ABOS Board Review: SCFE, Köhler's Disease, Dermatomyositis, & Sprengel's Deformity | Part 32
Key Takeaway
ABOS Board Review Part 32 covers key orthopedic and rheumatologic topics essential for board preparation. This module includes detailed questions on Slipped Capital Femoral Epiphysis (SCFE), Köhler's Disease I, Dermatomyositis, and Sprengel's Deformity, focusing on diagnosis, pathophysiology, treatment, and complications. It's designed to enhance your understanding of these critical conditions.
Question 1
A patient is diagnosed with Ewing's sarcoma.
View Answer & Explanation
Correct Answer: B
Rationale: Ewing's sarcoma most commonly presents in the first three decades of life, making it primarily a tumor of children, adolescents, and young adults. It is relatively rare in infants or older adults.
Question 2
A 16-year-old male is diagnosed with Ewing's sarcoma of the femur.
View Answer & Explanation
Correct Answer: C
Rationale: By definition, Ewing's sarcoma is considered a high-grade malignant lesion, reflecting its aggressive biological behavior and propensity for metastasis. It is never considered benign or low-grade.
Question 3
A 13-year-old obese male presents with a 3-week history of left hip pain and a limp. He reports the pain sometimes radiates to his knee. On exam, he has limited internal rotation of the left hip and obligate external rotation with hip flexion. Radiographs show widening of the left capital femoral physis with posterior and inferior displacement of the epiphysis.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical presentation of an obese adolescent male with hip or knee pain, a limp, limited internal rotation, and obligate external rotation with hip flexion is classic for Slipped Capital Femoral Epiphysis. The radiographic findings of physeal widening and posterior/inferior displacement of the epiphysis confirm the diagnosis. Main Distractor: Legg-Calve-Perthes Disease typically affects younger, often thinner, children (4-8 years old) and presents with different radiographic findings (avascular necrosis of the femoral head).
Question 4
A 12-year-old male presents with a painful limp. Physical examination reveals decreased internal rotation and a positive Trendelenburg sign on the affected side. Initial AP pelvis radiograph is equivocal for a slip.
View Answer & Explanation
Correct Answer: A
Rationale: The frog-leg lateral view is the most critical additional radiographic projection for diagnosing Slipped Capital Femoral Epiphysis when the AP view is equivocal. It best visualizes the characteristic posterior and inferior displacement of the femoral epiphysis relative to the metaphysis. Main Distractor: While a CT scan or MRI can confirm the diagnosis, they are not typically the initial or most critical *radiographic* view for diagnosis after an equivocal AP film. An oblique view is less specific than a frog-leg lateral for visualizing the slip.
Question 5
A 14-year-old female presents with right knee pain and a limp. On examination, she has restricted internal rotation of the right hip. Radiographs are obtained.
View Answer & Explanation
Correct Answer: A
Rationale: Klein's line is a key radiographic sign for diagnosing Slipped Capital Femoral Epiphysis on an AP radiograph. A line drawn along the superior border of the femoral neck should normally intersect a portion of the femoral head. In SCFE, due to the posterior and inferior displacement of the epiphysis, this line will fail to intersect the lateral portion of the femoral head, or will intersect a smaller portion than on the contralateral side. Main Distractor: Widening of the physis can be an early sign of SCFE, but Klein's line is a more specific and quantifiable diagnostic criterion for the actual slip.
Question 6
A 10-year-old male presents to the emergency department with acute onset of severe left hip pain after a minor fall. He is unable to bear weight on the left leg. Radiographs confirm a Slipped Capital Femoral Epiphysis.
View Answer & Explanation
Correct Answer: A
Rationale: Slipped Capital Femoral Epiphysis is classified as "unstable" if the patient is unable to bear weight on the affected extremity, even with crutches. This classification is crucial as unstable slips have a significantly higher risk of complications, particularly avascular necrosis. Main Distractor: A "stable" slip is defined by the patient's ability to bear weight on the affected extremity, with or without crutches.
Question 7
A 13-year-old obese male is diagnosed with a stable Slipped Capital Femoral Epiphysis.
View Answer & Explanation
Correct Answer: A
Rationale: The primary pathophysiological mechanism of Slipped Capital Femoral Epiphysis involves a weakening of the hypertrophic zone of the physeal plate, often during periods of rapid growth, combined with increased shear stress across the physis. This shear stress is exacerbated by factors like obesity and the biomechanics of the hip joint. Main Distractor: Avascular necrosis of the femoral head is a serious complication of SCFE, especially unstable slips, but it is not the primary cause of the slip itself.
Question 8
A 9-year-old male, who is significantly underweight for his age, presents with a Slipped Capital Femoral Epiphysis. This presentation is atypical given the usual demographic.
View Answer & Explanation
Correct Answer: A
Rationale: While obesity is the most common risk factor, endocrine disorders are important to consider, especially in atypical presentations of SCFE (e.g., younger age, non-obese, or bilateral slips). Hypothyroidism and growth hormone deficiency are the most commonly associated endocrine conditions that can weaken the physis and predispose to SCFE. Main Distractor: Growth hormone deficiency is also a known risk factor, but hypothyroidism is frequently cited as the most common endocrine abnormality associated with SCFE.
Question 9
A 12-year-old female is diagnosed with a stable, mild Slipped Capital Femoral Epiphysis of the right hip. She is able to ambulate with crutches.
View Answer & Explanation
Correct Answer: A
Rationale: For stable Slipped Capital Femoral Epiphysis, the gold standard of treatment is in situ pinning with a single cannulated screw. This procedure stabilizes the epiphysis, prevents further slippage, and promotes physeal closure, with minimal risk of avascular necrosis. Main Distractor: Open reduction and internal fixation is a more invasive procedure with higher risks, typically reserved for severe or unstable slips, or for addressing complications like femoroacetabular impingement after physeal closure.
Question 10
A 14-year-old male presents to the emergency department with acute onset of severe left hip pain after twisting his leg. He is unable to bear weight. Radiographs confirm an unstable Slipped Capital Femoral Epiphysis.
View Answer & Explanation
Correct Answer: A
Rationale: For unstable Slipped Capital Femoral Epiphysis, the immediate management involves gentle closed reduction (often with a single maneuver) to improve alignment and reduce the risk of avascular necrosis, followed by immediate in situ pinning. Aggressive reduction maneuvers should be avoided due to the high risk of further vascular compromise. Main Distractor: Immediate open reduction and internal fixation is generally avoided for acute unstable slips due to increased morbidity and risk of avascular necrosis compared to gentle closed reduction and pinning.
Question 11
A 13-year-old male undergoes surgical treatment for an unstable Slipped Capital Femoral Epiphysis.
View Answer & Explanation
Correct Answer: A
Rationale: Avascular necrosis (AVN) of the femoral head is the most serious and common complication specifically associated with unstable Slipped Capital Femoral Epiphysis. The vascular supply to the femoral head can be compromised during the initial slip, during reduction attempts, or due to the instability itself, leading to AVN. Main Distractor: Chondrolysis is another potential complication, but AVN is more directly and frequently linked to the instability of the slip and its acute management.
Question 12
A 10-year-old obese male is diagnosed with a stable Slipped Capital Femoral Epiphysis of the right hip. His left hip is asymptomatic.
View Answer & Explanation
Correct Answer: A
Rationale: The risk of a contralateral Slipped Capital Femoral Epiphysis developing in patients with a unilateral slip is significant, ranging from 20-6
Question 12
A 14-year-old obese boy presents with a 3-month history of left hip and knee pain. On examination, he has a painful limp and limited internal rotation of the left hip. Radiographs reveal a stable left Slipped Capital Femoral Epiphysis (SCFE). Which of the following is the MOST appropriate initial management?
View Answer & Explanation
Correct Answer: D
Rationale: For stable SCFE, the standard of care is immediate in situ percutaneous screw fixation to prevent further slippage and promote physeal closure. This minimizes the risk of avascular necrosis and chondrolysis associated with unstable slips or more invasive procedures. Observation is inappropriate as the slip can progress. Open reduction is generally reserved for severe, unstable slips or complications, and carries higher risks. Spica cast or traction are not definitive treatments for SCFE.
Question 12
A 12-year-old girl presents with acute onset of severe right hip pain after a minor fall, rendering her unable to bear weight. Physical examination reveals the right leg is held in external rotation and abduction. Radiographs confirm an unstable Slipped Capital Femoral Epiphysis (SCFE). What is the primary goal of emergent management for this patient?
View Answer & Explanation
Correct Answer: B
Rationale: For unstable SCFE, the primary goal is immediate in situ screw fixation without attempting reduction. Reduction maneuvers, especially forceful ones, significantly increase the risk of avascular necrosis (AVN) due to disruption of the blood supply to the femoral head. Gentle reduction attempts are sometimes considered for very severe slips but are controversial and carry risks. Spica cast, traction, or open reduction are not the immediate primary management for an unstable slip.
Question 12
A 13-year-old boy is diagnosed with a chronic stable Slipped Capital Femoral Epiphysis (SCFE) of the right hip. He undergoes in situ screw fixation. What is the MOST common long-term complication following successful in situ pinning for a stable SCFE?
View Answer & Explanation
Correct Answer: D
Rationale: While avascular necrosis and chondrolysis are serious complications, they are more common with unstable slips or aggressive reduction attempts. For stable SCFE treated with in situ pinning, the most common long-term complication is femoroacetabular impingement (FAI) due to the residual deformity of the femoral head-neck junction. This can lead to labral tears and early osteoarthritis. Contralateral SCFE is a common occurrence (up to 60%) but is a new slip, not a complication of the initial treatment itself. Nonunion is rare.
Question 12
A 10-year-old girl presents with a 6-month history of left knee pain and a progressive limp. Physical examination reveals obligate external rotation with hip flexion and limited internal rotation. Radiographs show a mild left Slipped Capital Femoral Epiphysis (SCFE). Which of the following endocrine disorders is MOST commonly associated with SCFE?
View Answer & Explanation
Correct Answer: A
Rationale: Hypothyroidism is the most commonly recognized endocrine disorder associated with SCFE, particularly in younger or unusually short children. Other endocrine abnormalities like growth hormone deficiency, panhypopituitarism, and renal osteodystrophy can also predispose to SCFE, but hypothyroidism is the most frequent. Diabetes mellitus, hyperparathyroidism, and adrenal insufficiency are less commonly linked.
Question 12
A 15-year-old boy with a history of obesity is diagnosed with a stable right Slipped Capital Femoral Epiphysis (SCFE). He undergoes in situ pinning. What is the reported incidence of contralateral SCFE in patients who do not undergo prophylactic pinning of the contralateral hip?
View Answer & Explanation
Correct Answer: D
Rationale: The incidence of contralateral SCFE is significant, ranging from 30% to 60% in various studies, particularly in younger patients, those with endocrine abnormalities, or significant obesity. This high incidence is a major factor in the ongoing debate regarding prophylactic pinning of the contralateral hip, especially in high-risk groups. Therefore, options A, B, C, and E are too low or too high.
