Master ABOS Orthopedic Board Review: Musculoskeletal Pathology & Bone Disorders | Part 12

Key Takeaway
This ABOS Orthopedic Board Review covers essential musculoskeletal pathology, including Camurati-Engelmann disease, multiple myeloma, Ewing's sarcoma, Paget's disease, hemophilia arthropathy, algodystrophy, stress fractures, and various arthropathies. It focuses on clinical presentation, radiographic findings, and pathological features for comprehensive exam preparation.
Question 1
A 20-year-old male with a known diagnosis of Camurati–Engelmann disease reports increasing difficulty with ambulation. His physical examination reveals significant muscle weakness, particularly in the proximal lower extremities, contributing to his observed waddling gait. What is the primary cause of the muscle weakness and waddling gait in patients with this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 1.119 states: "Sometimes decreased muscle and subcutaneous fat mass and thin habitus with columnar shaped extremities occur." This decreased muscle mass directly contributes to muscle weakness and the characteristic waddling gait. While the exact pathophysiology of muscle weakness is complex, the reduction in muscle bulk is a noted feature. Primary myopathy (A), direct muscle infiltration (B), spinal cord compression (D), or peripheral neuropathy (E) are not described as primary causes in the provided text.
Question 2
A 24-year-old male presents for evaluation of chronic leg pain and a thin build. Radiographs of his long bones show characteristic diaphyseal cortical thickening and sclerosis. He reports that his symptoms have been gradually worsening since childhood. This progressive nature of the disease is reflected in its name. Which term in the disease name specifically highlights this characteristic?
View Answer & Explanation
Correct Answer: C
Rationale: The full name of the condition is "Progressive Diaphyseal Dysplasia." The term "Progressive" (C) directly indicates the worsening nature of the disease over time, consistent with the patient's report of gradually worsening symptoms. "Diaphyseal" (A) refers to the affected bone segment, and "Dysplasia" (B) refers to abnormal development, while Camurati and Engelmann (D, E) are the names of the individuals who described the disease.
Question 3
A 12-year-old girl is diagnosed with Camurati–Engelmann disease after presenting with limb pain and characteristic radiographic findings. Her radiographs show involvement of the humerus, femur, tibia, and fibula. Which specific part of these long bones is primarily affected by the sclerosis and thickening in this condition?

View Answer & Explanation
Correct Answer: D
Rationale: The teaching case explicitly states that Progressive Diaphyseal Dysplasia "is an autosomal dominant disorder involving the diaphyses of the long bones, skull base, and clavicles." The radiographic images (Fig. 1.120) also clearly show cortical thickening and sclerosis in the diaphyses. Therefore, the diaphyses (D) are the primary affected part of the long bones.
Question 4
A 28-year-old male presents with a long history of limb pain and muscle weakness. Radiographs demonstrate periosteal and endosteal sclerosis and thickening of the diaphyses of the long bones. He also has a thin habitus with decreased muscle mass. Which of the following features, if present, would make the diagnosis of Camurati–Engelmann disease less likely and suggest an alternative sclerosing bone dysplasia?
View Answer & Explanation
Correct Answer: C
Rationale: Camurati–Engelmann disease is characterized by *diaphyseal* sclerosis and thickening, skull base, and clavicle involvement, not *generalized* skeletal osteosclerosis with bone fragility (C), which is more characteristic of severe forms of osteopetrosis. Involvement of the skull base (A), autosomal dominant inheritance (B), waddling gait (D), and columnar shaped extremities (E) are all consistent features of Camurati–Engelmann disease.
Question 5
A 24-year-old male is evaluated for chronic limb pain and a peculiar body habitus. Physical examination reveals decreased muscle and subcutaneous fat mass, and his extremities appear columnar shaped. Radiographs confirm diaphyseal cortical thickening and sclerosis of the long bones. What is the typical body habitus observed in patients with Camurati–Engelmann disease?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 1.119 explicitly states: "Sometimes decreased muscle and subcutaneous fat mass and thin habitus with columnar shaped extremities occur." This directly matches option C. The other options describe features of other conditions or are contrary to the described presentation.
Question 6
A 35-year-old female with a confirmed diagnosis of Progressive Diaphyseal Dysplasia presents with a new complaint of progressive hearing loss. Given the known features of her condition, what is the most likely anatomical basis for her deafness?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case mentions "sometimes deafness" as a symptom and states that the disease involves the "skull base." Sclerosis and thickening of the skull base can lead to narrowing of foramina, causing impingement on cranial nerves, including the vestibulocochlear nerve (CN VIII), which would result in hearing loss. While otosclerosis (A) can cause hearing loss, it's not a primary feature of Camurati–Engelmann disease. Cochlear malformation (B), recurrent infections (D), and tympanic membrane perforation (E) are not directly linked to the bone pathology of this condition.
Question 7
A 17-year-old male is diagnosed with Camurati–Engelmann disease. In addition to the long bones and skull base, which other bone is specifically mentioned in the teaching case as being involved in this autosomal dominant disorder?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case explicitly states that Progressive Diaphyseal Dysplasia "is an autosomal dominant disorder involving the diaphyses of the long bones, skull base, and clavicles." Therefore, clavicles (C) are also affected. The other bones listed are not specifically mentioned as primary sites of involvement in the provided text.
Question 8
A 22-year-old female with Camurati–Engelmann disease undergoes a bone biopsy to further understand the pathology of her condition. The characteristic radiographic findings include periosteal and endosteal sclerosis and thickening of the diaphyses. What is the underlying pathological process responsible for these changes?
View Answer & Explanation
Correct Answer: C
Rationale: The terms "sclerosis" and "thickening" imply an increase in bone density and volume. This is typically due to abnormal bone remodeling characterized by excessive bone formation (osteosclerosis) and/or reduced bone resorption, leading to a net increase in bone mass. While the exact molecular mechanism isn't detailed, the macroscopic findings point to an imbalance favoring bone formation. Increased osteoclastic activity (A) would lead to bone resorption and osteopenia. Decreased osteoblastic activity (B) would also lead to less bone. Fibrous tissue replacement (D) is characteristic of fibrous dysplasia, and cartilage calcification (E) is a different process.
Question 9
A 6-year-old boy is diagnosed with early-stage Camurati–Engelmann disease. His initial radiographs show mild diaphyseal cortical thickening. His parents ask about the expected progression of the disease. Based on the name and description of the condition, what is the most likely long-term radiographic course?
View Answer & Explanation
Correct Answer: C
Rationale: The name "Progressive Diaphyseal Dysplasia" itself indicates a worsening course. The text also refers to "definitive, late form" radiographs (Fig. 1.122), implying that the changes become more pronounced with age. Therefore, worsening of diaphyseal sclerosis and thickening over time (C) is the expected long-term radiographic course. Spontaneous resolution (A) or stable appearance (B) are inconsistent with the "progressive" nature. Development of osteolytic lesions (D) or malignant transformation (E) are not characteristic features of this disease.
Question 10
A 50-year-old patient with a long-standing diagnosis of Camurati–Engelmann disease presents for follow-up. Radiographs are taken to assess the extent of the disease. In addition to the long bones, skull, and clavicles, which other skeletal region is shown in the provided images to be affected in the definitive, late form of the disease?

View Answer & Explanation
Correct Answer: D
Rationale: Fig. 1.122 a–d shows "Definitive, late form of progressive diaphyseal dysplasia on anteroposterior radiographs of skull (a), hand (b), arm (c), forearm (d)". The image specifically includes a radiograph of the hand (b), demonstrating involvement of the metacarpals and phalanges. The other options are not explicitly shown or mentioned as affected in the provided images/text.
Question 11
A 24-year-old male presents with chronic leg pain and a waddling gait. Radiographs of his lower extremities are shown. Based on these images, what is the most striking radiographic feature that confirms the diagnosis of Camurati–Engelmann disease?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 1.120 a–c is captioned: "Diaphyseal cortical thickening and sclerosis of long tubular bones are the main characteristics of Camurati-Engelmann disease." The images clearly illustrate this feature in the humerus, femur, tibia, and fibula. Options A, B, D, and E describe features not seen in the provided images or characteristic of this disease.
Question 12
A 24-year-old male is evaluated for a thin habitus and chronic limb pain. His physical examination reveals decreased muscle mass and columnar shaped extremities. Radiographs confirm diaphyseal sclerosis. Despite these findings, the patient does not exhibit any gross skeletal deformities. This observation is consistent with the description of Camurati–Engelmann disease. What does the clinical context for Fig. 1.119 specifically state regarding deformities?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 1.119 explicitly states: "No special deformities of the body are revealing for diaphyseal dysplasia." This means that while there are internal bone changes and a specific habitus, gross external deformities are not typically present or diagnostic. Options A, B, D, and E describe deformities that are not characteristic of Camurati–Engelmann disease as per the provided text.
Question 13
A 40-year-old male with Progressive Diaphyseal Dysplasia has experienced progressive symptoms including limb pain, muscle weakness, and occasional deafness. The sclerosis of the skull base is a known feature of his condition. What is a potential long-term complication directly related to the skull base involvement in this disease?
View Answer & Explanation
Correct Answer: C
Rationale: Sclerosis and thickening of the skull base can narrow the foramina through which cranial nerves exit the skull. This can lead to compression of these nerves, resulting in various neurological deficits, such as hearing loss (deafness, as mentioned in the symptoms) or other cranial neuropathies. Hydrocephalus (B) is a possibility with severe skull base thickening but cranial nerve compression (C) is a more direct and commonly cited complication related to the specific involvement described. The other options are not directly supported by the provided text as typical complications.
Question 14
A 10-year-old girl is diagnosed with Camurati–Engelmann disease. She experiences mild limb pain and some muscle weakness, but her symptoms are not severely debilitating. Her parents inquire about treatment options. Based on the provided clinical information, what is the most appropriate general approach to managing her condition?
View Answer & Explanation
Correct Answer: C
Rationale: The provided text describes the clinical features and radiographic findings but does not mention specific curative treatments or complex surgical interventions. Given the symptoms of limb pain and muscle weakness, symptomatic management, including pain relief and physical therapy to maintain muscle strength and mobility, would be the most appropriate general approach. There are no "special deformities" to surgically correct (A), bisphosphonates (B) are not mentioned as a treatment, bone marrow transplantation (D) is for hematological disorders, and prophylactic osteotomy (E) is not indicated as bone fragility or specific fracture risk is not highlighted.
Question 15
A 24-year-old male presents with chronic limb pain and muscle weakness. Radiographs reveal diffuse periosteal and endosteal sclerosis and thickening primarily affecting the diaphyses of his long bones, including the humerus, femur, tibia, and fibula. His family history indicates a similar condition in his father.
View Answer & Explanation
Correct Answer: C
Rationale: Progressive diaphyseal dysplasia, or Camurati–Engelmann disease, is explicitly stated to be an autosomal dominant disorder. The family history of a similar condition in the father further supports this inheritance pattern. Autosomal recessive (A) and X-linked patterns (B, D) are incorrect as the disease is autosomal dominant. Sporadic mutation (E) is less likely given the family history.
Question 16
A 15-year-old male presents with a waddling gait and generalized limb pain. Physical examination reveals decreased muscle mass and a thin habitus. Radiographs of the lower extremities demonstrate significant cortical thickening and sclerosis of the femoral and tibial diaphyses.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical case explicitly states that "Diaphyseal cortical thickening and sclerosis of long tubular bones are the main characteristics of Camurati-Engelmann disease." This is the hallmark radiographic finding. Metaphyseal widening (A) and epiphyseal dysgenesis (B) are characteristic of other skeletal dysplasias, not Camurati-Engelmann. Vertebral plana (D) is seen in conditions like eosinophilic granuloma or osteogenesis imperfecta. Joint space narrowing (E) is indicative of arthritis.
Question 17
A 10-year-old girl is brought to the clinic by her parents due to increasing difficulty with walking and frequent complaints of leg pain, especially after activity. Her gait is noted to be somewhat unsteady. Radiographs confirm progressive diaphyseal dysplasia.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text lists "waddling gait" as one of the most frequent symptoms of Camurati–Engelmann disease, alongside limb pain and muscle weakness. Severe short stature (A), intellectual disability (B), recurrent fractures (D), and macrocephaly (E) are not described as frequent symptoms or characteristics of this condition in the provided text.
Question 18
A 30-year-old woman with a known history of Camurati-Engelmann disease presents for follow-up. Her radiographs show the definitive, late form of the disease. In addition to the long bones, which other skeletal areas are typically affected by sclerosis in this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The case description explicitly states that Progressive Diaphyseal Dysplasia "involv[es] the diaphyses of the long bones, skull base, and clavicles." While the hands can show sclerosis (as seen in Fig 1.122b), the skull base and clavicles are specifically mentioned as additional primary sites of involvement. The other options (A, B, D, E) are not listed as primary sites of involvement in the provided text.
