ABOS Orthopaedic Pathology Review: Bone Tumors, Infections & Synovial Lesions | Part 22
Key Takeaway
This ABOS Board Review focuses on key orthopaedic pathology topics including metastatic bone disease, acute hematogenous osteomyelitis, and synovial tumors. It covers clinical presentation, diagnostic imaging (radiographs, MRI, CT), common causative agents like Staphylococcus aureus, genetic inheritance patterns, and definitive histological diagnosis for these musculoskeletal conditions.
Question 1
A 60-year-old female presents with a 3-month history of progressive left thigh pain, which is constant and worse with weight-bearing. Radiographs show a large lytic lesion in the subtrochanteric region of the left femur. She has no known history of cancer. What is the most common malignant tumor in bones, which this presentation likely represents?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case explicitly states, "Metastases are the most common malignant tumor in bones." Given the patient's age, lytic lesion, and pain, metastatic bone disease is the most likely diagnosis, even without a known primary. The text also mentions that sometimes a bony metastasis will be the initial presentation of a tumor. Osteosarcoma and Ewing sarcoma are primary bone tumors more common in younger patients. Multiple myeloma is a differential but less common overall than metastases.
Question 2
A 57-year-old male presents with a lytic destruction of the shaft of the left humerus. A bone scan shows increased uptake in the lesion. A subsequent CT abdomen reveals a primary site in the kidney. Which of the following characteristics is most commonly associated with renal cell carcinoma metastases to bone?
View Answer & Explanation
Correct Answer: C
Rationale: While not explicitly detailed in the provided text, the image (Fig. 8.123) shows a lytic destruction of the humerus with a primary in the kidney, which is characteristic of renal cell carcinoma (RCC). RCC metastases are notoriously highly vascular, which is a critical consideration for surgical planning due to the risk of significant hemorrhage. They are typically lytic, not blastic, and can be aggressive. The text mentions kidney cancer as a frequent primary tumor. The other options are generally not characteristic of RCC bone metastases.
Question 3
A 63-year-old female with a history of lung cancer presents with new onset, severe pain in her right femur. She describes the pain as constant and worse with ambulation. Radiographs show a large lytic lesion involving more than 50% of the cortical width in the mid-diaphysis. This presentation most strongly suggests:
View Answer & Explanation
Correct Answer: C
Rationale: The vignette describes a patient with known cancer, a lytic lesion, and pain that is mechanical/activity-related, which the text states "may portend an impending pathologic fracture." A lesion involving more than 50% of the cortical width is a well-established criterion for high risk of impending fracture (Mirels' score). This is a classic presentation of an impending pathologic fracture due to metastatic disease. The other options are less likely given the history of cancer and the specific radiographic findings.
Question 4
A 70-year-old male presents with diffuse back pain and fatigue. He has no known history of cancer. Initial radiographs show multiple lytic lesions in the vertebral bodies and pelvis. Given his age and the radiographic findings, which of the following is an important differential diagnosis to consider alongside metastatic bone disease?
View Answer & Explanation
Correct Answer: D
Rationale: The teaching case states, "As these lesions tend to occur in an older age range than the primary tumors, the differential diagnosis includes myeloma and lymphoma." Multiple myeloma commonly presents with widespread lytic lesions in the axial skeleton in older patients, making it a critical differential for metastatic bone disease. Paget's disease typically has mixed lytic/blastic features and bone expansion. Fibrous dysplasia is usually solitary and in younger patients. Osteoporosis causes diffuse osteopenia but not typically discrete lytic lesions.
Question 5
A 58-year-old female with a history of thyroid cancer presents with a new painful lesion in her left tibia. Radiographs show a mixed lytic and sclerotic lesion. Which of the following statements best describes the radiographic appearance of metastatic bone disease?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case explicitly states, "The radiographic appearance of metastases is highly variable. The appearance will vary from radiolucent to radiodense; some tumors have a mixed character." This directly supports option C. Metastases are not always purely lytic or sclerotic. While some primary bone tumors can be difficult to distinguish, the variability is a key characteristic of metastases, and periosteal reaction is less common or less prominent than in many primary bone sarcomas.
Question 6
A 66-year-old male with a known history of prostate cancer presents with new onset back pain. A bone scan reveals multiple areas of increased uptake throughout the axial skeleton. Which of the following primary tumors is most commonly associated with predominantly osteoblastic (sclerotic) bone metastases?
View Answer & Explanation
Correct Answer: D
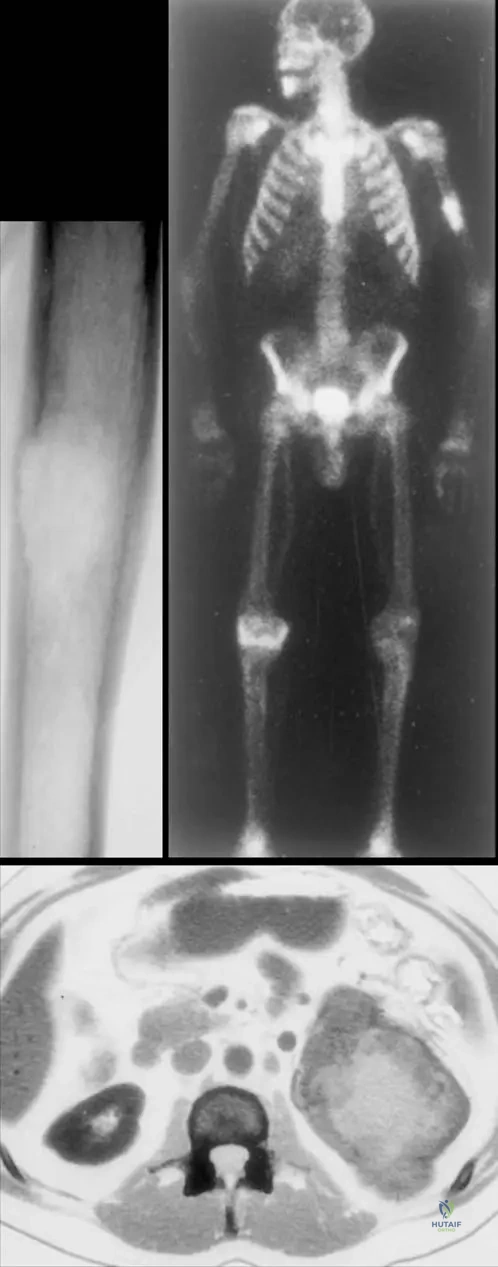
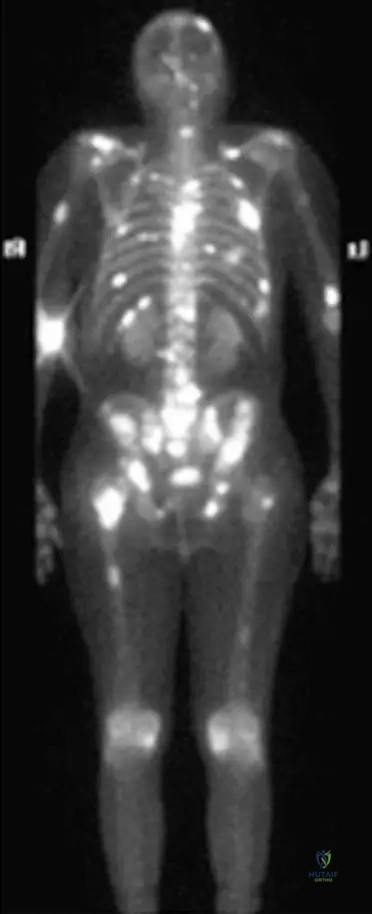
Rationale: Prostate cancer is classically known for producing predominantly osteoblastic (sclerotic) bone metastases, as often seen on bone scans like Fig. 8.122. While breast cancer can be mixed or blastic, it is more commonly lytic. Lung, kidney, and thyroid cancers are typically associated with lytic metastases. The clinical vignette and image context (Fig. 8.122 is a bone scan of multiple bony metastasis from prostate carcinoma) reinforce this association.
Question 7
A 50-year-old female with a history of breast cancer presents with right knee pain. Radiographs show a lytic lesion in the distal femur. She denies any trauma. What is the most common presenting symptom of metastatic bone disease?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states, "Patients often present with local or regional pain." While other symptoms like pathologic fracture, hypercalcemia, spinal cord compression, or a palpable soft tissue mass can occur, pain is the most frequent initial complaint. The vignette describes knee pain, which is a local symptom.
Question 8
A 62-year-old male presents with new onset left hip pain. MRI demonstrates a lytic destruction in the femoral neck. He has no known history of cancer. What is the most appropriate initial diagnostic step to identify the primary tumor?
View Answer & Explanation
Correct Answer: C
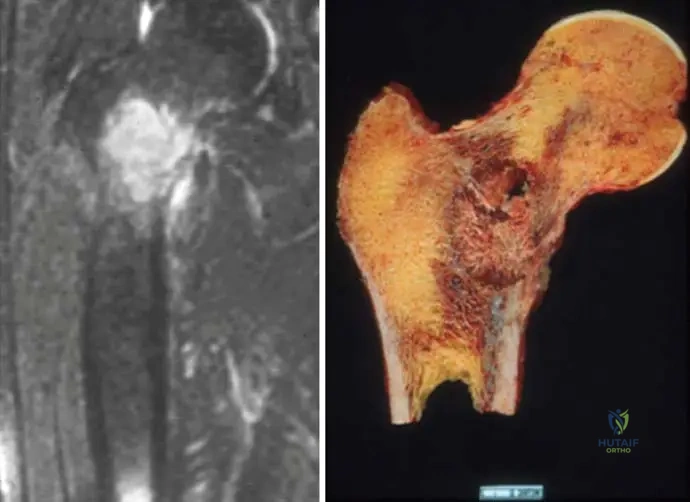
Rationale: When a bony metastasis is the initial presentation of a tumor, a CT scan of the chest, abdomen, and pelvis is typically the most efficient and comprehensive initial imaging study to search for the primary site, as it covers the most common locations for primary cancers that metastasize to bone (lung, breast, kidney, prostate, GI tract). While PET-CT is also effective, CT C/A/P is often the first-line, more readily available, and cost-effective option. Biopsy confirms the diagnosis but doesn't necessarily find the primary. Serum markers can be helpful but are not a standalone diagnostic for the primary site. The image (Fig. 8.125a) shows lytic destruction in the femoral neck, consistent with the vignette.
Question 9
A 75-year-old female presents with persistent right shoulder pain. Radiographs show a lytic lesion in the proximal humerus. She has a history of breast cancer treated 10 years prior. The pain is constant and present at rest. This type of pain pattern is characteristic of:
View Answer & Explanation
Correct Answer: D
Rationale: The teaching case states, "The pain is often at rest, while mechanical or activity-related pain may portend an impending pathologic fracture." Constant pain, especially at rest, in a patient with a history of cancer and a lytic lesion, is highly characteristic of malignant bone pain due to metastatic disease. Mechanical pain is typically activity-related and relieved by rest. Inflammatory arthritis and tendinopathy usually have different pain patterns and associated findings.
Question 10
A 60-year-old male presents with a painful lytic lesion in his left humerus. A bone scan shows increased uptake in the lesion, and a CT abdomen reveals a primary renal cell carcinoma. The patient is scheduled for surgical stabilization. What is a critical intraoperative consideration for managing bone metastases from renal cell carcinoma?
View Answer & Explanation
Correct Answer: B
Rationale: As discussed in the rationale for Question 25, renal cell carcinoma metastases (as indicated by Fig. 8.123 showing kidney as the primary) are known for being highly vascular. This significantly increases the risk of intraoperative hemorrhage, which is a critical consideration for surgical planning and execution. While poor bone quality can be an issue with any lytic lesion, the extreme vascularity is a specific characteristic of RCC metastases. The other options are less specific or universally critical for RCC metastases.
