Full Question & Answer Text (for Search Engines)
Question 1:
Which of the following populations is most at risk for compression fractures of the spine:
Options:
- Middle-aged black women
- Elderly caucasian men
- Menopausal females of Inuit (Alaskan native) descent
- Elderly fair-skinned women of northern European descent
- Heavy laborers
Correct Answer: Elderly fair-skinned women of northern European descent
Explanation:
Osteoporosis is an age-related decrease in bone mass usually associated with a loss of estrogen in postmenopausal women. Sedentary, thin white women of northern European descent are most severely affected. In addition, smoking, heavy drinking, and certain pharmacological agents, such as phenytoin, increase the severity of the disease. Women who breastfed their infants or those with low vitamin D or calcium diets are also at increased risk.
Question 2:
Following an osteoporotic compression fracture, the risk of sustaining another compression fracture at a different level is increased by:
Options:
- 2 times
- 5 times
- 8 times
- 10 times
- 15 times
Correct Answer: 5 times
Explanation:
Osteoporosis is a systemic disease affecting more than 24 million Americans. Osteoporosis results in progressive bone mineral loss and concurrent changes in bony architecture, which leave the spinal column vulnerable to compression fractures, often after minimal or no trauma. There are an estimated 700,000 osteoporotic vertebral compression fractures (VC Fs) in the United States each year, of which more than one third become chronically painful. Approximately 85% of VC Fs are due to primary osteoporosis and the remainder due to secondary osteoporosis or malignancies. These VC Fs lead to progressive sagittal spine deformity and changes in spinal biomechanics and are believed to contribute to a fivefold increased risk of further fracture by virtue of force transmission to weak vertebrae above or below. Whether the fracture is painful or not, the spinal deformity caused by two or more fractures dramatically impacts health, daily living, and medical costs through loss of lung capacity, loss of appetite, reduced mobility, chronic pain, and/or clinical depression.
Question 3:
The following are all purported benefits of percutaneous intraosseous methylmethacrylate injection (vertebroplasty) for the treatment of osteoporotic compression fractures except:
Options:
- Decreased stiffness of the segment, distributing stress at adjacent levels
- Rapid pain relief
- Prevention of further compression fractures by restoring sagittal alignment
- Faster return to ambulation
- Increased mobility leading to prevention of further osteoporosis
Correct Answer: Decreased stiffness of the segment, distributing stress at adjacent levels
Explanation:
Traditional treatment for patients with osteoporotic vertebral compression fractures (VC Fs) includes bed rest, analgesics, and bracing. This type of medical management does not restore spinal alignment, and the lack of mobility increases the rate of demineralization. Because of the inherent risks and invasive nature, surgical treatment of osteoporotic VCFs has been limited to patients with concurrent spinal instability or neurologic compromise. Reconstruction with structural bone graft and instrumentation may be performed from an anterior or posterior approach; however, the success of these techniques is limited by a patients poor bone quality and general medical condition. Augmentation of VC Fs with polymethylmethacrylate (PMMA), "vertebroplasty," involves the forced injection of low viscosity PMMA cement into the closed space of the collapsed vertebral body. Although vertebroplasty is currently being used successfully for pain relief in VC Fs, this technique does not restore the height of the collapsed vertebral body.
Question 4:
Acute thoracic compression fractures should have the following signal characteristics on magnetic resonance imaging:
Options:
- High signal on T1 and T2
- Low signal on T1 and T2
- High signal on T1 and low signal on T2
- Low signal on T1 and high signal on T2
- Intermediate signal on both T1 and T2
Correct Answer: High signal on T1 and T2
Explanation:
Acute fractures produce local hematomas that displace the adipose tissue normally present in the bone marrow and decrease the signal uptake from fat on T1-weighted sequences. Fractures also produce edema, which is bright on T2-weighted sequences. Acute thoracic compression fractures should be low signal intensity on T1 sequences and high on T2 sequences.
