Full Question & Answer Text (for Search Engines)
Question 1:
The radiographs (Slide) of a 13-year-old-boy are presented. The radiographs demonstrate characteristics of which of the following conditions:
Options:
- Osteoid osteoma
- Tibial hemimelia
- Congenital dysplasia
- Fracture growth arrest
- Osteomyelitis
Correct Answer: Fracture growth arrest
Explanation:
The radiographs show characteristics of a growth arrest from a medial distal tibial physeal fracture, either a Salter III or Salter IV. The fracture was not internally fixed, and the residual vertical fracture line and step-off are still visible. A growth plate bar developed and Park-Harris growth lines are seen on the lateral side of the bar. Some of the physis is open medially and, especially, laterally. The fibula has continued to grow.
Question 2:
An 11½ -year-old boy sustained a Salter IV fracture of the distal tibial physis. The fracture was treated in a cast. Two years later, his radiographs (Slide) are presented. The patient is starting to notice a deformity. Which of the following treatment plans is recommended:
Options:
- Medial physeal bar resection
- Right distal fibular epiphyseodesis
- Right distal tibial and fibular epiphyseodesis
- Left distal tibial and fibular epiphyseodesis
- Right distal tibial and fibular osteotomy, and bilateral distal tibial and fibular epiphyseodesis
Correct Answer: Right distal fibular epiphyseodesis
Explanation:
This patient has an unacceptable deformity, 2 cm of current shortening, and significant growth remaining. Only right distal tibial and fibular osteotomy, and bilateral distal tibial and fibular epiphyseodesis addresses all of the complications. Bar resection is not uniformly successful and would not correct existing deformity and length inequality, since there is minimal physis medial to the bar that could produce correction.
Question 3:
The radiographs (Slide) indicate which of the following diagnoses:
Options:
- Congenital dysplasia of the distal humerus
- Osteogenesis imperfecta
- Supracondylar humeral fracture
- Lateral condylar humeral fracture
- Normal elbow
Correct Answer: Supracondylar humeral fracture
Explanation:
The radiographs indicate a supracondylar fracture of the distal humerus. The anterior humeral line should bisect the capitellum on the lateral view. The anterior and posterior fat pads are elevated. The fracture line may be seen on the anteroposterior and the lateral radiographs, although it is subtle. The cortical break of the coronoid fossa is evident. Surgeons must recognize
these fractures so that the patient and family may be given proper activity restrictions and expectations for improvement.
Question 4:
A 5-year-old boy was imaged after being struck by a car. His radiographs (Slide) indicate which of the following diagnoses:
Options:
- Buckle fracture of the proximal humeral metaphysis
- Salter I fracture of the proximal humeral physis
- Salter II fracture of the proximal humeral physis
- Salter IV fracture of the proximal humeral physis
- Normal humerus
Correct Answer: Normal humerus
Explanation:
The proximal humeral physis has two planes and two ossification centers (in this way, it is analogous to the proximal femur).
When seen in some projections, the more distal extent of the physis may produce a lucent line. The smooth nature and characteristic location of the line should allow surgeons to make the correct interpretation. The two ossification centers of the humeral head may be misinterpreted as a fracture. This patient had a greenstick fracture of the clavicle (not included on this field), which was not noticed, and a humeral fracture was incorrectly diagnosised.
Question 5:
The largest available free muscle flap comes from which of the following muscles:
Options:
- Gracilis muscle
- Serratus anterior muscle
- Latissimus dorsi muscle
- Rectus abdominis muscle
- Brachialis muscle
Correct Answer: Latissimus dorsi muscle
Explanation:
The latissimus dorsi provides the largest available free muscle flap. The gracilis provides a long muscle slip and can be innervated and used for certain innervated muscle transfers. The serratus anterior muscle is thin and can be used when bulk is undesirable.