Question 11
A 68-year-old female with a history of breast cancer presents with new onset right thigh pain. Radiographs show a lytic lesion in the proximal femur. Which of the following primary tumors is NOT listed in the provided text as one of the most frequent causes of bony metastases?
View Answer & Explanation
Correct Answer: D
Rationale: The teaching case explicitly lists the most frequent primary tumors associated with bony metastases: "Lung, breast, prostate, kidney, and thyroid cancers are the most frequent primary tumors associated with bony metastases." Colon cancer is not included in this list, making it the correct answer as the one NOT listed.
Question 12
A 59-year-old male presents with a 2-month history of progressive left shoulder pain. Physical examination reveals local tenderness over the proximal humerus. Radiographs show a lytic lesion. He denies any prior cancer history. What is the significance of "local tenderness or joint irritability" in the context of metastatic bone disease?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states, "Local tenderness or joint irritability may be present." This indicates that these are common physical exam findings associated with metastatic bone disease, not indicative of benign processes or ruling out fractures. It is not specific to primary bone sarcomas, and while inflammatory arthritis can cause tenderness, the context of a lytic lesion points to metastasis.
Question 13
A 70-year-old female presents with a new lytic lesion in her right femoral neck, discovered incidentally on imaging for hip pain. She has no known history of cancer. The MRI shows the extent of the lytic destruction. What is the most likely initial presentation of metastatic bone disease in a patient without a known primary?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states, "Sometimes, however, a bony metastasis will be the initial presentation of a tumor." This means the discovery of the bone lesion itself (as in the vignette and Fig. 8.125a) can be the first sign of cancer, even before the primary tumor is identified or other systemic symptoms manifest. While a pathologic fracture can be the initial presentation, the bone metastasis itself is the underlying cause and can be discovered before a fracture occurs.
Question 14
A 65-year-old male with a history of lung cancer presents with severe, unremitting pain in his thoracic spine. Neurological examination reveals new onset lower extremity weakness and sensory changes. This clinical picture is most concerning for:
View Answer & Explanation
Correct Answer: B
Rationale: In a patient with known metastatic cancer and new onset severe spinal pain with neurological deficits (weakness, sensory changes), spinal cord compression due to epidural metastasis is a medical emergency. While not explicitly detailed in the provided text, it is a critical complication of metastatic bone disease that orthopaedic surgeons must recognize. The other options are less likely given the cancer history and neurological findings.
Question 15
A 52-year-old female with a history of breast cancer presents with a lytic lesion in her proximal femur. She is undergoing systemic therapy. What is the primary goal of surgical intervention for metastatic bone disease in the appendicular skeleton?
View Answer & Explanation
Correct Answer: C
Rationale: For metastatic bone disease, especially in the appendicular skeleton, surgical intervention is primarily palliative and prophylactic. The main goals are pain relief, prevention of impending pathologic fractures, and stabilization of existing pathologic fractures to improve function and quality of life. Cure is rarely achievable with surgery alone for widespread metastatic disease. Complete resection with wide margins is typically reserved for primary bone sarcomas or solitary metastases in specific circumstances, not the general approach for metastatic bone disease.
Question 16
A 67-year-old male presents with a lytic lesion in his left humerus. A bone scan shows increased uptake in the lesion. A CT abdomen reveals a primary site in the kidney. Which of the following statements about the prognosis of metastatic bone disease is most accurate?
View Answer & Explanation
Correct Answer: C
Rationale: While not explicitly detailed in the provided text, the general understanding of metastatic bone disease is that prognosis is highly variable. It is heavily influenced by the type of primary tumor (e.g., breast and prostate cancer generally have better prognoses than lung or pancreatic cancer), the overall burden of disease (number and location of metastases), and the patient's response to systemic therapies. The image (Fig. 8.123) shows a kidney primary, which can have a variable course. A uniformly poor prognosis is incorrect, and while extent of bone involvement is a factor, the primary tumor type is often more critical. Solitary metastases can still be aggressive depending on the primary. Surgical intervention primarily improves quality of life and function, not necessarily survival in most cases.
Question 17
A 7-year-old male presents with acute onset of right knee pain, fever, and refusal to bear weight. His mother reports a recent skin infection on his arm. Physical examination reveals a swollen, erythematous, and tender right knee.
View Answer & Explanation
Correct Answer: C
Rationale: Acute hematogenous osteomyelitis, by definition, arises from bacteremia, where pathogens spread through the bloodstream from a distant focus (like a skin infection) to the bone. This is the major predisposing factor for this specific type of osteomyelitis. Main Distractor Rationale: Contiguous spread (B) is a predisposing factor for osteomyelitis in general, but it describes a different mechanism of infection spread, not hematogenous.
Question 18
A 5-year-old child presents with a 3-day history of fever, malaise, and severe pain in the left distal femur. Physical examination reveals localized tenderness and warmth over the metaphysis. Blood cultures are drawn.
View Answer & Explanation
Correct Answer: D
Rationale: The provided text explicitly states that "The pathogens are in 90% of all cases Staphylococcus aureus colonies," making it the most likely causative agent in acute hematogenous osteomyelitis. Main Distractor Rationale: While Lactococcus (A) is mentioned in the case as a causative agent in a specific example, Staphylococcus aureus is overwhelmingly the most common pathogen overall.
Question 19
A 10-year-old boy presents with a 1-week history of left proximal tibial pain and limping. Initial radiographs taken 3 days ago were unremarkable. Today, repeat radiographs are performed.
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 2.1b specifically illustrates a "well-defined lytic lesion in the proximal metaphysis of the right tibia: no sclerotic margin is observed." This is characteristic of early bone destruction in acute osteomyelitis, which can become visible on radiographs after about 7-10 days. Main Distractor Rationale: A well-defined sclerotic lesion (A) or extensive cortical thickening (D) are typically seen in chronic osteomyelitis or benign bone lesions, not acute presentations.
Question 20
A 6-year-old girl is diagnosed with acute hematogenous osteomyelitis of the distal femur. Despite initial antibiotic therapy, her symptoms persist, and imaging shows progressive bone changes.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Bone necrosis and bone destruction occur early in the course of osteomyelitis, leading to a chronic process and eliminating the host’s ability to eradicate the pathogens." This early tissue damage is a critical factor in the disease's persistence. Main Distractor Rationale: Rapid bacterial replication rate (A) is generally associated with acute, aggressive infections, but the text specifically mentions "slow bacterial replication rate" as a factor for persistence, not rapid.
Question 21
A public health official is reviewing data on acute hematogenous osteomyelitis cases across different age groups.
View Answer & Explanation
Correct Answer: C
Rationale: The case text explicitly states that acute hematogenous osteomyelitis "may occur in newborn, infant, childhood and adult ages (in 75% at childhood and adolescents)." Main Distractor Rationale: While osteomyelitis can occur in adults over 65 (D), especially with comorbidities, childhood and adolescence represent the highest incidence according to the provided data.
Question 22
A 14-year-old male presents with a 2-month history of progressive left thigh pain and swelling. Radiographs reveal a permeative lesion in the femoral diaphysis with an "onion peel" periosteal reaction.
View Answer & Explanation
Correct Answer: C
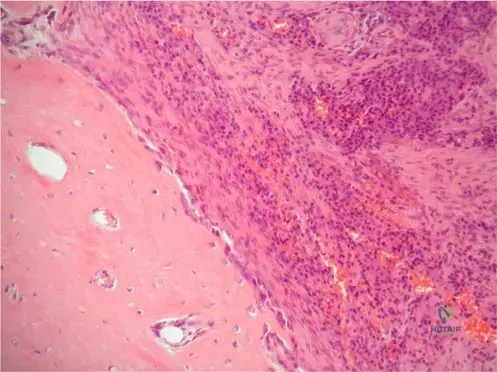
Rationale: The context for Fig. 2.3a,b explicitly states that the "onion peel" like periosteal reaction, seen in acute hematogenous osteomyelitis, "is also seen in malignant bone tumors (e.g. Ewing’s sarcoma)." This makes Ewing's sarcoma a critical differential diagnosis. Main Distractor Rationale: Osteosarcoma (A) typically presents with different periosteal reactions, such as a sunburst or spiculated pattern, rather than the classic "onion peel" appearance.
Question 23
A 9-year-old girl with suspected acute hematogenous osteomyelitis of the femur undergoes an MRI scan.

View Answer & Explanation
Correct Answer: C
Rationale: The context for Fig. 2.4 describes the MRI findings as "edema and pus formation in the bone marrow and perifocal edema in the surrounding soft tissues," which are hallmark features of acute osteomyelitis on MRI. Main Distractor Rationale: Extensive cortical thickening and sclerosis (A) are more indicative of chronic osteomyelitis, not the acute phase where edema and pus are predominant.
Question 24
A 45-year-old patient with a history of intravenous drug use develops acute hematogenous osteomyelitis of the lumbar spine. Despite appropriate antibiotic therapy, the infection recurs.
View Answer & Explanation
Correct Answer: D
Rationale: The text identifies "The presence of poorly vascularized tissues, the adherence to bone structures and implants and a slow bacterial replication rate" as important factors for the persistence of the infection. Poorly vascularized tissues limit antibiotic delivery and immune cell access. Main Distractor Rationale: A high rate of bacterial replication (A) is not listed as a factor for persistence; rather, a *slow* bacterial replication rate is mentioned as contributing to persistence.
Question 25
A patient diagnosed with Lactococcus-induced acute hematogenous femoral osteomyelitis develops sudden neurological symptoms and respiratory distress.
View Answer & Explanation
Correct Answer: C
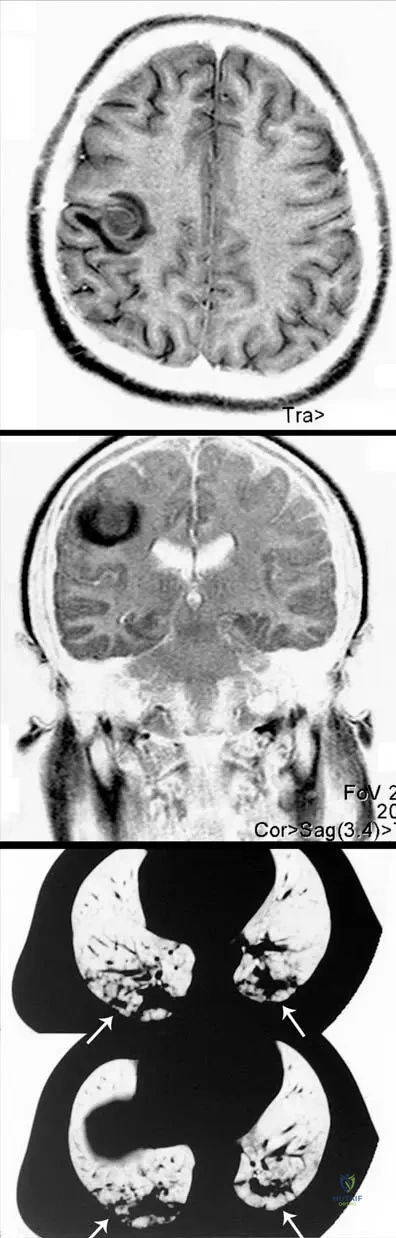
Rationale: The context for Fig. 2.5 explicitly states that "metastatic purulent foci are present in the brain and the lung (arrows), causing a life threatening condition" in the same patient with Lactococcus osteomyelitis. Neurological symptoms and respiratory distress are consistent with these metastatic foci. Main Distractor Rationale: Direct extension of femoral osteomyelitis to the spinal cord (A) is anatomically highly improbable and not supported by the case description.
Question 26
A 12-year-old boy presents with acute hematogenous osteomyelitis of the femur. Initial cultures reveal Lactococcus species.
