Orthopedic Board Review: Musculoskeletal Tumors, Ankylosing Spondylitis, Synovial Chondromatosis | Part 15

Key Takeaway
An orthopedic musculoskeletal pathology review covers key conditions like atypical lipomas, osteochondromas, Ankylosing Spondylitis, and synovial chondromatosis. It includes diagnostic criteria, imaging findings (MRI, X-ray), histological features, clinical presentations, and management strategies essential for board exam preparation.
Question 1
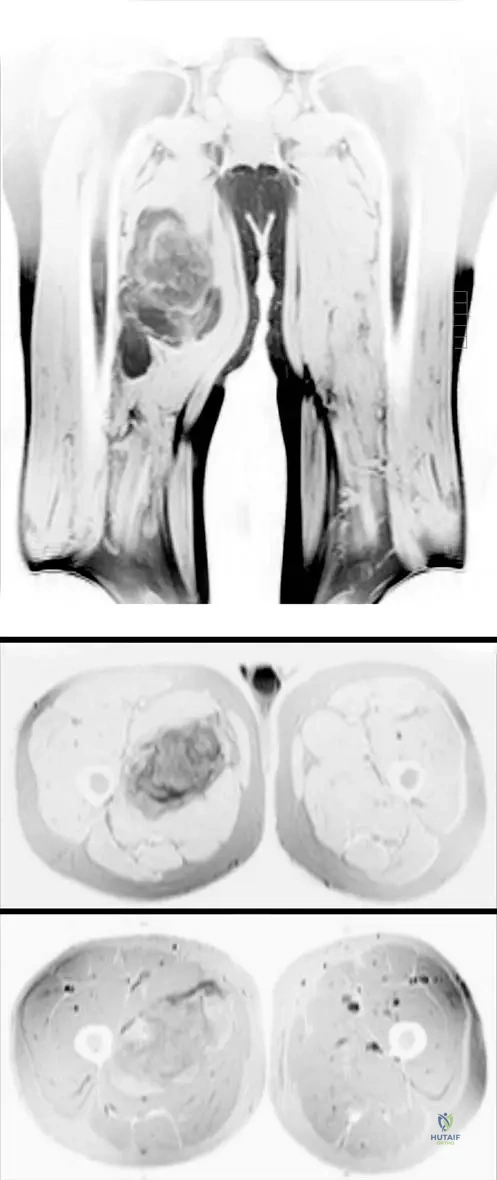
A 50-year-old male presents with a painless, palpable mass in his deep posterior thigh that has been present for several months. MRI images are provided, showing a large soft tissue mass. The lesion demonstrates high signal intensity on T1-weighted images, consistent with fat, but also contains areas of decreased signal intensity and thickened septations. What is the primary histological feature that differentiates an atypical lipoma from a conventional lipoma?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "There is more atypia on histologic examination." This refers to the presence of atypical adipocytes, often with enlarged, hyperchromatic nuclei, and scattered pleomorphic stromal cells, which are the defining histological features distinguishing an atypical lipoma (well-differentiated liposarcoma) from a benign conventional lipoma. While both contain mature adipocytes, the atypia is key. Myxoid stroma is characteristic of myxoid liposarcoma, and high mitotic activity would suggest a higher-grade sarcoma.
Question 2
A 67-year-old female presents with a large, deep soft tissue mass in her thigh. MRI images are provided, showing a lesion that is predominantly high signal intensity on T1-weighted images, consistent with fat. However, there are also areas of hazy, decreased signal intensity and thickened septations. Postcontrast images demonstrate enhancement within these non-fatty components. What is the significance of the "hazy, decreased signal intensity" on T1-weighted images in the context of an atypical lipoma?

View Answer & Explanation
Correct Answer: D
Rationale: The text describes the MRI findings: "nonlipomatous elements that can be in the form of thickened septations and/or scattered soft tissue nodularity. These latter features result in areas of hazy, decreased signal intensity in the background of a predominantly high signal intensity mass on T1-weighted images and create an appearance described as 'dirty fat.'" This directly links the hazy, decreased signal to the non-fatty components, not hemorrhage, necrosis, or mature fat itself.
Question 3
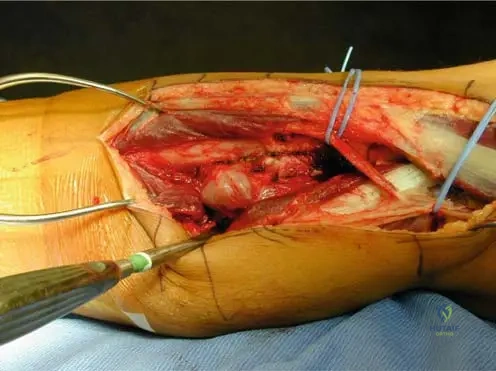
A 55-year-old male presents with a large, palpable mass in his posterior thigh. Clinical photograph is provided. The mass has been slowly growing for several months and is asymptomatic. MRI reveals a predominantly fatty lesion with internal septations and nodular components that enhance with contrast. What is the most appropriate management strategy for a diagnosed atypical lipoma in a deep extremity location?

View Answer & Explanation
Correct Answer: C
Rationale: Atypical lipomatous tumors (ALTs) are low-grade malignant tumors (well-differentiated liposarcomas in deep locations). The standard of care for these tumors is wide local excision with clear surgical margins to minimize the risk of local recurrence and prevent dedifferentiation. Radiation and chemotherapy are typically reserved for higher-grade sarcomas or in cases of positive margins/recurrence. Embolization and steroid injections are not appropriate treatments for ALTs.
Question 4
A 61-year-old female presents with a large, deep soft tissue mass in her thigh. MRI images are provided, showing a lesion with mixed signal characteristics, predominantly fat but with significant non-fatty components that enhance after contrast administration. The patient is asymptomatic. Which of the following is NOT a typical characteristic of atypical lipomas based on the provided clinical context?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states, "Grossly, lesions are more firm than lipomas and the tissue does not resemble mature fat." Therefore, being "softer than conventional lipomas" is an incorrect characteristic. The other options (A, B, C, E) are all accurate descriptions of atypical lipomas as provided in the clinical context.
Question 5
A 58-year-old male presents with a slowly growing, painless mass in his posterior thigh. Physical examination reveals a large, palpable soft tissue mass with overlying varicosities. MRI demonstrates a lesion composed predominantly of fat with thickened septations and scattered soft tissue nodularity, showing areas of hazy, decreased signal intensity on T1-weighted images. Postcontrast images show varying amounts of enhancement. What is the primary concern when differentiating an atypical lipoma from a simple lipoma?
View Answer & Explanation
Correct Answer: C
Rationale: Atypical lipomas are considered low-grade malignant tumors (well-differentiated liposarcomas in deep locations). The primary concern is their potential for local recurrence if inadequately excised and, more importantly, their ability to dedifferentiate into a higher-grade, more aggressive liposarcoma. This malignant potential is the key differentiator from a benign simple lipoma, which does not carry these risks. While large masses can cause cosmetic deformity or neurovascular compression, these are not the *primary* concerns driving the differentiation from a simple lipoma.
Question 6
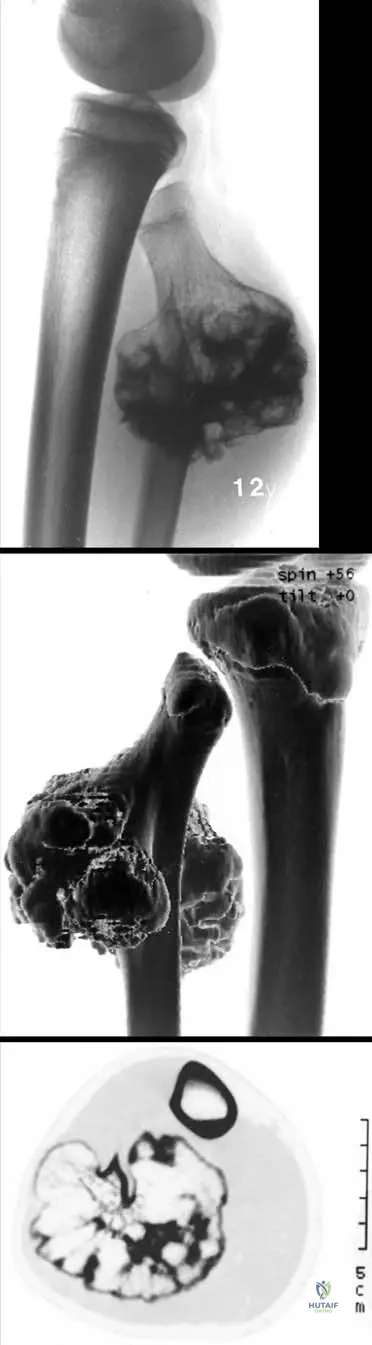
A 14-year-old male presents with a slowly growing, painless mass on the distal femur. Physical examination reveals a firm, non-tender, fixed bony prominence. Radiographs show a bony projection arising from the metaphysis of the distal femur, with clear continuity of the cortex and medullary bone between the lesion and the parent bone.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of a slowly growing, painless bony mass in an adolescent, combined with radiographic findings of cortical and medullary continuity with the parent bone, is pathognomonic for an osteochondroma. Enchondromas are intramedullary lesions, fibrous dysplasia has a characteristic ground-glass appearance, non-ossifying fibromas are typically cortical defects, and osteoid osteomas present with nocturnal pain relieved by NSAIDs and a nidus on imaging.
Question 7
A 10-year-old girl is evaluated for a palpable mass near her knee. Radiographs demonstrate a bony exostosis originating from the lateral aspect of the proximal tibia. The most critical radiographic feature to confirm the diagnosis of an osteochondroma is:
View Answer & Explanation
Correct Answer: C
Rationale: The radiographic hallmark of an osteochondroma is the demonstration of cortical and medullary continuity between the lesion and the parent bone. This feature distinguishes it from other bony exostoses or surface lesions. A sclerotic margin is non-specific, a lucent nidus is characteristic of an osteoid osteoma, periosteal reaction suggests inflammation or aggressive process, and soft tissue calcification is not a primary diagnostic feature of osteochondroma itself.
Question 8
A 22-year-old male presents with a new onset of pain and swelling over a previously asymptomatic bony prominence on his distal femur. He reports that the mass has been present since childhood. What is the most likely cause of his acute symptoms?
View Answer & Explanation
Correct Answer: C
Rationale: Sudden pain in a pre-existing osteochondroma is most commonly due to a fracture through its stalk. While malignant transformation is a concern, it typically presents with continued growth after skeletal maturity and increasing cartilage cap thickness, not sudden pain. Infection and avascular necrosis are rare complications. A ganglion cyst is not typically associated with acute pain in this context.
Question 9
A 16-year-old female presents with a painful mass on the medial aspect of her proximal tibia. She reports that the pain is worse with activity and direct pressure. Radiographs confirm a pedunculated osteochondroma. Which of the following is the most common mechanism for pain associated with an osteochondroma?
