Full Question & Answer Text (for Search Engines)
Question 1:
The primary restraint to anterior translation of the abducted and externally rotated glenohumeral joint is the:
Options:
- Coracohumeral ligament
- Superior glenohumeral ligament
- Middle glenohumeral ligament
- Inferior glenohumeral ligament
- Subscapularis muscle
Correct Answer: Inferior glenohumeral ligament
Explanation:
The inferior glenohumeral ligament is the primary restraint to anterior translation of the abducted and externally rotated glenohumeral joint. The Bankart lesion is an avulsion of the inferior glenohumeral ligament and represents the primary pathoanatomy of traumatic anterior shoulder dislocation.
Question 2:
The quadriceps angle or Q angle is defined as the angle formed by a line connecting the:
Options:
- Anterior inferior iliac spine to the center of the patella and a line connecting the center of the patella to the center of the tibial tuberosity
- Anterior superior iliac spine to the center of the patella and a line connecting the center of the patella to the center of the tibial tuberosity
- Anterior inferior iliac spine to the lateral aspect of the patella and a line connecting the center of the patella to the center of the tibial tuberosity
- Anterior superior iliac spine to the center of the patella and a line connecting the center of the patella to the center of the ankle
- Anterior inferior iliac spine to the center of the patella and a line connecting the center of the patella to the center of the ankle
Correct Answer: Anterior superior iliac spine to the center of the patella and a line connecting the center of the patella to the center of the tibial tuberosity
Explanation:
The quadriceps angle, or Q angle, is used to evaluate patellofemoral alignment. It is defined as the angle formed by a line connecting the anterior superior iliac spine to the center of the patella and a line connecting the center of the patella to the center of the tibial tuberosity. A normal angle is up to 10° in men and up to 15° in women. Unfortunately, no standard technique exists for measuring the Q angle, and its reliability and usefulness have recently come under question.
Question 3:
Innervation to the anterior cruciate ligament is provided by a branch of the:
Options:
- Sciatic nerve
- Obturator nerve
- Saphenous nerve
- Posterior tibial nerve
- Femoral nerve
Correct Answer: Posterior tibial nerve
Explanation:
The posterior articular branch of the posterior tibial nerve provides pain fibers and mechanoreceptors to the anterior cruciate ligament.
Question 4:
All of the following represent mechanisms of injury to the posterior cruciate ligament except:
Options:
- Posteriorly directed force on the anterior aspect of the flexed knee
- Fall onto a flexed knee
- Valgus force applied to a flexed and externally rotated knee
- Hyperflexion
- Hyperextension
Correct Answer: Valgus force applied to a flexed and externally rotated knee
Explanation:
All of the above except application of valgus force to a flexed and externally rotated knee have been described in posterior cruciate ligament injuries. Application of a valgus force to a flexed and externally rotated knee would more likely result in an anterior cruciate ligament injury.
Question 5:
Which of the following sets of compartment measurements confirms the diagnosis of exertional compartment syndrome:
Options:
- Preexercise >10 mm Hg, 1-minute postexercise >20 mm Hg, 5-minute postexercise >15 mm Hg
- Preexercise >15 mm Hg, 1-minute postexercise >30 mm Hg, 5-minute postexercise >20 mm Hg
- Preexercise >20 mm Hg, 1-minute postexercise >20 mm Hg, 5-minute postexercise >20 mm Hg
- Preexercise >10 mm Hg, 1-minute postexercise >30 mm Hg, 5-minute postexercise >10 mm Hg
- Preexercise >15 mm Hg, 1-minute postexercise >30 mm Hg, 5-minute postexercise >10 mm Hg
Correct Answer: Preexercise >10 mm Hg, 1-minute postexercise >20 mm Hg, 5-minute postexercise >15 mm Hg
Explanation:
If pressures at preexercise are >15 mm Hg, 1-minute postexercise >30 mm Hg, 5-minute postexercise >20 mm Hg, it will confirm a diagnosis of exertional compartment syndrome. Exertional compartment syndrome is becoming increasingly recognized as a source of pain in runners and cyclists. The onset of pain is gradual during exercise and ultimately restricts performance. Activity modification usually is effective. Refractory cases may require fasciotomy.
Question 6:
The most common adverse side effect of dietary supplementation with creatine in athletes is:
Options:
- Friable tendons
- Muscle cramping
- Myopathy
- Diabetes
- Osteoporosis
Correct Answer: Muscle cramping
Explanation:
Creatine has recently become a popular dietary supplement among athletes. The long-term effects of creatine are not known. However, it appears to cause muscle cramping and heat intolerance.