Question 19
A 24-year-old male presents with chronic limb pain and a thin body habitus. Radiographs confirm progressive diaphyseal dysplasia. Which of the following physical examination findings, though not universally present, is sometimes associated with this condition?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context for Fig. 1.119 states: "Sometimes decreased muscle and subcutaneous fat mass and thin habitus with columnar shaped extremities occur." This directly supports option B. Joint hypermobility (A), skin hyperpigmentation (C), shortened digits (D), and craniofacial dysmorphism (E) are not mentioned in the provided text as associated findings.
Question 20
A 35-year-old male with a long-standing diagnosis of Camurati-Engelmann disease reports progressive difficulty hearing. Given the known skeletal involvement of this condition, which anatomical area is most likely contributing to his new symptom?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states that "sometimes deafness" is a symptom and that the disease involves the "skull base." Sclerosis and thickening of the skull base can impinge on cranial nerves, including the auditory nerve, leading to deafness. While mandibular thickening (A) is not specified, vertebral body sclerosis (B), clavicular hypertrophy (D), and hand bone sclerosis (E) are not directly linked to deafness in the provided text.
Question 21
A 7-year-old boy presents with unexplained limb pain. Initial radiographs of his long bones show abnormal bone density. Further imaging reveals a characteristic pattern of bone changes consistent with Camurati-Engelmann disease. What specific type of bone sclerosis is described?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states: "The radiography shows a periosteal and endosteal sclerosis and thickening of the diaphysis of the long bones." This describes the characteristic radiographic finding. The other options describe different or opposite bone changes not associated with this condition.
Question 22
A 24-year-old male presents with chronic, diffuse limb pain and muscle weakness. Radiographs of his long bones show significant diaphyseal cortical thickening and sclerosis. His physical examination reveals a thin habitus and columnar shaped extremities, but no gross deformities. This presentation is consistent with progressive diaphyseal dysplasia.
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 1.119, depicting a 24-year-old male, notes "No special deformities of the body are revealing for diaphyseal dysplasia." This suggests that gross deformities may not be present, especially in earlier or less severe presentations, despite the underlying bone changes. The term "progressive" implies a worsening over time, but the initial presentation may not involve severe deformities. The disease primarily affects diaphyses, not epiphyses (D). The text does not suggest early mortality (B) or unilateral symptoms (E). Severe deformities in early childhood (A) are not mentioned as typical.
Question 23
A 24-year-old male is evaluated for chronic limb pain and muscle weakness. On physical examination, he is noted to have a thin habitus and extremities that appear unusually straight and uniform in width. Radiographs confirm progressive diaphyseal dysplasia. What term is used to describe the appearance of his extremities?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 1.119 explicitly states that "Sometimes decreased muscle and subcutaneous fat mass and thin habitus with columnar shaped extremities occur." This directly answers the question. The other options describe different types of limb deformities not specifically mentioned in the context of Camurati-Engelmann disease in the provided text.
Question 24
A 12-year-old boy presents with a history of increasing limb pain and a waddling gait. Radiographs of his long bones, including the humerus, femur, tibia, and fibula, show diffuse cortical thickening and sclerosis primarily affecting the central shafts. This pattern is highly suggestive of Camurati-Engelmann disease.
View Answer & Explanation
Correct Answer: C
Rationale: The radiographic findings of "cortical thickening and sclerosis" directly describe osteosclerosis, which is an increase in bone density. Osteoporosis (A) is decreased bone density. Osteopetrosis (B) is a generalized increase in bone density, often affecting the entire bone, not just the diaphysis, and typically presents with different clinical features. Osteomalacia (D) is defective mineralization of bone. Osteolysis (E) is bone destruction.
Question 25
A 20-year-old male presents with chronic leg pain and muscle weakness. Radiographs of his lower extremities show bilateral, symmetric diaphyseal cortical thickening and sclerosis of the femurs and tibias. The epiphyses and metaphyses appear relatively spared. This radiographic pattern is most characteristic of:
View Answer & Explanation
Correct Answer: C
Rationale: The description "bilateral, symmetric diaphyseal cortical thickening and sclerosis... epiphyses and metaphyses appear relatively spared" perfectly matches the definition and radiographic findings of Progressive Diaphyseal Dysplasia (Camurati-Engelmann disease) as described in the text. Osteogenesis Imperfecta (A) involves fragile bones and fractures, not sclerosis. Fibrous Dysplasia (B) presents with lytic lesions and ground-glass matrix. Achondroplasia (D) is a dwarfism characterized by rhizomelic shortening and metaphyseal abnormalities. Multiple Hereditary Exostoses (E) involves osteochondromas near growth plates.
Question 26
A 24-year-old male presents with chronic limb pain and muscle weakness. Radiographs show diffuse periosteal and endosteal sclerosis and thickening of the diaphysis of the long bones. What is the primary anatomical region of the long bones affected in Camurati-Engelmann disease?
View Answer & Explanation
Correct Answer: D
Rationale: The name of the disease itself, "Progressive Diaphyseal Dysplasia," and the explicit statement in the text, "involving the diaphyses of the long bones," clearly indicate that the diaphysis is the primary anatomical region affected. The epiphysis (A), metaphysis (B), physis (C), and articular cartilage (E) are not the primary sites of involvement as described.
Question 27
A 40-year-old male with a long-standing diagnosis of Camurati-Engelmann disease undergoes a skeletal survey. The radiographs show extensive sclerosis and cortical thickening. Which of the following images represents a definitive, late form of this condition, demonstrating involvement beyond just the long bone diaphyses?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 1.122 is specifically labeled "Definitive, late form of progressive diaphyseal dysplasia on anteroposterior radiographs of skull (a), hand (b), arm (c), forearm (d)." This image directly shows sclerosis in the skull and hand bones, which are areas mentioned in the text as being involved in the disease (skull base, and by extension, other skull bones can be affected, and hand bones are shown in the image). The other options describe findings inconsistent with Camurati-Engelmann disease.
Question 28
A 28-year-old female presents with a several-year history of progressive limb pain, muscle weakness, and a noticeable waddling gait. Her physical exam reveals a thin habitus. Radiographs of her long bones show diffuse diaphyseal cortical thickening and sclerosis. Based on this constellation of findings, what is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The combination of limb pain, muscle weakness, waddling gait, thin habitus, and characteristic radiographic findings of "diffuse diaphyseal cortical thickening and sclerosis" is the classic presentation of Camurati-Engelmann Disease (Progressive Diaphyseal Dysplasia) as described in the provided text. Osteoporosis (A) involves decreased bone density. Paget's Disease (B) typically involves localized areas of abnormal bone remodeling, often with characteristic radiographic findings like cotton wool skull or blade of grass sign, and is not primarily diaphyseal sclerosis. Rickets (D) involves defective mineralization, leading to bone softening and deformities, not sclerosis. Marfan Syndrome (E) is a connective tissue disorder with skeletal features like arachnodactyly and scoliosis, not diaphyseal sclerosis.
Question 29
A 5-year-old boy is diagnosed with Progressive Diaphyseal Dysplasia. His parents ask about the long-term outlook and how the disease might change over time. What does the term "Progressive" in the disease name primarily imply?
View Answer & Explanation
Correct Answer: B
Rationale: The term "Progressive" in Progressive Diaphyseal Dysplasia implies that the disease's manifestations, both clinical symptoms (pain, weakness, gait issues) and radiographic changes (sclerosis, thickening), tend to advance and worsen over time. The case describes "definitive, late form" images, supporting this progression. The disease is not described as curable (A) or reversible (E). It is an autosomal dominant hereditary condition (C). It affects multiple long bones bilaterally, not just one limb (D).
Question 30
A 24-year-old male with Camurati-Engelmann disease undergoes a skeletal survey. In addition to the diaphyses of the long bones and the skull base, which other specific bone is mentioned in the clinical description as being involved in this autosomal dominant disorder?
View Answer & Explanation
Correct Answer: C
Rationale: The introductory text for the case explicitly states that Progressive Diaphyseal Dysplasia "involv[es] the diaphyses of the long bones, skull base, and clavicles." Therefore, the clavicle is a specifically mentioned site of involvement. The other bones listed are not mentioned in the provided text as being typically involved.
Question 31
A 30-year-old patient with a confirmed diagnosis of Camurati-Engelmann disease reports new onset headaches and occasional visual disturbances. Given the known skeletal involvement, which of the following is the most likely underlying cause of these neurological symptoms?
View Answer & Explanation
Correct Answer: B
Rationale: The text mentions "skull base" involvement and "sometimes deafness." Thickening and sclerosis of the skull base can lead to narrowing of foramina, impinging on cranial nerves (like the auditory nerve causing deafness) or increasing intracranial pressure, which can manifest as headaches and visual disturbances. Spinal cord compression (A) is not mentioned as a typical complication. Peripheral nerve entrapment (C) and vascular compromise (D) are not directly linked to the described neurological symptoms in the text. Direct brain involvement (E) is not a feature of this skeletal dysplasia.
Question 32
A 24-year-old male presents with chronic limb pain and muscle weakness. Radiographs of his long bones show periosteal and endosteal sclerosis and thickening of the diaphysis. This finding indicates an abnormality in which of the following bone processes?
View Answer & Explanation
Correct Answer: B
Rationale: Periosteal and endosteal sclerosis and thickening indicate an imbalance in bone remodeling, specifically an excessive deposition of bone (formation) relative to its removal (resorption). This leads to increased bone density and cortical thickness. Cartilage formation (A) is primarily related to growth plates and articular surfaces. Hematopoiesis (C) occurs in the bone marrow. Joint lubrication (D) is a function of synovial fluid. Muscle contraction (E) is a muscular function, though muscle weakness is a symptom, it's not the primary bone process affected.
Question 33
A 24-year-old male presents with chronic limb pain. On examination, he has a thin habitus with decreased muscle and subcutaneous fat mass, and his extremities appear columnar shaped. Radiographs confirm diaphyseal cortical thickening and sclerosis of the long bones. This overall clinical picture, including the body habitus, is sometimes associated with:
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 1.119 explicitly states: "Sometimes decreased muscle and subcutaneous fat mass and thin habitus with columnar shaped extremities occur" in patients with diaphyseal dysplasia. This specific description of body habitus, combined with the limb pain and radiographic findings, is characteristic of Progressive Diaphyseal Dysplasia (Camurati-Engelmann disease). The other options describe contrasting body compositions or conditions.
Question 34
A 6-year-old boy presents with a waddling gait and bilateral knee pain. His parents note he has always been shorter than his peers. Physical examination reveals mild joint stiffness and limited range of motion in multiple joints. Radiographs show irregular and flattened epiphyses, particularly in the hips and knees, with delayed epiphyseal ossification.
View Answer & Explanation
Correct Answer: C
Rationale: Multiple Epiphyseal Dysplasia is characterized by predominantly epiphyseal involvement, leading to joint pain, waddling gait, and short stature due to irregular and flattened epiphyses. Achondroplasia primarily affects the metaphyses and growth plates, leading to disproportionate dwarfism with short limbs but a normal trunk. Spondyloepiphyseal Dysplasia Congenita involves both spine and epiphyses, often with more severe spinal involvement.
Question 35
A newborn is noted to have disproportionately short limbs, a normal trunk length, and a prominent forehead. Physical examination reveals rhizomelic shortening of the extremities. Radiographs demonstrate short long bones with characteristic metaphyseal flaring and a narrow interpedicular distance in the lumbar spine.
View Answer & Explanation
Correct Answer: D
Rationale: Achondroplasia is the most common form of disproportionate dwarfism, characterized by short limbs (rhizomelic shortening), a normal trunk, and distinct radiographic findings of metaphyseal involvement and a narrow interpedicular distance in the lumbar spine. Multiple Epiphyseal Dysplasia primarily affects the epiphyses. The other options are also metaphyseal dysplasias but present with different clinical and radiographic features.
Question 36
A 5-year-old girl presents with short stature, a short neck, and a barrel chest. Her parents report progressive stiffness in her spine and hips. Radiographs show platyspondyly (flattened vertebral bodies) and hypoplastic femoral epiphyses, along with early degenerative changes in the hips.
View Answer & Explanation
Correct Answer: C
Rationale: Spondyloepiphyseal Dysplasia Congenita (SEDc) is characterized by short trunk dwarfism, platyspondyly, and epiphyseal involvement, particularly in the hips, leading to early osteoarthritis. Mucopolysaccharidoses can also cause spinal and epiphyseal changes but typically present with coarse facial features and organomegaly. Achondroplasia primarily affects long bone metaphyses, not primarily the spine in this manner.
Question 37
A 3-year-old boy is brought to the clinic due to progressive joint stiffness, coarse facial features, and developmental delay. Physical examination reveals hepatosplenomegaly and corneal clouding. Radiographs show dysostosis multiplex, including oar-shaped ribs, bullet-shaped phalanges, and a J-shaped sella turcica.
