Supracondylar Humeral Osteotomy: A Masterclass in Cubitus Varus Correction
Key Takeaway
This masterclass details supracondylar humeral osteotomy for cubitus varus. We cover comprehensive anatomy, meticulous preoperative templating, and step-by-step intraoperative execution. Learn precise K-wire fixation, managing lateral condylar prominence, and critical neurovascular protection. Postoperative care and complication strategies are also thoroughly discussed, ensuring fellows gain a complete understanding of this challenging pediatric elbow deformity correction.
Introduction and Epidemiology
Cubitus varus, frequently referred to as a "gunstock deformity," is a complex three-dimensional deformity of the distal humerus characterized by a loss of the physiologic valgus carrying angle. Historically, prior to the widespread adoption of modern percutaneous pinning techniques for pediatric supracondylar humerus fractures, cubitus varus was the most frequently encountered complication. Historical literature cites an average incidence of 30%, with some series reporting rates as high as 60% following non-operative management or inadequate closed reduction and casting.
With the advent of closed reduction and percutaneous pinning (CRPP) as the gold standard for displaced supracondylar humerus fractures, the incidence of cubitus varus has decreased significantly but remains a recognized complication, particularly in cases of severe comminution, medial column collapse, or technical errors during index fixation.

While the deformity is often primarily perceived as a cosmetic issue by patients and their families, contemporary orthopedic understanding recognizes the long-term biomechanical consequences of the altered mechanical axis. The deformity is rarely isolated to the coronal plane; it typically presents as a triplanar malunion consisting of coronal varus angulation, sagittal extension, and axial internal rotation. Understanding this triplanar nature is critical for the orthopedic surgeon when evaluating the necessity and methodology of a corrective supracondylar humeral osteotomy.
Pathogenesis of the Deformity
Cubitus varus occurs predominantly as a sequela of a malunited supracondylar humerus fracture. The primary structural driver is coronal varus angulation of the distal humeral metaphysis. This varus angulation is most frequently caused by medial column comminution at the time of the initial fracture, which allows the distal fragment to collapse into varus either before or during the healing phase. Less commonly, varus angulation can be iatrogenically induced by lateral gaping at the fracture site during overzealous reduction or inadequate stabilization.
Unequal growth of the distal humerus can also contribute to cubitus varus, particularly if there is a medial physeal growth arrest following the initial trauma. However, true physeal arrest is rare in supracondylar fractures compared to lateral condyle fractures. The coexisting deformities of extension and internal rotation of the distal fragment compound the clinical appearance and biomechanical derangement. The internal rotation deformity, while often masked by the compensatory external rotation of the shoulder joint, exacerbates the apparent varus when the arm is extended and internally rotated.
Surgical Anatomy and Biomechanics
A thorough understanding of the osteology, neurovascular topography, and altered biomechanics of the distal humerus is requisite for executing a safe and effective corrective osteotomy.
Osteology of the Distal Humerus
The distal humerus is anatomically structured as a robust triangle comprising two structural columns of bone—medially and laterally—connected by the articular block (the trochlea and capitellum). The olecranon fossa posteriorly and the coronoid fossa anteriorly separate these two structural columns, creating a remarkably thin area of bone centrally.

In the pediatric population, the cortices of the distal humerus are significantly thinner than in adults, and the anteroposterior (AP) diameter of the distal humerus is decreased. This anatomical nuance dictates the selection of fixation constructs, as the limited bone stock in the distal fragment can compromise screw purchase or K-wire stability during an osteotomy. The orientation of the articular surface normally exhibits approximately 4 to 8 degrees of valgus relative to the humeral shaft, which is the primary parameter lost in cubitus varus.
Neurovascular Considerations
The neurovascular structures traversing the elbow joint are at significant risk during both the initial trauma and the subsequent corrective osteotomy.
The median nerve and brachial artery run along the medial border of the biceps brachii muscle in the upper arm. As they transition distally, they lie anterior and slightly medial in the cubital fossa, crossing the elbow joint anterior to the brachialis muscle.
The radial nerve enters the anterior compartment of the arm in the distal third of the upper arm after piercing the lateral intermuscular septum. It travels distally in the interval between the brachialis and brachioradialis muscles over the anterolateral distal humerus before entering the supinator muscle in the proximal forearm. The radial nerve is particularly vulnerable during the lateral approach to the distal humerus. Historical reports have even documented the radial nerve becoming encased within the fracture callus of a healing supracondylar fracture.
The ulnar nerve resides in the posterior compartment of the arm, passing posterior to the medial epicondyle within the cubital tunnel. Its position is critical in the context of cubitus varus, as the altered biomechanics can lead to chronic nerve irritation.
Biomechanics of Secondary Instability
The natural history of cubitus varus was historically considered benign, viewed as a static cosmetic deformity that did not evolve unless complicated by a medial physeal disturbance. However, modern biomechanical studies have elucidated the long-term functional consequences of the altered mechanical axis.