Question 7:
When testing an elbow for insufficiency of the medial collateral ligament, valgus stress should be applied with the elbow positioned at:
Options:
- Full extension
- 30° of flexion
- 45° of flexion
- 60° of flexion
- 90° of flexion
Correct Answer: 30° of flexion
Explanation:
When testing the medial collateral ligament of the elbow, it is important to apply valgus stress with the elbow flexed approximately 20° to 30° to disengage the olecranon from the olecranon fossa. It is always important to examine and compare the injured and uninjured side.
Question 8:
Internal impingement of the shoulder between the posterosuperior glenoid rim and the rotator cuff typically occurs with the arm in this position:
Options:
- Abduction and internal rotation
- Adduction and external rotation
- Adduction and internal rotation
- Abduction, external rotation, and extension
- Abduction, external rotation, and flexion
Correct Answer: Abduction, external rotation, and extension
Explanation:
Internal impingement of the shoulder occurs with the arm in the abducted, externally rotated, and extended position. This entity may be responsible for shoulder pain commonly occurring in overhead and throwing athletes. Initial treatment is focused on therapy that strengthens the anterior structures and scapular retractors and stretches the posterior structures. If nonoperative treatment fails, arthroscopic debridement, thermal capsular shrinkage, and humeral derotational osteotomy have all been used with varying degrees of success.
Question 9:
The following structure is most responsible for anterior stability of the glenohumeral joint with the arm in 45° of abduction:
Options:
- Inferior glenohumeral ligament
- Middle glenohumeral ligament
- Superior glenohumeral ligament
- Coracohumeral ligament
- Subscapularis muscle and tendon
Correct Answer: Middle glenohumeral ligament
Explanation:
The middle glenohumeral ligament, although absent in up to one third of shoulders, is the largest contributor to anterior stability of the shoulder with the arm abducted 45°. The inferior glenohumeral ligament is the primary restraint to anterior instability with the arm abducted to 90° and externally rotated.
Question 10:
The following structure is most responsible for resisting inferior translation of the glenohumeral joint with the arm at the side:
Options:
- Inferior glenohumeral ligament
- Middle glenohumeral ligament
- C oracoacromial ligament
- Coracohumeral ligament
- Subscapularis muscle and tendon
Correct Answer: Coracohumeral ligament
Explanation:
The coracohumeral ligament coupled with the superior glenohumeral ligament provides the primary restraint to inferior translation of the glenohumeral joint with the arm at the side. The coracohumeral ligament also provides restraint to external rotation with the arm at the side.
Question 11:
Maximal external rotation of the shoulder occurs during which phase of pitching:
Options:
- Wind-up
- Early cocking
- Late cocking
- Deceleration
- Follow through
Correct Answer: Late cocking
Explanation:
The pitching motion can be divided into 6 phases: wind-up, early cocking, late cocking, acceleration, deceleration, and follow through. Maximal external rotation at the shoulder occurs during late cocking.
Question 12:
A 35-year-old avid rock climber complains of persistent anterior elbow pain with climbing, particularly when pulling himself up with his arms. The following muscle would most likely show increased activity on an electromyogram:
Options:
- Long head of the biceps brachii
- Short head of the biceps brachii
- Brachialis
- Flexor carpi radialis
- Flexor carpi ulnaris
Correct Answer: Brachialis
Explanation:
Brachialis tendonitis, or climberâ s elbow, causes pain in the anterior elbow with the forearm in the pronated and flexed position. An electromyogram typically shows increased activity in the brachialis muscle.
Question 13:
A 16-year-old baseball pitcher complains of dominant-sided elbow pain when pitching. He has recently been removed from the pitching rotation because of "control" problems. Physical examination reveals pain when a supinated, flexed, and valgus stressed elbow is brought into progressive extension. The most likely diagnosis is:
Options:
- Posterolateral rotatory instability
- Ulnar collateral ligament tear
- Ulnar nerve entrapment
- Posteromedial impingement
- Radial nerve entrapment
Correct Answer: Posteromedial impingement
Explanation:
The process described is posteromedial impingement syndrome of the elbow. It typically presents as vague elbow pain with loss of control in pitchers. The valgus extension overload test typically elicits pain and sometimes crepitus. The pathological changes in posteromedial impingement syndrome start with chondromalacia on the medial aspect of the trochlear groove and may progress to osteophyte formation and loose bodies necessitating arthroscopic debridement.