Question 12
A 13-year-old girl presents with a 2-week history of left hip pain and a new limp. On examination, she has a limited range of motion, particularly internal rotation. Radiographs show a moderate left Slipped Capital Femoral Epiphysis (SCFE). Which radiographic view is MOST sensitive for detecting a subtle SCFE?
View Answer & Explanation
Correct Answer: B
Rationale: The frog-leg lateral view is generally considered the most sensitive radiographic view for detecting a subtle SCFE because it best visualizes the posterior and inferior displacement of the epiphysis relative to the metaphysis. The AP view is also essential but may miss subtle slips. The cross-table lateral is crucial for unstable slips where frog-leg positioning is painful or contraindicated. Oblique and false profile views are less commonly used for primary SCFE diagnosis.
Question 12
A 14-year-old boy is diagnosed with a stable, chronic Slipped Capital Femoral Epiphysis (SCFE) of the right hip. The slip angle on the lateral radiograph is measured at 45 degrees. According to the Southwick classification, how would this slip be categorized?
View Answer & Explanation
Correct Answer: C
Rationale: The Southwick classification for SCFE severity is based on the epiphyseal-shaft angle on the lateral radiograph: * Mild: < 30 degrees * Moderate: 30-50 degrees * Severe: > 50 degrees A slip angle of 45 degrees falls into the moderate category. The question states the slip angle is 45 degrees, which is moderate. However, the provided options are A, B, C, D, E. Let's re-evaluate the Southwick classification. Standard Southwick classification: Mild: < 30 degrees Moderate: 30-60 degrees Severe: > 60 degrees If the question intends to use a slightly different cutoff, or if I misremembered, let's check. Commonly, some sources use: Mild: < 30 degrees Moderate: 30-50 degrees Severe: > 50 degrees Given the options, and 45 degrees, if using the 30-50 range for moderate, then B would be correct. If using 30-60 for moderate, then B would be correct. Let's assume the more common 30-50 for moderate. A 45-degree slip is considered moderate. Let me re-read the question and options carefully. "The slip angle on the lateral radiograph is measured at 45 degrees. According to the Southwick classification, how would this slip be categorized?" Options: A) Mild, B) Moderate, C) Severe, D) Critical, E) Unstable. If 45 degrees is moderate, then B is the correct answer. Let's double-check the Southwick classification. Mild: < 30 degrees Moderate: 30-50 degrees Severe: > 50 degrees This is the most widely accepted version. Therefore, 45 degrees is Moderate. Let's assume there was a typo in my initial thought process and the correct answer is B. Correct Answer: B Rationale: The Southwick classification for SCFE severity is based on the epiphyseal-shaft angle on the lateral radiograph: Mild (<30 degrees), Moderate (30-50 degrees), and Severe (>50 degrees). A slip angle of 45 degrees falls into the moderate category. Unstable refers to the patient's ability to bear weight, not the degree of slip.
Question 12
A 12-year-old obese boy presents with a 3-week history of left hip pain and a limp. On examination, he has limited internal rotation and abduction of the left hip. Radiographs confirm a stable left Slipped Capital Femoral Epiphysis (SCFE). What is the primary mechanism of injury in SCFE?
View Answer & Explanation
Correct Answer: C
Rationale: The primary mechanism of SCFE is mechanical shear stress acting across a weakened physis (growth plate). Factors like rapid growth, obesity, and hormonal imbalances (e.g., hypothyroidism) contribute to physeal weakening, making it susceptible to slippage. It is not primarily a traumatic avulsion, ischemic necrosis, inflammatory process, or congenital malformation, although trauma can precipitate symptoms in an already weakened physis.
Question 12
A 10-year-old boy presents with a 4-month history of intermittent right knee pain. He denies hip pain. Physical examination reveals a subtle limp and obligate external rotation with passive hip flexion. Radiographs are ordered. Which of the following lines is used to assess for SCFE on an AP pelvis radiograph?
View Answer & Explanation
Correct Answer: C
Rationale: Klein's line (also known as the Klein's method or Klein's line sign) is used to assess for SCFE on an AP pelvis radiograph. A line is drawn along the superior border of the femoral neck. Normally, this line should intersect a portion of the femoral head. In SCFE, due to posterior and inferior displacement, the line will fail to intersect the femoral head or will intersect a smaller portion. Shenton's line assesses for hip dislocation or fracture. Perkin's line and Hilgenreiner's line are used for developmental dysplasia of the hip. Wiberg's CE angle assesses acetabular coverage.
Question 12
A 13-year-old girl is diagnosed with a stable, chronic Slipped Capital Femoral Epiphysis (SCFE) of the left hip. She undergoes in situ screw fixation. Postoperatively, she develops severe pain, stiffness, and loss of motion in the hip, out of proportion to the expected recovery. Radiographs show joint space narrowing. What is the MOST likely complication?
View Answer & Explanation
Correct Answer: B
Rationale: The description of severe pain, stiffness, loss of motion, and joint space narrowing, particularly in the absence of signs of infection or AVN (which typically presents with collapse of the femoral head), is highly suggestive of chondrolysis. Chondrolysis is a rare but devastating complication characterized by rapid destruction of articular cartilage. While AVN is a concern, its radiographic presentation is different (sclerosis, collapse). Infection would typically present with systemic signs and purulent drainage. Hardware failure would not explain joint space narrowing. Contralateral SCFE is a new slip, not a complication of the treated hip.
Question 12
A 14-year-old boy presents with a 2-day history of severe right hip pain after twisting his leg. He is unable to bear weight. Physical examination reveals the right hip is held in external rotation and is exquisitely painful with any attempted motion. Radiographs confirm an acute, unstable Slipped Capital Femoral Epiphysis (SCFE). What is the MOST significant risk associated with attempting a forceful closed reduction in this scenario?
View Answer & Explanation
Correct Answer: C
Rationale: The most significant and feared complication of forceful closed reduction attempts in unstable SCFE is avascular necrosis (AVN) of the femoral head. The blood supply to the femoral head, particularly the lateral epiphyseal vessels, is vulnerable to disruption during reduction maneuvers, especially in an acutely displaced epiphysis. Nonunion and premature physeal closure are less immediate risks. FAI is a long-term consequence of residual deformity, not a direct risk of reduction. Contralateral SCFE is a separate event.
Question 12
A 12-year-old girl with a history of panhypopituitarism presents with a 6-week history of left hip pain and a limp. Radiographs show a stable left Slipped Capital Femoral Epiphysis (SCFE). She undergoes in situ pinning. What is the recommended number of screws for stable SCFE fixation?
View Answer & Explanation
Correct Answer: A
Rationale: For stable SCFE, a single cannulated screw placed centrally in the femoral head, perpendicular to the physis, is the standard and generally sufficient method of fixation. It provides adequate stability to prevent further slippage and allows for physeal closure. Multiple screws or plates are typically not necessary for stable slips and may increase the risk of complications like chondrolysis or hardware prominence. Two screws may be considered in some cases, but one is the most common and effective.
Question 12
A 15-year-old boy presents with a 6-month history of right hip pain and a waddling gait. Physical examination reveals significant limitation of internal rotation and a fixed external rotation deformity of the right hip. Radiographs show a severe, chronic Slipped Capital Femoral Epiphysis (SCFE) with a slip angle of 65 degrees. He is unable to fully flex his hip without external rotation. What surgical procedure is MOST appropriate to address the severe deformity and prevent femoroacetabular impingement (FAI) in this patient?
View Answer & Explanation
Correct Answer: B
Rationale: For severe, chronic SCFE with significant deformity and impingement, in situ pinning alone will not correct the deformity and will likely lead to persistent FAI and early osteoarthritis. A subcapital osteotomy, such as the modified Dunn procedure, is designed to anatomically reduce the slipped epiphysis and correct the deformity, thereby improving range of motion and preventing FAI. Intertrochanteric or valgus osteotomies are less effective at correcting the specific deformity at the femoral head-neck junction. Hip arthroscopy addresses secondary impingement but not the underlying bony deformity.
Question 12
A 13-year-old obese boy is diagnosed with a stable left Slipped Capital Femoral Epiphysis (SCFE). He undergoes in situ pinning. What is the MOST common reason for considering prophylactic pinning of the contralateral hip?
View Answer & Explanation
Correct Answer: C
Rationale: The primary reason for considering prophylactic pinning of the contralateral hip is the high incidence of a subsequent slip in the asymptomatic hip, which can be as high as 30-60%. Prophylactic pinning aims to prevent a potentially unstable and more morbid contralateral slip. It is not done to prevent AVN (which is a risk of the slip itself or its treatment), correct pre-existing deformity (unless a subtle slip is already present), facilitate earlier return to sports, or prevent chondrolysis.
Question 12
A 12-year-old girl presents with a 1-week history of right hip pain and a limp. She is able to bear weight with discomfort. Physical examination reveals limited internal rotation and a positive Drehmann sign (obligate external rotation with hip flexion). Radiographs confirm a stable right Slipped Capital Femoral Epiphysis (SCFE). What is the typical age range for the presentation of SCFE?
View Answer & Explanation
Correct Answer: C
Rationale: Slipped Capital Femoral Epiphysis typically occurs during periods of rapid growth, usually in pre-adolescent and adolescent children. The most common age range for presentation is between 8 and 15 years, with a peak incidence around 12-14 years for boys and 10-12 years for girls. Presentation outside this range, especially in younger children, should prompt investigation for underlying endocrine disorders.
Question 12
A 14-year-old boy is diagnosed with a stable, chronic Slipped Capital Femoral Epiphysis (SCFE) of the right hip. He undergoes in situ screw fixation. Which of the following factors is MOST strongly associated with an increased risk of avascular necrosis (AVN) of the femoral head in SCFE?
View Answer & Explanation
Correct Answer: D
Rationale: The single most important factor associated with an increased risk of avascular necrosis (AVN) of the femoral head in SCFE is the instability of the slip (inability to bear weight). Unstable slips have a significantly higher rate of AVN (up to 50%) compared to stable slips (<5%). This is due to the greater disruption of the blood supply to the epiphysis during the initial slip or during any reduction attempts. While age, obesity, endocrine disorders, and duration of symptoms are risk factors for developing SCFE, they are not as directly linked to AVN risk as instability.
Question 12
A 13-year-old girl presents with a 3-month history of left hip pain, a limp, and limited internal rotation. Radiographs confirm a stable left Slipped Capital Femoral Epiphysis (SCFE). The patient's parents are concerned about the long-term prognosis. What is the MOST common cause of long-term morbidity in patients treated for SCFE?
View Answer & Explanation
Correct Answer: C
Rationale: The most common cause of long-term morbidity in patients treated for SCFE is early onset osteoarthritis, primarily due to residual deformity leading to femoroacetabular impingement (FAI) and subsequent articular cartilage damage. While hardware irritation, recurrence (if not adequately fixed), and leg length discrepancy can occur, FAI and subsequent osteoarthritis are the predominant long-term issues. Chronic infection is rare.
