Surgical Dislocation of the Hip: A Masterclass in Femoroacetabular Impingement Correction
Key Takeaway
This masterclass provides an immersive, step-by-step guide to surgical hip dislocation, a powerful technique for treating complex hip pathologies like femoroacetabular impingement (FAI). We cover detailed anatomy, meticulous patient positioning, granular intraoperative execution, and crucial pearls to ensure successful outcomes while preserving the femoral head's vascularity. Fellows will gain insights into managing cam and pincer lesions.
Introduction and Epidemiology
Surgical dislocation of the hip, pioneered by Reinhold Ganz and colleagues in 2001, represents a landmark advancement in joint-preserving hip surgery. This technique allows for safe, comprehensive, 360-degree access to the femoral head and acetabulum without compromising the delicate vascular supply to the proximal femur. The procedure is primarily utilized to treat complex structural abnormalities of the hip, most notably femoroacetabular impingement (FAI), but also serves as an essential approach for labral tears, chondral injuries, femoral head fractures (Pipkin lesions), selected acetabular fractures, excision of intra-articular tumors, and the reduction of acute, severe slipped capital femoral epiphysis (SCFE).
Femoroacetabular impingement is recognized as a primary etiology for the premature development of osteoarthritis in the non-dysplastic hip. Epidemiological data suggest that asymptomatic cam deformities are prevalent in up to 30 percent of the general population and significantly higher in athletic cohorts participating in high-impact, multidirectional sports. However, the transition from asymptomatic morphological variant to symptomatic FAI depends on a complex interplay of pelvic kinematics, activity level, and the severity of the osseous mismatch.
The primary advantage of surgical hip dislocation over arthroscopic management is the ability to perform a dynamic, functional assessment of motion intraoperatively. Because the majority of reoperations following FAI treatment stem from under-resection or over-resection of the deformity, direct visualization of the impingement-free arc of motion is the most critical step in optimizing femoral head-neck offset. Furthermore, the comprehensive nature of this approach facilitates the simultaneous assessment and treatment of extra-articular sources of impingement, such as anterior inferior iliac spine (AIIS) or subspinous impingement.
Surgical Anatomy and Biomechanics
The foundational principle of surgical hip dislocation relies on an intimate understanding of the vascular anatomy of the proximal femur. The blood supply to the femoral head is predominantly derived from the medial femoral circumflex artery (MFCA).

The MFCA originates from the profunda femoris and courses posteriorly. Its deep branch passes between the pectineus and iliopsoas, continuing posteriorly between the obturator externus and adductor brevis. Crucially, the vessel then travels posterior to the obturator externus tendon and anterior to the quadratus femoris. It crosses the posterior capsule of the hip joint, giving rise to the terminal subsynovial retinacular vessels that penetrate the femoral head at the head-neck junction.

During a surgical dislocation utilizing the trochanteric flip osteotomy, the intact short external rotator muscles—most notably the obturator externus—act as a protective soft-tissue hinge. This muscular tether prevents tension on the MFCA during anterior dislocation of the femoral head.
Biomechanics of Femoroacetabular Impingement
Anatomic deformity in FAI leads to abnormal contact between the proximal femur and the acetabular rim at the terminal extent of motion. This repetitive collision damages the soft tissue structures within the joint through distinct biomechanical pathways.

In cam impingement, an abnormal osseous prominence at the anterolateral femoral head-neck junction (decreased offset) is forcefully driven into the acetabulum during flexion and internal rotation. This creates massive shear forces at the chondrolabral junction, leading to an outside-in delamination of the articular cartilage from the subchondral bone, often leaving the labrum initially intact but detached from the articular surface.
Pincer impingement occurs due to global or focal overcoverage of the acetabular rim (e.g., coxa profunda, acetabular retroversion). The biomechanical insult here is linear contact. The prominent acetabular rim impacts the femoral neck, crushing the intervening labrum. With continued motion, the femoral head is levered out of the acetabulum, creating a contrecoup chondral lesion in the posteroinferior acetabulum. Both cam and pincer morphologies frequently coexist, leading to a complex pattern of chondrolabral destruction.
Indications and Contraindications
The indications for surgical hip dislocation have expanded as the understanding of hip pathomechanics has evolved. While arthroscopy has largely supplanted open surgery for isolated, mild-to-moderate FAI, surgical dislocation remains the gold standard for complex, multi-planar deformities, severe SCFE, and cases requiring extensive intra-articular access.
Operative Indications and Contraindications Summary
| Category | Specific Conditions |
|---|---|
| Primary Indications | Complex FAI (large cam lesions spanning posterior/inferior), severe acetabular retroversion requiring rim trimming, acute/severe SCFE (modified Dunn procedure), Legg-Calvé-Perthes disease sequelae, Pipkin femoral head fractures, synovial chondromatosis. |
| Relative Indications | Revision FAI surgery (failed arthroscopy with extensive capsular scarring), extra-articular impingement (AIIS, greater trochanteric impingement), prophylactic pinning of the contralateral hip in SCFE. |
| Absolute Contraindications | Advanced osteoarthritis (Tönnis grade 2 or 3), active joint infection, medical comorbidities precluding prolonged anesthesia. |
| Relative Contraindications | Severe osteopenia/osteoporosis (risk of trochanteric nonunion), heavy tobacco use (impairs osteotomy healing), advanced age (>55 years with degenerative changes). |


