Orthopedic Oncology Board Review: Soft Tissue Sarcomas, Chondroblastoma & Fibromatosis | Part 17

Key Takeaway
This Orthopedic Oncology Board Review covers key topics in musculoskeletal tumors, including soft tissue sarcomas (Atypical Lipomatous Tumors, Well-Differentiated Liposarcomas), chondroblastoma, and aggressive fibromatosis. It details clinical presentation, diagnostic imaging (MRI), pathology, and surgical management strategies for these complex conditions, crucial for exam preparation.
Question 1
A 58-year-old male presents to the clinic complaining of a firm mass in his posterior thigh. He states it has been present for approximately six months and has recently increased slightly in size. He denies any pain, numbness, or weakness associated with the mass.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical text states that patients with soft tissue sarcomas will note a firm mass that usually has been present for several months and that lesions are usually asymptomatic. Severe pain, rapid onset, systemic symptoms, or neurological deficits are less common initial presentations. Main Distractor: B) Severe, localized pain. Soft tissue sarcomas are typically asymptomatic, making severe pain an unlikely initial presentation.
Question 2
A 45-year-old female presents with a palpable, firm, non-tender mass located just beneath the skin in her proximal forearm. She is concerned about its nature.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical text states that "although most often these lesions will occur in a deep, subfascial location, approximately one in three soft tissue sarcomas occurs in the subcutaneous tissues." Main Distractor: C) Approximately one in two. While a significant proportion, the text specifically states "one in three" for subcutaneous locations, with the majority being deep.
Question 3
A 62-year-old male presents with a slowly enlarging, firm mass in his medial thigh. Plain radiographs of the thigh are obtained as part of the initial workup.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical text states that "radiographs are frequently negative, but may show a masslike area of soft tissue fullness." Cortical destruction or periosteal reaction are more typical of primary bone tumors or aggressive infections. Main Distractor: B) Cortical destruction of the adjacent bone. While possible in advanced cases, plain radiographs are frequently negative for soft tissue sarcomas, and cortical destruction is not the most common initial finding.
Question 4
A 50-year-old female presents with a firm, deep-seated mass in her calf. An MRI is performed to further characterize the lesion. On T1-weighted images, the mass appears similar in signal intensity to the surrounding muscle.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical text states that "Most soft tissue sarcomas are isodense with the adjacent muscle. Many soft tissue sarcomas have nonspecific signal characteristics on MRI, with low to intermediate signal intensity on T1." Main Distractor: B) Markedly high signal intensity, brighter than fat. This is incorrect; fat would be high signal on T1, and sarcomas are typically low to intermediate, isointense with muscle.
Question 5
A 68-year-old male presents with a large, firm mass in his proximal thigh. An MRI is performed, and on T2-weighted images, the lesion shows varying bright areas within it.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical text describes MRI characteristics of soft tissue sarcomas as having "heterogeneous primarily high signal intensity on T2." Main Distractor: B) Homogeneous low signal intensity. This is incorrect; sarcomas typically show high signal on T2, and often with heterogeneity, not homogeneous low signal.
Question 6
A 55-year-old female undergoes an MRI with gadolinium for a suspected soft tissue sarcoma in her gluteal region. The radiologist notes that the mass shows areas of enhancement but it is not uniform throughout the lesion.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical text states that soft tissue sarcomas exhibit "variable enhancement with gadolinium." Main Distractor: B) No enhancement with gadolinium. Malignant lesions typically enhance due to increased vascularity and capillary permeability, so no enhancement would be atypical for a sarcoma.
Question 7
A 70-year-old male presents with a rapidly growing, large mass in his popliteal fossa. MRI reveals a large, complex lesion with internal areas of fluid signal and signal voids.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical text states that "Areas of necrosis and/or hemorrhage are common in large lesions." These features contribute to the heterogeneous appearance on MRI. Main Distractor: B) Extensive calcification. While some sarcomas can calcify, the text specifically highlights necrosis and hemorrhage as common features in large lesions, which would correspond to fluid signal and signal voids.
Question 8
A 65-year-old patient presents with a mass near the elbow that has broken through the skin, appearing as an ulcerated, exophytic lesion.
View Answer & Explanation
Correct Answer: A
Rationale: Fig. 9.14 is described as "Subcutaneous soft tissue sarcoma fungating through the skin near the elbow." This directly matches the description of the image and the clinical presentation. Main Distractor: B) Deep intramuscular location with intact overlying skin. The image clearly shows a superficial lesion that has breached the skin, contradicting a deep intramuscular location with intact skin.
Question 9
A 52-year-old male presents with a firm mass in his proximal forearm. An MRI is performed to evaluate the extent and characteristics of the lesion.
View Answer & Explanation
Correct Answer: A
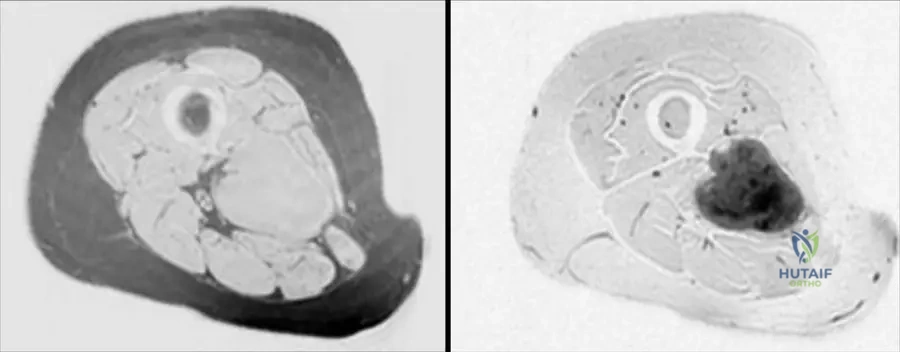
Rationale: The clinical context for Fig. 9.15 states: "Axial T1(a) and T2-weighted image with gadolinium and fat saturation (b) showing a heterogeneous soft tissue sarcoma in the proximal forearm that is predominantly in the subcutaneous tissues abutting the adjacent myofascial plane." Main Distractor: B) Entirely within the deep muscular compartment. The image context explicitly states the lesion is "predominantly in the subcutaneous tissues," which contradicts a purely deep muscular location.
Question 10
A 60-year-old female presents with a growing mass in her proximal forearm. MRI images are obtained to characterize the lesion.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 9.15 describes the lesion as a "heterogeneous soft tissue sarcoma." Heterogeneity is a common feature of sarcomas due to varying cellularity, necrosis, and hemorrhage. Main Distractor: B) Uniform signal intensity throughout the mass. This is incorrect, as the text explicitly describes the sarcoma in this image as "heterogeneous."
Question 11
A 48-year-old male presents with a firm mass in his lower leg. MRI is performed to assess the lesion's relationship to surrounding structures.

View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 9.17 states: "Proton density (a), T2 (b), images of the lesion. Note the heterogeneity and intimate association with the fibula." Main Distractor: B) Tibia. While the tibia is in the lower leg, the text specifically mentions the "intimate association with the fibula" for this particular image.
Question 12
A 59-year-old patient underwent surgical resection of a mass in the lower leg, which included a portion of the proximal fibula due to its close proximity to the tumor. The resected specimen is shown.

View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 9.18 explicitly states: "Resected proximal fibula with adjacent liposarcoma." Main Distractor: B) Malignant fibrous histiocytoma (MFH). While MFH is a type of soft tissue sarcoma mentioned in the general text, the specific image context identifies the tumor as a liposarcoma.
Question 13
A 63-year-old male presents with a deep-seated mass in his thigh. An MRI is performed to characterize the lesion. The axial T1-weighted image is shown.
View Answer & Explanation
Correct Answer: A
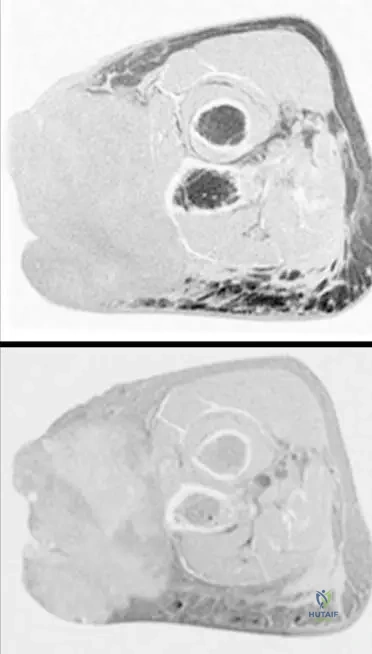
Rationale: The clinical context for Fig. 9.19 states: "Axial T1(a) and axial T2-weighted MRI with fat saturation (b) showing typical MRI features of a soft tissue sarcoma with intermediate signal intensity on T1 (isointense with muscle)." Main Distractor: B) Markedly high signal intensity, brighter than fat. This is incorrect; T1 signal for STS is typically intermediate, isointense with muscle, not markedly high like fat.
Question 14
A 63-year-old male presents with a deep-seated mass in his thigh. An MRI is performed to characterize the lesion. The axial T2-weighted MRI with fat saturation is shown.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 9.19 states: "Axial T1(a) and axial T2-weighted MRI with fat saturation (b) showing typical MRI features of a soft tissue sarcoma with intermediate signal intensity on T1 (isointense with muscle) and markedly heterogeneous predominantly high signal intensity on T2." Main Distractor: B) Homogeneous low signal intensity. This is incorrect; sarcomas typically show high signal on T2, and often with heterogeneity, not homogeneous low signal.
Question 15
A 63-year-old male presents with a deep-seated mass in his thigh. An MRI is performed to characterize the lesion and its anatomical origin.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 9.19 states: "Note that the tumor originates within the deep muscular compartment of the thigh." Main Distractor: B) Subcutaneous compartment. While some sarcomas are subcutaneous, the text specifically states this particular tumor (Fig 9.19) originates in the "deep muscular compartment."
Question 16
A 55-year-old male presents with a slowly enlarging, painless mass in his posterior thigh for the past two years. On examination, the mass is soft, mobile, and non-tender. MRI reveals a large, fat-containing lesion with some thickened septa and a few nodular, non-lipomatous areas. Core needle biopsy confirms an atypical lipomatous tumor.
View Answer & Explanation
Correct Answer: C
Rationale: Atypical lipomatous tumors (ALT), also known as well-differentiated liposarcomas, are locally aggressive tumors that require wide local excision with clear margins to minimize the risk of local recurrence. Marginal excision has a high recurrence rate. Observation is inappropriate for a confirmed ALT. Neoadjuvant radiation is not typically indicated for ALTs unless margins are expected to be very close or positive, and amputation is overly aggressive. The main distractor, marginal excision, is incorrect because it is associated with a high local recurrence rate for ALTs.
Question 17
A 48-year-old female presents with a deep-seated, palpable mass in her shoulder region. MRI demonstrates a large, predominantly fat-containing lesion with areas of non-adipose tissue and prominent, thick septations. A core needle biopsy is performed, and the pathologist reports findings consistent with an atypical lipomatous tumor. Which of the following genetic alterations is most characteristic of this tumor?
View Answer & Explanation
Correct Answer: C
Rationale: Atypical lipomatous tumors (ALT) / well-differentiated liposarcomas are characterized by supernumerary ring chromosomes and giant rod chromosomes, which result in amplification of the 12q13-15 region, including the MDM2 and CDK4 genes. These amplifications are crucial for diagnosis and distinguish ALTs from benign lipomas. FUS-DDIT3 fusion is characteristic of myxoid liposarcoma. EWSR1-FLI1 translocation is seen in Ewing sarcoma. COL1A1-PDGFB fusion is associated with dermatofibrosarcoma protuberans. H3F3A mutation is found in giant cell tumor of bone and chondroblastoma. The main distractor, FUS-DDIT3 fusion, is incorrect as it is associated with myxoid liposarcoma, not atypical lipoma.
Question 18
A 62-year-old male has a history of a resected atypical lipomatous tumor from his retroperitoneum five years ago. He now presents with new abdominal discomfort. Imaging reveals a large, heterogeneous mass in the retroperitoneum with both fatty and significant non-lipomatous components, including areas of necrosis and increased metabolic activity on PET scan. Biopsy shows a high-grade spindle cell component alongside well-differentiated liposarcoma areas.
View Answer & Explanation
Correct Answer: C
Rationale: Atypical lipomatous tumors (ALT) / well-differentiated liposarcomas, particularly in deep-seated locations like the retroperitoneum, have the potential to dedifferentiate into higher-grade non-lipogenic sarcomas. This dedifferentiation is characterized by the emergence of a high-grade spindle cell or pleomorphic sarcoma component within or adjacent to the well-differentiated liposarcoma. This is a significant prognostic event. While it is a form of local recurrence, the specific term "dedifferentiation" best describes the change in tumor biology. ALTs do not metastasize. A new primary sarcoma is less likely given the history and location. Benign fibrous histiocytoma is not consistent with the aggressive features described. The main distractor, local recurrence of atypical lipoma, is partially correct but less precise, as the tumor has undergone a significant biological transformation (dedifferentiation) rather than just a simple recurrence of the original low-grade tumor.