View Answer & Explanation
Correct Answer: C
Rationale: The context for Fig. 2.3a,b specifically describes the plain radiographs of the *Lactococcus*-induced femoral osteomyelitis as having a "permeative radiographic appearance with “onion peel”like periosteal reaction." Main Distractor
Question 26
A 7-year-old male presents with a 3-day history of right knee pain, limping, and fever. On examination, his right knee is swollen, warm, and erythematous. Radiographs of the knee reveal a well-defined lytic lesion in the proximal metaphysis of the right tibia without a sclerotic margin. Laboratory tests show elevated white blood cell count and inflammatory markers.
View Answer & Explanation
Correct Answer: C
Rationale: In a patient with suspected acute osteomyelitis, an MRI is the most sensitive imaging modality to assess the extent of bone marrow edema, pus formation, and perifocal soft tissue involvement, which is crucial for surgical planning and prognosis. While radiographs show a lytic lesion, MRI provides a more comprehensive picture. Initiating oral antibiotics (A) without definitive diagnosis or full extent assessment is suboptimal. Immediate surgical debridement (B) without full imaging assessment or culture results may be premature. Corticosteroids (D) are contraindicated in infection. Waiting for follow-up radiographs (E) delays definitive diagnosis and treatment, potentially leading to chronic disease.
Question 26
A 5-year-old girl develops acute onset of left hip pain and refusal to bear weight. She has a fever of 102°F. Physical examination reveals tenderness to palpation over the greater trochanter and pain with hip range of motion. Blood cultures are drawn, and empiric antibiotics are started. Given the typical epidemiology of acute hematogenous osteomyelitis in children, which organism is the most likely causative agent?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text explicitly states that *Staphylococcus aureus* colonies are the pathogens in 90% of all cases of osteomyelitis. While other organisms can cause osteomyelitis, *S. aureus* is overwhelmingly the most common cause, especially in acute hematogenous osteomyelitis in children. *Lactococcus* (A) is mentioned in the case as a cause of femoral osteomyelitis with severe complications, but it is not the most common overall. *Pseudomonas aeruginosa* (B) is more common in puncture wounds or immunocompromised patients. *Streptococcus pyogenes* (D) and *Escherichia coli* (E) are less common causes of osteomyelitis.
Question 26
A 12-year-old boy presents with persistent right thigh pain, low-grade fever, and malaise for several weeks. Initial plain radiographs of the femur show a subtle permeative radiographic appearance with an "onion peel" like periosteal reaction. An MRI is subsequently performed.
View Answer & Explanation
Correct Answer: C
Rationale: As shown in Fig. 2.4, an MR image of femoral osteomyelitis reveals edema and pus formation in the bone marrow and perifocal edema in the surrounding soft tissues. MRI is highly sensitive for detecting these early inflammatory changes, which are characteristic of osteomyelitis and are often not visible on plain radiographs. Lytic lesions with sclerotic margins (A) are more typical of chronic osteomyelitis or other benign bone lesions, and MRI's primary role here is not just to confirm a lytic lesion. Ruling out a stress fracture (B) might be part of a differential, but MRI's main utility in osteomyelitis is for infection assessment. Assessing joint effusion (D) is a secondary finding. Cortical thickening (E) is a late finding, better seen on CT or plain films, but MRI excels at soft tissue and marrow changes.
Question 26
A 10-year-old boy presents with progressive left thigh pain and swelling. Plain radiographs of the femur demonstrate a permeative radiographic appearance with an "onion peel" like periosteal reaction. Given this radiographic finding, which of the following is the most critical differential diagnosis to consider alongside acute osteomyelitis?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 2.3 explicitly states that the "onion peel" like periosteal reaction, seen in acute hematogenous femoral osteomyelitis, is also seen in malignant bone tumors such as Ewing's sarcoma. This makes Ewing's sarcoma a critical differential diagnosis that must be excluded, typically with biopsy. Osteoid osteoma (A) typically presents with a nidus and reactive sclerosis. Fibrous dysplasia (B) is a developmental anomaly with a characteristic ground-glass appearance. Osteochondroma (D) is a benign exostosis. A simple bone cyst (E) is a lytic lesion, often with a "fallen fragment" sign, but does not typically cause an "onion peel" reaction.
Question 26
A 6-year-old boy is diagnosed with acute hematogenous femoral osteomyelitis caused by *Lactococcus* species. Despite initial antibiotic therapy, his condition worsens, and he develops new neurological symptoms and respiratory distress. Imaging studies are performed.
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 2.5 a–c, which describes the same patient with *Lactococcus*-osteomyelitis, shows cranial MRI with metastatic purulent foci in the brain and a chest CT scan with metastatic purulent foci in the lung. These metastatic foci are described as causing a life-threatening condition. Therefore, the new neurological and respiratory symptoms are highly suggestive of systemic spread of the infection. While chronic osteomyelitis (B) can develop, it typically doesn't present with acute, life-threatening systemic symptoms. Antibiotic side effects (A), allergic reactions (D), or superinfection (E) are less likely to explain the specific pattern of brain and lung involvement seen in the images.
Question 26
A 9-year-old boy presents with recurrent pain and drainage from his left tibia, several months after being treated for acute hematogenous osteomyelitis. Despite initial resolution of acute symptoms, the infection has persisted. Which of the following factors is most critical in explaining the transition from acute to chronic osteomyelitis and the persistence of pathogens?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states: "Bone necrosis and bone destruction occur early in the course of osteomyelitis, leading to a chronic process and eliminating the host’s ability to eradicate the pathogens. The presence of poorly vascularized tissues, the adherence to bone structures and implants and a slow bacterial replication rate are recognized as important factors for the persistence of the infection." This directly explains why acute osteomyelitis can become chronic. While antibiotic duration (B) is important, the underlying pathological changes in the bone are more fundamental to chronicity. Age/gender (A), nutritional status (D), and localization (E) are less critical factors for the persistence mechanism itself, though they can influence the course.
Question 26
A 4-year-old child presents with a painful, swollen right ankle and fever. Radiographs are inconclusive, but an MRI suggests osteomyelitis of the distal tibia. To definitively diagnose the infection and guide targeted antibiotic therapy, what is the most appropriate next step?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 2.1b states, "Biopsy proved osteomyelitis." Biopsy with subsequent culture and histopathology is the gold standard for definitive diagnosis of osteomyelitis, allowing for identification of the causative organism and its antibiotic sensitivities, which is crucial for targeted therapy. While empiric antibiotics (A) are often started, definitive diagnosis is preferred. A bone scan (B) is sensitive but not specific for infection. Monitoring inflammatory markers (D) is useful for tracking response to treatment but not for definitive diagnosis. NSAIDs (E) would mask symptoms and delay diagnosis.
Question 26
A 6-year-old boy is diagnosed with acute hematogenous osteomyelitis. The infection is most commonly found in which specific anatomical region of long bones in children?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 2.1b shows a lytic lesion in the "proximal metaphysis of the right tibia." The metaphysis is the most common site for acute hematogenous osteomyelitis in children due to its rich, slow-flowing blood supply and fenestrated capillaries, which allow bacteria to settle and proliferate. The diaphysis (A) is less common. The epiphysis (B) is typically protected by the growth plate, though it can be involved in infants. Articular cartilage (D) and periosteum (E) are usually involved secondarily.
Question 26
A 2-year-old infant presents with irritability, fever, and swelling of the left arm. Radiographs are initially unremarkable, but an MRI confirms acute osteomyelitis of the humerus. Pending culture results, what is the most appropriate initial empiric intravenous antibiotic choice for this patient?
View Answer & Explanation
Correct Answer: B
Rationale: Given that *Staphylococcus aureus* is the causative agent in 90% of cases, and considering the increasing prevalence of Methicillin-Resistant *Staphylococcus aureus* (MRSA), Vancomycin is a common and appropriate empiric choice for acute hematogenous osteomyelitis, especially in areas with high MRSA rates or when the patient is severely ill. Ceftriaxone (C) would cover some Gram-negatives and sensitive *S. aureus* but not MRSA. Ciprofloxacin (A) is generally avoided in young children due to cartilage concerns. Clindamycin (D) can be used but has variable MRSA coverage depending on local resistance patterns. Penicillin G (E) would not cover *S. aureus* effectively due to widespread resistance.
Question 26
A 14-year-old adolescent with acute hematogenous osteomyelitis of the distal femur has failed to respond to appropriate intravenous antibiotic therapy after 72 hours, with persistent fever and worsening local pain and swelling. MRI shows significant pus formation and bone destruction. What is the most appropriate next step in management?
View Answer & Explanation
Correct Answer: C
Rationale: When acute osteomyelitis fails to respond to appropriate antibiotic therapy, especially with evidence of pus formation and bone destruction on imaging, surgical debridement and drainage are indicated. The presence of pus and necrotic bone creates an environment where antibiotics cannot effectively penetrate, necessitating surgical intervention to remove infected and devitalized tissue. Switching antibiotics (A), adding a second antibiotic (B), or increasing the dose (D) would be ineffective if there is a significant collection of pus or necrotic bone. Discharging the patient (E) would be inappropriate and dangerous given the worsening condition.
Question 26
A 10-year-old boy successfully treated for acute hematogenous osteomyelitis of the proximal tibia is now 6 months post-treatment. Despite resolution of acute symptoms, he occasionally experiences mild, localized pain in the affected area. Based on the natural history of osteomyelitis, what is a recognized long-term complication even after acute symptoms have resolved?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical text explicitly states: "Chronic pain and recurrence of infection still remain possible even when the acute symptoms of osteomyelitis have been resolved." This highlights the challenging nature of osteomyelitis and its potential for long-term morbidity. While other complications can occur, chronic pain and recurrence are directly mentioned as persistent issues. Malignant bone tumor (A) is not a direct complication of osteomyelitis itself, though some chronic infections can rarely predispose to squamous cell carcinoma in sinus tracts. Permanent joint stiffness (C) is more common if the infection extends into the joint. Systemic organ failure (D) is a complication of acute, severe, disseminated infection, not typically a long-term sequela after resolution. Autoimmune arthritis (E) is unrelated.
Question 26
A 35-year-old male presents with a 3-month history of intermittent right foot pain, swelling, and a draining sinus tract following a puncture wound. Radiographs show a lytic lesion with surrounding sclerosis and periosteal reaction in the calcaneus. A biopsy confirms osteomyelitis. What feature on imaging or pathology would most strongly suggest a chronic rather than acute process?
View Answer & Explanation
Correct Answer: D
Rationale: The presence of sequestrum (a piece of necrotic bone separated from healthy bone) and involucrum (new bone formation around the sequestrum) are classic radiographic and pathological hallmarks of chronic osteomyelitis. The clinical text mentions "Bone necrosis and bone destruction occur early... leading to a chronic process." Bone marrow edema (A) is characteristic of acute infection. Elevated CRP (B) is a general inflammatory marker, common in both acute and chronic phases. A well-defined lytic lesion without sclerotic margin (C) is described in Fig. 2.1b as acute osteomyelitis. Absence of fever (E) can occur in chronic osteomyelitis but is not a definitive imaging or pathological feature.
Question 26
A 50-year-old diabetic male develops acute onset of severe back pain and fever. MRI reveals osteomyelitis of a lumbar vertebra. He denies any recent trauma or surgery. Which of the following is the most likely predisposing factor for his acute hematogenous osteomyelitis?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical text lists "Bacteriaemia, contiguous focusses of infection, penetrating trauma or surgery are the major predisposing factors for this infection." In this case, with no history of trauma, surgery, or a local contiguous infection, bacteremia from a distant source (e.g., urinary tract infection, skin infection, dental abscess, or intravenous drug use in adults) is the most likely mechanism for hematogenous spread to the spine. Penetrating trauma (A), contiguous focus (B), and recent surgery (C) are other predisposing factors but are excluded by the vignette. Immunosuppressive medication use (E) is a risk factor for infection generally, but bacteremia is the direct mechanism for hematogenous spread.