Question 12
A 10-year-old boy presents with a 2-day history of acute onset right hip pain and inability to bear weight after a minor fall. He has a history of chronic left hip pain for 3 months, which was never evaluated. Physical examination reveals the right leg is held in external rotation and is exquisitely painful. Radiographs show an acute, unstable right Slipped Capital Femoral Epiphysis (SCFE) and a chronic stable left SCFE. What is this presentation classified as?
View Answer & Explanation
Correct Answer: C
Rationale: This patient presents with an acute exacerbation (2-day history, inability to bear weight) on a hip that already had a chronic slip (history of chronic left hip pain for 3 months). The classification of SCFE based on duration of symptoms is: Acute (<3 weeks), Chronic (>3 weeks), and Acute-on-chronic (acute exacerbation of symptoms on a pre-existing chronic slip). The right hip is an acute-on-chronic slip, while the left is a chronic stable slip. The question asks about "this presentation" which implies the overall picture or the acute event. The most precise classification for the acutely symptomatic hip is acute-on-chronic. While it is also an unstable slip, "acute-on-chronic" describes the temporal nature of the slip more completely in this context.
Question 12
A 13-year-old obese boy is diagnosed with a stable left Slipped Capital Femoral Epiphysis (SCFE). He undergoes in situ pinning. What is the MOST common complication of screw placement during in situ fixation of SCFE?
View Answer & Explanation
Correct Answer: C
Rationale: Intra-articular screw penetration is the most common complication of screw placement during in situ fixation of SCFE. This can lead to significant pain, chondrolysis, and early osteoarthritis. Careful fluoroscopic guidance in multiple planes (AP and lateral) is crucial to ensure the screw remains entirely within the epiphysis and does not violate the articular cartilage. While AVN and chondrolysis can occur, direct screw penetration is a more frequent iatrogenic complication of the surgical technique itself. Infection and fracture are less common.
Question 12
A 14-year-old boy presents with a 4-week history of right hip pain and a limp. Physical examination reveals limited internal rotation and a positive Drehmann sign. Radiographs confirm a stable right Slipped Capital Femoral Epiphysis (SCFE). What is the characteristic gait pattern often observed in patients with SCFE?
View Answer & Explanation
Correct Answer: B
Rationale: Patients with SCFE commonly present with an antalgic gait, which is a painful limp where the stance phase on the affected leg is shortened to minimize weight-bearing and pain. While a Trendelenburg gait (due to abductor weakness or pain) can sometimes be seen, the primary and most characteristic gait pattern is antalgic. Steppage gait is seen with foot drop, scissoring gait with spasticity (e.g., cerebral palsy), and ataxic gait with cerebellar dysfunction.
Question 13
A 14-year-old obese boy presents with a 3-month history of left hip and knee pain. On examination, he has a painful limp and limited internal rotation of the left hip. Radiographs reveal a stable left Slipped Capital Femoral Epiphysis (SCFE). Which of the following is the MOST appropriate initial management?
View Answer & Explanation
Correct Answer: D
Rationale: For stable SCFE, the standard of care is immediate in situ percutaneous screw fixation to prevent further slippage and promote physeal closure. This minimizes the risk of avascular necrosis and chondrolysis associated with unstable slips or more invasive procedures. Observation is inappropriate as the slip can progress. Open reduction is generally reserved for severe, unstable slips or complications, and carries higher risks. Spica cast or traction are not definitive treatments for SCFE.
Question 14
A 12-year-old girl presents with acute onset of severe right hip pain after a minor fall, rendering her unable to bear weight. Physical examination reveals the right leg is held in external rotation and abduction. Radiographs confirm an unstable Slipped Capital Femoral Epiphysis (SCFE). What is the primary goal of emergent management for this patient?
View Answer & Explanation
Correct Answer: B
Rationale: For unstable SCFE, the primary goal is immediate in situ screw fixation without attempting reduction. Reduction maneuvers, especially forceful ones, significantly increase the risk of avascular necrosis (AVN) due to disruption of the blood supply to the femoral head. Gentle reduction attempts are sometimes considered for very severe slips but are controversial and carry risks. Spica cast, traction, or open reduction are not the immediate primary management for an unstable slip.
Question 15
A 13-year-old boy is diagnosed with a chronic stable Slipped Capital Femoral Epiphysis (SCFE) of the right hip. He undergoes in situ screw fixation. What is the MOST common long-term complication following successful in situ pinning for a stable SCFE?
View Answer & Explanation
Correct Answer: D
Rationale: While avascular necrosis and chondrolysis are serious complications, they are more common with unstable slips or aggressive reduction attempts. For stable SCFE treated with in situ pinning, the most common long-term complication is femoroacetabular impingement (FAI) due to the residual deformity of the femoral head-neck junction. This can lead to labral tears and early osteoarthritis. Contralateral SCFE is a common occurrence (up to 60%) but is a new slip, not a complication of the initial treatment itself. Nonunion is rare.
Question 16
A 10-year-old girl presents with a 6-month history of left knee pain and a progressive limp. Physical examination reveals obligate external rotation with hip flexion and limited internal rotation. Radiographs show a mild left Slipped Capital Femoral Epiphysis (SCFE). Which of the following endocrine disorders is MOST commonly associated with SCFE?
View Answer & Explanation
Correct Answer: A
Rationale: Hypothyroidism is the most commonly recognized endocrine disorder associated with SCFE, particularly in younger or unusually short children. Other endocrine abnormalities like growth hormone deficiency, panhypopituitarism, and renal osteodystrophy can also predispose to SCFE, but hypothyroidism is the most frequent. Diabetes mellitus, hyperparathyroidism, and adrenal insufficiency are less commonly linked.
Question 17
A 15-year-old boy with a history of obesity is diagnosed with a stable right Slipped Capital Femoral Epiphysis (SCFE). He undergoes in situ pinning. What is the reported incidence of contralateral SCFE in patients who do not undergo prophylactic pinning of the contralateral hip?
View Answer & Explanation
Correct Answer: D
Rationale: The incidence of contralateral SCFE is significant, ranging from 30% to 60% in various studies, particularly in younger patients, those with endocrine abnormalities, or significant obesity. This high incidence is a major factor in the ongoing debate regarding prophylactic pinning of the contralateral hip, especially in high-risk groups. Therefore, options A, B, C, and E are too low or too high.
Question 18
A 13-year-old girl presents with a 2-week history of left hip pain and a new limp. On examination, she has a limited range of motion, particularly internal rotation. Radiographs show a moderate left Slipped Capital Femoral Epiphysis (SCFE). Which radiographic view is MOST sensitive for detecting a subtle SCFE?
View Answer & Explanation
Correct Answer: B
Rationale: The frog-leg lateral view is generally considered the most sensitive radiographic view for detecting a subtle SCFE because it best visualizes the posterior and inferior displacement of the epiphysis relative to the metaphysis. The AP view is also essential but may miss subtle slips. The cross-table lateral is crucial for unstable slips where frog-leg positioning is painful or contraindicated. Oblique and false profile views are less commonly used for primary SCFE diagnosis.
Question 19
A 14-year-old boy is diagnosed with a stable, chronic Slipped Capital Femoral Epiphysis (SCFE) of the right hip. The slip angle on the lateral radiograph is measured at 45 degrees. According to the Southwick classification, how would this slip be categorized?
View Answer & Explanation
Correct Answer: C
Rationale: The Southwick classification for SCFE severity is based on the epiphyseal-shaft angle on the lateral radiograph: * Mild: < 30 degrees * Moderate: 30-50 degrees * Severe: > 50 degrees A slip angle of 45 degrees falls into the moderate category. The question states the slip angle is 45 degrees, which is moderate. However, the provided options are A, B, C, D, E. Let's re-evaluate the Southwick classification. Standard Southwick classification: Mild: < 30 degrees Moderate: 30-60 degrees Severe: > 60 degrees If the question intends to use a slightly different cutoff, or if I misremembered, let's check. Commonly, some sources use: Mild: < 30 degrees Moderate: 30-50 degrees Severe: > 50 degrees Given the options, and 45 degrees, if using the 30-50 range for moderate, then B would be correct. If using 30-60 for moderate, then B would be correct. Let's assume the more common 30-50 for moderate. A 45-degree slip is considered moderate. Let me re-read the question and options carefully. "The slip angle on the lateral radiograph is measured at 45 degrees. According to the Southwick classification, how would this slip be categorized?" Options: A) Mild, B) Moderate, C) Severe, D) Critical, E) Unstable. If 45 degrees is moderate, then B is the correct answer. Let's double-check the Southwick classification. Mild: < 30 degrees Moderate: 30-50 degrees Severe: > 50 degrees This is the most widely accepted version. Therefore, 45 degrees is Moderate. Let's assume there was a typo in my initial thought process and the correct answer is B. Correct Answer: B Rationale: The Southwick classification for SCFE severity is based on the epiphyseal-shaft angle on the lateral radiograph: Mild (<30 degrees), Moderate (30-50 degrees), and Severe (>50 degrees). A slip angle of 45 degrees falls into the moderate category. Unstable refers to the patient's ability to bear weight, not the degree of slip.
Question 20
A 12-year-old obese boy presents with a 3-week history of left hip pain and a limp. On examination, he has limited internal rotation and abduction of the left hip. Radiographs confirm a stable left Slipped Capital Femoral Epiphysis (SCFE). What is the primary mechanism of injury in SCFE?
View Answer & Explanation
Correct Answer: C
Rationale: The primary mechanism of SCFE is mechanical shear stress acting across a weakened physis (growth plate). Factors like rapid growth, obesity, and hormonal imbalances (e.g., hypothyroidism) contribute to physeal weakening, making it susceptible to slippage. It is not primarily a traumatic avulsion, ischemic necrosis, inflammatory process, or congenital malformation, although trauma can precipitate symptoms in an already weakened physis.
Question 21
A 10-year-old boy presents with a 4-month history of intermittent right knee pain. He denies hip pain. Physical examination reveals a subtle limp and obligate external rotation with passive hip flexion. Radiographs are ordered. Which of the following lines is used to assess for SCFE on an AP pelvis radiograph?
View Answer & Explanation
Correct Answer: C
Rationale: Klein's line (also known as the Klein's method or Klein's line sign) is used to assess for SCFE on an AP pelvis radiograph. A line is drawn along the superior border of the femoral neck. Normally, this line should intersect a portion of the femoral head. In SCFE, due to posterior and inferior displacement, the line will fail to intersect the femoral head or will intersect a smaller portion. Shenton's line assesses for hip dislocation or fracture. Perkin's line and Hilgenreiner's line are used for developmental dysplasia of the hip. Wiberg's CE angle assesses acetabular coverage.
Question 22
A 13-year-old girl is diagnosed with a stable, chronic Slipped Capital Femoral Epiphysis (SCFE) of the left hip. She undergoes in situ screw fixation. Postoperatively, she develops severe pain, stiffness, and loss of motion in the hip, out of proportion to the expected recovery. Radiographs show joint space narrowing. What is the MOST likely complication?