Question 6:
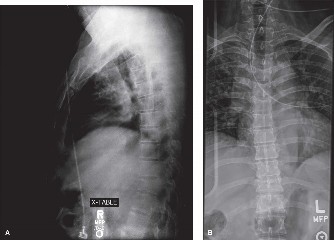
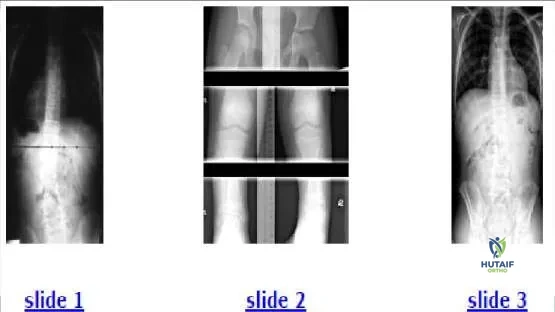
A 12-year-old boy presents for evaluation of a spinal curvature (Slide 1). Which of the following is the most likely cause of the spinal curve:
Options:
- Idiopathic scoliosis
- Neurofibromatosis
- Osteoid osteoma
- Limb length inequality
- Cerebral palsy
Correct Answer: Limb length inequality
Explanation:
This patient has a 2.5 cm shortening of the left lower extremity, which can be seen from the uneven pelvic height on the radiograph. The shortening produces a compensatory curve. No rotation is present within the curve. Scanogam (Slide 2) documents the inequality. When the patient stands on a 2.5-cm lift, the curve is eliminated (Slide 3).
Question 7:
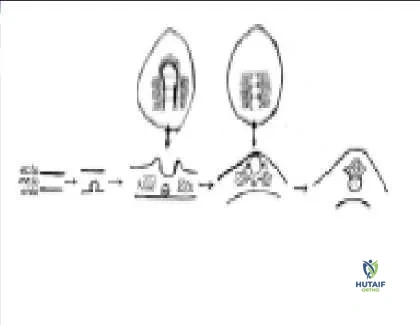
In the embryo, cells from the ectodermal layer give rise to which elements of the spine:
Options:
- Spinal cord
- Vertebral body
- Paraspinous muscle
- Nucleus pulposus
- Annulus fibrosis
Correct Answer: Spinal cord
Explanation:
The spine is formed from all three elements of the embryonic plate (Slide). The ectoderm develops into a groove, folding into a tube that becomes the spinal cord. The endoderm gives rise to the notochord, which serves as the organizing structure for the spinal column. The notochord persists as the
nucleus pulposus. The mesoderm gives rise to muscles and bony elements of the spinal column.
Question 8:
How many somites are involved in formation of each vertebral body of the thoracolumbar spine:
Options:
Correct Answer: Two
Explanation:
The somites are repeating groups of axial mesodermal cells that give rise to the osseous and musculoligamentous elements of the spine during embryonic formation. Each somite divides and contributes to two adjacent vertebral bodies.
Question 9:
A 6-year-old boy sustains a supracondylar fracture of the humerus. The 2 fragments are not completely displaced, but there is some overlap of the medial column and a gap on the lateral column of the distal humerus. Baumannâ s angle measures 85°. The alignment on the lateral film shows no significant translation, but approximately 15° of increased extension. The recommended treatment is:
Options:
- Accept this and treat in a long arm cast
- Closed reduction with supination of the forearm and application of long arm cast
- Closed reduction with the elbow in extension to better monitor the angulation
- Closed reduction and percutaneous pin fixation
- Open reduction and medial and lateral plate fixation
Correct Answer: Closed reduction with supination of the forearm and application of long arm cast
Explanation:
Closed reduction should allow regain of alignment and percutaneous pin fixation will allow it to be maintained. The elbow is in 10°-15° of varus and this will be an objectionable appearance in the future. Supination will increase the varus. Extension will exacerbate the deformity seen on the lateral and will cause further loss of contact of the fracture fragments. Medial and lateral plate fixation is needed in adolescents and adults with intercondylar fractures to allow early range of movement but is excessive treatment for this fracture in young children.
