Full Question & Answer Text (for Search Engines)
Question 1:
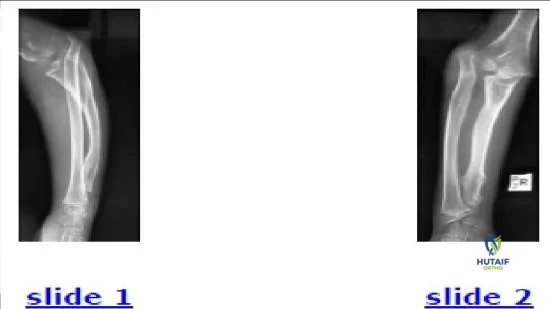
The parents of a 12-year-old boy notice an abnormal shape on their sonâ s forearm. He states that he does not feel any pain. Based on his radiograph (Slide), the most likely diagnosis is:
Options:
- Congenital dislocation of the radial head
- Unrecognized traumatic dislocation of the radial head
- Osteogenesis imperfecta
- Fibrous dysplasia
- Multiple exostoses
Correct Answer: Multiple exostoses
Explanation:
This patient has multiple exostoses. Multiple exostoses, which result from a mutation on one of three EXT genes, cause a growth disturbance of affected limb segments. This effect is most pronounced in the two-bone segments (forearm and lower leg). The bone with the exostoses grows less in length and often develops angulation. The less-affected bone often develops secondary deformity, such as the radial head dislocation in this patient. Fibrous dysplasia and osteogenesis imperfecta may lead to developmental dislocation of the radial head as well, but the associated bony changes allow correct diagnosis of each of these conditions.
Question 2:
The 9-year-old patient presented in the radiographs (Slide 1, Slide 2) should be diagnosed with:
Options:
- C ongenital dislocation of the radial head
- Unrecognized traumatic dislocation of the radial head
- Osteogenesis imperfecta
- Fibrous dysplasia
- Multiple exostoses
Correct Answer: Osteogenesis imperfecta
Explanation:
This patient has type V osteogenesis imperfecta, which is characterized by hereditary radial head dislocation in 86% of patients (this patients mother
and brother also have the condition bilaterally) as well as heterotopic calcification, osseous fragility, and scoliosis. Dislocation of the radial head occurs less often (0%-29%) in the other types of osteogenesis imperfecta and is linked to angular deformation of the long bones. The signs of osteogenesis imperfecta in this patient include thin long bones, several healed fractures, and angular deformations.
Question 3:
Which has a lower risk of compartment syndrome or delayed detection in a patient with a supracondylar fracture of the humerus:
Options:
- Median nerve injury
- Flexion greater than 110°
- Ipsilateral forearm fracture
- Ecchymosis or severe swelling
- Flexion-type mechanism of the fracture
Correct Answer: Flexion-type mechanism of the fracture
Explanation:
Median nerve injury increases the risk of delayed detection of the fracture because of the lack of sensation in the volar compartment and also increases risk of injury to the adjacent brachial artery. Flexion greater than 110° increases forearm pressures by compromising arterial inflow and venous return. An ipsilateral forearm fracture is associated with increased risk of compartment syndrome (7% with ipsilateral forearm fracture vs 0.3%without ipsilateral forearm fracture). Severe ecchymosis and swelling are also associated with an increased risk of compartment syndrome, even in the presence of a radial pulse. A flexiontype supracondylar fracture, by contrast, has a lower risk of compartment syndrome because of the lack of stretch or tension on the critical vascular structures.
Question 4:
In a lateral radiograph of a childâ s elbow, the anterior humeral line should be located:
Options:
- Anterior to the capitellum
- In the anterior one-third of the capitellum
- In the middle-third of the capitellum
- In the posterior-third of the capitellum
- Posterior to the capitellum
Correct Answer: In the middle-third of the capitellum
Explanation:
In a childs elbow, the anterior humeral line should be located in the middle- third of the capitellum.
Question 5:
A 3-year-old boy falls on his upper extremity and shows sign of pain. His radiograph only shows a posterior fat pad sign of the elbow. What is the most likely diagnosis:
Options:
- Nursemaid elbow
- Elbow sprain
- Supracondylar humerus fracture
- Proximal ulna fracture
- Lateral condyle fracture
Correct Answer: Supracondylar humerus fracture
Explanation:
A positive posterior fat pad sign is more suspicious for occult fracture than an anterior fat pad sign because flexing the elbow normally may elevate the anterior but not the posterior fat pad. A positive posterior fat pad sign is most likely to represent an undisplaced supracondylar fracture of the distal humerus, followed by proximal ulna, lateral conydle, and radial neck fracture. A nursemaid elbow is a diagnosis of exclusion and should be used only when the mechanism is one of traction rather than compression.
