Full Question & Answer Text (for Search Engines)
Question 1:
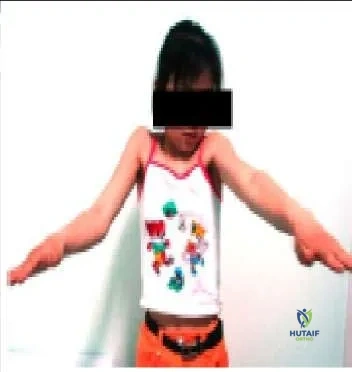
A 15-year-old girl is experiencing progressive weakness. She is unable to abduct her arms above 100° (pic). She has a progressive lordosis. Her facial expression is flat, and she cannot smile. Her mother has the same constellation of findings. No scoliosis is present. She and her mother are able to walk independently. The most likely diagnosis is:
Options:
- Parsonage-Turner syndrome
- Friedreich ataxia
- Facioscapulohumeral dystrophy
- Bells palsy
- Nemaline rod myopathy
Correct Answer: Facioscapulohumeral dystrophy
Explanation:
This patient most likely has facioscapulohumeral dystrophy. With a frequency of 1:20,000, it is a rare disorder inherited in an autosomal- dominant fashion. The genetic abnormality is found on chromosome 4, with a decreased number of D4Z4 tandem repeats, but this does not appear to code for a protein product. Scoliosis is not present. In this condition, selective weakness of the serratus anterior, trapezius, and rhomboid muscles is present. Therefore, the scapula is not effectively stabilized against the trunk during use.
Question 2:
A 10-year-old child, who has no history of fever, trauma, or infection, presents with minimal pain and a Trendelenburg gait on the left (Slide). Which of the following is the most likely diagnosis:
Options:
- Aneurysmal bone cyst
- Chronic osteomyelitis
- Fibrous dysplasia
- Unicameral bone cyst
- Enchondroma
Correct Answer: Fibrous dysplasia
Explanation:
This patient has fibrous dysplasia. The diffuse nature of the changes over a long portion of the bone, which includes blurring and thinning of the cortex, are classic signs of the disorder.
Question 3:
A patient who does not walk outdoors or independently but can walk with a walker in physical therapy is listed as what level according to the Gross Motor Function Measure (GMFM):
Options:
- Level 1
- Level 2
- Level 3
- Level 4
- Level 5
Correct Answer: Level 4
Explanation:
The GMF C lassification System (GMFC S) is a concise way of expressing overall motor ability. According to this system, level 1 is walking and running indoors and out with impaired speed, level 2 is impairment in running on uneven surfaces, level 3 is ambulation indoors and out with assistive devices, and level 4 is limited walking with a walker, and level 5 is nonambulatory.
Question 4:
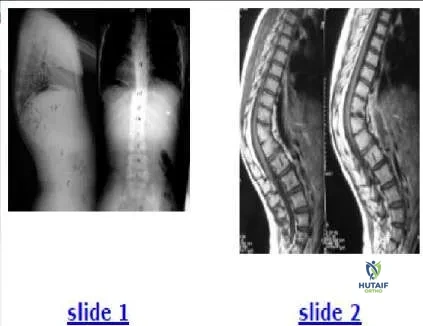
The patient shown in the clinical photograph (Slide 1) and radiograph (Slide 2) has which of the following conditions:
Options:
- Klippel-Trenaunay-Weber syndrome
- Neurofibromatosis-1
- Proteus syndrome
- Gorham disease
- Maffucci syndrome
Correct Answer: Klippel-Trenaunay-Weber syndrome
Explanation:
This patient has Klippel-Trenaunay-Weber syndrome. This syndrome is characterized by a triad of cutaneous nevi, varicose veins, and limb overgrowth in length and/or width.