Question 10:
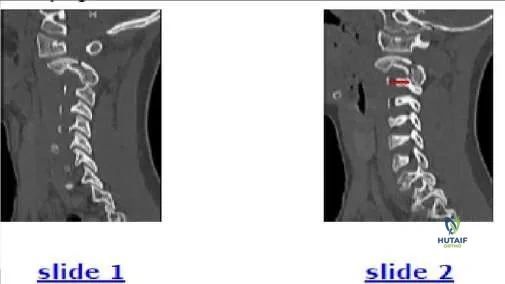
The 7-year-old patient shown in this image (Slide 1) is most likely presenting with:
Options:
- Atlas fracture
- Spondylolysis of the axis
- Facet subluxation
- Fracture of C 3
- Fracture and subluxation
Correct Answer: Fracture and subluxation
Explanation:
This patient has a spondylolisthesis of the axis, which is also known as a Hangmanâ s fracture. Additionally, a subluxation of the C 2-C 3 facet is present on the right side. Such a subluxation often accompanies a Hangmans fracture. The comparison image (Slide 2) of the opposite facet is shown as a reference to demonstrate the normal alignment.
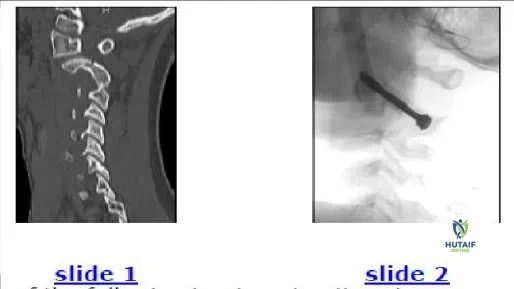
Question 11:
Which of the following treatment options is recommended for the patient shown in the image (Slide 1, Slide 2):
Options:
- Halo-vest immobilization
- Minerva cast immobilization
- Soft cervical collar
- Open reduction and internal fixation
- Atlantoaxial arthrodesis
Correct Answer: Open reduction and internal fixation
Explanation:
Treatment must address the fracture of the C 2 pars interarticularis and the C 2-C 3 facet subluxation. Options include traction to reduce the subluxation followed by external immobilization, or open reduction of the facet subluxation, which includes the opportunity to internally fix the fracture. Traction failed in this patient because the fracture eliminates a means to pull
on the arch of C 2. If facet subluxation is not present, then a cervicothoracic orthosis such as a Philadelphia collar is adequate for healing of the C 2 spondylolysis.
Question 12:
Flexion-type supracondylar fractures of the distal humerus in children are characterized by which of the following when compared to extension-type injuries:
Options:
- Younger age at presentation
- Higher risk of ulnar nerve injury
- Higher risk of anterior interosseous nerve injury
- Lower risk of needing open reduction
- Greater frequency of occurrence
Correct Answer: Higher risk of ulnar nerve injury
Explanation:
Flexion-type supracondylar fractures of the distal humerus in children include the following characteristics: Frequency is less than one-tenth as that of extension-type supracondylar fractures Tend to occur in older children Lower risk of anterior interosseous nerve injury Higher risk of ulnar nerve injury More often require open reduction
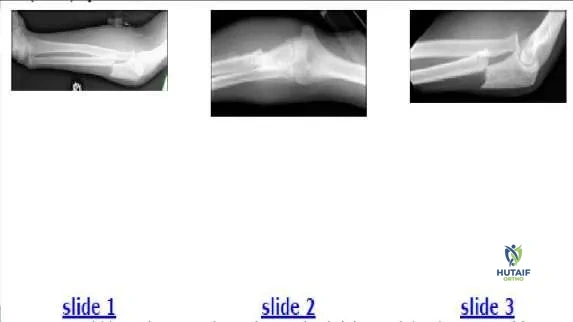
Question 13:
The 12-year-old boy shown in the radiographs (Slide 1, Slide 2) sustained his injury during a motor vehicle accident. Which of the following most accurately describes the injury:
Options:
- Oblique proximal ulna metaphyseal fracture
- Oblique proximal ulna fracture and elbow dislocation
- Type 1 Monteggia fracture
- Type I Galeazzi fracture
- Maisonneuve fracture
Correct Answer: Type 1 Monteggia fracture
Explanation:
This patient has a proximal ulna fracture and an anterior dislocation of the radial head. The ulna-trochlea relationship is intact. On the lateral film, the
radial head does not articulate with the capitellum. On the anteroposterior film, the radial head points to the capitellum, but the joint space is absent in contrast to that of the ulna-trochlear joint, which is normal. This injury is a type 1 (anterior) Monteggia fracture. The dislocation is clearly visible on Slide 3. A Galeazzi fracture refers to a distal radioulnar dislocation with a radial fracture. A Maisonneuve fracture is a related concept in the lower extremity: a proximal fibular fracture with an ankle mortise injury.