Early surgical intervention is paramount in physically active adolescents and young adults. The natural history of untreated FAI, particularly the pistol grip deformity of the femoral head, is a predictable progression to early arthrosis. End-stage osteoarthrosis of the hip, historically categorized as idiopathic, is now widely accepted to be the sequela of subtle morphological abnormalities including FAI, mild developmental dysplasia of the hip (DDH), and subclinical SCFE.
Pre Operative Planning and Patient Positioning
Thorough preoperative evaluation begins with a detailed history and physical examination. Patients typically present with insidious onset, activity-related groin pain. Exacerbating factors often include prolonged sitting, driving, or pivoting sports. A classic physical finding is the positive impingement test (FADIR: Flexion, Adduction, Internal Rotation), which reproduces sharp groin pain. The Drehmann sign (obligatory external rotation during passive hip flexion) is highly suggestive of a large cam lesion or chronic SCFE.
Radiographic Evaluation
Standard radiographic assessment must include a weight-bearing anteroposterior (AP) pelvis, a Dunn lateral, a cross-table lateral, and a false profile view.

The AP pelvis is scrutinized for acetabular version (crossover sign, ischial spine sign, posterior wall sign), lateral center-edge angle, and Tönnis grade. The lateral views are essential for calculating the alpha angle (normal < 50-55 degrees) and assessing the anterior femoral head-neck offset.

Magnetic Resonance Arthrography (MRA) with gadolinium is the imaging modality of choice for evaluating the integrity of the labrum and articular cartilage. Computed Tomography (CT) with 3D reconstruction is highly recommended for precise preoperative mapping of the osseous impingement, allowing the surgeon to template the exact location and depth of the planned osteochondroplasty.
Patient Positioning
The patient is placed in the lateral decubitus position on a standard radiolucent operating table. Rigid pelvic fixation using a bean bag or pelvic positioners is critical to maintain true lateral orientation during vigorous dislocation maneuvers. The operative leg is draped free to allow for a full, unrestricted range of motion intraoperatively. A sterile pouch may be utilized anteriorly to support the leg during the dislocation phase.

Detailed Surgical Approach and Technique
The surgical dislocation approach requires meticulous attention to soft tissue planes and osseous landmarks to preserve the MFCA.
Incision and Superficial Dissection
A straight lateral incision is made centered over the greater trochanter, extending proximally toward the iliac crest and distally along the femoral shaft.

The subcutaneous tissues are divided, and the fascia lata is incised longitudinally in line with the skin incision. Proximally, the fascial split is directed slightly posteriorly to split the fibers of the gluteus maximus, exposing the underlying greater trochanter and the vastus lateralis.
Trochanteric Flip Osteotomy
The critical step in this approach is the digastric trochanteric flip osteotomy. The goal is to osteotomize the greater trochanter while maintaining the continuity of the gluteus medius, gluteus minimus, and vastus lateralis attachments on the mobile fragment.

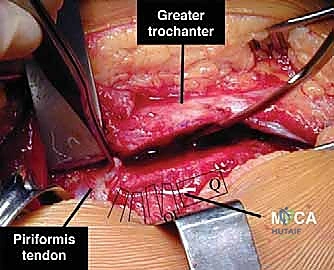
The posterior border of the gluteus medius is identified. The interval between the gluteus medius and the piriformis is developed. The osteotomy is initiated just posterior to the posterior border of the gluteus medius and exits distally at the vastus ridge. The osteotomy must be superficial to the piriformis fossa to leave the piriformis tendon and the short external rotators attached to the stable proximal femur. The thickness of the trochanteric wafer is typically 1.0 to 1.5 cm.

