Master ABOS Orthopedic Pathology Review: Fibrous Dysplasia, PVNS, & RA | Part 19

Key Takeaway
ABOS Orthopedic Pathology Review covers key musculoskeletal conditions like fibrous dysplasia, pigmented villonodular synovitis (PVNS), and rheumatoid arthritis (RA). It details their clinical presentation, diagnostic imaging (MRI, X-ray), pathology (hemosiderin, pannus, nodules), and management strategies, crucial for board exam preparation.
Question 1
A 40-year-old woman with a known history of polyostotic fibrous dysplasia is found to have multiple intramuscular myxomas in her thigh and calf muscles during a routine follow-up MRI.
View Answer & Explanation
Correct Answer: D
Rationale: Mazabraud's syndrome is a rare condition characterized by the co-occurrence of fibrous dysplasia (typically polyostotic) and multiple intramuscular myxomas. McCune-Albright syndrome involves fibrous dysplasia, café-au-lait spots, and endocrine dysfunction. Ollier's disease and Maffucci's syndrome are characterized by multiple enchondromas, with Maffucci's also including soft tissue hemangiomas. Paget's disease is a distinct disorder of abnormal bone remodeling.
Question 2
A 25-year-old man has an incidentally discovered, asymptomatic, small monostotic fibrous dysplasia lesion in his distal tibia on an X-ray performed for an ankle sprain. The lesion shows no signs of aggressive features.
View Answer & Explanation
Correct Answer: C
Rationale: Asymptomatic, stable monostotic fibrous dysplasia lesions, especially in non-weight-bearing bones or with minimal risk of fracture, are typically managed with observation and serial radiographic follow-up. Surgical intervention (curettage, grafting, or fixation) is reserved for symptomatic lesions, those at high risk of fracture, or those causing significant deformity. Bisphosphonates are for symptomatic disease. Radiation therapy is generally contraindicated due to the risk of malignant transformation.
Question 3
A 50-year-old woman with a known history of polyostotic fibrous dysplasia for over 30 years presents with new, severe, localized pain and rapid enlargement of a lesion in her humerus. Radiographs show cortical destruction and a soft tissue mass.
View Answer & Explanation
Correct Answer: D
Rationale: The development of new, severe pain, rapid lesion enlargement, cortical destruction, or a soft tissue mass in a patient with known fibrous dysplasia are red flags for malignant transformation. In such cases, a biopsy is mandatory to rule out malignancy, most commonly osteosarcoma. Routine follow-up, confirmation of diagnosis, or evaluation of bisphosphonate response would not be indicated given these alarming symptoms.
Question 4
A 10-year-old boy with polyostotic fibrous dysplasia presents with a progressive limp and noticeable bowing of his right thigh. Radiographs confirm an expansile lesion in the proximal femur with a characteristic severe varus deformity.
View Answer & Explanation
Correct Answer: D
Rationale: The "shepherd's crook deformity" is a classic and severe varus deformity of the proximal femur, characterized by marked bowing and thinning of the cortex, often leading to pathologic fractures and significant functional impairment. It is highly characteristic of fibrous dysplasia affecting the proximal femur. Genu varum/valgum refer to knee deformities, coxa valga is an increased neck-shaft angle, and Madelung's deformity affects the wrist.
Question 5
A 5-year-old child presents to the emergency department with a pathologic fracture of the humerus after a minor fall. Radiographs show an expansile, lytic lesion with a ground-glass appearance. The parents report no prior symptoms.
View Answer & Explanation
Correct Answer: B
Rationale: Fibrous dysplasia typically presents clinically in childhood and adolescence, often with pain, swelling, deformity, or pathologic fractures. While monostotic forms can be discovered incidentally in adulthood, symptomatic polyostotic disease or lesions causing significant complications usually manifest during the growth years. The GNAS1 mutation occurs post-zygotically, and the disease progresses with skeletal growth.
Question 6
A 14-year-old girl with extensive craniofacial fibrous dysplasia involving the sphenoid bone and optic canal develops progressive visual field deficits and decreased visual acuity in her right eye over several months.
View Answer & Explanation
Correct Answer: D
Rationale: Progressive optic nerve compression in craniofacial fibrous dysplasia is a surgical emergency. The expanding bone can directly impinge on the optic nerve, leading to irreversible vision loss if not promptly decompressed. Observation is inappropriate for progressive neurological deficits. Bisphosphonates may help with bone pain and stability but do not relieve acute compression. Radiation therapy is generally contraindicated due to the risk of malignant transformation. Systemic corticosteroids may offer temporary relief from edema but are not a definitive solution for mechanical compression.
Question 7
A 35-year-old female presents with generalized bone pain, multiple lytic bone lesions on skeletal survey, elevated serum calcium, low serum phosphate, and elevated parathyroid hormone levels. A biopsy of one lesion shows features consistent with a "brown tumor."
View Answer & Explanation
Correct Answer: D
Rationale: Secondary hyperparathyroidism can cause multiple lytic bone lesions (brown tumors) that may mimic fibrous dysplasia radiographically. The key differentiating factors are the characteristic biochemical abnormalities (elevated calcium, low phosphate, elevated PTH) and the presence of brown tumors on biopsy, which are histologically distinct from fibrous dysplasia. Paget's disease has characteristic radiographic features (bone enlargement, cortical thickening, coarsened trabeculae) and elevated alkaline phosphatase but normal calcium/phosphate. Osteogenesis imperfecta is a genetic collagen disorder. Rickets is a vitamin D deficiency. Multiple myeloma presents with punched-out lytic lesions and monoclonal gammopathy.
Question 8
A 40-year-old male presents with chronic, intermittent left knee swelling and pain for 2 years. He reports occasional locking and a feeling of fullness. Physical examination reveals a warm, swollen knee with a mild effusion. Radiographs show mild joint space narrowing.
View Answer & Explanation
Correct Answer: C
Rationale: Pigmented villonodular synovitis (PVNS) most commonly affects young adults (30s through 50s) and typically presents as monoarticular swelling, often in the knee or hip. Option C aligns perfectly with these demographic and clinical characteristics. Main Distractor: A) A 75-year-old female with polyarticular joint pain. This option describes an older patient with polyarticular involvement, which is inconsistent with the typical presentation of PVNS.
Question 9
A 35-year-old female presents with a 6-month history of recurrent left knee swelling and pain. She reports episodes of the knee feeling "full" and occasionally stiff. On examination, there is a moderate effusion. Arthrocentesis yields a dark, serosanguinous fluid.
View Answer & Explanation
Correct Answer: C
Rationale: PVNS is characterized by monoarticular swelling, recurrent effusions, and hemarthrosis, which is consistent with the serosanguinous fluid described. The clinical presentation often involves intermittent flares of pain and loss of motion. Main Distractor: B) Polyarticular involvement with symmetrical joint swelling. PVNS is typically a monoarticular condition, making polyarticular involvement an incorrect characteristic.
Question 10
A 38-year-old male presents with chronic left knee pain and swelling. Initial radiographs are obtained.
View Answer & Explanation
Correct Answer: B
Rationale: In the early stages of PVNS, radiographs often show periarticular lucencies and considerable effusions (soft tissue swelling). The clinical photograph (Fig. 10.5) shows visible swelling of the knee. Main Distractor: A) Extensive subchondral bone cysts and joint space narrowing. While these can occur in long-standing PVNS due to destructive changes and secondary degeneration, periarticular lucencies and soft tissue swelling are more characteristic early findings.
Question 11
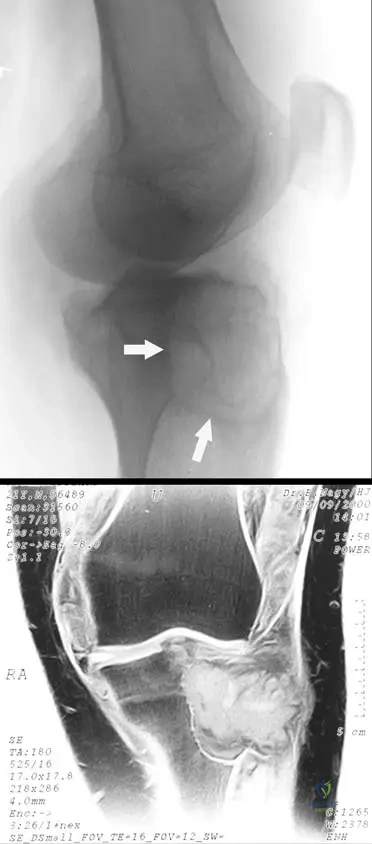
A 42-year-old female presents with long-standing, progressive left knee pain and swelling. She has a history of recurrent effusions. A lateral radiograph of her knee is shown.
View Answer & Explanation
Correct Answer: C
Rationale: The provided text states that "At long duration, the destructive proliferation of synovial-like tissue can affect the adjacent bone," leading to erosive changes as seen in Fig. 10.6a. Main Distractor: B) Secondary osteoarthritis due to cartilage loss. While secondary degenerative changes may be present, the primary cause of the extensive erosive changes in PVNS is the direct destructive proliferation of the synovial tissue into the bone, not solely cartilage loss.
Question 12
A 32-year-old male presents with chronic right hip pain and recurrent effusions. An MRI is performed.
View Answer & Explanation
Correct Answer: C
Rationale: The caption for Fig. 10.6b explicitly states, "PVNS characteristically has low signal characteristics because of the hemosiderin present in the lesion." Hemosiderin, a breakdown product of hemoglobin, causes magnetic susceptibility effects that lead to low signal intensity on T1- and T2-weighted MR images. Main Distractor: A) Fat. Fat typically exhibits high signal intensity on T1-weighted MR images, which is opposite to the characteristic finding in PVNS.
Question 13
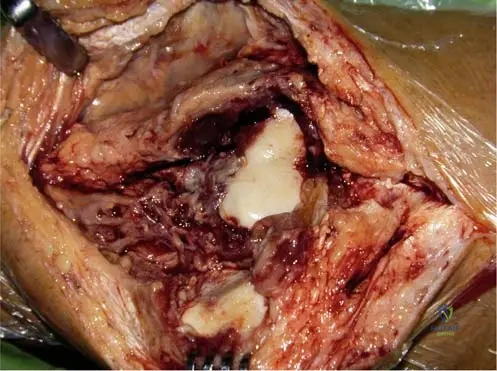
A 48-year-old female undergoes arthroscopy for chronic knee pain and swelling. During the procedure, the surgeon notes a diffuse proliferation of synovial tissue.
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "Grossly, the tissue is reddish brown in appearance," and that lesions may be "diffuse (villous) or localized (nodular)." Fig. 10.8 further demonstrates the intra-articular extent of the diffuse form. Main Distractor: E) Smooth, hypertrophied synovium. While synovium is hypertrophied, the specific reddish-brown color and villous/nodular morphology are characteristic of PVNS, differentiating it from other causes of synovial hypertrophy.
Question 14
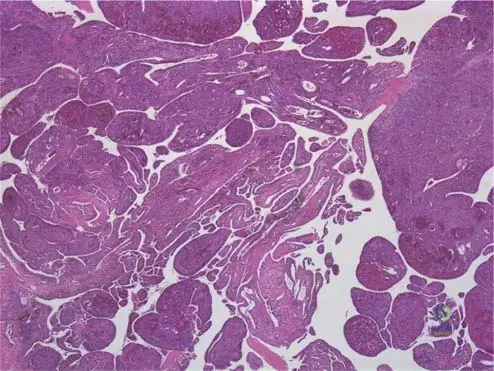
A synovial biopsy is obtained from a 39-year-old patient with chronic knee effusions and periarticular erosions.