View Answer & Explanation
Correct Answer: C
Rationale: The constellation of coarse facial features, joint stiffness, hepatosplenomegaly, corneal clouding, and dysostosis multiplex on radiographs is classic for Mucopolysaccharidoses. Osteogenesis Imperfecta is characterized by brittle bones and blue sclera. Marfan's syndrome involves connective tissue laxity and tall stature. Achondroplasia is a form of dwarfism with metaphyseal involvement.
Question 38
A 14-year-old boy presents with multiple hard, bony masses around his knees and shoulders. Some of these masses are painful, especially when bumped, and one near the fibular head is causing peroneal nerve symptoms. Radiographs show multiple pedunculated and sessile bony outgrowths arising from the metaphyses of long bones, with cortical and medullary continuity with the underlying bone.
View Answer & Explanation
Correct Answer: C
Rationale: Multiple Exostoses (hereditary multiple osteochondromas) is characterized by multiple bony outgrowths (osteochondromas) that arise from the external surface of bones, often near growth plates, and can cause pain, deformity, or nerve compression. Dysplasia Epiphysealis Hemimelica is typically a solitary lesion affecting an epiphysis. Enchondromatosis involves intramedullary cartilaginous lesions. Osteoid osteoma is a small, painful lesion with a lucent nidus, and fibrous dysplasia is a bone-replacing lesion.
Question 39
A 25-year-old woman presents with multiple enchondromas in her hands and feet, some of which are causing pathological fractures. She also has several soft tissue hemangiomas on her trunk and extremities. Radiographs confirm multiple lucent lesions in the small tubular bones, consistent with enchondromas.
View Answer & Explanation
Correct Answer: C
Rationale: Maffucci’s Disease is a rare, non-hereditary disorder characterized by the presence of multiple enchondromas and soft tissue hemangiomas. Ollier’s Disease also involves multiple enchondromas but lacks the associated hemangiomas. Multiple Exostoses are osteochondromas, not enchondromas. Osteopoikilosis is characterized by multiple small, dense bone islands.
Question 40
A 2-year-old child is brought to the emergency department with a new fracture of the femur after a minor fall. This is the third fracture in the past year. The child's mother mentions that the child's eyes have a bluish tint. Physical examination reveals hyperlaxity of joints and blue sclera. Radiographs show generalized osteopenia and multiple healed fractures in various stages of healing.
View Answer & Explanation
Correct Answer: C
Rationale: Osteogenesis Imperfecta is a genetic disorder characterized by brittle bones, recurrent fractures, blue sclera, and joint hyperlaxity due to defects in collagen synthesis. Osteopetrosis causes increased bone density and fragility. Marfan's syndrome involves connective tissue, leading to tall stature, arachnodactyly, and cardiovascular issues, not primarily brittle bones. Hypophosphatasia is a metabolic bone disease, and Caffey's disease is infantile cortical hyperostosis.
Question 41
A 6-month-old infant presents with recurrent fractures, anemia, and hepatosplenomegaly. Physical examination reveals a large head and optic atrophy. Radiographs show diffuse, symmetric increase in bone density, particularly in the skull and long bones, with obliteration of the medullary canals.
View Answer & Explanation
Correct Answer: B
Rationale: Osteopetrosis, also known as Albers-Schönberg’s Disease or marble bone disease, is characterized by abnormally dense but brittle bones due to defective osteoclast function, leading to recurrent fractures, anemia (due to obliteration of marrow space), and cranial nerve compression (e.g., optic atrophy). Osteogenesis Imperfecta causes decreased bone density. Progressive Diaphyseal Dysplasia causes cortical thickening of diaphyses, and Caffey's disease is localized cortical hyperostosis.
Question 42
A 7-year-old boy presents with a 3-day history of fever, localized pain, and swelling in his left distal femur. He refuses to bear weight on the leg. Laboratory tests show elevated white blood cell count, ESR, and CRP. Radiographs initially show soft tissue swelling, followed by subtle lucency in the metaphysis and periosteal reaction a week later.
View Answer & Explanation
Correct Answer: C
Rationale: Acute Hematogenous Pyogenic Osteomyelitis typically presents with acute onset of fever, localized pain, and swelling in a long bone metaphysis in children, with elevated inflammatory markers. Tuberculous osteomyelitis is more insidious. Chronic bacterial osteomyelitis is a later stage. Osteosarcoma and Ewing's sarcoma are bone tumors, which can mimic infection but have different radiographic and clinical progression.
Question 43
A 45-year-old immigrant man presents with chronic low back pain, night sweats, and weight loss over several months. Physical examination reveals tenderness over the thoracolumbar spine and a gibbus deformity. Radiographs show destruction of multiple vertebral bodies with associated disc space narrowing and a large paraspinal soft tissue mass.
View Answer & Explanation
Correct Answer: C
Rationale: The chronic nature of symptoms, constitutional signs (night sweats, weight loss), vertebral body destruction, disc space narrowing, and paraspinal abscess (Pott's abscess) are classic features of Tuberculous Osteomyelitis (Pott's disease). Pyogenic spondylodiscitis is typically more acute. Ankylosing spondylitis involves sacroiliitis and syndesmophytes. Metastatic bone disease can cause vertebral destruction but typically spares the disc space until late stages. Forestier's disease is diffuse idiopathic skeletal hyperostosis.
Question 44
A 55-year-old woman complains of symmetric pain and stiffness in her hands, wrists, and feet for the past 6 months. She describes morning stiffness lasting over an hour. Physical examination reveals swollen, tender metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints, and ulnar deviation of the fingers. Radiographs show periarticular osteopenia, joint space narrowing, and erosions at the MCP and PIP joints.
View Answer & Explanation
Correct Answer: D
Rationale: The clinical presentation of symmetric polyarthritis, prolonged morning stiffness, and characteristic radiographic findings of periarticular osteopenia and erosions in the MCP and PIP joints are highly suggestive of Rheumatoid Arthritis. Osteoarthritis typically affects DIP joints more, with less inflammation and no erosions. Psoriatic arthritis is often asymmetric and can involve DIP joints and dactylitis. SLE can cause arthralgia but less often erosive arthritis. Gout is typically monoarticular and acute.
Question 45
A 28-year-old man presents with chronic low back pain and stiffness that is worse in the morning and improves with exercise. He also reports intermittent buttock pain. Physical examination reveals decreased spinal mobility, particularly in flexion and extension. Radiographs of the pelvis show bilateral sacroiliitis with erosions and sclerosis. Laboratory tests are positive for HLA-B27.
View Answer & Explanation
Correct Answer: D
Rationale: The classic presentation of chronic inflammatory back pain improving with exercise, decreased spinal mobility, bilateral sacroiliitis on radiographs, and positive HLA-B27 is diagnostic for Ankylosing Spondylitis. Lumbar disc herniation causes mechanical back pain, often radiating, and does not involve sacroiliitis. Deforming spondylarthritis is a degenerative condition of older adults. Tuberculous osteomyelitis would have constitutional symptoms and destructive lesions. Rheumatoid arthritis primarily affects peripheral joints.
Question 46
A 60-year-old man with a history of diabetes mellitus presents with a swollen, deformed, and insensate right ankle. He denies any significant trauma. Physical examination reveals a warm, erythematous, and unstable ankle joint with palpable crepitus. Radiographs show severe disorganization of the ankle joint, fragmentation of the talus, and extensive new bone formation.
View Answer & Explanation
Correct Answer: D
Rationale: The combination of a deformed, swollen, unstable, and insensate joint in a patient with diabetes, along with radiographic evidence of severe joint disorganization and new bone formation, is characteristic of Neurogenic Osteoarthropathy, also known as Charcot’s Joint. Diabetes is a common cause. Gout and bacterial arthritis are typically acute and painful. Osteoarthritis is a degenerative process, usually less destructive and not insensate. Reflex sympathetic dystrophy involves pain and autonomic dysfunction, not primary joint destruction.
Question 47
A 48-year-old man presents with sudden onset of excruciating pain and swelling in his right great toe. He reports a similar episode a year ago that resolved spontaneously. Physical examination reveals a warm, erythematous, and exquisitely tender first metatarsophalangeal (MTP) joint. Laboratory tests show elevated serum uric acid.
View Answer & Explanation
Correct Answer: C
Rationale: The acute onset of severe monoarticular pain and inflammation, particularly in the first MTP joint (podagra), with elevated serum uric acid, is classic for Gout. Bacterial arthritis would also be acute but typically presents with systemic signs of infection and requires joint aspiration for diagnosis. Psoriatic arthritis can affect the MTP joints but is less typically acute and monoarticular. Osteoarthritis is chronic and less inflammatory. Morton neuroma causes forefoot pain, often burning, but not acute joint inflammation.
Question 48
An 80-year-old man presents with increasing pain in his left tibia and a progressive bowing deformity of the leg. He also mentions that his hats no longer fit. Physical examination reveals a warm, thickened tibia. Laboratory tests show a significantly elevated alkaline phosphatase level. Radiographs of the tibia show cortical thickening, coarsened trabeculae, and areas of osteolysis and osteosclerosis, with a characteristic "blade of grass" or "V-shaped" lesion.
View Answer & Explanation
Correct Answer: D
Rationale: The clinical picture of bone pain, bowing deformity, increased hat size, elevated alkaline phosphatase, and characteristic radiographic findings of cortical thickening, coarsened trabeculae, and mixed lytic/sclerotic lesions is diagnostic of Paget’s Disease (Osteitis Deformans). Osteoporosis is characterized by decreased bone density. Osteomalacia involves defective mineralization. Hyperparathyroidism causes bone resorption. Osteopetrosis results in diffusely dense, brittle bones.
Question 49
A 17-year-old male presents with a 3-month history of localized, dull aching pain in his right proximal tibia. The pain is worse at night and is consistently relieved by over-the-counter NSAIDs. Physical examination reveals localized tenderness over the anterior tibia. Radiographs show a small, lucent lesion (nidus) approximately 1 cm in diameter, surrounded by a dense sclerotic rim in the tibial cortex.
View Answer & Explanation
Correct Answer: C
Rationale: The classic presentation of localized bone pain, worse at night, and dramatically relieved by NSAIDs, along with a small lucent nidus surrounded by a sclerotic rim on radiographs, is characteristic of an Osteoid Osteoma. Osteoblastoma is a larger lesion (>2 cm), often less responsive to NSAIDs. Enchondroma is a cartilaginous tumor within the medullary cavity. Chondroblastoma is an epiphyseal lesion. Fibrous dysplasia is a benign bone-replacing lesion.
Question 50
A 10-year-old girl presents with a painless, hard lump near her left knee that has been slowly growing for the past year. Physical examination reveals a firm, immobile mass palpable on the medial aspect of the distal femur. Radiographs show a pedunculated bony projection arising from the metaphysis of the distal femur, pointing away from the joint, with continuity of the cortex and medullary cavity with the underlying bone.
View Answer & Explanation
Correct Answer: B
Rationale: An Osteochondroma is a benign bone tumor characterized by a bony outgrowth (exostosis) with a cartilaginous cap, typically arising from the metaphysis of long bones and growing away from the adjacent joint. It shows cortical and medullary continuity with the parent bone. Enchondroma is an intramedullary cartilaginous lesion. Chondroblastoma is an epiphyseal lesion. Dysplasia Epiphysealis Hemimelica is an irregular cartilaginous overgrowth of an epiphysis. Nonossifying fibroma is a benign fibrous cortical defect.
Question 51
A 28-year-old woman presents with progressive pain and swelling around her right knee for 4 months. Physical examination reveals a tender, warm mass in the distal femur. Radiographs show an eccentric, expansile lytic lesion in the distal femoral metaphysis, extending to the subchondral bone, with a narrow zone of transition and no significant periosteal reaction. MRI reveals fluid-fluid levels within the lesion.
View Answer & Explanation
Correct Answer: D
Rationale: Giant Cell Tumor of Bone (GCT) typically occurs in young adults (20-40 years old) and presents as an eccentric, expansile lytic lesion in the epiphysis/metaphysis, extending to the subchondral bone, often around the knee. Fluid-fluid levels can be seen in GCTs, but are more characteristic of Aneurysmal Bone Cysts (ABC). However, ABCs are typically seen in younger patients and are not as common in the epiphysis. Chondroblastoma is epiphyseal but usually in younger patients. Osteosarcoma is malignant and typically has a more aggressive appearance with periosteal reaction and matrix mineralization. Unicameral bone cysts are metaphyseal and centrally located, often in children.
Question 52
A 12-year-old boy presents with a 2-month history of left thigh pain, swelling, and intermittent fever. Physical examination reveals a tender, warm mass in the mid-diaphysis of the femur. Laboratory tests show elevated ESR and CRP. Radiographs show a large, destructive lytic lesion in the femoral diaphysis with a characteristic "onion skin" periosteal reaction and soft tissue mass. Biopsy confirms small round blue cells.
