Reduction and Stabilization of the Distal Radioulnar Joint Following Galeazzi Fractures

Comprehensive Introduction and Patho-Epidemiology
In 1934, Riccardo Galeazzi meticulously described a distinct fracture pattern involving the junction of the middle and distal thirds of the radial diaphysis, drawing critical attention to the obligatory associated dislocation or severe subluxation of the distal radioulnar joint (DRUJ). While isolated diaphyseal fractures of the radius do occur, the Galeazzi fracture-dislocation represents a complex, high-energy disruption of the entire forearm axis. The integrity of the DRUJ is inextricably linked to the anatomic length, alignment, and rotation of the radius. Consequently, any significant shortening or angular deformity of the radius invariably compromises the congruency and stability of the DRUJ.
The pathogenesis of the Galeazzi fracture-dislocation is classically rooted in an axial load applied to a hyper-pronated forearm, typically coupled with extreme wrist hyperextension. This mechanism drives a massive kinetic force from the radial side of the hand, proximally through the carpus, into the distal radius, and subsequently propagating down the interosseous membrane (IOM) to exit through the DRUJ. Acute dislocations of the DRUJ can also occur in forced supination. This supination variant is frequently observed following a fall with a rotating body on an outstretched hand, or in catastrophic industrial workplace accidents where the upper extremity is violently twisted by rotating machinery. In industrial settings, it is imperative for the examining surgeon to look beyond technical jargon and obtain a layman’s description of the machinery to accurately estimate the immense torque and sheer forces imparted to the limb.

Historically, the natural history of the Galeazzi fracture-dislocation was fraught with devastating functional outcomes when managed non-operatively. In 1957, Hughston brought widespread academic attention to the abysmal results of these injuries when treated with closed reduction and casting alone. Utilizing exceedingly strict criteria for a "perfect" functional result, Hughston reported a 92% failure rate in non-operatively managed cases. This profound clinical revelation cemented the Galeazzi injury as the quintessential "fracture of necessity," mandating open reduction and rigid internal fixation (ORIF) of the radius to restore the anatomic foundation required for DRUJ stability.

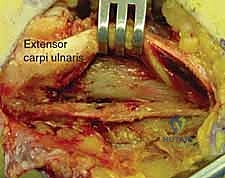
Even with modern internal fixation techniques, the DRUJ component of the Galeazzi fracture-dislocation remains a formidable challenge. After anatomic reduction and rigid fixation of the radius, the DRUJ must be meticulously re-evaluated. The joint can be conceptually divided into "simple" dislocations, which are concentrically reducible by closed means following radial length restoration, and "complex" dislocations, which are irreducible due to soft tissue interposition (such as the extensor carpi ulnaris tendon or capsular flaps) and mandate formal open reduction. The ultimate prognosis hinges heavily on the initial recognition of the DRUJ instability, the adequacy of the radial osteosynthesis, and the appropriate management of the ligamentous disruption at the ulnar head.
Detailed Surgical Anatomy and Biomechanics
The Triangular Fibrocartilage Complex (TFCC)
The triangular fibrocartilage complex is a highly specialized, heterogeneous structure that serves as the primary stabilizer of the DRUJ. It is anatomically bipartite, functioning partly as a meniscus to allow compressive load transfer while accommodating the relative shortening of the radius during pronation, and partly as a robust ligamentous restraint. The TFCC is characterized by its palmar and dorsal fibrous thickenings, designated as the palmar radioulnar ligament (PRUL) and dorsal radioulnar ligament (DRUL). These ligaments originate from the distal palmar and dorsal rims of the sigmoid notch of the radius as distinct, separable bundles.

The ulnar insertions of the PRUL and DRUL are biomechanically critical. They possess superficial fibers that attach to the base of the ulnar styloid and deep fibers that intricately criss-cross to form a complex weave, ultimately inserting into the foveal fossa of the distal ulna, adjacent to the articular cartilage of the ulnar head. This foveal attachment represents the true isometric center of rotation for the DRUJ. During forearm rotation, these deep interdigitating fibers create a "screw home" mechanism, functionally analogous to the cruciate ligaments of the knee. In pronation, the deep fibers of the DRUL are taut while the superficial fibers are lax; conversely, the superficial fibers of the PRUL are taut and its deep fibers are lax. The exact opposite tensioning pattern occurs in supination. Avulsion of this critical foveal attachment is a hallmark pathology in Galeazzi fracture-dislocations.
Osteology and Articular Kinematics
The ulnar head serves as the structural keystone of the DRUJ. It is slightly flattened distally where it interfaces with the articular disc of the TFCC, and rounded radially where it articulates with the sigmoid notch of the radius. The sigmoid notch itself is only mildly concave, presenting considerable osseous incongruity with the convexity of the ulnar head. This shallow bony architecture is functionally deepened by a horseshoe-shaped fibrocartilaginous labrum. A flimsy, inherently loose capsule attaches to this labrum, a necessary evolutionary adaptation to permit the nearly 180 degrees of pronosupination required for normal human forearm function. The capsule only becomes clinically relevant when it is pathologically thickened or scarred, resulting in debilitating rotational contractures.