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Lipidor hemosiderin-filled macrophages are present" in the microscopic examination of PVNS. Fig. 10.7 shows the villous masses, which microscopically contain these cells. Main Distractor: A) Lymphocytes and plasma cells. While some inflammatory cells may be present, the defining characteristic of PVNS microscopically is the presence of lipid- and hemosiderin-filled macrophages, not primarily lymphocytes and plasma cells, which are more indicative of chronic inflammatory arthritides.
Question 15
A 30-year-old male is diagnosed with PVNS of the ankle after presenting with chronic swelling and pain. His family asks about the cause of the condition.
View Answer & Explanation
Correct Answer: C
Rationale: The text describes PVNS as an "idiopathic condition" and refers to the "destructive proliferation of synovial-like tissue," indicating it is a proliferative disorder of the synovium of unknown cause. Main Distractor: E) A malignant neoplastic process. PVNS is a benign proliferative disorder, not a malignant neoplasm like synovial sarcoma.
Question 16
A 45-year-old female presents with chronic monoarticular swelling and pain. Imaging reveals features consistent with PVNS.
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states that PVNS "most commonly affects the knee or hip." The ankle may also be involved, but the knee is the most frequent site. Main Distractor: A) Shoulder. While PVNS can occur in other joints, the shoulder is not listed as one of the most commonly affected joints.
Question 17
A 37-year-old male is diagnosed with a diffuse proliferative synovial lesion in his knee. The pathologist's report mentions "diffuse-type giant cell tumor."
View Answer & Explanation
Correct Answer: C
Rationale: The text lists "diffuse-type giant cell tumor" and "pigmented villonodular tenosynovitis" as synonyms for pigmented villonodular synovitis. Main Distractor: E) Synovial sarcoma. Synovial sarcoma is a malignant tumor, whereas PVNS is a benign proliferative condition, despite some shared histological features like giant cells in certain forms.
Question 18
A 38-year-old female presents with a 2-year history of intermittent right hip pain, swelling, and stiffness. Radiographs show periarticular lucencies. Given the likely diagnosis of pigmented villonodular synovitis, which of the following joints is MOST commonly affected by this condition?
View Answer & Explanation
Correct Answer: C
Rationale: Pigmented villonodular synovitis (PVNS) most commonly affects the knee, followed by the hip and ankle. While other joints can be involved, the knee is the predominant site. The ankle is also mentioned as a possible site, but less common than the knee.
Question 19
A 42-year-old male undergoes a synovial biopsy for chronic knee effusion and pain. Histopathological examination reveals villous fingerlike and rounded masses underlying the synovial membrane. Which of the following cellular components is a characteristic finding in this condition?
View Answer & Explanation
Correct Answer: C
Rationale: Histologically, PVNS is characterized by the presence of lipidor hemosiderin-filled macrophages, which contribute to the pigmented appearance. Occasional multinucleated giant cells are also seen. Neutrophils are more indicative of septic arthritis, and plasma cells are not a primary feature.
Question 20
During an arthrotomy for a 35-year-old female with diffuse knee swelling and recurrent hemarthrosis, the surgeon observes the intra-articular tissue. What is the characteristic gross appearance of the synovial tissue in pigmented villonodular synovitis?
View Answer & Explanation
Correct Answer: C
Rationale: Grossly, the synovial tissue in PVNS is typically reddish-brown due to hemosiderin deposition, with some areas appearing more yellow due to fat content. This distinct coloration is a hallmark of the condition. Pale or white appearances are not characteristic.
Question 21
A 50-year-old male presents with chronic left knee pain and swelling. Radiographs reveal extensive erosive changes in the proximal tibia, as shown in the image. This finding is highly suggestive of long-standing pigmented villonodular synovitis. What is the underlying mechanism for these erosive changes?
View Answer & Explanation
Correct Answer: C
Rationale: In PVNS, the destructive proliferation of synovial-like tissue directly invades and erodes adjacent bone, leading to the characteristic periarticular lucencies and erosive changes seen on radiographs, especially in long-standing cases. It is not primarily an infection, ischemia, or autoimmune process.
Question 22
A 30-year-old female presents with recurrent right knee effusions. Arthrocentesis is performed. Given a suspected diagnosis of pigmented villonodular synovitis, what is the expected appearance of the joint aspirate?
View Answer & Explanation
Correct Answer: D
Rationale: Joint aspirates in PVNS can range from clear to bloody in appearance, often reflecting recurrent hemarthrosis. Turbid or purulent fluid suggests infection, while milky fluid is seen in gout. Clear, straw-colored fluid is typical of non-inflammatory effusions.
Question 23
A 25-year-old male presents with monoarticular swelling and pain in his left ankle. Radiographs show subtle periarticular lucencies. The clinical picture is consistent with pigmented villonodular synovitis. What is the typical age range for patients diagnosed with this condition?
View Answer & Explanation
Correct Answer: C
Rationale: PVNS most commonly affects young adults, typically in their 30s through 50s. While it can occur outside this range, this age group represents the highest incidence. It is not primarily a pediatric or elderly disease.
Question 24
A 40-year-old female is diagnosed with pigmented villonodular synovitis of the knee after presenting with chronic pain and swelling. When discussing the nature of the disease with the patient, what is the current understanding of its etiology?
View Answer & Explanation
Correct Answer: C
Rationale: Pigmented villonodular synovitis is currently considered an idiopathic condition, meaning its cause is unknown. While some theories exist, it is not definitively linked to autoimmune, infectious, or traumatic origins as a primary cause. Genetic factors are being investigated but not established as the primary etiology.
Question 25
A 33-year-old male presents with a several-month history of intermittent left knee swelling and pain, often resolving partially before recurring. He reports episodes where the joint feels warm and full. Which of the following clinical features is highly characteristic of pigmented villonodular synovitis?
View Answer & Explanation
Correct Answer: C
Rationale: Recurrent effusions and hemarthrosis with intermittent flares of pain are characteristic clinical presentations of PVNS. The presence of blood in the joint fluid is due to the friable, vascular nature of the synovial proliferation. Bilateral involvement, acute onset with fever, prolonged morning stiffness, or systemic symptoms are not typical of PVNS.
Question 26
A 48-year-old female undergoes an MRI for chronic knee pain and swelling, revealing findings consistent with pigmented villonodular synovitis. The T1-weighted image shows characteristic low signal intensity within the synovial tissue. What substance is primarily responsible for this specific MRI signal characteristic?
View Answer & Explanation
Correct Answer: C
Rationale: The low signal characteristics seen on T1-weighted MRI in PVNS are due to the paramagnetic effects of hemosiderin, which is abundantly deposited within the synovial tissue. This is a crucial diagnostic clue. Other substances like crystals or synovial fluid do not typically cause this specific low signal on T1-weighted images.
Question 27
A 37-year-old male is diagnosed with pigmented villonodular synovitis of the knee. When reviewing his medical records, the orthopaedic surgeon notes that the condition may also be referred to by other names. Which of the following is a recognized synonym for pigmented villonodular synovitis?
View Answer & Explanation
Correct Answer: C
Rationale: Pigmented villonodular synovitis (PVNS) is also known by synonyms such as diffuse-type giant cell tumor or pigmented villonodular tenosynovitis. These terms reflect the histological features and the proliferative nature of the lesion. The other options are distinct arthritic conditions.
Question 28
A 41-year-old female presents with chronic pain and swelling in her right knee, without involvement of any other joints. Physical examination reveals a warm, swollen knee with a large effusion. This monoarticular presentation is typical for pigmented villonodular synovitis. What does "monoarticular" imply about the disease's typical involvement?
View Answer & Explanation
Correct Answer: B
Rationale: PVNS is characteristically a monoarticular condition, meaning it affects a single joint. While very rare cases of polyarticular involvement have been reported, the vast majority of presentations are confined to one joint, most commonly the knee, hip, or ankle. The other options describe different patterns of joint involvement.
Question 29
During an arthroscopic synovectomy for a 39-year-old patient with PVNS, the surgeon notes the characteristic reddish-brown appearance of the synovial tissue. This coloration is a direct result of the accumulation of which specific type of cell?
View Answer & Explanation
Correct Answer: C
Rationale: The reddish-brown color of the synovial tissue in PVNS is due to the abundant accumulation of hemosiderin, which is iron-containing pigment derived from hemoglobin, primarily within macrophages. These hemosiderin-filled macrophages are a hallmark of the disease. The other cell types do not primarily contribute to this characteristic pigmentation.
Question 30
A 46-year-old female undergoes a biopsy of her knee synovium due to chronic swelling and pain. The low-power micrograph reveals villous fingerlike and rounded masses underlying the synovial membrane. What does the term "villous" specifically refer to in the context of pigmented villonodular synovitis?
View Answer & Explanation
Correct Answer: C
Rationale: The term "villous" in PVNS refers to the characteristic fingerlike projections and folds of the synovial membrane, which represent the proliferative nature of the disease. This contrasts with a smooth lining or discrete encapsulated nodules (which would be "nodular" form). The image clearly shows these villous structures.
Question 31
A 52-year-old male presents with long-standing left knee pain, swelling, and progressive loss of motion. Radiographs show significant periarticular lucencies and early degenerative changes. The destructive nature of pigmented villonodular synovitis can lead to which of the following long-term complications?
View Answer & Explanation
Correct Answer: C
Rationale: The destructive proliferation of synovial-like tissue in PVNS can lead to significant cartilage damage and bone erosion over time, ultimately resulting in secondary degenerative changes and arthritis. While PVNS is locally aggressive, malignant transformation is extremely rare, and systemic complications like amyloidosis or pathological fractures of long bones are not typical features.
Question 32
A 36-year-old female presents with chronic, intermittent right knee swelling and pain. Arthrocentesis yields bloody fluid. Radiographs show periarticular lucencies. Given these findings, which of the following conditions is most important to differentiate from pigmented villonodular synovitis due to similar presentations?
View Answer & Explanation
Correct Answer: C
Rationale: The presence of recurrent hemarthrosis (bloody joint fluid) is a key feature of PVNS. Conditions that also cause recurrent hemarthrosis, such as hemophilia or other coagulopathies, must be considered in the differential diagnosis. While meniscal tears can cause effusions, they typically don't cause recurrent frank hemarthrosis. Rheumatoid and septic arthritis have different clinical and aspirate profiles.
Question 33
A 44-year-old male presents with chronic left knee pain and swelling. MRI findings are consistent with pigmented villonodular synovitis. Which primary tissue type is affected by the proliferative process in PVNS?
View Answer & Explanation
Correct Answer: C
Rationale: Pigmented villonodular synovitis is a condition characterized by the destructive proliferation of the synovial membrane. While it can secondarily affect articular cartilage, subchondral bone, and other intra-articular structures through invasion, the primary tissue involved in the disease process is the synovium itself.
Question 34
A 32-year-old female has a 5-year history of recurrent right knee effusions and pain, initially managed conservatively. Recent radiographs show significant joint space narrowing and subchondral cysts. These findings, in the context of PVNS, represent which of the following?
View Answer & Explanation
Correct Answer: C
Rationale: In long-standing PVNS, the chronic destructive proliferation of the synovium leads to cartilage damage and bone erosion, which manifests radiographically as joint space narrowing, subchondral cysts, and osteophyte formation, consistent with secondary degenerative arthritis. These are not early manifestations or signs of resolution, nor typically malignant transformation.