Question 19
A 38-year-old female presents with a 3 cm, soft, mobile, subcutaneous mass on her forearm that has been present for several years without significant change. MRI shows a homogeneous, fat-attenuating lesion with thin septa, consistent with a benign lipoma. However, the patient requests excision. During the procedure, the surgeon notes the mass is well-encapsulated and easily shelled out. Histopathology confirms a benign lipoma. Which of the following features, if present on MRI, would have raised suspicion for an atypical lipomatous tumor and prompted further workup?
View Answer & Explanation
Correct Answer: D
Rationale: While benign lipomas are typically homogeneous fat-attenuating lesions with thin septa, atypical lipomatous tumors (ALT) often demonstrate features on MRI that suggest a more aggressive nature. These include thickened septa (often defined as >2mm), nodular non-lipomatous components, and areas of enhancement. A capsule, homogeneous fat signal, and subcutaneous location are typical of benign lipomas. Small size does not rule out an ALT, but larger, deep-seated lesions are more suspicious. The main distractor, presence of a capsule, is incorrect because both benign lipomas and ALTs can be encapsulated, and a capsule alone does not differentiate them.
Question 20
A 70-year-old male presents with a large, deep-seated mass in his popliteal fossa. MRI shows a 10 cm, predominantly fat-containing lesion with several thick septa and a few enhancing solid nodules. A core needle biopsy is performed, and the pathology report indicates an atypical lipomatous tumor. What is the most appropriate next step in management?
View Answer & Explanation
Correct Answer: C
Rationale: Once an atypical lipomatous tumor (ALT) is diagnosed by core needle biopsy, the definitive treatment is wide local excision with clear margins. Observation is inappropriate for a confirmed ALT due to its locally aggressive nature and potential for dedifferentiation. An incisional biopsy is generally not necessary if the core needle biopsy is diagnostic and representative. Radiation therapy and chemotherapy are not primary treatments for ALTs, though radiation may be considered in cases of positive or very close margins after surgery, or for dedifferentiated lesions. The main distractor, close observation with serial MRI scans, is incorrect because ALTs require surgical removal due to their locally aggressive nature and potential for recurrence and dedifferentiation.
Question 21
A 58-year-old female undergoes excision of a 7 cm mass from her anterior thigh. Preoperative MRI showed a fat-containing lesion with some internal septations. Postoperative pathology reveals an atypical lipomatous tumor with focally positive margins. What is the most appropriate management strategy for the positive margins?
View Answer & Explanation
Correct Answer: C
Rationale: For atypical lipomatous tumors (ALT), the primary goal is complete surgical resection with clear margins to minimize local recurrence. If margins are positive, re-excision to achieve clear margins is generally the preferred approach, especially in an extremity where it is feasible. Adjuvant radiation therapy may be considered if re-excision is not possible or would lead to unacceptable morbidity, but re-excision is typically favored for ALTs. Observation with positive margins carries a high risk of local recurrence. Chemotherapy and systemic targeted therapy are not indicated for ALTs. The main distractor, adjuvant radiation therapy, is a secondary option if re-excision is not feasible, but re-excision is the preferred initial approach for positive margins in ALTs.
Question 22
A 65-year-old male presents with a large, deep-seated mass in his groin. MRI shows a 12 cm fat-containing lesion with prominent non-lipomatous components and significant enhancement. A core needle biopsy is performed, and the pathology report confirms an atypical lipomatous tumor. Which of the following statements regarding the metastatic potential of this tumor is correct?
View Answer & Explanation
Correct Answer: C
Rationale: Atypical lipomatous tumors (ALT), also known as well-differentiated liposarcomas, are considered intermediate, locally aggressive tumors. They are characterized by a high rate of local recurrence if not adequately excised, but they have virtually no metastatic potential. Metastasis is a concern only if the tumor dedifferentiates into a higher-grade sarcoma, at which point it is no longer considered an ALT. The main distractor, it has a high risk of distant metastasis, is incorrect as ALTs are non-metastasizing tumors.
Question 23
A 50-year-old female presents with a 6 cm mass in her posterior calf. MRI shows a well-circumscribed, predominantly fatty lesion with some internal fibrous septa. The lesion is deep to the fascia. A core needle biopsy is performed, and the pathology report describes mature adipocytes with scattered atypical stromal cells and hyperchromatic nuclei, consistent with an atypical lipomatous tumor. What is the most common site of recurrence for this tumor after marginal excision?
View Answer & Explanation
Correct Answer: D
Rationale: Atypical lipomatous tumors (ALT) are characterized by a high rate of local recurrence if not adequately excised. Marginal excision is associated with a significantly higher local recurrence rate compared to wide local excision. ALTs do not metastasize, so recurrence in lymph nodes, lungs, liver, or bone is not expected unless the tumor has dedifferentiated. The main distractor, regional lymph nodes, is incorrect because ALTs do not metastasize to lymph nodes.
Question 24
A 60-year-old male presents with a large, deep-seated mass in his retroperitoneum. Imaging confirms a 15 cm fat-containing mass with significant non-lipomatous components. Due to its size and location, a percutaneous core needle biopsy is performed. The pathology report confirms an atypical lipomatous tumor. Which of the following is the most important factor influencing the prognosis of this patient?
View Answer & Explanation
Correct Answer: D
Rationale: For atypical lipomatous tumors (ALT), the most critical factor influencing prognosis and preventing local recurrence is achieving clear surgical margins during excision. While tumor size and location (especially retroperitoneal) can influence the difficulty of achieving clear margins and the risk of dedifferentiation, the adequacy of the surgical resection is paramount. MDM2 amplification is diagnostic but does not directly dictate prognosis beyond confirming the diagnosis. Patient age is generally not a primary prognostic factor for ALTs. The main distractor, tumor size, is incorrect because while larger tumors can be more challenging to excise with clear margins, the *result* of the excision (margin status) is the direct prognostic factor.
Question 25
A 52-year-old male presents with a slowly growing mass in his anterior abdominal wall. Physical examination reveals a firm, non-tender, immobile mass. MRI shows a 7 cm, predominantly fatty lesion with several thick, enhancing septa. A core needle biopsy is performed, confirming an atypical lipomatous tumor. Which of the following is the most appropriate follow-up protocol after successful wide local excision with clear margins?
View Answer & Explanation
Correct Answer: C
Rationale: Even after successful wide local excision with clear margins, atypical lipomatous tumors (ALT) have a risk of local recurrence, particularly in deep-seated or retroperitoneal locations, and a potential for dedifferentiation. Therefore, regular follow-up with clinical examination and local imaging (MRI) is recommended, typically every 6-12 months for at least 5 years. No further follow-up is inappropriate. Annual clinical examination alone may miss early recurrences. Whole-body PET scans are not routinely indicated for ALTs due to their lack of metastatic potential. Adjuvant chemotherapy is not indicated. The main distractor, annual clinical examination only, is incorrect because local imaging is crucial for detecting early, often asymptomatic, local recurrences or dedifferentiation.
Question 26
A 45-year-old female presents with a 5 cm, soft, mobile mass in her subcutaneous tissue of the upper arm. MRI shows a homogeneous, fat-attenuating lesion with thin septa, consistent with a benign lipoma. However, the patient is anxious and requests removal. During the discussion, she asks about the difference between her lesion and an "atypical lipoma." Which of the following is the key histological feature that distinguishes an atypical lipomatous tumor from a benign lipoma?
View Answer & Explanation
Correct Answer: C
Rationale: Both benign lipomas and atypical lipomatous tumors (ALT) are composed primarily of mature adipocytes and can have fibrous septa. The distinguishing histological feature of an ALT is the presence of scattered atypical stromal cells, often with hyperchromatic, enlarged nuclei, typically found within the fibrous septa. Myxoid degeneration and necrosis are not characteristic features of ALTs; necrosis would suggest dedifferentiation or a higher-grade sarcoma. The main distractor, presence of mature adipocytes, is incorrect because both benign lipomas and ALTs are composed of mature adipocytes; it is the *atypical* features within these cells or stromal cells that differentiate ALTs.
Question 27
A 68-year-old male presents with a large, deep-seated mass in his medial thigh. MRI reveals a 10 cm, predominantly fatty lesion with significant non-lipomatous components, including enhancing nodules. A core needle biopsy is performed, confirming an atypical lipomatous tumor. The surgeon plans for wide local excision. What is the primary reason for performing a core needle biopsy prior to definitive surgery for such a lesion?
View Answer & Explanation
Correct Answer: C
Rationale: The primary reason for performing a core needle biopsy for a suspicious soft tissue mass, including those suspected of being an atypical lipomatous tumor (ALT), is to obtain a definitive histological diagnosis. This diagnosis is crucial for guiding appropriate surgical planning (e.g., wide local excision vs. marginal excision, need for multidisciplinary approach) and patient counseling. Imaging determines size and vascularity. Biopsy does not rule out metastatic disease (which ALTs don't do anyway) or reduce tumor burden. The main distractor, to determine the exact size of the tumor, is incorrect as tumor size is best assessed by imaging (MRI).
Question 28
A 59-year-old female presents with a 9 cm mass in her gluteal region. MRI shows a fat-containing lesion with prominent thick septa and some nodular areas. A core needle biopsy confirms an atypical lipomatous tumor. The patient is concerned about the terminology and asks if this is a type of cancer. How should an atypical lipomatous tumor be best classified?
View Answer & Explanation
Correct Answer: C
Rationale: Atypical lipomatous tumors (ALT) are classified by the World Health Organization (WHO) as intermediate, locally aggressive tumors. They are also considered the same entity as well-differentiated liposarcoma, with the term "atypical lipomatous tumor" typically used for extremity and superficial lesions, and "well-differentiated liposarcoma" for deep-seated or retroperitoneal lesions. They are not benign, do not metastasize (unless dedifferentiated), and are not high-grade sarcomas (unless dedifferentiated). They are not merely precancerous but are themselves a neoplastic entity. The main distractor, malignant tumor with high metastatic potential, is incorrect because ALTs are non-metastasizing.
Question 29
A 72-year-old male presents with a large, slowly growing mass in his posterior thigh. MRI reveals a 14 cm, predominantly fatty lesion with several thick septa and enhancing non-lipomatous components. A core needle biopsy is performed, confirming an atypical lipomatous tumor. Which of the following surgical approaches is most appropriate to minimize local recurrence?
View Answer & Explanation
Correct Answer: C
Rationale: To minimize local recurrence of an atypical lipomatous tumor (ALT), wide local excision with a cuff of normal surrounding tissue (i.e., clear margins) is the standard of care. Intralesional debulking and marginal excision are associated with high local recurrence rates. Excisional biopsy is typically reserved for smaller, superficial lesions where the diagnosis is less certain. Amputation is an overly aggressive and inappropriate treatment for an ALT. The main distractor, marginal excision, is incorrect because it is associated with a high local recurrence rate for ALTs.
Question 30
A 60-year-old female presents with a 8 cm mass in her popliteal fossa. MRI shows a fat-containing lesion with thick septa and some nodular components. A core needle biopsy is performed, and the pathology report indicates an atypical lipomatous tumor. The patient is concerned about the possibility of this tumor spreading to other parts of her body. What is the most accurate statement regarding the natural history of an atypical lipomatous tumor?
View Answer & Explanation
Correct Answer: B
Rationale: Atypical lipomatous tumors (ALT) are characterized by a high risk of local recurrence if not adequately excised, but they do not metastasize. While they have the potential to dedifferentiate into a higher-grade sarcoma, this is not a rapid or universal process, and it is distinct from metastasis. They are not benign and do not commonly spread to lymph nodes. The main distractor, it frequently metastasizes to the lungs, is incorrect as ALTs are non-metastasizing tumors.
Question 31
A 50-year-old male presents with a large, deep-seated mass in his retroperitoneum. Imaging reveals a 15 cm fat-containing mass with significant non-lipomatous components. A core needle biopsy confirms an atypical lipomatous tumor. Given the retroperitoneal location, what is a particular concern regarding the long-term behavior of this tumor?
View Answer & Explanation
Correct Answer: B
Rationale: Atypical lipomatous tumors (ALT) in deep-seated locations, particularly the retroperitoneum, have a higher propensity for dedifferentiation into higher-grade sarcomas compared to those in the extremities. This dedifferentiation is a significant concern as it changes the tumor's biological behavior, introducing metastatic potential and requiring more aggressive treatment. ALTs do not metastasize, spontaneously regress, or have lower recurrence risk. They are generally not sensitive to chemotherapy. The main distractor, increased risk of distant metastasis, is incorrect because ALTs themselves do not metastasize; metastasis is a risk only *after* dedifferentiation.
Question 32
A 63-year-old female presents with a 7 cm mass in her posterior calf. MRI shows a well-circumscribed, predominantly fatty lesion with some internal fibrous septa. A core needle biopsy is performed, and the pathology report describes mature adipocytes with scattered atypical stromal cells and hyperchromatic nuclei, consistent with an atypical lipomatous tumor. Which of the following imaging modalities is most useful for initial evaluation and surgical planning for this lesion?
View Answer & Explanation
Correct Answer: D
Rationale: Magnetic Resonance Imaging (MRI) is the imaging modality of choice for evaluating soft tissue masses, including atypical lipomatous tumors (ALT). MRI provides excellent soft tissue contrast, allowing for detailed assessment of tumor size, location, relationship to neurovascular structures, presence of non-lipomatous components, and extent of involvement, all of which are critical for diagnosis and surgical planning. X-rays are poor for soft tissue. Ultrasound can be used for initial screening but lacks the detail of MRI. CT scans are useful but involve radiation and offer less soft tissue contrast than MRI. PET scans are used for metabolic activity and staging of malignant tumors, not typically for initial evaluation of ALTs. The main distractor, CT scan, is incorrect because MRI offers superior soft tissue contrast and detail for surgical planning of soft tissue tumors.
