Full Question & Answer Text (for Search Engines)
Question 1:
When using the tibial external rotation test on a patient, increased external rotation at 30° and 90° of knee flexion is indicative of:
Options:
- Anterior cruciate ligament injury
- Posterior cruciate ligament injury
- Isolated posterolateral corner injury
- Posterior cruciate and posterolateral corner injury
- Anterior cruciate and posterior cruciate ligament injury
Correct Answer: Posterior cruciate ligament injury
Explanation:
The tibial external rotation test is performed at 30° and 90° of knee flexion. The degree of foot external rotation with regard to the femur is evaluated. Increased external rotation at 30° is consistent with an isolated posterolateral corner injury. Increased external rotation at 30° and 90° is consistent with a combined posterolateral and posterior cruciate ligament injury.
Question 2:
The recommended treatment for an acute combined anterior cruciate ligament and complete posterolateral corner disruption in a young athlete is:
Options:
- Anterior cruciate ligament reconstruction alone
- Nonoperative treatment emphasizing quadriceps strengthening
- Anterior cruciate ligament reconstruction and posterolateral corner repair
- Anterior cruciate ligament repair and posterolateral corner repair
- Posterolateral corner repair alone
Correct Answer: Anterior cruciate ligament reconstruction alone
Explanation:
In cases of combined cruciate ligament and posterolateral corner injuries, most surgeons recommend addressing both injuries. In one study, the most common cause of anterior cruciate ligament failure was unrecognized and untreated concomitant posterolateral corner injuries.
Question 3:
The ideal timing for repair of an acute posterolateral corner knee injury is:
Options:
- In the first 3 weeks
- 4 to 6 weeks
- 8 to 12 weeks
- Acute repair is unsuccessful, and late reconstruction is recommended.
- Surgery is rarely needed for complete posterolateral corner injuries.
Correct Answer: In the first 3 weeks
Explanation:
Surgical repair of posterolateral corner injuries is recommended within the first several weeks because dissection can be difficult and can result in the need for a reconstruction with longer delays. Results of chronic posterolateral corner injury repairs are inferior to those for acute posterolateral corner injuries.
Question 4:
Which of the following exercises must be delayed for up to 3 months after posterolateral corner repair or reconstruction of the knee:
Options:
- Range of motion exercises
- Isometric quadriceps exercises
- Closed chain quadriceps exercises
- Hamstring exercises
- All of the above answers should be started immediately
Correct Answer: Hamstring exercises
Explanation:
Postoperative rehabilitation for posterolateral corner repair or reconstruction involves early protected or nonweight bearing, early range of motion exercises, and quadriceps exercises. Avoidance of hamstring exercises for up to 12 weeks is recommended to decrease external rotational torque and posterior subluxation forces at the knee joint.
Question 5:
For patients who sustain a knee dislocation, the role of clinical history, physical examination, and magnetic resonance imaging (MRI) is:
Options:
- Both physical examination and MRI are important, but physical examination is much more accurate.
- Neither physical examination or MRI is very accurate.
- Both physical examination and MRI are important, but MRI is more accurate.
- There is no role for MRI.
- C linical history is the more important than MRI.
Correct Answer: Both physical examination and MRI are important, but physical examination is much more accurate.
Explanation:
In a study of 17 knee dislocations, the accuracy of clinical examination ranged from 53% to 82% correct compared to an accuracy of 85% to 100% with MRI. The limitations of clinical examination were mainly due to associated injuries.
Question 6:
After high velocity knee dislocations, there is serious injury to the popliteal vessels in approximately what percentage of patients:
Options:
- 5%
- 10%
- 30%
- 75%
- More than 90%
Correct Answer: 30%
Explanation:
After reviewing several series from 1963 to 1992, investigators found serious injury to the popliteal vessels in approximately 30% of cases and peroneal nerve injuries in 25% of cases. The incidence of arterial and nerve injury with lower velocity mechanisms (some athletic injuries) is lower.
Question 7:
After high velocity knee dislocations, there is serious injury to the peroneal nerve in approximately what percentage of patients:
Options:
- Serious injury has not been reported.