Question 35
A 40-year-old male is diagnosed with pigmented villonodular synovitis of the knee. The pathology report describes the lesion as having extensive intra-articular involvement with villous proliferation. This description indicates which form of PVNS?
View Answer & Explanation
Correct Answer: B
Rationale: The text states that "Lesions may be diffuse (villous) or localized (nodular)." Extensive intra-articular involvement with villous proliferation directly corresponds to the diffuse form of PVNS. The localized form would typically present as a discrete nodule. Extra-articular, tenosynovial, and intraosseous forms are distinct presentations not described by this specific vignette.
Question 36
A 32-year-old male presents with a 6-month history of progressive right knee pain, swelling, and stiffness. He reports intermittent locking sensations and occasional "giving way." Physical examination reveals a large, boggy effusion with mild warmth and limited range of motion. Radiographs show joint space narrowing and subchondral cysts, but no osteophytes. An MRI is ordered.
View Answer & Explanation
Correct Answer: B
Rationale: Pigmented Villonodular Synovitis (PVNS) is characterized by hemosiderin deposition within the synovium. Hemosiderin contains iron, which causes magnetic susceptibility artifacts, leading to characteristic low signal intensity on both T1- and T2-weighted MRI sequences. This finding is highly suggestive of PVNS. The main distractor, option A, describes findings that might be seen with hemorrhage (high T1, variable T2 depending on age of blood), but not the chronic hemosiderin deposition characteristic of PVNS.
Question 37
A 45-year-old female undergoes arthroscopic synovectomy for chronic, diffuse knee pain and swelling. Histopathological examination of the resected synovial tissue is performed. Which of the following is the most characteristic histological finding for Pigmented Villonodular Synovitis (PVNS)?
View Answer & Explanation
Correct Answer: C
Rationale: The classic histological triad for Pigmented Villonodular Synovitis (PVNS) includes synovial hyperplasia (villonodular proliferation), abundant hemosiderin deposition (giving the characteristic brown color), and the presence of multinucleated giant cells. Lipid-laden macrophages are also commonly seen. The main distractor, option D, describes synovial chondromatosis, a different synovial proliferative disorder characterized by cartilaginous metaplasia and loose bodies.
Question 38
A 38-year-old male presents with a 9-month history of insidious onset of monoarticular joint pain and swelling. He denies any specific trauma or systemic symptoms. Given the suspected diagnosis of Pigmented Villonodular Synovitis (PVNS), which joint is most commonly affected?
View Answer & Explanation
Correct Answer: D
Rationale: The knee is by far the most commonly affected joint in Pigmented Villonodular Synovitis (PVNS), accounting for approximately 80% of cases. The hip is the second most common, followed by the ankle, shoulder, and elbow. The main distractor, option A (Hip), is the second most common site but significantly less frequent than the knee.
Question 39
A 28-year-old female presents with chronic pain and swelling in her left wrist. Radiographs are unremarkable. An MRI reveals a well-circumscribed, lobulated mass within the flexor tendon sheath, demonstrating low signal intensity on T1 and T2 sequences. This finding is consistent with the localized form of Pigmented Villonodular Synovitis (PVNS). What is the most appropriate term for this extra-articular variant?
View Answer & Explanation
Correct Answer: C
Rationale: The localized, extra-articular form of PVNS, particularly when affecting tendon sheaths, is commonly referred to as a Giant Cell Tumor of Tendon Sheath (GCTTS). Histologically, GCTTS is identical to PVNS, differing primarily in its gross presentation (localized nodule vs. diffuse synovial proliferation). The main distractor, option B (Synovial sarcoma), is a malignant tumor that can mimic GCTTS clinically but has distinct histological and genetic features, and a much worse prognosis.
Question 40
A 30-year-old male is diagnosed with localized Pigmented Villonodular Synovitis (PVNS) of the knee after an MRI and diagnostic arthroscopy. The lesion is small and well-defined. He is symptomatic with pain and intermittent swelling. What is the most appropriate initial treatment?
View Answer & Explanation
Correct Answer: B
Rationale: For localized PVNS, arthroscopic excision (or local resection for extra-articular forms) is the treatment of choice. It is less invasive than open synovectomy and typically curative for well-defined, localized lesions. The main distractor, option A (Open total synovectomy), is generally reserved for diffuse PVNS or recurrent localized disease that cannot be adequately addressed arthroscopically.
Question 41
A 50-year-old female presents with diffuse Pigmented Villonodular Synovitis (PVNS) of the knee, confirmed by biopsy. She has undergone two previous arthroscopic synovectomies, but her symptoms of pain, swelling, and limited range of motion have recurred rapidly. Radiographs show early degenerative changes. What is the most appropriate next step in management?
View Answer & Explanation
Correct Answer: B
Rationale: For diffuse PVNS, especially recurrent cases after arthroscopic attempts, open total synovectomy is often necessary to achieve a more complete resection of the diseased synovium. Adjuvant radiation therapy (either external beam or intra-articular radioisotope) is frequently considered in diffuse or recurrent cases to reduce the high risk of recurrence. The main distractor, option D (Total knee arthroplasty), would be considered for end-stage joint destruction with significant arthropathy, but a complete synovectomy should be attempted first to control the disease and prevent recurrence around the prosthesis.
Question 42
A 35-year-old male with diffuse Pigmented Villonodular Synovitis (PVNS) of the knee has undergone a complete open synovectomy. Given the high recurrence rate associated with diffuse disease, what adjuvant therapy is most commonly considered to reduce the risk of recurrence?
View Answer & Explanation
Correct Answer: C
Rationale: Adjuvant radiation therapy, either external beam or intra-articular radioisotope synovectomy, is commonly used after surgical synovectomy for diffuse PVNS, particularly in recurrent cases or those with incomplete resection, to reduce the high risk of local recurrence. The main distractor, option A (Intra-articular corticosteroid injections), provides only symptomatic relief and does not address the underlying proliferative nature of PVNS or reduce recurrence rates.
Question 43
A 40-year-old female presents with chronic knee pain and recurrent hemarthrosis. Arthrocentesis yields bloody fluid. An MRI shows synovial proliferation with hemosiderin deposition. Which of the following conditions is the most important differential diagnosis to consider, given the presentation?
View Answer & Explanation
Correct Answer: C
Rationale: Hemophilia and other coagulopathies can cause recurrent hemarthrosis, leading to synovial hypertrophy and hemosiderin deposition, which can mimic PVNS both clinically and on imaging. A thorough patient history and coagulation studies are crucial to differentiate these conditions. The main distractor, option A (Rheumatoid arthritis), typically presents with inflammatory synovitis, but recurrent hemarthrosis and extensive hemosiderin deposition are not characteristic features.
Question 44
A 33-year-old male is diagnosed with Pigmented Villonodular Synovitis (PVNS). He asks about the underlying cause of his condition. What is the current understanding of the pathogenesis of PVNS?
View Answer & Explanation
Correct Answer: C
Rationale: Current evidence suggests that PVNS is a benign neoplastic process rather than purely inflammatory. This is supported by the identification of clonal chromosomal abnormalities, most notably a translocation t(1;2)(p13;q37) leading to overexpression of colony-stimulating factor 1 (CSF1), which attracts CSF1R-expressing macrophages that constitute the bulk of the tumor. The main distractor, option A (autoimmune inflammatory disorder), is incorrect as PVNS does not fit the criteria for an autoimmune disease, although inflammation is a secondary feature.
Question 45
A 48-year-old female undergoes complete open synovectomy for diffuse Pigmented Villonodular Synovitis (PVNS) of the hip. She asks about the likelihood of the disease returning. What is the approximate recurrence rate for diffuse PVNS after surgical synovectomy?
View Answer & Explanation
Correct Answer: C
Rationale: The recurrence rate for diffuse PVNS after surgical synovectomy is significant, typically ranging from 30% to 50%, and can be even higher in some series, especially for large joints like the hip or knee. This high recurrence rate often necessitates adjuvant therapy. Localized PVNS has a much lower recurrence rate (typically <10%). The main distractor, option B (10-20%), is too low for diffuse PVNS, which is known for its aggressive recurrence potential.
Question 46
A 37-year-old male presents with chronic knee pain and swelling. An MRI confirms diffuse Pigmented Villonodular Synovitis (PVNS) with significant synovial hypertrophy and early cartilage erosion. He is not a candidate for a total knee arthroplasty due to his age and activity level. Which of the following medical therapies is an emerging treatment option for recurrent or unresectable diffuse PVNS?
View Answer & Explanation
Correct Answer: C
Rationale: Given the understanding of PVNS pathogenesis involving CSF1 overexpression and subsequent recruitment of CSF1R-expressing macrophages, CSF1R inhibitors (e.g., pexidartinib) represent an emerging targeted medical therapy for symptomatic, recurrent, or unresectable diffuse PVNS. These agents aim to reduce the tumor burden by inhibiting the growth and survival of the macrophage-like cells that constitute the bulk of the lesion. The main distractor, option A (TNF-alpha inhibitors), are used for inflammatory arthritides like rheumatoid arthritis and are not primary treatments for PVNS.
Question 47
A 62-year-old female with a long history of diffuse Pigmented Villonodular Synovitis (PVNS) of the knee presents with severe, debilitating pain and end-stage degenerative changes on radiographs, including significant joint space narrowing and subchondral bone loss. She has undergone multiple synovectomies in the past. What is the most appropriate definitive treatment for her condition?
View Answer & Explanation
Correct Answer: C
Rationale: For patients with end-stage arthropathy due to diffuse PVNS, total joint arthroplasty (TJA) combined with a thorough synovectomy is the definitive treatment. The synovectomy is crucial to remove as much diseased tissue as possible to minimize recurrence around the implant. The main distractor, option A (Repeat open synovectomy), would not address the severe degenerative changes and bone loss, which are the primary source of her current debilitating pain.
Question 48
During an arthroscopy for chronic knee pain, a surgeon observes a proliferative, reddish-brown synovial lining with villous and nodular formations. Biopsies are taken. Based on this gross appearance, what is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The description of a "proliferative, reddish-brown synovial lining with villous and nodular formations" is pathognomonic for Pigmented Villonodular Synovitis (PVNS). The reddish-brown color is due to hemosiderin deposition, and the villous and nodular appearance reflects the synovial hypertrophy. The main distractor, option B (Synovial chondromatosis), would typically present with cartilaginous loose bodies and a more grayish-white synovial appearance, not reddish-brown villonodular proliferation.
Question 49
A 25-year-old female presents with chronic, progressive swelling and pain in her right ankle. Radiographs show joint space narrowing and multiple subchondral erosions, but no osteophytes. An MRI confirms diffuse synovial proliferation with low signal intensity on T1 and T2 sequences. Which of the following is a characteristic radiographic finding often seen in PVNS that helps differentiate it from typical osteoarthritis?
View Answer & Explanation
Correct Answer: D
Rationale: A characteristic radiographic finding in PVNS, especially in later stages, is the presence of bone erosions (often "cup-like" or "scalloped") that can occur even with relatively preserved joint space, which is atypical for osteoarthritis where joint space narrowing precedes or accompanies erosions. The erosions are caused by direct pressure from the proliferating synovium. The main distractor, option A (Extensive osteophyte formation), is a hallmark of osteoarthritis, which is typically absent or minimal in PVNS until very late stages of secondary degeneration.
Question 50
A 30-year-old male is diagnosed with diffuse Pigmented Villonodular Synovitis (PVNS) of the knee. He is considering adjuvant external beam radiation therapy after surgical synovectomy to reduce recurrence. What is the most significant long-term complication associated with radiation therapy in this setting?
