cases of occult ganglions—where the patient presents with classic dorsal wrist pain exacerbated by extreme extension, but lacks a palpable mass—Magnetic Resonance Imaging (MRI) is the gold standard. MRI provides exquisite soft-tissue contrast, definitively localizing the micro-cyst and its capsular stalk, thereby guiding a targeted surgical approach. High-resolution ultrasound is also an excellent, cost-effective, and dynamic imaging alternative, particularly useful for mapping the precise relationship of a volar ganglion to the radial artery.
Patient positioning and operating room setup must be standardized to optimize surgical ergonomics and visualization. The patient is placed in the supine position with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal brachium. Anesthesia may consist of a regional block (such as an axillary brachial plexus block or a Bier block) or general anesthesia, depending on patient preference and anesthetic risk stratification. Recently, the WALANT (Wide Awake Local Anesthesia No Tourniquet) technique, utilizing a mixture of lidocaine and epinephrine, has gained traction for ganglion excisions, offering the benefits of intraoperative active motion testing and avoiding tourniquet discomfort.
If a traditional tourniquet is utilized, the limb is meticulously exsanguinated using an Esmarch bandage, and the tourniquet is inflated to 250 mm Hg (or approximately 100 mm Hg above the patient's systolic blood pressure). Loupe magnification (ranging from 2.5x to 3.5x) is not merely recommended; it is considered the standard of care. The use of magnification is absolutely critical for differentiating the delicate cyst wall from surrounding paratenon, identifying the microscopic capsular origin, and, most importantly, safeguarding the microscopic sensory nerve branches and the adventitia of the radial artery.
Step-by-Step Surgical Approach and Excision Technique
The surgical extirpation of a wrist ganglion must be viewed not as a simple mass enucleation, but as a precise anatomical dissection aimed at eradicating a pathological joint capsule complex. Adherence to strict, step-by-step anatomical principles minimizes the risk of recurrence and iatrogenic injury.
Excision of the Dorsal Wrist Ganglion
The dorsal approach begins with the precise placement of the skin incision. The surgeon may elect a transverse or a longitudinal orientation. A transverse incision, meticulously placed within Langer's lines (the natural skin tension lines of the wrist), generally yields a vastly superior cosmetic result, minimizing hypertrophic scarring. However, a longitudinal incision affords greater extensibility should the cyst track further proximally or distally than anticipated.
Following the skin incision, the subcutaneous tissues are spread longitudinally using fine tenotomy scissors or a hemostat. This blunt dissection technique is critical to identify and sweep away the delicate sensory branches of the superficial radial nerve (radially) and the dorsal branch of the ulnar nerve (ulnarly). These nerves must be gently retracted using blunt Ragnell or Sen retractors; excessive traction can induce a neuropraxia or a painful traction neuritis.
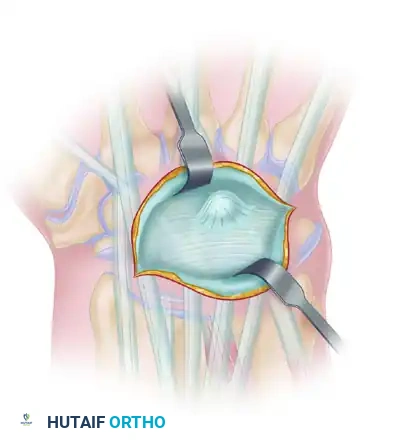
As the superficial dissection deepens, the glistening, transversely oriented fibers of the extensor retinaculum are exposed. The ganglion cyst will typically be visible as a bluish, translucent, tense bulge protruding through or stretching the retinacular fibers, classically localizing in the interval between the EPL (third compartment) and the EDC (fourth compartment).
The extensor retinaculum must be incised longitudinally directly over the apex of the cyst. The surgeon must exercise extreme caution during this step to avoid inadvertently incising the underlying, highly pressurized cyst wall. Premature rupture of the cyst leads to the immediate extravasation of thick, gelatinous mucin into the surgical field. While not biologically harmful, this deflation causes the mass to collapse, drastically altering the three-dimensional anatomy and rendering the subsequent tracing of the delicate stalk to its capsular origin significantly more arduous.
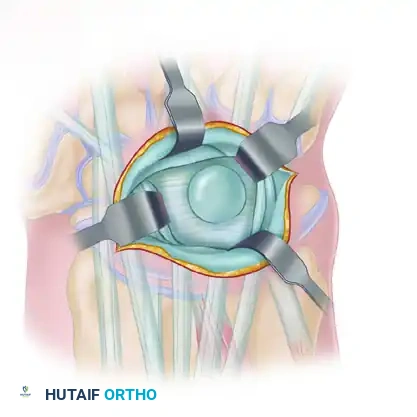
Once the retinaculum is sharply opened, the surgeon deploys self-retaining retractors (such as a small Weitlaner) or utilizes an assistant to maintain wide exposure. The Extensor Carpi Radialis Longus and Brevis tendons are mobilized radially, while the Extensor Digitorum Communis tendons are retracted ulnarly. Using a combination of sharp dissection with a #15 scalpel blade and blunt spreading with tenotomy scissors, the surgeon begins freeing the cyst from the surrounding paratenon and areolar tissue.