Question 5:
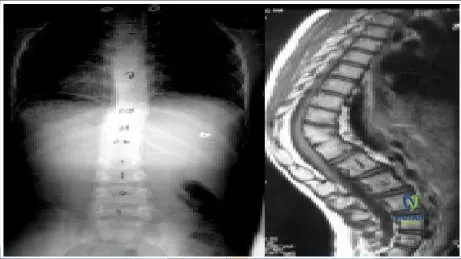
An 8-year-old girl with no history of fever, illness, or weakness presents with an increasing spinal deformity. She was born in Asia. The patient is neurologically normal. Based on radiographs (Slide 1) and magnetic resonance images (Slide 2), the most likely diagnosis is:
Options:
- Pyogenic spondylitis
- Tuberculous spondylitis
- C ompression fractures
- C ongenital kyphosis
- Scheuermann kyphosis
Correct Answer: C ongenital kyphosis
Explanation:
This patient has congenital kyphosis. The relative disk destruction with vertebral preservation argues against tuberculosis. The anterior bony wedging is atypical for remote bacterial infection. Anterior fusion is not seen in patients with Scheuermann kyphosis (rarely after maturity) or in patients with compression fractures.
Question 6:
An 8-year-old boy presents with progressive deformity. Recommended management includes:
Options:
- 3 months
- 6 months
- 9 months
- 12 months
- 24 months
Correct Answer: 24 months
Explanation:
This patient has a type II kyphosis (anterior bar). Because he is only 8 years old and the curve has progressed, further increase is likely. Observation is not indicated. Bracing has no influence on congenital curves. The kyphosis is >55° (78°) so a posterior fusion may not effectively halt the growth of these vertebral bodies in a posterior direction. Anterior and posterior fusion is the most likely procedure to control the curve.C orrect Answer: Anterior and posterior fusion 2291 A child with congenital below-elbow amputation is best fit with an active prosthesis at which age: A patient with congenital below-elbow amputation has sensation/proprioception in the limb and is able to perform most activities without assistance. Prostheses may interfere with crawling. Passive devices should not be started until walking begins, and active devices started at 2 to 4 years.
Question 7:
Which of the following is the most specific feature of congenital vertical talus that distinguishes it from other deformities:
Options:
- Hindfoot equinus
- Forefoot adduction
- Talonavicular dislocation
- Peroneal tightness
- Increased talonavicular angle
Correct Answer: Talonavicular dislocation
Explanation:
The essential lesion in congenital vertical talus is a dorsolateral dislocation of the talonavicular joint.
Question 8:
A 14-year-old boy sustains a hip dislocation in a motor vehicle accident. With closed reduction, he is at risk for all of the following except:
Options:
- Physeal separation
- Entrapped osteochondral fragment
- Degenerative joint disease
- Avascular necrosis
- Protrusio acetabulae
Correct Answer: Protrusio acetabulae
Explanation:
With a hip dislocation in a young adolescent, occult injury to the physis may occur. Reports of physeal separation during the reduction, as well as entrapped osteochondral fragments appear in the literature. Degenerative joint disease may eventually develop due to the cartilage injury. Avascular necrosis risk is approximately 10%.
Question 9:
A 12-year-old boy sustains a distal diaphyseal femur fracture with a large butterfly fragment. He weighs 110 lb. Which of the following treatments is most appropriate and best able to preserve alignment:
Options:
- Flexible intramedullary nails
- Immediate hip spica cast
- Submuscular plate fixation
- Retrograde nail
- Traction for 1 week followed by functional cast-brace
Correct Answer: Flexible intramedullary nails
Explanation:
A large butterfly fragment as well as the age and weight of the patient have been demonstrated to decrease the chances of success in treating children with femur fractures using flexible intramedullary nails. For similar reasons, the fracture is not suitable for an immediate spica or traction followed by functional bracing. The retrograde nail is not indicated due to open physis. Submuscular plate fixation is the best option.C orrect Answer: Submuscular plate fixation
Question 10:
Which of the following risks is associated with inserting a rigid femoral intramedullary nail through the piriformis fossa in a 10- to 14-year-old child:
Options:
- Obligatory varus deformity at the fracture
- Trochanteric overgrowth
- Avascular necrosis
- C hondrolysis
- Recurvatum
Correct Answer: Avascular necrosis
Explanation:
Avascular necrosis is a risk if a nail is inserted through the piriformis fossa in a patient younger than 15 years of age with open physes.