View Answer & Explanation
Correct Answer: C
Rationale: While rare, the most serious long-term complication of external beam radiation therapy is the development of a secondary malignancy, specifically radiation-induced sarcoma. This risk, though low, must be weighed against the high recurrence rate of diffuse PVNS. Other complications like skin changes and joint stiffness are more common but less severe. The main distractor, option B (Joint stiffness), is a common side effect of radiation and surgery, but it is not as severe or life-threatening as a radiation-induced sarcoma.
Question 51
Question 51
A 32-year-old male presents with a 6-month history of progressive right knee pain, swelling, and intermittent locking. He denies any specific trauma. Physical examination reveals a warm, boggy effusion and limited range of motion. Radiographs show a joint effusion but no significant degenerative changes. An MRI is ordered.
View Answer & Explanation
Correct Answer: C
Rationale: The knee is the most commonly affected joint in pigmented villonodular synovitis (PVNS), accounting for approximately 80% of cases. While PVNS can occur in any synovial joint, the knee is overwhelmingly the most frequent site of presentation. The hip is the second most common, but significantly less frequent than the knee. The main distractor, A) Hip, is incorrect because while the hip is the second most common joint affected, the knee is by far the most common.
Question 51
A 45-year-old female undergoes arthroscopic synovectomy for chronic knee pain and swelling. Histopathological examination of the synovial tissue is performed. The pathologist notes characteristic findings consistent with pigmented villonodular synovitis (PVNS).
View Answer & Explanation
Correct Answer: C
Rationale: The characteristic histological features of PVNS include synovial hyperplasia (proliferation of synovial lining cells), abundant hemosiderin deposition (from recurrent hemorrhage), and the presence of lipid-laden macrophages and multinucleated giant cells. These findings are pathognomonic for PVNS. The main distractor, A) Lymphocytic infiltration and pannus formation, is characteristic of rheumatoid arthritis, not PVNS.
Question 51
A 38-year-old male presents with chronic, progressive right knee pain and swelling. An MRI of the knee is performed to evaluate the extent of synovial involvement and aid in diagnosis. The radiologist identifies specific signal characteristics indicative of pigmented villonodular synovitis (PVNS).
View Answer & Explanation
Correct Answer: B
Rationale: The most characteristic MRI finding in PVNS is low signal intensity on both T1- and T2-weighted images within the synovium due to the paramagnetic effect of hemosiderin deposition. This "blooming" artifact on gradient echo sequences is highly suggestive of PVNS. The main distractor, A) High signal intensity on T2-weighted images with bone marrow edema, is a non-specific finding that can be seen in various inflammatory or traumatic conditions, but not characteristic of the hemosiderin in PVNS.
Question 51
A 25-year-old male with a history of hemophilia presents with recurrent knee swelling and pain. An MRI shows diffuse synovial proliferation and hemosiderin deposition. Given his medical history and imaging findings, the differential diagnosis includes pigmented villonodular synovitis (PVNS).
View Answer & Explanation
Correct Answer: E
Rationale: Hemophilic arthropathy is a critical differential diagnosis for PVNS, especially when considering recurrent hemarthrosis and hemosiderin deposition. Both conditions can present with chronic joint swelling, pain, and synovial changes with iron deposition. The patient's history of hemophilia makes this a particularly relevant consideration. The main distractor, D) Synovial chondromatosis, also involves synovial proliferation and can cause mechanical symptoms, but it is characterized by cartilaginous loose bodies and calcifications, and typically lacks the extensive hemosiderin deposition seen in PVNS or hemophilic arthropathy.
Question 51
A 29-year-old female presents with intermittent knee pain and a palpable, mobile mass in the suprapatellar pouch. MRI reveals a well-circumscribed, localized nodule within the synovium consistent with localized pigmented villonodular synovitis (PVNS). The patient has no significant joint effusion or diffuse synovial involvement.
View Answer & Explanation
Correct Answer: B
Rationale: For localized PVNS, arthroscopic excision of the nodule is the preferred initial treatment. This approach is minimally invasive, allows for complete removal of the lesion, and typically results in a low recurrence rate. The main distractor, A) Open total synovectomy, is an overly aggressive approach for localized disease and is typically reserved for diffuse PVNS.
Question 51
A 50-year-old male is diagnosed with diffuse pigmented villonodular synovitis (PVNS) of the knee after presenting with chronic pain, swelling, and progressive joint destruction. MRI confirms extensive synovial involvement throughout the joint.
View Answer & Explanation
Correct Answer: B
Rationale: For diffuse PVNS, the primary treatment is surgical synovectomy to remove as much of the affected synovium as possible. Open total synovectomy, or a combined arthroscopic and open approach, is often necessary to achieve adequate debridement and reduce recurrence rates, especially in cases with extensive involvement. The main distractor, A) Arthroscopic partial synovectomy, is generally insufficient for diffuse disease due to the difficulty in achieving complete removal of all affected synovium, leading to higher recurrence rates.
Question 51
A 35-year-old patient undergoes an open total synovectomy for diffuse pigmented villonodular synovitis (PVNS) of the knee. Despite a seemingly complete resection, the patient is counseled about the possibility of recurrence.
View Answer & Explanation
Correct Answer: D
Rationale: The recurrence rate for diffuse PVNS after surgical synovectomy is significant, typically ranging from 30% to 50%, and can be even higher in some series, particularly if resection is incomplete or if the disease is highly aggressive. This high recurrence rate often necessitates adjuvant therapies. The main distractor, B) 10-20%, is too low for diffuse PVNS, although it might be more representative of localized forms.
Question 51
A 48-year-old patient with diffuse pigmented villonodular synovitis (PVNS) of the knee has undergone two previous synovectomies, with recurrence noted on subsequent MRI. The orthopedic oncologist is considering adjuvant therapy to reduce the risk of further recurrence.
View Answer & Explanation
Correct Answer: C
Rationale: External beam radiation therapy (EBRT) is the most commonly used and effective adjuvant therapy for diffuse PVNS, particularly in cases of recurrent disease or when complete surgical resection is not feasible. It aims to reduce the proliferative activity of the synovial cells and decrease recurrence rates. The main distractor, B) Systemic methotrexate, is a disease-modifying antirheumatic drug (DMARD) used for autoimmune conditions like rheumatoid arthritis, but it is not a standard or effective treatment for PVNS.
Question 51
A 30-year-old patient is diagnosed with pigmented villonodular synovitis (PVNS) of the ankle. The patient asks about the underlying cause of this condition. While the exact etiology is still being researched, current understanding points towards a specific mechanism.
View Answer & Explanation
Correct Answer: C
Rationale: PVNS is now widely considered a benign neoplastic process rather than a purely inflammatory one. Genetic studies have identified specific chromosomal translocations, most notably t(1;2)(p13;q37), leading to overexpression of colony-stimulating factor 1 (CSF1). This overexpression attracts CSF1R-expressing macrophages, which contribute to the characteristic synovial proliferation and hemosiderin deposition. The main distractor, A) An autoimmune inflammatory process, was a historical theory but is not supported by current genetic and molecular evidence.
Question 51
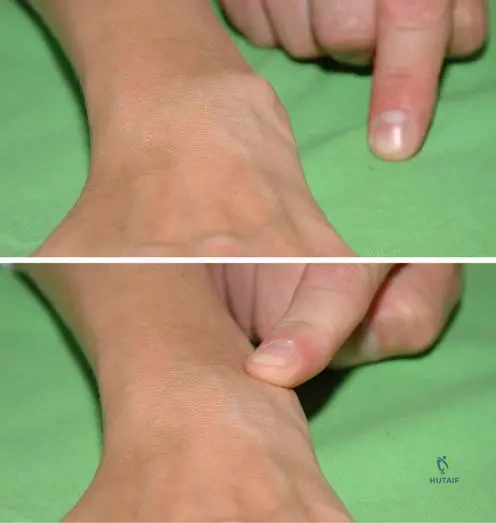
A 40-year-old female presents with a slowly growing, painless mass on the volar aspect of her finger. Excisional biopsy reveals a lesion histologically identical to localized pigmented villonodular synovitis (PVNS).
View Answer & Explanation
Correct Answer: C
Rationale: The most common extra-articular location for PVNS is within tendon sheaths, where it is known as a giant cell tumor of the tendon sheath (GCTTS). GCTTS is essentially a localized form of PVNS occurring outside of a joint capsule, most frequently affecting the fingers and hands. The main distractor, B) Bone, is incorrect as PVNS primarily affects synovial tissue, not bone, although it can cause secondary bone erosions.
Question 51
A patient is diagnosed with pigmented villonodular synovitis (PVNS) after presenting with chronic joint pain and swelling. Understanding the typical demographic profile can aid in early suspicion.
View Answer & Explanation
Correct Answer: C
Rationale: PVNS most commonly affects young to middle-aged adults, typically between the ages of 20 and 50 years. While it can occur at any age, this demographic represents the peak incidence. The main distractor, D) Elderly population (over 65 years), is incorrect as PVNS is less common in this age group, where degenerative conditions are more prevalent.
Question 51
During an arthroscopic procedure for chronic knee pain and effusion, the surgeon observes the synovial lining. The findings are highly suggestive of pigmented villonodular synovitis (PVNS).
View Answer & Explanation
Correct Answer: C
Rationale: The gross appearance of synovium in PVNS is characteristic: it is typically hypertrophied, forming villi or nodules, and has a distinctive brown, reddish-brown, or yellowish-brown discoloration due to extensive hemosiderin deposition. The main distractor, B) Red, inflamed, and edematous synovium with fibrinous exudates, is more characteristic of acute inflammatory arthritis or septic arthritis.
Question 51
A 55-year-old patient has a long history of untreated diffuse pigmented villonodular synovitis (PVNS) in the knee. Over time, the patient experiences increasing pain, stiffness, and functional limitations.
View Answer & Explanation
Correct Answer: C
Rationale: If left untreated, diffuse PVNS can lead to progressive erosion of articular cartilage and subchondral bone, resulting in severe joint destruction and secondary osteoarthritis. This is a major long-term complication that often necessitates joint replacement. The main distractor, A) Malignant transformation to sarcoma, is extremely rare and not considered a typical complication of PVNS, which is a benign condition.
Question 51
A 42-year-old female presents with chronic left knee pain and recurrent effusions. Physical examination reveals a boggy synovium. An MRI is ordered to evaluate the joint.
View Answer & Explanation
Correct Answer: C
Rationale: MRI is the imaging modality of choice for PVNS. It is highly effective in demonstrating the characteristic low signal intensity of hemosiderin on T1 and T2 sequences, as well as the extent of synovial proliferation and involvement (localized vs. diffuse), and any associated bone erosions. This information is crucial for diagnosis and surgical planning. The main distractor, B) It provides a definitive histological diagnosis without the need for biopsy, is incorrect. While MRI is highly suggestive, a definitive diagnosis of PVNS still requires histopathological confirmation via biopsy.
Question 51
A 37-year-old male has recurrent diffuse pigmented villonodular synovitis (PVNS) of the knee, despite multiple synovectomies and adjuvant radiation therapy. His orthopedic oncologist is considering novel targeted medical therapies.
View Answer & Explanation
Correct Answer: D
Rationale: Given the understanding of PVNS as a CSF1-driven neoplastic process, CSF1R inhibitors (e.g., pexidartinib) represent a promising targeted medical therapy for refractory or unresectable diffuse PVNS. These drugs block the CSF1 receptor, thereby inhibiting the proliferation and survival of the macrophages that contribute to the disease. The main distractor, C) TNF-alpha inhibitors, are used in inflammatory arthropathies like rheumatoid arthritis and are not effective for PVNS.