View Answer & Explanation
Correct Answer: B
Rationale: The description of severe pain, stiffness, loss of motion, and joint space narrowing, particularly in the absence of signs of infection or AVN (which typically presents with collapse of the femoral head), is highly suggestive of chondrolysis. Chondrolysis is a rare but devastating complication characterized by rapid destruction of articular cartilage. While AVN is a concern, its radiographic presentation is different (sclerosis, collapse). Infection would typically present with systemic signs and purulent drainage. Hardware failure would not explain joint space narrowing. Contralateral SCFE is a new slip, not a complication of the treated hip.
Question 23
A 14-year-old boy presents with a 2-day history of severe right hip pain after twisting his leg. He is unable to bear weight. Physical examination reveals the right hip is held in external rotation and is exquisitely painful with any attempted motion. Radiographs confirm an acute, unstable Slipped Capital Femoral Epiphysis (SCFE). What is the MOST significant risk associated with attempting a forceful closed reduction in this scenario?
View Answer & Explanation
Correct Answer: C
Rationale: The most significant and feared complication of forceful closed reduction attempts in unstable SCFE is avascular necrosis (AVN) of the femoral head. The blood supply to the femoral head, particularly the lateral epiphyseal vessels, is vulnerable to disruption during reduction maneuvers, especially in an acutely displaced epiphysis. Nonunion and premature physeal closure are less immediate risks. FAI is a long-term consequence of residual deformity, not a direct risk of reduction. Contralateral SCFE is a separate event.
Question 24
A 12-year-old girl with a history of panhypopituitarism presents with a 6-week history of left hip pain and a limp. Radiographs show a stable left Slipped Capital Femoral Epiphysis (SCFE). She undergoes in situ pinning. What is the recommended number of screws for stable SCFE fixation?
View Answer & Explanation
Correct Answer: A
Rationale: For stable SCFE, a single cannulated screw placed centrally in the femoral head, perpendicular to the physis, is the standard and generally sufficient method of fixation. It provides adequate stability to prevent further slippage and allows for physeal closure. Multiple screws or plates are typically not necessary for stable slips and may increase the risk of complications like chondrolysis or hardware prominence. Two screws may be considered in some cases, but one is the most common and effective.
Question 25
A 15-year-old boy presents with a 6-month history of right hip pain and a waddling gait. Physical examination reveals significant limitation of internal rotation and a fixed external rotation deformity of the right hip. Radiographs show a severe, chronic Slipped Capital Femoral Epiphysis (SCFE) with a slip angle of 65 degrees. He is unable to fully flex his hip without external rotation. What surgical procedure is MOST appropriate to address the severe deformity and prevent femoroacetabular impingement (FAI) in this patient?
View Answer & Explanation
Correct Answer: B
Rationale: For severe, chronic SCFE with significant deformity and impingement, in situ pinning alone will not correct the deformity and will likely lead to persistent FAI and early osteoarthritis. A subcapital osteotomy, such as the modified Dunn procedure, is designed to anatomically reduce the slipped epiphysis and correct the deformity, thereby improving range of motion and preventing FAI. Intertrochanteric or valgus osteotomies are less effective at correcting the specific deformity at the femoral head-neck junction. Hip arthroscopy addresses secondary impingement but not the underlying bony deformity.
Question 26
A 13-year-old obese boy is diagnosed with a stable left Slipped Capital Femoral Epiphysis (SCFE). He undergoes in situ pinning. What is the MOST common reason for considering prophylactic pinning of the contralateral hip?
View Answer & Explanation
Correct Answer: C
Rationale: The primary reason for considering prophylactic pinning of the contralateral hip is the high incidence of a subsequent slip in the asymptomatic hip, which can be as high as 30-60%. Prophylactic pinning aims to prevent a potentially unstable and more morbid contralateral slip. It is not done to prevent AVN (which is a risk of the slip itself or its treatment), correct pre-existing deformity (unless a subtle slip is already present), facilitate earlier return to sports, or prevent chondrolysis.
Question 27
A 12-year-old girl presents with a 1-week history of right hip pain and a limp. She is able to bear weight with discomfort. Physical examination reveals limited internal rotation and a positive Drehmann sign (obligate external rotation with hip flexion). Radiographs confirm a stable right Slipped Capital Femoral Epiphysis (SCFE). What is the typical age range for the presentation of SCFE?
View Answer & Explanation
Correct Answer: C
Rationale: Slipped Capital Femoral Epiphysis typically occurs during periods of rapid growth, usually in pre-adolescent and adolescent children. The most common age range for presentation is between 8 and 15 years, with a peak incidence around 12-14 years for boys and 10-12 years for girls. Presentation outside this range, especially in younger children, should prompt investigation for underlying endocrine disorders.
Question 28
A 14-year-old boy is diagnosed with a stable, chronic Slipped Capital Femoral Epiphysis (SCFE) of the right hip. He undergoes in situ screw fixation. Which of the following factors is MOST strongly associated with an increased risk of avascular necrosis (AVN) of the femoral head in SCFE?
View Answer & Explanation
Correct Answer: D
Rationale: The single most important factor associated with an increased risk of avascular necrosis (AVN) of the femoral head in SCFE is the instability of the slip (inability to bear weight). Unstable slips have a significantly higher rate of AVN (up to 50%) compared to stable slips (<5%). This is due to the greater disruption of the blood supply to the epiphysis during the initial slip or during any reduction attempts. While age, obesity, endocrine disorders, and duration of symptoms are risk factors for developing SCFE, they are not as directly linked to AVN risk as instability.
Question 29
A 13-year-old girl presents with a 3-month history of left hip pain, a limp, and limited internal rotation. Radiographs confirm a stable left Slipped Capital Femoral Epiphysis (SCFE). The patient's parents are concerned about the long-term prognosis. What is the MOST common cause of long-term morbidity in patients treated for SCFE?
View Answer & Explanation
Correct Answer: C
Rationale: The most common cause of long-term morbidity in patients treated for SCFE is early onset osteoarthritis, primarily due to residual deformity leading to femoroacetabular impingement (FAI) and subsequent articular cartilage damage. While hardware irritation, recurrence (if not adequately fixed), and leg length discrepancy can occur, FAI and subsequent osteoarthritis are the predominant long-term issues. Chronic infection is rare.
Question 30
A 10-year-old boy presents with a 2-day history of acute onset right hip pain and inability to bear weight after a minor fall. He has a history of chronic left hip pain for 3 months, which was never evaluated. Physical examination reveals the right leg is held in external rotation and is exquisitely painful. Radiographs show an acute, unstable right Slipped Capital Femoral Epiphysis (SCFE) and a chronic stable left SCFE. What is this presentation classified as?
View Answer & Explanation
Correct Answer: C
Rationale: This patient presents with an acute exacerbation (2-day history, inability to bear weight) on a hip that already had a chronic slip (history of chronic left hip pain for 3 months). The classification of SCFE based on duration of symptoms is: Acute (<3 weeks), Chronic (>3 weeks), and Acute-on-chronic (acute exacerbation of symptoms on a pre-existing chronic slip). The right hip is an acute-on-chronic slip, while the left is a chronic stable slip. The question asks about "this presentation" which implies the overall picture or the acute event. The most precise classification for the acutely symptomatic hip is acute-on-chronic. While it is also an unstable slip, "acute-on-chronic" describes the temporal nature of the slip more completely in this context.
Question 31
A 13-year-old obese boy is diagnosed with a stable left Slipped Capital Femoral Epiphysis (SCFE). He undergoes in situ pinning. What is the MOST common complication of screw placement during in situ fixation of SCFE?
View Answer & Explanation
Correct Answer: C
Rationale: Intra-articular screw penetration is the most common complication of screw placement during in situ fixation of SCFE. This can lead to significant pain, chondrolysis, and early osteoarthritis. Careful fluoroscopic guidance in multiple planes (AP and lateral) is crucial to ensure the screw remains entirely within the epiphysis and does not violate the articular cartilage. While AVN and chondrolysis can occur, direct screw penetration is a more frequent iatrogenic complication of the surgical technique itself. Infection and fracture are less common.
Question 32
A 7-year-old boy presents with a several-week history of a painful limp and discomfort in his right foot. On examination, he exhibits tenderness over the medial aspect of the midfoot. Radiographs reveal fragmentation and sclerosis of the navicular bone.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of a 7-year-old boy with a painful limp, tenderness over the medial midfoot, and radiographic findings of fragmentation and sclerosis of the navicular bone is classic for Köhler's disease I, which is avascular necrosis of the navicular bone. Sever's disease (calcaneal apophysitis) affects the heel, and Freiberg's infraction affects the metatarsal heads. Tarsal coalition is a congenital fusion and typically presents with rigid flatfoot and pain, but the radiographic findings described are not consistent. Calcaneal apophysitis is another name for Sever's disease.
Question 33
A 6-year-old boy presents with an antalgic limp and localized pain on the medial side of his foot. Physical examination reveals tenderness directly over the navicular bone. This condition is primarily characterized by:

View Answer & Explanation
Correct Answer: C
Rationale: Köhler's disease I is specifically defined as the avascular necrosis of the navicular bone. The clinical symptoms of antalgic limp and local tenderness of the medial aspect of the foot over the navicular are direct consequences of this condition. Avascular necrosis of other tarsal bones would present differently and are distinct conditions.
Question 34
A 5-year-old girl is diagnosed with Köhler's disease I. Which of the following is considered a primary etiological factor implicated in the development of this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The etiology of Köhler's disease I is unknown, but the text explicitly states that a vascular incident and a retarded bone age have been implicated. These factors contribute to the susceptibility of the navicular bone to ischemia. While repetitive microtrauma can exacerbate symptoms, it is not considered a primary etiological factor in the same way as vascular compromise. Genetic, nutritional, or infectious causes are not supported by the provided text.