View Answer & Explanation
Correct Answer: D
Question 52
A 6-year-old male presents with a 3-day history of fever, malaise, and severe pain in his right distal femur. On examination, the area is warm, swollen, and exquisitely tender to palpation. He refuses to bear weight on the affected leg. Laboratory tests reveal an elevated white blood cell count, ESR, and CRP. Radiographs show subtle soft tissue swelling around the distal femur, with no obvious bony changes. An MRI of the femur demonstrates diffuse bone marrow edema and a subperiosteal fluid collection in the distal metaphysis.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of fever, localized bone pain, refusal to bear weight, elevated inflammatory markers, and radiographic findings of soft tissue swelling with MRI showing bone marrow edema and subperiosteal fluid collection in the metaphysis of a long bone in a child are classic for acute hematogenous pyogenic osteomyelitis. This condition is typically caused by bacterial infection spreading through the bloodstream to the bone. Septic arthritis (A) would primarily involve the joint space, though it can occur concurrently. Cellulitis (B) is a soft tissue infection without bone involvement. Ewing's sarcoma (D) is a bone tumor that can mimic infection but typically presents with more chronic symptoms and characteristic "onion-skin" periosteal reaction on X-ray. A stress fracture (E) would not present with fever or elevated inflammatory markers.
Question 52
A 4-year-old female presents with a 6-month history of persistent swelling and pain in her left knee, accompanied by morning stiffness that improves throughout the day. She denies any specific trauma. Physical examination reveals a warm, swollen left knee with a limited range of motion, but no systemic signs of infection. Laboratory tests show a mildly elevated ESR and CRP, and negative rheumatoid factor. Radiographs of the knee demonstrate periarticular osteopenia and mild joint space widening.
View Answer & Explanation
Correct Answer: C
Rationale: The chronic nature of the knee swelling and pain (6 months), morning stiffness, and periarticular osteopenia in a young child, without a history of trauma or acute infection, are highly suggestive of juvenile idiopathic arthritis (JIA). Septic arthritis (A) would present with acute, severe pain, fever, and rapid joint destruction. Transient synovitis (B) is usually acute, self-limiting, and typically affects the hip. Legg-Calvé-Perthes disease (D) affects the hip, not typically the knee, and involves avascular necrosis of the femoral head. Osteochondritis dissecans (E) involves a lesion of articular cartilage and subchondral bone, often presenting with mechanical symptoms like locking, and is less likely to cause chronic, diffuse joint swelling and morning stiffness.
Question 52
A 28-year-old male complains of chronic low back pain and stiffness for the past 2 years. The pain is worse in the morning and improves with activity. He also reports intermittent buttock pain. Physical examination reveals limited lumbar spine flexion and extension, and tenderness over the sacroiliac joints. Laboratory tests show an elevated ESR and a positive HLA-B27 allele. Radiographs of the pelvis show bilateral sacroiliitis with erosions and sclerosis.
View Answer & Explanation
Correct Answer: D
Rationale: The patient's age, chronic inflammatory back pain (worse in the morning, improves with activity), limited spinal mobility, sacroiliac joint tenderness, positive HLA-B27, and radiographic evidence of bilateral sacroiliitis are classic features of ankylosing spondylitis. Lumbar disc herniation (A) typically causes radicular pain and does not present with sacroiliitis or morning stiffness improving with activity. Mechanical low back pain (B) is usually exacerbated by activity and relieved by rest. DISH (C) typically affects older individuals and involves flowing ossification along the anterior longitudinal ligament, sparing the sacroiliac joints initially. Psoriatic arthritis (E) can involve the spine and sacroiliac joints but is usually associated with psoriatic skin lesions and peripheral arthritis, which are not mentioned here as primary complaints.
Question 52
A 55-year-old male presents with sudden onset of excruciating pain, swelling, and redness in his right great toe MTP joint. He reports a similar episode in the past that resolved spontaneously. On examination, the joint is hot, swollen, and extremely tender to touch. He has a history of hypertension and is on a diuretic. Serum uric acid level is elevated. Arthrocentesis of the affected joint reveals turbid synovial fluid with numerous negatively birefringent needle-shaped crystals.
View Answer & Explanation
Correct Answer: C
Rationale: The acute onset of severe pain, swelling, and redness in the great toe MTP joint (podagra), elevated serum uric acid, and the presence of negatively birefringent needle-shaped crystals in the synovial fluid are pathognomonic for gout. Septic arthritis (A) would also present acutely but would typically show positive bacterial cultures and white blood cells without specific crystal morphology. Pseudogout (B) involves calcium pyrophosphate crystals, which are positively birefringent and rhomboid-shaped. Cellulitis (D) is a soft tissue infection without joint involvement, and arthrocentesis would not yield crystals. A bunion (E) is a chronic deformity, not an acute inflammatory attack.
Question 52
A 72-year-old male presents with progressive bowing of his left tibia, increasing hat size, and generalized bone pain. He also reports some hearing loss. Physical examination reveals a warm, tender left tibia and a slightly enlarged skull. Laboratory tests show a significantly elevated serum alkaline phosphatase level. Radiographs of the tibia and skull demonstrate cortical thickening, bone enlargement, and a mixed lytic and sclerotic pattern.
View Answer & Explanation
Correct Answer: D
Rationale: The patient's age, symptoms of bone pain, increasing hat size (skull involvement), bowing of long bones, hearing loss, markedly elevated alkaline phosphatase, and characteristic radiographic findings of cortical thickening, bone enlargement, and mixed lytic/sclerotic lesions are classic for Paget's disease of bone (Osteitis Deformans). Osteoporosis (A) is characterized by decreased bone density and increased fracture risk, not bone enlargement or elevated alkaline phosphatase. Osteomalacia (B) involves defective bone mineralization, leading to soft bones, but not typically the radiographic changes seen here. Metastatic bone disease (C) can cause bone pain and lytic/sclerotic lesions but usually does not cause diffuse bone enlargement or such a high alkaline phosphatase without liver involvement. Fibrous dysplasia (E) is a developmental anomaly of bone, typically presenting in younger individuals with "ground-glass" appearance, and is less likely to be widespread with these specific features in an elderly patient.
Question 52
A 16-year-old male presents with a 3-month history of localized pain in his right tibia. The pain is dull, persistent, worse at night, and consistently relieved by over-the-counter NSAIDs. Physical examination reveals localized tenderness over the anterior tibia. Radiographs show a small, well-circumscribed lucent lesion (nidus) approximately 1 cm in diameter, surrounded by a dense sclerotic rim, in the cortical bone of the tibia.
View Answer & Explanation
Correct Answer: C
Rationale: The classic presentation of an osteoid osteoma includes localized bone pain, worse at night, and dramatically relieved by NSAIDs, in an adolescent or young adult. Radiographically, it is characterized by a small lucent nidus (typically <1.5-2 cm) surrounded by a dense sclerotic reaction. Osteoblastoma (A) is histologically similar but larger (>2 cm), less sclerotic, and pain is less responsive to NSAIDs. Enchondroma (B) is a cartilaginous tumor typically found in the medullary cavity of small bones of the hands and feet, usually asymptomatic. Osteosarcoma (D) is a malignant tumor with aggressive features, often a "sunburst" or Codman's triangle appearance, and pain not relieved by NSAIDs. Chronic osteomyelitis (E) would typically have a history of infection, possibly drainage, and different radiographic features.
Question 52
A 25-year-old female presents with a 6-month history of progressive pain and swelling around her left knee. She reports some mechanical symptoms but no specific injury. Physical examination reveals a palpable mass and tenderness over the distal femur. Radiographs show a large, eccentric, purely lytic lesion in the epiphysis and metaphysis of the distal femur, extending to the subchondral bone, with no sclerotic rim. There is cortical thinning and some soft tissue extension.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical picture of a young adult with an eccentric, purely lytic lesion in the epiphysis/metaphysis of a long bone (especially around the knee), extending to the subchondral bone, without a sclerotic rim, is highly characteristic of a giant cell tumor of bone (GCT). Chondroblastoma (A) is also epiphyseal but typically smaller, with a sclerotic rim, and often has calcifications. Aneurysmal bone cyst (B) is expansile, lytic, and often multiloculated, but can occur in any age group and location, and is not typically purely epiphyseal. Unicameral bone cyst (D) is typically metaphyseal, centrally located, and seen in children. Osteosarcoma (E) is malignant, often has a more aggressive appearance with periosteal reaction and osteoid matrix, and is more common in the metaphysis of long bones in adolescents.
Question 52
An 8-year-old male presents with a 2-month history of worsening pain and swelling in his right thigh, accompanied by intermittent fever and weight loss. Physical examination reveals a tender, warm, and firm mass in the mid-diaphysis of the femur. Laboratory tests show elevated ESR and CRP. Radiographs of the femur demonstrate a large lytic lesion in the diaphysis with a characteristic "onion-skin" periosteal reaction.
View Answer & Explanation
Correct Answer: D
Rationale: The patient's age, diaphyseal location, systemic symptoms (fever, weight loss), and the classic "onion-skin" periosteal reaction on radiographs are highly suggestive of Ewing's sarcoma. Osteomyelitis (A) can mimic Ewing's but typically has a more acute onset, and while it can cause periosteal reaction, the "onion-skin" appearance is more characteristic of Ewing's. Osteosarcoma (B) is more common in the metaphysis and typically presents with a "sunburst" periosteal reaction and osteoid matrix. Langerhans cell histiocytosis (C) can cause lytic lesions but usually does not have the prominent "onion-skin" periosteal reaction or the same systemic symptoms. A stress fracture (E) would not present with fever, weight loss, or an "onion-skin" periosteal reaction.
Question 52
A 9-year-old male presents to the emergency department after a minor fall, complaining of mild pain in his left humerus. Radiographs taken to rule out a fracture reveal an incidental, well-defined, centrally located lucent lesion in the proximal metaphysis of the humerus. The lesion appears to thin the cortex and has a "fallen leaf" sign within it, indicating a pathologic fracture.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical scenario of an asymptomatic, centrally located, well-defined lucent metaphyseal lesion in a child, often discovered incidentally after a pathologic fracture (indicated by the "fallen leaf" sign), is classic for a unicameral bone cyst (UBC). Aneurysmal bone cyst (A) is typically expansile, eccentric, and multiloculated. Nonossifying fibroma (B) is usually eccentric, cortical, and has a sclerotic rim, often resolving spontaneously. Fibrous dysplasia (D) has a "ground-glass" appearance and can be expansile, but is not typically centrally located or associated with a "fallen leaf" sign. Enchondroma (E) is a cartilaginous tumor, usually in small bones of hands/feet, and does not typically present with a "fallen leaf" sign.
Question 52
A 14-year-old female presents with a history of recurrent fractures and progressive bowing of her right femur. She also has several café-au-lait spots on her trunk. Radiographs of the femur show a characteristic "shepherd's crook" deformity and a diffuse, expansile lesion with a "ground-glass" appearance in the bone marrow, thinning the cortex.
Question 53
A 6-year-old male presents with a 3-day history of fever, malaise, and severe pain in his right distal femur. On examination, the area is warm, swollen, and exquisitely tender to palpation. He refuses to bear weight on the affected leg. Laboratory tests reveal an elevated white blood cell count, ESR, and CRP. Radiographs show subtle soft tissue swelling around the distal femur, with no obvious bony changes. An MRI of the femur demonstrates diffuse bone marrow edema and a subperiosteal fluid collection in the distal metaphysis.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of fever, localized bone pain, refusal to bear weight, elevated inflammatory markers, and radiographic findings of soft tissue swelling with MRI showing bone marrow edema and subperiosteal fluid collection in the metaphysis of a long bone in a child are classic for acute hematogenous pyogenic osteomyelitis. This condition is typically caused by bacterial infection spreading through the bloodstream to the bone. Septic arthritis (A) would primarily involve the joint space, though it can occur concurrently. Cellulitis (B) is a soft tissue infection without bone involvement. Ewing's sarcoma (D) is a bone tumor that can mimic infection but typically presents with more chronic symptoms and characteristic "onion-skin" periosteal reaction on X-ray. A stress fracture (E) would not present with fever or elevated inflammatory markers.
Question 54
A 4-year-old female presents with a 6-month history of persistent swelling and pain in her left knee, accompanied by morning stiffness that improves throughout the day. She denies any specific trauma. Physical examination reveals a warm, swollen left knee with a limited range of motion, but no systemic signs of infection. Laboratory tests show a mildly elevated ESR and CRP, and negative rheumatoid factor. Radiographs of the knee demonstrate periarticular osteopenia and mild joint space widening.
View Answer & Explanation
Correct Answer: C
Rationale: The chronic nature of the knee swelling and pain (6 months), morning stiffness, and periarticular osteopenia in a young child, without a history of trauma or acute infection, are highly suggestive of juvenile idiopathic arthritis (JIA). Septic arthritis (A) would present with acute, severe pain, fever, and rapid joint destruction. Transient synovitis (B) is usually acute, self-limiting, and typically affects the hip. Legg-Calvé-Perthes disease (D) affects the hip, not typically the knee, and involves avascular necrosis of the femoral head. Osteochondritis dissecans (E) involves a lesion of articular cartilage and subchondral bone, often presenting with mechanical symptoms like locking, and is less likely to cause chronic, diffuse joint swelling and morning stiffness.