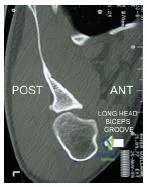
Question 14:
This slide is a computed tomogram of the shoulder of a 22-year-old rugby player. The most likely diagnosis is:
Options:
- Anterior shoulder instability
- Posterior shoulder instability
- Glenohumeral arthritis
- Supraspinatus tear
- Subscapularis tear
Correct Answer: Posterior shoulder instability
Explanation:
The computed tomogram shows a posterior avulsion of the glenoid rim and an impaction fracture of the anterior aspect of the humeral head consisted with a prior posterior dislocation.
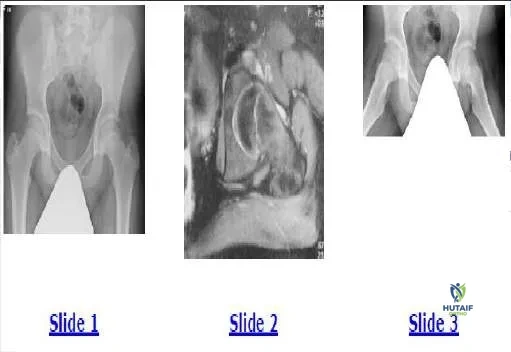
Question 15:
This slide is a computed tomogram of the dominant shoulder of a 45-year- old male tennis player. The most likely diagnosis is:
Options:
- Osteosarcoma
- Synovial osteochondromatosis
- Anterior glenoid fracture
- Synovial cell sarcoma
- Rotator cuff tear arthropathy
Correct Answer: Synovial osteochondromatosis
Explanation:
Synovial osteochondromatosis is a rare condition typically affecting middle- aged men. The computed tomogram demonstrates the osteocartilaginous nodules. Early in the disease, arthroscopic removal of loose bodies and synovectomy usually results in an acceptable outcome. In cases of progressive disease resulting in secondary shoulder arthrosis, shoulder arthroplasty may be required.
Question 16:
Weight training that employs constant resistance throughout the arc of motion is referred to as:
Options:
- Isometric
- Isotonic
- Isokinetic
- Plyometric
- Functional
Correct Answer: Isotonic
Explanation:
Isotonic training employs a constant resistance throughout the arc of joint motion
Question 17:
Weight training that employs a constant velocity and variable resistance is referred to as:
Options:
- Isometric
- Isotonic
- Isokinetic
- Plyometric
- Functional
Correct Answer: Isokinetic
Explanation:
Isokinetic training employs constant velocity and variable resistance. Special equipment, such as a C ybex device (C ybex, Medway, Mass), is required for isokinetic training.
Question 18:
During arthroscopic repair of a medial meniscal tear, the following structure is at greatest risk for damage:
Options:
- Popliteal artery
- Popliteal vein
- Saphenous nerve
- Sural nerve
- Popliteus tendon
Correct Answer: Saphenous nerve
Explanation:
No matter what technique for arthroscopic medial meniscal repair is used, the saphenous nerve must be protected to avoid a painful neuroma postoperatively.
Question 19:
During arthroscopic repair of a lateral meniscal tear, the following structure is at greatest risk for damage:
Options:
- Popliteal artery
- Popliteal vein
- Peroneal nerve
- Sural nerve
- Popliteus tendon
Correct Answer: Peroneal nerve
Explanation:
When performing arthroscopic lateral meniscal repair, the peroneal nerve must be protected from insult.
Question 20:
A 15-year-old male football player is discovered to have a reproducible painless pop with meniscal testing during a routine preparticipation physical examination. The patient states that he has never experienced any knee problems other than an occasional audible pop. His family physician orders a magnetic resonance image. It shows a discoid lateral meniscus without evidence of tearing. Recommended management should include:
Options:
- No intervention
- Abstinence from participation in football only
- Abstinence from participation in any sport requiring pivoting or
- Excision of the central portion of the discoid meniscus
- Lateral meniscectomy
Correct Answer: No intervention
Explanation:
A discoid lateral meniscus can be complete, incomplete, or a Wrisberg variant. If asymptomatic, the patient can simply be observed without restriction. In patients with symptoms, the preferred treatment is excision of the central portion of the meniscus. In individuals with a discoid meniscus and a peripheral tear, repair of the tear is performed with excision of the central portion of the meniscus.