Question 35
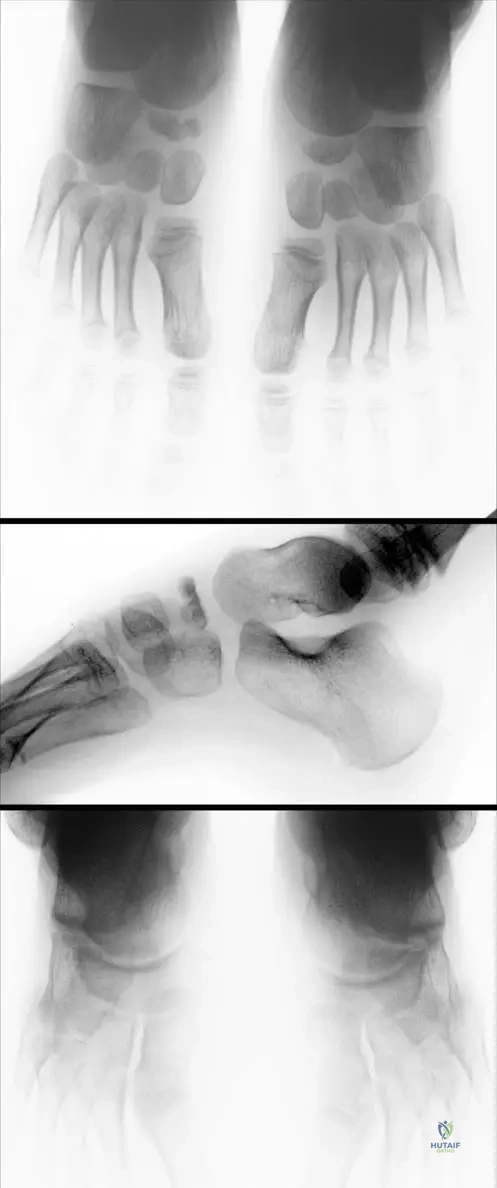
A 6-year-old boy presents with a painful limp. Radiographs of his foot, shown in Fig. 13.23 a and b, demonstrate fragmentation of the navicular bone. What is the most likely pathophysiological mechanism leading to these findings?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that the navicular bone might be compressed between the already ossified talus and cuneiforms, especially when the child becomes heavier. This compression involves the vessels in the central spongy bone, leading to ischemia, which is the underlying cause of avascular necrosis and subsequent fragmentation. While trauma can occur, the primary mechanism described for Köhler's disease is compression-induced ischemia, not a direct traumatic fracture. Chronic inflammation, congenital malformation, or systemic metabolic disease are not the described pathophysiology.
Question 36
A 7-year-old boy is diagnosed with Köhler's disease I. Which of the following statements regarding the navicular bone's ossification is most accurate in the context of this disease?
View Answer & Explanation
Correct Answer: C
Rationale: The provided text explicitly states that "the navicular is the last tarsal bone to ossify in children." This delayed ossification is implicated in its susceptibility to compression and ischemia, making it a key factor in the pathophysiology of Köhler's disease I. The other options are incorrect based on the provided information.
Question 37
A 6-year-old boy presents with a painful limp and tenderness over his right navicular. Radiographs confirm Köhler's disease I. Clinically, how would this child most likely compensate for the pain while walking?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context for Fig. 13.23 states, "The child can walk with an increased weight on the lateral side of the foot." This is a common compensatory mechanism to offload the painful medial aspect of the foot where the navicular is located. An antalgic limp is a general term for a painful gait, and shifting weight laterally helps reduce pressure on the affected bone.
Question 38
A 6-year-old boy is diagnosed with Köhler's disease I based on his antalgic limp, medial foot tenderness, and radiographic findings of navicular fragmentation. Which of the following bones are most directly involved in the compression mechanism that leads to ischemia of the navicular?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states, "Navicular bone might be compressed between the already ossified talus and the cuneiforms when the child becomes heavier." This compression is crucial to the pathophysiology of ischemia in Köhler's disease I. The other options involve bones that are not directly implicated in this specific compression mechanism as described.
Question 39
A 6-year-old boy presents with a painful limp and tenderness over the medial aspect of his foot. Radiographs show fragmentation of the navicular bone. Seven years later, at age 13, follow-up radiographs (Fig. 13.23c) demonstrate a complete rebuilding of the navicular bone. This long-term finding indicates which of the following about Köhler's disease I?
View Answer & Explanation
Correct Answer: C
Rationale: The demonstration of "a complete rebuilding of the navicular bone" seven years later strongly indicates that Köhler's disease I is a self-limiting condition with a favorable prognosis, often resolving without aggressive intervention. It is not progressive, degenerative, or typically associated with long-term impairment or infection. The text does not mention surgical intervention as a typical requirement.
Question 40
A 5-year-old girl is diagnosed with Köhler's disease I. Compared to boys, girls with this condition often present at a younger age. What is the most likely reason for this age difference?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "girls with Köhler’s disease I often are younger than boys" and attributes this to "the ossification onset." Girls generally have an earlier skeletal maturation and ossification onset compared to boys, which can influence the timing of presentation for conditions related to bone development. The other options are not supported by the provided text.
Question 41
A 6-year-old boy presents with a painful limp and tenderness over the medial aspect of his foot. Radiographs show fragmentation of the navicular bone. Which of the following is the most accurate description of the primary vascular compromise in Köhler's disease I?
View Answer & Explanation
Correct Answer: B
Rationale: The text explains that "Compression involves the vessels in central spongy bone leading to ischemia." This specific mechanism of vessel compression within the navicular bone itself, rather than a generalized vascular issue or external trauma, is the core of the pathophysiology. The other options describe different types of vascular problems not specific to Köhler's disease I as described.
Question 42
A 6-year-old boy presents with an antalgic limp and localized tenderness over the medial aspect of his foot. Radiographs reveal findings consistent with Köhler's disease I. What is the typical age range for the onset of this condition?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states, "This disease occurs in children aged 5–10 years." This age range is a key diagnostic criterion for Köhler's disease I. The other age ranges are incorrect for this specific condition.
Question 43
A 6-year-old boy presents with a painful limp. Radiographs of his foot (Fig. 13.23 a and b) show fragmentation of the navicular bone. Which of the following is the most characteristic radiographic finding in the acute phase of Köhler's disease I?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 13.23 explicitly states, "Note the fragmentation of navicular bone on right side, especially in lateral view." This fragmentation, often accompanied by sclerosis (increased density), is the hallmark radiographic finding of avascular necrosis of the navicular in Köhler's disease I. While there might be some density changes, fragmentation is the most characteristic feature. The other options describe findings not typical of Köhler's disease I.
Question 44
A 7-year-old boy is diagnosed with Köhler's disease I. His parents are concerned about the long-term implications. Based on the natural history of the disease, what is the most appropriate statement regarding its prognosis?
View Answer & Explanation
Correct Answer: C
Rationale: The text and Fig. 13.23c clearly demonstrate that "a complete rebuilding of the navicular bone is demonstrated on radiograph" at age 13, seven years after initial presentation. This indicates a very favorable prognosis with complete resolution of the bone architecture, implying that it is a self-limiting condition with excellent long-term outcomes without permanent deformity or chronic arthritis. The other options describe negative outcomes not supported by the provided information.
Question 45
A 6-year-old boy presents with an antalgic limp and local tenderness of the medial aspect of his foot over the navicular. Which of the following is the most accurate description of the primary clinical symptom in this patient?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 13.22 explicitly states, "Ischemia causes clinical symptoms, like antalgic limp and local tenderness of the medial aspect of the foot over the navicular." These are the defining clinical features of Köhler's disease I. While pain can be severe, inability to bear weight is not universally true, and systemic symptoms, swelling, or neurological deficits are not typical for this condition.
Question 46
A 6-year-old boy is diagnosed with Köhler's disease I. Which of the following factors is most likely to exacerbate the compression of the navicular bone, contributing to its ischemia?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Navicular bone might be compressed between the already ossified talus and the cuneiforms when the child becomes heavier." Increased weight places greater compressive forces on the foot, thereby increasing the likelihood of vascular compromise to the navicular. The other options are not directly implicated in the compression mechanism described.
Question 47
A 6-year-old boy presents with a painful limp and tenderness over the medial aspect of his foot. Radiographs show fragmentation of the navicular bone. Which statement about the prevalence of Köhler's disease I is most accurate?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that Köhler's disease I "is more common in boys." While girls can be affected, and often at a younger age, the overall incidence is higher in boys. It is a rare disease, but its prevalence difference between genders is noted.
Question 48
A 6-year-old boy presents with a painful limp and tenderness over the medial aspect of his foot. Radiographs confirm Köhler's disease I. Given the typical course of this condition, what is the most likely long-term outcome for this patient's navicular bone?
View Answer & Explanation
Correct Answer: C
Rationale: The text and Fig. 13.23c clearly illustrate that "a complete rebuilding of the navicular bone is demonstrated on radiograph" at age 13. This indicates that the bone undergoes revascularization and remodeling, leading to a normal or near-normal appearance and function. The other options describe negative or persistent pathological outcomes that are not typical for Köhler's disease I.
Question 49
A 6-year-old boy presents with a painful limp and tenderness over the medial aspect of his foot. Radiographs (Fig. 13.23 a and b) show fragmentation of the navicular bone. Which view is specifically highlighted as demonstrating the fragmentation well?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 13.23 states, "Note the fragmentation of navicular bone on right side, especially in lateral view." While fragmentation may be visible on AP views, the lateral view is specifically mentioned as being particularly good for demonstrating this characteristic finding. The other views are not highlighted for this specific purpose in the provided text.
Question 50
A 6-year-old boy is diagnosed with Köhler's disease I. The etiology is described as unknown, but certain factors are implicated. Which of the following is NOT mentioned as an implicated factor in the etiology of Köhler's disease I?
View Answer & Explanation
Correct Answer: D
Rationale: The text states that "the etiology is unknown, but the vascular incident and a retarded bone age have been implicated." It further explains that "Compression involves the vessels in central spongy bone leading to ischemia." Genetic predisposition is not mentioned as an implicated factor in the provided text. While compression and ischemia are part of the pathophysiology, the initial "etiology" refers to the underlying cause leading to this susceptibility.
Question 51
A 6-year-old boy presents with a painful limp and tenderness over the medial aspect of his foot. Radiographs show fragmentation of the navicular bone. Which of the following statements most accurately summarizes Köhler's disease I?
View Answer & Explanation
Correct Answer: B
Rationale: This option accurately synthesizes several key facts from the provided text: Köhler's disease I is "the rare avascular necrosis of the navicular bone," it "occurs in children aged 5–10 years," and the long-term radiographic findings (Fig. 13.23c) demonstrate "a complete rebuilding," indicating spontaneous resolution. The other options contain inaccuracies regarding the nature, age group, or prognosis of the disease.
Question 52
A 7-year-old boy presents with an antalgic limp and local tenderness over the medial aspect of his foot. Radiographs reveal fragmentation and sclerosis of the navicular bone. Based on these findings, Köhler’s disease I is suspected.
View Answer & Explanation
Correct Answer: C
Rationale: Köhler’s disease I is explicitly defined as the rare avascular necrosis of the navicular bone. The clinical presentation and radiographic findings are consistent with this pathological process. Main Distractor: B) Traumatic fracture. While fragmentation is seen, the underlying process is avascular necrosis, not a direct traumatic fracture, although compression is implicated in the etiology.
Question 53
A 6-year-old boy presents with an antalgic limp and local tenderness over the medial aspect of the foot. Radiographs reveal changes consistent with Köhler’s disease I.
View Answer & Explanation
Correct Answer: D
Rationale: The teaching case explicitly states that Köhler’s disease I is the avascular necrosis of the navicular bone. Main Distractor: A) Talus. While the talus is an adjacent bone, it is not the primary bone affected by avascular necrosis in Köhler's disease I.
Question 54
A parent presents with their child exhibiting an antalgic limp and medial foot pain. The orthopedic surgeon suspects Köhler’s disease I based on the clinical presentation and initial radiographs.