The dissection must proceed circumferentially around the cyst dome, progressing systematically from superficial to deep. As the dissection approaches the radiocarpal joint, the bulbous cyst will funnel down into a distinct, narrowed pedicle or "stalk" that dives deep between the carpal bones. The surgeon must resist the temptation to pull forcefully on the cyst dome; excessive traction will invariably avulse the stalk from the capsule, leaving the check-valve mechanism behind and guaranteeing a recurrence.
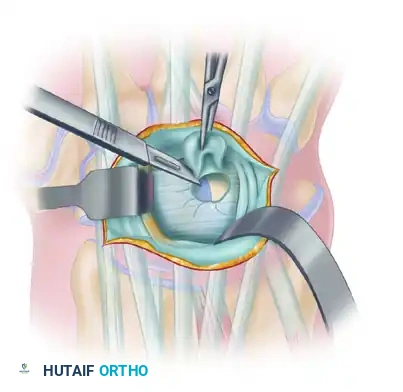
The most critical phase of the operation is the excision of the capsular origin. The stalk is meticulously traced down to its confluence with the dorsal wrist capsule, almost invariably located at the scapholunate interval.
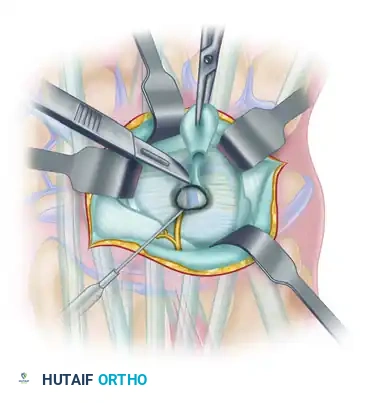
To ensure the complete eradication of the pathological check-valve mechanism, the surgeon must excise the stalk en bloc with a 5 mm to 1 cm rectangular or elliptical window of the surrounding dorsal capsule. During this capsular resection, the surgeon must clearly visualize the underlying, transversely oriented, stout fibers of the scapholunate interosseous ligament (SLIL). The scalpel blade must remain superficial to the SLIL. Iatrogenic transection of the dorsal SLIL is a catastrophic technical error that will immediately destabilize the scapholunate joint, leading to a Dorsal Intercalated Segment Instability (DISI) deformity and rapid progression to SLAC wrist arthrosis. Following excision, the capsular margins are lightly cauterized with bipolar electrocautery to destroy any residual microscopic satellite cysts. The capsular defect is intentionally left open; attempting to close it tightly can restrict terminal wrist flexion and is unnecessary for carpal stability.
Excision of the Volar Wrist Ganglion
The volar approach demands a heightened state of vigilance due to the unforgiving neurovascular anatomy. Under tourniquet control, a longitudinal or gently curvilinear incision is centered over the palpable mass, typically situated just radial to the FCR tendon. Meticulous, layer-by-layer dissection through the subcutaneous fat is performed. The surgeon must actively seek out and protect the palmar cutaneous branch of the median nerve (PCBMN), which lies ulnar to the FCR tendon but may exhibit aberrant branching patterns that cross the surgical field. The FCR tendon is identified, freed from its sheath, and retracted ulnarward.
The immediate next step is the definitive identification and mobilization of the radial artery. Utilizing loupe magnification and bipolar electrocautery, the surgeon carefully dissects the adventitia of the radial artery away from the adherent cyst wall. Fine tenotomy scissors are used to spread parallel to the vessel, never pointing the tips directly at the arterial wall. The artery must be mobilized over a sufficient length—often 3 to 4 cm—to allow it to be gently retracted radialward using a silicone vessel loop. Aggressive traction on the vessel loop must be strictly avoided to prevent vasospasm, intimal tearing, or subsequent thrombosis.
With the radial artery safely retracted radially and the FCR retracted ulnarly, the deep dissection commences. The ganglion cyst is dissected using a combination of blunt and sharp techniques, working in a proximal-to-distal direction. Volar ganglions frequently exhibit a multilobulated architecture, with extensions diving deep between the extrinsic flexor tendons. The stalk is traced down to its origin, which most commonly arises from the volar radioscaphoid joint capsule or the scaphotrapezial (ST) joint capsule. Similar to the dorsal approach, the origin of the stalk is excised en bloc with a small window of the surrounding volar capsule. Extreme care must be taken to avoid over-resecting the stout volar extrinsic carpal ligaments, such as the radioscaphocapitate (RSC) or long radiolunate (LRL) ligaments, as their compromise can lead to profound carpal instability.
