Orthopaedic Board Review: Synovial Chondromatosis, Charcot Joint, Fibrous Dysplasia, Bone Metastases | Part 21
Key Takeaway
This ABOS Board Review covers key orthopaedic pathologies: synovial chondromatosis, neurogenic osteoarthropathy (Charcot joint), fibrous dysplasia, and metastatic bone disease. It details their clinical presentations, diagnostic features, and management principles, providing essential knowledge for orthopaedic surgeons preparing for their board examinations.
Question 1
A 25-year-old male presents with intermittent right knee pain, swelling, and mechanical locking. He recalls a twisting injury to his knee a few months prior. Physical exam reveals a joint effusion and pain with specific maneuvers. Plain radiographs are normal. What is the most important differential diagnosis to consider alongside synovial chondromatosis in this patient?
View Answer & Explanation
Correct Answer: C
Rationale: The symptoms of intermittent pain, swelling, and mechanical locking, especially after a twisting injury, are highly suggestive of a meniscal tear with a displaced fragment (bucket-handle tear) which can cause true locking. While synovial chondromatosis can cause similar mechanical symptoms, the history of trauma and the possibility of a displaced meniscal fragment make this a critical differential. Gout and septic arthritis typically present with acute, severe inflammation. Rheumatoid arthritis presents with chronic inflammatory polyarthritis. Osteoarthritis is less common in a 25-year-old and typically presents with crepitus and stiffness rather than acute locking from a loose body.
Question 2
A 55-year-old patient has a long-standing history of untreated synovial chondromatosis in the knee, characterized by numerous loose bodies and chronic inflammation. What is the most common long-term complication associated with this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The chronic presence of multiple loose bodies and synovial inflammation in synovial chondromatosis can lead to progressive damage to the articular cartilage, ultimately resulting in secondary degenerative arthritis. While malignant transformation to chondrosarcoma is a rare but serious complication, it is far less common than the development of osteoarthritis. Pathologic fracture, systemic amyloidosis, and peripheral neuropathy are not typical complications of synovial chondromatosis.
Question 3
A 62-year-old male with a history of synovial chondromatosis in his knee presents with rapidly worsening pain, swelling, and a palpable mass. Imaging reveals an aggressive, destructive lesion with cortical erosion. Biopsy is performed. What rare but serious complication should be considered?
View Answer & Explanation
Correct Answer: C
Rationale: Although rare, synovial chondromatosis has a documented potential for malignant transformation into secondary chondrosarcoma. This should be suspected in cases of rapidly worsening symptoms, aggressive bone destruction, or the development of a soft tissue mass in a patient with a known history of synovial chondromatosis. Recurrent benign disease would not typically present with aggressive destruction. Septic arthritis would have acute inflammatory signs. PVNS is a benign proliferative condition. Stress fractures are typically related to overuse and do not present with an aggressive mass.
Question 4
A 30-year-old female undergoes arthroscopic removal of loose bodies for synovial chondromatosis of the knee. To minimize the risk of recurrence, what additional procedure is often recommended, especially in cases with diffuse synovial involvement?
View Answer & Explanation
Correct Answer: B
Rationale: The primary source of synovial chondromatosis is the metaplastic synovium. If only the loose bodies are removed, and active intrasynovial disease (Milgram Stage I or II) is present, the risk of recurrence is high. Therefore, partial or complete synovectomy (arthroscopic or open, depending on extent) is often recommended to remove the source of the chondral nodules and reduce recurrence rates. Corticosteroid injections, NSAIDs, and joint aspiration are conservative measures that do not address the underlying pathology. Radiation therapy is not a standard treatment for benign synovial chondromatosis.
Question 5
A 68-year-old male presents with knee pain and a single, large calcified loose body on plain radiographs, along with significant degenerative changes. This presentation differs from a typical case of primary synovial chondromatosis. What is the most likely distinction?
View Answer & Explanation
Correct Answer: B
Rationale: Synovial chondromatosis can be classified as primary (idiopathic) or secondary. Primary synovial chondromatosis typically affects younger individuals, involves multiple small loose bodies, and is due to synovial metaplasia. Secondary synovial chondromatosis usually occurs in older patients with pre-existing degenerative joint disease, often involves fewer, larger loose bodies, and is thought to be a reactive process. The patient's age, single large loose body, and degenerative changes are characteristic of secondary synovial chondromatosis. PVNS, OCD, gout, and rheumatoid arthritis have distinct clinical and radiographic features.
Question 6
A 32-year-old female is diagnosed with synovial chondromatosis of the hip, with multiple loose bodies identified on MRI. The surgeon is planning surgical intervention. What is a key consideration when deciding between an arthroscopic versus an open approach for hip synovial chondromatosis?
View Answer & Explanation
Correct Answer: C
Rationale: The choice between arthroscopic and open surgery for synovial chondromatosis, especially in complex joints like the hip, largely depends on the extent of the disease. Arthroscopy is preferred for smaller, fewer loose bodies and limited synovial involvement. However, for numerous or very large loose bodies, extensive diffuse synovial proliferation, or difficult-to-access areas, an open approach may be necessary to ensure complete removal and reduce recurrence. While patient preference, labral tears, BMI, and equipment are factors, the extent of the pathology is the primary determinant of surgical approach.
Question 7
A 48-year-old male presents with chronic elbow pain and mechanical symptoms. Plain radiographs show subtle calcifications. A CT scan is ordered to further characterize the intra-articular pathology. What specific advantage does CT offer over plain radiographs or MRI in the diagnosis of synovial chondromatosis?
View Answer & Explanation
Correct Answer: C
Rationale: CT scans excel at visualizing bone and calcified structures. In synovial chondromatosis, CT provides superior detail regarding the number, size, morphology, and precise location of calcified loose bodies compared to plain radiographs. While MRI is better for soft tissue and non-calcified bodies (A, B), and can assess cartilage (D), CT's strength lies in calcification. Differentiation between benign and malignant lesions (E) often requires biopsy, though imaging can raise suspicion.
Question 8
A 37-year-old female presents with recurrent knee effusions and mechanical symptoms. Plain radiographs are unremarkable. Arthrocentesis is performed, and the synovial fluid is analyzed. Which of the following findings would be most consistent with synovial chondromatosis?
View Answer & Explanation
Correct Answer: C
Rationale: Synovial chondromatosis is a benign metaplastic process, not typically inflammatory or infectious. Therefore, the synovial fluid is usually non-inflammatory, appearing clear and viscous, with a normal or mildly elevated cell count and no crystals. Turbid fluid with elevated WBC and positive Gram stain indicates septic arthritis. Bloody fluid with hemosiderin suggests PVNS or trauma. Milky fluid with urate crystals indicates gout. Cloudy fluid with calcium pyrophosphate crystals indicates pseudogout.
Question 9
A 65-year-old male presents with progressive, painless destruction of his right knee joint. He reports a long history of poorly controlled diabetes mellitus. Physical examination reveals significant joint laxity, effusions, and crepitus, but surprisingly minimal pain despite the severe degenerative changes. Sensory examination demonstrates diminished proprioception and deep sensation in the affected limb. Radiographs show severe disorganization of the joint with fragmentation and sclerosis.
View Answer & Explanation
Correct Answer: D
Rationale: The clinical presentation of painless joint destruction, loss of proprioception and deep sensation, and association with diabetes mellitus are classic features of neurogenic osteoarthropathy, also known as Charcot joint. This condition is characterized by bone and joint changes secondary to loss of sensation. Osteoarthritis typically presents with pain proportional to the degeneration, and rheumatoid arthritis involves inflammatory synovitis with specific serological markers. Gout presents with acute, severe pain and crystal deposition. Septic arthritis involves signs of infection.
Question 10
A 58-year-old female with a history of syringomyelia presents with a rapidly destructive left shoulder joint. She denies significant pain despite marked instability and crepitus. Neurological examination reveals a cape-like distribution of pain and temperature sensation loss, along with diminished proprioception in the left upper extremity. Radiographs demonstrate severe joint disorganization, subluxation, and bone fragmentation.
View Answer & Explanation
Correct Answer: C
Rationale: The text states that the pathophysiology of neurogenic osteoarthropathy (Charcot joint) is that "the loss of proprioception and deep sensation result in recurrent trauma, and ultimately lead to progressive destruction." Syringomyelia is listed as an associated condition. Autoimmune inflammation, bacterial infection, collagen defects, or steroid use are not described as primary mechanisms for this condition in the provided text.
Question 11
A 72-year-old male with a history of tabes dorsalis presents with a swollen, unstable right ankle. He reports minimal discomfort despite significant joint deformity and instability. Physical examination reveals absent deep tendon reflexes and impaired vibratory and position sense in the lower extremities. Radiographs show severe degenerative changes, osteolysis, and new bone formation in the ankle joint.
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Charcot first described the relationship between loss of sensation and arthropathy in 1868." The clinical scenario describes a Charcot joint, and tabes dorsalis is listed as an associated condition. The other individuals are not credited with this specific description in the provided text.
Question 12
A 45-year-old male with a history of chronic alcohol abuse and peripheral neuropathy presents with a rapidly progressing, painless destruction of his midfoot. Physical examination reveals significant swelling, erythema, and warmth, along with a rocker-bottom deformity. Sensory testing confirms a stocking-glove distribution of sensory loss. Radiographs show extensive bone resorption, fragmentation, and joint subluxation.
View Answer & Explanation
Correct Answer: C
Rationale: The text describes an alternative theory for the pathophysiology of neurogenic osteoarthropathy: "Another theory postulates that neurally mediated vascular reflex results in hyperemia, which can cause osteoclast bone resorption." The patient's history of alcohol abuse with peripheral neuropathy is listed as an associated condition. The other options are not described as primary mechanisms in the provided text.
Question 13
A 30-year-old male paraplegic due to a traumatic spinal cord injury sustained 5 years prior presents with a swollen, unstable left ankle. He reports no pain. Examination reveals complete loss of sensation below the level of injury. Radiographs show severe disorganization of the ankle joint with extensive osteolysis and new bone formation.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical vignette describes a neurogenic osteoarthropathy in a patient with a history of traumatic paralysis, which is explicitly listed as an associated condition for Charcot's joint. Osteomyelitis is an infection, psoriatic arthritis is an inflammatory condition, rheumatoid arthritis is an autoimmune disease, and hemophilic arthropathy is due to recurrent bleeding, none of which fit the described etiology of sensory loss leading to joint destruction.
Question 14
A 15-year-old female with a known history of spinal dysraphism presents with a progressively deforming and painless right hip joint. Physical examination reveals significant sensory deficits in the lower extremity. Radiographs show severe destruction of the femoral head and acetabulum, with fragmentation and sclerosis.