Question 6:
Which of the following is not an indication to urgently treat a supracondylar humerus fracture:
Options:
- Antecubital ecchymosis
- Firm compartments
- Associated forearm fracture
- Poor perfusion
- Medial comminution
Correct Answer: Medial comminution
Explanation:
Medial comminution is an indication of potential bony instability but does not convey any increased vascular risk. All of the other indications convey a vascular risk, and treatment should not be delayed.
Question 7:
The lung attains half of its adult volume at what age:
Options:
- 2 years
- 4 years
- 6 years
- 8 years
- 10 years
Correct Answer: 8 years
Explanation:
The lung attains 30% of its adult volume at 4 years and 50% at 8 years.
Question 8:
Which of the following conditions is not associated with an increased risk of cavus foot:
Options:
- Freidreich ataxia
- Spina bifida
- C harcot-Marie-Tooth disease
- Tethered cord
- C alcaneonavicular coalition
Correct Answer: C alcaneonavicular coalition
Explanation:
Calcaneonavicular coalition is typically associated with a planovalgus foot. Freidreich ataxia, spina bifida, Charcot-Marie-Tooth disease, and tethered cord are often associated with a cavus foot.
Question 9:
Which of the following factors has not been proven to increase the risk of thermal necrosis to a limb with a cast:
Options:
- Use of plaster
- Use of fiberglass
- Folding a splint into double-thickness
- Placing a recently casted limb on a pillow
- Using a dip water temperature more than 30°
Correct Answer: Use of fiberglass
Explanation:
Fiberglass is less likely than plaster to produce thermal injury, likely because of the increased porosity. All of the other factors listed increase the risk of thermal necrosis.
Question 10:
Which shape of the olecranon apophysis correlates most closely with closure of the triradiate cartilage of the hips:
Options:
- Formation of initial ossification center
- Initial appearance of two ossification centers
- Formation of a curved single ossification center
- Formation of a rectangular ossification center
- Closure of the olecranon ossification center
Correct Answer: Formation of initial ossification center
Explanation:
The olecranon ossifies from two centers that merge and form one banana- shaped ossification center. When the ossificaiton center is rectangular in shape, it correlates with closure of the triradiate cartilage of the pelvis.
Question 11:
A 15-year-old female patient undergoes spine fusion from T2 to the pelvis for scoliosis associated with cerebral palsy. Her past medical history is remarkable for seizure disorder, ventriculoperitoneal shunt, baclofen pump, and gastrostomy tube. Her postoperative course is complicated by disorientation and visual hallucinations on postoperative day 3, whereas she had been communicative preoperatively. The most likely cause of this change is:
Options:
- Seizure activity
- Postoperative anemia
- Sepsis
- Baclofen withdrawal syndrome
- Hydrocephalus
Correct Answer: Seizure activity
Explanation:
This patient most likely has baclofen withdrawal due to interference with the catheter at some point along its path to the thecal sac. Baclofen withdrawal is characterized by increased spasticity, pruritus, hyperthermia, delusions, and hallucination. The pump reservoir should be checked, and a leak may be confirmed by filling the reservoir with a radionuclide and performing a scan. Treatment involves repleting baclofen by oral or intrathecal means and fixing the leak.Correct Answer: Baclofen withdrawal syndrome
Question 12:
A 5-year-old patient with Legg-Calva-Perthes disease has lateral pillar B involvement. He has 15% epiphyseal extrusion. Treatment should consist of:
Options:
- Observation
- Femoral osteotomy
- Iliac osteotomy
- C ombined femoral and iliac osteotomy
- External fixation
Correct Answer: Observation
Explanation:
Patients who have Legg-C alvé-Perthes disease with onset before 6 years of age have a good prognosis unless they have lateral pillar involvement in the B/C border or C categories.
Question 13:
Which of the following characteristics is more commonly found in patients with Meyer dysplasia than in patients with Legg- C alvé-Perthes disease:
Options:
- Bilateral involvement
- Asynchronous onset
- Metaphyseal widening
- Epiphyseal extrusion
- Later degenerative change
Correct Answer: Bilateral involvement
Explanation:
Meyer dysplasia is a rare condition that affects children before age 4. A characteristic of the condition includes delayed ossification of the epiphyses, which eventually develop normal ossification. Meyer dysplasia is synchronous, meaning that both heads have symmetrical involvement unlike Legg-C alvÃ-Perthes disease. Meyer dysplasia is usually bilateral, in contrast to Legg-C alvÃ- Perthes disease, which is bilateral in fewer than 10% of patients. There is no metaphyseal widening and no treatment is indicated.