Question 51
A 28-year-old female is diagnosed with localized pigmented villonodular synovitis (PVNS) in her knee, presenting as a single nodule. Her friend, a 40-year-old male, has diffuse PVNS in his knee. They discuss their prognoses.
View Answer & Explanation
Correct Answer: C
Rationale: Localized PVNS generally has a much better prognosis than diffuse PVNS. After complete arthroscopic excision, the recurrence rate for localized disease is low (typically less than 10-15%), whereas diffuse PVNS has a high recurrence rate (30-50% or more) even after extensive synovectomy. The main distractor, B) Diffuse PVNS is more easily treated with arthroscopic surgery, is incorrect. Diffuse PVNS often requires extensive open or combined open/arthroscopic synovectomy due to its widespread nature, making complete resection challenging.
Question 51
During an arthroscopic examination of a 33-year-old patient's knee, the surgeon observes a thickened, brownish, and nodular synovial lining with prominent villi. There are no loose bodies or significant cartilage erosions noted at this stage.
View Answer & Explanation
Correct Answer: E
Rationale: The description of a thickened, brownish, nodular, and villous synovial lining is pathognomonic for pigmented villonodular synovitis (PVNS). The brown discoloration is due to hemosiderin deposition. The main distractor, D) Synovial chondromatosis, would typically present with cartilaginous loose bodies within the joint, which are not described in the vignette.
Question 51
A 40-year-old male presents with chronic knee pain and swelling.
Question 52
A 32-year-old male presents with a 6-month history of progressive right knee pain, swelling, and intermittent locking. He denies any specific trauma. Physical examination reveals a warm, boggy effusion and limited range of motion. Radiographs show a joint effusion but no significant degenerative changes. An MRI is ordered.
View Answer & Explanation
Correct Answer: C
Rationale: The knee is the most commonly affected joint in pigmented villonodular synovitis (PVNS), accounting for approximately 80% of cases. While PVNS can occur in any synovial joint, the knee is overwhelmingly the most frequent site of presentation. The hip is the second most common, but significantly less frequent than the knee. The main distractor, A) Hip, is incorrect because while the hip is the second most common joint affected, the knee is by far the most common.
Question 53
A 45-year-old female undergoes arthroscopic synovectomy for chronic knee pain and swelling. Histopathological examination of the synovial tissue is performed. The pathologist notes characteristic findings consistent with pigmented villonodular synovitis (PVNS).
View Answer & Explanation
Correct Answer: C
Rationale: The characteristic histological features of PVNS include synovial hyperplasia (proliferation of synovial lining cells), abundant hemosiderin deposition (from recurrent hemorrhage), and the presence of lipid-laden macrophages and multinucleated giant cells. These findings are pathognomonic for PVNS. The main distractor, A) Lymphocytic infiltration and pannus formation, is characteristic of rheumatoid arthritis, not PVNS.
Question 54
A 38-year-old male presents with chronic, progressive right knee pain and swelling. An MRI of the knee is performed to evaluate the extent of synovial involvement and aid in diagnosis. The radiologist identifies specific signal characteristics indicative of pigmented villonodular synovitis (PVNS).
View Answer & Explanation
Correct Answer: B
Rationale: The most characteristic MRI finding in PVNS is low signal intensity on both T1- and T2-weighted images within the synovium due to the paramagnetic effect of hemosiderin deposition. This "blooming" artifact on gradient echo sequences is highly suggestive of PVNS. The main distractor, A) High signal intensity on T2-weighted images with bone marrow edema, is a non-specific finding that can be seen in various inflammatory or traumatic conditions, but not characteristic of the hemosiderin in PVNS.
Question 55
A 25-year-old male with a history of hemophilia presents with recurrent knee swelling and pain. An MRI shows diffuse synovial proliferation and hemosiderin deposition. Given his medical history and imaging findings, the differential diagnosis includes pigmented villonodular synovitis (PVNS).
View Answer & Explanation
Correct Answer: E
Rationale: Hemophilic arthropathy is a critical differential diagnosis for PVNS, especially when considering recurrent hemarthrosis and hemosiderin deposition. Both conditions can present with chronic joint swelling, pain, and synovial changes with iron deposition. The patient's history of hemophilia makes this a particularly relevant consideration. The main distractor, D) Synovial chondromatosis, also involves synovial proliferation and can cause mechanical symptoms, but it is characterized by cartilaginous loose bodies and calcifications, and typically lacks the extensive hemosiderin deposition seen in PVNS or hemophilic arthropathy.
Question 56
A 29-year-old female presents with intermittent knee pain and a palpable, mobile mass in the suprapatellar pouch. MRI reveals a well-circumscribed, localized nodule within the synovium consistent with localized pigmented villonodular synovitis (PVNS). The patient has no significant joint effusion or diffuse synovial involvement.
View Answer & Explanation
Correct Answer: B
Rationale: For localized PVNS, arthroscopic excision of the nodule is the preferred initial treatment. This approach is minimally invasive, allows for complete removal of the lesion, and typically results in a low recurrence rate. The main distractor, A) Open total synovectomy, is an overly aggressive approach for localized disease and is typically reserved for diffuse PVNS.
Question 57
A 50-year-old male is diagnosed with diffuse pigmented villonodular synovitis (PVNS) of the knee after presenting with chronic pain, swelling, and progressive joint destruction. MRI confirms extensive synovial involvement throughout the joint.
View Answer & Explanation
Correct Answer: B
Rationale: For diffuse PVNS, the primary treatment is surgical synovectomy to remove as much of the affected synovium as possible. Open total synovectomy, or a combined arthroscopic and open approach, is often necessary to achieve adequate debridement and reduce recurrence rates, especially in cases with extensive involvement. The main distractor, A) Arthroscopic partial synovectomy, is generally insufficient for diffuse disease due to the difficulty in achieving complete removal of all affected synovium, leading to higher recurrence rates.
Question 58
A 35-year-old patient undergoes an open total synovectomy for diffuse pigmented villonodular synovitis (PVNS) of the knee. Despite a seemingly complete resection, the patient is counseled about the possibility of recurrence.
View Answer & Explanation
Correct Answer: D
Rationale: The recurrence rate for diffuse PVNS after surgical synovectomy is significant, typically ranging from 30% to 50%, and can be even higher in some series, particularly if resection is incomplete or if the disease is highly aggressive. This high recurrence rate often necessitates adjuvant therapies. The main distractor, B) 10-20%, is too low for diffuse PVNS, although it might be more representative of localized forms.
Question 59
A 48-year-old patient with diffuse pigmented villonodular synovitis (PVNS) of the knee has undergone two previous synovectomies, with recurrence noted on subsequent MRI. The orthopedic oncologist is considering adjuvant therapy to reduce the risk of further recurrence.
View Answer & Explanation
Correct Answer: C
Rationale: External beam radiation therapy (EBRT) is the most commonly used and effective adjuvant therapy for diffuse PVNS, particularly in cases of recurrent disease or when complete surgical resection is not feasible. It aims to reduce the proliferative activity of the synovial cells and decrease recurrence rates. The main distractor, B) Systemic methotrexate, is a disease-modifying antirheumatic drug (DMARD) used for autoimmune conditions like rheumatoid arthritis, but it is not a standard or effective treatment for PVNS.
Question 60
A 30-year-old patient is diagnosed with pigmented villonodular synovitis (PVNS) of the ankle. The patient asks about the underlying cause of this condition. While the exact etiology is still being researched, current understanding points towards a specific mechanism.
View Answer & Explanation
Correct Answer: C
Rationale: PVNS is now widely considered a benign neoplastic process rather than a purely inflammatory one. Genetic studies have identified specific chromosomal translocations, most notably t(1;2)(p13;q37), leading to overexpression of colony-stimulating factor 1 (CSF1). This overexpression attracts CSF1R-expressing macrophages, which contribute to the characteristic synovial proliferation and hemosiderin deposition. The main distractor, A) An autoimmune inflammatory process, was a historical theory but is not supported by current genetic and molecular evidence.
Question 61
A 40-year-old female presents with a slowly growing, painless mass on the volar aspect of her finger. Excisional biopsy reveals a lesion histologically identical to localized pigmented villonodular synovitis (PVNS).
View Answer & Explanation
Correct Answer: C
Rationale: The most common extra-articular location for PVNS is within tendon sheaths, where it is known as a giant cell tumor of the tendon sheath (GCTTS). GCTTS is essentially a localized form of PVNS occurring outside of a joint capsule, most frequently affecting the fingers and hands. The main distractor, B) Bone, is incorrect as PVNS primarily affects synovial tissue, not bone, although it can cause secondary bone erosions.
Question 62
A patient is diagnosed with pigmented villonodular synovitis (PVNS) after presenting with chronic joint pain and swelling. Understanding the typical demographic profile can aid in early suspicion.
View Answer & Explanation
Correct Answer: C
Rationale: PVNS most commonly affects young to middle-aged adults, typically between the ages of 20 and 50 years. While it can occur at any age, this demographic represents the peak incidence. The main distractor, D) Elderly population (over 65 years), is incorrect as PVNS is less common in this age group, where degenerative conditions are more prevalent.
Question 63
During an arthroscopic procedure for chronic knee pain and effusion, the surgeon observes the synovial lining. The findings are highly suggestive of pigmented villonodular synovitis (PVNS).
View Answer & Explanation
Correct Answer: C
Rationale: The gross appearance of synovium in PVNS is characteristic: it is typically hypertrophied, forming villi or nodules, and has a distinctive brown, reddish-brown, or yellowish-brown discoloration due to extensive hemosiderin deposition. The main distractor, B) Red, inflamed, and edematous synovium with fibrinous exudates, is more characteristic of acute inflammatory arthritis or septic arthritis.
Question 64
A 55-year-old patient has a long history of untreated diffuse pigmented villonodular synovitis (PVNS) in the knee. Over time, the patient experiences increasing pain, stiffness, and functional limitations.
View Answer & Explanation
Correct Answer: C
Rationale: If left untreated, diffuse PVNS can lead to progressive erosion of articular cartilage and subchondral bone, resulting in severe joint destruction and secondary osteoarthritis. This is a major long-term complication that often necessitates joint replacement. The main distractor, A) Malignant transformation to sarcoma, is extremely rare and not considered a typical complication of PVNS, which is a benign condition.
Question 65
A 42-year-old female presents with chronic left knee pain and recurrent effusions. Physical examination reveals a boggy synovium. An MRI is ordered to evaluate the joint.
View Answer & Explanation
Correct Answer: C
Rationale: MRI is the imaging modality of choice for PVNS. It is highly effective in demonstrating the characteristic low signal intensity of hemosiderin on T1 and T2 sequences, as well as the extent of synovial proliferation and involvement (localized vs. diffuse), and any associated bone erosions. This information is crucial for diagnosis and surgical planning. The main distractor, B) It provides a definitive histological diagnosis without the need for biopsy, is incorrect. While MRI is highly suggestive, a definitive diagnosis of PVNS still requires histopathological confirmation via biopsy.
Question 66
A 37-year-old male has recurrent diffuse pigmented villonodular synovitis (PVNS) of the knee, despite multiple synovectomies and adjuvant radiation therapy. His orthopedic oncologist is considering novel targeted medical therapies.