Question 26
A 9-year-old boy presents with right knee pain, swelling, and erythema. Radiographs show a well-defined lytic lesion in the proximal metaphysis of the right tibia, notably without a sclerotic margin. This radiographic appearance, as seen in Fig. 2.1b, is most characteristic of which stage or type of osteomyelitis?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 2.1b specifically describes "a well-defined lytic lesion in the proximal metaphysis of the right tibia: no sclerotic margin is observed. Biopsy proved osteomyelitis." This appearance is characteristic of early acute osteomyelitis, where bone destruction is occurring without sufficient time for reactive bone formation (sclerosis) or involucrum. Chronic osteomyelitis (A) typically shows sclerotic margins, sequestrum, and involucrum. Brodie's abscess (B) is a subacute form with a well-defined lytic lesion often with a sclerotic rim. Extensive cortical destruction (D) might be present but the lack of sclerosis is key. Post-traumatic osteomyelitis (E) can be acute or chronic, but the specific radiographic finding points to the acute stage.
Question 26
A 6-month-old infant is diagnosed with acute hematogenous osteomyelitis of the femur. The course of the disease in this patient, including the effectiveness of antibiotic delivery and the potential for chronic infection, is significantly influenced by several factors. Which of the following factors plays a crucial role in determining the disease course by affecting the host's ability to eradicate pathogens?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical text states: "The course of the disease depends on the age of the patient, on the virulence of the causative agent, on the immunological state of the host, on the localization and on the blood supply." It further emphasizes: "The presence of poorly vascularized tissues... are recognized as important factors for the persistence of the infection." Poorly vascularized tissues limit antibiotic penetration and the host's immune response, making pathogen eradication difficult and contributing to chronicity. Birth weight (A), feeding method (C), day of symptom onset (D), and number of siblings (E) are not directly identified as crucial factors influencing the course of osteomyelitis in the provided text.
Question 26
A 7-year-old boy with acute hematogenous osteomyelitis due to *Lactococcus* species presents with sudden onset of severe headache, confusion, and seizures. Concurrently, he develops shortness of breath and a productive cough. What is the most likely explanation for this constellation of symptoms?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 2.5 a–c explicitly shows cranial MRI with metastatic purulent foci in the brain and chest CT scan with metastatic purulent foci in the lung in the same patient with *Lactococcus*-osteomyelitis, causing a life-threatening condition. The neurological symptoms (headache, confusion, seizures) are consistent with brain involvement, and respiratory symptoms (shortness of breath, cough) are consistent with lung involvement. This indicates systemic dissemination of the infection. Adverse reactions to antibiotics (A) or co-infection (D) are less likely to present with such specific multi-organ involvement. A localized abscess (B) would not explain systemic symptoms. Septic arthritis (E) is a localized complication, not a systemic one.
Question 26
A 4-year-old boy is diagnosed with acute hematogenous osteomyelitis of the femur. Considering the overall epidemiology of this condition, which age group is most frequently affected?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states: "Acute hematogenous osteomyelitis may occur in newborn, infant, childhood and adult ages (in 75% at childhood and adolescents)." This clearly indicates that childhood and adolescence represent the most frequently affected age group for this condition. While it can occur at any age, the vast majority of cases fall within this demographic.
Question 26
A 5-year-old boy presents with acute onset of severe right leg pain and fever. Physical examination reveals localized tenderness and swelling over the distal tibia. Initial plain radiographs of the tibia are reported as normal. What is the most appropriate interpretation of these radiographic findings in the context of suspected acute osteomyelitis?
View Answer & Explanation
Correct Answer: C
Rationale: Plain radiographs are often normal in the very early stages of acute osteomyelitis because bone changes (lysis, periosteal reaction) take time to develop and become radiographically visible, typically 7-10 days or more after the onset of symptoms. Therefore, normal radiographs do not rule out early osteomyelitis (A). Radiographs are not highly sensitive for early acute osteomyelitis (B). While a non-infectious cause should be considered (D), the clinical picture is highly suspicious for osteomyelitis. MRI (not CT) is the next best imaging modality for early confirmation (E) due to its sensitivity for bone marrow edema.
Question 27
A 7-year-old male presents with a 3-day history of right knee pain, limping, and fever. On examination, his right knee is swollen, warm, and erythematous. Radiographs of the knee reveal a well-defined lytic lesion in the proximal metaphysis of the right tibia without a sclerotic margin. Laboratory tests show elevated white blood cell count and inflammatory markers.
View Answer & Explanation
Correct Answer: C
Rationale: In a patient with suspected acute osteomyelitis, an MRI is the most sensitive imaging modality to assess the extent of bone marrow edema, pus formation, and perifocal soft tissue involvement, which is crucial for surgical planning and prognosis. While radiographs show a lytic lesion, MRI provides a more comprehensive picture. Initiating oral antibiotics (A) without definitive diagnosis or full extent assessment is suboptimal. Immediate surgical debridement (B) without full imaging assessment or culture results may be premature. Corticosteroids (D) are contraindicated in infection. Waiting for follow-up radiographs (E) delays definitive diagnosis and treatment, potentially leading to chronic disease.
Question 28
A 5-year-old girl develops acute onset of left hip pain and refusal to bear weight. She has a fever of 102°F. Physical examination reveals tenderness to palpation over the greater trochanter and pain with hip range of motion. Blood cultures are drawn, and empiric antibiotics are started. Given the typical epidemiology of acute hematogenous osteomyelitis in children, which organism is the most likely causative agent?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text explicitly states that *Staphylococcus aureus* colonies are the pathogens in 90% of all cases of osteomyelitis. While other organisms can cause osteomyelitis, *S. aureus* is overwhelmingly the most common cause, especially in acute hematogenous osteomyelitis in children. *Lactococcus* (A) is mentioned in the case as a cause of femoral osteomyelitis with severe complications, but it is not the most common overall. *Pseudomonas aeruginosa* (B) is more common in puncture wounds or immunocompromised patients. *Streptococcus pyogenes* (D) and *Escherichia coli* (E) are less common causes of osteomyelitis.
Question 29
A 12-year-old boy presents with persistent right thigh pain, low-grade fever, and malaise for several weeks. Initial plain radiographs of the femur show a subtle permeative radiographic appearance with an "onion peel" like periosteal reaction. An MRI is subsequently performed.
View Answer & Explanation
Correct Answer: C
Rationale: As shown in Fig. 2.4, an MR image of femoral osteomyelitis reveals edema and pus formation in the bone marrow and perifocal edema in the surrounding soft tissues. MRI is highly sensitive for detecting these early inflammatory changes, which are characteristic of osteomyelitis and are often not visible on plain radiographs. Lytic lesions with sclerotic margins (A) are more typical of chronic osteomyelitis or other benign bone lesions, and MRI's primary role here is not just to confirm a lytic lesion. Ruling out a stress fracture (B) might be part of a differential, but MRI's main utility in osteomyelitis is for infection assessment. Assessing joint effusion (D) is a secondary finding. Cortical thickening (E) is a late finding, better seen on CT or plain films, but MRI excels at soft tissue and marrow changes.
Question 30
A 10-year-old boy presents with progressive left thigh pain and swelling. Plain radiographs of the femur demonstrate a permeative radiographic appearance with an "onion peel" like periosteal reaction. Given this radiographic finding, which of the following is the most critical differential diagnosis to consider alongside acute osteomyelitis?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 2.3 explicitly states that the "onion peel" like periosteal reaction, seen in acute hematogenous femoral osteomyelitis, is also seen in malignant bone tumors such as Ewing's sarcoma. This makes Ewing's sarcoma a critical differential diagnosis that must be excluded, typically with biopsy. Osteoid osteoma (A) typically presents with a nidus and reactive sclerosis. Fibrous dysplasia (B) is a developmental anomaly with a characteristic ground-glass appearance. Osteochondroma (D) is a benign exostosis. A simple bone cyst (E) is a lytic lesion, often with a "fallen fragment" sign, but does not typically cause an "onion peel" reaction.
Question 31
A 6-year-old boy is diagnosed with acute hematogenous femoral osteomyelitis caused by *Lactococcus* species. Despite initial antibiotic therapy, his condition worsens, and he develops new neurological symptoms and respiratory distress. Imaging studies are performed.
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 2.5 a–c, which describes the same patient with *Lactococcus*-osteomyelitis, shows cranial MRI with metastatic purulent foci in the brain and a chest CT scan with metastatic purulent foci in the lung. These metastatic foci are described as causing a life-threatening condition. Therefore, the new neurological and respiratory symptoms are highly suggestive of systemic spread of the infection. While chronic osteomyelitis (B) can develop, it typically doesn't present with acute, life-threatening systemic symptoms. Antibiotic side effects (A), allergic reactions (D), or superinfection (E) are less likely to explain the specific pattern of brain and lung involvement seen in the images.
Question 32
A 9-year-old boy presents with recurrent pain and drainage from his left tibia, several months after being treated for acute hematogenous osteomyelitis. Despite initial resolution of acute symptoms, the infection has persisted. Which of the following factors is most critical in explaining the transition from acute to chronic osteomyelitis and the persistence of pathogens?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states: "Bone necrosis and bone destruction occur early in the course of osteomyelitis, leading to a chronic process and eliminating the host’s ability to eradicate the pathogens. The presence of poorly vascularized tissues, the adherence to bone structures and implants and a slow bacterial replication rate are recognized as important factors for the persistence of the infection." This directly explains why acute osteomyelitis can become chronic. While antibiotic duration (B) is important, the underlying pathological changes in the bone are more fundamental to chronicity. Age/gender (A), nutritional status (D), and localization (E) are less critical factors for the persistence mechanism itself, though they can influence the course.
Question 33
A 4-year-old child presents with a painful, swollen right ankle and fever. Radiographs are inconclusive, but an MRI suggests osteomyelitis of the distal tibia. To definitively diagnose the infection and guide targeted antibiotic therapy, what is the most appropriate next step?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 2.1b states, "Biopsy proved osteomyelitis." Biopsy with subsequent culture and histopathology is the gold standard for definitive diagnosis of osteomyelitis, allowing for identification of the causative organism and its antibiotic sensitivities, which is crucial for targeted therapy. While empiric antibiotics (A) are often started, definitive diagnosis is preferred. A bone scan (B) is sensitive but not specific for infection. Monitoring inflammatory markers (D) is useful for tracking response to treatment but not for definitive diagnosis. NSAIDs (E) would mask symptoms and delay diagnosis.
Question 34
A 6-year-old boy is diagnosed with acute hematogenous osteomyelitis. The infection is most commonly found in which specific anatomical region of long bones in children?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 2.1b shows a lytic lesion in the "proximal metaphysis of the right tibia." The metaphysis is the most common site for acute hematogenous osteomyelitis in children due to its rich, slow-flowing blood supply and fenestrated capillaries, which allow bacteria to settle and proliferate. The diaphysis (A) is less common. The epiphysis (B) is typically protected by the growth plate, though it can be involved in infants. Articular cartilage (D) and periosteum (E) are usually involved secondarily.
Question 35
A 2-year-old infant presents with irritability, fever, and swelling of the left arm. Radiographs are initially unremarkable, but an MRI confirms acute osteomyelitis of the humerus. Pending culture results, what is the most appropriate initial empiric intravenous antibiotic choice for this patient?
View Answer & Explanation
Correct Answer: B
Rationale: Given that *Staphylococcus aureus* is the causative agent in 90% of cases, and considering the increasing prevalence of Methicillin-Resistant *Staphylococcus aureus* (MRSA), Vancomycin is a common and appropriate empiric choice for acute hematogenous osteomyelitis, especially in areas with high MRSA rates or when the patient is severely ill. Ceftriaxone (C) would cover some Gram-negatives and sensitive *S. aureus* but not MRSA. Ciprofloxacin (A) is generally avoided in young children due to cartilage concerns. Clindamycin (D) can be used but has variable MRSA coverage depending on local resistance patterns. Penicillin G (E) would not cover *S. aureus* effectively due to widespread resistance.
Question 36
A 14-year-old adolescent with acute hematogenous osteomyelitis of the distal femur has failed to respond to appropriate intravenous antibiotic therapy after 72 hours, with persistent fever and worsening local pain and swelling. MRI shows significant pus formation and bone destruction. What is the most appropriate next step in management?
