Full Question & Answer Text (for Search Engines)
Question 1:
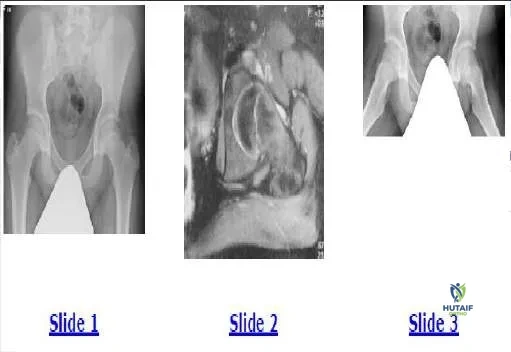
A 9-year-old girl sustains an injury (Slide) as a result of a fall. What is her risk of avascular necrosis:
Options:
Correct Answer: 25%
Explanation:
This patient has a displaced basicervical fracture of the femur that is classified as Delbet type III. The risk of avascular necrosis is approximately 20% to 25%. She should be monitored closely for the first 12 to 18 months after injury for this complication.
Question 2:
A 9-year-old girl sustains an injury (Slide 1) as a result of a fall. What is the recommended treatment:
Options:
- Traction
- C losed reduction and spica cast application
- C losed reduction and Steinmann pin fixation
- Open reduction and Steinmann pin fixation
- Open reduction and fixation with hip screw
Correct Answer: Open reduction and Steinmann pin fixation
Explanation:
This patient has a basicervical fracture, which is prone to development of varus. Traction, spica cast, and Steinman pin fixation do not provide adequate control of this process. Steinmann pins do not allow compression
across the fracture site. C losed or open reduction and internal fixation with a compression screw fixation, preferably a hip screw, provide the best control of the fracture. A hip screw provides the best protection against the development of varus. If the fracture is not opened, then aspiration of the hematoma is recommended.
Question 3:
A 6-year-old boy presents with a 3-month history of medial midfoot pain. Based on his radiograph (Slide), which of the following is the correct diagnosis:
Options:
- Kohler s disease
- Panner s disease
- Eosinophilic granuloma
- Accessory navicular
- Freiberg s disorder
Correct Answer: Kohler s disease
Explanation:
This child has avascular necrosis of the tarsal navicular. This is an idiopathic phenomenon more common in boys of this age than girls. The condition responds to rest and orthotics or cast immobilization. The navicular revascularizes over the ensuing year.
Question 4:
Which of the following syndromes has the highest incidence of scoliosis as a percentage of affected patients:
Options:
- Marfan syndrome
- Loeys-Dietz syndrome
- Down syndrome
- Rett syndrome
- Prader-Willi syndrome
Correct Answer: Marfan syndrome
Explanation:
Marfan syndrome, due to a mutation in fibrillin-1, causes spinal deformity in two-thirds of patients. Rett syndrome, caused by a mutation in MEC P-2, results in neurological balance disorder and may cause scoliosis in up to half of affected patients. Scoliosis is seen in smaller numbers of patients with Prader-Willi, Down, and Loeys-Dietz syndromes.
Question 5:
Acute pain that presents in the lateral arm and shoulder is suggestive of:
Options:
- Cervical myelopathy
- Thoracic outlet syndrome
- Radial tunnel syndrome
- Cervical disk herniation
- Diabetic neuropathy
Correct Answer: Cervical disk herniation
Explanation:
Acute radiculopathies of the upper extremity are suggestive of soft cervical disk herniations. Three types of soft disk herniations have been described: Intraforaminal is the most common and is often evidenced by radicular symptoms in a dermatomal distribution. Posterolateral herniation results in predominantly motor symptoms. Midline disk herniations may result in myelopathy.
Question 6:
A cervical disk herniation that causes weakness in the wrist extensors will likely produce sensory changes in the:
Options:
- Lateral arm
- Ulnar forearm
- Radial forearm
- Long finger
- Hypothenar eminance
Correct Answer: Radial forearm
Explanation:
The wrist extensors are innervated by C6. Weakness would likely be the result of a C5-C6 cervical disk herniation, thus causing a C 6 radiculopathy. The dermatome of C 6 includes the radial side of the forearm and radial digits.
Question 7:
In order to diagnose a disk herniation, the preferred test is:
Options:
- Electromyogram
- Flexion-extension roentgenograms
- C omputerized tomography scan
- Magnetic resonance imaging (MRI) with gadolinium
- MRI without gadolinium
Correct Answer: MRI without gadolinium
Explanation:
Magnetic resonance imaging (MRI) has become the modality of choice for diagnosis of disk herniation. It is readily available, noninvasive, and has proven as accurate as post-myelogram computerized tomography scans in the evaluation of cervical radiculopathy. An MRI study should include a T1- and T2-weighted image sequence with both sagittal and axial images.