View Answer & Explanation
Correct Answer: B
Rationale: Osteochondromas often become painful due to compression of overlying structures (e.g., nerves, vessels, tendons) or due to overlying bursa formation. While a fracture through the stalk can cause sudden pain, compression and bursa formation are more common causes of chronic or activity-related pain. Intrinsic pain from the cartilage cap, muscle invasion, or marrow edema are not typical pain mechanisms for benign osteochondromas.
Question 10
A 35-year-old male, skeletally mature, presents with a previously stable osteochondroma on his humerus that has recently begun to grow rapidly. MRI reveals a cartilage cap thickness of 3 cm. What is the most appropriate next step in management?
View Answer & Explanation
Correct Answer: C
Rationale: Continued growth after skeletal maturity and a cartilage cap thickness greater than 1-2 cm are significant signs of potential malignant degeneration to a low-grade chondrosarcoma. In this scenario, excisional biopsy is indicated for definitive diagnosis and treatment. Reassurance and observation would be inappropriate given the concerning features. Genetic counseling is relevant for multiple osteochondromatosis but not the primary concern for a solitary, degenerating lesion. Physical therapy and aspiration are not diagnostic or therapeutic for suspected malignancy.
Question 11
A 28-year-old female with a known solitary osteochondroma of the proximal tibia is concerned about malignant transformation. Which of the following features is most indicative of malignant degeneration?
View Answer & Explanation
Correct Answer: D
Rationale: In a skeletally mature patient, a cartilage cap thickness greater than 1-2 cm is a key indicator of potential malignant degeneration of an osteochondroma to a chondrosarcoma. Growing away from the joint, the presence of a cartilage cap (of normal thickness), and cortical/medullary continuity are all characteristic features of a benign osteochondroma. An overlying bursa is a common benign complication causing pain, not a sign of malignancy.
Question 12
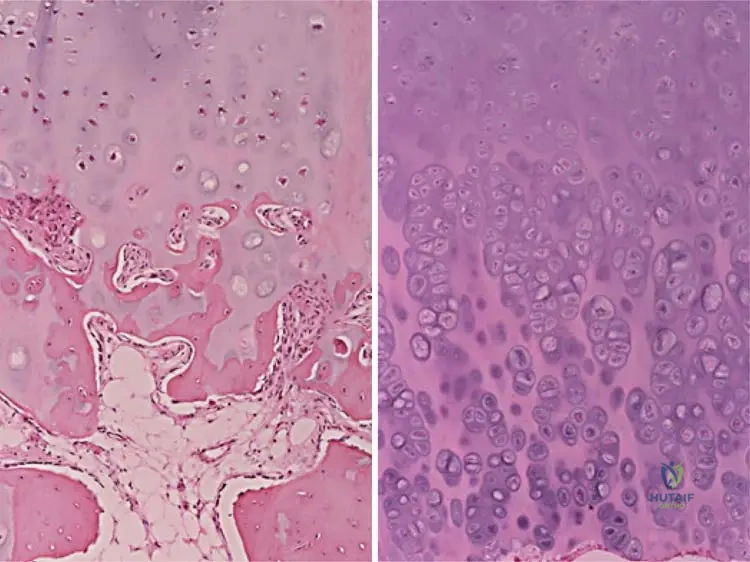
A biopsy is performed on a bony lesion from a 12-year-old boy. Histological examination reveals a cartilage cap undergoing enchondral ossification, with continuity of the marrow space with the underlying bone. This histological appearance most closely resembles which normal anatomical structure?
View Answer & Explanation
Correct Answer: B
Rationale: Histologically, osteochondromas resemble physes (growth plates) due to their cartilage cap undergoing enchondral ossification. This is a key characteristic that explains their growth pattern and origin. Articular cartilage, epiphyseal bone, synovial membrane, and periosteum have distinct histological features that do not match the description.
Question 13
A 7-year-old boy is diagnosed with an osteochondroma of the distal femur. His parents inquire about the typical growth pattern of these lesions. You inform them that osteochondromas generally:

View Answer & Explanation
Correct Answer: B
Rationale: Osteochondromas typically grow away from the joint. This is a characteristic feature often observed on imaging and is believed to be related to their origin from the physis and subsequent outward growth. Concentric growth is seen in other lesions, and they do grow during skeletal development.
Question 14
A 5-year-old boy presents with multiple bony exostoses affecting his bilateral femurs, tibias, and humeri, associated with mild limb length discrepancies and angular deformities. His mother reports that her father also had similar bony growths. This condition, multifocal osteochondromatosis, is characterized by which inheritance pattern?
View Answer & Explanation
Correct Answer: B
Rationale: Multifocal osteochondromatosis (also known as hereditary multiple exostoses) is an autosomal dominant inherited disorder. The presence of multiple lesions and a family history (mother's father) strongly supports this inheritance pattern. It is not autosomal recessive, X-linked, mitochondrial, or solely due to sporadic mutation.
Question 15
A 17-year-old male presents with numbness and tingling in the sole of his foot, accompanied by weakness in ankle plantarflexion and toe flexion. Physical examination reveals a palpable, firm mass in the popliteal fossa. Radiographs show a large osteochondroma arising from the posterior aspect of the distal femur. Which nerve is most likely being compressed by this lesion?

View Answer & Explanation
Correct Answer: D
Rationale: The symptoms of numbness and tingling in the sole of the foot, along with weakness in ankle plantarflexion and toe flexion, are classic signs of tibial nerve compression. The tibial nerve runs through the popliteal fossa, making it susceptible to compression by an osteochondroma in this location. The common peroneal nerve affects the dorsum of the foot and ankle dorsiflexion, the sciatic nerve is more proximal, and the femoral and sural nerves have different distributions.
Question 16
A 15-year-old male with multiple osteochondromatosis presents with progressive bowing of his forearm and limited range of motion at the wrist. Radiographs show significant shortening of the ulna relative to the radius, with an osteochondroma at the distal ulnar metaphysis. This deformity is best described as:
View Answer & Explanation
Correct Answer: A
Rationale: Madelung deformity is characterized by premature physeal arrest or growth disturbance of the distal ulna, leading to ulnar shortening, dorsal subluxation of the ulnar head, and radial bowing. While classically associated with genetic conditions, osteochondromas near physes, especially in multifocal osteochondromatosis, can cause similar developmental deformities. The other options describe acute traumatic injuries or ischemic contracture, not chronic developmental deformities.
Question 17
A 9-year-old boy presents with a firm, non-tender mass on the anterior aspect of his distal tibia. Radiographs confirm a sessile osteochondroma. From which part of the bone do osteochondromas typically arise?
View Answer & Explanation
Correct Answer: D
Rationale: Osteochondromas are benign cartilage-capped bony projections arising from the external surface of the bone, typically in the metaphyseal region, near the physis. They are not primarily epiphyseal, diaphyseal, articular cartilage, or purely intramedullary lesions (though their marrow communicates with the medullary canal).
Question 18
During an intraoperative procedure to excise a symptomatic osteochondroma from the distal femur of a 19-year-old patient, the surgeon notes a distinct cap of mature-appearing cartilage covering the bony projection. What other key feature should the surgeon observe to confirm the benign nature and complete excision of the osteochondroma?
View Answer & Explanation
Correct Answer: C
Rationale: A critical feature of an osteochondroma, both radiographically and intraoperatively, is the continuity of its cortex and medullary bone with the underlying parent bone. This confirms its origin and helps ensure complete removal at the base. While a clear plane of dissection is desirable, and a smooth cartilage cap is typical, the cortical continuity is a defining characteristic. Periosteal stripping and vascular supply are not primary diagnostic features for confirming the nature of the lesion during excision.
Question 19
A gross pathology specimen of an excised bony lesion from a 13-year-old patient reveals a stalked bony projection covered by a distinct, glistening cap. Upon sectioning, the marrow space within the projection is observed to be continuous with the marrow space of the parent bone. What is the composition of the glistening cap?
View Answer & Explanation
Correct Answer: B
Rationale: Osteochondromas are characterized by a cartilage cap, which is composed of hyaline cartilage. This cap is responsible for the growth of the lesion through enchondral ossification, mimicking a physis. Fibrous tissue, adipose tissue, dense connective tissue, or immature woven bone are not the primary components of the cap.
Question 20
A 6-year-old boy with multiple osteochondromatosis is noted to have progressive genu valgum and ankle valgus deformities. These deformities are a common consequence of multiple osteochondromas located near:
View Answer & Explanation
Correct Answer: D
Rationale: Patients with multiple osteochondromatosis or with lesions close to physes frequently have developmental deformity. The presence of osteochondromas near growth plates can disrupt normal enchondral ossification, leading to angular deformities and limb length discrepancies, such as genu valgum or ankle valgus. Lesions near joint capsules, muscle insertions, tendon sheaths, or articular surfaces are more likely to cause pain or mechanical impingement rather than growth deformities.
Question 21
A 40-year-old male presents with a long-standing, previously stable osteochondroma on his proximal humerus. He reports that the lesion has recently increased in size and become painful. Which of the following findings, in conjunction with his symptoms, would raise the highest suspicion for malignant transformation?
View Answer & Explanation
Correct Answer: C
Rationale: Continued growth of an osteochondroma after skeletal maturity is a significant warning sign for malignant degeneration to a low-grade chondrosarcoma. While an adventitial bursa and palpable tenderness can cause pain, they are benign complications. A fracture through the stalk causes sudden pain but is not a sign of malignancy. A cartilage cap thickness of 0.5 cm is within the normal benign range; malignant transformation is typically associated with a cap >1-2 cm.
Question 22
A 10-year-old boy is diagnosed with a solitary osteochondroma of the distal tibia. His parents ask about the fundamental nature of this lesion. You explain that an osteochondroma is best characterized as a:
View Answer & Explanation
Correct Answer: C
Rationale: An osteochondroma is fundamentally a benign cartilage-capped bony projection arising from the external surface of the bone. It is not a primary malignant tumor, nor does it arise within the medullary canal (like an enchondroma), replace bone with fibrous tissue (like fibrous dysplasia), or present as a simple cyst. This definition encompasses its key morphological and histological features.
Question 23
A 14-year-old male presents with a painless bony mass on his proximal femur. Radiographs show a pedunculated lesion with cortical and medullary continuity. Which of the following is NOT a typical characteristic or complication of an osteochondroma?
View Answer & Explanation
Correct Answer: C
Rationale: The risk of malignant transformation of a solitary osteochondroma is small, typically less than 1%. A high risk of malignant transformation (>10%) is incorrect and would be a significant overestimation. Autosomal dominant inheritance is characteristic of multifocal osteochondromatosis. Growth away from the joint, potential for nerve compression, and histological resemblance to a physis are all typical characteristics or complications of osteochondromas.
Question 24
A 12-year-old boy has an asymptomatic osteochondroma of the distal femur, discovered incidentally on radiographs for a minor injury. The lesion is small, and there are no signs of compression or deformity. What is the most appropriate management for this patient?
View Answer & Explanation
Correct Answer: C
Rationale: Asymptomatic osteochondromas, especially in children, often require no intervention other than observation and reassurance. Surgical excision is reserved for symptomatic lesions (pain, nerve compression, deformity) or those with signs of malignant transformation. MRI surveillance is not routinely indicated for asymptomatic benign lesions. Chemotherapy and radiation therapy are treatments for malignancy and are not applicable here.