Question 14:
A 12-year-old boy sustained the injury shown (Slide 1, Slide 2, and Slide 3). A postreduction film is also presented (Slide 4). Which of the following treatments is the most likely to produce satisfactory results:
Options:
- Accept reduction and continue immobilization for 6 weeks
- Increase pronation of forearm and reapply cast
- Increase elbow extension and reapply cast
- Plate fixation of ulna
- Stabilize radiocapitellar joint with pin
Correct Answer: Plate fixation of ulna
Explanation:
This patient has a type 1 (anterior) Monteggia fracture. The radial head is not reduced in the splint. Although supination and flexion may stabilize the radius, the radius remained unstable in this patient because it was dislocated with only a slight offset of the ulna. Plate fixation of the ulna is more likely to stabilize the radius in a patient with this injury. After the ulna is fixed with a plate (Slide 5), the radial head cannot be dislocated. Radiocapitellar pinning should be used only as a final option because of the associated risks of stiffness and breakage.
Question 15:
A 7-year-old boy is intubated after being involved in a motor vehicle accident. His lateral cervical film (Slide 1) reveals a:
Options:
- Normal study
- Jefferson fracture
- Hangmanâ s fracture
- Occiput-C 2 subluxation
- Subaxial subluxation
Correct Answer: Occiput-C 2 subluxation
Explanation:
Extensive prevertebral soft tissue swelling is present. This patient received an injury that disrupted the ligaments of the atlantooccipital and atlantoaxial joint. Additionally, he has a congenital synchondrosis of the C1 ring. The dens-basion distance (dens to the anterior rim of the foramen magnum) is 13 mm; the normal distance is less than 10 mm to 12 mm. The patient is pentaplegic. Three-dimensional computed tomography scans (Slide 2, Slide 3) are presented.
Question 16:
The images presented (Slide 1, Slide 2) depict which process:
Options:
- Spondylolisthesis
- Spondylolysis (pars defect)
- Aneurysmal bone cyst
- Herniated nucleus pulposus
- Degenerative disk disease
Correct Answer: Spondylolysis (pars defect)
Explanation:
The images presented depict a pars interarticularis fracture of the third lumbar vertebra.
Question 17:
Patients who have had a unilateral slipped capital femoral epiphysis (SC FE) are at what odds of a contralateral slip compared to the general population:
Options:
- 2 times
- 20 times
- 200 times
- 2,000 times
- 20,000 times
Correct Answer: 2,000 times
Explanation:
Patients who have presented with a unilateral SC FE are at approximately 2,000 times the risk of a contralateral slip compared to the general population. The risk of a contralateral slip in a juvenile is approximately 1/10,000, which provides justification for prophylactic pinning of a second side if a surgeon thinks it is warranted.
Question 18:
Which of the following conditions is represented in the clinical photographs (Slide 1, Slide 2):
Options:
- Ectrodactyly
- C onstriction band syndrome
- Macrodactyly
- Microdactyly
- C lubfoot
Correct Answer: Ectrodactyly
Explanation:
This patient has ectrodactyly, which is a condition characterized by the central absence of rays. Ectrodactyly, also known as cleft foot or lobster- claw, may affect the upper or lower extremities. The incidence is rare (approximately 1/90,000 live births). The condition may result from a defect in the apical ectodermal ridge. Associated anomalies are not always present but may include cleft hand, deafness, tibial hemimelia, or urinary tract anomalies. Patients with ectrodactyly have nearly normal function, as long as the foot is not so wide as to prohibit normal shoe wear. If shoe wear is difficult, then the foot can be reconstructed using flaps to close the cleft and metatarsal osteotomies as indicated.
