Full Question & Answer Text (for Search Engines)
Question 1:
Which of the following groups is not at increased risk for community- acquired methicillin-resistant Staphylococcus aureus (C AMRSA):
Options:
- Athletes who participate in physical contact sports
- Patients who have had recent antibiotics
- People traveling abroad
- People living in crowded conditions
- Prison inmates
Correct Answer: People traveling abroad
Explanation:
People traveling abroad are not considered at increased risk for C A-MRSA. Athletes who participate in physical contact sports, patients who have had recent antibiotics, people living in crowded conditions, and prison inmates are considered at increased risk for C A-MRSA.
Question 2:
Which of the following toxins is responsible for the virulence of community- acquired methicillin-resistant Staphylococcus aureus (C A-MRSA):
Options:
- Beta-lactam
- Panton-Valentine leukocidin
- Oxazolidine
- mecA
- Streptolysin
Correct Answer: Panton-Valentine leukocidin
Explanation:
Panton-Valentine leukocidin is a toxin that produces necrosis of tissue and white blood cells. This toxin is much more common in CA-MRSA than in hospital-acquired MRSA.
Question 3:
A 5-year-old girl presents to the emergency department with pain in her hip. Her temperature is 102° F, pulse is 96, and blood pressure is 104/60. Magnetic resonance imaging reveals edema in the obturator muscles. Blood cultures are negative. Ultrasound-guided aspiration reveals no abscess, but fluid obtained grows methicillin-resistant Staphylococcus aureus (MRSA). In addition to antibiotic treatment, what other treatment option is recommended:
Options:
- Surgical irrigation and debridement
- Indwelling catheter drainage
- Repeated aspiration with ultrasound guidance
- Observation
- Spica cast application
Correct Answer: Observation
Explanation:
This patient has community-acquired MRSA but does not have an evident fluid collection. There is no evidence of systemic infection or necrotizing fasciitis. There is no indication for drainage or debridement of any type. Therefore, antibiotics alone with clinical observation are indicated.
Question 4:
A 5-year-old girl who presents to the emergency department has obturator muscle infection without abscess formation, which is seen on magnetic resonance imaging. She has no clinical evidence of sepsis. Aspiration yields methicillin-resistant Staphylococcus aureus (MRSA). Which of the following antibiotics is recommended:
Options:
- Vancomycin
- C lindamycin
- Rifampin
- Tetracycline
- Linezolid
Correct Answer: C lindamycin
Explanation:
To treat this patient, clindamycin is the drug of choice. Vancomycin is not recommended for uncomplicated MRSA in the nonseptic patient. Rifampin is not recommended to be used alone because of the rapid development of resistance. Tetracycline is not recommended for children under 8 years old because it causes permanent staining of the teeth. Linezolid is to be used only after infectious disease consultation because of its toxicity (thrombocytopenia in 3.5% of patients) and expense. Another option for this patient would be trimetoprim/sulfamethoxazole.
Question 5:
A nonverbal 12-year-old patient with totally involved cerebral palsy and developmental delay has been in pain for the past week. The source of the pain cannot be localized. Pelvis radiographs and urinalysis are unremarkable. The next recommended study is:
Options:
- Ultrasound of the hips
- Magnetic resonance imaging (MRI) of the brain
- Whole-body bone scan
- Computed tomography (C T) of the lumbar spine
- Thermography
Correct Answer: Whole-body bone scan
Explanation:
In a nonverbal child with longstanding pain, the whole-body bone scan is the most sensitive and specific test. Whole-body bone scans detected a cause of pain in more than half of such children in one study; most causes of pain were fractures. MRI cannot be focused enough, and C T has the same limitation as well as increased radiation exposure. Thermography is not widely available and has not been studied in children with cerebral palsy.
Question 6:
A 2-month-old infant has a midshaft humeral fracture. The fracture has 45° angulation with an anterolateral apex and is 6 mm short. Recommended treatment includes:
Options:
- Immobilizing the arm against the torso
- A shoulder abduction cast
- Percutaneous pin fixation
- Plate fixation
- External fixation
Correct Answer: Immobilizing the arm against the torso
Explanation:
The humerus has unlimited remodeling potential at this age. The goal of treatment is pain relief. Immobilization against the torso is the most practical method of treatment.
Question 7:
A 23-month-old patient demonstrates intoeing. He walked at 21 months. His height is in the 3rd quantile, and he is cognitively normal. Possible diagnoses include all of the following except:
Options:
- Osteogenesis imperfecta
- Rickets
- Internal tibial torsion
- Achondroplasia
- Metaphyseal chondrodysplasia
Correct Answer: Internal tibial torsion
Explanation:
The upper limit of normal age for onset of walking is 18 months. All of the diagnoses, except for internal tibial torsion, may explain the delayed walking, short stature, and intoeing.
