Full Question & Answer Text (for Search Engines)
Question 1:
What is the mechanism of injury that leads to the clinical diagnosis of "turf toe":
Options:
- Forced lateral stress
- Forced medial stress
- Forced plantarflexion
- Forced compression of the first MTP
- Forced dorsiflexion
Correct Answer: Forced dorsiflexion
Explanation:
Turf toe is a sprain of the plantar capsuloligamentous complex of the first MTP joint that is associated with play on artificial playing surfaces. The classic mechanism of injury is a forced hyperextension injury to the 1st MTP joint. Dorsiflexion in excess of a normal range of motion can lead to varying degrees of soft tissue capsular disruption or injury to the articular cartilage and subchondral bone. Factors that predispose a player to injury are increasing age, number of years in professional football, pes planus, and decreased range of motion in the ankle and/or 1st MTP joint.
Question 2:
The gold standard for evaluation of chronic compartment syndrome in the athlete is:
Options:
- C linical examination
- Electromyogram post exercise
- Resting compartment measurements
- Elevated post exercises compartment pressures
- Elevated compartment pressures during exercise
Correct Answer: Elevated post exercises compartment pressures
Explanation:
The gold standard for diagnosing chronic or exertional compartment syndrome in the athlete is demonstration of elevated compartment pressures post exercise. Normal increases in compartment pressures with exercise will decrease to normal within 2 minutes of exercise cessation. Pedowitz et al has developed a criteria for diagnosis with any of the following: pre-exercise pressure > 15 mm Hg, 1 minute post exercise pressure > 30 mm Hg, or 5 min post exercise of > 20 mm Hg.
Question 3:
Internal impingement of the shoulder between the posterosuperior glenoid rim and the rotator cuff occurs in which phase of throwing:
Options:
- Wind-up
- Early cocking
- Late cocking
- Acceleration
- Follow-through
Correct Answer: Late cocking
Explanation:
Internal impingement of the shoulder occurs with the arm in the abducted, externally rotated, and extended position that corresponds with the late cocking phase of throwing. Internal impingement is responsible for shoulder pain commonly occurring in overhead and throwing athletes. Initial treatment is focused on therapy that strengthens the anterior structures, stretches the posterior structures, and controls the scapular position in space. If nonoperative treatment fails, arthroscopic debridement, thermal capsular shrinkage, and humeral derotational osteotomy have been used with varying degrees of success.
Question 4:
When comparing open distal clavicle resection with arthroscopic distal clavicle resection for osteolysis of the distal clavicle, arthroscopic techniques:
Options:
- Less reliably resect the appropriate amount of distal clavicle
- Less reliably provide pain relief
- Have a higher complication rate
- Result in a longer delay in return to sports
- Have no different outcomes
Correct Answer: Have no different outcomes
Explanation:
A study comparing arthroscopic and open techniques of distal clavicular resection in the treatment of osteolysis of the distal clavicle found no difference in the amount of bone resected or amount of pain relief obtained. The arthroscopic group had a shorter hospital stay and less complications, and returned to activity nearly twice as fast as the open technique group.7
Question 5:
A magnetic resonance image (MRI) of the dominant elbow of a 19-year-old minor league baseball pitcher is presented (pic). He has been unable to pitch for the past 6 weeks secondary to pain. The recommended treatment includes:
Options:
- Physical therapy for triceps strengthening
- Physical therapy for pronator strengthening
- Ulnar nerve transpostion
- Radial collateral ligament reconstruction
- Ulnar collateral ligament reconstruction
Correct Answer: Ulnar collateral ligament reconstruction
Explanation:
The MRI shows a disruption of the humeral attachment of the ulnar collateral ligament. The ulnar collateral ligament of the elbow is the most frequently observed ligamentous elbow injury in baseball pitchers. Recommended treatment in the throwing athlete is reconstruction of the ulnar collateral ligament with an autogenous palmaris longus graft.
Question 6:
Following acute lateral traumatic patellar dislocation, the surgical procedure that most closely reconstructs the injured structure is:
Options:
- Arthroscopic lateral release
- Vastus medialis obliquus advancement
- Medial patellofemoral ligament reconstruction
- Medial patellotibial ligament reconstruction
- Tibial tubercle transfer
Correct Answer: Medial patellofemoral ligament reconstruction
Explanation:
The medial patellofemoral ligament is the primary restraint to lateral subluxation of the patella. The other structures contribute less substantially to patellofemoral stability. In the majority of cases of acute traumatic patellar dislocation, the medial patellofemoral ligament is disrupted.