Hemostasis and Closure Strategies
Prior to any wound closure, the pneumatic tourniquet must be deflated. This is an absolutely non-negotiable step, particularly following volar ganglion excisions. The surgeon must directly observe the radial artery to ensure brisk, pulsatile flow and the absence of vasospasm or pseudoaneurysm formation. Capillary refill in the digits must be confirmed. Meticulous hemostasis is then achieved using bipolar electrocautery to control any reactive bleeding from the capsular margins or subcutaneous venous plexus. Failure to achieve absolute hemostasis will result in a postoperative hematoma, which serves as a nidus for infection, increases fibroblastic scarring, and significantly exacerbates postoperative stiffness.
Closure of the extensor retinaculum (in dorsal approaches) is a subject of nuanced debate. Some surgeons prefer to leave the retinaculum completely open to prevent any constriction of the extensor tendons. Others advocate for a loose reapproximation or a step-cut lengthening repair to prevent postoperative tendon bowstringing. The subcutaneous tissues are closed meticulously with interrupted buried absorbable sutures (e.g., 4-0 or 5-0 Vicryl) to eliminate dead space and reduce tension on the skin edges. The skin is then closed according to surgeon preference, typically utilizing a running subcuticular closure with an absorbable monofilament (e.g., 4-0 Monocryl) or interrupted non-absorbable sutures (e.g., 5-0 Nylon). A sterile, non-adherent dressing (such as Xeroform or Telfa) is applied, followed by a bulky, compressive soft dressing. A volar resting splint is applied with the wrist in slight extension (10-15 degrees for dorsal excisions) or neutral position (for volar excisions) to protect the surgical site and mitigate immediate postoperative edema.
Complications, Incidence Rates, and Salvage Management
While the excision of a wrist ganglion is frequently perceived as a routine, entry-level outpatient procedure, the reality is that the margin for error is razor-thin. Complications, when they occur, can be profoundly debilitating and functionally devastating for the patient. A thorough understanding of these potential pitfalls and their salvage management is essential for the operating surgeon.
The most frequent complication, and the primary metric of surgical failure, is recurrence. Historically, simple aspiration yielded recurrence rates exceeding 60%. With modern open excision techniques emphasizing the removal of the capsular stalk and a window of the joint capsule, the recurrence rate for dorsal ganglions has been driven down to approximately 1% to 5%. Volar ganglions, however, historically demonstrate a slightly higher recurrence rate, ranging from 5% to 15%, largely due to the surgeon's understandable reluctance to perform a wide capsular resection in the immediate vicinity of the radial artery and volar extrinsic ligaments. Recurrences are managed initially with a return to conservative measures; if re-operation is mandated, the surgical field will be scarred, making neurovascular identification significantly more treacherous.
Neurovascular injuries represent the most catastrophic complications. Iatrogenic injury to the Palmar Cutaneous Branch of the Median Nerve (PCBMN) during a volar approach, or the Superficial Radial Nerve (SRN) during a dorsal approach, frequently results in a highly symptomatic neuroma. Patients present with severe, burning neuropathic pain, allodynia, and a positive Tinel's sign over the surgical scar. Management of an established neuroma is notoriously difficult, often requiring secondary surgery for neuroma excision and transposition of the proximal nerve stump deep into the pronator quadratus or brachioradialis muscle bellies, or utilizing advanced techniques such as Targeted Muscle Reinnervation (TMR). Vascular injury, specifically to the radial artery, can manifest as an acute hemorrhage, a delayed pseudoaneurysm, or arterial thrombosis. If the artery is inadvertently transected, and the patient has an incomplete palmar arch, immediate microsurgical primary repair or interposition vein grafting is mandatory to prevent digital ischemia.
Carpal instability is a rare but entirely preventable iatrogenic disaster. As previously detailed, overzealous resection of the dorsal capsule that inadvertently incorporates the dorsal band of the Scapholunate Interosseous Ligament (SLIL) will precipitate a DISI deformity. The patient will develop a painful "clunk" and progressive weakness. Salvage requires complex ligament reconstruction (e.g., Brunelli or modified Brunelli tenodesis) or, in delayed presentations with arthritic changes, salvage procedures such as a proximal row carpectomy (PRC) or partial wrist fusion.
| Complication | Estimated Incidence | Etiology / Risk Factors | Avoidance and Salvage Management |
|---|---|---|---|
| Recurrence | Dorsal: 1-5% |