View Answer & Explanation
Correct Answer: A
Rationale: The text states that the pathophysiology of neurogenic osteoarthropathy is "that the loss of proprioception and deep sensation result in recurrent trauma, and ultimately lead to progressive destruction." Spinal dysraphism is listed as an associated condition. While other factors might be present in spinal dysraphism, the primary mechanism for Charcot joint formation, according to the text, is sensory loss.
Question 15
A 68-year-old male with a long-standing history of poorly controlled type 2 diabetes mellitus presents with a swollen, warm, and deformed left foot. He reports minimal pain despite the severe changes. Physical examination reveals diminished sensation in a stocking-glove distribution. Radiographs show midfoot collapse, fragmentation, and sclerosis, consistent with a Charcot foot.
View Answer & Explanation
Correct Answer: C
Rationale: The provided text explicitly lists "diabetes mellitus" as one of the peripheral neuropathies associated with Charcot's joint. The clinical presentation is classic for a diabetic Charcot foot. Osteoporosis, gout, rheumatoid arthritis, and septic arthritis are distinct conditions with different etiologies and primary pathophysiologies.
Question 16
A 55-year-old female with a history of transverse myelitis presents with a rapidly progressive, painless destruction of her right knee. She has significant sensory deficits below the level of her spinal cord lesion. Radiographs reveal severe joint disorganization, subluxation, and extensive osteolysis.
View Answer & Explanation
Correct Answer: C
Rationale: The text states that the pathophysiology of neurogenic osteoarthropathy is "that the loss of proprioception and deep sensation result in recurrent trauma, and ultimately lead to progressive destruction." Transverse myelitis is listed as an associated condition. The other options are not described as the primary mechanism for Charcot joint in the provided text.
Question 17
A 60-year-old male with a long history of late-stage alcohol abuse and associated peripheral neuropathy presents with a painless, swollen, and unstable left ankle. Physical examination reveals diminished sensation in both lower extremities. Radiographs show severe joint destruction, fragmentation, and sclerosis.
View Answer & Explanation
Correct Answer: D
Rationale: The clinical presentation of painless joint destruction in the setting of late-stage alcohol abuse with peripheral neuropathy (leading to sensory loss) is characteristic of neurogenic osteoarthropathy. The text explicitly lists "alcohol abuse (late stage with peripheral neuropathy)" as an associated condition. Gout, pseudogout, osteoarthritis, and septic arthritis have different etiologies and clinical presentations, typically involving significant pain (except for very advanced osteoarthritis) and not primarily driven by sensory loss.
Question 18
A 40-year-old female with a history of syringomyelia presents with a painless, rapidly destructive right elbow joint. Examination reveals a loss of pain and temperature sensation in a cape-like distribution. Radiographs show severe joint disorganization, fragmentation, and osteolysis.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Charcot’s joint is associated with some degenerative diseases of the spinal cord and other peripheral neuropathies, including syringomyelia..." The clinical vignette describes a Charcot joint in a patient with syringomyelia. The other options are not supported by the provided text as general associations or causes of Charcot joint.
Question 19
A 62-year-old male with a history of diabetes mellitus presents with a progressive, painless deformity of his left foot. Physical examination reveals significant swelling, warmth, and a rocker-bottom deformity. Sensory testing confirms severe peripheral neuropathy. Radiographs show extensive bone fragmentation, joint subluxation, and osteopenia.
View Answer & Explanation
Correct Answer: C
Rationale: The text clearly states that the pathophysiology of neurogenic osteoarthropathy is "that the loss of proprioception and deep sensation result in recurrent trauma, and ultimately lead to progressive destruction." Diabetes mellitus is a listed associated condition. The other options describe different disease processes not aligned with the primary mechanism of Charcot joint as described.
Question 20
A 70-year-old male with a history of tabes dorsalis presents with a painless, swollen, and unstable right knee. Physical examination reveals a positive Romberg sign and absent deep tendon reflexes. Radiographs show severe joint disorganization with extensive osteolysis and new bone formation.
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that "the loss of proprioception and deep sensation result in recurrent trauma, and ultimately lead to progressive destruction" in neurogenic osteoarthropathy. Tabes dorsalis is listed as an associated condition. While hyperemia is mentioned as an alternative theory, it leads to osteoclast bone resorption, not osteoblast activation. The other options are not primary mechanisms for Charcot joint according to the text.
Question 21
A 35-year-old male with a history of traumatic spinal cord injury resulting in paraplegia presents with a painless, swollen, and warm left ankle. He has complete sensory loss below the level of his injury. Radiographs show severe joint destruction, fragmentation, and sclerosis.
View Answer & Explanation
Correct Answer: C
Rationale: The text describes an alternative theory for the pathophysiology of neurogenic osteoarthropathy: "Another theory postulates that neurally mediated vascular reflex results in hyperemia, which can cause osteoclast bone resorption." Traumatic paralysis is listed as an associated condition. The other options are not described as primary mechanisms for Charcot joint in the provided text.
Question 22
A 50-year-old female with a history of diabetes mellitus presents with a painless, rapidly progressing deformity of her right foot. Physical examination reveals significant swelling, warmth, and a rocker-bottom deformity. Sensory examination confirms severe peripheral neuropathy. Radiographs show extensive bone fragmentation, joint subluxation, and osteolysis.
View Answer & Explanation
Correct Answer: A
Rationale: The text defines neurogenic osteoarthropathy as "the bone and joint changes that occur secondary to loss of sensation and accompany a variety of disorders." The clinical vignette describes a classic presentation of diabetic Charcot foot, which is a form of neurogenic osteoarthropathy. The other options describe different disease processes not aligned with the definition provided.
Question 23
A 65-year-old male with a history of syringomyelia presents with a painless, swollen, and unstable left shoulder. He has significant loss of pain and temperature sensation in his left upper extremity. Radiographs show severe joint disorganization, fragmentation, and osteolysis.
View Answer & Explanation
Correct Answer: B
Rationale: The text states that "the loss of proprioception and deep sensation result in recurrent trauma, and ultimately lead to progressive destruction." This highlights the critical role of proprioception in protecting the joint from unperceived trauma. The other options misrepresent or deny the role of proprioception as described in the text.
Question 24
A 58-year-old female with a history of tabes dorsalis presents with a painless, rapidly destructive right hip. Physical examination reveals impaired vibratory and position sense in the lower extremities. Radiographs show severe destruction of the femoral head and acetabulum, with fragmentation and sclerosis.
View Answer & Explanation
Correct Answer: C
Rationale: The text states that "the loss of proprioception and deep sensation result in recurrent trauma, and ultimately lead to progressive destruction." This indicates that loss of deep sensation is a key factor in the pathophysiology of neurogenic osteoarthropathy. Tabes dorsalis is listed as an associated condition. The other options misrepresent or deny the role of deep sensation as described in the text.
Question 25
A 45-year-old male with a history of chronic alcohol abuse and peripheral neuropathy presents with a swollen, warm, and deformed left foot. He reports minimal pain despite the severe changes. Radiographs show extensive bone resorption, fragmentation, and joint subluxation.
View Answer & Explanation
Correct Answer: C
Rationale: The text describes an alternative theory: "Another theory postulates that neurally mediated vascular reflex results in hyperemia, which can cause osteoclast bone resorption." This directly links hyperemia to bone destruction via osteoclast activity. The other options are incorrect interpretations of the role of hyperemia in this context according to the provided text.
Question 26
A 30-year-old female with spinal dysraphism presents with a painless, rapidly progressing deformity of her right ankle. She has significant sensory deficits in the affected limb. Radiographs show severe joint disorganization, fragmentation, and sclerosis.
View Answer & Explanation
Correct Answer: B
Rationale: The text states that "the loss of proprioception and deep sensation result in recurrent trauma, and ultimately lead to progressive destruction." This directly links recurrent trauma to the ultimate outcome of progressive destruction. Spinal dysraphism is listed as an associated condition. The other options do not accurately describe the outcome of recurrent trauma in this context according to the text.
Question 27
A 68-year-old male with a history of both diabetes mellitus and late-stage alcohol abuse with peripheral neuropathy presents with a severely deformed and painless left foot. Physical examination reveals significant sensory loss in a stocking-glove distribution. Radiographs show extensive bone fragmentation, joint subluxation, and sclerosis.
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly lists "diabetes mellitus" and "alcohol abuse (late stage with peripheral neuropathy)" as conditions associated with Charcot's joint. The clinical vignette describes a patient with both these risk factors and a classic presentation of neurogenic osteoarthropathy. The other options are either unrelated conditions or other causes of Charcot joint not directly mentioned as co-occurring in the vignette.
Question 28
A 55-year-old female presents with severe, painful, inflammatory arthritis affecting multiple small joints of her hands and feet, associated with morning stiffness and positive rheumatoid factor. Radiographs show symmetric joint space narrowing, erosions, and juxta-articular osteopenia. She denies any history of neurological deficits or sensory loss.
View Answer & Explanation
Correct Answer: D
Rationale: The clinical vignette describes a classic presentation of rheumatoid arthritis, characterized by painful, inflammatory polyarthritis, morning stiffness, and positive rheumatoid factor, without any sensory loss. Syringomyelia, tabes dorsalis, diabetes mellitus, and traumatic paralysis are all conditions explicitly listed in the text as being associated with neurogenic osteoarthropathy (Charcot joint), which is characterized by *loss of sensation* and *painless* joint destruction. Therefore, rheumatoid arthritis is the condition that *best fits* the description and is *not* an associated cause of Charcot joint as per the provided text.
Question 29
A 65-year-old male presents with progressive deformity and instability in his right ankle. He reports diminished sensation in the foot. Radiographs show significant joint destruction, subluxation, and osteophyte formation.
View Answer & Explanation
Correct Answer: C
Rationale: The text defines neurogenic osteoarthropathy as "the bone and joint changes that occur secondary to loss of sensation and accompany a variety of disorders." The patient's presentation with progressive deformity, instability, joint destruction, and diminished sensation directly aligns with this definition. The main distractor, osteoarthritis, is a common joint disease but is primarily due to mechanical wear and tear, not specifically initiated by loss of sensation.
Question 30
A 72-year-old female with a history of diabetes mellitus presents with a swollen, warm, and deformed left foot. Physical examination reveals decreased proprioception and vibratory sensation. Radiographs demonstrate severe disorganization of the midfoot joints.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Charcot first described the relationship between loss of sensation and arthropathy in 1868." This historical fact directly attributes the initial description of this condition to Charcot. Hippocrates is a general historical figure in medicine but is not specifically associated with the initial description of neurogenic osteoarthropathy.