Question 7:
A 22-year-old male tennis player has dominant side shoulder pain when serving and hitting overheads. Despite a prolonged course of physiotherapy, he is unable to return to tennis because of shoulder pain. His treating physician recommend arthroscopy of his shoulder with debridement of associated lesions. What is the likelihood that he will be playing tennis at his preinjury level of competition at 1 year following surgery:
Options:
Correct Answer: 50%
Explanation:
This patient has internal impingement of the shoulder, presumably with associated labral and rotator cuff lesions. Sonnery-Cottet and colleagues reported results of 28 tennis players with internal impingement treated with arthroscopic debridement of associated lesions. Although 22 of the 28 tennis players were able to return to tennis following surgery, only 14 of the players were able to return to their preinjury level of competition.
Question 8:
A glenoid profile radiograph (Slide) of a 21-year-old male rugby player with multiple traumatic anterior shoulder dislocations is presented. Which of the following is the preferred treatment:
Options:
- Sling for a period of 6 weeks
- Physiotherapy emphasizing strengthening of dynamic shoulder stabilizers
- C apsular shift
- Bankart reconstruction
- Bony augmentation procedure(iliac crest)
Correct Answer: Bony augmentation procedure(iliac crest)
Explanation:
The radiograph demonstrates anterior glenoid rim insufficiency, which is a risk factor for failure of soft tissue reconstructions especially in contact athletes. The arrows on the figure represent the anterior border of the glenoid rim. A coracoid transfer procedure to reconstruct the anterior bony deficiency maximizes the possibility for successful restoration of shoulder stability.
Question 9:
Which of the following statements is true regarding humeral retroversion in a throwers dominant shoulder:
Options:
- Humeral retroversion in a throwerâ s dominant shoulder is the same as in the nondominant shoulder.
- Humeral retroversion in a throwerâ s dominant shoulder is less than humeral retroversion in the nondominant shoulder.
- Humeral retroversion in a throwerâ s dominant shoulder is greater than humeral retroversion in the nondominant shoulder.
- Humeral retroversion in a throwerâ s dominant shoulder is the same humeral retroversion in a nonthrowerâ s dominant shoulder.
- Humeral retroversion in a throwerâ s dominant shoulder is less than humeral retroversion in a nonthrowerâ s dominant shoulder.
Correct Answer: Humeral retroversion in a throwerâ s dominant shoulder is the same as in the nondominant shoulder.
Explanation:
Throwers have increased humeral retroversion in their dominant shoulder compared to their contralateral shoulder and to the dominant shoulder of nonthrowers. This represents an adaptive change that probably occurs through the physis (a pathologic expression of this adaptation probably exists in the form of proximal humeral epiphysealysis or little leaguerâ s shoulder) and has two benefits. First, humeral retroversion allows increased external rotation during throwing activities. Second, humeral retroversion acts as a protective mechanism against impingement of the greater tuberosity on the posterosuperior glenoid rim during throwing.
Question 10:
An arthroscopic photo (Slide) looking from the posterior portal is presented. The arrows point to which structure:
Options:
- Superior glenohumeral ligament
- Inferior glenohumeral ligament
- Middle glenohumeral ligament
- C oracohumeral ligament
- C oracoacromial ligament
Correct Answer: Middle glenohumeral ligament
Explanation:
The middle glenohumeral ligament is readily visualized crossing the subscapularis from the posterior arthroscopic portal. The middle glenohumeral ligament may be absent in as many as 30% of shoulders.
Question 11:
When performing a Latarjet coracoid transfer for anterior shoulder instability with bony anterior glenoid rim insufficiency, glenoid surface of the coracoid transfer must be positioned.
Options:
- Flush with the glenoid rim
- 5 mm medial to the glenoid rim
- 10 mm medial to the glenoid rim
- 5 mm lateral to the glenoid rim
- 10 mm lateral to the glenoid rim
Correct Answer: Flush with the glenoid rim
Explanation:
Allain and colleagues have clearly demonstrated that a coracoid transfer overhanging laterally to the glenoid rim is associated with the development of arthritis. One of the functions of the coracoid transfer is to increase the anteroposterior diameter of the glenoid, not to serve as a â bone block.
Question 12:
An arthroscopic photo (Slide) during shoulder arthroscopy looking from the posterior portal is presented. The arrows point to which structure:
Options:
- Biceps tendon
- Subscapularis tendon
- Supraspinatus tendon
- Teres minor tendon
- Inferior glenohumeral ligament
Correct Answer: Supraspinatus tendon
Explanation:
The insertion of the supraspinatus tendon is readily visible through the posterior arthroscopic portal.
Question 13:
An arthroscopic photo (Slide) of the shoulder looking from the posterior portal is presented. The large white structure at the top of the figure is the biceps tendon. The arrows point to which structure:
Options:
- Middle glenohumeral ligament
- Inferior glenohumeral ligament
- Superior glenoid labrum
- Anterior glenoid labrum
- Ligamentous pulley
Correct Answer: Ligamentous pulley
Explanation:
The arrows point to the ligamentous pulley. The ligamentous pulley is responsible for stabilizing the biceps within the bicipital groove of the humerus. An intact ligamentous pulley precludes arthroscopic diagnosis of superior subscapularis tendon tears.