Question 25
A 16-year-old female presents with a firm, non-tender mass on her distal tibia. Radiographs show a bony projection with a broad base, exhibiting cortical and medullary continuity with the parent bone. This type of osteochondroma, lacking a distinct stalk, is specifically termed:
View Answer & Explanation
Correct Answer: B
Rationale: Osteochondromas can be classified by their morphology as either pedunculated (having a stalk) or sessile (having a broad base). The description of a bony projection with a broad base directly corresponds to a sessile osteochondroma. Intracortical, juxtacortical, and subperiosteal describe other locations or types of lesions, not the specific morphology of an osteochondroma's base.
Question 26
A 15-year-old male presents with a slowly growing, painless mass near his knee. Physical examination reveals a firm, fixed lesion on the distal femur. Radiographs show a bony projection with cortical and medullary continuity with the underlying femur, growing away from the joint. What is the most common age range for presentation of such lesions?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical text states that "Most patients present in the first three decades." This makes the first three decades the most common age range for presentation. The other options are less common or incorrect. The main distractor, "Fourth to fifth decades," is incorrect as the majority present earlier.
Question 27
A 12-year-old girl undergoes excision of a benign bony lesion from her proximal tibia. Histological examination of the resected specimen is performed. What histological feature is characteristic of an osteochondroma?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Histologically, osteochondromas resemble physes (enchondral ossification)." This is a key diagnostic feature. The main distractor, "Resemblance to mature articular cartilage," is incorrect because while it has a cartilage cap, the internal structure and growth mechanism resemble a physis.
Question 28
A 10-year-old boy presents with a palpable mass on the distal femur. Radiographs confirm an osteochondroma. Based on typical growth patterns, in which direction would this lesion most likely grow?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 8.31 a, b states, "Lesions typically grow away from the joint." This is a characteristic growth pattern of osteochondromas. The main distractor, "Towards the joint space," is incorrect as this is contrary to the typical growth pattern.
Question 29
A 7-year-old girl is diagnosed with multiple osteochondromatosis, presenting with several bony deformities. Her parents are concerned about the genetic implications for future children. What is the inheritance pattern for multifocal osteochondromatosis?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 8.33 explicitly states, "This represents an autosomal dominant inheritance." The main distractor, "Autosomal recessive," is incorrect as the condition is inherited in an autosomal dominant manner.
Question 30
A 28-year-old male presents with progressive numbness and tingling in the sole of his foot and weakness in ankle plantarflexion. Physical examination reveals a palpable mass in the popliteal fossa. Imaging confirms an osteochondroma originating from the posterior aspect of the distal femur. Which nerve is most likely being compressed by this lesion?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical context for Fig. 8.34 states, "Patient presented with symptoms related to compression of the tibial nerve." The symptoms described (numbness/tingling in sole, weakness in plantarflexion) are consistent with tibial nerve compression in the popliteal fossa. The main distractor, "Common peroneal nerve," would typically present with foot drop and sensory loss over the dorsum of the foot, which is not described.
Question 31
A 14-year-old boy presents with a firm, non-tender mass on his proximal humerus. Radiographs show a bony exostosis. What is the radiographic hallmark that confirms the diagnosis of an osteochondroma?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context for Fig. 8.31 a, b explicitly states, "This lesion demonstrates cortical and medullary continuity between the lesion and parent bone that is a radiographic hallmark of osteochondroma." The main distractor, "A purely lytic lesion with a sclerotic rim," describes features of other benign bone lesions but not an osteochondroma.
Question 32
A 9-year-old girl is found to have a bony growth on her distal radius during a routine physical examination. It is asymptomatic. What is the fundamental nature of an osteochondroma?
View Answer & Explanation
Correct Answer: B
Rationale: The first sentence of the text defines osteochondromas as "benign cartilage capped bony projections arising from the external surface of the bone." The main distractor, "A malignant bone tumor," is incorrect as osteochondromas are benign, although they have a small risk of malignant transformation.
Question 33
A 16-year-old male with a known osteochondroma of the proximal tibia experiences sudden onset of severe pain and swelling over the lesion after a minor fall. What is the most likely cause of his acute symptoms?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Sudden pain may be due to a fracture through the stalk." This aligns with the patient's acute symptoms following trauma. The main distractor, "Malignant degeneration of the lesion," typically presents with continued growth after skeletal maturity or increasing cartilage cap thickness, not usually sudden pain after minor trauma.
Question 34
A 35-year-old male, who has had an asymptomatic osteochondroma on his distal femur since adolescence, is concerned about its long-term prognosis. What is the approximate risk of malignant transformation of a solitary osteochondroma?
View Answer & Explanation
Correct Answer: C
Rationale: The text specifies, "There is a small (less than 1%) risk of transformation to a low-grade chondrosarcoma." The main distractor, "5-10%," is significantly higher than the stated risk.
Question 35
A 45-year-old male presents with a previously stable osteochondroma on his proximal tibia that has recently started to grow and become painful. Imaging reveals an increase in the size of the cartilage cap. What cartilage cap thickness is a concerning sign for malignant degeneration?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Lesions that continue to grow after skeletal maturity and that have cartilage caps greater than 1–2 cm should be examined carefully for malignant degeneration." The main distractor, "0.5-1.0 cm," is generally considered within the benign range for cartilage cap thickness in adults.
Question 36
A 30-year-old woman, skeletally mature, reports that a previously stable osteochondroma on her distal femur has recently increased in size. She denies any acute trauma or new pain. What is this continued growth after skeletal maturity a concerning indicator of?
View Answer & Explanation
Correct Answer: C
Rationale: The text indicates, "Lesions that continue to grow after skeletal maturity... should be examined carefully for malignant degeneration." The main distractor, "Normal physiological remodeling," is incorrect as osteochondromas are generally stable after skeletal maturity; continued growth is abnormal.
Question 37
An 8-year-old boy with multiple osteochondromatosis presents with progressive bowing of his forearm. Radiographs show multiple osteochondromas around the distal ulna and radius physes. What is the most likely consequence of these lesions being located close to physes?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Patients with multiple osteochondromatosis or with lesions close to physes frequently have developmental deformity." The main distractor, "Accelerated growth of the affected limb," is incorrect; lesions near physes typically cause growth disturbances leading to deformity, often shortening or angulation.
Question 38
During surgical excision of an osteochondroma from the proximal tibia of a 17-year-old patient, the surgeon observes the lesion's attachment to the underlying bone. What key feature is noted intraoperatively that confirms the diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 8.36 states, "Intraoperative photo of an osteochondroma. Note the continuity with the underlying cortex and cap of mature-appearing cartilage." This is a defining characteristic. The main distractor, "A distinct fibrous capsule separating the lesion from the bone," is incorrect as osteochondromas are characterized by continuity with the parent bone's cortex and marrow.
Question 39
A gross pathology specimen of an excised osteochondroma from a 13-year-old patient is being examined. What feature would be observed that confirms its identity as an osteochondroma?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 8.38 states, "Gross photo of an osteochondroma. Note again the cartilage cap and the continuity between the marrow space of the osteochondroma and that of the involved bone." The main distractor, "A solid, white, cartilaginous mass with no bony component," describes a chondroma, not an osteochondroma which has both bone and cartilage components and continuity with the parent bone.
Question 40
A 20-year-old college athlete develops pain and swelling over a known osteochondroma on his distal tibia, which was previously asymptomatic. The pain is exacerbated by activity. What is the most common reason for an osteochondroma to become painful?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "They may become painful due to compression of overlying structures or due to overlying bursa formation." This is a very common cause of symptoms. The main distractor, "Malignant transformation," is a less common cause of pain, and typically presents with continued growth after skeletal maturity or increased cartilage cap thickness, rather than just pain from activity.
Question 41
A 10-year-old boy is incidentally found to have a small osteochondroma on his proximal femur during an MRI for an unrelated hip injury. He has no pain or functional limitations related to the lesion. What is the typical clinical presentation of most osteochondromas?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Osteochondromas are benign cartilage capped bony projections arising from the external surface of the bone that are often asymptomatic." The main distractor, "Rapidly growing, painful mass," describes a more aggressive lesion, which is not typical for an asymptomatic osteochondroma.
Question 42
A 16-year-old male presents with a firm, non-tender mass on the anterior aspect of his distal tibia. Radiographs confirm an osteochondroma. From which part of the bone do osteochondromas typically arise?
View Answer & Explanation
Correct Answer: D
Rationale: The text states, "Osteochondromas are benign cartilage capped bony projections arising from the external surface of the bone." The main distractor, "The medullary canal," is incorrect as osteochondromas are exophytic lesions, growing outwards from the bone surface.
Question 43
A pathologist is reviewing a biopsy of a bony lesion from a 14-year-old patient. The report notes features of enchondral ossification. This process is characteristic of which type of benign bone tumor?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states, "Histologically, osteochondromas resemble physes (enchondral ossification)." The main distractor, "Enchondroma," is a cartilaginous tumor that grows within the medullary cavity, but its histological resemblance is not specifically to physes in the same manner as an osteochondroma.
Question 44
A 50-year-old male, who completed skeletal maturity decades ago, presents with a previously stable osteochondroma on his proximal humerus that has recently shown significant growth. What is the primary concern in this patient's presentation?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Lesions that continue to grow after skeletal maturity... should be examined carefully for malignant degeneration." This is the most significant concern in a skeletally mature patient with a growing osteochondroma. The main distractor, "Development of an overlying bursitis," while a possible complication, is not the primary concern when there is significant growth after skeletal maturity, which points towards malignant transformation.
Question 45
A 28-year-old male presents with chronic low back pain for 6 months. He reports the pain is worse with rest and improves with activity. Physical examination reveals limited lumbar spine range of motion.
View Answer & Explanation
Correct Answer: D
Rationale: The text states that the age at onset for Ankylosing Spondylitis ranges from adolescence to age 35 years, with a peak around 28 years. It also notes a male/female frequency of 3–5/1, indicating a strong male predominance. Therefore, a 28-year-old male fits the typical demographic profile most closely. Option B (Male, age 15) is within the age range but 28 is the peak. Option E (Male, age 45) is outside the typical age of onset range.
Question 46
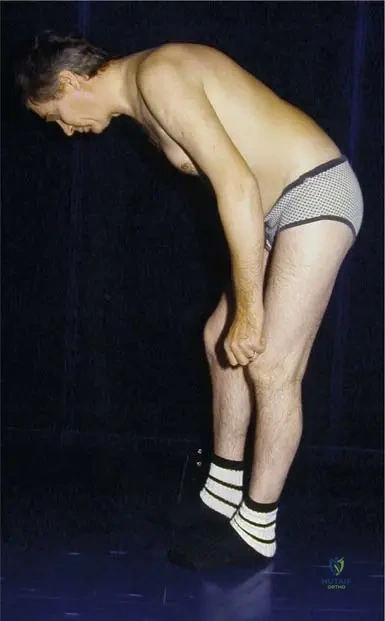
A 25-year-old male presents with a 4-month history of insidious onset low back pain that improves with exercise. On physical examination, his lumbar spine range of motion is limited.