View Answer & Explanation
Correct Answer: C
Rationale: When acute osteomyelitis fails to respond to appropriate antibiotic therapy, especially with evidence of pus formation and bone destruction on imaging, surgical debridement and drainage are indicated. The presence of pus and necrotic bone creates an environment where antibiotics cannot effectively penetrate, necessitating surgical intervention to remove infected and devitalized tissue. Switching antibiotics (A), adding a second antibiotic (B), or increasing the dose (D) would be ineffective if there is a significant collection of pus or necrotic bone. Discharging the patient (E) would be inappropriate and dangerous given the worsening condition.
Question 37
A 10-year-old boy successfully treated for acute hematogenous osteomyelitis of the proximal tibia is now 6 months post-treatment. Despite resolution of acute symptoms, he occasionally experiences mild, localized pain in the affected area. Based on the natural history of osteomyelitis, what is a recognized long-term complication even after acute symptoms have resolved?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical text explicitly states: "Chronic pain and recurrence of infection still remain possible even when the acute symptoms of osteomyelitis have been resolved." This highlights the challenging nature of osteomyelitis and its potential for long-term morbidity. While other complications can occur, chronic pain and recurrence are directly mentioned as persistent issues. Malignant bone tumor (A) is not a direct complication of osteomyelitis itself, though some chronic infections can rarely predispose to squamous cell carcinoma in sinus tracts. Permanent joint stiffness (C) is more common if the infection extends into the joint. Systemic organ failure (D) is a complication of acute, severe, disseminated infection, not typically a long-term sequela after resolution. Autoimmune arthritis (E) is unrelated.
Question 38
A 35-year-old male presents with a 3-month history of intermittent right foot pain, swelling, and a draining sinus tract following a puncture wound. Radiographs show a lytic lesion with surrounding sclerosis and periosteal reaction in the calcaneus. A biopsy confirms osteomyelitis. What feature on imaging or pathology would most strongly suggest a chronic rather than acute process?
View Answer & Explanation
Correct Answer: D
Rationale: The presence of sequestrum (a piece of necrotic bone separated from healthy bone) and involucrum (new bone formation around the sequestrum) are classic radiographic and pathological hallmarks of chronic osteomyelitis. The clinical text mentions "Bone necrosis and bone destruction occur early... leading to a chronic process." Bone marrow edema (A) is characteristic of acute infection. Elevated CRP (B) is a general inflammatory marker, common in both acute and chronic phases. A well-defined lytic lesion without sclerotic margin (C) is described in Fig. 2.1b as acute osteomyelitis. Absence of fever (E) can occur in chronic osteomyelitis but is not a definitive imaging or pathological feature.
Question 39
A 50-year-old diabetic male develops acute onset of severe back pain and fever. MRI reveals osteomyelitis of a lumbar vertebra. He denies any recent trauma or surgery. Which of the following is the most likely predisposing factor for his acute hematogenous osteomyelitis?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical text lists "Bacteriaemia, contiguous focusses of infection, penetrating trauma or surgery are the major predisposing factors for this infection." In this case, with no history of trauma, surgery, or a local contiguous infection, bacteremia from a distant source (e.g., urinary tract infection, skin infection, dental abscess, or intravenous drug use in adults) is the most likely mechanism for hematogenous spread to the spine. Penetrating trauma (A), contiguous focus (B), and recent surgery (C) are other predisposing factors but are excluded by the vignette. Immunosuppressive medication use (E) is a risk factor for infection generally, but bacteremia is the direct mechanism for hematogenous spread.
Question 40
A 9-year-old boy presents with right knee pain, swelling, and erythema. Radiographs show a well-defined lytic lesion in the proximal metaphysis of the right tibia, notably without a sclerotic margin. This radiographic appearance, as seen in Fig. 2.1b, is most characteristic of which stage or type of osteomyelitis?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 2.1b specifically describes "a well-defined lytic lesion in the proximal metaphysis of the right tibia: no sclerotic margin is observed. Biopsy proved osteomyelitis." This appearance is characteristic of early acute osteomyelitis, where bone destruction is occurring without sufficient time for reactive bone formation (sclerosis) or involucrum. Chronic osteomyelitis (A) typically shows sclerotic margins, sequestrum, and involucrum. Brodie's abscess (B) is a subacute form with a well-defined lytic lesion often with a sclerotic rim. Extensive cortical destruction (D) might be present but the lack of sclerosis is key. Post-traumatic osteomyelitis (E) can be acute or chronic, but the specific radiographic finding points to the acute stage.
Question 41
A 6-month-old infant is diagnosed with acute hematogenous osteomyelitis of the femur. The course of the disease in this patient, including the effectiveness of antibiotic delivery and the potential for chronic infection, is significantly influenced by several factors. Which of the following factors plays a crucial role in determining the disease course by affecting the host's ability to eradicate pathogens?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical text states: "The course of the disease depends on the age of the patient, on the virulence of the causative agent, on the immunological state of the host, on the localization and on the blood supply." It further emphasizes: "The presence of poorly vascularized tissues... are recognized as important factors for the persistence of the infection." Poorly vascularized tissues limit antibiotic penetration and the host's immune response, making pathogen eradication difficult and contributing to chronicity. Birth weight (A), feeding method (C), day of symptom onset (D), and number of siblings (E) are not directly identified as crucial factors influencing the course of osteomyelitis in the provided text.
Question 42
A 7-year-old boy with acute hematogenous osteomyelitis due to *Lactococcus* species presents with sudden onset of severe headache, confusion, and seizures. Concurrently, he develops shortness of breath and a productive cough. What is the most likely explanation for this constellation of symptoms?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 2.5 a–c explicitly shows cranial MRI with metastatic purulent foci in the brain and chest CT scan with metastatic purulent foci in the lung in the same patient with *Lactococcus*-osteomyelitis, causing a life-threatening condition. The neurological symptoms (headache, confusion, seizures) are consistent with brain involvement, and respiratory symptoms (shortness of breath, cough) are consistent with lung involvement. This indicates systemic dissemination of the infection. Adverse reactions to antibiotics (A) or co-infection (D) are less likely to present with such specific multi-organ involvement. A localized abscess (B) would not explain systemic symptoms. Septic arthritis (E) is a localized complication, not a systemic one.
Question 43
A 4-year-old boy is diagnosed with acute hematogenous osteomyelitis of the femur. Considering the overall epidemiology of this condition, which age group is most frequently affected?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states: "Acute hematogenous osteomyelitis may occur in newborn, infant, childhood and adult ages (in 75% at childhood and adolescents)." This clearly indicates that childhood and adolescence represent the most frequently affected age group for this condition. While it can occur at any age, the vast majority of cases fall within this demographic.
Question 44
A 35-year-old male presents with a 6-month history of intermittent knee swelling and pain, particularly after activity. On examination, a soft, palpable mass is noted in the suprapatellar region, and there is a moderate effusion. Arthrocentesis yields a blood-stained synovial fluid. Conventional radiographs of the knee are unremarkable. What is the most appropriate next diagnostic step?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of a palpable mass, recurrent effusion, and particularly blood-stained synovial fluid, in the setting of unremarkable conventional radiographs, is highly suggestive of a synovial tumor or tumor-like lesion. The provided text states that "More helpful are modern imaging methods such as computed tomography (CT) or magnetic resonance imaging (MRI)" for diagnosis. MRI is superior for soft tissue evaluation and can characterize synovial lesions. Main Distractor: Option D, performing an open biopsy immediately, is premature. While a definitive diagnosis requires histology, advanced imaging like MRI is typically performed first to characterize the lesion, assess its extent, and guide the surgical approach if needed.
Question 45
A 42-year-old female complains of a slowly enlarging, non-tender mass along her wrist flexor tendons for the past year. She denies any trauma or systemic symptoms. Physical examination reveals a firm, mobile mass that moves with tendon excursion. Radiographs of the wrist show no bony abnormalities. Based on the likely origin of this lesion, which of the following is true regarding its potential location?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Joints, bursae, and tendon sheaths have the same type of synovial membrane, so similar tumors can develop from all of these structures." This indicates that synovial tumors and tumor-like lesions, including synovial hemangioma, are not restricted to a single anatomical location but can arise from any structure lined by synovial membrane. Main Distractor: Option A, stating it can only develop within a joint capsule, is incorrect as the text clearly lists bursae and tendon sheaths as other possible sites of origin.
Question 46
A 28-year-old male presents with chronic, intermittent swelling of his ankle joint. He reports no specific injury but notes that the swelling sometimes resolves partially, only to recur. On examination, a mild effusion is present. Arthrocentesis is performed, and the fluid is described as xanthochromic. Conventional radiographs are normal. Which of the following imaging modalities is most likely to provide additional diagnostic information regarding a potential synovial lesion?
View Answer & Explanation
Correct Answer: C
Rationale: The text highlights that "More helpful are modern imaging methods such as computed tomography (CT) or magnetic resonance imaging (MRI)" for diagnosing synovial tumors and tumor-like lesions when conventional radiographs are uninformative. Given the xanthochromic effusion and chronic swelling, a synovial lesion is suspected, making CT a valuable next step for characterizing soft tissue involvement. While MRI is often preferred for soft tissue, CT is also explicitly mentioned as a helpful modern imaging method. Main Distractor: Option A, plain radiographs with stress views, is unlikely to be helpful as the initial radiographs were already normal, and stress views primarily assess ligamentous stability, not soft tissue masses.
Question 47
A 50-year-old patient presents with a several-month history of a progressively enlarging, soft tissue mass around the elbow joint. The mass is palpable and causes some discomfort with movement. Conventional radiographs show no osseous involvement. The patient is concerned about the nature of the mass. What is the definitive method for diagnosing a synovial tumor or tumor-like lesion in most cases?
View Answer & Explanation
Correct Answer: D
Rationale: The provided text explicitly states, "a definitive diagnosis can be obtained, however, after surgical intervention and histological examination of the removed tissue in most cases." This emphasizes that while imaging is helpful, the final diagnosis relies on tissue pathology. Main Distractor: Option C, advanced imaging characteristics, is incorrect as imaging provides strong clues and characterization but is not definitive. Imaging can suggest a diagnosis, but histology confirms it.
Question 48
A 15-year-old athlete presents with recurrent, painful swelling of the knee, particularly after sports activities. The swelling is often accompanied by a feeling of warmth. On physical examination, a diffuse, boggy synovitis is noted, and a moderate effusion is present. Arthrocentesis reveals a bloody aspirate. Conventional radiographs are normal. Considering the possibility of a synovial hemangioma, what is a key characteristic of synovial tumors and tumor-like lesions regarding their clinical presentation?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Th e clinical symptoms of synovial tumors and tumorlike lesions are uniform and present as swelling or visible and palpable masses within and/or around the joints." This directly describes the common presentation. Main Distractor: Option B, that they are usually asymptomatic until very large, is incorrect. While some may be subtle, the text indicates that swelling or a palpable mass is a common presenting symptom, implying they can cause symptoms even before reaching a very large size.
Question 49
A 60-year-old male presents with chronic knee pain and stiffness. Radiographs show degenerative changes but also reveal multiple intra-articular calcifications. This finding is most suggestive of which specific synovial tumor-like lesion, as mentioned in the provided text?
View Answer & Explanation
Correct Answer: C
Rationale: The text specifically mentions, "Conventional radiographs are informative in only a minority of cases, such as synovial chondromatosis." Synovial chondromatosis is characterized by cartilaginous nodules that can calcify and ossify, making them visible on conventional radiographs. Main Distractor: Option A, synovial hemangioma, is incorrect. While it is the chapter's title, the text does not state that synovial hemangiomas are typically visible on conventional radiographs due to calcifications. The text uses synovial chondromatosis as the example where radiographs *are* informative.