During dynamic forearm rotation, a highly complex kinematic interaction unfolds between the radius and the ulna. From approximately 50 degrees of pronation to 50 degrees of supination, the radius undergoes nearly pure rotation around the stationary ulna, with the center of rotation passing directly through the fovea of the ulnar head. To facilitate this, the ulna subtly translates out of the path of the rotating radius via a 9-degree varus-valgus arc of motion occurring proximally at the elbow joint. However, at the extremes of rotation (beyond 50 degrees of pronation or supination), a distinct translational slide of the radius occurs on the ulna at the DRUJ. In full pronation, the radius slides volarly, rendering the ulnar head prominent dorsally; in full supination, the radius slides dorsally, making the ulnar head prominent volarly.

The Interosseous Membrane (IOM)
The distal aspect of the interosseous membrane acts synergistically with the TFCC as a primary stabilizer of the DRUJ. Experimental biomechanical sectioning studies have demonstrated that with an artificial osteotomy of the radius, up to 5 mm of proximal radial migration (shortening) can occur with an intact IOM. However, catastrophic radial shortening of greater than 10 mm simply cannot occur unless both the central band of the interosseous ligament and the triangular fibrocartilage are completely ruptured. This highlights the IOM's role in longitudinal load transfer and its critical contribution to preventing proximal migration of the radius in high-energy Galeazzi variants.
Exhaustive Indications and Contraindications
Garcia-Elias and Dobyns elegantly classified DRUJ dislocations into three distinct types, which dictates the surgical algorithm. Type I injuries are pure soft tissue dislocations without associated fractures. Type II injuries are intra-articular fracture-dislocations involving the joint surface of the sigmoid notch. Type III injuries represent extra-articular DRUJ fracture-dislocations, which are further subdivided. Type IIIa involves an abnormal joint surface orientation, usually associated with fractures of the distal two-thirds of the radius without complete longitudinal disruption of the forearm axis. Type IIIb involves a gross radioulnar length discrepancy with complete longitudinal disruption of the forearm, classically known as the Essex-Lopresti injury. In the context of this chapter, the term "Galeazzi fracture-dislocation" specifically refers to a Type IIIa extra-articular fracture of the distal radius with any degree of DRUJ soft-tissue disruption.
Surgical intervention is universally indicated for the radial shaft fracture in a Galeazzi injury. The indications for addressing the DRUJ depend entirely on the intraoperative assessment of joint stability after the radius has been anatomically reduced and rigidly plated. If the DRUJ remains subluxated, dislocated, or grossly unstable to manual stress testing (the Shuck test), operative stabilization of the DRUJ is absolutely indicated. Failure to recognize and treat DRUJ instability will result in chronic pain, severe limitation of pronosupination, and early post-traumatic arthrosis.
Contraindications to immediate operative intervention are relatively few but clinically significant. They include active, overwhelming local soft tissue infection, severe medical comorbidities rendering the patient unfit for anesthesia, or a polytraumatized patient in extremis where damage control orthopedics dictates temporary spanning external fixation rather than definitive internal fixation.
| Indication Category | Specific Clinical Scenario | Recommended Intervention |
|---|---|---|
| Absolute Indications | Displaced radius shaft fracture (Galeazzi) | ORIF of the radius with rigid plate fixation |
| Absolute Indications | Irreducible DRUJ post-radius fixation | Open reduction of DRUJ, removal of interposed tissue (ECU/capsule), TFCC repair |
| Relative Indications | DRUJ instability (Grade II/III) post-fixation | Closed reduction, percutaneous pinning in stable rotation, or direct foveal repair |
| Contraindications | Active volar/dorsal forearm infection | Temporary spanning external fixation, delayed ORIF |
| Contraindications | Medically unstable polytrauma patient | Damage control orthopedics, splinting/ex-fix |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and the Shuck Test
Patients with an acute Galeazzi fracture-dislocation present with severe, debilitating pain, exquisite tenderness over the radial diaphysis, and marked swelling. Motion of the forearm, wrist, and digits is typically entirely precluded by pain. A classic "caput ulna" deformity—a striking dorsal prominence of the distal ulna—is frequently observed due to the volar displacement of the radius relative to the ulnar head. It is vital to elicit the mechanism of injury; a fall from a height or a high-speed motor vehicle collision imparts significantly more kinetic energy than a ground-level fall, increasing the likelihood of extensive IOM tearing and profound DRUJ instability.
The initial emergency department evaluation must rigorously rule out acute carpal tunnel syndrome and forearm compartment syndrome. The fingers must be passively extended; severe pain on passive extension combined with a tense, woody forearm is the most reliable indicator of an impending compartment syndrome, necessitating emergent fasciotomy. Vascularity is assessed via radial and ulnar pulses and digital capillary refill. A sensory examination utilizing static two-point discrimination is mandatory to evaluate the median, ulnar, and superficial radial nerves.