- 5%
- 25%
- 75%
- More than 90%
Correct Answer: 5%
Explanation:
After reviewing several series from 1963 to 1992, investigators found serious injury to the popliteal vessels in approximately 30% of cases and peroneal nerve injuries in 25% of cases. The incidence of arterial and nerve injury with lower velocity mechanisms (some athletic injuries) is lower.
Question 8:
The strongest bundle in the posterior cruciate ligament is the:
Options:
- Anteromedial bundle
- Posteromedial bundle
- Anterolateral bundle
- Posterolateral bundle
- Both bands are of equal strength
Correct Answer: Anterolateral bundle
Explanation:
The posterior cruciate ligament is made up of two bundles (anterolateral and posteromedial) that are named according to their origin on the femur and insertion on the tibia. The anterolateral bundle is the larger and stronger of the two bundles. The anterolateral bundle is tight in flexion, and the posteromedial bundle is tight in extension.
Question 9:
In the posterior cruciate ligament the anterolateral bundle is tight in ______ and the posteromedial bundle is tight in ______:
Options:
- Flexion, extension
- Extension, flexion
- Extension, extension
- Flexion, flexion
- Neither bundle tightens throughout the kneeâ s range of motion.
Correct Answer: Flexion, extension
Explanation:
The posterior cruciate ligament is made up of two bundles (anterolateral and posteromedial) that are named according to their origin on the femur and insertion on the tibia. The anterolateral bundle is the larger and stronger of the two bundles. The anterolateral bundle is tight in flexion, and the posteromedial bundle is tight in extension.
Question 10:
When applying valgus stress, over which arc of motion is the anterior band of the anterior oblique component of the ulnar collateral ligament of the elbow under tension:
Options:
- 0° to 20°
- 0° to 45°
- 0° to 85°
- 55° to 115°
- 55° to 145°
Correct Answer: 0° to 85°
Explanation:
Biomechanical studies demonstrate that the anterior band of the oblique component of the ulnar collateral ligament of the elbow is at greatest tension from full extension to 85° of elbow flexion.
Question 11:
When applying valgus stress, over which arc of motion is the posterior band of the anterior oblique component of the ulnar collateral ligament of the elbow under tension:
Options:
- 0° to 35°
- 0° to 65°
- 0° to 85°
- 55° to 85°
- 55° to 145°
Correct Answer: 55° to 145°
Explanation:
Biomechanical studies demonstrate that the posterior band of the oblique component of the ulnar collateral ligament of the elbow is at greatest tension from 55° to full elbow flexion.
Question 12:
Which of the following structures is the main stabilizer of the elbow to valgus stress:
Options:
- Anterior oblique component of the ulnar collateral ligament
- Posterior oblique component of the ulnar collateral ligament
- Transverse oblique component of the ulnar collateral ligament
- Ulnohumeral articulation
- Radiohumeral articulation
Correct Answer: Anterior oblique component of the ulnar collateral ligament
Explanation:
The anterior oblique component of the ulnar collateral ligament is the most important stabilizer of the elbow to valgus stress. The most important secondary stabilizer is the radiohumeral articulation. The transverse oblique component of the ulnar collateral ligament imparts little stability to the elbow.
Question 13:
Disruption of which of the following ligaments represents the primary lesion in posterolateral rotatory instability of the elbow:
Options:
- Radial collateral ligament
- Radial ulnohumeral ligament
- Annular ligament
- Accessory radial collateral ligament
- Ulnohumeral articulation
Correct Answer: Radial ulnohumeral ligament
Explanation:
Of Driscoll and associates demonstrated that the radial ulnohumeral ligament must be disrupted to produce posterolateral rotator instability of the elbow.
Question 14:
Elbow injury usually occurs during which phase of throwing:
Options:
- Wind-up
- Early cocking
- Late cocking
- Acceleration
- Follow through
Correct Answer: Acceleration
Explanation:
Peak valgus stresses on the elbow occur during the acceleration phase of throwing making it the phase during which the elbow is most vulnerable to injury.