Question 14:
An arthroscopic photo (Slide) looking from the posterior portal is presented. The arrows point to which structure:
Options:
- Biceps tendon
- Subscapularis tendon
- Supraspinatus tendon
- Middle glenohumeral ligament
- Inferior glenohumeral ligament
Correct Answer: Subscapularis tendon
Explanation:
The identified structure is the subscapularis tendon, which is readily visible during shoulder arthroscopy. The middle glenohumeral ligament crosses the superior border of the subscapularis tendon.
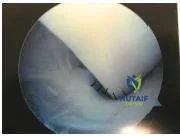
Question 15:
An arthroscopic photo (Slide) looking from the posterior portal at the anterior inferior aspect of the glenoid is presented. What is the proper treatment in this case based on the finding:
Options:
- Debridement
- Biceps tenotomy
- Open repair
- Arthroscopic repair
- No treatment necessary
Correct Answer: No treatment necessary
Explanation:
The photo shows normal anterior inferior labrum; therefore, no treatment is necessary for this structure.
Question 16:
An arthroscopic photo (Slide) looking from the posterior portal is presented. Identify the torn structure:
Options:
- Middle glenohumeral ligament
- Inferior glenohumeral ligament
- Subscapularis tendon
- Infraspinatus tendon
- Ligamentous pulley of long head biceps
Correct Answer: Ligamentous pulley of long head biceps
Explanation:
This photo demonstrates a torn ligamentous pulley that has possibly resulted in an unstable biceps tendon. Pathology of the ligamentous pulley is often associated with rotator cuff pathology.
Question 17:
When comparing anterior cruciate ligament (AC L) reconstruction using autogenous hamstrings and AC L reconstruction using autogenous patellar tendon, the most consistent difference is:
Options:
- The patellar tendon group has more patellofemoral pain.
- The hamstring group has more loss of motion.
- The patellar tendon group is more likely to return to activity.
- The hamstring group has a higher incidence of graft failures.
- The hamstring group has better results with arthrometer testing.
Correct Answer: The patellar tendon group has more patellofemoral pain.
Explanation:
Shaieb and associates recently reported a prospective randomized study comparing autogenous hamstring AC L reconstruction to autogenous patellar tendon AC L reconstruction. The only significant differences that were elicited between the groups at a minimum of 2-yearsâ follow-up were the incidences of patellofemoral pain and loss of motion, both in favor of the hamstring group.
Question 18:
Muscle contusions are clinically graded according to:
Options:
- Offending activity
- Objective swelling
- Pain as determined by analog pain scale
- The degree of myositis ossificans
- Range of motion of the adjacent joint
Correct Answer: Range of motion of the adjacent joint
Explanation:
Muscle contusions are graded according to the range of motion of the adjacent joint. Mild muscle contusion â two-thirds normal range of motion Moderate muscle contusion â one-third to two-thirds normal range of motion Severe muscle contusions â less than one-third normal range of motion The offending activity does not determine the grade of injury. Although swelling is variable, it is not the final determinant of grading. Pain is variable and unreliable in classifying muscle contusion. Although myositis ossificans is more often a result of more severe contusions, it is a later and infrequent finding.
Question 19:
The treatment protocol found to hasten recovery after quadriceps contusion is:
Options:
- Extension protocol
- Flexion protocol
- Immobilization
- Aggressive stretching protocol
- Nonweight bearing protocol
Correct Answer: Flexion protocol
Explanation:
An initial period of rest with the knee in flexion followed by rehabilitation focusing on regaining knee flexion has resulted in reduced morbidity and faster return to full activity. Extension protocols are associated with resultant longer recovery times. Immobilization is not associated with early recovery. Aggressive stretching increases morbidity and the formation of myositis ossificans. Nonweight bearing has not demonstrated decreased recovery times.
Question 20:
The differential diagnosis for patients presenting with radiographs consistent with myositis ossificans includes all of the following except:
Options:
- Osteosarcoma
- Osteochondroma
- Osteomyelitis
- C hondrosarcoma
- Rhabdomyosarcoma
Correct Answer: Rhabdomyosarcoma
Explanation:
When evaluating a patient with calcification or ossification in abnormal regions, a thorough differential including all of the mentioned conditions should be considered. Osteochondromas will typically have an intramedullary canal continuous with the adjacent bone. Osteomyelitis will sometimes have associated constitutional symptoms. Osteosarcoma will typically have a radiodense center as opposed to the radiodense periphery of mature myositis ossificans. Chondrosarcoma can be confused with myositis ossificans.



 This photo demonstrates a torn ligamentous pulley that has possibly resulted in an unstable biceps tendon. Pathology of the ligamentous pulley is often associated with rotator cuff pathology.
This photo demonstrates a torn ligamentous pulley that has possibly resulted in an unstable biceps tendon. Pathology of the ligamentous pulley is often associated with rotator cuff pathology.