View Answer & Explanation
Correct Answer: D
Rationale: Given the understanding of PVNS as a CSF1-driven neoplastic process, CSF1R inhibitors (e.g., pexidartinib) represent a promising targeted medical therapy for refractory or unresectable diffuse PVNS. These drugs block the CSF1 receptor, thereby inhibiting the proliferation and survival of the macrophages that contribute to the disease. The main distractor, C) TNF-alpha inhibitors, are used in inflammatory arthropathies like rheumatoid arthritis and are not effective for PVNS.
Question 67
A 28-year-old female is diagnosed with localized pigmented villonodular synovitis (PVNS) in her knee, presenting as a single nodule. Her friend, a 40-year-old male, has diffuse PVNS in his knee. They discuss their prognoses.
View Answer & Explanation
Correct Answer: C
Rationale: Localized PVNS generally has a much better prognosis than diffuse PVNS. After complete arthroscopic excision, the recurrence rate for localized disease is low (typically less than 10-15%), whereas diffuse PVNS has a high recurrence rate (30-50% or more) even after extensive synovectomy. The main distractor, B) Diffuse PVNS is more easily treated with arthroscopic surgery, is incorrect. Diffuse PVNS often requires extensive open or combined open/arthroscopic synovectomy due to its widespread nature, making complete resection challenging.
Question 68
During an arthroscopic examination of a 33-year-old patient's knee, the surgeon observes a thickened, brownish, and nodular synovial lining with prominent villi. There are no loose bodies or significant cartilage erosions noted at this stage.
View Answer & Explanation
Correct Answer: E
Rationale: The description of a thickened, brownish, nodular, and villous synovial lining is pathognomonic for pigmented villonodular synovitis (PVNS). The brown discoloration is due to hemosiderin deposition. The main distractor, D) Synovial chondromatosis, would typically present with cartilaginous loose bodies within the joint, which are not described in the vignette.
Question 69
A 42-year-old female presents with a 3-month history of bilateral hand and foot pain, swelling, and morning stiffness lasting approximately 2 hours. Physical examination reveals symmetrical swelling and tenderness in the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints of both hands, as well as mild swelling in both knees. Serum rheumatoid factor is elevated.

View Answer & Explanation
Correct Answer: D
Rationale: The vignette describes several criteria for rheumatoid arthritis (RA) diagnosis according to the American Rheuma Association (ARA) simplified criteria: morning stiffness (minimally 1 hour, lasting for more than 6 weeks), arthritis of hand joints (lasting for more than 6 weeks), and symmetrical arthritis (lasting for more than 6 weeks). While rheumatoid nodules are a criterion for RA, their presence is not required for diagnosis, and the patient's current presentation does not include them. The other options (A, B, C, E) describe conditions that would argue against a diagnosis of confirmed RA based on the ARA criteria (e.g., morning stiffness <1h, <3 joint areas, asymmetrical, <6 weeks duration). The main distractor, A, is incorrect because morning stiffness must be at least 1 hour for RA diagnosis.
Question 70
A 55-year-old female with long-standing rheumatoid arthritis undergoes a knee arthroscopy for persistent pain and swelling. Intraoperative findings reveal an extremely hypertrophic synovium filling the intercondylar space, with visible invasion of the cartilage surface by this tissue.

View Answer & Explanation
Correct Answer: C
Rationale: The hypertrophic synovial tissue, known as pannus, is characteristic of rheumatoid arthritis. This proliferative pannus destroys cartilage both mechanically through its expansion and by releasing enzymes that degrade the cartilage matrix. This is a central pathomechanism of joint destruction in RA. The main distractor, A, is incorrect because osteophyte formation is more characteristic of osteoarthritis, not the primary mechanism of cartilage destruction in RA.
Question 71
A 68-year-old female with a 20-year history of rheumatoid arthritis presents with severe hand deformities. On examination of her right index finger, the proximal interphalangeal (PIP) joint is in extension, and the distal interphalangeal (DIP) joint is in flexion. The metacarpophalangeal (MCP) joint is subluxed.

View Answer & Explanation
Correct Answer: B
Rationale: A swan-neck deformity is characterized by hyperextension of the PIP joint and flexion of the DIP joint, often accompanied by MCP joint subluxation. This is a typical deformity seen in severe rheumatoid arthritis. The main distractor, A, describes the opposite deformity (PIP flexion, DIP extension).
Question 72
A 58-year-old female with advanced rheumatoid arthritis exhibits a specific finger deformity. On examination, her left middle finger shows the proximal interphalangeal (PIP) joint in flexion and the distal interphalangeal (DIP) joint in extension. The metacarpophalangeal (MCP) joint is also subluxed.
View Answer & Explanation
Correct Answer: B
Rationale: A Boutonnière (buttonhole) deformity is characterized by flexion of the PIP joint and hyperextension of the DIP joint. This is a common and typical deformity in rheumatoid arthritis. The main distractor, A, describes the opposite deformity (PIP extension, DIP flexion).
Question 73
A 62-year-old female with a history of rheumatoid arthritis presents with wrist pain and a prominent dorsal swelling. On physical examination, the ulnar head is dislocated dorsally. When moderate pressure is applied, the ulnar head can be reduced, but it immediately returns to the dislocated position upon release of pressure.
View Answer & Explanation
Correct Answer: B
Rationale: The described phenomenon, where the dorsally dislocated ulnar head can be reduced but springs back upon release of pressure, is known as the "piano-key sign." This is indicative of synovitis of the radioulnar joint and instability of the distal radioulnar joint (DRUJ) due to ligamentous laxity and extensor carpi ulnaris tendon subluxation, common in RA. The main distractor, C, is a nerve compression syndrome, not a specific sign of DRUJ instability.
Question 74
A 38-year-old female presents with early symptoms of rheumatoid arthritis. Radiographs of her hands are obtained to assess for initial changes. What is a typical early radiographic finding in rheumatoid arthritis?

View Answer & Explanation
Correct Answer: C
Rationale: Early radiographic changes in rheumatoid arthritis typically include soft tissue swelling, juxta-articular osteopenia (often described as striped periarticular atrophy or osteoporosis), and marginal erosions. Diffuse osteosclerosis, joint space widening, large subchondral cysts, and carpal ankylosis are not characteristic early findings; ankylosis is a late-stage change. The main distractor, A, is incorrect as osteosclerosis is not an early feature of RA; rather, osteopenia is seen.
Question 75
A 70-year-old male with a 30-year history of severe, uncontrolled rheumatoid arthritis presents with profound wrist stiffness and pain. Radiographs of his wrist show complete obliteration of the radiocarpal and intercarpal joint spaces, with the carpal bones appearing fused into a single osseous mass.

View Answer & Explanation
Correct Answer: C
Rationale: In severe, end-stage rheumatoid arthritis, the chronic inflammation and destruction can lead to complete fusion of the carpal bones, forming a single osseous mass referred to as an "os carpi." This represents severe carpal ankylosis. The main distractor, A, describes features more typical of osteoarthritis, not end-stage RA.
Question 76
A 50-year-old female with confirmed rheumatoid arthritis develops firm, non-tender subcutaneous nodules. These nodules are most commonly found in which of the following locations?
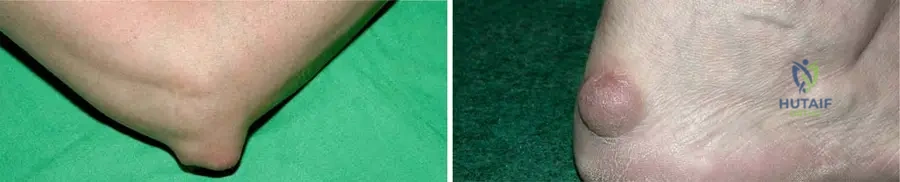
View Answer & Explanation
Correct Answer: C
Rationale: Rheumatoid nodules are typical extra-articular manifestations of RA and are most commonly found subcutaneously on the extensor sides of limbs, especially over the olecranon, Achilles tendon, and other areas subjected to pressure. The main distractor, B, is incorrect as nodules typically appear on extensor surfaces, not flexor surfaces.
Question 77
A biopsy is performed on a subcutaneous nodule from a 65-year-old male with long-standing rheumatoid arthritis. Microscopic examination of the nodule reveals a central necrotic area surrounded by a peripheral palisading arrangement of histiocytes.
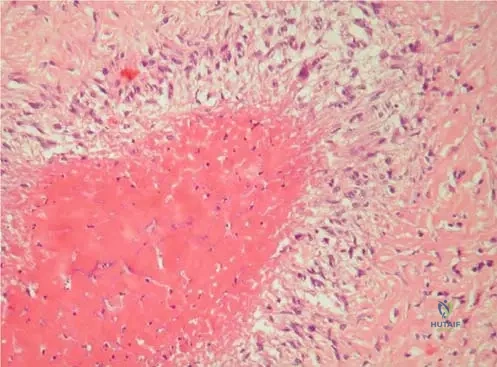
View Answer & Explanation
Correct Answer: B
Rationale: The microscopic appearance of a rheumatoid nodule is highly characteristic and diagnostic. It consists of a central necrotic area (fibrinoid necrosis) surrounded by a peripheral layer of palisading histiocytes (macrophages). The main distractor, A, describes the characteristic pathology of tuberculosis, not rheumatoid nodules.
Question 78
A 48-year-old female with early-stage rheumatoid arthritis reports mild neck stiffness. An X-ray and MRI of the cervical spine are performed. The images show incipient atlanto-axial synovitis with moderate subluxation, but the MRI confirms a normal liquor space around the spinal cord without cord involvement.

View Answer & Explanation
Correct Answer: D
Rationale: Even in early RA, atlanto-axial synovitis and moderate subluxation can occur. Given that the liquor space is normal and there is no cord involvement, immediate surgery is not indicated. However, the potential for progression to severe subluxation and cord compression necessitates close monitoring. The main distractor, A, is incorrect because surgical indication is typically based on severe subluxation (e.g., posterior atlantodental interval <14mm) or neurological signs, neither of which are present here.
Question 79
A 72-year-old male with severe, late-stage rheumatoid arthritis presents with progressive gait disturbance and upper extremity weakness. MRI of the cervical spine reveals severe atlanto-axial subluxation with dorsal and cranial displacement of the dens, resulting in spinal cord compression. The distance between the posterior wall of the dens and the anterior wall of the posterior arch of the atlas measures 12 mm.

View Answer & Explanation
Correct Answer: C
Rationale: In late-stage RA, severe atlanto-axial subluxation can lead to spinal cord compression, which is a life-threatening complication. The text explicitly states that when the distance between the posterior wall of the dens and the anterior wall of the posterior arch of the atlas is 14 mm or less, surgical indication is established regardless of neurological signs. This patient's measurement of 12 mm falls within this critical range. Neurological signs are generally not reversible. The main distractor, A, is incorrect as conservative management is insufficient for severe subluxation with cord compression and a critical measurement.
Question 80
A 60-year-old female with long-standing rheumatoid arthritis complains of significant foot pain and difficulty wearing shoes. Physical examination reveals severe forefoot deformities, including hallux valgus, hammer toes, and a flat foot appearance. Radiographs confirm fibular deviation of the toes, metatarsophalangeal (MTP) joint destruction, and erosions.

View Answer & Explanation
Correct Answer: D
Rationale: The described deformities—hallux valgus, hammer toes, MTP joint destruction, flat foot, and fibular deviation of toes—are classic and severe forefoot manifestations of rheumatoid arthritis. These result from chronic synovitis, ligamentous laxity, and bone erosion. The main distractor, B, describes a pes cavus deformity, which is the opposite of the flat foot often seen in RA, and claw toes are different from hammer toes, though both involve toe contractures.