Question 31
A 58-year-old male with a history of spinal cord injury presents with a rapidly destructive right knee joint. He has profound loss of sensation in the affected limb.
View Answer & Explanation
Correct Answer: C
Rationale: One of the described pathophysiological theories states, "The pathophysiology of the disease is that the loss of proprioception and deep sensation result in recurrent trauma, and ultimately lead to progressive destruction." This directly explains the mechanism in the context of sensory loss. Primary cartilage degeneration (D) is characteristic of osteoarthritis, but in neurogenic osteoarthropathy, the degeneration is secondary to the neurological deficit, not a primary process.
Question 32
A 45-year-old female with syringomyelia develops a swollen, erythematous, and painful shoulder joint. Radiographs show early signs of bone resorption and joint disorganization.
View Answer & Explanation
Correct Answer: B
Rationale: The text describes an alternative pathophysiological theory: "Another theory postulates that neurally mediated vascular reflex results in hyperemia, which can cause osteoclast bone resorption." This directly links hyperemia to bone destruction. Ischemia and avascular necrosis (A) represent a lack of blood flow, which is the opposite of hyperemia (increased blood flow) and is not mentioned as a mechanism for neurogenic osteoarthropathy in the text.
Question 33
A 68-year-old male with a 20-year history of poorly controlled type 2 diabetes mellitus presents with a painless, swollen, and deformed left foot. Examination reveals significant peripheral neuropathy. Radiographs show fragmentation and disorganization of the tarsometatarsal joints.
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly lists "diabetes mellitus" as one of the peripheral neuropathies associated with Charcot's joint. The patient's history and presentation are classic for diabetic neurogenic osteoarthropathy. Rheumatoid arthritis (A) is an autoimmune inflammatory arthritis, not a neurogenic condition, and is not listed as an associated cause in the provided text.
Question 34
A 35-year-old female presents with progressive weakness and sensory loss in her upper extremities, diagnosed with syringomyelia. She subsequently develops a rapidly destructive right elbow joint with minimal pain.
View Answer & Explanation
Correct Answer: C
Rationale: The text states that "Charcot’s joint is associated with some degenerative diseases of the spinal cord and other peripheral neuropathies, including syringomyelia." The patient's diagnosis directly links to this listed cause. Multiple sclerosis (A) is a neurological condition but is not listed in the provided text as an associated cause of neurogenic osteoarthropathy.
Question 35
A 55-year-old male with a history of untreated syphilis presents with ataxia and a progressively unstable and deformed left knee. Physical exam reveals diminished proprioception. Radiographs show severe joint destruction and subluxation.
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly lists "tabes dorsalis" as an associated condition for Charcot's joint. Tabes dorsalis is a late-stage manifestation of syphilis affecting the spinal cord, consistent with the patient's history and symptoms. Lyme disease (A) can cause arthropathy, but it is not listed in the provided text as a cause of neurogenic osteoarthropathy.
Question 36
A 28-year-old male, 5 years post-spinal cord injury resulting in paraplegia, presents with a swollen, erythematous, and unstable ankle joint in his paralyzed limb. He reports no pain.
View Answer & Explanation
Correct Answer: B
Rationale: The text lists "traumatic paralysis" as an associated condition for Charcot's joint. A spinal cord injury leading to paraplegia is a form of traumatic paralysis, and the presentation is consistent with neurogenic osteoarthropathy. Osteomyelitis (A) is an infection of the bone, which can occur in patients with sensory loss but is not the primary neurogenic cause of the joint destruction described.
Question 37
A 60-year-old chronic alcoholic male presents with severe peripheral neuropathy and a rapidly destructive, painless right foot. Radiographs show typical features of neurogenic osteoarthropathy.
View Answer & Explanation
Correct Answer: C
Rationale: The text specifically includes "alcohol abuse (late stage with peripheral neuropathy)" as an associated condition for Charcot's joint. The patient's history of chronic alcohol abuse and severe peripheral neuropathy directly matches this description. Cirrhosis (A) is a common complication of alcohol abuse but is not directly listed as the cause of neurogenic osteoarthropathy in the provided text; the neuropathy is the key link.
Question 38
A 50-year-old female with a history of a peripheral nerve lesion presents with a progressively deforming foot. She has significant loss of sensation in the affected area.
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly defines neurogenic osteoarthropathy as "the bone and joint changes that occur secondary to loss of sensation." This highlights the fundamental role of sensory loss in the condition. While motor function (A) can also be affected by nerve lesions, the text specifically identifies loss of sensation as the primary driver for the bone and joint changes in neurogenic osteoarthropathy.
Question 39
A 62-year-old male with diabetes presents with a Charcot foot. His physical examination reveals intact light touch but significantly diminished vibratory sense and proprioception.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "The pathophysiology of the disease is that the loss of proprioception and deep sensation result in recurrent trauma, and ultimately lead to progressive destruction." This directly identifies the specific sensory losses involved in the mechanical theory. While loss of pain (B) is also critical in Charcot, the text specifically highlights proprioception and deep sensation as leading to recurrent trauma in one of the primary pathophysiological theories.
Question 40
A 48-year-old patient with a spinal cord injury develops a warm, swollen, and rapidly destructive ankle joint. Imaging suggests increased vascularity.
View Answer & Explanation
Correct Answer: B
Rationale: The text explains the neurovascular theory: "Another theory postulates that neurally mediated vascular reflex results in hyperemia, which can cause osteoclast bone resorption." Hyperemia (increased vascularity) directly leads to osteoclast activity and bone destruction. Cartilage regeneration (A) is the opposite of the destructive process seen in neurogenic osteoarthropathy and is not a result of hyperemia in this context.
Question 41
A 70-year-old patient with a long-standing history of diabetes presents with a severely deformed and unstable ankle. Radiographs show extensive joint destruction, fragmentation, and new bone formation.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Charcot’s joint is associated with some degenerative diseases of the spinal cord and other peripheral neuropathies." This provides the overarching category for the specific conditions listed, including diabetes mellitus (a peripheral neuropathy). While diabetes is a metabolic disorder (B), the text specifically categorizes the associated conditions under "degenerative diseases of the spinal cord and other peripheral neuropathies" as the direct link to Charcot's joint.
Question 42
A 25-year-old patient with a known history of spinal dysraphism presents with a painless, swollen, and unstable foot. Radiographs show severe disorganization of the midfoot joints.
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly lists "spinal dysraphism" as one of the conditions associated with Charcot's joint. The patient's history directly matches this listed cause. Osteogenesis imperfecta (A) is a genetic disorder causing brittle bones, but it is not listed in the provided text as an associated cause of neurogenic osteoarthropathy.
Question 43
A 40-year-old patient with a history of transverse myelitis presents with a rapidly progressive, painless destruction of her left knee joint.
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly lists "transverse myelitis" as one of the conditions associated with Charcot's joint. The patient's history directly matches this listed cause. Multiple sclerosis (A) is a demyelinating disease that can cause transverse myelitis, but the text specifically lists "transverse myelitis" as the associated condition, not MS itself as the primary cause of Charcot.
Question 44
A 10-year-old male presents with a several-month history of mild left thigh pain. Radiographs reveal a well-circumscribed lesion in the femoral diaphysis with a "ground glass" appearance.
View Answer & Explanation
Correct Answer: A
Rationale: Fibrous dysplasia is explicitly described as a fibro-osseous benign lesion in the provided text. It is not malignant, precancerous, inflammatory, or metabolic in nature. Main Distractor Rationale: Option B is incorrect because fibrous dysplasia is a benign condition, not a malignant tumor like osteosarcoma.
Question 45
A 15-year-old female is diagnosed with fibrous dysplasia after presenting with a pathologic fracture of her right tibia.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context states that patients with fibrous dysplasia "may present with pain, limp, or pathologic fracture." Pathologic fracture is a common presentation due to the weakened bone structure. Main Distractor Rationale: Option C is incorrect; while soft tissue myxomas can be associated with Mazabraud's syndrome, the primary bone lesion itself does not typically present as a rapidly enlarging soft tissue mass.
Question 46
A 25-year-old male is found to have a single lesion consistent with fibrous dysplasia in his left femur during a workup for unrelated trauma.
View Answer & Explanation
Correct Answer: A
Rationale: The text clearly distinguishes between "monostotic or polyostotic" fibrous dysplasia. A single lesion is characteristic of monostotic disease. Main Distractor Rationale: Option B is incorrect because polyostotic disease involves multiple bones, whereas this patient has only a single lesion.
Question 47
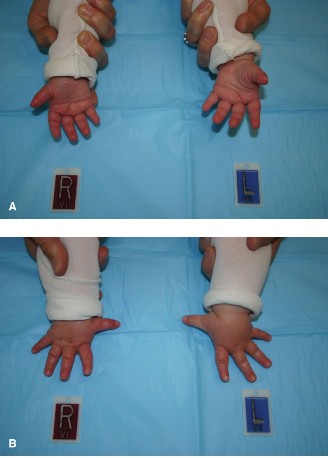
A 5-year-old girl presents with premature breast development and irregular café-au-lait spots on her trunk. Radiographs show multiple lytic lesions in her long bones and pelvis.
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "Patients with McCune–Albright’s syndrome have abnormal cutaneous pigmentation, endocrine abnormalities, and multiple bone involvement. These patients may present with precocious puberty." The vignette describes all these classic features. Main Distractor Rationale: Option B is incorrect. Mazabraud's syndrome is an association of fibrous dysplasia with soft tissue myxomas, not cutaneous pigmentation or endocrine abnormalities.
Question 48
A 30-year-old male with a known history of polyostotic fibrous dysplasia presents with a new, painless soft tissue mass in his left thigh. Biopsy of the mass reveals a myxoma.
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly defines "Mazabraud’s syndrome is an association of fi brous dysplasia with soft tissue myxomas." This patient's presentation perfectly matches this definition. Main Distractor Rationale: Option B is incorrect. McCune-Albright's syndrome involves abnormal cutaneous pigmentation and endocrine abnormalities, not soft tissue myxomas.
Question 49
A 12-year-old boy is diagnosed with fibrous dysplasia. His parents ask about common sites where the lesions might occur.
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "Lesions can occur in the ribs, skull and jaw, and the long and flat bones." Ribs are a common site. Main Distractor Rationale: Option B is incorrect. Fibrous dysplasia affects bones, not the spinal cord, which is nervous tissue.