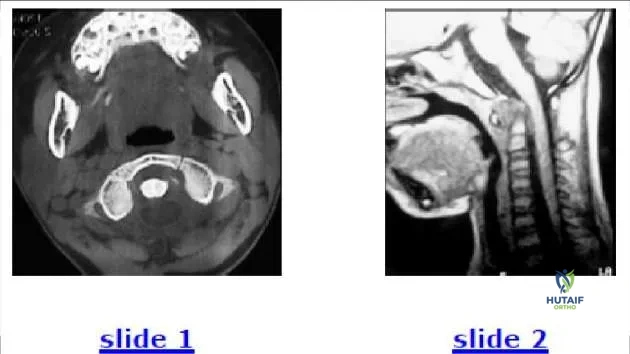
Question 19:
A 6-year-old child is involved in a motor vehicle accident. What injury is demonstrated by the computed tomography (C T) (Slide
Options:
- Jefferson fracture
- Transverse ligament injury
- Odontoid fracture
- Hangmans fracture
- Pseudosubluxation
Correct Answer: Transverse ligament injury
Explanation:
This patient has an avulsion injury of the transverse ligament of the atlas. The bony avulsion is visible from its attachment to the left lateral mass and allows the atlas to move forward in relation to the axis. Hematoma and occiptocervical flexion is visible on the MRI. If it were an
odontoid injury, the odontoid would still have a normal relationship to the ring of C 1 on the C T. Treatment involves reduction and fusion of C 1-C 2.
Question 20:
The radiograph (Slide 1) of an 11-year-old boy with significant leg pain is presented. No other abnormalities are found during the patientâ s history or physical examination. The most likely diagnosis is:
Options:
- Osteomyelitis
- Fibrous dysplasia
- Enchondroma
- Unicameral bone cyst
- Ewing sarcoma
Correct Answer: Fibrous dysplasia
Explanation:
Fibrous dysplasia is chronically expansile with vague transition to normal bone and a â ground-glassâ appearance. These characteristics differentiate fibrous dysplasia from aneurysmal and unicameral bone cysts. Additionally, the lack of periosteal reaction differentiates fibrous dysplasia from malignancy or osteomyelitis. The patients magnetic resonance image (Slide 2) is also provided.

 these fractures so that the patient and family may be given proper activity restrictions and expectations for improvement.
these fractures so that the patient and family may be given proper activity restrictions and expectations for improvement.
 When seen in some projections, the more distal extent of the physis may produce a lucent line. The smooth nature and characteristic location of the line should allow surgeons to make the correct interpretation. The two ossification centers of the humeral head may be misinterpreted as a fracture. This patient had a greenstick fracture of the clavicle (not included on this field), which was not noticed, and a humeral fracture was incorrectly diagnosised.
When seen in some projections, the more distal extent of the physis may produce a lucent line. The smooth nature and characteristic location of the line should allow surgeons to make the correct interpretation. The two ossification centers of the humeral head may be misinterpreted as a fracture. This patient had a greenstick fracture of the clavicle (not included on this field), which was not noticed, and a humeral fracture was incorrectly diagnosised.
 on the arch of C 2. If facet subluxation is not present, then a cervicothoracic orthosis such as a Philadelphia collar is adequate for healing of the C 2 spondylolysis.
on the arch of C 2. If facet subluxation is not present, then a cervicothoracic orthosis such as a Philadelphia collar is adequate for healing of the C 2 spondylolysis.
 radial head does not articulate with the capitellum. On the anteroposterior film, the radial head points to the capitellum, but the joint space is absent in contrast to that of the ulna-trochlear joint, which is normal. This injury is a type 1 (anterior) Monteggia fracture. The dislocation is clearly visible on Slide 3. A Galeazzi fracture refers to a distal radioulnar dislocation with a radial fracture. A Maisonneuve fracture is a related concept in the lower extremity: a proximal fibular fracture with an ankle mortise injury.
radial head does not articulate with the capitellum. On the anteroposterior film, the radial head points to the capitellum, but the joint space is absent in contrast to that of the ulna-trochlear joint, which is normal. This injury is a type 1 (anterior) Monteggia fracture. The dislocation is clearly visible on Slide 3. A Galeazzi fracture refers to a distal radioulnar dislocation with a radial fracture. A Maisonneuve fracture is a related concept in the lower extremity: a proximal fibular fracture with an ankle mortise injury.

 odontoid injury, the odontoid would still have a normal relationship to the ring of C 1 on the C T. Treatment involves reduction and fusion of C 1-C 2.
odontoid injury, the odontoid would still have a normal relationship to the ring of C 1 on the C T. Treatment involves reduction and fusion of C 1-C 2.