Question 81
A 52-year-old female is diagnosed with rheumatoid arthritis. Her physician explains the underlying mechanism of joint destruction in this condition. Which of the following best describes the primary mechanism of cartilage destruction in rheumatoid arthritis?
View Answer & Explanation
Correct Answer: C
Rationale: The hallmark of joint destruction in RA is the formation of a proliferative synovial pannus. This pannus, composed of hypertrophic synovial tissue, invades the cartilage surface and subchondral bone, destroying them through both mechanical pressure and the release of proteolytic enzymes. The main distractor, B, describes the primary mechanism of osteoarthritis, not rheumatoid arthritis.
Question 82
A 67-year-old female has been suffering from severe rheumatoid arthritis for 20 years and has been on long-term steroid treatment. On examination, she exhibits typical hand and foot deformities, and her face appears altered with features consistent with chronic steroid use.

View Answer & Explanation
Correct Answer: C
Rationale: Long-term steroid treatment, commonly used in severe rheumatoid arthritis, can lead to iatrogenic Cushing's syndrome, characterized by features such as a "moon face," "buffalo hump," truncal obesity, skin atrophy, and osteoporosis. The altered face is a direct consequence of these effects. The main distractor, E, is incorrect as long-term steroid use typically leads to decreased bone density (osteoporosis), not increased bone density.
Question 83
A 58-year-old female with rheumatoid arthritis presents with pain and swelling over the dorsal aspect of her wrist, accompanied by difficulty extending her fingers. An ultrasound confirms extensor tenosynovitis. Intraoperatively, hypertrophic synovial tissue is observed penetrating into the extensor tendons.

View Answer & Explanation
Correct Answer: B
Rationale: In rheumatoid arthritis, the hypertrophic synovial tissue (pannus) not only invades joints but also tendon sheaths. This inflamed synovium and the enzymes it produces directly damage the ligaments and tendons running within their sheets, leading to tenosynovitis, tendon weakening, and ultimately ruptures and deformities. The main distractor, A, is incorrect as direct trauma is not the primary mechanism for tenosynovitis in RA; it's an inflammatory process.
Question 84
A 45-year-old female is diagnosed with rheumatoid arthritis. Her family history reveals that her mother and maternal aunt also had RA. Which of the following genetic factors is most commonly associated with an increased risk of developing rheumatoid arthritis?
View Answer & Explanation
Correct Answer: B
Rationale: The HLA-DR4 tissue antigen is detectable in approximately 50% of patients with rheumatoid arthritis and is strongly associated with an increased familial occurrence and susceptibility to the disease. HLA-B27 is associated with seronegative spondyloarthropathies. The main distractor, A, is incorrect as HLA-B27 is primarily associated with ankylosing spondylitis and other spondyloarthropathies, not RA.
Question 85
A 63-year-old female with severe, long-standing rheumatoid arthritis presents with skin changes on her lower extremities. Examination reveals areas of hyperpigmentation, skin atrophy, and healed ulcers with scarring. She denies any recent trauma.

View Answer & Explanation
Correct Answer: C
Rationale: Skin manifestations in RA can include hyperpigmentation or pigment loss, skin atrophy (often due to the disease itself or steroid treatment), and skin ulcers, which can occur due to vasculitis. The presence of healed ulcers with scarring is consistent with this. The main distractor, A, describes skin lesions characteristic of psoriasis, a different inflammatory arthropathy.
Question 86
A 68-year-old female with a 25-year history of rheumatoid arthritis presents with severe bilateral knee pain and a progressive valgus deformity. Radiographs of her knees show significant joint space narrowing and erosions. Additionally, a linear lucency is noted in the proximal tibia, consistent with a stress fracture.
View Answer & Explanation
Correct Answer: B
Rationale: Milkman fractures, also known as Looser's zones, are pseudofractures or stress fractures that occur in osteomalacia, which can be a complication in RA patients due to chronic inflammation, steroid use, or nutritional deficiencies. Valgus deformity of the knee is also common in RA. The main distractor, A, is a condition affecting articular cartilage and subchondral bone, typically in younger individuals, and not directly related to the described linear lucency in the tibia in an RA patient.
Question 87
A 50-year-old female with rheumatoid arthritis experiences significant limitations in her daily activities. She can perform self-care and vocational activities, but her non-vocational activities are limited. She is able to ambulate and use her hands for most tasks, but with some difficulty and pain.
View Answer & Explanation
Correct Answer: C
Rationale: The Steinbrocker functional classification for RA is as follows: Class I (complete functional capacity), Class II (adequate for normal activities despite discomfort/limited motion), Class III (limited to few or none of the duties of usual occupation or self-care), Class IV (largely or wholly incapacitated, bedridden or confined to wheelchair). The patient's description of being able to perform self-care and vocational activities but with limitations in non-vocational activities, and difficulty with ambulation/hand use, best fits Class III. The main distractor, B, would imply less severe limitations, where the patient is still adequate for normal activities despite discomfort.
Question 88
A 40-year-old female presents with a 4-month history of symmetrical polyarthritis affecting her MCP, PIP, and wrist joints, accompanied by morning stiffness lasting over an hour. Laboratory tests reveal elevated rheumatoid factor and anti-citrullinated protein antibodies (ACPA). Which of the following is a key distinguishing feature of rheumatoid arthritis compared to osteoarthritis?
- A) Involvement of the distal interphalangeal (DIP) joints
- B) Asymmetrical joint involvement
- C) Presence of morning stiffness lasting less than 30 minutes
- D) Symmetrical polyarticular inflammation with prominent synovitis
Question 88
A 50-year-old female with a 10-year history of rheumatoid arthritis presents with progressive hand deformities. On examination of her right index finger, the proximal interphalangeal (PIP) joint is in hyperextension, and the distal interphalangeal (DIP) joint is in flexion. The metacarpophalangeal (MCP) joints show mild subluxation.
View Answer & Explanation
Correct Answer: A
Rationale: The description of PIP joint hyperextension and DIP joint flexion is characteristic of a swan-neck deformity, a common hand deformity in rheumatoid arthritis. The image (Fig. 3.6 a) explicitly labels this deformity. Main Distractor: A buttonhole (or Boutonniere) deformity is characterized by PIP joint flexion and DIP joint extension, which is the opposite of the described findings.
Question 88
A 45-year-old female with established rheumatoid arthritis undergoes a knee arthroscopy for persistent pain and swelling. Intraoperative findings reveal extremely hypertrophic synovium filling the intercondylar space, with the pannus visibly invading the cartilage surface.
View Answer & Explanation
Correct Answer: A
Rationale: The provided text states, "The proliferative synovial pannus destroys the cartilage partly mechanically, partly by its enzymes." This dual mechanism of mechanical erosion and enzymatic degradation is the primary way the hypertrophic synovium (pannus) damages articular cartilage in RA. Main Distractor: Direct bacterial infection is not the primary mechanism of cartilage destruction in sterile rheumatoid arthritis, although secondary infection can occur.
Question 88
A 60-year-old male with long-standing, seropositive rheumatoid arthritis presents with palpable, firm, non-tender subcutaneous nodules over his olecranon processes. A biopsy of one of these nodules is performed.
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly states, "The microscopic picture of rheumatoid nodule is of diagnostic value. Central necrotic area with peripheral histiocytic pallisading." This histological appearance is pathognomonic for rheumatoid nodules. Main Distractor: Granulomatous inflammation without necrosis is characteristic of other conditions like sarcoidosis, but not typical for rheumatoid nodules which feature central necrosis.
Question 88
A 55-year-old female with a history of rheumatoid arthritis complains of chronic wrist pain and a noticeable prominence on the dorsal aspect of her wrist. On physical examination, the dorsal prominence of the ulnar head can be reduced with moderate pressure, but it immediately returns to its dislocated position when the pressure is released.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical description, "It can be reduced with moderate pressure, but as soon as the pressure is released it returns to the dislocated position," is precisely how the "piano-key" sign is described in the text (Fig. 3.5 b) in the context of dorsal dislocation of the ulnar head due to synovitis of the radioulnar joint. Main Distractor: Finkelstein's test is used to diagnose De Quervain's tenosynovitis, which involves pain at the radial styloid, not dorsal ulnar head instability.
Question 88
A 62-year-old female with severe, long-standing rheumatoid arthritis presents with significant forefoot pain and difficulty wearing shoes. Clinical examination reveals severe hallux valgus, hammer toes, and a flat foot with lateral deviation of the lesser toes. Radiographs are obtained to assess the extent of joint damage.
View Answer & Explanation
Correct Answer: A
Rationale: The text and image (Fig. 3.13 b) explicitly state, "X-ray confirms fibular deviation of toes, MTP destruction, and erosions." This lateral (fibular) deviation of the toes is a characteristic radiographic finding in severe RA forefoot deformities. Main Distractor: Medial deviation of toes is not a typical finding in rheumatoid forefoot deformities; lateral (fibular) deviation is characteristic.
Question 88
A 70-year-old female with a 20-year history of rheumatoid arthritis presents with progressive neck pain, occipital headaches, and new-onset gait instability. MRI of the cervical spine reveals severe atlanto-axial synovitis and subluxation with evidence of spinal cord compression.
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "When the distance between the posterior wall of the dens and anterior wall of the posterior arch of the atlas is 14 mm or less, indication of surgery is established regardless of neurological signs." This measurement is a critical indicator for surgical intervention due to the risk of spinal cord compression. Main Distractor: An anterior atlanto-dens interval (AADI) greater than 3 mm is indicative of atlanto-axial instability but does not, by itself, establish a surgical indication regardless of neurological signs in the same definitive way as the posterior space measurement, which directly reflects the space available for the cord.
Question 88
A 40-year-old female recently diagnosed with early-stage rheumatoid arthritis undergoes an MRI of her cervical spine due to mild, intermittent neck stiffness. The MRI reveals incipient atlanto-axial synovitis with moderate subluxation.
View Answer & Explanation
Correct Answer: A
Rationale: The text, referring to Fig. 3.19 b, states, "MR shows normal liquor space around the spinal cord, cordal involvement is not present" in the early stage of atlanto-axial synovitis with moderate subluxation. This indicates that while instability may be present, significant neurological compromise is typically absent early on. Main Distractor: Significant spinal cord compression is characteristic of late-stage atlanto-axial subluxation in RA, not typically seen in the early stages where liquor space is often preserved.
Question 88
A 65-year-old female with a 25-year history of severe rheumatoid arthritis presents with complete loss of wrist motion and severe pain. Radiographs show destruction of the ulnar epiphysis and markedly decreased radiocarpal and intercarpal joint spaces.
View Answer & Explanation
Correct Answer: A
Rationale: The text, referring to Fig. 3.8 b, describes the end result of severe wrist changes in RA as "the wrist is ankylosed, the bones of the carpus are fused creating a single bone (os carpi)." This complete fusion is the characteristic end-stage radiographic appearance. Main Distractor: While isolated fusions can occur, the "os carpi" represents a more complete and severe ankylosis of the entire carpus, which is the ultimate end-stage described.
Question 88
A 58-year-old female with long-standing rheumatoid arthritis experiences progressive hand deformities, including tendon ruptures and joint subluxations. An intraoperative image shows hypertrophic synovial tissue penetrating into the tendons.
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "The hypertrophic synovial tissue and its enzymes damage the ligaments and the tendons running in their sheets. This is the mechanism of development of the joint deformities, subluxations, tendon ruptures." This highlights the combined effect of enzymatic degradation and mechanical disruption by the proliferating synovium. Main Distractor: While increased vascularity is part of the inflammatory process, the direct damage to tendons and ligaments is primarily attributed to the enzymes and mechanical pressure from the hypertrophic synovium, not just vascularity itself.