Question 50
A 30-year-old female presents with a 3-month history of intermittent, painless swelling of her right wrist. On examination, a soft, ill-defined fullness is noted on the dorsal aspect of the wrist. Arthrocentesis is not performed. Conventional radiographs are normal. Given the general characteristics of synovial tumors and tumor-like lesions, how would you classify the rarity of such conditions?
View Answer & Explanation
Correct Answer: C
Rationale: The very first sentence of the provided text states, "Th e rather rare synovial tumors and tumorlike lesions represent a distinct entity within the family of soft tissue tumors." This directly answers the question about their rarity and classification. Main Distractor: Option B, relatively common, is directly contradicted by the text's description of them as "rather rare."
Question 51
A 12-year-old boy presents with recurrent hemarthrosis of the knee without a history of trauma or coagulopathy. Physical examination reveals a warm, swollen knee with a palpable effusion. Conventional radiographs are unremarkable. Which characteristic of the synovial fluid is most consistent with a synovial hemangioma or similar vascular synovial lesion?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Synovial eff usion, if any, can be blood stained or xanthochromic." Recurrent hemarthrosis (blood in the joint) is a classic presentation for vascular synovial lesions like synovial hemangioma, making blood-stained fluid the most consistent finding. Main Distractor: Option A, clear, viscous fluid, is typical of normal synovial fluid or non-inflammatory effusions, which is inconsistent with recurrent hemarthrosis.
Question 52
A 55-year-old male presents with a chronic, vague ache in his shoulder, accompanied by intermittent swelling. On examination, a subtle fullness is noted in the subacromial region. Conventional radiographs are negative for fracture or dislocation. Given the potential for a synovial tumor or tumor-like lesion, which of the following is true regarding the utility of conventional radiographs?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Conventional radiographs are informative in only a minority of cases, such as synovial chondromatosis." This indicates their limited utility for most synovial tumors and tumor-like lesions. Main Distractor: Option B, informative in a majority of cases, directly contradicts the information provided in the text.
Question 53
A 38-year-old female presents with a 9-month history of a progressively enlarging, soft tissue mass located adjacent to her ankle joint. The mass is firm and mildly tender to palpation. She denies any history of trauma. Conventional radiographs are unremarkable. What is the most appropriate initial advanced imaging study to evaluate this suspected synovial lesion?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "More helpful are modern imaging methods such as computed tomography (CT) or magnetic resonance imaging (MRI)." While both are mentioned, MRI is generally considered superior for soft tissue characterization, especially for synovial lesions, due to its excellent contrast resolution. Given the palpable soft tissue mass, MRI would be the most informative initial advanced imaging. Main Distractor: Option A, diagnostic ultrasound, can be useful for initial evaluation of superficial soft tissue masses, but MRI provides a more comprehensive assessment of the lesion's extent, relationship to adjacent structures, and internal characteristics, which is crucial for synovial lesions.
Question 54
A 25-year-old male presents with a recurrent, painful swelling in his popliteal fossa. On examination, a fluctuant mass is palpable. Arthrocentesis of the knee joint yields a yellowish, slightly cloudy fluid (xanthochromic). Conventional radiographs are normal. What is the primary reason why modern imaging methods like CT or MRI are preferred over conventional radiographs for diagnosing synovial tumors?
View Answer & Explanation
Correct Answer: B
Rationale: The text implies that modern imaging (CT/MRI) is "more helpful" than conventional radiographs. The primary advantage of CT and especially MRI over conventional radiographs in the context of synovial tumors is their superior ability to visualize and characterize soft tissue structures, including the synovial membrane and any associated masses or effusions. Main Distractor: Option C, definitively differentiating benign from malignant lesions without biopsy, is incorrect. While imaging can provide strong clues, the text states that "a definitive diagnosis can be obtained... after surgical intervention and histological examination," indicating that imaging alone is not definitive for malignancy.
Question 55
A 40-year-old patient presents with chronic pain and swelling in the wrist. Physical examination reveals a diffuse, boggy swelling around the carpal bones. Arthrocentesis is performed, and the fluid is noted to be xanthochromic. Given the general characteristics of synovial tumors and tumor-like lesions, what is the significance of xanthochromic synovial fluid?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "Synovial eff usion, if any, can be blood stained or xanthochromic." Xanthochromia refers to a yellowish discoloration, often due to the presence of bilirubin from lysed red blood cells, indicating either a chronic inflammatory process or a previous hemorrhage. This is a recognized feature of synovial tumors and tumor-like lesions, including synovial hemangioma, which can cause intermittent bleeding. Main Distractor: Option E, implying a recent traumatic injury, is incorrect. While trauma can cause bleeding, xanthochromic fluid specifically suggests older blood products or a chronic process, not necessarily an acute injury.
Question 56
A 19-year-old female presents with a 4-month history of a progressively enlarging, soft tissue mass on the dorsum of her foot, near the extensor tendons. The mass is firm, non-tender, and mobile. Conventional radiographs are normal. If this lesion is a synovial tumor or tumor-like lesion, what is the most likely anatomical structure from which it originated?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Joints, bursae, and tendon sheaths have the same type of synovial membrane, so similar tumors can develop from all of these structures." Given the location near the extensor tendons, a tendon sheath origin is highly plausible for a synovial tumor or tumor-like lesion. Main Distractor: Option B, muscle belly, is incorrect. Synovial tumors arise from synovial membranes, not directly from muscle tissue.
Question 57
A 70-year-old male presents with chronic, unexplained knee pain and swelling. He has undergone multiple arthrocenteses, which consistently yield a serosanguinous (blood-tinged) fluid. Conventional radiographs show mild degenerative changes but no specific mass. An MRI is performed, revealing a lobulated intra-articular mass with prominent vascularity. What is the most appropriate next step for definitive diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The text clearly states, "a definitive diagnosis can be obtained, however, after surgical intervention and histological examination of the removed tissue in most cases." Given the chronic symptoms, serosanguinous fluid, and an MRI-identified mass, a biopsy is necessary for definitive diagnosis, especially to rule out malignancy. Main Distractor: Option B, repeating MRI in 6 months, is inappropriate given the chronic symptoms, bloody effusion, and identified mass. Delaying definitive diagnosis could be detrimental if the lesion is malignant or causing ongoing damage.
Question 58
A 33-year-old female presents with a 7-month history of intermittent knee swelling and discomfort. She reports no specific trauma. On examination, a soft, compressible mass is palpable in the medial gutter of the knee. Conventional radiographs are normal. Which of the following statements best describes the nature of synovial tumors and tumor-like lesions?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Th e rather rare synovial tumors and tumorlike lesions represent a distinct entity within the family of soft tissue tumors." This directly addresses their classification and nature. Main Distractor: Option A, typically aggressive malignant neoplasms, is incorrect. While some synovial lesions can be malignant (e.g., synovial sarcoma), the general category of "synovial tumors and tumor-like lesions" encompasses a range of pathologies, many of which are benign, and the text emphasizes their distinct entity rather than universal malignancy.
Question 59
A 48-year-old male presents with chronic, dull pain and swelling in his hip. Physical examination reveals limited range of motion and a deep, ill-defined fullness. Conventional radiographs are unremarkable. An MRI is ordered and shows a diffuse synovial proliferation with hemosiderin deposition. Given the clinical picture and imaging findings, what is the most likely characteristic of the synovial effusion, if present?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Synovial eff usion, if any, can be blood stained or xanthochromic." The MRI finding of hemosiderin deposition strongly suggests previous bleeding, which would manifest as blood-stained or xanthochromic fluid if an effusion were present. This is consistent with lesions like synovial hemangioma or pigmented villonodular synovitis. Main Distractor: Option A, clear and non-viscous, is characteristic of normal or non-inflammatory fluid and contradicts the suspicion of a synovial lesion with hemosiderin deposition.
Question 60
A 65-year-old female presents with a 1-year history of a slowly growing, painless mass on the plantar aspect of her foot, near the metatarsophalangeal joint. The mass is firm and fixed to deeper structures. Conventional radiographs are normal. What is the most common clinical presentation for synovial tumors and tumor-like lesions?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Th e clinical symptoms of synovial tumors and tumorlike lesions are uniform and present as swelling or visible and palpable masses within and/or around the joints." This directly describes the most common presentation. Main Distractor: Option A, acute onset of severe pain and fever, is more indicative of an acute inflammatory or infectious process, not the typical presentation of synovial tumors.
Question 61
A 22-year-old male presents with chronic, intermittent swelling of his elbow joint. He reports no specific injury. On examination, a diffuse, boggy synovitis is noted. Arthrocentesis yields a yellowish, slightly cloudy fluid (xanthochromic). Conventional radiographs are normal. Which of the following statements accurately describes the role of conventional radiographs in diagnosing this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Conventional radiographs are informative in only a minority of cases, such as synovial chondromatosis." This implies that for most synovial tumors and tumor-like lesions, including those causing xanthochromic effusion, conventional radiographs are generally uninformative. Main Distractor: Option A, they are the most sensitive diagnostic tool, is incorrect. The text clearly indicates that modern imaging (CT/MRI) is "more helpful" and that radiographs are informative only in a minority of cases, demonstrating their limited sensitivity for these conditions.
Question 62
A 39-year-old male presents with a 5-month history of a recurrent, painful swelling in his knee. He reports no specific trauma. On examination, a soft, compressible mass is palpable in the suprapatellar pouch. Arthrocentesis yields a blood-stained synovial fluid. An MRI is performed, showing a lobulated intra-articular mass with T2 hyperintensity and flow voids, consistent with a synovial hemangioma. What is the most appropriate next step to achieve a definitive diagnosis and treatment?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "a definitive diagnosis can be obtained, however, after surgical intervention and histological examination of the removed tissue in most cases." Given the strong suspicion of a synovial hemangioma based on MRI and the recurrent symptoms, surgical excision serves both diagnostic (histology) and therapeutic purposes. Main Distractor: Option A, observation with serial MRI scans, is not appropriate for a symptomatic lesion with a strong suspicion of a synovial tumor, as definitive diagnosis and often treatment involve surgical intervention.
Question 63
A 52-year-old female presents with a 6-month history of intermittent pain and swelling in her shoulder. She denies any trauma. Physical examination reveals a mild effusion and a deep, ill-defined fullness. Conventional radiographs are unremarkable. An MRI is performed, showing a synovial lesion. Which of the following anatomical structures, besides joints, can give rise to similar synovial tumors or tumor-like lesions?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Joints, bursae, and tendon sheaths have the same type of synovial membrane, so similar tumors can develop from all of these structures." Therefore, bursae are a recognized site of origin for these lesions. Main Distractor: Option B, articular cartilage, is incorrect. Articular cartilage does not have a synovial membrane and is not a site of origin for synovial tumors.
Question 64
A 12-year-old male presents with recurrent, painful swelling of his knee joint, often associated with activity. Physical examination reveals a palpable, soft mass along the joint line and a mild effusion. Arthrocentesis yields blood-stained synovial fluid. Conventional radiographs are unremarkable. Given the suspicion of a synovial tumor, which imaging modality would be most helpful for further characterization?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical vignette describes symptoms consistent with a synovial tumor, including recurrent swelling and blood-stained effusion, with unremarkable conventional radiographs. The text states that "More helpful are modern imaging methods such as computed tomography (CT) or magnetic resonance imaging (MRI)" for definitive diagnosis. While MRI is often preferred for soft tissue, CT is explicitly mentioned as a helpful modern imaging method. Ultrasound can be useful but often lacks the comprehensive detail of CT or MRI for deep-seated lesions. The main distractor, B) Ultrasound, can identify effusions and some soft tissue masses, but CT or MRI provide superior anatomical detail and characterization for synovial tumors.