Question 33
A 55-year-old male presents with a slowly enlarging, painless mass in his anterior abdominal wall. On examination, the mass is firm and fixed. MRI reveals a 9 cm, fat-containing lesion with prominent thick septa and enhancing nodular components. A core needle biopsy confirms an atypical lipomatous tumor. The patient is otherwise healthy. What is the most appropriate initial management strategy?
Question 33
A 55-year-old male presents with a slowly enlarging, painless mass in his posterior thigh for the past 2 years. On physical exam, the mass is soft, mobile, and non-tender, approximately 8 cm in greatest dimension. MRI reveals a large, predominantly fatty mass with some thickened septa and a few small, nodular, non-lipomatous components. Biopsy confirms an atypical lipomatous tumor.
View Answer & Explanation
Correct Answer: D
Rationale: Atypical lipomatous tumor (ALT), also known as well-differentiated liposarcoma (WDLPS) in deep locations, requires wide local excision with clear margins to minimize the risk of local recurrence. While it has a low metastatic potential, local recurrence can lead to dedifferentiation into higher-grade liposarcoma. Marginal excision (C) is insufficient due to the infiltrative nature and risk of recurrence. Observation (A) is inappropriate for a biopsy-proven ALT. Intralesional excision (B) is contraindicated. Neoadjuvant radiation (E) is typically reserved for higher-grade sarcomas or cases where clear margins are difficult to achieve with surgery alone, and is not the primary treatment for ALT/WDLPS.
Question 33
A 62-year-old female presents with a 10 cm, deep-seated, soft tissue mass in her shoulder region that has been slowly growing over several years. MRI demonstrates a predominantly fatty mass with prominent, thick septations and scattered non-lipomatous foci. A core needle biopsy is performed, showing mature adipocytes with nuclear atypia and hyperchromasia. Which of the following molecular findings is most characteristic of this diagnosis?
View Answer & Explanation
Correct Answer: B
Rationale: Atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS) is characterized by amplification of the 12q13-15 region, which includes the MDM2 and CDK4 genes. This molecular signature is highly specific and aids in differentiating ALT/WDLPS from benign lipomas and other soft tissue tumors. FUS-DDIT3 fusion (A) is characteristic of myxoid liposarcoma. EWSR1-FLI1 translocation (C) is seen in Ewing sarcoma. COL1A1-PDGFB fusion (D) is associated with dermatofibrosarcoma protuberans. t(X;18)(p11.2;q11.2) translocation (E) is characteristic of synovial sarcoma.
Question 33
A 48-year-old male presents with a palpable mass in his groin region that has been present for approximately 1 year. Physical examination reveals a firm, non-tender, immobile mass, approximately 6 cm in diameter. MRI shows a large, predominantly fatty lesion with areas of signal heterogeneity, nodular components, and thick septa. What is the most appropriate initial diagnostic step after imaging?
View Answer & Explanation
Correct Answer: D
Rationale: For a deep-seated, suspicious soft tissue mass, a core needle biopsy is the most appropriate initial diagnostic step after imaging. It provides sufficient tissue for histopathological diagnosis, including immunohistochemistry and molecular studies if needed, while minimizing contamination of tissue planes. FNA (C) often yields insufficient tissue for definitive diagnosis of sarcomas. Excisional biopsy (B) is generally discouraged for suspicious masses due to the risk of inadequate margins and potential compromise of definitive surgical planning. Incisional biopsy (A) is an option but core needle biopsy is often preferred due to less invasiveness and similar diagnostic yield. Immediate wide local excision (E) without a definitive diagnosis is inappropriate.
Question 33
A 58-year-old female undergoes MRI for a 7 cm deep thigh mass. The MRI report describes a well-circumscribed, predominantly fatty lesion with several thick, enhancing septa and a few small, non-fatty nodules. The radiologist suggests the possibility of an atypical lipomatous tumor. Which of the following features on MRI is LEAST suggestive of a benign lipoma and more indicative of an atypical lipomatous tumor?
View Answer & Explanation
Correct Answer: D
Rationale: The presence of nodular, non-lipomatous components within a fatty mass is a strong indicator of an atypical lipomatous tumor (ALT) or well-differentiated liposarcoma (WDLPS), suggesting areas of increased cellularity or dedifferentiation. Thick septa (>2mm) and internal enhancement are also concerning features. Thin septa (A), homogeneous fat signal (B), and absence of internal enhancement (C) are typically associated with benign lipomas. While ALT can occur subcutaneously, a deep location is more common and concerning, making subcutaneous location (E) less indicative of ALT than a deep location, and certainly less indicative than nodular components.
Question 33
A 70-year-old male presents with a recurrent, deep-seated mass in his retroperitoneum. He had a mass excised from the same location 5 years prior, which was diagnosed as an atypical lipomatous tumor. Current imaging shows a larger, heterogeneous mass with both fatty and significant non-fatty components. Biopsy now reveals a high-grade spindle cell sarcoma. This change in pathology is best described as:
View Answer & Explanation
Correct Answer: C
Rationale: The transformation of a well-differentiated liposarcoma (atypical lipomatous tumor) into a higher-grade, non-lipogenic sarcoma (e.g., pleomorphic or spindle cell sarcoma) is known as dedifferentiation. This is a well-recognized phenomenon, particularly in recurrent or deeply located WDLPS, and is associated with a worse prognosis. Metaplasia (A) is the reversible change of one differentiated cell type to another. Anaplasia (B) refers to a lack of differentiation. Neoplasia (D) is simply new, uncontrolled growth. Hyperplasia (E) is an increase in the number of cells. None of these accurately describe the specific progression from WDLPS to a higher-grade sarcoma.
Question 33
A 50-year-old female presents with a 6 cm, firm, non-tender mass in her popliteal fossa. MRI shows a predominantly fatty mass with thick septa and a few enhancing nodules. A core needle biopsy confirms an atypical lipomatous tumor. What is the most critical factor for preventing local recurrence of this tumor?
View Answer & Explanation
Correct Answer: C
Rationale: For atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS), the most critical factor for preventing local recurrence is achieving wide surgical margins. These tumors are locally aggressive and can infiltrate surrounding tissues, even if they appear well-circumscribed on imaging. Inadequate margins are the primary risk factor for recurrence. Adjuvant chemotherapy (A) is not indicated for WDLPS. Adjuvant radiation therapy (B) may be considered in cases of positive or close margins, or for very large/deep tumors, but it is secondary to achieving clear surgical margins. Intralesional injection (D) is not a treatment for ALT. Close observation (E) is not appropriate after diagnosis and is not a preventative measure for recurrence.
Question 33
A 65-year-old male presents with a large, deep-seated mass in his retroperitoneum, causing vague abdominal discomfort. CT scan reveals a large, heterogeneous mass with significant fatty components, thick septa, and areas of soft tissue attenuation. Biopsy confirms an atypical lipomatous tumor. What is the primary concern regarding the natural history of this tumor, especially given its location?
View Answer & Explanation
Correct Answer: C
Rationale: Atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS) has a very low metastatic potential. However, it is locally aggressive, especially in deep-seated locations like the retroperitoneum, where complete surgical excision with wide margins can be challenging. The primary concern is local recurrence, which carries a significant risk of dedifferentiation into a higher-grade, more aggressive liposarcoma with metastatic potential. High risk of distant metastasis (A) and rapid growth (B) are incorrect for WDLPS. Spontaneous regression (D) does not occur. Malignant transformation into osteosarcoma (E) is not a characteristic of liposarcoma.
Question 33
A 52-year-old female presents with a 5 cm, firm, non-tender mass in her anterior thigh. MRI shows a well-circumscribed, predominantly fatty mass with a few thin septa (<2mm) and no enhancing nodules. The radiologist suggests it could be a benign lipoma or an atypical lipomatous tumor. Which of the following histological features, if present on biopsy, would definitively classify it as an atypical lipomatous tumor rather than a benign lipoma?
View Answer & Explanation
Correct Answer: C
Rationale: The defining histological feature that differentiates an atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS) from a benign lipoma is the presence of nuclear atypia and hyperchromasia in the adipocytes, often accompanied by scattered atypical stromal cells and prominent, often thickened, fibrous septa. Mature adipocytes (A) and fibrous septa (B) are present in both benign lipomas and ALT. Myxoid change (D) is characteristic of myxoid liposarcoma, a different subtype. Scattered inflammatory cells (E) are non-specific and can be seen in various benign and malignant lesions.
Question 33
A 60-year-old male presents with a large, deep-seated mass in his gluteal region. MRI shows a 12 cm predominantly fatty mass with multiple thick septa, nodular components, and areas of enhancement. Biopsy confirms an atypical lipomatous tumor. Following wide local excision with clear margins, what is the most appropriate long-term follow-up strategy?
View Answer & Explanation
Correct Answer: C
Rationale: Despite achieving clear margins, atypical lipomatous tumors (ALT) / well-differentiated liposarcomas (WDLPS) have a significant risk of local recurrence, especially large and deep-seated lesions. Therefore, long-term surveillance with clinical examination and serial imaging (MRI is preferred for soft tissue) of the surgical site is crucial. Follow-up typically involves imaging every 6-12 months for at least 5-10 years, or even longer for high-risk sites. No further follow-up (A) is incorrect. Annual physical exam only (B) is insufficient. PET-CT (D) is not routinely used for surveillance of WDLPS due to its low metabolic activity and low metastatic potential. Adjuvant therapy (E) is not standard for WDLPS with clear margins.
Question 33
A 55-year-old female presents with a 7 cm, deep-seated, soft tissue mass in her posterior calf. MRI shows a predominantly fatty lesion with some thick septa and a few small, enhancing non-fatty nodules. The biopsy confirms an atypical lipomatous tumor. Which of the following statements regarding the metastatic potential of this tumor is most accurate?
View Answer & Explanation
Correct Answer: C
Rationale: Atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS) is characterized by a very low metastatic potential. The primary concern with these tumors is local recurrence. However, if the tumor dedifferentiates into a higher-grade liposarcoma (e.g., dedifferentiated liposarcoma), then its metastatic potential significantly increases. High (A) or moderate (B) metastatic potential is incorrect. Lymph node metastasis (D) is rare for most sarcomas, including WDLPS. Metastasis is not common (E) for WDLPS.
Question 33
A 68-year-old male presents with a 9 cm, deep-seated mass in his retroperitoneum causing vague discomfort. Imaging reveals a large, heterogeneous fatty mass with prominent septations and solid components. Biopsy confirms an atypical lipomatous tumor. Given the challenging anatomical location, what is the most significant risk associated with incomplete surgical resection?
View Answer & Explanation
Correct Answer: C
Rationale: Incomplete surgical resection of an atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS), particularly in challenging locations like the retroperitoneum, significantly increases the risk of local recurrence. Furthermore, recurrent WDLPS has a higher propensity to dedifferentiate into a higher-grade liposarcoma, which then carries a much greater risk of distant metastasis and a worse prognosis. Distant metastasis (A) is rare for WDLPS itself. Rapid tumor necrosis (B), systemic inflammatory response (D), and pathologic fracture (E) are not primary risks associated with incomplete resection of WDLPS.
Question 33
A 45-year-old female presents with a 4 cm, soft, mobile mass in her subcutaneous tissue of the forearm. MRI shows a well-circumscribed, homogeneous fatty mass with no septa or enhancing components. The radiologist suggests it is likely a benign lipoma. However, the patient is concerned and requests a biopsy. If this were an atypical lipomatous tumor, which of the following locations would be considered unusual?
View Answer & Explanation
Correct Answer: D
Rationale: Atypical lipomatous tumors (ALT) / well-differentiated liposarcomas (WDLPS) are predominantly deep-seated tumors. While they can rarely occur in subcutaneous locations, it is much less common than in deep soft tissues. The deep thigh (A), retroperitoneum (B), mediastinum (C), and spermatic cord (E) are all common or recognized sites for ALT/WDLPS. A subcutaneous forearm location (D) for an ALT would be unusual, and such a lesion would more commonly be a benign lipoma.
Question 33
A 59-year-old male presents with a 10 cm, deep-seated mass in his posterior thigh. MRI shows a predominantly fatty mass with thick septa and nodular components. A core needle biopsy is performed, and the pathologist identifies mature adipocytes with nuclear atypia and hyperchromasia, along with scattered atypical stromal cells. The pathologist also notes that the tumor is "non-dedifferentiated." What is the most appropriate classification for this tumor in this deep location?
View Answer & Explanation
Correct Answer: D
Rationale: According to the current WHO classification, "atypical lipomatous tumor" (ALT) is the preferred term for well-differentiated liposarcoma (WDLPS) when it occurs in superficial, surgically resectable locations where local recurrence is the primary concern and metastatic potential is negligible. However, in deep-seated locations, especially those where complete resection is challenging (e.g., retroperitoneum, deep thigh), the term "well-differentiated liposarcoma" (WDLPS) is often used to emphasize its malignant potential for local recurrence and dedifferentiation. The histological findings described are classic for WDLPS. Benign lipoma (A) lacks atypia. Pleomorphic (B) and Myxoid (C) liposarcomas have distinct histological features. Lipoma variant (E) is too vague and does not reflect the malignant nature.