Question 11:
Which of the following is a description of a closed kinetic chain exercise:
Options:
- The distal ends of a limb are against fixed resistance
- The distal ends of a limb are free to travel in space
- The distal limb exerts force against an elastic chain
- The limb is suspended from a chain
- Two limbs move together
Correct Answer: The distal ends of a limb are against fixed resistance
Explanation:
A closed kinetic chain exercise is one in which the ends of a limb are fixed from free movement by resistance.
Question 12:
The action of bisphosphonates is primarily upon which component of bone:
Options:
- Osteoclast
- Osteoblasts
- Cartilage
- Periosteum
- Nutrient vessel
Correct Answer: Osteoclast
Explanation:
Bisphosphonates act to inhibit osteoclasts, thereby decreasing resorption and increasing bone mineral density in many conditions.
Question 13:
Which of the following is not a common finding in patients with Prader- Willi syndrome:
Options:
- Short stature
- Developmental delay
- Scoliosis
- Osteopenia
- Arachnodactyly
Correct Answer: Arachnodactyly
Explanation:
Prader-Willi syndrome is characterized by early hypotonia, short stature, severe obesity, developmental delay, scoliosis, and osteopenia.
Question 14:
Which of the following disease processes is demonstrated in the radiograph (Slide):
Options:
- Pigmented villonodular synovitis
- Slipped capital femoral epiphysis
- Developmental dysplasia of the hip
- Legg-C alve-Perthes disease
- Multiple epiphyseal dysplasia
Correct Answer: Legg-C alve-Perthes disease
Explanation:
The left femoral epiphysis shows avascular changes characteristic of Legg-C alve-Perthes disease without slippage. Although developmental dysplasia of the hip may also be complicated by avascular changes, the femoral neck and acetabulum would manifest more longstanding growth alterations as well. The contralateral hip would be symmetric in patients with multiple epiphyseal dysplasia.
Question 15:
Which of the following accurately describes this radiograph (Slide):
Options:
- Catterall 2
- Catterall 3
- Lateral pillar C
- Stulberg 3
- Salter-Thompson A
Correct Answer: Lateral pillar C
Explanation:
According to Herringâ s classification, this radiograph demonstrates a lateral pillar C because the lateral pillar is collapsed by more than 50%.
Question 16:
An 11-year-old girl presents with bilateral painful flatfeet. A computed tomography image is shown (Slide). The most likely diagnosis is:
Options:
- Idiopathic planovalgus feet
- Talocalcaneal coalition
- Degenerative joint disease
- Osteoid osteoma
- Osteochondritis dissecans
Correct Answer: Talocalcaneal coalition
Explanation:
This patient has evolving medial talocalcaneal facet coalition. The computed tomography is remarkable for obliquity of the medial facet, along with irregularity and narrowing of this facet, which is not evident on plain radiographs. Normally the medial subtalar facet should be parallel to the posterior facet. Treatment options for this patient include immobilization, resection, or subtalar fusion.
Question 17:
Which of the following is not a common feature of constriction band syndrome:
Options:
- Annular rings
- Fenestrated syndactyly
- Digital amputation
- Equinovarus foot
- Hip dislocation
Correct Answer: Hip dislocation
Explanation:
Constriction band syndrome is not commonly associated with developmental dislocation of the hip. However, annular rings, fenestrated syndactyly, digital amputation, and equinovarus foot are often seen in patients with constriction band syndrome.
Question 18:
An 8-year-old child presents with a mass on the posteromedial side of the popliteal fossa. The mass, which has been present for more than 1 month, is nontender and moderately soft. The knee examination is stable. No knee effusion is present, and the patient has no signs or symptoms of infection. Radiographs are normal. Which of the following is the next step to aid in diagnosis:
Options:
- Magnetic resonance imaging
- Bone scan
- C omputed tomography
- Transillumination
- Biopsy
Correct Answer: Transillumination
Explanation:
This patient demonstrates the classic presentation of a popliteal cyst. Transillumination often confirms the diagnosis of popliteal cyst, thereby avoiding the use of advanced imaging.