Question 55
A 28-year-old male complains of chronic low back pain and stiffness for the past 2 years. The pain is worse in the morning and improves with activity. He also reports intermittent buttock pain. Physical examination reveals limited lumbar spine flexion and extension, and tenderness over the sacroiliac joints. Laboratory tests show an elevated ESR and a positive HLA-B27 allele. Radiographs of the pelvis show bilateral sacroiliitis with erosions and sclerosis.
View Answer & Explanation
Correct Answer: D
Rationale: The patient's age, chronic inflammatory back pain (worse in the morning, improves with activity), limited spinal mobility, sacroiliac joint tenderness, positive HLA-B27, and radiographic evidence of bilateral sacroiliitis are classic features of ankylosing spondylitis. Lumbar disc herniation (A) typically causes radicular pain and does not present with sacroiliitis or morning stiffness improving with activity. Mechanical low back pain (B) is usually exacerbated by activity and relieved by rest. DISH (C) typically affects older individuals and involves flowing ossification along the anterior longitudinal ligament, sparing the sacroiliac joints initially. Psoriatic arthritis (E) can involve the spine and sacroiliac joints but is usually associated with psoriatic skin lesions and peripheral arthritis, which are not mentioned here as primary complaints.
Question 56
A 55-year-old male presents with sudden onset of excruciating pain, swelling, and redness in his right great toe MTP joint. He reports a similar episode in the past that resolved spontaneously. On examination, the joint is hot, swollen, and extremely tender to touch. He has a history of hypertension and is on a diuretic. Serum uric acid level is elevated. Arthrocentesis of the affected joint reveals turbid synovial fluid with numerous negatively birefringent needle-shaped crystals.
View Answer & Explanation
Correct Answer: C
Rationale: The acute onset of severe pain, swelling, and redness in the great toe MTP joint (podagra), elevated serum uric acid, and the presence of negatively birefringent needle-shaped crystals in the synovial fluid are pathognomonic for gout. Septic arthritis (A) would also present acutely but would typically show positive bacterial cultures and white blood cells without specific crystal morphology. Pseudogout (B) involves calcium pyrophosphate crystals, which are positively birefringent and rhomboid-shaped. Cellulitis (D) is a soft tissue infection without joint involvement, and arthrocentesis would not yield crystals. A bunion (E) is a chronic deformity, not an acute inflammatory attack.
Question 57
A 72-year-old male presents with progressive bowing of his left tibia, increasing hat size, and generalized bone pain. He also reports some hearing loss. Physical examination reveals a warm, tender left tibia and a slightly enlarged skull. Laboratory tests show a significantly elevated serum alkaline phosphatase level. Radiographs of the tibia and skull demonstrate cortical thickening, bone enlargement, and a mixed lytic and sclerotic pattern.
View Answer & Explanation
Correct Answer: D
Rationale: The patient's age, symptoms of bone pain, increasing hat size (skull involvement), bowing of long bones, hearing loss, markedly elevated alkaline phosphatase, and characteristic radiographic findings of cortical thickening, bone enlargement, and mixed lytic/sclerotic lesions are classic for Paget's disease of bone (Osteitis Deformans). Osteoporosis (A) is characterized by decreased bone density and increased fracture risk, not bone enlargement or elevated alkaline phosphatase. Osteomalacia (B) involves defective bone mineralization, leading to soft bones, but not typically the radiographic changes seen here. Metastatic bone disease (C) can cause bone pain and lytic/sclerotic lesions but usually does not cause diffuse bone enlargement or such a high alkaline phosphatase without liver involvement. Fibrous dysplasia (E) is a developmental anomaly of bone, typically presenting in younger individuals with "ground-glass" appearance, and is less likely to be widespread with these specific features in an elderly patient.
Question 58
A 16-year-old male presents with a 3-month history of localized pain in his right tibia. The pain is dull, persistent, worse at night, and consistently relieved by over-the-counter NSAIDs. Physical examination reveals localized tenderness over the anterior tibia. Radiographs show a small, well-circumscribed lucent lesion (nidus) approximately 1 cm in diameter, surrounded by a dense sclerotic rim, in the cortical bone of the tibia.
View Answer & Explanation
Correct Answer: C
Rationale: The classic presentation of an osteoid osteoma includes localized bone pain, worse at night, and dramatically relieved by NSAIDs, in an adolescent or young adult. Radiographically, it is characterized by a small lucent nidus (typically <1.5-2 cm) surrounded by a dense sclerotic reaction. Osteoblastoma (A) is histologically similar but larger (>2 cm), less sclerotic, and pain is less responsive to NSAIDs. Enchondroma (B) is a cartilaginous tumor typically found in the medullary cavity of small bones of the hands and feet, usually asymptomatic. Osteosarcoma (D) is a malignant tumor with aggressive features, often a "sunburst" or Codman's triangle appearance, and pain not relieved by NSAIDs. Chronic osteomyelitis (E) would typically have a history of infection, possibly drainage, and different radiographic features.
Question 59
A 25-year-old female presents with a 6-month history of progressive pain and swelling around her left knee. She reports some mechanical symptoms but no specific injury. Physical examination reveals a palpable mass and tenderness over the distal femur. Radiographs show a large, eccentric, purely lytic lesion in the epiphysis and metaphysis of the distal femur, extending to the subchondral bone, with no sclerotic rim. There is cortical thinning and some soft tissue extension.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical picture of a young adult with an eccentric, purely lytic lesion in the epiphysis/metaphysis of a long bone (especially around the knee), extending to the subchondral bone, without a sclerotic rim, is highly characteristic of a giant cell tumor of bone (GCT). Chondroblastoma (A) is also epiphyseal but typically smaller, with a sclerotic rim, and often has calcifications. Aneurysmal bone cyst (B) is expansile, lytic, and often multiloculated, but can occur in any age group and location, and is not typically purely epiphyseal. Unicameral bone cyst (D) is typically metaphyseal, centrally located, and seen in children. Osteosarcoma (E) is malignant, often has a more aggressive appearance with periosteal reaction and osteoid matrix, and is more common in the metaphysis of long bones in adolescents.
Question 60
An 8-year-old male presents with a 2-month history of worsening pain and swelling in his right thigh, accompanied by intermittent fever and weight loss. Physical examination reveals a tender, warm, and firm mass in the mid-diaphysis of the femur. Laboratory tests show elevated ESR and CRP. Radiographs of the femur demonstrate a large lytic lesion in the diaphysis with a characteristic "onion-skin" periosteal reaction.
View Answer & Explanation
Correct Answer: D
Rationale: The patient's age, diaphyseal location, systemic symptoms (fever, weight loss), and the classic "onion-skin" periosteal reaction on radiographs are highly suggestive of Ewing's sarcoma. Osteomyelitis (A) can mimic Ewing's but typically has a more acute onset, and while it can cause periosteal reaction, the "onion-skin" appearance is more characteristic of Ewing's. Osteosarcoma (B) is more common in the metaphysis and typically presents with a "sunburst" periosteal reaction and osteoid matrix. Langerhans cell histiocytosis (C) can cause lytic lesions but usually does not have the prominent "onion-skin" periosteal reaction or the same systemic symptoms. A stress fracture (E) would not present with fever, weight loss, or an "onion-skin" periosteal reaction.
Question 61
A 9-year-old male presents to the emergency department after a minor fall, complaining of mild pain in his left humerus. Radiographs taken to rule out a fracture reveal an incidental, well-defined, centrally located lucent lesion in the proximal metaphysis of the humerus. The lesion appears to thin the cortex and has a "fallen leaf" sign within it, indicating a pathologic fracture.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical scenario of an asymptomatic, centrally located, well-defined lucent metaphyseal lesion in a child, often discovered incidentally after a pathologic fracture (indicated by the "fallen leaf" sign), is classic for a unicameral bone cyst (UBC). Aneurysmal bone cyst (A) is typically expansile, eccentric, and multiloculated. Nonossifying fibroma (B) is usually eccentric, cortical, and has a sclerotic rim, often resolving spontaneously. Fibrous dysplasia (D) has a "ground-glass" appearance and can be expansile, but is not typically centrally located or associated with a "fallen leaf" sign. Enchondroma (E) is a cartilaginous tumor, usually in small bones of hands/feet, and does not typically present with a "fallen leaf" sign.
Question 62
A 68-year-old male presents with chronic low back pain that has recently worsened significantly. He also reports generalized fatigue and unintentional weight loss over the past few months. Radiographs of the lumbar spine show diffuse lytic lesions. Which of the following is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Multiple myeloma is described as the most common primary malignancy of bone, typically affecting patients older than 50, and presenting with pain, malaise, and weight loss. The diffuse lytic lesions are consistent with its presentation. Osteosarcoma, chondrosarcoma, Ewing sarcoma, and fibrosarcoma are less common primary bone malignancies or typically affect different age groups/present differently. Ewing sarcoma typically affects younger patients, and osteosarcoma is the most common primary malignant bone tumor in children and young adults, not the most common primary malignancy of bone overall.
Question 63
A 72-year-old female presents with new onset severe hip pain after a minor fall. She has a history of generalized fatigue and has lost 10 pounds in the last 3 months. Radiographs show a pathologic fracture of the proximal femur. Given the most likely diagnosis, what is the typical age group affected by this condition?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical vignette describes a presentation highly suggestive of multiple myeloma (older patient, fatigue, weight loss, pathologic fracture). The text explicitly states that multiple myeloma "typically affects patients older than 50." Other age groups are not characteristic for this condition.
Question 64
A 65-year-old male presents to the clinic complaining of persistent, dull pain in his thoracic spine that has been present for several months. He denies any specific injury. On physical examination, there are no focal neurological deficits. Given the most common presenting symptom for multiple myeloma, what is this patient's primary complaint?
View Answer & Explanation
Correct Answer: D
Rationale: The text states, "Pain is the most common patient complaint" for multiple myeloma. While peripheral neuropathy, palpable mass, pathologic fracture, and anemia can be associated with myeloma, pain is specifically highlighted as the most common presenting symptom. Peripheral neuropathy is associated with osteosclerotic myeloma, a specific variant, and anemia is a laboratory finding, not a complaint.
Question 65
A 70-year-old female with a known history of multiple myeloma experiences a sudden, sharp increase in her chronic back pain after a minor movement. She now has difficulty bearing weight. What does a sudden increase in pain in a patient with multiple myeloma most commonly indicate?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "A sudden increase in pain may indicate a pathologic fracture." This is a critical clinical sign in patients with myeloma due to the bone-weakening nature of the disease. The other options are either incorrect interpretations of worsening pain or unrelated to a sudden increase in pain.
Question 66
A 62-year-old male presents with a several-month history of generalized weakness, fatigue, and a 15-pound unintentional weight loss. He also reports diffuse bone pain. These systemic symptoms are commonly associated with which primary bone malignancy?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Many patients will also have systemic symptoms such as malaise and weight loss" in the context of multiple myeloma. Osteochondroma, enchondroma, osteoid osteoma, and non-ossifying fibroma are benign bone lesions and typically do not present with systemic symptoms like malaise and weight loss.
Question 67
A 75-year-old female presents with diffuse bone pain and fatigue. Laboratory investigations are initiated. Which of the following findings on serum electrophoresis is highly suggestive of multiple myeloma?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states, "In addition to a monoclonal gammopathy noted on serum electrophoresis, patients are often anemic." This is a hallmark diagnostic feature of multiple myeloma. Polyclonal gammopathy suggests a reactive process, while hypogammaglobulinemia is a deficiency. Elevated CRP is non-specific, and a normal electrophoresis would argue against the diagnosis.
Question 68
A 60-year-old male presents with persistent back pain and generalized weakness. Blood tests reveal a low hemoglobin level. Given the most likely diagnosis of multiple myeloma, what is another common laboratory finding mentioned in the clinical context?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "In addition to a monoclonal gammopathy noted on serum electrophoresis, patients are often anemic." The vignette mentions a low hemoglobin (anemia). Therefore, monoclonal gammopathy is the other common laboratory finding explicitly mentioned. Thrombocytosis, leukocytosis, and elevated alkaline phosphatase are not mentioned as common findings in the provided text.
Question 69
A 58-year-old male with a history of multiple myeloma develops progressive numbness and tingling in his feet and hands. This symptom is most specifically associated with which variant of multiple myeloma?
View Answer & Explanation
Correct Answer: C
Rationale: The text specifically notes, "Patients with osteosclerotic myeloma may develop peripheral neuropathy." This directly links the symptom of peripheral neuropathy (numbness and tingling) to the osteosclerotic variant. The other options are types or presentations of myeloma but are not specifically linked to peripheral neuropathy in the provided text.
Question 70
A 67-year-old male undergoes a biopsy of a lytic lesion in his proximal femur, suspected to be multiple myeloma. During gross examination of the resected specimen, the tumor tissue is described as having a characteristic appearance. What is this appearance?