Question 33
A 63-year-old female presents with a 5 cm, firm, non-tender mass in her groin. MRI shows a predominantly fatty mass with some thick septa and a few small, enhancing non-fatty nodules. Biopsy confirms an atypical lipomatous tumor. Which of the following is considered a relative contraindication to performing an excisional biopsy for this type of lesion?
View Answer & Explanation
Correct Answer: C
Rationale: For suspicious soft tissue masses, especially those deep-seated, an excisional biopsy is generally discouraged. A deep-seated location (C) makes it challenging to achieve adequate margins with an excisional biopsy, potentially contaminating surrounding tissue planes and complicating subsequent definitive wide local excision. This can negatively impact the patient's prognosis by increasing the risk of local recurrence. Small size (A) and superficial location (B) might make excisional biopsy seem feasible, but a core needle biopsy is still preferred for definitive diagnosis and planning. Patient preference (D) and absence of pain (E) do not override oncologic principles.
Question 33
A 50-year-old male presents with a 6 cm, slowly growing mass in his posterior thigh. MRI reveals a predominantly fatty mass with thick septa and a few small, enhancing non-lipomatous components. Biopsy confirms an atypical lipomatous tumor. The surgeon plans for wide local excision. What is the primary goal of this surgical approach?
View Answer & Explanation
Correct Answer: C
Rationale: The primary goal of wide local excision for an atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS) is to remove the tumor with a margin of normal, uninvolved tissue. This approach aims to achieve clear surgical margins, which is the most critical factor in preventing local recurrence. Intralesional debulking (A) is not an oncologically sound approach for this tumor. A definitive diagnosis (B) should be obtained via biopsy *before* definitive surgery. While preventing local recurrence indirectly reduces the risk of dedifferentiation and subsequent metastasis, preventing distant metastasis (D) is not the primary goal of surgery for WDLPS itself, as its metastatic potential is very low. Facilitating adjuvant chemotherapy (E) is not relevant as chemotherapy is not standard for WDLPS.
Question 33
A 67-year-old female presents with a 8 cm, deep-seated mass in her groin. MRI shows a predominantly fatty mass with thick septa and a few enhancing nodules. Biopsy confirms an atypical lipomatous tumor. Which of the following statements best describes the typical growth pattern of an atypical lipomatous tumor?
View Answer & Explanation
Correct Answer: B
Rationale: Atypical lipomatous tumors (ALT) / well-differentiated liposarcomas (WDLPS) are typically slow-growing tumors. Patients often report the presence of a mass for months to years before seeking medical attention. Rapid growth (A, D) is more characteristic of higher-grade sarcomas. Intermittent growth (C) or stable size (E) are not typical for these lesions, which, while slow, do progressively enlarge.
Question 33
A 53-year-old male presents with a 7 cm, firm, non-tender mass in his deep posterior thigh. MRI shows a predominantly fatty mass with thick septa and a few small, enhancing non-fatty nodules. Biopsy confirms an atypical lipomatous tumor. What is the most common presenting symptom for patients with atypical lipomatous tumors?
View Answer & Explanation
Correct Answer: C
Rationale: The most common presenting symptom for atypical lipomatous tumors (ALT) / well-differentiated liposarcomas (WDLPS) is a painless, slowly enlarging mass. Due to their slow growth and often deep location, they may reach a significant size before becoming noticeable or causing symptoms. Severe pain (A) or rapidly enlarging/tender mass (B) are more suggestive of higher-grade sarcomas or inflammatory conditions. Systemic symptoms (D) are rare. Pathologic fracture (E) is not a typical presentation unless there is direct bone involvement, which is uncommon.
Question 33
A 61-year-old female presents with a 9 cm, deep-seated mass in her retroperitoneum. CT scan reveals a large, heterogeneous mass with significant fatty components, thick septa, and areas of soft tissue attenuation. Biopsy confirms an atypical lipomatous tumor. If the tumor is found to have positive surgical margins after initial excision, what is the most appropriate next step?
View Answer & Explanation
Correct Answer: C
Rationale: For atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS) with positive surgical margins, the most appropriate next step is re-excision to achieve clear margins. This is crucial for reducing the high risk of local recurrence and potential dedifferentiation. Observation (A) is inappropriate for positive margins. Adjuvant chemotherapy (B) is not indicated for WDLPS. Adjuvant radiation therapy (D) may be considered in conjunction with re-excision or if re-excision is not feasible, but achieving clear surgical margins remains the primary goal. Palliative care (E) is not indicated for a resectable WDLPS.
Question 33
A 57-year-old male presents with a 6 cm, firm, non-tender mass in his deep posterior thigh. MRI shows a predominantly fatty mass with thick septa and a few small, enhancing non-fatty nodules. Biopsy confirms an atypical lipomatous tumor. Which of the following is the most important prognostic factor for local recurrence in atypical lipomatous tumors?
View Answer & Explanation
Correct Answer: C
Rationale: The most important prognostic factor for local recurrence in atypical lipomatous tumors (ALT) / well-differentiated liposarcomas (WDLPS) is the surgical margin status. Inadequate or positive margins significantly increase the risk of the tumor growing back locally. While tumor size (B) and deep location can influence the difficulty of achieving clear margins and thus indirectly affect recurrence risk, the margin status itself is the direct and most critical factor. Patient age (A), gender (D), and presence of pain (E) are not primary prognostic factors for local recurrence.
Question 33
A 64-year-old female presents with a 10 cm, deep-seated mass in her retroperitoneum. Imaging reveals a large, heterogeneous fatty mass with prominent septations and solid components. Biopsy confirms an atypical lipomatous tumor. Which of the following statements accurately describes the relationship between atypical lipomatous tumor and well-differentiated liposarcoma?
Question 34
A 55-year-old male presents with a slowly enlarging, painless mass in his posterior thigh for the past 2 years. On physical exam, the mass is soft, mobile, and non-tender, approximately 8 cm in greatest dimension. MRI reveals a large, predominantly fatty mass with some thickened septa and a few small, nodular, non-lipomatous components. Biopsy confirms an atypical lipomatous tumor.
View Answer & Explanation
Correct Answer: D
Rationale: Atypical lipomatous tumor (ALT), also known as well-differentiated liposarcoma (WDLPS) in deep locations, requires wide local excision with clear margins to minimize the risk of local recurrence. While it has a low metastatic potential, local recurrence can lead to dedifferentiation into higher-grade liposarcoma. Marginal excision (C) is insufficient due to the infiltrative nature and risk of recurrence. Observation (A) is inappropriate for a biopsy-proven ALT. Intralesional excision (B) is contraindicated. Neoadjuvant radiation (E) is typically reserved for higher-grade sarcomas or cases where clear margins are difficult to achieve with surgery alone, and is not the primary treatment for ALT/WDLPS.
Question 35
A 62-year-old female presents with a 10 cm, deep-seated, soft tissue mass in her shoulder region that has been slowly growing over several years. MRI demonstrates a predominantly fatty mass with prominent, thick septations and scattered non-lipomatous foci. A core needle biopsy is performed, showing mature adipocytes with nuclear atypia and hyperchromasia. Which of the following molecular findings is most characteristic of this diagnosis?
View Answer & Explanation
Correct Answer: B
Rationale: Atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS) is characterized by amplification of the 12q13-15 region, which includes the MDM2 and CDK4 genes. This molecular signature is highly specific and aids in differentiating ALT/WDLPS from benign lipomas and other soft tissue tumors. FUS-DDIT3 fusion (A) is characteristic of myxoid liposarcoma. EWSR1-FLI1 translocation (C) is seen in Ewing sarcoma. COL1A1-PDGFB fusion (D) is associated with dermatofibrosarcoma protuberans. t(X;18)(p11.2;q11.2) translocation (E) is characteristic of synovial sarcoma.
Question 36
A 48-year-old male presents with a palpable mass in his groin region that has been present for approximately 1 year. Physical examination reveals a firm, non-tender, immobile mass, approximately 6 cm in diameter. MRI shows a large, predominantly fatty lesion with areas of signal heterogeneity, nodular components, and thick septa. What is the most appropriate initial diagnostic step after imaging?
View Answer & Explanation
Correct Answer: D
Rationale: For a deep-seated, suspicious soft tissue mass, a core needle biopsy is the most appropriate initial diagnostic step after imaging. It provides sufficient tissue for histopathological diagnosis, including immunohistochemistry and molecular studies if needed, while minimizing contamination of tissue planes. FNA (C) often yields insufficient tissue for definitive diagnosis of sarcomas. Excisional biopsy (B) is generally discouraged for suspicious masses due to the risk of inadequate margins and potential compromise of definitive surgical planning. Incisional biopsy (A) is an option but core needle biopsy is often preferred due to less invasiveness and similar diagnostic yield. Immediate wide local excision (E) without a definitive diagnosis is inappropriate.
Question 37
A 58-year-old female undergoes MRI for a 7 cm deep thigh mass. The MRI report describes a well-circumscribed, predominantly fatty lesion with several thick, enhancing septa and a few small, non-fatty nodules. The radiologist suggests the possibility of an atypical lipomatous tumor. Which of the following features on MRI is LEAST suggestive of a benign lipoma and more indicative of an atypical lipomatous tumor?
View Answer & Explanation
Correct Answer: D
Rationale: The presence of nodular, non-lipomatous components within a fatty mass is a strong indicator of an atypical lipomatous tumor (ALT) or well-differentiated liposarcoma (WDLPS), suggesting areas of increased cellularity or dedifferentiation. Thick septa (>2mm) and internal enhancement are also concerning features. Thin septa (A), homogeneous fat signal (B), and absence of internal enhancement (C) are typically associated with benign lipomas. While ALT can occur subcutaneously, a deep location is more common and concerning, making subcutaneous location (E) less indicative of ALT than a deep location, and certainly less indicative than nodular components.
Question 38
A 70-year-old male presents with a recurrent, deep-seated mass in his retroperitoneum. He had a mass excised from the same location 5 years prior, which was diagnosed as an atypical lipomatous tumor. Current imaging shows a larger, heterogeneous mass with both fatty and significant non-fatty components. Biopsy now reveals a high-grade spindle cell sarcoma. This change in pathology is best described as:
View Answer & Explanation
Correct Answer: C
Rationale: The transformation of a well-differentiated liposarcoma (atypical lipomatous tumor) into a higher-grade, non-lipogenic sarcoma (e.g., pleomorphic or spindle cell sarcoma) is known as dedifferentiation. This is a well-recognized phenomenon, particularly in recurrent or deeply located WDLPS, and is associated with a worse prognosis. Metaplasia (A) is the reversible change of one differentiated cell type to another. Anaplasia (B) refers to a lack of differentiation. Neoplasia (D) is simply new, uncontrolled growth. Hyperplasia (E) is an increase in the number of cells. None of these accurately describe the specific progression from WDLPS to a higher-grade sarcoma.
Question 39
A 50-year-old female presents with a 6 cm, firm, non-tender mass in her popliteal fossa. MRI shows a predominantly fatty mass with thick septa and a few enhancing nodules. A core needle biopsy confirms an atypical lipomatous tumor. What is the most critical factor for preventing local recurrence of this tumor?
View Answer & Explanation
Correct Answer: C
Rationale: For atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS), the most critical factor for preventing local recurrence is achieving wide surgical margins. These tumors are locally aggressive and can infiltrate surrounding tissues, even if they appear well-circumscribed on imaging. Inadequate margins are the primary risk factor for recurrence. Adjuvant chemotherapy (A) is not indicated for WDLPS. Adjuvant radiation therapy (B) may be considered in cases of positive or close margins, or for very large/deep tumors, but it is secondary to achieving clear surgical margins. Intralesional injection (D) is not a treatment for ALT. Close observation (E) is not appropriate after diagnosis and is not a preventative measure for recurrence.
Question 40
A 65-year-old male presents with a large, deep-seated mass in his retroperitoneum, causing vague abdominal discomfort. CT scan reveals a large, heterogeneous mass with significant fatty components, thick septa, and areas of soft tissue attenuation. Biopsy confirms an atypical lipomatous tumor. What is the primary concern regarding the natural history of this tumor, especially given its location?
View Answer & Explanation
Correct Answer: C
Rationale: Atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS) has a very low metastatic potential. However, it is locally aggressive, especially in deep-seated locations like the retroperitoneum, where complete surgical excision with wide margins can be challenging. The primary concern is local recurrence, which carries a significant risk of dedifferentiation into a higher-grade, more aggressive liposarcoma with metastatic potential. High risk of distant metastasis (A) and rapid growth (B) are incorrect for WDLPS. Spontaneous regression (D) does not occur. Malignant transformation into osteosarcoma (E) is not a characteristic of liposarcoma.
Question 41
A 52-year-old female presents with a 5 cm, firm, non-tender mass in her anterior thigh. MRI shows a well-circumscribed, predominantly fatty mass with a few thin septa (<2mm) and no enhancing nodules. The radiologist suggests it could be a benign lipoma or an atypical lipomatous tumor. Which of the following histological features, if present on biopsy, would definitively classify it as an atypical lipomatous tumor rather than a benign lipoma?