Question 14:
A 10-year-old girl is seen for limb-length inequality. She has 10° of valgus of the left knee and a shortened left fibula. Her projected shortening at maturity is 1 cm in the left femur and 2.1 cm in the left tibia. Her left foot is normal in shape but one-half size smaller than the right. Her overall height and maturity are at the median for her age. For this patient, recommended treatment for limb-length inequality is:
Options:
- Observation
- Epiphysiodesis of the left tibia
- Epiphysiodesis of the right tibia
- Shortening of the right tibia
- Lengthening of the left tibia
Correct Answer: Epiphysiodesis of the left tibia
Explanation:
This patient has a projected discrepancy at maturity of 3.1 cm. Most experts agree that the risk of later gait disturbance or back pain is increased above a normal threshold when limb length inequality exceeds 2.5 cm. A shoe lift is noninvasive but not likely to be permanently adopted. Epiphysiodesis of the right tibia is the least invasive and least complicated option for permanent equalization and should be performed in this patient. Shortening of the right tibia would be an option if the patient desired correction after skeletal maturity, but is a more invasive procedure with risk of compartment syndrome, nonunion, and pain. Lengthening of the left tibia is a valid option, which could also allow correction of the valgus and maintenance of stature. However, the procedure leaves scars and complications are more significant. Most surgeons would not think that it is worthwhile for gain of an inch because a left tibial hemiepiphysiodesis could easily correct the valgus.
Question 15:
Which of the following is an accurate mean age for a motor milestone:
Options:
- Sit up without assistance at 6 months
- Walk independently at 24 months
- Hop on one foot at 2 years
- Roll from prone to supine position at 2 months
- Able to run at 36 months
Correct Answer: Sit up without assistance at 6 months
Explanation:
Motor milestones provide a way of assessing a childs motor development. If they are not met, a physician or parent may be more alert for neurological or connective tissue disorders. Common pediatric milestone include: Sit up without assistance at 6 months Walk independently at 12 months Hop on one foot at 4 years Roll from prone to supine position at 4 months Able to run at 18 months
Question 16:
In the workup of scoliosis, what is/are the best method(s) to assess skeletal maturity during a patients peak height velocity (Risser grade 0):
Options:
- Greulich and Pyle atlas (hand/wrist radiographs)
- Modified Sauvegrain method (olecranon radiographs)
- Tanner-Whitehouse-III RUS (radius, ulna, small bones of hand) method
- Triradiate cartilage closure
- B, C , and D
Correct Answer: B, C , and D
Explanation:
Precise information about skeletal maturity during peak growth rate is important in deciding treatment options in patients with scoliosis. The modified Sauvegrain method, Tanner-Whitehouse-III RUS method, and triradiate cartilage closure are each accurate and reliable markers of maturity that the orthopedic surgeon can use to quickly assess pediatric patients.
Question 17:
Following triple arthrodesis, total ankle range of motion is:
Options:
- Not affected because the tibiotalar joint is not fused in a triple arthrodesis
- Is increased because it must compensate for the loss of motion through the hindfoot joints
- Is increased in plantarflexion only; dorsiflexion is unchanged
- Is decreased in both dorsiflexion and plantarflexion
- Is decreased in plantarflexion only; dorsiflexion is unchanged
Correct Answer: Is decreased in both dorsiflexion and plantarflexion
Explanation:
Total ankle motion is a combination of tibiotalar motion as well as motion in the hindfoot joints. A 10-year follow-up study by Smith and colleagues evaluated the change in range of motion following triple arthrodesis. The authors found a 27% loss of ankle plantarflexion following triple arthrodesis, but no loss of dorsiflexion. Despite this loss of motion, 93% of patients were satisfied at average 10-year follow-up.
Question 18:
Three years ago, a 20-year-old female patient underwent posterior spinal fusion for adolescent idiopathic scoliosis. She asks what would happen if the implants were removed. The surgeons most likely response will be:
Options:
- The spine will not change alignment, if the fusion is solid.
- The sagittal alignment will likely change, even if the fusion is solid.
- The scoliosis is likely to increase, even if the fusion is solid.
- Fracture of the fusion mass is likely.
- Increased back pain is likely.
Correct Answer: The sagittal alignment will likely change, even if the fusion is solid.
Explanation:
After removal of implants, the sagittal alignment is likely to change, with kyphosis increasing by 10º in nearly half of all patients and by more than 20º in 10% of patients. By contrast, scoliosis increases significantly in only 5% of patients. Most patients who have implants removed experience an improvement in symptoms. Fracture of the fusion mass is rare.
Question 19:
Which of the following factors best predicts the risk of disk degeneration in young adults:
Options:
- Smoking history
- Occupational exposure
- Gender
- Family history
- Participation in sports
Correct Answer: Family history
Explanation:
Genetic factors are most predictive of disk degeneration. However, various genes have been identified as possible causative factors, possibly operating in different ways and interacting with environmental and other factors.
Question 20:
Which of the following treatments decreases hip subluxation in patients with cerebral palsy who have displaced hips:
Options:
- Passive stretching
- Hip abduction bracing
- Hip abduction bracing and botulinum toxin type A
- Electrical stimulation of the hip abductors
- Surgical adductor lengthening
Correct Answer: Surgical adductor lengthening
Explanation:
Only hip adductor lengthening has been shown to decrease hip subluxation in patients with displaced hips. Patients treated with botulinum toxin type A and hip abduction still result in progression.