Question 50
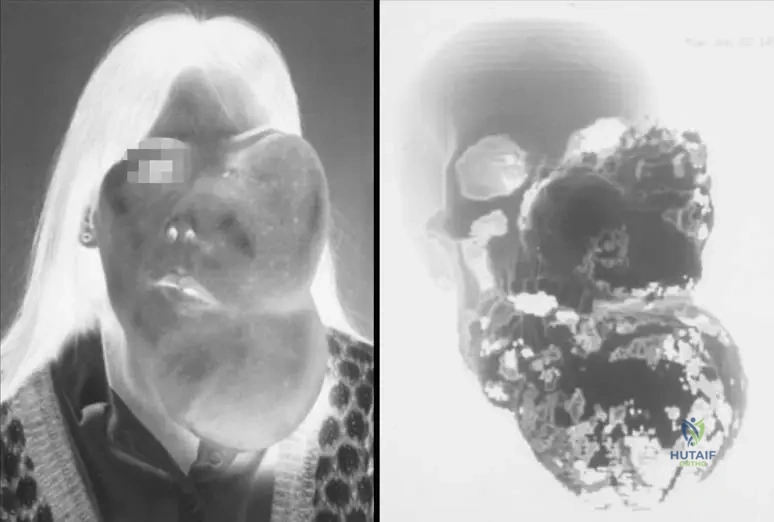
A 20-year-old patient presents with significant asymmetry and swelling of the left side of their face and jaw, causing cosmetic and functional concerns. A 3D CT scan reveals extensive involvement of the facial bones.
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly states, "Skull and facial lesions can cause significant deformity, exophthalmos, etc." The image (Fig. 11.25 a, b) also visually demonstrates "Massive deformity secondary to fi brous dysplasia of the left face and jaw." Main Distractor Rationale: Option B is incorrect. Acute respiratory distress syndrome is not a direct consequence of fibrous dysplasia affecting the facial bones.
Question 51
A 14-year-old male presents with a limp. Radiographs of the proximal femur show a well-circumscribed lesion with a sclerotic rim and a hazy, increased density within the medullary canal.

View Answer & Explanation
Correct Answer: A
Rationale: The text states, "The fi brous tissue may impart areas of hazy increased density within the lesion that have been described as “ground glass” density." This is a classic radiographic feature of fibrous dysplasia. Main Distractor Rationale: Option B is incorrect. A sunburst pattern is typically associated with aggressive bone tumors like osteosarcoma, not benign fibrous dysplasia.
Question 52
A 10-year-old girl undergoes imaging for a suspected bone lesion. The radiologist notes that the lesion appears to originate within the medullary canal of the affected bone.
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly states, "Radiographically, lesions originate in the medullary canal and may be metaphyseal or diaphyseal in location." Main Distractor Rationale: Option B is incorrect. While some bone lesions involve the periosteum, fibrous dysplasia is characterized by its origin within the medullary canal.
Question 53
A 17-year-old male has a mixed lytic and sclerotic lesion in his distal femur. Imaging reveals a narrow zone of transition and a sclerotic margin.

View Answer & Explanation
Correct Answer: A
Rationale: The text states, "The lesions are usually benign-appearing, presenting a bubbly lytic or mixed lytic and sclerotic lesions with a narrow zone of transition and a sclerotic margin." A narrow zone of transition and sclerotic margin are classic signs of a benign, slow-growing lesion. Main Distractor Rationale: Option B is incorrect. Aggressive malignancies typically present with a wide zone of transition and ill-defined margins, indicating rapid, infiltrative growth.
Question 54
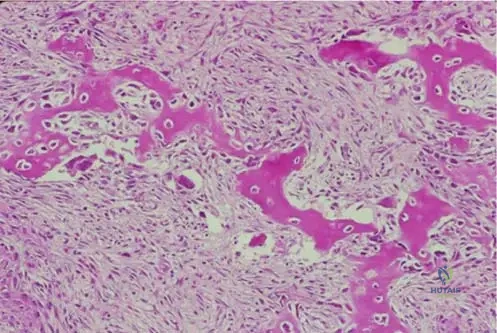
A bone biopsy is performed on a 9-year-old patient with a lytic lesion in the tibia. Histological examination reveals benign, proliferating fibroblastic cells and islands of woven bone arranged in an erratic pattern.

View Answer & Explanation
Correct Answer: A
Rationale: The text states, "The bony trabeculae area arranged in an erratic pattern sometimes referred to as “an alphabet soup”." This is a pathognomonic histological description for fibrous dysplasia. Main Distractor Rationale: Option B is incorrect. A mosaic pattern of bone is characteristic of Paget's disease, not fibrous dysplasia.
Question 55
A pathologist is reviewing a biopsy specimen from a patient with suspected fibrous dysplasia.
View Answer & Explanation
Correct Answer: A
Rationale: The text describes the histology: "Histologically, one will see a combination of benign, proliferating fi broblastic cells, and islands of woven bone." Main Distractor Rationale: Option B is incorrect. Malignant chondrocytes and osteoid would suggest a malignant tumor like osteosarcoma or chondrosarcoma, whereas fibrous dysplasia is a benign lesion.
Question 56
A 6-year-old girl with polyostotic fibrous dysplasia and café-au-lait spots is noted to have early signs of puberty.
View Answer & Explanation
Correct Answer: A
Rationale: The text states that patients with McCune-Albright's syndrome (which includes polyostotic fibrous dysplasia, abnormal cutaneous pigmentation, and endocrine abnormalities) "may present with precocious puberty." Main Distractor Rationale: Option B is incorrect. While other endocrine abnormalities can occur in McCune-Albright's, precocious puberty is specifically mentioned and is a classic, defining feature of the syndrome.
Question 57
A radiologist is interpreting an X-ray of a long bone affected by fibrous dysplasia.
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "Radiographically, lesions originate in the medullary canal and may be metaphyseal or diaphyseal in location." Main Distractor Rationale: Option B is incorrect. Fibrous dysplasia lesions are not restricted to the epiphyseal region; they are commonly found in the metaphysis and diaphysis.
Question 58
A 40-year-old patient is concerned about a recent diagnosis of fibrous dysplasia in their humerus. They ask about the prognosis.
View Answer & Explanation
Correct Answer: A
Rationale: The very first sentence of the text defines fibrous dysplasia as "a fi bro-osseous benign lesion." Main Distractor Rationale: Option B is incorrect. Fibrous dysplasia is explicitly stated to be a benign lesion, not malignant.
Question 59
A 16-year-old patient with extensive fibrous dysplasia involving the skull and orbital bones presents with a noticeable protrusion of the right eye.
View Answer & Explanation
Correct Answer: A
Question 59
A 12-year-old female presents with a several-month history of right thigh pain and a limp. Radiographs reveal a well-circumscribed lytic lesion in the proximal femur with a sclerotic rim and a hazy, increased density described as "ground glass" appearance. A biopsy is performed.
View Answer & Explanation
Correct Answer: C
Rationale: Histologically, fibrous dysplasia is characterized by benign, proliferating fibroblastic cells and islands of woven bone arranged in an erratic pattern, often described as "alphabet soup." This is a classic description for fibrous dysplasia. Option D describes a giant cell tumor, and Option E describes osteosarcoma, neither of which matches the benign fibro-osseous nature of fibrous dysplasia.
Question 60
A 10-year-old boy presents with a pathologic fracture of his left humerus. Radiographs show an expansile, lytic lesion in the diaphysis with a characteristic "ground glass" appearance. The lesion originates in the medullary canal.
View Answer & Explanation
Correct Answer: C
Rationale: The description of a medullary lesion with a "ground glass" appearance is pathognomonic for fibrous dysplasia. Enchondromas are typically lytic but lack the ground glass matrix. Osteosarcoma would show malignant osteoid and often a more aggressive appearance.
Question 61
A 6-year-old girl is diagnosed with fibrous dysplasia affecting her right femur, left tibia, and multiple ribs. She also has several café-au-lait spots on her trunk and a history of early menarche. Which of the following syndromes is most consistent with this presentation?
View Answer & Explanation
Correct Answer: D
Rationale: McCune-Albright's syndrome is characterized by polyostotic fibrous dysplasia, abnormal cutaneous pigmentation (café-au-lait spots), and endocrine abnormalities, such as precocious puberty (early menarche). Mazabraud's syndrome is associated with soft tissue myxomas, while Ollier's and Maffucci's syndromes involve enchondromas.
Question 62
A 25-year-old male presents with a new onset of pain in his left hip. Radiographs show a well-circumscribed, mixed lytic and sclerotic lesion in the femoral neck with a narrow zone of transition. He denies any history of trauma. What is the most likely initial clinical presentation for fibrous dysplasia?
View Answer & Explanation
Correct Answer: C
Rationale: Patients with fibrous dysplasia are often asymptomatic, with lesions discovered incidentally. While pain, limp, or pathologic fracture can occur, asymptomatic presentation is common. Rapidly enlarging soft tissue mass or systemic symptoms are not typical initial presentations for benign fibrous dysplasia.
Question 63
A 7-year-old girl with polyostotic fibrous dysplasia is noted to have café-au-lait spots. Her parents report that she began developing breast buds and pubic hair at age 5. Which endocrine abnormality is specifically associated with this presentation?
View Answer & Explanation
Correct Answer: C
Rationale: Precocious puberty is a classic endocrine abnormality associated with McCune-Albright's syndrome, which includes polyostotic fibrous dysplasia and abnormal cutaneous pigmentation (café-au-lait spots). The other endocrine conditions listed are not specifically linked to McCune-Albright's syndrome in the provided text.
Question 64
A 30-year-old male with a known history of fibrous dysplasia presents with a new, slowly growing, painless mass in his left thigh muscle. Imaging confirms a soft tissue myxoma adjacent to an area of fibrous dysplasia in the femur. This specific association is known as:
View Answer & Explanation
Correct Answer: C
Rationale: Mazabraud's syndrome is defined as the association of fibrous dysplasia with soft tissue myxomas. McCune-Albright's syndrome involves endocrine abnormalities and skin pigmentation, while Ollier's and Maffucci's syndromes are characterized by enchondromas and hemangiomas, respectively. Gardner's syndrome involves osteomas, colon polyps, and soft tissue tumors but not typically myxomas with fibrous dysplasia.
Question 65
A 15-year-old female is diagnosed with monostotic fibrous dysplasia. Based on typical locations, which of the following bones is a common site for this lesion?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states that lesions can occur in the ribs, skull and jaw, and the long and flat bones. Ribs are a common site for fibrous dysplasia. The other options are less commonly affected or not specifically mentioned as common sites in the provided text.
Question 66
A 9-year-old boy presents with a limp and pain in his left hip. Radiographs show a lytic lesion in the proximal femur. The lesion appears benign with a narrow zone of transition and a sclerotic margin. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: D
Rationale: The description of a benign-appearing lesion with a narrow zone of transition and a sclerotic margin is characteristic of fibrous dysplasia. Malignant lesions like osteosarcoma, Ewing's sarcoma, chondrosarcoma, or metastatic disease typically present with a wide zone of transition and aggressive features, not a sclerotic margin indicating a benign process.