View Answer & Explanation
Correct Answer: C
Rationale: The defining histological feature that differentiates an atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS) from a benign lipoma is the presence of nuclear atypia and hyperchromasia in the adipocytes, often accompanied by scattered atypical stromal cells and prominent, often thickened, fibrous septa. Mature adipocytes (A) and fibrous septa (B) are present in both benign lipomas and ALT. Myxoid change (D) is characteristic of myxoid liposarcoma, a different subtype. Scattered inflammatory cells (E) are non-specific and can be seen in various benign and malignant lesions.
Question 42
A 60-year-old male presents with a large, deep-seated mass in his gluteal region. MRI shows a 12 cm predominantly fatty mass with multiple thick septa, nodular components, and areas of enhancement. Biopsy confirms an atypical lipomatous tumor. Following wide local excision with clear margins, what is the most appropriate long-term follow-up strategy?
View Answer & Explanation
Correct Answer: C
Rationale: Despite achieving clear margins, atypical lipomatous tumors (ALT) / well-differentiated liposarcomas (WDLPS) have a significant risk of local recurrence, especially large and deep-seated lesions. Therefore, long-term surveillance with clinical examination and serial imaging (MRI is preferred for soft tissue) of the surgical site is crucial. Follow-up typically involves imaging every 6-12 months for at least 5-10 years, or even longer for high-risk sites. No further follow-up (A) is incorrect. Annual physical exam only (B) is insufficient. PET-CT (D) is not routinely used for surveillance of WDLPS due to its low metabolic activity and low metastatic potential. Adjuvant therapy (E) is not standard for WDLPS with clear margins.
Question 43
A 55-year-old female presents with a 7 cm, deep-seated, soft tissue mass in her posterior calf. MRI shows a predominantly fatty lesion with some thick septa and a few small, enhancing non-fatty nodules. The biopsy confirms an atypical lipomatous tumor. Which of the following statements regarding the metastatic potential of this tumor is most accurate?
View Answer & Explanation
Correct Answer: C
Rationale: Atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS) is characterized by a very low metastatic potential. The primary concern with these tumors is local recurrence. However, if the tumor dedifferentiates into a higher-grade liposarcoma (e.g., dedifferentiated liposarcoma), then its metastatic potential significantly increases. High (A) or moderate (B) metastatic potential is incorrect. Lymph node metastasis (D) is rare for most sarcomas, including WDLPS. Metastasis is not common (E) for WDLPS.
Question 44
A 68-year-old male presents with a 9 cm, deep-seated mass in his retroperitoneum causing vague discomfort. Imaging reveals a large, heterogeneous fatty mass with prominent septations and solid components. Biopsy confirms an atypical lipomatous tumor. Given the challenging anatomical location, what is the most significant risk associated with incomplete surgical resection?
View Answer & Explanation
Correct Answer: C
Rationale: Incomplete surgical resection of an atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS), particularly in challenging locations like the retroperitoneum, significantly increases the risk of local recurrence. Furthermore, recurrent WDLPS has a higher propensity to dedifferentiate into a higher-grade liposarcoma, which then carries a much greater risk of distant metastasis and a worse prognosis. Distant metastasis (A) is rare for WDLPS itself. Rapid tumor necrosis (B), systemic inflammatory response (D), and pathologic fracture (E) are not primary risks associated with incomplete resection of WDLPS.
Question 45
A 45-year-old female presents with a 4 cm, soft, mobile mass in her subcutaneous tissue of the forearm. MRI shows a well-circumscribed, homogeneous fatty mass with no septa or enhancing components. The radiologist suggests it is likely a benign lipoma. However, the patient is concerned and requests a biopsy. If this were an atypical lipomatous tumor, which of the following locations would be considered unusual?
View Answer & Explanation
Correct Answer: D
Rationale: Atypical lipomatous tumors (ALT) / well-differentiated liposarcomas (WDLPS) are predominantly deep-seated tumors. While they can rarely occur in subcutaneous locations, it is much less common than in deep soft tissues. The deep thigh (A), retroperitoneum (B), mediastinum (C), and spermatic cord (E) are all common or recognized sites for ALT/WDLPS. A subcutaneous forearm location (D) for an ALT would be unusual, and such a lesion would more commonly be a benign lipoma.
Question 46
A 59-year-old male presents with a 10 cm, deep-seated mass in his posterior thigh. MRI shows a predominantly fatty mass with thick septa and nodular components. A core needle biopsy is performed, and the pathologist identifies mature adipocytes with nuclear atypia and hyperchromasia, along with scattered atypical stromal cells. The pathologist also notes that the tumor is "non-dedifferentiated." What is the most appropriate classification for this tumor in this deep location?
View Answer & Explanation
Correct Answer: D
Rationale: According to the current WHO classification, "atypical lipomatous tumor" (ALT) is the preferred term for well-differentiated liposarcoma (WDLPS) when it occurs in superficial, surgically resectable locations where local recurrence is the primary concern and metastatic potential is negligible. However, in deep-seated locations, especially those where complete resection is challenging (e.g., retroperitoneum, deep thigh), the term "well-differentiated liposarcoma" (WDLPS) is often used to emphasize its malignant potential for local recurrence and dedifferentiation. The histological findings described are classic for WDLPS. Benign lipoma (A) lacks atypia. Pleomorphic (B) and Myxoid (C) liposarcomas have distinct histological features. Lipoma variant (E) is too vague and does not reflect the malignant nature.
Question 47
A 63-year-old female presents with a 5 cm, firm, non-tender mass in her groin. MRI shows a predominantly fatty mass with some thick septa and a few small, enhancing non-fatty nodules. Biopsy confirms an atypical lipomatous tumor. Which of the following is considered a relative contraindication to performing an excisional biopsy for this type of lesion?
View Answer & Explanation
Correct Answer: C
Rationale: For suspicious soft tissue masses, especially those deep-seated, an excisional biopsy is generally discouraged. A deep-seated location (C) makes it challenging to achieve adequate margins with an excisional biopsy, potentially contaminating surrounding tissue planes and complicating subsequent definitive wide local excision. This can negatively impact the patient's prognosis by increasing the risk of local recurrence. Small size (A) and superficial location (B) might make excisional biopsy seem feasible, but a core needle biopsy is still preferred for definitive diagnosis and planning. Patient preference (D) and absence of pain (E) do not override oncologic principles.
Question 48
A 50-year-old male presents with a 6 cm, slowly growing mass in his posterior thigh. MRI reveals a predominantly fatty mass with thick septa and a few small, enhancing non-lipomatous components. Biopsy confirms an atypical lipomatous tumor. The surgeon plans for wide local excision. What is the primary goal of this surgical approach?
View Answer & Explanation
Correct Answer: C
Rationale: The primary goal of wide local excision for an atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS) is to remove the tumor with a margin of normal, uninvolved tissue. This approach aims to achieve clear surgical margins, which is the most critical factor in preventing local recurrence. Intralesional debulking (A) is not an oncologically sound approach for this tumor. A definitive diagnosis (B) should be obtained via biopsy *before* definitive surgery. While preventing local recurrence indirectly reduces the risk of dedifferentiation and subsequent metastasis, preventing distant metastasis (D) is not the primary goal of surgery for WDLPS itself, as its metastatic potential is very low. Facilitating adjuvant chemotherapy (E) is not relevant as chemotherapy is not standard for WDLPS.
Question 49
A 67-year-old female presents with a 8 cm, deep-seated mass in her groin. MRI shows a predominantly fatty mass with thick septa and a few enhancing nodules. Biopsy confirms an atypical lipomatous tumor. Which of the following statements best describes the typical growth pattern of an atypical lipomatous tumor?
View Answer & Explanation
Correct Answer: B
Rationale: Atypical lipomatous tumors (ALT) / well-differentiated liposarcomas (WDLPS) are typically slow-growing tumors. Patients often report the presence of a mass for months to years before seeking medical attention. Rapid growth (A, D) is more characteristic of higher-grade sarcomas. Intermittent growth (C) or stable size (E) are not typical for these lesions, which, while slow, do progressively enlarge.
Question 50
A 53-year-old male presents with a 7 cm, firm, non-tender mass in his deep posterior thigh. MRI shows a predominantly fatty mass with thick septa and a few small, enhancing non-fatty nodules. Biopsy confirms an atypical lipomatous tumor. What is the most common presenting symptom for patients with atypical lipomatous tumors?
View Answer & Explanation
Correct Answer: C
Rationale: The most common presenting symptom for atypical lipomatous tumors (ALT) / well-differentiated liposarcomas (WDLPS) is a painless, slowly enlarging mass. Due to their slow growth and often deep location, they may reach a significant size before becoming noticeable or causing symptoms. Severe pain (A) or rapidly enlarging/tender mass (B) are more suggestive of higher-grade sarcomas or inflammatory conditions. Systemic symptoms (D) are rare. Pathologic fracture (E) is not a typical presentation unless there is direct bone involvement, which is uncommon.
Question 51
A 61-year-old female presents with a 9 cm, deep-seated mass in her retroperitoneum. CT scan reveals a large, heterogeneous mass with significant fatty components, thick septa, and areas of soft tissue attenuation. Biopsy confirms an atypical lipomatous tumor. If the tumor is found to have positive surgical margins after initial excision, what is the most appropriate next step?
View Answer & Explanation
Correct Answer: C
Rationale: For atypical lipomatous tumor (ALT) / well-differentiated liposarcoma (WDLPS) with positive surgical margins, the most appropriate next step is re-excision to achieve clear margins. This is crucial for reducing the high risk of local recurrence and potential dedifferentiation. Observation (A) is inappropriate for positive margins. Adjuvant chemotherapy (B) is not indicated for WDLPS. Adjuvant radiation therapy (D) may be considered in conjunction with re-excision or if re-excision is not feasible, but achieving clear surgical margins remains the primary goal. Palliative care (E) is not indicated for a resectable WDLPS.
Question 52
A 57-year-old male presents with a 6 cm, firm, non-tender mass in his deep posterior thigh. MRI shows a predominantly fatty mass with thick septa and a few small, enhancing non-fatty nodules. Biopsy confirms an atypical lipomatous tumor. Which of the following is the most important prognostic factor for local recurrence in atypical lipomatous tumors?
View Answer & Explanation
Correct Answer: C
Rationale: The most important prognostic factor for local recurrence in atypical lipomatous tumors (ALT) / well-differentiated liposarcomas (WDLPS) is the surgical margin status. Inadequate or positive margins significantly increase the risk of the tumor growing back locally. While tumor size (B) and deep location can influence the difficulty of achieving clear margins and thus indirectly affect recurrence risk, the margin status itself is the direct and most critical factor. Patient age (A), gender (D), and presence of pain (E) are not primary prognostic factors for local recurrence.
Question 53
A 16-year-old male presents with chronic knee pain that has been present for several years. Physical examination reveals tenderness around the knee. Radiographs show a lytic lesion in the proximal tibial epiphysis. An MRI confirms an epiphyseal lesion.
View Answer & Explanation
Correct Answer: C
Rationale: Chondroblastoma is a benign cartilage-producing tumor typically found in the epiphysis or apophysis of adolescents or young adults, often presenting with chronic pain. The age (16-year-old) and epiphyseal location are classic for chondroblastoma. Main Distractor: Giant Cell Tumor (GCT) typically occurs in a slightly older age group (20-40s) and usually involves the epiphysis after physeal closure, although it can cross the physis.
Question 54
A 16-year-old male presents with chronic knee pain. Radiographs reveal a lytic lesion in the proximal tibial epiphysis. An MRI confirms an epiphyseal lesion. The patient's pain has been present for an extended period.
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context states that matrix calcifications are present in approximately one-quarter of chondroblastomas, making this a characteristic radiographic feature, though not universally present. Main Distractor: A sclerotic rim can be seen in some benign lesions, but matrix calcifications are specifically highlighted for chondroblastoma.
Question 55
A 16-year-old male presents with chronic knee pain. Biopsy of an epiphyseal lesion reveals a uniform background of mononuclear cells with occasional giant cells.
View Answer & Explanation
Correct Answer: C
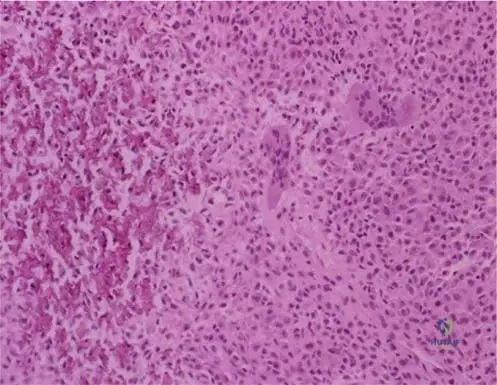
Rationale: The provided image context (Fig. 8.42) and text explicitly describe chondroblastoma histology as showing a uniform background of mononuclear cells with occasional giant cells. Main Distractor: While Giant Cell Tumor (GCT) also contains giant cells, the "uniform background of mononuclear cells" is a key distinguishing feature of chondroblastoma.
Question 56
A 16-year-old male undergoes surgical resection of a benign epiphyseal bone tumor. Gross examination of the resected specimen reveals a grey or pink tissue with occasional areas of calcification.