View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 3.30 explicitly states: "Apart from back pain, the first clinical symptom in the AS, limited chest expansion, less than 1 in. at forced inhale." While other options like uveitis (A) or cardiac involvement (E) are extra-articular manifestations, they are not described as the *first* clinical symptom apart from back pain. Limited hip range of motion (B) and peripheral joint arthritis (D) are articular manifestations but not the first described symptom after back pain.
Question 47
A 30-year-old male presents with chronic low back pain for 5 months. He notes the pain is worse in the morning and improves after he exercises. Physical examination shows limited lumbar spine movement. Radiographs of the pelvis reveal bilateral grade 3 sacroileitis.
View Answer & Explanation
Correct Answer: D
Rationale: The Modified New York criteria for the diagnosis of AS include: (1) Low-back pain of more than 3 months’ duration/improved by exercise and not relieved by rest, (2) Limitation of movement of lumbar spine in sagittal and frontal planes, (3) Chest expansion decreased relative to normal values for age and sex, and (4) Bilateral sacroileitis, grade 2–4, or unilateral sacroileitis, grade 3–4. Unilateral sacroileitis, grade 1, is not a diagnostic criterion; it must be grade 3-4 for unilateral involvement. Options A, B, C, and E are all correct criteria.
Question 48
A 22-year-old male presents with a 6-month history of inflammatory back pain. He has a family history of similar symptoms. Initial workup is being considered.
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states: "AS is characterized by a close association with the HLA-B27 antigen, which is found in more than 90% of the patients." HLA-DR4 (A) is associated with Rheumatoid Arthritis, as are Rheumatoid Factor (C) and Anti-CCP antibody (D). ANA (E) is associated with systemic lupus erythematosus and other autoimmune conditions, but not specifically AS.
Question 49
A 32-year-old male presents with chronic low back pain. Radiographs of the pelvis are obtained.

View Answer & Explanation
Correct Answer: B
Rationale: The Modified New York criteria for the diagnosis of AS specify "Bilateral sacroileitis, grade 2–4, or unilateral sacroileitis, grade 3–4." The image (Fig. 3.31a) shows bilateral grade 2-3 sacroileitis, which falls within the 2-4 range. Grade 1 (A) is typically considered too mild for a definitive bilateral diagnosis according to these criteria. Grade 0 (C) indicates no sacroileitis, and Grade 5 (D) is not a standard grading in this context.
Question 50
A 35-year-old male with a known history of Ankylosing Spondylitis presents for a routine follow-up. He reports no new musculoskeletal symptoms but mentions recent eye irritation.
View Answer & Explanation
Correct Answer: C
Rationale: The text states: "less frequently, inflammatory lesions of extraarticular organs such as eye and heart may occur." This directly identifies the eye and heart as potential extra-articular manifestations. While other organs can be affected in various systemic diseases, the provided text specifically mentions the eye and heart in the context of AS. Lungs (B) can be affected in advanced AS, but eye and heart are explicitly listed as extra-articular organs in the initial description.
Question 51
A 40-year-old male with long-standing Ankylosing Spondylitis presents with increasing spinal stiffness. A thoracic spine radiograph is obtained.
View Answer & Explanation
Correct Answer: C
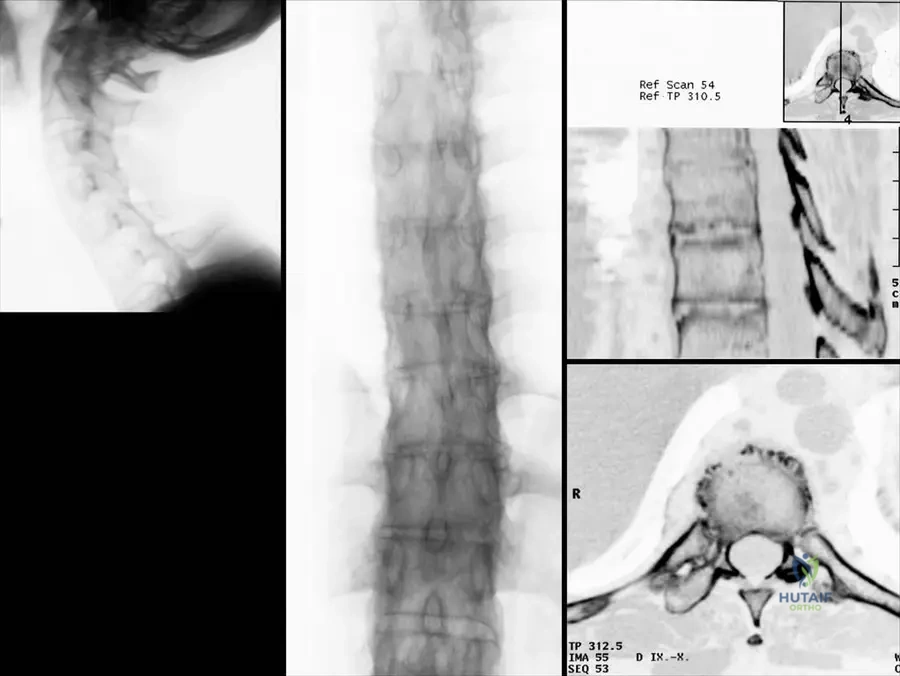
Rationale: The clinical context for Fig. 3.34b explicitly describes the image as showing "Typical “bamboo” appearance of the thoracic vertebral column." This appearance is due to the widespread syndesmophyte formation and fusion of the vertebral bodies. Romanus lesion (A) refers to erosions at the vertebral body corners, which are early changes, not the overall fused appearance. Andersson lesion (B) refers to inflammatory lesions in the vertebral bodies or discs. Dagger sign and Trolley track sign are also radiographic findings in AS but describe different aspects (ossification of supraspinous/interspinous ligaments and facet joint fusion, respectively) and are not the specific term used for the overall appearance of the thoracic column in the text.
Question 52
A 50-year-old male with advanced Ankylosing Spondylitis undergoes a CT scan of his lumbar spine due to increasing rigidity.
View Answer & Explanation
Correct Answer: C
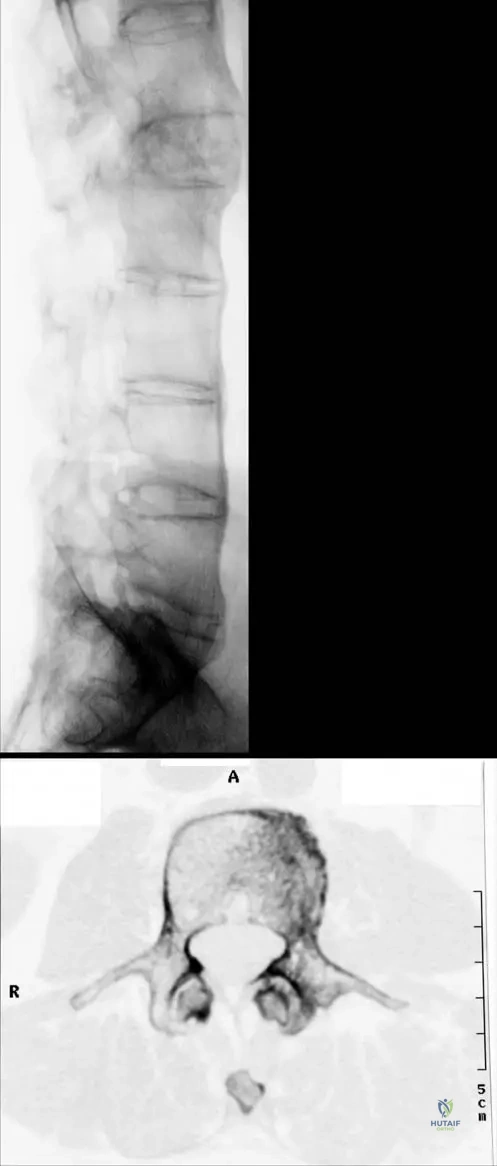
Rationale: The clinical context for Fig. 3.35a describes "Typical marginal syndesmophytes." The context for Fig. 3.34c further clarifies that "Reconstruction CT picture reveals erosions of the end-plates of the vertebral bodies and marginal syndesmophytes." Syndesmophytes are characteristic bony outgrowths that bridge vertebral bodies, leading to spinal fusion. They are distinct from osteophytes (A), which are degenerative. While they involve ligamentous ossification, "bony outgrowths from the vertebral body corners" (C) is the most accurate description of their appearance and consequence. Enthesitis (E) is the inflammation at ligament/tendon insertions, which can lead to syndesmophytes, but the syndesmophyte itself is the bony outgrowth.
Question 53
A 60-year-old male with a long history of poorly managed Ankylosing Spondylitis presents with severe functional limitations.
- A) Cervical fixation in flexion
- B) Pronounced dorsal kyphosis
- C) Involution of the chest
- D) Compensatory flexion of the knees
- E)
Question 53
A 28-year-old male presents with a 6-month history of insidious onset low back pain that improves with activity and worsens with rest. Physical examination reveals limited lumbar spine movement in all planes and decreased chest expansion to less than 1 inch at forced inhale. Radiographs of the pelvis show bilateral grade 2 sacroileitis. Which of the following is considered the first clinical symptom apart from back pain in this condition?
View Answer & Explanation
Correct Answer: C
Rationale: According to the clinical context for Fig. 3.30, "Apart from back pain, the first clinical symptom in the AS, limited chest expansion, less than 1 in. at forced inhale." This is a key diagnostic feature and often an early manifestation. Peripheral joint arthritis, uveitis, cardiac valve disease, and cervical spine stiffness are later or less common manifestations, or not specifically noted as the "first" symptom apart from back pain.
Question 53
A 30-year-old male presents with chronic inflammatory back pain and stiffness. Imaging confirms sacroileitis and early syndesmophyte formation. Genetic testing is performed. Which genetic marker is most strongly associated with this condition, found in over 90% of patients?
View Answer & Explanation
Correct Answer: B
Rationale: The teaching case explicitly states, "AS is characterized by a close association with the HLA-B27 antigen, which is found in more than 90% of the patients." HLA-DR4 is associated with rheumatoid arthritis, while Rheumatoid Factor, Anti-CCP antibodies, and ANA are also associated with other autoimmune conditions and are not the primary genetic marker for Ankylosing Spondylitis.
Question 53
A 25-year-old male presents with persistent low back pain. Radiographs of the pelvis are obtained, revealing bilateral grade 2–3 sacroileitis with sclerosis and erosions. Which of the following imaging modalities is most sensitive for detecting early sacroileitis, particularly before changes are evident on plain radiographs?
View Answer & Explanation
Correct Answer: C
Rationale: While plain radiographs can show sacroileitis (as seen in Fig. 3.31a, b), MRI (Fig. 3.31c) is generally considered the most sensitive imaging modality for detecting early inflammatory changes in the sacroiliac joints, such as bone marrow edema, before structural changes like erosions and sclerosis become apparent on plain radiographs or CT. CT is good for bony detail but less sensitive for early inflammation than MRI. Bone scintigraphy is less specific, and ultrasound is not typically used for sacroiliac joint assessment.