Question 8:
Initial management of cervical radiculopathy includes all of the following except:
Options:
- Nonsteroidal anti-inflammatory drugs
- Cervical immobilization
- Physical therapy
- Anterior cervical discectomy and fusion
- Home traction
Correct Answer: Anterior cervical discectomy and fusion
Explanation:
Initial management of cervical radiculopathy is nonoperative. This includes: Nonsteroidal anti-inflammatory drugs Occasional narcotic analgesic medications Immobilization in a soft collar for 10 to 14 days Physical therapy with emphasis on isometric exercises Home traction Surgical intervention is indicated for patients who fail nonoperative treatment. Motor deficits intertractable pain may serve as indication for early surgical therapy. In addition, patients with intertractable pain or motor deficits may be recommended for early surgery.
Question 9:
This patient has a wide-based gait and hyper-reflexia in his lower extremities. His magnetic resonance image is presented. Other physical findings in this patient would likely include:
Options:
- Negative Hoffman sign
- Negative Babinski sign
- Carpal tunnel syndrome
- Hand intrinsic wasting
- Thoracic outlet syndrome
Correct Answer: Hand intrinsic wasting
Explanation:
This patientâ s clinical presentation is suggestive of cervical spondylotic myelopathy. The T2 sagittal magnetic resonance image shows multiple areas of spinal cord compression due to spondylosis. In this situation, one sees evidence of upper motor neuron dysfunction in the lower extremites such as hyper-reflexia, Hoffman sign, clonus, wide-based gait, and sexual or bladder dysfunction. The upper extremities may demonstrate upper and lower motor neuron findings, hypo-reflexia or hyper-reflexia, crossed radial reflex, Hoffman sign, and hand intrinsic wasting.
Question 10:
A useful test to differentiate cervical radiculopathy from diabetic peripheral neuropathy is:
Options:
- Hemoglobin A1C
- Magnetic resonance imaging
- Computerized tomography-myelogram
- Electrodiagnostic testing
- Cervical flexion/extension roentgenograms
Correct Answer: Electrodiagnostic testing
Explanation:
An electromyogram detects motor changes as a result of nerve compression. It can be used to differentiate cervical radiculopathy from peripheral neuropathy.
Question 11:
With a left-sided anterior cervical spine approach, the structure at increased risk for injury is the:
Options:
- Recurrent laryngeal nerve
- Superior laryngeal nerve
- Hypoglossal nerve
- Thoracic duct
- Esophagus
Correct Answer: Thoracic duct
Explanation:
On the left side of the neck, the thoracic duct ascends lateral to the carotid sheath and is at potential risk for laceration with resulting chylothorax. This potential risk must be avoided by remaining medial to the carotid sheath during the left-sided anterior cervical spine approach.
Question 12:
With a right-sided anterior cervical spine approach, the structure at increased risk is the:
Options:
- Recurrent laryngeal nerve
- Superior laryngeal nerve
- Hypoglossal nerve
- Thoracic duct
- Esophagus
Correct Answer: Recurrent laryngeal nerve
Explanation:
The left recurrent laryngeal nerve enters the thorax within the carotid sheath before looping around the aortic arch and ascending into the neck between the trachea and the esophagus. On the right side, the nerve exits the carotid sheath at a higher level, making the nerve susceptible to injury during the surgical dissection.
Question 13:
The structure most at risk during lateral mass screw placement is the:
Options:
- Vertebral artery
- Nerve root
- Spinal cord
- Recurrent laryngeal nerve
- Thoracic duct
Correct Answer: Nerve root
Explanation:
Lateral mass screws placed in the cervical spine for plate fixation are directed 30° lateral and 15° cephalad from a point 1 mm medial to the mid- portion of the particular pillar. The nerve root exits at the anterolateral portion of the facet joint and is at risk of injury. The vertebral artery may be injured in screws placed too medially. The spinal cord is essentially free of danger with accepted techniques.
Question 14:
After undergoing an anterior cervical discectomy and fusion through a left- sided neck incision, the patient is noted to have a drooping eyelid and a right pinpoint pupil. This is likely due to:
Options:
- Spinal cord injury
- Nerve root injury
- Retractor placement
- C arotid sheath compression
- Vertebral artery injury
Correct Answer: Retractor placement
Explanation:
This patient has postoperative Horner syndrome. The sympathetic chain lies lateral to the longus colli muscles. Retractors must be placed deep into these muscles. Retractors placed ventrally to the longus colli muscles can cause injury to the sympathetic chain, esophagus medially, and carotid sheath contents laterally.