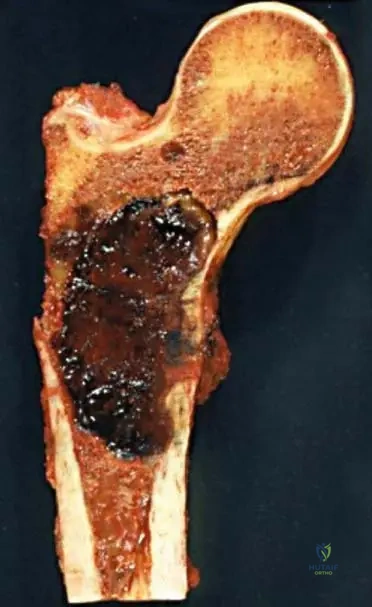
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 8.115, which shows a gross resection of a proximal femur, has the caption: "Note current jelly-appearance to tumor." This is a specific gross pathological description for myeloma. The other descriptions are characteristic of other types of tumors or normal tissue.
Question 71
A 63-year-old female undergoes a bone marrow biopsy for suspected multiple myeloma. Microscopic examination of the biopsy reveals a characteristic cellularity and matrix production pattern. What is the typical description of myeloma lesions on low power photomicrography?
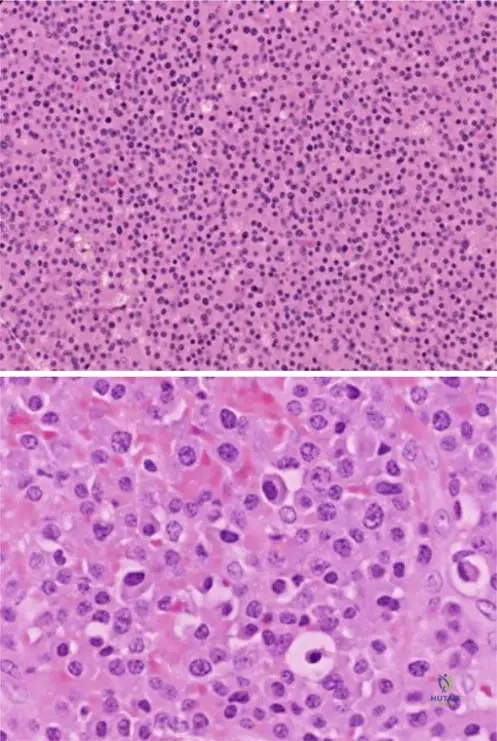
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 8.114 a, b's caption states, "Low power photomicrograph of myeloma (a). Lesions are hypercellular without matrix production." This directly describes the microscopic appearance. The other options contradict this specific histological description.
Question 72
A pathologist examines a high-power photomicrograph of a bone lesion from a 69-year-old male with suspected multiple myeloma. Which of the following cellular features would be characteristic of myeloma cells?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 8.114 a, b's caption states, "Eccentric nuclei and prominent cytoplasm are evident on higher power (b). Myeloma cells are secretory and have well-developed golgi apparatus." This precisely describes the characteristic features of myeloma cells. The other options describe features of different cell types or tumors.
Question 73
A 71-year-old female presents with diffuse back pain. MRI and CT scans of the lumbar spine are performed. The images show widespread involvement of the vertebral bodies. This pattern of involvement on imaging is characteristic of which condition?
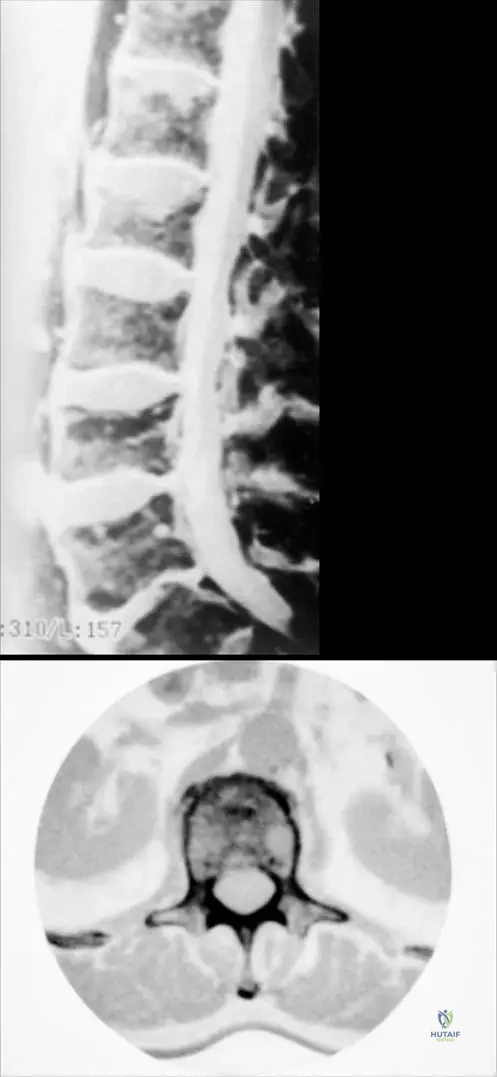
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 8.113 a, b's caption states, "Diffuse involvement of the lumbar spine in a patient with myeloma presented on MR (a) and CT (b)." This directly links the imaging findings of diffuse spinal involvement to multiple myeloma. While other conditions can affect the spine, diffuse involvement as depicted is characteristic of myeloma in this context.
Question 74
A 66-year-old male is diagnosed with multiple myeloma after presenting with bone pain and anemia. From which lineage of cells does this malignancy originate?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states, "Multiple myeloma is a hematopoietic malignancy." This indicates its origin from blood-forming cells, specifically plasma cells. Osteoblastic, chondrocytic, fibroblastic, and epithelial origins are incorrect for multiple myeloma.
Question 75
A 70-year-old female presents with a palpable mass in her humerus, in addition to diffuse bone pain. What does the presence of a palpable mass in a patient with multiple myeloma typically indicate?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "A palpable mass may be present in patients with extraosseous extension." This directly links the presence of a palpable mass to the spread of the tumor beyond the bone. The other options are incorrect interpretations of a palpable mass in this context.
Question 76
A 64-year-old male with a new diagnosis of multiple myeloma undergoes a bone marrow biopsy. The high-power photomicrograph reveals cells with well-developed Golgi apparatus. What is the functional significance of a well-developed Golgi apparatus in myeloma cells?
View Answer & Explanation
Correct Answer: C
Rationale: The caption for Fig. 8.114 a, b states, "Myeloma cells are secretory and have well-developed golgi apparatus." The Golgi apparatus is a key organelle involved in processing and packaging proteins for secretion. Therefore, a well-developed Golgi apparatus indicates a secretory function. The other options are not directly related to the function of the Golgi apparatus in this context.
Question 77
A 55-year-old female presents with persistent bone pain and fatigue. Her initial workup includes a complete blood count, which reveals anemia. What type of malignancy is multiple myeloma classified as?
View Answer & Explanation
Correct Answer: E
Rationale: The text explicitly states, "Multiple myeloma is a hematopoietic malignancy." While it is a type of plasma cell dyscrasia, which can be considered a type of lymphoma in a broader sense, the most precise classification given in the text is "hematopoietic malignancy." Carcinoma and sarcoma are solid tumors of epithelial and mesenchymal origin, respectively. Leukemia primarily involves the bone marrow and peripheral blood, while myeloma primarily involves bone with plasma cell proliferation.
Question 78
A 68-year-old male presents with diffuse bone pain and a recent pathologic fracture of his humerus. His serum protein electrophoresis shows a monoclonal gammopathy. What is the most common primary malignancy of bone?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Multiple myeloma is the most common primarily malignancy of bone." This is a direct factual statement from the provided information. Osteosarcoma is the most common primary malignant bone tumor in children and young adults, but not the most common overall primary malignancy of bone.
Question 79
A 73-year-old female presents with severe, unremitting back pain and new onset weakness in her lower extremities. Imaging reveals diffuse involvement of the lumbar spine with multiple lytic lesions. Given the diagnosis of multiple myeloma, what is the primary characteristic of the bone lesions regarding matrix production?
View Answer & Explanation
Correct Answer: C
Rationale: The caption for Fig. 8.114 a, b states, "Lesions are hypercellular without matrix production." This is a key histological feature of myeloma lesions, explaining their lytic nature. The other options describe matrix production that is not characteristic of multiple myeloma.
Question 80
A 60-year-old male presents with chronic bone pain and fatigue. A complete blood count reveals anemia. What is the typical appearance of the bone involvement on imaging studies such as MRI and CT, as shown in the provided figures?
View Answer & Explanation
Correct Answer: B
Rationale: Fig. 8.113 a, b's caption states, "Diffuse involvement of the lumbar spine in a patient with myeloma presented on MR (a) and CT (b)." This directly describes the typical pattern of bone involvement shown in the images. The other options describe specific radiographic patterns associated with other bone tumors or conditions.
Question 81
A 71-year-old male presents with persistent back pain, malaise, and a recent diagnosis of anemia. Serum protein electrophoresis is performed to evaluate for a specific protein abnormality. What is the primary purpose of serum electrophoresis in the diagnosis of multiple myeloma?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "In addition to a monoclonal gammopathy noted on serum electrophoresis, patients are often anemic." This indicates that serum electrophoresis is used to detect the characteristic monoclonal gammopathy, which is a hallmark of multiple myeloma. While other tests might assess inflammatory markers, red blood cell count, or kidney function, serum electrophoresis specifically identifies the monoclonal protein.
Question 82
A 65-year-old male presents with generalized fatigue and unintentional weight loss over several months, in addition to diffuse back pain. Physical exam is unremarkable except for mild pallor.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states that "Many patients will also have systemic symptoms such as malaise and weight loss." Malaise directly aligns with the patient's reported fatigue. Polyuria can be associated with hypercalcemia, a complication of myeloma, but malaise is explicitly listed as a systemic symptom in the provided text.
Question 83
A 70-year-old male with a known history of osteosclerotic multiple myeloma presents with new onset numbness and tingling in his feet. Physical examination reveals diminished sensation in a stocking-glove distribution.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text specifically mentions, "Patients with osteosclerotic myeloma may develop peripheral neuropathy." The patient's symptoms of numbness and tingling in a stocking-glove distribution are classic for peripheral neuropathy. While spinal cord compression can cause neurological symptoms, peripheral neuropathy is directly linked to osteosclerotic myeloma in the provided information.
Question 84
A 68-year-old female with a history of diffuse bone pain attributed to multiple myeloma reports a sudden, sharp increase in her right hip pain after a minor fall. Radiographs show a lytic lesion in the proximal femur.
View Answer & Explanation
Correct Answer: B
Rationale: The clinical text states, "A sudden increase in pain may indicate a pathologic fracture." The patient's history of a minor fall combined with a sudden increase in pain and a lytic lesion strongly points to a pathologic fracture. While tumor progression is occurring, the acute increase in pain with a minor event is the hallmark of a fracture through weakened bone.
Question 85
A 72-year-old male presents with a several-month history of worsening back pain. On physical examination, a firm, non-tender mass is palpable in the paravertebral region. Imaging reveals diffuse lytic lesions in the spine.
View Answer & Explanation
Correct Answer: B
Rationale: The clinical text indicates, "A palpable mass may be present in patients with extraosseous extension." The presence of a palpable mass in the context of multiple myeloma suggests the tumor has extended beyond the confines of the bone. Lymphadenopathy is not specifically mentioned as a cause for a palpable mass in this context for myeloma.
Question 86
A 60-year-old male presents to his primary care physician complaining of persistent, dull aches throughout his axial skeleton that have been worsening over the past six months. He denies any specific injury.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text explicitly states, "Pain is the most common patient complaint." The patient's presentation of persistent, dull aches throughout the axial skeleton is consistent with this common complaint. Other options are not identified as the most common complaint for multiple myeloma.
Question 87
A 55-year-old female is undergoing evaluation for unexplained anemia and diffuse skeletal pain. Her serum protein electrophoresis shows a monoclonal gammopathy.
View Answer & Explanation
Correct Answer: D
Rationale: The clinical text states that multiple myeloma "typically affects patients older than 50." The patient's age of 55 falls directly into this demographic. While it can occur in older individuals, "older than 50" is the specific age group mentioned.
Question 88
A 63-year-old male is diagnosed with multiple myeloma following a bone marrow biopsy. The biopsy confirms a plasma cell proliferative disorder.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text defines multiple myeloma as a "hematopoietic malignancy." This classification refers to malignancies originating from blood-forming tissues, which includes plasma cells. Mesenchymal refers to connective tissue, which is incorrect for myeloma.
Question 89
A 67-year-old female presents with widespread lytic bone lesions and hypercalcemia. A bone biopsy confirms the presence of malignant plasma cells.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text explicitly states, "Multiple myeloma is the most common primarily malignancy of bone." This means it is the most common cancer that originates within the bone itself. While metastatic disease is the most common malignancy *found in* bone, myeloma is the most common *primary* bone malignancy.