View Answer & Explanation
Correct Answer: C
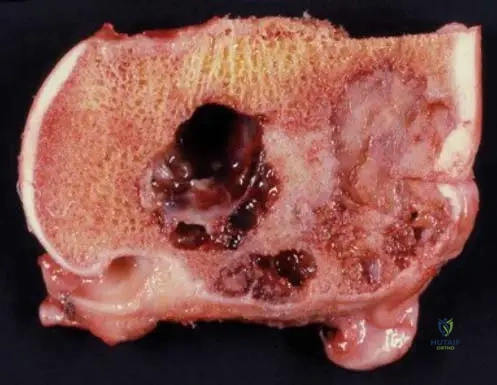
Rationale: The provided image context (Fig. 8.43) and text state that grossly, chondroblastoma is usually grey or pink, with occasional areas of calcification in the tissue. Main Distractor: Simple bone cysts are typically fluid-filled, not solid grey or pink tissue.
Question 57
A 16-year-old male presents with several years of knee pain. Physical examination reveals tenderness around the knee joint and mild regional muscle atrophy. Radiographs show a lytic lesion in the proximal tibial epiphysis.
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states that "Pain is the most common clinical finding" for chondroblastoma, and it "may be present for many years before diagnosis." Tenderness, regional muscle atrophy, and antalgic gait are also mentioned. Main Distractor: Acute onset of pain is incorrect, as the pain is typically chronic and long-standing.
Question 58
A 16-year-old male presents with knee pain. Imaging reveals a lytic lesion located in the epiphysis of the proximal tibia. The patient has open growth plates.
View Answer & Explanation
Correct Answer: C
Rationale: The text states that chondroblastomas "occur in primary or secondary ossification centers" and are "usually localized to the epiphysis or apophysis." Main Distractor: The metaphysis is a common location for many other bone tumors (e.g., osteosarcoma, osteochondroma), but chondroblastoma's predilection for the epiphysis/apophysis is a key diagnostic feature.
Question 59
A patient presents with chronic knee pain and a lytic epiphyseal lesion. The diagnosis of chondroblastoma is suspected.
View Answer & Explanation
Correct Answer: C
Rationale: The text states that chondroblastoma "usually occurring in patients in adolescence or early adulthood" and are "two times more common in males than in females." Main Distractor: Young adult females is incorrect because males are more commonly affected.
Question 60
A 16-year-old male undergoes biopsy of an epiphyseal lesion. Gross examination of the specimen shows areas of chondroid-appearing tissue as well as more cystic regions.
View Answer & Explanation
Correct Answer: B
Rationale: The provided image context (Fig. 8.44) and text explicitly state that "Chondroblastomas can have components of secondary aneurysmal bone cyst," which explains the presence of cystic regions. Main Distractor: While simple bone cysts are cystic, the specific association mentioned in the text is with aneurysmal bone cysts.
Question 61
A 16-year-old male with open growth plates presents with a chondroblastoma in the proximal tibial epiphysis. The surgeon is considering the tumor's relationship to the physis.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Although usually localized to the epiphysis or apophysis, these lesions occasionally cross an open growth plate." Main Distractor: Stating that it "always respects the growth plate" is incorrect, as the text specifies that it can occasionally cross it.
Question 62
A 16-year-old male presents with a lytic epiphyseal lesion diagnosed as chondroblastoma. The patient is concerned about the nature of the tumor.
View Answer & Explanation
Correct Answer: D
Rationale: The first sentence of the text defines chondroblastoma as a "benign cartilage-producing tumor." Main Distractor: Malignant cartilage-producing is incorrect; chondroblastoma is benign.
Question 63
A 16-year-old male presents with chronic knee pain. Radiographs show a lytic lesion in the proximal tibial epiphysis. The patient has open physes.
View Answer & Explanation
Correct Answer: D
Rationale: Given the patient's age (adolescent with open physes) and the epiphyseal location of the lytic lesion, chondroblastoma is the most classic and important differential diagnosis. Main Distractor: Giant Cell Tumor (GCT) is a common differential for epiphyseal lesions, but it typically occurs in young adults (20-40s) after physeal closure, making it less likely in a 16-year-old with open physes compared to chondroblastoma.
Question 64
A 16-year-old male presents with chronic knee pain due to a chondroblastoma in the proximal tibial epiphysis. On physical examination, the patient exhibits a noticeable alteration in their walking pattern.
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that patients with chondroblastoma "may also present with regional muscle atrophy and an antalgic gait." An antalgic gait is a compensatory gait pattern adopted to minimize pain during weight-bearing. Main Distractor: A Trendelenburg gait is associated with hip abductor weakness, which is not a primary feature described for chondroblastoma.
Question 65
A 16-year-old male presents with knee pain. Radiographs (AP and lateral) and MRI (sagittal plane) show a lytic lesion in the proximal tibial epiphysis posteriorly.
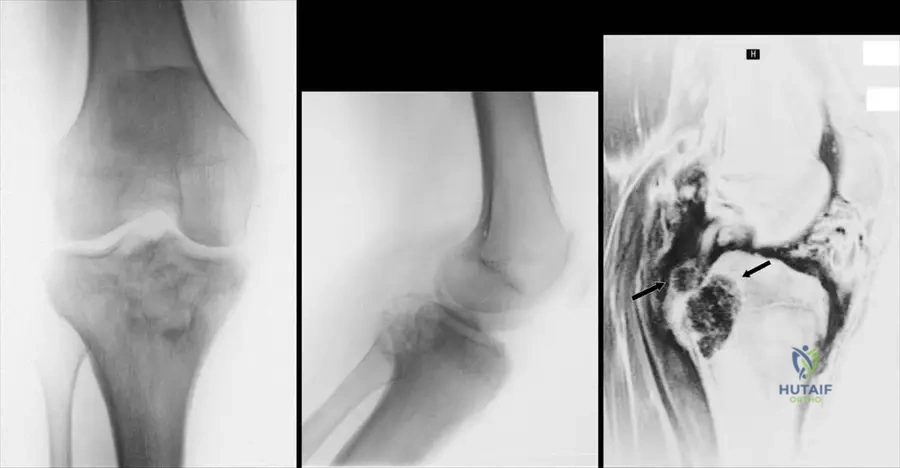
View Answer & Explanation
Correct Answer: C
Rationale: A lytic lesion on a radiograph indicates an area of bone destruction or resorption, appearing darker or less dense than surrounding bone. Main Distractor: Increased bone density would describe a sclerotic lesion, which is the opposite of lytic.
Question 66
A 16-year-old male is diagnosed with a chondroblastoma in the proximal tibial epiphysis. He reports experiencing knee pain for an extended period prior to diagnosis, which is a common characteristic of this tumor.
View Answer & Explanation
Correct Answer: B
Rationale: The text states that pain "may be present for many years before diagnosis" in patients with chondroblastoma. Main Distractor: Acute onset is incorrect, as the pain is typically chronic and insidious.
Question 67
A 16-year-old male presents with chronic knee pain. Prior to referral for evaluation of a lytic epiphyseal lesion, he underwent knee arthroscopy.
View Answer & Explanation
Correct Answer: C
Rationale: The image context (Fig. 8.39) mentions "a 16-year-old who underwent knee arthroscopy prior to referral." This implies that the patient's chronic knee pain was initially attributed to more common intra-articular pathologies, leading to arthroscopic investigation before the underlying bone tumor was identified. Main Distractor: While arthroscopy can be used for biopsy, it's typically a targeted procedure for a known lesion, not a general knee arthroscopy for an undiagnosed bone tumor. The phrasing "prior to referral" suggests an initial misdirection in diagnosis.
Question 68
A 16-year-old male presents with chronic knee pain. An AP radiograph of the knee is shown.
View Answer & Explanation
Correct Answer: D
Rationale: The image context (Fig. 8.39) explicitly describes the lesion as "a lytic lesion." On the AP radiograph (a), the lesion appears as an area of decreased bone density
Question 68
A 16-year-old male presents with chronic knee pain. Radiographs reveal a lytic lesion in the proximal tibial epiphysis. A biopsy is performed. Low magnification histology shows a uniform background of mononuclear cells with occasional multinucleated giant cells. Which of the following is the most likely diagnosis?
View Answer & Explanation
Correct Answer: B
Rationale: Chondroblastoma is characterized histologically by a uniform background of mononuclear cells (chondroblast-like cells) with occasional multinucleated giant cells, as described and shown in the provided image. Giant Cell Tumor would have a much more prominent and diffuse giant cell component. Osteosarcoma would show malignant osteoid formation. Enchondroma and Osteochondroma have distinct cartilaginous matrices and growth patterns.
Question 68
A 16-year-old male undergoes surgical resection of a benign cartilage-producing tumor from the proximal tibial epiphysis. Upon gross examination of the resected specimen, what color and consistency would be most characteristic of this tumor?
View Answer & Explanation
Correct Answer: C
Rationale: Grossly, chondroblastoma is usually grey or pink, with occasional areas of calcification in the tissue, as described in the text and depicted in Fig. 8.43. The other options describe features more typical of other bone tumors (e.g., lipoma, aneurysmal bone cyst, fibrous dysplasia).
Question 68
A 16-year-old female presents with chronic hip pain. Imaging reveals an epiphyseal lytic lesion in the femoral head. Surgical curettage is performed. Gross examination of the specimen shows an area of chondroid-appearing tissue as well as more cystic regions. Which additional component is commonly found in chondroblastomas, contributing to cystic areas?
View Answer & Explanation
Correct Answer: C
Rationale: Chondroblastomas can have components of secondary aneurysmal bone cyst, which explains the presence of cystic regions within the tumor, as described and illustrated in Fig. 8.44. The other options are distinct tumor types or components not typically associated with chondroblastoma in this manner.
Question 68
A 16-year-old male presents with knee pain. Radiographs show a lytic lesion in the proximal tibial epiphysis. While most chondroblastomas are purely lytic, what percentage of cases may demonstrate matrix calcifications on imaging?
View Answer & Explanation
Correct Answer: B
Rationale: Matrix calcifications are present in approximately one-quarter of chondroblastomas, as explicitly stated in the clinical context for Fig. 8.39. This is an important diagnostic clue, though not universally present. The other percentages are incorrect based on the provided text.
Question 68
A 16-year-old presents with chronic shoulder pain. Imaging reveals a lytic lesion in the humeral head epiphysis. Considering the epidemiology of chondroblastoma, what is the typical gender predilection for this tumor?
View Answer & Explanation
Correct Answer: C
Rationale: Chondroblastomas are two times more common in males than in females, as stated in the text. This epidemiological detail can aid in differential diagnosis. The other options are incorrect.
Question 68
A 16-year-old male presents with knee pain. Radiographs show a lytic lesion in the proximal tibia. Which specific anatomical location within the bone is most characteristic for chondroblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: Chondroblastomas usually occur in primary or secondary ossification centers and are localized to the epiphysis or apophysis. This epiphyseal/apophyseal location is a key distinguishing feature from many other bone tumors. The other locations are less typical for chondroblastoma.
Question 68
A 16-year-old male presents with knee pain and a lytic lesion in the proximal tibial epiphysis, consistent with chondroblastoma. Given the typical age of presentation, what is a notable characteristic regarding the tumor's interaction with the growth plate?
View Answer & Explanation
Correct Answer: D
Rationale: Although usually localized to the epiphysis or apophysis, these lesions occasionally cross an open growth plate. This is an important feature to consider in surgical planning and understanding tumor behavior. The other options are incorrect based on the text.
Question 68
A 16-year-old female presents with chronic knee pain, which has been present for several years. Physical examination reveals tenderness over the proximal tibia. In addition to pain and tenderness, what other associated clinical findings might be present in a patient with chondroblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: Patients with chondroblastoma may present with regional muscle atrophy and an antalgic gait, in addition to pain and tenderness. These are common secondary findings due to chronic pain and disuse. The other options describe symptoms not typically associated with chondroblastoma.
Question 68
A 16-year-old male presents with chronic knee pain. Radiographs show a lytic lesion in the proximal tibial epiphysis. Given the patient's age and the epiphyseal location of the lesion, which of the following is the most important differential diagnosis to consider alongside chondroblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: Giant cell tumor (GCT) is a critical differential diagnosis for an epiphyseal lytic lesion, especially in adolescents and young adults, as it can also present in this location and age group, though GCT typically occurs after growth plate closure. Chondroblastoma is the classic epiphyseal tumor in skeletally immature patients. Osteoid osteoma is typically metaphyseal/diaphyseal. Non-ossifying fibroma is metaphyseal. Fibrous dysplasia and enchondroma are less common in the epiphysis and have distinct radiographic features.
Question 68
A 16-year-old female presents with a lytic lesion in the distal femoral epiphysis. Biopsy confirms chondroblastoma, but also notes areas consistent with a secondary aneurysmal bone cyst (ABC). What is the clinical significance of this secondary ABC component?
View Answer & Explanation
Correct Answer: C
Rationale: Chondroblastomas can have components of secondary aneurysmal bone cyst, which is a common benign secondary change that can lead to cystic regions within the tumor. It does not indicate malignancy or necessarily a higher risk of recurrence compared to other chondroblastomas, nor does it alter the fundamental benign nature of the primary tumor. The text describes it as a component, not a sign of malignancy or requiring chemotherapy.
Question 68
A 16-year-old male presents with chronic ankle pain. Imaging reveals a lytic lesion in the talar epiphysis. Biopsy confirms chondroblastoma. Based on its classification, what is the primary tissue type produced by this tumor?
View Answer & Explanation
Correct Answer: C
Rationale: Chondroblastoma is explicitly described as a "benign cartilage-producing tumor." This defines its histogenesis and primary tissue type. The other options are incorrect.