Question 65
A 25-year-old female complains of a slowly growing, painless mass in her wrist for the past 6 months. On examination, a soft, mobile, non-tender mass is palpable over the extensor tendon sheaths. The patient denies any trauma. Based on the potential origin of such a lesion, which of the following structures is most likely involved?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that "Joints, bursae, and tendon sheaths have the same type of synovial membrane, so similar tumors can develop from all of these structures." A mass over the extensor tendon sheaths points directly to the synovial membrane of the tendon sheath as the origin for a synovial tumor or tumor-like lesion. The main distractor, D) Joint capsule ligaments, while anatomically close, are not composed of synovial membrane and are therefore not the primary origin for synovial tumors.
Question 66
A 40-year-old male presents with chronic knee pain and intermittent swelling. Arthrocentesis reveals a xanthochromic effusion. Conventional radiographs are normal. An MRI suggests a vascular-appearing mass within the joint. What is the most appropriate next step to achieve a definitive diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that "a definitive diagnosis can be obtained, however, after surgical intervention and histological examination of the removed tissue in most cases." Given the suspicion of a synovial tumor (like a hemangioma suggested by the vascular appearance on MRI and xanthochromic effusion), surgical intervention (diagnostic arthroscopy) with biopsy for histological examination is the definitive diagnostic step. The main distractor, A) Repeat MRI with contrast, while potentially providing more imaging detail, does not provide a definitive histological diagnosis, which is crucial for synovial tumors.
Question 67
A 7-year-old girl presents with recurrent hemarthrosis of the elbow without a history of trauma. Physical examination reveals a subtle, soft swelling around the joint. Conventional radiographs are normal. The most likely characteristic of the synovial fluid, if aspirated, would be:
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Synovial effusion, if any, can be blood stained or xanthochromic." Recurrent hemarthrosis in a child without trauma is highly suggestive of a synovial hemangioma or other vascular synovial lesion. Therefore, the aspirated fluid would most likely be blood-stained or xanthochromic. The main distractor, A) Clear and viscous, describes normal synovial fluid, which is inconsistent with recurrent hemarthrosis.
Question 68
A 30-year-old male presents with a several-month history of intermittent knee swelling and pain. He reports no specific injury. On examination, a subtle, diffuse swelling is noted, but no distinct mass is palpable. Conventional radiographs are unremarkable. Which of the following statements regarding the diagnostic utility of conventional radiographs for synovial tumors is most accurate?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Conventional radiographs are informative in only a minority of cases, such as synovial chondromatosis." This indicates their limited utility for most synovial tumors, including synovial hemangiomas, where soft tissue changes are primary. The main distractor, A) They are highly sensitive for detecting early synovial tumors, is incorrect as conventional radiographs often miss early soft tissue lesions and are not sensitive for synovial tumors in general.
Question 69
A 15-year-old athlete presents with chronic ankle pain and swelling that worsens with activity. Physical examination reveals a diffuse, boggy swelling around the joint. An MRI has been ordered to evaluate for a potential synovial lesion. What is the primary reason MRI is considered more helpful than conventional radiographs in this scenario?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "More helpful are modern imaging methods such as computed tomography (CT) or magnetic resonance imaging (MRI)." MRI's primary advantage over conventional radiographs in evaluating synovial tumors and tumor-like lesions is its superior ability to visualize and characterize soft tissue structures, including the synovial membrane, effusions, and masses. The main distractor, C) MRI exposes the patient to less radiation, is true compared to CT, but the primary diagnostic advantage over radiographs for synovial lesions is soft tissue detail, not radiation exposure.
Question 70
A 50-year-old woman presents with a 9-month history of a slowly enlarging, non-tender mass in her popliteal fossa. The mass is palpable and appears to be associated with the knee joint. Given the general characteristics of synovial tumors, what is the most common clinical presentation for such a lesion?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "The clinical symptoms of synovial tumors and tumorlike lesions are uniform and present as swelling or visible and palpable masses within and/or around the joints." This directly matches the description of the most common clinical presentation. The main distractor, A) Acute, severe pain with fever, is more indicative of an acute inflammatory or infectious process, not the typical presentation of a synovial tumor.
Question 71
A 10-year-old boy presents with recurrent knee swelling and pain. An MRI suggests a lobulated mass within the suprapatellar pouch, consistent with a synovial hemangioma. The patient's parents inquire about the rarity of this condition. Based on the provided text, how are synovial tumors generally characterized in terms of incidence?
View Answer & Explanation
Correct Answer: B
Rationale: The text begins by stating, "The rather rare synovial tumors and tumorlike lesions represent a distinct entity within the family of soft tissue tumors." This directly indicates their rarity. The main distractor, A) They are among the most common soft tissue tumors, is incorrect as the text clearly states they are "rather rare."
Question 72
A 35-year-old male presents with chronic pain and swelling in his shoulder. An MRI reveals a mass within the subacromial bursa. Given that synovial tumors can arise from various synovial-lined structures, which of the following is also a common site of origin for such lesions?
View Answer & Explanation
Correct Answer: D
Rationale: The text states, "Joints, bursae, and tendon sheaths have the same type of synovial membrane, so similar tumors can develop from all of these structures." Therefore, tendon sheaths are a common site of origin for synovial tumors, alongside joints and bursae. The main distractor, A) Muscle belly, is incorrect as muscle tissue does not contain synovial membrane and is not a site of origin for synovial tumors.
Question 73
A 14-year-old girl presents with a several-month history of intermittent knee swelling and pain. Physical examination reveals a subtle effusion. Arthrocentesis is performed, and the fluid is noted to be xanthochromic. This finding is most suggestive of which of the following?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Synovial effusion, if any, can be blood stained or xanthochromic." Xanthochromia (yellowish discoloration) in synovial fluid typically indicates the presence of old blood products or a chronic inflammatory process. In the context of a potential synovial tumor like a hemangioma, it suggests chronic microhemorrhages or a long-standing effusion. The main distractor, A) Acute bacterial arthritis, would typically present with a purulent effusion, not xanthochromic fluid.
Question 74
A 45-year-old male presents with a chronic, vague ache in his hip, accompanied by intermittent swelling. Physical examination is largely unremarkable, but an MRI reveals a soft tissue mass within the hip joint. The patient is concerned about the nature of the mass. What is the most reliable method to differentiate between a benign synovial tumor and a malignant one?
View Answer & Explanation
Correct Answer: D
Rationale: The text clearly states, "a definitive diagnosis can be obtained, however, after surgical intervention and histological examination of the removed tissue in most cases." Histological examination is the gold standard for differentiating between benign and malignant lesions and for definitive subtyping of tumors. The main distractor, B) Advanced imaging characteristics (CT/MRI), while helpful for characterization and surgical planning, cannot provide a definitive histological diagnosis.
Question 75
A 22-year-old female presents with a 3-month history of a painful, palpable mass in her wrist, located near the carpal bones. Imaging studies are inconclusive regarding the exact nature of the mass. If this is a synovial tumor, what is the most likely initial step in its management after imaging?
View Answer & Explanation
Correct Answer: C
Rationale: The text emphasizes that "a definitive diagnosis can be obtained... after surgical intervention and histological examination of the removed tissue in most cases." For a palpable mass suspected to be a synovial tumor, surgical excision serves both diagnostic and often therapeutic purposes. The main distractor, D) Long-term observation, is generally not appropriate for an undiagnosed, palpable mass that could be a tumor, especially if symptomatic.
Question 76
A 60-year-old male presents with chronic knee pain and a history of intermittent swelling. Conventional radiographs show no significant abnormalities. An MRI is performed and reveals a soft tissue mass within the joint. Which of the following conditions is specifically mentioned in the text as an exception where conventional radiographs *can* be informative for synovial lesions?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Conventional radiographs are informative in only a minority of cases, such as synovial chondromatosis." This condition involves cartilaginous metaplasia within the synovium, which can calcify and become visible on plain radiographs. The main distractor, A) Synovial hemangioma, is a soft tissue lesion that typically does not show up on conventional radiographs unless there are secondary changes like phleboliths, which are not consistently present or diagnostic.
Question 77
A 17-year-old female presents with recurrent, unexplained knee effusions. Arthrocentesis has consistently yielded blood-stained fluid. Despite multiple aspirations, the effusion recurs. Given the suspicion of a synovial hemangioma, what is the primary reason for the recurrent blood-stained effusion?
View Answer & Explanation
Correct Answer: C
Rationale: While the text doesn't explicitly define "hemangioma," its name implies a vascular lesion. The text states that synovial effusions "can be blood stained or xanthochromic." In the context of a synovial hemangioma, the recurrent blood-stained effusion is due to the fragile, vascular nature of the lesion, which can bleed into the joint space with activity or minor trauma. The main distractor, D) Traumatic injury to the joint capsule, is less likely to cause recurrent, unexplained hemarthrosis without a clear history of repeated trauma.
Question 78
A 28-year-old male presents with a several-month history of intermittent swelling and discomfort in his wrist. Physical examination reveals a subtle, soft mass near the radiocarpal joint. An MRI is performed and suggests a synovial lesion. Which of the following statements best describes the relationship between synovial tumors and tumor-like lesions?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "The rather rare synovial tumors and tumorlike lesions represent a distinct entity within the family of soft tissue tumors." This indicates that they are grouped together as a specific category of soft tissue lesions originating from synovial tissue. The main distractor, A) They are entirely distinct entities with no shared characteristics, is incorrect as the text groups them together as a "distinct entity" implying shared characteristics related to their synovial origin.
Question 79
A 19-year-old female presents with chronic knee pain and swelling. An MRI reveals a synovial mass. The patient is concerned about the diagnostic process. According to the provided text, what is the most definitive method for diagnosing a synovial tumor?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states, "a definitive diagnosis can be obtained, however, after surgical intervention and histological examination of the removed tissue in most cases." This highlights that while imaging is helpful, the final diagnosis relies on tissue pathology. The main distractor, B) Advanced imaging (CT or MRI), is helpful for characterization and localization but does not provide a definitive histological diagnosis.
Question 80
A 42-year-old male presents with a several-month history of intermittent swelling and discomfort in his elbow. Physical examination reveals a palpable, soft mass within the olecranon bursa. If this is a synovial tumor, from which specific tissue type does it originate?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Joints, bursae, and tendon sheaths have the same type of synovial membrane, so similar tumors can develop from all of these structures." A mass within the olecranon bursa, which is lined by synovial membrane, would originate from this tissue type. The main distractor, A) Fibrous connective tissue, while present in the bursa, is not the specific origin for *synovial* tumors.
Question 81
A 9-year-old boy presents with a history of recurrent, painful swelling in his knee. Physical examination reveals a mild effusion and a subtle, soft tissue fullness. Conventional radiographs are normal. An MRI is performed and shows a vascular-appearing mass within the joint. Which of the following is a key characteristic of the clinical symptoms of synovial tumors and tumor-like lesions?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "The clinical symptoms of synovial tumors and tumorlike lesions are uniform and present as swelling or visible and palpable masses within and/or around the joints." This is the most accurate description of their typical presentation. The main distractor, C) Exclusively cause acute, severe pain, is incorrect as the pain can be chronic or intermittent, and swelling/masses are the primary features.
Question 82
A 55-year-old female presents with chronic shoulder pain and a palpable mass. An MRI suggests a synovial lesion. The patient asks if a simple aspiration of the mass would be sufficient for diagnosis. Based on the provided text, why is aspiration alone generally insufficient for a definitive diagnosis of a synovial tumor?
View Answer & Explanation
Correct Answer: B
Rationale: The text clearly states, "a definitive diagnosis can be obtained, however, after surgical intervention and histological examination of the removed tissue in most cases." Aspiration typically yields fluid, which may show some cellular elements, but it rarely provides sufficient tissue architecture for a definitive histological diagnosis of a synovial tumor. The main distractor, D) Aspiration can spread tumor cells, while a concern for some malignant tumors, is not the primary reason cited in the text for why aspiration is insufficient for *definitive diagnosis* of synovial tumors in general.
Question 83
A 3-year-old male presents with disproportionate short stature and bowing of the legs. Physical examination reveals genu varum, varus ankle deformities, and short, pudgy hands and feet. Radiographs of the hands show metaphyseal shortening of the metacarpals and phalanges, while radiographs of the lower extremities demonstrate metaphyseal changes in the long bones with normal epiphyses. Which of the following is the most likely diagnosis?