Question 53
A 45-year-old male with a long history of Ankylosing Spondylitis presents with severe spinal stiffness. Lateral radiographs of his thoracic spine show extensive ossification of the anterior longitudinal ligament and annulus fibrosus, leading to a characteristic appearance. What is this radiographic appearance commonly referred to as?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 3.34b specifically labels the image as "Typical 'bamboo' appearance of the thoracic vertebral column." This term describes the extensive syndesmophyte formation and ossification that fuses the vertebral bodies, resembling a bamboo stalk. Romanus lesions (erosions at vertebral body corners), Andersson lesions (disc space inflammation/erosion), Dagger sign (ossification of supraspinous and interspinous ligaments), and Shiny corner sign (sclerosis at vertebral body corners) are other radiographic findings in AS but do not describe the overall fused spinal appearance.
Question 53
A 32-year-old male diagnosed with Ankylosing Spondylitis reports new onset eye redness and pain. On examination, he is found to have uveitis. Which of the following extra-articular organs is also frequently involved in AS, as mentioned in the clinical text?
View Answer & Explanation
Correct Answer: D
Rationale: The teaching case states, "less frequently, inflammatory lesions of extraarticular organs such as eye and heart may occur." While uveitis (eye involvement) is a known extra-articular manifestation, the heart is also mentioned as another organ that can be affected. The lungs, kidneys, brain, and liver are not specifically mentioned as frequently involved extra-articular organs in the provided text.
Question 53
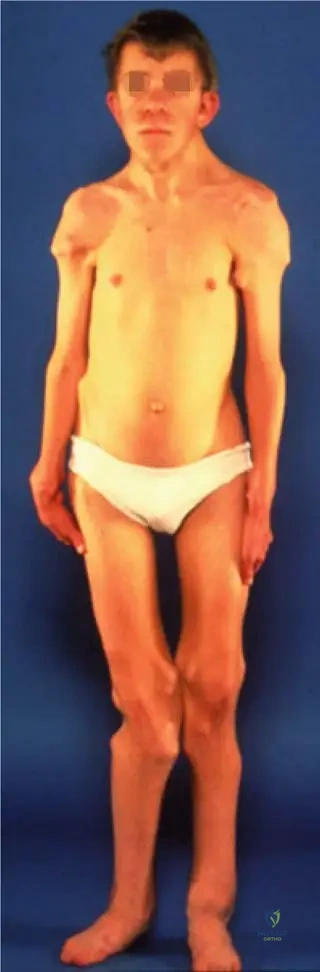
A 60-year-old male with long-standing, poorly managed Ankylosing Spondylitis presents with significant functional limitations. His physical examination reveals a fixed flexed cervical spine, a pronounced dorsal kyphosis, and compensatory flexion of the knees, making it difficult for him to see straight ahead. What is this characteristic posture indicative of?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 3.38 explicitly describes this as "Typical posture of patient with advanced AS: Cervical fixation in flexion, pronounced dorsal kyphosis, involution of the chest, and compensatory flexion of the knees." This posture is a hallmark of severe, progressive disease, often due to insufficient physiotherapy management, and is not indicative of early or mild disease, nor is it a rare complication.
Question 53
A 22-year-old male reports chronic low back pain for the past 4 months. He notes that the pain is worse in the mornings and after periods of inactivity, but it improves significantly with exercise and physical activity. He denies any history of trauma. Which characteristic of his back pain is a key diagnostic criterion for Ankylosing Spondylitis?
View Answer & Explanation
Correct Answer: C
Rationale: One of the Modified New York criteria for the diagnosis of AS is: "(1) Low-back pain of more than 3 months’ duration/improved by exercise and not relieved by rest." This distinguishes inflammatory back pain from mechanical back pain, which typically worsens with activity and improves with rest. Radiating pain is more indicative of radiculopathy, and acute onset after injury suggests trauma.
Question 53
A 38-year-old male with a known history of Ankylosing Spondylitis undergoes a lateral radiograph of his lumbar spine. The image reveals characteristic bony outgrowths bridging the vertebral bodies, originating from the outer fibers of the annulus fibrosus. What are these specific bony formations called?
View Answer & Explanation
Correct Answer: B
Rationale: Fig. 3.35a explicitly labels these as "Typical marginal syndesmophytes." Syndesmophytes are characteristic of spondyloarthropathies like AS, representing ossification within the annulus fibrosus, leading to spinal fusion. Osteophytes are typically seen in degenerative disc disease, enthesophytes refer to ossification at tendon/ligament insertions, spondylophytes is a general term for bony outgrowths, and Schmorl's nodes are intravertebral disc herniations.
Question 53
A 29-year-old male is diagnosed with Ankylosing Spondylitis. The disease is described as an inflammatory condition characterized by ascending and progressive inflammation of spinal joints. What is the ultimate end-stage outcome of this progressive inflammation in the spine?
View Answer & Explanation
Correct Answer: C
Rationale: The definition of Ankylosing Spondylitis in the text states it is "characterized by ascending and progressive inflammation of spinal joints and adjacent structures, with bony fusion of the spine in the end stage." While other spinal issues might occur, bony fusion is the defining end-stage outcome of the inflammatory process in AS. Spinal stenosis, disc herniation, osteoporosis, and scoliosis are not the primary end-stage outcome described for the inflammatory process itself.
Question 53
A 33-year-old male with a 10-year history of Ankylosing Spondylitis presents with increasing pain and stiffness in his right hip. Physical examination reveals limited range of motion in the hip. Based on the clinical text, what is the approximate frequency of hip and shoulder involvement in AS cases?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states, "In one third of cases, hips and shoulders may become involved." This indicates a significant, but not universal, involvement of these peripheral joints. The other options are incorrect based on the provided text.
Question 53
A 26-year-old male presents with chronic back pain. During his physical examination, the physician measures his chest expansion, which is found to be less than 1 inch at forced inhale. This finding is considered a diagnostic criterion for Ankylosing Spondylitis. What is the specific criterion related to chest expansion?
View Answer & Explanation
Correct Answer: C
Rationale: One of the Modified New York criteria for the diagnosis of AS is: "(3) Chest expansion decreased relative to normal values for age and sex." Fig. 3.30 further illustrates this by stating "limited chest expansion, less than 1 in. at forced inhale." The other options describe findings inconsistent with AS or are not part of the diagnostic criteria.
Question 53
A 40-year-old male with advanced Ankylosing Spondylitis undergoes a CT scan of his thoracic spine. The scan reveals erosions of the end-plates of the vertebral bodies and marginal syndesmophytes. What is the significance of these end-plate erosions in the context of AS?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 3.34c shows "Reconstruction CT picture reveals erosions of the end-plates of the vertebral bodies and marginal syndesmophytes." These erosions (Romanus lesions or "shiny corners" on plain film) are inflammatory lesions at the vertebral body corners where the annulus fibrosus attaches, and they are considered precursors to the formation of syndesmophytes, which eventually lead to spinal fusion. They are not primarily signs of degenerative disease, osteoporosis, or infection.
Question 53
A physician is reviewing the demographics of Ankylosing Spondylitis. A 28-year-old male is diagnosed with the condition. What is the typical male to female frequency ratio for AS?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states, "Male/Female frequency: 3–5/1". This indicates a clear male predominance in the incidence of Ankylosing Spondylitis. The other ratios are incorrect based on the provided text.
Question 53
A 20-year-old male presents with symptoms suggestive of Ankylosing Spondylitis. His symptoms began around age 18. What is the typical age range for the onset of AS, with a peak incidence around 28 years?
View Answer & Explanation
Correct Answer: B
Rationale: The teaching case specifies the "age at onset range from adolescence to age 35 years, peak around 28 years." This makes adolescence to age 35 the correct typical age range for disease onset. The other age ranges are outside this typical window.
Question 53
A 30-year-old patient is diagnosed with Ankylosing Spondylitis. The physician explains that it is an inflammatory disease of unknown etiology. What is the primary characteristic of this disease process?
View Answer & Explanation
Correct Answer: C
Rationale: The definition provided in the text states, "Ankylosing spondylitis (AS)... is an inflammatory disease of unknown etiology characterized by ascending and progressive inflammation of spinal joints and adjacent structures, with bony fusion of the spine in the end stage." This directly describes the primary characteristic. The other options describe features of other joint diseases (e.g., osteoarthritis, rheumatoid arthritis, gout, osteomyelitis).
Question 53
A 55-year-old male with advanced Ankylosing Spondylitis undergoes a CT scan of his lumbar spine due to severe stiffness. The CT scan reveals bony union of the lumbar facet joints. What is the significance of this finding in AS?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 3.35b shows a "CT scan of the lumbar spine: Bony union of the lumbar facet joints." This bony fusion of the facet joints is a characteristic pathological feature of advanced Ankylosing Spondylitis, contributing significantly to the severe spinal stiffness and immobility seen in the disease. It is not a normal age-related change, a sign of infection, or a rare finding, but rather a direct consequence of the inflammatory process.
Question 53
A 27-year-old male presents with chronic inflammatory back pain. Radiographs of his pelvis show unilateral grade 3 sacroileitis. According to the Modified New York criteria for the diagnosis of AS, what is the significance of this finding?
View Answer & Explanation
Correct Answer: B
Rationale: The Modified New York criteria for AS state: "(4) Bilateral sacroileitis, grade 2–4, or unilateral sacroileitis, grade 3–4." Therefore, unilateral grade 3 sacroileitis meets the radiographic criterion. While HLA-B27 is highly associated, it is not an explicit part of the Modified New York *radiographic* criterion itself, which focuses on the imaging findings.
Question 53
A 48-year-old male with long-standing Ankylosing Spondylitis experiences increasing difficulty with deep breathing. A CT scan of his thoracic spine is performed, revealing bony fusion of the costovertebral joints. What is the clinical implication of this specific finding?
View Answer & Explanation
Correct Answer: B
Rationale: Fig. 3.34d shows a "CT scan of a thoracic vertebra with bony fusion of the costovertebral joint." The costovertebral joints connect the ribs to the thoracic vertebrae, and their fusion directly restricts rib movement, thereby contributing to the decreased chest expansion, which is a hallmark clinical symptom and diagnostic criterion of AS. It is not directly related to neuropathy, hip pain, or spinal fracture risk, and it is certainly not asymptomatic in terms of respiratory mechanics.
Question 53
A 31-year-old male is diagnosed with Ankylosing Spondylitis. The disease is characterized by progressive inflammation of spinal joints. Which of the following best describes the ultimate pathological outcome of this chronic inflammation in the spine?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case defines AS as an inflammatory disease "with bony fusion of the spine in the end stage." This bony fusion is also known as bony ankylosis, where joints become stiff and immobile due to bone growth across the joint space. While other issues might arise, bony ankylosis is the defining pathological outcome of the inflammatory process in AS. Cartilage degeneration is more typical of osteoarthritis, ligamentous laxity is not characteristic, muscle atrophy is a secondary effect, and nerve root compression is a potential complication but not the primary pathological outcome of the inflammation itself.