Question 67
A 14-year-old female with known polyostotic fibrous dysplasia of the femur presents to the emergency department after falling from a standing height and experiencing acute thigh pain. Radiographs confirm a fracture through the dysplastic lesion. What is a recognized clinical presentation of fibrous dysplasia?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that patients with fibrous dysplasia may present with pain, limp, or pathologic fracture. A pathologic fracture occurs through bone weakened by an underlying disease process, which is consistent with the clinical scenario. Stress fractures are due to repetitive microtrauma in otherwise normal bone, and the other options are not typical presentations of fibrous dysplasia.
Question 68
A 20-year-old patient with extensive fibrous dysplasia of the left face and jaw presents with significant facial asymmetry and difficulty closing their eyelid. Which specific complication is directly mentioned as a potential consequence of skull and facial lesions in fibrous dysplasia?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that "Skull and facial lesions can cause significant deformity, exophthalmos, etc." Exophthalmos (protrusion of the eyeball) is a direct complication mentioned. While other complications might occur, exophthalmos is specifically listed.
Question 69
A bone biopsy from a 10-year-old patient with a "ground glass" lesion in the distal humerus reveals characteristic features of fibrous dysplasia. What type of bone is typically found interspersed within the fibrous tissue?
View Answer & Explanation
Correct Answer: D
Rationale: Histologically, fibrous dysplasia demonstrates bland-appearing fibrous areas with interspersed trabeculae of woven bone. Woven bone is immature bone, characteristic of this lesion. Lamellar bone is mature bone, and cortical/compact/trabecular are structural classifications rather than types of bone matrix in this context.
Question 70
A 16-year-old female with polyostotic fibrous dysplasia affecting her femur and pelvic bone undergoes an MRI for further evaluation of a painful lesion. What general appearance would be expected on MRI, consistent with the radiographic findings?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that "The lesions are usually benign-appearing, presenting a bubbly lytic or mixed lytic and sclerotic lesions with a narrow zone of transition and a sclerotic margin as seen in this patient with polyostotic disease affecting both the femur and pelvic bone as presented on the radiograph (a) and MR imaging (b)." This description directly applies to the expected appearance on MRI as well, reflecting the mixed fibrous and osseous components. Aggressive periosteal reaction would suggest a malignant process.
Question 71
A 10-year-old male presents with a lesion in the distal humerus noted on radiographs. The lesion is less defined than typical, but still shows areas of hazy increased density described as "ground glass" density. What is the primary tissue component responsible for this radiographic appearance?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "The fibrous tissue may impart areas of hazy increased density within the lesion that have been described as 'ground glass' density." Therefore, the fibrous tissue is the primary component responsible for this characteristic radiographic appearance. Cartilaginous matrix would suggest an enchondroma or chondrosarcoma.
Question 72
A biopsy is performed on a 14-year-old patient with a lytic lesion in the proximal tibia, consistent with fibrous dysplasia. Histological examination reveals a combination of benign, proliferating cells and islands of woven bone. What type of cells are primarily proliferating in this lesion?
View Answer & Explanation
Correct Answer: D
Rationale: Histologically, fibrous dysplasia shows a combination of benign, proliferating fibroblastic cells and islands of woven bone. This is a key diagnostic feature. Osteocytes are mature bone cells, and chondrocytes are cartilage cells, neither of which are the primary proliferating cell type in fibrous dysplasia.
Question 73
A 22-year-old male presents with a long-standing, asymptomatic lesion in his right femur, discovered incidentally on radiographs for an unrelated injury. The lesion is described as a well-circumscribed, "ground glass" density. What is the fundamental nature of fibrous dysplasia?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly defines fibrous dysplasia as "a fibro-osseous benign lesion." This is its fundamental nature. It is not malignant, nor is it primarily a vascular anomaly or inflammatory condition.
Question 74
A 5-year-old girl is evaluated for multiple bone lesions and irregular café-au-lait spots on her skin. Her mother reports early breast development. This constellation of findings is most indicative of which syndrome?
View Answer & Explanation
Correct Answer: C
Rationale: McCune-Albright's syndrome is characterized by polyostotic fibrous dysplasia, abnormal cutaneous pigmentation (café-au-lait spots), and endocrine abnormalities, such as precocious puberty (early breast development). Neurofibromatosis type 1 also has café-au-lait spots but typically presents with neurofibromas and Lisch nodules, not fibrous dysplasia and precocious puberty as the primary bone and endocrine issues.
Question 75
A 40-year-old male with a long history of polyostotic fibrous dysplasia presents with a new, slowly enlarging, painless mass in his calf muscle. Biopsy of the muscle mass reveals a soft tissue myxoma. This specific association is known as:
View Answer & Explanation
Correct Answer: C
Rationale: Mazabraud's syndrome is the specific association of fibrous dysplasia with soft tissue myxomas. Maffucci's syndrome involves enchondromas and hemangiomas, and Ollier's disease involves multiple enchondromas, neither of which matches the clinical presentation.
Question 76
A 13-year-old boy undergoes imaging for a lesion in his distal femur. Radiographs show a lytic lesion with a "ground glass" appearance. Based on the typical origin of fibrous dysplasia, where would this lesion be expected to arise?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Radiographically, lesions originate in the medullary canal and may be metaphyseal or diaphyseal in location." Therefore, the medullary canal is the expected origin. Lesions arising from the periosteum or cortical surface would suggest different pathologies.
Question 77
A pathologist is reviewing a bone biopsy from a patient suspected of having fibrous dysplasia. The slide shows benign, proliferating fibroblastic cells and islands of woven bone. The bony trabeculae are arranged in an erratic pattern. Which term is sometimes used to describe this erratic histological pattern?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "The bony trabeculae area arranged in an erratic pattern sometimes referred to as 'an alphabet soup'." "Onion skin" and "Codman's triangle" are radiographic signs associated with Ewing's sarcoma and aggressive lesions, respectively. "Sunburst" pattern is associated with osteosarcoma. "Soap bubble" describes a radiographic appearance, not a histological pattern.
Question 78
A 68-year-old male presents with a 3-month history of worsening left hip pain, particularly at night and while resting. He denies any specific injury. Physical examination reveals tenderness over the greater trochanter and pain with hip rotation. Radiographs show a lytic lesion in the proximal femur. He has no prior history of cancer. What is the most common malignant tumor found in bones?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical text explicitly states, "Metastases are the most common malignant tumor in bones." This is a fundamental concept in orthopaedic oncology. Multiple Myeloma (E) is a common primary bone tumor in older adults but is not as prevalent as metastatic disease overall.
Question 79
A 72-year-old female with a known history of breast cancer presents with new onset right shoulder pain. She describes the pain as a dull ache, constant, and worse at night, often waking her from sleep. She denies any specific trauma. Physical examination reveals diffuse tenderness around the shoulder joint. Which characteristic of her pain is most suggestive of metastatic bone disease?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical text states, "Patients often present with local or regional pain. The pain is often at rest, while mechanical or activity-related pain may portend an impending pathologic fracture." Pain at rest, particularly nocturnal pain, is a classic symptom of neoplastic bone involvement. Pain primarily with movement (C) is more typical of mechanical issues, and pain relieved by activity (B) is incorrect.
Question 80
A 65-year-old male with a history of prostate cancer presents with increasing left thigh pain over the past month. Initially, the pain was intermittent and mild, but now it is constant and exacerbated by weight-bearing. Radiographs show a large lytic lesion in the subtrochanteric region of the left femur. The patient is concerned about his ability to walk. What does the worsening, activity-related pain in this context most likely indicate?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states, "The pain is often at rest, while mechanical or activity-related pain may portend an impending pathologic fracture." Worsening pain with activity and weight-bearing in the presence of a lytic lesion strongly suggests structural compromise and an increased risk of fracture. Progression of soft tissue metastasis (A) might cause pain, but the mechanical nature points to bone integrity issues. Resolution of the lesion (D) is highly unlikely with worsening pain.
Question 81
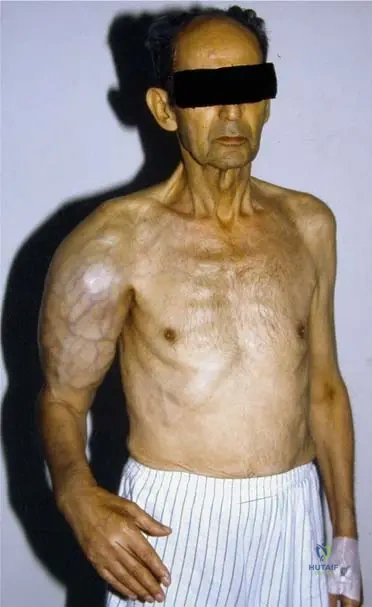
A 58-year-old female presents with a new, firm, non-tender mass in her right upper arm, accompanied by diffuse arm pain. She is cachectic and has a known history of lung cancer. Radiographs reveal extensive bone destruction in the humerus with a large associated soft tissue component. Which of the following primary tumors is most frequently associated with bony metastases?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical text lists "Lung, breast, prostate, kidney, and thyroid cancers are the most frequent primary tumors associated with bony metastases." Lung cancer is explicitly mentioned and is consistent with the vignette and the provided image (Fig. 8.116) which shows a cachectic patient with lung cancer and a large soft tissue extension. Lymphoma (C) can involve bone but is not listed among the most frequent primary tumors causing bony metastases in the text.
Question 82
A 62-year-old male presents with new onset back pain. He has no prior history of cancer. A bone scan is performed, revealing multiple areas of increased uptake throughout the axial and appendicular skeleton, as shown in the image. Given the typical presentation of metastatic bone disease, what is a common scenario regarding the diagnosis of the primary tumor?