Question 68
A 16-year-old female presents with persistent knee pain. Initial radiographs show a subtle lytic lesion in the proximal tibial epiphysis. To better delineate the extent of the lesion and its relationship to surrounding structures, an MRI is ordered. What would be the expected finding on the sagittal plane MRI?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 8.39 explicitly states that "The lateral radiograph (b) and the MR picture in sagittal plane show a lytic lesion in the proximal tibial epiphysis posteriorly." This directly answers the question. The other options describe features of different bone pathologies (e.g., osteoid osteoma, aneurysmal bone cyst, osteosarcoma).
Question 68
A 16-year-old male presents with knee pain. He reports that the pain has been intermittent but present for approximately two years. Radiographs show an epiphyseal lytic lesion. What is a common characteristic of the duration of symptoms for chondroblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that pain, the most common clinical finding, "may be present for many years before diagnosis." This indicates a chronic, often insidious onset of symptoms. The other options describe different clinical courses.
Question 68
A 16-year-old female presents with chronic wrist pain. Radiographs of the distal radius show a well-defined lesion in the epiphysis. What is the most common radiographic appearance of a chondroblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: The radiographs (Fig. 8.39 a-c) and descriptions consistently refer to chondroblastoma as a "lytic lesion." While some may have matrix calcifications, the primary appearance is lytic. Sclerotic lesions, mixed lesions, and aggressive features like cortical breakthrough or Codman's triangle are characteristic of other bone tumors.
Question 68
A 16-year-old male undergoes biopsy for an epiphyseal lesion in the proximal humerus. Histological examination reveals a uniform background of mononuclear cells. These cells are characteristic of chondroblastoma and are often described as resembling what specific cell type?
View Answer & Explanation
Correct Answer: C
Rationale: Chondroblastoma is a cartilage-producing tumor, and its characteristic mononuclear cells are often described as chondroblast-like. The name itself, "chondroblastoma," refers to these immature cartilage-forming cells. The other cell types are not characteristic of this tumor.
Question 68
A 16-year-old female undergoes surgical resection of a chondroblastoma from the distal femoral epiphysis. During gross examination, the pathologist notes areas of "chondroid-appearing tissue." What does this term primarily suggest about the consistency or appearance of these areas?
View Answer & Explanation
Correct Answer: C
Rationale: "Chondroid-appearing tissue" refers to tissue that resembles cartilage, which is typically rubbery, firm, or gelatinous in consistency. Since chondroblastoma is a cartilage-producing tumor, this gross appearance is expected. The other options describe different tissue types or states.
Question 68
A 16-year-old male presents with chronic knee pain. He underwent knee arthroscopy by an outside surgeon prior to referral to an orthopedic oncologist. Imaging now reveals a lytic lesion in the proximal tibial epiphysis. What is the most likely reason for the initial arthroscopy in this case?
View Answer & Explanation
Correct Answer: B
Rationale: The vignette states the patient underwent knee arthroscopy "prior to referral." This implies that the initial presentation of chronic knee pain was likely attributed to a common intra-articular issue (e.g., meniscal tear, ligament injury, chondral defect) before the underlying bone tumor was identified or suspected. Arthroscopy is typically not the primary approach for diagnosing or treating an epiphyseal bone tumor unless it has an intra-articular component or is misdiagnosed. The text implies a delay in diagnosis, suggesting initial misdirection. While a meniscal tear (D) could be found, the primary reason for arthroscopy in the context of undiagnosed chronic knee pain is to rule out intra-articular pathology.
Question 68
A 16-year-old female is diagnosed with a chondroblastoma in the distal femoral epiphysis. The tumor is confirmed to be benign. What is the generally accepted primary surgical management principle for a symptomatic chondroblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: As a benign tumor, the standard surgical treatment for symptomatic chondroblastoma is intralesional curettage, often augmented with local adjuvants (e.g., cryotherapy, phenol) and bone grafting to fill the defect and reduce recurrence risk. Wide en bloc resection (A) is typically reserved for malignant tumors or aggressive benign tumors with significant cortical destruction. Amputation (B) and chemotherapy/radiation (D) are for malignant conditions. Long-term observation (E) is usually for asymptomatic, quiescent lesions or non-ossifying fibromas, not typically for symptomatic chondroblastomas.
Question 68
A 16-year-old male presents with knee pain. Radiographs show a lytic lesion in the proximal tibial epiphysis with subtle areas of matrix calcification. Considering this imaging finding, which other diagnosis might also present with epiphyseal involvement and calcifications, making it a key differential?
View Answer & Explanation
Correct Answer: D
Rationale: Clear cell chondrosarcoma is a rare low-grade malignant cartilage tumor that can occur in the epiphysis of long bones, particularly in young adults, and often contains calcifications. This makes it a critical differential for chondroblastoma, especially when calcifications are present. Osteosarcoma (A) is typically metaphyseal and shows osteoid matrix. Chondrosarcoma (B) is usually in older adults and often metaphyseal/diaphyseal. Enchondroma (C) is typically metaphyseal/diaphyseal. Fibrous cortical defect (E) is metaphyseal and lacks calcifications.
Question 68
A 16-year-old female presents with chronic knee pain. On physical examination, the most common finding associated with chondroblastoma is:
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Tenderness is the most common finding on physical examination." While other findings like restricted range of motion or muscle atrophy can occur, tenderness is highlighted as the most frequent. Joint effusion and palpable mass are less consistently present, and skin discoloration is not typical.
Question 69
A 16-year-old male presents with chronic knee pain. Radiographs reveal a lytic lesion in the proximal tibial epiphysis. A biopsy is performed. Low magnification histology shows a uniform background of mononuclear cells with occasional multinucleated giant cells. Which of the following is the most likely diagnosis?
View Answer & Explanation
Correct Answer: B
Rationale: Chondroblastoma is characterized histologically by a uniform background of mononuclear cells (chondroblast-like cells) with occasional multinucleated giant cells, as described and shown in the provided image. Giant Cell Tumor would have a much more prominent and diffuse giant cell component. Osteosarcoma would show malignant osteoid formation. Enchondroma and Osteochondroma have distinct cartilaginous matrices and growth patterns.
Question 70
A 16-year-old male undergoes surgical resection of a benign cartilage-producing tumor from the proximal tibial epiphysis. Upon gross examination of the resected specimen, what color and consistency would be most characteristic of this tumor?
View Answer & Explanation
Correct Answer: C
Rationale: Grossly, chondroblastoma is usually grey or pink, with occasional areas of calcification in the tissue, as described in the text and depicted in Fig. 8.43. The other options describe features more typical of other bone tumors (e.g., lipoma, aneurysmal bone cyst, fibrous dysplasia).
Question 71
A 16-year-old female presents with chronic hip pain. Imaging reveals an epiphyseal lytic lesion in the femoral head. Surgical curettage is performed. Gross examination of the specimen shows an area of chondroid-appearing tissue as well as more cystic regions. Which additional component is commonly found in chondroblastomas, contributing to cystic areas?
View Answer & Explanation
Correct Answer: C
Rationale: Chondroblastomas can have components of secondary aneurysmal bone cyst, which explains the presence of cystic regions within the tumor, as described and illustrated in Fig. 8.44. The other options are distinct tumor types or components not typically associated with chondroblastoma in this manner.
Question 72
A 16-year-old male presents with knee pain. Radiographs show a lytic lesion in the proximal tibial epiphysis. While most chondroblastomas are purely lytic, what percentage of cases may demonstrate matrix calcifications on imaging?
View Answer & Explanation
Correct Answer: B
Rationale: Matrix calcifications are present in approximately one-quarter of chondroblastomas, as explicitly stated in the clinical context for Fig. 8.39. This is an important diagnostic clue, though not universally present. The other percentages are incorrect based on the provided text.
Question 73
A 16-year-old presents with chronic shoulder pain. Imaging reveals a lytic lesion in the humeral head epiphysis. Considering the epidemiology of chondroblastoma, what is the typical gender predilection for this tumor?
View Answer & Explanation
Correct Answer: C
Rationale: Chondroblastomas are two times more common in males than in females, as stated in the text. This epidemiological detail can aid in differential diagnosis. The other options are incorrect.
Question 74
A 16-year-old male presents with knee pain. Radiographs show a lytic lesion in the proximal tibia. Which specific anatomical location within the bone is most characteristic for chondroblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: Chondroblastomas usually occur in primary or secondary ossification centers and are localized to the epiphysis or apophysis. This epiphyseal/apophyseal location is a key distinguishing feature from many other bone tumors. The other locations are less typical for chondroblastoma.
Question 75
A 16-year-old male presents with knee pain and a lytic lesion in the proximal tibial epiphysis, consistent with chondroblastoma. Given the typical age of presentation, what is a notable characteristic regarding the tumor's interaction with the growth plate?
View Answer & Explanation
Correct Answer: D
Rationale: Although usually localized to the epiphysis or apophysis, these lesions occasionally cross an open growth plate. This is an important feature to consider in surgical planning and understanding tumor behavior. The other options are incorrect based on the text.
Question 76
A 16-year-old female presents with chronic knee pain, which has been present for several years. Physical examination reveals tenderness over the proximal tibia. In addition to pain and tenderness, what other associated clinical findings might be present in a patient with chondroblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: Patients with chondroblastoma may present with regional muscle atrophy and an antalgic gait, in addition to pain and tenderness. These are common secondary findings due to chronic pain and disuse. The other options describe symptoms not typically associated with chondroblastoma.
Question 77
A 16-year-old male presents with chronic knee pain. Radiographs show a lytic lesion in the proximal tibial epiphysis. Given the patient's age and the epiphyseal location of the lesion, which of the following is the most important differential diagnosis to consider alongside chondroblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: Giant cell tumor (GCT) is a critical differential diagnosis for an epiphyseal lytic lesion, especially in adolescents and young adults, as it can also present in this location and age group, though GCT typically occurs after growth plate closure. Chondroblastoma is the classic epiphyseal tumor in skeletally immature patients. Osteoid osteoma is typically metaphyseal/diaphyseal. Non-ossifying fibroma is metaphyseal. Fibrous dysplasia and enchondroma are less common in the epiphysis and have distinct radiographic features.
Question 78
A 16-year-old female presents with a lytic lesion in the distal femoral epiphysis. Biopsy confirms chondroblastoma, but also notes areas consistent with a secondary aneurysmal bone cyst (ABC). What is the clinical significance of this secondary ABC component?
View Answer & Explanation
Correct Answer: C
Rationale: Chondroblastomas can have components of secondary aneurysmal bone cyst, which is a common benign secondary change that can lead to cystic regions within the tumor. It does not indicate malignancy or necessarily a higher risk of recurrence compared to other chondroblastomas, nor does it alter the fundamental benign nature of the primary tumor. The text describes it as a component, not a sign of malignancy or requiring chemotherapy.
Question 79
A 16-year-old male presents with chronic ankle pain. Imaging reveals a lytic lesion in the talar epiphysis. Biopsy confirms chondroblastoma. Based on its classification, what is the primary tissue type produced by this tumor?
View Answer & Explanation
Correct Answer: C
Rationale: Chondroblastoma is explicitly described as a "benign cartilage-producing tumor." This defines its histogenesis and primary tissue type. The other options are incorrect.
Question 80
A 16-year-old female presents with persistent knee pain. Initial radiographs show a subtle lytic lesion in the proximal tibial epiphysis. To better delineate the extent of the lesion and its relationship to surrounding structures, an MRI is ordered. What would be the expected finding on the sagittal plane MRI?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 8.39 explicitly states that "The lateral radiograph (b) and the MR picture in sagittal plane show a lytic lesion in the proximal tibial epiphysis posteriorly." This directly answers the question. The other options describe features of different bone pathologies (e.g., osteoid osteoma, aneurysmal bone cyst, osteosarcoma).
Question 81
A 16-year-old male presents with knee pain. He reports that the pain has been intermittent but present for approximately two years. Radiographs show an epiphyseal lytic lesion. What is a common characteristic of the duration of symptoms for chondroblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that pain, the most common clinical finding, "may be present for many years before diagnosis." This indicates a chronic, often insidious onset of symptoms. The other options describe different clinical courses.
Question 82
A 16-year-old female presents with chronic wrist pain. Radiographs of the distal radius show a well-defined lesion in the epiphysis. What is the most common radiographic appearance of a chondroblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: The radiographs (Fig. 8.39 a-c) and descriptions consistently refer to chondroblastoma as a "lytic lesion." While some may have matrix calcifications, the primary appearance is lytic. Sclerotic lesions, mixed lesions, and aggressive features like cortical breakthrough or Codman's triangle are characteristic of other bone tumors.
Question 83
A 16-year-old male undergoes biopsy for an epiphyseal lesion in the proximal humerus. Histological examination reveals a uniform background of mononuclear cells. These cells are characteristic of chondroblastoma and are often described as resembling what specific cell type?
View Answer & Explanation
Correct Answer: C
Rationale: Chondroblastoma is a cartilage-producing tumor, and its characteristic mononuclear cells are often described as chondroblast-like. The name itself, "chondroblastoma," refers to these immature cartilage-forming cells. The other cell types are not characteristic of this tumor.
Question 84
A 16-year-old female undergoes surgical resection of a chondroblastoma from the distal femoral epiphysis. During gross examination, the pathologist notes areas of "chondroid-appearing tissue." What does this term primarily suggest about the consistency or appearance of these areas?