Question 8:
The most common form of rickets in the United States is:
Options:
- Nutritional deficiency of calcium
- Hypophosphatasia
- Vitamin D-dependent rickets (1-alpha-hydroxylase deficiency)
- Fanconi syndrome
- X-linked hypophosphatemic rickets
Correct Answer: Hypophosphatasia
Explanation:
Although rickets due to deficiency of vitamin D is common due to inadequate sunlight or prolonged breast feeding, nutritional deficiency of calcium is uncommon in the US. The most common cause of rickets in the US is X-linked hypophosphatemic rickets. Hypophosphatasia, caused by alkaline phosphatase deficiency, is a rare recessive condition. Fanconi syndrome is a failure of tubular reabsorption of small molecules and resembles X-linked hypophosphatemic rickets, although it is more rare. Vitamin Ddependent rickets is also rare.
Question 9:
The gene most likely to be associated with inherited rickets is:
Options:
- PHEX
- FGF23
- SLC 34A3
- EXT1
- C OL1A1
Correct Answer: PHEX
Explanation:
PHEX is a gene whose product regulates transport of renal phosphates that leads to isolated renal phosphate wasting and consequent hypophosphatemia. This is the syndrome known as X-linked hypophosphatemic rickets, which is the most common cause of inherited rickets.
Question 10:
Genetic testing performed for a patient reveals a defect in PHEX. The family history provided by the patient is most likely to include:
Options:
- An affected father and son in the family
- More females relatives affected than male relatives
- A negative family history for the disorder
- An equal number of affected male relatives and females relatives
- Affected siblings but no prior ancestors or relatives
Correct Answer: More females relatives affected than male relatives
Explanation:
PHEX is the gene for a product that regulates renal tubular phosphate reabsorption. A defect in this gene causes X-linked hypophosphatemic rickets, which is the most common inherited rickets. It is an X-linked dominant condition; therefore, male-tomale transmission cannot occur. An excess of affected female relatives to male relatives is approximately 2:1. Spontaneous mutation can occur but is less common than inheritance of the disorder.
Question 11:
A toddler with bowing is suspected of X-linked hypophosphatemic rickets (XLH). The most likely laboratory abnormalities will include:
Options:
- Low alkaline phosphatase
- High PO4
- Low calcium
- Low 25-(OH)2D3
- Low 1,25-(OH)2D3
Correct Answer: Low 1,25-(OH)2D3
Explanation:
The most common laboratory abnormalities in XLH include high alkaline phosphatase (in attempt to mobilize phosphate from the bone); low serum phosphate; normal calcium and 25-(OH)2D3; and low 1,25-(OH)2D3, presumably due to defective renal hydroxylation.
Question 12:
An 18-month-old patient is suspected of X-linked hypophosphatemic rickets. The clinical findings are most likely to include all of the following except:
Options:
- Below average stature
- Exaggerated genu varus
- Dental abscesses or caries
- Delayed motor milestones
- Alopecia
Correct Answer: Alopecia
Explanation:
Patients with X-linked hypophosphatemic rickets may present with below average stature, exaggerated genu varus, dental abscesses or caries, and delayed motor milestones. Alopecia is not common in patients with this condition but is characteristic of the rare condition of end-organ insensitivity to vitamin D (vitamin D-resistant rickets).
Question 13:
A newborn is brought in for consultation due to a foot deformity. The left foot is dorsiflexed at the ankle, and the dorsum of the foot is able to be placed against the tibia. Neurologic and vascular examination is normal. Recommended treatment includes:
Options:
- Magnetic resonance imaging for completion of diagnosis
- Serial casting
- Observation
- Ankle-foot orthosis
- Lengthening of the anterior tibialis tendon
Correct Answer: Observation
Explanation:
The newborn is presenting with a calcaneovalgus foot. This condition resolves spontaneously, therefore, no additional work-up is needed.
Question 14:
In a newborn, how much angulation is acceptable in a fracture of the humeral diaphysis:
Options:
Correct Answer: 50°
Explanation:
In the humeral diaphysis of a newborn, one can accept virtually any alignment because of the tremendous remodeling capacity of the child. Complete remodeling of 66° within 1 year has been documented.
Question 15:
Which of the following radiographic parameters remains essentially fixed throughout life:
Options:
- Pelvic tilt
- Sacral slope
- Pelvic incidence
- T1 tilt
- Lumbar lordosis
Correct Answer: Pelvic incidence
Explanation:
Pelvic incidence is a measure of the relationship between the superior sacral endplate and the hips. It does not change significantly during life unless there is a major pelvic fracture. Pelvic incidence is defined as the angle between a line connecting the hip center and the midpoint of the S1 endplate, and a perpendicular to the midpoint of the S1 endplate. This angle is fixed in bone. By contrast, all of the other angles vary with posture and age.