Question 15:
After an anterior cervical discectomy and fusion with autogenous iliac crest bone graft, the patient reports numbness in the lateral thigh. This is due to:
Options:
- Nerve root injury
- Intraoperative positioning
- Lateral femoral cutaneous nerve injury
- Genitofemoral nerve injury
- Sciatic nerve injury
Correct Answer: Lateral femoral cutaneous nerve injury
Explanation:
The lateral femoral cutaneous nerve emerges from the lateral border of the psoas major muscle and crosses the ilium as it runs toward the anterior superior iliac spine. The course of the nerve is variable. The nerve is at risk of injury, with resulting meralgia paresthetica, in approximately 10% of patients.
Question 16:
One advantage of posterior laminoforaminotomy in the treatment of cervical radiculopathy is:
Options:
- Obviates the need for fusion
- Improves nerve root decompression
- Easier access to midline disk herniations
- Improves wound healing
- Improves postoperative alignment
Correct Answer: Obviates the need for fusion
Explanation:
The posterior cervical foraminotomy has a surgical success rate similar to an anterior cervical discectomy and fusion. Proponents argue that the posterior procedure obviates the need for fusion, therefore, postoperative immobilization is unnecessary. The posterior approach cannot address segmental kyphosis or recreate disk space height.
Question 17:
The most frequently involved spinal segment in rheumatoid arthritis is:
Options:
- C1-C2
- C7-T1
- C5-C6
- T12-L1
- L5-S1
Correct Answer: C1-C2
Explanation:
C 1-C2 is the most frequently involved spinal segment in rheumatoid arthritis (RA), and it is also the most clinically significant. These articulations are exclusively synovial and the primary target of RA.
Question 18:
The most useful measurement for predicting neurological deficit in rheumatoid arthritis involvement of the cervical spine is:
Options:
- Flexion angle
- Posterior atlantodens interval (PADI)
- Anterior atlantodens interval (AADI)
- Lordosis angle
- C2-C3 disk height
Correct Answer: Posterior atlantodens interval (PADI)
Explanation:
The posterior atlantodens interval (PADI) is the distance between the posterior surface of the dens and the anterior edge of the posterior ring of C 1, as seen on a lateral radiograph. A PADI < 14 mm was 97% sensitive in predicting the presence of neurological deficit. Patients with a PADI >14 mm had a 94% chance of being neurologically intact.
Question 19:
A relative contraindication to cervical laminectomy for the treatment of cervical spondylosis is:
Options:
- Positive Babinski sign
- C ervical lordosis
- Positive Hoffman sign
- Wrist extensor weakness
- C ervical kyphosis
Correct Answer: C ervical kyphosis
Explanation:
Cervical laminectomy for spondylosis is performed to allow the spinal cord to migrate posteriorly in order to decompress the spine. This can be accomplished only if the spine is lordotic. If kyphosis exists, then the cord may remain draped over anterior osteophytes and continued compression may exist. In cases of cervical kyphosis, anterior decompression is preferred.
Question 20:
The major risk factor for nonunion in a type 2 odontoid fracture is:
Options:
- Age >35 years old
- Posterior displacement >5 mm
- Anterior displacement >5 mm
- Smoking history
- Flexion 30°
Correct Answer: Posterior displacement >5 mm
Explanation:
A posterior displacement >5 mm has the greatest risk of nonunion. However, age >65 years old is a next risk factor. Type 2 odontoid fractures have the highest rate of nonunion of the 3 types and there has been reported to be >60% nonunion when not treated with a halo immobilization. Halo traction is a viable alternative for a patient who has minimal displacement and/or is not a candidate for surgery.

 across the fracture site. C losed or open reduction and internal fixation with a compression screw fixation, preferably a hip screw, provide the best control of the fracture. A hip screw provides the best protection against the development of varus. If the fracture is not opened, then aspiration of the hematoma is recommended.
across the fracture site. C losed or open reduction and internal fixation with a compression screw fixation, preferably a hip screw, provide the best control of the fracture. A hip screw provides the best protection against the development of varus. If the fracture is not opened, then aspiration of the hematoma is recommended.
 This child has avascular necrosis of the tarsal navicular. This is an idiopathic phenomenon more common in boys of this age than girls. The condition responds to rest and orthotics or cast immobilization. The navicular revascularizes over the ensuing year.
This child has avascular necrosis of the tarsal navicular. This is an idiopathic phenomenon more common in boys of this age than girls. The condition responds to rest and orthotics or cast immobilization. The navicular revascularizes over the ensuing year.