Significant cubitus varus medialize the mechanical axis of the upper extremity. This medial shift alters the line of pull of the triceps muscle. As the triceps vector shifts medially, it creates a repetitive supinating moment on the ulna during active elbow extension. Over time, this chronic supinating force attenuates the lateral ulnar collateral ligament (LUCL) complex, potentially leading to posterolateral rotatory instability (PLRI).
Furthermore, the medial shift of the olecranon within the olecranon fossa can cause chronic malpositioning of the medial head of the triceps. This structural shift can result in dynamic snapping of the triceps over the medial epicondyle and subsequent compression or friction of the ulnar nerve, manifesting clinically as tardy ulnar nerve palsy. Additionally, children with cubitus varus exhibit a mechanically increased risk of sustaining subsequent lateral condyle fractures due to the altered transmission of forces through the elbow joint during falls.
Indications and Contraindications
The decision to proceed with a supracondylar humeral osteotomy must be carefully weighed, balancing the complexity of the procedure against the patient's symptoms and the natural history of the deformity.
While the appearance of the deformity remains the major concern for parents and patients, functional deficits are the primary absolute indications for surgical intervention. The deformity is often not fully appreciated until several months after the index fracture heals and the elbow flexion contracture—a common sequela of casting—resolves.
| Indication Category | Specific Clinical Findings | Recommendation Level |
|---|---|---|
| Operative Indications | Tardy ulnar nerve palsy | Absolute |
| Symptomatic posterolateral rotatory instability (PLRI) | Absolute | |
| Chronic lateral elbow pain | Relative / Strong | |
| Severe cosmetic deformity causing psychosocial distress | Relative | |
| Progressive deformity (indicating physeal arrest) | Absolute | |
| Non-Operative Indications | Mild, asymptomatic deformity (<10 degrees varus) | Recommended |
| Lack of functional impairment or pain | Recommended | |
| Patient/family unwilling to accept surgical risks | Absolute | |
| Contraindications | Active local or systemic infection | Absolute |
| Poor soft tissue envelope around the elbow | Relative | |
| Severe pre-existing elbow stiffness | Relative |
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is the cornerstone of a successful supracondylar osteotomy. The triplanar nature of the deformity requires comprehensive clinical and radiographic evaluation to determine the exact geometry of the corrective wedge.
Clinical Evaluation
A detailed history is essential to understand parental and patient expectations. The surgeon must clearly delineate that the primary goal of surgery is functional restoration and prevention of late sequelae, with cosmesis being a secondary benefit.
Physical examination must quantify the varus change in the carrying angle compared to the contralateral, unaffected extremity. The difference in carrying angle between the affected and unaffected side dictates the magnitude of coronal correction required. Elbow and forearm range of motion must be meticulously documented. Hyperextension of the elbow indicates a coexisting sagittal plane extension deformity at the malunion site, which must be addressed during the osteotomy to restore normal flexion kinematics.
A loss of external rotation can be attributed to shoulder pathology but, in the context of cubitus varus, is frequently due to an internal rotation malunion of the distal humerus. A thorough neurological examination is mandatory, with specific attention to ulnar nerve function (Tinel's sign, intrinsic muscle strength, sensory changes) to rule out tardy ulnar nerve palsy.
Radiographic Analysis and Templating
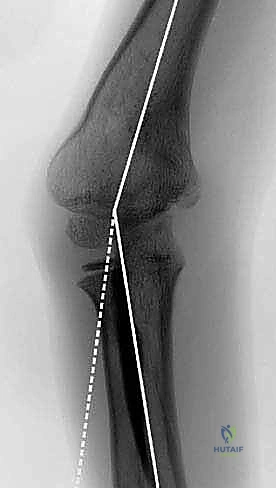
Standard plain anteroposterior (AP) and lateral radiographs of the affected elbow are the initial diagnostic steps. However, standard AP views are often distorted by the internal rotation and extension deformities.