View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of disproportionate short stature, genu varum, varus ankle deformities, short and pudgy hands/feet, and radiographic findings of metaphyseal shortening with normal epiphyses are classic for Metaphyseal Dysplasia, McKusick type (also known as cartilage-hair hypoplasia). Achondroplasia typically involves rhizomelic dwarfism and specific epiphyseal/metaphyseal growth plate abnormalities, but not the specific hand/foot findings or the "rachitic rosary" associated with McKusick. Spondyloepiphyseal and multiple epiphyseal dysplasias primarily affect the epiphyses, which are described as normal in this case. Osteogenesis imperfecta is characterized by bone fragility and fractures, not primarily metaphyseal dysplasia.
Question 84
A 5-year-old female is diagnosed with Metaphyseal Dysplasia, McKusick type, based on clinical features including short stature, genu varum, and characteristic radiographic findings. Her parents are concerned about the genetic implications for future children. What is the inheritance pattern of McKusick type metaphyseal dysplasia?
View Answer & Explanation
Correct Answer: B
Rationale: McKusick type metaphyseal dysplasia, also known as cartilage-hair hypoplasia, is transmitted as an autosomal recessive trait. This is a key distinguishing feature from the Schmid type, which is autosomal dominant. Understanding the inheritance pattern is crucial for genetic counseling. Autosomal dominant inheritance (A) is characteristic of Schmid type, making it a common distractor.
Question 85
A 2-year-old male presents with short stature and difficulty with ambulation. Clinical examination reveals short and pudgy hands and feet. Radiographs of the hands, as shown in the image, demonstrate metaphyseal shortening of the metacarpals and phalanges. These hand findings are characteristic of which type of metaphyseal dysplasia?
View Answer & Explanation
Correct Answer: D
Rationale: The description of "short and pudgy hands and feet" with metaphyseal shortening of metacarpals and phalanges on radiographs is a typical deformity seen in McKusick type metaphyseal dysplasia (cartilage-hair hypoplasia). While other types of metaphyseal dysplasia exist, the specific clinical and radiographic hand findings described are most characteristic of McKusick type. Schmid type (A) typically has milder upper extremity involvement.
Question 86
A 4-year-old child with a known diagnosis of Metaphyseal Dysplasia, McKusick type, is being evaluated for lower extremity deformities. Which of the following is a characteristic finding in the lower extremities for this condition?
View Answer & Explanation
Correct Answer: C
Rationale: In McKusick type metaphyseal dysplasia, genu varum and varus ankle deformity due to distal fibular overgrowth are characteristic lower extremity findings. Coxa vara (A) is characteristic of Schmid type metaphyseal dysplasia, making it a key distractor. Genu valgum (B) is the opposite of the typical genu varum seen. Hip flexion contractures and patellar instability are not specifically highlighted as characteristic features of McKusick type.
Question 87
A 1-year-old infant presents with disproportionate short stature and recurrent respiratory infections. On physical examination, the pediatrician notes prominent costochondral junctions, described as a "rachitic rosary." This finding, in the context of metaphyseal dysplasia, is most characteristic of which specific type?
View Answer & Explanation
Correct Answer: C
Rationale: Chest-wall involvement with enlargement of costochondral junctions, causing a "rachitic rosary," is a specific and characteristic finding of McKusick type metaphyseal dysplasia (cartilage-hair hypoplasia). While other forms of metaphyseal dysplasia exist, this particular chest wall manifestation is explicitly linked to the McKusick type in the provided text. Schmid type (A) does not typically present with a rachitic rosary.
Question 88
A 6-month-old infant is diagnosed with metaphyseal dysplasia. The parents report a history of frequent infections and poor weight gain. Which of the following systemic associations is frequently observed in younger children with metaphyseal dysplasia, including the McKusick type?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states that metaphyseal dysplasia "frequently associates with malabsorption, neutropenia and recurrent infections in younger children." These systemic issues are important to recognize in the overall management of patients with this condition, including the McKusick type. The other options are not specifically mentioned as frequent associations for metaphyseal dysplasia in the provided text.
Question 89
A genetic counselor is discussing two distinct forms of metaphyseal dysplasia with a family. One form, Schmid type, is known to present later and is transmitted in an autosomal dominant manner. The other form, McKusick type, is characterized by disproportionate short stature and short, pudgy hands. What is the primary genetic difference between Schmid type and McKusick type metaphyseal dysplasia?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that "Schmid-type is transmitted in autosomal dominant manner" and "McKusick type also called cartilage-hair hypoplasia, is transmitted as an autosomal recessive trait." This difference in inheritance pattern is a fundamental distinction between these two types of metaphyseal dysplasia. Option A is incorrect as Schmid is autosomal dominant. Option C, D, and E are incorrect based on the stated inheritance patterns.
Question 90
A 7-year-old boy presents with short stature and bowing of the lower extremities. His upper extremities show mild wrist swelling and elbow flexion contractures. Radiographs reveal metaphyseal changes in the long bones and characteristic coxa vara. Based on these findings, which type of metaphyseal dysplasia is most likely?
View Answer & Explanation
Correct Answer: B
Rationale: The description of "mild upper extremity involvement, evidenced by wrist swelling and flexion contractures of the elbows" along with "characteristic coxa vara" and bowing of tibia and femur, points to Schmid type metaphyseal dysplasia. McKusick type (A) typically presents with short and pudgy hands and feet, and distal fibular overgrowth, rather than coxa vara or elbow flexion contractures.
Question 91
A 10-year-old patient with metaphyseal dysplasia presents with significant bowing of the tibia and femur, and characteristic coxa vara. In contrast, a 3-year-old patient with a different type of metaphyseal dysplasia presents with genu varum and varus ankle deformity due to distal fibular overgrowth. Which of the following correctly pairs the lower extremity findings with the specific type of metaphyseal dysplasia?
View Answer & Explanation
Correct Answer: B
Rationale: The teaching case clearly differentiates these features: "Schmid-type... presents with bowing of tibia and femur, with characteristic coxa vara." In contrast, "McKusick type... with genu varum and varus ankle deformity due to distal fibular overgrowth." Therefore, coxa vara is characteristic of Schmid type, and distal fibular overgrowth leading to varus ankle deformity is characteristic of McKusick type.
Question 92
A 1-year-old child presents with short stature. Radiographs of the hands, as depicted in the image, show metaphyseal shortening of the metacarpals and phalanges. What is the primary radiographic characteristic of metaphyseal dysplasia in the tubular bones?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states that "Metaphyseal dysplasia is characterized by typical radiographical changes in the metaphyses of the short and long tubular bones, with normal epiphyses." The image also highlights "metaphyseal shortening of the metacarpals and phalanges." Options A, B, D, and E describe findings characteristic of other skeletal dysplasias or conditions, but not the defining radiographic feature of metaphyseal dysplasia.
Question 93
A 4-year-old child is undergoing radiographic evaluation for short stature. The radiologist notes characteristic changes in the metaphyses of the long tubular bones, while the epiphyses appear normal. This pattern is consistent with a diagnosis of metaphyseal dysplasia. Which of the following best describes the typical radiographic appearance of the epiphyses in metaphyseal dysplasia?
View Answer & Explanation
Correct Answer: C
Rationale: A defining characteristic of metaphyseal dysplasia, as stated in the text, is "typical radiographical changes in the metaphyses of the short and long tubular bones, with normal epiphyses." This distinction helps differentiate it from epiphyseal dysplasias. Options A and B describe features of epiphyseal dysplasias, making them incorrect for metaphyseal dysplasia.
Question 94
A pediatrician is counseling the parents of a newborn diagnosed with Metaphyseal Dysplasia, McKusick type. The parents are curious about the prevalence of this condition. In which specific population is the incidence of McKusick type metaphyseal dysplasia notably higher, approximately 1/1,000 live births?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case explicitly states: "In Amish population the incidence is 1/1,000 live births, but in other populations it is less frequent than the Schmidt type." This high incidence in the Amish population is a well-known epidemiological fact for McKusick type metaphyseal dysplasia (cartilage-hair hypoplasia). The other populations are not noted to have a similarly high incidence for this specific condition.
Question 95
A 3-year-old child is referred to an orthopedic surgeon due to concerns about growth. The child's height is significantly below average for age, and the parents note that the trunk appears relatively normal in length compared to the limbs. This clinical presentation of "disproportionate short stature" is a characteristic feature of which type of metaphyseal dysplasia?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that "Disproportionate short stature is characteristic" of McKusick type metaphyseal dysplasia. While other forms of short stature exist, the disproportionate nature, often with relatively shorter limbs compared to the trunk, is a hallmark of McKusick type. Schmid type (A) also causes decreased standing height, but the term "disproportionate short stature" is specifically used for McKusick.
Question 96
A 6-year-old patient diagnosed with Metaphyseal Dysplasia, McKusick type, presents with a progressive varus deformity of the ankles. Radiographic evaluation confirms the varus ankle deformity. What is the specific anatomical cause for this deformity in McKusick type metaphyseal dysplasia?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case explicitly states that in McKusick type, there is "varus ankle deformity due to distal fibular overgrowth." This specific mechanism is a key diagnostic feature and understanding it is important for potential surgical planning. Proximal tibial varus (E) would contribute to genu varum, but the specific ankle deformity is due to the fibular overgrowth.
Question 97
A 9-month-old infant with suspected Metaphyseal Dysplasia, McKusick type, is examined. The physician notes palpable and visible enlargements at the costochondral junctions, giving the appearance of a "rachitic rosary." This finding indicates involvement of which anatomical region?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that "Chest-wall involvement with enlargement of costochondral junctions causes 'rachitic rosary'." This clinical sign specifically refers to the junctions between the ribs and their cartilages in the chest wall. While long bone metaphyses (E) are affected in metaphyseal dysplasia, the "rachitic rosary" specifically describes the chest wall manifestation.
Question 98
A 12-year-old boy presents with progressive bowing of his legs and a waddling gait. Radiographs show significant varus deformity of the knees and ankles, bowing of the tibia and femur, and characteristic coxa vara. These findings are most consistent with which type of metaphyseal dysplasia?
View Answer & Explanation
Correct Answer: B
Rationale: The combination of "varus deformity of the ankles and knees is present with bowing of tibia and femur, with characteristic coxa vara" is explicitly described as a feature of Schmid type metaphyseal dysplasia. McKusick type (A) also has genu varum and varus ankles, but specifically due to distal fibular overgrowth, and does not mention coxa vara as a characteristic feature for McKusick, but rather for Schmid.
Question 99
A 9-year-old girl is diagnosed with Schmid type metaphyseal dysplasia. Her parents inquire about potential upper extremity involvement. Which of the following is typically observed in the upper extremities in Schmid type metaphyseal dysplasia?
View Answer & Explanation
Correct Answer: B
Rationale: The text states that in Schmid type, "Upper extremity involvement is mild, evidenced by wrist swelling and flexion contractures of the elbows." This indicates that while not as prominent as lower extremity issues, there are specific upper extremity manifestations. Severe brachydactyly (A) is more characteristic of McKusick type (short, pudgy hands). Normal upper extremity appearance (D) is incorrect as mild involvement is noted.
Question 100
A 2-year-old child presents with skeletal abnormalities. Radiographs show significant widening and irregularity of the metaphyses of the long bones. The epiphyses, however, appear well-formed and of normal size. This specific radiographic pattern, with normal epiphyses, is a hallmark of which general category of skeletal dysplasia?
View Answer & Explanation
Correct Answer: C
Rationale: The defining characteristic of metaphyseal dysplasia, as stated in the text, is "typical radiographical changes in the metaphyses of the short and long tubular bones, with normal epiphyses." This differentiates it from conditions primarily affecting the epiphyses (D), diaphyses (B), or both epiphyses and spine (A, E). The vignette directly describes this key feature.
You Might Also Like