Question 5:
In this slide of a lumbar burst fracture, which column is disrupted to distinguish it from a compression fracture:
Options:
- Anterior
- Lateral
- Posterior
- Middle
- Medial
Correct Answer: Middle
Explanation:
Denis was the first surgeon to include the middle column in his description of thoracolumbar fractures and to accentuate its importance in fracture stability. The defining characteristic of a burst fracture is disruption of the middle column, which distinguishes these fractures from compression fractures. Involvement of the middle column indicates an unstable fracture pattern.
Question 6:
When evaluating thoracolumbar burst fractures, it is important to remember that the spinal cord ends in the conus medullaris, which typically is present at what level:
Options:
Correct Answer: L1
Explanation:
While the conus medullaris can end anywhere from T12 to L3, in the majority of patients it is present at the L1 level. Injury at this level is much different from injury to the spinal cord or the cauda equina.
Question 7:
Canal compromise in burst fractures (Slide) is caused by:
Options:
- Lamina fracture and anterior migration
- Migration of the posteroinferior vertebral body
- Retropulsion of the posterosuperior vertebral body
- Narrowing of the interpedicular distance
- Herniated disk material
Correct Answer: Retropulsion of the posterosuperior vertebral body
Explanation:
An essential component of burst fractures, as described first by Denis, is the involvement of the middle column. Typically, the posterosuperior vertebral body is separated from the remainder of the body and encroaches into the spinal canal, causing damage to the neural elements. No other part of the middle column is a standard component of the injury.
Question 8:
A 16-year-old boy sustains a burst fracture of L2. Radiographs indicate loss of approximately 20% of vertebral height anteriorly and 10° of kyphosis. He is neurologically intact. Management should include:
Options:
- Anterior decompression and strut graft reconstruction
- Posterior indirect decompression with transpedicular instrumentation and fusion
- Laminectomy, open reduction of the bony intrusion, and fusion
- An initial period of bed rest, monitoring the patient for ileus, and early mobilization in an extension orthosis or body cast
- Delayed reconstruction of the spine when the initial injury has been determined
Correct Answer: An initial period of bed rest, monitoring the patient for ileus, and early mobilization in an extension orthosis or body cast
Explanation:
Burst fractures represent 17% of major spine fractures. Instability and failure occur in the anterior and middle columns. Fifty percent of patients have a neurologic deficit. These fractures are considered unstable if there is more than 50% to 60% anterior compression, 20° to 25° of kyphosis, more than 50% of canal compromise, and posterior injury. Incomplete or progressive neurologic deficits require early decompression and stabilization. Treatment of the stable fracture without neurologic deficit is hyperextension bracing for 3 to 4 months.
Question 9:
The sagittal plumb line should fall:
Options:
- Anterior to the C 4 vertebral body
- Through the L3-L4 intervertebral disk
- Posterior to the anterosuperior corner of S1
- Through the T11 intervertebral disk
- Anterior to the S1 body
Correct Answer: Posterior to the anterosuperior corner of S1
Explanation:
Radiographic assessment of the sagittal balance is usually made with a patient standing, with his or her arms flexed forward 90° and supported on a bar. Radiographic assessment is recorded on a 36-inch cassette. Several reference points regarding this technique have appeared in the literature. These points include a plumb line through the center of the C 7 vertebral body, passing 35 mm to 56 mm posterior to the anterosuperior border of S1.
Question 10:
Normal sagittal thoracic alignment is:
Options:
- 5° to 10° of kyphosis due to the adjacent lordotic cervical and lumbar segments
- Straight because of the rib cage
- Lordotic to support the body weight anteriorly
- 20° to 50° of kyphosis between T1 and T10
- 60° to 80° of kyphosis between T1 and T10
Correct Answer: 20° to 50° of kyphosis between T1 and T10
Explanation:
Thoracic kyphosis has contributions from the trapezoidal shapes of the thoracic vertebrae, from the intevertebral disk positions, and from the stiffness of the ribs and sternum. The reported normal values range from 20° to 50°.