To accurately plan the osteotomy, an AP radiograph of both the affected and unaffected elbows in full extension and maximal supination must be obtained. This view should include the distal humerus, forearm, and wrist to allow for precise measurement of the humeroulnar angle.
The Baumann angle (the angle between the longitudinal axis of the humeral shaft and the physeal line of the lateral condyle) is a critical radiographic parameter. A normal Baumann angle is typically between 70 and 75 degrees. An increase in this angle correlates with varus deformity.
Templating involves calculating the exact angle of the wedge to be resected. For a standard lateral closing wedge osteotomy, the angle of the wedge is equal to the varus deformity of the affected side plus the normal valgus carrying angle of the contralateral side.
Advanced imaging, such as magnetic resonance imaging (MRI) or computed tomography (CT) with 3D reconstruction, may be indicated in complex cases, particularly if a physeal bar is suspected or if the triplanar deformity is severe and requires a custom cutting guide or a multi-planar dome osteotomy.
Patient Positioning and Setup
The patient is typically positioned supine on the operating table. The affected arm can be placed on a radiolucent hand table, allowing for unencumbered access to the lateral and anterior aspects of the elbow. Alternatively, the arm can be draped free and brought across the patient's chest.

A sterile tourniquet is highly recommended to provide a bloodless surgical field, which is critical for identifying and protecting the radial nerve. Intraoperative fluoroscopy is mandatory; the C-arm should be positioned to allow for easy AP and lateral imaging without compromising the sterile field.
Detailed Surgical Approach and Technique
Multiple osteotomy techniques have been described, including the lateral closing wedge (French osteotomy), dome osteotomy, step-cut osteotomy, and pentalateral osteotomy. The lateral closing wedge remains the most common and technically straightforward approach, though it requires careful execution to avoid a secondary lateral condylar prominence.
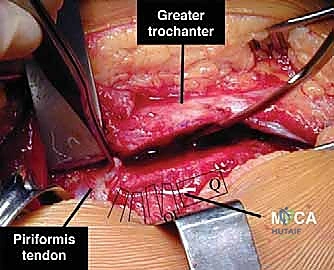
Surgical Exposure and Internervous Planes
A lateral approach to the distal humerus is utilized. An incision is made along the lateral supracondylar ridge, extending distally towards the lateral epicondyle.

The superficial dissection identifies the interval between the triceps posteriorly and the brachioradialis and extensor carpi radialis longus (ECRL) anteriorly. This is an internervous plane, as the triceps is innervated by the radial nerve (branches given off proximally), and the brachioradialis/ECRL are innervated by the radial nerve distally.
The radial nerve must be meticulously identified and protected. It is found in the anterior aspect of the wound, lying between the brachialis and brachioradialis. Once identified, a vessel loop can be placed around the nerve for continuous visualization and protection. The periosteum over the lateral distal humerus is incised, and subperiosteal dissection is carried out anteriorly and posteriorly. Hohmann retractors are carefully placed to expose the metaphysis while protecting the anterior neurovascular structures and the posterior triceps.
Osteotomy Execution
Using the preoperative template, the osteotomy cuts are marked on the bone using electrocautery or a sterile marker. K-wires can be placed as cutting guides to ensure the correct trajectory.

The distal cut is typically made parallel to the elbow joint line (transverse axis of the condyles) to ensure the articular surface remains horizontal after correction. The proximal cut is made at an angle relative to the distal cut, equal to the calculated wedge angle.
An oscillating saw is used to perform the osteotomy. Copious irrigation is utilized to prevent thermal necrosis of the bone. In a traditional closing wedge osteotomy, the medial cortex is left intact to serve as a hinge, which provides inherent stability. However, if correction of internal rotation or significant extension is required, the medial hinge must be completed to allow for multi-planar manipulation.
Deformity Correction and Fixation
Once the wedge of bone is removed, the osteotomy is closed by applying a valgus force to the distal fragment. If a medial hinge is intact, it will plastically deform. If the hinge is cut, the distal fragment must be carefully translated medially as the wedge is closed to prevent the lateral condylar prominence ("lazy S" deformity) that commonly plagues simple closing wedge osteotomies.