Question 19:
Which of the following features is not associated with congenital muscular torticollis:
Options:
- Developmental dysplasia of the hip
- Metatarsus adductus
- Flattening of the occiput contralateral to the tight sternomastoid
- Asymmetrical facial features
- Imperforate anus
Correct Answer: Imperforate anus
Explanation:
Congenital muscular torticollis is caused by in-utero molding, as are developmental dysplasia of the hip and metatarsus adductus. Contralateral occipital flattening and asymmetrical facial features develop secondarily with torticollis. Imperforate anus is associated with congenital hemivertebrae but not with muscular torticollis.
Question 20:
A 3-month-old female infant presents with the dorsum of the foot almost in contact with the anterior tibia. She has no pain with movement; plantar flexion and inversion of the feet are not restricted, but there is difficulty in manipulating the foot to the neutral position. She is normal otherwise. Which of the following treatments is most appropriate:
Options:
- Observation ± passive stretching
- Serial casting
- Botulinum toxin to peroneals
- Serial casting and then surgery
- Surgical reduction
Correct Answer: Observation ± passive stretching
Explanation:
This is a patient with positional calcaneovalgus, which is a more common condition than congenital vertical talus (C VT). Patients with such deformity should be evaluated carefully and differentiated from the more serious CVT. In calcaneovalgus foot, the problem is in the ankle, which is in calcaneus position. The arch itself may be normal. In C VT, the ankle is normal and the problem is in the foot. The foot is essentially plantigrade, but the arch is reversed. Typically, a deep crease in the sinus tarsi and some forefoot abduction are present. No difference was found between the calcaneovalgus feet that underwent manipulation and casting versus observation alone, when assessed at 3 to 11 years of follow-up. Surgery is never required for a positional calcaneovalgus deformity, which is not true for C VT. Long-term prognosis of positional calcaneovalgus is excellent.
 This patient most likely has facioscapulohumeral dystrophy. With a frequency of 1:20,000, it is a rare disorder inherited in an autosomal- dominant fashion. The genetic abnormality is found on chromosome 4, with a decreased number of D4Z4 tandem repeats, but this does not appear to code for a protein product. Scoliosis is not present. In this condition, selective weakness of the serratus anterior, trapezius, and rhomboid muscles is present. Therefore, the scapula is not effectively stabilized against the trunk during use.
This patient most likely has facioscapulohumeral dystrophy. With a frequency of 1:20,000, it is a rare disorder inherited in an autosomal- dominant fashion. The genetic abnormality is found on chromosome 4, with a decreased number of D4Z4 tandem repeats, but this does not appear to code for a protein product. Scoliosis is not present. In this condition, selective weakness of the serratus anterior, trapezius, and rhomboid muscles is present. Therefore, the scapula is not effectively stabilized against the trunk during use.
 This patient has Klippel-Trenaunay-Weber syndrome. This syndrome is characterized by a triad of cutaneous nevi, varicose veins, and limb overgrowth in length and/or width.
This patient has Klippel-Trenaunay-Weber syndrome. This syndrome is characterized by a triad of cutaneous nevi, varicose veins, and limb overgrowth in length and/or width.
 This patient has congenital kyphosis. The relative disk destruction with vertebral preservation argues against tuberculosis. The anterior bony wedging is atypical for remote bacterial infection. Anterior fusion is not seen in patients with Scheuermann kyphosis (rarely after maturity) or in patients with compression fractures.
This patient has congenital kyphosis. The relative disk destruction with vertebral preservation argues against tuberculosis. The anterior bony wedging is atypical for remote bacterial infection. Anterior fusion is not seen in patients with Scheuermann kyphosis (rarely after maturity) or in patients with compression fractures.