View Answer & Explanation
Correct Answer: C
Rationale: "Chondroid-appearing tissue" refers to tissue that resembles cartilage, which is typically rubbery, firm, or gelatinous in consistency. Since chondroblastoma is a cartilage-producing tumor, this gross appearance is expected. The other options describe different tissue types or states.
Question 85
A 16-year-old male presents with chronic knee pain. He underwent knee arthroscopy by an outside surgeon prior to referral to an orthopedic oncologist. Imaging now reveals a lytic lesion in the proximal tibial epiphysis. What is the most likely reason for the initial arthroscopy in this case?
View Answer & Explanation
Correct Answer: B
Rationale: The vignette states the patient underwent knee arthroscopy "prior to referral." This implies that the initial presentation of chronic knee pain was likely attributed to a common intra-articular issue (e.g., meniscal tear, ligament injury, chondral defect) before the underlying bone tumor was identified or suspected. Arthroscopy is typically not the primary approach for diagnosing or treating an epiphyseal bone tumor unless it has an intra-articular component or is misdiagnosed. The text implies a delay in diagnosis, suggesting initial misdirection. While a meniscal tear (D) could be found, the primary reason for arthroscopy in the context of undiagnosed chronic knee pain is to rule out intra-articular pathology.
Question 86
A 16-year-old female is diagnosed with a chondroblastoma in the distal femoral epiphysis. The tumor is confirmed to be benign. What is the generally accepted primary surgical management principle for a symptomatic chondroblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: As a benign tumor, the standard surgical treatment for symptomatic chondroblastoma is intralesional curettage, often augmented with local adjuvants (e.g., cryotherapy, phenol) and bone grafting to fill the defect and reduce recurrence risk. Wide en bloc resection (A) is typically reserved for malignant tumors or aggressive benign tumors with significant cortical destruction. Amputation (B) and chemotherapy/radiation (D) are for malignant conditions. Long-term observation (E) is usually for asymptomatic, quiescent lesions or non-ossifying fibromas, not typically for symptomatic chondroblastomas.
Question 87
A 16-year-old male presents with knee pain. Radiographs show a lytic lesion in the proximal tibial epiphysis with subtle areas of matrix calcification. Considering this imaging finding, which other diagnosis might also present with epiphyseal involvement and calcifications, making it a key differential?
View Answer & Explanation
Correct Answer: D
Rationale: Clear cell chondrosarcoma is a rare low-grade malignant cartilage tumor that can occur in the epiphysis of long bones, particularly in young adults, and often contains calcifications. This makes it a critical differential for chondroblastoma, especially when calcifications are present. Osteosarcoma (A) is typically metaphyseal and shows osteoid matrix. Chondrosarcoma (B) is usually in older adults and often metaphyseal/diaphyseal. Enchondroma (C) is typically metaphyseal/diaphyseal. Fibrous cortical defect (E) is metaphyseal and lacks calcifications.
Question 88
A 30-year-old woman presents with a slowly enlarging, firm mass in her right thigh. Physical examination reveals a non-tender, immobile mass deep to the fascia. MRI shows a large, infiltrative lesion within the quadriceps muscle. Biopsy reveals a clonal fibroblastic proliferation arising from musculoaponeurotic structures.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of a deep, infiltrative mass combined with the histological finding of a clonal fibroblastic proliferation arising from musculoaponeurotic structures is characteristic of extra-abdominal aggressive fibromatosis (desmoid tumor). This entity is defined by these specific cellular origins and growth patterns. Main Distractor: Liposarcoma (A) is a malignant tumor of adipocytic origin, which would have different histological features and typically presents with metastatic potential, unlike fibromatosis.
Question 89
A 25-year-old female presents with a new, firm mass in her left shoulder girdle. She reports no specific trauma. Her medical history is otherwise unremarkable.
View Answer & Explanation
Correct Answer: B
Rationale: The text states that extra-abdominal aggressive fibromatosis has a peak age of occurrence between puberty and 40 years and is more prevalent in women. The patient's age and gender align perfectly with these demographic characteristics. Main Distractor: Option A presents an incorrect age range and gender prevalence for this condition.
Question 90
A 35-year-old woman develops a firm, palpable mass in her abdominal wall 6 months after an uncomplicated vaginal delivery. She reports no other symptoms. Imaging confirms a deep soft tissue mass.
View Answer & Explanation
Correct Answer: C
Rationale: The provided text explicitly lists "rapid abdominal wall contraction after delivery" as a predisposing factor for extra-abdominal aggressive fibromatosis. This patient's history directly matches this factor. Main Distractor: While radiation exposure (B) can be a risk factor for some soft tissue tumors, it is not listed as a predisposing factor for fibromatosis in the provided text.
Question 91
A 28-year-old male presents with a gradually enlarging, firm mass in his right forearm. Physical examination reveals a deep-seated, non-mobile lesion. MRI confirms a soft tissue mass involving the flexor compartment.
View Answer & Explanation
Correct Answer: C
Rationale: The text states that extra-abdominal aggressive fibromatosis is observed most frequently in the shoulder girdle, chest wall, upper arm, thigh, pelvis, and forearm. Among the given options, the shoulder girdle is explicitly mentioned as a frequent location. Main Distractor: The foot sole (A) is typically associated with plantar fibromatosis, which is a superficial counterpart, not the deep extra-abdominal aggressive fibromatosis described in the case.
Question 92
A 32-year-old patient undergoes biopsy of a recurrent mass in the popliteal fossa. Histopathological examination is performed.
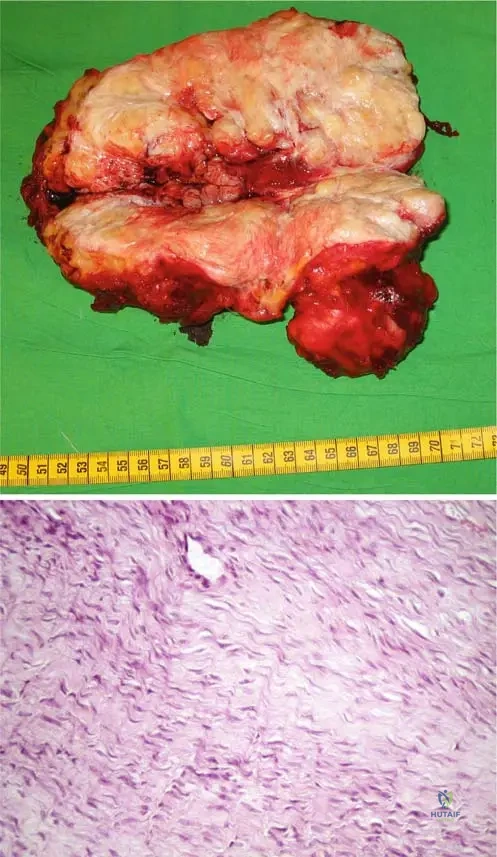
View Answer & Explanation
Correct Answer: D
Rationale: The description for Fig. 9.13b explicitly states that the characteristic histological picture of fibromatosis includes "ill-defined woven fascicles composed of spindle-shaped fibroblasts and abundant collagen fibers," and critically, "No atypical mitosis is present." Therefore, atypical mitosis would be the least expected feature. Main Distractor: Ill-defined woven fascicles (A) are a characteristic feature of fibromatosis, as described in the text.
Question 93
A 38-year-old male presents with progressive enlargement of his right leg and difficulty with knee flexion. MRI is performed.
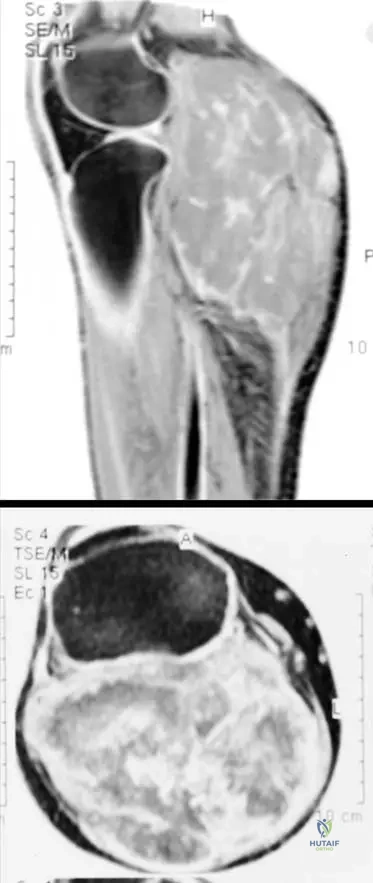
View Answer & Explanation
Correct Answer: B
Rationale: The description for Fig. 9.11 a, b directly states that the sagittal and axial MRI pictures present "the enormous tumor that affects the whole popliteal region and the flexor muscles of the leg. It is attached to the dorsal part of the joint capsule and reaches the subcutis." This accurately describes the typical MRI appearance. Main Distractor: Extra-abdominal fibromatosis is typically infiltrative and locally aggressive, not well-circumscribed and encapsulated (A).
Question 94
A 40-year-old patient presents with a significant enlargement of his right leg, noting a scar from a previous surgical operation in the same area.

View Answer & Explanation
Correct Answer: C
Rationale: The term "recidive" in the description for Fig. 9.10 means recurrent. This directly indicates that extra-abdominal fibromatosis has a significant tendency for local recurrence, which is a hallmark of its aggressive behavior. Main Distractor: Extra-abdominal fibromatosis is locally aggressive but does not have metastatic potential (B), distinguishing it from true sarcomas.
Question 95
A 30-year-old female presents with contractures in her left hip and knee joint. Imaging reveals multiple lesions.
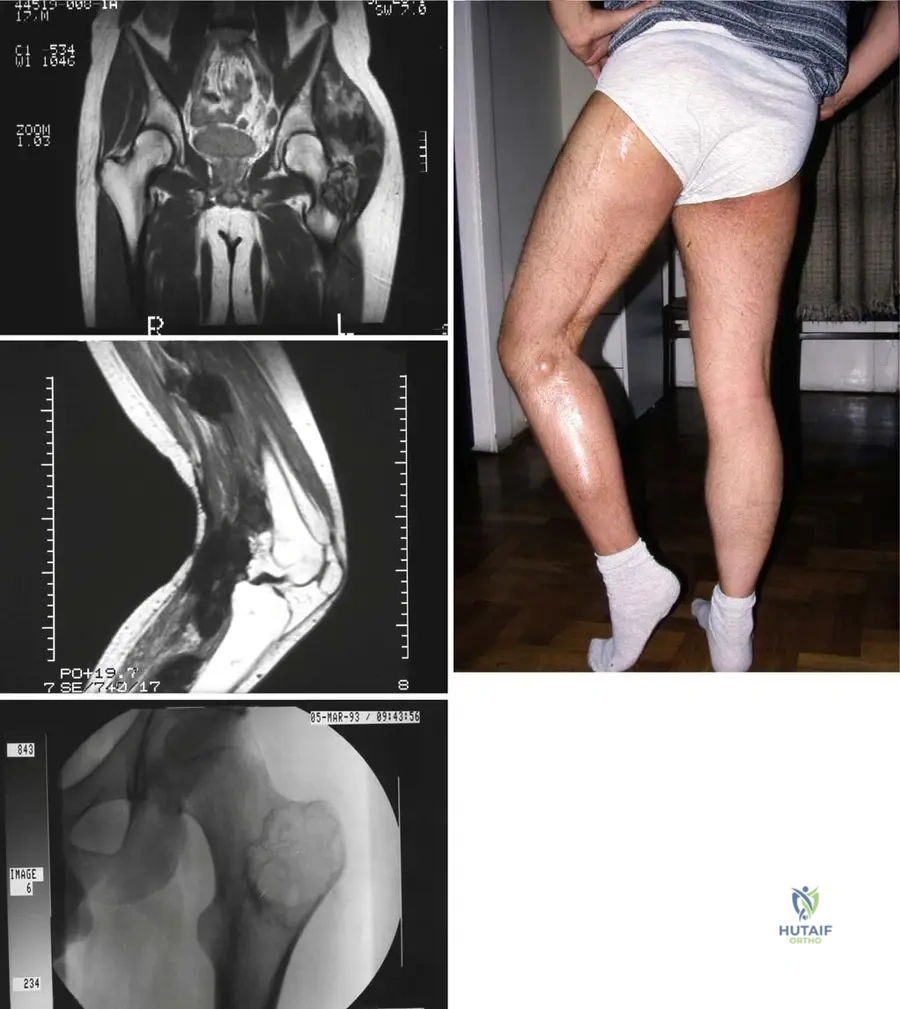
View Answer & Explanation
Correct Answer: C
Rationale: The description for Fig. 9.12 a–d explicitly states
Question 95
A 35-year-old female presents with a slowly enlarging mass in her right thigh. Biopsy reveals a spindle cell proliferation. Histological examination shows ill-defined woven fascicles composed of spindle-shaped fibroblasts and abundant collagen fibers. Which of the following is a characteristic histological feature of extra-abdominal aggressive fibromatosis?
View Answer & Explanation
Correct Answer: C
Rationale: The provided text and Fig. 9.13b explicitly state that the characteristic histological picture of fibromatosis includes "ill-defined woven fascicles composed of spindle-shaped fibroblasts and abundant collagen fibers. No atypical mitosis is present." This distinguishes it from malignant sarcomas. High mitotic activity with atypical forms (A) would suggest malignancy
You Might Also Like