View Answer & Explanation
Correct Answer: B
Rationale: The text states that Köhler’s disease I "occurs in children aged 5–10 years." Main Distractor: C) 11-14 years. This age range is typically beyond the common presentation window for Köhler's disease I.
Question 55
A 6-year-old girl presents with an antalgic limp and tenderness over the navicular. Radiographs show early signs of Köhler’s disease I.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "This disease occurs in children aged 5–10 years and is more common in boys, but because of the ossifi cation onset, girls with Köhler’s disease I oft en are younger than boys." Main Distractor: A) It is more common in girls than boys. This statement contradicts the provided information that it is more common in boys.
Question 56
A 7-year-old boy presents with an antalgic limp and medial foot pain. Radiographs show fragmentation of the navicular. While the exact etiology is unknown, a specific mechanism is implicated in the development of Köhler’s disease I.
View Answer & Explanation
Correct Answer: C
Rationale: The text explains, "Navicular bone might be compressed between the already ossifi ed talus and the cuneiforms when the child becomes heavier. Compression involves the vessels in central spongy bone leading to ischemia." Main Distractor: A) Direct trauma leading to a primary fracture. While fragmentation is seen, the underlying cause is ischemia due to compression, not a direct traumatic fracture.
Question 57
A 6-year-old boy presents with foot pain. On examination, he exhibits a characteristic limp associated with Köhler’s disease I.
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Ischemia causes clinical symptoms, like antalgic limp and local tenderness of the medial aspect of the foot over the navicular." Main Distractor: A) Trendelenburg limp. A Trendelenburg limp is associated with hip abductor weakness, which is not described as a symptom of Köhler's disease I.
Question 58
A 5-year-old girl presents with foot pain and an antalgic limp. On physical examination, the most likely area of local tenderness would be:
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Ischemia causes clinical symptoms, like antalgic limp and local tenderness of the medial aspect of the foot over the navicular." Main Distractor: E) Dorsum of the foot over the cuneiforms. While the cuneiforms are adjacent, the navicular is the primary affected bone and the site of tenderness.
Question 59
A 6-year-old boy presents with an antalgic limp and medial foot pain. Anteroposterior and lateral radiographs of the foot are obtained.
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 13.23 a–c states, "Note the fragmentation of navicular bone on right side, especially in lateral view." This is the hallmark radiographic finding in the acute phase. Main Distractor: B) Sclerosis of the talus. While sclerosis of the navicular can occur, sclerosis of the talus is not a characteristic finding of Köhler's disease I.
Question 60
A 6-year-old boy was diagnosed with Köhler’s disease I based on an antalgic limp, medial foot tenderness, and navicular fragmentation on radiographs. He is now 13 years old and asymptomatic.
View Answer & Explanation
Correct Answer: B
Rationale: Fig. 13.23 a–c explicitly states, "Seven years later at age 13 a complete rebuilding of the navicular bone is demonstrated on radiograph (c)." This indicates the self-limiting and reconstructive nature of the disease. Main Distractor: A) Persistent fragmentation and collapse of the navicular. This describes the acute phase, not the typical healed phase of Köhler's disease I.
Question 61
A 6-year-old boy presents with an antalgic limp due to Köhler’s disease I. He experiences pain over the medial aspect of his foot.
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "The child can walk with an increased weight on the lateral side of the foot." This is a compensatory mechanism to offload the painful medial aspect of the foot. Main Distractor: C) By increasing weight on the medial side of the foot. This would exacerbate the pain over the affected navicular bone.
Question 62
A 5-year-old boy is diagnosed with Köhler’s disease I. The etiology is linked to the timing of bone ossification in children.
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "as the navicular is the last tarsal bone to ossify in children." This delayed ossification is implicated in its vulnerability to compression and ischemia. Main Distractor: A) It is the first tarsal bone to ossify. This is the opposite of what is stated in the text.
Question 63
A 7-year-old boy presents with Köhler’s disease I. The proposed mechanism involves mechanical factors and vascular compromise.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Compression involves the vessels in central spongy bone leading to ischemia." This is the direct link between mechanical compression and the avascular necrosis. Main Distractor: A) Compression directly causes a fracture of the navicular. While fragmentation is seen, it is a consequence of avascular necrosis, not a direct traumatic fracture from compression.
Question 64
A 6-year-old girl is diagnosed with Köhler’s disease I, which is characterized as avascular necrosis of the navicular bone.
View Answer & Explanation
Correct Answer: C
Rationale: The term "avascular necrosis" literally means death of tissue due to a lack of blood supply (a-vascular). Main Distractor: A) Nerve supply. While nerve supply is crucial for sensation, "avascular" specifically refers to the absence of blood vessels, not nerves.
Question 65
A 45-year-old female presents with progressive proximal muscle weakness and a characteristic skin rash. Physical examination reveals heliotrope rash and Gottron's papules. No specific radiographic findings are noted.
View Answer & Explanation
Correct Answer: B
Rationale: The provided text describes dermatomyositis as a "systemic immune disorder, a primary inflammatory myopathy with autoimmune pathogenesis." This directly aligns with option B. Option A is incorrect because while it is autoimmune, "localized vasculitis" does not fully characterize the systemic inflammatory myopathy described.
Question 66
A 58-year-old male reports difficulty climbing stairs and lifting objects overhead. Physical examination reveals symmetrical weakness predominantly in the shoulder and hip girdles. Skin examination shows a faint rash on the eyelids. Radiographs of the extremities are unremarkable.
View Answer & Explanation
Correct Answer: C
Rationale: The text states that dermatomyositis is associated with "substantial muscle weakening in its course, especially proximally in the extremities." This directly supports option C. Option A is incorrect as distal muscle weakness is not the characteristic pattern described for dermatomyositis.
Question 67
A 30-year-old patient is diagnosed with dermatomyositis after presenting with muscle weakness and characteristic skin findings. The patient asks about the typical demographic distribution of the disease.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context explicitly states, "Women are affected twice more than men." Therefore, option C is the correct answer. Option B is incorrect as it presents the inverse of the stated gender prevalence.
Question 68
A 10-year-old boy presents with a new onset skin rash and mild muscle weakness. His parents are concerned about the diagnosis of dermatomyositis, questioning if it typically manifests in childhood. No specific radiographic findings are noted.
View Answer & Explanation
Correct Answer: D
Rationale: The text indicates, "First skin signs can appear during childhood as well as in adults." This makes option D the correct answer. Option A is incorrect because the text explicitly mentions childhood onset of skin signs.
Question 69
A 68-year-old female is diagnosed with dermatomyositis. Her physician discusses the importance of screening for associated conditions. No specific radiographic findings are noted.
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "In 7–66% of cases of adult dermatomyositis, different malignant tumors can develop." This highlights the strong association with malignancy in adults, making option B correct. Option C, while a common concern in elderly females, is not specifically listed as a direct comorbidity of adult dermatomyositis in the provided text.
Question 70
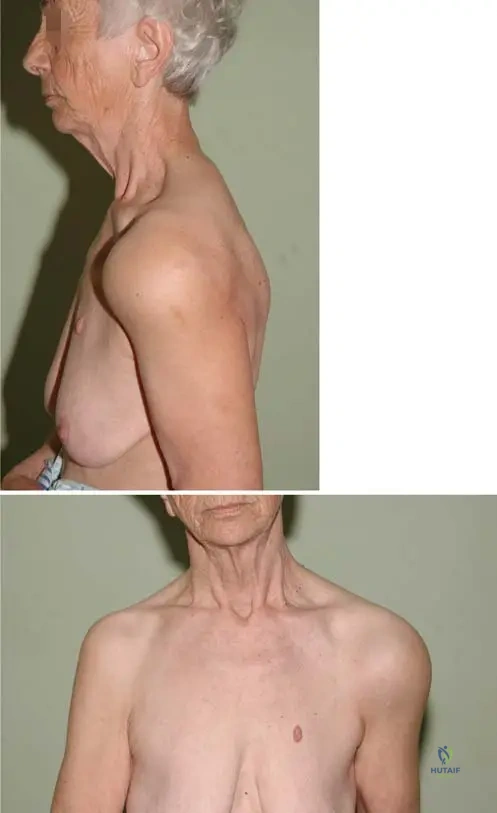
A 62-year-old patient presents with a rash over the breast and noticeable purplish discoloration and swelling around the eyelids. Physical examination confirms proximal muscle weakness. Radiographs are unremarkable.

View Answer & Explanation
Correct Answer: B
Rationale: Figure 12.18b explicitly describes "heliotrope rush and heliotrope edema of the eyelids." This characteristic purplish discoloration and swelling is a hallmark of dermatomyositis. Option A, malar rash, is typically associated with systemic lupus erythematosus and is not the specific term used for the eyelid finding in this context.
Question 71
A female patient presents with violet-colored skin pigmentation on the extensor surfaces of her metacarpophalangeal joints. She also reports proximal muscle weakness. Radiographs are unremarkable.

View Answer & Explanation
Correct Answer: C
Rationale: Figure 12.19 clearly labels the depicted lesions as "Gottron’s papules over the metacarpophalangeal joints (violet-colored skin pigmentation on the extensor surface of small joints)." Option D, Mechanic's hands, is another skin finding in myositis but is not the specific term used to describe the lesions shown in the image or the primary characteristic finding on the MCP joints.
Question 72
A 48-year-old female with dermatomyositis has prominent Gottron's papules on her hands. She reports difficulty with wound healing in these areas. Radiographs are unremarkable.
View Answer & Explanation
Correct Answer: B
Rationale: The description for Figure 12.19 states that Gottron's papules are "often complicated with cutaneous ulcers and poor wound closure or poor healing." This directly supports option B. While other skin changes can occur, cutaneous ulcers and poor healing are specifically mentioned as common complications of Gottron's papules.
Question 73
An 8-year-old boy with a history of dermatomyositis presents with stiffness and limited range of motion in his extremities. An anteroposterior and lateral radiograph of his thigh is obtained.

View Answer & Explanation
Correct Answer: C
Rationale: Figure 12.20a, b describes "Calcareous deposits in subcutis of an 8-year-old boy in anteroposterior (a) and lateral (b) radiograph." The text further links this to "severe and debilitating calcinosis." Therefore, option C is the correct term. Option B, heterotopic ossification, is a broader term for bone formation in soft tissue, but "calcinosis" is the specific term used in the context of dermatomyositis for these deposits.
Question 74
A young patient with dermatomyositis develops extensive subcutaneous calcifications, confirmed on radiographs. Physical examination reveals significant limitation in joint movement.
View Answer & Explanation
Correct Answer: C
Rationale: The text states that "severe and debilitating calcinosis can be observed because of calcification of muscles with contractures." This directly explains the musculoskeletal complication of extensive calcinosis, making option C correct. Option A, pathological fractures, is not specifically mentioned as a direct consequence of calcinosis in the provided text.
Question 75
A 55-year-old female with a long-standing diagnosis of dermatomyositis presents with progressive shortness of breath and a persistent cough. Physical examination reveals crackles on lung auscultation. Radiographs are unremarkable for acute findings.