Question 90
A 70-year-old male presents with chronic back pain and fatigue. Initial laboratory workup reveals an elevated total protein level. Further investigation is warranted.
View Answer & Explanation
Correct Answer: B
Rationale: The clinical text notes, "In addition to a monoclonal gammopathy noted on serum electrophoresis, patients are often anemic." A monoclonal gammopathy, characterized by an abnormal proliferation of a single clone of plasma cells producing a single type of immunoglobulin, is a hallmark diagnostic feature of multiple myeloma. Polyclonal gammopathy is associated with chronic inflammation or infection, not myeloma.
Question 91
A 62-year-old female with diffuse bone pain and a history of recurrent infections is being evaluated for multiple myeloma. Her complete blood count shows a hemoglobin of 9.5 g/dL.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states that "patients are often anemic." A hemoglobin level of 9.5 g/dL is indicative of anemia, which is a very common hematologic abnormality in patients with multiple myeloma due to bone marrow infiltration and other factors. Leukocytosis is not a typical finding; patients may have normal or even low white blood cell counts.
Question 92
A bone biopsy is performed on a 68-year-old male with suspected multiple myeloma. The low power photomicrograph of the lesion is provided.

View Answer & Explanation
Correct Answer: C
Rationale: The description for Fig. 8.114 states, "Lesions are hypercellular without matrix production." This is a key histological feature of multiple myeloma, where malignant plasma cells proliferate densely without forming bone matrix. Abundant matrix production is characteristic of osteosarcoma, not myeloma.
Question 93
A 45-year-old male presents to the clinic two weeks after a distal radius fracture treated with cast immobilization. He complains of severe, burning pain in his right hand, disproportionate to the injury. On examination, the hand is swollen, warm, and erythematous with marked stiffness.

View Answer & Explanation
Correct Answer: C
Rationale: The patient's symptoms of disproportionate pain, swelling, warmth, redness, and stiffness in the distal limb following trauma and immobilization are classic for the acute stage of Reflex Sympathetic Dystrophy (RSD), also known as Algodystrophy or Sudeck syndrome. Cellulitis typically lacks the hyperesthesia and disproportionate pain, while compartment syndrome presents with severe pain on passive stretch and neurological deficits. DVT is less common in the upper extremity and would present differently.
Question 94
A 58-year-old female presents with persistent pain, swelling, and stiffness in her left foot, which began after a minor ankle sprain three months ago. Initial radiographs taken shortly after the injury were unremarkable. Current radiographs of the foot are obtained.
View Answer & Explanation
Correct Answer: B
Rationale: In the acute stage of Algodystrophy (RSD), radiographs are initially normal. However, approximately two months later, a characteristic patchy osteoporosis develops in the bones of the affected limb. Joint space narrowing and osteophytes are typical of osteoarthritis, not the early/dystrophic stages of RSD.
Question 95
A 32-year-old patient develops algodystrophy following a crush injury to the hand. The underlying pathophysiology involves a complex interplay of neural and vascular changes.
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that "Disturbance of circulation (precapillary sphincter spasm, opening of arteriovenous shunts, capillary stasis) develops following neurogen stimulus" in the pathophysiology of algodystrophy. This leads to metabolic changes and subsequent osteoporosis.
Question 96
A 28-year-old male presents with severe pain, swelling, and warmth in his right foot after prolonged immobilization for a metatarsal fracture. Clinical suspicion for algodystrophy is high. A bone scan is performed to aid in diagnosis.
View Answer & Explanation
Correct Answer: C
Rationale: In the acute stage of algodystrophy, a three-phase bone scan typically shows increased radioisotope uptake in the affected limb, particularly in the tarsal bones if the foot is involved, due to increased blood flow and bone turnover. This is a sensitive diagnostic finding.
Question 97
A 65-year-old female has a long-standing history of algodystrophy in her left foot, which initially presented with pain and swelling after a minor injury. Over several months, her symptoms have progressed.

View Answer & Explanation
Correct Answer: C
Rationale: The atrophic stage of algodystrophy is characterized by pain extending proximally, atrophy of the skin, subcutaneous tissue, and general soft tissue, along with flexion contractures of the joint. Warm, erythematous skin and marked edema are more characteristic of the acute stage.
Question 98
A 40-year-old patient is diagnosed with algodystrophy following a wrist sprain. The physician discusses various factors that can contribute to the development of this condition.
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that "The inappropriate immobilization after minor injuries and the personality of the patient (psychological changes) are also contributive factors" to algodystrophy. While other diseases like neurological or rheumatologic conditions are mentioned, inappropriate immobilization is a specific and direct factor.
Question 99
A 20-year-old male army recruit presents with insidious onset of pain in his right shin that worsens with marching and improves with rest. He denies any specific traumatic event.
- A) A single, high-impact traumatic event
- B) Cyclic, long-continued or oft-repeated stress
- C) A metabolic bone disorder
- D)
Question 99
A 45-year-old male presents with persistent pain, swelling, and hyperesthesia in his right hand following a minor wrist sprain two months prior. Examination reveals warmth, redness, and marked stiffness of the hand and fingers. Initial radiographs taken at the time of injury were unremarkable. Current radiographs are shown.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of pain, swelling, hyperesthesia, warmth, redness, and stiffness in the distal limb following trauma, along with the development of patchy osteoporosis on radiographs two months later, is characteristic of the acute stage of Algodystrophy, also known as Reflex Sympathetic Dystrophy (RSD) or Sudeck syndrome. Cellulitis and septic arthritis would typically present with more acute signs of infection and often systemic symptoms. Gout and rheumatoid arthritis would have different radiographic patterns and clinical histories, though some symptoms can overlap. The image (Fig. 4.16c) specifically shows patchy osteoporosis characteristic of this stage.
Question 99
A 60-year-old female develops severe pain, swelling, and limited range of motion in her left shoulder, hand, and wrist three months after sustaining a distal radius fracture that required immobilization. She describes her hand as feeling "burning" and appears to have skin atrophy and flexion contractures in her fingers. Which stage of Algodystrophy is most consistent with her current presentation?
View Answer & Explanation
Correct Answer: C
Rationale: The atrophic stage of Algodystrophy is characterized by pain extending proximally on the involved limb, atrophy of the skin, subcutaneous tissue, and general soft tissue, and flexion contractures of the joints. The "hand-shoulder syndrome" is also a known manifestation of upper limb involvement. The acute stage would typically present with warmth, redness, and marked swelling, while the dystrophic stage is transitional. The patient's symptoms of skin atrophy and contractures point to the later, atrophic stage.
Question 99
A 55-year-old male presents with a several-week history of severe, burning pain and swelling in his right foot following a minor ankle sprain. Physical examination reveals a warm, erythematous, and exquisitely tender foot. A bone scan is performed.
View Answer & Explanation
Correct Answer: C
Rationale: In the acute stage of Algodystrophy (RSD), a bone scan typically shows increased radioisotope uptake, particularly in the affected bones, such as the tarsal bones in a foot involvement. This reflects the increased metabolic activity and vascular changes occurring in the affected limb. The image (Fig. 4.18) explicitly demonstrates increased radioisotope uptake in the tarsal bones in the acute stage.
Question 99
A 22-year-old female ballet dancer presents with insidious onset of forefoot pain that worsens with dancing and improves with rest. Physical examination reveals localized tenderness and mild swelling over the dorsum of her left foot. Radiographs are initially unremarkable, but a follow-up MRI is performed.

View Answer & Explanation
Correct Answer: A
Rationale: In the context of a stress fracture, especially in its early stages where radiographs may be normal, MRI is highly sensitive for detecting bone marrow edema and edema in the surrounding soft tissue, which are characteristic findings. The image (Fig. 5.1c) specifically shows edema in the surrounding soft tissue on an MR picture associated with a metatarsal stress fracture. The other options are less likely given the clinical presentation of a stress fracture.
Question 99
A 19-year-old male army recruit presents with progressive pain in his right shin that began after an increase in marching drills. The pain is worse with activity and relieved by rest. Physical examination reveals localized tenderness over the midshaft of the tibia. Radiographs are initially negative, but a follow-up radiograph two weeks later shows a faint hairline crack and early callus formation.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of a young adult unaccustomed to sudden physical activity, with pain increasing with activity and decreasing at rest, localized tenderness, and radiographic evidence of a hairline crack and callus formation, is highly characteristic of a stress fracture. Shin splints typically do not show a fracture line or callus. Osteomyelitis would have systemic symptoms and different radiographic features. Ewings sarcoma is a malignant tumor with distinct imaging characteristics. Compartment syndrome presents with acute pain, paresthesias, and muscle tightness, often not relieved by rest.
Question 99
A 25-year-old male marathon runner complains of persistent pain in his left foot. He has been increasing his training intensity significantly. Physical examination reveals swelling above the second and third metatarsal heads. Radiographs show a new subcapital stress fracture in the third metatarsal bone and an old one in the second, surrounded by extensive callus formation.
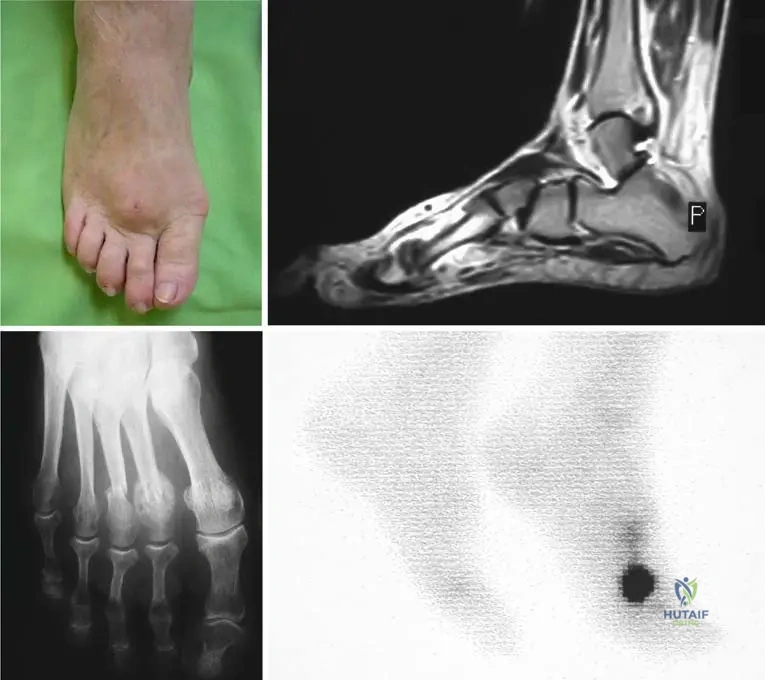
View Answer & Explanation
Correct Answer: C
Rationale: The patient's history of repetitive stress (marathon runner), localized swelling and pain, and radiographic findings of a subcapital fracture with extensive callus formation are classic signs of a stress fracture. The image (Fig. 5.1b) clearly depicts these radiographic findings. Osteoid osteoma is a benign bone tumor with a characteristic nidus and sclerotic rim, not typically presenting with extensive callus from a fracture. Gout would involve inflammatory arthritis. Plantar fasciitis and Morton's neuroma are soft tissue conditions without bone fracture or callus formation.
Question 99
A 30-year-old female athlete presents with a swollen forefoot and pain that has progressively worsened over several weeks. She denies any specific acute injury but has recently increased her training regimen. CT imaging is performed.

View Answer & Explanation
Correct Answer: B
Rationale: In the context of a stress fracture, particularly in an athlete with repetitive stress, massive callus formation can occur around the diaphysis, sometimes mimicking a tumor on imaging. The CT image (Fig. 5.2c) reveals a fractured bone within such callus. Osteosarcoma would have different imaging characteristics and clinical course. Septic arthritis and Charcot arthropathy have distinct clinical presentations and imaging findings. Avascular necrosis would typically affect joint surfaces and not present with massive diaphyseal callus.
Question 99
A 7-year-old boy presents to the emergency department with acute, spontaneous swelling and severe pain in his right knee. His medical history is significant for an inherited bleeding disorder. Physical examination reveals a tense, warm, and tender knee joint with limited range of motion. There is no history of trauma.

View Answer & Explanation
Correct Answer: C
Rationale: The presentation of acute, spontaneous bleeding into a joint (hemarthrosis) in a patient with a known inherited bleeding disorder, especially without trauma, is highly indicative of severe hemophilia. The image (Fig. 6.1) shows acute spontaneous bleeding into the soft tissues and knee joint in a patient with severe hemophilia. Septic arthritis would typically present with fever and elevated inflammatory markers. Juvenile Idiopathic Arthritis has a more chronic course. Traumatic effusion would require a history of trauma. Osgood-Schlatter disease is an apophysitis of the tibial tubercle, not a joint effusion.