Simultaneous correction of the sagittal and axial planes is performed by flexing the distal fragment (to correct extension) and externally rotating it (to correct internal rotation).
Once the desired reduction is achieved and verified clinically by assessing the carrying angle and radiographically via fluoroscopy, fixation is applied.

Fixation options include crossed K-wires, lateral pediatric locking plates, or a combination of both. In younger children with limited bone stock, robust crossed K-wires (typically 2.0 mm or 5/64 inch) may suffice. In older children or adolescents, lateral plate fixation provides superior biomechanical stability, allowing for earlier mobilization and a lower rate of loss of fixation. The plate is contoured to the lateral column, and screws are placed to secure the osteotomy, ensuring no screws penetrate the olecranon or coronoid fossae.
Complications and Management
Supracondylar humeral osteotomies are technically demanding procedures associated with a notable complication profile. Meticulous surgical technique and rigid fixation are paramount to minimizing these risks.

| Complication | Estimated Incidence | Etiology and Management Strategy |
|---|---|---|
| Lateral Condylar Prominence | 20% - 30% | Caused by a simple lateral closing wedge without medial translation of the distal fragment. Management: Medial translation during reduction, or utilize a dome/step-cut osteotomy. Asymptomatic cases require no treatment; symptomatic cases may require lateral condylectomy. |
| Nerve Palsy (Radial) | 2% - 5% | Usually a neuropraxia secondary to retraction or thermal injury during the saw cut. Management: Observation. Most resolve spontaneously within 3-6 months. EMG at 6 weeks if no improvement. |
| Loss of Fixation / Recurrence | 5% - 10% | Inadequate fixation construct, particularly with K-wires in older children. Management: Revision osteotomy with rigid plate fixation. |
| Infection (Pin Tract or Deep) | 1% - 5% | Associated with percutaneous K-wires. Management: Oral antibiotics for superficial pin tract infections. Deep infections require hardware removal (once healed) and surgical debridement. |
| Elbow Stiffness | 5% - 15% | Prolonged immobilization or intra-articular hardware. Management: Aggressive postoperative physical therapy. Hardware removal if impinging. Rarely requires capsular release. |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is dictated by the stability of the fixation construct achieved intraoperatively.
If K-wire fixation is utilized, the patient is typically placed in a long arm cast or well-padded posterior splint with the elbow at 90 degrees of flexion and neutral rotation. Immobilization is maintained for approximately 4 to 6 weeks. Radiographs are obtained at 3 to 4 weeks to assess callus formation. Once bridging callus is evident, the K-wires are removed in the clinic, and active range of motion (AROM) is initiated.
If rigid plate fixation is employed, the period of strict immobilization can be significantly reduced. The patient may be placed in a posterior splint for 1 to 2 weeks to allow for soft tissue healing, followed by an early transition to a hinged elbow brace and initiation of AROM.
Passive stretching and forceful manipulation are strictly contraindicated in the early rehabilitation phase due to the high risk of inducing myositis ossificans or heterotopic ossification around the pediatric elbow. Return to full contact sports and heavy lifting is generally restricted until complete radiographic consolidation and restoration of near-normal strength and range of motion are achieved, typically around 3 to 4 months postoperatively.
Summary of Key Literature and Guidelines
The academic literature surrounding cubitus varus correction has evolved significantly, shifting from purely cosmetic rationales to biomechanical preservation.
Classic studies by O'Driscoll et al. were instrumental in defining the link between long-standing cubitus varus and the subsequent development of posterolateral rotatory instability (PLRI) and tardy ulnar nerve palsy. This literature established the modern functional indications for corrective osteotomy.
The surgical technique has also seen considerable debate. The traditional French lateral closing wedge osteotomy, while technically straightforward, was historically plagued by the "lazy S" deformity. Modern modifications emphasizing medial translation of the distal fragment have mitigated this issue. Comparative studies evaluating the dome osteotomy versus the step-cut osteotomy demonstrate that while dome osteotomies prevent the lateral prominence by maintaining the center of rotation, they are technically more demanding and require highly accurate triplanar cuts.
Current guidelines suggest that the choice of osteotomy should be tailored to the surgeon's experience and the specific geometry of the deformity. However, there is a strong consensus in recent literature advocating for rigid internal fixation (plate and screws) over K-wires in patients nearing skeletal maturity to minimize the risk of loss of correction and allow for early mobilization.
Clinical & Radiographic Imaging
You Might Also Like