Question 53
A 50-year-old male with advanced Ankylosing Spondylitis presents with a severely stooped posture, unable to look forward without compensatory knee flexion. His medical history indicates inconsistent adherence to physical therapy. According to the clinical text, what is a significant contributing factor to this severe fixed posture?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context for Fig. 3.38 states, "At insufficient physiotherapy management, the patient neck and trunk is fixed in a fully bent position, so that he can not see ahead." This highlights the critical role of physiotherapy in managing the progression of spinal deformity in AS. While the disease itself causes the fusion, proper management can mitigate the severity of the fixed posture. The other options are not mentioned as direct contributing factors to this specific postural outcome in the provided text.
Question 54
A 28-year-old male presents with a 6-month history of insidious onset low back pain that improves with activity and worsens with rest. Physical examination reveals limited lumbar spine movement in all planes and decreased chest expansion to less than 1 inch at forced inhale. Radiographs of the pelvis show bilateral grade 2 sacroileitis. Which of the following is considered the first clinical symptom apart from back pain in this condition?
View Answer & Explanation
Correct Answer: C
Rationale: According to the clinical context for Fig. 3.30, "Apart from back pain, the first clinical symptom in the AS, limited chest expansion, less than 1 in. at forced inhale." This is a key diagnostic feature and often an early manifestation. Peripheral joint arthritis, uveitis, cardiac valve disease, and cervical spine stiffness are later or less common manifestations, or not specifically noted as the "first" symptom apart from back pain.
Question 55
A 30-year-old male presents with chronic inflammatory back pain and stiffness. Imaging confirms sacroileitis and early syndesmophyte formation. Genetic testing is performed. Which genetic marker is most strongly associated with this condition, found in over 90% of patients?
View Answer & Explanation
Correct Answer: B
Rationale: The teaching case explicitly states, "AS is characterized by a close association with the HLA-B27 antigen, which is found in more than 90% of the patients." HLA-DR4 is associated with rheumatoid arthritis, while Rheumatoid Factor, Anti-CCP antibodies, and ANA are also associated with other autoimmune conditions and are not the primary genetic marker for Ankylosing Spondylitis.
Question 56
A 25-year-old male presents with persistent low back pain. Radiographs of the pelvis are obtained, revealing bilateral grade 2–3 sacroileitis with sclerosis and erosions. Which of the following imaging modalities is most sensitive for detecting early sacroileitis, particularly before changes are evident on plain radiographs?
View Answer & Explanation
Correct Answer: C
Rationale: While plain radiographs can show sacroileitis (as seen in Fig. 3.31a, b), MRI (Fig. 3.31c) is generally considered the most sensitive imaging modality for detecting early inflammatory changes in the sacroiliac joints, such as bone marrow edema, before structural changes like erosions and sclerosis become apparent on plain radiographs or CT. CT is good for bony detail but less sensitive for early inflammation than MRI. Bone scintigraphy is less specific, and ultrasound is not typically used for sacroiliac joint assessment.
Question 57
A 45-year-old male with a long history of Ankylosing Spondylitis presents with severe spinal stiffness. Lateral radiographs of his thoracic spine show extensive ossification of the anterior longitudinal ligament and annulus fibrosus, leading to a characteristic appearance. What is this radiographic appearance commonly referred to as?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 3.34b specifically labels the image as "Typical 'bamboo' appearance of the thoracic vertebral column." This term describes the extensive syndesmophyte formation and ossification that fuses the vertebral bodies, resembling a bamboo stalk. Romanus lesions (erosions at vertebral body corners), Andersson lesions (disc space inflammation/erosion), Dagger sign (ossification of supraspinous and interspinous ligaments), and Shiny corner sign (sclerosis at vertebral body corners) are other radiographic findings in AS but do not describe the overall fused spinal appearance.
Question 58
A 32-year-old male diagnosed with Ankylosing Spondylitis reports new onset eye redness and pain. On examination, he is found to have uveitis. Which of the following extra-articular organs is also frequently involved in AS, as mentioned in the clinical text?
View Answer & Explanation
Correct Answer: D
Rationale: The teaching case states, "less frequently, inflammatory lesions of extraarticular organs such as eye and heart may occur." While uveitis (eye involvement) is a known extra-articular manifestation, the heart is also mentioned as another organ that can be affected. The lungs, kidneys, brain, and liver are not specifically mentioned as frequently involved extra-articular organs in the provided text.
Question 59
A 60-year-old male with long-standing, poorly managed Ankylosing Spondylitis presents with significant functional limitations. His physical examination reveals a fixed flexed cervical spine, a pronounced dorsal kyphosis, and compensatory flexion of the knees, making it difficult for him to see straight ahead. What is this characteristic posture indicative of?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 3.38 explicitly describes this as "Typical posture of patient with advanced AS: Cervical fixation in flexion, pronounced dorsal kyphosis, involution of the chest, and compensatory flexion of the knees." This posture is a hallmark of severe, progressive disease, often due to insufficient physiotherapy management, and is not indicative of early or mild disease, nor is it a rare complication.
Question 60
A 22-year-old male reports chronic low back pain for the past 4 months. He notes that the pain is worse in the mornings and after periods of inactivity, but it improves significantly with exercise and physical activity. He denies any history of trauma. Which characteristic of his back pain is a key diagnostic criterion for Ankylosing Spondylitis?
View Answer & Explanation
Correct Answer: C
Rationale: One of the Modified New York criteria for the diagnosis of AS is: "(1) Low-back pain of more than 3 months’ duration/improved by exercise and not relieved by rest." This distinguishes inflammatory back pain from mechanical back pain, which typically worsens with activity and improves with rest. Radiating pain is more indicative of radiculopathy, and acute onset after injury suggests trauma.
Question 61
A 38-year-old male with a known history of Ankylosing Spondylitis undergoes a lateral radiograph of his lumbar spine. The image reveals characteristic bony outgrowths bridging the vertebral bodies, originating from the outer fibers of the annulus fibrosus. What are these specific bony formations called?
View Answer & Explanation
Correct Answer: B
Rationale: Fig. 3.35a explicitly labels these as "Typical marginal syndesmophytes." Syndesmophytes are characteristic of spondyloarthropathies like AS, representing ossification within the annulus fibrosus, leading to spinal fusion. Osteophytes are typically seen in degenerative disc disease, enthesophytes refer to ossification at tendon/ligament insertions, spondylophytes is a general term for bony outgrowths, and Schmorl's nodes are intravertebral disc herniations.
Question 62
A 29-year-old male is diagnosed with Ankylosing Spondylitis. The disease is described as an inflammatory condition characterized by ascending and progressive inflammation of spinal joints. What is the ultimate end-stage outcome of this progressive inflammation in the spine?
View Answer & Explanation
Correct Answer: C
Rationale: The definition of Ankylosing Spondylitis in the text states it is "characterized by ascending and progressive inflammation of spinal joints and adjacent structures, with bony fusion of the spine in the end stage." While other spinal issues might occur, bony fusion is the defining end-stage outcome of the inflammatory process in AS. Spinal stenosis, disc herniation, osteoporosis, and scoliosis are not the primary end-stage outcome described for the inflammatory process itself.
Question 63
A 33-year-old male with a 10-year history of Ankylosing Spondylitis presents with increasing pain and stiffness in his right hip. Physical examination reveals limited range of motion in the hip. Based on the clinical text, what is the approximate frequency of hip and shoulder involvement in AS cases?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states, "In one third of cases, hips and shoulders may become involved." This indicates a significant, but not universal, involvement of these peripheral joints. The other options are incorrect based on the provided text.
Question 64
A 26-year-old male presents with chronic back pain. During his physical examination, the physician measures his chest expansion, which is found to be less than 1 inch at forced inhale. This finding is considered a diagnostic criterion for Ankylosing Spondylitis. What is the specific criterion related to chest expansion?
View Answer & Explanation
Correct Answer: C
Rationale: One of the Modified New York criteria for the diagnosis of AS is: "(3) Chest expansion decreased relative to normal values for age and sex." Fig. 3.30 further illustrates this by stating "limited chest expansion, less than 1 in. at forced inhale." The other options describe findings inconsistent with AS or are not part of the diagnostic criteria.
Question 65
A 40-year-old male with advanced Ankylosing Spondylitis undergoes a CT scan of his thoracic spine. The scan reveals erosions of the end-plates of the vertebral bodies and marginal syndesmophytes. What is the significance of these end-plate erosions in the context of AS?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 3.34c shows "Reconstruction CT picture reveals erosions of the end-plates of the vertebral bodies and marginal syndesmophytes." These erosions (Romanus lesions or "shiny corners" on plain film) are inflammatory lesions at the vertebral body corners where the annulus fibrosus attaches, and they are considered precursors to the formation of syndesmophytes, which eventually lead to spinal fusion. They are not primarily signs of degenerative disease, osteoporosis, or infection.
Question 66
A physician is reviewing the demographics of Ankylosing Spondylitis. A 28-year-old male is diagnosed with the condition. What is the typical male to female frequency ratio for AS?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states, "Male/Female frequency: 3–5/1". This indicates a clear male predominance in the incidence of Ankylosing Spondylitis. The other ratios are incorrect based on the provided text.
Question 67
A 20-year-old male presents with symptoms suggestive of Ankylosing Spondylitis. His symptoms began around age 18. What is the typical age range for the onset of AS, with a peak incidence around 28 years?
View Answer & Explanation
Correct Answer: B
Rationale: The teaching case specifies the "age at onset range from adolescence to age 35 years, peak around 28 years." This makes adolescence to age 35 the correct typical age range for disease onset. The other age ranges are outside this typical window.
Question 68
A 30-year-old patient is diagnosed with Ankylosing Spondylitis. The physician explains that it is an inflammatory disease of unknown etiology. What is the primary characteristic of this disease process?
View Answer & Explanation
Correct Answer: C
Rationale: The definition provided in the text states, "Ankylosing spondylitis (AS)... is an inflammatory disease of unknown etiology characterized by ascending and progressive inflammation of spinal joints and adjacent structures, with bony fusion of the spine in the end stage." This directly describes the primary characteristic. The other options describe features of other joint diseases (e.g., osteoarthritis, rheumatoid arthritis, gout, osteomyelitis).
Question 69
A 55-year-old male with advanced Ankylosing Spondylitis undergoes a CT scan of his lumbar spine due to severe stiffness. The CT scan reveals bony union of the lumbar facet joints. What is the significance of this finding in AS?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 3.35b shows a "CT scan of the lumbar spine: Bony union of the lumbar facet joints." This bony fusion of the facet joints is a characteristic pathological feature of advanced Ankylosing Spondylitis, contributing significantly to the severe spinal stiffness and immobility seen in the disease. It is not a normal age-related change, a sign of infection, or a rare finding, but rather a direct consequence of the inflammatory process.
Question 70
A 27-year-old male presents with chronic inflammatory back pain. Radiographs of his pelvis show unilateral grade 3 sacroileitis. According to the Modified New York criteria for the diagnosis of AS, what is the significance of this finding?
View Answer & Explanation
Correct Answer: B
Rationale: The Modified New York criteria for AS state: "(4) Bilateral sacroileitis, grade 2–4, or unilateral sacroileitis, grade 3–4." Therefore, unilateral grade 3 sacroileitis meets the radiographic criterion. While HLA-B27 is highly associated, it is not an explicit part of the Modified New York *radiographic* criterion itself, which focuses on the imaging findings.