Once the osteotomy is complete, the mobile trochanteric fragment is mobilized anteriorly. The fibers of the gluteus minimus are carefully peeled off the superior hip capsule. This anterior retraction exposes the entire superior and anterior hip capsule.
Capsulotomy
Meticulous capsulotomy design is essential to avoid transecting the retinacular vessels. The retinacular vessels run along the posterosuperior aspect of the femoral neck.

A Z-shaped capsulotomy is utilized for the right hip, and a reverse Z-shaped capsulotomy is used for the left hip. The first limb is made anterolaterally along the long axis of the femoral neck. The proximal limb is directed anteriorly, parallel to the acetabular rim, staying 1 to 2 cm away from the labrum to leave a cuff for subsequent repair. The distal limb is directed posteriorly along the intertrochanteric line.

This specific capsulotomy configuration ensures that the posterosuperior capsule, which houses the critical blood supply, remains completely undisturbed.
Surgical Dislocation
Following capsulotomy, the hip is prepared for anterior dislocation. The ligamentum teres must be divided. This is accomplished by applying gentle traction and external rotation, allowing the introduction of curved scissors or a specialized ligamentum teres cutter into the joint.

Once the ligamentum teres is transected, the hip is dislocated anteriorly by flexing the hip to 90 degrees, externally rotating, and adducting the leg. The femoral head is delivered into the surgical field, providing a 360-degree view of the articular surface and the head-neck junction.

During this maneuver, the intact obturator externus and quadratus femoris act as a hinge, preventing any tension on the MFCA.
Intraoperative Assessment and Osteochondroplasty
With the hip dislocated, a comprehensive assessment of the labrum, acetabular cartilage, and femoral head morphology is performed.

For cam impingement, the loss of offset at the anterolateral head-neck junction is identified. Spherical templates can be utilized to precisely demarcate the boundaries of the non-spherical portion of the femoral head.

High-speed burrs or sharp curved osteotomes are used to perform the osteochondroplasty. The goal is to recreate a normal concavity at the head-neck junction. It is critical not to resect more than 30 percent of the diameter of the femoral neck to avoid significantly weakening the proximal femur and risking an iatrogenic femoral neck fracture.

If pincer impingement is present, the prominent acetabular rim is trimmed. The labrum is typically detached, the underlying osseous overcoverage is resected, and the labrum is subsequently refixed to the new rim using suture anchors.

The most crucial step of the procedure is the dynamic functional assessment. The hip is reduced, and the leg is moved through a full range of motion, specifically testing flexion, adduction, and internal rotation to ensure that all impingement has been eliminated and the osseous recontouring is sufficient.
Closure and Trochanteric Fixation
Once optimal kinematics are confirmed, the joint is thoroughly irrigated to remove all osseous debris.

The capsule is loosely approximated with absorbable sutures. A tight capsular closure must be avoided to prevent stricture or tension on the retinacular vessels.

The trochanteric fragment is reduced to its anatomical bed. Fixation is typically achieved using two or three 3.5 mm or 4.5 mm fully threaded cortical screws directed medially and slightly proximally toward the lesser trochanter.


The fascia lata is closed securely, followed by routine subcutaneous and skin closure.
Complications and Management
While surgical dislocation is highly effective, it is a major open procedure with specific inherent risks. Meticulous surgical technique is required to minimize morbidity.
Complications and Salvage Strategies
| Complication | Incidence | Etiology and Management Strategy |
|---|---|---|
| Avascular Necrosis (AVN) | < 1% | Etiology: Violation of the MFCA or retinacular vessels during deep dissection or capsulotomy. Management: Early stages may be observed or treated with core decompression. Late-stage collapse requires Total Hip Arthroplasty (THA). |
| Trochanteric Nonunion | 2 - 5% | Etiology: Inadequate fixation, early weight-bearing, smoking, or excessive osteotomy thickness. Management: Revision open reduction internal fixation (ORIF) utilizing a tension band construct or trochanteric claw plate, often supplemented with bone grafting. |
| Heterotopic Ossification (HO) | 5 - 10% | Etiology: Extensive muscle dissection and bone debris. Management: Prophylaxis is critical (Ind |
Clinical & Radiographic Imaging
You Might Also Like