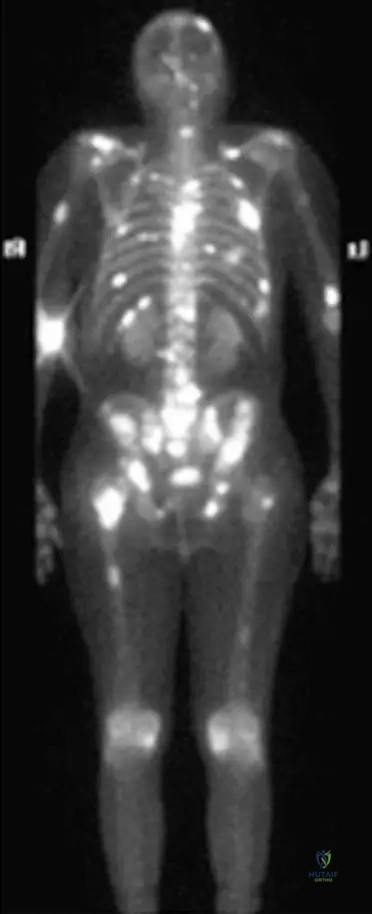
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states, "Patients may present with solitary or multiple lesions, often with a history of cancer. Sometimes, however, a bony metastasis will be the initial presentation of a tumor." This highlights that a new diagnosis of metastatic bone disease can precede the discovery of the primary malignancy. Options A and B are directly contradicted by the text. The image (Fig. 8.122) shows multiple bony metastases, which could be the first sign of an occult primary.
Question 83
A 57-year-old male presents with a 2-month history of progressive left arm pain and weakness. Radiographs reveal a lytic destruction of the shaft of the left humerus. A subsequent bone scan shows increased uptake in the affected area, and a CT abdomen identifies a primary site in the kidney. What is the expected radiographic appearance of metastatic bone disease?
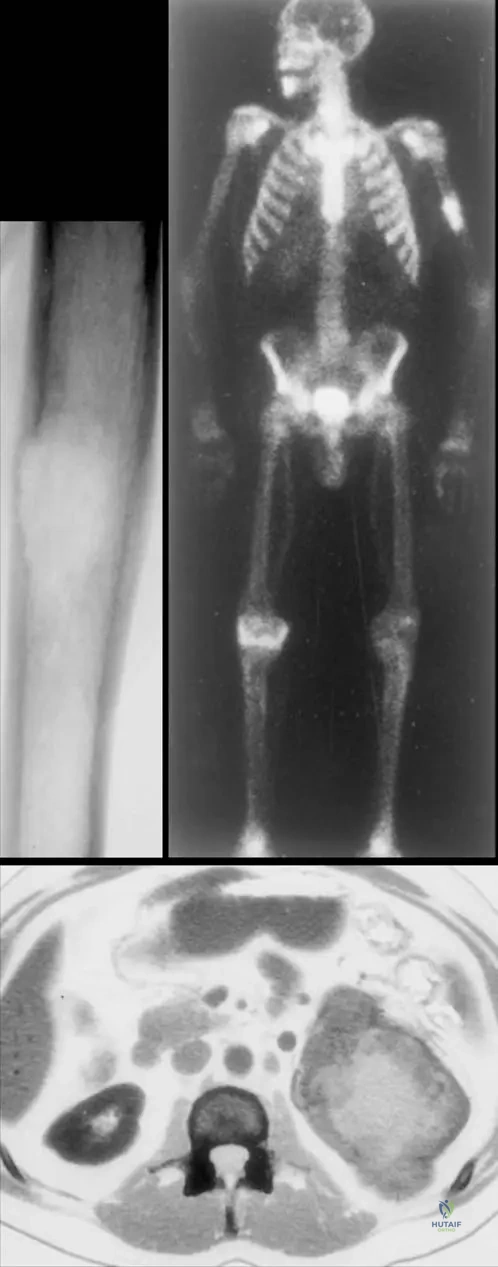
View Answer & Explanation
Correct Answer: D
Rationale: The clinical text explicitly states, "The radiographic appearance of metastases is highly variable. The appearance will vary from radiolucent to radiodense; some tumors have a mixed character." This directly addresses the variability in radiographic presentation. The image (Fig. 8.123a) shows a lytic lesion, but the text emphasizes the broad spectrum. Options A, B, and C are incorrect because they suggest a single, consistent appearance.
Question 84
An 80-year-old male presents with diffuse, generalized bone pain and fatigue. Initial radiographs show multiple small lytic lesions throughout the spine and pelvis. Given his age and the radiographic findings, which of the following conditions should be included in the differential diagnosis alongside metastatic bone disease?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical text states, "As these lesions tend to occur in an older age range than the primary tumors, the differential diagnosis includes myeloma and lymphoma." Multiple Myeloma is a common malignancy in older adults that presents with multifocal lytic bone lesions, making it a critical differential diagnosis for metastatic disease in this age group. Osteomyelitis (A) is an infection, and Paget's disease (B) typically has a mixed lytic/blastic appearance with bone enlargement, not diffuse lytic lesions.
Question 85
A 60-year-old female with a history of thyroid cancer presents with new onset right hip pain. An MRI of the hip demonstrates extensive lytic destruction in the femoral neck, as shown in the image. What is the primary advantage of MRI in evaluating this lesion compared to plain radiographs?
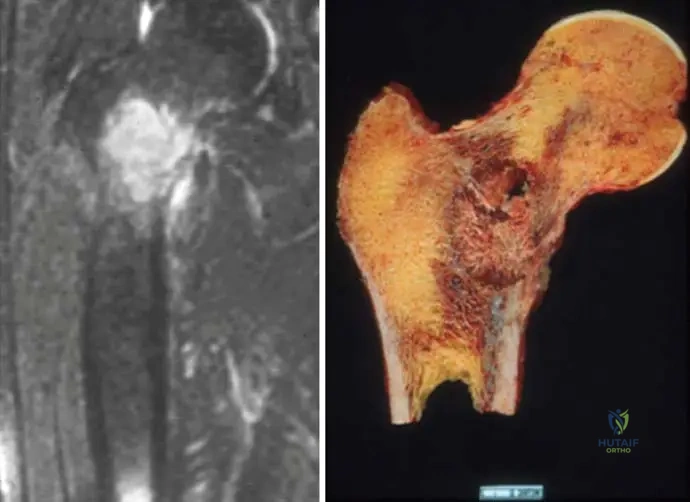
View Answer & Explanation
Correct Answer: B
Rationale: While not explicitly detailed in the text, the image (Fig. 8.125a) shows an MRI demonstrating the extent of lytic destruction. MRI is superior for evaluating soft tissue extension, intramedullary involvement, and the full extent of bone marrow pathology, which is crucial for surgical planning and assessing fracture risk. Plain radiographs are good for cortical bone (A) but lack soft tissue detail. While MRI has no ionizing radiation (D), its primary advantage here is detailed anatomical assessment. CT is generally better for cortical bone detail than MRI.
Question 86
A 70-year-old male with a known history of prostate cancer presents with new onset diffuse bone pain. A technetium-99m bone scan is performed, revealing multiple areas of increased radiotracer uptake throughout the axial skeleton, consistent with the image provided. What is the most likely characteristic of these metastatic lesions from prostate cancer?
View Answer & Explanation
Correct Answer: C
Rationale: The image (Fig. 8.122) is a bone scan of multiple bony metastases from prostate carcinoma, showing increased uptake. Increased uptake on a bone scan typically indicates osteoblastic activity, which corresponds to blastic (radiodense) lesions on plain radiographs. While the text states radiographic appearance is variable, prostate cancer is classically associated with blastic metastases. Purely lytic (A) is less common for prostate, and soft tissue masses without bone involvement (D) would not show increased uptake on a bone scan.
Question 87
A 55-year-old female with a history of breast cancer presents with new onset pain in her right femur. Radiographs show a lytic lesion in the mid-diaphysis. She denies any trauma. What is the most appropriate initial diagnostic step to assess for additional metastatic disease?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text mentions patients may present with solitary or multiple lesions and shows a bone scan (Fig. 8.122, 8.123b) as a diagnostic tool. Whole-body bone scintigraphy (bone scan) is a highly sensitive and commonly used initial screening tool to detect additional bony metastases throughout the skeleton, especially in patients with a known primary cancer and a new bone lesion. While PET-CT (D) is also effective, bone scan is often the first-line for bone-specific screening. Biopsy (A) is for definitive diagnosis of the specific lesion, not for screening the entire skeleton. MRI of the spine (B) is too limited for whole-body assessment.
Question 88
A 68-year-old male presents with a new, painful, palpable mass in his right upper arm. He appears cachectic. Imaging reveals a large soft tissue mass with extensive underlying humeral destruction. Biopsy confirms metastatic adenocarcinoma. Given the clinical presentation and the image, which primary cancer is most likely?
View Answer & Explanation
Correct Answer: D
Rationale: The image (Fig. 8.116) explicitly states it is "Photograph taken from a cachectic patient suffering on a lung cancer. Note the enormous soft tissue extension of the metastasis in the right upper arm." This directly links the described clinical scenario (cachexia, large soft tissue mass, upper arm location) to lung cancer. While other cancers can metastasize to bone, lung cancer is specifically highlighted in the image and text as a frequent primary with such presentations.
Question 89
A 57-year-old male presents with a lytic destruction of the shaft of the left humerus. A bone scan shows increased uptake in the lesion, and a CT abdomen reveals the primary site in the kidney. What is a characteristic feature of metastatic lesions originating from kidney cancer?
View Answer & Explanation
Correct Answer: B
Rationale: The image (Fig. 8.123a) shows a lytic destruction of the humerus, and the caption states the primary site is the kidney. Kidney cancer (renal cell carcinoma) metastases are classically known for being purely lytic and highly vascular, often presenting with significant bone destruction and sometimes hemorrhage. Blastic lesions (A) are more typical of prostate cancer. The text mentions kidney cancer as a frequent primary for bony metastases, and the image provides a specific example of a lytic lesion from a kidney primary.
Question 90
A 75-year-old female with a history of breast cancer presents with new onset right hip pain. Radiographs show a large lytic lesion in the intertrochanteric region of the femur. She describes the pain as constant and worsening with weight-bearing. Given the high risk of impending pathologic fracture, what is the most appropriate immediate management strategy?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states, "mechanical or activity-related pain may portend an impending pathologic fracture." A large lytic lesion in a weight-bearing bone with worsening pain on weight-bearing indicates a high risk of fracture. Surgical stabilization (e.g., intramedullary nailing) is often indicated to prevent fracture and alleviate pain, combined with non-weight-bearing to protect the bone. While chemotherapy (A) and radiation (E) are important for tumor control, they do not immediately address the mechanical instability. Observation (B) is inappropriate given the impending fracture risk.
Question 91
A 63-year-old male presents with a new, painful lesion in his sacrum. He has no known history of cancer. A biopsy is performed, confirming metastatic adenocarcinoma. Which of the following primary tumors is NOT listed in the provided text as one of the most frequent sources of bony metastases?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical text explicitly lists "Lung, breast, prostate, kidney, and thyroid cancers are the most frequent primary tumors associated with bony metastases." Colon cancer is not included in this specific list. While colon cancer can metastasize to bone, it is not highlighted as one of the *most frequent* in this context.