Question 11:
A 70-year-old man complains of severe, burning pain in both calves after he ambulates approximately one block. He denies significant back pain. He has long-standing, insulin-dependent diabetes mellitus and a history of coronary artery disease. The patient has smoked two packs of cigarettes each day for more than 30 years. What questions from his history can help differentiate vascular from neurogenic claudication:
Options:
- Distribution of pain
- Pattern of sensory loss
- Posture changes
- Relief of pain with rest
- Timing of symptom onset
Correct Answer: Posture changes
Explanation:
Pain distribution may be similar in vascular and neurogenic claudication. The pattern of patient-reported sensory loss is unlikely to be contributory due to the patientâ s history of insulin-dependent diabetes and, presumably, a diabetic peripheral neuropathy. In both syndromes, pain is relieved with rest. Usually, pain relief is quicker in vascular claudication. In neurogenic claudication, standing alone may not relieve patient symptoms; sitting is usually required. Timing of symptom onset is variable in both syndromes. Vascular claudication usually produces less variability in exercise tolerance. Relief of pain with changes in posture (bending over a walker or shopping cart) is found only in neurogenic claudication.
Question 12:
A 70-year-old man complains of severe, burning pain in both calves after he ambulates approximately one block. He denies significant back pain. He has long-standing, insulin-dependent diabetes mellitus and a history of coronary artery disease. The patient has smoked two packs of cigarettes each day for more than 30 years. The patient is diagnosed with neurogenic claudication. What is the most likely source of his symptoms:
Options:
- Herniated lumbar disk
- Isthmic spondylolisthesis
- Degenerative spinal stenosis at L3-L4
- Degenerative spinal stenosis at L4-L5
- Metastatic tumor
Correct Answer: Degenerative spinal stenosis at L3-L4
Explanation:
The most common cause of neurogenic claudication in this patient is degenerative stenosis. L4-L5 is the most commonly affected level. Herniated lumbar disk is less likely. Although a metastatic tumor is possible, especially in light of the patientâ s smoking history, the absence of back pain makes this unlikely.
Question 13:
A 70-year-old man complains of severe, burning pain in both calves after he ambulates approximately one block. He denies significant back pain. He has long-standing, insulin-dependent diabetes mellitus and a history of coronary artery disease. The patient has smoked two packs of cigarettes each day for more than 30 years. A magnetic resonance image (MRI) of the patient is obtained (Slide). What does the MRI show:
Options:
- C ritically severe stenosis at L3-L4 and L4-L5
- Moderate lumbar spinal stenosis at L3-L4 and L4-L5
- Herniated lumbar disk
- Moderate lumbar stenosis at L3-L4, L4-L5, and L5-S1
- Lumbar metastatic disease
Correct Answer: Moderate lumbar spinal stenosis at L3-L4 and L4-L5
Explanation:
The MRI shows moderately severe lumbar stenosis at L3-L4 and L4-L5. While the degree or severity of stenosis remains subjective, terming this stenosis critical is an exaggeration. The section of the axial images at L5-S1 is not in plane with the disk, hence there appears to be lateral recess stenosis at this level also. The sagittal images, however, do not confirm this diagnosis. There is no evident lumbar disk herniation, and there are no findings indicative of lumbar metastatic disease.
Question 14:
A 70-year-old man complains of severe, burning pain in both calves after he ambulates approximately one block. He denies significant back pain. He has long-standing, insulin-dependent diabetes mellitus and a history of coronary artery disease. The patient has smoked two packs of cigarettes each day for more than 30 years. A magnetic resonance image (MRI) of the patient is obtained, as well as a myelogram (Slide). Conservative options in this patient include:
Options:
- Medication
- Epidural steroids
- C onditioning exercise
- All of the above
- None of the above, proceed to surgery
Correct Answer: All of the above
Explanation:
The myelogram confirms the diagnosis of lumbar spinal stenosis at L3-L4 and L4-L5. There is no myelographic block, although the stenosis is significant. A trial of conservative therapy is appropriate for this patient.