Question 99
A 3-year-old male is diagnosed with an inherited bleeding disorder. His blood clotting activity for Factor VIII is measured at 0.5% of normal. Based on this finding, how would his hemophilia be classified?
View Answer & Explanation
Correct Answer: C
Rationale: According to the provided text, severe hemophilia is classified as having less than 1% of clotting factor activity. A Factor VIII activity of 0.5% falls into this category. Mild hemophilia is 5-25%, and moderate is 2-5%. Von Willebrand's disease is a different clotting disorder, and acquired hemophilia is not inherited.
Question 99
A 10-year-old boy with severe hemophilia A experiences recurrent bleeding into his right ankle joint. This joint has become swollen, painful, and has a limited range of motion. What term is used to describe a joint that displays a tendency towards recurrent bleeding in hemophilia?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that "A joint that displays a tendency towards recurrent bleeding is termed a 'target joint.'" This term is crucial in the management and prognosis of hemophilic arthropathy. The image (Fig. 6.2) also refers to hemophilic arthropathy in a target joint.
Question 99
A 15-year-old male with a history of hemophilia presents with chronic pain and stiffness in his elbow. During arthroscopy, the synovium is noted to be hypertrophic and has a characteristic "mahogany brown" appearance.
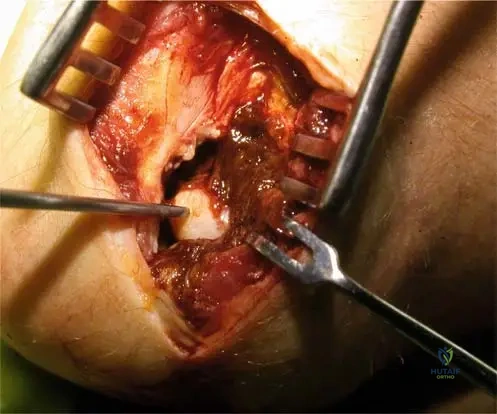
View Answer & Explanation
Correct Answer: C
Rationale: The characteristic "mahogany brown" synovium seen in hemophilic arthropathy is due to hemosiderin deposition, which results from the breakdown of recurrent intra-articular blood. The image (Fig. 6.5) shows this characteristic appearance. Chronic infection would present differently. Gouty tophi are urate crystal deposits. Rheumatoid pannus is an inflammatory granulation tissue, but the specific color is due to hemosiderin in hemophilia. Amyloidosis is a systemic disorder with different synovial findings.
Question 99
A 20-year-old male with severe hemophilia has developed chronic hemophilic synovitis in his right knee. Which of the following is a primary mechanism leading to this chronic synovitis?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "When hemarthroses become frequent and/or intense, the synovium may not be able to reabsorb the blood. To compensate for such reabsorptive deficiency, the synovium will become hypertrophic, resulting in what is called chronic hemophilic synovitis." This is the direct mechanism described. The image (Fig. 6.6a) illustrates chronic hemophilic synovitis. The other options are not the primary mechanism for hemophilic synovitis.
Question 99
A 12-year-old boy with hemophilia presents with chronic ankle pain and swelling. Radiographs of his ankles are obtained.
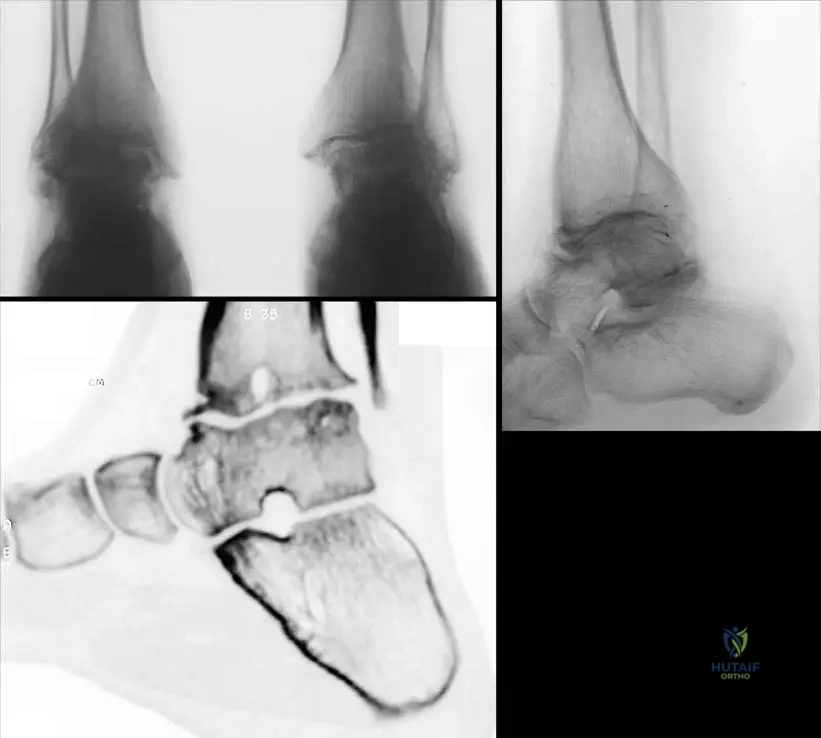
View Answer & Explanation
Correct Answer: B
Rationale: Hemophilic arthritis, especially in young patients, is characterized by significant joint destruction. The text and image (Fig. 6.7c) describe and show "juxta-articular cysts, destroyed articular surfaces, and diffuse osteoporosis" as key features best evaluated on reconstructive CT pictures, which are also visible on plain radiographs (Fig. 6.7a, b). Joint space narrowing is an indirect sign of cartilage destruction. The other options describe features not typical of hemophilic arthropathy or are incorrect.
Question 99
An adult patient with long-standing severe hemophilia presents with significant functional limitations. Physical examination reveals fixed deformities of his knees and ankles. Which of the following is a common late-stage manifestation of hemophilic arthritis?

View Answer & Explanation
Correct Answer: B
Rationale: The text states that "Late stage of hemophilic arthritis in adult patients: axial deformities, secondary contractures of the knees, hips and equinus of the ankles are frequently seen." These contractures significantly compromise joint function and potential for joint replacement. The image (Fig. 6.8a, b) illustrates these late-stage contractures. Acute inflammatory synovitis is an earlier manifestation. Spontaneous fracture healing is unrelated. Joint pain typically persists, and hyperlaxity is not a feature; rather, contractures lead to stiffness.
Question 99
A 40-year-old male with hemophilia has chronic knee pain and stiffness. Radiographs show significant joint space narrowing, bony erosions, and subchondral cysts. What is the primary reason that recurrent joint bleeding in hemophilia leads to a "vicious cycle" of inflammation and further bleeding?
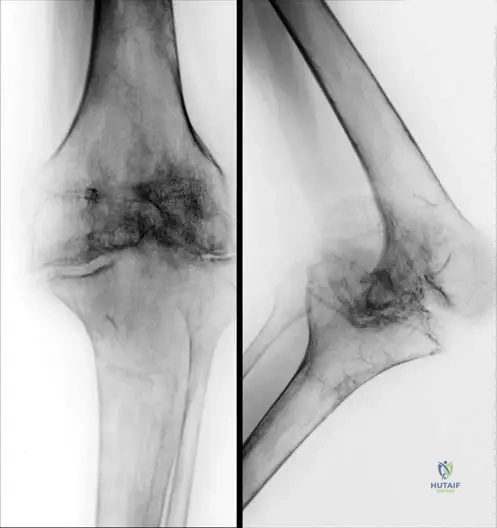
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly describes this vicious cycle: "If a joint bleeding is not adequately treated, it tends to recur. The inflamed, swollen synovium bleeds more easily than the normal synovium and causes further swelling and inflammation. This vicious cycle must be broken to prevent the development of arthritis." The image (Fig. 6.9a, b) shows radiological signs of knee arthritis in a hemophilic patient, emphasizing the need to break this cycle. The other options are incorrect mechanisms.
Question 99
A young hemophilic male undergoes knee arthroscopy for chronic pain and limited motion. The surgeon notes destroyed cartilage surfaces and a pannus creeping over the joint surfaces. Histological examination of the synovium would most likely reveal:

View Answer & Explanation
Correct Answer: B
Rationale: The text describes the pathology of hemophilic arthritis: "Synovium shows marked vascular hyperplasia, hemosiderin deposits. Hemosiderin-stained pannus begins to creep over the joint surfaces." This is a direct consequence of recurrent bleeding and the body's response to blood products within the joint. The image (Fig. 6.10) shows destroyed cartilage surfaces and describes these synovial findings. The other options describe different pathologies.
Question 99
A 28-year-old female presents with chronic, diffuse pain in her left foot, which is worse with activity and improves with rest. She is a recreational runner who recently increased her mileage. Physical examination reveals diffuse swelling and tenderness across the midfoot. A bone scan shows a "hot spot" in the tarsal bones. Which of the following conditions is the most likely diagnosis?
View Answer & Explanation
Correct Answer: B
Rationale: The history of increased activity, pain worse with activity and better with rest, and a "hot spot" on bone scan are classic indicators of a stress fracture. While Algodystrophy can also show increased uptake on bone scan (Fig. 4.18), its clinical presentation typically involves more pronounced vasomotor changes (warmth, redness), hyperesthesia, and often follows a specific trauma or immobilization, rather than just increased activity. The diffuse swelling and tenderness across the midfoot in a runner points more strongly to a stress fracture in the tarsals or metatarsals. Septic arthritis would have more acute inflammatory signs and often systemic symptoms. Gout would have a more acute, episodic presentation. Plantar fasciitis is a soft tissue condition and would not typically cause a "hot spot" on bone scan in the bone itself.
Question 99
A 35-year-old male presents with persistent right thigh pain that began after an intense cycling regimen. Initial radiographs are unremarkable. A CT scan is performed.
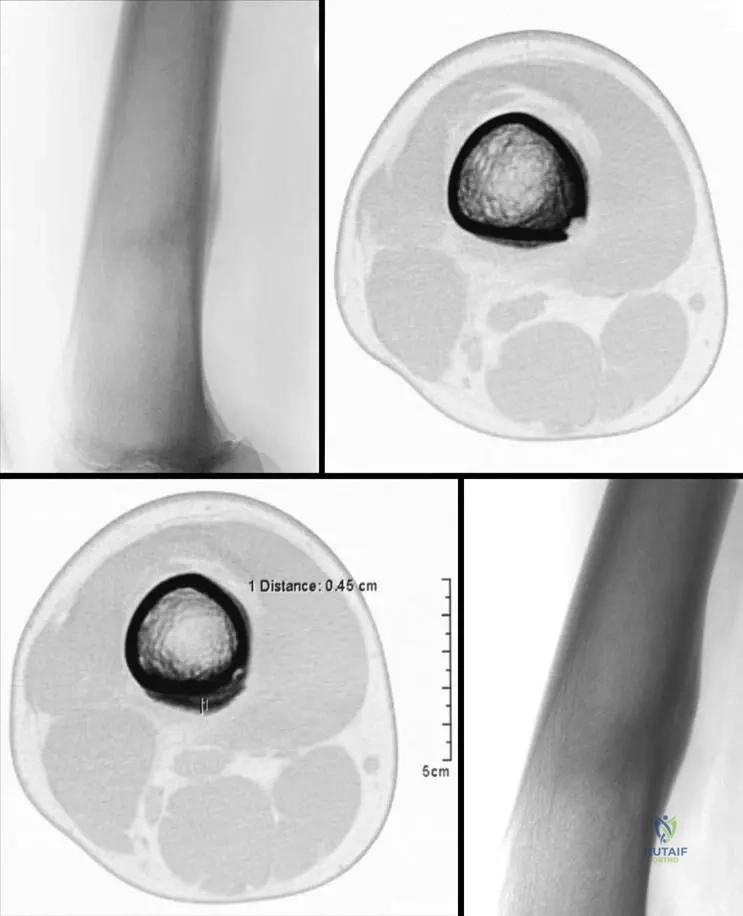
View Answer & Explanation
Correct Answer: A
Rationale: In the early stage of a stress fracture, especially in the femur, the infraction may not be recognizable on plain radiographs. CT scans can reveal an atypical fracture
Question 100
A 45-year-old male presents with persistent pain, swelling, and hyperesthesia in his right hand following a minor wrist sprain two months prior. Examination reveals warmth, redness, and marked stiffness of the hand and fingers. Initial radiographs taken at the time of injury were unremarkable. Current radiographs are shown.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of pain, swelling, hyperesthesia, warmth, redness, and stiffness in the distal limb following trauma, along with the development of patchy osteoporosis on radiographs two months later, is characteristic of the acute stage of Algodystrophy, also known as Reflex Sympathetic Dystrophy (RSD) or Sudeck syndrome. Cellulitis and septic arthritis would typically present with more acute signs of infection and often systemic symptoms. Gout and rheumatoid arthritis would have different radiographic patterns and clinical histories, though some symptoms can overlap. The image (Fig. 4.16c) specifically shows patchy osteoporosis characteristic of this stage.
You Might Also Like