Question 92
A 70-year-old male with a history of prostate cancer presents with diffuse back pain. A bone scan (Fig. 8.122) shows multiple areas of increased uptake throughout the spine and pelvis. What is the most likely reason for the increased uptake observed on the bone scan?
View Answer & Explanation
Correct Answer: C
Rationale: Bone scans (technetium-99m) detect areas of increased bone turnover or osteoblastic activity, where new bone formation is occurring. In the context of metastatic disease, particularly from prostate cancer which is often blastic, the tumor stimulates the surrounding bone to lay down new bone, leading to increased radiotracer uptake. While osteoclastic activity (B) is also involved in bone destruction, the increased uptake on a bone scan primarily reflects the reactive osteoblastic response. Direct visualization of tumor cells (A) is not how bone scans work.
Question 93
A 60-year-old female presents with a new, painful lesion in her left femur. She has no known history of cancer. Radiographs show a solitary lytic lesion. What is the most appropriate next step in the diagnostic workup?
View Answer & Explanation
Correct Answer: C
Rationale: When a patient presents with a solitary lytic lesion and no known history of cancer, the priority is to determine if it is a primary bone tumor or a metastasis, and if metastatic, to find the primary source. The text mentions that "a bony metastasis will be the initial presentation of a tumor." A whole-body bone scan helps identify other potential bony lesions, and imaging (e.g., CT chest/abdomen/pelvis, mammogram, thyroid ultrasound) is crucial to search for the primary. While a biopsy will eventually be needed for definitive diagnosis, a broader workup for the primary is often performed first or concurrently. Observation (A) is inappropriate for a painful lytic lesion. Open biopsy (B) might be too invasive as a first step without further staging.
Question 94
A 72-year-old male with a history of lung cancer presents with increasing pain in his right humerus. Radiographs show a large lytic lesion with cortical destruction. He is cachectic. What is the significance of the cachectic state in this patient?
View Answer & Explanation
Correct Answer: C
Rationale: The image (Fig. 8.116) shows a "cachectic patient suffering on a lung cancer." Cachexia, characterized by severe weight loss, muscle atrophy, and fatigue, is a well-recognized paraneoplastic syndrome and a common systemic manifestation of advanced malignancy, particularly lung cancer. It signifies a poor prognostic indicator and systemic disease burden, not a benign lesion (A) or early-stage cancer (B). While poor nutritional intake contributes, it's often driven by the cancer itself (D is incorrect).
Question 95
A 66-year-old female with a known history of breast cancer presents with new onset left knee pain. Radiographs are inconclusive, but a bone scan shows increased uptake in the distal femur. An MRI is then performed, demonstrating lytic destruction extending into the femoral condyle. What is the primary role of MRI in this scenario?
View Answer & Explanation
Correct Answer: B
Rationale: The image (Fig. 8.125a) shows an MRI demonstrating lytic destruction extent in the femoral neck. MRI is excellent for delineating the precise extent of intramedullary tumor involvement, cortical breach, and any associated soft tissue mass, which is critical for surgical planning and assessing fracture risk. While a bone scan (D) is better for distant metastases, MRI provides detailed local assessment. MRI does not typically confirm blastic lesions (A) or provide definitive diagnosis without biopsy (C). Bone mineral density (E) is assessed by DEXA scan.
Question 96
A 78-year-old male presents with persistent right shoulder pain. Radiographs show a mixed lytic and blastic lesion in the proximal humerus. He has a history of lymphoma diagnosed 5 years prior. Given his age and the radiographic findings, what is a key differential diagnosis for this lesion in addition to metastatic carcinoma?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical text states, "As these lesions tend to occur in an older age range than the primary tumors, the differential diagnosis includes myeloma and lymphoma." Given the patient's age and history of lymphoma, direct bone involvement by lymphoma is a crucial differential diagnosis for a new bone lesion, especially when considering metastatic disease. Osteomyelitis (A) is an infection, and aneurysmal bone cyst (B) and osteoid osteoma (E) are typically benign lesions seen in younger patients. Chondrosarcoma (C) is a primary bone tumor but lymphoma is specifically mentioned in the text as a differential for metastatic disease in older patients.
Question 97
A 65-year-old female presents with a 4-month history of progressive left thigh pain. Radiographs show a large lytic lesion in the distal femur. She has no known history of cancer. A biopsy is planned. What is the most common histological type of malignancy expected if this lesion is a metastasis?
View Answer & Explanation
Correct Answer: C
Rationale: The most common primary tumors that metastasize to bone (lung, breast, prostate, kidney, thyroid) are predominantly adenocarcinomas (e.g.,
Question 97
A 68-year-old male presents with new onset, constant, dull pain in his right hip that is worse at night and not relieved by rest. He has a known history of prostate cancer. Radiographs show a sclerotic lesion in the proximal femur. Which of the following imaging modalities would be most appropriate to assess the extent of bony involvement throughout the skeleton?
View Answer & Explanation
Correct Answer: D
Rationale: Technetium-99m bone scintigraphy (bone scan) is highly sensitive for detecting osteoblastic activity, making it excellent for screening the entire skeleton for metastatic disease, especially from prostate cancer which often produces blastic lesions. The provided image (Fig. 8.122) demonstrates a bone scan showing multiple bony metastases from prostate carcinoma. While PET-CT is also very sensitive, bone scintigraphy is a more traditional and often initial screening tool for widespread bony involvement. MRI is excellent for local staging and soft tissue involvement but not for whole-body screening in this context. Plain radiographs are less sensitive for early lesions.
Question 97
A 55-year-old female with a history of breast cancer presents with increasing pain in her left humerus. Physical examination reveals localized tenderness and a palpable soft tissue mass in the mid-diaphysis. Radiographs show a lytic lesion with cortical destruction. Which of the following is the most appropriate next step in management to assess the local extent of the lesion and potential impending fracture?
View Answer & Explanation
Correct Answer: C
Rationale: MRI of the affected bone (left humerus) is the most appropriate next step to accurately assess the local extent of the lytic lesion, evaluate soft tissue involvement, and determine the risk of impending pathologic fracture. The text mentions that lesions are often contained in bone, but some patients present with a palpable soft tissue mass, which MRI can characterize well. While a bone scan would show increased uptake, it doesn't provide the detailed local anatomical information needed for surgical planning or fracture risk assessment. Biopsy is typically performed after imaging to confirm diagnosis, and serum markers are for systemic monitoring.
Question 97
A 72-year-old male presents with worsening right shoulder pain and a new, rapidly growing mass in his right upper arm. He appears cachectic. Imaging reveals an extensive soft tissue mass originating from the humerus with underlying bone destruction. Given the clinical presentation and image, which primary cancer is most likely?
View Answer & Explanation
Correct Answer: C
Rationale: The provided image (Fig. 8.116) explicitly states it is from a cachectic patient suffering from lung cancer, noting the enormous soft tissue extension of the metastasis in the right upper arm. Lung cancer is one of the most frequent primary tumors associated with bony metastases and can present with significant soft tissue involvement. While other cancers can metastasize to bone, the direct caption links this specific presentation to lung cancer.
Question 97
A 60-year-old female presents with a 3-month history of progressive left thigh pain, which is constant and worse with weight-bearing. Radiographs show a large lytic lesion in the subtrochanteric region of the left femur. She has no known history of cancer. What is the most common malignant tumor in bones, which this presentation likely represents?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case explicitly states, "Metastases are the most common malignant tumor in bones." Given the patient's age, lytic lesion, and pain, metastatic bone disease is the most likely diagnosis, even without a known primary. The text also mentions that sometimes a bony metastasis will be the initial presentation of a tumor. Osteosarcoma and Ewing sarcoma are primary bone tumors more common in younger patients. Multiple myeloma is a differential but less common overall than metastases.
Question 97
A 57-year-old male presents with a lytic destruction of the shaft of the left humerus. A bone scan shows increased uptake in the lesion. A subsequent CT abdomen reveals a primary site in the kidney. Which of the following characteristics is most commonly associated with renal cell carcinoma metastases to bone?
View Answer & Explanation
Correct Answer: C
Rationale: While not explicitly detailed in the provided text, the image (Fig. 8.123) shows a lytic destruction of the humerus with a primary in the kidney, which is characteristic of renal cell carcinoma (RCC). RCC metastases are notoriously highly vascular, which is a critical consideration for surgical planning due to the risk of significant hemorrhage. They are typically lytic, not blastic, and can be aggressive. The text mentions kidney cancer as a frequent primary tumor. The other options are generally not characteristic of RCC bone metastases.
Question 97
A 63-year-old female with a history of lung cancer presents with new onset, severe pain in her right femur. She describes the pain as constant and worse with ambulation. Radiographs show a large lytic lesion involving more than 50% of the cortical width in the mid-diaphysis. This presentation most strongly suggests:
View Answer & Explanation
Correct Answer: C
Rationale: The vignette describes a patient with known cancer, a lytic lesion, and pain that is mechanical/activity-related, which the text states "may portend an impending pathologic fracture." A lesion involving more than 50% of the cortical width is a well-established criterion for high risk of impending fracture (Mirels' score). This is a classic presentation of an impending pathologic fracture due to metastatic disease. The other options are less likely given the history of cancer and the specific radiographic findings.
Question 97
A 70-year-old male presents with diffuse back pain and fatigue. He has no known history of cancer. Initial radiographs show multiple lytic lesions in the vertebral bodies and pelvis. Given his age and the radiographic findings, which of the following is an important differential diagnosis to consider alongside metastatic bone disease?
View Answer & Explanation
Correct Answer: D
Rationale: The teaching case states, "As these lesions tend to occur in an older age range than the primary tumors, the differential diagnosis includes myeloma and lymphoma." Multiple myeloma commonly presents with widespread lytic lesions in the axial skeleton in older patients, making it a critical differential for metastatic bone disease. Paget's disease typically has mixed lytic/blastic features and bone expansion. Fibrous dysplasia is usually solitary and in younger patients. Osteoporosis causes diffuse osteopenia but not typically discrete lytic lesions.
Question 97
A 58-year-old female with a history of thyroid cancer presents with a new painful lesion in her left tibia. Radiographs show a mixed lytic and sclerotic lesion. Which of the following statements best describes the radiographic appearance of metastatic bone disease?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case explicitly states, "The radiographic appearance of metastases is highly variable. The appearance will vary from radiolucent to radiodense; some tumors have a mixed character." This directly supports option C. Metastases are not always purely lytic or sclerotic. While some primary bone tumors can be difficult to distinguish, the variability is a key characteristic of metastases, and periosteal reaction is less common or less prominent than in many primary bone sarcomas.