Question 15:
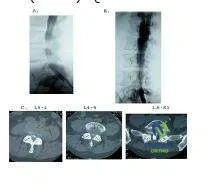
A 70-year-old man complains of severe, burning pain in both calves after he ambulates approximately one block. He denies significant back pain. He has long-standing, insulin-dependent diabetes mellitus and a history of coronary artery disease. The patient has smoked two packs of cigarettes each day for more than 30 years. Based upon the patientâ s history, magnetic resonance image (MRI) (Slide 1), and computed tomography (CT)-myelogram (Slide 2) available for your review, what is the correct diagnosis in this patient:
Options:
- Lumbar metastatic disease
- Lumbar spinal stenosis
- Lumbar herniated disk
- Degenerative lumbar spondylolisthesis
- Ankylosing spondylitis
Correct Answer: Lumbar spinal stenosis
Explanation:
There is no evidence of lumbar metastases in this patient. The C T- myelogram shows compression arising posterior to the thecal sac, making a disk herniation less likely. Similarly, there is no evidence of a lumbar disk herniation on MRI. The patientâ s sagittal alignment is well maintained, with no spondylolisthesis evident. Ankylosing spondylitis generally presents in younger patients, and the classic radiographic finding of spontaneous arthrodesis is not present.
Question 16:
A 75-year-old woman presents with low back pain that is worse with motion and bilateral lower extremity pain that is worse with ambulation. She notes that the pain extends down the posterior aspects of her lower extremities, from the buttocks to the calves. The pain limits her activity â she can only ambulate approximately one block before having to rest. She reports that lumbar flexion, notably leaning over a walker or a shopping cart, considerably diminishes her lower extremity pain. She has a significant past medical history of coronary artery disease, and she has had previous angioplasty of her coronary vessels. On examination, her lower extremity pulses are easily palpable. What would you expect to find on this patientâ s neurological examination:
Options:
- No abnormal findings on the neurological examination
- Mild proximal lower extremity weakness
- Severe proximal lower extremity weakness
- Mild distal lower extremity weakness
- Severe distal lower extremity weakness
Correct Answer: No abnormal findings on the neurological examination
Explanation:
Lumbar spinal stenosis is a dynamic process. Patients classically have no deficit until they are physically active. Therefore, this patient may not have a deficit during her clinic examination. It would be unusual for her to present with a fixed lower extremity deficit.
Question 17:
A 75-year-old woman presents with low back pain that is worse with motion and bilateral lower extremity pain that is worse with ambulation. She notes that the pain extends down the posterior aspects of her lower extremities, from the buttocks to the calves. The pain limits her activity â she can only ambulate approximately one block before having to rest. She reports that lumbar flexion, notably leaning over a walker or a shopping cart, considerably diminishes her lower extremity pain. She has a significant past medical history of coronary artery disease, and she has had previous angioplasty of her coronary vessels. On examination, her lower extremity pulses are easily palpable. What radiographic evaluation would you obtain to best establish her diagnosis:
Options:
- Plain L-spine films
- Angiogram of lower extremity vessels
- MRI of cervical spine
- C omputed tomography (C T) of lumbar spine
- Magnetic resonance image (MRI) of lumbar spine
Correct Answer: Magnetic resonance image (MRI) of lumbar spine
Explanation:
The most efficacious and least invasive means of evaluation for lumbar spinal stenosis is MRI. A CT scan, while showing bony anatomy well, may not provide adequate information about soft tissue structures. Plain films are nonspecific and, although they are often used as an initial evaluation, may not yield adequate diagnosis. This patientâ s symptom complex does not correlate with vascular claudication.