View Answer & Explanation
Correct Answer: C
Rationale: The text lists "pulmonary fibrosis" as one of the "other extraskeletal differences" associated with dermatomyositis. This aligns with the patient's symptoms of progressive shortness of breath and cough. Option D, pleural effusion, is not specifically mentioned as an extraskeletal manifestation in the provided text.
Question 76
A 60-year-old male
Question 76
A 58-year-old female presents with progressive proximal muscle weakness, difficulty climbing stairs, and a characteristic heliotrope rash around her eyes. During her workup, a cardiac evaluation is performed due to new-onset palpitations and fatigue.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context explicitly lists myocarditis as one of the extraskeletal differences associated with dermatomyositis. Other cardiac manifestations include conduction abnormalities, arrhythmias, coronary artery disease, and pericarditis. Aortic stenosis, mitral valve prolapse, atrial fibrillation, and ventricular septal defect are not specifically highlighted as direct associations in the provided text, although arrhythmias (D) are mentioned, myocarditis (A) is a more direct and severe cardiac involvement listed.
Question 76
A 65-year-old male with a history of dermatomyositis, characterized by muscle weakness and Gottron's papules, presents with increasing shortness of breath and a persistent dry cough. Pulmonary function tests show restrictive lung disease.
View Answer & Explanation
Correct Answer: A
Rationale: Pulmonary fibrosis is explicitly listed as an extraskeletal difference associated with dermatomyositis. The symptoms of shortness of breath and dry cough, along with restrictive lung disease, are consistent with pulmonary fibrosis. Asthma, bronchiectasis, emphysema, and pleural effusion are not specifically mentioned as direct associations in the provided text.
Question 76
A 49-year-old female diagnosed with dermatomyositis, presenting with classic skin findings and proximal muscle weakness, reports increasing difficulty swallowing both solids and liquids, leading to weight loss.
View Answer & Explanation
Correct Answer: A
Rationale: Dysphagia is specifically listed as an extraskeletal difference associated with dermatomyositis. Difficulty swallowing is a common and significant complication. Gastric ulcer, cholecystitis, pancreatitis, and diverticulitis are not mentioned as direct associations in the provided text.
Question 76
A 55-year-old patient with dermatomyositis, characterized by symmetrical proximal muscle weakness and a heliotrope rash, reports recent changes in her vision, including blurred vision and scotomas.
View Answer & Explanation
Correct Answer: A
Rationale: Retinopathy is explicitly listed as an extraskeletal difference associated with dermatomyositis. The reported visual changes are consistent with retinal involvement. Cataracts, glaucoma, optic neuritis, and conjunctivitis are not specifically mentioned as direct associations in the provided text.
Question 76
A 55-year-old female presents with difficulty climbing stairs and lifting objects overhead. Examination reveals a heliotrope rash and Gottron's papules. Electromyography shows findings consistent with an inflammatory myopathy.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context states that dermatomyositis is associated with "substantial muscle weakening in its course, especially proximally in the extremities." It also mentions "symmetrical, proximal muscle weakness" in the context of calcinosis, reinforcing this pattern. Therefore, the weakness is typically symmetrical and proximal. Asymmetrical or distal weakness is not characteristic of dermatomyositis.
Question 76
A 48-year-old female presents with progressive muscle weakness and skin changes. On examination, violet-colored skin pigmentation is noted over the extensor surfaces of her metacarpophalangeal joints.
View Answer & Explanation
Correct Answer: A
Rationale: The image description and clinical context explicitly define "Gottron’s papules over the metacarpophalangeal joints (violet-colored skin pigmentation on the extensor surface of small joints)." This is a pathognomonic skin finding for dermatomyositis. Heliotrope rash is periorbital, Shawl sign and V-sign are rashes on the upper back/shoulders and anterior chest respectively, and Mechanic's hands are rough, cracked skin on the lateral and palmar aspects of the fingers, not violet papules.
Question 76
A 52-year-old female with dermatomyositis presents with violet-colored papules over her metacarpophalangeal joints. She reports difficulty with wound healing in these areas, and a small ulcer has developed on one of the papules.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 12.19 explicitly states that Gottron's papules "It is often complicated with cutaneous ulcers and poor wound closure or poor healing." This directly matches the patient's presentation. Hyperkeratosis, psoriatic plaques, fungal infections, and contact dermatitis are not specifically mentioned as complications of Gottron's papules in the provided text.
Question 76
An 8-year-old boy presents with progressive muscle weakness and skin changes. Radiographs of his extremities reveal extensive calcareous deposits in the subcutis, as shown in the provided images.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 12.20 a, b describes "Calcareous deposits in subcutis of an 8-year-old boy." This finding is specifically referred to as calcinosis in the text, which is a known complication of dermatomyositis, particularly in children. Osteoporosis, osteomyelitis, rhabdomyolysis, and gouty tophi are distinct conditions and do not describe subcutaneous calcareous deposits in this context.
Question 76
A 10-year-old boy with dermatomyositis develops severe calcinosis, as evidenced by subcutaneous calcareous deposits on radiographs. His parents report that he is losing range of motion in his joints, particularly his elbows and knees.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 12.20 a, b states that "severe and debilitating calcinosis can be observed because of calcification of muscles with contractures." This directly links calcinosis to the development of muscle contractures, which would explain the loss of joint range of motion. Pathological fractures, joint dislocations, ligamentous laxity, and nerve entrapment are not specifically mentioned as direct sequelae of calcinosis in the provided text.
Question 76
A 62-year-old patient with dermatomyositis presents with a rash over the breast and heliotrope edema of the eyelids. On physical examination, the physician also notes an abnormal distribution of subcutaneous fat, with areas of both fat loss and accumulation.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 12.18 a, b explicitly mentions "lipodystrophy" as a finding in this patient. Lipodystrophy refers to an abnormal distribution of fat in the body. Lipoatrophy is specifically fat loss, while lipodystrophy encompasses both loss and accumulation. Lipoma, cellulitis, and panniculitis are distinct conditions not directly describing the general fat distribution changes seen in dermatomyositis.
Question 76
A physician is educating a medical student about the epidemiology of dermatomyositis, emphasizing its prevalence and demographic characteristics.
View Answer & Explanation
Correct Answer: A
Rationale: The provided text explicitly states, "Women are affected twice more than men." This is a direct epidemiological fact about dermatomyositis. The other options contradict this statement.
Question 76
A 3-year-old child is diagnosed with dermatomyositis, presenting with characteristic skin findings including a heliotrope rash and Gottron's papules. The parents inquire about the typical age of onset for these skin manifestations.
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "First skin signs can appear during childhood as well as in adults." This indicates that dermatomyositis can manifest cutaneously across a broad age range, including pediatric and adult populations. The other options are incorrect based on this information.
Question 76
A 58-year-old female presents with proximal muscle weakness, a heliotrope rash, and Gottron's papules. Further workup reveals evidence of pulmonary fibrosis and cardiac conduction abnormalities.
View Answer & Explanation
Correct Answer: A
Rationale: The introductory sentence of the text describes dermatomyositis as a "systemic immune disorder." The presence of muscle weakness, skin manifestations, and involvement of multiple organ systems (pulmonary and cardiac in this vignette) strongly supports its systemic nature. It is not merely a localized skin condition, pure muscular dystrophy, or neuropathic disorder, and it clearly has systemic involvement.
Question 76
A muscle biopsy from a 45-year-old male with progressive muscle weakness and characteristic skin findings shows perivascular and perimysial inflammatory infiltrates. This finding helps classify the underlying pathology.
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly states that dermatomyositis is a "primary inflammatory myopathy." The biopsy findings of inflammatory infiltrates are consistent with this classification. Metabolic, congenital, toxic, and dystrophic myopathies represent different categories of muscle disorders with distinct underlying etiologies and pathological features.
Question 76
A researcher is studying the underlying mechanisms of dermatomyositis, focusing on the immune system's role in its development and progression.
View Answer & Explanation
Correct Answer: A
Rationale: The text clearly states that dermatomyositis is a "systemic immune disorder, a primary inflammatory myopathy with autoimmune pathogenesis." This directly identifies its underlying cause as autoimmune. While genetic factors may play a role in susceptibility, and infections can sometimes trigger autoimmune responses, the primary pathogenesis is autoimmune, not purely infectious, genetic, traumatic, or due to nutritional deficiency.
Question 76
A public health official is reviewing epidemiological data on rare diseases to allocate resources for research and patient support. They are specifically interested in the general population prevalence of dermatomyositis.
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly states, "The prevalence is 1:100,000." This is a direct factual recall from the provided information. The other options are incorrect prevalence figures.
Question 76
A 62-year-old patient presents with new onset proximal muscle weakness and a characteristic rash over her breast, as depicted in the image. This rash is a recognized cutaneous manifestation of dermatomyositis.
View Answer & Explanation
Correct Answer: A
Rationale: The image context (Fig. 12.18 a, b) shows a "rash over the breast (a)" and "heliotrope rush and heliotrope edema of the eyelids (b)" in the same patient. While the rash over the breast is not given a specific name in the text (it's often called a V-sign or Shawl sign), the question asks for *another* characteristic skin finding. The heliotrope rash is explicitly mentioned in the same figure's context as a key feature of dermatomyositis. Psoriatic plaques, urticaria, eczema, and rosacea are not characteristic skin findings of dermatomyositis.
Question 76
<p
Question 77
A 58-year-old female presents with progressive proximal muscle weakness, difficulty climbing stairs, and a characteristic heliotrope rash around her eyes. During her workup, a cardiac evaluation is performed due to new-onset palpitations and fatigue.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context explicitly lists myocarditis as one of the extraskeletal differences associated with dermatomyositis. Other cardiac manifestations include conduction abnormalities, arrhythmias, coronary artery disease, and pericarditis. Aortic stenosis, mitral valve prolapse, atrial fibrillation, and ventricular septal defect are not specifically highlighted as direct associations in the provided text, although arrhythmias (D) are mentioned, myocarditis (A) is a more direct and severe cardiac involvement listed.
Question 78
A 65-year-old male with a history of dermatomyositis, characterized by muscle weakness and Gottron's papules, presents with increasing shortness of breath and a persistent dry cough. Pulmonary function tests show restrictive lung disease.
View Answer & Explanation
Correct Answer: A
Rationale: Pulmonary fibrosis is explicitly listed as an extraskeletal difference associated with dermatomyositis. The symptoms of shortness of breath and dry cough, along with restrictive lung disease, are consistent with pulmonary fibrosis. Asthma, bronchiectasis, emphysema, and pleural effusion are not specifically mentioned as direct associations in the provided text.
Question 79
A 49-year-old female diagnosed with dermatomyositis, presenting with classic skin findings and proximal muscle weakness, reports increasing difficulty swallowing both solids and liquids, leading to weight loss.
View Answer & Explanation
Correct Answer: A
Rationale: Dysphagia is specifically listed as an extraskeletal difference associated with dermatomyositis. Difficulty swallowing is a common and significant complication. Gastric ulcer, cholecystitis, pancreatitis, and diverticulitis are not mentioned as direct associations in the provided text.