Once the radius is stabilized intraoperatively, DRUJ laxity is formally assessed utilizing the "Shuck test." With the elbow flexed to 90 degrees, the head of the ulna is grasped with a chuck pinch grip, and the distal radius is held with a span grasp. The radius is stabilized while the ulna is translated in a palmar-dorsal direction. This is performed in neutral rotation, full pronation, and full supination, and must be compared to the contralateral uninjured wrist. At full rotation, the joint should be locked with no relative translation. In neutral rotation, the DRUJ ligaments are physiologically lax, and up to 1 cm of translation is considered normal.
Imaging Modalities
Standard orthogonal plain radiographs of the entire forearm, including the wrist and elbow joints, are the cornerstone of preoperative planning. These views allow for precise templating of the radius fracture. On the posteroanterior (PA) view of the wrist, ulnar variance is scrutinized. Less than 5 mm of positive ulnar variance suggests the TFCC may be intact, whereas greater than 1 cm of positive variance is pathognomonic for complete interosseous membrane disruption.

Mino et al. described a highly reliable technique for evaluating DRUJ subluxation on the true lateral wrist radiograph. The radial styloid must be perfectly aligned with the center of the lunate. In a normal joint, the head of the ulna should be completely obscured by the radius. If the ulnar head is partially visible, subluxation is present; if it is completely unobscured, the joint is frankly dislocated.

Advanced imaging, particularly Computed Tomography (CT), is invaluable for quantifying the precise degree of subluxation, especially in chronic or delayed presentations. The "Radioulnar Ratio" is the most validated method for interpreting axial CT cuts. The center of the ulnar head is determined using concentric circles. A line (A-B) is drawn connecting the dorsal and volar margins of the sigmoid notch. A perpendicular line (C) is drawn from line A-B to the center of the ulnar head. The ratio of the distance from the volar sigmoid margin to the perpendicular intersection (AD) over the total sigmoid length (AB) yields the radioulnar ratio. Normal values are tightly clustered: 0.50–0.71 in pronation, 0.42–0.58 in neutral, and 0.19–0.55 in supination. Magnetic Resonance Imaging (MRI) is exquisitely sensitive for identifying foveal avulsions of the TFCC and tears of the extensor carpi ulnaris (ECU) subsheath.
Patient positioning involves placing the patient supine on the operating table with a radiolucent hand table extension. A well-padded proximal arm tourniquet is applied. The fluoroscopy (C-arm) unit is positioned either parallel or perpendicular to the hand table, ensuring unimpeded access for both PA and lateral imaging throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
Anatomic Reduction of the Radius
The absolute prerequisite for managing the DRUJ in a Galeazzi injury is the perfect anatomic restoration of the radius. The fracture is typically approached via a volar Henry approach, exploiting the internervous plane between the flexor carpi radialis (median nerve) and the brachioradialis (radial nerve). Alternatively, a dorsal Thompson approach can be utilized for middle-third fractures. The fracture ends are meticulously debrided of hematoma and interposed periosteum.
Rigid internal fixation is achieved using a 3.5 mm dynamic compression plate (DCP) or locking compression plate (LCP). At least six cortices of purchase (three screws) are required both proximal and distal to the fracture site. The surgeon must pay obsessive attention to restoring the native radial bow; failure to recreate the precise coronal and sagittal contours of the radius will result in a mechanical block to pronosupination and obligate DRUJ incongruity.