Question 97
A 66-year-old male with a known history of prostate cancer presents with new onset back pain. A bone scan reveals multiple areas of increased uptake throughout the axial skeleton. Which of the following primary tumors is most commonly associated with predominantly osteoblastic (sclerotic) bone metastases?
View Answer & Explanation
Correct Answer: D
Rationale: Prostate cancer is classically known for producing predominantly osteoblastic (sclerotic) bone metastases, as often seen on bone scans like Fig. 8.122. While breast cancer can be mixed or blastic, it is more commonly lytic. Lung, kidney, and thyroid cancers are typically associated with lytic metastases. The clinical vignette and image context (Fig. 8.122 is a bone scan of multiple bony metastasis from prostate carcinoma) reinforce this association.
Question 97
A 50-year-old female with a history of breast cancer presents with right knee pain. Radiographs show a lytic lesion in the distal femur. She denies any trauma. What is the most common presenting symptom of metastatic bone disease?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states, "Patients often present with local or regional pain." While other symptoms like pathologic fracture, hypercalcemia, spinal cord compression, or a palpable soft tissue mass can occur, pain is the most frequent initial complaint. The vignette describes knee pain, which is a local symptom.
Question 97
A 62-year-old male presents with new onset left hip pain. MRI demonstrates a lytic destruction in the femoral neck. He has no known history of cancer. What is the most appropriate initial diagnostic step to identify the primary tumor?
View Answer & Explanation
Correct Answer: C
Rationale: When a bony metastasis is the initial presentation of a tumor, a CT scan of the chest, abdomen, and pelvis is typically the most efficient and comprehensive initial imaging study to search for the primary site, as it covers the most common locations for primary cancers that metastasize to bone (lung, breast, kidney, prostate, GI tract). While PET-CT is also effective, CT C/A/P is often the first-line, more readily available, and cost-effective option. Biopsy confirms the diagnosis but doesn't necessarily find the primary. Serum markers can be helpful but are not a standalone diagnostic for the primary site. The image (Fig. 8.125a) shows lytic destruction in the femoral neck, consistent with the vignette.
Question 97
A 75-year-old female presents with persistent right shoulder pain. Radiographs show a lytic lesion in the proximal humerus. She has a history of breast cancer treated 10 years prior. The pain is constant and present at rest. This type of pain pattern is characteristic of:
View Answer & Explanation
Correct Answer: D
Rationale: The teaching case states, "The pain is often at rest, while mechanical or activity-related pain may portend an impending pathologic fracture." Constant pain, especially at rest, in a patient with a history of cancer and a lytic lesion, is highly characteristic of malignant bone pain due to metastatic disease. Mechanical pain is typically activity-related and relieved by rest. Inflammatory arthritis and tendinopathy usually have different pain patterns and associated findings.
Question 97
A 60-year-old male presents with a painful lytic lesion in his left humerus. A bone scan shows increased uptake in the lesion, and a CT abdomen reveals a primary renal cell carcinoma. The patient is scheduled for surgical stabilization. What is a critical intraoperative consideration for managing bone metastases from renal cell carcinoma?
View Answer & Explanation
Correct Answer: B
Rationale: As discussed in the rationale for Question 25, renal cell carcinoma metastases (as indicated by Fig. 8.123 showing kidney as the primary) are known for being highly vascular. This significantly increases the risk of intraoperative hemorrhage, which is a critical consideration for surgical planning and execution. While poor bone quality can be an issue with any lytic lesion, the extreme vascularity is a specific characteristic of RCC metastases. The other options are less specific or universally critical for RCC metastases.
Question 97
A 68-year-old female with a history of breast cancer presents with new onset right thigh pain. Radiographs show a lytic lesion in the proximal femur. Which of the following primary tumors is NOT listed in the provided text as one of the most frequent causes of bony metastases?
View Answer & Explanation
Correct Answer: D
Rationale: The teaching case explicitly lists the most frequent primary tumors associated with bony metastases: "Lung, breast, prostate, kidney, and thyroid cancers are the most frequent primary tumors associated with bony metastases." Colon cancer is not included in this list, making it the correct answer as the one NOT listed.
Question 97
A 59-year-old male presents with a 2-month history of progressive left shoulder pain. Physical examination reveals local tenderness over the proximal humerus. Radiographs show a lytic lesion. He denies any prior cancer history. What is the significance of "local tenderness or joint irritability" in the context of metastatic bone disease?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states, "Local tenderness or joint irritability may be present." This indicates that these are common physical exam findings associated with metastatic bone disease, not indicative of benign processes or ruling out fractures. It is not specific to primary bone sarcomas, and while inflammatory arthritis can cause tenderness, the context of a lytic lesion points to metastasis.
Question 97
A 70-year-old female presents with a new lytic lesion in her right femoral neck, discovered incidentally on imaging for hip pain. She has no known history of cancer. The MRI shows the extent of the lytic destruction. What is the most likely initial presentation of metastatic bone disease in a patient without a known primary?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states, "Sometimes, however, a bony metastasis will be the initial presentation of a tumor." This means the discovery of the bone lesion itself (as in the vignette and Fig. 8.125a) can be the first sign of cancer, even before the primary tumor is identified or other systemic symptoms manifest. While a pathologic fracture can be the initial presentation, the bone metastasis itself is the underlying cause and can be discovered before a fracture occurs.
Question 97
A 65-year-old male with a history of lung cancer presents with severe, unremitting pain in his thoracic spine. Neurological examination reveals new onset lower extremity weakness and sensory changes. This clinical picture is most concerning for:
View Answer & Explanation
Correct Answer: B
Rationale: In a patient with known metastatic cancer and new onset severe spinal pain with neurological deficits (weakness, sensory changes), spinal cord compression due to epidural metastasis is a medical emergency. While not explicitly detailed in the provided text, it is a critical complication of metastatic bone disease that orthopaedic surgeons must recognize. The other options are less likely given the cancer history and neurological findings.
Question 97
A 52-year-old female with a history of breast cancer presents with a lytic lesion in her proximal femur. She is undergoing systemic therapy. What is the primary goal of surgical intervention for metastatic bone disease in the appendicular skeleton?
View Answer & Explanation
Correct Answer: C
Rationale: For metastatic bone disease, especially in the appendicular skeleton, surgical intervention is primarily palliative and prophylactic. The main goals are pain relief, prevention of impending pathologic fractures, and stabilization of existing pathologic fractures to improve function and quality of life. Cure is rarely achievable with surgery alone for widespread metastatic disease. Complete resection with wide margins is typically reserved for primary bone sarcomas or solitary metastases in specific circumstances, not the general approach for metastatic bone disease.
Question 97
A 67-year-old male presents with a lytic lesion in his left humerus. A bone scan shows increased uptake in the lesion. A CT abdomen reveals a primary site in the kidney. Which of the following statements about the prognosis of metastatic bone disease is most accurate?
View Answer & Explanation
Correct Answer: C
Rationale: While not explicitly detailed in the provided text, the general understanding of metastatic bone disease is that prognosis is highly variable. It is heavily influenced by the type of primary tumor (e.g., breast and prostate cancer generally have better prognoses than lung or pancreatic cancer), the overall burden of disease (number and location of metastases), and the patient's response to systemic therapies. The image (Fig. 8.123) shows a kidney primary, which can have a variable course. A uniformly poor prognosis is incorrect, and while extent of bone involvement is a factor, the primary tumor type is often more critical. Solitary metastases can still be aggressive depending on the primary. Surgical intervention primarily improves quality of life and function, not necessarily survival in most cases.
Question 97
A 55-year-old female with a known history of lung cancer presents with new onset right hip pain. Radiographs show a lytic lesion in the femoral neck. An MRI confirms extensive lytic destruction. What is the most common histological type of primary tumor that metastasizes to bone?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case lists "Lung, breast, prostate, kidney, and thyroid cancers" as the most frequent primary tumors associated with bony metastases. All of these are carcinomas (epithelial cell origin). Therefore, carcinoma is the most common histological type of primary tumor that metastasizes to bone. While lymphoma and myeloma are mentioned as differential diagnoses, and melanoma can metastasize, carcinomas are overwhelmingly the most common source of bone metastases. The image (Fig. 8.125a) shows a lytic lesion consistent with metastatic carcinoma.
Question 98
A 68-year-old male presents with new onset, constant, dull pain in his right hip that is worse at night and not relieved by rest. He has a known history of prostate cancer. Radiographs show a sclerotic lesion in the proximal femur. Which of the following imaging modalities would be most appropriate to assess the extent of bony involvement throughout the skeleton?
View Answer & Explanation
Correct Answer: D
Rationale: Technetium-99m bone scintigraphy (bone scan) is highly sensitive for detecting osteoblastic activity, making it excellent for screening the entire skeleton for metastatic disease, especially from prostate cancer which often produces blastic lesions. The provided image (Fig. 8.122) demonstrates a bone scan showing multiple bony metastases from prostate carcinoma. While PET-CT is also very sensitive, bone scintigraphy is a more traditional and often initial screening tool for widespread bony involvement. MRI is excellent for local staging and soft tissue involvement but not for whole-body screening in this context. Plain radiographs are less sensitive for early lesions.
Question 99
A 55-year-old female with a history of breast cancer presents with increasing pain in her left humerus. Physical examination reveals localized tenderness and a palpable soft tissue mass in the mid-diaphysis. Radiographs show a lytic lesion with cortical destruction. Which of the following is the most appropriate next step in management to assess the local extent of the lesion and potential impending fracture?
View Answer & Explanation
Correct Answer: C
Rationale: MRI of the affected bone (left humerus) is the most appropriate next step to accurately assess the local extent of the lytic lesion, evaluate soft tissue involvement, and determine the risk of impending pathologic fracture. The text mentions that lesions are often contained in bone, but some patients present with a palpable soft tissue mass, which MRI can characterize well. While a bone scan would show increased uptake, it doesn't provide the detailed local anatomical information needed for surgical planning or fracture risk assessment. Biopsy is typically performed after imaging to confirm diagnosis, and serum markers are for systemic monitoring.
Question 100
A 72-year-old male presents with worsening right shoulder pain and a new, rapidly growing mass in his right upper arm. He appears cachectic. Imaging reveals an extensive soft tissue mass originating from the humerus with underlying bone destruction. Given the clinical presentation and image, which primary cancer is most likely?
View Answer & Explanation
Correct Answer: C
Rationale: The provided image (Fig. 8.116) explicitly states it is from a cachectic patient suffering from lung cancer, noting the enormous soft tissue extension of the metastasis in the right upper arm. Lung cancer is one of the most frequent primary tumors associated with bony metastases and can present with significant soft tissue involvement. While other cancers can metastasize to bone, the direct caption links this specific presentation to lung cancer.
You Might Also Like