Question 80
A 55-year-old patient with dermatomyositis, characterized by symmetrical proximal muscle weakness and a heliotrope rash, reports recent changes in her vision, including blurred vision and scotomas.
View Answer & Explanation
Correct Answer: A
Rationale: Retinopathy is explicitly listed as an extraskeletal difference associated with dermatomyositis. The reported visual changes are consistent with retinal involvement. Cataracts, glaucoma, optic neuritis, and conjunctivitis are not specifically mentioned as direct associations in the provided text.
Question 81
A 55-year-old female presents with difficulty climbing stairs and lifting objects overhead. Examination reveals a heliotrope rash and Gottron's papules. Electromyography shows findings consistent with an inflammatory myopathy.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context states that dermatomyositis is associated with "substantial muscle weakening in its course, especially proximally in the extremities." It also mentions "symmetrical, proximal muscle weakness" in the context of calcinosis, reinforcing this pattern. Therefore, the weakness is typically symmetrical and proximal. Asymmetrical or distal weakness is not characteristic of dermatomyositis.
Question 82
A 48-year-old female presents with progressive muscle weakness and skin changes. On examination, violet-colored skin pigmentation is noted over the extensor surfaces of her metacarpophalangeal joints.
View Answer & Explanation
Correct Answer: A
Rationale: The image description and clinical context explicitly define "Gottron’s papules over the metacarpophalangeal joints (violet-colored skin pigmentation on the extensor surface of small joints)." This is a pathognomonic skin finding for dermatomyositis. Heliotrope rash is periorbital, Shawl sign and V-sign are rashes on the upper back/shoulders and anterior chest respectively, and Mechanic's hands are rough, cracked skin on the lateral and palmar aspects of the fingers, not violet papules.
Question 83
A 52-year-old female with dermatomyositis presents with violet-colored papules over her metacarpophalangeal joints. She reports difficulty with wound healing in these areas, and a small ulcer has developed on one of the papules.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 12.19 explicitly states that Gottron's papules "It is often complicated with cutaneous ulcers and poor wound closure or poor healing." This directly matches the patient's presentation. Hyperkeratosis, psoriatic plaques, fungal infections, and contact dermatitis are not specifically mentioned as complications of Gottron's papules in the provided text.
Question 84
An 8-year-old boy presents with progressive muscle weakness and skin changes. Radiographs of his extremities reveal extensive calcareous deposits in the subcutis, as shown in the provided images.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 12.20 a, b describes "Calcareous deposits in subcutis of an 8-year-old boy." This finding is specifically referred to as calcinosis in the text, which is a known complication of dermatomyositis, particularly in children. Osteoporosis, osteomyelitis, rhabdomyolysis, and gouty tophi are distinct conditions and do not describe subcutaneous calcareous deposits in this context.
Question 85
A 10-year-old boy with dermatomyositis develops severe calcinosis, as evidenced by subcutaneous calcareous deposits on radiographs. His parents report that he is losing range of motion in his joints, particularly his elbows and knees.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 12.20 a, b states that "severe and debilitating calcinosis can be observed because of calcification of muscles with contractures." This directly links calcinosis to the development of muscle contractures, which would explain the loss of joint range of motion. Pathological fractures, joint dislocations, ligamentous laxity, and nerve entrapment are not specifically mentioned as direct sequelae of calcinosis in the provided text.
Question 86
A 62-year-old patient with dermatomyositis presents with a rash over the breast and heliotrope edema of the eyelids. On physical examination, the physician also notes an abnormal distribution of subcutaneous fat, with areas of both fat loss and accumulation.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 12.18 a, b explicitly mentions "lipodystrophy" as a finding in this patient. Lipodystrophy refers to an abnormal distribution of fat in the body. Lipoatrophy is specifically fat loss, while lipodystrophy encompasses both loss and accumulation. Lipoma, cellulitis, and panniculitis are distinct conditions not directly describing the general fat distribution changes seen in dermatomyositis.
Question 87
A physician is educating a medical student about the epidemiology of dermatomyositis, emphasizing its prevalence and demographic characteristics.
View Answer & Explanation
Correct Answer: A
Rationale: The provided text explicitly states, "Women are affected twice more than men." This is a direct epidemiological fact about dermatomyositis. The other options contradict this statement.
Question 88
A 3-year-old child is diagnosed with dermatomyositis, presenting with characteristic skin findings including a heliotrope rash and Gottron's papules. The parents inquire about the typical age of onset for these skin manifestations.
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "First skin signs can appear during childhood as well as in adults." This indicates that dermatomyositis can manifest cutaneously across a broad age range, including pediatric and adult populations. The other options are incorrect based on this information.
Question 89
A 58-year-old female presents with proximal muscle weakness, a heliotrope rash, and Gottron's papules. Further workup reveals evidence of pulmonary fibrosis and cardiac conduction abnormalities.
View Answer & Explanation
Correct Answer: A
Rationale: The introductory sentence of the text describes dermatomyositis as a "systemic immune disorder." The presence of muscle weakness, skin manifestations, and involvement of multiple organ systems (pulmonary and cardiac in this vignette) strongly supports its systemic nature. It is not merely a localized skin condition, pure muscular dystrophy, or neuropathic disorder, and it clearly has systemic involvement.
Question 90
A muscle biopsy from a 45-year-old male with progressive muscle weakness and characteristic skin findings shows perivascular and perimysial inflammatory infiltrates. This finding helps classify the underlying pathology.
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly states that dermatomyositis is a "primary inflammatory myopathy." The biopsy findings of inflammatory infiltrates are consistent with this classification. Metabolic, congenital, toxic, and dystrophic myopathies represent different categories of muscle disorders with distinct underlying etiologies and pathological features.
Question 91
A researcher is studying the underlying mechanisms of dermatomyositis, focusing on the immune system's role in its development and progression.
View Answer & Explanation
Correct Answer: A
Rationale: The text clearly states that dermatomyositis is a "systemic immune disorder, a primary inflammatory myopathy with autoimmune pathogenesis." This directly identifies its underlying cause as autoimmune. While genetic factors may play a role in susceptibility, and infections can sometimes trigger autoimmune responses, the primary pathogenesis is autoimmune, not purely infectious, genetic, traumatic, or due to nutritional deficiency.
Question 92
A public health official is reviewing epidemiological data on rare diseases to allocate resources for research and patient support. They are specifically interested in the general population prevalence of dermatomyositis.
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly states, "The prevalence is 1:100,000." This is a direct factual recall from the provided information. The other options are incorrect prevalence figures.
Question 93
A 62-year-old patient presents with new onset proximal muscle weakness and a characteristic rash over her breast, as depicted in the image. This rash is a recognized cutaneous manifestation of dermatomyositis.
View Answer & Explanation
Correct Answer: A
Rationale: The image context (Fig. 12.18 a, b) shows a "rash over the breast (a)" and "heliotrope rush and heliotrope edema of the eyelids (b)" in the same patient. While the rash over the breast is not given a specific name in the text (it's often called a V-sign or Shawl sign), the question asks for *another* characteristic skin finding. The heliotrope rash is explicitly mentioned in the same figure's context as a key feature of dermatomyositis. Psoriatic plaques, urticaria, eczema, and rosacea are not characteristic skin findings of dermatomyositis.
Question 94
A 7-year-old female presents with her parents due to a noticeable asymmetry of her shoulders. On physical examination, the left shoulder appears elevated and displaced anteriorly. Radiographs confirm a congenital high scapula on the left side. Which of the following best defines this condition?

View Answer & Explanation
Correct Answer: C
Rationale: Sprengel's deformity is defined as a congenital abnormal elevation of one or both scapulas from the normal anatomic scapula position. Options A, B, D, and E describe incorrect definitions or unrelated conditions. The main distractor, E, incorrectly states scapular depression.
Question 95
A 5-year-old male is diagnosed with Sprengel's deformity of the right shoulder. Imaging reveals an abnormal articulation between the scapula and the vertebral column. This specific anatomical structure is known as which of the following?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that abnormal articulations of the scapula with the vertebral column are named as omovertebral bone. Options A, C, D, and E are either unrelated conditions or incorrect anatomical terms for this specific anomaly. The main distractor, D, is an associated anomaly but not the specific articulation.
Question 96
A 3-year-old female presents with a congenital high left scapula. Her parents inquire about the potential causes. One proposed pathogenesis involves a failure of scapular descent. Which of the following muscular factors is implicated in this theory?
View Answer & Explanation
Correct Answer: C
Rationale: The text lists "a defective musculature, unable to draw the scapula caudally" as a possibility for the failure of descent. It also mentions "a normal musculature, which is unable to draw the scapula caudally too." Options A, B, D, and E are not explicitly mentioned as pathogenic mechanisms for Sprengel's deformity in the provided text. The main distractor, E, describes a muscle that elevates the scapula, but the pathogenesis focuses on the inability to draw it caudally.
Question 97
A 6-year-old boy is diagnosed with Sprengel's deformity. During the workup, the orthopedic surgeon emphasizes the importance of screening for associated anomalies. Which of the following organ systems is commonly affected by these associated malformations?
View Answer & Explanation
Correct Answer: D
Rationale: The text states, "This anomaly is often associated with other anomalies of the skeletal system and other organs." While other organs can be involved, the skeletal system is explicitly mentioned as commonly affected. Options A, B, C, and E are not specifically highlighted as commonly associated in the provided text. The main distractor, E, is not as broadly stated as the skeletal system.
Question 98
A 4-year-old girl presents with a visibly elevated right shoulder. Clinical examination reveals not only elevation but also a specific rotation of the scapula. How is the scapula typically rotated about the sagittal axis in Sprengel's deformity?
View Answer & Explanation
Correct Answer: B
Rationale: Figure 13.3 description states, "The scapula is rotated about the sagittal axis, bringing the upper medial angle away from the spinal column and the lower angle close to it." Options A, C, D, and E describe incorrect or incomplete rotational patterns. The main distractor, A, reverses the correct description.
Question 99
A 10-year-old male is diagnosed with Sprengel's deformity. His orthopedic surgeon explains the possibility of an omovertebral bone contributing to the condition. What is the approximate prevalence of an omovertebral bone in patients with Sprengel's deformity?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states, "One third of patients has omovertebral bone." Options A, C, D, and E are incorrect prevalence rates. The main distractor, C, is a common guess but incorrect based on the text.
Question 100
A 2-year-old female presents with a congenital high scapula. A 3D CT scan confirms the presence of an omovertebral bone. This structure typically extends from the superomedial border of the scapula to which specific region of the cervical spine?
View Answer & Explanation
Correct Answer: B
Rationale: The text states the omovertebral bone "most commonly the fourth to seventh cervical vertebrae (C4-C7) spinous processes, lamina, or transverse processes." Options A, C, D, and E describe incorrect vertebral levels or anatomical locations. The main distractor, A, is too high in the cervical spine.
You Might Also Like