Question 71
A 48-year-old male with long-standing Ankylosing Spondylitis experiences increasing difficulty with deep breathing. A CT scan of his thoracic spine is performed, revealing bony fusion of the costovertebral joints. What is the clinical implication of this specific finding?
View Answer & Explanation
Correct Answer: B
Rationale: Fig. 3.34d shows a "CT scan of a thoracic vertebra with bony fusion of the costovertebral joint." The costovertebral joints connect the ribs to the thoracic vertebrae, and their fusion directly restricts rib movement, thereby contributing to the decreased chest expansion, which is a hallmark clinical symptom and diagnostic criterion of AS. It is not directly related to neuropathy, hip pain, or spinal fracture risk, and it is certainly not asymptomatic in terms of respiratory mechanics.
Question 72
A 31-year-old male is diagnosed with Ankylosing Spondylitis. The disease is characterized by progressive inflammation of spinal joints. Which of the following best describes the ultimate pathological outcome of this chronic inflammation in the spine?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case defines AS as an inflammatory disease "with bony fusion of the spine in the end stage." This bony fusion is also known as bony ankylosis, where joints become stiff and immobile due to bone growth across the joint space. While other issues might arise, bony ankylosis is the defining pathological outcome of the inflammatory process in AS. Cartilage degeneration is more typical of osteoarthritis, ligamentous laxity is not characteristic, muscle atrophy is a secondary effect, and nerve root compression is a potential complication but not the primary pathological outcome of the inflammation itself.
Question 73
A 45-year-old male presents with a 6-month history of intermittent right knee swelling, progressive pain, and occasional catching. Physical examination reveals a mild effusion and limited range of motion. Plain radiographs show multiple intra-articular calcified bodies within the knee joint. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: D
Rationale: Synovial chondromatosis is characterized by intermittent swelling, effusions, progressive pain, mechanical symptoms like catching, and radiographs showing intra-articular calcified cartilaginous bodies. Rheumatoid arthritis and gout typically present with inflammatory signs and different radiographic findings (erosions, tophi). Pigmented villonodular synovitis usually presents with hemosiderin deposition and often lacks calcified bodies. Osteoarthritis is a degenerative condition, and while it can cause pain and effusions, the presence of multiple calcified intra-articular bodies points more specifically to synovial chondromatosis.
Question 74
A 38-year-old female complains of chronic left hip pain, stiffness, and a sensation of locking. Radiographs demonstrate an enlarged joint capsule with multiple calcified intra-articular bodies. Which of the following joints is *least* commonly affected by this condition?
View Answer & Explanation
Correct Answer: D
Rationale: The provided text states that synovial chondromatosis most commonly affects the knee, hip, and elbow. While it can occur in other joints, the shoulder is not listed among the most common locations, making it the least common among the options provided based on the text. All are not equally common.
Question 75
A 52-year-old male presents with a 9-month history of worsening right elbow pain, stiffness, and occasional inability to fully extend his arm. Physical exam shows decreased range of motion and palpable crepitus. Radiographs reveal multiple calcified loose bodies within the elbow joint. Which of the following is a characteristic symptom of synovial chondromatosis?
View Answer & Explanation
Correct Answer: C
Rationale: The text describes synovial chondromatosis as presenting with "intermittent swelling, effusions, and progressive pain in the involved joint. Mechanical symptoms such as stiffness, joint locking, or catching may be present." Systemic fever, bilateral involvement, acute onset severe pain, and skin rash are not characteristic features of synovial chondromatosis as described in the text.
Question 76
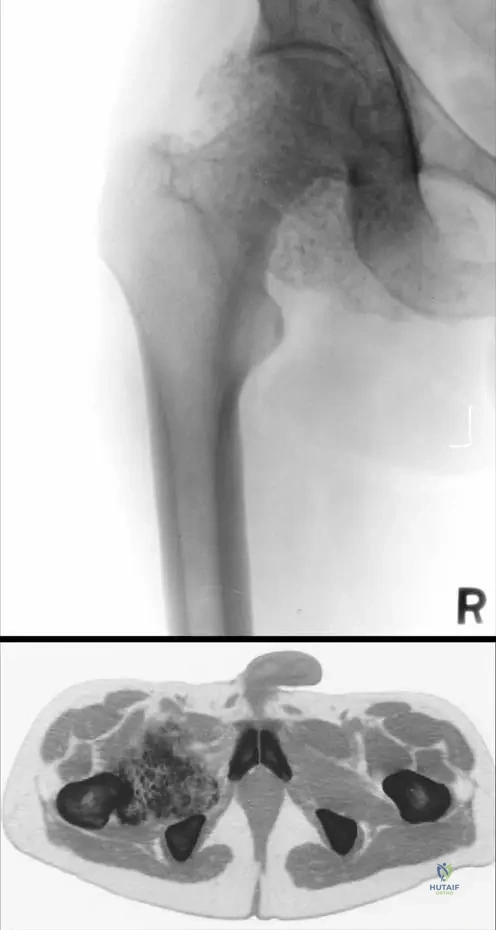
A 48-year-old patient presents with chronic left hip pain and limited range of motion. Plain radiographs and a CT scan are obtained. The CT scan reveals an enlarged joint capsule filled by a large mass of intra-articular calcified cartilaginous free bodies. This finding is highly suggestive of synovial chondromatosis. What is the primary radiographic characteristic described for this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states: "Radiographs show intra- and periarticular soft tissue masses with varying amounts of calcification." The image provided also clearly demonstrates calcified intra-articular bodies. Juxta-articular erosions and diffuse osteopenia are more characteristic of inflammatory arthropathies. Subchondral cysts can be seen in osteoarthritis but are not the primary characteristic of synovial chondromatosis, especially without calcification. Joint space narrowing is a feature of osteoarthritis, which can be secondary to synovial chondromatosis, but not its primary radiographic characteristic.
Question 77
A 55-year-old male undergoes arthroscopic synovectomy for chronic right knee pain, swelling, and mechanical symptoms. Histopathological examination of the excised synovial tissue and loose bodies is performed. What microscopic finding is characteristic of synovial chondromatosis?
View Answer & Explanation
Correct Answer: C
Rationale: The text states: "Microscopically, nodules of hyaline cartilage are seen. There may be some degree of cytologic atypia. Surrounding synovium is hyperplastic." Granulomatous inflammation is seen in conditions like tuberculosis. Hemosiderin deposition and villous hypertrophy are characteristic of pigmented villonodular synovitis. Urate crystal deposition is seen in gout. Lymphocytic infiltration and pannus formation are characteristic of rheumatoid arthritis.
Question 78
A 60-year-old patient with a long-standing history of untreated synovial chondromatosis in the left hip presents with severe pain and markedly restricted hip motion. Radiographs show significant joint space narrowing and subchondral sclerosis in addition to the calcified intra-articular bodies. What long-term complication is indicated by these findings?
View Answer & Explanation
Correct Answer: C
Rationale: The text states: "Depending on the chronicity of the process, patients may develop secondary osteoarthritic changes." The described radiographic findings of joint space narrowing and subchondral sclerosis are hallmarks of osteoarthritis. While malignant transformation is a rare theoretical concern, the text does not mention it as a common complication. Pathologic fracture, systemic amyloidosis, and septic arthritis are not described as complications of synovial chondromatosis in the provided text.
Question 79
A 40-year-old male presents with chronic right hip pain and mechanical symptoms. A CT scan of the hip is provided. Based on the image and clinical context, what is the most prominent feature observed?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 10.1 a, b explicitly states: "Note the enlarged joint capsule filled by large mass of intra-articular calcified cartilaginous free bodies." This is clearly visible on the CT scan (b). Avascular necrosis, labral tears, insufficiency fractures, and periosteal reactions are not the primary features highlighted in the image or text for synovial chondromatosis.
Question 80
A 30-year-old patient reports intermittent swelling and pain in her left knee for the past year. She denies any similar symptoms in other joints. Radiographs show multiple calcified intra-articular bodies. This condition is best described as:
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states: "It is a monoarticular process that most commonly affects the knee, hip, and elbow." It also describes it as a "benign proliferation of cartilaginous tissue." Therefore, a monoarticular proliferative process is the most accurate description. It is not described as polyarticular, systemic, septic, or a crystal arthropathy.
Question 81
A 42-year-old male presents with chronic left hip pain, stiffness, and occasional catching. He denies any fevers, chills, or systemic symptoms. Laboratory tests, including ESR and CRP, are within normal limits. Radiographs show multiple calcified intra-articular bodies. The absence of systemic inflammatory markers helps differentiate synovial chondromatosis from which of the following conditions?
View Answer & Explanation
Correct Answer: C
Rationale: The text describes synovial chondromatosis as a benign, localized process without mention of systemic inflammatory markers. Rheumatoid arthritis is a systemic autoimmune disease characterized by elevated inflammatory markers (ESR, CRP) and often presents with polyarticular involvement and erosions, which are not typical for synovial chondromatosis. Osteoarthritis, traumatic loose bodies, pigmented villonodular synovitis, and chondromalacia patellae are generally not associated with elevated systemic inflammatory markers in the same way as rheumatoid arthritis.
Question 82
A 50-year-old patient presents with a 2-year history of progressive right knee pain and swelling. Radiographs show multiple intra-articular calcifications and a moderate joint effusion. What additional radiographic finding may be present in chronic cases of synovial chondromatosis?
View Answer & Explanation
Correct Answer: B
Rationale: The text states: "Depending on the chronicity of the process, patients may develop secondary osteoarthritic changes." Osteoarthritis is characterized by joint space narrowing, subchondral sclerosis, and subchondral cysts. Periosteal new bone formation, diffuse soft tissue calcification unrelated to the joint, pathological fractures, and osteonecrosis are not described as typical chronic radiographic findings of synovial chondromatosis in the provided text.
Question 83
A biopsy of a synovial lesion from a 35-year-old patient with chronic knee pain and multiple intra-articular calcifications reveals nodules of cartilage. What specific type of cartilage is typically observed in synovial chondromatosis?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states: "Microscopically, nodules of hyaline cartilage are seen." While articular cartilage is also hyaline cartilage, the specific description in the text is "hyaline cartilage" in the context of the nodules. Fibrocartilage and elastic cartilage are distinct types of cartilage not mentioned. Calcified cartilage describes a state, not the primary type of cartilage tissue itself.
Question 84
A 47-year-old female presents with a 1-year history of intermittent right hip pain and a feeling that her hip "catches" or "locks" during certain movements. She also reports increasing stiffness. Radiographs show intra-articular calcified bodies. Which of the following symptoms is considered a "mechanical symptom" in this context?
View Answer & Explanation
Correct Answer: C
Rationale: The text states: "Mechanical symptoms such as stiffness, joint locking, or catching may be present." Intermittent swelling, progressive pain, and effusions are general symptoms but not specifically categorized as "mechanical" in the provided text. Loss of appetite is not a symptom of synovial chondromatosis.