Question 15:
Which of the following structures is the most important dynamic stabilizer of the elbow to valgus stresses during throwing:
Options:
- Anterior oblique component of the ulnar collateral ligament
- Posterior oblique component of the ulnar collateral ligament
- Flexor-pronator musculature
- Brachialis
- Biceps brachii
Correct Answer: Flexor-pronator musculature
Explanation:
The flexor-pronator muscle mass on the medial side of the elbow dynamically resists valgus stresses during throwing. Compromise or fatigue of this muscle group with activity may be a predecessor to injury to the ligamentous stabilizing structures.
Question 16:
The following is a hip magnetic resonance image (MRI) of a 28-year-old male triathlete who has noticed progressive activityrelated left hip pain. Recommended treatment includes:
Options:
- Arthroscopic debridement
- Open reduction internal fixation
- Percutaneous pinning in situ
- Period of nonweight bearing with continued observation
- C ontinuation of current training regimen
Correct Answer: Period of nonweight bearing with continued observation
Explanation:
The MRI depicts a compression sided incomplete femoral neck fracture. Compression sided fractures of the femoral neck are treated with nonweight bearing and close observation. In the advent of fracture line extension, these fractures must be urgently percutaneously pinned. Complete stress fractures and incomplete tension sided fractures of the femoral neck must be urgently percutaneously pinned.
Question 17:
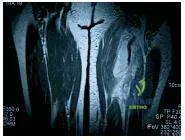
The following radiographs are of a 19-year-old female collegiate distance runner who complained of pain in her right distal tibia. She reports having shin splints 2 years earlier that affected her right proximal tibia. She has been unable to run secondary to symptoms for 3 weeks. She reports being amenorrheic for approximately the last 3 years. Which of the following should be included in her initial treatment regimen:
Options:
- Treatment with nonsteroidal anti-inflammatory medications
- Localized steroid injection
- Intramedullary nailing with bone grafting
- C ontinuation of current training regimen
- Initiation of hormone replacement therapy
Correct Answer: Initiation of hormone replacement therapy
Explanation:
This individual has a distal tibial stress fracture as evidenced by the early periosteal reaction shown on radiography. Radiographs also show a healed proximal tibial stress fracture. Amenorrhea is a risk factor for stress fractures and should be addressed with hormone replacement therapy. The other possible answers are inappropriate for initial treatment.
Question 18:
The following figure is the magnetic resonance image (MRI) of a 40-year- old avid female water-skier who felt a pop in her left hip as she was pulled over the front of her ski. Recommended treatment includes:
Options:
- Percutaneous pinning
- Nonweight bearing crutch ambulation
- Physical therapy
- Operative repair of the injured structures
- Reassurance and symptomatic treatment
Correct Answer: Operative repair of the injured structures
Explanation:
The MRI shows a complete avulsion of the hamstring tendons off the ischial tuberosity. In active individuals, operative repair is recommended for complete avulsions. Nonoperative treatment of complete hamstring avulsion injury yields a low rate of return to sport at preinjury activity level.
Question 19:
During which phase of throwing is the flexor-pronator muscle mass most electrically active:
Options:
- Wind-up
- Early cocking
- Late cocking
- Acceleration
- Follow through
Correct Answer: Acceleration
Explanation:
Peak valgus stresses on the elbow occur during the acceleration phase of throwing making it the phase during which the elbow is most vulnerable to injury. The flexor-pronator muscle mass peaks in activity during the acceleration phase to dynamically stabilize the elbow.
Question 20:
Which of the following is a risk factor for anterior cruciate ligament (AC L) injury in noncontact athletes:
Options:
- Smaller than average cross sectional size of the AC L
- High shoe-surface coefficient of friction
- Smaller than average diameter of the femoral notch
- Failure to use a knee brace
- Failure to modify activity of female athletes during certain phases of the menstrual cycle
Correct Answer: High shoe-surface coefficient of friction
Explanation:
A high coefficient of friction at the shoe-surface interface is a risk factor for AC L injury in noncontact athletes. Insufficient evidence exists to definitively implicate the other possible answers as risk factors.