Intraoperative DRUJ Assessment and Management Algorithm
Following definitive fixation of the radius, the tourniquet is deflated, hemostasis is achieved, and the DRUJ is interrogated. Fluoroscopic images are obtained in neutral rotation to confirm concentric reduction. The Shuck test is then performed and graded to dictate subsequent management:
- Grade I (Stable): Less than 0.5 cm of motion at the extremes of rotation with a firm endpoint. This indicates probable intrasubstance stretching of the radioulnar ligaments without complete avulsion. Management consists of immobilization in a long-arm cast in neutral rotation for 4 weeks.
- Grade II (Subluxatable): Greater than 0.5 cm of motion at extremes with a soft, indistinct endpoint, but no frank dislocation. This is highly correlated with a foveal avulsion of the TFCC without rupture of the distal IOM. The joint is typically stable in either mid-pronation or mid-supination. Management involves casting in the stable position, or increasingly, arthroscopic or open direct repair of the foveal avulsion.
- Grade III (Dislocatable): The joint is concentrically reduced at rest but frankly dislocates upon stress at the extremes of rotation. This implies rupture of both the TFCC and the distal aspect of the interosseous membrane. Management requires anatomic repair of the foveal avulsion and supplementary trans-articular pinning of the DRUJ in mid-supination.
- Grade IV (Irreducible): The joint remains dislocated despite anatomic radius fixation and exhibits a "mushy" feeling upon attempted reduction. This is the classic complex Galeazzi variant described by Alexander and Lichtman. The irreducibility is caused by soft tissue interposition—most commonly the ECU tendon, the ECU subsheath, folded capsular flaps, or osteochondral fragments from the sigmoid notch. This mandates immediate open reduction.

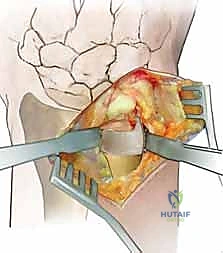
Open Reduction and TFCC Repair
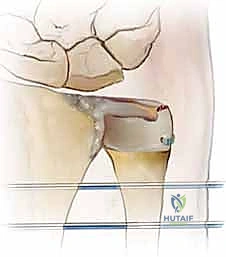
When open reduction is indicated, a dorsal longitudinal incision is made over the DRUJ, centered over the 5th extensor compartment. The extensor digiti minimi (EDM) is identified and retracted radially. The dorsal capsule of the DRUJ is incised longitudinally, creating thick capsular flaps for later repair.

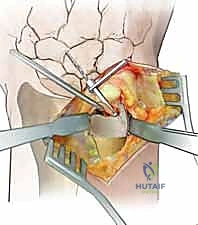
The joint is inspected, and any interposed structures (such as a subluxated ECU tendon) are extricated. The foveal footprint at the base of the ulnar styloid is meticulously debrided to bleeding cancellous bone using a curette or a motorized burr to promote a robust healing response.

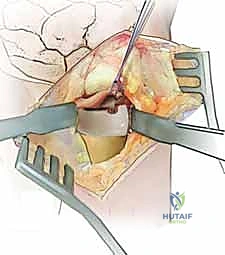
The avulsed deep fibers of the TFCC are identified. Repair is most reliably achieved using a bony anchor or transosseous suture tunnels. A 1.5 mm or 2.0 mm suture anchor double-loaded with high-strength non-absorbable suture is driven directly into the anatomic fovea.
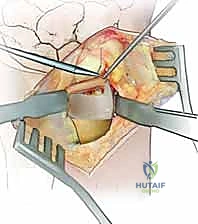
The sutures are passed through the deep radioulnar ligaments of the TFCC using a horizontal mattress configuration. The knot is tied with the forearm held in neutral rotation, firmly apposing the TFCC to the foveal footprint.
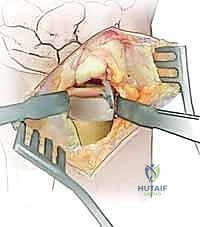
If the joint remains tenuously stable despite repair, or in cases of severe Grade III instability, the DRUJ is pinned. The forearm is placed in the position of maximum stability (usually supination for dorsal instability). Two 0.062-inch Kirschner wires are driven from the ulnar shaft, proximal to the ulnar head articular surface, transversely across the interosseous space into the radius, engaging four cortices. The pins are left protruding through the skin, bent, and capped for easy removal in the clinic.