Question 88
A 68-year-old female with a 20-year history of severe rheumatoid arthritis, managed with long-term steroid treatment, presents for follow-up. On examination, her skin appears thin and fragile, and she has some areas of hyperpigmentation.
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "Atrophy of skin is effected by the disease or steroid treatment." Long-term steroid use is well-known to cause skin thinning and atrophy, which aligns with the clinical vignette. Hyperpigmentation and pigment loss are also characteristic, as are skin ulcers due to vasculitis, but skin atrophy is directly linked to steroid treatment. Main Distractor: Psoriasis is a distinct autoimmune skin condition and not a direct skin manifestation of RA or its steroid treatment, although some patients may have both conditions (psoriatic arthritis is a separate entity).
Question 88
A 40-year-old female is diagnosed with Rheumatoid Arthritis after presenting with characteristic symptoms and positive serological markers.
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "Incidence of RA is approximately 1% of the adult population." Main Distractor: The female-male proportion is 3:1, not 1:3. Onset is mostly between 35 and 55 years, not typically before age 20. HLA-Dr4 is detectable in 50% of patients, not nearly all. Increased familial occurrence is often present, not rare.
Question 88
A 38-year-old female presents with symmetrical swelling and pain in her metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints for 3 months, associated with morning stiffness lasting 2 hours. Laboratory tests reveal an elevated serum rheumatoid factor.
View Answer & Explanation
Correct Answer: A
Rationale: Based on the simplified ARA criteria provided: 1. Morning joint stiffness (minimally 1 h, lasting for more than 6 weeks) - Fulfilled (2 hours, 3 months). 2. Arthritis (minimally three areas of joints, lasting for more than 6 weeks) - Fulfilled (MCP and PIP joints are more than 3 areas, 3 months). 3. Arthritis of hand joints (lasting for more than 6 weeks) - Fulfilled (MCP and PIP joints, 3 months). 4. Symmetrical arthritis lasting for more than 6 weeks - Fulfilled (symmetrical, 3 months). 5. Rheumatoid nodule - Not mentioned. 6. Elevated serum rheumatoid factor - Fulfilled. 7. Radiological changes (marginal erosions or striped osteoporosis) - Not mentioned. To be "confirmed," at least four criteria must be fulfilled. This patient fulfills criteria 1, 3, 4, and 6, totaling 4 criteria. Main Distractor: While the patient has arthritis in multiple areas (criterion 2), criteria 1, 3, 4, and 6 are sufficient to meet the "at least four criteria" for confirmed RA, making 4 the correct count.
Question 88
An intraoperative image of a knee joint in a patient with rheumatoid arthritis shows extremely hypertrophic synovium filling the intercondylar space, with the pannus visibly invading the cartilage surface.
Question 89
A 50-year-old female with a 10-year history of rheumatoid arthritis presents with progressive hand deformities. On examination of her right index finger, the proximal interphalangeal (PIP) joint is in hyperextension, and the distal interphalangeal (DIP) joint is in flexion. The metacarpophalangeal (MCP) joints show mild subluxation.
View Answer & Explanation
Correct Answer: A
Rationale: The description of PIP joint hyperextension and DIP joint flexion is characteristic of a swan-neck deformity, a common hand deformity in rheumatoid arthritis. The image (Fig. 3.6 a) explicitly labels this deformity. Main Distractor: A buttonhole (or Boutonniere) deformity is characterized by PIP joint flexion and DIP joint extension, which is the opposite of the described findings.
Question 90
A 45-year-old female with established rheumatoid arthritis undergoes a knee arthroscopy for persistent pain and swelling. Intraoperative findings reveal extremely hypertrophic synovium filling the intercondylar space, with the pannus visibly invading the cartilage surface.
View Answer & Explanation
Correct Answer: A
Rationale: The provided text states, "The proliferative synovial pannus destroys the cartilage partly mechanically, partly by its enzymes." This dual mechanism of mechanical erosion and enzymatic degradation is the primary way the hypertrophic synovium (pannus) damages articular cartilage in RA. Main Distractor: Direct bacterial infection is not the primary mechanism of cartilage destruction in sterile rheumatoid arthritis, although secondary infection can occur.
Question 91
A 60-year-old male with long-standing, seropositive rheumatoid arthritis presents with palpable, firm, non-tender subcutaneous nodules over his olecranon processes. A biopsy of one of these nodules is performed.
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly states, "The microscopic picture of rheumatoid nodule is of diagnostic value. Central necrotic area with peripheral histiocytic pallisading." This histological appearance is pathognomonic for rheumatoid nodules. Main Distractor: Granulomatous inflammation without necrosis is characteristic of other conditions like sarcoidosis, but not typical for rheumatoid nodules which feature central necrosis.
Question 92
A 55-year-old female with a history of rheumatoid arthritis complains of chronic wrist pain and a noticeable prominence on the dorsal aspect of her wrist. On physical examination, the dorsal prominence of the ulnar head can be reduced with moderate pressure, but it immediately returns to its dislocated position when the pressure is released.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical description, "It can be reduced with moderate pressure, but as soon as the pressure is released it returns to the dislocated position," is precisely how the "piano-key" sign is described in the text (Fig. 3.5 b) in the context of dorsal dislocation of the ulnar head due to synovitis of the radioulnar joint. Main Distractor: Finkelstein's test is used to diagnose De Quervain's tenosynovitis, which involves pain at the radial styloid, not dorsal ulnar head instability.
Question 93
A 62-year-old female with severe, long-standing rheumatoid arthritis presents with significant forefoot pain and difficulty wearing shoes. Clinical examination reveals severe hallux valgus, hammer toes, and a flat foot with lateral deviation of the lesser toes. Radiographs are obtained to assess the extent of joint damage.
View Answer & Explanation
Correct Answer: A
Rationale: The text and image (Fig. 3.13 b) explicitly state, "X-ray confirms fibular deviation of toes, MTP destruction, and erosions." This lateral (fibular) deviation of the toes is a characteristic radiographic finding in severe RA forefoot deformities. Main Distractor: Medial deviation of toes is not a typical finding in rheumatoid forefoot deformities; lateral (fibular) deviation is characteristic.
Question 94
A 70-year-old female with a 20-year history of rheumatoid arthritis presents with progressive neck pain, occipital headaches, and new-onset gait instability. MRI of the cervical spine reveals severe atlanto-axial synovitis and subluxation with evidence of spinal cord compression.
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "When the distance between the posterior wall of the dens and anterior wall of the posterior arch of the atlas is 14 mm or less, indication of surgery is established regardless of neurological signs." This measurement is a critical indicator for surgical intervention due to the risk of spinal cord compression. Main Distractor: An anterior atlanto-dens interval (AADI) greater than 3 mm is indicative of atlanto-axial instability but does not, by itself, establish a surgical indication regardless of neurological signs in the same definitive way as the posterior space measurement, which directly reflects the space available for the cord.
Question 95
A 40-year-old female recently diagnosed with early-stage rheumatoid arthritis undergoes an MRI of her cervical spine due to mild, intermittent neck stiffness. The MRI reveals incipient atlanto-axial synovitis with moderate subluxation.
View Answer & Explanation
Correct Answer: A
Rationale: The text, referring to Fig. 3.19 b, states, "MR shows normal liquor space around the spinal cord, cordal involvement is not present" in the early stage of atlanto-axial synovitis with moderate subluxation. This indicates that while instability may be present, significant neurological compromise is typically absent early on. Main Distractor: Significant spinal cord compression is characteristic of late-stage atlanto-axial subluxation in RA, not typically seen in the early stages where liquor space is often preserved.
Question 96
A 65-year-old female with a 25-year history of severe rheumatoid arthritis presents with complete loss of wrist motion and severe pain. Radiographs show destruction of the ulnar epiphysis and markedly decreased radiocarpal and intercarpal joint spaces.
View Answer & Explanation
Correct Answer: A
Rationale: The text, referring to Fig. 3.8 b, describes the end result of severe wrist changes in RA as "the wrist is ankylosed, the bones of the carpus are fused creating a single bone (os carpi)." This complete fusion is the characteristic end-stage radiographic appearance. Main Distractor: While isolated fusions can occur, the "os carpi" represents a more complete and severe ankylosis of the entire carpus, which is the ultimate end-stage described.
Question 97
A 58-year-old female with long-standing rheumatoid arthritis experiences progressive hand deformities, including tendon ruptures and joint subluxations. An intraoperative image shows hypertrophic synovial tissue penetrating into the tendons.
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "The hypertrophic synovial tissue and its enzymes damage the ligaments and the tendons running in their sheets. This is the mechanism of development of the joint deformities, subluxations, tendon ruptures." This highlights the combined effect of enzymatic degradation and mechanical disruption by the proliferating synovium. Main Distractor: While increased vascularity is part of the inflammatory process, the direct damage to tendons and ligaments is primarily attributed to the enzymes and mechanical pressure from the hypertrophic synovium, not just vascularity itself.
Question 98
A 68-year-old female with a 20-year history of severe rheumatoid arthritis, managed with long-term steroid treatment, presents for follow-up. On examination, her skin appears thin and fragile, and she has some areas of hyperpigmentation.
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "Atrophy of skin is effected by the disease or steroid treatment." Long-term steroid use is well-known to cause skin thinning and atrophy, which aligns with the clinical vignette. Hyperpigmentation and pigment loss are also characteristic, as are skin ulcers due to vasculitis, but skin atrophy is directly linked to steroid treatment. Main Distractor: Psoriasis is a distinct autoimmune skin condition and not a direct skin manifestation of RA or its steroid treatment, although some patients may have both conditions (psoriatic arthritis is a separate entity).
Question 99
A 40-year-old female is diagnosed with Rheumatoid Arthritis after presenting with characteristic symptoms and positive serological markers.
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "Incidence of RA is approximately 1% of the adult population." Main Distractor: The female-male proportion is 3:1, not 1:3. Onset is mostly between 35 and 55 years, not typically before age 20. HLA-Dr4 is detectable in 50% of patients, not nearly all. Increased familial occurrence is often present, not rare.
Question 100
A 38-year-old female presents with symmetrical swelling and pain in her metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints for 3 months, associated with morning stiffness lasting 2 hours. Laboratory tests reveal an elevated serum rheumatoid factor.
View Answer & Explanation
Correct Answer: A
Rationale: Based on the simplified ARA criteria provided: 1. Morning joint stiffness (minimally 1 h, lasting for more than 6 weeks) - Fulfilled (2 hours, 3 months). 2. Arthritis (minimally three areas of joints, lasting for more than 6 weeks) - Fulfilled (MCP and PIP joints are more than 3 areas, 3 months). 3. Arthritis of hand joints (lasting for more than 6 weeks) - Fulfilled (MCP and PIP joints, 3 months). 4. Symmetrical arthritis lasting for more than 6 weeks - Fulfilled (symmetrical, 3 months). 5. Rheumatoid nodule - Not mentioned. 6. Elevated serum rheumatoid factor - Fulfilled. 7. Radiological changes (marginal erosions or striped osteoporosis) - Not mentioned. To be "confirmed," at least four criteria must be fulfilled. This patient fulfills criteria 1, 3, 4, and 6, totaling 4 criteria. Main Distractor: While the patient has arthritis in multiple areas (criterion 2), criteria 1, 3, 4, and 6 are sufficient to meet the "at least four criteria" for confirmed RA, making 4 the correct count.
You Might Also Like