Question 85
A 33-year-old male presents with chronic left knee pain, swelling, and a palpable mass. Radiographs confirm multiple intra-articular calcified bodies. Given the typical presentation of synovial chondromatosis, which of the following statements about its location is true?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states: "It is a monoarticular process that most commonly affects the knee, hip, and elbow." It does not exclusively affect large weight-bearing joints (elbow is not weight-bearing). It is monoarticular, not polyarticular. It does not primarily affect the small joints of the hands and feet or the axial skeleton.
Question 86
A 58-year-old patient presents with a long history of left hip pain, stiffness, and limited range of motion. Imaging reveals an enlarged joint capsule filled with numerous calcified cartilaginous bodies. Histological examination confirms synovial chondromatosis. How is this condition generally classified?
View Answer & Explanation
Correct Answer: B
Rationale: The text begins by stating: "Synovial chondromatosis is a benign proliferation of cartilaginous tissue..." It is not classified as a malignant tumor, inflammatory arthropathy, infectious process, or autoimmune disorder based on the provided text.
Question 87
A 44-year-old male presents with chronic right hip pain and limited mobility. Plain radiographs of the hip are obtained. Based on the image, what is a key radiographic finding indicative of synovial chondromatosis?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 10.1 a, b explicitly states: "Note the enlarged joint capsule filled by large mass of intra-articular calcified cartilaginous free bodies." This is clearly visible on the plain radiograph (a). Widening of the joint space is not typical. Significant osteophyte formation and subchondral lucencies can be seen in osteoarthritis, which can be secondary, but the primary finding for synovial chondromatosis is the calcified bodies within an enlarged capsule. Bone marrow edema is a finding on MRI, not plain radiographs.
Question 88
A 39-year-old female presents with chronic left knee pain, swelling, and occasional locking. Imaging reveals multiple intra-articular calcified bodies. The cartilaginous tissue in synovial chondromatosis originates from which specific tissue?
View Answer & Explanation
Correct Answer: C
Rationale: The text states: "Synovial chondromatosis is a benign proliferation of cartilaginous tissue arising in the synovium of joints, tendon sheath, and bursae." Therefore, the origin is the synovium. Articular cartilage, subchondral bone, meniscus, and ligamentous tissue are not the primary origin of the cartilaginous proliferation in this condition.
Question 89
A 65-year-old patient with a long history of synovial chondromatosis in the right elbow presents with severe limitation of elbow extension and flexion. Physical examination reveals a fixed deformity. This loss of mobility and fixed deformity is best described as:
View Answer & Explanation
Correct Answer: C
Rationale: The text states: "Over time, patients may lose mobility and develop contractures." The description of severe limitation and fixed deformity aligns with the development of contractures. Acute inflammation, septic complications, neuropathic arthropathy, and tendon rupture are not described as the specific cause of long-term loss of mobility and fixed deformity in the provided text.
Question 90
A pathologist examines a synovial biopsy from a 41-year-old patient diagnosed with synovial chondromatosis. The report notes nodules of hyaline cartilage and hyperplastic synovium. What additional microscopic feature, if present, is consistent with synovial chondromatosis?
View Answer & Explanation
Correct Answer: C
Rationale: The text states: "Microscopically, nodules of hyaline cartilage are seen. There may be some degree of cytologic atypia." Extensive necrosis, high mitotic activity, and vascular invasion would raise concerns for malignancy, which is not the primary classification of synovial chondromatosis. While calcification occurs, the text does not mention bone formation within the cartilaginous nodules as a microscopic feature.
Question 91
A 28-year-old male presents with acute right knee pain and swelling after a twisting injury. Radiographs show a single, small intra-articular loose body. This differs from synovial chondromatosis, which typically presents with:
View Answer & Explanation
Correct Answer: B
Rationale: The text and images describe synovial chondromatosis as involving "intra-articular calcified cartilaginous free bodies" and "large mass of intra-articular calcified cartilaginous free bodies." The presence of *multiple* calcified bodies is a hallmark, distinguishing it from a single traumatic loose body. A single large osteochondral fragment could be traumatic. Non-calcified synovial hypertrophy is seen in other conditions like PVNS. Absence of intra-articular bodies or rapidly progressive joint destruction are not characteristic of synovial chondromatosis.
Question 92
A 51-year-old patient presents with chronic left hip pain, intermittent swelling, and a sensation of catching. Radiographs show an enlarged joint capsule with multiple calcified intra-articular bodies. Which of the following statements best summarizes the nature of synovial chondromatosis?
View Answer & Explanation
Correct Answer: C
Rationale: The text defines synovial chondromatosis as "a benign proliferation of cartilaginous tissue arising in the synovium of joints, tendon sheath, and bursae." It is monoarticular, not systemic, and primarily cartilaginous, not bone-forming. It is not a malignant tumor or an inflammatory condition leading to cartilage erosion as its primary pathology.
Question 93
A 45-year-old male presents with chronic, progressive pain and stiffness in his right hip. He reports intermittent locking and catching sensations. Radiographs show multiple intra-articular calcified bodies and an enlarged joint capsule. A CT scan confirms a large mass of intra-articular calcified cartilaginous free bodies filling the joint capsule.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of chronic pain, stiffness, mechanical symptoms (locking/catching), and radiographic findings of multiple intra-articular calcified cartilaginous free bodies within an enlarged joint capsule are classic for synovial chondromatosis. This condition is characterized by a benign proliferation of cartilaginous tissue in the synovium that can detach and form loose bodies. Osteochondroma is a bone tumor with a cartilaginous cap, typically exophytic from bone, not intra-articular loose bodies. Pigmented villonodular synovitis presents with hemosiderin deposition and often causes effusions and erosions but typically does not produce calcified cartilaginous loose bodies. Chondrosarcoma is a malignant tumor and while it involves cartilage, its presentation and radiographic features differ significantly from the benign, multifocal loose bodies of synovial chondromatosis. Gouty arthritis involves uric acid crystal deposition and presents with acute inflammatory episodes, not calcified cartilaginous loose bodies.
Question 94
A 38-year-old female presents with a 6-month history of intermittent swelling and pain in her left knee. She occasionally experiences a sensation of something "moving" within the joint. Radiographs reveal several calcified intra-articular bodies. Which of the following is the most characteristic microscopic finding for this condition?
View Answer & Explanation
Correct Answer: B
Rationale: Synovial chondromatosis is characterized microscopically by nodules of hyaline cartilage within the synovium, which can then detach and become free bodies. The surrounding synovium is often hyperplastic. Hemosiderin-laden macrophages are characteristic of pigmented villonodular synovitis. Uric acid crystals are pathognomonic for gout. Synovial hypertrophy with lymphocytic infiltration is more typical of inflammatory arthritides like rheumatoid arthritis. Fibrous tissue with myxoid degeneration is not a primary characteristic of synovial chondromatosis.
Question 95
A 52-year-old male presents with a several-year history of worsening right elbow pain, stiffness, and a decreased range of motion. He reports occasional locking. Imaging reveals multiple calcified intra-articular bodies. Which of the following describes the typical joint involvement pattern of synovial chondromatosis?
View Answer & Explanation
Correct Answer: B
Rationale: Synovial chondromatosis is characteristically a monoarticular process, meaning it affects a single joint, and is therefore asymmetrical. It most commonly affects large joints such as the knee, hip, and elbow. Polyarticular involvement, axial skeleton involvement, or small joint involvement are not typical features of this condition. It is also not a systemic disease with widespread calcifications.
Question 96
A 48-year-old patient presents with chronic hip pain, swelling, and mechanical symptoms. Radiographs show an enlarged joint capsule filled with numerous calcified cartilaginous bodies. What is the primary tissue from which these cartilaginous bodies originate?
View Answer & Explanation
Correct Answer: D
Rationale: Synovial chondromatosis is defined as a benign proliferation of cartilaginous tissue arising in the synovium of joints, tendon sheath, and bursae. The cartilaginous bodies are formed from metaplastic changes within the synovial membrane. While they can be found in the joint, they do not originate from the articular cartilage or subchondral bone itself. The joint capsule is involved in containing the process, but the primary origin is the synovium. Tendon sheath is a possible site, but the question specifies "intra-articular" which points to synovial origin within the joint.
Question 97
A 60-year-old male with a long-standing history of synovial chondromatosis in his knee now presents with worsening pain and crepitus, along with significant loss of joint space on radiographs. What secondary change is most likely to have developed in this patient?
View Answer & Explanation
Correct Answer: C
Rationale: The presence of chronic intra-articular loose bodies and mechanical irritation from synovial chondromatosis can lead to progressive joint damage over time. The text explicitly states, "Depending on the chronicity of the process, patients may develop secondary osteoarthritic changes." Septic arthritis is an infection, avascular necrosis is bone death due to lack of blood supply, and stress fractures are related to repetitive loading, none of which are direct secondary consequences of synovial chondromatosis. While malignant transformation to chondrosarcoma is a rare complication, secondary osteoarthritis is a much more common and expected long-term sequela of chronic synovial chondromatosis.
Question 98
A 30-year-old patient presents with chronic right hip pain and mechanical symptoms. Radiographs and CT scan confirm synovial chondromatosis with numerous calcified intra-articular bodies. Which of the following is a common symptom associated with this condition?
View Answer & Explanation
Correct Answer: C
Rationale: Patients with synovial chondromatosis commonly present with intermittent swelling, effusions, and progressive pain in the involved joint. Mechanical symptoms such as stiffness, joint locking, or catching may also be present. Acute, severe, migratory polyarthritis is characteristic of conditions like rheumatic fever or viral arthritis. Systemic fever and malaise are more indicative of infection or systemic inflammatory conditions. Numbness and tingling suggest nerve impingement. Skin rash and photosensitivity are associated with autoimmune diseases like lupus. These are not typical presentations of synovial chondromatosis.
Question 99
A 40-year-old male presents with a history of recurrent left knee swelling and pain. Physical examination reveals a mild effusion and crepitus with range of motion. Radiographs show multiple intra-articular calcifications. What is the most likely composition of these calcified bodies?
View Answer & Explanation
Correct Answer: C
Rationale: Synovial chondromatosis is characterized by the proliferation of cartilaginous tissue within the synovium. These cartilaginous nodules can detach and become free bodies, which then undergo varying amounts of calcification. Therefore, the calcified bodies are primarily composed of cartilage. While they may ossify over time, their primary origin and composition are cartilaginous. Bone would suggest osteochondral fragments, fibrous tissue is not typically calcified in this manner, uric acid is gout, and calcium pyrophosphate dihydrate is pseudogout.
Question 100
A 55-year-old patient presents with chronic right hip pain and limited range of motion. Radiographs show an enlarged joint capsule with numerous calcified intra-articular bodies. The CT scan confirms these findings. Which of the following statements regarding the prognosis of synovial chondromatosis is most accurate?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Depending on the chronicity of the process, patients may develop secondary osteoarthritic changes." This indicates that synovial chondromatosis can lead to progressive joint damage over time due to the mechanical irritation from the loose bodies and the proliferative synovium. While malignant transformation to chondrosarcoma is a rare, reported complication, it is not frequent. The condition does not typically resolve spontaneously and is not self-limiting without long-term sequelae. It is a functional problem, not primarily cosmetic.
You Might Also Like