Question 18:
A 75-year-old woman presents with low back pain that is worse with motion and bilateral lower extremity pain that is worse with ambulation. She notes that the pain extends down the posterior aspects of her lower extremities, from the buttocks to the calves. The pain limits her activity â she can only ambulate approximately one block before having to rest. She reports that lumbar flexion, notably leaning over a walker or a shopping cart, considerably diminishes her lower extremity pain. She has a significant past medical history of coronary artery disease, and she has had previous angioplasty of her coronary vessels. On examination, her lower extremity pulses are easily palpable. This patient is diagnosed with degenerative spondylolisthesis with significant lateral recess stenosis. Treatment of this patient could include:
Options:
- Epidural steroids
- Decompression alone
- Decompression with noninstrumented fusion
- Decompression with instrumented fusion
- All of the above
Correct Answer: All of the above
Explanation:
Treatment options for this patient are legion. Considering her significant coronary artery disease, a conservative approach using anti-inflammatory drugs, physical therapy, and epidural steroids might be chosen by some physicians. Surgical options include decompression alone or decompression with fusion. This patientâ s significant mechanical low back pain encourages some surgeons to include a fusion with the decompression.
Question 19:
The distinguishing phenotypic feature that differentiates a schwannoma from a neurofibroma is:
Options:
- The consistently hard and irregular surface of a schwannoma tumor
- The lack of a capsule around a neurofibroma tumor
- The presence of a dissection plane between the tissue and a schwannoma tumor
- Distinctly differing locations of occurrence along the spinal axis
- There is no phenotypic distinguishing characteristic that differentiates a schwannoma from a neurofibroma.
Correct Answer: The presence of a dissection plane between the tissue and a schwannoma tumor
Explanation:
Nerve sheath tumors account for 25% of intradural spinal cord tumors in adults and can be further broken down into either schwannomas or neurofibromas. Schwannomas are more common than neurofibromas, most commonly occurring in patients 30 to 50 years of age, equally between the sexes. Most schwannomas arise in the dorsal nerve root. Neurofibromas, however, have a predilection to the ventral root. Both tumors primarily are intradural but as many as 10% to 15% can escape through the dura to form a dumbbell shape and exist as both an intradural and extradural tumor. Histologically, fibrous tissue and nerve fibers make up a neurofibroma. Grossly, neurofibromas appear as a fusiform enlargement of the nerve, making a clear distinction between tumor and nerve impossible. Macroscopically, schwannomas look like smooth globoid masses sitting on the nerve fiber and a clear resection plane is apparent.
Question 20:
What is the advantage of performing a magnetic resonance image (MRI) to evaluate spinal tumors:
Options:
- The post-contrast enhancement pattern is sensitive and specific in diagnosing malignant tumors.
- The diagnosis is often made based on imaging location of a tumor, thus avoiding the need for invasive tissue diagnosis.
- Magnetic resonance imaging is more sensitive than computed tomography (C T) myelography.
- Magnetic resonance imaging has no advantage as a diagnostic tool in evaluating spinal cord lesions.
- Magnetic resonance imaging is a helpful, adjunct diagnostic tool that can elucidate characteristics of spinal cord lesions and help narrow the differential diagnosis.
Correct Answer: Magnetic resonance imaging is more sensitive than computed tomography (C T) myelography.
Explanation:
Although diagnosis and localization of spinal column tumors depends on a patientâ s history and physical examination, differentiation of intramedullary versus extramedullary location of a tumor relies primarily on image findings. The most common imaging modality is MRI. Lesion signal abnormalities, cerebral spinal fluid (CSF) capping, and cord or cauda equina displacement signify extramedullary masses, even without contrast. Gadolinium enhancement increases the sensitivity of the MRI, as almost all spinal cord tumors demonstrate some contrast enhancement. Although more sensitive than MRI, myelography and postmyelography CT are rarely used initially due to their invasive nature.