Question 16:
A 6-year-old boy presents with a linear area of swelling in the region of the posterior paraspinous muscles. He has no history of weight loss or fevers. He also has bilateral great toe deformities consisting of valgus and shortening. The most likely diagnosis is:
Options:
- Multiple hereditary exostoses
- Ewingâ s sarcoma
- Osteosarcoma
- Fibrodysplasia ossificans progressiva
- Synovial sarcoma
Correct Answer: Fibrodysplasia ossificans progressiva
Explanation:
Fibrodysplasia ossificans progressiva is characterized by linear swelling and progressive ossification from a posterior-central origin. Patients also have a characteristic shortened and valgus great toe. The natural history of this disorder is one of progressive ossification, and it eventually impairs nutrition.
Question 17:
Based on the presented radiographs (Slide 1, Slide 2), what is the proper diagnosis of this 12-month-old female patient:
Options:
- Normal study
- Avascular necrosis of the femoral head
- Developmental coxa vara of the right femur
- Physeal fracture
- Osteogenesis imperfecta
Correct Answer: Physeal fracture
Explanation:
This patient had a physeal fracture of the right proximal femur, which was the result of a non-accidental injury. Notice the displacement of the right femoral metaphysic anteriorly on the frog view despite comparable degrees of rotation. A metaphyseal calcification is apparent posterior to the femoral neck. Treatment involved spica cast application.
Question 18:
A 23-month-old patient is evaluated for intoeing. Based on his radiograph (Slide), what is the most likely diagnosis:
Options:
- Osteogenesis imperfecta
- Tibial torsion
- Physiologic bowing
- Rickets
- Fibrous dysplasia
Correct Answer: Rickets
Explanation:
This patient has rickets. Note the diffuse osteopenia, â grainy nature, thinning of the tibial and femoral diaphyseal cortex, varus of both the proximal and distal tibial metaphyses, and widened and irregular physes at all levels.
Question 19:
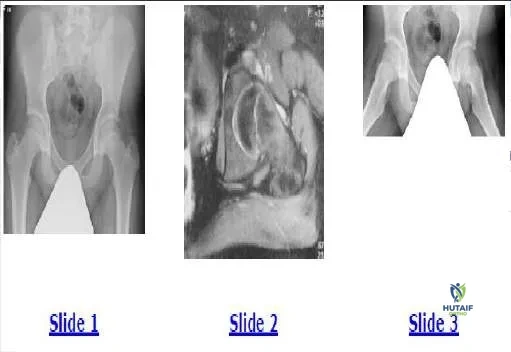
A 13-year-old boy has been experiencing hip pain for 1 month. The pain is worse with activity. The patient has no history of fever or weight loss, and both of his hips flex to 90°. Based on his radiograph (Slide 1) and magnetic resonance image (Slide 2), which of the following is the most likely diagnosis:
Options:
- Leukemia
- Pincer-type impingement
- Psoas tendonitis
- Slipped epiphysis
- Avascular necrosis
Correct Answer: Slipped epiphysis
Explanation:
This patient has a subtle grade 1 slipped capital femoral epiphysis. He is a male Risser 0 and is overweight. He has decreased internal rotation of the involved hip in flexion. The plain pelvis radiograph shows slightly less epiphyseal height on the left side, slight posterior metaphyseal overlap, and increased irregularity of the physis. MRI confirms a lucent plane in the physis and surrounding edema. A plain film (Slide 3) confirms the diagnosis. In situ fixation was performed on this patient.
Question 20:
A 13-year-old boy has been experiencing hip pain for 1 month. The pain is worse with activity. The patient has no history of fever or weight loss, and both of his hips flex to 90°. , which of the following is the most likely diagnosis:
Options:
- Leukemia
- Pincer-type impingement
- Psoas tendonitis
- Slipped epiphysis
- Avascular necrosis
Correct Answer: Slipped epiphysis
Explanation:
This patient has a subtle grade 1 slipped capital femoral epiphysis. He is a male Risser 0 and is overweight. He has decreased internal rotation of the involved hip in flexion. The plain pelvis radiograph shows slightly less epiphyseal height on the left side, slight posterior metaphyseal overlap, and increased irregularity of the physis. MRI confirms a lucent plane in the physis and surrounding edema. A plain film (Slide 3) confirms the diagnosis. In situ fixation was performed on this patient.